Embed Size (px)
Citation preview

Kurs “Allgemeine und systematische Pharmakologie und Toxikologie” SoSe 2019 Seminarthema: Bakterielle Toxine - Virulenzfaktoren, Medikamente, biologische Kampfstoffe
Dr. Katharina Ernst N26/427 0731-50065528 [email protected] Der Inhalt bzw. die Gliederung der Referate ist frühzeitig mit der/dem zuständigen Dozentin/en abzusprechen. Alle Referate sollen 20 Minuten dauern und den Einsatz von Hilfsmitteln (Folien) umfassen. Bei Wiederverwendung von Powerpoint-Folien von Kolleginnen/en vorangegangener Seminare werden keine Creditpunkte (siehe Link "Creditpunkte") vergeben.
Referat 1: Clostridium difficile assoziierte Krankheiten
L. Napolitano and C. E. Edmiston: Clostridium difficile disease: Diagnosis, pathogenesis, and treatment update. Surgery (2017) http//doi.org/10.1016/j.surg.2017.01.018
K. Aktories, C. Schwan, and T. Jank: Clostridium difficile Toxins Biology. Annual Reviews (2017), 71:281-307
Das Referat soll Epidemiologie, Pathogenese inkl. Aufnahme und molekularer Wirkmechanismus der Toxine A und B, Diagnose, klinisches Bild, medikamentöse Therapie und Therapiestrategien Clostridium difficile assoziierter Krankheiten erläutern. Operative Behandlungsmethoden, sowie das binäre CDT Toxin sollen hier nicht im Fokus stehen. Referat 2: Botulinum-Neurotoxine in der klinischen Anwendung
D. Dressler: Clinical applications of botulinum toxin. Current Opinion in Microbiology (2012), 15, 325–336
E. Fonfria et al.: The expanding therapeutic utility of botulinum neurotoxins. Toxins (2018), 10, 208
Fallbeispiel
In diesem Referat soll die Struktur, Aufnahme und Wirkungsweise, der Botulinum-Neurotoxine, sowie therapeutische Anwendungsgebiete (inkl. Fallbeispiel) vorgestellt werden. Das Krankheitsbild Botulismus soll hier nicht thematisiert werden. Für die Grundlagen des Wirkmechanismus ist das Lehrbuch Marquardt/Schäfer/Barth „Toxikologie“ zu empfehlen. Referat 3: Anthrax als biologischer Kampfstoff
M. Doganay and H. Demiraslan: Human Anthrax as a Re-Emerging Disease. Recent Pat on Anti-Infect Drug Discov (2015), 10, 10-29
S. Liu, M. Moayeri and S. H. Leppla: Anthrax lethal and edema toxins in anthrax pathogenesis. Trends Microbiol. (2014), 22, 317-325
R. M. Atlas: Bioterrorism: From Threat to Reality. Annu. Rev. Microbiol. (2002), 56, 167-85 (Fokus nur auf Anthrax)
Innerhalb des Referates sollen Aufnahme und Wirkmechanismus der Anthrax-Toxine, sowie Krankheitsbild (Fokus inhalative Form), Diagnose und Therapie vorgestellt werden. Zudem soll auf die Geschichte bzw. das Potential von Anthrax als biologischer Kampfstoff im Kontext Bioterrorismus eingegangen werden.

