Embed Size (px)
Citation preview
BEHANDLUNG DER SEKUNDÄREN EISENÜBERLADUNG NACH HÄMATOPOETISCHER STAMMZELLTRANSPLANTATION
PD Dr. med. Ansgar Schulz und Prof. Dr. med. Holger Cario Klinik für Kinder- und Jugendmedizin, Universitätsklinikum Ulm Dr. Andrea Jarisch Zentrum für Kinder- und Jugendmedizin Pädiatrische Hämatologie und Onkologie, Universitätsklinikum Frankfurt am Main
Schulz, Hämatologie heute, Folie 1
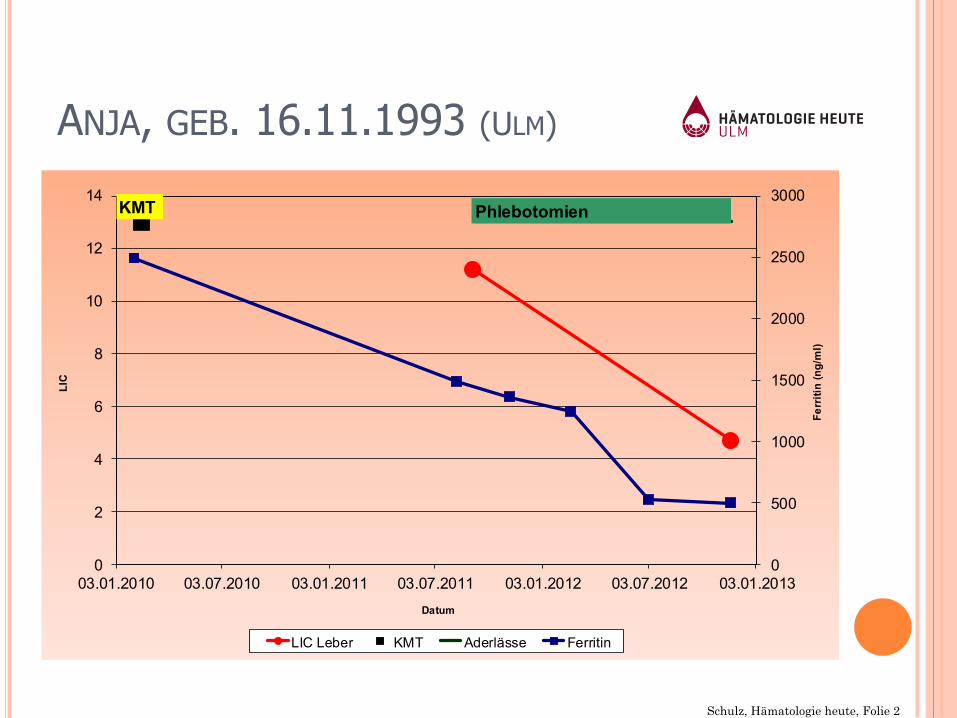
ANJA, GEB. 16.11.1993 (ULM)
¢ AML M1 (ED: 07.10.2007) ¢ Frühes Knochenmarkrezidiv (Ende der Dauertherapie 04/2009) ¢ systemische Pilzinfektion in Aplasie, Z.n. Sepsis ohne
Erregernachweis in Aplasie ¢ Allogene Stammzelltransplantation mit Knochenmark vom HLA-
kompatiblen Fremdspender am 16.02.2010 in CR 2 ¢ GvHD I° (Haut 1°) EBV Infektion, Therapie mit Rituximab ¢ Sekundäre Kardiomyopathie, ztw. Therapie mit Enalapril ¢ Eisenüberladung der Leber (200 mmol/kg dry tissue)
0
500
1000
1500
2000
2500
3000
0
2
4
6
8
10
12
14
03.01.2010 03.07.2010 03.01.2011 03.07.2011 03.01.2012 03.07.2012 03.01.2013
