Embed Size (px)
Citation preview
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

Active Aging: The Contribution of Psychology
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
About the author
Rocío Fernández-Ballesteros is Professor at the Autonomous University of Madrid,Spain. She researches and teaches in psychology of aging as well as psychologicalassessment and evaluation. She is the author of more than 250 publication, amongthem Encyclopedia of Psychological Assessment (2003) and GeroPsychology: Euro-pean perspectives for an aging world (2007). She is the former President of the Eu-ropean Association of Psychological Assessment (EAPA), Founder and former Ed-itor-in-Chief of the European Journal of Psychological Assessment, Past-President ofthe Division on Applied Gerontology of the International Association of AppliedPsychology (IAAP), and a Fellow of the Gerontological Society of America (GSA).In 2005, she received the Aristotle Prize from the European Federation of Psychol-ogists Associations (EFPA), and in 2006 the Award for Distinguished Contributionfrom the IAAP.
Acknowledgments
The manuscript for this book was prepared during a sabbatical awarded by theAutonoma University of Madrid and supported by the University State SecretaryProgram (PR2005-0031), in the Inter-University Center for Research on Motiva-tion at the University La Sapienza, Rome. I would like to express my gratitude tothe organizations that awarded and supported the sabbatical, as well as to Prof.Gian Vittorio Caprara and other colleagues at the research center and faculty inRome.
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
Active Aging:The Contributionof PsychologyRocío Fernández-Ballesteros
Autonoma University of Madrid, Spain
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
Library of Congress Cataloging in Publication
is available via the Library of Congress Marc Database under theLC Control Number 2008927620.
Library and Archives Canada Cataloguing in Publication
Fernández Ballesteros, RocíoActive aging : the contribution of psychology / Rocío Fernández-Ballesteros.
Includes bibliographical references.ISBN 978-0-88937-360-0
1. Older people—Psychology. 2. Aging—Psychological aspects.I. Title.BF724.8.F47 2008 155.67 C2008-903560-7
© 2008 by Hogrefe & Huber Publishers
PUBLISHING OFFICESUSA: Hogrefe & Huber Publishers, 875 Massachusetts Avenue, 7th Floor,
Cambridge, MA 02139Phone (866) 823-4726, Fax (617) 354-6875; E-mail [email protected]
EUROPE: Hogrefe & Huber Publishers, Rohnsweg 25, 37085 Göttingen, GermanyPhone +49 551 49609-0, Fax +49 551 49609-88, E-mail [email protected]
SALES & DISTRIBUTIONUSA: Hogrefe & Huber Publishers, Customer Services Department,
30 Amberwood Parkway, Ashland, OH 44805Phone (800) 228-3749, Fax (419) 281-6883, E-mail [email protected]
EUROPE: Hogrefe & Huber Publishers, Rohnsweg 25, 37085 Göttingen, GermanyPhone +49 551 49609-0, Fax +49 551 49609-88, E-mail [email protected]
OTHER OFFICESCANADA: Hogrefe & Huber Publishers, 1543 Bayview Avenue, Toronto,
Ontario M4G 3B5SWITZERLAND: Hogrefe & Huber Publishers, Länggass-Strasse 76, CH-3000 Bern 9
Hogrefe & Huber Publishers. Incorporated and registered in the State of Washington,USA, and in Göttingen, Lower Saxony, Germany.
No part of this book may be reproduced, stored in a retrieval system or transmitted, inany form or by any means, electronic, mechanical, photocopying, microfilming, record-ing or otherwise, without written permission from the publisher.
Printed and bound in the USAISBN 978-0-88937-360-0
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
Active Aging / Foreword Active Aging / Foreword
Foreword
We all age. Active Aging, aging with well-being and a high quality of life, is oneof the most important issues facing science and society in our time of increasinglongevity and demographic change. Never before have so many people been ableto live to such an advanced age. There has been an enormous extension of the lifespan during the last decades in all European countries, but also across the world.We live longer and remain more active into later life than our parents and grand-parents. This is due to the progress of modern medicine, the improvement ofsocio-economic living conditions, and it is also very much influenced by lifestylesand human behavior. It is important to not just add years to life, but also to addlife to years!
This very interesting and stimulating book, based on a critical analysis of thegerontological and especially psychological research literature on aging, empha-sizes a new paradigm in scientific gerontology that has a more positive view ofaging processes. What is “active aging,” “healthy aging,” “quality of life,” “success-ful aging,” “life satisfaction,” “well-being,” “positive aging”? Amongst many otherthings, this book also addresses these questions of definition. An analysis of theliterature of the last decades shows an interesting development: In the 1960s,there were many articles on the subject of “life satisfaction,” followed some yearslater by the topic of “successful aging.” In the 1970s, the subject of “quality oflife” came to prominence, originally introduced by medical doctors; and then inthe 1980s and beyond, the topic of “subjective well-being” became dominant. Lifesatisfaction (in the sense of satisfaction with the development of one’s life as wellas with the current situation) is recognized as an indicator of successful aging.Life satisfaction (often measured with a so-called “life satisfaction scale”) in thiscontext is valued as an aspect of adjusting successfully to the aging process. As isshown in the following, the definition of all these concepts is very difficult. In theliterature, they sometimes overlap and it is not possible to differentiate betweenthem, and there is some confusion regarding theoretical and methodological con-cepts.
