Embed Size (px)
Citation preview

Polyp ist nicht gleich Polyp
Wann operieren, wann kontrollieren?
Kolorektale Karzinome 2012
Besser:
Was bedeutet der histologische Befund für den Patienten
oder den weiteren Verlauf

„Historischer“ Rückblick:
1987/90 Morson, Jass JR: Gastrointestinal Pathology, 3rd ed.
Polyp ist nicht gleich Polyp
Type Single or smal number Multiple
Dysmature Hyperplastic (metaplastic)
polyp
Hyperplastic (metaplastic)
polyposis
Neoplastic Adenoma (tubular,
tubulovillous, villous)
Adenomatosis (familial
adenomatous polyposis)
Hamartomatous Juvenile polyp
Peutz-Jegehrs polyp
Juvenile Polyposis
Peutz-Jeghers syndrome
Cowden‘s syndrome
Cronkhite-Canada syndrome
Inflammatory Inflammatory polyp
(pseudopolyp)
Inflammatory polyposis
(pseudopolyposis)



• Lymphangiosis carcinomatosa (L0 vs. L1)
dies schließt auch die Invasion kleiner postkapillärer Venolen ein (nicht unterscheidbar)
• Grading: G1, G2 vs. G3 und entdiff.
• Resektionsstatus R0 vs. R1
R1 = Abstand ≤ 1mm,
anglo-amerikanische Literatur teilweise ≤ 2 mm
Histopathologische Parameter zur Einschätzung des
Risikos einer lymphogenen Metastasierung beim
pT1-Karzinom.
anglo-amerikanische Literatur teilweise ≤ 2 mm
• Infiltrationstiefe in die Submucosa
sm1 u. sm2 vs. Sm3 bei flachen Adenomen oder
Haggitt 1-3 vs. Haggitt 4


Carcinom pT1 im Polypen / Adenom
Low risk:G1 oder G2
L0 (schließt hier V0 mit ein)
R0 Abstand angeben und beachten
sm1 o. sm2 ≤ 1000�
� Wahrscheinlichkeit von 95-99%, dass im Resektat nichts mehr gefunden wird� Wahrscheinlichkeit von 95-99%, dass im Resektat nichts mehr gefunden wird
High risk:G3
L1 und oder V1
R1
sm3
� Risiko der LK-Metastasen je nach Literatur zw. 5 und 15%

Serratierte Läsionen des Colons
Warum haben diese plötzlich solch einen Stellenwert?
„Sägeblatt – Polypen“
neuer Weg der Karzinogenese
(ca. 30% der Kolonkarzinome entstehen via Promotor-(ca. 30% der Kolonkarzinome entstehen via Promotor-
methylierung)
Jahrzehnte wahrscheinlich unterdiagnostiziert als
„dysmature“ Läsionen ohne Risiko der Karzinomentsehung
lange Zeit fehlklassifiziert,
d.h. inadäquate Therapie und Nachsorge
möglicherweise dadurch verantwortlich für „Intervallkarzinome“

Polyp ist nicht gleich Polyp
1996/2011:
Hyperplastische Polypen:
3Typen: 1. mikrovesikaler Typ
2. becherzellreicher Typ
3. muzinarmer Typ (selten)3. muzinarmer Typ (selten)
1996 Torlacovic & Snover:serrated adenomatous polyposis, Gastroenterology2011 Consensuskonferenz Gastroenterologische Pathologie, Pathologe


Serratiertes Adenom?


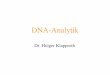
Comparison of Microsatellite Instability, CpG Island Methylation Phenotype, BRAF and KRAS Status in Serrated Polyps and Traditional Adenomas Indicates Separate Pathways to Distinct Colorectal Carcinoma End Points
O'Brien, Michael J.; Yang, Shi; Mack, Charline; Xu, Huihong; Huang, Christopher S.; Mulcahy, Elizabeth; Amorosino, Mark; Farraye, Francis A.The American Journal of Surgical Pathology. 30(12):1491-1501, December 2006.doi: 10.1097/01.pas.0000213313.36306.85
FIGURE 5. Panel A is a scanning power of a slide with 2 sections of a single SA that exhibits a focus of early invasive carcinoma. Rectangles identify areas of the polyp (Panels B1, C1, D1, and E1) which were microdissected and assayed individually for BRAF(V600E) mutations and MSI. Panel B1 was sampled as representative of an area showing the histologic features of SPAP; C1 SA; D1 SA contiguous to the invasive adenocarcinoma showing a nonserrated dysplastic phenotype, and E1 corresponds to the area of invasive undifferentiated (medullary) carcinoma. All samples had a BRAF(V600E) mutation. The MSI assay for each is illustrated in the corresponding electropherogram; B2 and C2 show a single cluster for both BAT25 (color blue) and BAT26 (color black); D2 and E2 show 2 discrete clusters indicating altered microsatellite size (smaller) and MSI-H. Higher magnification detail of IHC staining for hMLH1 in corresponding serial sections is illustrated in panels B3, C3, D3, and E3. SPAP and SA illustrated in B3 and C3, respectively, show positive staining of epithelial nuclei for hMLH1 protein, contrasting with negative staining of epithelial nuclei in D3 and E3.