Ferr
itin
(ng/
ml)
LIC
Datum
LIC Leber KMT Aderlässe Ferritin
KMT Phlebotomien
Schulz, Hämatologie heute, Folie 2
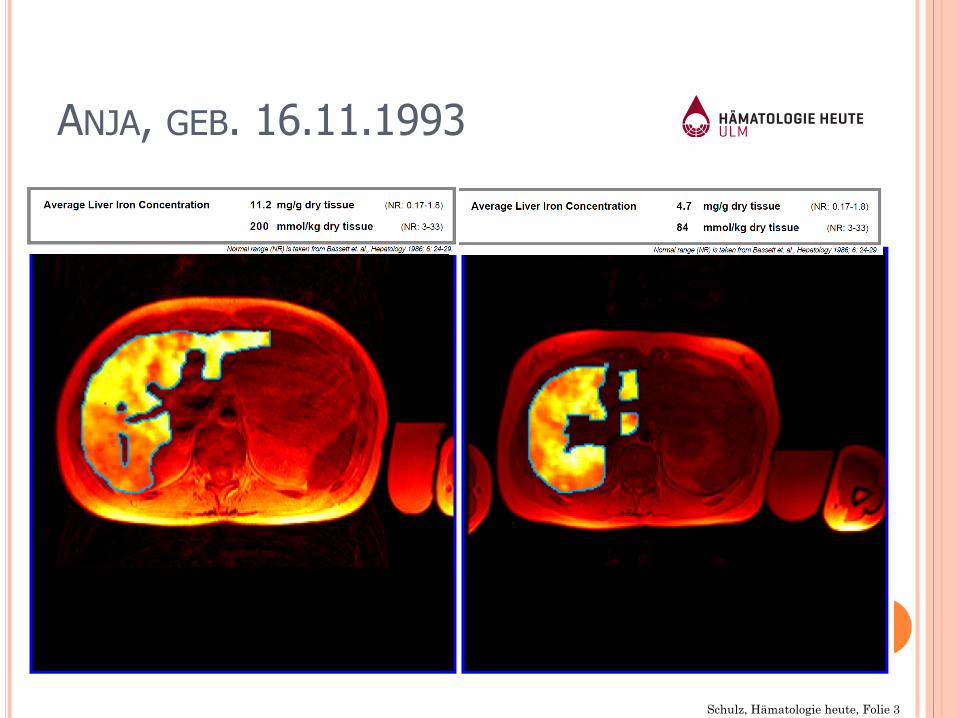
ANJA, GEB. 16.11.1993
Schulz, Hämatologie heute, Folie 3

Schulz, Hämatologie heute, Folie 4
http://www.fcbayern-frauenfussball.de/news/Nahaufnahme%3A+Anja+Pfluger,18315.htm
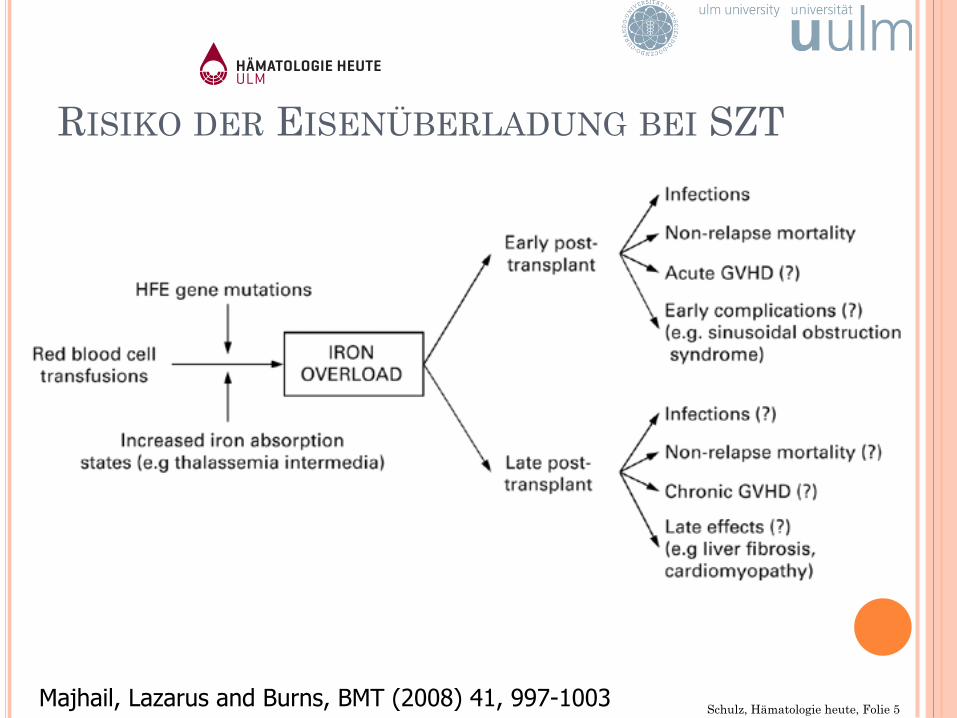
RISIKO DER EISENÜBERLADUNG BEI SZT
Schulz, Hämatologie heute, Folie 5 Majhail, Lazarus and Burns, BMT (2008) 41, 997-1003
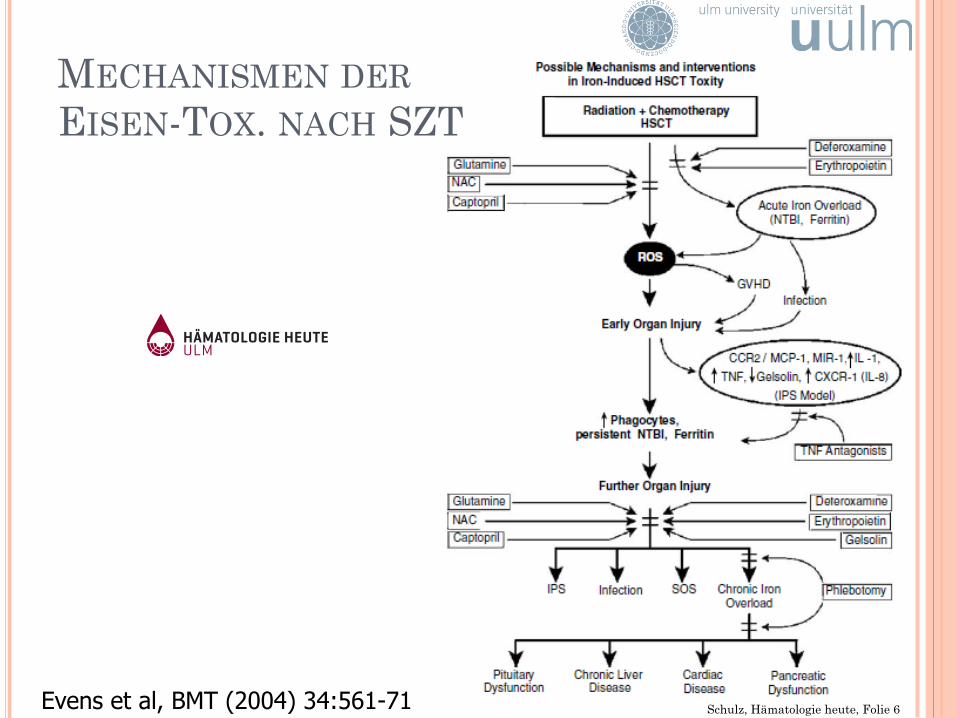
MECHANISMEN DER EISEN-TOX. NACH SZT
Evens et al, BMT (2004) 34:561-71 Schulz, Hämatologie heute, Folie 6
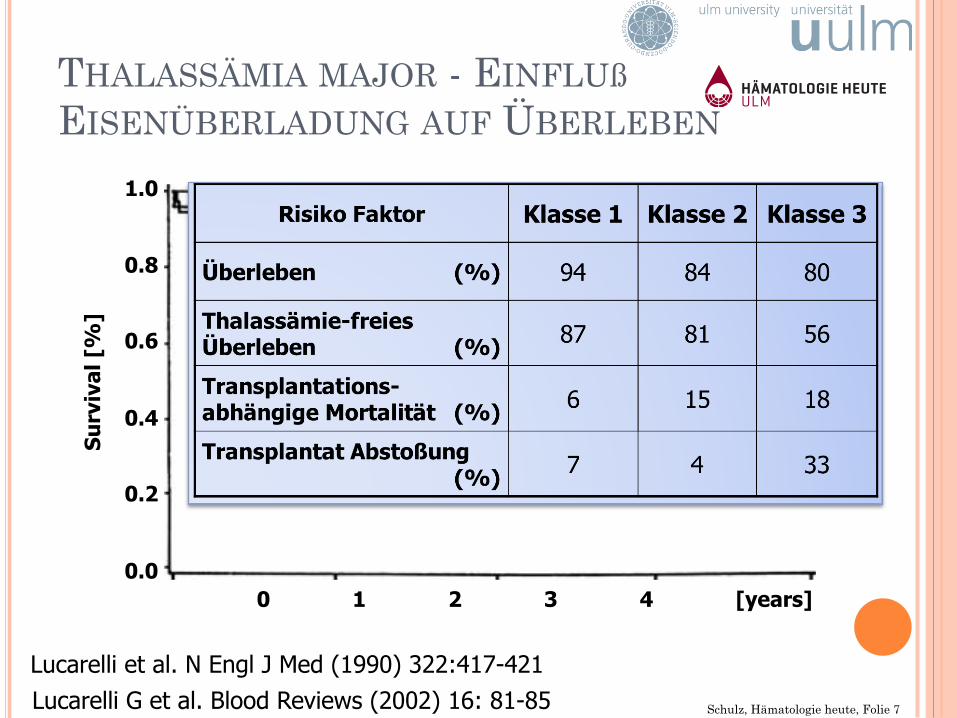
THALASSÄMIA MAJOR - EINFLUß EISENÜBERLADUNG AUF ÜBERLEBEN
No hepatomegaly, no portal fibrosis (n=39)
hepatomegaly or portal fibrosis (n=36)
Hepatomegaly and portal fibrosis (n=24)
0 1 2 3 4 [years]
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
[%
]