ARTICLE IN PRESS
Accepte
ReprintMCCM,Care, UUniversiArbor, M
0039-60
� 2017
http://d
Clostridium difficile disease:Diagnosis, pathogenesis, andtreatment update
Lena M. Napolitano, MD, FACS, FCCP, MCCM,a andCharles E. Edmiston, Jr, PhD, CIC FIDSA, FSHEA, FAPIC,b Ann Arbor, MI, and Milwaukee, WIClostridium difficile infections are the leading cause of health care–associated infectious diarrhea,posing a significant risk for both medical and surgical patients. Because of the significant morbidity andmortality associated with C difficile infections, knowledge of the epidemiology of C difficile in com-bination with a high index of suspicion and susceptible patient populations (including surgical, post-colectomy, and inflammatory bowel disease patients) is warranted. C difficile infections present with awide spectrum of disease, ranging from mild diarrhea to fulminant colitis or small bowel enteritis andrecurrent C difficile infections. Early implementation of medical and operative treatment strategies forC difficile infections is imperative for optimal patient outcomes. National and international guidelinesrecommend early operative consultation and total abdominal colectomy with end ileostomy and preser-vation of rectum. Diverting loop ileostomy and colonic lavage followed by intravenous metronidazole andintracolonic vancomycin administered via the efferent limb of the ileostomy should be considered as analternative to total colectomy in selected patients. New and emerging strategies for C difficile infectiontreatment include monoclonal antibodies, vaccines, probiotics, biotherapeutics, and new antibiotics. Asuccessful C difficile prevention and eradication program requires a multidisciplinary approach thatincludes early disease recognition, implementation of guidelines for monitoring adherence to environ-mental control, judicious hand hygiene, evidence-based treatment and management strategies, and afocused antibiotic stewardship program. Surgeons are an important part of the clinical team in themanagement of C difficile infection prevention and treatment. (Surgery 2017;j:j-j.)
From the Department of Surgery,a University of Michigan Health System, Ann Arbor, Michigan; and theDepartment of Surgery,b Medical College of Wisconsin, Milwaukee, Wisconsin
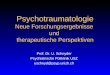
A 64-YEAR-OLD MAN developed pneumonia afteremergency repair of an incarcerated inguinal her-nia (small bowel incarcerated, but no intestinalresection required). He was treated with broad-spectrum intravenous antibiotics for pneumonia.He then developed increasing abdominal disten-tion and increasing leukocytosis (maximum whiteblood cell count 80,000u/L) and obstipation.Abdominal radiographs confirmed evidence of in-testinal ileus and abdomen/pelvis computed to-mography (CT) imaging confirmed pancolitisand ascites (Fig 1). Laboratory testing confirmedClostridium difficile, and medical management was
d for publication January 25, 2017.
requests: Lena M. Napolitano, MD, FACS, FCCP,Acute Care Surgery and Trauma and Surgical Criticalniversity of Michigan Health System, Room 1C340-UH,ty Hospital, 1500 East Medical Drive, SPC 5033, AnnI 48109-5033. E-mail: [email protected].
60/$ - see front matter
Elsevier Inc. All rights reserved.
x.doi.org/10.1016/j.surg.2017.01.018
initiated with intravenous metronidazole andenteral and rectal vancomycin. He failed toimprove with medical management and requiredloop ileostomy with antegrade vancomycin instilla-tion. He fully recovered and subsequently under-went closure of ileostomy without complication.
As in this patient case, C difficile infection (CDI)is a common problem in surgical patients and canpresent with ileus and obstipation or with diarrhea.We provide an update regarding diagnosis, epide-miology, pathogenesis, and clinical treatment inthis review.1,2
EPIDEMIOLOGY
It has been conservatively estimated that CDI isresponsible for over 500,000 enteric infections, themajority of which are hospital acquired.3 Over thepast decade, there has been a significant increasein both the incidence and economic burden asso-ciated with CDI. Estimates of the annual economicburden ranges from $436 million to $3 billion dol-lars in the United States.4-7 The morbidity associ-ated with this disease process is significant, with
SURGERY 1

Fig 1. CT scan of abdomen/pelvis. Scout with colonic ileus (A). Marked diffuse colonic wall thickening (B, C, and D)compatible with infectious pancolitis. Asictes, moderate to large amount (C). No pneumatosis, no free intraperitonealgas. Patent central mesenteric vessels without portal venous gas. No intra-abdominal abscess.
