Embed Size (px)
Citation preview

Deep Neural Networks for the Assessment of Surgical Skills: A Systematic
Review
Erim Yanik1, Xavier Intes2, Uwe Kruger2, Pingkun Yan2, David Diller3, Brian Van Voorst3,
Basiel Makled4, Jack Norfleet4, Suvranu De1
1Department of Mechanical, Aerospace, and Nuclear Engineering, Rensselaer Polytechnic
Institute, USA
2 Department of Biomedical Engineering, Rensselaer Polytechnic Institute, USA
3Raytheon BBN Technologies, USA
4Simulation and Training Technology Center, Army Research Laboratory, USA
One Sentence Summary
This paper provides a comprehensive review of the current state of the literature on automated
surgical skill assessment based on deep neural networks (DNN).
Abstract
Surgical training in medical school residency programs has followed the apprenticeship model.
The learning and assessment process is inherently subjective and time-consuming. Thus, there is
a need for objective methods to assess surgical skills. Here, we use the Preferred Reporting Items
for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to systematically survey the
literature on the use of Deep Neural Networks for automated and objective surgical skill
assessment, with a focus on kinematic data as putative markers of surgical competency. There is
considerable recent interest in deep neural networks (DNN) due to the availability of powerful
algorithms, multiple datasets, some of which are publicly available, as well as efficient
computational hardware to train and host them. We have reviewed 530 papers, of which we
selected 25 for this systematic review. Based on this review, we concluded that DNNs are powerful
tools for automated, objective surgical skill assessment using both kinematic and video data. The
field would benefit from large, publicly available, annotated datasets that are representative of the
surgical trainee and expert demographics and multimodal data beyond kinematics and videos.
Keywords
Deep learning, deep neural network, artificial intelligence, convolutional neural network, LSTM,
GRU, RNN, surgical skill assessment, laparoscopic surgery, robotic surgery, virtual surgical
simulators.

1. Introduction
Surgical procedures require high dexterity, fine motor control, and hand-eye coordination. Surgical
training has followed the Halstedian apprenticeship model of learning with an expert in the
operating room (OR).1,2 Traditional surgical assessment methods, such as direct observations by
an experienced trainer to assess the skills of the trainee, are generally subjective and use global
rating scales (GRS), e.g., the Objective Structure Assessment of Technical Skills (OSATS), to
score competency.3 These observational methods allow experienced surgeons to use structured
checklists for technical criteria and rate the surgical performance of the trainee under direct
observation. Surgical training programs also utilize other checklist-based approaches, e.g., In-
Training Evaluation Reports (ITERs), to evaluate trainees. These approaches suffer from the well-
known limitations of being subjective with poor inter-rater reliability, distribution errors, recall
bias, and halo effects.4-6
Increasingly, simulators are being used to provide an efficient training environment outside the
OR and certify surgeons, eliminating risks to human patients. Notably, the Fundamentals of
Laparoscopic Surgery (FLS) program, developed by a joint committee of the American
Gastrointestinal and Endoscopic Surgeons (SAGES) and the American College of Surgeons
(ACS), is a pre-requisite for board certification in general and ob/GYN surgery.7,8 The
Fundamentals of Endoscopic Surgery (FES) utilizes a virtual reality-based simulator and is
required for general surgery board certification.9 Moreover, a more recent curriculum, namely,
Fundamentals of Robotic Surgery (FRS) offers standardization to assess surgeons in robotic
surgery.10 Simulators such as these use metrics based on time and error to provide performance
scores to certify surgeons. The definition of error in these simulators is subjective and may not
correlate with operative errors. The evaluation of these errors, e.g., calculating the deviation of a
cut-trajectory from a pre-marked circle in the pattern cutting task of the FLS is also manually
intensive and subjective. Also, time to completion is heavily weighted, with no evidence that
completing a task faster is indicative of surgical proficiency.
There is currently an intense focus on developing data-driven techniques to overcome the
limitations of surgical skill assessment. Two of the major categories of data that are collected for
skills assessment include kinematic and video-based data. Kinematic data is collected by placing
sensors at tooltips, hand, or on other locations of the body of the trainee to collect motion-related
data. 12-16 Data for features such as location, velocity, and rotation of a surgical tool can be
collected directly using these sensors. This type of data collection is invasive due to the presence
of the sensor that might interfere with the motion of the trainees. The kinematic data can also be
collected virtually using software such as EndoVis for virtual training applications, which does
not suffer from the limitations of physical sensors.17 Unlike kinematic data, video-based data is
gathered in a non-invasive manner and is easier to work with. However, video-based data requires
extensive post-processing to extract meaningful information. Crowdsourcing has been proposed
as a method to leverage the wisdom of the crowd and reduce the need for time-intensive work by
medical professionals for scoring surgical videos.18
Automated data processing is a pre-requisite to automating skill assessment. Earlier works derive
statistical representations from the collected data to represent surgical performance.19-21 Anh et
al.22 used the mean, min-max-standard deviation (SD) of each sequence together with more
complex representations, e.g., the average absolute difference, the average root sum of squared
level, the average root square difference, and binned distribution to represent the kinematic tool
motion data collected for elementary surgical tasks performed using surgical robots.13 With the
statistical features of choice, they were able to differentiate experts from novices with accuracies
between 87.25% and 95.42%. Moreover, Kim et al.23 employed crowd-sourced tool tip velocities
(TTV), and optical flow fields (OFF) to represent tool motion during capsulorhexis and were able
to differentiate between experts and novices with accuracies of 84.8% and 63.4% for TTV and
OFF, respectively.
Although statistical representations prove useful in specific scenarios, manual extraction of the
features, needed for domain knowledge, and time-effectiveness are critical limitations. Machine
learning (ML) techniques, including hidden Markov models (HMM), support vector machines
(SVM), and bag of words (BoW) are data-driven models, extensively used for surgical skill
assessment.25-28 In a hybrid study, Fard et al.29 extracted statistical features, including duration,
path length, and smoothness, from the kinematic tool motion data provided by the DaVinci surgical
robot (dVSS). The features were selected to represent the surgeon’s dexterity based on tool motion.
Logistic regression (LR) and support vector machine (SVM) were applied for binary classification
of eight surgeons performing suturing, and a global rating score was utilized to annotate the
surgeon’s performance. As a result, a maximum of 85.7% overall accuracy was reported using LR
with leave-one-super-trial-out (LOSO) cross-validation (CV). In another study conducted by Zia
et al.31, various ML techniques were compared, including HMM, BoW, Motion Textures, and
Discrete Cosine Transform (DCT), which performs well with repetitive tasks. They collected
video-based data on suturing and knot-tying and used OSATS to establish ground-truth for the
performance. As a result, they showed the benefit of using frequency domain-based techniques,
i.e., DCT, over the techniques mentioned above for repetitive tasks.
While ML techniques are promising, they rely on manual features that are task-specific and require
significant effort to define and optimize. Also, neither statistical features nor ML techniques are
end-to-end, i.e., they need multiple steps to produce the desired output, e.g., extracting information
from the collected data, computing features, and then using the ML model or an equation to assess
performance. Deep learning (DL), is rapidly emerging as a method of choice to overcome these
limitations of ML approaches.32 DL is a powerful supervised learning technique that consists of
hidden layers with neurons within. The neurons extract and represent complex features, and the
complexity can be enhanced by adding more layers and neurons. The utility of DL is used to
identify surgical tools in every frame of surgical videos, automatically, based on the
extractedfeatures that are otherwise non-detectible to human eye.
The availability of powerful algorithms, large labeled datasets, and inexpensive high-power
computing is fueling the growth in DL-based approaches in surgical assessment33,34. In recent
years complex recurrent neural networks (RNNs) such as Long Short Term Memory (LSTM),
Gated Recurring Unit (GRU), and their combinations with convolutional neural networks (CNN)
have been utilized for surgical skill assessment.35,36 CNN’s were also used to assess skills and
generate meaningful feedback to the trainee.37-40 Moreover, CNNs such as Hourglass Network,
Faster Region-Based CNN (Faster RCNN), and Temporal Segment Networks (TSN), and others
were used to extract tool locations from surgical videos.41-45
In this paper, we systematically analyzed automated and objective surgical skill assessment
techniques based on deep neural networks (DNN) using the Preferred Reporting Items for
Systematic Reviews and Meta-Analyses (PRISMA) guidelines.46 While there are multiple review
papers that have been recently published in similar areas, they lack technical analysis on DNNs
and do not state the benefits of DNNs over traditional machine learning techniques for surgical
skill assessment, such as visual feedback or end-to-end learning.33,34
The rest of the paper is organized as follows. The review criteria are presented in Section 2. Section
3 discusses the major findings from the review, including the available datasets, deep learning
models utilized, prevalent cross-validation methods, and skill assessment techniques. Sections 4
and 5 present discussions and conclusions, respectively.
2. Review criteria
We used Google Scholar as the database and included all the published works through June 2020
in the analysis. We did not have a designated start date and the earliest work we could find in this
field belonged November 2013. Eight different keywords and fourteen different keyword
combinations were used to identify the 527 potential publications. The keywords related to surgical
skills, namely “surgical skill assessment,” “surgical skill classification,” and “surgical skill
evaluation,” were used together with deep learning terminology, including “deep learning,”
“artificial intelligence,” “deep neural networks,” LSTM,” and “convolutional neural networks”.