Lucarelli et al. N Engl J Med (1990) 322:417-421 Lucarelli G et al. Blood Reviews (2002) 16: 81-85 Schulz, Hämatologie heute, Folie 7
DIAGNOSTIK UND RISIKOABSCHÄTZUNG
Schulz, Hämatologie heute, Folie 8
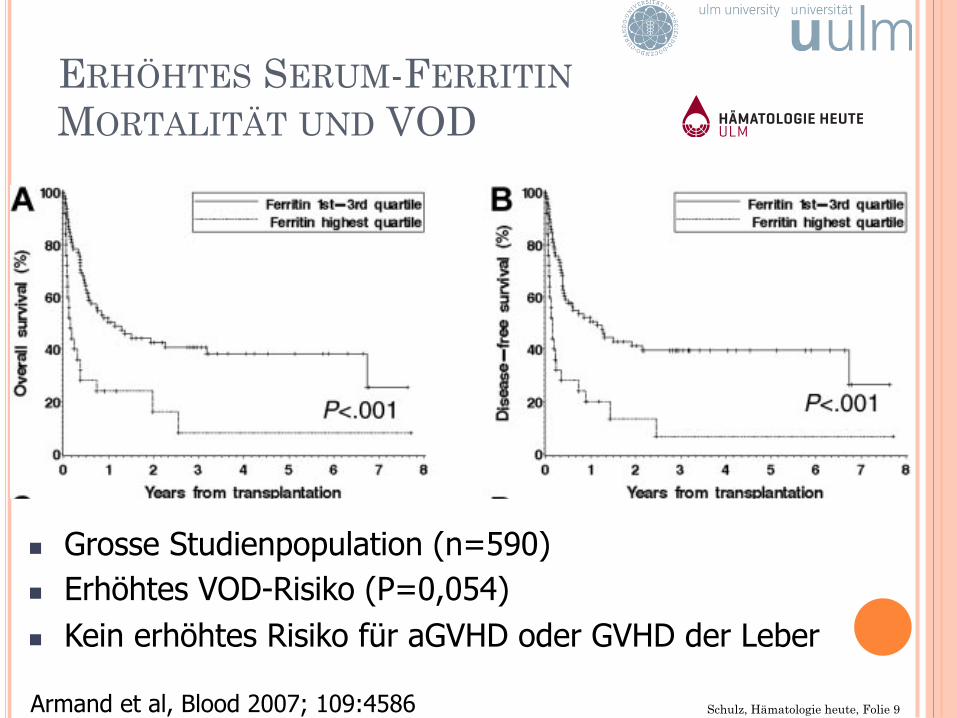
ERHÖHTES SERUM-FERRITIN MORTALITÄT UND VOD
n Grosse Studienpopulation (n=590) n Erhöhtes VOD-Risiko (P=0,054) n Kein erhöhtes Risiko für aGVHD oder GVHD der Leber
Armand et al, Blood 2007; 109:4586 Schulz, Hämatologie heute, Folie 9
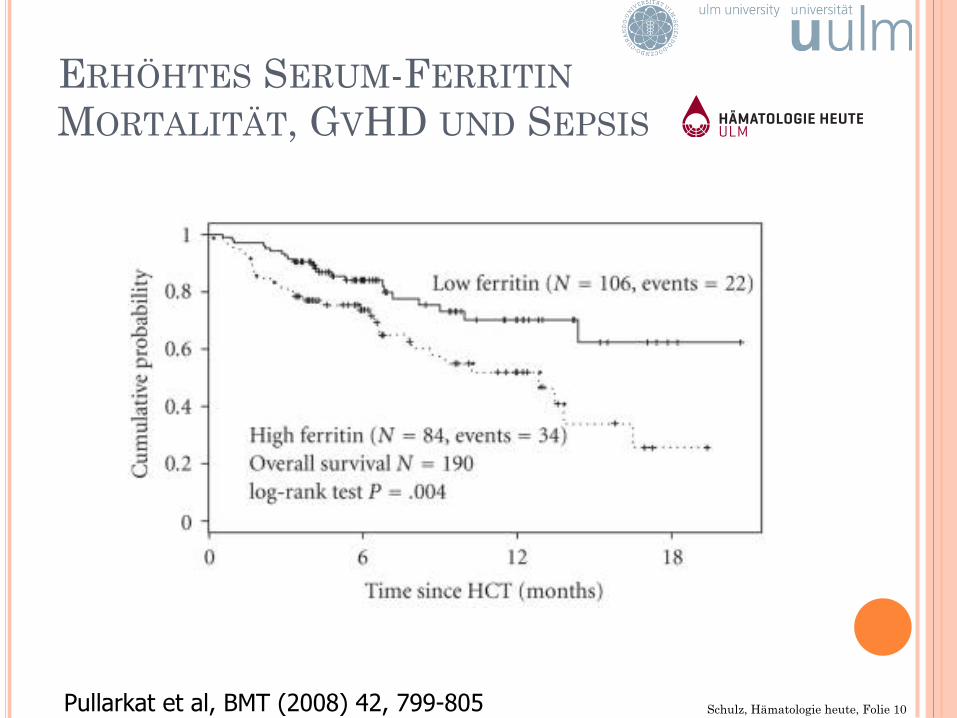
¢ Iron overload adversely affects outcome of
allogeneic hematopoietic cell transplantation:
¢ Erhöhte aGVHD-Rate
¢ Erhöhte Mortalität d100
¢ Reduziertes Overall Survival
¢ Erhöhte Rate an Sepsen
Pullarkat et al, BMT (2008) 42, 799-805 Schulz, Hämatologie heute, Folie 10
ERHÖHTES SERUM-FERRITIN MORTALITÄT, GVHD UND SEPSIS
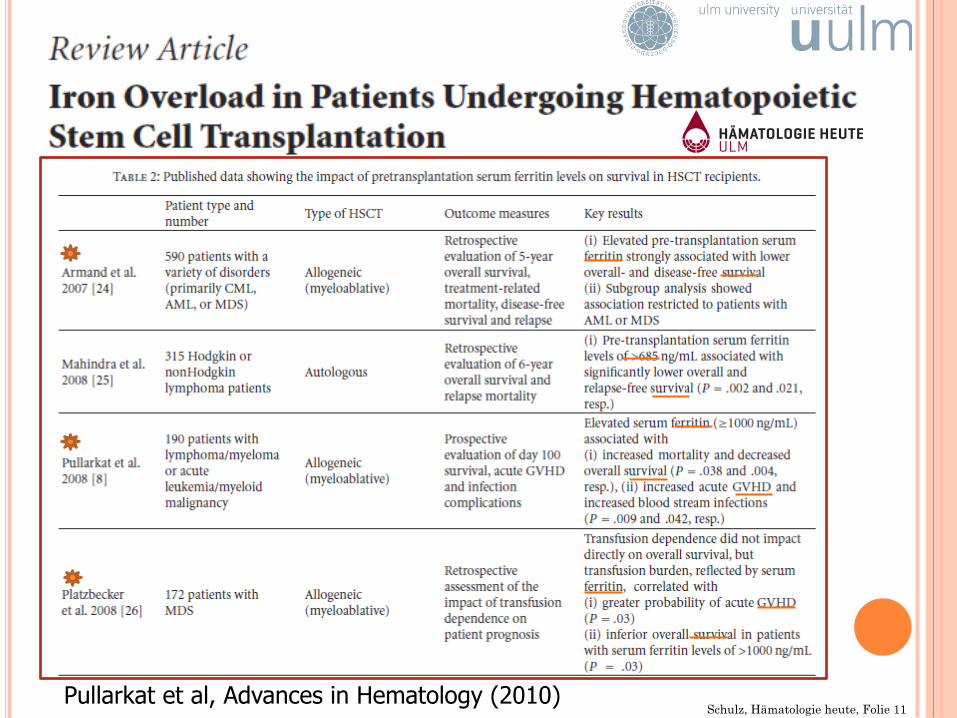
Pullarkat et al, Advances in Hematology (2010) Schulz, Hämatologie heute, Folie 11
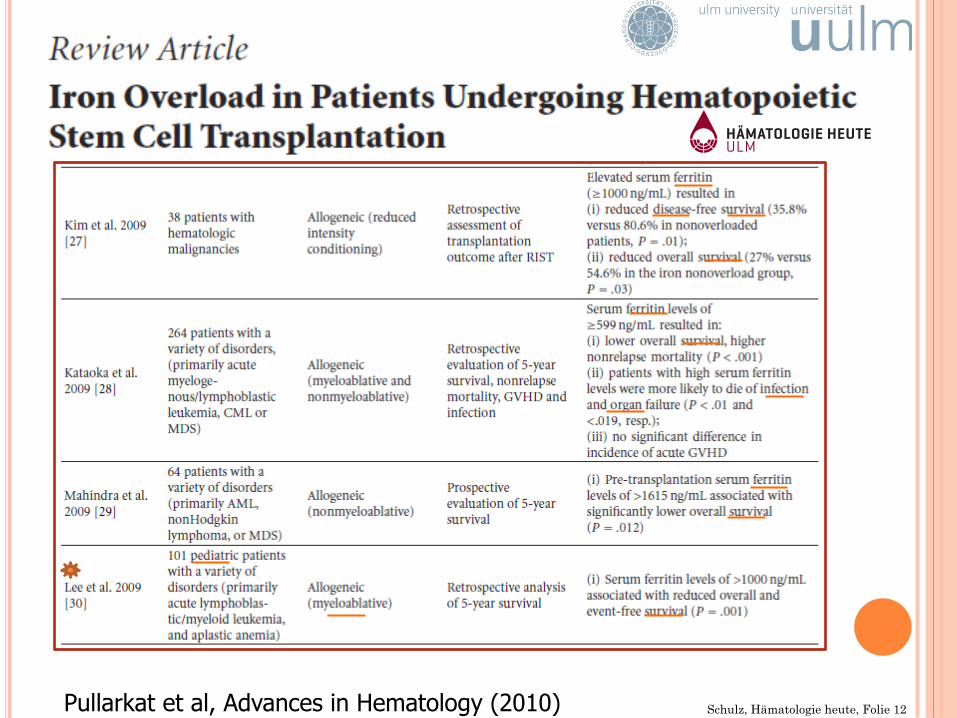
Pullarkat et al, Advances in Hematology (2010) Schulz, Hämatologie heute, Folie 12