ARTICLE IN PRESSSurgeryj 2017
2 Napolitano and Edmiston
more than 9% of hospital admissions for CDI re-sulting in death.8
In the United States, C difficile is the mostfrequently reported health care–associated path-ogen, and CDI rates continue to rise.9,10
Community-associated CDI is also increasing, anddisease onset outside of the hospital setting hasincreased as well. Nursing home–onset CDI sawapproximately 113,000 infections in the UnitedStates in 2012, representing approximately one-quarter of all US CDI cases, and was associatedwith a 19% recurrence rate and 8% 30-day mortal-ity rate.11
Epidemiologic data document that CDI isincreasing in US surgical patients and is mostprevalent after emergency operations and intesti-nal resection.12 In 2006–2010, compared with theprior 5 years, the C difficile colitis rate increasedby 47%, and a 32% increase in the rate of colecto-mies for CDI was noted in the Nationwide Inpa-tient Sample.13
The spectrum of CDI ranges from mild diarrheato toxic megacolon, fulminant colitis, colonicperforation, multiple organ failure, and ultimatelydeath.14 Patients with severe CDI manifest a severesystemic inflammatory response, which differs
significantly from mild/moderate infection.15
The majority of all-cause gastroenteritis deathsare associated with CDI.16 Infection with C difficileis an independent predictor of increased intensivecare unit and hospital duration of stay, totalcharges, and mortality rate after operative careand represents a considerable burden to both pa-tients and hospitals.
There has also been a significant increase inmorbidity and mortality related to CDI, in partrelated to new hypervirulent strains (C difficile BI/NAP1/027 clones that produce binary toxin [Cdifficile transferase toxin] in addition to toxins Aand B), causing increased mortality and increaseduse of colectomy since CDI was refractory to med-ical management. The BI/NAP1/027 strain ischaracterized by high-level fluoroquinolone resis-tance, efficient sporulation, markedly high toxinproduction,17,18 and a mortality rate 3-fold higherthan less virulent strains, such as the 001 or 014 ri-botypes.19,20 Rates of CDI caused by BI/NAP1/027remain high in the United States, where 28.4% of2,057 recent C difficile isolates were NAP1.21 It isimportant to understand C difficile epidemiologyand transmission because it has a significantimpact on the clinical management of CDI.22

Table I. Risk factors for initial, recurrent, severe, and BI/NAP1/027 CDI
Initial CDI Recurrent CDI Severe CDI BI/NAP1/027 CDI
Antibiotic exposureIncreased patient agePrior hospitalizationSeverity of underlying illnessProton pump inhibitors and
H2 blocker useAbdominal operationNasogastric tubeLong duration of
hospitalizationLong-term care residencyIBDOrgan transplantationChemotherapyChronic kidney diseaseImmunodeficiency
Any prior episodes of CDIAdditional antibiotic useAdvanced ageProlonged or recent stay inhealth care facility
High severity of Horn Indexfor underlying illness
Proton pump inhibitor useInfection with NAP1/BI/027strain type
Absence of an antitoxin Aantibody response
Absence of an antitoxin Bantibody response
White blood cell count>15,000/mL
Serum creatinine levelgreater than 1.53 baseline
Low serum albumin levelIncreased C-reactive proteinlevel
Infection with NAP7-8-9/BK/078 and NAP1/BI/027 C difficile strains
Age >65 yearsFluoroquinoloneantibiotic exposure
Adapted from Gerding et al.148
ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 3
HISTORY
The first description of a C difficile–associateddisease (CDAD)-like process was recorded in a sur-gical patient at Johns Hopkins University in 1892.23
The patient was a 22-year-old woman who under-went operative care by Dr William Osler for resec-tion of a tumor in the gastric pylorus. Early in thepostoperative period, she developed severe diar-rhea and died on the 15th postoperative day. Thepostmortem revealed a pseudomembranous “diph-theritic membrane” in the small bowel which uponcytological examination presented with the key in-flammatory features of CDAD.
