Embed Size (px)
Citation preview
* Prof. Dr. Lukas Radbruch, 11. DGP Kongress Leipzig 2016










20



S3 Leitlinie “Palliativmedizin für Patienten mit einer nicht heilbaren Krebserkrankung”LEITLINIENUNDEM
PFEH
LUNGE
NS3 Leitlinie “Palliativmedizin für Patienten mit einer nicht heilbaren Krebserkrankung”
LEITLINIENUNDEM
PFEH
LUNGE
N
Schwerpunkt: Palliativmedizin
Patient mit nichtheilbarerKrebserkrankung– Integration von
von Palliativversorgung
Niedrig/mittel
Tod des Patienten
Erfassen der Patienten- und Angehörigenbedürfnisse
und Ermittlung derder Komplexität
Hoch
Trauerbegleitung(Angehörige)
(Re-)Evaluation
Allgemeine Krankenhausstation/onkologische Station/
Pflegeeinrichtungen
Palliativ-dienst im
Krankenhaus
Palliativ-station
Palliativmed. Tagesklinik
Allgemeine ambulante Palliativversorgung
Spezialisierte ambulante Palliativver-
sorgung
Spezialisierte Palliativ-
ambulanzTageshospiz
Stationäres Hospiz
Hospizdienste/Ehrenamt
Durchführung einer Intervention derspezialisierten Palliativversorgung
Durchführung einer Intervention derallgemeinen Palliativversorgung
Festlegung einer Interventionder Palliativversorgung
Stationär
Ambulant
Sektoren-übergreifend
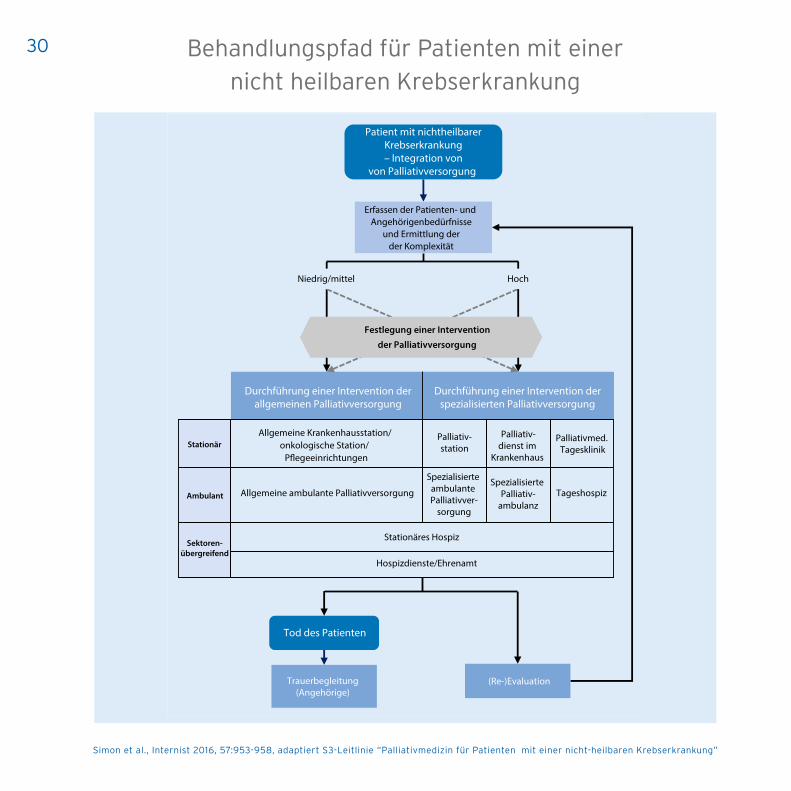
Abb. 19 Behandlungs-pfad für Patienten undAn-gehörige. (Adaptiert nachS3-Leitlinie „Palliativmedi-zin für Patientenmit einernicht heilbaren Krebser-krankung“ [6])
gleiten. Deshalb wurden die Empfehlun-gen der S3-Leitlinie sowohl für die all-gemeine (APV) als auch für die speziali-sierte Palliativversorgung (SPV) formu-liert. Ein Behandlungspfad macht deut-lich, welche Strukturen der Palliativver-sorgung den Patienten und Angehörigenim Krankheitsverlauf zur Verfügung ste-hen (. Abb. 1).
