Embed Size (px)
Citation preview

STW – eingeschränkte NIERENFUNKTION
MAßGEBLICHE BEFUNDE ?
FOLGESCHÄDEN
THERAPIEOPTIONEN
Begleitende THERAPIE Kurt Derfler, Interne Klinik III-Nephrologie, AKH-Uni-Wien
CT_12072012
BLUTFETTE und NIERENERINSUFFIZIENZ
Die halbe
Wahrheit
! ? ! ? ! ?
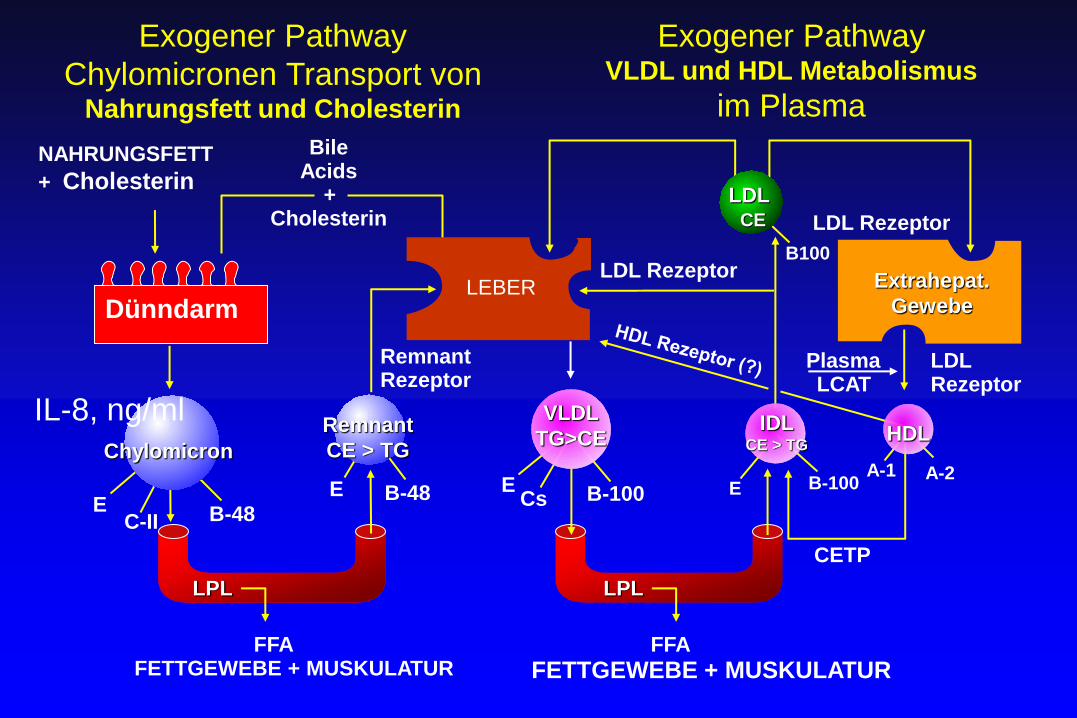
IL-8, ng/ml
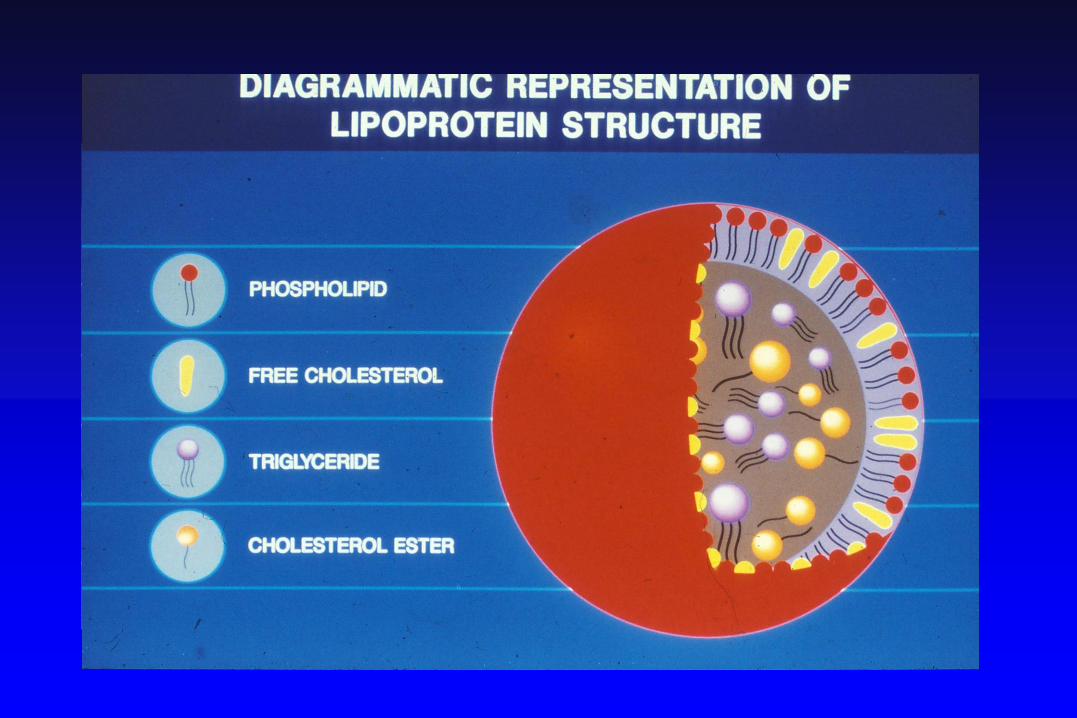
Chylomicron
E C-II B-48
Remnant
CE > TG
B-48 E
Remnant Rezeptor
FFA FETTGEWEBE + MUSKULATUR
Bile Acids
+ Cholesterin
NAHRUNGSFETT
+ Cholesterin
Dünndarm
LDL Rezeptor
LDL Rezeptor
B100
LDL Rezeptor
Plasma LCAT
B-100 E
FFA
FETTGEWEBE + MUSKULATUR
E Cs B-100
A-1 A-2
CETP
Exogener Pathway
Chylomicronen Transport von Nahrungsfett und Cholesterin
Exogener Pathway VLDL und HDL Metabolismus
im Plasma
LDL CE
LEBER Extrahepat.
Gewebe
LPL LPL
VLDL
TG>CE HDL IDL
CE > TG
12
10
8
6
4
2
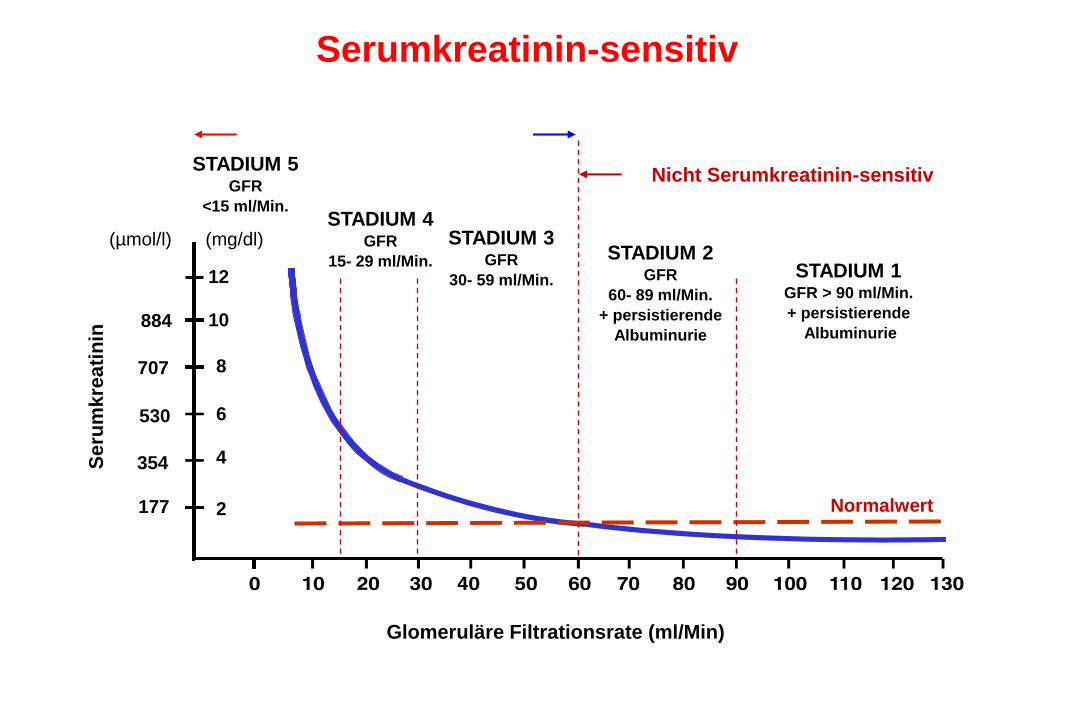
884
707
530
354
177
(mg/dl) (µmol/l)
Se
rum
kre
ati
nin
STADIUM 1 GFR > 90 ml/Min.
+ persistierende
Albuminurie
STADIUM 2 GFR
60- 89 ml/Min.
+ persistierende
Albuminurie
STADIUM 3 GFR
30- 59 ml/Min.
STADIUM 4 GFR
15- 29 ml/Min.
STADIUM 5 GFR
<15 ml/Min.