Each keyword combination was treated individually. Papers cited in the obtained papers were also
included in our list. We excluded 364 papers that were duplicates, and patents, books, theses, and
publications in foreign languages. The screening was done by reading the title and the abstract of
each paper. The papers that were excluded at this stage were mostly related to different applications
of surgery or were not utilizing DL techniques. We believe that these papers were included in the
repository due to the articles they cited. After the screening process, we identified 46 papers for
an extensive review. In this step, we read each paper thoroughly. We removed the papers about
tool detection & localization, workflow and action recognition, and video segmentation in surgery
using DNNs. The reason is that even though these steps are required for skill assessment, the
authors did not utilize their technology to do so. Furthermore, some studies that were eliminated
reported results by using ML techniques and claimed that DL is their next study aim. This process
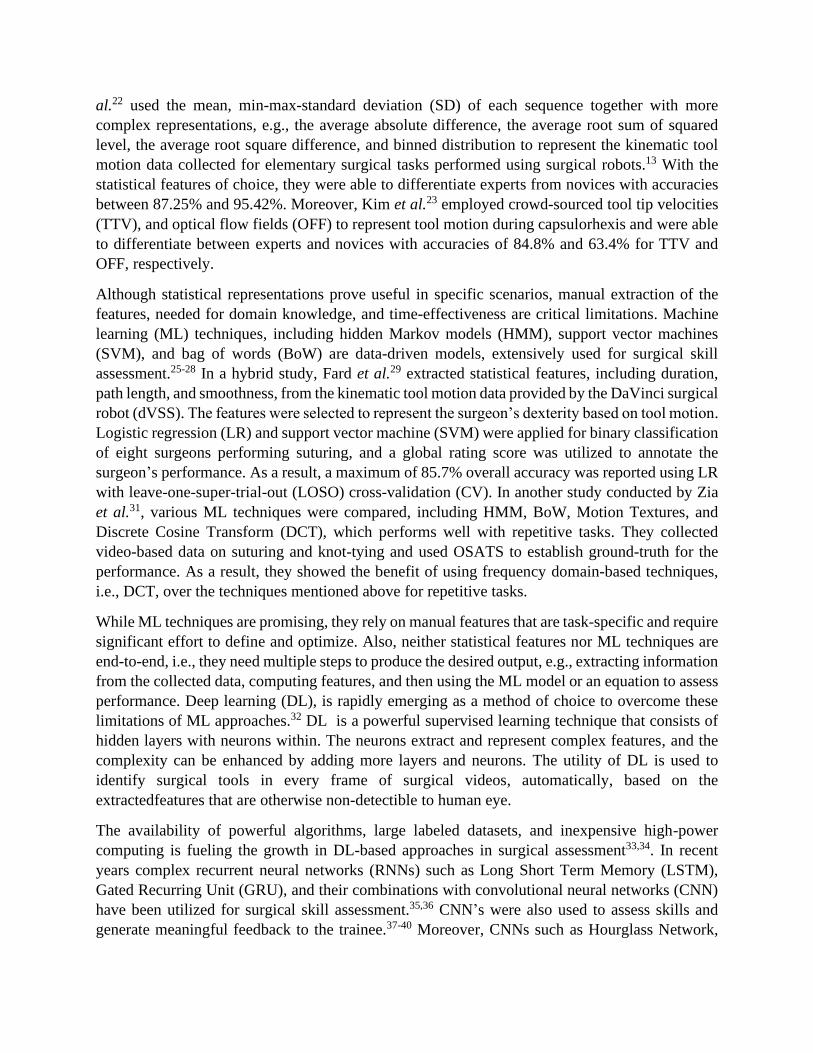
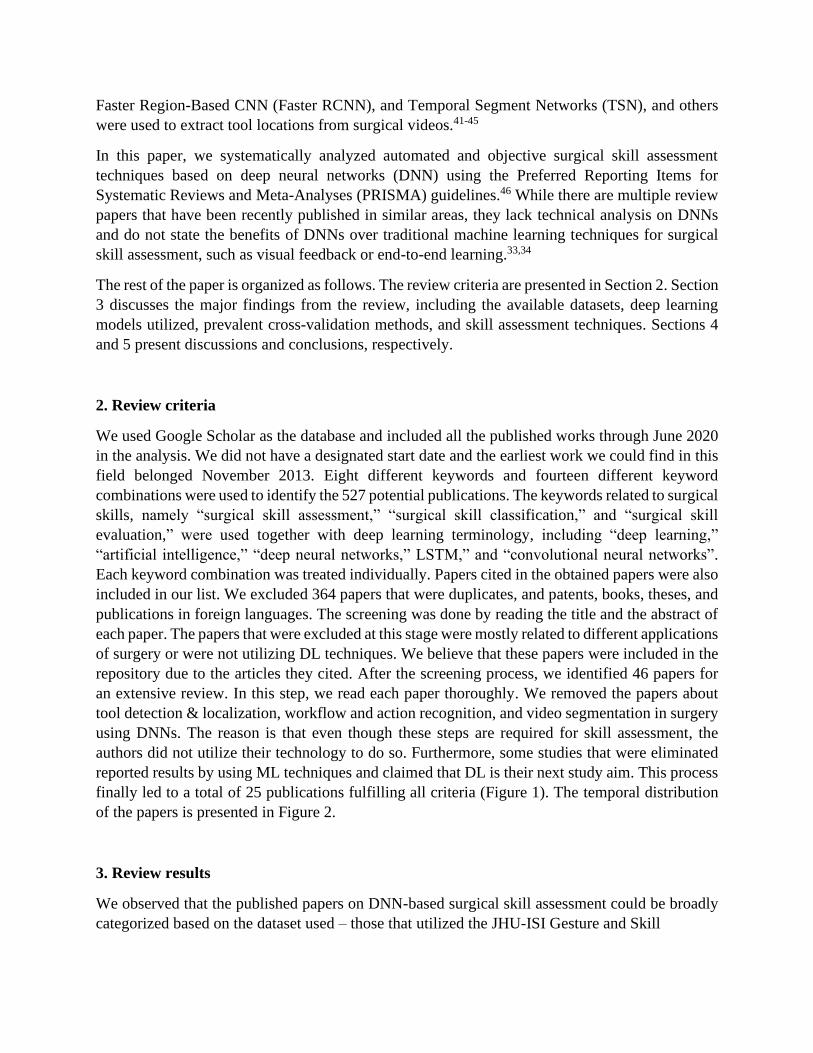
finally led to a total of 25 publications fulfilling all criteria (Figure 1). The temporal distribution
of the papers is presented in Figure 2.
3. Review results
We observed that the published papers on DNN-based surgical skill assessment could be broadly
categorized based on the dataset used – those that utilized the JHU-ISI Gesture and Skill
Figure 1. PRISMA flowchart for study selection.
Figure 2. Published papers that were chosen for this review.
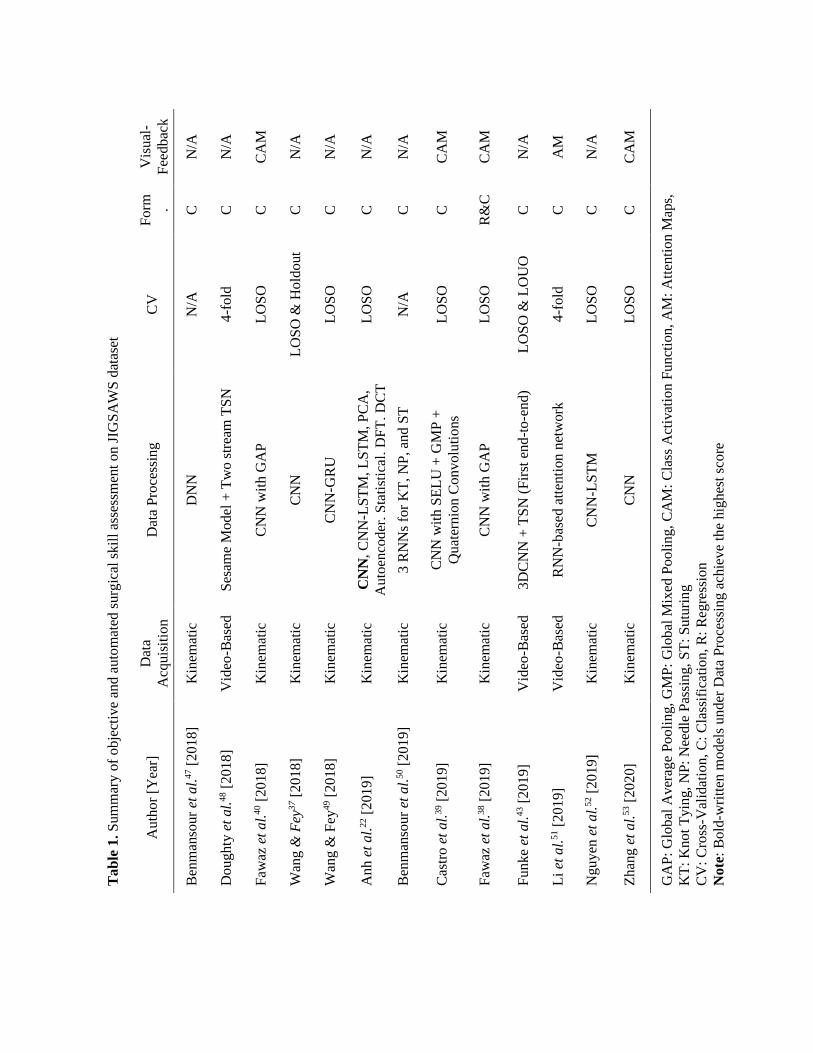
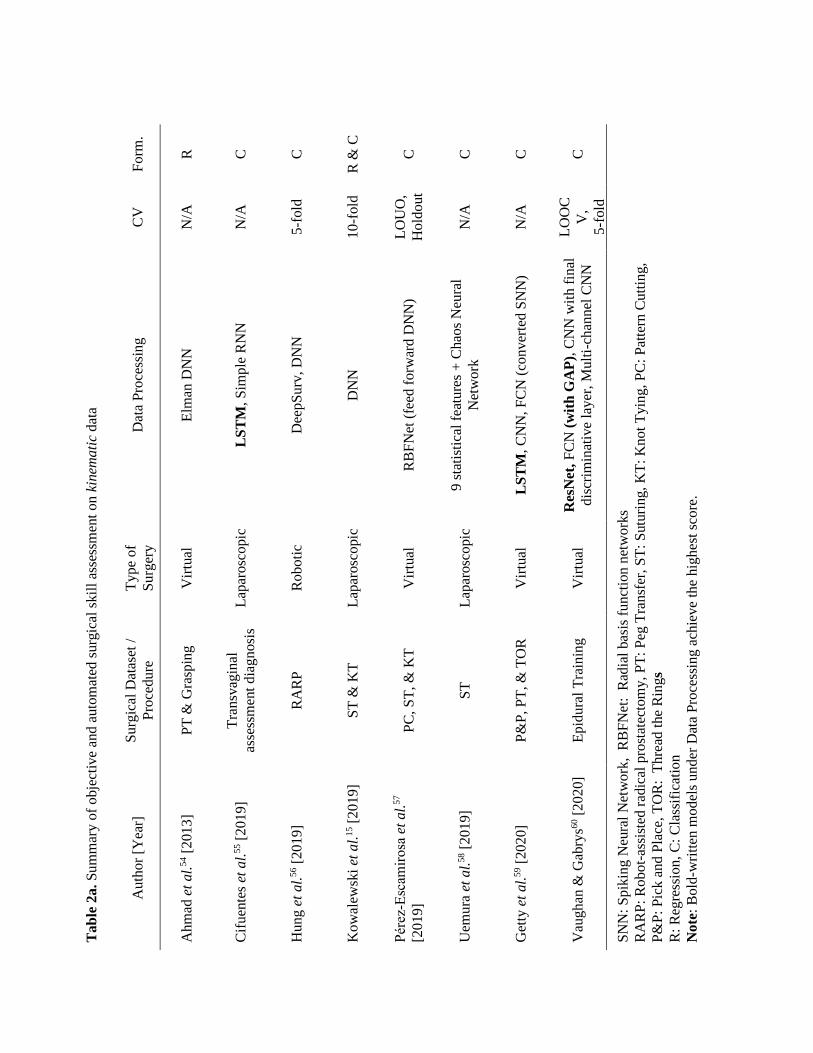
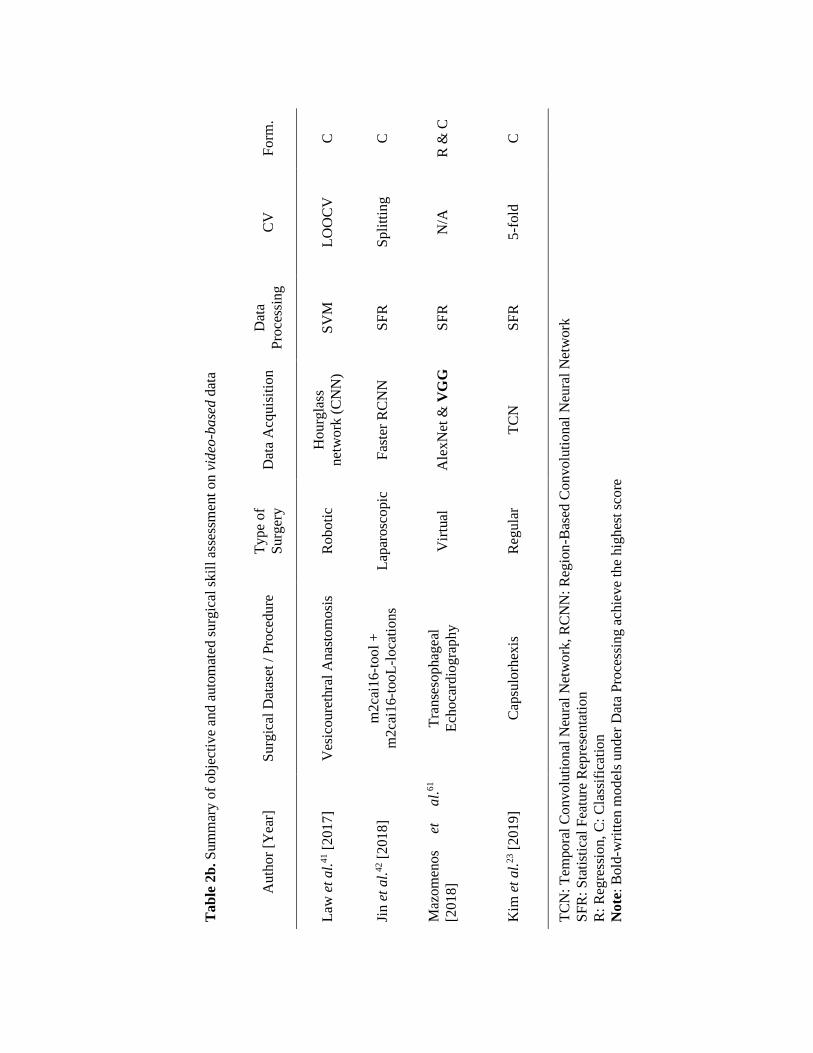
Assessment Working Set (JIGSAWS) dataset and those that used other datasets.13 The papers also
differed in the data acquisition, DNN models, cross-validation, and skill assessment techniques, as
presented below and summarized in Tables 1 and 2.
Ta
ble
1.
Sum
mar
y o
f o
bje
ctiv
e an
d a
uto
mat
ed s
urg
ical
skil
l as
