Embed Size (px)
Citation preview
Aus der
Klinik für Unfallchirurgie
Medizinische Hochschule Hannover
Direktor: Prof. Dr. med. C. Krettek
“Die Inzidenz ulnokarpaler Beschwerden nach distaler Radiusfraktur
in Abhängigkeit von einer Fraktur des Processus styloideus ulnae”
Dissertation zur Erlangung des
Doktorgrades der Medizin in der
Medizinischen Hochschule Hannover
vorgelegt von
Stefan Krämer
aus Hannover, 2014
Angenommen vom Senat der Medizinischen Hochschule Hannover
am
23.04.2014
Gedruckt mit Genehmigung der
Medizinischen Hochschule Hannover
Präsident: Prof. Dr. med. Christopher Baum
Betreuer: PD Dr. med. Ralph Gaulke
Referent: Prof. Dr. med. Philipp Lobenhoffer
Korreferent: Prof. Dr. med. Martinius Richter
Tag der mündlichen Prüfung:
23.04.2014
Promotionsausschussmitglieder:
PD Dr. med. Matthias Wellmann
Prof. Dr. med Claus Petersen
Prof. Dr. med Michael Winkler
Inhalt
1. Publikation ........................................................................................................................... 1
2. Die Autoren .......................................................................................................................... 9
3. Zusammenfassung .............................................................................................................. 10
3.1 Einleitung ....................................................................................... ........................................ 10
3.2 Material und Methoden ............................................................................ ............................ 12
3.3 Ergebnisse........................................................................................ ...................................... 13
3.4 Diskussion ....................................................................................... ....................................... 16
3.5 Zusammenfassung .................................................................................. ............................... 18
3.6 Literaturverzeichnis ............................................................................. .................................. 18
4. Publikationsverzeichnis .......................................................................................................... 21
5. Erklärung gemäß § 2 Abs. 2 Nr. 6 und 7 PromO ........................................................................ 22
6. Lebenslauf .............................................................................................................................. 23
7. Danksagung ............................................................................................................................ 25
The Journal of Hand Surgery(European Volume)38E(7) 710 –717© The Author(s) 2012Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1753193412469582jhs.sagepub.com
JHS(E)
Introduction
Distal radial fractures are the most common frac-tures in the upper extremity (Chung and Spilson, 2001) and are associated with a fracture of the ulnar styloid in approximately 55% of cases (May et al., 2002; Villar et al., 1987). The ulnar styloid is the ulnar anchor of the triangular fibrocartilage complex (TFCC). The TFCC preserves the congruency between distal radius, ulnar head, and proximal carpal row. It
originates at the distal edge of the sigmoid notch of the radius and runs to the base of the ulnar styloid.
The incidence of ulnocarpal complaints after distal radial fracture in relation to the fracture of the ulnar styloid
S. KrämerKlinik für Unfallchirurgie, Medizinische Hochschule, Hannover, Germany
H. MeyerKlinik für Unfallchirurgie, Medizinische Hochschule, Hannover, Germany
P. F. O’LoughlinDepartment of Orthopedic Surgery, Hospital of Special Surgery, New York, NY, USA
B. VaskeInstitut für Biometrie, Medizinische Hochschule, Hannover, Germany
C. KrettekKlinik für Unfallchirurgie, Medizinische Hochschule, Hannover, Germany
R. GaulkeKlinik für Unfallchirurgie, Medizinische Hochschule, Hannover, Germany
Abstract
Two hundred distal radial fractures, with a mean follow up of 20 months (range 6–49), were divided into three groups according to the presence and healing status of an ulnar styloid fracture. The patients underwent both clinical and radiological examination and completed two different questionnaires. One hundred and one, of 200 distal radial fractures, were associated with an ulnar styloid fracture. Forty-six of these developed an ulnar styloid nonunion. The authors encountered significantly higher pain scores (ulnar sided pain p = 0.012), a higher rate of DRUJ instability (p = 0.032), a greater loss of motion and grip strength (p = 0.001), and a poorer clinical outcome in cases with an ulnar styloid fracture, but no differences were apparent when those with healed ulnar styloid fractures or ulnar styloid nonunions were compared (p > 0.05). The investigators propose that the incidence of ulnocarpal complaints following distal radial fracture depends on the presence but not the healing status of an ulnar styloid fracture.
Keywords
Ulnar styloid fracture, processus styloideus ulnae nonunion, processus styloideus ulnae fracture, radial fracture, DRUJ
Date received: 28th August 2012; revised: 31st October 2012; accepted: 1st November 2012
Corresponding author:
Stefan Krämer, Klinik für Unfallchirurgie, Medizinische Hochschule Hannover, Stresemannallee 10, Hannover, 30173, Germany Email: [email protected]
469582 JHS38E710.1177/1753193412469582The Journal of Hand SurgeryKrämer et al.
Full length article
at MHH-Bibliothek on April 12, 2014jhs.sagepub.comDownloaded from
Krämer et al. 711
Therefore, ulnar styloid fracture may ultimately affect the clinical outcome causing instability, disability, and pain in the distal radioulnar joint (DRUJ) (af Ekenstam and Hagert, 1985; Gabl et al., 1993; Kihara et al., 1995; Melone and Nathan, 1992; Schuind et al., 1991; Shaw et al., 1990; Stoffelen et al., 1998). With that in mind, it may be prudent to pursue surgical treatment of ulnar styloid fractures to prevent wrist disability, DRUJ instability, and patients’ complaints.
To date, studies on the clinical relevance of ulnar styloid fracture have produced conflicting results. Some authors have encountered loss of grip strength and wrist mobility in cases of distal radius fractures associated with a fracture of the ulnar styloid (Belloti et al., 2009; Orhun et al., 2011; Oskarsson et al., 1997) resulting in poorer functional outcomes and Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire scores. The incidence of DRUJ instabil-ity in cases with distal radial fractures was found to be higher with concomitant ulnar styloid fractures by May et al. (2002).
Conversely, there are several studies that demon-strate no significant differences in the clinical outcome of distal radial fractures treated with open reduction and internal fixation (ORIF), with or without associated untreated ulnar styloid fractures (Belloti et al., 2009; Buijze and Ring, 2010; Kazemian et al., 2011; Kim et al., 2010a; 2010b; Reichl et al., 2010; Sammer et al., 2009; Zenke et al., 2009; Zhao et al., 2011).
The aim of the current study was to evaluate the clinical relevance of ulnar styloid fractures associated with distal radial fractures.
Methods
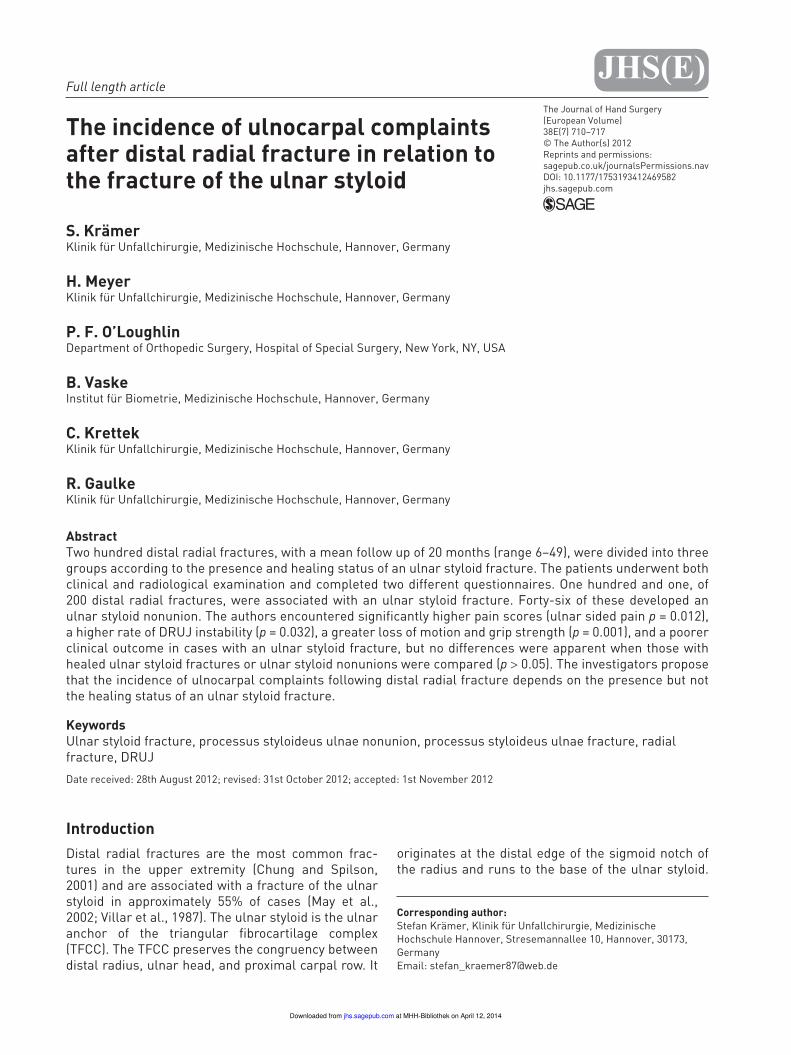
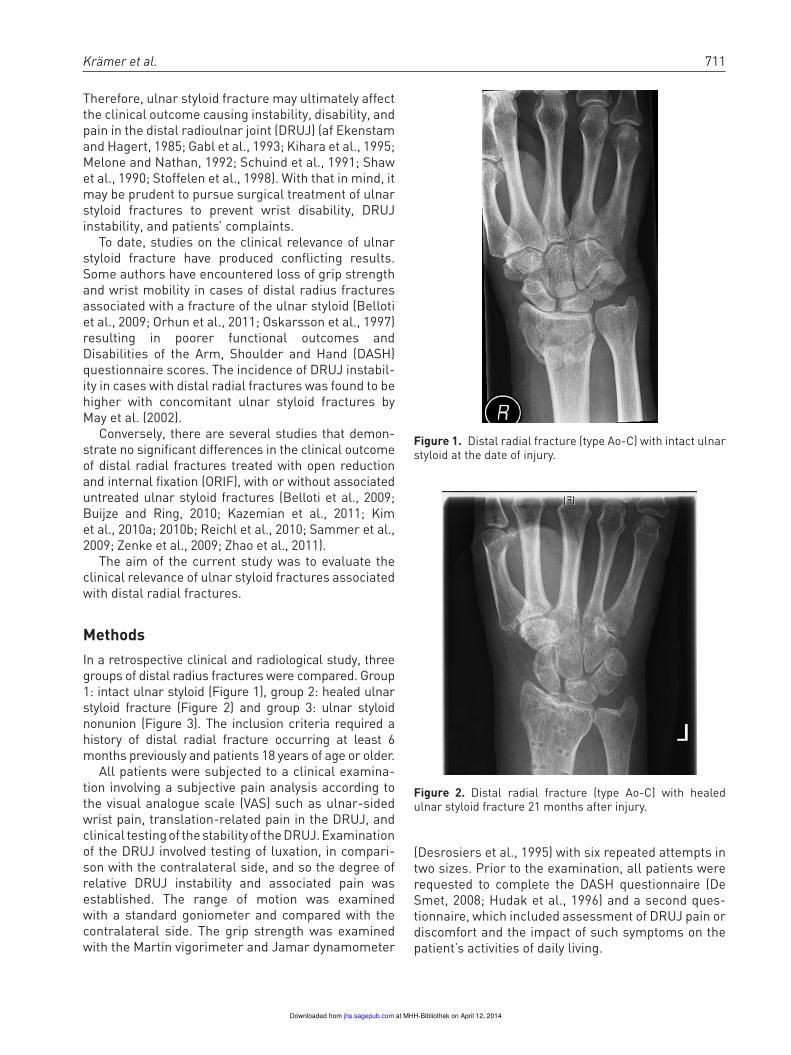
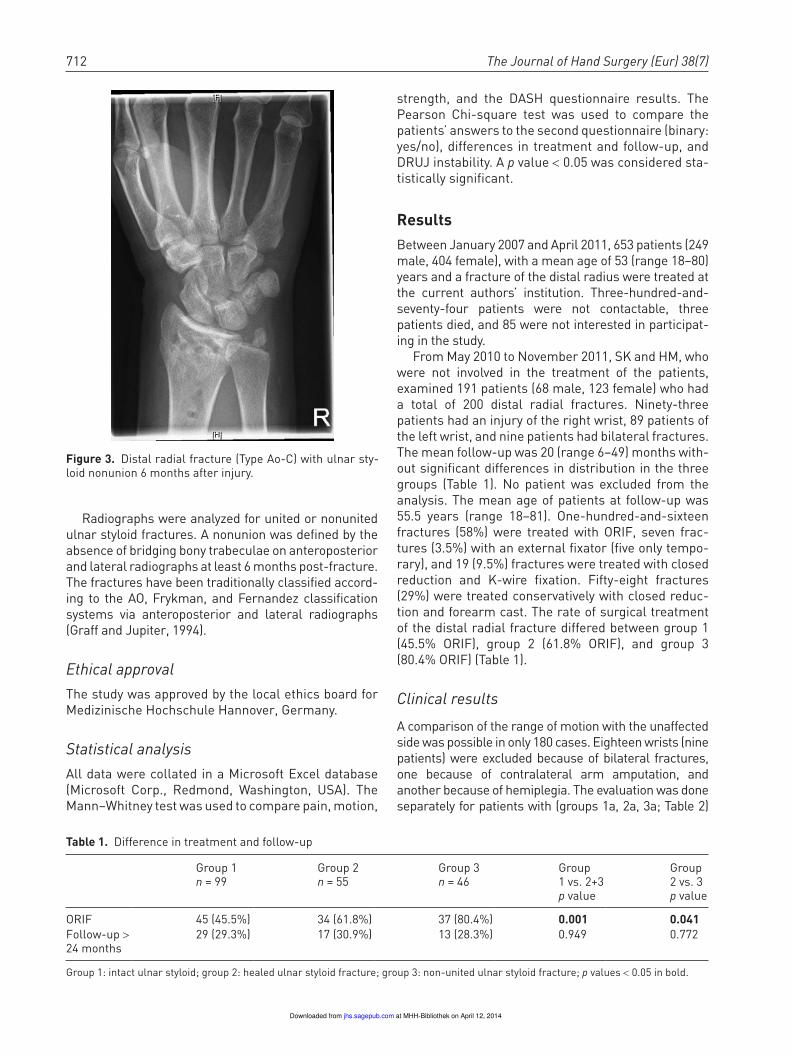
In a retrospective clinical and radiological study, three groups of distal radius fractures were compared. Group 1: intact ulnar styloid (Figure 1), group 2: healed ulnar styloid fracture (Figure 2) and group 3: ulnar styloid nonunion (Figure 3). The inclusion criteria required a history of distal radial fracture occurring at least 6 months previously and patients 18 years of age or older.
