Embed Size (px)
Citation preview

Digitalisierung in der MedizinFluch oder Segen ?
Prof. Dr. Hans-Ulrich Prokosch
Lehrstuhl für Medizinische Informatik der FAU Erlangen-NürnbergCIO Universitätsklinikum Erlangen
Konsortialleiter MIRACUM

Wie digital ist das deutsche Gesundheitswesen ?

Wie digital ist das deutsche Gesundheitswesen ?

https://www.bertelsmann-stiftung.de/de/unsere-projekte/der-digitale-patient/projektthemen/smarthealthsystems/estland/
Wie digital ist das deutsche Gesundheitswesen ?
PolicyAktivität
Digital HealthReadiness
TatsächlicheDatennutzung

https://www.mckinsey.de/news/presse/2018-09-27-digitalisierung-im-gesundheitswesen
Wie digital ist das deutsche Gesundheitswesen ?

Digitalisierung in der Medizin
Fluch oder Segen ?

Digitalisierung in der MedizinFluch oder Segen ?
DieSchwarzseher

Digitale GesundheitsakteVom Widerstand der Ärzte
• „Hochsensible Gesundheitsdaten von Erwachsenen und Kindern sollen in einer Cloud gespeichert werden.
• Wie wir wissen, sind Daten die einmal im Netz sind, praktisch nicht mehr zurückzuholen.“
Süddeutsche Zeitung Nr. 56, 7. März 2019, 13Süddeutsche Zeitung Nr. 56, 7. März 2019, 13

Digitale GesundheitsakteVom Widerstand der Ärzte
• „Hochsensible Gesundheitsdaten von Erwachsenen und Kindern sollen in einer Cloud gespeichert werden.
• Wie wir wissen, sind Daten die einmal im Netz sind, praktisch nicht mehr zurückzuholen.“
Süddeutsche Zeitung Nr. 56, 7. März 2019, 13Machen Sie Online-Banking?
Wollen Sie darauf heute noch verzichten?
Landen die Daten wirklich in der Cloud?Was ist überhaupt die „Cloud“?

Digitalisierung des GesundheitswesenFluch oder Segen?
„Ich sehe fassungslos vor einer Entwicklung in diesem Land,
in der man blind an die Allheilwirkung einer totalen Digitalisierung
zu glauben scheint und zunehmend
hochempfindliche Infrastrukturen allein digitalen Technologien
anvertraut“
Süddeutsche Zeitung Nr. 56, 7. März 2019, 13

Digitalisierung des GesundheitswesenFluch oder Segen?
„Wer also hat etwas von dieser sehr teuren „Digitalisierung“?
Der finanzielle Vorteil bei Unternehmen, die über die Verfügbarkeit von
Daten auf zentralen Servern ihre Märkte besser erschließen wollen oder
durch die Bereitstellung von Hard- und Software
im Milliarden-Eurobereich profitieren, ist offenkundig.
Süddeutsche Zeitung Nr. 56, 7. März 2019, 13

Digitalisierung des GesundheitswesenFluch oder Segen?
„Warum also sollten sich Heilberufler überhaupt an einem
Prozess beteiligen, bei dem IT-Firmen massive Gewinne
einfahren, der aber nicht erkennbar zur verbesserten
Patientenversorgung beiträgt“
Süddeutsche Zeitung Nr. 56, 7. März 2019, 13

Digitalisierung des GesundheitswesenFluch oder Segen?
Süddeutsche Zeitung Nr. 48, 26. Februar 2019, 2
„Die Privatsphäre von Arzt und Patient ist bedroht“
https://www.sueddeutsche.de/politik/2.220/aussenansicht-das-glaeserne-behandlungszimmer-1.4344293

Digitalisierung in der MedizinFluch oder Segen
DieWeißseher

https://www.pwc.de/de/gesundheitswesen-und-pharma/digitalisierung-im-gesundheitswesen.html
Big Data und KI sind die Zukunft

Der Einsatz von „Artificial Intelligence“ könnte Millionen Menschen zu besseren Therapien verhelfen –
und gleichzeitig dazu beitragen, die Gesundheitskosten signifikant zu senken.
KI revolutioniert die Medizin

AIpowers digital medicine

AIpowers digital medicine
Artificial intelligence (AI) has recently surpassed human performance in several domains,
and there is great hope that in healthcare,
AI may allow for better prevention, detection, diagnosis, and treatment of disease.

Fitbit and IBM Watson
are rapidly democratizing the access to personal health data
as well as access to complex computational capability, and placing it, literally, in people’s hands.
IBM Watsontransfering the power of healthcare data
https://www.cio.com/article/2922332/how-fitbit-and-ibm-watson-are-transferring-the-power-of-healthcare-data-from-one-hand-to-another.html

We have set an ambitious goal to improve lives and give hope
by addressing the world’s most pressing health challenges.
IBM Watsontransfering the power of healthcare data
https://www.ibm.com/watson/health/about/

IBM Watsontransfering the power of healthcare data
https://www.ibm.com/watson/health/about/

IBM Watsontransfering the power of healthcare data
https://www.zeit.de/digital/internet/2018-08/deep-learning-medizin-kuenstliche-intelligenz-neurologie-augenheilkundeMittwoch, 15. August 2018
Transform the way oncology professionals deliver care

IBM Watsontransfering the power of healthcare data
Transform the way oncology professionals deliver care
Wirklich?
Das 2013 groß angekündigte Pilotprojekt[1] für ein onkologisches Expertensystem auf Basis von Watson am MD-Anderson-Krebszentrum der Universität Texas etwa liegt mittlerweile auf Eis.