Schulz, Hämatologie heute, Folie 13 Wermke et al, Clin Cancer Res (2012) 18:6460-6468
PROSPEKTIVE STUDIE: LEBEREISEN UND FERRITIN
n Prospektive Studie (n=88, MDS und AML, Erwachsene)
n Leber-MRI vor SZT (Liver Iron Content) n Hohes Ferritin und Transfusionsmenge keine
prognostische Relevanz n Aber: Eisenüberladung (LIC) assoziiert mit
erhöhter nicht Rezidiv assoziierter Mortalität
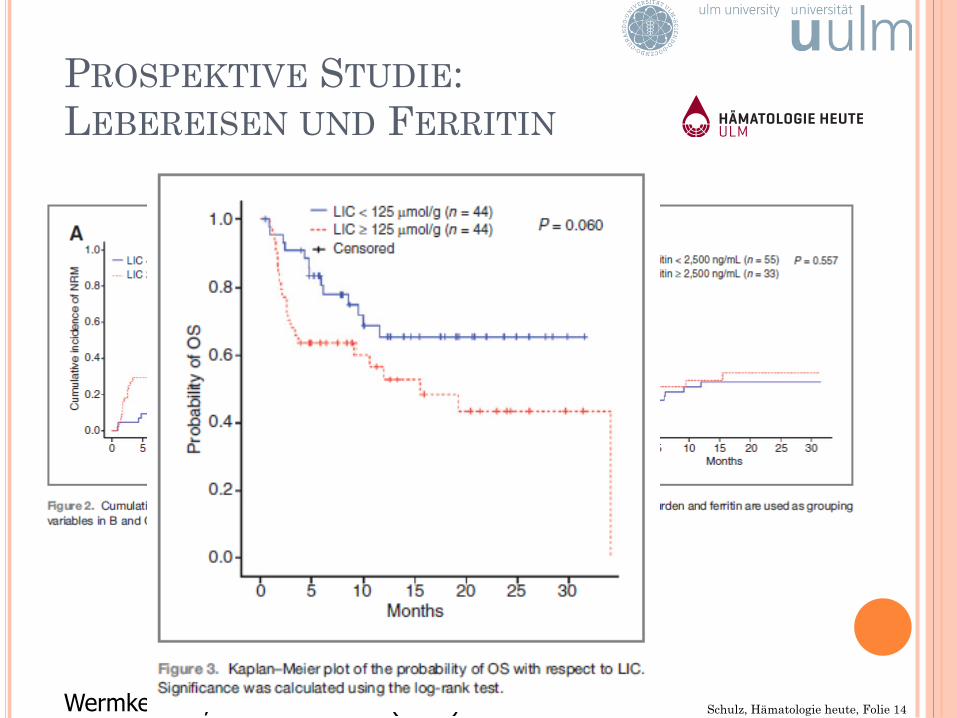
Schulz, Hämatologie heute, Folie 14 Wermke et al, Clin Cancer Res (2012) 18:6460-6468
PROSPEKTIVE STUDIE: LEBEREISEN UND FERRITIN
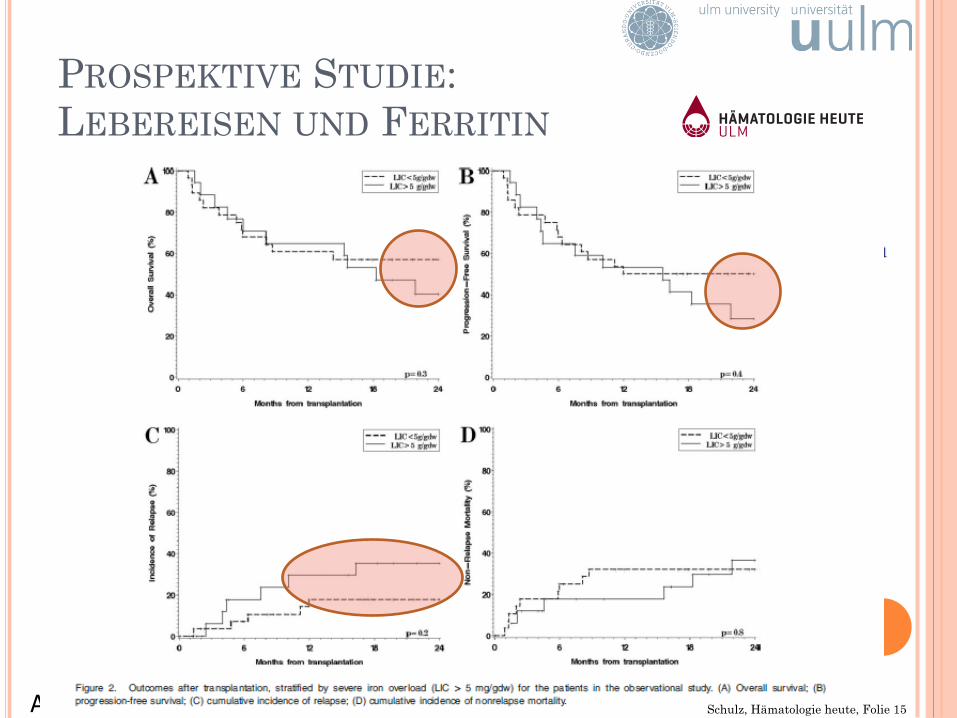
PROSPEKTIVE STUDIE: LEBEREISEN UND FERRITIN
Armand et al, 2012; Am. J. Hematol. 87:569-572 Schulz, Hämatologie heute, Folie 15
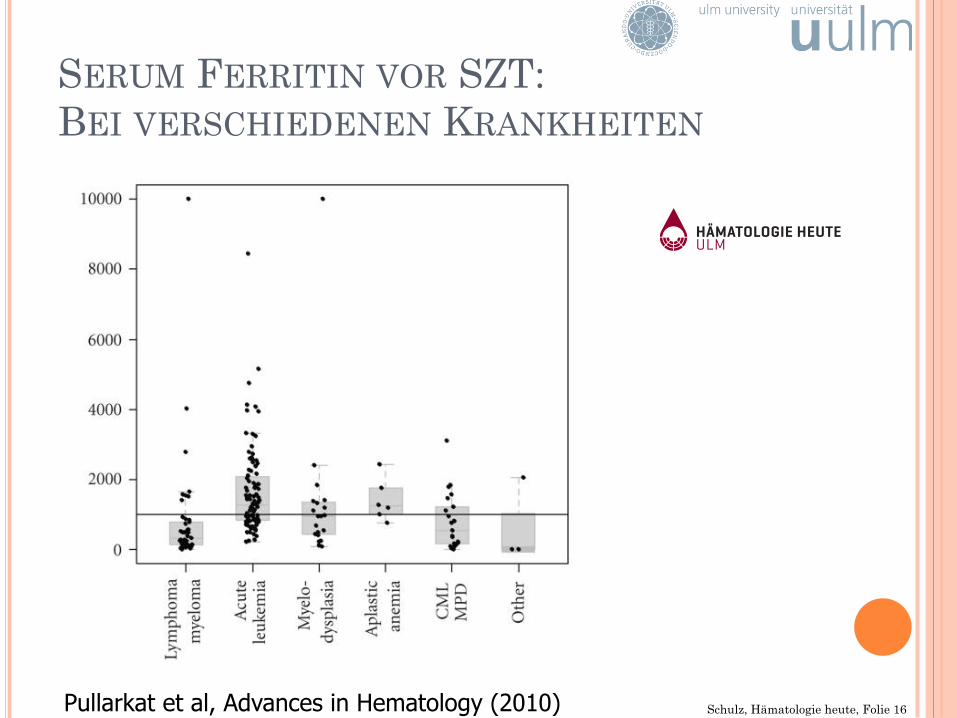
SERUM FERRITIN VOR SZT: BEI VERSCHIEDENEN KRANKHEITEN
Pullarkat et al, Advances in Hematology (2010) Schulz, Hämatologie heute, Folie 16
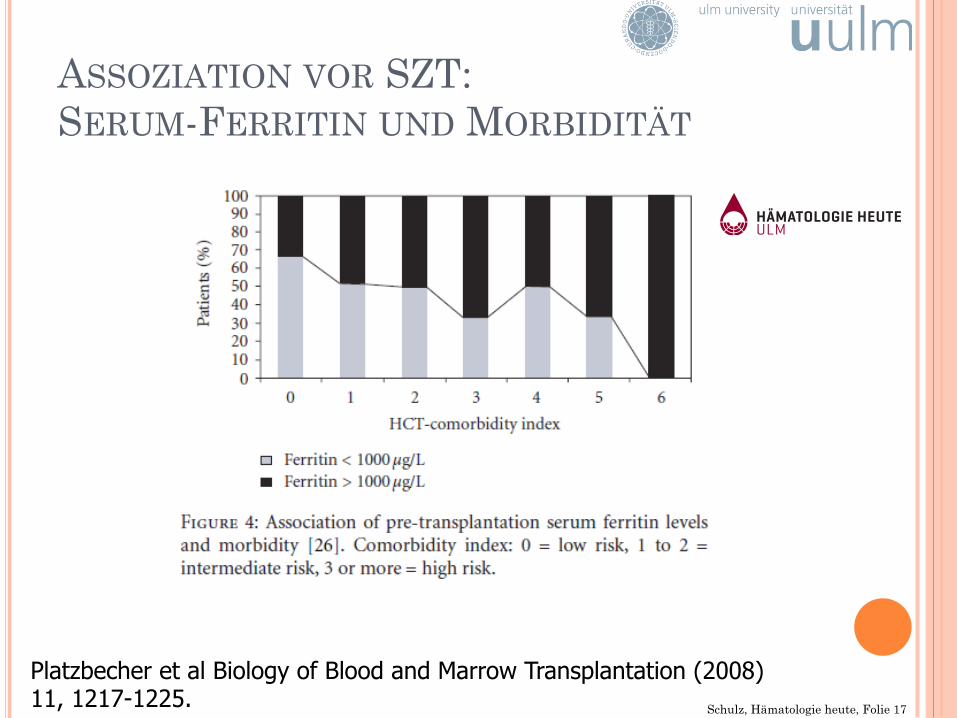
ASSOZIATION VOR SZT: SERUM-FERRITIN UND MORBIDITÄT
