Embed Size (px)
Citation preview
Metabolische Chirurgie –
wem empfehlen wir eine Operation?
Stefan Aczél
13. Juni 2019
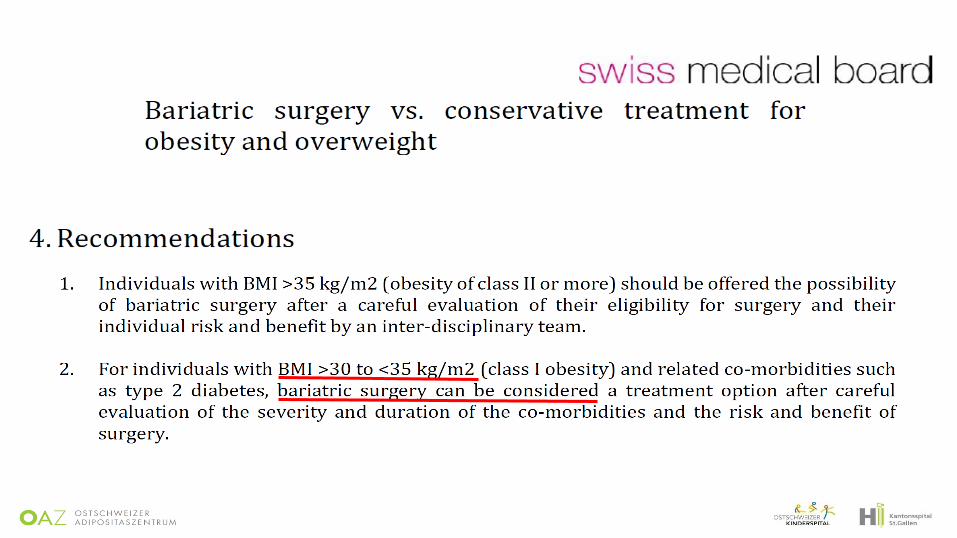
Indikationen gemäss SMOB
• BMI >= 35 kg/m2
• Eine zweijährige, adäquate Therapie zur Gewichtsreduktion war erfolglos
(BMI von >= 50 kg/m2: Dauer von 12 Monaten ausreichend).
• Schriftliche Einwilligung in die Verpflichtung zu lebenslanger Nachsorge
im bariatrischen Netzwerk eines akkreditierten Zentrums.
• Spezielle Kriterien bei < 18 bzw > 65 Jahren
• Metabolic surgery should be recommended as an option to treat type 2 diabetes in appropriate
surgical candidates with BMI ≥ 40 kg/m2 (BMI ≥ 37.5 kg/m2 in Asian Americans) and in adults with BMI
35.0–39.9 kg/m2 (32.5–37.4 kg/m2 in Asian Americans) who do not achieve durable weight loss and
improvement in comorbidities (including hyperglycemia) with reasonable nonsurgical methods. A
• Metabolic surgery may be considered as an option for adults with type 2 diabetes and BMI 30.0–34.9
kg/m2 (27.5–32.4 kg/m2 in Asian Americans) who do not achieve durable weight loss and
improvement in comorbidities (including hyperglycemia) with reasonable nonsurgical methods. A
• Metabolic surgery should be performed in high-volume centers with multidisciplinary teams that
understand and are experienced in the management of diabetes and gastrointestinal surgery. C
• Long-term lifestyle support and routine monitoring of micronutrient and nutritional status must be
provided to patients after surgery, according to guidelines for postoperative management of metabolic
surgery by national and international professional societies. C
• People presenting for metabolic surgery should receive a comprehensive readiness and mental
health assessment. B
• People who undergo metabolic surgery should be evaluated to assess the need for ongoing mental
health services to help them adjust to medical and psychosocial changes after surgery. C
ADA-Leitlinien
Diabetes Care 2019;42(Suppl. 1):S81–S89
Swedish Obese Subjects (SOS) Study
Beobachtungsstudie, Alter 37-60J., BMI Männer > 34 kg/m2, Frauen > 38 kg/m2
2010 Pat operiert vs 2037 in Kontrollgruppe, für 18 Variablen «gematcht»
Review: J Intern Med 2013, 273: 219-34
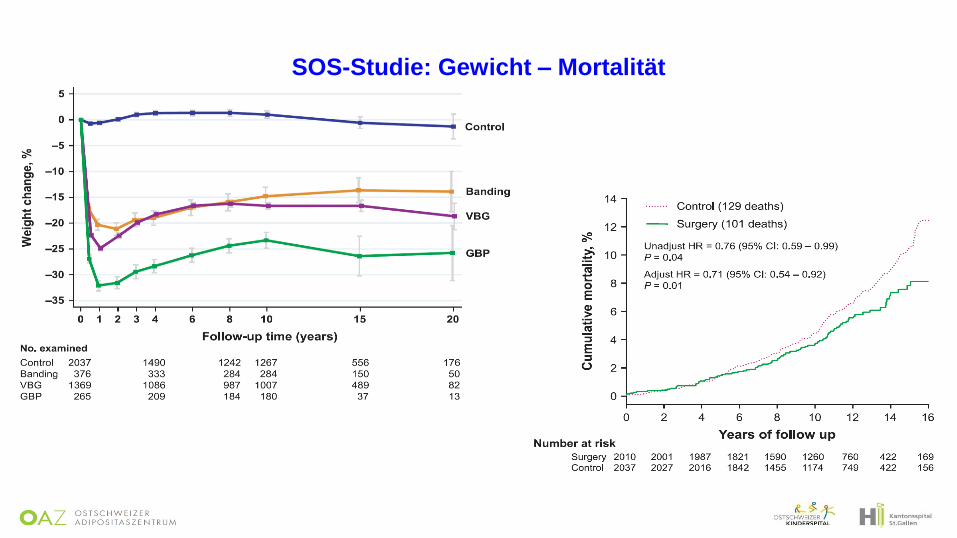
SOS-Studie: Gewicht – Mortalität
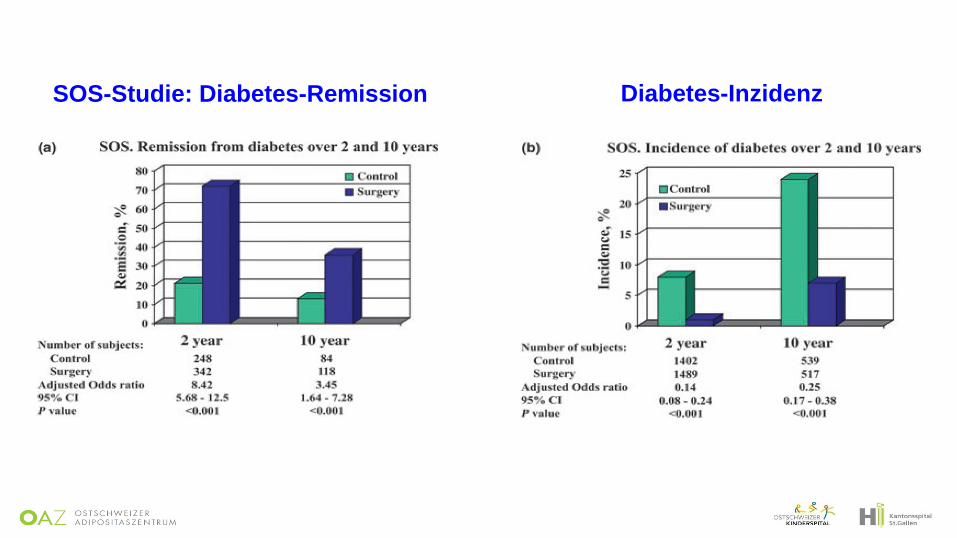
SOS-Studie: Diabetes-Remission Diabetes-Inzidenz
JAMA 2014; 311:2297-304
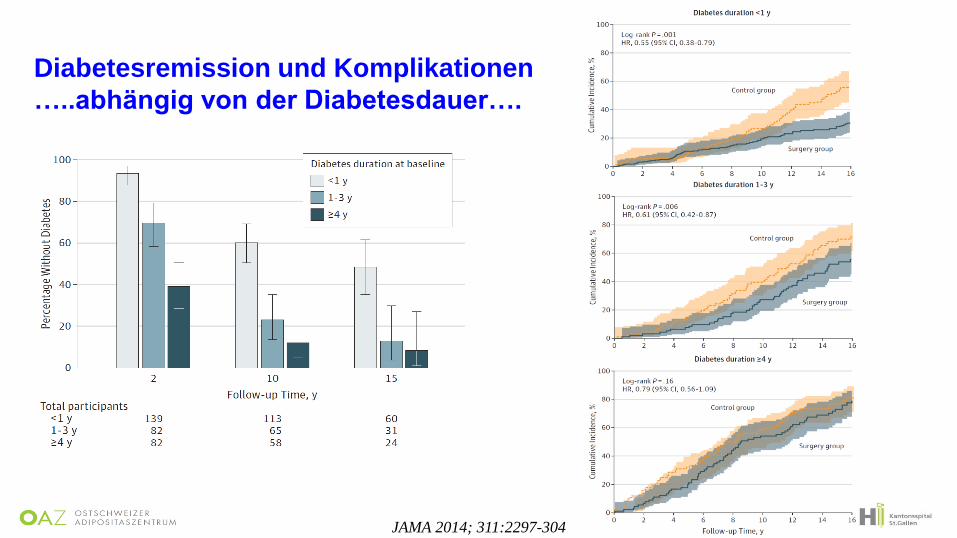
Diabetesremission und Komplikationen
…..abhängig von der Diabetesdauer….
