Embed Size (px)
Citation preview

1
Influenza
2009
Christoph Wenisch4.Medizinische Abteilung
SMZ-Süd KFJ Spital
2
Übertragen
► Tröpfcheninfektion► Schmierinfektion (Schneuzen, Nasenbohren)
Viren auf Gegenständen, Körperoberflächen, Kot
►mechanisch auf Haaren, Haut
2.5-4 Tage nach Ansteckung wird man krank►Longini 2009, Fergurson 2008
Influenza und Reise
Respiratory viruses were detected in 44 out of 118 (37%) travelers included in the study, representing56% of the patients with respiratory symptoms. Themost frequently viruses detected were influenza virus(38%), rhinovirus (23%), adenovirus (9%), and respiratory syncytial virus (9%).
► J Med Virol. 2008 Apr;80(4):711-5. Incidence of respiratoryviruses among travelers with a febrile syndrome returningfrom tropical and subtropical areas. Camps M, Vilella A, Marcos MA, Letang E, Muñoz J, Salvadó E, González A, Gascón J, Jiménez de Anta MT, Pumarola T.

3
Influenza beim Pilgern
► Fifty-four patients (10.8%) had positive viral throatcultures. Of these, 27 (50%) were influenza B, 13 (24.1%) were HSV, 7 (12.9%) were RSV, 4 (7.4%) were parainfluenza, and 3 (5.6%) were influenza A. No enteroviruses or adenoviruses were detected, and no multiple infections were detected. Only 22 (4.7%) pilgrims received the influenza vaccine. When theresults are applied to the total number of pilgrims in 2003, an estimate of 24,000 cases of influenza isobtained.
► J Travel Med. 2004 Mar-Apr;11(2):82-6. Influenza a common viral infection among Hajj pilgrims: time forroutine surveillance and vaccination. Balkhy HH, Memish ZA, Bafaqeer S, Almuneef MA.

4
Influenza und HIV► Fifty patients (median CD4(+) T cell count, 325
cells/microL; median HIV RNA level, <50 copies/mL). A causative pathogen was identified in 25 patients (50%). Even though 76% of subjects had received influenzavaccine, viral infections were diagnosed in 21 patients(42%), as follows: influenza A, 10 patients; influenza B, 10; and parainfluenza virus type 3 infection, 1.
►Antibiotic prescriptions were common: 70% of patientsreceived antibiotics. No patients with influenza requiredhospitalization, compared with 21% of other patients(P=.03).
► Clin Infect Dis. 2007 Jul 15;45(2):234-40. Epub 2007 Jun 12.Influenzavirus infection is a primary cause of febrilerespiratory illness in HIV-infected adults, despitevaccination. Klein MB, Lu Y, DelBalso L, Coté S, Boivin

5
Letalität
► Alter Tot durch Influenza►<1 88► 1-4 175► 5-49 2569► 50-64 4392►>64 43979► Total/Jahr 51203
Thompson, JAMA 2003; 289:179
Österreich 10 Fälle/Jahr

6
Influenza und Herz► Eur Heart J. 2007 May;28(10):1205-10. Epub 2007 Apr 17.
Influenza epidemics and acute respiratory diseaseactivity are associated with a surge in autopsy-confirmed coronary heart disease death: results from8 years of autopsies in 34,892 subjects Madjid M, Miller CC, Zarubaev VV, Marinich IG, Kiselev OI, LobzinYV, Filippov AE, Casscells SW 3rd.
►Median age was 75 for women and 65 for men. ►When comparing the average influenza epidemic weeks
to average off-season weeks, the odds for AMI and chronic IHD death increased by 1.30 (95% confidenceinterval (CI): 1.08-1.56) and 1.10 (95% CI: 0.97-1.26), respectively.
Neuraminidase
Hemagglutinin
RNA
M2 protein(only on type A)
Influenza Surface ProteinsInfluenza Surface Proteins