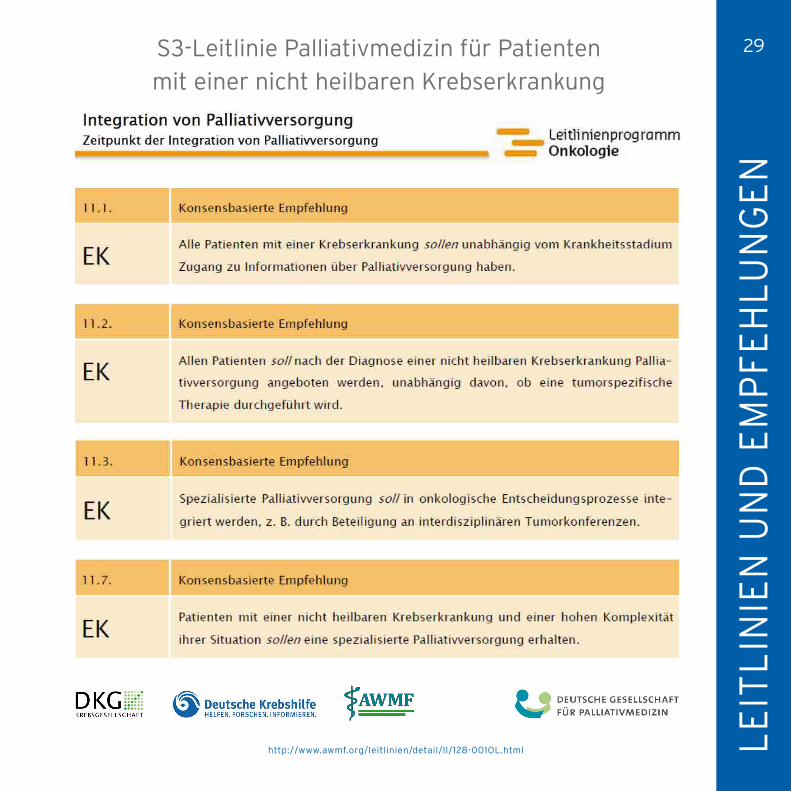
Zeitpunkt der Integration vonPalliativversorgung
Der Behandlungspfad beginnt mit derFeststellung der Nichtheilbarkeit einerKrebserkrankung. Ab diesem Zeitpunktsoll den Patienten in einfühlsamen Ge-sprächenundmitRücksicht auf ihreAuf-klärungswünsche ein Zugang zur Pallia-tivmedizin angeboten werden. Palliativ-medizin und tumorspezifische palliati-ve Therapien wie Chemo- oder Radio-
therapie schließen sich gegenseitig nichtaus. Wichtig ist die Frühintegration derPalliativversorgung, die es ermöglicht,Patienten und Angehörige im gesamtenKrankheitsverlaufzubegleitenundihneneine bedürfnisorientierteVersorgungan-zubieten.DieBedeutungder frühen Inte-grationwurde imKonsensderLeitlinien-gruppe auf der Basis von Studienevidenzhervorgehoben. In der Literatur zeigensich Vorteile bei Modellen, die eine SPVfrühzeitig, d. h. zeitnah nach der Dia-
954 Der Internist 10 · 2016



3434

www.asco.org/palliative-care-guideline ©American Society of Clinical Oncology 2016. All rights reserved.