NEJM 2017, 376:641-51
Surgical Treatment and Medications Potentially Eradicate Diabetes
Efficiently (STAMPEDE)
NEJM 2017, 376:641-51
Intensive konservative Therapie alleine oder plus RYGB oder plus Sleeve
Alter 49 Jahre, DM-Dauer 8 J., HbA1c: ca. 9% mit ca. 2.5 Antidiabetika, 45% Insulin
BMI ca 36 kg/m2, 34% < 35 kg/m2
NEJM 2017; 376:641-51
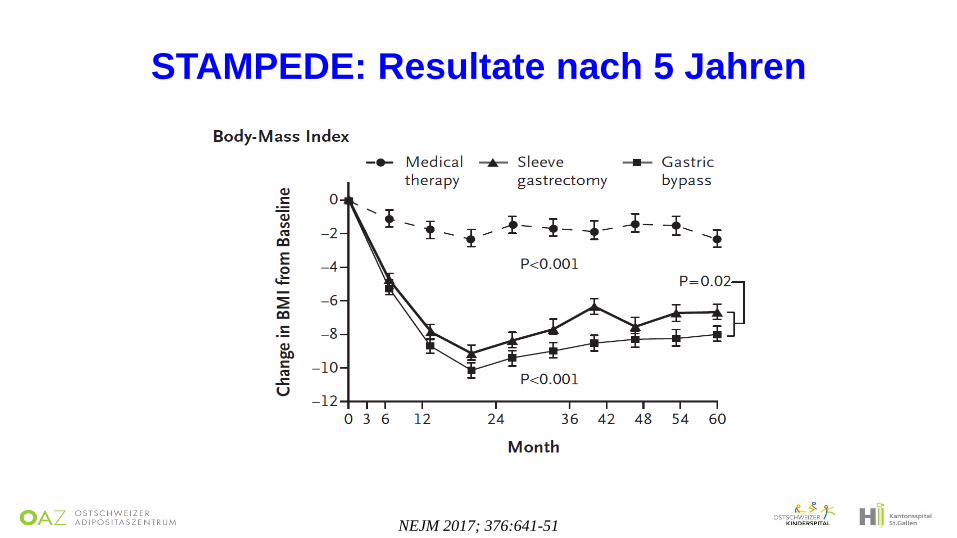
STAMPEDE: Resultate nach 5 Jahren
NEJM 2017; 376:641-51
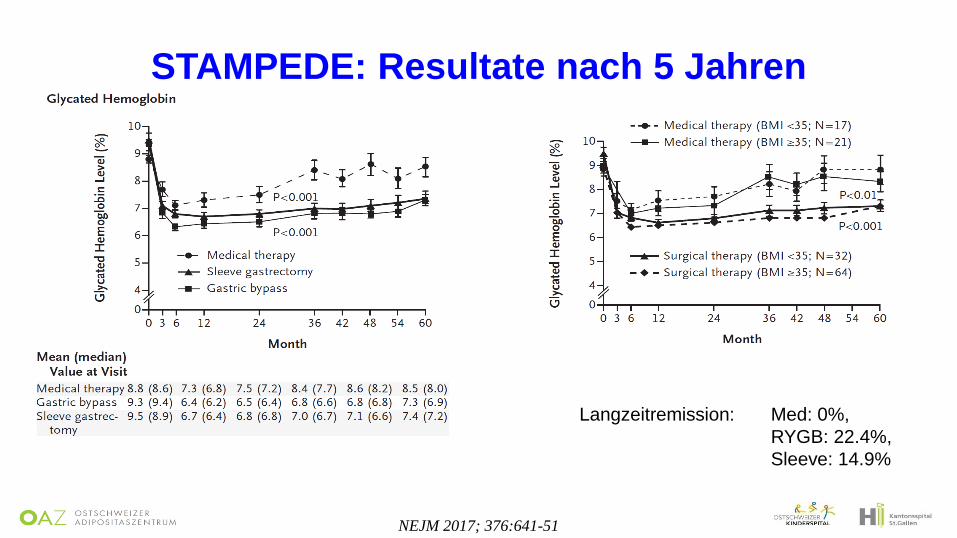
STAMPEDE: Resultate nach 5 Jahren
Langzeitremission: Med: 0%,
RYGB: 22.4%,
Sleeve: 14.9%
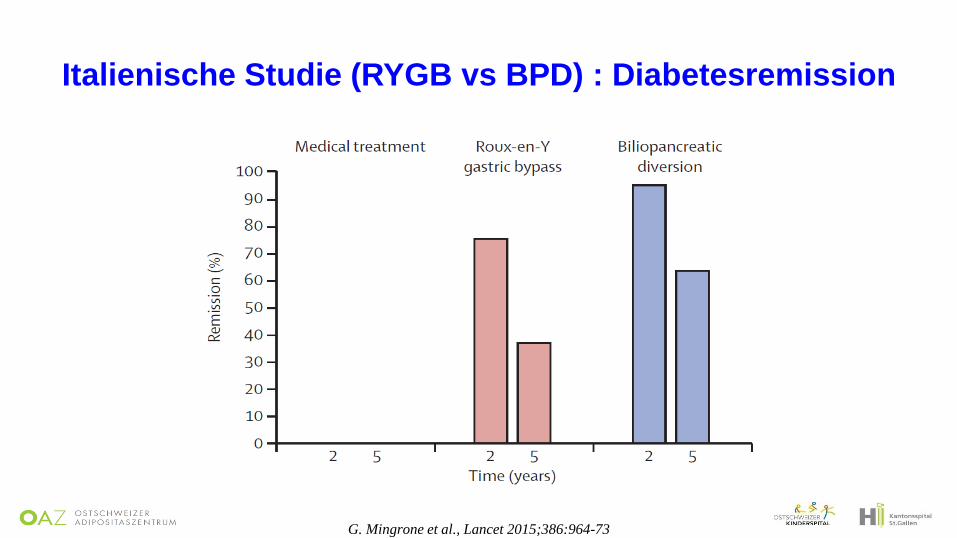
G. Mingrone et al., Lancet 2015;386:964-73
Italienische Studie (RYGB vs BPD) : Diabetesremission
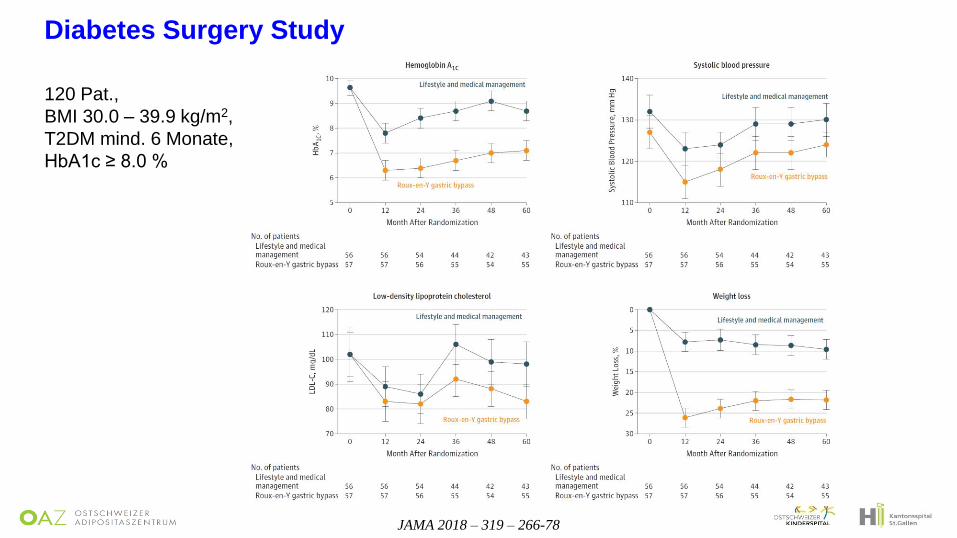
JAMA 2018 – 319 – 266-78
Diabetes Surgery Study
120 Pat.,
