Embed Size (px)
Citation preview
Das Pankreas bei Diabetes mellitusMorphologie und mehr
Matthias LöhrProfessor of Gastroenterology
Gastrocentrum
Karolinska University Hospital
©M. Löhr 2012
ThemenThemen
• Pankreasphysiologie
• Die Philosophie der Evolution
• Pankreasmorphologie bei Diabetes mellitus
• Pankreasfunktion bei Diabetes mellitus
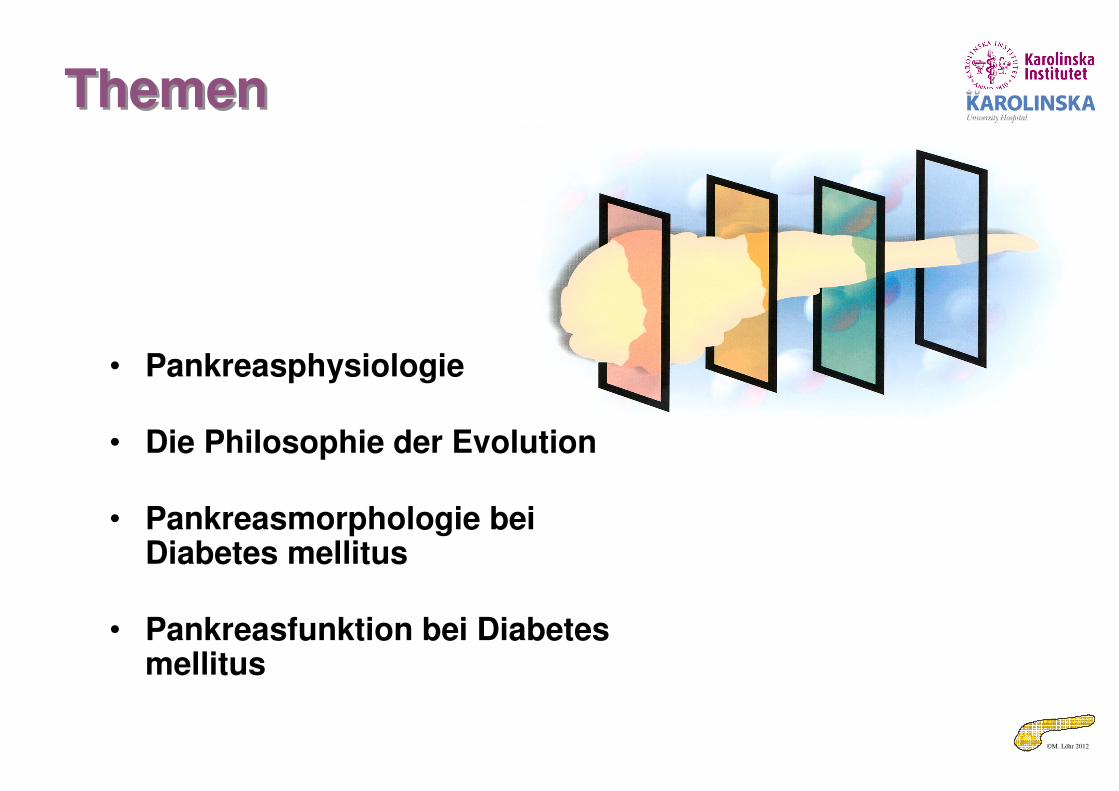
©M. Löhr 2012Löhr & Klöppel in Hahn/Riemann, Gastroenterologie, Thieme 1994
Die morphologische GrundlageDie morphologische Grundlage• Intime „geographische“
Beziehung zwischen exokrinem und endokrinem Pankreas
• Blutfluß arteriell => Insel => exokrines Pankreas
©M. Löhr 2012
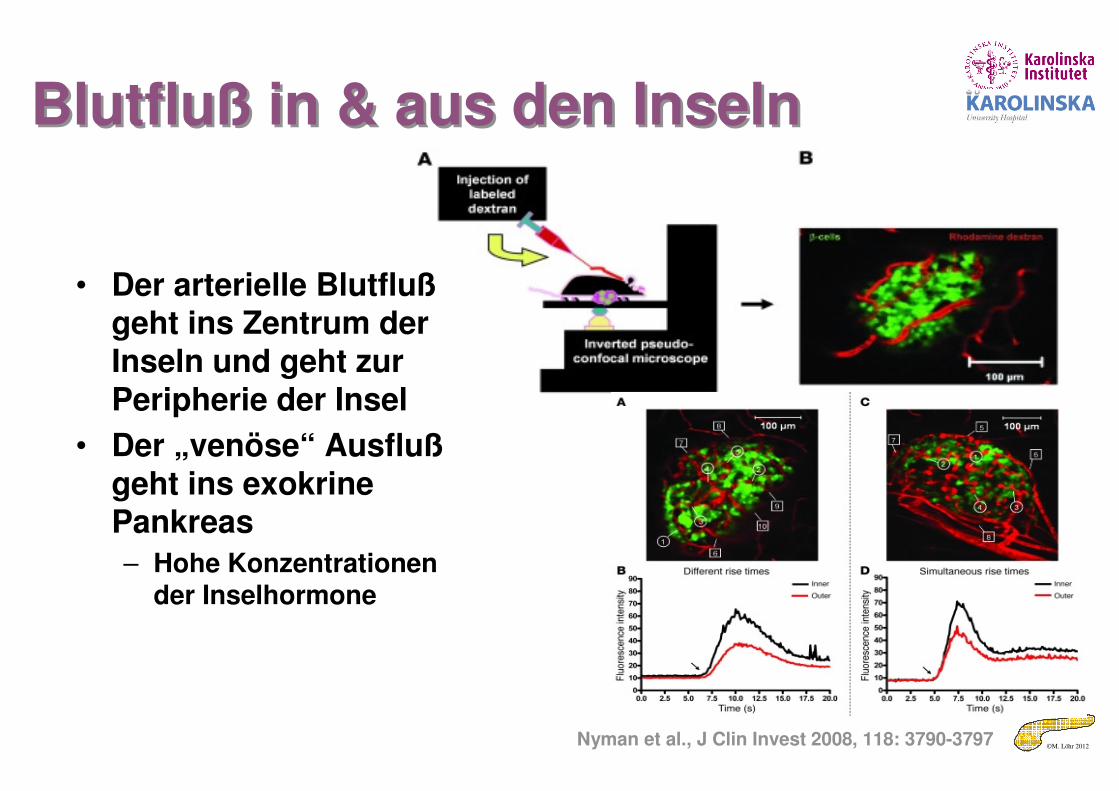
Blutfluß in & aus den InselnBlutfluß in & aus den Inseln
Nyman et al., J Clin Invest 2008, 118: 3790-3797
• Der arterielle Blutflußgeht ins Zentrum der Inseln und geht zur Peripherie der Insel
• Der „venöse“ Ausflußgeht ins exokrine Pankreas
– Hohe Konzentrationen der Inselhormone
©M. Löhr 2012
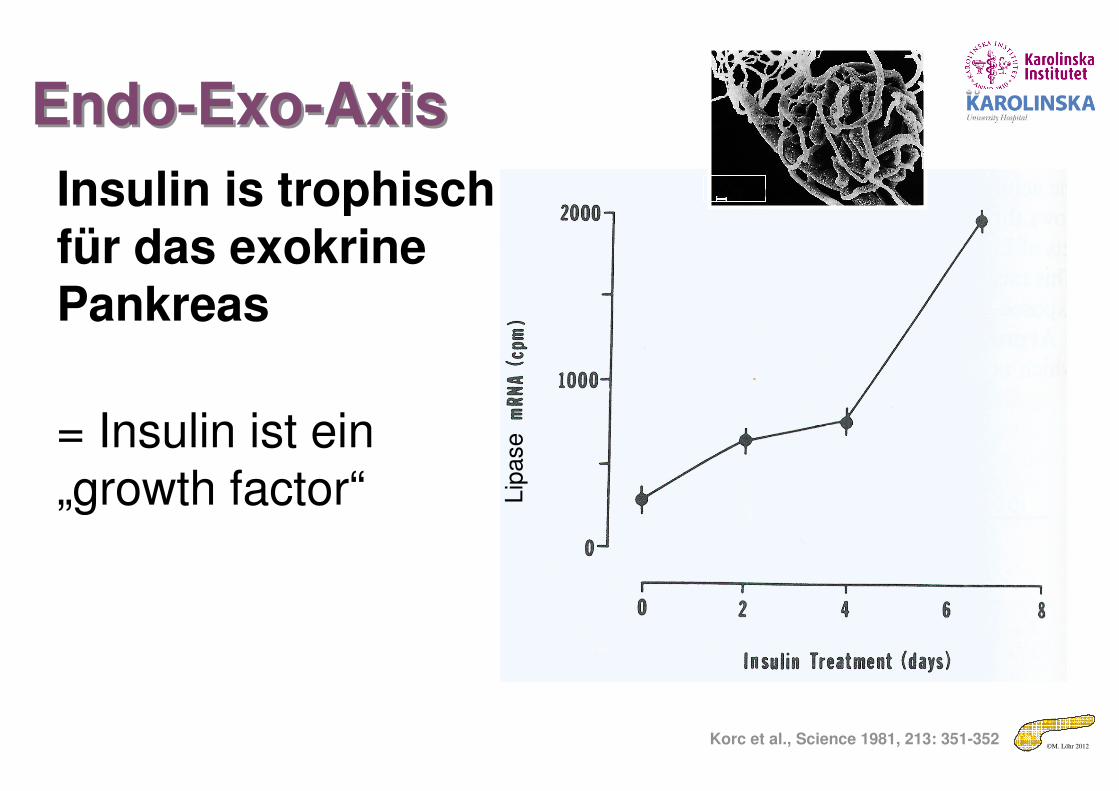
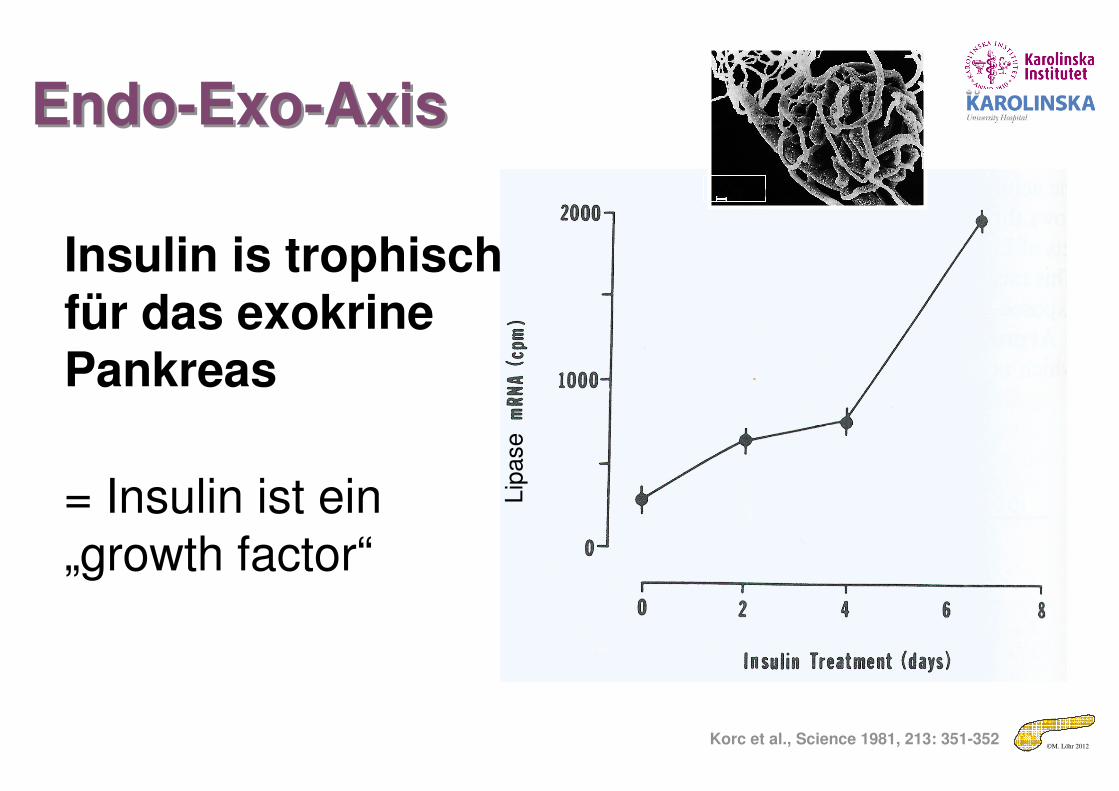
Endo-Exo-AxisEndo-Exo-Axis
Korc et al., Science 1981, 213: 351-352
Insulin is trophisch für das exokrine Pankreas
= Insulin ist ein „growth factor“ L
ipase
100 µm
©M. Löhr 2012
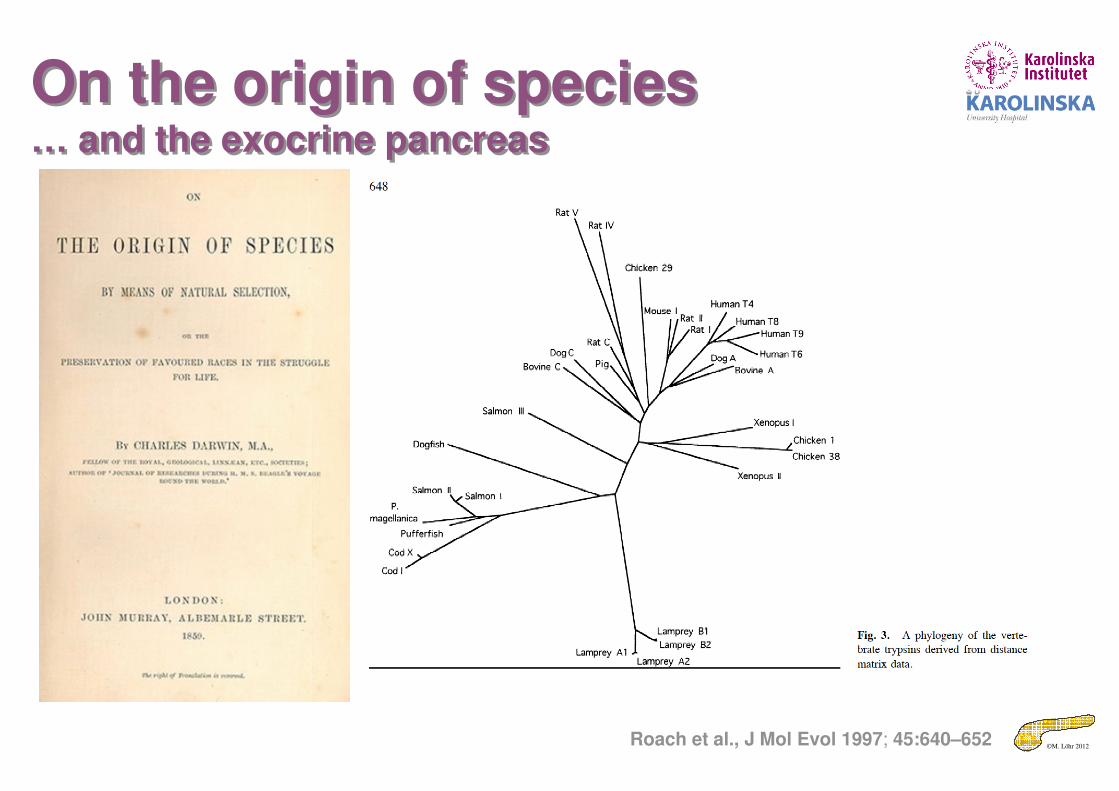
On the origin of species… and the exocrine pancreas
On the origin of species… and the exocrine pancreas
Roach et al., J Mol Evol 1997; 45:640–652
