Embed Size (px)
Citation preview

Vol. 117 No. 3 March 2014
Factors influencing the necessity for preoperative vascularimaging before harvesting a vascularized fibular flapAlireza Ghassemi, MD, DMD, PhD,a Maike Jost, DMD,b Christina Fitzner, MA,c Houman Jalaie, MD,d
Frank Hölzle, MD, DMD, PhD,a Jonas Apitzsch, MD,e Ali Modabber, MD, DMD,a and Lloyd Nanhekhan, MDf
University Hospital of Rheinisch-Westfälische Technische Hochschule Aachen, Aachen, Germany; Private Dental Practice, Oberhausen, Germany;University Hospitals Leuven, Leuven, Belgium
Objective. This study was carried out to identify groups of patients who would benefit from this angiography. The
angiographic images of a random group of patients were studied; the correlations between the vascular state of the lower
extremities and vessel pathology were investigated; and the possible links of these findings with certain medical conditions
were explored.
Study Design. Three experienced observers independently evaluated the angiograms of 185 patients. The status of all 3 vessels
of the lower extremities (anterior tibial artery, posterior tibial artery, and peroneal artery) was evaluated. The patients’ gender,
age, drinking and smoking habits, and medical conditions were documented.
Results. We found a significant correlation between pathology of the arteries of the lower extremity and blood cholesterol
level, blood pressure, coronary heart disease, diabetes mellitus, and age.
Conclusions. We suggest that preoperative vascular imaging be carried out in patients with comorbidities to reduce the
potential for flap failure and to minimize donor site complications. (Oral Surg Oral Med Oral Pathol Oral Radiol 2014;117:
289-292)
Reconstructive procedures of the head and neck regioncan be technically challenging; however, with refine-ments in microvascular techniques, surgical outcomeshave improved both functionally and esthetically.1,2 Thesuccess of a reconstruction, however, is not exclusivelydependent on the esthetic and functional result ofthe reconstructed deficit. The success of the reconstruc-tion is additionally dependent on minimal donor sitemorbidity.1,2 Free vascularized bone flaps offer the bestoption for reconstructing large bony defects, especiallyload-bearing and continuity defects.3 The decision touse a vascularized versus a nonvascularized bone graftis extremely important when considering donor sitemorbidity.1,2
Typically, the vascularized fibula flap offers suffi-cient bone length with a long pedicle and can also beharvested as a composite flap.3 In most cases, because
Coauthors Ghassemi and Jost contributed equally to this article as firstauthors.aDepartment of Oral, Maxillofacial and Plastic Facial Surgery, Uni-versity Hospital of Rheinisch-Westfälische Technische HochschuleAachen.bPrivate Dental Practice, Oberhausen, Germany.cInstitute of Medical Statistics, University of Rheinisch-WestfälischeTechnische Hochschule Aachen.dDepartment of Vascular Surgery, University Hospital of Rheinisch-Westfälische Technische Hochschule Aachen.eDepartment of Diagnostic and Interventional Radiology, UniversityHospital of Rheinisch-Westfälische Technische Hochschule Aachen.fDepartment of Plastic, Reconstructive and Aesthetic Surgery, Uni-versity Hospitals Leuven.Received for publication May 21, 2013; returned for revision Oct 13,2013; accepted for publication Nov 4, 2013.� 2014 Elsevier Inc. All rights reserved.2212-4403/$ - see front matterhttp://dx.doi.org/10.1016/j.oooo.2013.11.492
the vascular state of the lower extremity is independentof the presence of the peroneal artery, routine perfor-mance of preoperative vascular imaging of the vesselsof the lower leg is controversial.4,5 However, there arearterial conditions that can adversely affect the lowerextremity when harvesting the fibula. These includesignificant arteriosclerotic disease of the tibioperonealvessels, arterial anatomic variations (such as the pero-neal arteria magna and the absence of the peroneal ar-tery), or congenital or traumatic arterial defects.6-9
Harvesting of the free fibula flap in the presence ofmany of these anatomic conditions may jeopardize thedonor leg, the fibula flap, or both.
Based on the assumption that certain medical con-ditions lead to arterial disease, we evaluated additionalfactors that would require the preoperative vascularimaging of the lower extremity if a fibula flap is to beconsidered as the donor site.