All patients were subjected to a clinical examina-tion involving a subjective pain analysis according to the visual analogue scale (VAS) such as ulnar-sided wrist pain, translation-related pain in the DRUJ, and clinical testing of the stability of the DRUJ. Examination of the DRUJ involved testing of luxation, in compari-son with the contralateral side, and so the degree of relative DRUJ instability and associated pain was established. The range of motion was examined with a standard goniometer and compared with the contralateral side. The grip strength was examined with the Martin vigorimeter and Jamar dynamometer
(Desrosiers et al., 1995) with six repeated attempts in two sizes. Prior to the examination, all patients were requested to complete the DASH questionnaire (De Smet, 2008; Hudak et al., 1996) and a second ques-tionnaire, which included assessment of DRUJ pain or discomfort and the impact of such symptoms on the patient’s activities of daily living.
Figure 1. Distal radial fracture (type Ao-C) with intact ulnar styloid at the date of injury.
Figure 2. Distal radial fracture (type Ao-C) with healed ulnar styloid fracture 21 months after injury.
at MHH-Bibliothek on April 12, 2014jhs.sagepub.comDownloaded from
712 The Journal of Hand Surgery (Eur) 38(7)
Radiographs were analyzed for united or nonunited ulnar styloid fractures. A nonunion was defined by the absence of bridging bony trabeculae on anteroposterior and lateral radiographs at least 6 months post-fracture. The fractures have been traditionally classified accord-ing to the AO, Frykman, and Fernandez classification systems via anteroposterior and lateral radiographs (Graff and Jupiter, 1994).
Ethical approval
The study was approved by the local ethics board for Medizinische Hochschule Hannover, Germany.
Statistical analysis
All data were collated in a Microsoft Excel database (Microsoft Corp., Redmond, Washington, USA). The Mann–Whitney test was used to compare pain, motion,
strength, and the DASH questionnaire results. The Pearson Chi-square test was used to compare the patients’ answers to the second questionnaire (binary: yes/no), differences in treatment and follow-up, and DRUJ instability. A p value < 0.05 was considered sta-tistically significant.
Results
Between January 2007 and April 2011, 653 patients (249 male, 404 female), with a mean age of 53 (range 18–80) years and a fracture of the distal radius were treated at the current authors’ institution. Three-hundred-and-seventy-four patients were not contactable, three patients died, and 85 were not interested in participat-ing in the study.
From May 2010 to November 2011, SK and HM, who were not involved in the treatment of the patients, examined 191 patients (68 male, 123 female) who had a total of 200 distal radial fractures. Ninety-three patients had an injury of the right wrist, 89 patients of the left wrist, and nine patients had bilateral fractures. The mean follow-up was 20 (range 6–49) months with-out significant differences in distribution in the three groups (Table 1). No patient was excluded from the analysis. The mean age of patients at follow-up was 55.5 years (range 18–81). One-hundred-and-sixteen fractures (58%) were treated with ORIF, seven frac-tures (3.5%) with an external fixator (five only tempo-rary), and 19 (9.5%) fractures were treated with closed reduction and K-wire fixation. Fifty-eight fractures (29%) were treated conservatively with closed reduc-tion and forearm cast. The rate of surgical treatment of the distal radial fracture differed between group 1 (45.5% ORIF), group 2 (61.8% ORIF), and group 3 (80.4% ORIF) (Table 1).
Clinical results
A comparison of the range of motion with the unaffected side was possible in only 180 cases. Eighteen wrists (nine patients) were excluded because of bilateral fractures, one because of contralateral arm amputation, and another because of hemiplegia. The evaluation was done separately for patients with (groups 1a, 2a, 3a; Table 2)
Figure 3. Distal radial fracture (Type Ao-C) with ulnar sty-loid nonunion 6 months after injury.
Table 1. Difference in treatment and follow-up
Group 1n = 99
Group 2n = 55
Group 3n = 46
Group1 vs. 2+3p value
Group2 vs. 3p value
ORIF 45 (45.5%) 34 (61.8%) 37 (80.4%) 0.001 0.041
Follow-up > 24 months
29 (29.3%) 17 (30.9%) 13 (28.3%) 0.949 0.772
Group 1: intact ulnar styloid; group 2: healed ulnar styloid fracture; group 3: non-united ulnar styloid fracture; p values < 0.05 in bold.
at MHH-Bibliothek on April 12, 2014jhs.sagepub.comDownloaded from
Krämer et al. 713
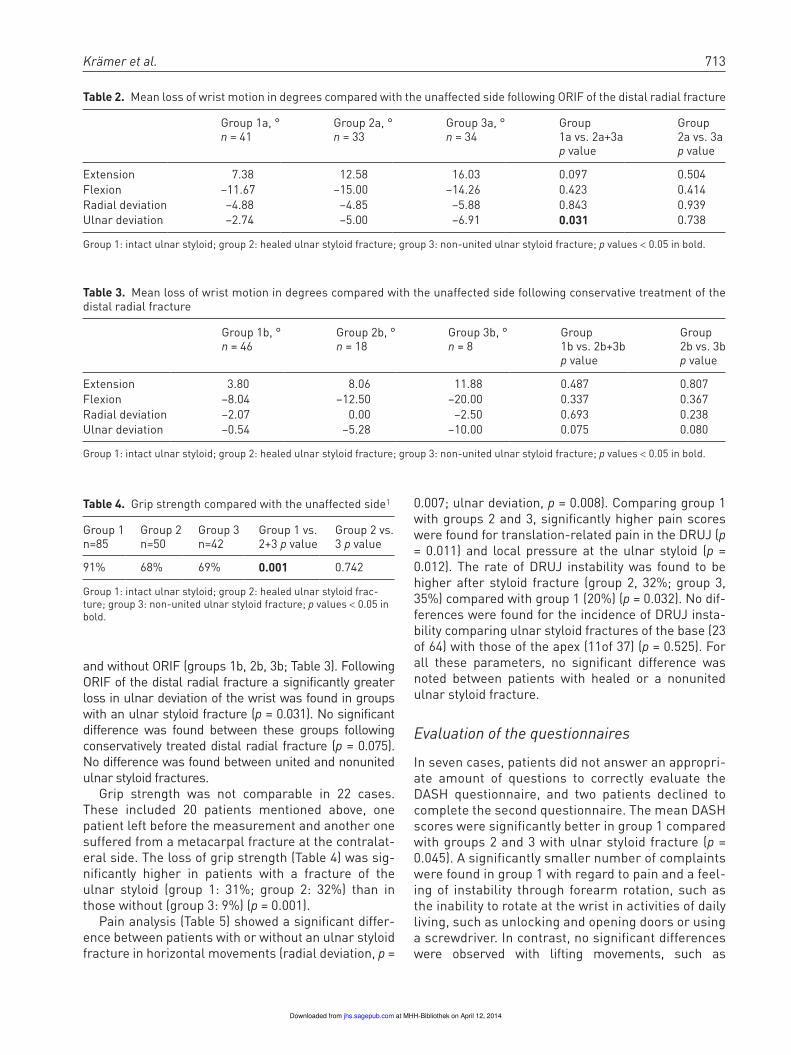
and without ORIF (groups 1b, 2b, 3b; Table 3). Following ORIF of the distal radial fracture a significantly greater loss in ulnar deviation of the wrist was found in groups with an ulnar styloid fracture (p = 0.031). No significant difference was found between these groups following conservatively treated distal radial fracture (p = 0.075). No difference was found between united and nonunited ulnar styloid fractures.
Grip strength was not comparable in 22 cases. These included 20 patients mentioned above, one patient left before the measurement and another one suffered from a metacarpal fracture at the contralat-eral side. The loss of grip strength (Table 4) was sig-nificantly higher in patients with a fracture of the ulnar styloid (group 1: 31%; group 2: 32%) than in those without (group 3: 9%) (p = 0.001).
Pain analysis (Table 5) showed a significant differ-ence between patients with or without an ulnar styloid fracture in horizontal movements (radial deviation, p =
0.007; ulnar deviation, p = 0.008). Comparing group 1 with groups 2 and 3, significantly higher pain scores were found for translation-related pain in the DRUJ (p = 0.011) and local pressure at the ulnar styloid (p = 0.012). The rate of DRUJ instability was found to be higher after styloid fracture (group 2, 32%; group 3, 35%) compared with group 1 (20%) (p = 0.032). No dif-ferences were found for the incidence of DRUJ insta-bility comparing ulnar styloid fractures of the base (23 of 64) with those of the apex (11of 37) (p = 0.525). For all these parameters, no significant difference was noted between patients with healed or a nonunited ulnar styloid fracture.
Evaluation of the questionnaires
In seven cases, patients did not answer an appropri-ate amount of questions to correctly evaluate the DASH questionnaire, and two patients declined to complete the second questionnaire. The mean DASH scores were significantly better in group 1 compared with groups 2 and 3 with ulnar styloid fracture (p = 0.045). A significantly smaller number of complaints were found in group 1 with regard to pain and a feel-ing of instability through forearm rotation, such as the inability to rotate at the wrist in activities of daily living, such as unlocking and opening doors or using a screwdriver. In contrast, no significant differences were observed with lifting movements, such as
Table 2. Mean loss of wrist motion in degrees compared with the unaffected side following ORIF of the distal radial fracture
Group 1a, °n = 41
Group 2a, °n = 33
Group 3a, °n = 34
Group1a vs. 2a+3ap value
Group2a vs. 3ap value
Extension 7.38 12.58 16.03 0.097 0.504Flexion –11.67 –15.00 –14.26 0.423 0.414Radial deviation –4.88 –4.85 –5.88 0.843 0.939Ulnar deviation –2.74 –5.00 –6.91 0.031 0.738
Group 1: intact ulnar styloid; group 2: healed ulnar styloid fracture; group 3: non-united ulnar styloid fracture; p values < 0.05 in bold.