Glomeruläre Filtrationsrate (ml/Min)
Nicht Serumkreatinin-sensitiv
Serumkreatinin-sensitiv
Normalwert
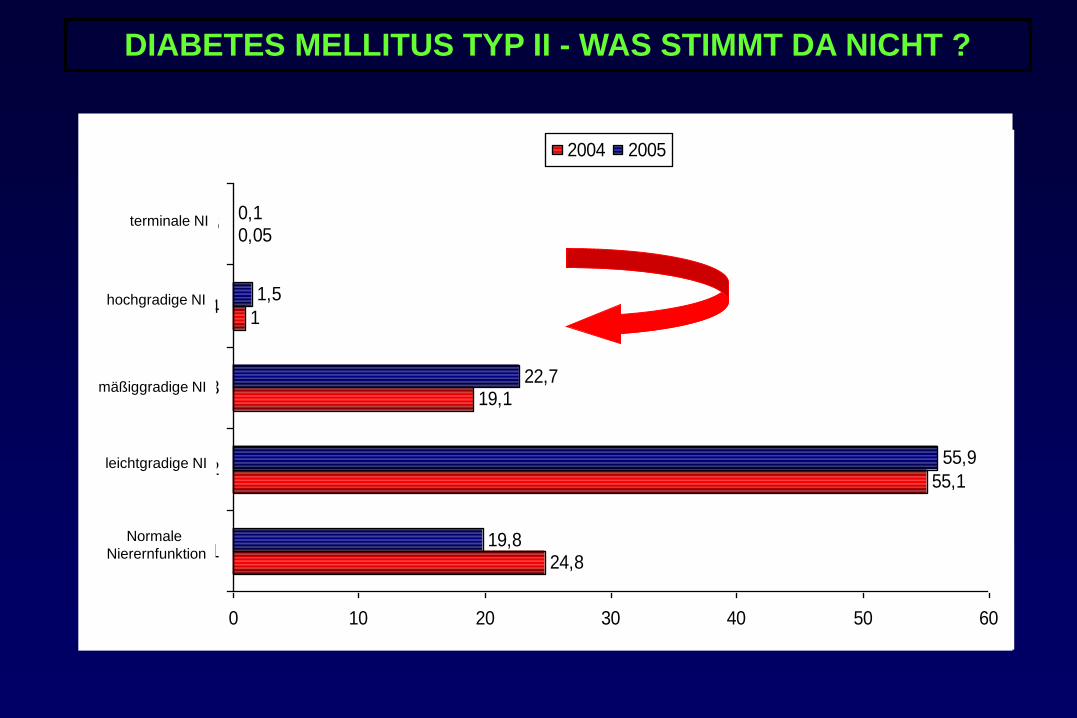
24,8
55,1
19,1
1
0,05
19,8
55,9
22,7
1,5
0,1
0 10 20 30 40 50 60
1
2
3
4
5
2004 2005
Normale
Nierernfunktion
leichtgradige NI
mäßiggradige NI
hochgradige NI
terminale NI
DIABETES MELLITUS TYP II - WAS STIMMT DA NICHT ?
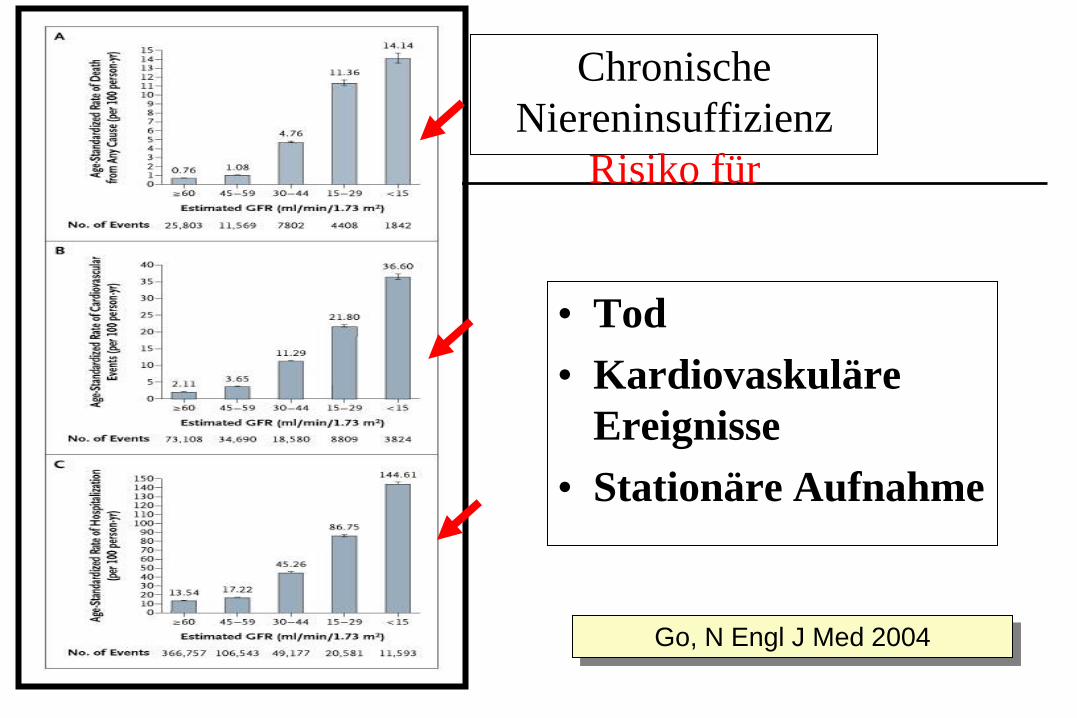
Chronische
Niereninsuffizienz
Risiko für
• Tod
• Kardiovaskuläre
Ereignisse
• Stationäre Aufnahme
Go, N Engl J Med 2004
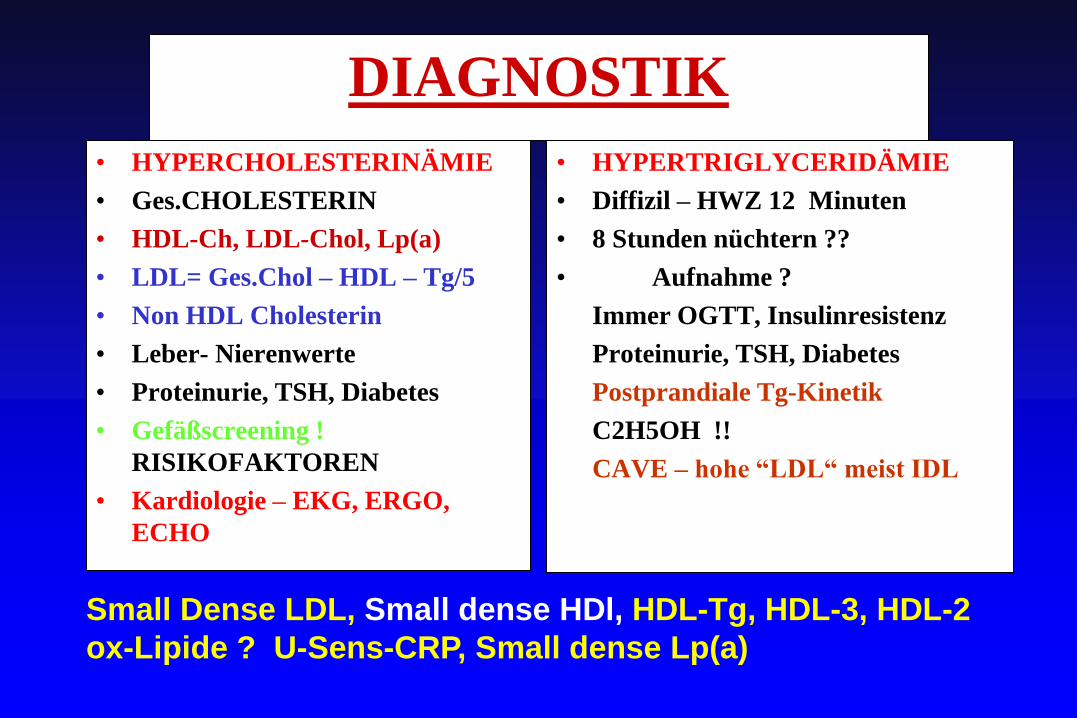
DIAGNOSTIK
• HYPERCHOLESTERINÄMIE
• Ges.CHOLESTERIN
• HDL-Ch, LDL-Chol, Lp(a)
• LDL= Ges.Chol – HDL – Tg/5
• Non HDL Cholesterin
• Leber- Nierenwerte
• Proteinurie, TSH, Diabetes
• Gefäßscreening !
RISIKOFAKTOREN
• Kardiologie – EKG, ERGO,
ECHO
• HYPERTRIGLYCERIDÄMIE
• Diffizil – HWZ 12 Minuten
• 8 Stunden nüchtern ??
• Aufnahme ?
Immer OGTT, Insulinresistenz
Proteinurie, TSH, Diabetes
Postprandiale Tg-Kinetik
C2H5OH !!