IBM Watsontransfering the power of healthcare data
Transform the way oncology professionals deliver care
Wirklich?
Der Supercomputer Watson von IBM wurde schon als Heilsbringer im Kampf gegen Krebs und andere schwere Krankheiten angepriesen.
Man habe in dem amerikanischen Konzern den „idealen Partner“ gefunden, um die „Schätze aus dem Datendschungel“ zu heben, frohlockte der DKFZ-Chef.
Computermesse Cebit in Hannover (2011)

IBM Watsontransfering the power of healthcare data
Transform the way oncology professionals deliver care
Wirklich?
heutiger DKFZ-Stiftungsvorstand Michael Baumann (2018)
… beschränkt sich nach außen auf eine nüchterne Tatsachenbeschreibung:
„Der Rahmenvertrag ist ausgelaufen, ohne dass Geld an IBM geflossen ist.“

IBM Watsontransfering the power of healthcare data
Transform the way oncology professionals deliver care
Wirklich?
Rhön-Klinikum / Marburg:
„Pleiten, Pech und Pannen“
Die Technik sei nicht brauchbar für den Krankenhausalltag.
„… habe sich die Lücke zwischen Anspruch und Wirklichkeit als so groß erwiesen, dass wir rasch unternehmerisch handeln mussten“

IBM Watsontransfering the power of healthcare data
Transform the way oncology professionals deliver care
Wirklich?
Memorial Sloan Kettering Cancer Center in New York
„Ich habe mir Watson dort ansehen können“, sagt der deutsche Krebsmediziner Michael Hallek
„Das hätte man alles auch in jeder anderen Forschungsdatenbank oder in einem Lehrbuch nachschlagen können“

transfering the power of healthcare data
IBM Watson
Google Deep Mind
AlphaGo

transfering the power of healthcare data
Süddeutsche Zeitung Nr. 56, 7. März 2019, 13
Egal wie komplex das Spiel Go auch sein mag,es basiert auf einem ganz klar definierten Regelwerk

Süddeutsche Zeitung Nr. 56, 7. März 2019, 13
Medizinische Versorgung lässt sich nicht durch ein klar definiertes Regelwerk
beschreiben

Künstliche Intelligenz
. . . wird oft mit „Maschinellem Lernen“
oder auch „Deep Learning“ gleichgesetzt . . .
und beruht auf sogenannten neuronalen Netzen(die es übrigens auch schon in den 80er Jahren gab)
. . .und es wird oft behauptet, dass KI selbstlernend sei

Künstliche Intelligenz
Maschinelles Lernen
. . . erfordert große Mengen an Daten
was aber häufig verschwiegen wird:
Maschinelles Lernen
. . . erfordert große Mengen an von Klinikern annotierten Daten

transfering the power of healthcare data
The CNN achieves performance on par with all tested experts. . . , demonstrating an artificial intelligence capable
of classifying skin cancer with a level of competence
comparable to dermatologists.
CNN = Deep convolutional neural network

transfering the power of healthcare data

transfering the power of healthcare data
Here we demonstrate the effectiveness of deep learning in dermatology, . . .
Further research is necessary to evaluate performance ina real-world, clinical setting,
in order to validate this technique across the full distribution and spectrum of lesions encountered in typical practice.

IBM WatsonIt´s nowhere close
https://www.statnews.com/2017/09/05/watson-ibm-cancer/

AI in MedicinePromise and Perils
Circulation Research 018;123:1282-1284.

AI in Medicinethe peak of inflated expectations
With machine learning situated at the peak of inflated expectations,
we can soften a subsequent crash into a “trough of disillusionment”
by fostering a stronger appreciation of the technology's capabilities and limitations.
Whether such artificial-intelligence systems are “smarter” than human practitioners makes for a stimulating debate — but is largely irrelevant.
Combining machine-learning software with the best human clinician “hardware” will permit delivery of care that outperforms what either can do alone.

KI: Arztunterstützend !
Combining machine-learning software with the best human clinician “hardware” will permit delivery of care that outperforms what either can do alone.
Arztunterstützend,
nicht arztersetzend!
Prozess-unterstützend

Digitalisierung:was heißt das überhaupt?
• Prozesse des Gesundheitswesens
- werden durch digitale Anwendungen unterstützt
- innerhalb einzelner Versorgungsinstitutionen
- aber auch über deren Grenzen hinweg
• Digitale Technologien sind Alltag in Praxen und Kliniken
• Digitale Technologien unterstützen direkt den Patienten
• Spitzenreiter im Bertelsmann-Ranking haben effektive nationale Strategien, politische Führung und eine nationale Koordinationsstelle

Digitalisierung:was heißt das überhaupt?
• Prozesse des Gesundheitswesens
- werden durch digitale Anwendungen unterstützt
- innerhalb einzelner Versorgungsinstitutionen
- aber auch über deren Grenzen hinweg
• Digitale Technologien sind Alltag in Praxen und Kliniken
• Digitale Technologien unterstützen direkt den Patienten
• Spitzenreiter im Bertelsmann-Ranking haben effektive nationale Strategien, politische Führung und eine nationale Koordinationsstelle
Digitale Prozesse generieren Daten
Medical Data Scientists kurieren und integrieren diese Daten . . .
und machen sie für Analysen zu neuem Erkenntnisgewinn nutzbar

Nationale StrategienDie Medizininformatik - Initiative
Daten aus Krankenversorgung und Forschung integrieren
• zur Verbesserung der medizinischen Forschung und der Krankenversorgung
• Aufbau von Datenintegrationszentren
• Entwicklung innovativer IT-Lösungen für medizinische Use Cases
• 150 Mio Euro
• zur Vernetzung der Daten der deutschen Universitätsklinika
November 2015

1. Konzeptphase2. Aufbau &
Vernetzungsphase
3. Konsolidierungs-&
Ausbauphase
Audit Audit2016 - 17 2018 - 21 2022 - 25
Phase 1: 7 Konsortien Phase 2: 4 Konsortien (120M€) begleitendeMaßnahmen
• Neuaufnahmen(30M€)
• NSG / Koordinierungs-stelle
• Ergänzende Fördermodule
Announcement 2015
DGP KongressMünchen 15.03.2019
Digitalisierung führt zu DatenDaten müssen effizient genutzt werden

MI-I: die geförderten Konsortien

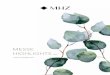
MIRACUMUnsere Konsortialpartner . . .
• zehn Universitätskliniken und Medizinische Fakultäten
• zwei Hochschulen
• ein Industriepartner (Averbis GmbH)
• . . . verteilt übersieben Bundesländer

Was macht MIRACUM?