Table 3. Mean loss of wrist motion in degrees compared with the unaffected side following conservative treatment of the distal radial fracture
Group 1b, °n = 46
Group 2b, °n = 18
Group 3b, °n = 8
Group1b vs. 2b+3bp value
Group2b vs. 3bp value
Extension 3.80 8.06 11.88 0.487 0.807Flexion –8.04 –12.50 –20.00 0.337 0.367Radial deviation –2.07 0.00 –2.50 0.693 0.238Ulnar deviation –0.54 –5.28 –10.00 0.075 0.080
Group 1: intact ulnar styloid; group 2: healed ulnar styloid fracture; group 3: non-united ulnar styloid fracture; p values < 0.05 in bold.
Table 4. Grip strength compared with the unaffected side1
Group 1 n=85
Group 2 n=50
Group 3 n=42
Group 1 vs. 2+3 p value
Group 2 vs. 3 p value
91% 68% 69% 0.001 0.742
Group 1: intact ulnar styloid; group 2: healed ulnar styloid frac-ture; group 3: non-united ulnar styloid fracture; p values < 0.05 in bold.
at MHH-Bibliothek on April 12, 2014jhs.sagepub.comDownloaded from
714 The Journal of Hand Surgery (Eur) 38(7)
carrying a bag or plate, between the groups (Table 6). The questionnaire results did not significantly dif-fer between groups 2 and 3.
Radiological results
Of a total of 200 radial fractures, 30 (15%) AO-type A, 34 (17%) type B, and 136 (68%) type C fractures, were evident. According to Frykman, these fractures were classed as 13 type I (6.5%), eight type II (4%), 27 type III (13.4%), 10 type IV (5%), 31 type V (15%), 27 type VI (13%), 32 type VII (16%), and 52 type VIII fractures (25%).
A concomitant fracture of the ulnar styloid was found in 101 cases (51%). Seventy-eight percent of all ulnar styloid fractures had an associated multiple fragmented intra-articular radial fracture (AO-type C). In 46 (46%) cases, an ulnar styloid nonunion was detected. The Fernandez classification stratified these injuries into 32 type 1a, five type 1b, four type 2a, 59 type 2b, and one type 3a fracture.
Discussion
The aim of the current study was to evaluate the clini-cal relevance of ulnar styloid fractures associated
with distal radial fractures. The results suggest that a fracture of the ulnar styloid in combination with a dis-tal radial fracture is an indicator for poorer prelimi-nary clinical outcomes.
This is especially relevant to motions and actions that stress the DRUJ, such as forearm rotation, ulnar deviation, or DRUJ translation, cause pain in these patients. This could be due to a lesion of the TFCC and soft tissue damage. TFCC lesions were demonstrated by Geissler (1995) via arthroscopy in four of 25 cases with an ulnar styloid fracture and three of 35 without. Lindau et al. (1997) found 39 TFCC tears in 50 distal radial fractures with a statistical correlation to an avulsed ulnar styloid. In 24 of 27 distal radial frac-tures with an associated ulnar styloid fracture, TFCC tears were found, but only 15 TFCC tears were found in 23 wrist with an intact ulnar styloid (p = 0.05). Another explanation for the higher rate of complaints following ulnar styloid fracture in the current study may be the higher rate of concomitant severe frac-tures of the distal radius (80% AO-type C fractures) and a consequent higher rate of ORIF, which in itself could explain the poor outcomes. These results are consistent with those of Belloti et al. (2009), who found worse DASH scores and more wrist pain at a follow-up of 24 months in their analysis of 100 patients
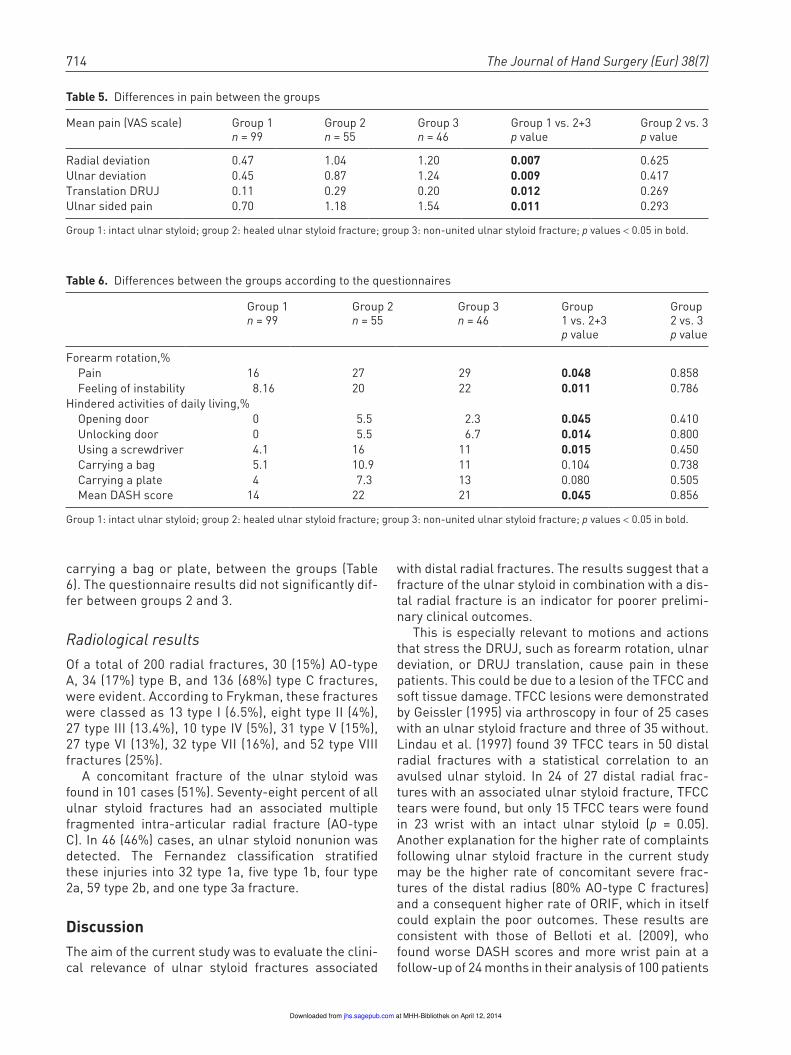
Table 5. Differences in pain between the groups
Mean pain (VAS scale) Group 1 n = 99
Group 2 n = 55
Group 3 n = 46
Group 1 vs. 2+3 p value
Group 2 vs. 3 p value
Radial deviation 0.47 1.04 1.20 0.007 0.625Ulnar deviation 0.45 0.87 1.24 0.009 0.417Translation DRUJ 0.11 0.29 0.20 0.012 0.269Ulnar sided pain 0.70 1.18 1.54 0.011 0.293
Group 1: intact ulnar styloid; group 2: healed ulnar styloid fracture; group 3: non-united ulnar styloid fracture; p values < 0.05 in bold.
Table 6. Differences between the groups according to the questionnaires
Group 1n = 99
Group 2n = 55
Group 3n = 46
Group1 vs. 2+3p value
Group2 vs. 3p value
Forearm rotation,% Pain 16 27 29 0.048 0.858 Feeling of instability 8.16 20 22 0.011 0.786Hindered activities of daily living,% Opening door 0 5.5 2.3 0.045 0.410 Unlocking door 0 5.5 6.7 0.014 0.800 Using a screwdriver 4.1 16 11 0.015 0.450 Carrying a bag 5.1 10.9 11 0.104 0.738 Carrying a plate 4 7.3 13 0.080 0.505 Mean DASH score 14 22 21 0.045 0.856
Group 1: intact ulnar styloid; group 2: healed ulnar styloid fracture; group 3: non-united ulnar styloid fracture; p values < 0.05 in bold.
at MHH-Bibliothek on April 12, 2014jhs.sagepub.comDownloaded from

Krämer et al. 715
with distal radial fractures. This is similar to the mean follow-up of 20 months in the current study. Oskarsson et al. (1997) also demonstrated a greater loss of wrist mobility and grip strength in cases of distal radial fractures with a concomitant fracture of the ulnar sty-loid. A significantly greater loss of flexion in cases with a fracture of the ulnar styloid was noted by Villar et al. (1987) in 90 patients 3 years after Colles’ frac-ture. Instability of the DRUJ was significantly more frequent according to May et al. (2002) following anal-ysis with CT scan and clinical examination in distal radial fractures with ulnar styloid involvement.
Several authors report on the influence of ulnar styloid fractures on clinical outcomes (Lindau et al., 2000b; Stoffelen et al., 1998). In the current study, the complaints of the ulnar wrist and DRUJ instabil-ity did not depend on the location of the ulnar styloid fracture.
Dislocation of the ulnar styloid as it pertains to the clinical outcome was investigated by Orhun et al. (2011) in 44 combined distal radial and ulnar styloid fractures. They found that ulnar styloid displacement exerted a negative effect on both Gartland and Werley scores (Gartland and Werley, 1951) and upon the radi-ological result according to Steward’s radiological scoring method (Stewart et al., 1985) at a mean fol-low-up of 18 weeks.
There have been conflicting results reported in the literature, however. Although there is a higher rate of DRUJ instability in the current investigators’ study groups with an ulnar styloid fracture, Scheer and Adolfsson (2011) concluded that an ulnar styloid frac-ture does not influence the clinical outcome (DASH, VAS) after 2 years following a study of 40 patients with an undisplaced radial fracture, with 20 patients exhib-iting pathological laxity in the DRUJ. Reichl et al. (2010) analysed data from 238 patients with a distal radial fracture in a combined retro- and prospective study that looked at functional and radiological results, such as the Gartland–Werley, Castaing (1964), and DASH scores, at a minimum follow-up of 1 year. They did not find any significant differences between the groups with a fracture of the ulnar styloid tip or base, or an intact ulnar styloid. Kazemian et al. (2011) tested the stability of the DRUJ in 112 cases of distal radial fractures treated by ORIF, of which 26 had an ulnar styloid fracture, with the aid of CT and found no significant correlation between ulnar styloid fractures and DRUJ instability at a follow-up of only 3 months. A similar conclusion was proposed by Zhao et al. (2011), who compared three groups of distal radial fractures 3 months and 1 year after ORIF. Their 20 cases with-out ulnar styloid fractures showed equal clinical and radiological results compared with 12 cases with a
fracture of the tip of the ulnar styloid and the 10 cases with a fracture of the ulnar styloid’s base. Roysam (1993) studied the influence of DRUJ involvement in Colles’ fractures and found no effect from an ulnar styloid fracture on functional outcome at a follow-up of 6 weeks, 6 months, and 1 year. Souer et al. (2009) compared two matched cohorts with 76 patients and found that a fracture of the ulnar styloid base does not affect the overall clinical outcome. In contrast, they found a loss of grip strength in the first 6 months such as a deficit in wrist flexion and ulnar deviation for 24 months after surgical treatment. That is consistent with the findings in the current study. They did not analyze instability in the distal radioulnar joint.
Kim et al. (2010a), in a study of 138 consecutive patients with distal radial fractures at a mean follow-up of 19 months, found no correlation between the presence, displacement, or level of ulnar styloid frac-ture and functional outcome. Using the Michigan Hand Outcome Questionnaire (Chung et al., 1999), Sammer et al. (2009) found that patients’ complaints did not depend on the presence or healing status of concomitant ulnar styloid fractures in their series of 144 distal radial fractures treated by ORIF in a pro-spective study between 6 weeks and 1 year postoper-atively. Zenke et al. (2009) compared three groups of distal radial fractures treated with palmar locking plates and did not find any significant difference between a fracture of the ulnar styloid base or tip, and no ulnar styloid fracture. Their 118 patients were examined with regard to grip strength, range of move-ment, and DASH score. They also found no evidence that an ulnar styloid nonunion leads to ulnar-sided wrist pain.