©M. Löhr 2012
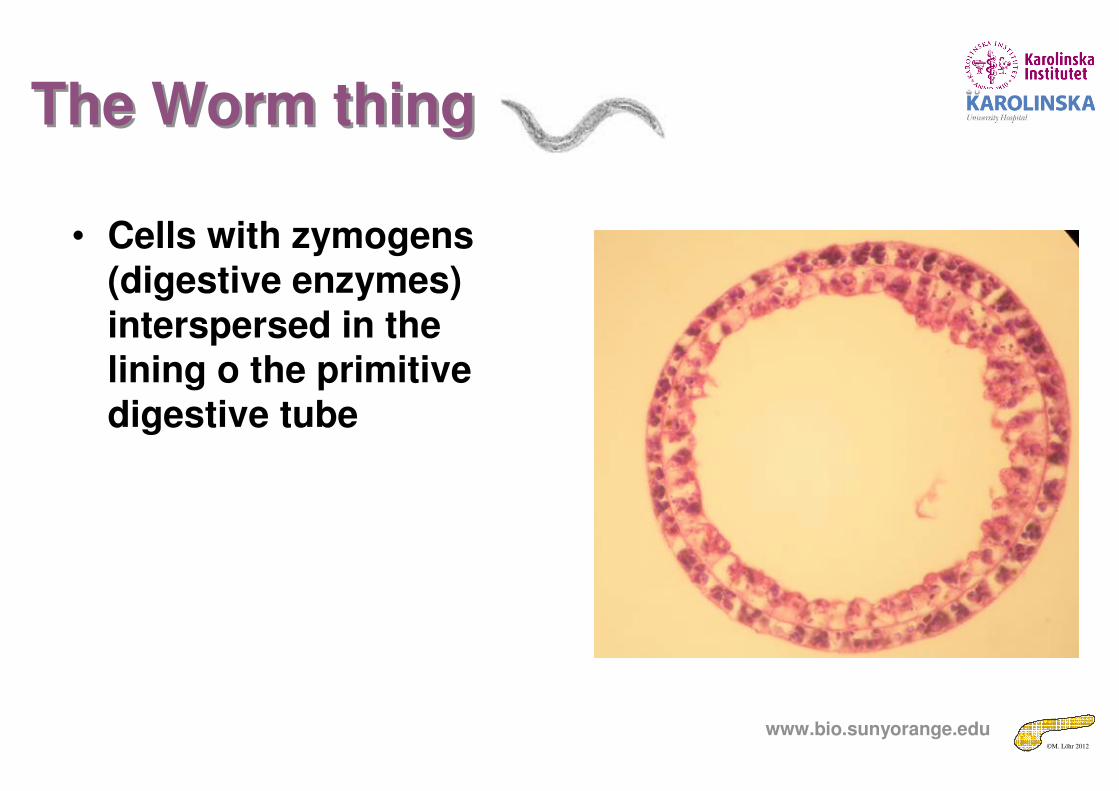
The Worm thingThe Worm thing
• Cells with zymogens (digestive enzymes) interspersed in the lining o the primitive digestive tube
www.bio.sunyorange.edu
©M. Löhr 2012
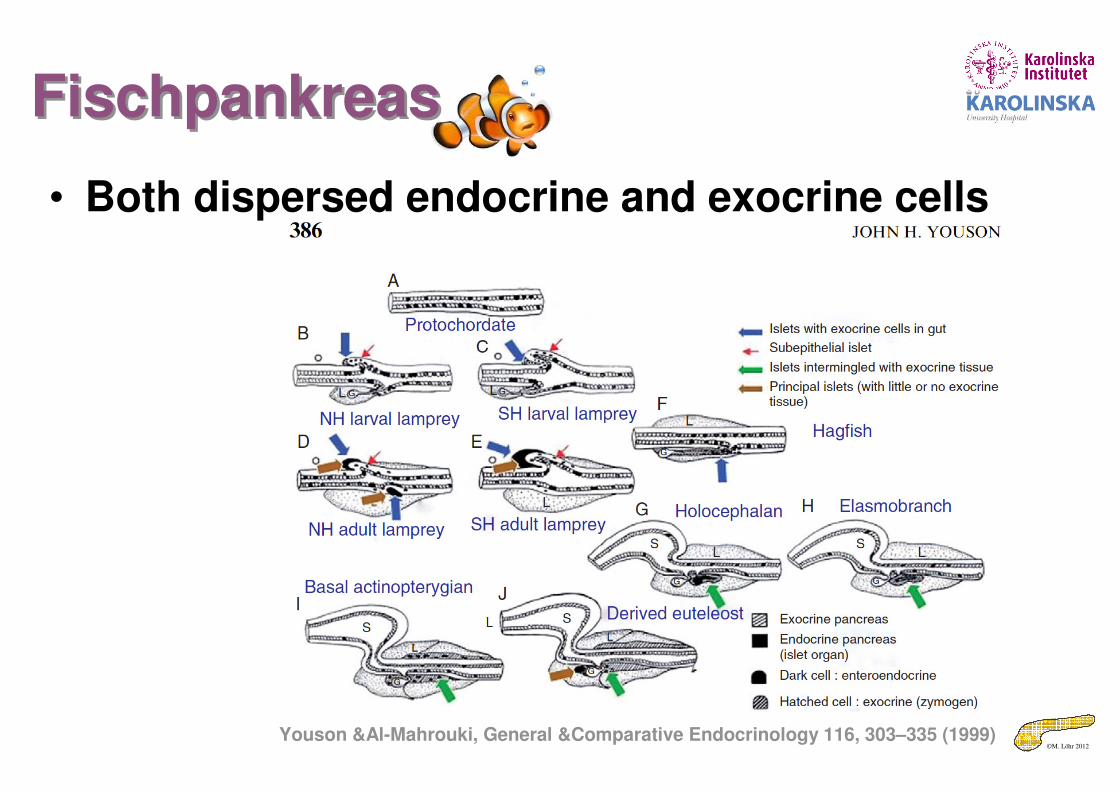
FischpankreasFischpankreas
• Both dispersed endocrine and exocrine cells
Youson &Al-Mahrouki, General &Comparative Endocrinology 116, 303–335 (1999)
©M. Löhr 2012
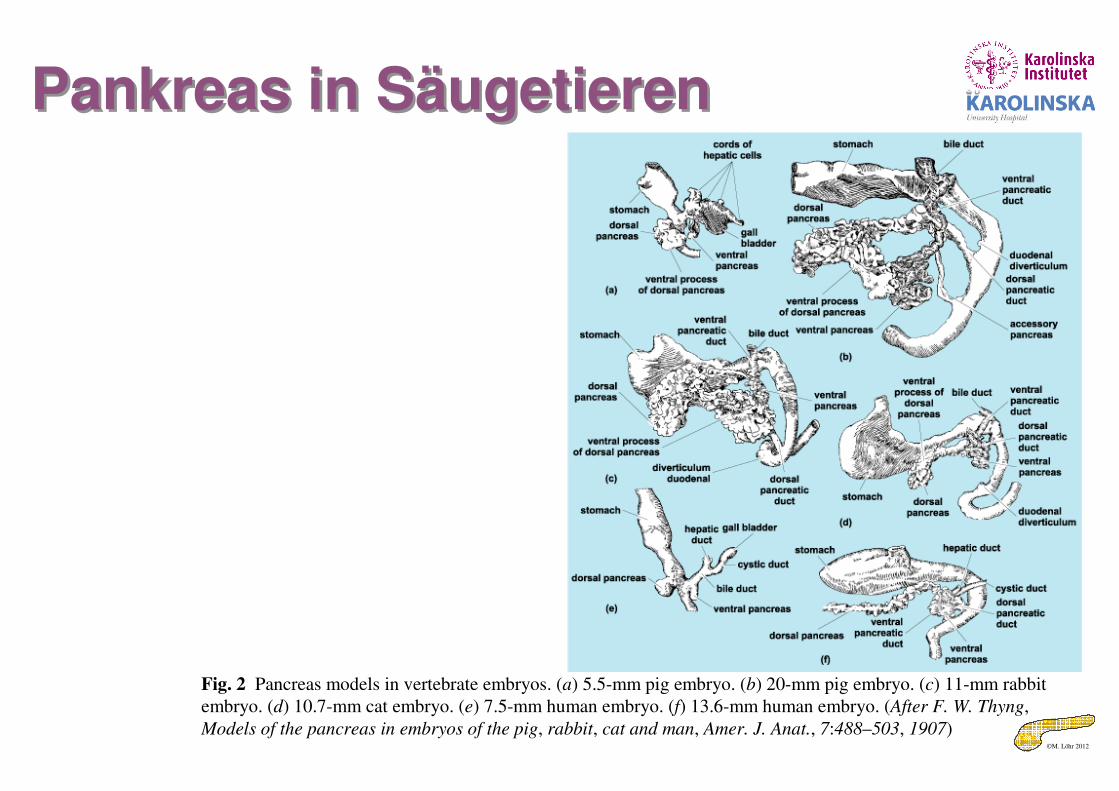
Pankreas in SäugetierenPankreas in Säugetieren
Fig. 2 Pancreas models in vertebrate embryos. (a) 5.5-mm pig embryo. (b) 20-mm pig embryo. (c) 11-mm rabbit
embryo. (d) 10.7-mm cat embryo. (e) 7.5-mm human embryo. (f) 13.6-mm human embryo. (After F. W. Thyng,
Models of the pancreas in embryos of the pig, rabbit, cat and man, Amer. J. Anat., 7:488–503, 1907)
©M. Löhr 2012
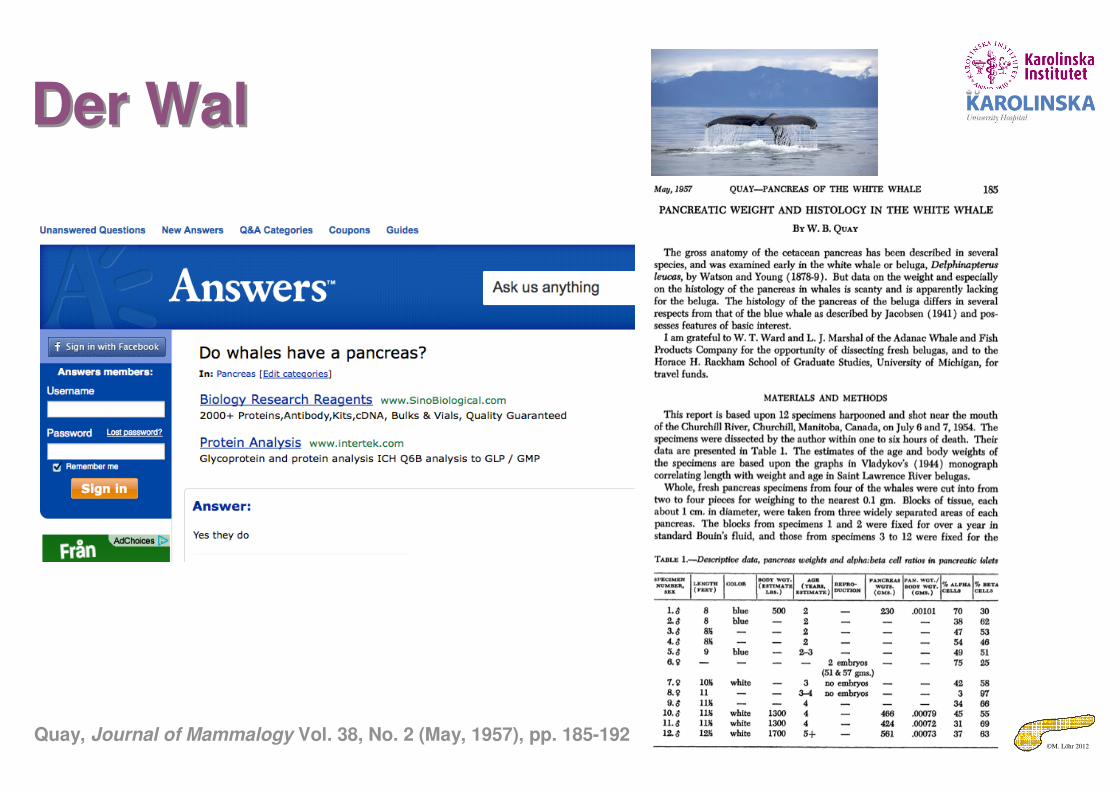
Der WalDer Wal
Quay, Journal of Mammalogy Vol. 38, No. 2 (May, 1957), pp. 185-192
©M. Löhr 2012
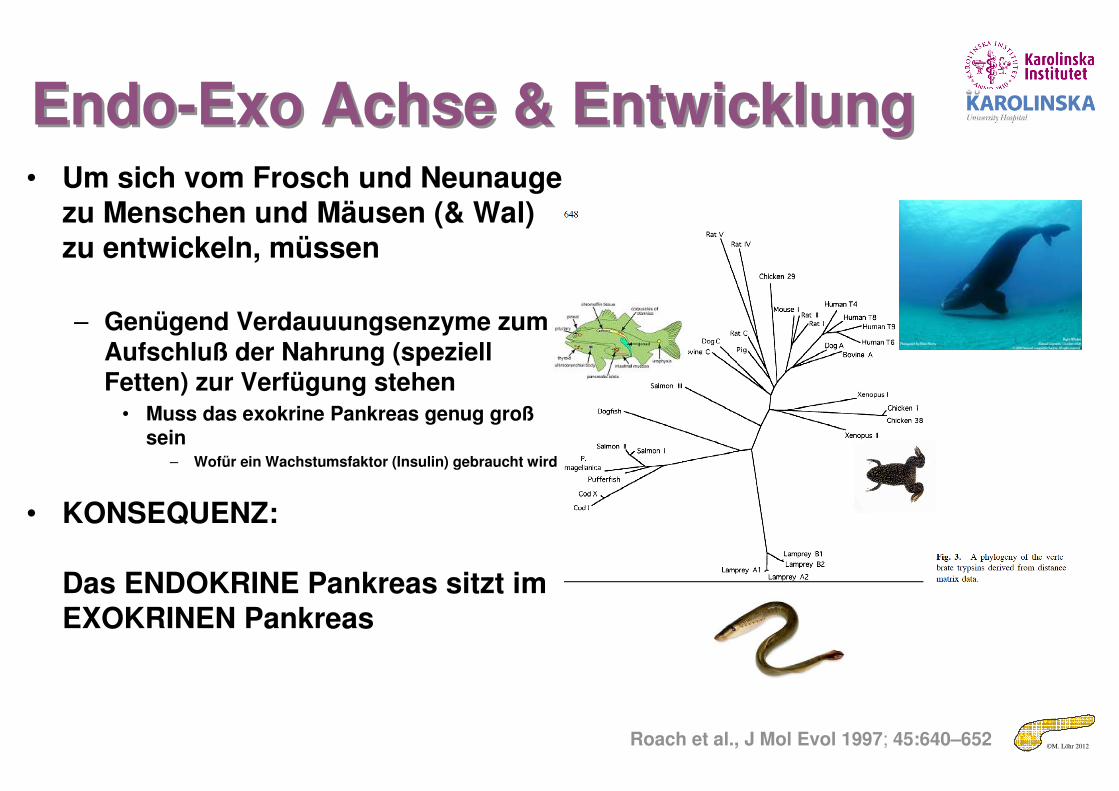
Endo-Exo Achse & EntwicklungEndo-Exo Achse & Entwicklung• Um sich vom Frosch und Neunauge
zu Menschen und Mäusen (& Wal) zu entwickeln, müssen
– Genügend Verdauuungsenzyme zum Aufschluß der Nahrung (speziell Fetten) zur Verfügung stehen
• Muss das exokrine Pankreas genug großsein
– Wofür ein Wachstumsfaktor (Insulin) gebraucht wird
• KONSEQUENZ:
Das ENDOKRINE Pankreas sitzt im EXOKRINEN Pankreas