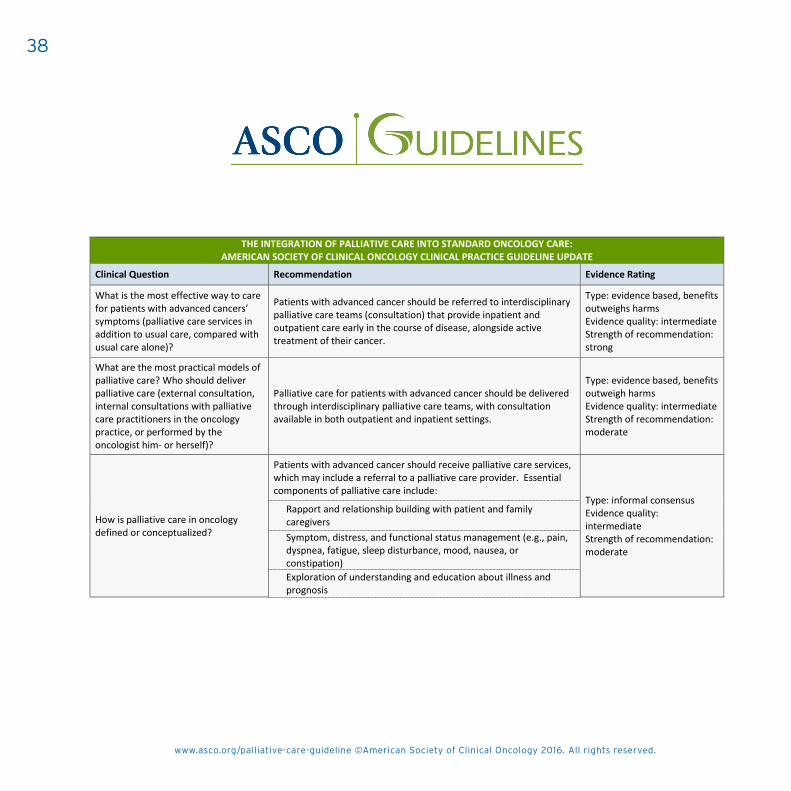
THE INTEGRATION OF PALLIATIVE CARE INTO STANDARD ONCOLOGY CARE: AMERICAN SOCIETY OF CLINICAL ONCOLOGY CLINICAL PRACTICE GUIDELINE UPDATE
Clinical Question Recommendation Evidence Rating
What is the most effective way to care
for patients with advanced cancers’
symptoms (palliative care services in
addition to usual care, compared with
usual care alone)?
Patients with advanced cancer should be referred to interdisciplinary
palliative care teams (consultation) that provide inpatient and
outpatient care early in the course of disease, alongside active
treatment of their cancer.
Type: evidence based, benefits
outweighs harms
Evidence quality: intermediate
Strength of recommendation:
strong
What are the most practical models of
palliative care? Who should deliver
palliative care (external consultation,
internal consultations with palliative
care practitioners in the oncology
practice, or performed by the
oncologist him- or herself)?
Palliative care for patients with advanced cancer should be delivered
through interdisciplinary palliative care teams, with consultation
available in both outpatient and inpatient settings.
Type: evidence based, benefits
outweigh harms
Evidence quality: intermediate
Strength of recommendation:
moderate
How is palliative care in oncology
defined or conceptualized?
Patients with advanced cancer should receive palliative care services,
which may include a referral to a palliative care provider. Essential
components of palliative care include:
Type: informal consensus
Evidence quality:
intermediate
Strength of recommendation:
moderate
Rapport and relationship building with patient and family
caregivers
Symptom, distress, and functional status management (e.g., pain,
dyspnea, fatigue, sleep disturbance, mood, nausea, or
constipation)
Exploration of understanding and education about illness and
prognosis
www.asco.org/palliative-care-guideline ©American Society of Clinical Oncology 2016. All rights reserved.
THE INTEGRATION OF PALLIATIVE CARE INTO STANDARD ONCOLOGY CARE: AMERICAN SOCIETY OF CLINICAL ONCOLOGY CLINICAL PRACTICE GUIDELINE UPDATE
Clinical Question Recommendation Evidence Rating
What is the most effective way to care
for patients with advanced cancers’
symptoms (palliative care services in
addition to usual care, compared with
usual care alone)?
Patients with advanced cancer should be referred to interdisciplinary
palliative care teams (consultation) that provide inpatient and
outpatient care early in the course of disease, alongside active
treatment of their cancer.