5
MIRACUM DIZ Architektur
Research Data
Repositories
MI-I Kerndatensatz(fünf Basis Module):• Person• Demographie• Falldaten• Diagnosen• Prozeduren
OMOPDaten
Harmonisierung4b
DIZ = Datenintegrationszentrum

MIRACUM Datenschutzkonzept Mai 2018
• keine Daten verlassen den Standort an dem sie erhoben wurden
• verteilte Analysen „bring the analysis to the data“
Aus Sicht des Bayerischen Landesbeauftragten für den Datenschutz gibt es zum anliegenden Datenschutzkonzept . . . Keine weiteren Anmerkungen.

48
MIRACUM Föderation„Bring the analysis to the data“
R-ScriptSQL-
Statement
Erlangen
Magdeburg
Frankfurt GießenFreiburg
Mainz MarburgMannheim
OMOP OMOPOMOPOMOP
OMOPOMOP
OMOP OMOP
Greifswald
OMOP
Dresden
OMOP
Prokosch H.U: MIRACUM –Standortübergreifende Datennutzung für ein lernendes Gesundheitssystem

49
R-ScriptSQL-
Statement
Erlangen
Magdeburg
Frankfurt GießenFreiburg
Mainz MarburgMannheim
OMOP OMOPOMOPOMOP
OMOPOMOP
OMOP OMOP
Greifswald
OMOP
Dresden
OMOP
aggregierte Ergebnisse
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
Prokosch H.U: MIRACUM –Standortübergreifende Datennutzung für ein lernendes Gesundheitssystem
MIRACUM Föderation„Bring the analysis to the data“

50
R-ScriptSQL-
Statement
Erlangen
Magdeburg
Frankfurt GießenFreiburg
Mainz MarburgMannheim
OMOP OMOPOMOPOMOP
OMOPOMOP
OMOP OMOP
Greifswald
OMOP
Dresden
OMOP
Proof-of-Concept Analysen:
• Stroke / Thrombektomie: Leitlinien Adhärenz• Kolorektales Karzinom: Analyse der Therapiemuster
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
SQL / R
Prokosch H.U: MIRACUM –Standortübergreifende Datennutzung für ein lernendes Gesundheitssystem
MIRACUM Föderation„Bring the analysis to the data“

• Proof-of-Concept Analysen:• Stroke / Thrombektomie: Leitlinien Adhärenz
• Kolorektales Karzinom: Analyse der Therapiemuster
MIRACUMfrüher „Nutzen“ für Kliniker/med. Forscher
„Harvesting Low Hanging Fruit“

From Data to Knowledge„Maschinelles Lernen“

MIRACUM Use Case 2Prädiktionsmodellefür COPD/Asthma und Hirntumoren
• Modelle zur Vorhersage von prognostisch relevanten Untergruppen entwickeln
• Vorhersagemodelle in die klinische Praxis bringen
• Das Ganze am Beispiel von
• Asthma/COPD und
• Hirntumoren Unsaubere klinische Routinedaten
hochdimensionaler Datensatz mit genetischen Daten

Internationale KooperationenVerteiltes Maschinelles Lernen
Budin-Ljøsne I, et al. DataSHIELD: an ethically robust solution to multiple-site individual-level data analysis. Public Health Genomics. 2015;18(2):87-96.
Gaye A, et al. DataSHIELD: taking the analysis to the data, not the data to the analysis. Int J Epidemiol. 2014 Dec;43(6):1929-44.

Internationale KooperationenVerteiltes Maschinelles Lernen
Budin-Ljøsne I, et al. DataSHIELD: an ethically robust solution to multiple-site individual-level data analysis. Public Health Genomics. 2015;18(2):87-96.
Gaye A, et al. DataSHIELD: taking the analysis to the data, not the data to the analysis. Int J Epidemiol. 2014 Dec;43(6):1929-44.
. . . taking the analysis to the data, not the data to the analysis
. . . an ethically robust solutionto multiple-site individual-level data analysis

(oder beliebige Analyse)
Verteiltes Deep Learning mit generativen Modellen
2
2
3
Forscher
Klinik 1
1
Klinik 2
1
Vielen Dank an Stefan Lenz (Universität Freiburg)

Daten, Daten, und nochmal Daten
Konsolidierung eines gemeinsamen Datensatzes für COPD/ Asthma
• Welche Items sind für die Diagnose/ Beschreibung von COPD/ Asthma wichtig bzw. notwendig?
• Welche Items werden an den Standorten regelmäßig erhoben?
• Welche Items sind an den Standorten mit vertretbarem Aufwand für UC2 nutzbar?
Vielen Dank an Martin Boeker (Universität Freiburg)

Daten, Daten, und nochmal Daten
Ausgangsbasis aus Antragstellung
• Items• 12 Demographie und Vitalparameter
• 422 Labor (davon 349 Allergen-bezogen)
• 38 Lungenfunktion
• 4 kardial
• 4 Standardfragebögen
• 5 Diagnose und Medikation
• 2 Bildgebung
• Ergänzt um Items zu Funktionstests