sess
men
t on J
IGS
AW
S d
atas
et
Vis
ual
-
Fee
db
ack
N/A
N/A
CA
M
N/A
N/A
N/A
N/A
CA
M
CA
M
N/A
AM
N/A
CA
M
GA
P:
Glo
bal
Av
erag
e P
oo
lin
g,
GM
P:
Glo
bal
Mix
ed P
ooli
ng,
CA
M:
Cla
ss A
ctiv
atio
n F
un
ctio
n,
AM
: A
tten
tio
n M
aps,
KT
: K
no
t T
yin
g, N
P:
Nee
dle
Pas
sing,
ST
: S
utu
ring
CV
: C
ross
-Val
idat
ion
, C
: C
lass
ific
atio
n,
R:
Reg
ress
ion
No
te:
Bold
-wri
tten
mo
del
s u
nder
Dat
a P
roce
ssin
g a
chie
ve
the
hig
hes
t sc
ore
Fo
rm . C
C
C
C
C
C
C
C
R&
C
C
C
C
C
CV
N/A
4-f
old
LO
SO
LO
SO
& H
old
out
LO
SO
LO
SO
N/A
LO
SO
LO
SO
LO
SO
& L
OU
O
4-f
old
LO
SO
LO
SO
Dat
a P
roce
ssin
g
DN
N
Ses
ame
Model
+ T
wo s
trea
m T
SN
CN
N w
ith G
AP
CN
N
CN
N-G
RU
CN
N,
CN
N-L
ST
M,
LS
TM
, P
CA
,
Auto
enco
der
, S
tati
stic
al,
DF
T,
DC
T
3 R
NN
s fo
r K
T,
NP
, an
d S
T
CN
N w
ith S
EL
U +
GM
P +
Quat
ernio
n C
onvolu
tions
CN
N w
ith G
AP
3D
CN
N +
TS
N (
Fir
st e
nd
-to-e
nd)
RN
N-b
ased
att
enti
on n
etw
ork
CN
N-L
ST
M
CN
N
Dat
a
Acq
uis
itio
n
Kin
emat
ic
Vid
eo-B
ased
Kin
emat
ic
Kin
emat
ic
Kin
emat
ic
Kin
emat
ic
Kin
emat
ic
Kin
emat
ic
Kin
emat
ic
Vid
eo-B
ased
Vid
eo-B
ased
Kin
emat
ic
Kin
emat
ic
Au
tho
r [Y
ear]
Ben
man
sour
et a
l.47 [
20
18]
Do
ug
hty
et
al.
48 [
201
8]
Faw
az e
t a
l.40 [
20
18]
Wan
g &
Fey
37 [
20
18]
Wan
g &
Fey
49 [
20
18]
An
h e
t al.
22 [
201
9]
Ben
man
sour
et a
l.50 [
20
19]
Cas
tro
et
al.
39 [
20
19]
Faw
az e
t a
l.38 [
20
19]
Fu
nk
e et
al.
43 [
20
19]
Li
et a
l.51 [
20
19]
Ng
uy
en e
t a
l.52 [
20
19]
Zh
ang
et
al.
53 [
20
20]
T
ab
le 2
a.
Su
mm
ary
of
obje
ctiv
e an
d a
uto
mat
ed s
urg
ical
skil
l as
sess
men
t on k
inem
ati
c dat
a
Fo
rm.
R
C
C
R &
C
C
C
C
C
SN
N:
Spik
ing
Neu
ral
Net
wo
rk,
RB
FN
et:
Rad
ial
bas
is f
unct
ion n
etw
ork
s
RA
RP
: R
ob
ot-
assi
sted
rad
ical
pro
stat
ecto
my,
PT
: P
eg T
ransf
er,
ST
: S
utu
ring,
KT
: K
not
Tyin
g,
PC
: P
atte
rn C
utt
ing
,
P&
P:
Pic
k a
nd
Pla
ce, T
OR
: T
hre
ad t
he
Rin
gs
R:
Reg
ress
ion
, C
: C
lass
ific
atio
n
Note
: B
old
-wri
tten
mo
del
s u
nd
er D
ata
Pro
cess
ing a
chie
ve
the
hig
hes
t sc
ore
.