In this book, Rocío Fernández-Ballesteros makes a convincing case for a mul-tidimensional, multilevel model of active aging, including several theoretical con-structs, and states: “In conclusion, positive aging can be defined as the life-courseadaptation process for arriving at an optimal physical (including health), psycho-logical (optimal cognition and emotion-motivation regulation), and social func-tioning of the individual. Therefore, the promotion of active aging will imply theoptimization of those conditions through biomedical, physical, psychological,and socio-environmental interventions. It should also be emphasized that pro-
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

moting active aging is preventing illness and disability, and increasing well-beingin old age.”(p. 58)
Aging is not only a biological process; it is a process determined by a numberof biological, social, psychological, and ecological factors. Healthy aging is activeaging! The focus of this book is on active, healthy aging and the behavioral andpsychosocial factors that contribute to it. Healthy aging is the result of a lifelongprocess. It is therefore necessary to optimize the development of the individualfrom early childhood on. We know that a variety of influences in early childhood,in adolescence, during early and middle adulthood, but also in the current livingcircumstances of the aged determine the processes of aging and well-being in oldage.
Achieving healthy aging is a challenge for society but also for every individual.Measures of health promotion and primary prevention are necessary to maintainand increase competencies in later life. What can be done to secure a high qualityof life in old age?
There are many studies that demonstrate that physical activity is a prerequisitefor successful aging. Age-determined physical changes – such as functional im-pairments of the organs, changes in the motor and muscular system as well aschanges in the respiratory organs (which, of course, depending on the individual,can appear at any age) – are similar to the effects brought about by a lack ofexercise. A young but physically inactive individual seems old, just as an old butactive individual appears young. Physical activity also has positive effects on psy-chological well-being by promoting mental abilities, subjective well-being, socialskills, and self-concept.
Cognitive activity is another prerequisite for successful aging. Many studieshave found that mentally active individuals who have a wide range of interests, atime perspective reaching farther into the future, and a larger number of socialcontacts reach old age with greater feelings of psycho-physical well-being thanthose who lack such activity and perspective. It has been established that cognitiveactivity is essential for healthy aging. It is therefore, important that older peoplehave mental tasks – they must be challenged to mental activity, as a reduction insuch activity can speed up the process of aging.
Emotional and motivational functioning influences healthy and active aging.Aging is associated with life-change units and such changes require adaptationand adjustment; elderly people sometimes have to cope with multiple critical lifeevents. Last but not least, social functioning and social participation also have aninfluence on healthy and active aging.
“Promoting active aging” is the main goal of this very important book, whichaims to strengthen a theory- and research-based practical approach, a programfor healthy active aging. Overall, we need a more positive view of aging; we haveto do everything we can to change the negative image of the aged into a morerealistic one. Old age is every young person’s future, so we have to strengthenevery individual’s physical, cognitive, emotional-motivational, and social devel-
vi Active Aging / Foreword
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

opment from very early on in life. In this, health promotion is the most importantprerequisite for active aging. This is a challenge for psychologists, who can con-tribute to effecting behavioral changes towards healthier behavior. To promoteaging well, to achieve long life as free of disability as possible, and to reduce mor-bidity at the end of life should be the aim of the necessary multidomain-based,multidimensional intervention programs. “The process of aging well, at the in-dividual, community, and population level, depends on complex psychologicalself-regulation functioning because the individual is always an active agent whorequires the exercise of control.” (p. 154)
Old age and longevity should not be seen as a problem but as a chance and achallenge – a challenge for everyone: for the aging individual, for their family, andfor our society. We should not only talk about the losses, problems, and deficitsof aging and old age. We have to talk about – and we have to open our eyes to –the potentials of the elderly, and also the competencies and potentials of the veryold. We have to see the aged of the 21st century as human capital. This book willhelp to such a new view of the older population.
Ursula LehrJune 2008
Active Aging / Foreword vii
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

Table of Contents Table of Contents
Table of Contents
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vTable of Contents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ix
PART I: CONCEPTUAL ISSUES . . . . . . . . . . . . . . . . . . . . . . . . . 1
1 A New Paradigm in the Study of Aging . . . . . . . . . . . . . . . . . . . . 3
Traditions in the Study of Aging, Age, and the Aged . . . . . . . . . . . . 3Evolution in Research on Active Aging . . . . . . . . . . . . . . . . . . . 6Empirical Bases of Active Aging . . . . . . . . . . . . . . . . . . . . . . . 9Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
2 Population Aging: Facts and Projections . . . . . . . . . . . . . . . . . . 16
Life Expectancy Enlargement . . . . . . . . . . . . . . . . . . . . . . . . . 16Population Aging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Years to Life and Life to Years . . . . . . . . . . . . . . . . . . . . . . . . . 18Morbidity Hypotheses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Determinants of Morbidity . . . . . . . . . . . . . . . . . . . . . . . . . . 26Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
3 Working, Empirical, and Lay Definitions, and Theoretical Models . . . 29
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Controversial Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Working Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32Empirical Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Lay Concepts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Theoretical Models . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49Toward a Multidimensional-Multilevel Proposal of Active Aging . . . . . 55Psychological Domains Contributing to Active Aging . . . . . . . . . . . 57Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
PART II: BEHAVIORAL AND PSYCHOLOGICAL DOMAINSOF ACTIVE AGING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
4 Behavioral Health and Physical Fitness . . . . . . . . . . . . . . . . . . . 63
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63Physical Exercise . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Diet and Nutrition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69Smoking and Drinking . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

5 Cognitive Functioning . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74Education and Socioeconomic Status . . . . . . . . . . . . . . . . . . . . 77Physical Exercise . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84Cognitive Training and Interventions . . . . . . . . . . . . . . . . . . . . 88Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