7
Influenza, respiratorische Erkrankungen und KHK-Todesfälle
•Madjid M et al. Eur Heart J 2007;28:1205-10
•Autopsieresultate über 8 Jahre in St. Petersburg; 34892 Autopsien
•Influenzaepidemien sind mit einer Erhöhung der autopsiegesicherten koronaren Todesfälle assoziiert
0
20
40
60
80
100
12019
93
1994
1995
1996
1997
1998
1999
2000
InfarktmortalitätAtemwegserkrankungen
•Fälle pro Woche
•Influenzaepidemie
AtemwegskomplikationenSekundäre bakterielle Pneumonie
– Betrifft ca. 75% der Patienten mit Influenza-Pneumonien
– Erreger: S. aureus (ca. 70%) in 1957-1958 Pandemie.
S. aureus mit 28 % Letalität, andere Erreger 12% Letalität
– 2-3 Tage nach Influenzabeginn akut Husten, Thoraxschmerzen und Dyspnoe. Klinisch Rasselgeräusche, selten Dämpfung.
– >> Dyspnoe, Tachypnoe, Zyanose und Hämoptoeschlechte Prognose: Tod nach 4-5 Tagen.
Pathologie: Hämorrhagien, keine Konsolidation. Hyperämie der Mucosa

8
Influenzapneumonie mit S.aureus Superinfektion
Influenza und Pneumokokken
►Asymptomatische Kolonisation►Epithelschaden durch Influenza►Adhärenz/Invasion von. S. pneumoniae
erleichtert►Verschlechterte anti-Streptokokken
Immunantwort►Amplifikation der inflammatorischen
Kaskade durch KoinfektionMcKuller JA, Clin Microbiol Rev 2006;19:571

9

10

11
Klinik der InfluenzaUntersuchung bei 520 Erwachsenen
HustenAbgeschlagenheitFiebergefühlplötzliches AuftretenSchüttelfrostKopfschmerzAppetitlosigkeitMyalgienHalswehSputumSchwindelgefühlHeiserkeitThoraxschmerzenNauseaFieber >37.8 ºC
% Influenza Fälle mit dem entsprechenden SymptomK.G. Nicholson: Managing Influenza in Primary Care. Blackwell Science,19
Differentialdiagnose Influenza versus“grippaler Infekt”
Influenza Grippaler InfektErreger: Influenzavirus A,B Rhinoviren, Adenoviren,
RS-viren, CoronavirenKlinischesSpektrum:
systemisch lokalisiert
Krankheitsbeginn: abrupt schrittweiseFieber: 38-41°C subfebrilTypischeSymptome:
Schüttelfrost, Myalgien,Husten, Halsschmerzen,Appetitlosigkeit
Niesen, Rhinorrhoe,trockener kratzender Hals
Krankheitsgefühl: ausgeprägt mildKrankheitsdauer: 1-2 Wochen (ev.
Postinfluenza-Asthenie)rasche Erholung
Komplikationen: hoch, incl. Mortalität geringAuftreten: Nördliche Hemisphäre: Nov.-
AprilSüdl. Hemisphäre: Mai-Okt.
ganzjährig
Das Lehrbuch, nicht die moderne PatientIn
12
Influenza und Lebensalter►>65 Jahre vs. < 65 Jahre► Krankheitsgefühl in 76.4% vs 92.6%, p = 0.07 ►Muskelschmerzen: 56.9% vs 77.8%, p = 0.06► Fieber: 54.2% vs 70.4%, p = 0.08► Kopfschmerzen: 35.2% vs 66.7%, p = 0.005► Leistungsknick: 47.2% vs 66.7%, p = 0.08►Husten: 94.4% vs 77.8%, p = 0.02 ► Spitalsaufnahme 65.3% vs 40.7%, p = 0.03 ► Antibiotika: 81.9% vs 63.0%, p = 0.046 ► Spitalsaufnahme korreliert mit
Begleiterkrankungen und fehlender Impfung►OR = 4.5, 95% IC 1.27-15.95, p = 0.02
► Infection. 2004 Apr;32(2):89-97. Unmasking influenza virus infection in patientsattended to in the emergency department. Monmany J, Rabella N, Margall N, Domingo P Gich I Vázquez G