After the introduction of antibiotics in the late1940s and early 1950s, case reports of pseudo-membranous enterocolitis became much morenumerous with Staphylococcus aureus implicated asthe causative organism based up routine stool cul-tures.24,25 In 1974, clindamycin was linked to a se-ries of patients who developed fulminant diarrheawhile being treated for anaerobic infections.26 Ina subsequent prospective study, 21% of patientswho received clindamycin developed diarrheawith 50% of patients demonstrating pseudomem-branous lesions on endoscopy.27 The character-ization of the disease process and toxigenicnature of the pseudomembranous colitis was veri-fied by investigators at the University of Michiganand in the United Kingdom.28,29 Eventually,several investigators were able to isolate C difficilefrom the stool of patients with pseudomembra-nous colitis.30,31
RISK FACTORS FOR CDI
Clinicians must be aware of the risk factors forCDI (Table I), because this will assist them in hav-ing a high index of suspicion in making an earlydiagnosis. Antibiotic use is the most common riskfactor for initial and recurrent CDI.32 Althoughall antibiotics are associated with increased CDIrisk, clindamycin, fluoroquinolones, and second-generation and higher cephalosporins areassociated with the highest CDI risk. Protonpump inhibitors were identified as risk factors insome studies but not confirmed in others.32-35
Other risk factors include increased age, nasogas-tric tube, and kidney disease.36-38
Abdominal operations, specifically colorectaloperations, are a significant CDI risk factor. Arecent study examined risk factors and variationassociated with the development of nosocomialCDI among patients undergoing colorectal resec-tion in New York State from 2005–2013. Of 150,878colorectal resection patients, 3,323 (2.2%) devel-oped CDI. This study documented that colorectalsurgery patients are at high risk for CDI. There wasan approximately 5-fold difference in adjusted CDIrates across hospitals (0%–11.3% among surgeons;0%–6.8% among hospitals), confirming significantvariation unexplained by patient, surgeon, andhospital factors.39
Solid-organ transplant recipients are atincreased risk for hospital-onset CDI, 5-fold higherthan among general medicine patients (209 vs 40per 10,000 hospital discharges from the University

ARTICLE IN PRESSSurgeryj 2017
4 Napolitano and Edmiston
Health System Consortium 2012–2014).40 Furtherefforts to detect, prevent, and manage CDI amongtransplant recipients are needed.41
PATHOGENESIS
The gastrointestinal tract is a complexecosystem exposed to a constant flow of microbialpopulations, many of which transit through thelength of the bowel without establishing residencyor causing disease. This microbial population ofthe gastrointestinal tract represents great geneticand ecologic diversity with an estimated 15,000 to36,000 different species of bacteria residing withinthe lumen and on the mucosal surfaces.42
Clostridia are a heterogeneous group of organ-isms that exist in both the lumen of the bowel andon the epithelial brush-border surface of the largeintestines. C difficile colonizes the intestinal tract inapproximately 1% to 15% of healthy adults, and ithas been estimated that colonization in newbornscan approach 80%, but rarely does the organismcause disease in this population.43,44
In healthy adults, the intrinsic combination of acompetent (intact) normal intestinal flora and theproduction of antibodies to toxin A protect againstC difficile colonization and infection. Antitoxin IgGhas been found to be more common in asymptom-atic carriers than patients with active disease.45,46 Ithas been hypothesized that individuals who arecolonized early in life most likely develop an im-mune memory, which has a protective effectthrough adulthood but wanes in the sixth or sev-enth decade.
Microbial virulence. The principal virulencefactors (Table II) associated with CDAD are 2 largemolecular weight cytotoxins, toxin A and toxin B,which have enterotoxigenic and cytotoxic activity.Both toxins can cause significant colonic inflamma-tion and disruption of the epithelial mucosal sur-face. These toxins are coded in the region of thegenome called the pathogenicity locus (PaLoc).