The effect of an ulnar styloid nonunion was the secondary focus in the current study. The incidence of ulnar styloid nonunions was 46%, which is consistent with rates ranging from 22% to 63% reported in the literature (Bacorn and Kurtzke, 1953; Buijze and Ring, 2010a; Catalano et al., 1997; Geissler et al., 1996; Kim et al., 2010a; Reichl et al., 2010).
In the current study, it appeared that the overall clinical result did not depend on the healing status of the ulnar styloid. Lindau et al. (2000a) also reported that both fracture and nonunion of the ulnar styloid were not correlated with DRUJ instability. Buijze and Ring (2010) analyzed the clinical outcome of 36 patients with ulnar styloid fractures and demon-strated no significant differences in the Gartland and Werley, DASH, and Mayo scores, as well as in the 10 point ordinal pain scale, grip strength, or motion between healed ulnar styloid fractures or ulnar sty-loid nonunion. Similar results and an additional anal-ysis of DRUJ instability were reported by Kim et al.
at MHH-Bibliothek on April 12, 2014jhs.sagepub.comDownloaded from

716 The Journal of Hand Surgery (Eur) 38(7)
(2010b). They noted that 78% of ulnar styloid nonun-ions in a group of 91 patients with ORIF-treated distal radial fracture and ulnar styloid avulsion exhibited similar clinical outcome compared with those with an ulnar styloid fracture union. Seventeen of 44 patients who developed an ulnar styloid nonunion in a study by Orhun et al. (2011) showed no differences in clinical outcomes compared with those with a united healed ulnar styloid fracture.
The statement that an ulnar styloid nonunion may cause DRUJ instability and worse functional results is based on the presence of TFCC tears and the supposi-tion that bone fragments could provoke irritation and pain. Extensor carpi ulnaris tendon impingement caused by malalignment of a fibrous nonunion may also be responsible for a poor clinical outcome (Burgess and Watson, 1988; Hauck et al., 1996; Kim et al., 2010b; Protopsaltis and Ruch, 2010). Tsukazaki and Iwasaki (1993) found an ulnar styloid nonunion in 13 of 17 cases, with ulnar head instability in 109 patients with distal radial fractures. Abid et al. (2008) found six patients with a poor clinical outcome of their 46 juvenile ulnar styloid fractures, which all showed nonunion. They attributed a TFCC tear as the reason for their complaints. Nakamura et al. (1998) fixed dis-placed ulnar styloid fractures in four wrists and cited a benefit in all from this surgical treatment. Those results were consistent with that of Hauck et al. (1996), who treated 20 symptomatic ulnar styloid fractures with excision (17 cases) or ORIF (three cases). All but one patient showed excellent or good results at the mean follow-up period of 64 months. These results were not in keeping with the results of the current study, but those groups analyzed only symptomatic cases of a fractured ulnar styloid in small patient cohorts.
The current study has certain limitations. It is ret-rospective in nature. The three groups that were com-pared were not matched, and there were no exclusion criteria with regard to the treatment, fracture type, and remaining dislocation of the distal radial fracture, which may have influenced the results (Finsen et al., 2012). The patients ultimately decided themselves whether to participate in the study or not, and this might have caused a certain selection bias towards patients with complaints.
In this study, the current authors found that the incidence of ulnocarpal complaints after distal radial fracture depends on the presence but not on the healing status of the ulnar styloid fracture. Nevertheless, there exists a great deal of speculation on the reasons for ulnar-sided wrist pain and an association with ulnar styloid fracture in the litera-ture. The current authors believe that a prospective, randomized study of a greater number of patients,
with the inclusion of MRI or wrist arthroscopy, is warranted to generate more information on the pathology of ulnar wrist pain.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Ethical approval
The study was approved by the local ethics board for Medizinische Hochschule Hannover, Germany.
Note
1. Mean of with six repeated attempts in two sizes of each three with Martin vigorimeter and the JAMAR dynamometer
References
Abid A, Accadbled F, Kany J, de Gauzy JS, Darodes P, Cahuzac JP. Ulnar styloid fracture in children: a retro-spective study of 46 cases. J Pediatr Orthop B. 2008, 17: 15–9.
af Ekenstam F, Hagert CG. Anatomical studies on the geom-etry and stability of the distal radio ulnar joint. Scand J Plast Reconstr Surg. 1985, 19: 17–25.
Bacorn RW, Kurtzke JF. Colles’ fracture; a study of two thousand cases from the New York State Workmen’s Compensation Board. J Bone Joint Surg Am. 1953, 35-A: 643–58.
Belloti JC, Moraes VY, Albers MB, Faloppa F, Dos Santos JB. Does an ulnar styloid fracture interfere with the results of a distal radius fracture? J Orthop Sci. 2009, 15: 216–22.
Buijze GA, Ring D. Clinical impact of united versus nonu-nited fractures of the proximal half of the ulnar styloid following volar plate fixation of the distal radius. J Hand Surg Am. 2010, 35: 223–7.
Burgess RC, Watson HK. Hypertrophic ulnar styloid nonun-ions. Clin Orthop Relat Res. 1988: 215–7.
Castaing J. [Recent fractures of the lower extremity of the radius in adults]. Rev Chir Orthop Reparatrice Appar Mot. 1964, 50: 581–696.
Catalano LW, 3rd, Cole RJ, Gelberman RH, Evanoff BA, Gilula LA, Borrelli J, Jr. Displaced intra-articular frac-tures of the distal aspect of the radius. Long-term results in young adults after open reduction and internal fixation. J Bone Joint Surg Am. 1997, 79: 1290–302.
Chung KC, Hamill JB, Walters MR, Hayward RA. The Michigan Hand Outcomes Questionnaire (MHQ): assess-ment of responsiveness to clinical change. Ann Plast Surg. 1999, 42: 619–22.
Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am. 2001, 26: 908–15.
at MHH-Bibliothek on April 12, 2014jhs.sagepub.comDownloaded from
Krämer et al. 717
De Smet L. The DASH questionnaire and score in the evalu-ation of hand and wrist disorders. Acta Orthop Belg. 2008, 74: 575–81.
Desrosiers J, Hebert R, Bravo G, Dutil E. Comparison of the Jamar dynamometer and the Martin vigorimeter for grip strength measurements in a healthy elderly population. Scand J Rehabil Med. 1995, 27: 137–43.
Finsen V, Rod O, Rod K, Rajabi B, Alm-Paulsen PS, Russwurm H. The relationship between displacement and clinical outcome after distal radius (Colles’) frac-ture. J Hand Surg Eur Vol. 2012 (epub).
Gabl M, Lener M, Pechlaner S, Kathrein A, Judmaier W. [Destabilization of the discus articularis with rupture of the ulnar styloid apex in distal radius fracture. Diagnosis with dynamic MR]. Unfallchirurgie. 1993, 19: 108–11.
Gartland JJ, Jr., Werley CW. Evaluation of healed Colles’ fractures. J Bone Joint Surg Am. 1951, 33-A: 895–907.
Geissler WB. Arthroscopically assisted reduction of intra-articular fractures of the distal radius. Hand Clin. 1995, 11: 19–29.
Geissler WB, Fernandez DL, Lamey DM. Distal radioul-nar joint injuries associated with fractures of the distal radius. Clin Orthop Relat Res. 1996: 135–46.
Graff S, Jupiter J. Fracture of the distal radius: classifica-tion of treatment and indications for external fixation. Injury. 1994, 25 Suppl 4: S-D14–25.
Hauck RM, Skahen J, 3rd, Palmer AK. Classification and treatment of ulnar styloid nonunion. J Hand Surg Am. 1996, 21: 418–22.
Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (Disabilities of the Arm, Shoulder and Hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med. 1996, 29: 602–8.
Kazemian GH, Bakhshi H, Lilley M et al. DRUJ instability after distal radius fracture: A comparison between cases with and without ulnar styloid fracture. Int J Surg. 2011, 9: 648–51.
Kihara H, Short WH, Werner FW, Fortino MD, Palmer AK. The stabilizing mechanism of the distal radioulnar joint during pronation and supination. J Hand Surg Am. 1995, 20: 930–6.
Kim JK, Koh YD, Do NH. Should an ulnar styloid fracture be fixed following volar plate fixation of a distal radial frac-ture? J Bone Joint Surg Am. 2010a, 92: 1–6.
Kim JK, Yun YH, Kim DJ, Yun GU. Comparison of united and nonunited fractures of the ulnar styloid following volar-plate fixation of distal radius fractures. Injury. 2010b, 42: 371–5.
Lindau T, Arner M, Hagberg L. Intraarticular lesions in distal fractures of the radius in young adults. A descriptive arthro-scopic study in 50 patients. J Hand Surg Br. 1997, 22: 638–43.
Lindau T, Adlercreutz C, Aspenberg P. Peripheral tears of the triangular fibrocartilage complex cause distal radi-oulnar joint instability after distal radial fractures. J Hand Surg Am. 2000a, 25: 464–8.
Lindau T, Hagberg L, Adlercreutz C, Jonsson K, Aspenberg P. Distal radioulnar instability is an independent wors-ening factor in distal radial fractures. Clin Orthop Relat Res. 2000b: 229–35.
May MM, Lawton JN, Blazar PE. Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am. 2002, 27: 965–71.
Melone CP, Jr., Nathan R. Traumatic disruption of the tri-angular fibrocartilage complex. Pathoanatomy. Clin Orthop Relat Res. 1992: 65–73.
Nakamura R, Horii E, Imaeda T, Nakao E, Shionoya K, Kato H. Ulnar styloid malunion with dislocation of the distal radioulnar joint. J Hand Surg Br. 1998, 23: 173–5.
Orhun H, Dursun M, Gurkan V, Sarioglu E, Altun G, Akca O. A new index for the assessment of distal radius frac-tures involving the ulnar styloid. Acta Orthop Traumatol Turc. 2011, 45: 261–5.
Oskarsson GV, Aaser P, Hjall A. Do we underestimate the predictive value of the ulnar styloid affection in Colles fractures? Arch Orthop Trauma Surg. 1997, 116: 341–4.
Protopsaltis TS, Ruch DS. Triangular fibrocartilage com-plex tears associated with symptomatic ulnar styloid nonunions. J Hand Surg Am. 2010, 35: 1251–5.
Reichl M, Piatek S, Adolf D, Winckler S, Westphal T. [Unrepaired fracture of the styloid process of the ulna: not a bad treatment result at distal radius fracture]. Unfallchirurg. 2010, 114: 1099–104.
Roysam GS. The distal radio-ulnar joint in Colles’ fractures. J Bone Joint Surg Br. 1993, 75: 58–60.
Sammer DM, Shah HM, Shauver MJ, Chung KC. The effect of ulnar styloid fractures on patient-rated outcomes after volar locking plating of distal radius fractures. J Hand Surg Am. 2009, 34: 1595–602.
Scheer JH, Adolfsson LE. Radioulnar laxity and clinical out-come do not correlate after a distal radius fracture. J Hand Surg Eur Vol. 2011, 36: 503–8.
Schuind F, An KN, Berglund L et al. The distal radioulnar ligaments: a biomechanical study. J Hand Surg Am. 1991, 16: 1106–14.
Shaw JA, Bruno A, Paul EM. Ulnar styloid fixation in the treatment of posttraumatic instability of the radioulnar joint: a biomechanical study with clinical correlation. J Hand Surg Am. 1990, 15: 712–20.
Souer JS, Ring D, Matschke S, Audige L, Marent-Huber M, Jupiter JB. Effect of an unrepaired fracture of the ulnar styloid base on outcome after plate-and-screw fixation of a distal radial fracture. J Bone Joint Surg Am. 2009, 91: 830–8.
Stewart HD, Innes AR, Burke FD. Factors affecting the out-come of Colles’ fracture: an anatomical and functional study. Injury. 1985, 16: 289–95.
Stoffelen D, De Smet L, Broos P. The importance of the dis-tal radioulnar joint in distal radial fractures. J Hand Surg Br. 1998, 23: 507–11.