MATERIALS AND METHODSOwing to the retrospective course of the study,no ethical approval was required. Written informedconsent was obtained from each patient for the
Statement of Clinical Relevance
Preoperative vascular imaging of the lower extrem-ity provides information on vascular pathology (ifpresent) and therefore reduces the risk of fibular flapfailure and helps to avoid potential donor sitecomplications.
289
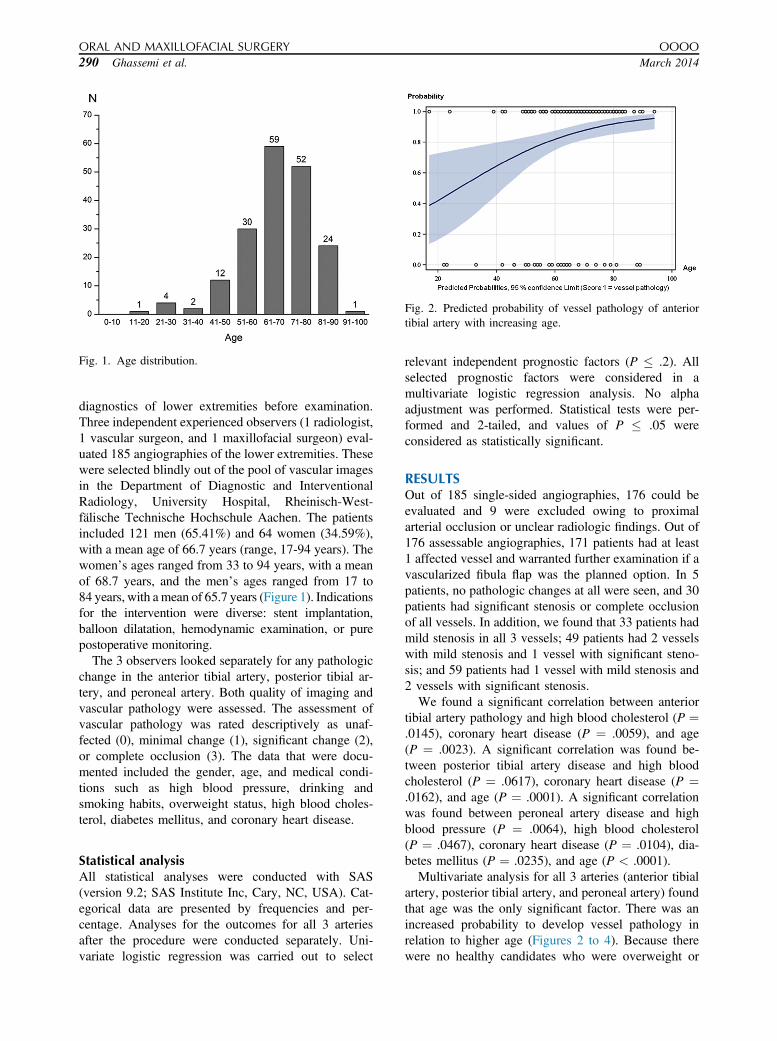
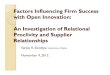
Fig. 1. Age distribution.
Fig. 2. Predicted probability of vessel pathology of anteriortibial artery with increasing age.
ORAL AND MAXILLOFACIAL SURGERY OOOO
290 Ghassemi et al. March 2014
diagnostics of lower extremities before examination.Three independent experienced observers (1 radiologist,1 vascular surgeon, and 1 maxillofacial surgeon) eval-uated 185 angiographies of the lower extremities. Thesewere selected blindly out of the pool of vascular imagesin the Department of Diagnostic and InterventionalRadiology, University Hospital, Rheinisch-West-fälische Technische Hochschule Aachen. The patientsincluded 121 men (65.41%) and 64 women (34.59%),with a mean age of 66.7 years (range, 17-94 years). Thewomen’s ages ranged from 33 to 94 years, with a meanof 68.7 years, and the men’s ages ranged from 17 to84 years, with a mean of 65.7 years (Figure 1). Indicationsfor the intervention were diverse: stent implantation,balloon dilatation, hemodynamic examination, or purepostoperative monitoring.
The 3 observers looked separately for any pathologicchange in the anterior tibial artery, posterior tibial ar-tery, and peroneal artery. Both quality of imaging andvascular pathology were assessed. The assessment ofvascular pathology was rated descriptively as unaf-fected (0), minimal change (1), significant change (2),or complete occlusion (3). The data that were docu-mented included the gender, age, and medical condi-tions such as high blood pressure, drinking andsmoking habits, overweight status, high blood choles-terol, diabetes mellitus, and coronary heart disease.