CV
N/A
N/A
5-f
old
10-f
old
LO
UO
,
Ho
ldo
ut
N/A
N/A
LO
OC
V,
5-f
old
Dat
a P
roce
ssin
g
Elm
an D
NN
LS
TM
, S
imp
le R
NN
Dee
pS
urv
, D
NN
DN
N
RB
FN
et (
feed
forw
ard
DN
N)
9 s
tati
stic
al f
eatu
res
+ C
hao
s N
eura
l
Net
work
LS
TM
, C
NN
, F
CN
(co
nv
erte
d S
NN
)
Res
Net
, F
CN
(w
ith
GA
P),
CN
N w
ith
fin
al
dis
crim
inat
ive
layer
, M
ult
i-ch
ann
el C
NN
Type
of
Surg
ery
Vir
tual
Lap
arosc
opic
Roboti
c
Lap
arosc
opic
Vir
tual
Lap
arosc
opic
Vir
tual
Vir
tual
Su
rgic
al D
atas
et /
Pro
cedure
PT
& G
rasp
ing
Tra
nsv
agin
al
asse
ssm
ent
dia
gnosi
s
RA
RP
ST
& K
T
PC
, S
T,
& K
T
ST
P&
P,
PT
, &
TO
R
Ep
idura
l T
rain
ing
Au
tho
r [Y
ear]
Ahm
ad e
t al.
54 [
201
3]
Cif
uen
tes
et a
l.55 [
20
19]
Hung e
t al.
56 [
20
19
]
Kow
alew
ski
et a
l.15 [
20
19]
Pér
ez‑E
scam
iro
sa e
t al.
57
[2019]
Uem
ura
et
al.
58 [
20
19]
Get
ty e
t al.
59 [
20
20
]
Vau
ghan
& G
abry
s60 [
20
20]
Tab
le 2
b. S
um
mar
y o
f o
bje
ctiv
e an
d a
uto
mat
ed s
urg
ical
skil
l as
sess
men
t on v
ideo
-base
d d
ata
Fo
rm.
C
C
R &
C
C
TC
N:
Tem
po
ral
Co
nv
olu
tio
nal
Neu
ral
Net
work
, R
CN
N:
Reg
ion
-Bas
ed C
onvolu
tional
Neu
ral
Net
work
SF
R:
Sta
tist
ical
Fea
ture
Rep
rese
nta
tion
R:
Reg
ress
ion
, C
: C
lass
ific
atio
n
Note
: B
old
-wri
tten
mo
del
s u
nd
er D
ata
Pro
cess
ing a
chie
ve
the
hig
hes
t sc
ore
CV
LO
OC
V
Sp
litt
ing
N/A
5-f
old
Dat
a
Pro
cess
ing
SV
M
SF
R
SF
R
SF
R
Dat
a A
cquis
itio
n
Hourg
lass
net
work
(C
NN
)
Fas
ter
RC
NN
Ale
xN
et &
VG
G
TC
N
Type
of
Surg
ery
Roboti
c
Lap
arosc
opic
Vir
tual
Reg
ula
r
Su
rgic
al D
atas
et /
Pro
cedure
Ves
icou
reth
ral
Anas
tom
osi
s
m2ca
i16-t
ool
+
m2
cai1
6-t
ooL
-loca
tions
Tra
nse
sophag
eal
Ech
oca
rdio
gra
phy
Cap
sulo
rhex
is
Au
tho
r [Y
ear]
Law
et
al.
41 [
201
7]
Jin e
t al.
42 [
201
8]
Maz
om
eno
s et
a
l.61
[2018]
Kim
et
al.
23 [
201
9]
3.1. Datasets
The availability of relatively large datasets, including publicly available ones, has spurred
significant growth of DNL-based techniques. Both kinematic and video-based data were collected
and utilized in these datasets. The kinematic data was gathered using sensors, simulators, and/or
surgical robots, whereas the video-based data were obtained either using virtual simulators or
cameras. For instance, JIGSAWS is a publicly available dataset that is used in multiple studies.13
It is a robotic surgery dataset containing data from three elementary tasks performed using the da
Vinci surgical system (dVSS), including suturing, needle passing, and knot-tying. Suturing is done
by passing a needle through a synthetic tissue. Needle passing, like suturing, is where a needle is
passed through metal hoops from one side to the other. Knot-tying is when the subject ties a single
loop knot using the ends of the suture. There are 39 suturing, 36 knot-tying, and 28 needle passing
trials conducted by 8 subjects, which includes two experts with 100+ hours of experience, four
novices with less than 10 hours of experience, and two intermediates with between 10 and 100
hours of experience. Here, the hours of expertise are self-proclaimed and expert and intermediate
subjects are underrepresented in comparison to novices. In addition, each trial is annotated using
a modified version of OSATS. The dataset includes a total of 76 variables representing kinematic
data associated with tooltip positions in Cartesian coordinates, tooltip rotation matrix, tip linear
and rotational velocities, and gripper angle velocity for four robotic arms, including two master
and two patient side manipulators. The kinematic data has been collected by dVSS along with
video-based data recorded by endoscopic cameras at 30 FPS at a resolution of 640 x 480. The
dataset has gesture-based verbal annotations yet does not possess spatial annotation for the tools
used during the tasks.
Another publicly available dataset is Cholec80, which consists of 80 videos of laparoscopic
cholecystectomy performed by 13 experts and captured at 25 FPS.44 The binary tool presence
annotation was provided at 1 FPS rate, offering a suitable environment to study DNN for tool
detection.62 In addition, mc2cai16-tool and mc2ai16-workflow are other datasets constructed
based on Cholec80 for the 2016 M2CAI Challenge.44,63 Mc2cai16-tool was later expanded by Jin
et al.42, who introduced spatial annotation for the tools so that the dataset would be suitable for
tracking tool motion and the technical assessment of surgical skills. They were also the first ones
to use the dataset. Their results matched with OSATS classification for four experts. Other than
public datasets, studies reported assessment on private datasets collected using the dVSS,
simulators, sensors, and cameras.54-56,58,60
Following our analysis, we found 5 studies out of 25 that acquired data virtually using simulators.
In addition, 15 papers, including the JIGSAWS studies, were robotic, and four were of
laparoscopic surgery. One paper studied Capsulorhexis hence, labeled as general surgery. Based
on works besides JIGSAWS, we found that half of the papers utilizing kinematic data acquire it
virtually. In contrast, only a quarter of the papers obtained data from virtual simulations for video-
based studies. Additionally, our survey showed that only tool motion (23 studies) and hand motion
(2 studies) were utilized. We could not find papers employing other methods, including eye motion
tracking and muscle contractions used in earlier ML techniques.64 Between tool and hand motion,
tool motion was favored as 92% of the papers are based on tracking tool motion to assess skills.
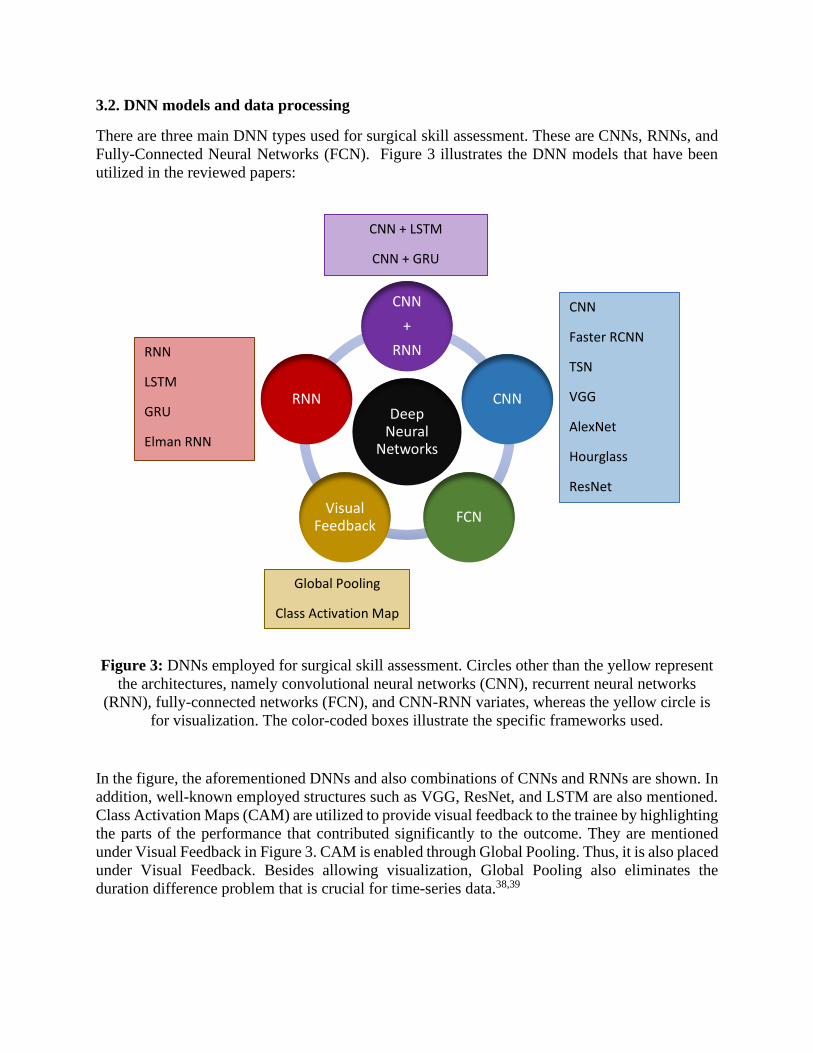
3.2. DNN models and data processing
There are three main DNN types used for surgical skill assessment. These are CNNs, RNNs, and
Fully-Connected Neural Networks (FCN). Figure 3 illustrates the DNN models that have been
utilized in the reviewed papers:
Figure 3: DNNs employed for surgical skill assessment. Circles other than the yellow represent
the architectures, namely convolutional neural networks (CNN), recurrent neural networks
(RNN), fully-connected networks (FCN), and CNN-RNN variates, whereas the yellow circle is
for visualization. The color-coded boxes illustrate the specific frameworks used.
In the figure, the aforementioned DNNs and also combinations of CNNs and RNNs are shown. In
addition, well-known employed structures such as VGG, ResNet, and LSTM are also mentioned.