BMI 30.0 – 39.9 kg/m2,
T2DM mind. 6 Monate,
HbA1c ≥ 8.0 %
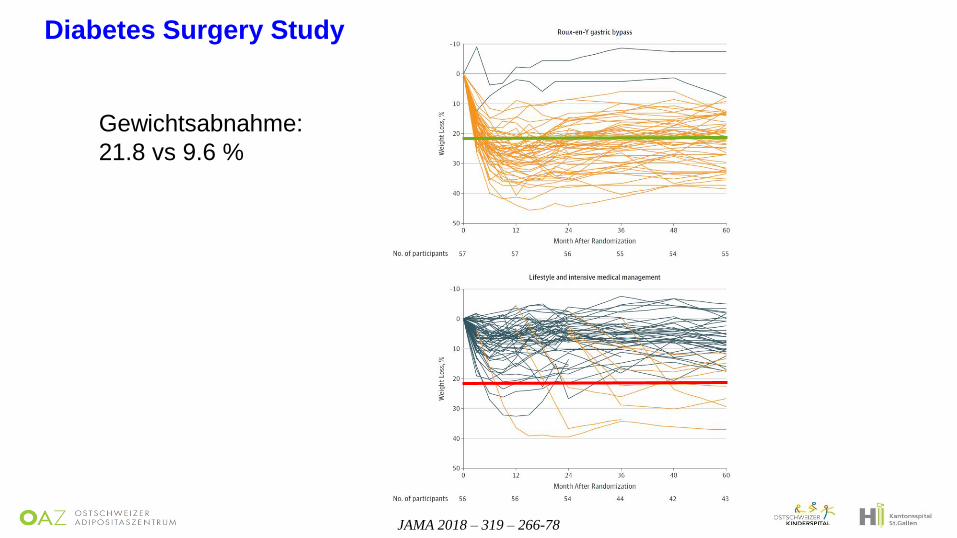
JAMA 2018 – 319 – 266-78
Diabetes Surgery Study
Gewichtsabnahme:
21.8 vs 9.6 %
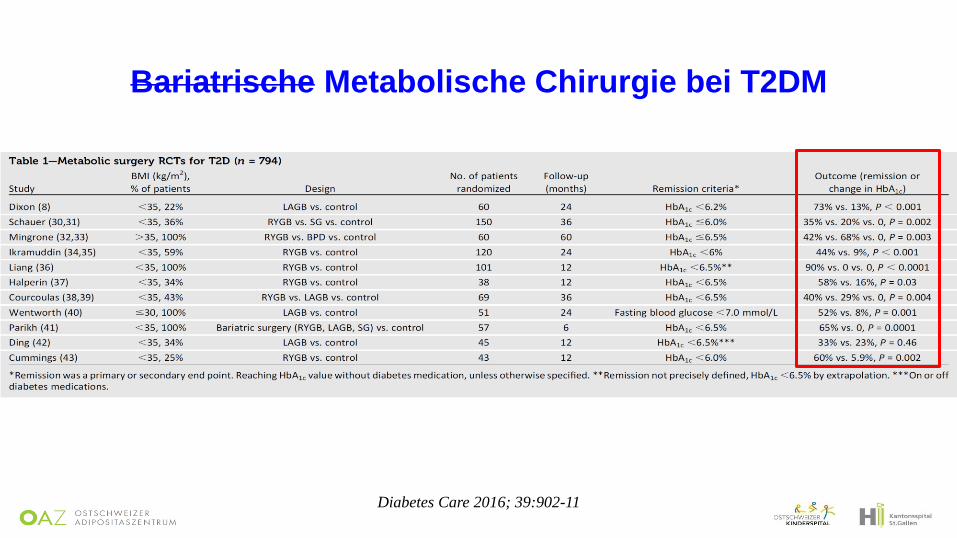
Diabetes Care 2016; 39:902-11
Bariatrische Metabolische Chirurgie bei T2DM
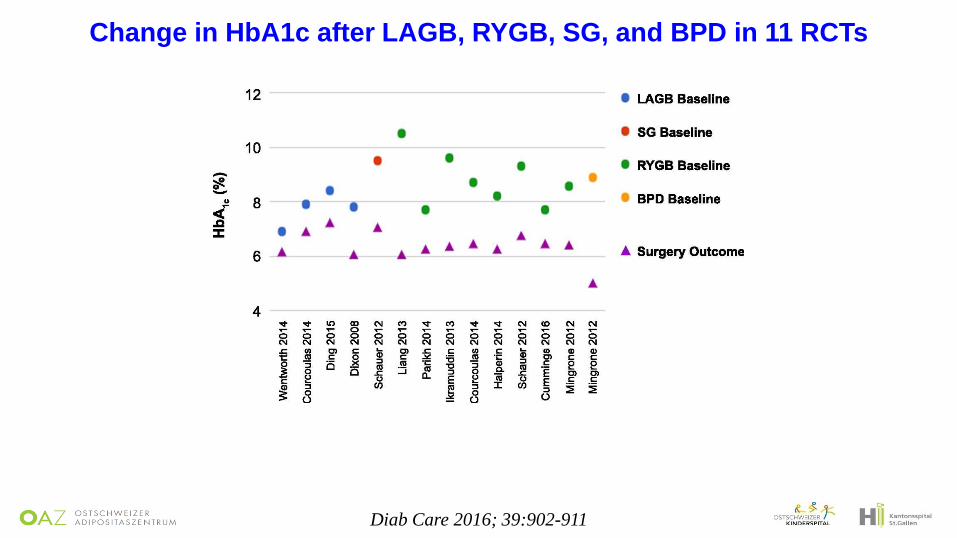
Change in HbA1c after LAGB, RYGB, SG, and BPD in 11 RCTs
Diab Care 2016; 39:902-911
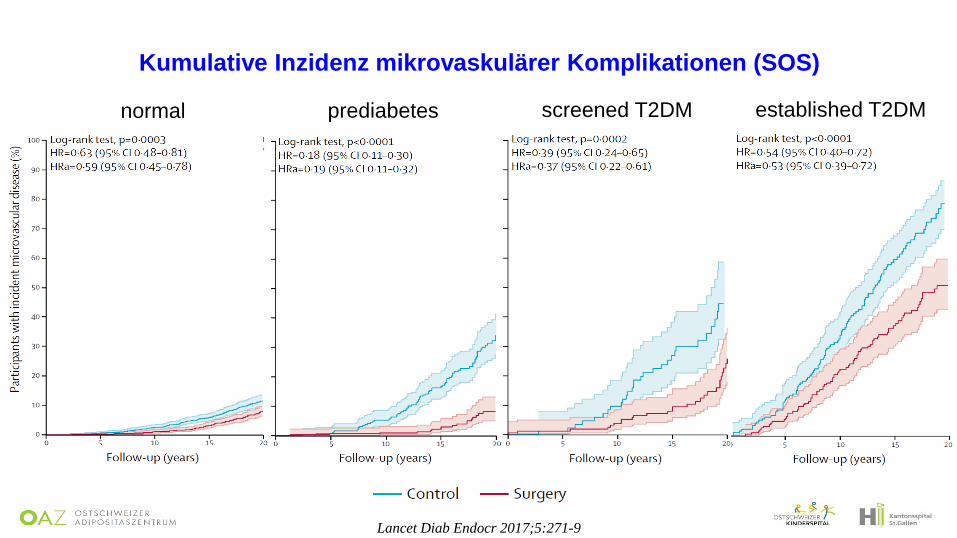
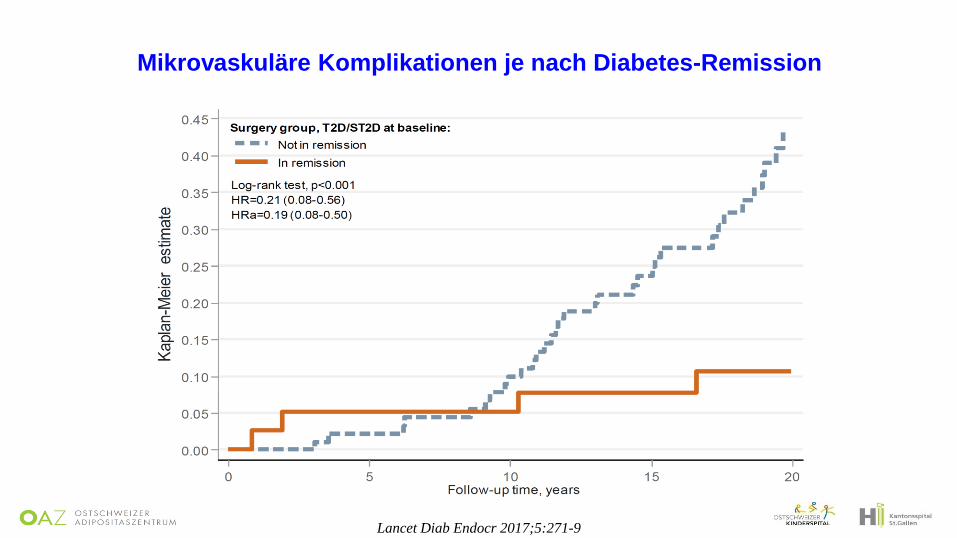
Lancet Diab Endocr 2017;5:271-9
normal prediabetes screened T2DM established T2DM
Kumulative Inzidenz mikrovaskulärer Komplikationen (SOS)
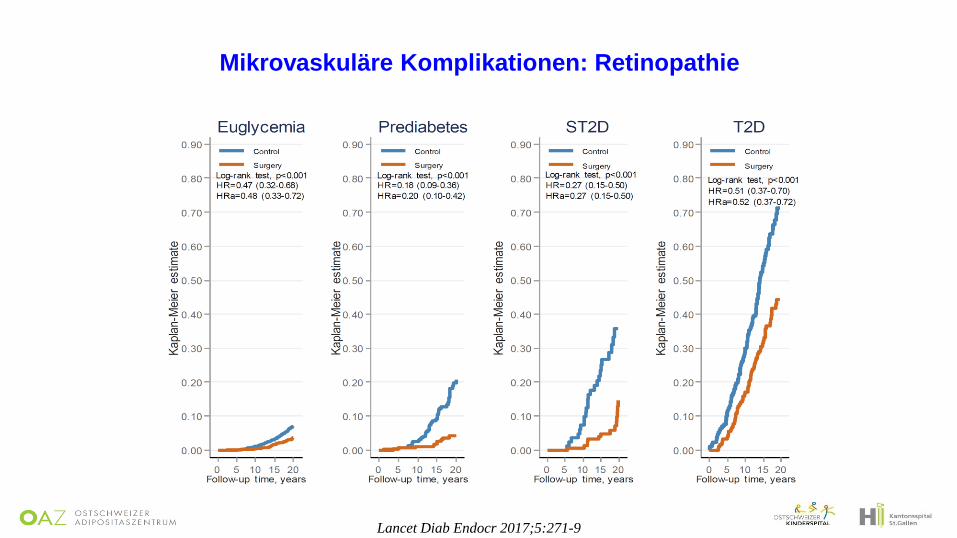
Lancet Diab Endocr 2017;5:271-9
Mikrovaskuläre Komplikationen: Retinopathie
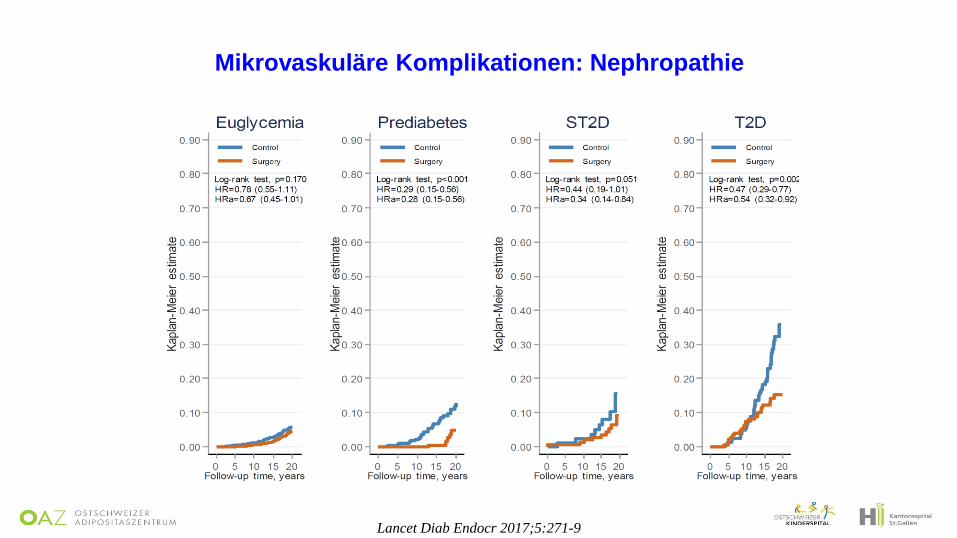
Lancet Diab Endocr 2017;5:271-9