Statistical analysisAll statistical analyses were conducted with SAS(version 9.2; SAS Institute Inc, Cary, NC, USA). Cat-egorical data are presented by frequencies and per-centage. Analyses for the outcomes for all 3 arteriesafter the procedure were conducted separately. Uni-variate logistic regression was carried out to select
relevant independent prognostic factors (P � .2). Allselected prognostic factors were considered in amultivariate logistic regression analysis. No alphaadjustment was performed. Statistical tests were per-formed and 2-tailed, and values of P � .05 wereconsidered as statistically significant.
RESULTSOut of 185 single-sided angiographies, 176 could beevaluated and 9 were excluded owing to proximalarterial occlusion or unclear radiologic findings. Out of176 assessable angiographies, 171 patients had at least1 affected vessel and warranted further examination if avascularized fibula flap was the planned option. In 5patients, no pathologic changes at all were seen, and 30patients had significant stenosis or complete occlusionof all vessels. In addition, we found that 33 patients hadmild stenosis in all 3 vessels; 49 patients had 2 vesselswith mild stenosis and 1 vessel with significant steno-sis; and 59 patients had 1 vessel with mild stenosis and2 vessels with significant stenosis.
We found a significant correlation between anteriortibial artery pathology and high blood cholesterol (P ¼.0145), coronary heart disease (P ¼ .0059), and age(P ¼ .0023). A significant correlation was found be-tween posterior tibial artery disease and high bloodcholesterol (P ¼ .0617), coronary heart disease (P ¼.0162), and age (P ¼ .0001). A significant correlationwas found between peroneal artery disease and highblood pressure (P ¼ .0064), high blood cholesterol(P ¼ .0467), coronary heart disease (P ¼ .0104), dia-betes mellitus (P ¼ .0235), and age (P < .0001).
Multivariate analysis for all 3 arteries (anterior tibialartery, posterior tibial artery, and peroneal artery) foundthat age was the only significant factor. There was anincreased probability to develop vessel pathology inrelation to higher age (Figures 2 to 4). Because therewere no healthy candidates who were overweight or
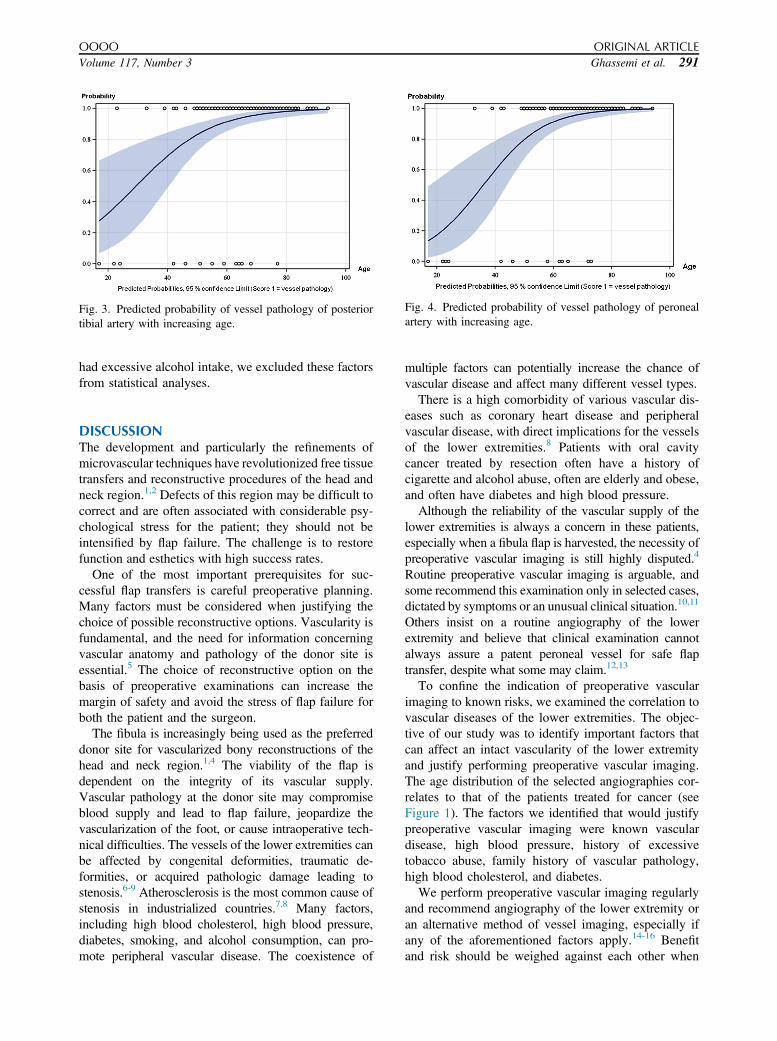
Fig. 3. Predicted probability of vessel pathology of posteriortibial artery with increasing age.