6 Emotional and Motivational Functioning: Affect, Control, and Coping 98
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98Positive Emotions and Positive Aging . . . . . . . . . . . . . . . . . . . . 102Personal Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107Coping with Stress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 112Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119
7 Social Functioning and Social Participation . . . . . . . . . . . . . . . 120
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 120Social Functioning and Positive Emotions Across the Life Span . . . . . 121Social Functioning and Health . . . . . . . . . . . . . . . . . . . . . . . . 123Social Functioning and Cognitive Impairment . . . . . . . . . . . . . . 126Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 128
PART III: PROMOTING ACTIVE AGING . . . . . . . . . . . . . . . . . . . 129
8 Active Aging Promotion Programs . . . . . . . . . . . . . . . . . . . . . 131
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131Lifelong Health Promotion . . . . . . . . . . . . . . . . . . . . . . . . . . 133Promoting Healthy Aging During Adulthood . . . . . . . . . . . . . . . 135Cognitive Impairment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 137Active-Aging Promotion Projects . . . . . . . . . . . . . . . . . . . . . . 145Population-Based Projects . . . . . . . . . . . . . . . . . . . . . . . . . . 150Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 159
Selected Websites on Active Aging . . . . . . . . . . . . . . . . . . . . . . . . 192
x Table of Contents
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

Active Aging / Part I: Conceptual Issues Chapter 1: A New Paradigm in the Study ofAging
PART ICONCEPTUAL ISSUES
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
1A New Paradigm in the Study of Aging
Traditions in the Study of Aging, Age, and the Aged
Assumptions about aging have two main scopes, based in two main philosophicaltraditions of thinking. From Plato (427–347 BC) a tradition emerges of a positiveand individualistic view of aging in which the human being ages as he/she lives,and that he/she must prepare for aging throughout the lifespan. Following thistradition, Cicero (106–43 BC) wrote “De Senectute” describing how human vir-tue grows through age. By contrast, from an Aristotelian (384–322 BC) point ofview, it is stated that old age, as the last stage of human life, could be consideredas a natural illness. In the same line Seneca (4 BC–65 AD) proposes physical andmental impairment in the individual as consequences of aging.
From these two traditions, across the history of the study of aging, theoriesand authors can be found who emphasized a positive view of aging (e.g., theactivity theory, Havighurst, 1963; or the continuity theory, Atchley, 1989, 1999)and those who underline the negative aspects that explain the decline in socialparticipation and engagement during old age (e.g., disengagement theory, Cum-mings & Henry, 1961; see also Fernández-Ballesteros, 2000; Lupien & Wand,2004; Juengst, 2005).
Aging is a biological phenomenon and throughout aging there is a decline inthe efficiency and efficacy of all biological systems, therefore, during this processthere is an increase in vulnerability to chronic and acute disease. Nevertheless, itcan also be stated that within the biological aging process of decline there are wideindividual differences and, therefore, there are also broad differences in vulnera-bility.
However, a human being is not only a biological organism but he/she is also abio-psycho-cultural entity; moreover, an active agent who is constructinghim/herself throughout the lifespan, in interaction with an active world, and inan ongoing and dynamic process (Bandura, 1986; Gould, 1977, 1981). Intraindi-vidual and interindividual differences attributed to age are not exclusively theresult of age but of the ongoing and dynamic process through which the individ-ual as a biological organism and his/her behavioral and psychological conditionsinteract with the external factors – sociocultural, economic, environmental, etc.During the process of aging, what the human being does, thinks, and feels and
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
how he/she interacts with the environmental and its historical circumstances aredecisive for aging outcomes.
As Birren (1996) pointed out, the science of gerontology is mainly devoted tothe multidisciplinary study of aging, age, and the aged, therefore, even the scien-tific subject of gerontology embraces primary aging (caused by age), secondaryaging (caused by disease), and their individual differences as well as the processof aging itself and aged people. This diversity in the subject of study has influ-enced a certain bias in the selected topics: authors studying the “aging” processemphasize small intraindividual changes; authors studying differences between“age” groups are going to find high interindividual differences attributed to age,and finally, those authors studying “the aged” are devoted to illnesses, impair-ments, and needs of care, therefore, they are going to focus on impairment andsuffering during the process of aging.
Moreover, the intrinsic characteristic of gerontology is to have a complex sub-ject of study but also to be multidisciplinary; that is, aging, age, and the agedshould be studied from a bio-psycho-social perspective. Nevertheless Juengst(2005) emphasized that “from a biomedical model of pathology, human senes-cence carries all the hallmarks of a disease process: Specific underlying molecularchanges create abnormalities in cells that inhibit the functional efficiency andstructural resiliency of tissues and organs, causing disabilities, deformities, anddistress” (p. 3). Also, Blazer (2006), in his Introduction to a Special Issue of theAmerican Journal of Geriatric Psychiatry devoted to successful aging, stated that“success in late life has, therefore, been tied to the success of physicians and otherhealth care providers in treating the maladies of late life” (p. 3). However, al-though as people age biophysical systems become less efficient and illness and ageare covariants, since the human being is a bio-psycho-social entity not all humanfunctioning fits into this biomedical model. Therefore, it can be concluded thatthis biomedical reductionism cannot be generalized to the entire field of study.
Thus, a biomedical model of aging cannot be transferred to all aging condi-tions; as Gould (1981) emphasized, psychosocial functioning cannot be under-stood under the same principles that those guiding organisms as biological enti-ties since human functioning is also determined by sociocultural context. In fact,as Bandura (1986) posited from his sociocognitive theory, psychological func-tioning is determined by the reciprocal interactions between the biological or-ganism, his/her basic learned behavioral repertoire and the sociocultural context.
Finally, the mere concept of “age,” the process of aging, or the individual differ-ences in how a given person, in a given society, ages are,to some extent, socioculturalphenomena. The importance of sociocultural factors on aging does not ignore – asseems to be claimed by some constructivistic authors such as Gergen and Gergen(2001) – the existence of illness, decline, or impairment linked to biological aging.Nevertheless, the ways in which the human organism ages are modulated by psycho-social and cultural factors. The process of aging cannot be reduced to biomedicalconditions but neither can it be reduced to sociocultural ones.