Mikrovaskuläre Komplikationen: Nephropathie
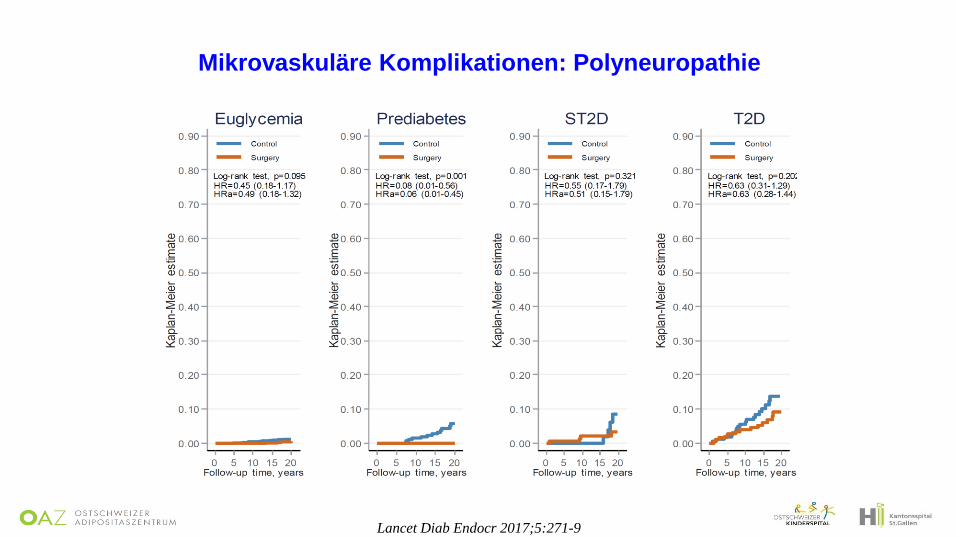
Lancet Diab Endocr 2017;5:271-9
Mikrovaskuläre Komplikationen: Polyneuropathie
Lancet Diab Endocr 2017;5:271-9
Mikrovaskuläre Komplikationen je nach Diabetes-Remission
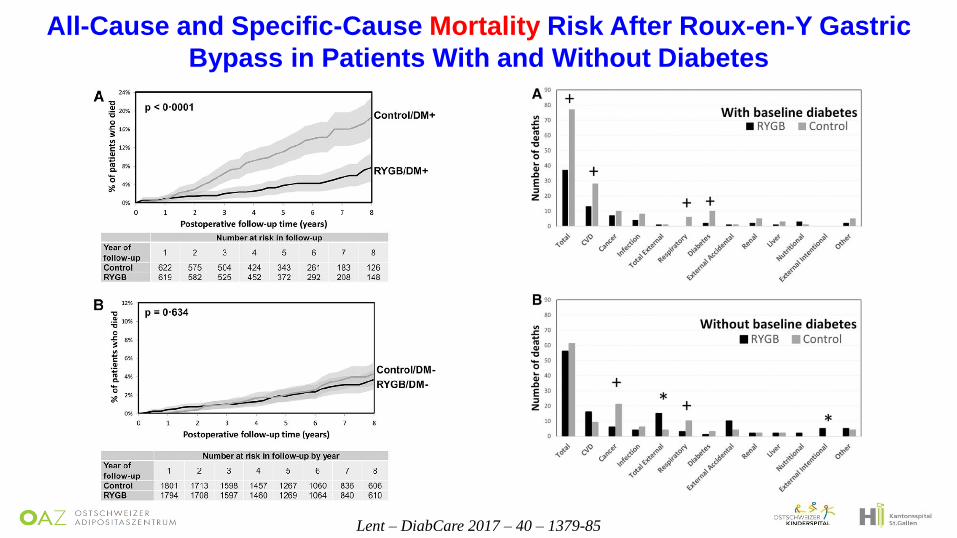
Lent – DiabCare 2017 – 40 – 1379-85
All-Cause and Specific-Cause Mortality Risk After Roux-en-Y Gastric
Bypass in Patients With and Without Diabetes
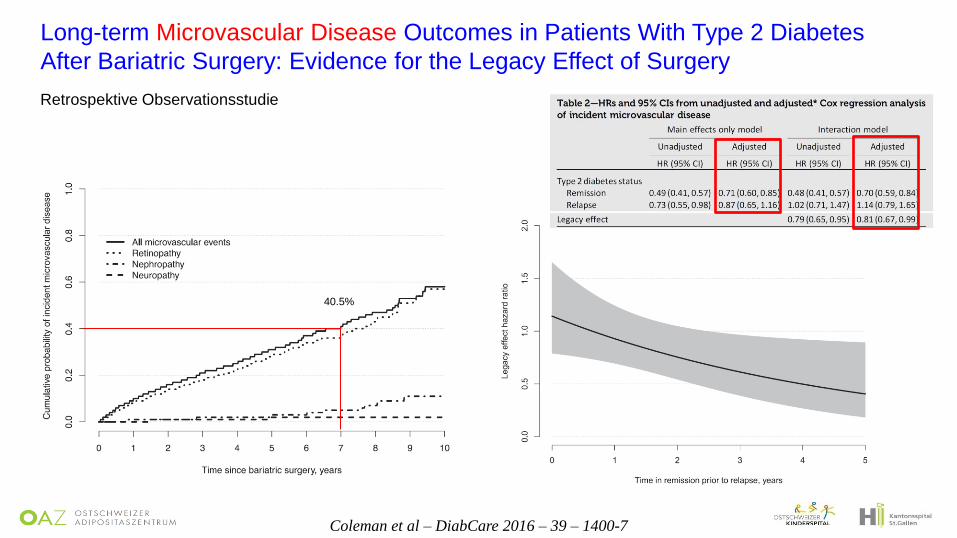
Coleman et al – DiabCare 2016 – 39 – 1400-7
Long-term Microvascular Disease Outcomes in Patients With Type 2 Diabetes
After Bariatric Surgery: Evidence for the Legacy Effect of Surgery
40.5%
Retrospektive Observationsstudie
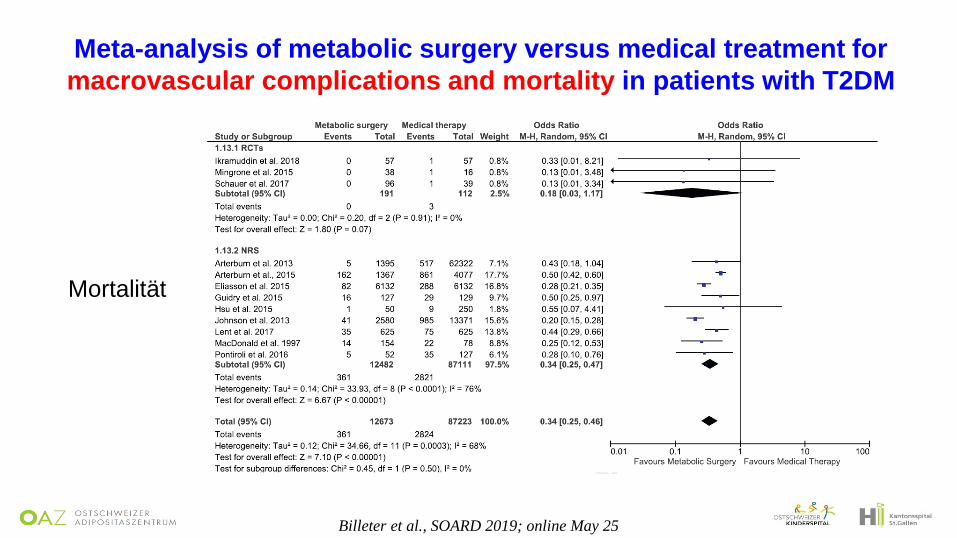
Billeter et al., SOARD 2019; online May 25