Type: evidence based, benefits
outweighs harms
Evidence quality: intermediate
Strength of recommendation:
strong
What are the most practical models of
palliative care? Who should deliver
palliative care (external consultation,
internal consultations with palliative
care practitioners in the oncology
practice, or performed by the
oncologist him- or herself)?
Palliative care for patients with advanced cancer should be delivered
through interdisciplinary palliative care teams, with consultation
available in both outpatient and inpatient settings.
Type: evidence based, benefits
outweigh harms
Evidence quality: intermediate
Strength of recommendation:
moderate
How is palliative care in oncology
defined or conceptualized?
Patients with advanced cancer should receive palliative care services,
which may include a referral to a palliative care provider. Essential
components of palliative care include:
Type: informal consensus
Evidence quality:
intermediate
Strength of recommendation:
moderate
Rapport and relationship building with patient and family
caregivers
Symptom, distress, and functional status management (e.g., pain,
dyspnea, fatigue, sleep disturbance, mood, nausea, or
constipation)
Exploration of understanding and education about illness and
prognosis
www.asco.org/palliative-care-guideline ©American Society of Clinical Oncology 2016. All rights reserved.
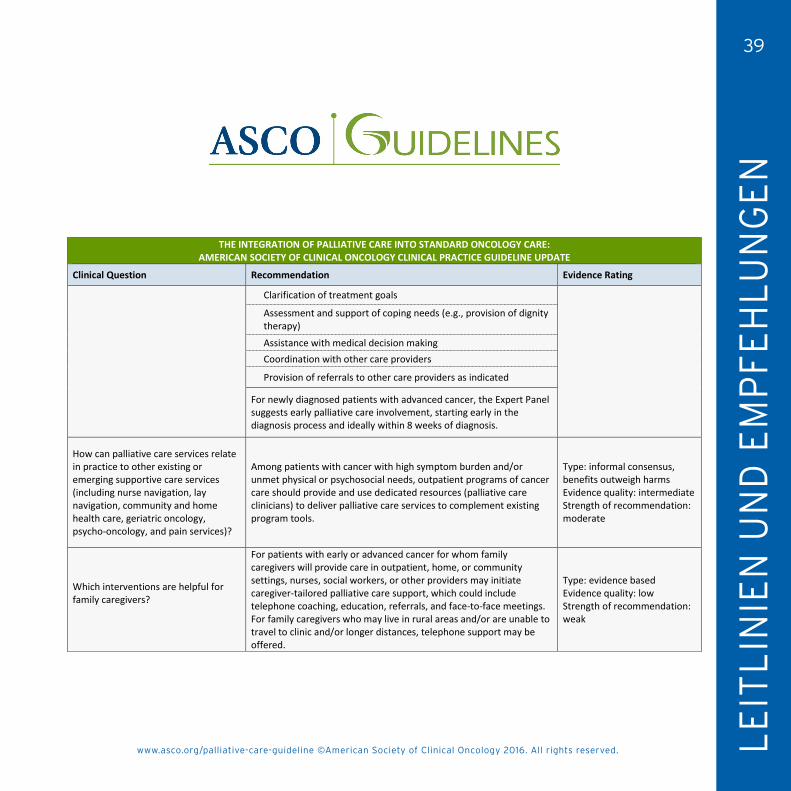
THE INTEGRATION OF PALLIATIVE CARE INTO STANDARD ONCOLOGY CARE: AMERICAN SOCIETY OF CLINICAL ONCOLOGY CLINICAL PRACTICE GUIDELINE UPDATE
Clinical Question Recommendation Evidence Rating
Clarification of treatment goals
Assessment and support of coping needs (e.g., provision of dignity
therapy)
Assistance with medical decision making
Coordination with other care providers
Provision of referrals to other care providers as indicated
For newly diagnosed patients with advanced cancer, the Expert Panel
suggests early palliative care involvement, starting early in the
diagnosis process and ideally within 8 weeks of diagnosis.
How can palliative care services relate
in practice to other existing or
emerging supportive care services
(including nurse navigation, lay
navigation, community and home
health care, geriatric oncology,
psycho-oncology, and pain services)?