4 Active Aging / Part I: Conceptual Issues
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

As Lupien and Wan (2004) pointed out, gerontologists’ speech is promotingthe spread of negative views of age and aging and reinforcing the existing stereo-types in society as a whole. These authors recall Butler’s statements accusinghealth professionals of promoting these stereotypes when he coined the conceptof “ageism” as the process of discrimination against the elderly as a consequenceof systematic stereotyping (Butler, 1969). Moreover, as is demonstrated by em-pirical evidence (e.g., World Health Organization [WHO], 1990b), negative viewsof aging have a perverse repercussion in society in a double sense: They reinforcenegative beliefs and negatives views at the macro and micro levels, they threatenindividuals and groups, and act as self-fulfilling prophecies during aging (Levyand Langer, 1994). A common schema or script is: Illness (as a main biologicalcondition) is unavoidable in old age, cognitive impairment is normative, old in-dividuals cannot learn, social withdraw is a standard situation at the end of life;social responses to these images go from nihilism to paternalism. Finally, the in-dividual is threatened by this profile into acting as predicted and society is alsothreatened by an increase in the aging population under the assumption that theyspend more than they contribute to society. In fact, all these assumptions comefrom one of the more extensive sociological theories in gerontology: the disen-gagement theory mentioned above.
Unfortunately, these negative images seem to be very common; for example,in one of our studies more than 60% of the individuals surveyed – from a repre-sentative sample (by age and sex) of people older than eighteen – agreed thatpeople older than 65 are cognitively impaired, have serious memory problems,cannot learn, are rigid and inflexible, are worse than younger people in problem-solving, have bad humor, and are “as children” (Fernández-Ballesteros, 1992,2006). Most important, after covariant analysis, no differences were found be-tween age groups, gender, social position, and education. Although this negativeview has improved in the last decade, it can be considered as a social threat and,therefore, any policy on aging should be preceded by changes in this negative viewof aging (e.g., UN, 2002; UNECE, 2003; WHO, 1990b). Finally, and most impor-tant, this negative view is against scientific evidence and, therefore, comes fromfalse beliefs.
In conclusion, from an Aristotelian tradition, gerontology (the scientific studyof aging, age, and the aged), has been more devoted to those biomedical andpsychosocial negative covariants that decline through age than to those that showpositive development or are stable across aging. It can be assumed that this biashas been disseminated in society through negative images. However, it must beemphasized that an opposite perspective (taking into consideration only the pos-itive conditions) would also be biased. In our view, positive aging is not a super-ficial, simplistic, and reductionistic conceptualization about aging, age, and theaged. On the contrary, it is an empirically based concept of aging that includesnot only decline and losses but growth, stability, and positive events as part of theaging process. Moreover, without denying the probability of negative conditions,
Chapter 1: A New Paradigm in the Study of Aging 5
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

they can be prevented and/or modified since human beings have, throughout thelifecycle, high levels of plasticity (Baltes & Baltes, 1990b; Fernández-Ballesteros,1986, 2003; Fries, 1989; Lehr, 1980, 1982; Whitebourn, 2005).
As a result of human and social development – including biomedical and tech-nological progress in education, health care, hygiene, nutrition, etc. – during thetwentieth century, all over the world, human lifespan increased and, in those de-veloped countries, life expectancy at birth has doubled. Also, since the second halfof the twentieth century, the fertility rate has been going down all over the world,approaching the level of replacement in most of the developed countries. Thesetwo demographic changes have produced an increase of older people, both inabsolute and relative numbers, all over the world. The aging population can beconsidered as one of the most important demographic revolution throughouthuman history.
Since science is accumulative and historical, new findings about a scientificsubject under study can change its conceptualization. From an individual pointof view, a 70-year-old man or woman born at the beginning of the twentiethcentury, who had about 40 years of life expectancy at birth, today has not only ahigh probability of living longer than his/her parents but, also, of living in betterbio-psycho-social conditions. Both multicohort and family studies have shownresults in this direction (Schaie, 2005a, 2005b).
In sum, these changes from both demographic and individual points of viewsupport the existence of a new perspective in the study of aging, age, and the aged.
Evolution in Research on Active Aging
From an evidence-based point of view, it has been during the last decades oftwentieth century that the so-called “new paradigm” or “revolution” in the fieldof aging research and, in a broader sense, in the science of gerontology started: apositive view. Pioneers in this new paradigm are from several gerontological dis-ciplines, including the fields of biomedicine and social sciences such as Fries andCrapo (1981); Fries (1989); Rowe and Khan (1987), or Baltes and Baltes (1990b).
This positive view of aging adopted several verbal rubrics: “healthy” (WHO,1990b), “successful” (Thomae, 1975; Rowe & Khan, 1987; Baltes & Baltes, 1990a),“optimal”(Palmore, 1979), “vital”(Erikson et al., 1986), “productive”(Butler & Glea-son, 1985), “active” (WHO, 2002), “positive” (Gergen & Gergen, 2001), or simply“aging well” (Fries, 1989) or “good life” (Bearon, 1996). It is important to emphasizethat all these terms are taken almost interchangeably by experts when they review thefield and in this text all of them are considered under the term “active aging” (e.g.,Depp & Jeste, 2006; Lupien & Wan, 2004; Peel, McClure, & Bartlett, 2005).
Taking into consideration all these verbal key words, two searches were con-
6 Active Aging / Part I: Conceptual Issues
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
ducted: on the Internet and within scientific literature. On the Internet (Google,May, 2007), the most often cited term was “active aging” (4,250,000) followed by“healthy aging” (2,650,000), “successful aging” (2,150,000), “optimal aging”(2,010,000), and “productive aging” (1,800,000).
