Embed Size (px)
Citation preview
Kitakanto Med J
2003 : 53 : 289•`291
289
Rheumatoid Arthritis Preceded by Interstitial Pneumonia
Associated with Myelodysplastic Syndrome : A Case Report
Yoshinori Mita,1 Kunio Dobashi,1 Yasuo Shimizu,1
Tsugio Nakazawa,2 and Masatomo Mori1
A 75-year-old male was admitted because of dyspnea. A chest X-ray showed interstitial shadows in
both lung fields, and hematology studies revealed a normochronic anemia. Examination of bone
marrow smears led to a diagnosis of myelodysplastic syndrome. The rheumatoid factor test was positive,
but the patient did not have arthritis. Twenty-one months later, he began to experience joint pain and
swelling, and he fulfilled the diagnostic criteria for rheumatoid arthritis. This is the first case ever
reported of rheumatoid arthritis preceded by interstitial pneumonia associated with myelodysplastic
syndrome. (Kitakanto Med J 2003 ; 53 : 289•`291)
Key words rheumatoid arthritis, myelodysplastic syndrome, interstitial pneumonia
Introduction
Diagnostic criteria for the various types of
myelodysplastic syndrome (MDS) have been proposed,
and a detailed description of features that may help
define MDS has been published.1 MDS refers to
disorders in which the abnormal findings are thought
to be confined to the myeloid cell series.2 Raskind et
al. hypothesized that at least two events are involved in
the pathogenesis of the myelodysplasia : one causing
proliferation of a clone of genetically unstable plur-
ipotent stem cells, and the other inducing
chromosomal abnormalities in its descendants.3 Vari-
ous rheumatic manifestations have been described in
patients with MDS.4•`6 However, there have been no
reports rheumatoid arthritis preceded by interstitial
pneumonia associated with MDS. We report the first
case of rheumatoid arthritis preceded by interstitial
pneumonia associated with MDS.
Case Report
A 75-year-old male was admitted to a hospital
because of dyspnea. He had no history of morning
stiffness, pain, or swelling of the joints. On physical