Tsukazaki T, Iwasaki K. Ulnar wrist pain after Colles’ frac-ture. 109 fractures followed for 4 years. Acta Orthop Scand. 1993, 64: 462–4.
Villar RN, Marsh D, Rushton N, Greatorex RA. Three years after Colles’ fracture. A prospective review. J Bone Joint Surg Br. 1987, 69: 635–8.
Zenke Y, Sakai A, Oshige T, Moritani S, Nakamura T. The effect of an associated ulnar styloid fracture on the out-come after fixation of a fracture of the distal radius. J Bone Joint Surg Br. 2009, 91: 102–7.
Zhao L, Wang BJ, Li YD et al. [Clinical follow-up study of ulnar styloid fractures and classification of distal radial fractures]. Beijing Da Xue Xue Bao. 2011, 43: 675–80.
at MHH-Bibliothek on April 12, 2014jhs.sagepub.comDownloaded from
9
2. Die Autoren
Stefan Krämer – Klinik für Unfallchirurgie, Medizinische Hochschule Hannover
• Verfassen der Publikation
• Datenanalyse und -interpretation
• Klinische und radiologische Untersuchung der Patienten
• Patientenrecherche und Kontaktierung
Hendrik Meyer – Klinik für Unfallchirurgie, Medizinische Hochschule Hannover
• Klinische und radiologische Untersuchung der Patienten
• Patientenrecherche und Kontaktierung
Padhraig F. O´Loughlin – Department of Orthopedic Surgery, Hospital of Special Surgery, New York,
NY, USA
• Sprachliche Überarbeitung der Publikation
Bernhard Vaske – Institut für Biometrie, Medizinische Hochschule Hannover
• Statistische Berechnungen
Prof. Dr. med. Christian Krettek – Klinik für Unfallchirurgie, Medizinische Hochschule Hannover
• Klinikdirektor
• Bereitstellung von Untersuchungskapazitäten
PD Dr. med. Ralph Gaulke – Klinik für Unfallchirurgie, Medizinische Hochschule Hannover
• Leiter der Studie
• Studiendesign
• Supervision der klinischen Untersuchung
• Hilfestellung beim Verfassen der Publikation
10
Abbildung 1 - Anatomie des DRUG
3. Zusammenfassung
3.1 Einleitung
Die Geschichte der distalen Radiusfraktur als isolierte Verletzung geht auf die Erstbeschreibung von
Colles [1] im Jahre 1814 zurück. Es handelt sich um eine Fraktur des handgelenksnahen Radius mit
oder ohne Beteiligung des Handgelenkes und wird im Volksmund häufig als „Handgelenkbruch“ be-
zeichnet. Diese Verletzung ist mit 10-25% aller Frakturen die häufigste des menschlichen Körpers [2]
und zeigt eine Inzidenz von 200.000 pro Jahr in Deutschland mit einem gehäuften Vorkommen in der
Altersgruppe der über Fünfzigjährigen (80%) [3]. Der Verletzungsmechanismus ist eine direkte oder
indirekte Gewalteinwirkung meist durch einen Sturz auf die flektierte oder dorsalextendierte Hand.
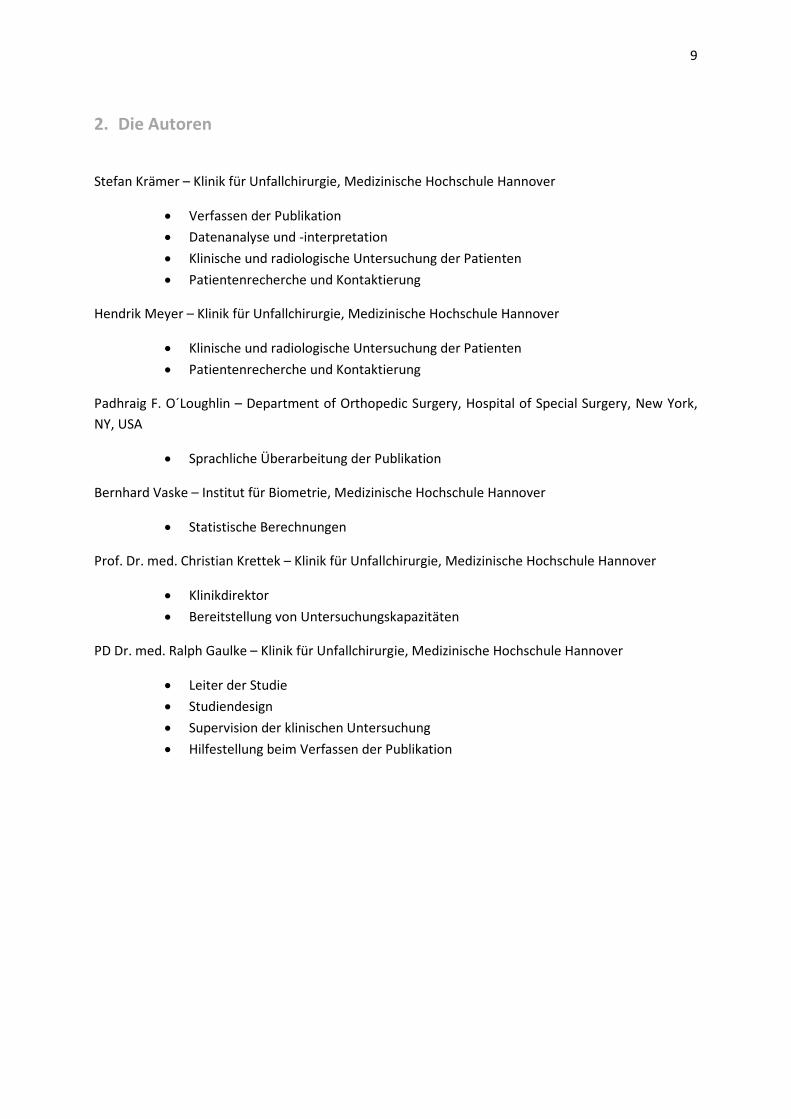
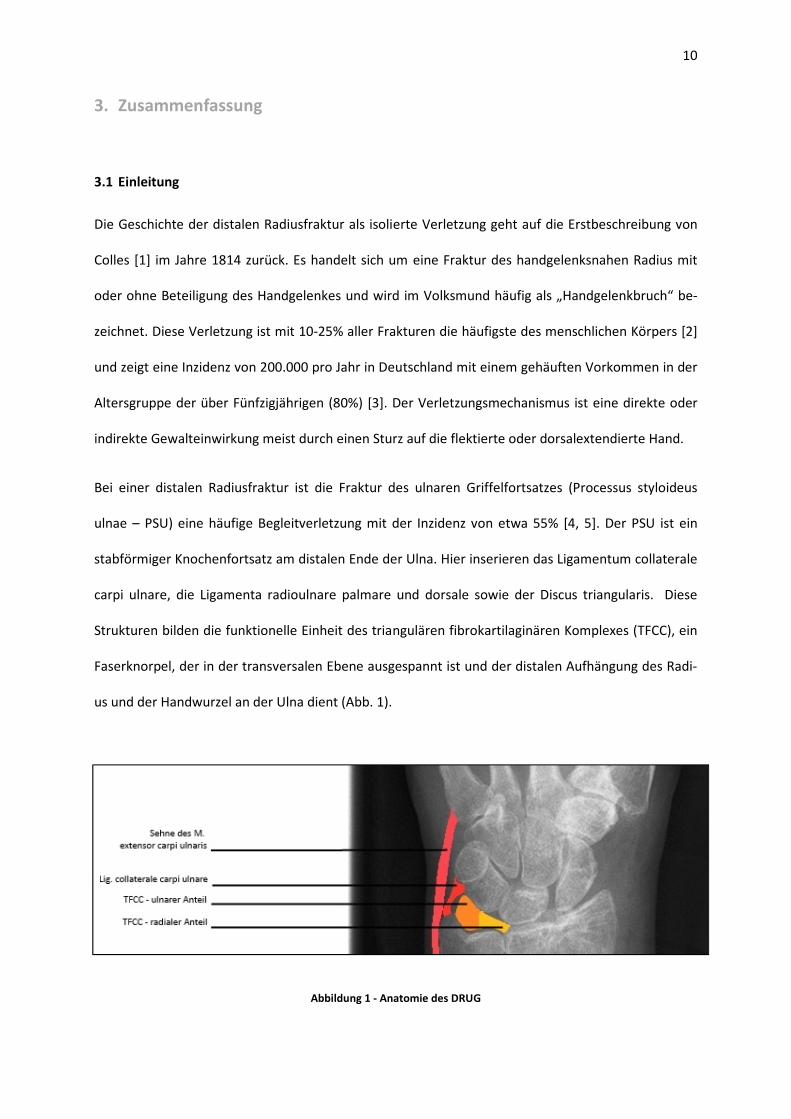
Bei einer distalen Radiusfraktur ist die Fraktur des ulnaren Griffelfortsatzes (Processus styloideus
ulnae – PSU) eine häufige Begleitverletzung mit der Inzidenz von etwa 55% [4, 5]. Der PSU ist ein
stabförmiger Knochenfortsatz am distalen Ende der Ulna. Hier inserieren das Ligamentum collaterale
carpi ulnare, die Ligamenta radioulnare palmare und dorsale sowie der Discus triangularis. Diese
Strukturen bilden die funktionelle Einheit des triangulären fibrokartilaginären Komplexes (TFCC), ein
Faserknorpel, der in der transversalen Ebene ausgespannt ist und der distalen Aufhängung des Radi-
us und der Handwurzel an der Ulna dient (Abb. 1).
11
Vor allem die zentralen und radialen Anteile des TFCC sind nicht vaskularisiert und heilen nach Ver-
letzungen daher nicht. Eine Fraktur des PSU kann somit Ursache von ulnokarpalen Beschwerden bzw.
Instabilität im distalen Radioulnargelenk (DRUG) sein.
Die Anatomie des Handgelenkes zeigt, dass der nach radial ziehende Anteil des TFCC insbesondere an
der Basis des PSU inseriert. Die Differenzierung von PSU-Verletzungen in Basis- (Typ I) und Spitzen-
frakturen (Typ II) nach Fernandez [6] beruht auf der Annahme, dass ligamentäre Strukturen des
DRUG bei Basisfrakturen eher in Mitleidenschaft gezogen werden und diese daher per Definition als
instabil bezeichnet werden.