CAVE – hohe “LDL“ meist IDL
Small Dense LDL, Small dense HDl, HDL-Tg, HDL-3, HDL-2
ox-Lipide ? U-Sens-CRP, Small dense Lp(a)
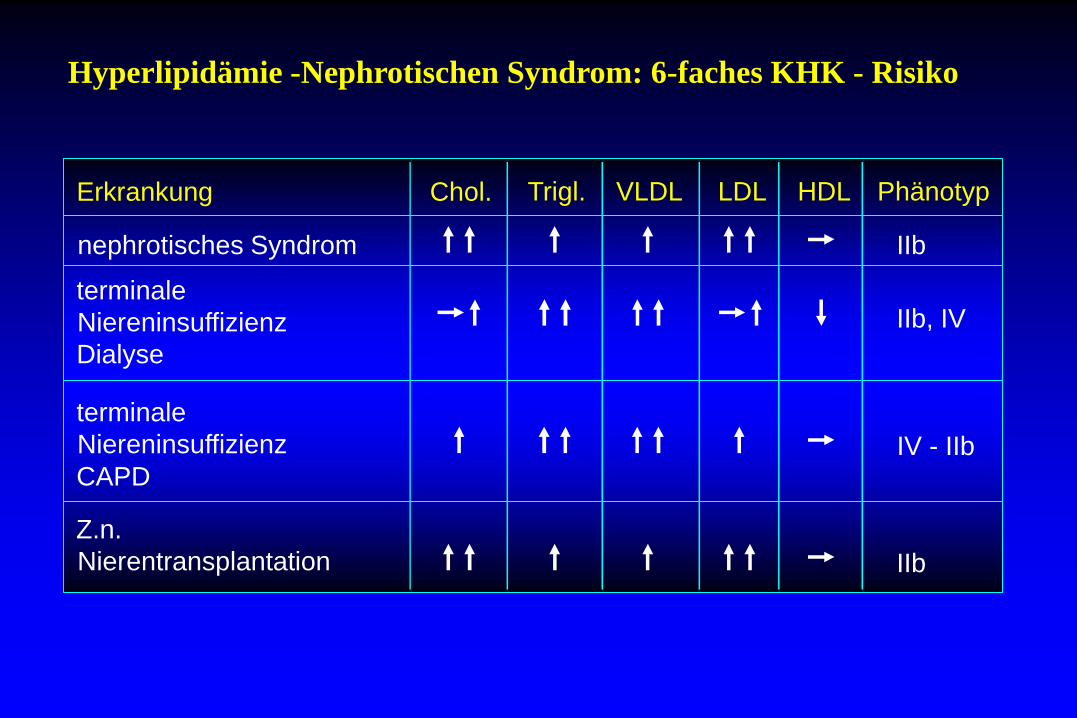
Hyperlipidämie -Nephrotischen Syndrom: 6-faches KHK - Risiko
Trigl. VLDL LDL HDL Phänotyp Erkrankung Chol.
nephrotisches Syndrom
terminale
Niereninsuffizienz
Dialyse
terminale
Niereninsuffizienz
CAPD
Z.n.
Nierentransplantation
IIb
IIb, IV
IV - IIb
IIb
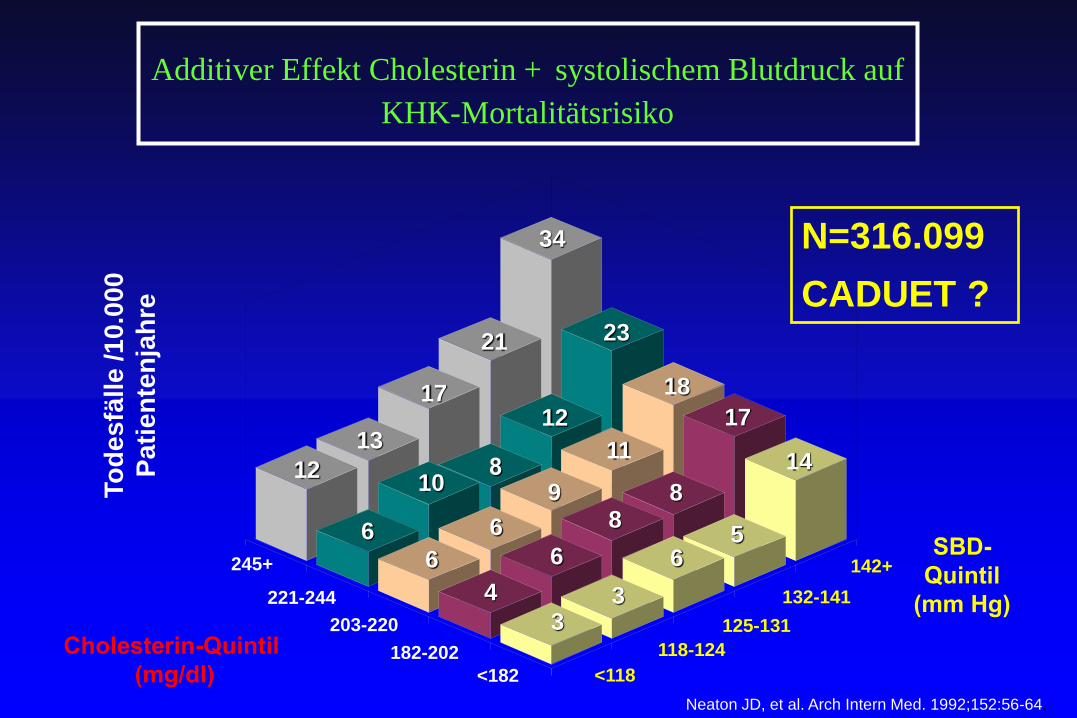
Neaton JD, et al. Arch Intern Med. 1992;152:56-64.
142+
125-131
<182
182-202
203-220
221-244
<118
118-124
132-141
34
21
13
6
23
12
10
6
18
11
9
6
4
17
8 8
6
3
To
de
sfä
lle
/1
0.0
00
Pa
tie
nte
nja
hre
245+
14
5 6
3
12
17
N=316.099
CADUET ?
Additiver Effekt Cholesterin + systolischem Blutdruck auf
KHK-Mortalitätsrisiko
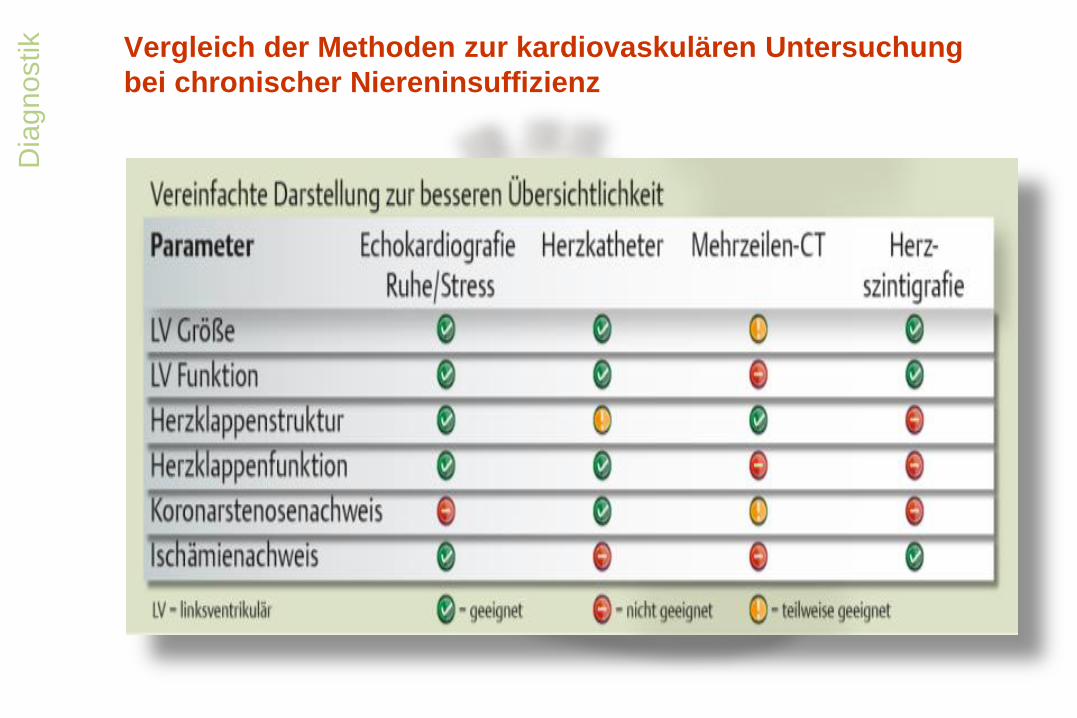
Vergleich der Methoden zur kardiovaskulären Untersuchung
bei chronischer Niereninsuffizienz
Dia
gnostik
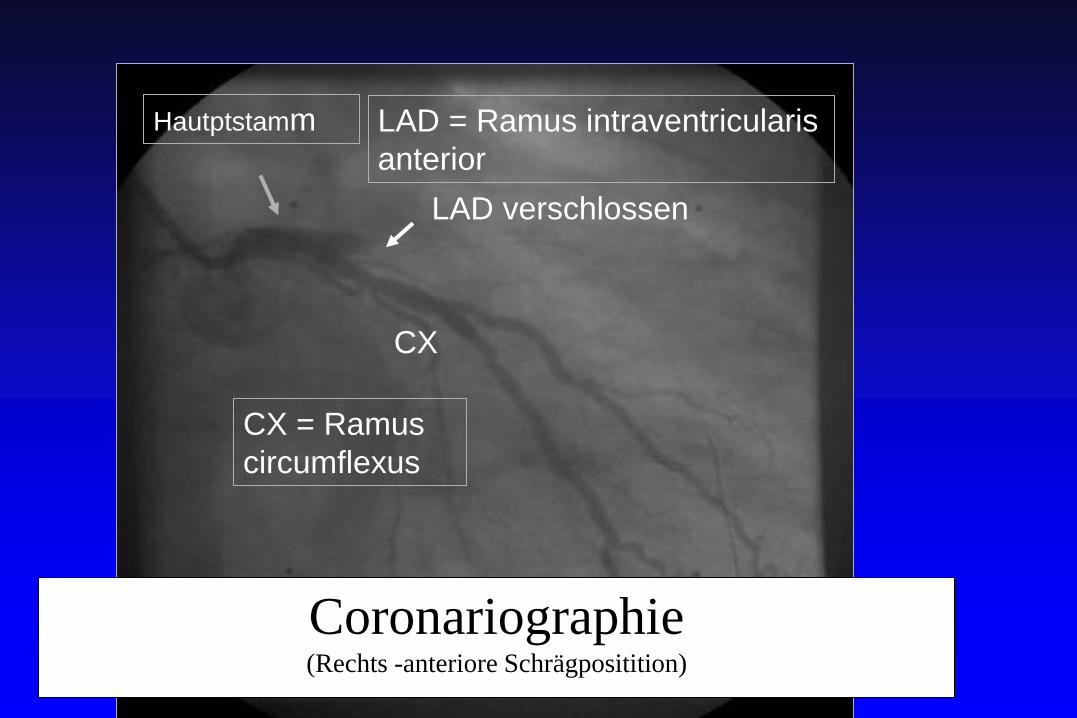
LAD verschlossen
CX
LAD = Ramus intraventricularis
anterior
CX = Ramus
circumflexus
Hautptstamm
Coronariographie (Rechts -anteriore Schrägpositition)
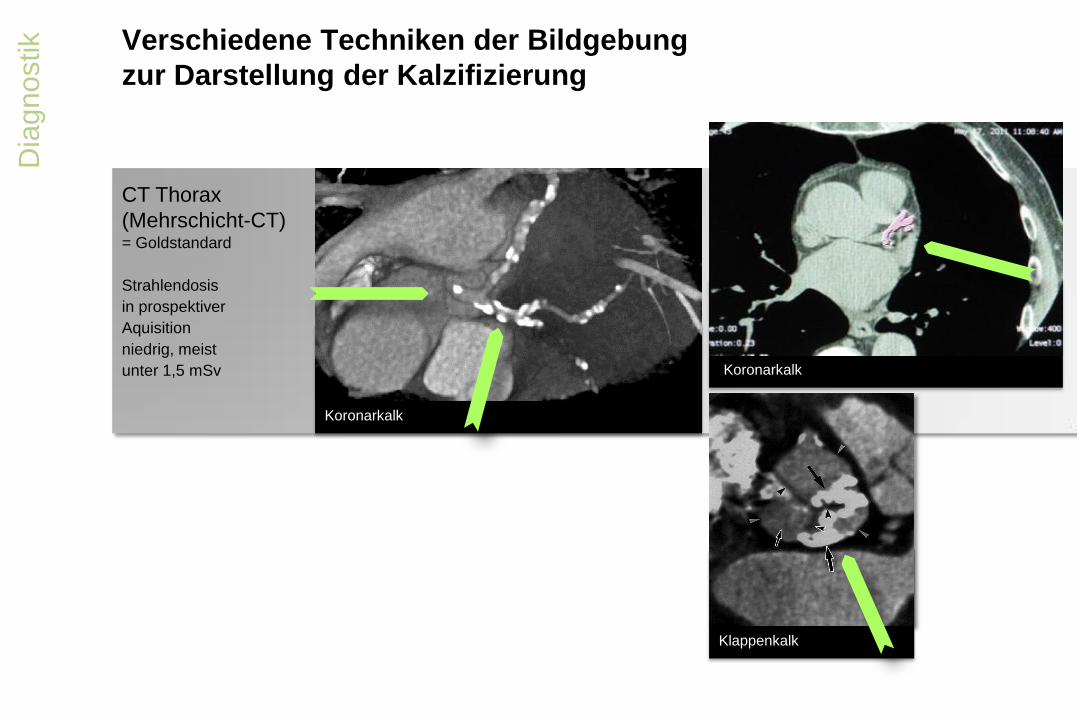
Verschiedene Techniken der Bildgebung