examination, blood pressure was 128/82mmHg, pulse
rate 83/min, and body temperature 36.1•Ž, and his
conjunctivae were pale. Chest examination revealed
Velcro rales in the inferior lung fields bilaterally.
Laboratory studies showed a hemoglobin level of 9.2g/
dL, hematocrit 28.8%, WBC count 4900/ƒÊL, platelet
count 109,000/ƒÊL, LDH 240IU/L, RAPA 2560X.
CRP, the erythrocyte sedimentation rate (ESR), the
ANA test, and direct and indirect Coombs' tests were
normal. A bone marrow biopsy revealed normocel-
lularity with erythroid hyperplasia and dysplasia, a
myeloid to erythroid (M : E) ratio 4 : 1, and pseudo-
Pelger anomalies of neutrophils and micro-
megakaryocytes. A diagnosis of myelodysplastic syn-
drome (MDS) was made based on these findings. A
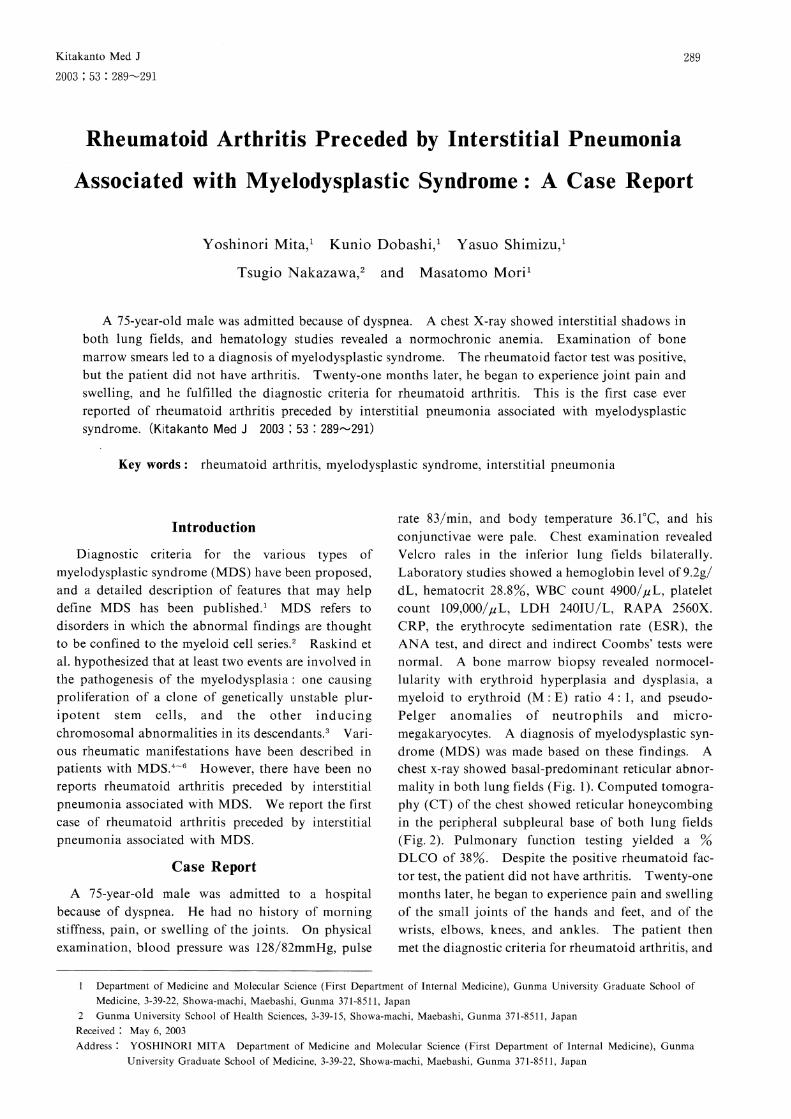
chest x-ray showed basal-predominant reticular abnor-
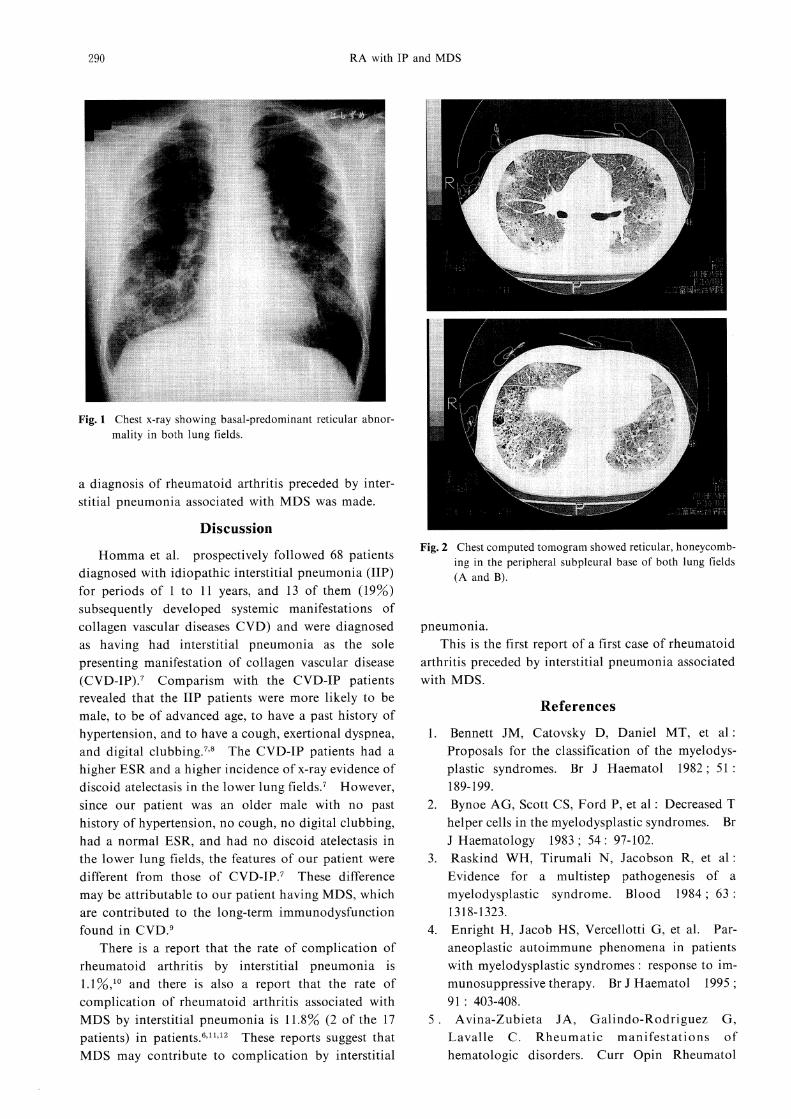
mality in both lung fields (Fig. 1). Computed tomogra-
phy (CT) of the chest showed reticular honeycombing
in the peripheral subpleural base of both lung fields
(Fig. 2). Pulmonary function testing yielded a %
DLCO of 38%. Despite the positive rheumatoid fac-
tor test, the patient did not have arthritis. Twenty-one
months later, he began to experience pain and swelling
of the small joints of the hands and feet, and of the
wrists, elbows, knees, and ankles. The patient then
met the diagnostic criteria for rheumatoid arthritis, and
1 Department of Medicine and Molecular Science (First Department of Internal Medicine), Gunma University Graduate School of Medicine, 3-39-22, Showa-machi, Maebashi, Gunma 371-8511, Japan
2 Gunma University School of Health Sciences, 3-39-15, Showa-machi, Maebashi, Gunma 371-8511, Japan
Received : May 6, 2003 Address : YOSHINORI MITA Department of Medicine and Molecular Science (First Department of Internal Medicine), Gunma
University Graduate School of Medicine, 3-39-22, Showa-machi, Maebashi, Gunma 371-8511, Japan
290 RA with IP and MDS
a diagnosis of rheumatoid arthritis preceded by inter-
stitial pneumonia associated with MDS was made.