Platzbecher et al Biology of Blood and Marrow Transplantation (2008) 11, 1217-1225. Schulz, Hämatologie heute, Folie 17
BEWERTUNG
Haematologica (2010)
Advances in Hematology (2010)
Journal of Hematology & Oncology (2009)
Schulz, Hämatologie heute, Folie 18

THERAPIE
Schulz, Hämatologie heute, Folie 19
¢ 41 Patienten ¢ Hb > 9 g/L ¢ RRs > 90 mmHG ¢ 6 ml/kg alle 14 Tage ¢ bis Serum Ferritin < 300 µg/L alle 21 Tage
Angelucci et al, Blood, 90;3 1997
PHLEBOTOMIE NACH SZT
Schulz, Hämatologie heute, Folie 20
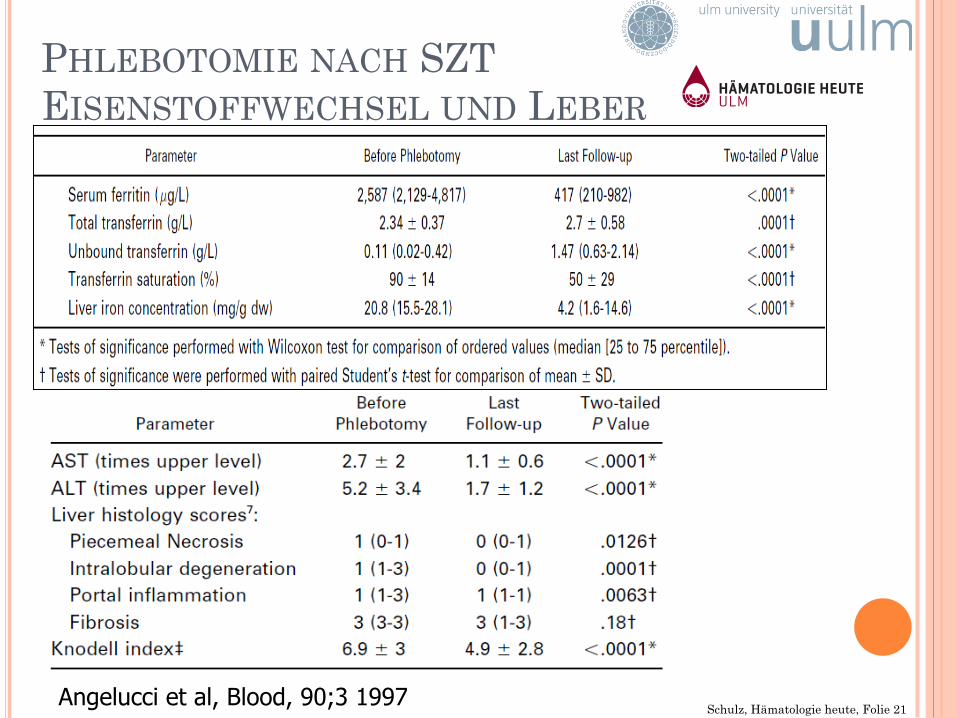
Angelucci et al, Blood, 90;3 1997 Schulz, Hämatologie heute, Folie 21
PHLEBOTOMIE NACH SZT EISENSTOFFWECHSEL UND LEBER
PHLEBOTOMIE UND DESFERAL KARDIALE FUNKTION NACH SZT
Mariotti et al, Br J Haematol, 1998
¢ 32 Patienten: Phlebotomie und Desferal®-Therapie ¢ Normalisierung der Kontraktilität ¢ Normalisierung der diastolischen Funktion (%FS/ESWS)
Schulz, Hämatologie heute, Folie 22
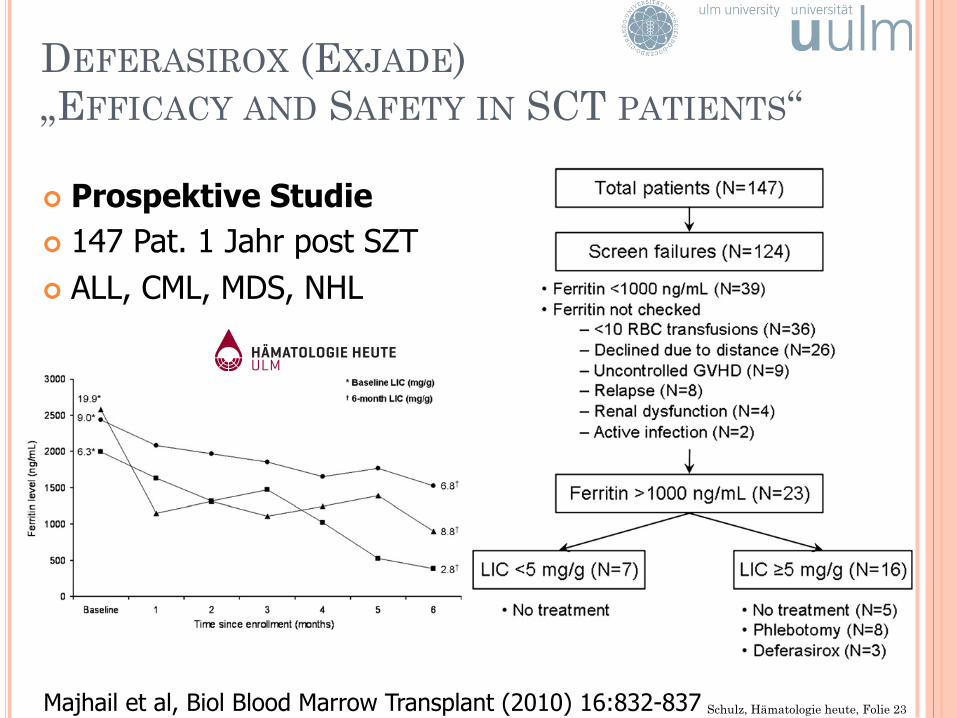
DEFERASIROX (EXJADE) „EFFICACY AND SAFETY IN SCT PATIENTS“