Class Activation Maps (CAM) are utilized to provide visual feedback to the trainee by highlighting
the parts of the performance that contributed significantly to the outcome. They are mentioned
under Visual Feedback in Figure 3. CAM is enabled through Global Pooling. Thus, it is also placed
under Visual Feedback. Besides allowing visualization, Global Pooling also eliminates the
duration difference problem that is crucial for time-series data.38,39
CNN
Faster RCNN
TSN
VGG
AlexNet
Hourglass
ResNet
RNN
LSTM
GRU
Elman RNN
CNN + LSTM
CNN + GRU
Global Pooling
Class Activation Map
Deep Neural
Networks
CNN
+
RNN
CNN
FCNVisual
Feedback
RNN
Two main data processing approaches were observed. For the kinematic inputs, the data can
directly be fed to the DNN, and the model outputs either the regressed score or the computed class.
As for the video-based inputs, data processing is usually a two-step process. A DL model first
localizes either the tool or the hand motion, which is subsequently utilized by a second DNN to
assess skill. Notwithstanding, there is one study where the authors developed a Temporal Segment
Networks (TSN) as a Siamese architecture.43,65 Multiple CNNs working on different segments of
a video were aggregated in the consensus layer for classification. To the best of our knowledge,
this is the first and only end-to-end model for video-based surgical skill assessment using DNN.
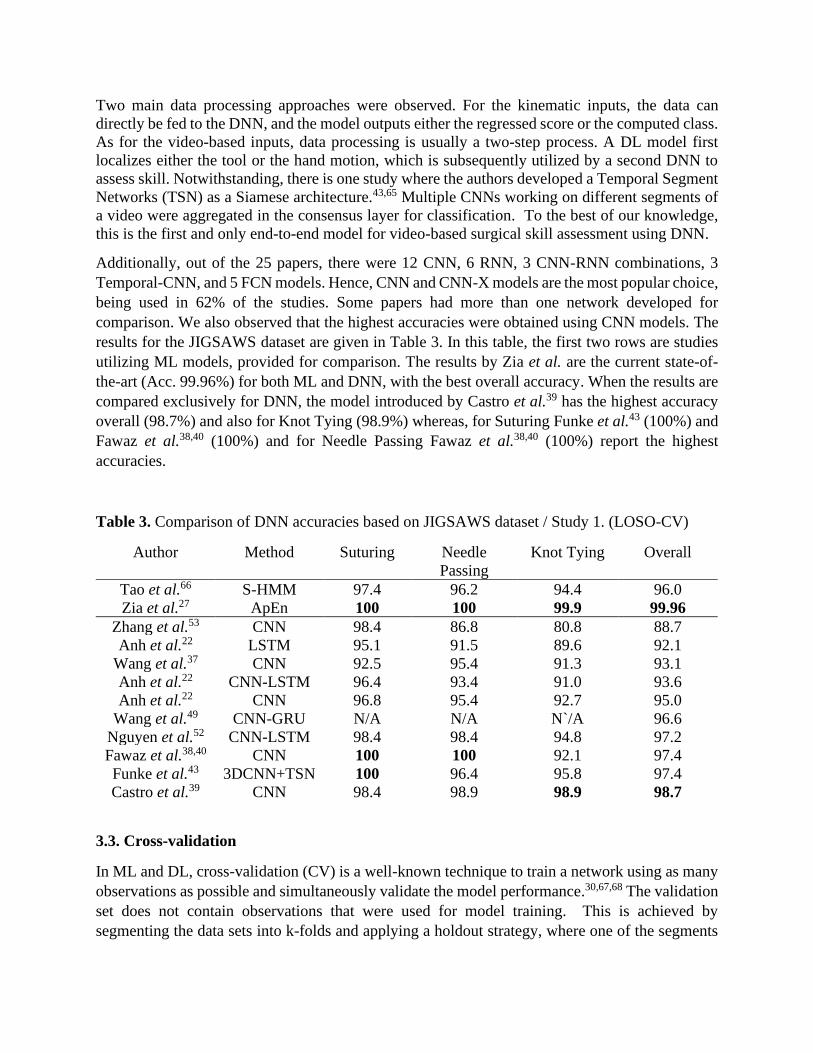
Additionally, out of the 25 papers, there were 12 CNN, 6 RNN, 3 CNN-RNN combinations, 3
Temporal-CNN, and 5 FCN models. Hence, CNN and CNN-X models are the most popular choice,
being used in 62% of the studies. Some papers had more than one network developed for
comparison. We also observed that the highest accuracies were obtained using CNN models. The
results for the JIGSAWS dataset are given in Table 3. In this table, the first two rows are studies
utilizing ML models, provided for comparison. The results by Zia et al. are the current state-of-
the-art (Acc. 99.96%) for both ML and DNN, with the best overall accuracy. When the results are
compared exclusively for DNN, the model introduced by Castro et al.39 has the highest accuracy
overall (98.7%) and also for Knot Tying (98.9%) whereas, for Suturing Funke et al.43 (100%) and
Fawaz et al.38,40 (100%) and for Needle Passing Fawaz et al.38,40 (100%) report the highest
accuracies.
Table 3. Comparison of DNN accuracies based on JIGSAWS dataset / Study 1. (LOSO-CV)
Author Method Suturing Needle
Passing
Knot Tying Overall
Tao et al.66 S-HMM 97.4 96.2 94.4 96.0
Zia et al.27 ApEn 100 100 99.9 99.96
Zhang et al.53 CNN 98.4 86.8 80.8 88.7
Anh et al.22 LSTM 95.1 91.5 89.6 92.1
Wang et al.37 CNN 92.5 95.4 91.3 93.1
Anh et al.22 CNN-LSTM 96.4 93.4 91.0 93.6
Anh et al.22 CNN 96.8 95.4 92.7 95.0
Wang et al.49 CNN-GRU N/A N/A N`/A 96.6
Nguyen et al.52 CNN-LSTM 98.4 98.4 94.8 97.2
Fawaz et al.38,40 CNN 100 100 92.1 97.4
Funke et al.43 3DCNN+TSN 100 96.4 95.8 97.4
Castro et al.39 CNN 98.4 98.9 98.9 98.7
3.3. Cross-validation
In ML and DL, cross-validation (CV) is a well-known technique to train a network using as many
observations as possible and simultaneously validate the model performance.30,67,68 The validation
set does not contain observations that were used for model training. This is achieved by
segmenting the data sets into k-folds and applying a holdout strategy, where one of the segments
is removed. The network is trained using the remaining (k–1) folds, and the model performance
on the fold left out is then recorded. The CV procedure methodically removes one fold at the time
until each fold has served as a validation set. The 25 articles surveyed here apply three distinct
CV strategies, which are as follows:
• Leave-one-super-trial-out (LOSO): The ith trial from each participant is removed and used to
validate the performance of the DNN model while the remaining data is used for training. The
performance of the DNN model is then evaluated after k-folds of super trials have been left
out for model validation. k is 5 for JIGSAWS dataset.13
• Leave-one-user-out (LOUO): removing the trials conducted by a single user to validate the
model performance until each user has been left out once.
• k-fold cross-validation, here the trials are concatenated in a randomized fashion and the
combined dataset is divided into k folds. The aim of a randomized arrangement of trials is to
avoid biasing the model validation to particular users.
LOSO is employed for studies utilizing the JIGSAWS dataset and those involving robotic surgery.
9 out of 25 papers have utilized LOSO to cross-validate their models. It is because JIGSAWS lacks
sufficient data, and LOSO allows DNN to observe all but one data point for each participant during
training. Moreover, LOSO achieved higher accuracy for skewed datasets such as, JIGSAWS.
LOUO, which is another CV technique, have only been used to compare it with the other CV
schemes. In addition, 7 out of 25 papers used k-folds (k=4, 5, & 10) to cross-validate their models.
Here, two out of 7 was LOOCV, which is a special version of k-fold where k is equal to the data
size. Furthermore, k-fold is the most popular CV method simultaneously amongst non-JIGSAWS
and video-based skill assessment studies. Other than those above, four studies utilized
Train/Test/Validation Set Splits, and one paper did not provide a validation during the training.
Also, 6 out of 25 did not report any CV method. The models that were not cross-validated were
trained and tested once; hence, there is no guarantee that the fixed set covers all possible variations
of movements.
3.4. Skills assessment techniques
We found that the two skills assessment techniques used in this field are classification and
regression. Out of the 25 papers analyzed, we found three papers that use regression in addition to
classification, and only one used regression alone. For instance, in a study based on the JIGSAWS
kinematic data, Fawaz et al.38,40 used a fully connected neural network (FCN) to predict the
OSATS score for each trial. They used Spearman’s correlation coefficient to assess the model
performance and computed 0.6, 0,57, and 0.65 for Suturing, Needle Passing, and Knot Tying,
respectively. Secondly, Kowalewski et al.15 also developed an FCN to predict OSATS score for
Suturing and Knot Tying and reported an overall mean squared error (MSE) of 3.71 ± 0.64 and R2
of 0.03 ± 0.81. They also did binary classification analysis and computed 70% accuracy.
For the classification studies, the papers based on the JIGSAWS datasets favored classification
into three categories - Novice, Intermediate, and Expert. The Intermediate class suffers the most
from misclassification. For example, Funke et al.43 misclassified all the intermediate surgeons into

either expert or novice using optical flow data with 3D-CNN for knot tying. Their model was
cross-validated by LOUO, and they claimed that the uneven distribution of the dataset leads the
DNN to fail to generalize the features. The lack of a sufficient number of expert surgeons might
also explain why we did not find any study using LOUO alone. In another study, Wang and Fey37
computed their lowermost Intermediate class score as 0.57 for knot-tying. Furthermore, the
Intermediate class score was consistently lower for the other two JIGSAWS tasks. Anh et al.22 also
had similar performance issues for the Intermediate class, especially for Knot Tying.
In addition to these studies, Getty et al.59 took another approach and classified four expert surgeons
with similar expertise. They achieved 83.4% accuracy using LSTM. Also, three studies trained
DNN only with expert data and ranked the non-expert surgeons based on the deviation.47,50,54 The
most common metrics to formulate regression were R2 and Root Mean Squared Error (RMSE)
whereas, it was accuracy, precision, recall, and F1 score for classification.