Items für die Diagnostik von Asthma/COPD Bitte kreuzen Sie bei jedem Item an, für wie wichtig Sie es in der Diagnostik von Asthma/COPD einschätzen: -2 = keine Bedeutung, -1 = weniger wichtig, 1 = wichtig, 2 = entscheidend für Diagnose. Geben Sie bitte auch an, ob das Item regelmäßig bei Ihnen während der Diagnostik von Asthma/COPD erhoben wird. Durch wiederholtes Klicken wird eine Markierung wieder entfernt.
Item oder Gruppe Nützlich für Diagnostik Erhebung
-2 -1 1 2 NEIN JA
Demographie Geburtsdatum
Nationalität
Geschlecht
Ethnizität
Vitalparameter bei Aufnahme Größe
Gewicht
BMI
Temp
RR
Puls
SO2
Atemfrequenz
Labor Leukozyten
Erythrozyten
Thrombozyten
Hämoglobin
Hämatokrit
Neutrophile in Prozent
Lymphozyten in Prozent
Monozyten in Prozent
Eosinophile in Prozent
Basophile in Prozent
Serum-Kreatinin
Harnstoff im Serum
Harnsäure
CRP
Alpha-1-Antitrypsin
Triglyceride
Vielen Dank an Martin Boeker (Universität Freiburg)
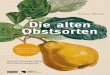
Daten, Daten, und nochmal Daten aber haben wir diese Daten überhaupt?
Konsolidierung auf 165 Datenelemente

Vielen Dank an Martin Boeker (Universität Freiburg)
Daten, Daten, und nochmal Daten aber haben wir diese Daten überhaupt?
0% 50% 100%
G eb ur tsd at um
N ati on ali tät
G es chl ec ht
Et hn iz itä t
V ita lpa ra me te r b ei Au fn ah m e
G rö ße
G ew ic ht
B MI
Te m p
R R
P uls
SO 2
A tem f req ue nz
La bo r
Le uk oz yt en
Er yt hr ozy te n
Th ro m bo zy ten
H äm og lo bin
H äm at ok rit
N eu tro ph ile in P roz en t
Ly m ph oz yte n in Pr oze nt
M on oz yt en in Pr oz en t
Eo si no ph ile in Pr oz en t
B aso ph ile in P ro zen t
Se ru m -Kr ea tin in
H arn st of f im S er um
H arn sä ur e
C RP
A lph a- 1-A n titr yp sin
Tr ig lyc eri de
G es am t-C h ole ste ri n
LD L- Ch ol est er in
H DL -C ho les te rin
G luk os e
H BA 1c
K rea tin in in U rin
Ig E g es am t
A NA
A NC A
R F
C CP
Tr yp ta se (A lle rge n- Ak tiv ie run gs m ark er )
B SG (B lut se nk un gs ge sch w ind ig ke it)
D iffe re nz ial blu tb ild
K lein e s B lut bi ld
Le uk oz yt en (G /l)
Er yt hr ozy te n ( T/ l)
H äm og lo bin (g /l )
H äm at ok rit (l/ l)
M CV (f l)
M CH ( pg )
M CH C (g /l E ry )
N eu tro ph ile (% )
Ly m ph oz yte n (% )
M on oz yt en (% )
Eo si no ph ile (% )
B aso ph ile (% )
Th ro m bo zy ten (G /l )
N eu tro ph ile (a bs .) (G /l)
Ly m ph oz yte n (ab s. ) (G /l )
M on oz yt en (a bs .) ( G/ l)
Eo si no ph ile (a bs .) ( G/ l)
B aso ph ile (a bs .) (G /L)
Eo si no ph ile (A sz ite s)
Eo si no ph ile (D ia lys at)
Eo si no ph ile (L iqu or )
Eo si no ph ile (P leu ra pu nk ta t)
Eo si no ph ile (S hu nt liq uo r)
Eo si no ph ile (S yn ov ia)
Le uk oz yt en (A sz ite s)
Le uk oz yt en (D ial ys at)
Le uk oz yt en (L iqu or )
Le uk oz yt en (P leu ra pu nk ta t)
Le uk oz yt en (S hu nt liq uo r)
Le uk oz yt en (S yn ov ia)
a1 -A nt itr yp sin
B rai n n at riu re tic pe pt id e ( BN P)
C -re ak tiv es Pr ote in
Ig A
Ig E, ge sa mt
Ig G
Ig M
In te rle uk in 6
In te rle uk in 8
P roc al cit on in
TN F al ph a
Fi br ino ge n
IL 17
IL 23
M PO
A lle rge ne
A lle rge n mo ld m ix 1
A lle rge n mo ld m ix 2
A lle rge n mo ld m ix 3
A lle rge n mo ld m ix 4
A lle rge n mo ld m ix 5
A lle rge n mo ld m ix 6
A lle rge n mo ld m ix 7
Lu ng en fu nk tio n
V or Ly se
V cin
FV C
FE V 1
IC
Sr to t
R tot
TL C
R V
D LC Oc
D LC Oc / V A
P EF
MEF 7 5
MEF 5 0
MEF 2 5
N ac h L ys e
V cin
FV C
FE V 1
IC
Sr to t
R tot
TL C
R V
D LC Oc
D LC Oc / V A
P EF
MEF 7 5
MEF 5 0
MEF 2 5
B lut ga san al ys e
R L v s. O2
p H
p O2
p CO 2
SO 2
B ika rb on at
B ase E xce ss
6 MW T
G eh str ec ke
SO 2 un te r B el ast un g
B org -S ka la Be gin n
B org -S ka la En de
D SP
B GA n ach B ela st un g
A rt d e r B ela st un g
p H
p O2
p CO 2
SO 2
B ika rb on at
B ase E xce ss
Fe N O
U ns pe zif isc he Pr ov ok ati on ste st s
FE V 1 - -pr e d o se me th ac ho lin e
FE V 1 - -po st do se m et ha ch oli ne
M et ha ch oli ne [M a ss] of D ose
FE V 1 - -po st 0. 02 5 m g /m L m e th ac ho lin e
FE V 1 - -po st 0. 25 m g/ mL m et ha ch oli ne
FE V 1 - -po st 2. 5 m g /m L m e th ac ho lin e
FE V 1 - -po st 10 m g/ m L m et ha ch ol ine
FE V 1 - -po st 25 m g/ m L m et ha ch ol ine
K ard ia le Dia gn os tik
EK G
U KG
LZ -E KG
St an da rd fra ge bö ge n
C OP D
m M RC
C AT
SG R Q
A sth m a
A CT
D iag no se n u n d M e ds
V oll stä nd ig e D ia gn ose nl ist e
H au ptd ia gn os e
A mb ul an t/S ta tio nä r
V oll stä nd ig e M e dik am e nte nl ist e
B eru fs an am ne se
B ild ge bu ng
R ö-T ho ra x
C T-T ho ra x
Verfügbarkeit
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
GeburtsdatumNationalitätGeschlecht
Ethnizität
Vitalparameter bei AufnahmeGröße
GewichtBMI
TempRR
PulsSO2
Atemfrequenz
LaborLeukozyten
ErythrozytenThrombozyten
HämoglobinHämatokrit
Neutrophile in ProzentLymphozyten in Prozent
Monozyten in ProzentEosinophile in Prozent
Basophile in ProzentSerum-Kreatinin
Harnstoff im SerumHarnsäure
CRPAlpha-1-Antitrypsin
Triglyceride
Gesamt-CholesterinLDL-CholesterinHDL-Cholesterin
GlukoseHBA1c
Kreatinin in UrinIgE gesamt
ANAANCA
RFCCP
Tryptase (Allergen-Aktivierungsmarker)BSG (Blutsenkungsgeschwindigkeit)
DifferenzialblutbildKleines Blutbild
Leukozyten (G/l)Erythrozyten (T/l)Hämoglobin (g/l)
Hämatokrit (l/l)MCV (fl)
MCH (pg)MCHC (g/l Ery)
Neutrophile (%)Lymphozyten (%)
Monozyten (%)Eosinophile (%)
Basophile (%)Thrombozyten (G/l)
Neutrophile (abs.) (G/l)Lymphozyten (abs.) (G/l)
Monozyten (abs.) (G/l)Eosinophile (abs.) (G/l)
Basophile (abs.) (G/L)
Eosinophile (Aszites)Eosinophile (Dialysat)
Eosinophile (Liquor)Eosinophile (Pleurapunktat)
Eosinophile (Shuntliquor)Eosinophile (Synovia)Leukozyten (Aszites)
Leukozyten (Dialysat)Leukozyten (Liquor)
Leukozyten (Pleurapunktat)Leukozyten (Shuntliquor)
Leukozyten (Synovia)a1-Antitrypsin
Brain natriuretic peptide (BNP)C-reaktives Protein
IgAIgE, gesamt
IgGIgM
Interleukin 6Interleukin 8Procalcitonin
TNF alphaFibrinogen
IL17IL23
MPO
AllergeneAllergen mold mix 1Allergen mold mix 2Allergen mold mix 3Allergen mold mix 4Allergen mold mix 5
Allergen mold mix 6Allergen mold mix 7
LungenfunktionVor Lyse
VcinFVC
FEV1IC
SrtotRtotTLCRV
DLCOcDLCOc / VA
PEFMEF 75MEF 50MEF 25
Nach LyseVcinFVC
FEV1IC
SrtotRtotTLCRV
DLCOcDLCOc / VA
PEFMEF 75
MEF 50MEF 25
BlutgasanalyseRL vs. O2
pHpO2
pCO2SO2
BikarbonatBase Excess
6MWTGehstrecke
SO2 unter BelastungBorg-Skala Beginn
Borg-Skala EndeDSP
BGA nach BelastungArt der Belastung
pHpO2
pCO2SO2
BikarbonatBase Excess
FeNO
Unspezifische ProvokationstestsFEV1 --pre dose methacholine
FEV1 --post dose methacholineMethacholine [Mass] of Dose
FEV1 --post 0.025 mg/mL methacholineFEV1 --post 0.25 mg/mL methacholine
FEV1 --post 2.5 mg/mL methacholineFEV1 --post 10 mg/mL methacholineFEV1 --post 25 mg/mL methacholine
Kardiale DiagnostikEKGUKG
LZ-EKG
StandardfragebögenCOPD
mMRCCAT
SGRQAsthma
ACT
Diagnosen und MedsVollständige Diagnosenliste
HauptdiagnoseAmbulant/Stationär
Vollständige MedikamentenlisteBerufsanamnese
BildgebungRö-ThoraxCT-Thorax
Keine Bedeutung Weniger wichtig Wichtig Entscheidend für Diagnose