¢ Prospektive Studie ¢ 147 Pat. 1 Jahr post SZT ¢ ALL, CML, MDS, NHL
Majhail et al, Biol Blood Marrow Transplant (2010) 16:832-837 Schulz, Hämatologie heute, Folie 23
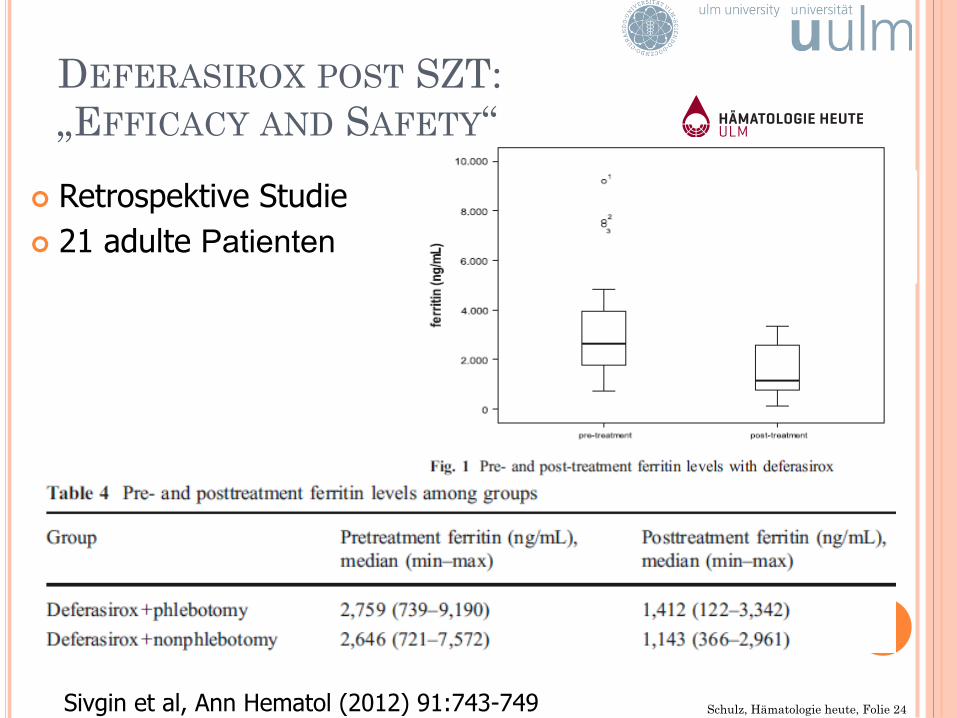
DEFERASIROX POST SZT: „EFFICACY AND SAFETY“
Sivgin et al, Ann Hematol (2012) 91:743-749
¢ Retrospektive Studie ¢ 21 adulte Patienten
Schulz, Hämatologie heute, Folie 24
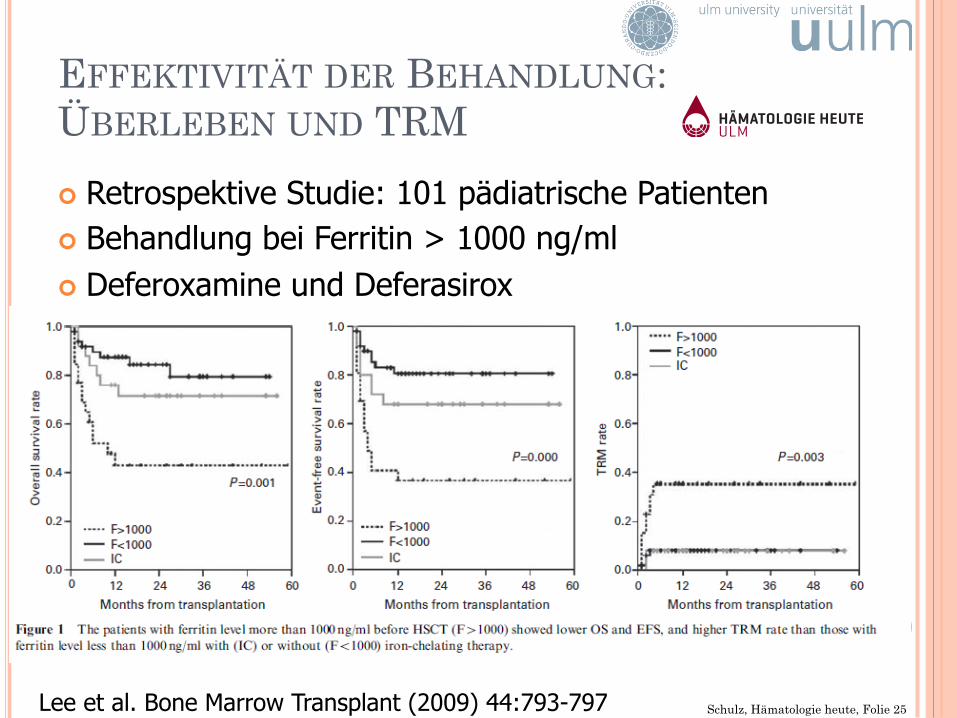
EFFEKTIVITÄT DER BEHANDLUNG: ÜBERLEBEN UND TRM
¢ Retrospektive Studie: 101 pädiatrische Patienten ¢ Behandlung bei Ferritin > 1000 ng/ml ¢ Deferoxamine und Deferasirox
Lee et al. Bone Marrow Transplant (2009) 44:793-797 Schulz, Hämatologie heute, Folie 25
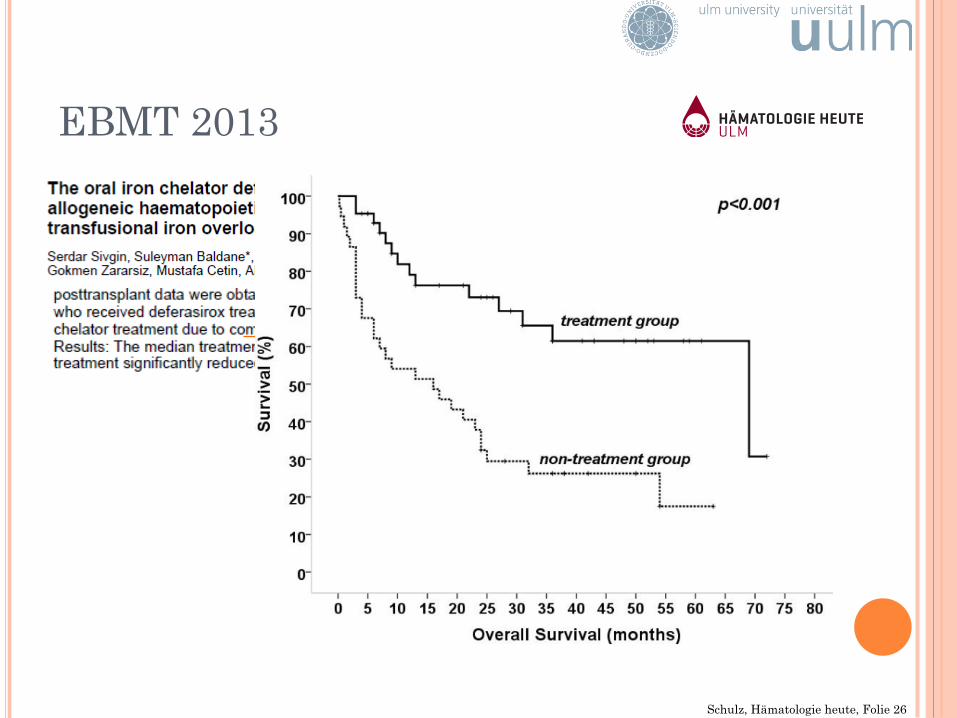
EBMT 2013
Schulz, Hämatologie heute, Folie 26
RICHTLINIEN UND „STATE OR THE ART“
Schulz, Hämatologie heute, Folie 27
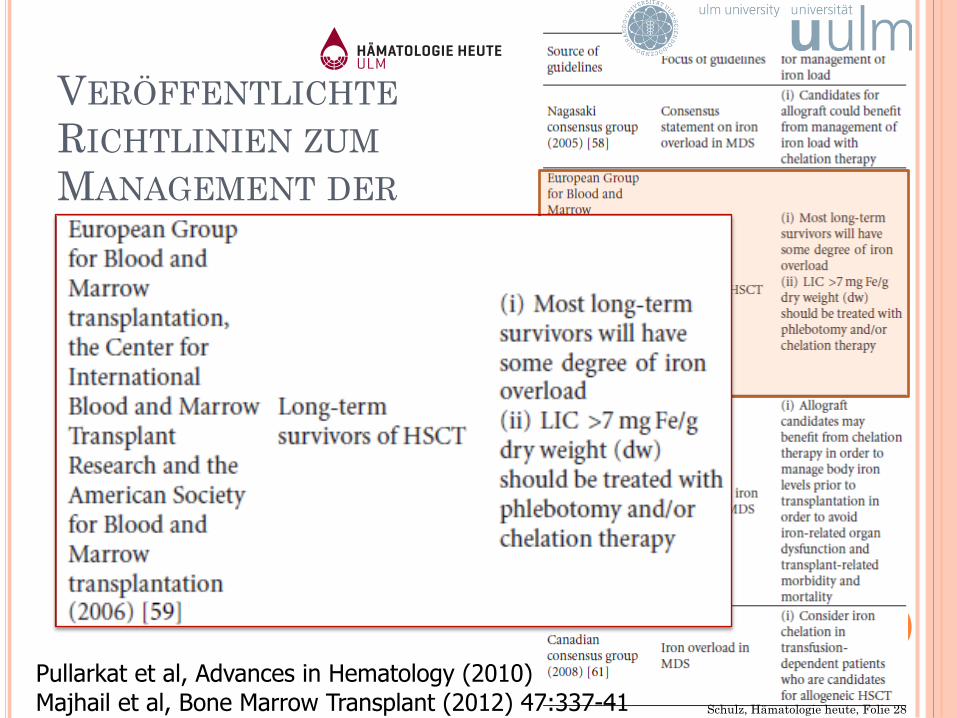
VERÖFFENTLICHTE RICHTLINIEN ZUM MANAGEMENT DER EISENÜBERLADUNG
Pullarkat et al, Advances in Hematology (2010) Schulz, Hämatologie heute, Folie 28 Majhail et al, Bone Marrow Transplant (2012) 47:337-41