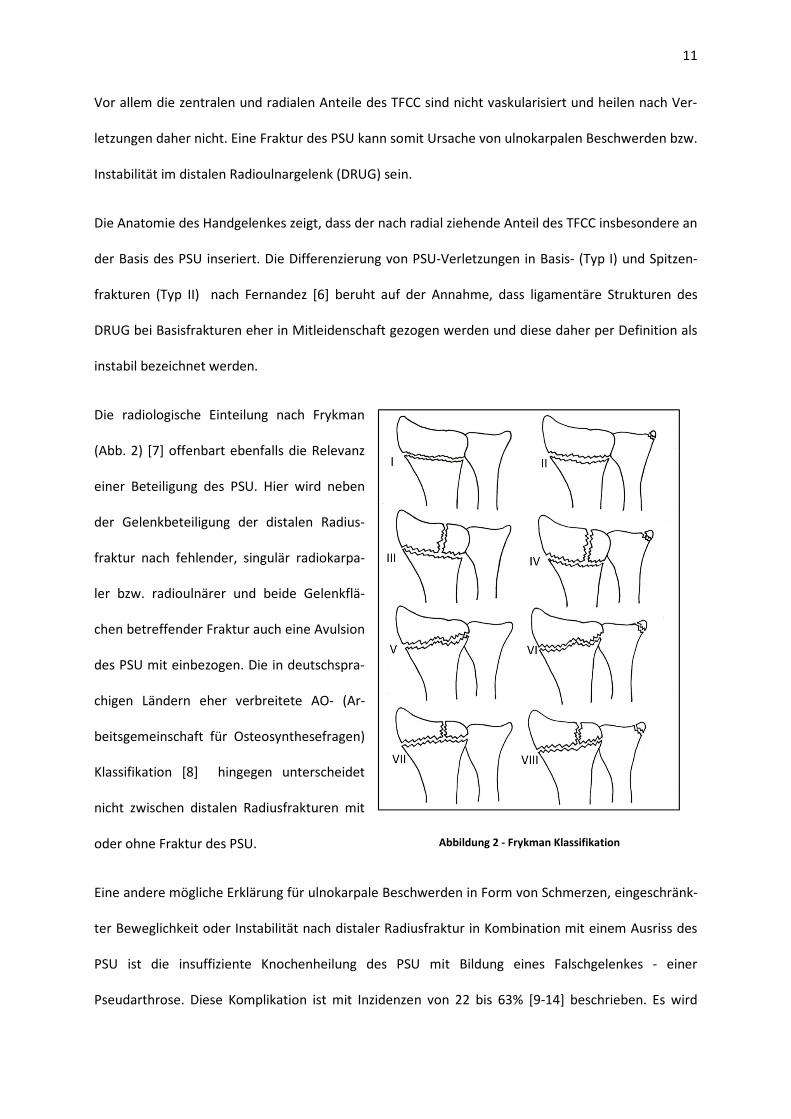
Die radiologische Einteilung nach Frykman
(Abb. 2) [7] offenbart ebenfalls die Relevanz
einer Beteiligung des PSU. Hier wird neben
der Gelenkbeteiligung der distalen Radius-
fraktur nach fehlender, singulär radiokarpa-
ler bzw. radioulnärer und beide Gelenkflä-
chen betreffender Fraktur auch eine Avulsion
des PSU mit einbezogen. Die in deutschspra-
chigen Ländern eher verbreitete AO- (Ar-
beitsgemeinschaft für Osteosynthesefragen)
Klassifikation [8] hingegen unterscheidet
nicht zwischen distalen Radiusfrakturen mit
oder ohne Fraktur des PSU.
Eine andere mögliche Erklärung für ulnokarpale Beschwerden in Form von Schmerzen, eingeschränk-
ter Beweglichkeit oder Instabilität nach distaler Radiusfraktur in Kombination mit einem Ausriss des
PSU ist die insuffiziente Knochenheilung des PSU mit Bildung eines Falschgelenkes - einer
Pseudarthrose. Diese Komplikation ist mit Inzidenzen von 22 bis 63% [9-14] beschrieben. Es wird
Abbildung 2 - Frykman Klassifikation
12
angenommen, dass die Beschwerden durch Irritationen der Knochenfragmente verursacht werden
oder, dass durch eine Fibrosierung des umgebenden Gewebes ein Einklemmen der Sehne des
Musculus extensor carpi ulnaris entsteht [15, 16].
Sowohl in der radiologischen Einteilung von distalen Radiusfrakturen als auch in der klinischen Prog-
nose und kontroversen Studienergebnissen in der Literatur ist die Relevanz einer begleitenden Frak-
tur des Processus styloideus ulnae strittig. In der vorliegenden Studie werden der Einfluss dieser
Fraktur und der einer Pseudarthrose des PSU auf das klinische Gesamtergebnis bei Patienten mit
distaler Radiusfraktur untersucht.
3.2 Material und Methoden
Es handelt sich um eine retrospektive klinisch radiologische Studie. Die Einschlusskriterien sind eine
distale Radiusfraktur von Januar 2007 bis April 2011, versorgt in der Medizinischen Hochschule Han-
nover, bei Patienten im Alter von mindestens 18 Jahren zum Zeitpunkt der Fraktur und einem Na-
chuntersuchungsintervall von sechs Monaten oder mehr. Zu allen potenziellen Studienteilnehmern
war die Recherche der Telefonnummer und Adresse notwendig, um diese in die Hand-, Fuß- und
Rheumasprechstunde der Medizinischen Hochschule Hannover einzuladen. Patienten, die telefonisch
in die Untersuchung eingewilligt hatten, erhielten vor der Untersuchung auf postalischem Weg den
Disability of the Arm, Shoulder and Hand-Fragebogen (DASH) [17] und einen zweiten selbst entwor-
fenen Fragebogen, der insbesondere Beschwerden im DRUG erfasst. Alle Patienten stimmten der
Teilnahme an einer klinischen Studie schriftlich zu. Die Untersuchung beinhaltete eine Feststellung
des Bewegungsumfanges der Hand- und der Fingergrundgelenke (Metacarpophalangealgelenk –
MCP) im Seitenvergleich mit einem Standard-Winkelmesser in allen Ebenen nach der Neutral-Null-
Methode. Da in der Literatur (s.u.) meist operativ behandelte (ORIF = open reduction and internal
fixation) distale Radiusfrakturen betrachtet werden, die vorliegende Studienpopulation jedoch ope-
rativ und konservativ behandelte Fälle erfasst, ist die Analyse des Bewegungsumfanges dieser bei-
13
den Kollektive für die Publikation getrennt durchgeführt worden. Zu allen Bewegungen bewerteten
die Patienten den dabei auftretenden Schmerz nach der Visuellen Analog Skala (VAS). Ebenso wurde
der Schmerz bei ulnarseitiger Druckausübung und Translation im DRUG beurteilt. Die relative Stabili-
tät des DRUG wurde mittels einer forcierten (Sub-)Luxation im Vergleich zur Gegenseite geprüft.
Zudem fand eine Kraftprüfung mit dem Jamar Dynamometer und dem Martin Vigorimeter [18] in je
drei Versuchen rechts wie links und die Messung des Finger-Hohlhand-Abstandes beider Seiten statt.
Die Analyse und Interpretation dieser Daten erfolgte nach der Hypothese, dass die klinisch objektiv
erfassbaren Messwerte und die subjektive Einschränkung im Alltag, erfasst durch die Fragebögen,
eine Abhängigkeit vom Vorhandensein und/oder dem Heilungsstatus einer Fraktur des PSU zeigen.
Hierzu wurden drei Patientengruppen gebildet. Gruppe eins: intakter PSU, Gruppe zwei: geheilte
PSU-Fraktur, Gruppe drei: PSU Pseudarthrose. Es wurden die nicht parametrischen Mann-Whitney
und Pearson-Chi-Square Tests zur Gegenüberstellung der Daten angewandt. Eine statistische Signifi-
kanz wurde mit einem p-Wert ≤ 0,05 festgelegt. Die Berechnungen erfolgten in Kooperation mit
Bernhard Vaske vom Institut für Biometrie der Medizinischen Hochschule Hannover. Zur Vermeidung
von Selektions-Bias fand eine Berechnung der Verteilung von relevanten Einflussfaktoren auf die
genannten Gruppen statt. Hierzu wurden ein Nachuntersuchungsintervall von mehr oder weniger als
24 Monaten, die Therapie der distalen Radiusfraktur (operativ versus konservativ) und die radiologi-
sche Kategorisierung nach AO, Frykman bzw. nach Fernandez [8] bei PSU-Fraktur gezählt. Eine
Pseudarthrose des PSU wurde definiert als ein Fehlen überbrückender Knochentrabekel im
anteroposterioren und seitlichen Röntgenbild sechs Monate nach der Verletzung.
3.3 Ergebnisse
Von Mai 2010 bis November 2011 unterzogen sich 191 Patienten der klinischen Untersuchung von S.
Krämer und H. Meyer unter Supervision von PD Dr. med. R. Gaulke. Hierbei wurde eine erhebliche
Masse an Rohdaten gesammelt, die nach der schriftlichen Erfassung auf Untersuchungsbögen zu-
nächst in Microsoft Excel® (Microsoft Corp., Redmond, WA, USA) übertragen und geordnet wurde.
14
Die Gruppe eins (n=99) stellt zur Evaluation der Relevanz einer Existenz einer zusätzlichen PSU-
Fraktur das Pendant zu den zusammengefassten Patienten der Gruppen zwei und drei mit insgesamt
101 kombinierten distalen Unterarmfrakturen dar. Analog hierzu dient der Vergleich der Gruppen
zwei (n=55) und drei (n=46) zur Erfassung der Bedeutsamkeit einer entstandenen Pseudarthrose. Es
zeigt sich ein signifikant höherer Anteil multifragmentär intraartikulärer (AO-C) und operativ versorg-
ter Radiusfrakturen in den Gruppen zwei und drei.
Der Schwerpunkt der veröffentlichten Resultate liegt auf der Betrachtung ulnokarpaler Beschwerden.
Es lässt sich tendenziell eine Einschränkung der Ulnarduktion in den Gruppen zwei und drei erken-
nen, die jedoch nur bei Patienten mit ORIF signifikant ist. Die Auswertung der Schmerzanalyse be-
schränkt sich auf die horizontalen Bewegungen, ulnaren Druckschmerz und Translationsschmerz im
DRUG. Es ergibt sich dort ein signifikant höherer Punktwert in der Schmerzangabe nach der VAS bei
Patienten mit einer begleitenden Fraktur des PSU. Die Instabilität im DRUG weist in der klinischen
Testung und nach Patientenempfinden eine signifikant höhere Inzidenz bei Fällen mit PSU-
Beteiligung auf, jedoch unabhängig von der Lokalisation dieser Fraktur (Basis versus Spitze). Der Ver-
gleich von Patienten mit und ohne Bildung einer Pseudarthrose des PSU ergibt in den genannten
Untersuchungen keine relevanten Unterschiede.
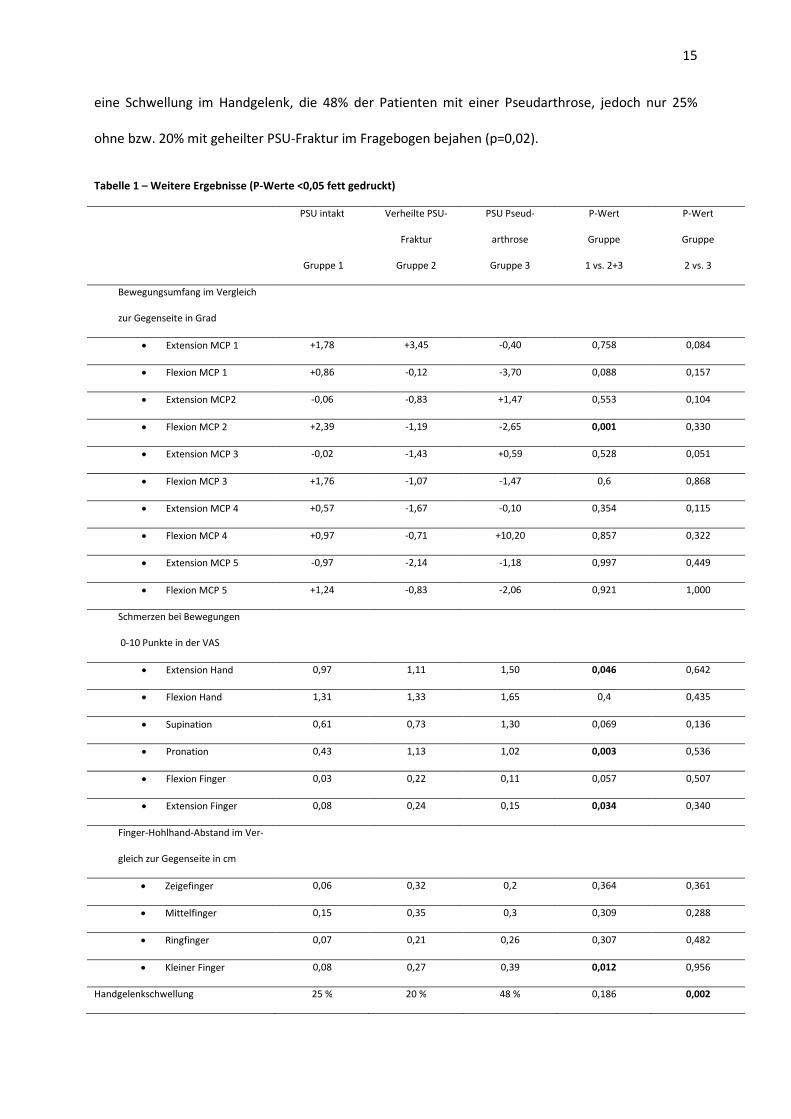
Um den Rahmen des Zeitschriftenartikels nicht zu sprengen, wurde auf die Darstellung einiger Studi-
energebnisse verzichtet, welche ich im Folgenden demonstriere (Tabelle 1): So kann eine statistisch
signifikante (p=0,001) relative Einschränkung des Flexionsgrades des Zeigefingers in Fällen mit PSU-
Beteiligung dokumentiert werden, wohingegen bei fehlender PSU-Fraktur das Flexionsausmaß im
Seitenvergleich größer ist. Der gemessene Finger-Hohlhand-Abstand weist ebenfalls Unterschiede
auf. Die Zunahme in Relation zur unverletzten Seite ist den fünften Finger betreffend in Gruppe eins
durchschnittlich geringer als in den Gruppen mit PSU-Fraktur (p=0,012). Im Bezug auf bewegungsab-
hängigen Schmerz werden auch bei Extension der Finger (p=0,034) und Hand (p=0,046) sowie bei der
Pronation (p=0,003) signifikant höhere Werte in der Schmerzskala für Patienten mit Verletzung des
PSU detektiert. Der Parameter, der im Vergleich der Gruppen zwei und drei eine Auffälligkeit zeigt, ist
15
eine Schwellung im Handgelenk, die 48% der Patienten mit einer Pseudarthrose, jedoch nur 25%
ohne bzw. 20% mit geheilter PSU-Fraktur im Fragebogen bejahen (p=0,02).