Discussion
Homma et al. prospectively followed 68 patients
diagnosed with idiopathic interstitial pneumonia (IIP)
for periods of 1 to 11 years, and 13 of them (19%)
subsequently developed systemic manifestations of
collagen vascular diseases CVD) and were diagnosed
as having had interstitial pneumonia as the sole
presenting manifestation of collagen vascular disease
(CVD-IP).7 Comparism with the CVD-IP patients revealed that the IIP patients were more likely to be
male, to be of advanced age, to have a past history of
hypertension, and to have a cough, exertional dyspnea,
and digital clubbing.7'8 The CVD-IP patients had a
higher ESR and a higher incidence of x-ray evidence of
discoid atelectasis in the lower lung fields.7 However,
since our patient was an older male with no past
history of hypertension, no cough, no digital clubbing,
had a normal ESR, and had no discoid atelectasis in
the lower lung fields, the features of our patient were
different from those of CVD-IP.7 These difference
may be attributable to our patient having MDS, which
are contributed to the long-term immunodysfunction
found in CVD.9
There is a report that the rate of complication of
rheumatoid arthritis by interstitial pneumonia is
1.1%,10 and there is also a report that the rate of
complication of rheumatoid arthritis associated with
MDS by interstitial pneumonia is 11.8% (2 of the 17
patients) in patients.6,11,12 These reports suggest that MDS may contribute to complication by interstitial
pneumonia. This is the first report of a first case of rheumatoid
arthritis preceded by interstitial pneumonia associated
with MDS.
References
1. Bennett JM, Catovsky D, Daniel MT, et al:
Proposals for the classification of the myelodys-
plastic syndromes. Br J Haematol 1982 ; 51 : 189-199.
2. Bynoe AG, Scott CS, Ford P, et al : Decreased T
helper cells in the myelodysplastic syndromes. Br
J Haematology 1983 ; 54 : 97-102.
3. Raskind WH, Tirumali N, Jacobson R, et al :
Evidence for a multistep pathogenesis of a
myelodysplastic syndrome. Blood 1984 ; 63 :
1318-1323.
4. Enright H, Jacob HS, Vercellotti G, et al. Par-
aneoplastic autoimmune phenomena in patients
with myelodysplastic syndromes : response to im-
munosuppressive therapy. Br J Haematol 1995 ;
91 : 403-408.
5. Avina-Zubieta JA, Galindo-Rodriguez G,
Lavalle C. Rheumatic manifestations of
hematologic disorders. Curr Opin Rheumatol
Fig. 1 Chest x-ray showing basal-predominant reticular abnor-
mality in both lung fields.
Fig. 2 Chest computed tomogram showed reticular, honeycomb-ing in the peripheral subpleural base of both lung fields
(A and B).

291
1998 ; 10 : 86-90.
6. Kuzmich PV, Ecker GA, Karsh J : Rheumatic
manifestations in patients with myelodysplastic
and myeloproliferative diseases. J Rheumatol
1994 ; 21 : 1649-1654.
7. Homma Y, Ohtsuka Y, Tanimura K, et al. Can
interstitial pneumonia as the sole presentation of
collagen vascular diseases be differentiated from
idiopathic interstitial pneumonia? Respiration
1995 ; 62 : 248-251.
8. Ishioka S, Nakamura K, Maeda A, et al. Clini-
cal evaluation of idiopathic interstitial pneumo-
nia and interstitial pneumonia associated with
collagen vascular disease using logistic regression
analysis. Intern Med 2000 ; 39 : 213-219.
9. Takashima H, Eguchi K, Origuchi T, et al.
Collagen diseases complicated with myelodysplas-
tic syndrome (MDS)-report of three cases.
Ryumachi 1994 ; 34 : 48-53.
10. Patterson CD, Harville WE, Pierce JA, et al :
Rheumatoid lung disease. Ann Intern Med
1965 ; 62 : 685-697.
11. Hisakawa N, Nishiya K, Hashimoto K, et al. A
case of malignant rheumatoid arthritis associated
with myelodysplastic syndrome. Ryumachi
1997 ; 37 : 30-35.
12 . Nam EJ, Kang YM, Kang HR, et al :
Rheumatoid arthritis associated with myelodys-
plastic syndrome : A case report. J Korean Med Sci 1999 ; 14 : 319-322.





![Pilzkolonisation bei Patienten mit Septischem Schock ... · Bei allen beatmeten Patienten kann eine beatmungsassoziierte Pneumonie (VAP [Ventilation associated pneumonia]) als Sepsisquelle](https://img.pdfslide.org/doc/110x75/5d57597c88c993461c8b5693/pilzkolonisation-bei-patienten-mit-septischem-schock-bei-allen-beatmeten.jpg)