Vielen Dank an Martin Boeker (Universität Freiburg)
Daten, Daten, und nochmal Daten aber haben wir diese Daten überhaupt?
0% 50% 100%
G eb ur tsd at um
N ati on ali tät
G es chl ec ht
Et hn iz itä t
V ita lpa ra me te r b ei Au fn ah m e
G rö ße
G ew ic ht
B MI
Te m p
R R
P uls
SO 2
A tem f req ue nz
La bo r
Le uk oz yt en
Er yt hr ozy te n
Th ro m bo zy ten
H äm og lo bin
H äm at ok rit
N eu tro ph ile in P roz en t
Ly m ph oz yte n in Pr oze nt
M on oz yt en in Pr oz en t
Eo si no ph ile in Pr oz en t
B aso ph ile in P ro zen t
Se ru m -Kr ea tin in
H arn st of f im S er um
H arn sä ur e
C RP
A lph a- 1-A n titr yp sin
Tr ig lyc eri de
G es am t-C h ole ste ri n
LD L- Ch ol est er in
H DL -C ho les te rin
G luk os e
H BA 1c
K rea tin in in U rin
Ig E g es am t
A NA
A NC A
R F
C CP
Tr yp ta se (A lle rge n- Ak tiv ie run gs m ark er )
B SG (B lut se nk un gs ge sch w ind ig ke it)
D iffe re nz ial blu tb ild
K lein e s B lut bi ld
Le uk oz yt en (G /l)
Er yt hr ozy te n ( T/ l)
H äm og lo bin (g /l )
H äm at ok rit (l/ l)
M CV (f l)
M CH ( pg )
M CH C (g /l E ry )
N eu tro ph ile (% )
Ly m ph oz yte n (% )
M on oz yt en (% )
Eo si no ph ile (% )
B aso ph ile (% )
Th ro m bo zy ten (G /l )
N eu tro ph ile (a bs .) (G /l)
Ly m ph oz yte n (ab s. ) (G /l )
M on oz yt en (a bs .) ( G/ l)
Eo si no ph ile (a bs .) ( G/ l)
B aso ph ile (a bs .) (G /L)
Eo si no ph ile (A sz ite s)
Eo si no ph ile (D ia lys at)
Eo si no ph ile (L iqu or )
Eo si no ph ile (P leu ra pu nk ta t)
Eo si no ph ile (S hu nt liq uo r)
Eo si no ph ile (S yn ov ia)
Le uk oz yt en (A sz ite s)
Le uk oz yt en (D ial ys at)
Le uk oz yt en (L iqu or )
Le uk oz yt en (P leu ra pu nk ta t)
Le uk oz yt en (S hu nt liq uo r)
Le uk oz yt en (S yn ov ia)
a1 -A nt itr yp sin
B rai n n at riu re tic pe pt id e ( BN P)
C -re ak tiv es Pr ote in
Ig A
Ig E, ge sa mt
Ig G
Ig M
In te rle uk in 6
In te rle uk in 8
P roc al cit on in
TN F al ph a
Fi br ino ge n
IL 17
IL 23
M PO
A lle rge ne
A lle rge n mo ld m ix 1
A lle rge n mo ld m ix 2
A lle rge n mo ld m ix 3
A lle rge n mo ld m ix 4
A lle rge n mo ld m ix 5
A lle rge n mo ld m ix 6
A lle rge n mo ld m ix 7
Lu ng en fu nk tio n
V or Ly se
V cin
FV C
FE V 1
IC
Sr to t
R tot
TL C
R V
D LC Oc
D LC Oc / V A
P EF
MEF 7 5
MEF 5 0
MEF 2 5
N ac h L ys e
V cin
FV C
FE V 1
IC
Sr to t
R tot
TL C
R V
D LC Oc
D LC Oc / V A
P EF
MEF 7 5
MEF 5 0
MEF 2 5
B lut ga san al ys e
R L v s. O2
p H
p O2
p CO 2
SO 2
B ika rb on at
B ase E xce ss
6 MW T
G eh str ec ke
SO 2 un te r B el ast un g
B org -S ka la Be gin n
B org -S ka la En de
D SP
B GA n ach B ela st un g
A rt d e r B ela st un g
p H
p O2
p CO 2
SO 2
B ika rb on at
B ase E xce ss
Fe N O
U ns pe zif isc he Pr ov ok ati on ste st s
FE V 1 - -pr e d o se me th ac ho lin e
FE V 1 - -po st do se m et ha ch oli ne
M et ha ch oli ne [M a ss] of D ose
FE V 1 - -po st 0. 02 5 m g /m L m e th ac ho lin e
FE V 1 - -po st 0. 25 m g/ mL m et ha ch oli ne
FE V 1 - -po st 2. 5 m g /m L m e th ac ho lin e
FE V 1 - -po st 10 m g/ m L m et ha ch ol ine
FE V 1 - -po st 25 m g/ m L m et ha ch ol ine
K ard ia le Dia gn os tik
EK G
U KG
LZ -E KG
St an da rd fra ge bö ge n
C OP D
m M RC
C AT
SG R Q
A sth m a
A CT
D iag no se n u n d M e ds
V oll stä nd ig e D ia gn ose nl ist e
H au ptd ia gn os e
A mb ul an t/S ta tio nä r
V oll stä nd ig e M e dik am e nte nl ist e
B eru fs an am ne se
B ild ge bu ng
R ö-T ho ra x
C T-T ho ra x
Verfügbarkeit
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
GeburtsdatumNationalitätGeschlecht
Ethnizität
Vitalparameter bei AufnahmeGröße
GewichtBMI
TempRR
PulsSO2
Atemfrequenz
LaborLeukozyten
ErythrozytenThrombozyten
HämoglobinHämatokrit
Neutrophile in ProzentLymphozyten in Prozent
Monozyten in ProzentEosinophile in Prozent
Basophile in ProzentSerum-Kreatinin
Harnstoff im SerumHarnsäure
CRPAlpha-1-Antitrypsin
Triglyceride
Gesamt-CholesterinLDL-CholesterinHDL-Cholesterin