zur Darstellung der Kalzifizierung
Dia
gnostik
Koronarkalk
Klappenkalk
Koronarkalk
CT Thorax
(Mehrschicht-CT) = Goldstandard
Strahlendosis
in prospektiver
Aquisition
niedrig, meist
unter 1,5 mSv
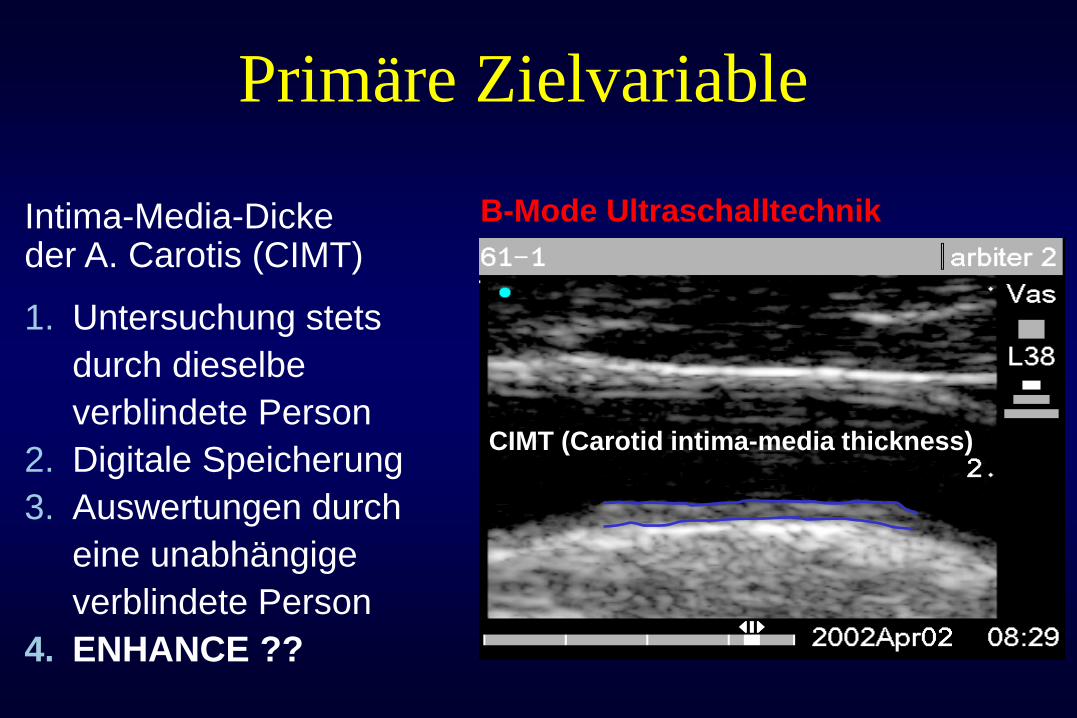
Primäre Zielvariable
Intima-Media-Dicke der A. Carotis (CIMT)
1. Untersuchung stets
durch dieselbe
verblindete Person
2. Digitale Speicherung
3. Auswertungen durch
eine unabhängige
verblindete Person
4. ENHANCE ??
B-Mode Ultraschalltechnik
CIMT (Carotid intima-media thickness)
Risk factors for Degenerative Aortic Stenosis
• Age (risk doubles every 10.years)
• Male sex (double risk)
• Smoking (35% increased risk)
• Hypertension (20% increased risk)
• Elevated Lp(a)
• Elevated LDL-cholesterol
• Height
(n = 5201 patients 65 years)
Cardiovascular Health Study, JACC 1997;29:630-634
The
rap
ie
Wann ist der richtige Zeitpunkt
für den Therapiebeginn?
1. Kidney International 2009; 76 (Suppl 113): S1–S130
Quelle*: Autoren
Diagnostik und
Therapie
ab Stadium 3 einer chron. Nieren-
insuffizienz (GFR < 60 ml/min)
Empfehlungen der Leitlinien (KDIGO1)
berücksichtigen
individuelle Umstände berücksichtigen
z.B. relevante Begleit-erkrankungen,
Risikofaktoren etc.