Tabelle 1 – Weitere Ergebnisse (P-Werte <0,05 fett gedruckt)
PSU intakt
Gruppe 1
Verheilte PSU-
Fraktur
Gruppe 2
PSU Pseud-
arthrose
Gruppe 3
P-Wert
Gruppe
1 vs. 2+3
P-Wert
Gruppe
2 vs. 3
Bewegungsumfang im Vergleich
zur Gegenseite in Grad
• Extension MCP 1 +1,78 +3,45 -0,40 0,758 0,084
• Flexion MCP 1 +0,86 -0,12 -3,70 0,088 0,157
• Extension MCP2 -0,06 -0,83 +1,47 0,553 0,104
• Flexion MCP 2 +2,39 -1,19 -2,65 0,001 0,330
• Extension MCP 3 -0,02 -1,43 +0,59 0,528 0,051
• Flexion MCP 3 +1,76 -1,07 -1,47 0,6 0,868
• Extension MCP 4 +0,57 -1,67 -0,10 0,354 0,115
• Flexion MCP 4 +0,97 -0,71 +10,20 0,857 0,322
• Extension MCP 5 -0,97 -2,14 -1,18 0,997 0,449
• Flexion MCP 5 +1,24 -0,83 -2,06 0,921 1,000
Schmerzen bei Bewegungen
0-10 Punkte in der VAS
• Extension Hand 0,97 1,11 1,50 0,046 0,642
• Flexion Hand 1,31 1,33 1,65 0,4 0,435
• Supination 0,61 0,73 1,30 0,069 0,136
• Pronation 0,43 1,13 1,02 0,003 0,536
• Flexion Finger 0,03 0,22 0,11 0,057 0,507
• Extension Finger 0,08 0,24 0,15 0,034 0,340
Finger-Hohlhand-Abstand im Ver-
gleich zur Gegenseite in cm
• Zeigefinger 0,06 0,32 0,2 0,364 0,361
• Mittelfinger 0,15 0,35 0,3 0,309 0,288
• Ringfinger 0,07 0,21 0,26 0,307 0,482
• Kleiner Finger 0,08 0,27 0,39 0,012 0,956
Handgelenkschwellung 25 % 20 % 48 % 0,186 0,002
16
3.4 Diskussion
Die Ergebnisse der Studie zeigen ein insgesamt gehäuftes Vorkommen ulnokarpaler Beschwerden bei
Patienten mit distaler Radiusfraktur in Kombination mit einer Fraktur des PSU. Dies ist vereinbar mit
den Erkenntnissen von Bellotti et al. [19], die in solchen Fällen vermehrten Handgelenkschmerz ver-
knüpft mit Behinderung im Alltag konstatieren. Die festgestellten Bewegungseinschränkungen lassen
den Schluss zu, dass eine Kombination von distaler Radius- und PSU-Fraktur auch Bewegungen im
Radiokarpalgelenk und zum Teil in den Fingergrundgelenken einschränkt. Der Unterschied im
Signifikanzniveau deutet hierbei auf einen größeren Einfluss von PSU-Frakturen auf die Beweglichkeit
bei operativ versorgten, also kürzer immobilisierten Handgelenken hin. Eine Abnahme des Bewe-
gungsumfanges und/oder ein Kraftverlust werden auch in Arbeiten von Villar et al. [5], Oskarrsson et
al. [20] und mit Einschränkungen von Souer et al. [21] in Fällen mit begleitender Fraktur des PSU
nachgewiesen. Die Untersuchungsergebnisse des DRUG suggerieren die Relevanz des TFCC als Stabi-
lisator dieses Gelenkes. Ein Weichteilschaden entsteht demnach vermehrt bei PSU-Frakturen - auch
wenn nur die Spitze betroffen ist. So sind Risse des TFCC gehäuft bei einem begleitenden PSU-Ausriss
beschrieben [22, 23]. Diverse Studien zeigen ebenfalls einen Zusammenhang zwischen Beschwerden
im DRUG und der Inzidenz von PSU-Frakturen [24, 25]. Der signifikant niedrigere Punktwert im DASH-
Fragebogen, aber vor allem die Auswertung des zweiten Fragebogens legt dar, dass Supinations- und
Pronationsbewegungen in den Patientengruppen mit klinisch objektiv detektierter und subjektiv
empfundener Instabilität im DRUG im Alltag behindert sind. In der Studie von May et al. [4] werden
Instabilitäten im DRUG in Fällen kombinierter PSU- und distaler Radiusfraktur zusätzlich mittels com-
putertomographischer Untersuchung nachgewiesen.
Es existieren ebenfalls gegenteilige Literaturmeinungen und Studienergebnisse im Bezug auf die klini-
sche Relevanz eines PSU-Abrisses. So konstatieren Scheer et al. trotz eines höheren Anteils an DRUG-
Instabilität keine Auswirkung von PSU-Frakturen auf eine alltägliche Beeinträchtigung in Form des
Punktewertes im DASH-Fragebogen [26]. Bei einem Nachuntersuchungsintervall von nur drei Mona-
ten kann in einer Studie von Kazemian et al. kein Zusammenhang von Instabilität des DRUG und PSU-
17
Fraktur dokumentiert werden [27]. Diverse Studien [21, 28-32] zeigen keinen signifikanten Einfluss
einer kombinierten Fraktur des ulnaren Griffelfortsatzes bei konsequent operativ versorgter distaler
Radiusfraktur auf das klinische Gesamtergebnis. Die Analyse von konservativ behandelten distalen
Radiusfrakturen in der Arbeit von Roysam et al. [30] zeigt eine Beschwerdeabhängigkeit von der Be-
teiligung des DRUG, nicht jedoch einer Fraktur des PSU.
Die Lokalisation der PSU-Fraktur (Basis vs. Spitze) hat in der durchgeführten Analyse keinen Einfluss
auf die Stabilität des distalen Radioulnargelenkes. Dies ist auch das Ergebnis von Reichl et al., die im
Vergleich von intakten, basisnah frakturierten und PSU-Spitzenfrakturen keinen Unterschied im klini-
schen Resultat feststellen [14].
In Bezug auf den Einfluss einer Pseudarthrose des PSU auf die Beschwerdehäufigkeit der Patienten
wird ein kausaler Zusammenhang vermutet. In der Literatur ist dieses jedoch spärlich belegt und dies
in Studien mit geringer Fallzahl oder jugendlichen Patienten [33-35]. Die geläufigere Meinung ist mit
den dargelegten Ergebnissen konsistent. Die Pseudarthrose des PSU bei distaler Radiusfraktur ist mit
einem Vorkommen in etwa der Hälfte der Fälle keine seltene Komplikation, führt jedoch zu keinerlei
klinisch objektiv feststellbarer oder subjektiv empfundener Beeinträchtigung des Patienten. Bei einer
Fallzahl von n=200 kann diese Studie jene der vorbeschriebenen Analysen solcher Patientengruppen
bestätigen [24, 36-38].
Das Studiendesign beinhaltet zu erwähnende Schwächen. Es ist eine retrospektive Analyse ohne sta-
tistisches Matching und Ausschlusskriterien mit Patienten, die sich selbst für eine Teilnahme ent-
schieden. Dadurch könnte eine unbewusste Selektion von Patienten mit Beschwerden entstanden
sein. Zudem ist der Anteil von radiologisch intraartikulären und auch der Anteil der operativ thera-
pierten Patienten in den Gruppen mit PSU-Fraktur signifikant höher, sodass die Aussagekraft der
PSU-Fraktur als kausaler Faktor für die Inzidenz ulnokarpaler Beschwerden an Gewicht verliert.
18
3.5 Zusammenfassung
Zusammenfassend zeigt die Studie, dass bei einer heterogenen Zusammenstellung der Patienten mit
einer umfangreichen klinischen Untersuchung die Inzidenz ulnokarpaler Schmerzen und Funktions-
einschränkungen bei distaler Radiusfraktur in Fällen mit kombinierter Fraktur des PSU insgesamt
höher ist. Damit stellt diese einen relevanten Prognosefaktor für das spätere Auftreten von Be-
schwerden dar. Sowohl die Lokalisation der PSU-Fraktur als auch die Bildung einer Pseudarthrose
haben hingegen keinen Einfluss auf das klinische Ergebnis.
In Anbetracht der erwähnten Schwächen der Studie und der kontroversen Literaturmeinung bedarf
es weiterer prospektiver Studien mit größeren Fallzahlen und aufwändigeren bildgebenden Verfah-
ren.
3.6 Literaturverzeichnis
1. Colles A. Edinburgh Med J, 1814
2. Chung, K.C. and S.V. Spilson, The frequency and epidemiology of hand and forearm fractures
in the United States. J Hand Surg Am, 2001. 26(5): p. 908-15.
3. Siebert, H.R. and A. Klonz, [Fracture of the distal radius]. Chirurg, 2006. 77(6): p. 545-562;
quiz 563.
4. May, M.M., J.N. Lawton, and P.E. Blazar, Ulnar styloid fractures associated with distal radius
fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am, 2002.
27(6): p. 965-71.
5. Villar, R.N., et al., Three years after Colles' fracture. A prospective review. J Bone Joint Surg Br,
1987. 69(4): p. 635-8.
6. Fernandez, D.L., Correction of post-traumatic wrist deformity in adults by osteotomy, bone-
grafting, and internal fixation. J Bone Joint Surg Am, 1982. 64(8): p. 1164-78.
7. Frykman, G., Fracture of the distal radius including sequelae--shoulder-hand-finger syndrome,
disturbance in the distal radio-ulnar joint and impairment of nerve function. A clinical and
experimental study. Acta Orthop Scand, 1967: p. Suppl 108:3+.
8. Graff, S. and J. Jupiter, Fracture of the distal radius: classification of treatment and indications
for external fixation. Injury, 1994. 25 Suppl 4: p. S-D14-25.
19
9. Bacorn, R.W. and J.F. Kurtzke, Colles' fracture; a study of two thousand cases from the New
York State Workmen's Compensation Board. J Bone Joint Surg Am, 1953. 35-A(3): p. 643-58.
10. Buijze, G.A. and D. Ring, Clinical impact of United versus nonunited fractures of the proximal
half of the ulnar styloid following volar plate fixation of the distal radius. J Hand Surg Am. 35(2): p.
223-7.
11. Catalano, L.W., 3rd, et al., Displaced intra-articular fractures of the distal aspect of the radius.
Long-term results in young adults after open reduction and internal fixation. J Bone Joint Surg Am,
1997. 79(9): p. 1290-302.
12. Geissler, W.B., D.L. Fernandez, and D.M. Lamey, Distal radioulnar joint injuries associated
with fractures of the distal radius. Clin Orthop Relat Res, 1996(327): p. 135-46.