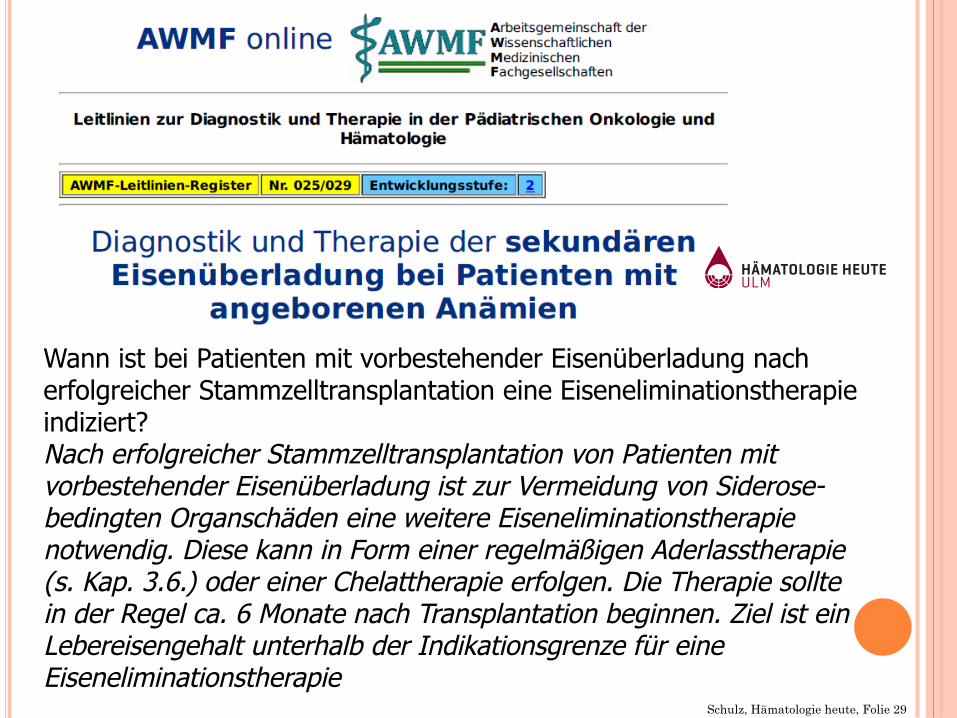
Wann ist bei Patienten mit vorbestehender Eisenüberladung nach erfolgreicher Stammzelltransplantation eine Eiseneliminationstherapie indiziert? Nach erfolgreicher Stammzelltransplantation von Patienten mit vorbestehender Eisenüberladung ist zur Vermeidung von Siderose-bedingten Organschäden eine weitere Eiseneliminationstherapie notwendig. Diese kann in Form einer regelmäßigen Aderlasstherapie (s. Kap. 3.6.) oder einer Chelattherapie erfolgen. Die Therapie sollte in der Regel ca. 6 Monate nach Transplantation beginnen. Ziel ist ein Lebereisengehalt unterhalb der Indikationsgrenze für eine Eiseneliminationstherapie
Schulz, Hämatologie heute, Folie 29
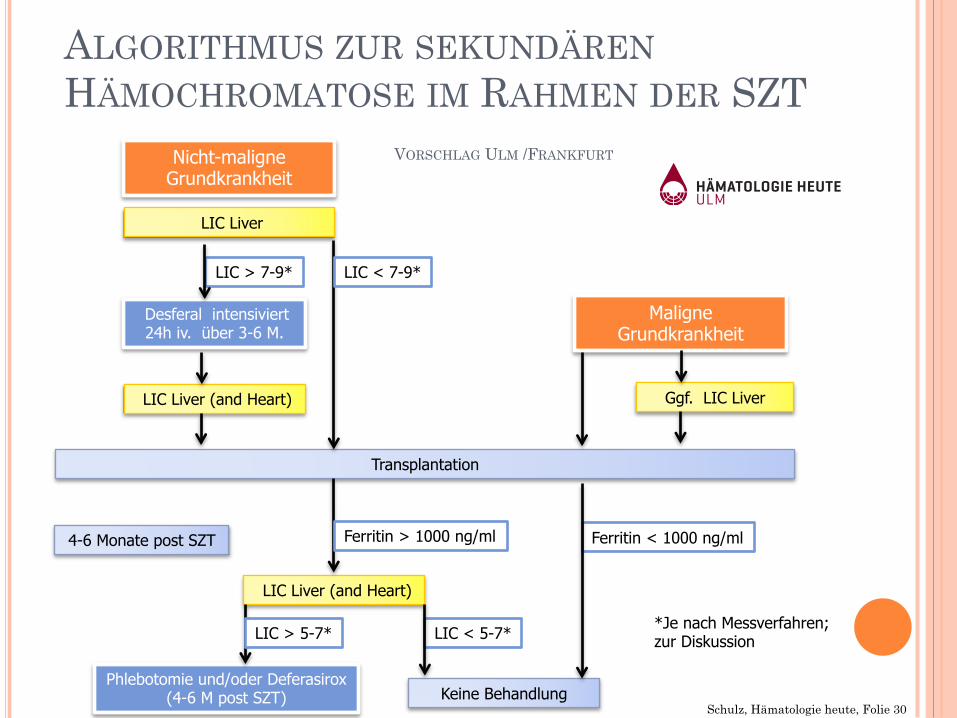
ALGORITHMUS ZUR SEKUNDÄREN HÄMOCHROMATOSE IM RAHMEN DER SZT
Nicht-maligne Grundkrankheit
Maligne Grundkrankheit
Desferal intensiviert 24h iv. über 3-6 M.
LIC Liver
LIC > 7-9*
LIC Liver (and Heart)
Transplantation
LIC Liver (and Heart)