Therapieziele
extraossäre Kalzifikationen
verhindern
Progression verlangsamen
kardiovaskuläre Prognose
verbessern
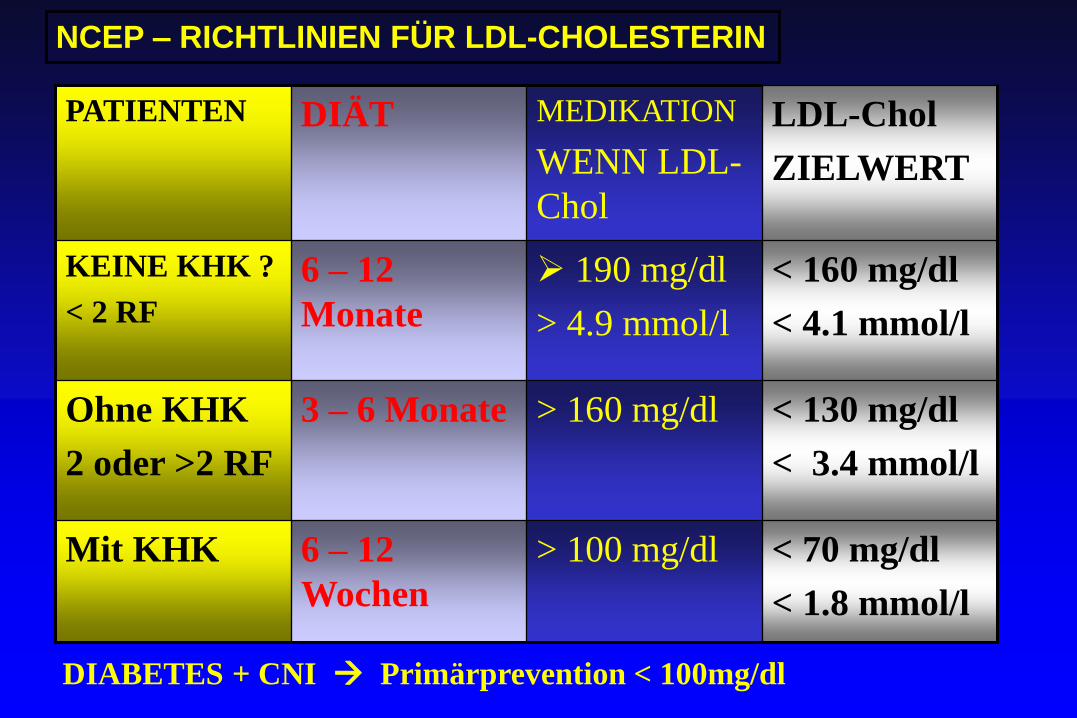
PATIENTEN DIÄT MEDIKATION
WENN LDL-
Chol
LDL-Chol
ZIELWERT
KEINE KHK ?
< 2 RF
6 – 12
Monate
190 mg/dl
> 4.9 mmol/l
< 160 mg/dl
< 4.1 mmol/l
Ohne KHK
2 oder >2 RF
3 – 6 Monate > 160 mg/dl < 130 mg/dl
< 3.4 mmol/l
Mit KHK 6 – 12
Wochen
> 100 mg/dl < 70 mg/dl
< 1.8 mmol/l
NCEP – RICHTLINIEN FÜR LDL-CHOLESTERIN
DIABETES + CNI Primärprevention < 100mg/dl
+ KHK
CHRONISCHE NIERENERKRANKUNG
KARDIOVASCULÄRE / VASCULÄRE MORTALITÄT
• GFR > 50ml/min Proteinurie <
2g/24h
• Hypertonie > 2 Mio
• LV_Hypertrophie
• 800.000 met.Sy
• Diabetes mellitus Typ 2
• GFR < 50ml/min Proteinurie > 2g/24h
• FSTW-Störung
• Anämie
• Hypertonie
• GFR< 30ml/min
• Ca-Phos
• GFR< 20 ml/min
• Katabolismus, Azidose
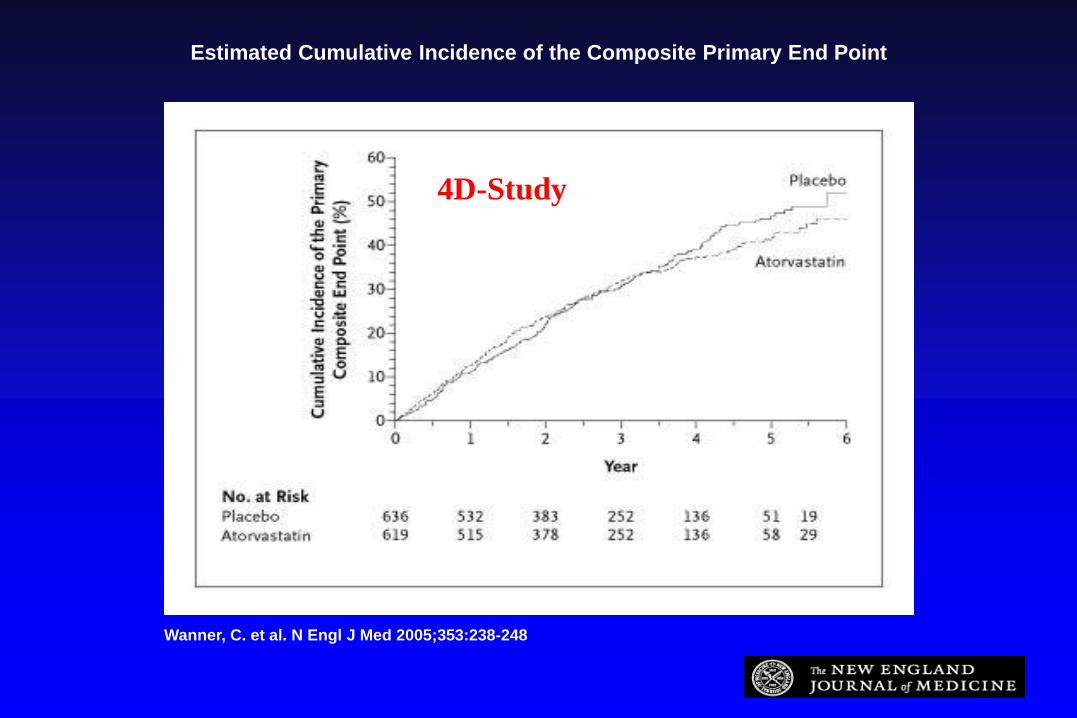
Estimated Cumulative Incidence of the Composite Primary End Point
Wanner, C. et al. N Engl J Med 2005;353:238-248
4D-Study
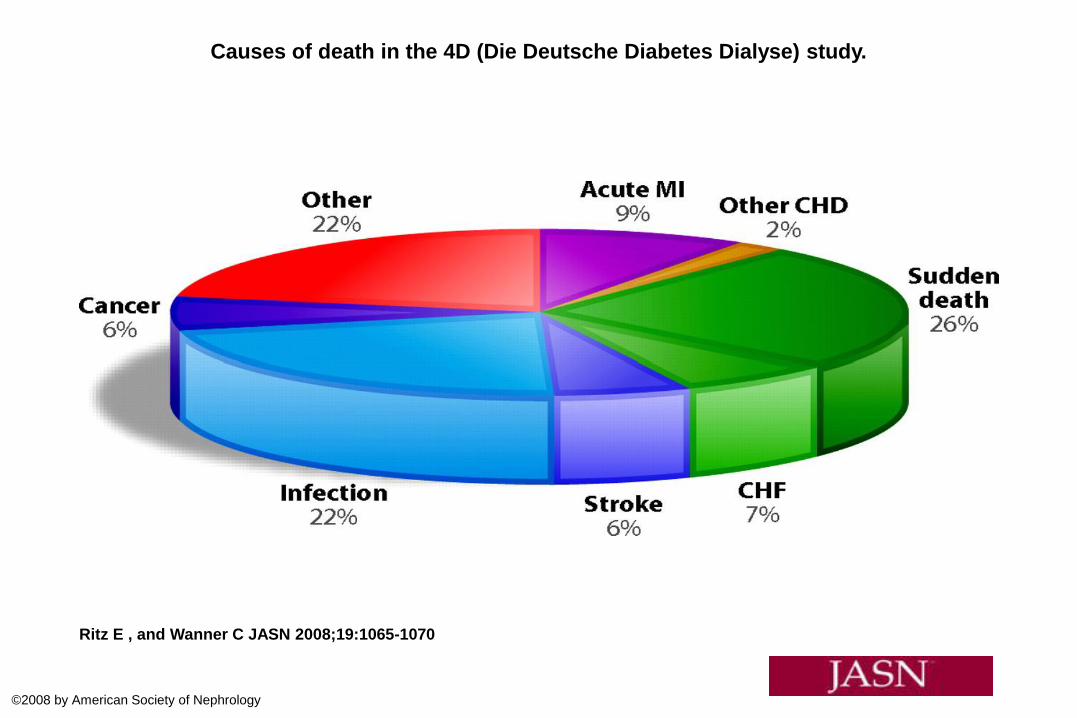
Causes of death in the 4D (Die Deutsche Diabetes Dialyse) study.
Ritz E , and Wanner C JASN 2008;19:1065-1070
©2008 by American Society of Nephrology
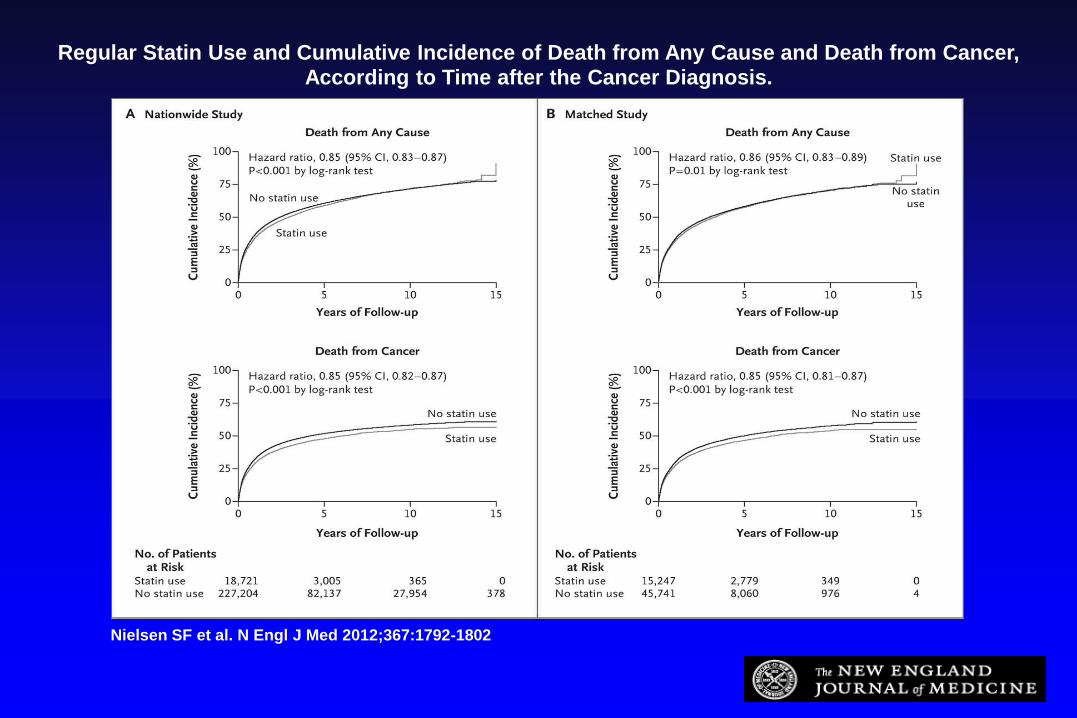
Regular Statin Use and Cumulative Incidence of Death from Any Cause and Death from Cancer, According to Time after the Cancer Diagnosis.