Roach et al., J Mol Evol 1997; 45:640–652
©M. Löhr 2012
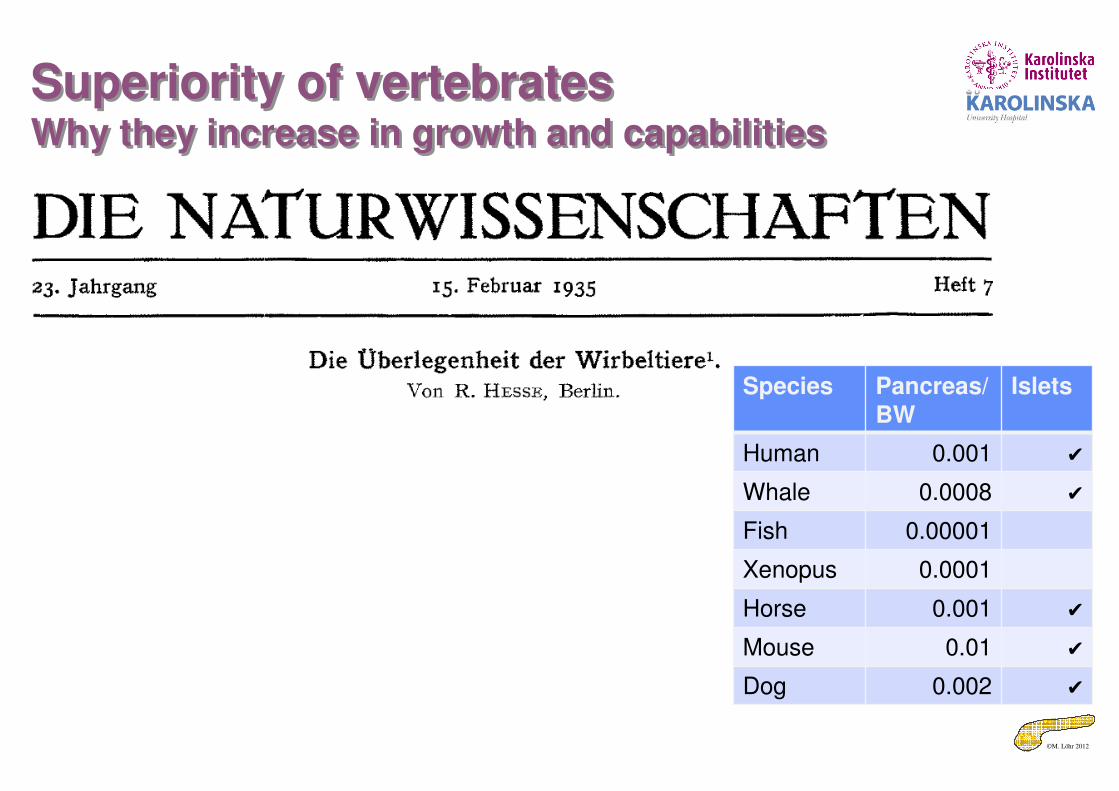
Superiority of vertebratesWhy they increase in growth and capabilities
Superiority of vertebratesWhy they increase in growth and capabilities
Species Pancreas/BW
Islets
Human 0.001 ✔
Whale 0.0008 ✔
Fish 0.00001
Xenopus 0.0001
Horse 0.001 ✔
Mouse 0.01 ✔
Dog 0.002 ✔
©M. Löhr 2012
Endo-Exo-AxisEndo-Exo-Axis
Korc et al., Science 1981, 213: 351-352
Insulin is trophisch für das exokrine Pankreas
= Insulin ist ein
„growth factor“Lip
ase
100 µm
©M. Löhr 2012
No insulin – no growth?!No insulin – no growth?!
©M. Löhr 2012
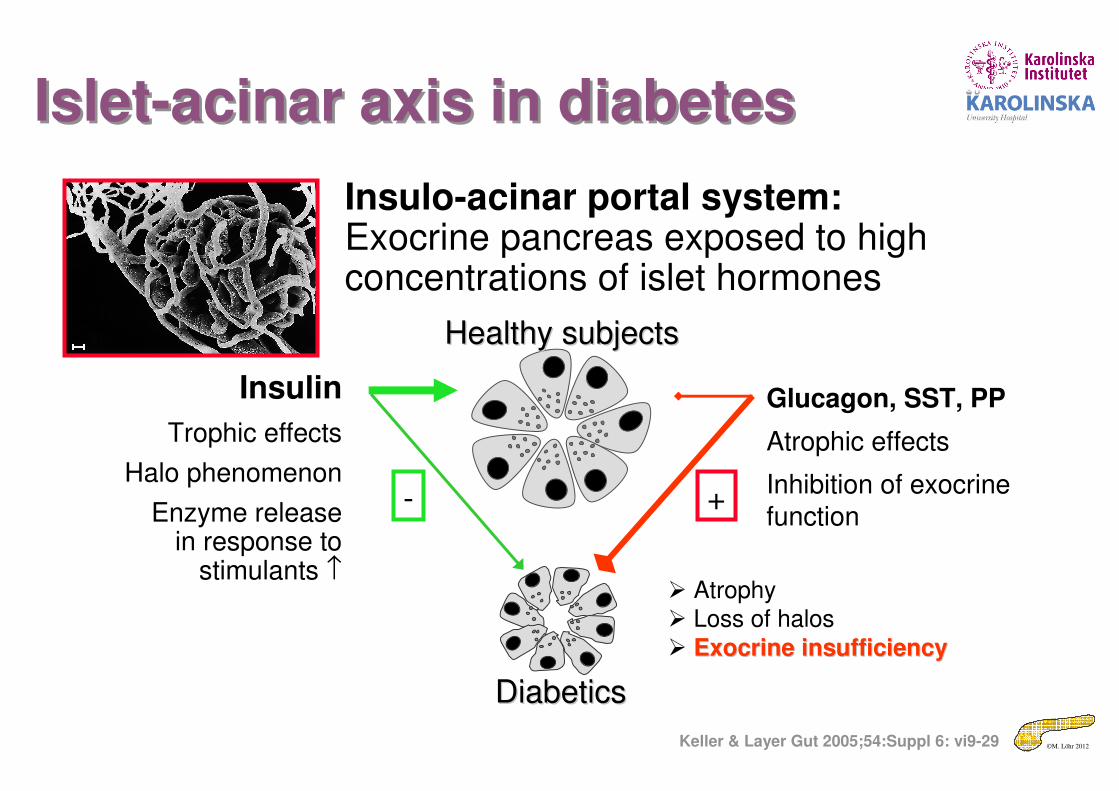
Insulo-acinar portal system: Exocrine pancreas exposed to high concentrations of islet hormones
100 µm
Insulin
Trophic effects
Halo phenomenon
Enzyme releasein response to
stimulants ↑
Glucagon, SST, PP
Atrophic effects
Inhibition of exocrine
function
Healthy subjectsHealthy subjects
� Atrophy � Loss of halos
� Exocrine insufficiencyExocrine insufficiency
- +
DiabeticsDiabetics
Islet-acinar axis in diabetesIslet-acinar axis in diabetes
Keller & Layer Gut 2005;54:Suppl 6: vi9-29
©M. Löhr 2012
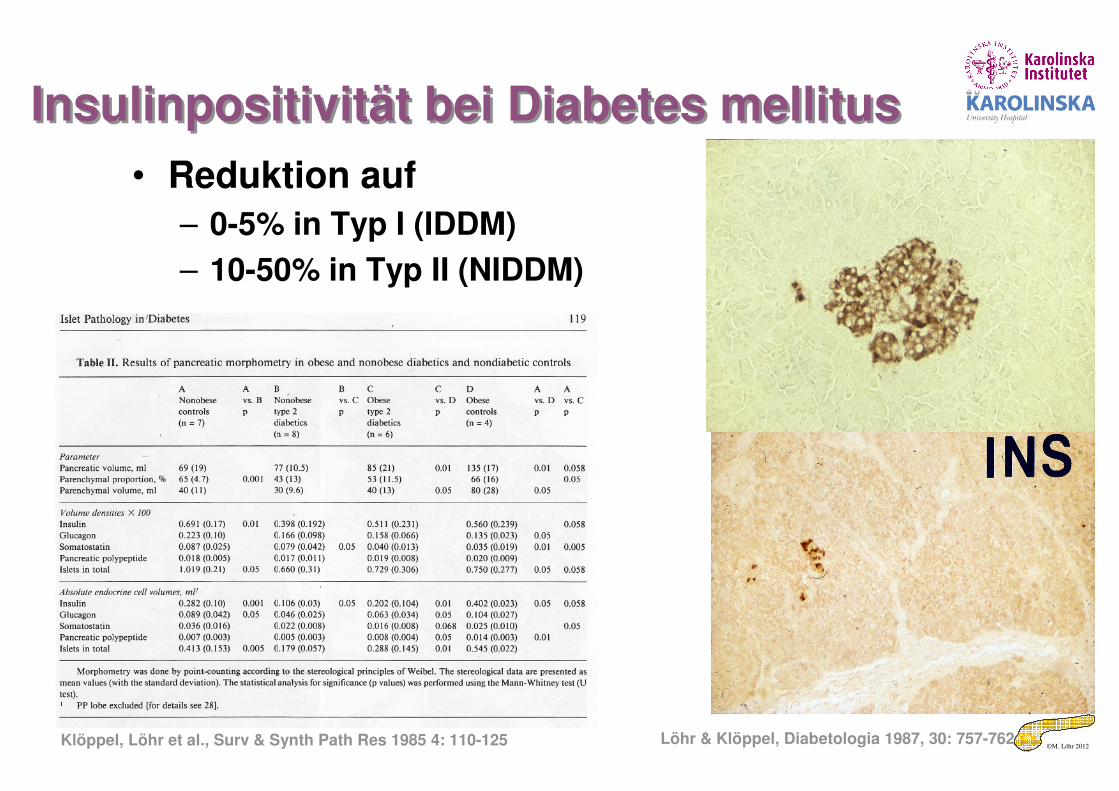
Insulinpositivität bei Diabetes mellitusInsulinpositivität bei Diabetes mellitus
• Reduktion auf
– 0-5% in Typ I (IDDM)
– 10-50% in Typ II (NIDDM)
Löhr & Klöppel, Diabetologia 1987, 30: 757-762Klöppel, Löhr et al., Surv & Synth Path Res 1985 4: 110-125