GlukoseHBA1c
Kreatinin in UrinIgE gesamt
ANAANCA
RFCCP
Tryptase (Allergen-Aktivierungsmarker)BSG (Blutsenkungsgeschwindigkeit)
DifferenzialblutbildKleines Blutbild
Leukozyten (G/l)Erythrozyten (T/l)Hämoglobin (g/l)
Hämatokrit (l/l)MCV (fl)
MCH (pg)MCHC (g/l Ery)
Neutrophile (%)Lymphozyten (%)
Monozyten (%)Eosinophile (%)
Basophile (%)Thrombozyten (G/l)
Neutrophile (abs.) (G/l)Lymphozyten (abs.) (G/l)
Monozyten (abs.) (G/l)Eosinophile (abs.) (G/l)
Basophile (abs.) (G/L)
Eosinophile (Aszites)Eosinophile (Dialysat)
Eosinophile (Liquor)Eosinophile (Pleurapunktat)
Eosinophile (Shuntliquor)Eosinophile (Synovia)Leukozyten (Aszites)
Leukozyten (Dialysat)Leukozyten (Liquor)
Leukozyten (Pleurapunktat)Leukozyten (Shuntliquor)
Leukozyten (Synovia)a1-Antitrypsin
Brain natriuretic peptide (BNP)C-reaktives Protein
IgAIgE, gesamt
IgGIgM
Interleukin 6Interleukin 8Procalcitonin
TNF alphaFibrinogen
IL17IL23
MPO
AllergeneAllergen mold mix 1Allergen mold mix 2Allergen mold mix 3Allergen mold mix 4Allergen mold mix 5
Allergen mold mix 6Allergen mold mix 7
LungenfunktionVor Lyse
VcinFVC
FEV1IC
SrtotRtotTLCRV
DLCOcDLCOc / VA
PEFMEF 75MEF 50MEF 25
Nach LyseVcinFVC
FEV1IC
SrtotRtotTLCRV
DLCOcDLCOc / VA
PEFMEF 75
MEF 50MEF 25
BlutgasanalyseRL vs. O2
pHpO2
pCO2SO2
BikarbonatBase Excess
6MWTGehstrecke
SO2 unter BelastungBorg-Skala Beginn
Borg-Skala EndeDSP
BGA nach BelastungArt der Belastung
pHpO2
pCO2SO2
BikarbonatBase Excess
FeNO
Unspezifische ProvokationstestsFEV1 --pre dose methacholine
FEV1 --post dose methacholineMethacholine [Mass] of Dose
FEV1 --post 0.025 mg/mL methacholineFEV1 --post 0.25 mg/mL methacholine
FEV1 --post 2.5 mg/mL methacholineFEV1 --post 10 mg/mL methacholineFEV1 --post 25 mg/mL methacholine
Kardiale DiagnostikEKGUKG
LZ-EKG
StandardfragebögenCOPD
mMRCCAT
SGRQAsthma
ACT
Diagnosen und MedsVollständige Diagnosenliste
HauptdiagnoseAmbulant/Stationär
Vollständige MedikamentenlisteBerufsanamnese
BildgebungRö-ThoraxCT-Thorax
Keine Bedeutung Weniger wichtig Wichtig Entscheidend für Diagnose
0% 50% 100%
G eb ur tsd at um
N ati on ali tät
G es chl ec ht
Et hn iz itä t
V ita lpa ra me te r b ei Au fn ah m e
G rö ße
G ew ic ht
B MI
Te m p
R R
P uls
SO 2
A tem f req ue nz
La bo r
Le uk oz yt en
Er yt hr ozy te n
Th ro m bo zy ten
H äm og lo bin
H äm at ok rit
N eu tro ph ile in P roz en t
Ly m ph oz yte n in Pr oze nt
M on oz yt en in Pr oz en t
Eo si no ph ile in Pr oz en t
B aso ph ile in P ro zen t
Se ru m -Kr ea tin in
H arn st of f im S er um
H arn sä ur e
C RP
A lph a- 1-A n titr yp sin
Tr ig lyc eri de
G es am t-C h ole ste ri n
LD L- Ch ol est er in
H DL -C ho les te rin
G luk os e
H BA 1c
K rea tin in in U rin
Ig E g es am t
A NA
A NC A
R F
C CP
Tr yp ta se (A lle rge n- Ak tiv ie run gs m ark er )
B SG (B lut se nk un gs ge sch w ind ig ke it)
D iffe re nz ial blu tb ild
K lein e s B lut bi ld
Le uk oz yt en (G /l)
Er yt hr ozy te n ( T/ l)
H äm og lo bin (g /l )
H äm at ok rit (l/ l)
M CV (f l)
M CH ( pg )
M CH C (g /l E ry )
N eu tro ph ile (% )
Ly m ph oz yte n (% )
M on oz yt en (% )
Eo si no ph ile (% )
B aso ph ile (% )
Th ro m bo zy ten (G /l )
N eu tro ph ile (a bs .) (G /l)
Ly m ph oz yte n (ab s. ) (G /l )
M on oz yt en (a bs .) ( G/ l)
Eo si no ph ile (a bs .) ( G/ l)
B aso ph ile (a bs .) (G /L)
Eo si no ph ile (A sz ite s)
Eo si no ph ile (D ia lys at)
Eo si no ph ile (L iqu or )
Eo si no ph ile (P leu ra pu nk ta t)
Eo si no ph ile (S hu nt liq uo r)
Eo si no ph ile (S yn ov ia)
Le uk oz yt en (A sz ite s)
Le uk oz yt en (D ial ys at)
Le uk oz yt en (L iqu or )
Le uk oz yt en (P leu ra pu nk ta t)
Le uk oz yt en (S hu nt liq uo r)
Le uk oz yt en (S yn ov ia)
a1 -A nt itr yp sin
B rai n n at riu re tic pe pt id e ( BN P)
C -re ak tiv es Pr ote in
Ig A
Ig E, ge sa mt
Ig G
Ig M
In te rle uk in 6
In te rle uk in 8
P roc al cit on in
TN F al ph a
Fi br ino ge n
IL 17
IL 23
M PO
A lle rge ne
A lle rge n mo ld m ix 1
A lle rge n mo ld m ix 2