Nielsen SF et al. N Engl J Med 2012;367:1792-1802
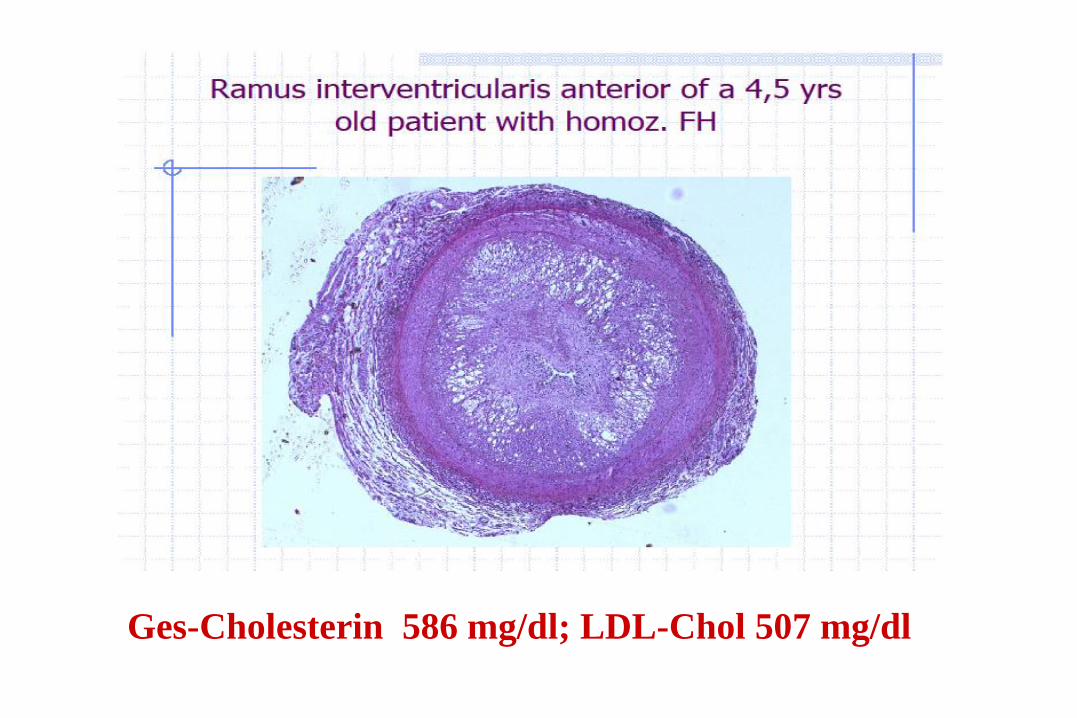
Ges-Cholesterin 586 mg/dl; LDL-Chol 507 mg/dl
IL-8, ng/ml
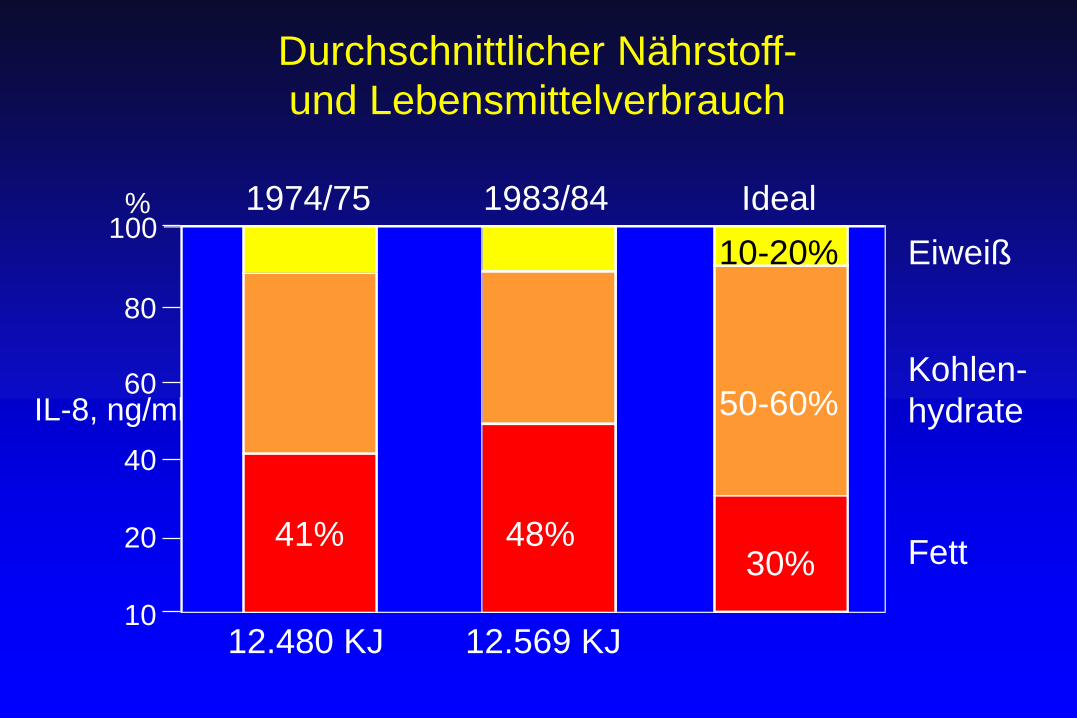
Durchschnittlicher Nährstoff-
und Lebensmittelverbrauch
41% 48% 30% Fett
50-60% Kohlen-
hydrate
Eiweiß 10-20%
12.480 KJ 12.569 KJ
1974/75
80
60
40
20
10
100 % 1983/84 Ideal
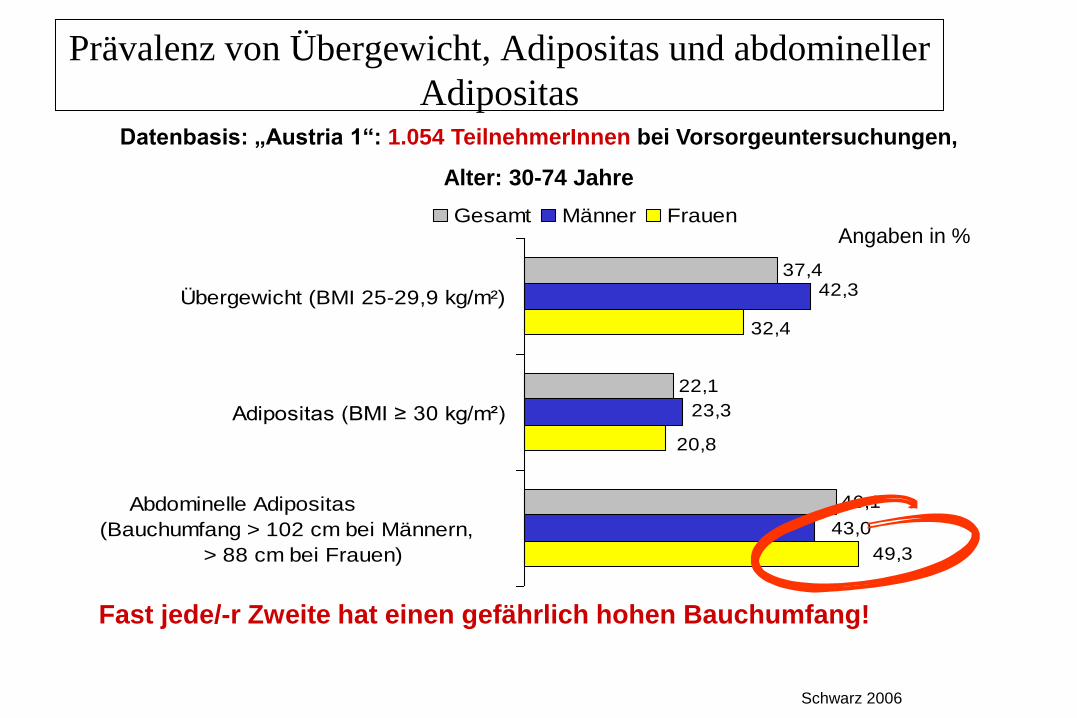
Prävalenz von Übergewicht, Adipositas und abdomineller
Adipositas
Schwarz 2006
37,4
22,1
46,1
42,3
23,3
43,0
49,3
20,8
32,4
Übergewicht (BMI 25-29,9 kg/m²)
Adipositas (BMI ≥ 30 kg/m²)
Abdominelle Adipositas
(Bauchumfang > 102 cm bei Männern,
> 88 cm bei Frauen)
Gesamt Männer FrauenAngaben in %
Datenbasis: „Austria 1“: 1.054 TeilnehmerInnen bei Vorsorgeuntersuchungen,
Alter: 30-74 Jahre
Fast jede/-r Zweite hat einen gefährlich hohen Bauchumfang!