©M. Löhr 2012
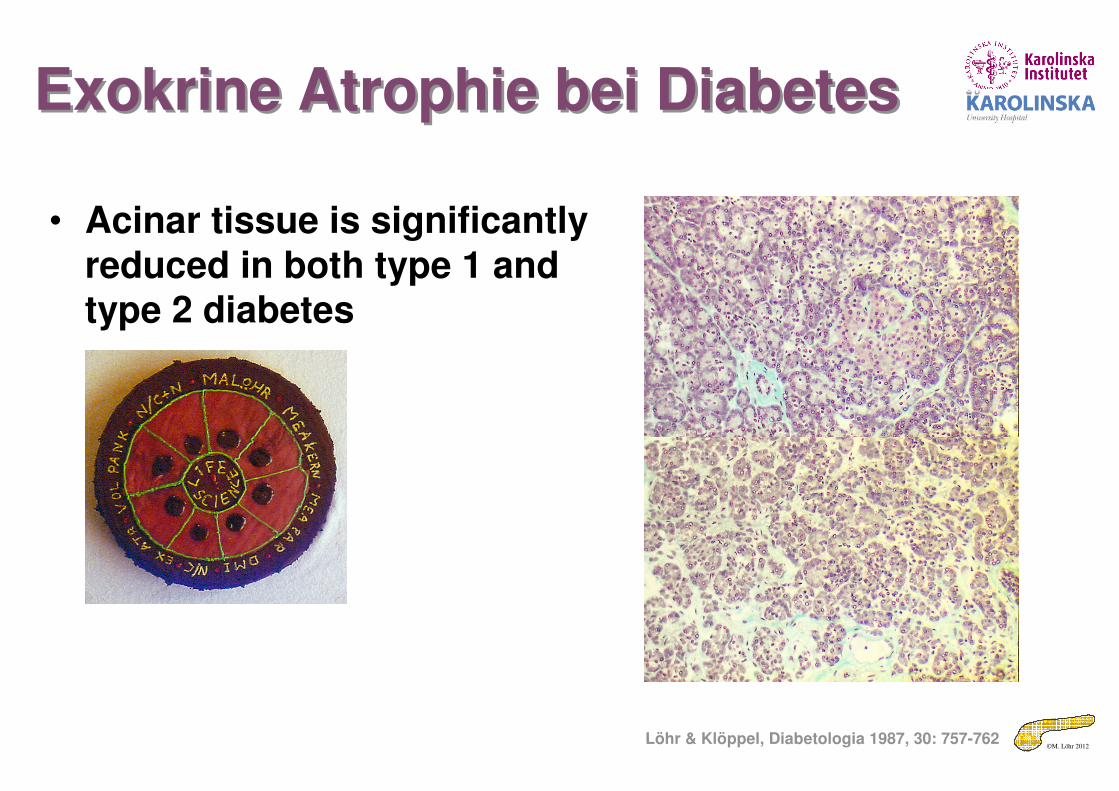
Exokrine Atrophie bei DiabetesExokrine Atrophie bei Diabetes
Löhr & Klöppel, Diabetologia 1987, 30: 757-762
• Acinar tissue is significantly reduced in both type 1 and type 2 diabetes
©M. Löhr 2012
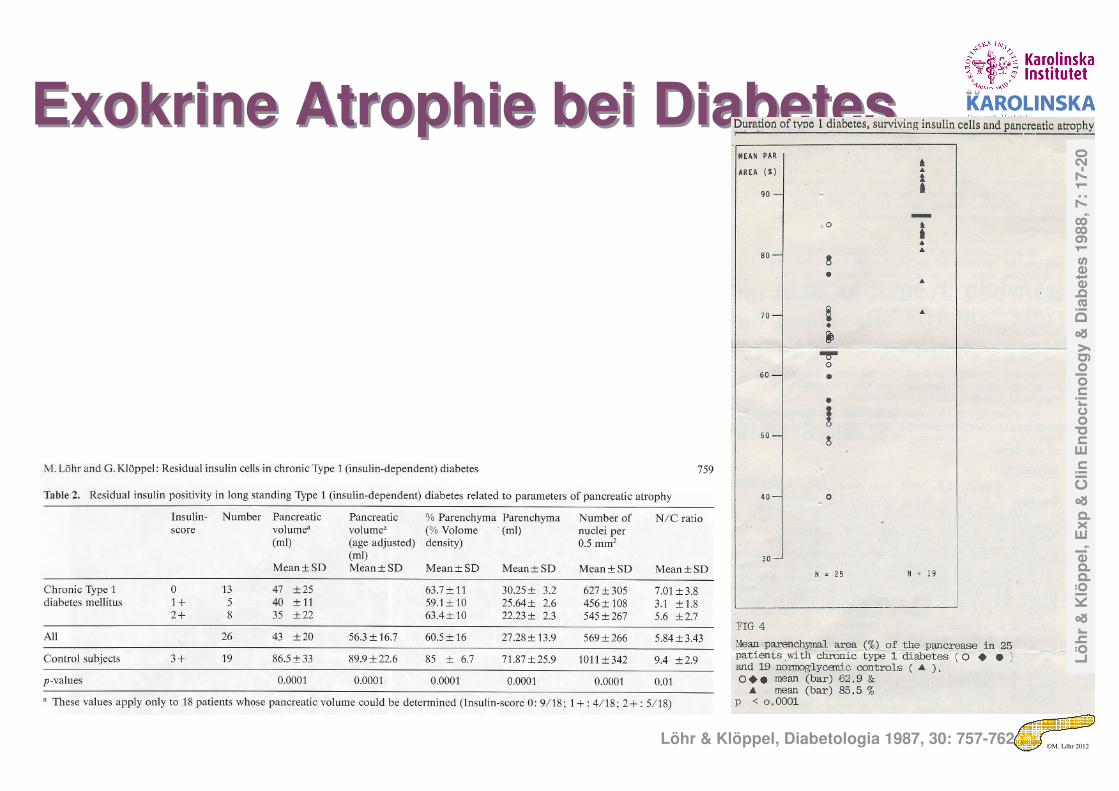
Exokrine Atrophie bei DiabetesExokrine Atrophie bei Diabetes
Löhr & Klöppel, Diabetologia 1987, 30: 757-762
Lö
hr
& K
löp
pe
l, E
xp
& C
lin
En
do
cri
no
log
y &
Dia
be
tes
198
8, 7:
17
-20
©M. Löhr 2012
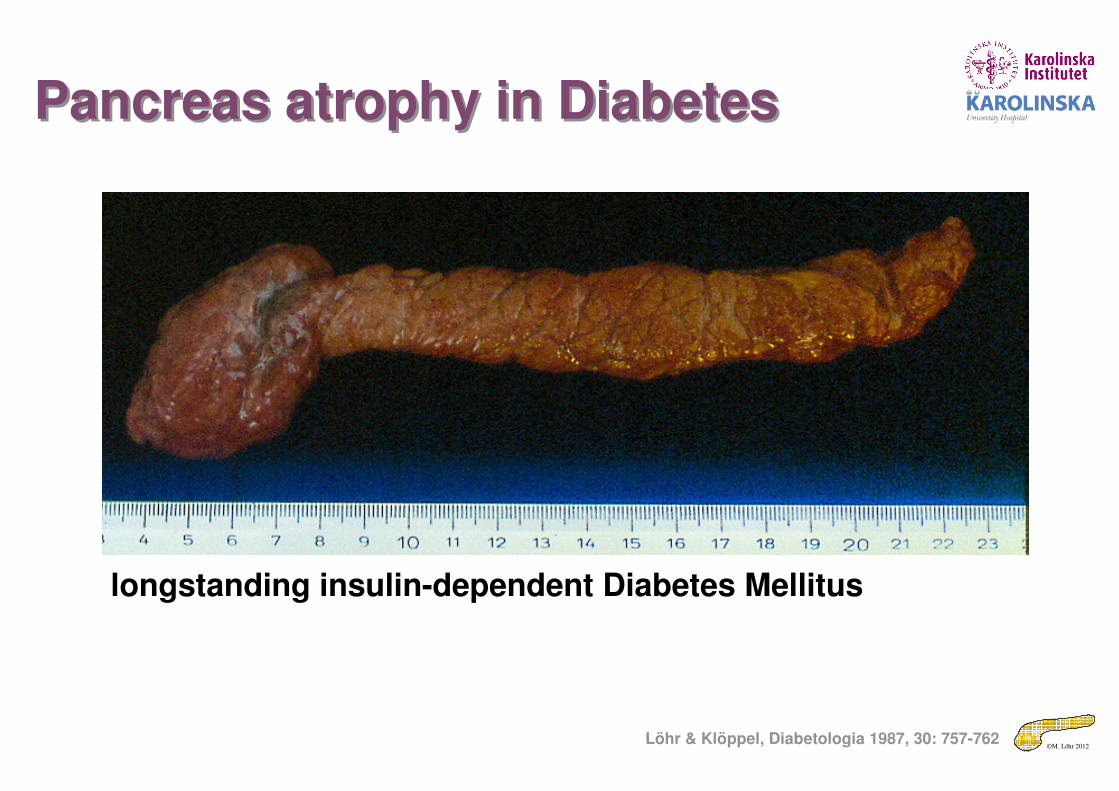
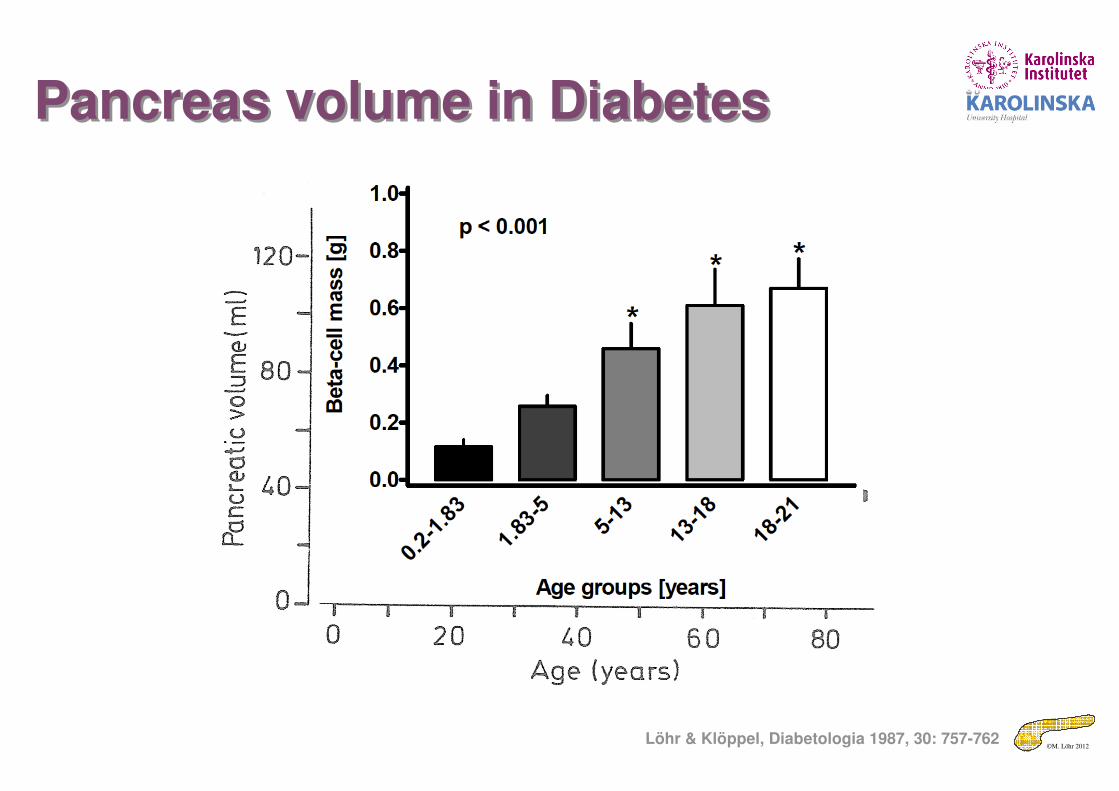
Pancreas atrophy in DiabetesPancreas atrophy in Diabetes
longstanding insulin-dependent Diabetes Mellitus
Löhr & Klöppel, Diabetologia 1987, 30: 757-762
©M. Löhr 2012
Pancreas volume in DiabetesPancreas volume in Diabetes
Löhr & Klöppel, Diabetologia 1987, 30: 757-762
©M. Löhr 2012
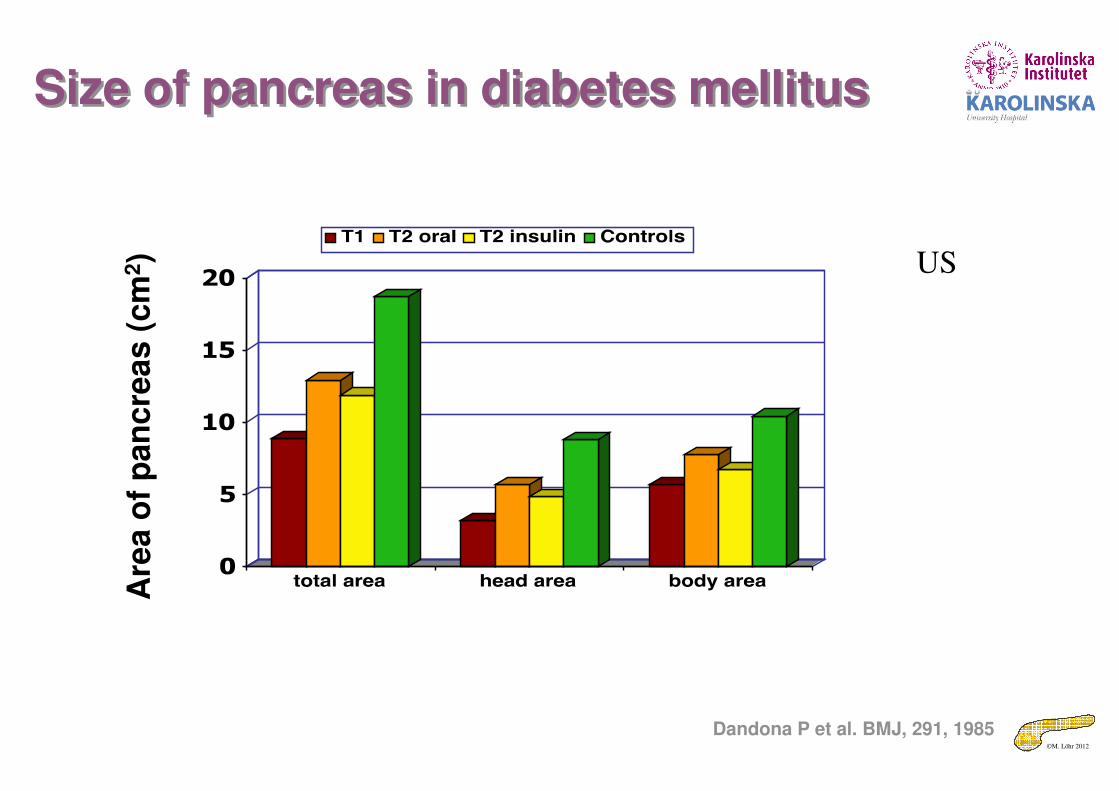
Size of pancreas in diabetes mellitusSize of pancreas in diabetes mellitusA
rea o
f p
an
cre
as (
cm
2)
Dandona P et al. BMJ, 291, 1985
US
©M. Löhr 2012
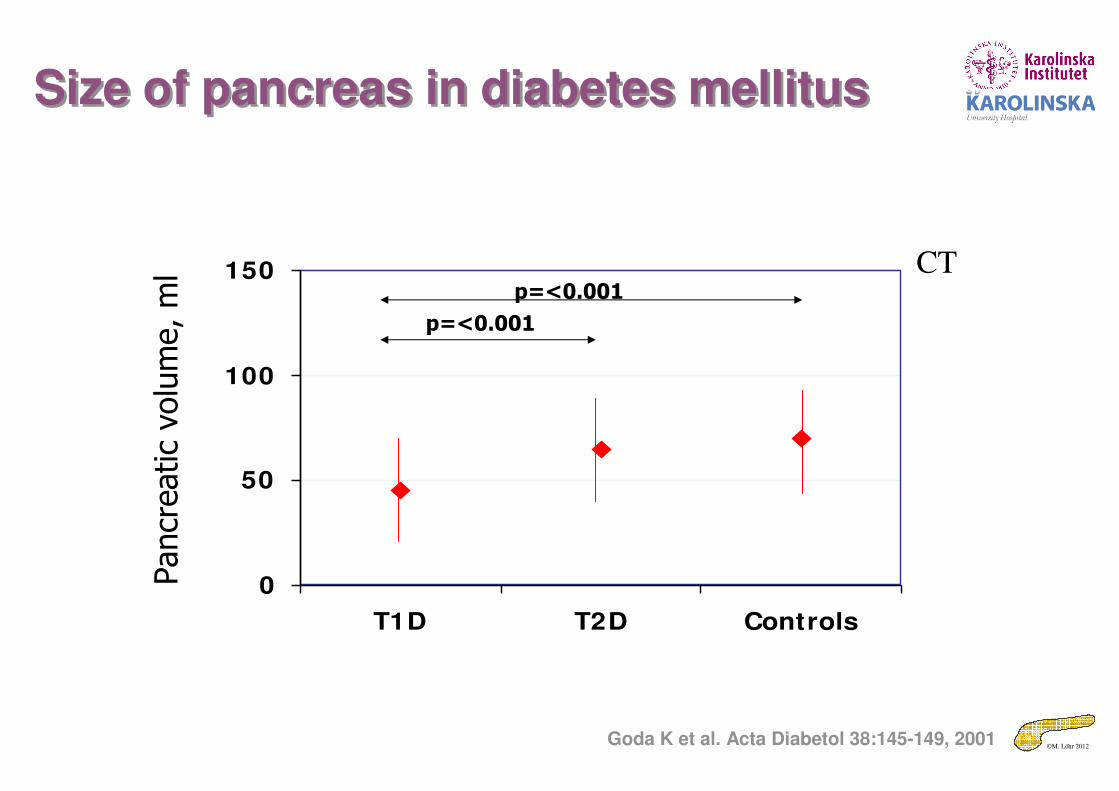
Size of pancreas in diabetes mellitusSize of pancreas in diabetes mellitus
0
50
100
150
T1D T2D Controls
Pancreatic volume, ml
p=<0.001
p=<0.001
CT
Goda K et al. Acta Diabetol 38:145-149, 2001
©M. Löhr 2012
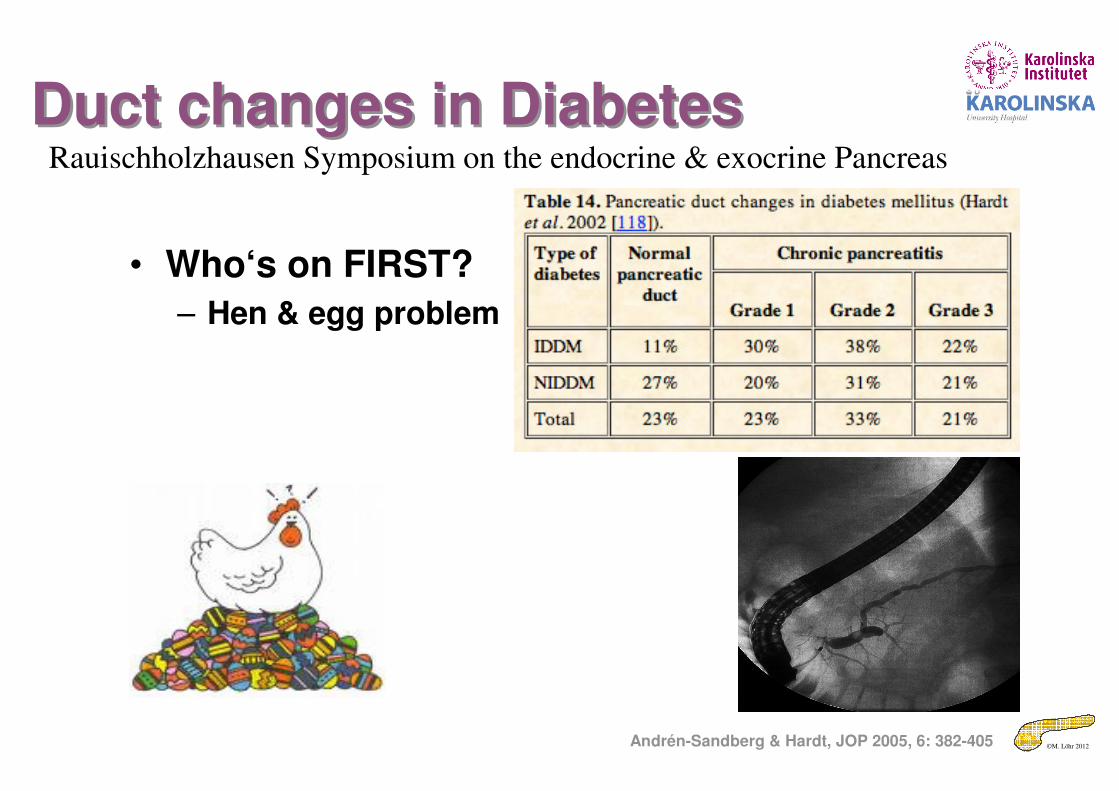
Duct changes in DiabetesDuct changes in Diabetes
• Who‘s on FIRST?