4. Discussion
Automation of technical skill assessment has the promise of objective evaluation, reduction of
resource requirements, and personalized training with real-time feedback. In this study, we
analyzed the current literature on the use of DNN for objective surgical skill assessment. Our first
finding was that only tool and hand motion studies were available in the literature that fit our
criteria. This may be attributed to the lack of public datasets or resources available for other data.
We also observed that kinematic and video-based data are the only two types of data utilized in
the studies, with kinematic data being used in two-thirds of the published papers. We believe this
is due to the fact that the sensors can record the kinematic data of the tool and hand motion directly,
as opposed to video-based data. Moreover, it can be directly be fed to the DNN without any
intermediate steps. Video-based data, on the other hand, requires an additional preprocessing step
to locate the tools and hands. Authors either annotated certain portion of the dataset spatially or
relied on crowdsourcing perform the same task. Amazon Mechanical Turk was the method of
crowdsourcing for all the surveyed studies that utilized crowdsourcing. Then, DNNs were trained
respectively, to detect and localize the tools for the rest of the dataset. However, collecting
kinematic data is easier in robotic surgery or in virtual reality-based simulators and not in open or
laparoscopic surgery, where tools will have to be instrumented during the operation. In addition,
the features extracted from the kinematic data, such as tooltip location or rotation, might not cover
the information that the collected data possess; hence, might not necessarily be optimal for the
given surgical task. On the other hand, video data is easy to collect and unobtrusive and collected
during laparoscopic and robotic surgeries. Although video-based data requires significant
annotation and preprocessing and the localization DNNs require high computational power, they
can be used to assess skills solemnly based on the recordings of performance without any explicit
preparation once the network is trained and cross-validated.
Among the different techniques employed, CNNs were found to be superior to the other DNNs
such as LSTM and FCN. This might be because RNNs are optimized for data sequences, and the
public datasets are not rich with long sequences of surgical data. In addition, most CNNs take
statistical features as input, which eliminates the need for LSTM since the temporal information is
represented by the features of choice. Among the studies sharing the same dataset, JIGSAWS, we
found that a model proposed by Castro et al.39 achieved the highest overall score. They achieved
98.7% accuracy using a CNN with SELU activation, GMP, and quaternion convolutional layers.
However, the current state-of-the-art for JIGSAWS dataset is due to Zia et al.27 in which the
predictability of the tool motion is encoded using approximate entropy [ApEn].24 They reported
99.96% overall accuracy in differentiating surgeons into categories. Even though there is 1.26%
difference in accuracy between these two models, we believe we should also consider two main
advantages that Castro et al.39 have over Zia et al.27. First, the ML model needs to extract
information from the kinematics before feeding them into the nearest neighbor classifier. But, in
Castro et al.39, the kinematics are fed directly into CNN without an explicit step; therefore, it is an
end-to-end model. Second, Castro et al.39 embed the CAM to the DNN based on the work of Fawaz
et al.38,40 It fits the time-series data into a color segregated diagram with respect to the contribution
of each timestamp. This visual feedback helps the participant on which parts of the performance
he/she should improve. This is a quality missing in Zia et al.27.We believe these advantages are
more than enough to favor the work of Castro et al.39 over Zia et al.27 especially considering the
increasing amount of studies published over the years, as seen in Figure 3.
Our analysis suggested that LOSO is the most commonly used CV method for surgical skill
assessment. Results obtained by LOSO are reported to be higher in comparison to LOUO. We
believe this is because of the skewed nature of the datasets. For instance, JIGSAWS only has two
experts and two intermediates, whereas there are four novices present. In LOSO the model is
trained by seeing data from all the surgeons thus is exposed to all different styles. But, the same is
not valid for LOUO because the DNN does not see data from one surgeon, and in a case the surgeon
is an expert or an intermediate, the DNN is left with only one expert or intermediate data to train
with. This has an adversarial effect on the generalization power of the DNN. In addition, models
cross-validated by LOSO have already achieved accuracies up to 98.7%. Therefore, the field for
LOSO CV is almost saturated. We hypothesized that, even though LOUO reports poorer scores,
we will see more papers published to improve LOUO to compensate for the gap in the literature.
We were surprised to find that k-fold CV is favored by the video-based studies over LOSO and
LOUO. We expected the opposite due to the fact that video-based data is computationally
expensive to work with and the aforementioned CV techniques require multiple runs of the same
network. We assume k-fold CV is utilized to prevent bias in the dataset, hence, overfitting
regardless of the expensive computational requirements.
Finally, we noted that the majority of the papers formulate skill assessment as a classification
problem. There are only four papers that predict the performance score directly. However, the
model developed by Kowalewski et al.15 suggests R2 of 0.03 with SD of 0.81; hence, we assume
their model has limited or no generalization power. This leads us to believe that there is still room
for improvement of regression accuracy. A reason for limited regression studies is, unlike
classification, regression requires a ground-truth scoring system. However, such scoring systems
are limited and not necessarily publicly available, e.g., the Fundamentals of Laparoscopic Surgery
scores used for board certification are IP protected. In contrast, classification can be done based
on their operative expertise.

We observed that intermediate surgeons are the most difficult to classify, which may have multiple
reasons. First, the chosen categorization method may not reflect true surgical experience. For
JIGSAWS, we hypothesize that there’s a very large performance improvement that’s seen between
10 and 100 hours of expertise, which might be making classification harder. Secondly, the DNN
may be biased toward novice data. This is because expert behavior may not adequately represented
due to an unbalanced size of the datasets, containing a significantly larger amount of novice data.
This is particularly prevalent in the JIGSAW studies. Lastly, a surgeon may actually be an expert
or a novice. Hence, any DNN classification for such cases would be considered correct by default.
Additionally, we observed the Intermediate surgeons were classified poorly, primarily for the Knot
Tying task of JIGSAWS. This might be because the ground-truth performance of the experts and
intermediates was reported to be similar to each other for the Knot Tying task in the literature.
5. Concluding remarks
In this paper, we examined papers related to the automation of surgical skill assessment using
DNN. We used PRISMA guidelines to process papers and ended up analyzing 25 papers. As a
result of the systematic review, we observed that DNN is useful to assess the surgical skills and
has already reported higher accuracies comparing top ML models, with the work of Zia et al. being
the only exception as tabulated in Table 3.Tool and hand motion data obtained from sensors and
videos have been used for DNNs, though the use of other sensor-based metrics is possible. In
recent work, we have shown that noninvasive brain imaging can be utilized to predict FLS scores
in pattern cutting using a CNN framework named Brain-NET.11 In our analysis CNN outperformed
various machine learning techniques, namely, Kernel-Partial Least Squares, Support Vector
Regression, and Random Forests.11 This survey yielded that the best performing models all rely
on convolutional neural networks, including the current state-of-the-art model in DL, achieving
overall 98.7% accuracy on the JIGSAWS dataset.39 Finally, we found that the most preferred
method to report technical skills to classify surgeons into distinct categories, namely Expert,
Intermediate, and Novice.
Several limitations of the current studies are evident from the analysis, which points to future
research directions. The most important limitation is, of course, the lack of publicly available
datasets of significant size. Surgical data is expensive to collect, and participation is voluntary.
Having sufficient numbers of expert surgeons dedicate time to generate datasets is challenging due
to their clinical obligations. Moreover, there is no consensus on the datasets regarding the effects
of gender and handedness to the outcome. Thus, we expect to see future datasets to focus on the
diversity as much as the quantity.
Moreover, we noticed a lack of rigor in establishing ground-truth performance scores. Most of the
studies suggest they had an expert on the team who did the annotation, which might adversely
affect inter-rater reliability. Moreover, some studies did not even cite the source of their
supervision, meaning it is not clear whether they had consulted an expert or not to annotate the
ground-truth performance. Additionally, the majority of the papers utilized kinematic data over
video-based data, possibly due to limited video information in existing surgical datasets.

Moreover, there is only one end-to-end DNN model based on video analysis. With the advances
in data augmentation to dilute the effect of sample size, we believe there will be more studies
focusing on end-to-end frameworks via video sequences.
We were only able to find four regression studies in the literature. Regression differs from
classification as the aim is to predict scores for each performance based on GRS. This makes
regression advantageous as it is continuous, and the progress can be tracked by the trainee even
when the assigned class for the performances does not change. Unlike regression, classification
puts surgeons into discrete categories that leave gray areas. For example, for JIGSAWS, the self-
proclaimed range of expertise was large for intermediates (10-100 hours), with novices up to 10
hours. Experts were 100+ hours, but we don’t know the actual hours required to classify surgical
skills. However, regression requires more data to pinpoint the performance. Also, there is not an
agreement in the literature as to how should the different regression models be evaluated.38. We
see this as a limitation for regressive models and expect more studies to be published in this field.
Finally, we found only one study based in the OR setting, while the rest of the studies either used
physical or virtual simulators for skill assessment. While the training and certification of surgeons
can be done on simulators, it is critical to be able to quantify their skills in clinical situations
objectively. There are multiple challenges to doing this due to the inherent messiness of the
operative environment where more than one surgeon may be involved in performing a procedure,
annotation of the operative videos to provide high-quality training datasets and privacy issues
related to the acquisition and use of the datasets.
In conclusion, we believe that DNNs possess strong potential for assessing surgical skills rapidly
and objectively, providing real-time feedback, and certifying and credentialing surgeons in the
near future. The availability of large, high-quality, publicly available annotated datasets will
accelerate the achievement of that goal.
6. References
1 Nataraja RM, Webb N, Lopez PJ. Simulation in paediatric urology and surgery, part 2: An
overview of simulation modalities and their applications. Journal of pediatric urology. 2018 Apr
1;14(2):125-31.