Meta-analysis of metabolic surgery versus medical treatment for
macrovascular complications and mortality in patients with T2DM
Mortalität
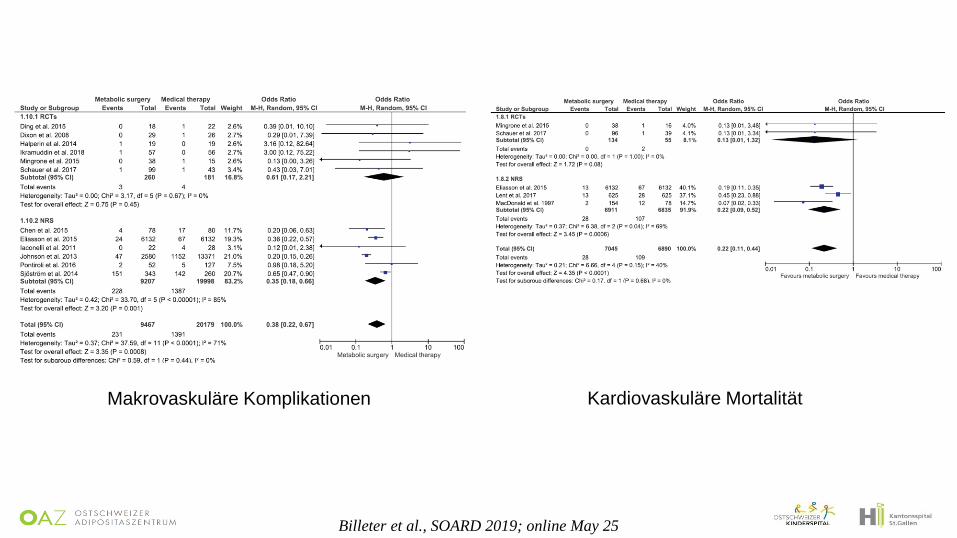
Billeter et al., SOARD 2019; online May 25
Makrovaskuläre Komplikationen Kardiovaskuläre Mortalität
Bariatrische OP: es profitieren besonders Patienten…
…mit Diabetes
…mit Prädiabetes
…mit kurzer Diabetesdauer
…mit Diabetesremission postoperativ
…unabhängig vom Ausgangs-BMI
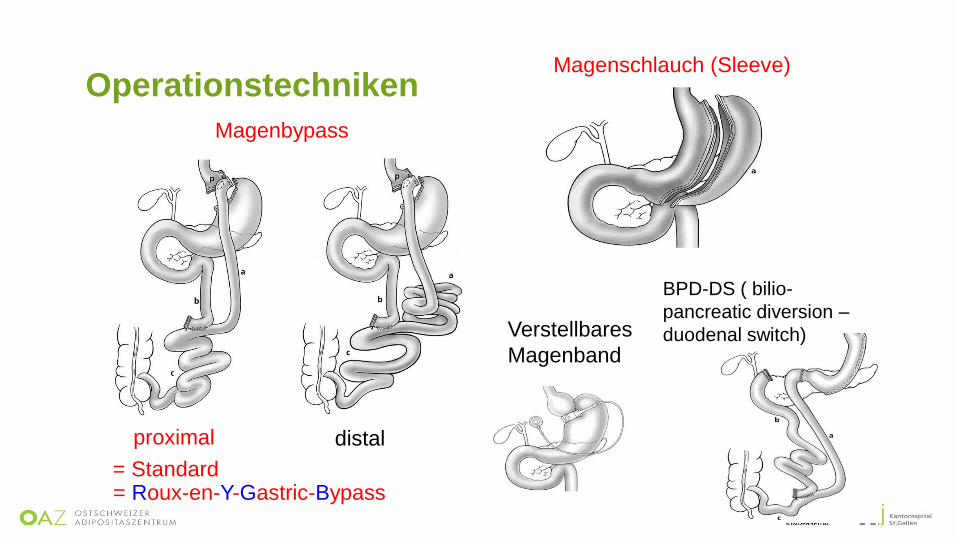
Magenbypass
proximal distal
Magenschlauch (Sleeve)
Verstellbares
Magenband
BPD-DS ( bilio-
pancreatic diversion –
duodenal switch)
= Standard = Roux-en-Y-Gastric-Bypass
Operationstechniken
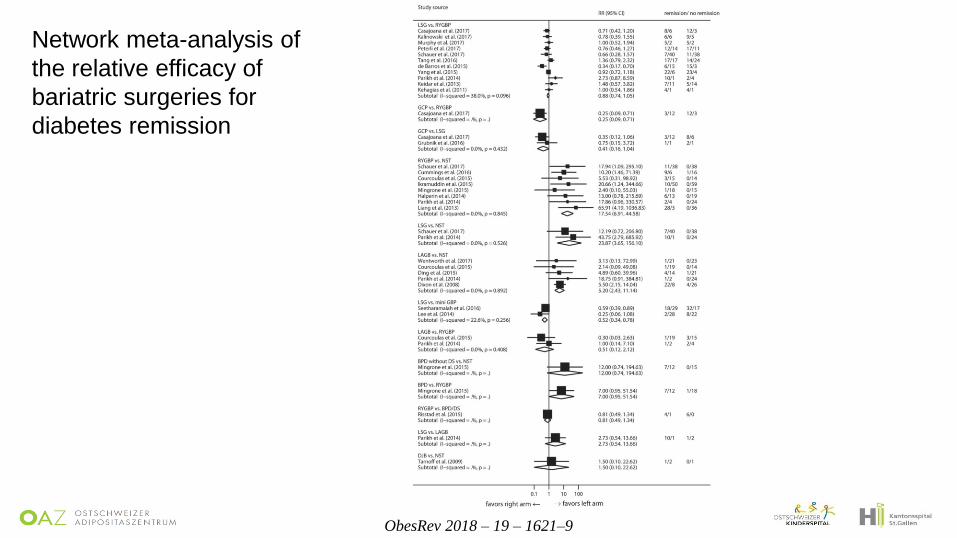
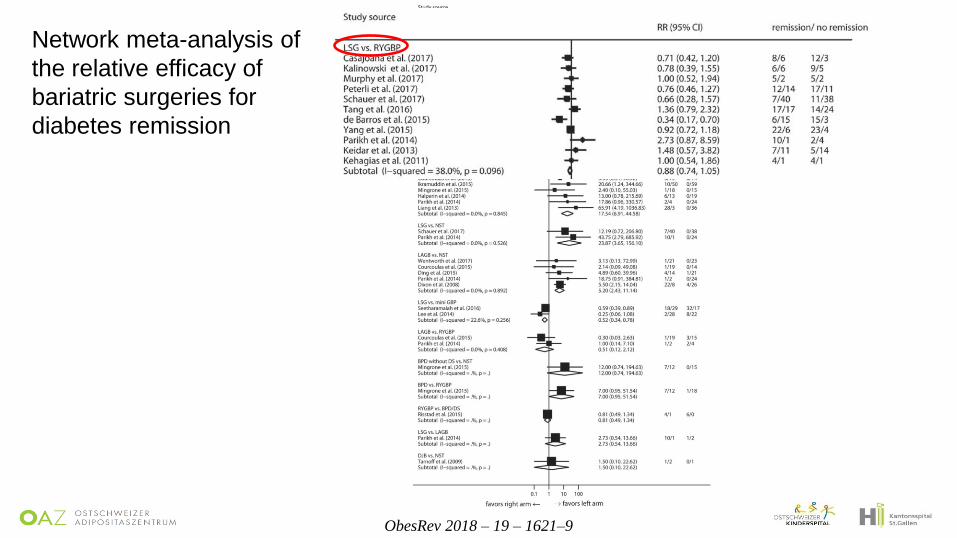
ObesRev 2018 – 19 – 1621–9
Network meta-analysis of