The search of scientific literature was conducted in three scientific data bases:PubMed, PsycINFO, and Sociological Abstract. This search were performed from1970 to 2007 by decades using aging/aging and successful, healthy, active, opti-mal, and productive1 in all fields (the last period covers from 2000 through 2007).
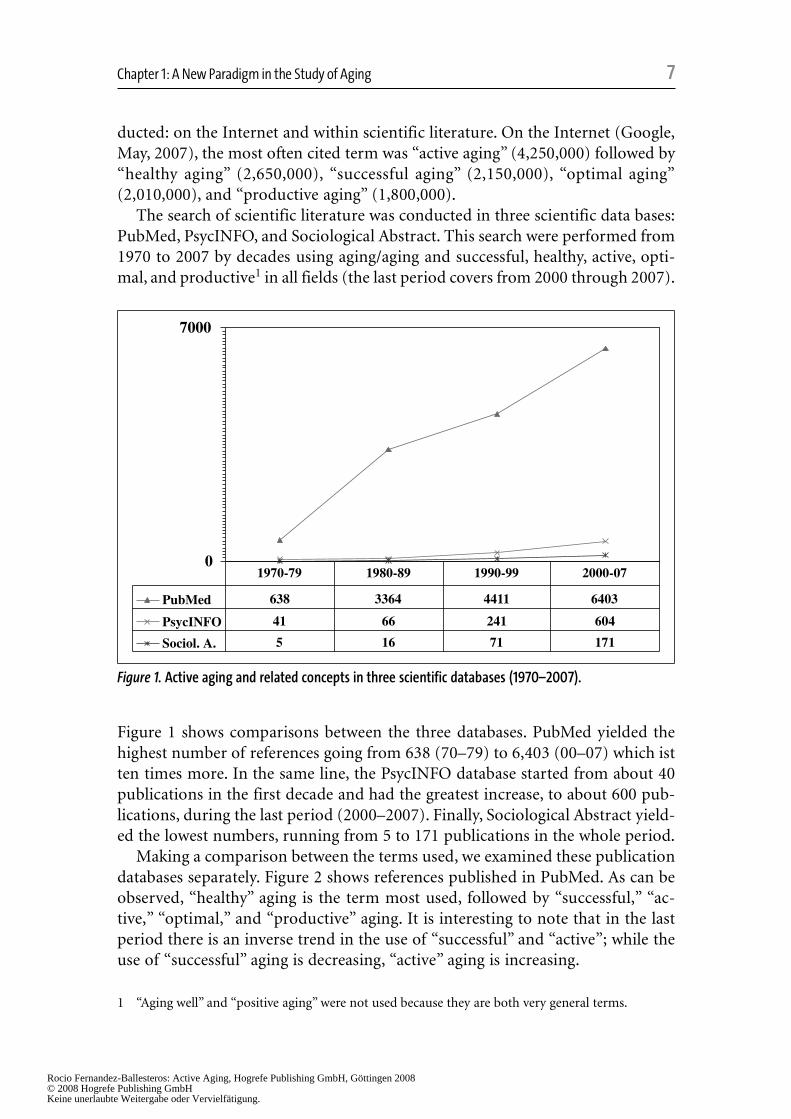
Figure 1 shows comparisons between the three databases. PubMed yielded thehighest number of references going from 638 (70–79) to 6,403 (00–07) which istten times more. In the same line, the PsycINFO database started from about 40publications in the first decade and had the greatest increase, to about 600 pub-lications, during the last period (2000–2007). Finally, Sociological Abstract yield-ed the lowest numbers, running from 5 to 171 publications in the whole period.
Making a comparison between the terms used, we examined these publicationdatabases separately. Figure 2 shows references published in PubMed. As can beobserved, “healthy” aging is the term most used, followed by “successful,” “ac-tive,” “optimal,” and “productive” aging. It is interesting to note that in the lastperiod there is an inverse trend in the use of “successful” and “active”; while theuse of “successful” aging is decreasing, “active” aging is increasing.
0
7000
PubMed 638 3364 4411 6403
PsycINFO 41 66 241 604
Sociol. A. 5 16 71 171
1970-79 1980-89 1990-99 2000-07
Figure 1. Active aging and related concepts in three scientific databases (1970–2007).
Chapter 1: A New Paradigm in the Study of Aging 7
1 “Aging well” and “positive aging” were not used because they are both very general terms.