LIC < 7-9*
Ggf. LIC Liver
4-6 Monate post SZT Ferritin > 1000 ng/ml Ferritin < 1000 ng/ml
Phlebotomie und/oder Deferasirox (4-6 M post SZT)
LIC < 5-7*
Keine Behandlung
LIC > 5-7*
VORSCHLAG ULM /FRANKFURT
*Je nach Messverfahren; zur Diskussion
Schulz, Hämatologie heute, Folie 30
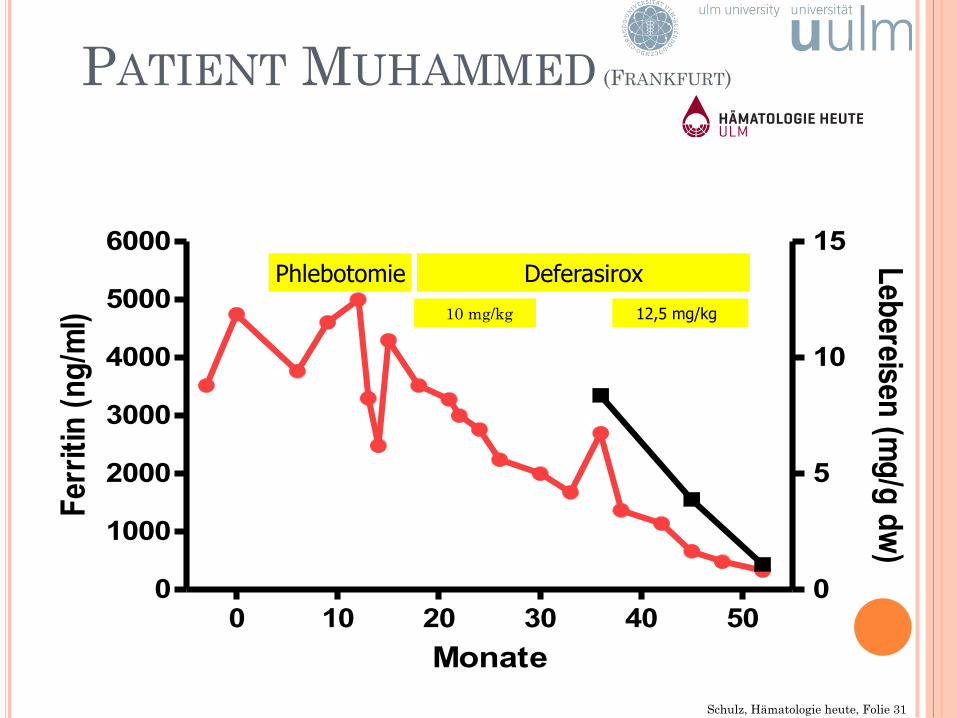
0 10 20 30 40 500
1000
2000
3000
4000
5000
6000
0
5
10
15
Monate
Ferr
itin
(ng/
ml)
Lebereisen (mg/g dw)
PATIENT MUHAMMED (FRANKFURT)
Phlebotomie 12,5 mg/kg
Deferasirox 10 mg/kg
Schulz, Hämatologie heute, Folie 31
ZUSAMMENFASSUNG
Diagnostik: ¢ Ferritin möglicherweise sinnvoll als Surrogatmarker
für TRM und als Verlaufsparameter ¢ MRT-Leber (T2*) Diagnostik der Wahl zur Beurteilung
der Eisenbelastung Therapie: ¢ Phlebotomie Standardverfahren ¢ Orale Chelattherapie mit Deferasirox möglich (niedrige
Startdosis, Nephrotoxizität beachten) à Größere prospektive Studien bei Kindern erforderlich
Schulz, Hämatologie heute, Folie 32
DANKE FÜR IHRE AUFMERKSAMKEIT
Schulz, Hämatologie heute, Folie 33