the relative efficacy of
bariatric surgeries for
diabetes remission
ObesRev 2018 – 19 – 1621–9
Network meta-analysis of
the relative efficacy of
bariatric surgeries for
diabetes remission
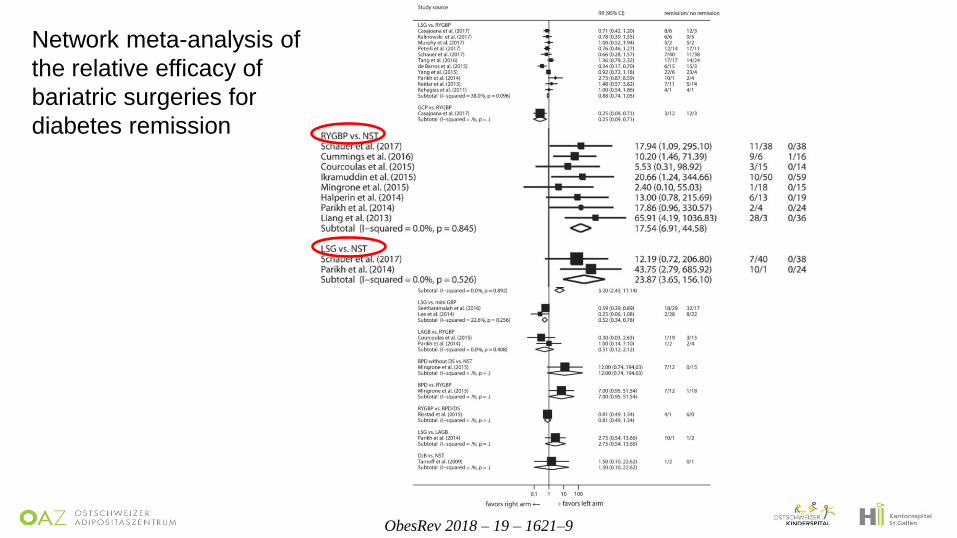
ObesRev 2018 – 19 – 1621–9
Network meta-analysis of
the relative efficacy of
bariatric surgeries for
diabetes remission
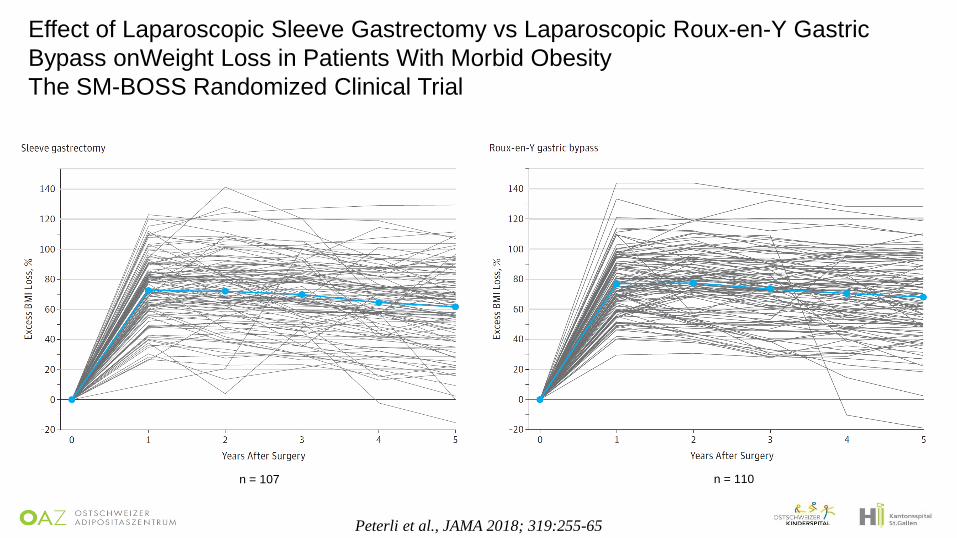
Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-en-Y Gastric
Bypass onWeight Loss in Patients With Morbid Obesity
The SM-BOSS Randomized Clinical Trial
Peterli et al., JAMA 2018; 319:255-65
n = 107 n = 110
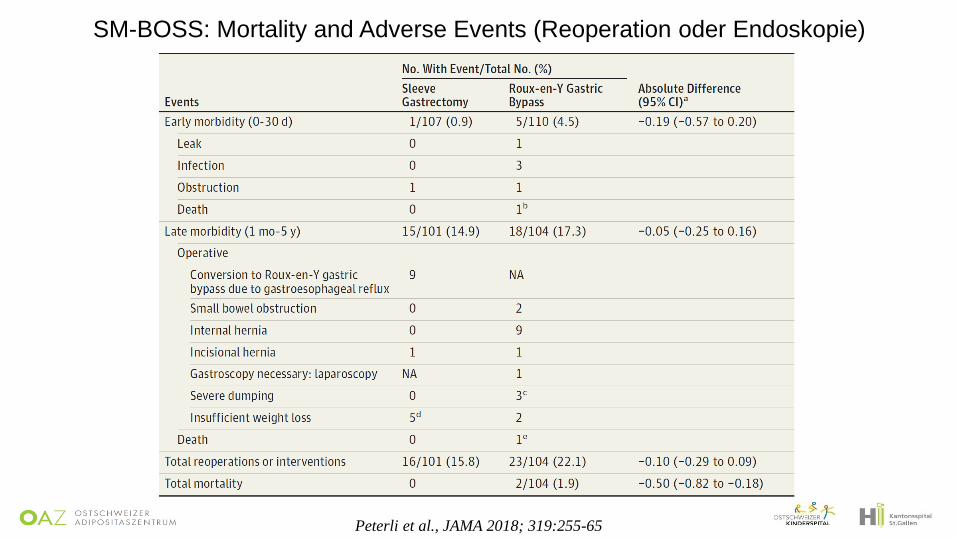
SM-BOSS: Mortality and Adverse Events (Reoperation oder Endoskopie)
Peterli et al., JAMA 2018; 319:255-65
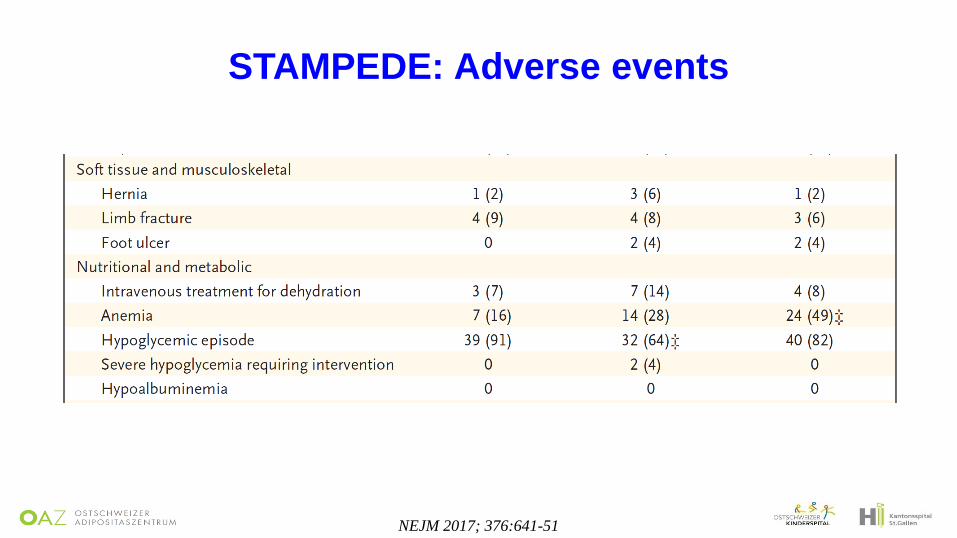
NEJM 2017; 376:641-51