– Hen & egg problem
Andrén-Sandberg & Hardt, JOP 2005, 6: 382-405
Rauischholzhausen Symposium on the endocrine & exocrine Pancreas
©M. Löhr 2012
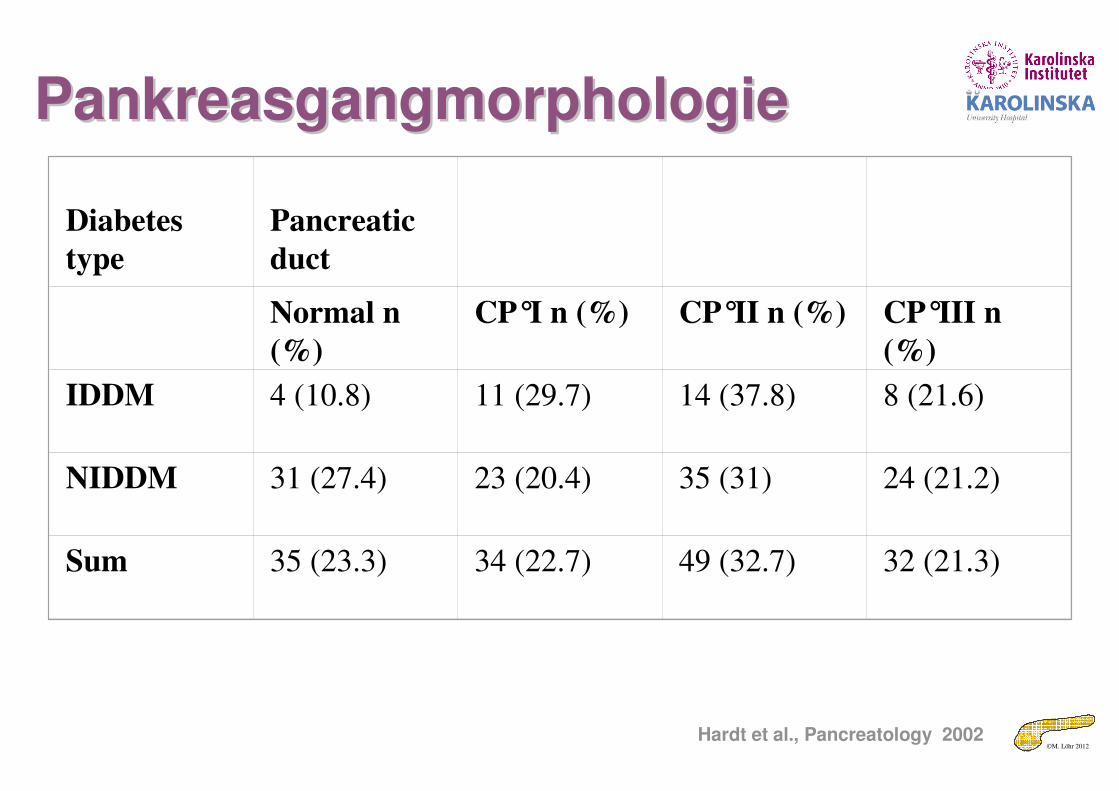
Diabetes
type
Pancreatic
duct
Normal n
(%)
CP°I n (%) CP°II n (%) CP°III n
(%)
IDDM 4 (10.8) 11 (29.7) 14 (37.8) 8 (21.6)
NIDDM 31 (27.4) 23 (20.4) 35 (31) 24 (21.2)
Sum 35 (23.3) 34 (22.7) 49 (32.7) 32 (21.3)
Hardt et al., Pancreatology 2002
PankreasgangmorphologiePankreasgangmorphologie
©M. Löhr 2012
The patient with diabetes mellitusThe patient with diabetes mellitus
• Do patients with diabetes mellitushave
– Exocrine insufficiency
– Clinical symptoms
©M. Löhr 2012
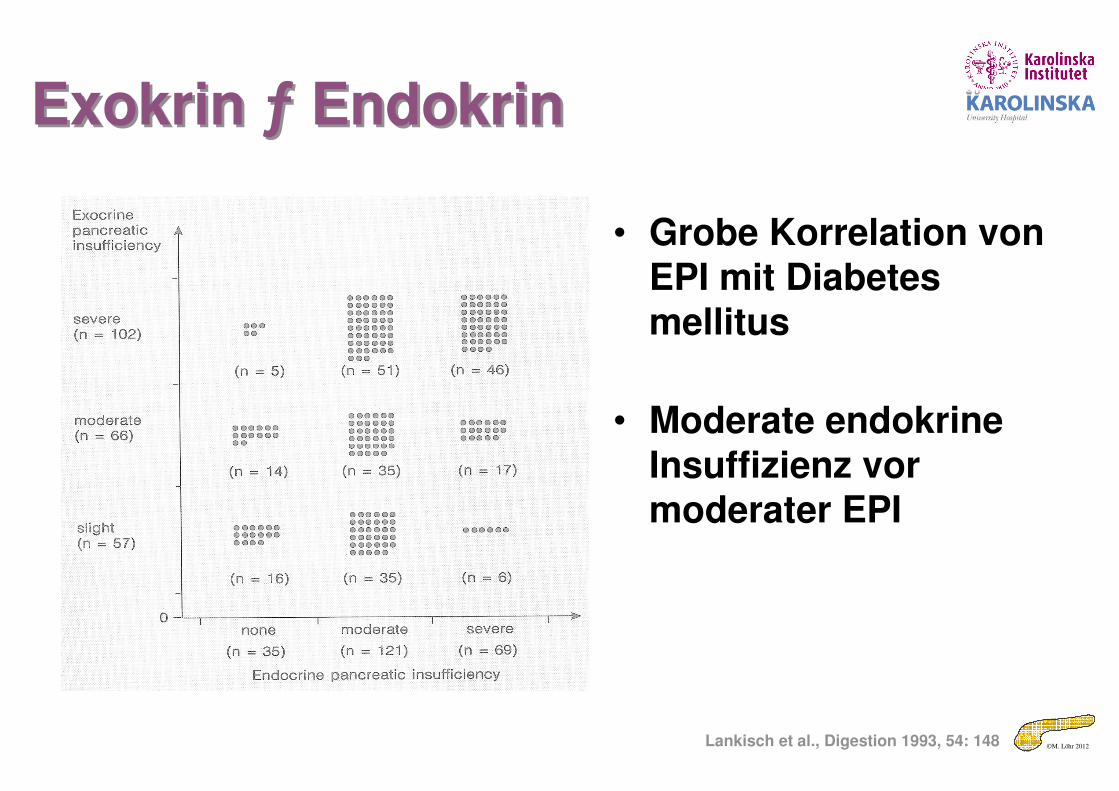
• Grobe Korrelation von EPI mit Diabetes mellitus
• Moderate endokrine Insuffizienz vor moderater EPI
Lankisch et al., Digestion 1993, 54: 148
Exokrin ƒ EndokrinExokrin ƒ Endokrin
©M. Löhr 2012
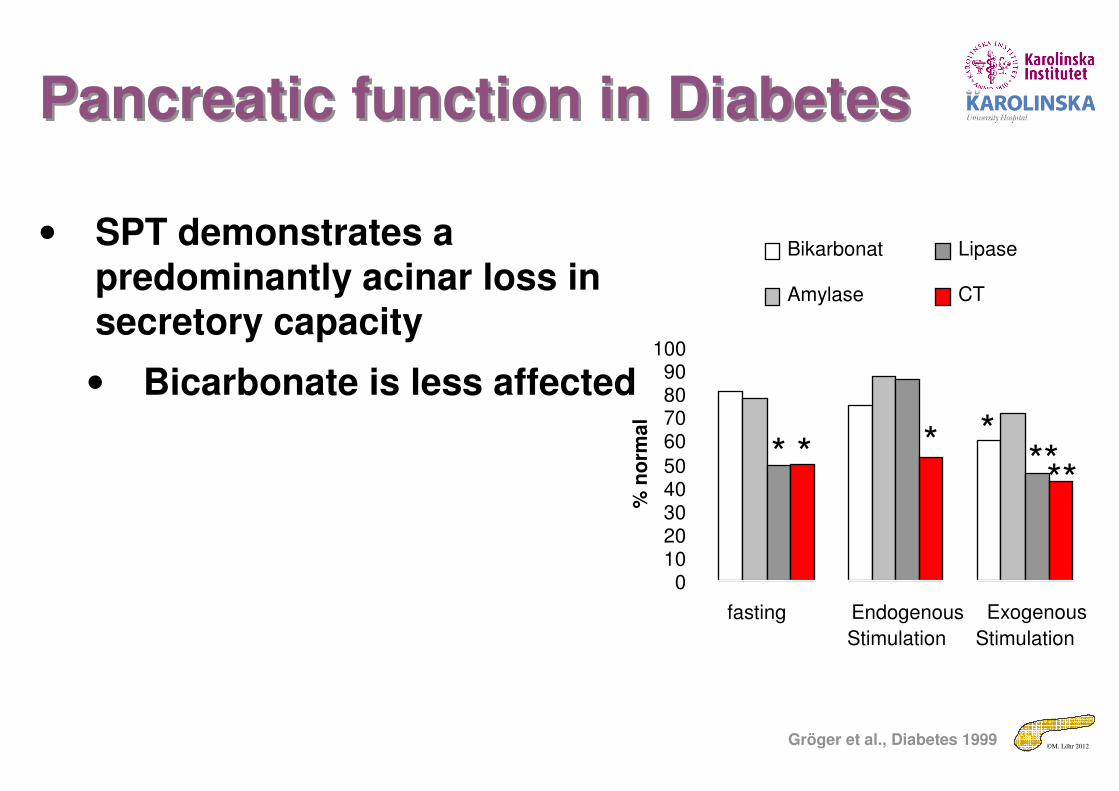
• SPT demonstrates a predominantly acinar loss in secretory capacity
• Bicarbonate is less affected
01020304050
60708090
100
fasting Endogenous
Stimulation
Exogenous
Stimulation%
no
rma
l
Bikarbonat
Amylase
Lipase
CT
* * * *****
Gröger et al., Diabetes 1999
Pancreatic function in DiabetesPancreatic function in Diabetes
©M. Löhr 2012
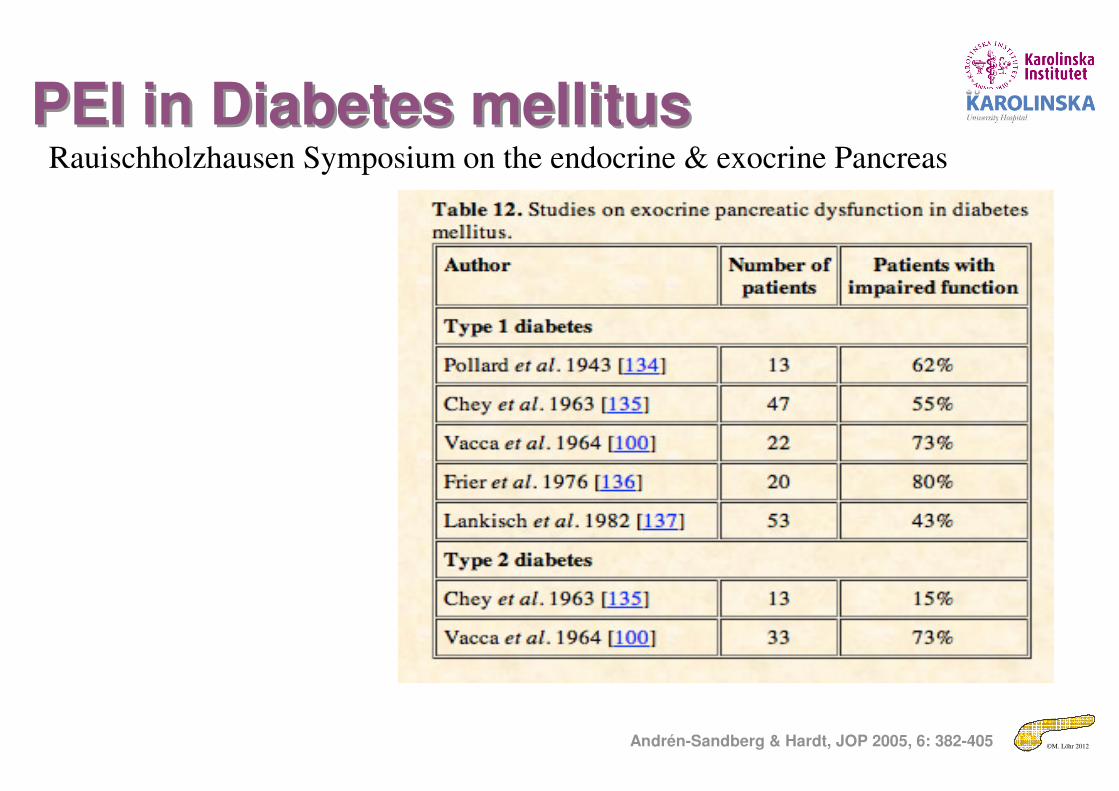
PEI in Diabetes mellitusPEI in Diabetes mellitus
Andrén-Sandberg & Hardt, JOP 2005, 6: 382-405
Rauischholzhausen Symposium on the endocrine & exocrine Pancreas