IL-8, ng/ml
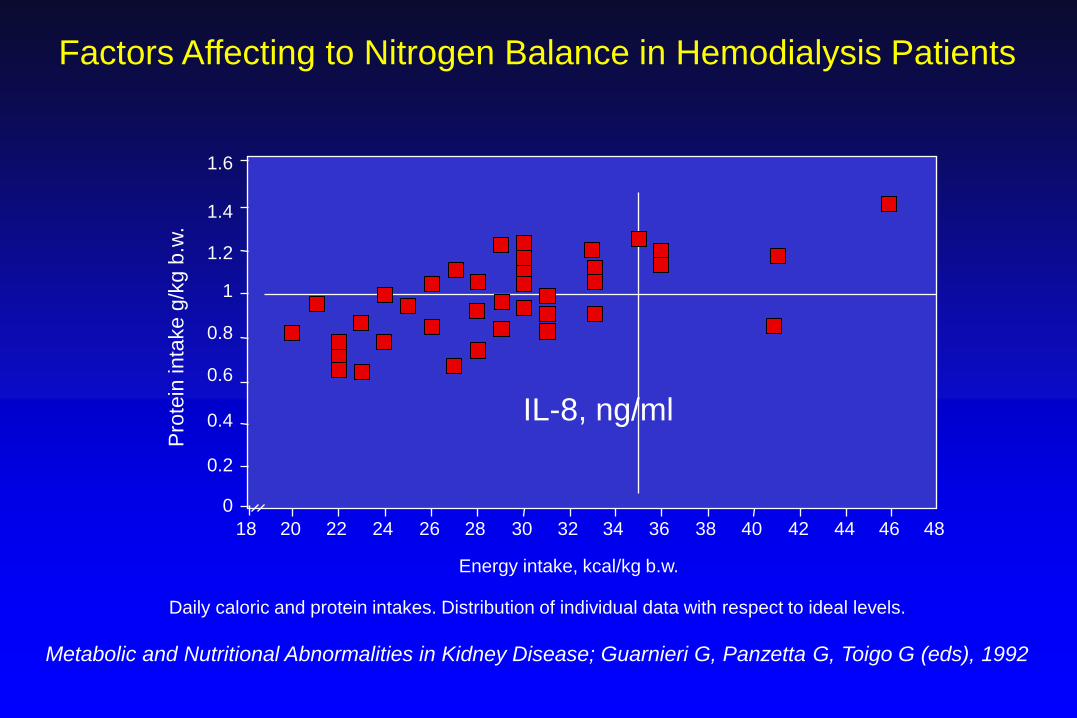
Factors Affecting to Nitrogen Balance in Hemodialysis Patients
Pro
tein
inta
ke g
/kg b
.w.
1.6
1.4
1.2
1
0.8
0.6
0.4
0.2
18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48
Energy intake, kcal/kg b.w.
Daily caloric and protein intakes. Distribution of individual data with respect to ideal levels.
Metabolic and Nutritional Abnormalities in Kidney Disease; Guarnieri G, Panzetta G, Toigo G (eds), 1992
0
15 g gesättigtes Fett/ Tag
Trichopoulou A, Katsouyanni K, Gnardellis Ch (1993).
The traditional Greek diet. Eur J Clin Nutr 47(suppl.
1):S76-S81.
(c) 2003: AG-Fettkrankheit: H. Kritz, H. Sinzinger
IL-8, ng/ml
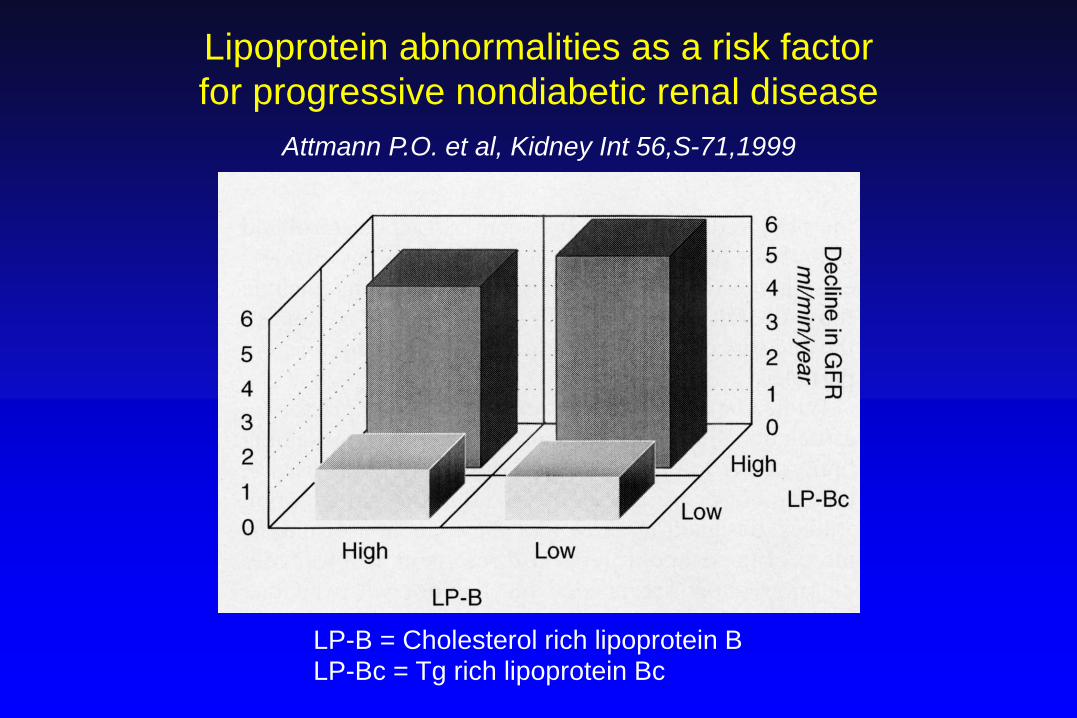
Lipoprotein abnormalities as a risk factor
for progressive nondiabetic renal disease
Attmann P.O. et al, Kidney Int 56,S-71,1999
LP-B = Cholesterol rich lipoprotein B
LP-Bc = Tg rich lipoprotein Bc
IL-8, ng/ml
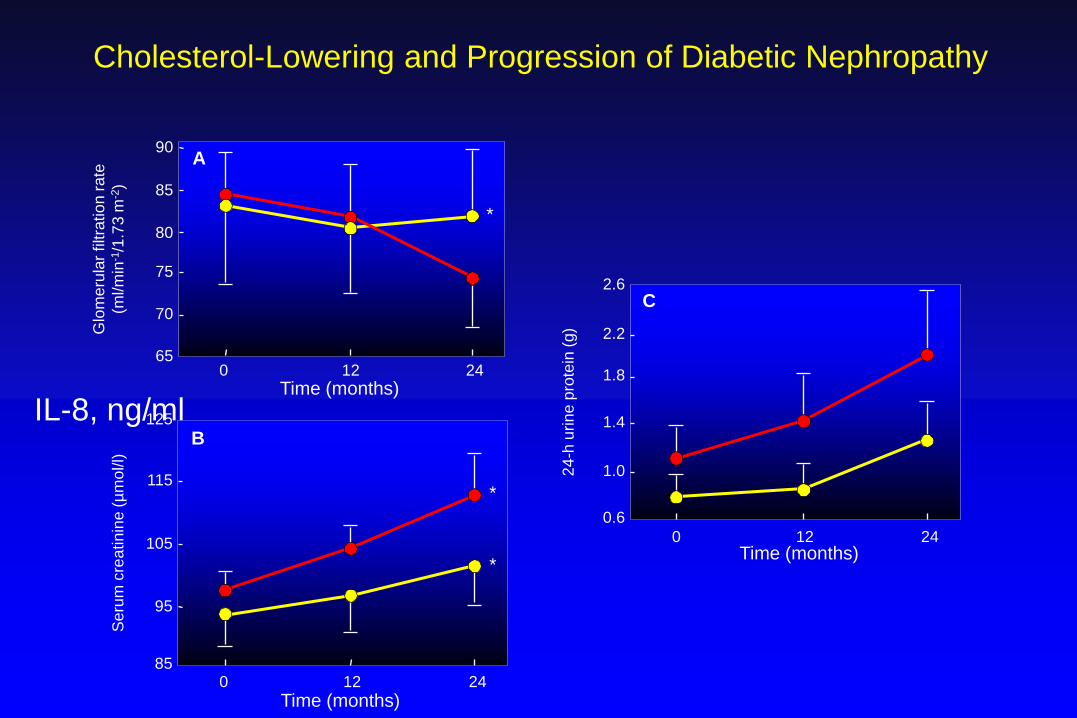
Time (months)
2.6
2.2
1.8
1.4
1.0
0.6
0 12 24
24
-h u
rin
e p
rote
in (
g)
Cholesterol-Lowering and Progression of Diabetic Nephropathy
*
*
125
115
105
95
85 0 12 24
Se
rum
cre
atin
ine (
µm
ol/l)
Time (months)
90
*
85
80
75
70
65 0 12 24
Glo
me
rula
r filtra
tion
rate
(ml/m