STAMPEDE: Adverse events
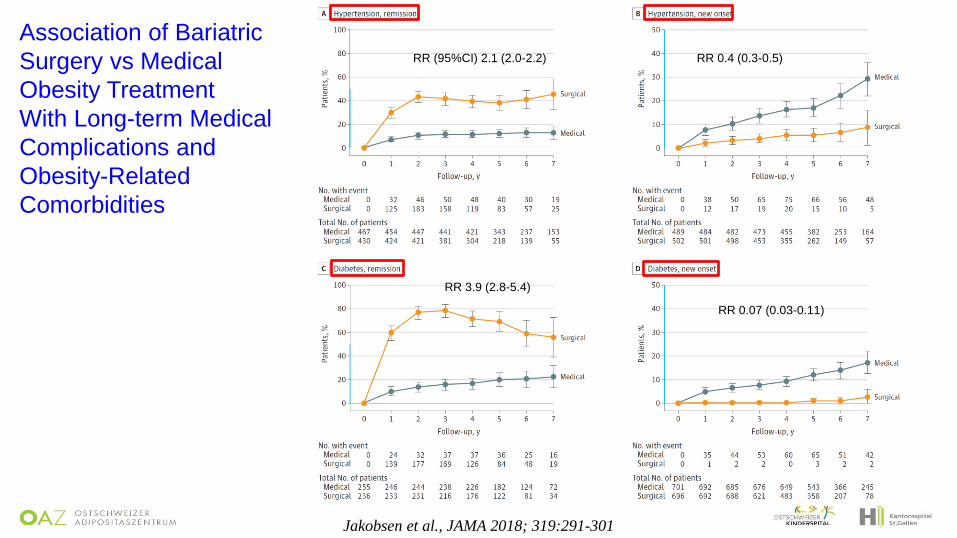
Jakobsen et al., JAMA 2018; 319:291-301
Association of Bariatric
Surgery vs Medical
Obesity Treatment
With Long-term Medical
Complications and
Obesity-Related
Comorbidities
RR (95%CI) 2.1 (2.0-2.2) RR 0.4 (0.3-0.5)
RR 0.07 (0.03-0.11)
RR 3.9 (2.8-5.4)
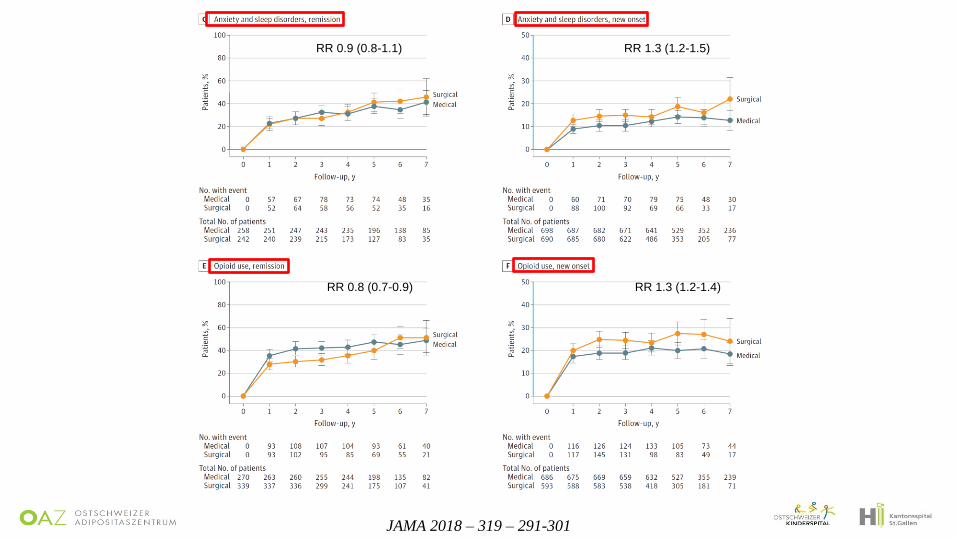
JAMA 2018 – 319 – 291-301
RR 0.8 (0.7-0.9) RR 1.3 (1.2-1.4)
RR 0.9 (0.8-1.1) RR 1.3 (1.2-1.5)
ObesRev 2019 – 20 – 633–47
Metabolic surgery for the treatment of type 2 diabetes in patients with BMI
lower than 35 kg/m2: Why caution is still needed
Dauerhaftes Verfahren
Risiko für Protein-, Vitamin- und Mineralstoffmangel; Folgeoperationen
Langzeitverlauf?
Relativ kleine Patientenzahl mit „moderater“ („leichterer“) Adipositas in Studien
Bedeutung der absoluten Gewichtsreduktion?