Among patients with cancer with high symptom burden and/or
unmet physical or psychosocial needs, outpatient programs of cancer
care should provide and use dedicated resources (palliative care
clinicians) to deliver palliative care services to complement existing
program tools.
Type: informal consensus,
benefits outweigh harms
Evidence quality: intermediate
Strength of recommendation:
moderate
Which interventions are helpful for
family caregivers?
For patients with early or advanced cancer for whom family
caregivers will provide care in outpatient, home, or community
settings, nurses, social workers, or other providers may initiate
caregiver-tailored palliative care support, which could include
telephone coaching, education, referrals, and face-to-face meetings.
For family caregivers who may live in rural areas and/or are unable to
travel to clinic and/or longer distances, telephone support may be
offered.
Type: evidence based
Evidence quality: low
Strength of recommendation:
weak
www.asco.org/palliative-care-guideline ©American Society of Clinical Oncology 2016. All rights reserved.
THE INTEGRATION OF PALLIATIVE CARE INTO STANDARD ONCOLOGY CARE: AMERICAN SOCIETY OF CLINICAL ONCOLOGY CLINICAL PRACTICE GUIDELINE UPDATE
Clinical Question Recommendation Evidence Rating
What is the most effective way to care
for patients with advanced cancers’
symptoms (palliative care services in
addition to usual care, compared with
usual care alone)?
Patients with advanced cancer should be referred to interdisciplinary
palliative care teams (consultation) that provide inpatient and
outpatient care early in the course of disease, alongside active
treatment of their cancer.
Type: evidence based, benefits
outweighs harms
Evidence quality: intermediate
Strength of recommendation:
strong
What are the most practical models of
palliative care? Who should deliver
palliative care (external consultation,
internal consultations with palliative
care practitioners in the oncology
practice, or performed by the
oncologist him- or herself)?
Palliative care for patients with advanced cancer should be delivered
through interdisciplinary palliative care teams, with consultation
available in both outpatient and inpatient settings.
Type: evidence based, benefits
outweigh harms
Evidence quality: intermediate
Strength of recommendation:
moderate
How is palliative care in oncology
defined or conceptualized?
Patients with advanced cancer should receive palliative care services,
which may include a referral to a palliative care provider. Essential
components of palliative care include:
Type: informal consensus
Evidence quality:
intermediate
Strength of recommendation:
moderate
Rapport and relationship building with patient and family
caregivers
Symptom, distress, and functional status management (e.g., pain,
dyspnea, fatigue, sleep disturbance, mood, nausea, or
constipation)
Exploration of understanding and education about illness and
prognosis
Hospiz- und Palliativgesetz Bessere Versorgung schwerstkranker Menschen
Schwerstkranke Menschen sollen überall dort gut versorgt sein und begleitet werden, wo sie die letzte Phase ihres Lebens verbringen – ob zu Hause, im Pflegeheim, im Hospiz oder Krankenhaus.
Warum muss die Hospiz- und Palliativversorgung weiterentwickelt werden?