13

14

15

16

17

18

19
20

21

22
Dr.Wenisch, Seuchenkurs, Würzburg - 2003

23
Global Preparedness plan (2005)Recommendations on global and
regional preparednessRecommendations on stockpiling and
use of antivirals and vaccines
The World Needs to Prepare for a Potential Influenza Pandemic
“The virus (H5N1) could ignite the next human flu pandemic. I do not need to tell you of the terrible consequences that could bring to all nations and all people. To be truly prepared we will need to mount a massive effort”Kofi Annan, Former Secretary General of the United Nations
“Community influenza preparedness and response planning” (November 2005)
A(H1N1) A(H2N2) A(H3N2)
“Spanish Flu” “Asian Flu” “Hong Kong Flu”
20-40 million deaths 1-4 million deaths 1-4 million deaths
Credit: US National Museum of Health and Medicine
20th Century Pandemics Have Caused Substantial Mortality and Morbidity
1918: 1957: 1968:

24
Weeks
How long is phase likely to last?
Decades Years Months 1-2 years
Status Could Progress from Current Alert to Full Pandemic
in a Few Monthsh5n1
What Will a Pandemic Mean for Society ?
►Pandemic life cycle►6 weeks to 3 months
Increasing absentee rates (≈20%)
Peak absentee rates (≈40–50%)
Falling absentee rates
Late deliveries Operations/offices shut down where critical employees affected
No deliveriesStores / offices / schools close
Operations resumeLower staff levelsConsumer demand remains depressed
Stressed infrastructure (e.g. call centre)Cancellation of events/meetings
Trade (food etc) markedly reducedHospitals full
Ongoing supply outages Repair costs
Peak impact RecoveryOutbreakPandemic life cycle:
6 weeks to 3 months
Estimated:• 1-1.5 billion people will require medical care
• 7-28 million hospitalizations
• 2-7.5 million deaths
Societalimpact
25
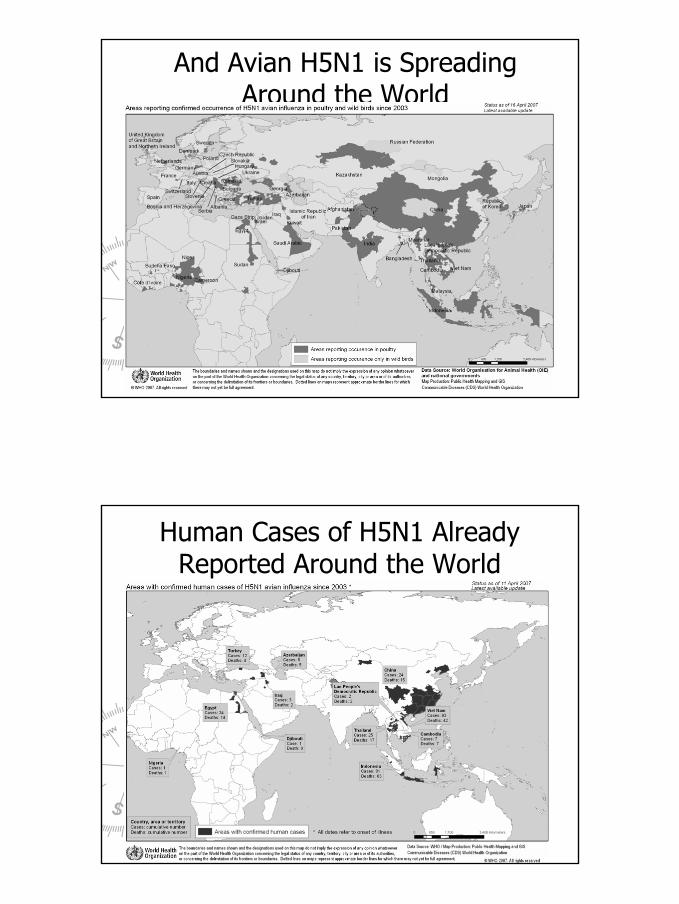
And Avian H5N1 is Spreading Around the World
Human Cases of H5N1 Already Reported Around the World

26
Weeks
How long is phase likely to last?
Decades Years Months 1-2 years
Status Could Progress from Current Alert to Full Pandemic
in a Few Monthsh5n1 h1n1
Dunn, J Am Med Assoc. 1958 Mar 8;166(10):1140-8
Example timings from 1957 Influenza Pandemic
An Influenza Pandemic Could Cross the World in a Few Months