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
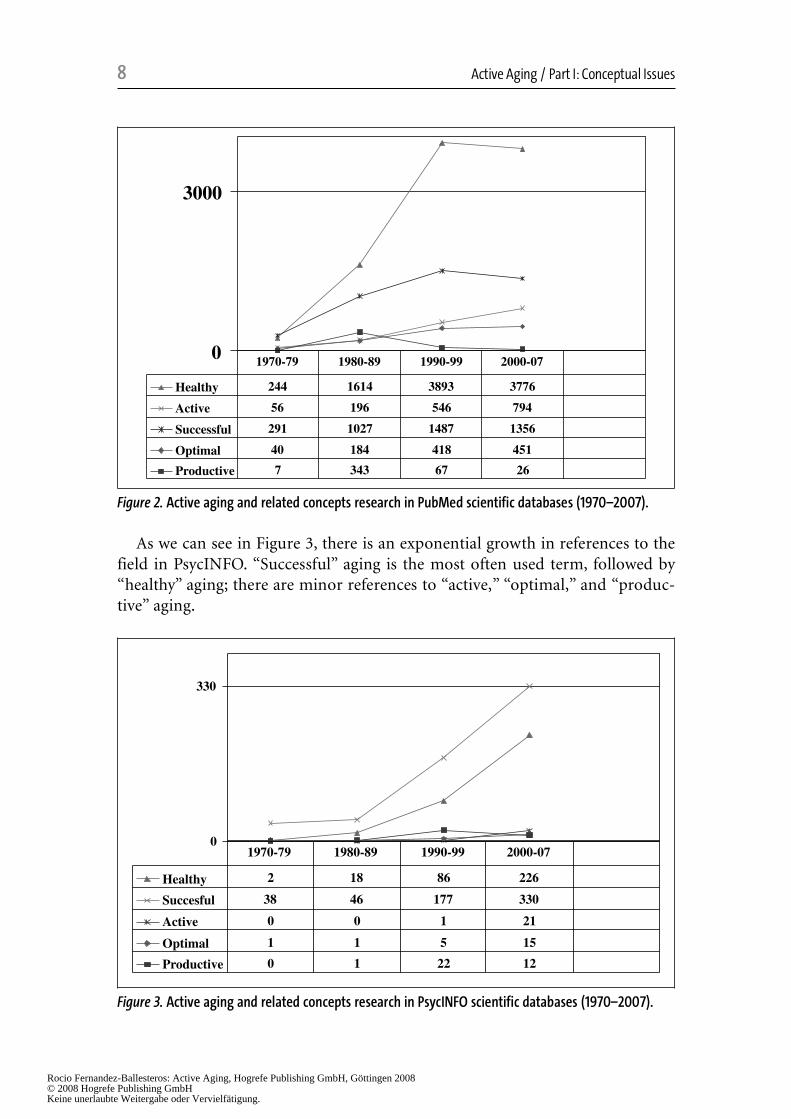
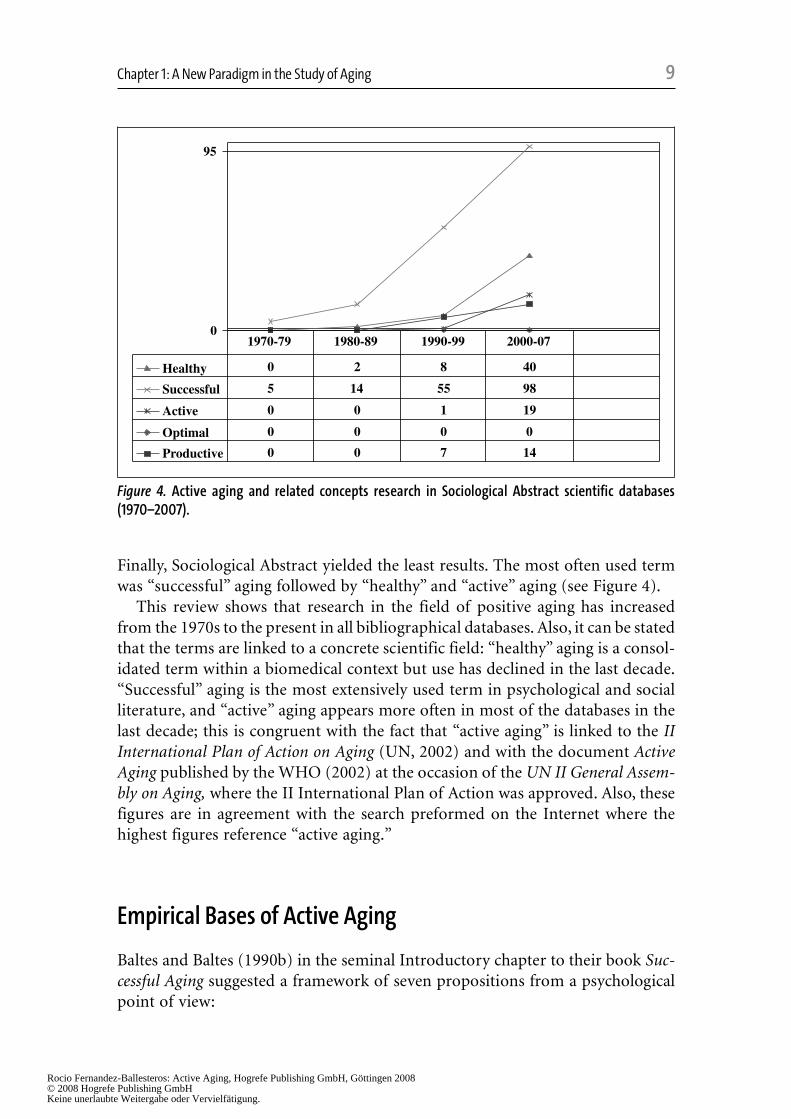
As we can see in Figure 3, there is an exponential growth in references to thefield in PsycINFO. “Successful” aging is the most often used term, followed by“healthy” aging; there are minor references to “active,” “optimal,” and “produc-tive” aging.
0
3000
Healthy 244 1614 3893 3776
Active 56 196 546 794
Successful 291 1027 1487 1356
Optimal 40 184 418 451
Productive 7 343 67 26
1970-79 1980-89 1990-99 2000-07
Figure 2. Active aging and related concepts research in PubMed scientific databases (1970–2007).
0
330
Healthy 2 18 86 226
Succesful 38 46 177 330
Active 0 0 1 21
Optimal 1 1 5 15
Productive 0 1 22 12
1970-79 1980-89 1990-99 2000-07
Figure 3. Active aging and related concepts research in PsycINFO scientific databases (1970–2007).