Darauf kommt es anGUTE PFLEGE
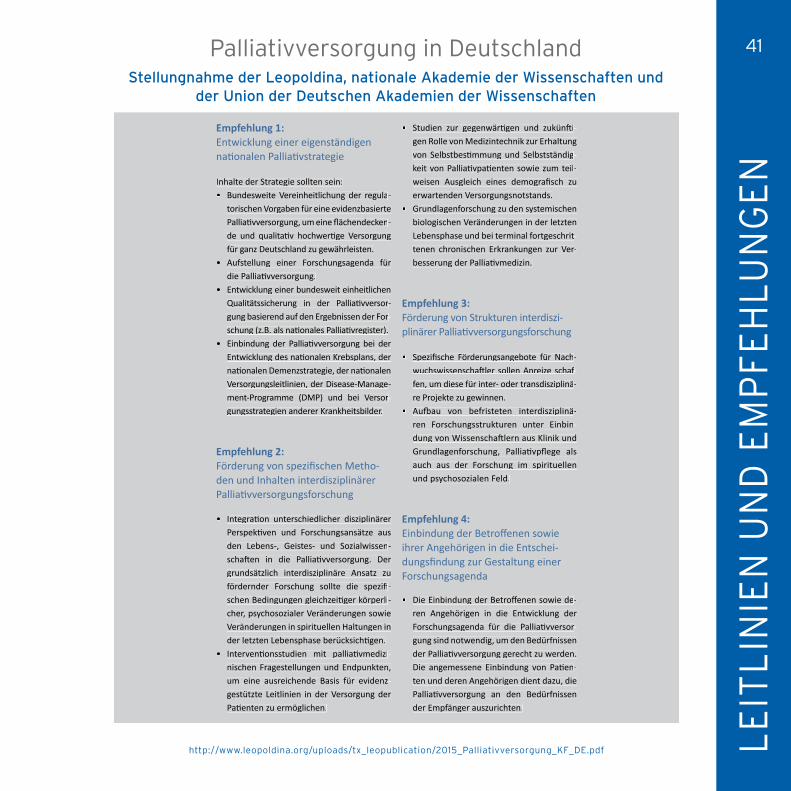
Empfehlungen
Empfehlung 1:Entwicklung einer eigenständigennationalen Palliativstrategie
Inhalte der Strategie sollten sein:• Bundesweite Vereinheitlichung der regula-
torischen Vorgaben für eine evidenzbasierte Palliativversorgung, um eine flächendecken-de und qualitativ hochwertige Versorgung für ganz Deutschland zu gewährleisten.
• Aufstellung einer Forschungsagenda für die Palliativversorgung.
• Entwicklung einer bundesweit einheitlichen Qualitätssicherung in der Palliativversor-gung basierend auf den Ergebnissen der For-schung (z.B. als nationales Palliativregister).
• Einbindung der Palliativversorgung bei der Entwicklung des nationalen Krebsplans, der nationalen Demenzstrategie, der nationalen Versorgungsleitlinien, der Disease-Manage-ment-Programme (DMP) und bei Versor-gungsstrategien anderer Krankheitsbilder.
Empfehlung 2:Förderung von spezifischen Metho-den und Inhalten interdisziplinärer Palliativversorgungsforschung
• Integration unterschiedlicher disziplinärer Perspektiven und Forschungsansätze aus den Lebens-, Geistes- und Sozialwissen-schaften in die Palliativversorgung. Der grundsätzlich interdisziplinäre Ansatz zu fördernder Forschung sollte die spezifi-schen Bedingungen gleichzeitiger körperli-cher, psychosozialer Veränderungen sowie Veränderungen in spirituellen Haltungen in der letzten Lebensphase berücksichtigen.
• Interventionsstudien mit palliativmedizi-nischen Fragestellungen und Endpunkten, um eine ausreichende Basis für evidenz-gestützte Leitlinien in der Versorgung der Patienten zu ermöglichen.
• Studien zur gegenwärtigen und zukünfti-gen Rolle von Medizintechnik zur Erhaltung von Selbstbestimmung und Selbstständig-keit von Palliativpatienten sowie zum teil-weisen Ausgleich eines demografisch zu erwartenden Versorgungsnotstands.
• Grundlagenforschung zu den systemischen biologischen Veränderungen in der letzten Lebensphase und bei terminal fortgeschrit-tenen chronischen Erkrankungen zur Ver-besserung der Palliativmedizin.
Empfehlung 3:Förderung von Strukturen interdiszi-plinärer Palliativversorgungsforschung
• Spezifische Förderungsangebote für Nach-wuchswissenschaftler sollen Anreize schaf-wuchswissenschaftler sollen Anreize schaf-wuchswissenschaftler sollen Anreize schaffen, um diese für inter- oder transdisziplinä-re Projekte zu gewinnen.
• Aufbau von befristeten interdisziplinä-ren Forschungsstrukturen unter Einbin-dung von Wissenschaftlern aus Klinik und Grundlagenforschung, Palliativpflege als auch aus der Forschung im spirituellen und psychosozialen Feld.