Auswahl der Patienten? – Adipositas Grad 1: OP bei schlechter DM-Kontrolle?
Vergleich mit moderner Diabetestherapie?
DM-Management nach bariatrischer OP?
Verfügbarkeit von Operationen?, Kosteneffizienz?
(Verdoppelung der potentiellen Patienten)
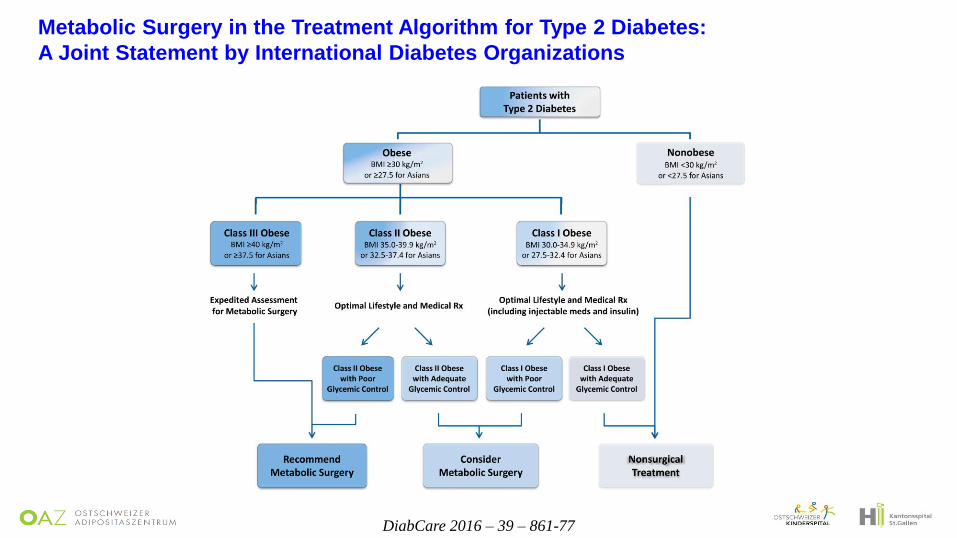
Metabolic Surgery in the Treatment Algorithm for Type 2 Diabetes:
A Joint Statement by International Diabetes Organizations
DiabCare 2016 – 39 – 861-77
Metabolische Chirurgie –
wem empfehlen wir eine Operation?
∙ T2DM und BMI ≥ 40 kg/m2: empfehlen
∙ T2DM und BMI ≥ 35 kg/m2: empfehlen
∙ T2DM und BMI 30-35 kg/m2: erwägen (Kontrolle des Diabetes?)
Mögliche Kriterien unabhängig vom BMI:
∙ Diabetesdauer?
∙ Kontrolle des Diabetes?
∙ Andere Co-Morbiditäten?
Viele Fragen noch offen……..





