A lle rge n mo ld m ix 3
A lle rge n mo ld m ix 4
A lle rge n mo ld m ix 5
A lle rge n mo ld m ix 6
A lle rge n mo ld m ix 7
Lu ng en fu nk tio n
V or Ly se
V cin
FV C
FE V 1
IC
Sr to t
R tot
TL C
R V
D LC Oc
D LC Oc / V A
P EF
M EF 7 5
M EF 5 0
M EF 2 5
N ac h L ys e
V cin
FV C
FE V 1
IC
Sr to t
R tot
TL C
R V
D LC Oc
D LC Oc / V A
P EF
M EF 7 5
M EF 5 0
M EF 2 5
B lut ga san al ys e
R L v s. O2
p H
p O2
p CO 2
SO 2
B ika rb on at
B ase E xce ss
6 MW T
G eh str ec ke
SO 2 un te r B el ast un g
B org -S ka la Be gin n
B org -S ka la En de
D SP
B GA n ach B ela st un g
A rt d e r B ela st un g
p H
p O2
p CO 2
SO 2
B ika rb on at
B ase E xce ss
Fe N O
U ns pe zif isc he Pr ov ok ati on ste st s
FE V 1 - -pr e d o se me th ac ho lin e
FE V 1 - -po st do se m et ha ch oli ne
M et ha ch oli ne [M a ss] of D ose
FE V 1 - -po st 0. 02 5 m g /m L m e th ac ho lin e
FE V 1 - -po st 0. 25 m g/ mL m et ha ch oli ne
FE V 1 - -po st 2. 5 m g /m L m e th ac ho lin e
FE V 1 - -po st 10 m g/ m L m et ha ch ol ine
FE V 1 - -po st 25 m g/ m L m et ha ch ol ine
K ard ia le Dia gn os tik
EK G
U KG
LZ -E KG
St an da rd fra ge bö ge n
C OP D
m M RC
C AT
SG R Q
A sth m a
A CT
D iag no se n u n d M e ds
V oll stä nd ig e D ia gn ose nl ist e
H au ptd ia gn os e
A mb ul an t/S ta tio nä r
V oll stä nd ig e M e dik am e nte nl ist e
B eru fs an am ne se
B ild ge bu ng
R ö-T ho ra x
C T-T ho ra x
Verfügbarkeit
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
GeburtsdatumNationalitätGeschlecht
Ethnizität
Vitalparameter bei AufnahmeGröße
GewichtBMI
TempRR
PulsSO2
Atemfrequenz
LaborLeukozyten
ErythrozytenThrombozyten
HämoglobinHämatokrit
Neutrophile in ProzentLymphozyten in Prozent
Monozyten in ProzentEosinophile in Prozent
Basophile in ProzentSerum-Kreatinin
Harnstoff im SerumHarnsäure
CRPAlpha-1-Antitrypsin
Triglyceride
Gesamt-CholesterinLDL-CholesterinHDL-Cholesterin
GlukoseHBA1c
Kreatinin in UrinIgE gesamt
ANAANCA
RFCCP
Tryptase (Allergen-Aktivierungsmarker)BSG (Blutsenkungsgeschwindigkeit)
DifferenzialblutbildKleines Blutbild
Leukozyten (G/l)Erythrozyten (T/l)Hämoglobin (g/l)
Hämatokrit (l/l)MCV (fl)
MCH (pg)MCHC (g/l Ery)
Neutrophile (%)Lymphozyten (%)
Monozyten (%)Eosinophile (%)
Basophile (%)Thrombozyten (G/l)
Neutrophile (abs.) (G/l)Lymphozyten (abs.) (G/l)
Monozyten (abs.) (G/l)Eosinophile (abs.) (G/l)
Basophile (abs.) (G/L)
Eosinophile (Aszites)Eosinophile (Dialysat)
Eosinophile (Liquor)Eosinophile (Pleurapunktat)
Eosinophile (Shuntliquor)Eosinophile (Synovia)Leukozyten (Aszites)
Leukozyten (Dialysat)Leukozyten (Liquor)
Leukozyten (Pleurapunktat)Leukozyten (Shuntliquor)
Leukozyten (Synovia)a1-Antitrypsin
Brain natriuretic peptide (BNP)C-reaktives Protein
IgAIgE, gesamt
IgGIgM
Interleukin 6Interleukin 8Procalcitonin
TNF alphaFibrinogen
IL17IL23
MPO
AllergeneAllergen mold mix 1Allergen mold mix 2Allergen mold mix 3Allergen mold mix 4Allergen mold mix 5
Allergen mold mix 6Allergen mold mix 7
LungenfunktionVor Lyse
VcinFVC
FEV1IC
SrtotRtotTLCRV
DLCOcDLCOc / VA
PEFMEF 75MEF 50MEF 25
Nach LyseVcinFVC
FEV1IC
SrtotRtotTLCRV
DLCOcDLCOc / VA
PEFMEF 75
MEF 50MEF 25
BlutgasanalyseRL vs. O2
pHpO2
pCO2SO2
BikarbonatBase Excess
6MWTGehstrecke
SO2 unter BelastungBorg-Skala Beginn
Borg-Skala EndeDSP
BGA nach BelastungArt der Belastung
pHpO2
pCO2SO2
BikarbonatBase Excess
FeNO
Unspezifische ProvokationstestsFEV1 --pre dose methacholine
FEV1 --post dose methacholineMethacholine [Mass] of Dose
FEV1 --post 0.025 mg/mL methacholineFEV1 --post 0.25 mg/mL methacholine
FEV1 --post 2.5 mg/mL methacholineFEV1 --post 10 mg/mL methacholineFEV1 --post 25 mg/mL methacholine
Kardiale DiagnostikEKGUKG
LZ-EKG
StandardfragebögenCOPD
mMRCCAT
SGRQAsthma
ACT
Diagnosen und MedsVollständige Diagnosenliste
HauptdiagnoseAmbulant/Stationär
Vollständige MedikamentenlisteBerufsanamnese
BildgebungRö-ThoraxCT-Thorax
Keine Bedeutung Weniger wichtig Wichtig Entscheidend für Diagnose