13. Kim, J.K., et al., Comparison of united and nonunited fractures of the ulnar styloid following
volar-plate fixation of distal radius fractures. Injury. 42(4): p. 371-5.
14. Reichl, M., et al., [Unrepaired fracture of the styloid process of the ulna: not a bad treatment
result at distal radius fracture]. Unfallchirurg, 2010. 114(12): p. 1099-104.
15. Schmit-Neuerburg, K.P. and A. Berger, Tscherne Unfallchirurgie: Ellenbogen, Unterarm; Hand
/ K.-P. Schmit-Neuerburg ... (Hrsg.). Hand : mit 21 Tabellen / unter Mitarb. von A. Berger ... Zeichn.
von R. Henkel: Springer.
16. Protopsaltis, T.S. and D.S. Ruch, Triangular fibrocartilage complex tears associated with
symptomatic ulnar styloid nonunions. J Hand Surg Am, 2010. 35(8): p. 1251-5.
17. De Smet, L., The DASH questionnaire and score in the evaluation of hand and wrist disorders.
Acta Orthop Belg, 2008. 74(5): p. 575-81.
18. Desrosiers, J., et al., Comparison of the Jamar dynamometer and the Martin vigorimeter for
grip strength measurements in a healthy elderly population. Scand J Rehabil Med, 1995. 27(3): p.
137-43.
19. Belloti, J.C., et al., Does an ulnar styloid fracture interfere with the results of a distal radius
fracture? J Orthop Sci, 2009. 15(2): p. 216-22.
20. Oskarsson, G.V., P. Aaser, and A. Hjall, Do we underestimate the predictive value of the ulnar
styloid affection in Colles fractures? Arch Orthop Trauma Surg, 1997. 116(6-7): p. 341-4.
21. Souer, J.S., et al., Effect of an unrepaired fracture of the ulnar styloid base on outcome after
plate-and-screw fixation of a distal radial fracture. J Bone Joint Surg Am, 2009. 91(4): p. 830-8.
22. Geissler, W.B., Arthroscopically assisted reduction of intra-articular fractures of the distal
radius. Hand Clin, 1995. 11(1): p. 19-29.
23. Lindau, T., M. Arner, and L. Hagberg, Intraarticular lesions in distal fractures of the radius in
young adults. A descriptive arthroscopic study in 50 patients. J Hand Surg Br, 1997. 22(5): p. 638-43.
20
24. Lindau, T., C. Adlercreutz, and P. Aspenberg, Peripheral tears of the triangular fibrocartilage
complex cause distal radioulnar joint instability after distal radial fractures. J Hand Surg Am, 2000.
25(3): p. 464-8.
25. Stoffelen, D., L. De Smet, and P. Broos, The importance of the distal radioulnar joint in distal
radial fractures. J Hand Surg Br, 1998. 23(4): p. 507-11.
26. Scheer, J.H. and L.E. Adolfsson, Radioulnar laxity and clinical outcome do not correlate after a
distal radius fracture. J Hand Surg Eur Vol, 2011. 36(6): p. 503-8.
27. Kazemian, G.H., et al., DRUJ instability after distal radius fracture: A comparison between
cases with and without ulnar styloid fracture. Int J Surg, 2011. 9(8): p. 648-51.
28. Zenke, Y., et al., The effect of an associated ulnar styloid fracture on the outcome after
fixation of a fracture of the distal radius. J Bone Joint Surg Br, 2009. 91(1): p. 102-7.
29. Zhao, L., et al., [Clinical follow-up study of ulnar styloid fractures and classification of distal
radial fractures]. Beijing Da Xue Xue Bao, 2011. 43(5): p. 675-80.
30. Roysam, G.S., The distal radio-ulnar joint in Colles' fractures. J Bone Joint Surg Br, 1993. 75(1):
p. 58-60.
31. Kim, J.K., Y.D. Koh, and N.H. Do, Should an ulnar styloid fracture be fixed following volar plate
fixation of a distal radial fracture? J Bone Joint Surg Am, 2010. 92(1): p. 1-6.
32. Sammer, D.M., et al., The effect of ulnar styloid fractures on patient-rated outcomes after
volar locking plating of distal radius fractures. J Hand Surg Am, 2009. 34(9): p. 1595-602.
33. Burgess, R.C. and H.K. Watson, Hypertrophic ulnar styloid nonunions. Clin Orthop Relat Res,
1988(228): p. 215-7.
34. Hauck, R.M., J. Skahen, 3rd, and A.K. Palmer, Classification and treatment of ulnar styloid
nonunion. J Hand Surg Am, 1996. 21(3): p. 418-22.
35. Abid, A., et al., Ulnar styloid fracture in children: a retrospective study of 46 cases. J Pediatr
Orthop B, 2008. 17(1): p. 15-9.
36. Buijze, G.A. and D. Ring, Clinical impact of United versus nonunited fractures of the proximal
half of the ulnar styloid following volar plate fixation of the distal radius. J Hand Surg Am, 2010. 35(2):
p. 223-7.
37. Kim, J.K., et al., Comparison of united and nonunited fractures of the ulnar styloid following
volar-plate fixation of distal radius fractures. Injury, 2010. 42(4): p. 371-5.
38. Orhun, H., et al., A new index for the assessment of distal radius fractures involving the ulnar
styloid. Acta Orthop Traumatol Turc, 2011. 45(4): p. 261-5.
21
4. Publikationsverzeichnis
Krämer, S., Meyer H., O´Laughlin, PF., Vaske, B., Krettek, C., Gaulke, R., The incidence of ulnocarpal
complaints after distal radial fracture in relation to the fracture of the ulnar styloid. J Hand Surg Eur
Vol. 38(7): p. 710-7.
Meyer, H., Krämer S., O´Laughlin, PF., Vaske, B., Krettek, C., Gaulke, R., Union of the ulnar styloid
fracture as a function of fracture morphology on conventional radiographs. Skeletal Radiol. 42(8): p.
1135-41.
22
5. Erklärung gemäß § 2 Abs. 2 Nr. 6 und 7 PromO
Ich erkläre, dass ich die der Medizinischen Hochschule Hannover zur Promotion eingerichtete Disser-
tation mit dem Titel “Die Inzidenz ulnokarpaler Beschwerden nach distaler Radiusfraktur in Abhän-
gigkeit von einer Fraktur des Processus styloideus ulnae” in der Klinik für Unfallchirurgie unter Be-
treuung von PD Dr. med. Ralph Gaulke mit der Unterstützung durch die genannten Koautoren ohne
sonstige Hilfe durchgeführt und bei der Abfassung der Dissertation keine anderen als die dort aufge-
führten Hilfsmittel benutzt habe. Die Gelegenheit zum vorliegenden Promotionsverfahren ist mir
nicht kommerziell vermittelt worden. Insbesondere habe ich keine Organisation eingeschaltet, die
gegen Entgelt Betreuerinnen und Betreuer für die Anfertigung von Dissertationen sucht oder die mir
obliegenden Pflichten hinsichtlich der Prüfungsleistungen für mich ganz oder teilweise erledigt. Ich
habe diese Dissertation bisher an keiner in- oder ausländischen Hochschule zur Promotion einge-
reicht. Weiterhin versichere ich, dass ich den beantragten Titel noch nicht erworben habe.
Die Ergebnisse der Studie wurden im Dezember 2012 in der Online-First Version des „Journal of Hand
Surgery – European Volume“ veröffentlicht.
Hannover, den 24.04.2014
Stefan Krämer
23
6. Lebenslauf
Persönliche Daten:
Name: Stefan Krämer
Geburtsdatum: 05.02.1987
Geburtsort: Lingen (Ems)
Familienstand: ledig
Qualifikation: Approbierter Arzt
Berufliche Laufbahn:
Seit 01.2014 Arzt in Weiterbildung Neurologie, Diakoniekrankenhaus Friederikenstift
Hannover, Klinik für Neurologie
Studium:
2007 – 2013 Studium der Humanmedizin an der Medizinischen Hochschule Hannover
Abschluss: Zweiter Abschnitt der Ärztlichen Prüfung (Note: sehr gut)
08.2012 – 07.2013 Praktisches Jahr:
• 03.2013 – 07.2013 Klinik für Allgemein- und Viszeralchirurgie, Klinik
für Thorax- und Gefäßchirurgie, Klinikum Oststadt-Heidehaus, Klini-kum Region Hannover
• 12.2012 – 03.2013 Klinik für Innere Medizin, St. Bonifatius Hospital
Lingen (Ems)
• 08.2012 – 12.2012 Klinik für Neurologie, Medizinische Hochschule
Hannover
2010 – 2012 Famulaturen:
• 19.03.2012 – 22.04.2012 Hausärztliche Versorgung, Dr. M. Kraemer, Dr. M. Richter, Laatzen
• 16.08.2011 – 14.09.2011 St. Thomas Hospital & Leprosy Centre,
Chettapattu, Tamilnadu, India
• 28.03.2011 – 10.04.2011 Zentrum Anästhesiologie, Klinikum Siloah /
Oststadt-Heidehaus, Klinikum Region Hannover
• 09.08.2010 – 05.09.2010 Klinik für Unfallchirurgie, Medizinische Hochschule Hannover
24
• 29.03.2010 – 11.04.2010 Abteilung für Innere Medizin, St. Bonifatius
Hospital, Lingen (Ems)
Forschung:
2009 – 2013 Doktorrand in der Klinik für Unfallchirurgie, Medizinische Hochschule Hanno-
ver
Publikationen:
• Krämer, S., Meyer H., O´Laughlin, PF., Vaske, B., Krettek, C., Gaulke, R., The incidence of ulnocarpal complaints after distal radial fracture
in relation to the fracture of the ulnar styloid. J Hand Surg Eur Vol.
38(7): p. 710-7.
• Meyer, H., Krämer S., O´Laughlin, PF., Vaske, B., Krettek, C., Gaulke,
R., Union of the ulnar styloid fracture as a function of fracture
morphology on conventional radiographs. Skeletal Radiol. 42(8): p. 1135-41.
Vorträge:
• Gaulke R, Krämer S, Meyer H, Krettek C (2013) Die klinische Bedeu-
tung des Prozessus styloideus ulnae-Abrisses bei der distalen Radius-
fraktur 9. Deutscher Kongress für Orthopädie und Unfallchirurgie in
Berlin
Dissertation:
• „Die Inzidenz ulnokarpaler Beschwerden nach distaler Radiusfraktur
in Abhängigkeit von einer Fraktur des Processus styloideus ulnae“
Schulische Ausbildung:
1999 – 2006 Franziskusgymnasium in Lingen (Ems)
Abschluss: Allgemeine Hochschulreife (Note 1,2)
Zusatzqualifikation:
2007 - 2013 Neben- und ehrenamtliche Tätigkeit Deutsches Rotes Kreuz, Rettungsdienst
der Region Hannover, Laatzen
2008 – 2010 Studentische Hilfskraft im Institut für Pathologie, KRH Klinikum Nordstadt
2006 – 2007 Zivildienst Deutsches Rotes Kreuz, Kreisverband Lingen, Bereich Notfallret-
tung und qualifizierter Krankentransport
Abschluss: Rettungssanitäter
Hannover, den 24.04.2014
25
7. Danksagung
Mein erster Dank geht an PD Dr. med. R. Gaulke, der als Studienleiter alle Voraussetzungen für die
wissenschaftliche Arbeit gelegt hat und mich sowohl bei der klinischen und radiologischen Untersu-
chung als auch beim Verfassen der Publikation unterstütze, motivierte und mir nebenbei zur Weiter-
entwicklung meiner Fähigkeiten und Kenntnisse im Bereich der Unfallchirurgie verhalf.
Desweiteren gilt großer Dank dem Team der unfallchirurgischen Poliklinik der MHH Hiba Assaid, Ni-
cole Schwarz und Marlis Marquardt sowie allen Koautoren, die mir die Erfassung der Daten und de-
ren Veröffentlichung ermöglichten.
Zum Schluss danke ich meinem Kollegen und Freund Hendrik Meyer, der nicht nur den Arbeitsauf-
wand dieser Studie mittrug, sondern mir auch daneben stets zur Seite stand und steht.