©M. Löhr 2012Löhr & Klöppel, Diabetologia 1987, 30: 757
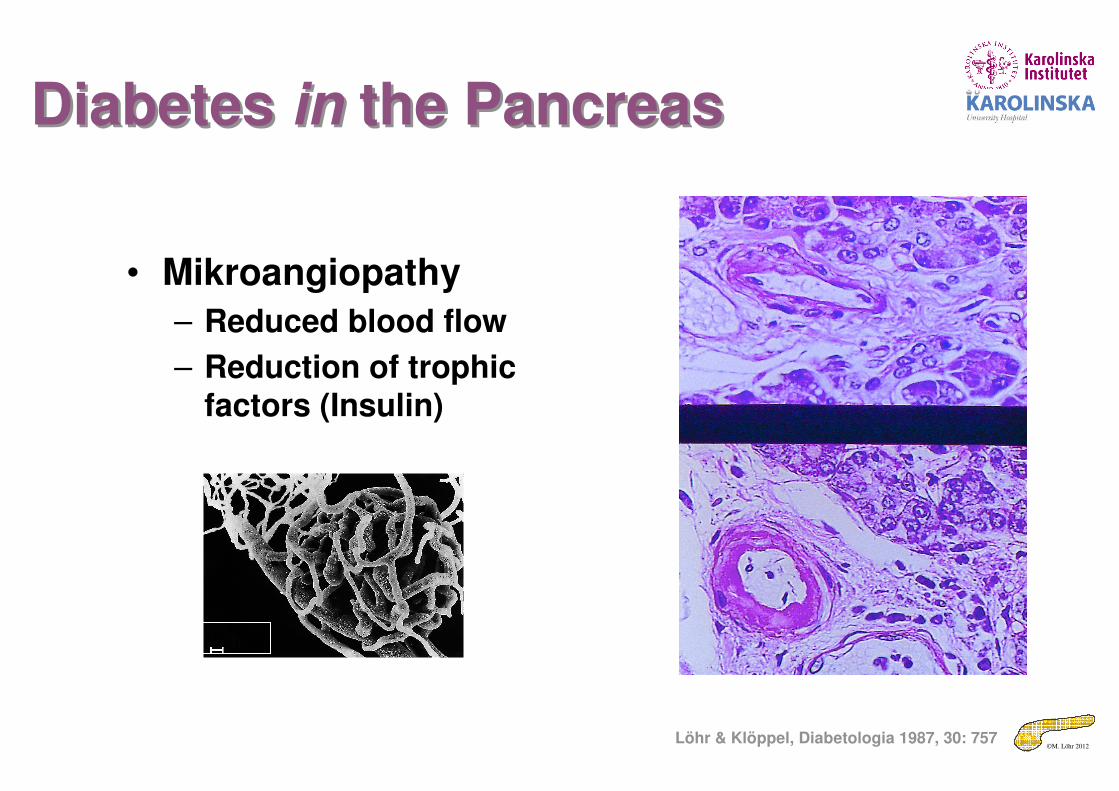
Diabetes in the PancreasDiabetes in the Pancreas
• Mikroangiopathy
– Reduced blood flow
– Reduction of trophic factors (Insulin)
100 µm
©M. Löhr 2012
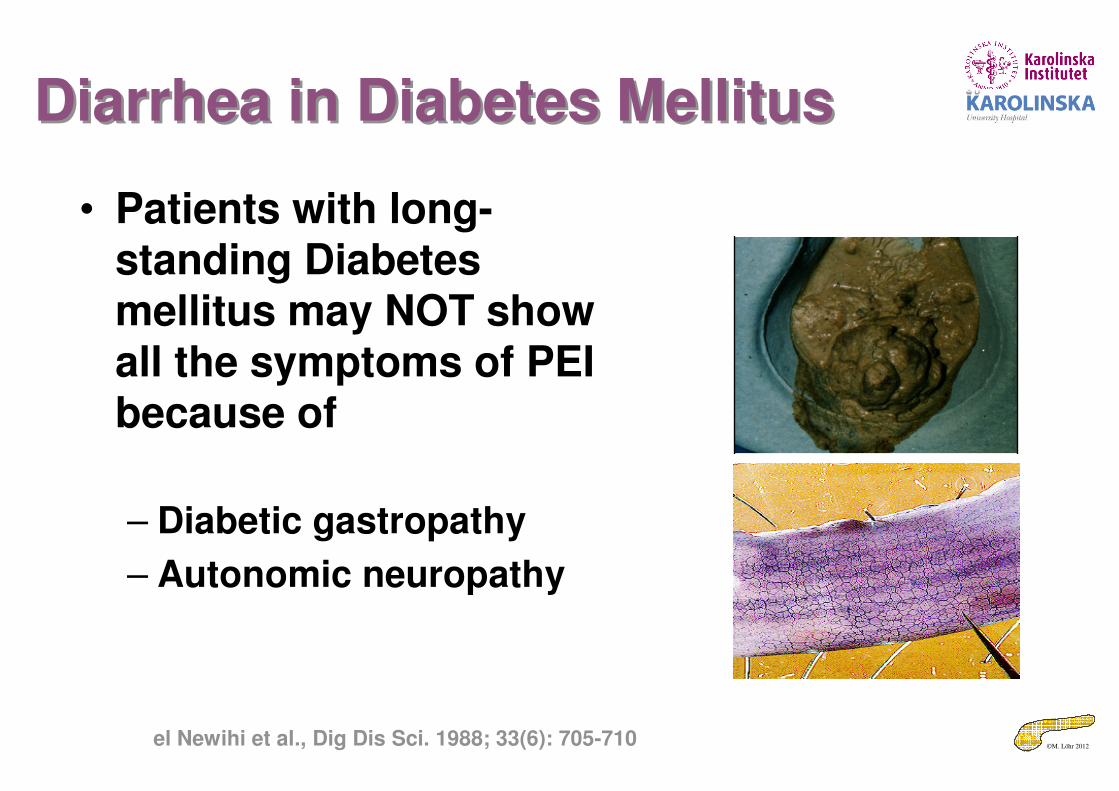
Diarrhea in Diabetes MellitusDiarrhea in Diabetes Mellitus
• Patients with long-standing Diabetes mellitus may NOT show all the symptoms of PEI because of
– Diabetic gastropathy
– Autonomic neuropathy
el Newihi et al., Dig Dis Sci. 1988; 33(6): 705-710
©M. Löhr 2012
The patient with diabetes mellitusThe patient with diabetes mellitus
• Natural course and consequences of exocrine insufficiency
©M. Löhr 2012
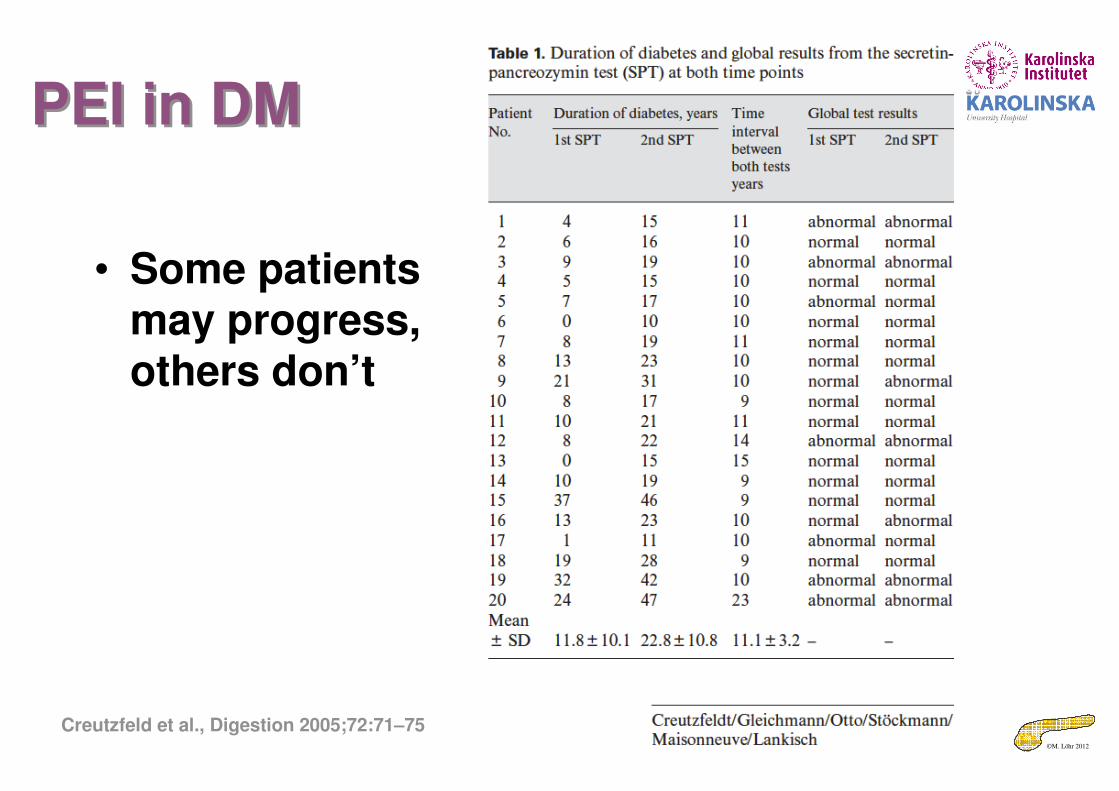
PEI in DMPEI in DM
• Some patients may progress, others don’t
Creutzfeld et al., Digestion 2005;72:71–75
©M. Löhr 2012
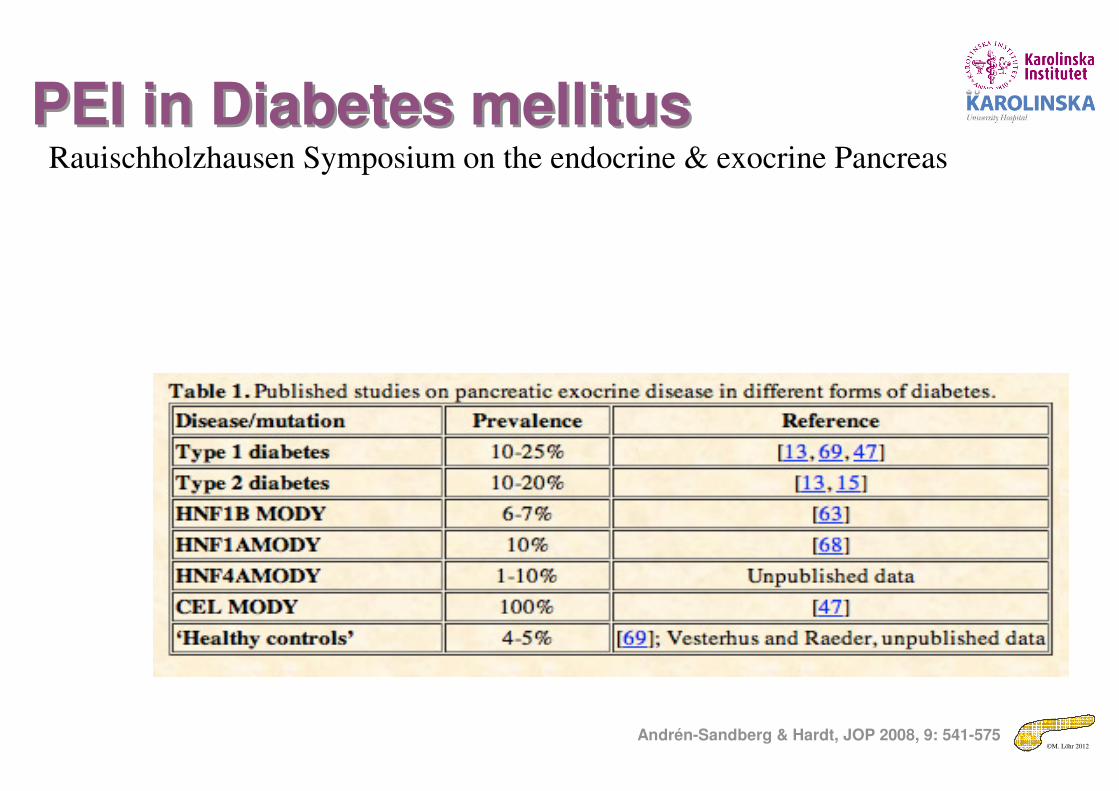
PEI in Diabetes mellitusPEI in Diabetes mellitus
Andrén-Sandberg & Hardt, JOP 2008, 9: 541-575
Rauischholzhausen Symposium on the endocrine & exocrine Pancreas
©M. Löhr 2012
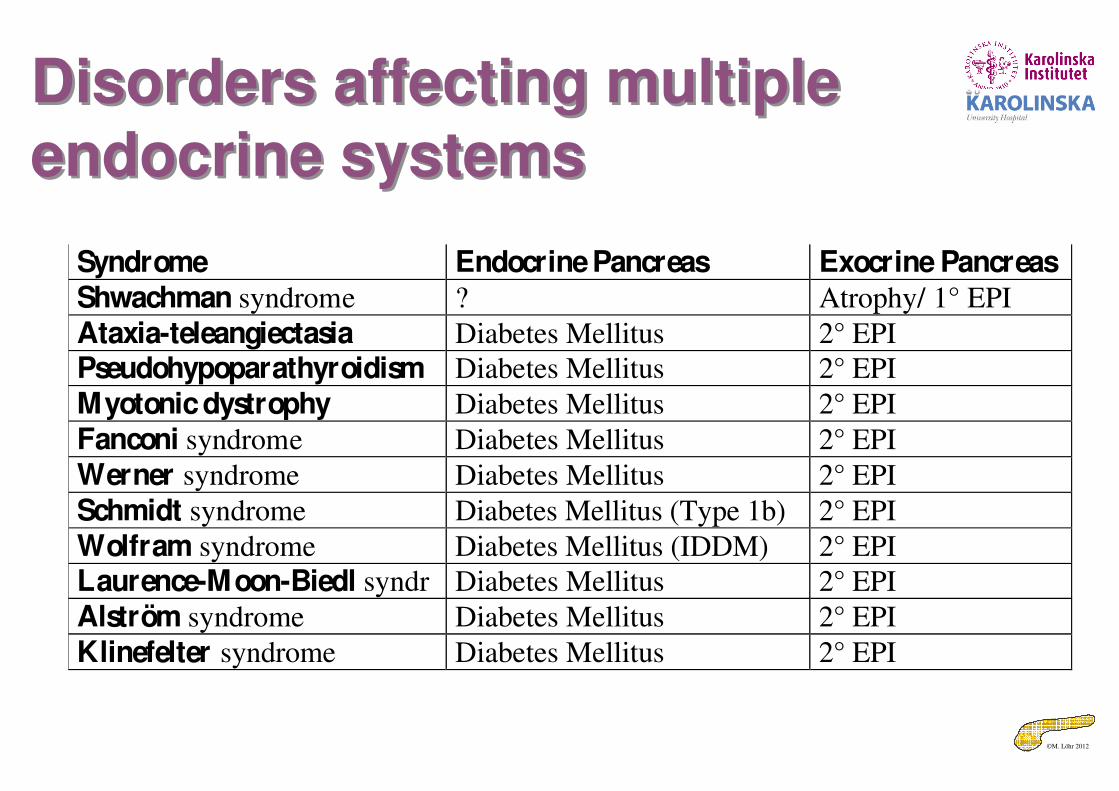
Disorders affecting multiple endocrine systems
Disorders affecting multiple endocrine systems
Syndrome Endocrine Pancreas Exocrine PancreasShwachman syndrome ? Atrophy/ 1° EPI
Ataxia-teleangiectasia Diabetes Mellitus 2° EPI
Pseudohypoparathyroidism Diabetes Mellitus 2° EPI
Myotonic dystrophy Diabetes Mellitus 2° EPI
Fanconi syndrome Diabetes Mellitus 2° EPI