8 Active Aging / Part I: Conceptual Issues
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
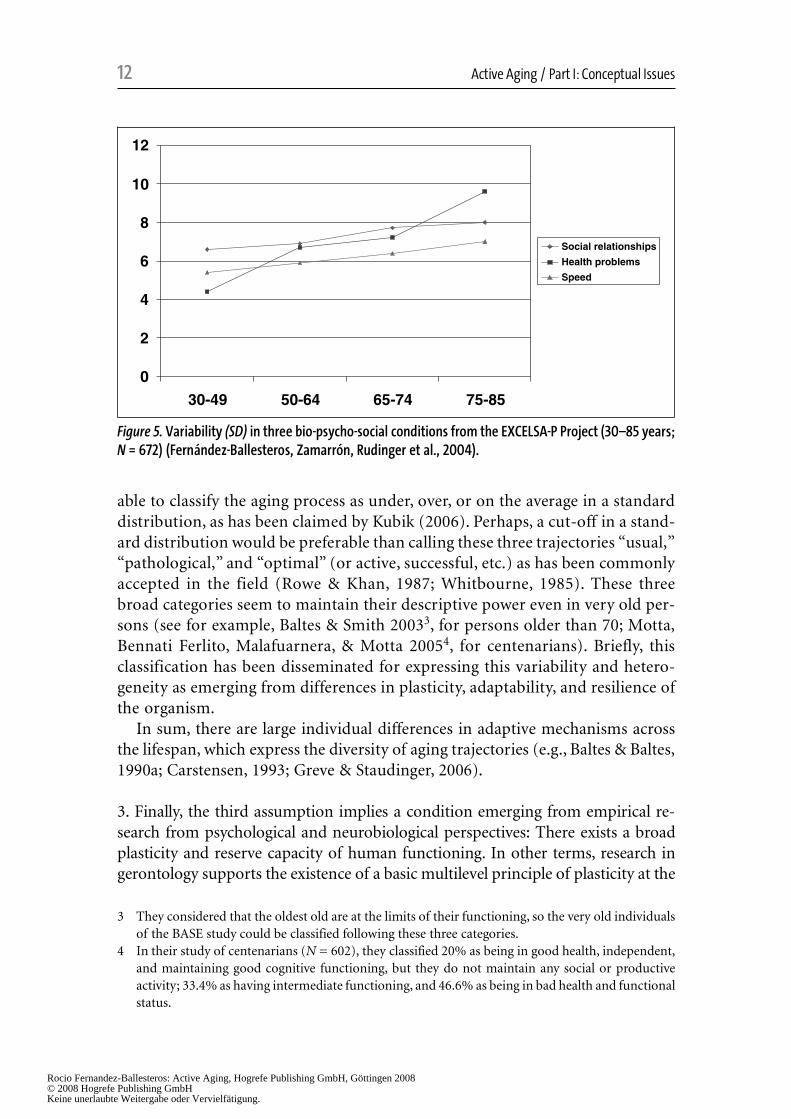
Finally, Sociological Abstract yielded the least results. The most often used termwas “successful” aging followed by “healthy” and “active” aging (see Figure 4).
This review shows that research in the field of positive aging has increasedfrom the 1970s to the present in all bibliographical databases. Also, it can be statedthat the terms are linked to a concrete scientific field: “healthy” aging is a consol-idated term within a biomedical context but use has declined in the last decade.“Successful” aging is the most extensively used term in psychological and socialliterature, and “active” aging appears more often in most of the databases in thelast decade; this is congruent with the fact that “active aging” is linked to the IIInternational Plan of Action on Aging (UN, 2002) and with the document ActiveAging published by the WHO (2002) at the occasion of the UN II General Assem-bly on Aging, where the II International Plan of Action was approved. Also, thesefigures are in agreement with the search preformed on the Internet where thehighest figures reference “active aging.”
Empirical Bases of Active Aging
Baltes and Baltes (1990b) in the seminal Introductory chapter to their book Suc-cessful Aging suggested a framework of seven propositions from a psychologicalpoint of view:
0
95
Healthy 0 2 8 40
Successful 5 14 55 98
Active 0 0 1 19
Optimal 0 0 0 0
Productive 0 0 7 14
1970-79 1980-89 1990-99 2000-07
Figure 4. Active aging and related concepts research in Sociological Abstract scientific databases(1970–2007).
Chapter 1: A New Paradigm in the Study of Aging 9
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

1. The first proposition emphasizes the major differences between normal, opti-mal, and sick (pathological) aging.
2. The second proposition emerges from the first and refers to a broad interindi-vidual variability in level, rate and direction of change. In sum, there is muchheterogeneity (variability) in aging.
3. The third proposition assumes the concept of plasticity and latent reserveacross the lifespan and, therefore, in old age.
4. The fourth proposition emerges from the empirical research establishing limitsfor behavioral plasticity and adaptive capacity.
5. With the fifth proposition authors try to reconcile propositions 3 and 4, thatis, knowledge-based pragmatics and technology can compensate for decline.
6. The sixth proposition argues that with aging the balance between gains andlosses becomes less positive. This decline or negative balance is in accord withindividuals’ subjective evaluation as well as with social stereotypes.
7. Finally, the last proposition is based on empirical evidence that there are minorage differences between life satisfaction and other positive psychological char-acteristics, therefore, it is assumed that the self remains resilient in old age.
Some of these propositions have also been supported from a biomedical perspective.Fries (Fries & Crapo, 1981; Fries, 1989) emphasized the variability of the ways ofaging (1 and 2), plasticity of aging under the assumption that major manifestationsof senescence are shown to be modifiable (3 and 4), diseases of aging may be post-poned by personal decision (for example, changing lifestyles), and, therefore, hesupports the other assumptions (5 and 6). Moreover, Fries introduced a new sourceof information about population aging: the rectangularization of the survivalcurves, which means that the shapes of survival curves are expressing not only lon-gevity but the compression of morbidity and, therefore, that sociohistorical develop-ment coincides not only with more years to life but, also, more life to years.