Vielen Dank an Martin Boeker (Universität Freiburg)
• Daten Mapping (LOINC, SNOMED)• Gemeinsames Datenmodell (OMOP)
Daten, Daten, und nochmal Daten … müssen harmonisiert werden

Vielen Dank an Martin Boeker (Universität Freiburg)
• Daten Mapping (LOINC, SNOMED)• Gemeinsames Datenmodell (OMOP)
Daten, Daten, und nochmal Daten … müssen harmonisiert werden

5
Daten, Daten, und nochmal Daten … müssen aufbereitet und zusammengeführt werden
Research Data
Repositories
MI-I Kerndatensatz(fünf Basis Module):• Person• Demographie• Falldaten• Diagnosen• Prozeduren• Daten für die
MIRACUM Use Cases
OMOPDaten
Harmonisierung4b
Datenbefüllung(ETL)

• Wir dürfen weder zu schwarz, noch zu weiß sehen
• Nicht jedem Hype blind hinterher laufen
• Koordinierte Digitalisierung auf Basis eines nationalen Konzepts kann zum Segen werden
• Digitalisierung bringt Daten
• Daten sind der Schatz aus dem Erkenntnisse reifen
• (qualitativ hochwertige) Daten nutzbar machen ist die wichtigste, aber auch aufwändigste Aufgabe
Digitalisierung: Fluch oder Segen?

Vielen Dank dem MIRACUM Team
Förderkennzeichen: 01ZZ1801A
. . . und für Ihre Aufmerksamkeit