Empfehlung 4:Einbindung der Betroffenen sowie ihrer Angehörigen in die Entschei-dungsfindung zur Gestaltung einer Forschungsagenda
• Die Einbindung der Betroffenen sowie de-ren Angehörigen in die Entwicklung der Forschungsagenda für die Palliativversor-gung sind notwendig, um den Bedürfnissen der Palliativversorgung gerecht zu werden. Die angemessene Einbindung von Patien-ten und deren Angehörigen dient dazu, die Palliativversorgung an den Bedürfnissen der Empfänger auszurichten.
Palliativversorgung in Deutschland | Empfehlungen

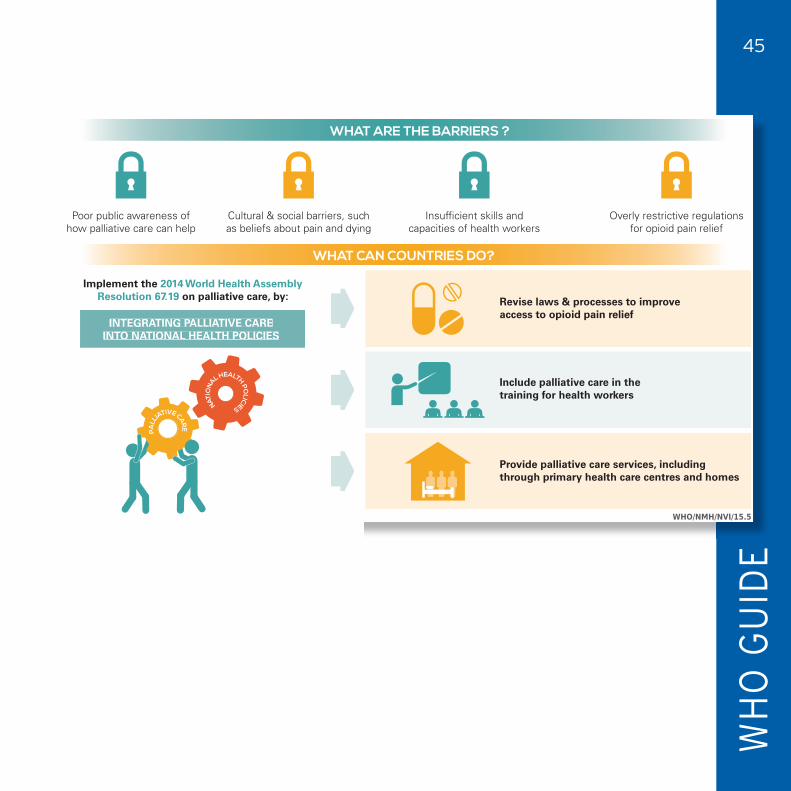
WHAT CAN COUNTRIES DO?
WHAT ARE THE BARRIERS ?
Diagnosis Death Bereavementsupport
PALLIATIVE CARE
DISEASE PROGRESSION
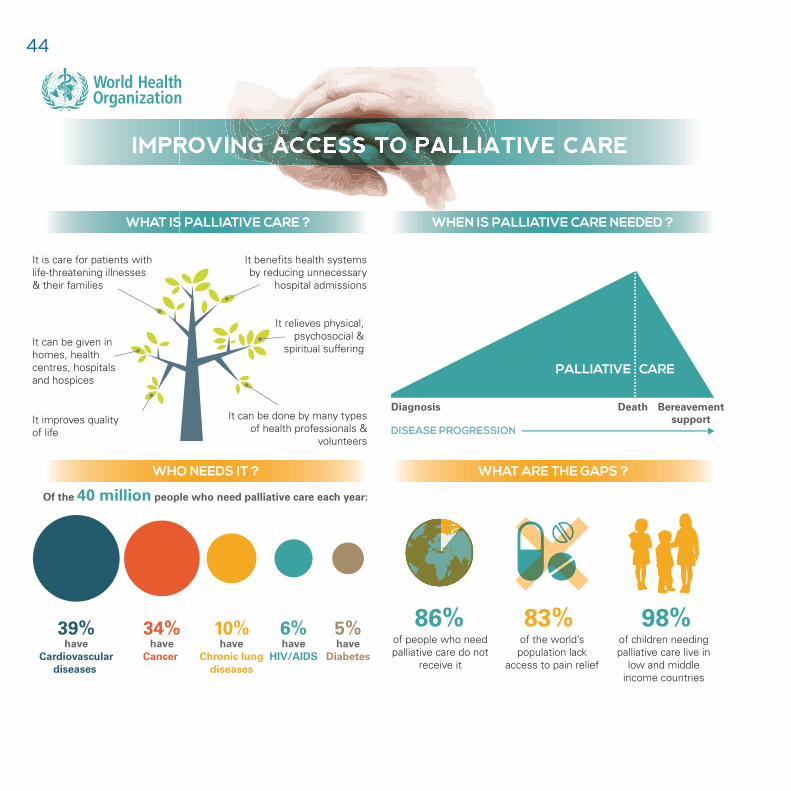
It is care for patients withlife-threatening illnesses& their families
It improves qualityof life
It relieves physical, psychosocial &
spiritual suffering
It benefits health systemsby reducing unnecessary
hospital admissions
of the world’s population lack
access to pain relief
83% of people who need palliative care do not
receive it
86%of children needing palliative care live in
low and middle income countries
98%
Of the 40 million people who need palliative care each year:
WHAT ARE THE GAPS ?WHO NEEDS IT ?
It can be given in homes, health centres, hospitals and hospices
It can be done by many types of health professionals &
volunteers
Insufficient skills andcapacities of health workers
Overly restrictive regulations for opioid pain relief
Poor public awareness ofhow palliative care can help
Cultural & social barriers, suchas beliefs about pain and dying
Implement the 2014 World Health AssemblyResolution 67.19 on palliative care, by:
IMPROVING ACCESS TO PALLIATIVE CARE
39%have
Cardiovasculardiseases
34%have
Cancer
10%have
Chronic lungdiseases
6%have
HIV/AIDS
5%have
Diabetes
PALL
IATIVE CARE
NATIO
NA
L HEALTH POLICIES