in-1
/1.7
3 m
-2)
Time (months)
C
B
A
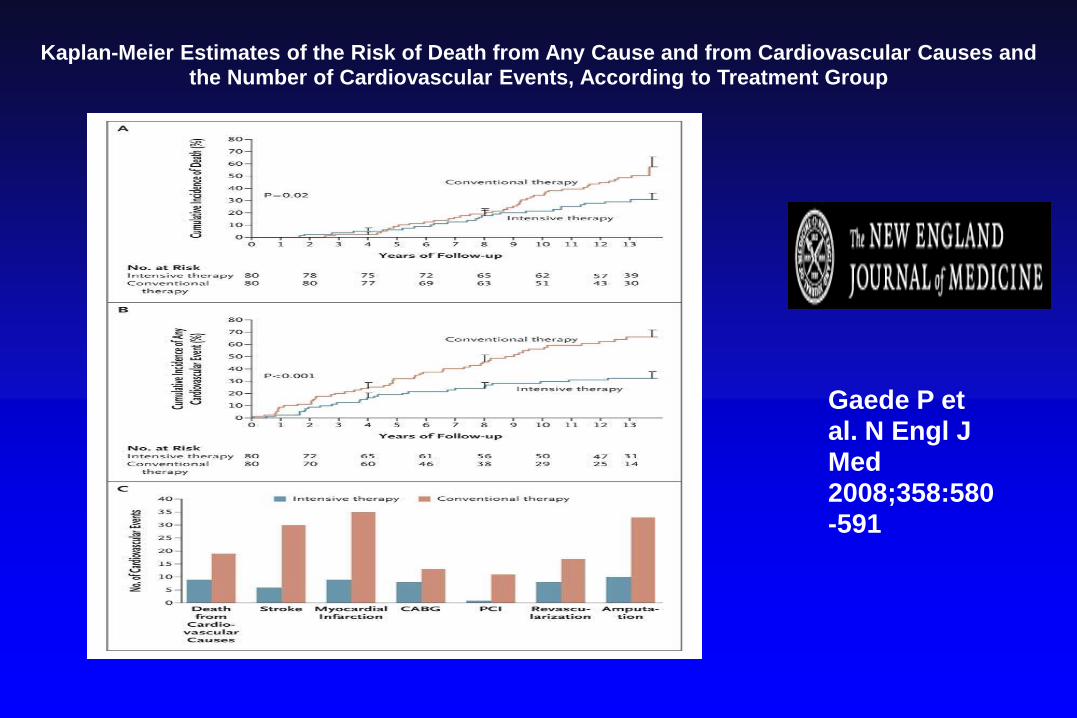
Kaplan-Meier Estimates of the Risk of Death from Any Cause and from Cardiovascular Causes and the Number of Cardiovascular Events, According to Treatment Group
Gaede P et al. N Engl J Med 2008;358:580-591
N = 10.001
3107 CKD
Stage 3= 30-59 ml/min
N= 3078
Stage 4=GFR 15-
29ml/minm
N=29
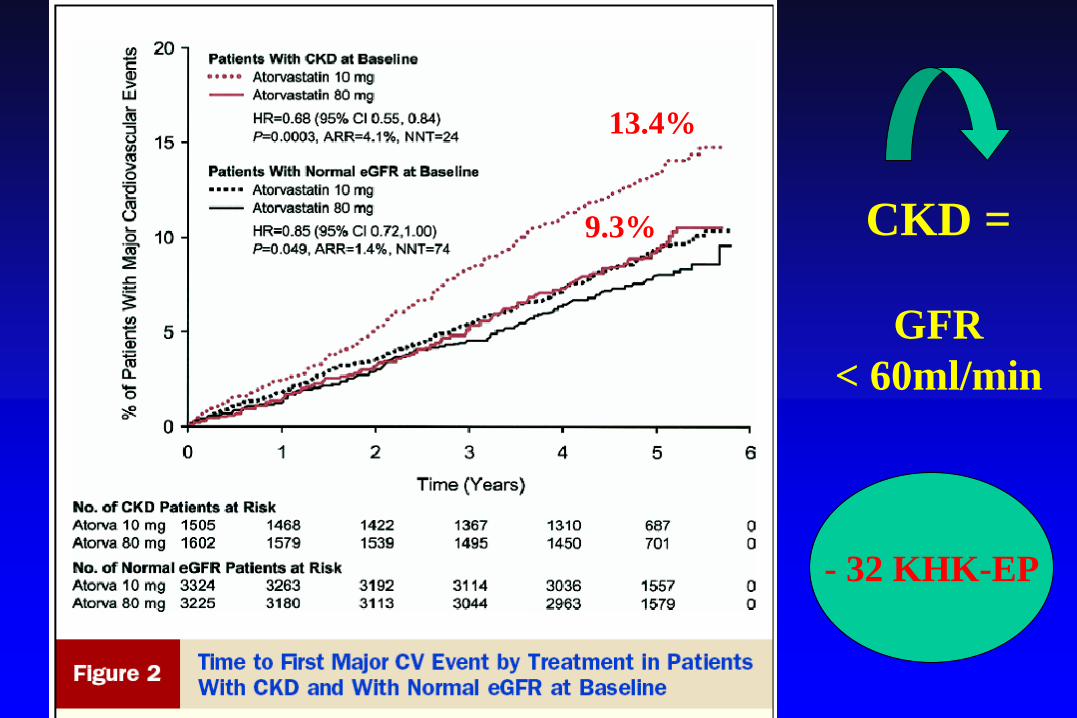
CKD =
GFR
< 60ml/min
- 32 KHK-EP
13.4%
9.3%
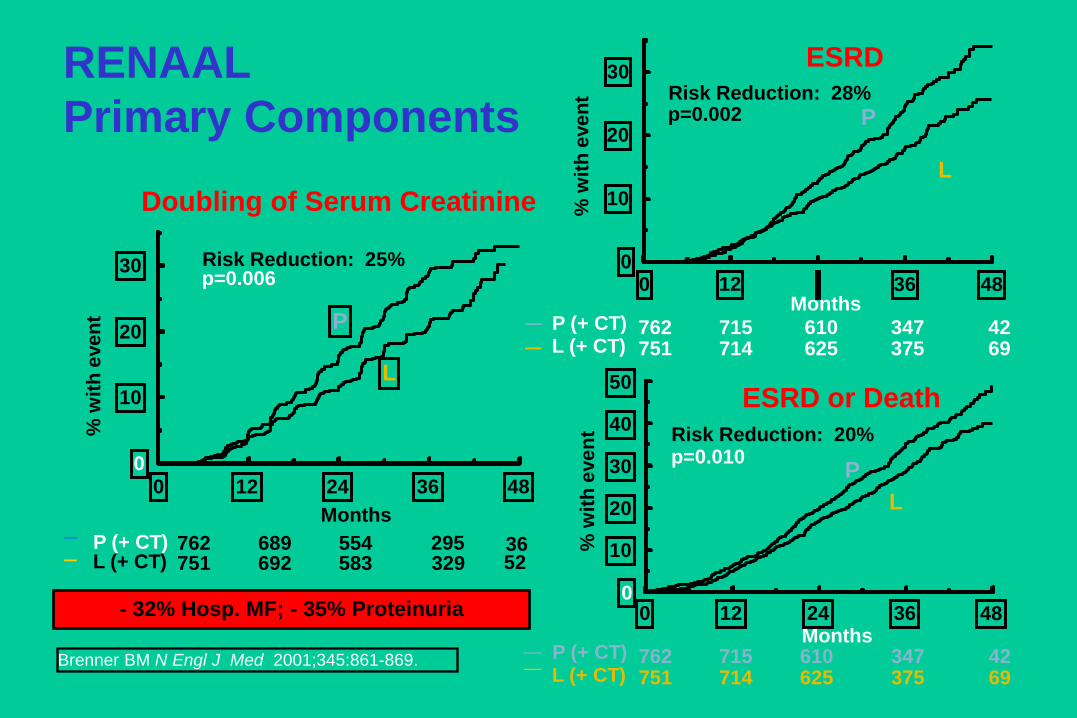
RENAAL
Primary Components
ESRD
Months
% w
ith
eve
nt
0 12 36 48 0
10
20
30
p=0.002 Risk Reduction: 28%
P
L
ESRD or Death
P (+ CT) L (+ CT)
Months
% w
ith
eve
nt
0 12 24 36 48 0
10
20
30
40
50
751 714 625 375 69 762 715 610 347 42
P
L
p=0.010 Risk Reduction: 20%
Doubling of Serum Creatinine
Months
% w
ith
eve
nt
p=0.006 Risk Reduction: 25%
751 692 583 329 52 762 689 554 295 36 P (+ CT)
L (+ CT)
0 12 24 36 48 0
10
20
30
P
L
P (+ CT) L (+ CT) 751 714 625 375 69
762 715 610 347 42
Brenner BM N Engl J Med 2001;345:861-869.
- 32% Hosp. MF; - 35% Proteinuria

THERAPIEOPTIONEN-STATINE
chron. NIERENERKRANKUNG ?
FRÜHZEITIG – GFR > 50 ml/min
PROTEINURIE
Save + EFFEKTIV– aber KONTROLLEN –
Labor / THERAPIERICHTLINIEN
Cave Medikamenten Kombi !!
D a n k e !!