27
Wer wurde krank?
28
WHO Has Recommended Antivirals for Use in case of an Influenza Pandemic
► Antiviral treatment in patients with confirmed or strongly suspected H5N1 infection
Applies to adults (including pregnant women) and children Regimen for H5N1 is as recommended for seasonal influenza
► Antiviral chemoprophylaxis in management of avian (H5N1) influenza
In high risk exposure groups oseltamivir / zanamivir (alternative) should be administered (strong recommendation)In moderate risk exposure groups oseltamivir / zanamivir might be administered (weak recommendation) Continuing for 7-10 days after the last known exposure
The Favourable Resistance Profile of Relenza is Important in Choice of Antivirals for Stockpiling in
case of an influenza pandemic
“..although both (Relenza zanamivir and Tamiflu oseltamivir) have similar efficacy, Relenza …..a favorable resistance profile.
The resistance factor would be an important consideration in a pandemic situation”
Tsang KW et al.Lancet 2005;366;533-534
“If this frequent emergence of resistant mutants is found to be a general occurrence in children, it is a serious concern, especially
since children are an important source of the spread of infection in the community.”
Moscona A. NEJM, Sept 2005; 353: 1363-1373

29
5%

30
31
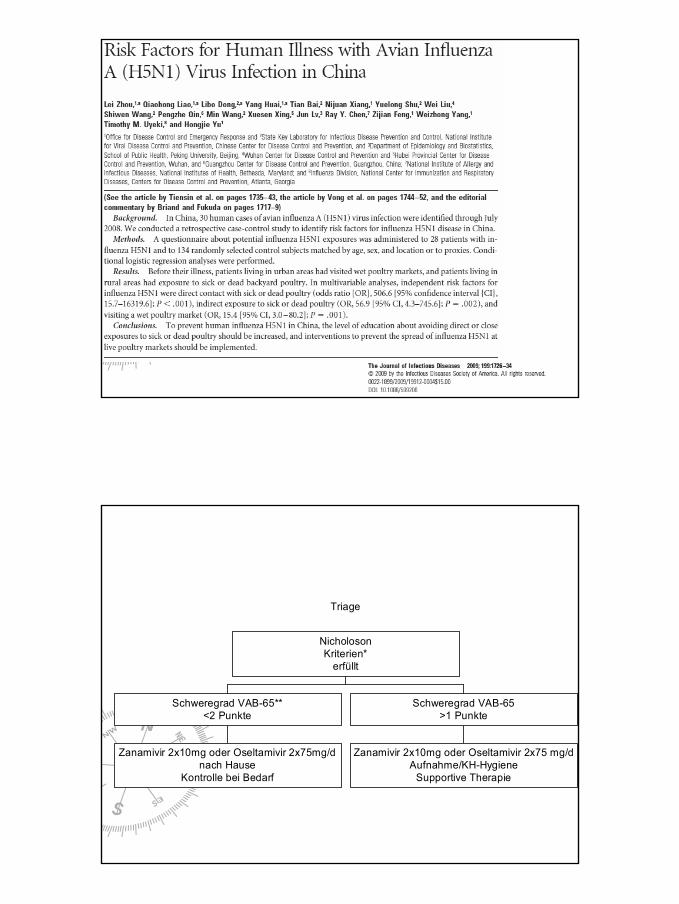
Triage
Zanamivir 2x10mg oder Oseltamivir 2x75mg/dnach Hause
Kontrolle bei Bedarf
Schweregrad VAB-65**<2 Punkte
Zanamivir 2x10mg oder Oseltamivir 2x75 mg/dAufnahme/KH-Hygiene
Supportive Therapie
Schweregrad VAB-65>1 Punkte
NicholosonKriterien*
erfüllt
32
Therapie-Anekdoten
►Rascher Therapiebeginn►Oseltamivir 2x150mg►Oseltamivir 2x150mg plus Amantadin
3x100mg►Kein Steroid►Oseltamivir plus Zanamivir
2009
Christoph Wenisch4.Medizinische Abteilung
SMZ-Süd KFJ Spital














![02 Moehrke Welpenaufzucht.ppt [Kompatibilitätsmodus] · Eigenständiger Kot-und Harnabsatz Vergrößerung des Aktionsradius Erstes Verlassen der Wurfbox ... Stronghold ® eliminiert](https://img.pdfslide.org/doc/110x75/5c78cf7e09d3f294278be961/02-moehrke-kompatibilitaetsmodus-eigenstaendiger-kot-und-harnabsatz-vergroesserung.jpg)