Werner syndrome Diabetes Mellitus 2° EPI
Schmidt syndrome Diabetes Mellitus (Type 1b) 2° EPI
Wolfram syndrome Diabetes Mellitus (IDDM) 2° EPI
Laurence-Moon-Biedl syndr Diabetes Mellitus 2° EPI
Alström syndrome Diabetes Mellitus 2° EPI
Klinefelter syndrome Diabetes Mellitus 2° EPI
©M. Löhr 2012
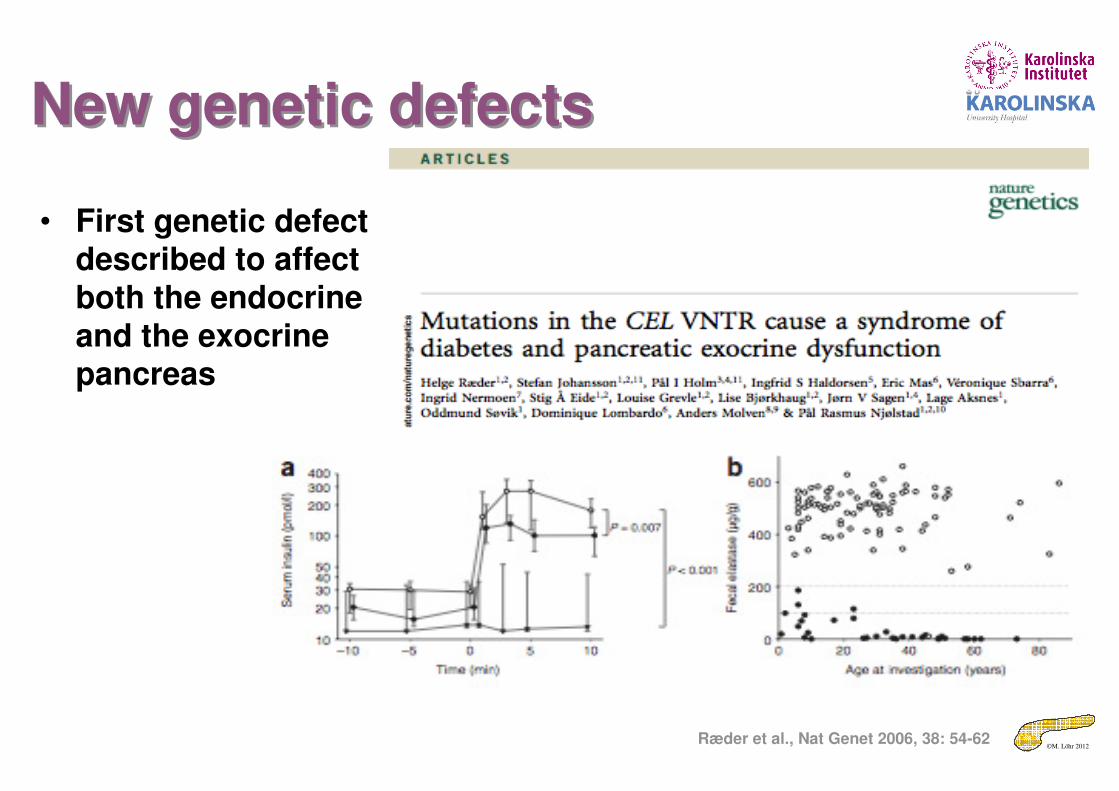
New genetic defectsNew genetic defects
• First genetic defect described to affect both the endocrine and the exocrine pancreas
Ræder et al., Nat Genet 2006, 38: 54-62
©M. Löhr 2012
BücherBücher
Thank you very much for your attention
©M. Löhr 2012
Epidemiology of chronic pancreatitisEpidemiology of chronic pancreatitis
• Incidence (new diagnoses)
– 5/100.000 inhabitants
• Prevalence (number of patients with disease)
– 25/100.000 inhabitants
• For comparison
– Diabetes: 4000/100.000 inhabitants
– Pancreatic cancer: 10/100.000 inhabitants
©M. Löhr 2012
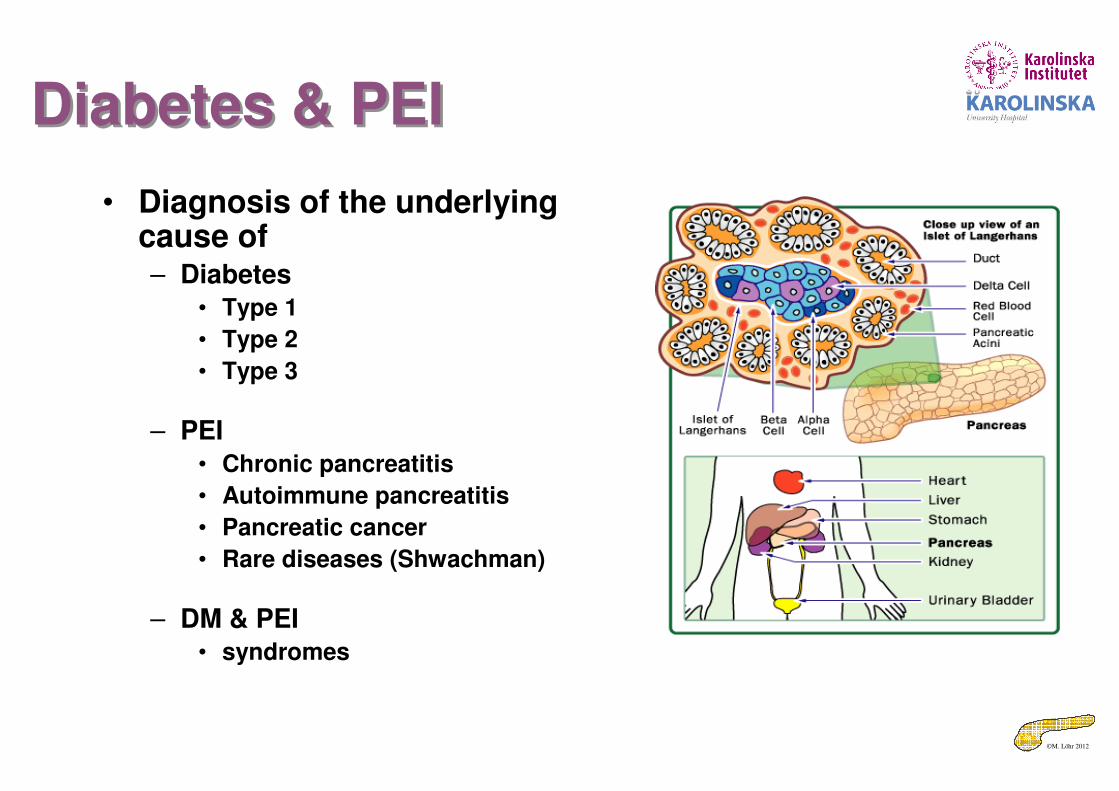
Diabetes & PEIDiabetes & PEI
• Diagnosis of the underlying cause of– Diabetes
• Type 1
• Type 2
• Type 3
– PEI• Chronic pancreatitis
• Autoimmune pancreatitis
• Pancreatic cancer
• Rare diseases (Shwachman)
– DM & PEI• syndromes
©M. Löhr 2012
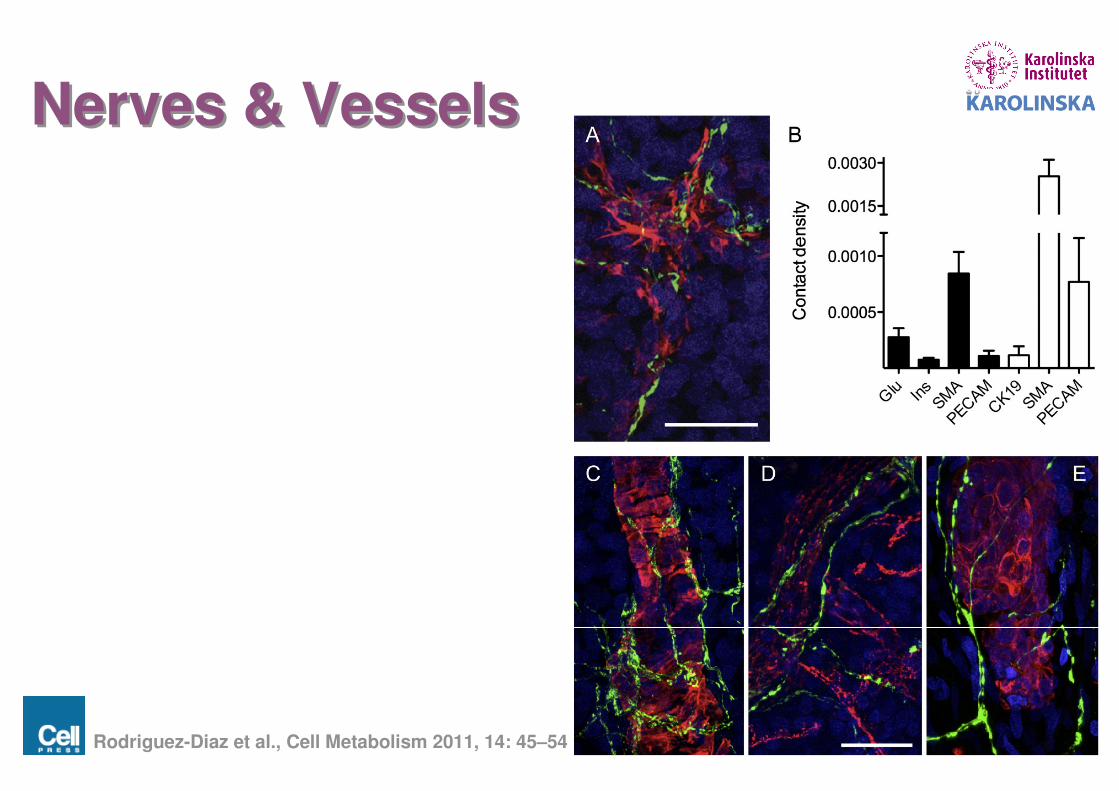
Nerves & VesselsNerves & Vessels
Rodriguez-Diaz et al., Cell Metabolism 2011, 14: 45–54
©M. Löhr 2012
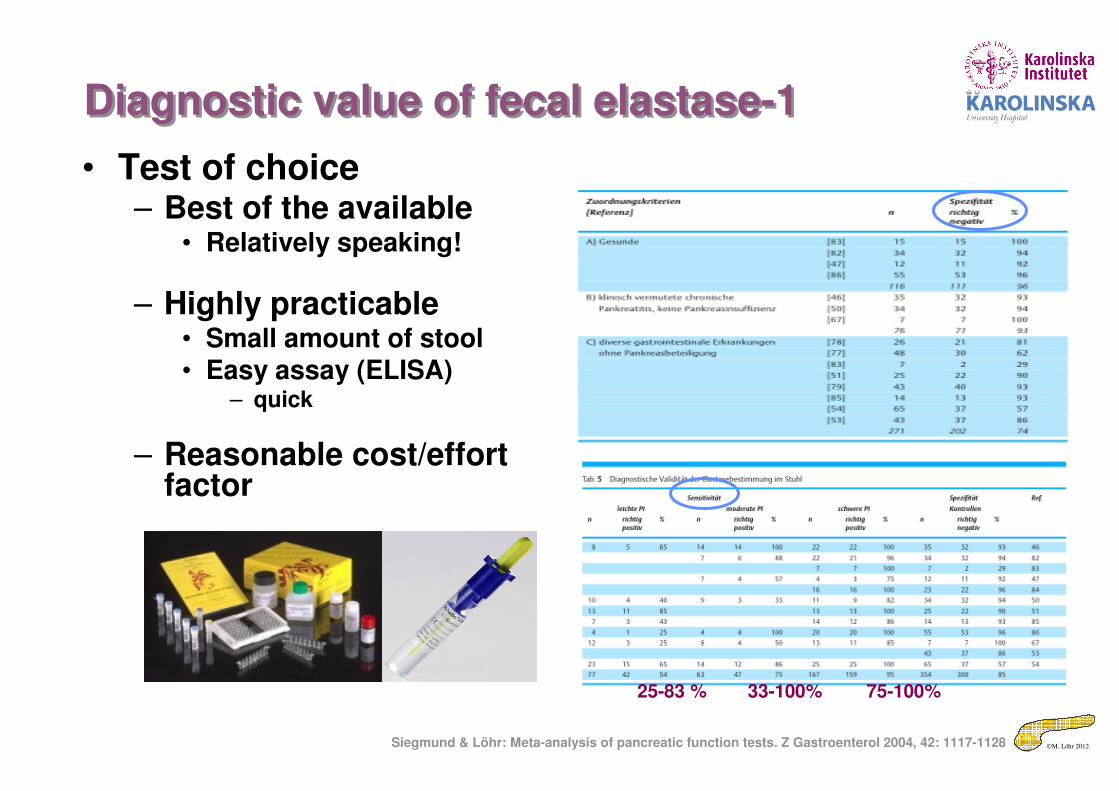
Diagnostic value of fecal elastase-1Diagnostic value of fecal elastase-1
• Test of choice– Best of the available
• Relatively speaking!