2 Dutta S, Krummel TM. Simulation: a new frontier in surgical education. Advances in surgery.
2006 Sep 1;40:249-63.
3 Martin JA, Regehr G, Reznick R, Macrae H, Murnaghan J, Hutchison C, Brown M. Objective
structured assessment of technical skill (OSATS) for surgical residents. British journal of surgery.
1997 Feb;84(2):273-8.
4 Reiley CE, Lin HC, Yuh DD, Hager GD. Review of methods for objective surgical skill
evaluation. Surgical endoscopy. 2011 Feb 1;25(2):356-66.
5 DaRosa DA, Zwischenberger JB, Meyerson SL, George BC, Teitelbaum EN, Soper NJ, Fryer
JP. A theory-based model for teaching and assessing residents in the operating room. Journal of
surgical education. 2013 Jan 1;70(1):24-30.
6 Darzi A, Smith S, Taffinder N. Assessing operative skill: needs to become more objective.
7 Fried GM. FLS assessment of competency using simulated laparoscopic tasks. Journal of
Gastrointestinal Surgery. 2008 Feb 1;12(2):210-2.
8 Scott DJ, Ritter EM, Tesfay ST, Pimentel EA, Nagji A, Fried GM. Certification pass rate of 100%
for fundamentals of laparoscopic surgery skills after proficiency-based training. Surgical
endoscopy. 2008 Aug 1;22(8):1887-93.
9 Poulose BK, Vassiliou MC, Dunkin BJ, Mellinger JD, Fanelli RD, Martinez JM, Hazey JW,
Sillin LF, Delaney CP, Velanovich V, Fried GM. Fundamentals of endoscopic surgery cognitive
examination: development and validity evidence. Surgical endoscopy. 2014 Feb 1;28(2):631-8.
10 Smith R, Patel V, Satava R. Fundamentals of robotic surgery: a course of basic robotic surgery
skills based upon a 14‐society consensus template of outcomes measures and curriculum
development. The International Journal of Medical Robotics and Computer Assisted Surgery. 2014
Sep;10(3):379-84.
11 Gao Y, Yan P, Kruger U, Cavuoto L, Schwaitzberg S, De S, Intes X. Functional brain imaging
reliably predicts bimanual motor skill performance in a standardized surgical task. IEEE
Transactions on Biomedical Engineering. 2020 Aug 5.
12 Rupprecht C, Lea C, Tombari F, Navab N, Hager GD. Sensor substitution for video-based action
recognition. In2016 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS)
2016 Oct 9 (pp. 5230-5237). IEEE.
13 Gao Y, Vedula SS, Reiley CE, Ahmidi N, Varadarajan B, Lin HC, Tao L, Zappella L, Béjar B,
Yuh DD, Chen CC. Jhu-isi gesture and skill assessment working set (jigsaws): A surgical activity
dataset for human motion modeling. InMiccai workshop: M2cai 2014 Sep (Vol. 3, p. 3).
14 Wanzel KR, Hamstra SJ, Caminiti MF, Anastakis DJ, Grober ED, Reznick RK. Visual-spatial
ability correlates with efficiency of hand motion and successful surgical performance. Surgery.
2003 Nov 1;134(5):750-7.
15 Kowalewski KF, Garrow CR, Schmidt MW, Benner L, Müller-Stich BP, Nickel F. Sensor-based
machine learning for workflow detection and as key to detect expert level in laparoscopic suturing
and knot-tying. Surgical Endoscopy. 2019 Nov 1;33(11):3732-40.
16 Bouget D, Allan M, Stoyanov D, Jannin P. Vision-based and marker-less surgical tool detection
and tracking: a review of the literature. Medical image analysis. 2017 Jan 1;35:633-54.
17 Pérez-Escamirosa F, Alarcón-Paredes A, Alonso-Silverio GA, Oropesa I, Camacho-Nieto O,
Lorias-Espinoza D, Minor-Martínez A. Objective classification of psychomotor laparoscopic
skills of surgeons based on three different approaches. International Journal of Computer Assisted
Radiology and Surgery. 2020 Jan 1;15(1):27-40.
18 Kirsch S, Comstock B, Warren J, Schaffhausen C, Kowalewski T, Lendvay T. Crowd Sourced
Assessment of Technical Skills (CSATS): A Scalable Assessment Tool for the Nursing Workforce.
J Invest Med. 2015 Jan 1;63(1):92.
19 Hofstad EF, Våpenstad C, Chmarra MK, Langø T, Kuhry E, Mårvik R. A study of psychomotor
skills in minimally invasive surgery: what differentiates expert and nonexpert performance.
Surgical endoscopy. 2013 Mar 1;27(3):854-63.
20 Bajka M, Tuchschmid S, Fink D, Székely G, Harders M. Establishing construct validity of a
virtual-reality training simulator for hysteroscopy via a multimetric scoring system. Surgical
endoscopy. 2010 Jan 1;24(1):79.
21 Pellen M, Horgan L, Barton JR, Attwood S. Laparoscopic surgical skills assessment: can
simulators replace experts?. World journal of surgery. 2009 Mar 1;33(3):440-7.
22 Anh NX, Nataraja RM, Chauhan S. Towards near real-time assessment of surgical skills: A
comparison of feature extraction techniques. Computer Methods and Programs in Biomedicine.
2020 Apr 1;187:105234.
23 Kim TS, O’Brien M, Zafar S, Hager GD, Sikder S, Vedula SS. Objective assessment of
intraoperative technical skill in capsulorhexis using videos of cataract surgery. International
journal of computer assisted radiology and surgery. 2019 Jun 1;14(6):1097-105.
24 Zia A, Sharma Y, Bettadapura V, Sarin EL, Essa I. Video and accelerometer-based motion
analysis for automated surgical skills assessment. International journal of computer assisted
radiology and surgery. 2018 Mar 1;13(3):443-55.
25 Winkler-Schwartz A, Bissonnette V, Mirchi N, Ponnudurai N, Yilmaz R, Ledwos N, Siyar S,
Azarnoush H, Karlik B, Del Maestro RF. Artificial intelligence in medical education: best
practices using machine learning to assess surgical expertise in virtual reality simulation. Journal
of surgical education. 2019 Nov 1;76(6):1681-90.
26 Winkler-Schwartz A, Yilmaz R, Mirchi N, Bissonnette V, Ledwos N, Siyar S, Azarnoush H,
Karlik B, Del Maestro R. Machine learning identification of surgical and operative factors
associated with surgical expertise in virtual reality simulation. JAMA network open. 2019 Aug
2;2(8):e198363-.
27 Zia A, Essa I. Automated surgical skill assessment in RMIS training. International journal of
computer assisted radiology and surgery. 2018 May 1;13(5):731-9.
28 Ahmidi N, Tao L, Sefati S, Gao Y, Lea C, Haro BB, Zappella L, Khudanpur S, Vidal R, Hager
GD. A dataset and benchmarks for segmentation and recognition of gestures in robotic surgery.
IEEE Transactions on Biomedical Engineering. 2017 Jan 4;64(9):2025-41.
29 Fard MJ, Ameri S, Chinnam RB, Pandya AK, Klein MD, Ellis RD. Machine learning approach
for skill evaluation in robotic-assisted surgery. arXiv preprint arXiv:1611.05136. 2016 Nov 16.
30 Schaffer C. Selecting a classification method by cross-validation. Machine Learning. 1993 Oct
1;13(1):135-43.
31 Zia A, Sharma Y, Bettadapura V, Sarin EL, Ploetz T, Clements MA, Essa I. Automated video-
based assessment of surgical skills for training and evaluation in medical schools. International
journal of computer assisted radiology and surgery. 2016 Sep 1;11(9):1623-36.
32 Goodfellow I, Bengio Y, Courville A. Deep learning. MIT press; 2016 Nov 10.
33 Levin M, McKechnie T, Khalid S, Grantcharov TP, Goldenberg M. Automated methods of
technical skill assessment in surgery: A systematic review. Journal of surgical education. 2019
Nov 1;76(6):1629-39.
34 Khalid S, Goldenberg M, Grantcharov T, Taati B, Rudzicz F. Evaluation of Deep Learning
Models for Identifying Surgical Actions and Measuring Performance. JAMA Network Open. 2020
Mar 2;3(3):e201664.
35 Hochreiter S, Schmidhuber J. Long short-term memory. Neural computation. 1997 Nov
15;9(8):1735-80.
36 Cho K, Van Merriënboer B, Gulcehre C, Bahdanau D, Bougares F, Schwenk H, Bengio Y.
Learning phrase representations using RNN encoder-decoder for statistical machine translation.
arXiv preprint arXiv:1406.1078. 2014 Jun 3.
37 Wang Z, Fey AM. Deep learning with convolutional neural network for objective skill
evaluation in robot-assisted surgery. International journal of computer assisted radiology and
surgery. 2018 Dec 1;13(12):1959-70.
38 Fawaz HI, Forestier G, Weber J, Idoumghar L, Muller PA. Accurate and interpretable evaluation
of surgical skills from kinematic data using fully convolutional neural networks. International
journal of computer assisted radiology and surgery. 2019 Sep 1;14(9):1611-7.
39 Castro D, Pereira D, Zanchettin C, Macêdo D, Bezerra BL. Towards Optimizing Convolutional
Neural Networks for Robotic Surgery Skill Evaluation. In 2019 International Joint Conference on
Neural Networks (IJCNN) 2019 Jul 14 (pp. 1-8). IEEE.
40 Fawaz HI, Forestier G, Weber J, Idoumghar L, Muller PA. Evaluating surgical skills from
kinematic data using convolutional neural networks. InInternational Conference on Medical Image
Computing and Computer-Assisted Intervention 2018 Sep 16 (pp. 214-221). Springer, Cham.
41 Law H, Ghani K, Deng J. Surgeon technical skill assessment using computer vision based
analysis. InMachine learning for healthcare conference 2017 Nov 6 (pp. 88-99).