Trying to make a synthesis, this positive view on the field of aging emergesfrom three main observed facts supported by empirical research (demographic,epidemiological, cross-sectional, longitudinal, and experimental studies): thecompression of morbidity; the extreme variability of any bio-psycho-social condi-tion in old age, and the plasticity of human beings expressed through modifiabilityof most of those declined or impaired conditions.
1. The first assumption states that, at the population level, across history, humanbeings are living longer and in better conditions. Fries and Crapo (1981) argueagainst the medical model for the study of aging. Using new knowledge aboutaging (morbidity, mortality, and survival) they arrive at a syllogism:1. The human lifespan is fixed,2. The age at first infirmity will increase,3. Therefore, the duration of infirmity will decrease and, as a conclusion,4. The period of vitality may be prolonged.
10 Active Aging / Part I: Conceptual Issues
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.

This syllogism can be tested through the improvement of life expectancy in goodhealth, which is supported by the postponement of chronic disease and morbidityand, therefore, the “rectangularization” shape of the survival curve across time,which means that survival rate in humans is increasing not only throughout his-tory but across ages as well (see Figure 10, in Chapter 2). The decline in mortality(not only infant mortality but mortality at all ages) has raised life expectancyalmost all over the planet (Kannisto, 1996; Jeune & Vaupel, 1995). But, livinglonger does not mean living well; and increase in life expectancy could be andincrease in morbidity and disability and, therefore, in suffering at the individual,family, and population levels. Presently, the increase in life expectancy is not onlya general phenomenon but, most important, there are data supporting that mor-bidity has been concentrated in the later years of life; disability-free life expectan-cy and healthy life expectancy are slowly increasing in several of the countrieswith high life expectancy and, at least, for severe disability (see Chapter 2, Fries& Crapo, 1981; Fries, 2002; Robine, 2003; Meslé & Vallin, 2003; Robine & Michel,2004).
As is well known, this demographic revolution should be attributed to socialdevelopment, improvements in living conditions (hygiene, health services, edu-cation, etc.) but also should be taken as a consequence of the plasticity and mod-ifiability of human being throughout the lifecycle, at all ages.
2. Therefore, our second assumption emerged from the well-tested variability ofthe aging phenomenon itself, which can be classified as: usual, pathological, andoptimal aging (e.g., Baltes & Baltes, 1990b; Fries, 1989; Lerner, 1984; Plomin &Thompson, 1986; Rowe & Khan, 1997). Any pattern of decline across ages hashigh variability and variability increases throughout the lifespan (Smith & Baltes,1999). As Vaupel et al. (1998) said from a bio-demographic point of view, “evengenetically identical populations display phenotypic differences . . . Some indi-viduals are frailer than others, innately or because of acquired frailty” (p. 857).Therefore, there is high heterogeneity in the way of aging, as expressed at the levelof individuals: from successful aging to disability.
As an example, Figure 5 shows the variability (SD) in three physical (speedassessed by tapping test), health (number of health problems reported), and so-cial (social interaction frequency) conditions from the EXCELSA study per-formed in 7 European countries (N = 672), ages ranging from 30 to 85 years.Standard deviation increases by age in these three measures (Fernandez-Balles-teros, Zamarrón, Rudinger, Schroots et al., 2004).
Although this heterogeneity could be considered a continuum2, under theassumption that any individual would have a true score on this continuum(based on the mean and standard deviation of a standard distribution), we are
Chapter 1: A New Paradigm in the Study of Aging 11
2 For example, Smith and Baltes (1999) required 9 subgroups to describe a set of psychological di-mensions in persons older than 70.
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.
able to classify the aging process as under, over, or on the average in a standarddistribution, as has been claimed by Kubik (2006). Perhaps, a cut-off in a stand-ard distribution would be preferable than calling these three trajectories “usual,”“pathological,” and “optimal” (or active, successful, etc.) as has been commonlyaccepted in the field (Rowe & Khan, 1987; Whitbourne, 1985). These threebroad categories seem to maintain their descriptive power even in very old per-sons (see for example, Baltes & Smith 20033, for persons older than 70; Motta,Bennati Ferlito, Malafuarnera, & Motta 20054, for centenarians). Briefly, thisclassification has been disseminated for expressing this variability and hetero-geneity as emerging from differences in plasticity, adaptability, and resilience ofthe organism.
In sum, there are large individual differences in adaptive mechanisms acrossthe lifespan, which express the diversity of aging trajectories (e.g., Baltes & Baltes,1990a; Carstensen, 1993; Greve & Staudinger, 2006).
3. Finally, the third assumption implies a condition emerging from empirical re-search from psychological and neurobiological perspectives: There exists a broadplasticity and reserve capacity of human functioning. In other terms, research ingerontology supports the existence of a basic multilevel principle of plasticity at the
0
2
4
6
8
10
12
30-49 50-64 65-74 75-85
Social relationships
Health problems
Speed
Figure 5. Variability (SD) in three bio-psycho-social conditions from the EXCELSA-P Project (30–85 years;N = 672) (Fernández-Ballesteros, Zamarrón, Rudinger et al., 2004).
12 Active Aging / Part I: Conceptual Issues
3 They considered that the oldest old are at the limits of their functioning, so the very old individualsof the BASE study could be classified following these three categories.
4 In their study of centenarians (N = 602), they classified 20% as being in good health, independent,and maintaining good cognitive functioning, but they do not maintain any social or productiveactivity; 33.4% as having intermediate functioning, and 46.6% as being in bad health and functionalstatus.
Rocio Fernandez-Ballesteros: Active Aging, Hogrefe Publishing GmbH, Göttingen 2008© 2008 Hogrefe Publishing GmbHKeine unerlaubte Weitergabe oder Vervielfätigung.