– Highly practicable• Small amount of stool• Easy assay (ELISA)
– quick
– Reasonable cost/effort factor
25-83 % 33-100% 75-100%
Siegmund & Löhr: Meta-analysis of pancreatic function tests. Z Gastroenterol 2004, 42: 1117-1128
©M. Löhr 2012
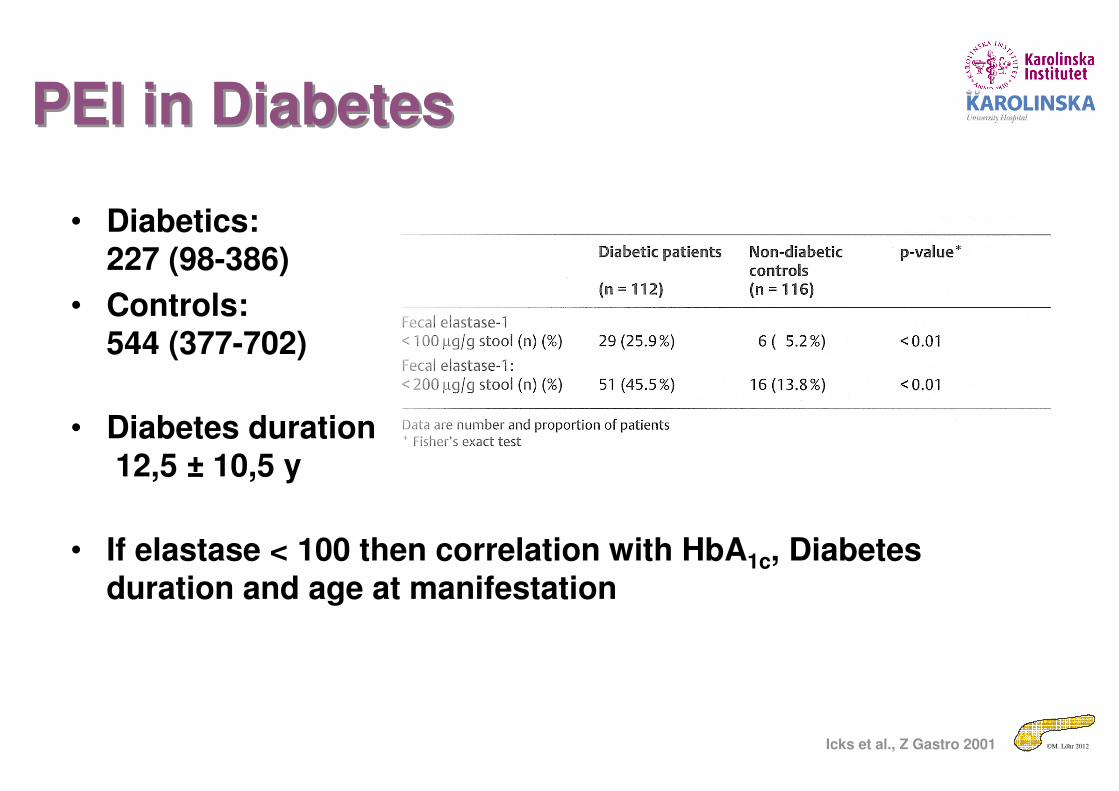
• Diabetics:227 (98-386)
• Controls:544 (377-702)
• Diabetes duration12,5 ± 10,5 y
• If elastase < 100 then correlation with HbA1c, Diabetes duration and age at manifestation
Icks et al., Z Gastro 2001
PEI in DiabetesPEI in Diabetes
©M. Löhr 2012
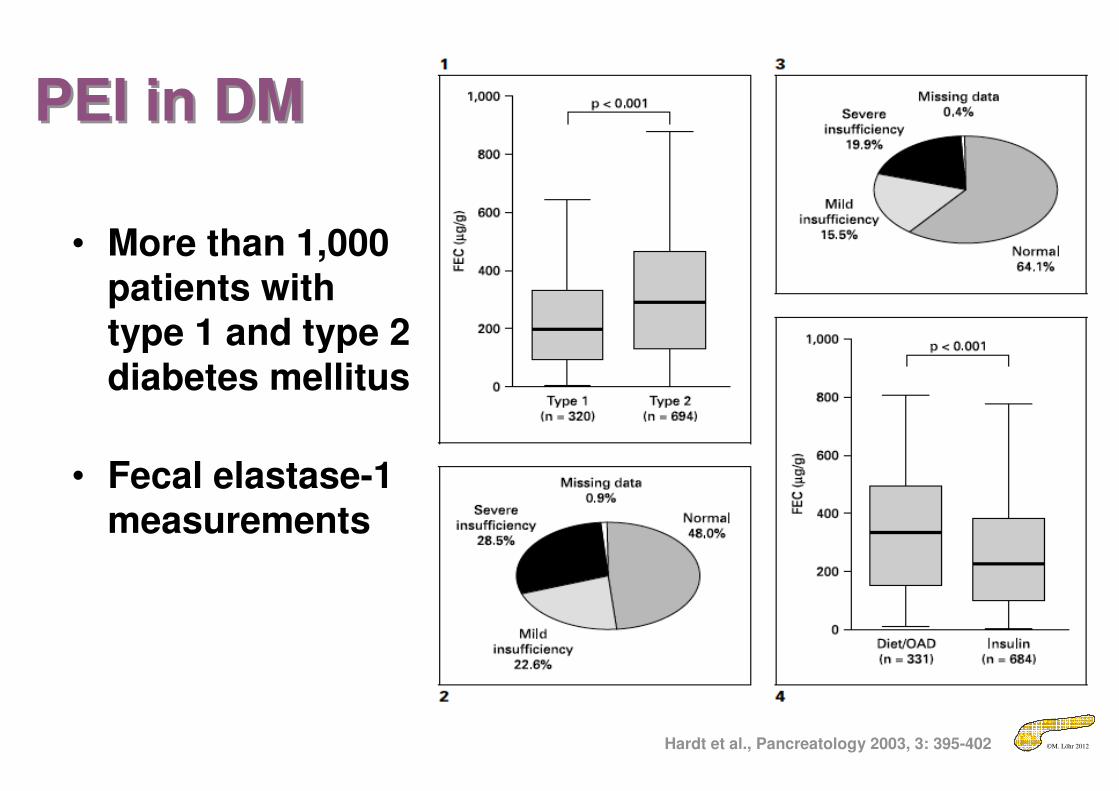
PEI in DMPEI in DM
Hardt et al., Pancreatology 2003, 3: 395-402
• More than 1,000 patients with type 1 and type 2 diabetes mellitus
• Fecal elastase-1 measurements
©M. Löhr 2012
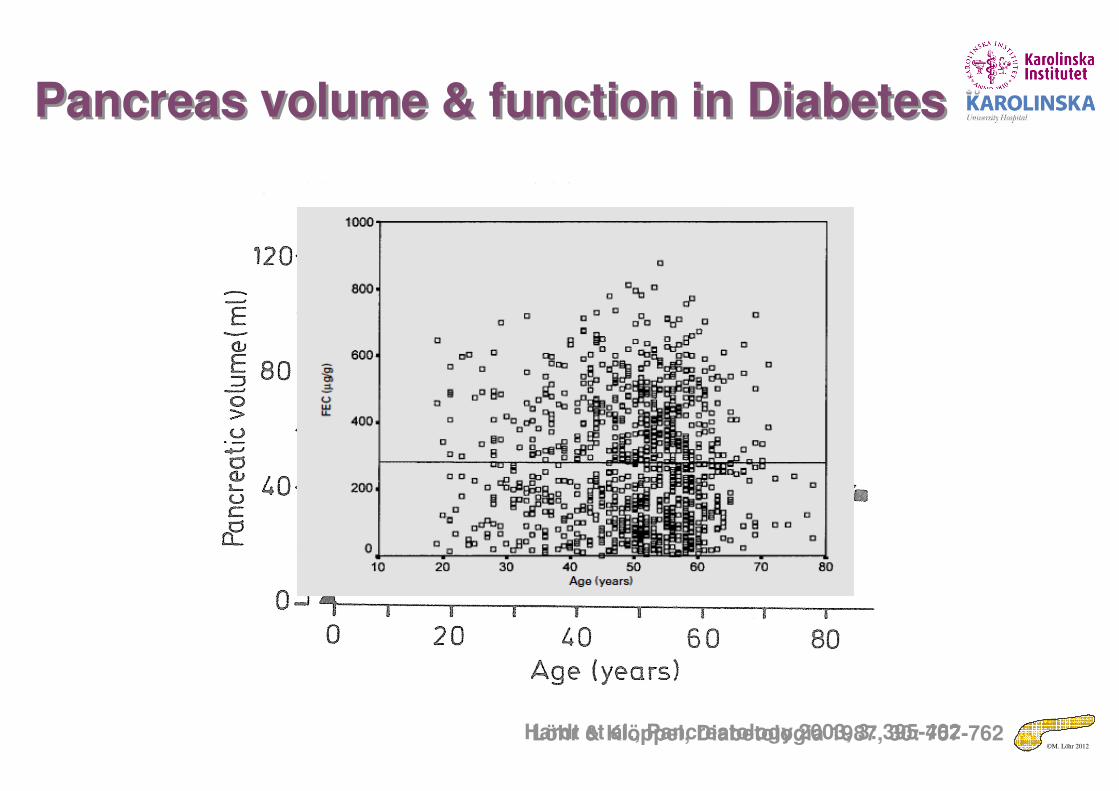
Pancreas volume & function in DiabetesPancreas volume & function in Diabetes
Löhr & Klöppel, Diabetologia 1987, 30: 757-762Hardt et al., Pancreatology 2003, 3: 395-402
©M. Löhr 2012
There is an elephant in the roomThere is an elephant in the room
• Animal also suffered from diarrhea
©M. Löhr 2012
PEI in Diabetes MellitusPEI in Diabetes Mellitus
• Mild to moderate PEI may have a clinical impact– Clinical context
• Patients with Diabetes mellitus have an increased risk to develop PEI– Pancreatic function tests should
be employed
Evidence 2b
©M. Löhr 2012
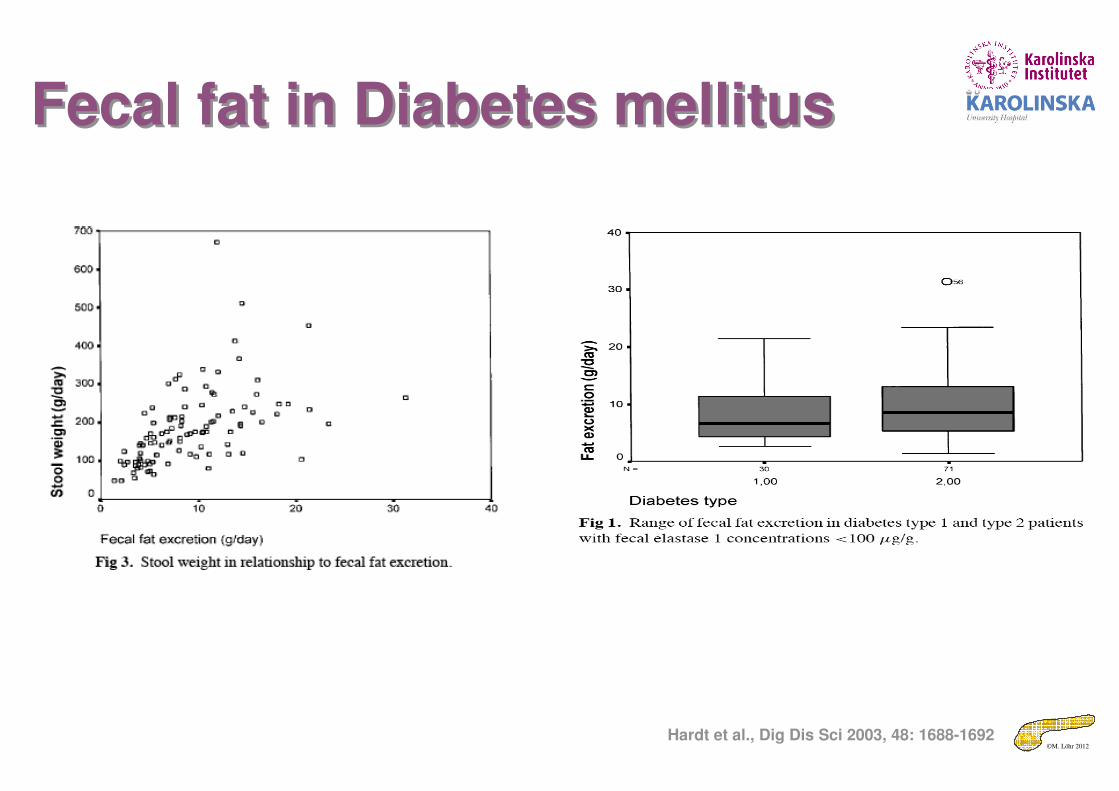
Fecal fat in Diabetes mellitusFecal fat in Diabetes mellitus
Hardt et al., Dig Dis Sci 2003, 48: 1688-1692
©M. Löhr 2012
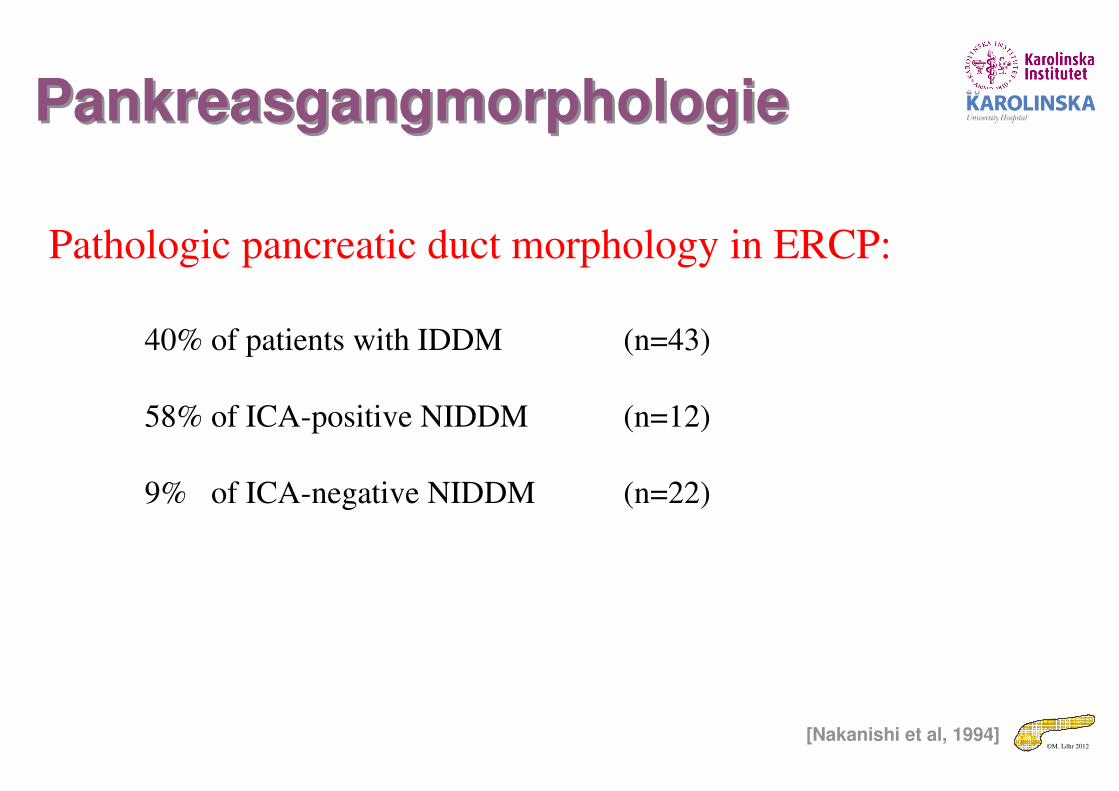
Pathologic pancreatic duct morphology in ERCP:
40% of patients with IDDM (n=43)
58% of ICA-positive NIDDM (n=12)
9% of ICA-negative NIDDM (n=22)
PankreasgangmorphologiePankreasgangmorphologie
[Nakanishi et al, 1994]













![[ger] KOHLENWASSERSTOFFE : Monatlich 11-1985 [eng] …aei.pitt.edu/80080/1/1985_-_11.pdf · 2016. 9. 30. · 501 665 371 490 438 483 347 198 486 326 434 353 3790 3065 19,1 12135 12119](https://img.pdfslide.org/doc/110x75/61232bd9c63bc323454ab026/ger-kohlenwasserstoffe-monatlich-11-1985-eng-aeipittedu8008011985-11pdf.jpg)