42 Jin A, Yeung S, Jopling J, Krause J, Azagury D, Milstein A, Fei-Fei L. Tool detection and
operative skill assessment in surgical videos using region-based convolutional neural networks. In
2018 IEEE Winter Conference on Applications of Computer Vision (WACV) 2018 Mar 12 (pp.
691-699). IEEE.
43 Funke I, Mees ST, Weitz J, Speidel S. Video-based surgical skill assessment using 3D
convolutional neural networks. International journal of computer assisted radiology and surgery.
2019 Jul 1;14(7):1217-25.
44 Twinanda AP, Shehata S, Mutter D, Marescaux J, De Mathelin M, Padoy N. Endonet: a deep
architecture for recognition tasks on laparoscopic videos. IEEE transactions on medical imaging.
2016 Jul 22;36(1):86-97.
45 Sarikaya D, Corso JJ, Guru KA. Detection and localization of robotic tools in robot-assisted
surgery videos using deep neural networks for region proposal and detection. IEEE transactions
on medical imaging. 2017 Feb 8;36(7):1542-9.
46 Moher D, Liberati A, Tetzlaff J, Altman DG, Prisma Group. Preferred reporting items for
systematic reviews and meta-analyses: the PRISMA statement. PLoS med. 2009 Jul
21;6(7):e1000097.
47 Benmansour M, Handouzi W, Malti A. A neural network architecture for automatic and
objective surgical skill assessment. In 2018 International Conference on Electrical Sciences and
Technologies in Maghreb (CISTEM) 2018 Oct 28 (pp. 1-5). IEEE.
48 Doughty H, Damen D, Mayol-Cuevas W. Who’s better, who’s best: Skill determination in video
using deep ranking. CoRR, abs/1703.0. 2017:6057-66.
49 Wang Z, Fey AM. SATR-DL: improving surgical skill assessment and task recognition in robot-
assisted surgery with deep neural networks. In 2018 40th Annual International Conference of the
IEEE Engineering in Medicine and Biology Society (EMBC) 2018 Jul 18 (pp. 1793-1796). IEEE.
50 Benmansour M, Malti A. Simple and efficient recurrent neural network to evaluate classified
surgery tasks. In5th International Conference on Automation, Control Engineering and Computer
Science-ACECS 2018.
51 Li Z, Huang Y, Cai M, Sato Y. Manipulation-skill assessment from videos with spatial attention
network. In Proceedings of the IEEE International Conference on Computer Vision Workshops
2019 (pp. 0-0).
52 Nguyen XA, Ljuhar D, Pacilli M, Nataraja RM, Chauhan S. Surgical skill levels: Classification
and analysis using deep neural network model and motion signals. Computer methods and
programs in biomedicine. 2019 Aug 1;177:1-8.
53 Zhang D, Wu Z, Chen J, Gao A, Chen X, Li P, Wang Z, Yang G, Lo B, Yang GZ. Automatic
Microsurgical Skill Assessment Based on Cross-Domain Transfer Learning. IEEE Robotics and
Automation Letters. 2020 Apr 20;5(3):4148-55.
54 Ahmad MA, Mansoor SB, Khan ZA, Aqeel WA, Kabir SH. Benchmarking expert surgeons' path
for evaluating a trainee surgeon's performance. In Proceedings of the 12th acm siggraph
international conference on virtual-reality continuum and its applications in industry 2013 Nov 17
(pp. 57-62).
55 Cifuentes J, Boulanger P, Pham MT, Prieto F, Moreau R. Gesture Classification Using LSTM
Recurrent Neural Networks. In 2019 41st Annual International Conference of the IEEE
Engineering in Medicine and Biology Society (EMBC) 2019 Jul 23 (pp. 6864-6867). IEEE.
56 Hung AJ, Chen J, Ghodoussipour S, Oh PJ, Liu Z, Nguyen J, Purushotham S, Gill IS, Liu Y. A
deep‐learning model using automated performance metrics and clinical features to predict urinary
continence recovery after robot‐assisted radical prostatectomy. BJU international. 2019
Sep;124(3):487-95.
57 Pérez-Escamirosa F, Alarcón-Paredes A, Alonso-Silverio GA, Oropesa I, Camacho-Nieto O,
Lorias-Espinoza D, Minor-Martínez A. Objective classification of psychomotor laparoscopic
skills of surgeons based on three different approaches. International Journal of Computer Assisted
Radiology and Surgery. 2020 Jan 1;15(1):27-40.
58 Uemura M, Tomikawa M, Miao T, Souzaki R, Ieiri S, Akahoshi T, Lefor AK, Hashizume M.
Feasibility of an AI-based measure of the hand motions of expert and novice surgeons.
Computational and mathematical methods in medicine. 2018 Jan 1;2018.
59 Getty N, Zhou Z, Gruessner S, Chen L, Xia F. Recurrent and Spiking Modeling of Sparse
Surgical Kinematics. arXiv preprint arXiv:2005.05868. 2020 May 12.
60 Vaughan N, Gabrys B. Scoring and assessment in medical VR training simulators with dynamic
time series classification. Engineering Applications of Artificial Intelligence. 2020 Sep
1;94:103760.
61 Mazomenos EB, Bansal K, Martin B, Smith A, Wright S, Stoyanov D. Automated Performance
Assessment in Transoesophageal Echocardiography with Convolutional Neural Networks.
InInternational Conference on Medical Image Computing and Computer-Assisted Intervention
2018 Sep 16 (pp. 256-264). Springer, Cham.
62 Alshirbaji TA, Jalal NA, Möller K. Surgical tool classification in laparoscopic videos using
convolutional neural network. Current Directions in Biomedical Engineering. 2018 Sep
1;4(1):407-10.
63 Stauder R, Ostler D, Kranzfelder M, Koller S, Feußner H, Navab N. The TUM LapChole dataset
for the M2CAI 2016 workflow challenge. arXiv preprint arXiv:1610.09278. 2016 Oct 28.
64 Ahmidi N, Ishii M, Fichtinger G, Gallia GL, Hager GD. An objective and automated method
for assessing surgical skill in endoscopic sinus surgery using eye‐tracking and tool‐motion data.
In International forum of allergy & rhinology 2012 Nov (Vol. 2, No. 6, pp. 507-515). Hoboken:
Wiley Subscription Services, Inc., A Wiley Company.
65 Bromley J, Guyon I, LeCun Y, Säckinger E, Shah R. Signature verification using a" siamese"
time delay neural network. Advances in neural information processing systems. 1994 Nov 28:737-
.
66 Tao L, Elhamifar E, Khudanpur S, Hager GD, Vidal R. Sparse hidden markov models for
surgical gesture classification and skill evaluation. InInternational conference on information
processing in computer-assisted interventions 2012 Jun 27 (pp. 167-177). Springer, Berlin,
Heidelberg.
67 Arlot S, Celisse A. A survey of cross-validation procedures for model selection. Statistics
surveys. 2010;4:40-79.
68 Rodriguez JD, Perez A, Lozano JA. Sensitivity analysis of k-fold cross validation in prediction
error estimation. IEEE transactions on pattern analysis and machine intelligence. 2009 Dec
1;32(3):569-75.
Author biographies
Erim Yanik, M.S.,
is a Ph..D. student in the Department of Mechanical, Aerospace and Nuclear Engineering. He
received his Bachelor of Science degree in Mechanical Engineering from Istanbul Technical
University and obtained his M.S. from Southern Illinois University Edwardsville. His research
interests are Computer Vision, and Deep Neural Networks for surgical training and skill
assessment.
Xavier Intes, Ph.D.,
is a professor in the Department of Biomedical Engineering, codirector of the Center for Modeling,
Simulation, & Imaging in Medicine, and an AIMBE/SPIE/OSA fellow. He acted as the chief
scientist of Advanced Research Technologies Inc., Montreal, Canada. His research interests are on
the application of diffuse functional and molecular optical techniques for biomedical imaging in
preclinical and clinical settings.
Uwe Kruger, EngD.,
is a Professor of Practice in Biomedical Engineering at RPI and engaged in research related to
biomedical data science. Dr. Kruger is also a member of the Center for Modeling, Simulation and
Imaging in Medicine where he provides oversight to projects involving statistical and machine
learning problems. His research interests focus on developing and applying innovative solution
methods to solve nonlinear regression and classification problems.
Pingkun Yan, Ph.D.,
is an Assistant Professor at the Department of Biomedical Engineering at Rensselaer Polytechnic
Institute. He obtained his Ph.D. from National University of Singapore. His research interests
include medical imaging informatics and image-guided intervention using machine learning and
computer vision techniques.
David Diller, Ph.D.,
is a Senior Scientist at Raytheon BBN Technologies. He received his Ph.D. from Indiana
University Bloomington. His research interests are AI, computer vision, and human performance
modelling.
Brian Van Voorst, M.S.,
is a Lead Scientist at Raytheon BBN Technologies. He obtained his M.S. from Michigan
Technological University. His research interests are AI and computer vision.
Basiel Makled, M.S.,
is a Science and Technology Manager and Engineer at the United States Army Combat
Capabilities Development Command. His work is focused on Medical Simulation and Human
Performance Training out of Orlando, FL. Basiel completed his Master of Science in Biomedical
Engineering at the University of Central Florida and completed his undergraduate schooling at
Florida State University where he received a Bachelor of Science in Engineering with Honors
Distinction. Mr. Makled’s primary research interests lie at the cross-roads of Medical Simulation,
Training, Human Performance, Artificial Intelligence, and Virtual Reality.
Jack Norfleet, Ph.D.,
is a Chief Engineer at the United States Army Combat Capabilities Development Command. He
received his degree from the University of Central Florida. His interests are medical simulations
and human tissue properties.
Suvranu De, Sc.D.,
currently serves as the J. Erik Jonsson '22 Distinguished Professor of Engineering, Director of the
Center for Modeling, Simulation and Imaging in Medicine and Head of the Department of
Mechanical, Aerospace and Nuclear Engineering. His research interests are medical simulations,
virtual reality, surgical training, machine learning