Revise laws & processes to improve access to opioid pain relief
Include palliative care in the training for health workers
Provide palliative care services, includingthrough primary health care centres and homes
WHO/NMH/NVI/15.5
WHEN IS PALLIATIVE CARE NEEDED ?WHAT IS PALLIATIVE CARE ?
WHAT CAN COUNTRIES DO?
WHAT ARE THE BARRIERS ?
Diagnosis Death Bereavementsupport
PALLIATIVE CARE
It is care for patients withlife-threatening illnesses& their families
It improves qualityof life
It relieves physical, psychosocial &
spiritual suffering
It benefits health systemsby reducing unnecessary
hospital admissions
of the world’s population lack
access to pain relief
83% of people who need palliative care do not
receive it
86%of children needing palliative care live in
low and middle income countries
98%
Of the 40 million people who need palliative care each year:
WHAT ARE THE GAPS ?WHO NEEDS IT ?
It can be given in homes, health centres, hospitals and hospices
It can be done by many types of health professionals &
volunteers
Insufficient skills andcapacities of health workers
Overly restrictive regulations for opioid pain relief
Poor public awareness ofhow palliative care can help
Cultural & social barriers, suchas beliefs about pain and dying
Implement the 2014 World Health AssemblyResolution 67.19 on palliative care, by:
IMPROVING ACCESS TO PALLIATIVE CARE
39%have
Cardiovasculardiseases
34%have
Cancer
10%have
Chronic lungdiseases
6%have
HIV/AIDS
5%have
Diabetes
INTEGRATING PALLIATIVE CAREINTO NATIONAL HEALTH POLICIES
PALL
IATIVE CARE
NATIO
NA
L HEALTH POLICIES
Revise laws & processes to improve access to opioid pain relief
Include palliative care in the training for health workers
Provide palliative care services, includingthrough primary health care centres and homes
WHO/NMH/NVI/15.5
WHEN IS PALLIATIVE CARE NEEDED ?WHAT IS PALLIATIVE CARE ?


49

50





