Warum ist das wichtig?
Typ mvHPBecherz.
HPmpHP SSA/P
SSA Dysplasie
TSA
BRAF Hoch Niedrig Hoch Hoch Hoch Niedrig
KRAS Selten Hoch Selten Niedrig Mittel Niedrig
CIMP Mittel Niedrig Mittel Hoch Hoch Mittel
MSI Fehlt Fehlt Fehlt Selten Niedrig Selten

Karzinogenese – KolonVerschiedene Karzinogenesewege einer
Kolonstammzelle: Eine Stammzelle des
Kolons kann in Abhängigkeit von verschiedenen
Mutationen unterschiedliche Karzinogenesewege
einschlagen.
Der CIMP-Pathway umfasst unterschiedliche
Karzinogenesewege, die sich wesentlichKarzinogenesewege, die sich wesentlich
durch eine vorliegende oder nicht vorliegende
Methylierung des MLH1-Gens unterscheiden.
CIN: chromosomale Instabilität;
MIN: Mikrosatelliteninstabilität;
CIMP: CpG-island methylator pathway;
MSI-H: hochgradige Mikrosatelliteninstabilität;
MSI-L: mäßige Mikrosatelliteninstabilität;
MSS: mikrosatellitenstabil;
HNPCC: hereditary non-polyposis colorectal cancer

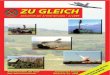
Comparison of Microsatellite Instability, CpG Island Methylation Phenotype, BRAF and KRAS Status in Serrated Polyps and Traditional Adenomas Indicates Separate Pathways to Distinct Colorectal Carcinoma End Points
O'Brien, Michael J.; Yang, Shi; Mack, Charline; Xu, Huihong; Huang, Christopher S.; Mulcahy, Elizabeth; Amorosino, Mark; Farraye, Francis A.
The American Journal of Surgical
FIGURE 7. Diagrammatic
representation of BRAF(V600E)
serrated polyp neoplasia pathway. The
diagram depicts BRAF(V600E) as an
early or instigating mutation, CpG island
methylation as increasing with more
advanced histologic stage, and MSI-H
occurring late, at the interface of SA and
invasive adenocarcinoma.
16
The American Journal of Surgical Pathology. 30(12):1491-1501, December 2006.
doi: 10.1097/01.pas.0000213313.36306.85



Serratierte Polypen / Adenome – empfohlene Nachsorge lt. Aktueller S3-Leitlinie
Schmiegel et al. 2008
Diagnose Karzinomrisiko Kontrollintervall
HP Keines Keine Indikation zur
NachsorgeNachsorge
SSA Ja, unklar wie hoch 3 Jahre
TSA Ja, wie klassische
Adenome, evtl. �
3 Jahre
Gemischter Polyp Ja 3 Jahre
Aber:





Polypose Syndrome
Kriterien der Polyposis:
− positive Amsterdam- Kriterien
− positive Bethesda-Kriterien
− > 10 Adenome bei einem Patienten
− Individuen mit mehreren hamartomatösen Polypen oder− Individuen mit mehreren hamartomatösen Polypen oder
− serratiertem Polypose Syndrom

Serratiertes/Hyperplatisches Polypose Syndrom
Definition WHO 2000:
Multiple oder große hyperplastische Polypen des Colon ,
typischerweise proximal und familiär gehäuft.
Diagnose-Kriterien:
1. mind. 5 histolog. gesicherte HP (SSA) proximal1. mind. 5 histolog. gesicherte HP (SSA) proximal
des Sigma, davon 2 > 10mm
oder
2. mind. 1 histolog. diagnostizierter HP (SSA) prox. des Sigma
bei erstgrad. Verwandten eines Pat. mit SPS
oder
3. über 30 (20 lt. NCCN) histolog. diagnostizierte HP jeglicher Größe
im gesamten Kolon (NCCN: Sigma und Rektum ausgenommen)
Risiko für Kolorektales Karzinom >50%!!

Fazit:
Polyp ist nicht gleich Polyp
Hyperplastische Polypen:
Wo? Wieviele? Sessil serratiertes Adenom?
Flache Adenome - gestielte Adenome
IN high-grade? R0? Wieviele?
Karzinom im Adenom
R0 sicher? L0? sm? gestielt oder flach? G?