Fig. 4. Predicted probability of vessel pathology of peronealartery with increasing age.
OOOO ORIGINAL ARTICLE
Volume 117, Number 3 Ghassemi et al. 291
had excessive alcohol intake, we excluded these factorsfrom statistical analyses.
DISCUSSIONThe development and particularly the refinements ofmicrovascular techniques have revolutionized free tissuetransfers and reconstructive procedures of the head andneck region.1,2 Defects of this region may be difficult tocorrect and are often associated with considerable psy-chological stress for the patient; they should not beintensified by flap failure. The challenge is to restorefunction and esthetics with high success rates.
One of the most important prerequisites for suc-cessful flap transfers is careful preoperative planning.Many factors must be considered when justifying thechoice of possible reconstructive options. Vascularity isfundamental, and the need for information concerningvascular anatomy and pathology of the donor site isessential.5 The choice of reconstructive option on thebasis of preoperative examinations can increase themargin of safety and avoid the stress of flap failure forboth the patient and the surgeon.
The fibula is increasingly being used as the preferreddonor site for vascularized bony reconstructions of thehead and neck region.1,4 The viability of the flap isdependent on the integrity of its vascular supply.Vascular pathology at the donor site may compromiseblood supply and lead to flap failure, jeopardize thevascularization of the foot, or cause intraoperative tech-nical difficulties. The vessels of the lower extremities canbe affected by congenital deformities, traumatic de-formities, or acquired pathologic damage leading tostenosis.6-9 Atherosclerosis is the most common cause ofstenosis in industrialized countries.7,8 Many factors,including high blood cholesterol, high blood pressure,diabetes, smoking, and alcohol consumption, can pro-mote peripheral vascular disease. The coexistence of
multiple factors can potentially increase the chance ofvascular disease and affect many different vessel types.
There is a high comorbidity of various vascular dis-eases such as coronary heart disease and peripheralvascular disease, with direct implications for the vesselsof the lower extremities.8 Patients with oral cavitycancer treated by resection often have a history ofcigarette and alcohol abuse, often are elderly and obese,and often have diabetes and high blood pressure.
Although the reliability of the vascular supply of thelower extremities is always a concern in these patients,especially when a fibula flap is harvested, the necessity ofpreoperative vascular imaging is still highly disputed.4
Routine preoperative vascular imaging is arguable, andsome recommend this examination only in selected cases,dictated by symptoms or an unusual clinical situation.10,11
Others insist on a routine angiography of the lowerextremity and believe that clinical examination cannotalways assure a patent peroneal vessel for safe flaptransfer, despite what some may claim.12,13
To confine the indication of preoperative vascularimaging to known risks, we examined the correlation tovascular diseases of the lower extremities. The objec-tive of our study was to identify important factors thatcan affect an intact vascularity of the lower extremityand justify performing preoperative vascular imaging.The age distribution of the selected angiographies cor-relates to that of the patients treated for cancer (seeFigure 1). The factors we identified that would justifypreoperative vascular imaging were known vasculardisease, high blood pressure, history of excessivetobacco abuse, family history of vascular pathology,high blood cholesterol, and diabetes.
We perform preoperative vascular imaging regularlyand recommend angiography of the lower extremity oran alternative method of vessel imaging, especially ifany of the aforementioned factors apply.14-16 Benefitand risk should be weighed against each other when

ORAL AND MAXILLOFACIAL SURGERY OOOO
292 Ghassemi et al. March 2014
considering the patients’ and surgeons’ expectationsand the goal of the reconstruction. These images pro-vide information on vascular pathology and thereforereduce the risk of flap failure and help to avoid potentialdonor site complications. Furthermore, these imagescan also enable preoperative navigated planning ofexact bony reconstruction.17,18
REFERENCES1. Hurvitz KA, Kobayashi M, Evans GR. Current options in
head and neck reconstruction. Plast Reconstr Surg. 2006;118:122e-133e.
2. Balasundaram I, Al-Hadad I, Parmar S. Recent advances inreconstructive oral and maxillofacial surgery. Br J Oral Max-illofac Surg. 2012;50:695-705.
3. Jacobson AS, Buchbinder D, Urken ML. Reconstruction ofbilateral osteoradionecrosis of the mandible using a single fibularfree flap. Laryngoscope. 2010;120:273-275.
4. Whitley SP, Sandhu S, Cardoza A. Preoperative vascularassessment of the lower limb for harvest of a fibular flap: theviews of vascular surgeons in the United Kingdom. Br J OralMaxillofac Surg. 2004;42:307-310.
5. Kelly AM, Cronin P, Hussain HK, Londy F, Chepeha D,Carlos R. Preoperative MR angiography in free fibula flap transferfor head and neck cancer: clinical application and influence onsurgical decision making. AJR. 2007;188:268-274.
6. Bardsley JL, Staple TW. Variations in branching of the poplitealartery. Radiology. 1970;94:581-587.
7. Gordon T, Kannel WB. Predisposition to atherosclerosis in thehead, heart, and legs: the Framingham study. JAMA. 1972;221:661-666.
8. Espinola-Klein C, Rupprecht HJ, Blankenberg S, et al. Manifes-tationen der Atherosklerose in verschiedenen Gefäßregionen:Gemeinsamkeit und Unterschiede hinsichtlich Epidemiologie,Äthiologie und Prognose. Med Klin. 2002;97:221-228.
9. Hölzle F, Ristow O, Rau A, et al. Evaluation of the vessels of thelower leg before microsurgical fibular transfer, part I: anatomicalvariations in the arteries of the lower leg. Br J Oral MaxillofacSurg. 2011;49:270-274.
10. Dublin BA, Karp NS, Kasabian AK, Kolker AR, Shah MH. Se-lective use of preoperative lower extremity angiography in freeflap reconstruction. Ann Plast Surg. 1997;38:404-407.
11. Lutz BS, Wie FC, Ng SH, Chen ICH, Chen SHT. Routine donorleg angiography before vascularized free fibula transplantation isnot necessary: a prospective study in 120 clinical cases. PlastReconstr Surg. 1999;103:121-127.
12. Young DM, Trabulsky PP, Anthony JP. The need for preopera-tive leg angiography in fibula free flaps. J Reconstr Microsurg.1994;10:283-287.
13. Seres L, Csaszar J, Voros E, Borbely L. Donor site angiographybefore mandibular reconstruction with fibula free flap.J Craniofac Surg. 2001;12:608-613.
14. Hölzle F, Ristow O, Rau A, et al. Evaluation of the vessels of thelower leg before microsurgical fibular transfer, part II: magneticresonance angiography for standard preoperative assessment. Br JOral Maxillofac Surg. 2011;49:275-280.
15. Tregaskiss AP, Goodwin AN, Bright LD, Ziegler CH,Acland RD. Three-dimensional CT angiography: a new techniquefor imaging microvascular anatomy. Clin Anat. 2007;20:116-123.
16. Fukaya E, Grossman RF, Saloner D, Leon P, Nozaki M,Mathes SJ. Magnetic resonance angiography for free fibula flaptransfer. J Reconstr Microsurg. 2007;23:205-212.
17. Modabber A, Gerressen M, Stiller MB, et al. Computer-assistedmandibular reconstruction with vascularised iliac crest bone graft.Aesthetic Plast Surg. 2012;36:653-659.
18. Modabber A, Legros C, Rana M, Gerressen M, Riediger D,Ghassemi A. Evaluation of computer-assisted jaw reconstruc-tion with free vascularized fibular flap compared to conven-tional surgery: a clinical pilot study. Int J Med Robot. 2012;8:215-220.
Reprint requests:
Alireza GhassemiDepartment of Oral, Maxillofacial and Plastic Facial SurgeryUniversity Hospital of RWTH-AachenPauwelsstrasse 3052074 [email protected]