The mechanistic action of toxin A (TcdA) and B(TcdB) most likely begins with the binding of thetoxin C-terminus to one or more target receptorspresent on the colonic epithelial cell surface.Upon binding to the receptor, the toxins are endo-cytosed, where the toxins are acidified prior totranslocation into the cell cytosol.47 Once insidethe cell, a host cytoplasmic inositol hexaphosphateinduces autocleavage of the toxin mediated by a Cdifficile asparate protease, resulting in a biologicallyactive toxin.48 Upon entry into the cell, the toxinstarget Rho GTPases, which play a central role in amultitude of cellular processes, including
organization of the actin cytoskeleton, controllingepithelial barrier function, and the signaling andmotility of host immune cells.49
The cumulative effect of this intoxication is theeventual loss of the intestinal barrier function. Thenormal tight junctions between individual epithe-lial cells are disrupted, allowing the migration ofcells, such as neutrophils, into the intestines,which play a role in the inflammatory responsethat is typically seen with colitis. The loss-of-barrierfunction leads to increased intestinal permeabilityand fluid accumulation followed by diarrhea.50
Two additional genes, which are not on thePaLoc, encode the binary toxin. Another potentialvirulence loci includes slpA, a gene that codes theS-layer proteins (adherence and inflammatorystimulation); genes that code for the extracellularmatrix-binding domain; a collagen protease gene;a gene for the surface anchor protein requiredfor covalent attachment to peptidoglycan; a pilusbiosynthesis locus involved in fimbrial biosynthesis;and a cluster of genes involved in extracellularpolysaccharide synthesis.51 The nontoxigenic Cdifficile strains lack the PaLoc gene locus.
In 2003, a severe outbreak of CDAD occurred inboth the United States and Canada, which wascaused by a clone that was designated as BI/NAP1/027. Studies have demonstrated that thisstrain (027) produces both toxins A and B fasterand in large quantity (hyperproduction). Theseclones are also capable of producing an actin-ADP-ribosylating toxin, called binary toxin (C difficiletransferase toxin), which is not encoded on thePaLoc and contributes to CDAD by cytotoxic activ-ity, inducing the formation of thin microtubuleson the outer surface of the epithelial cell (colono-cyte), leading to increased clostridial adherence.49
This strain also expresses resistance to the fluoro-quinolones, levofloxacin, and moxifloxacin. Inmany geographical areas of the United States,B1/NAP1/027 accounts for >50% all strains recov-ered from CDI.52,53
An interesting finding in a recent study foundthat isolates recovered from relapse cases show asignificantly higher germination rate compared toisolates recovered from single cases.54 Whether thishigher germination rate has an impact on diseaserecurrence is unknown. Although our primaryknowledge of the microbial virulence of C difficilehinges on deciphering the genetic components ofthe PaLoc and its toxigenic variations, other viru-lence factors, such as adherence and motility, arelikely to emerge as we further probe the biology ofthis significant health care pathogen.

Table II. Selective microbial virulence factors for Clostridium difficile
Virulence factor Target effect on host cells
Toxin A (PaLoc-TcdA gene) Cytotoxic loss of gastrointestinal cell barrier functionToxin B (PaLoc-TcdB gene) Synergistic interaction with toxin AVariant toxin A–/B+ Cardiotoxic-multiorgan failureBinary toxin Increases clostridial adherence to intestinal cell surface–fluoroquinolone resistanceS-layer protein Gene encoding cell surface adherence/stimulates inflammationS-anchor protein Mediates covalent attachment to cell wall peptidoglycanSporulation/germination Outer spore coat protein that induces inflammation
Adapted from Badger et al.2
ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 5
DIAGNOSIS AND LABORATORY TESTING
The diagnosis of CDI requires rapid and accu-rate technologies for individual patient manage-ment and prevention of nosocomial transmission.Accurate diagnosis of CDI relies on a combinationof clinical history and laboratory tests.55 Anaerobicculture of C difficile from stool remains a sensitivemethod for diagnosis, but acquisition of C difficilealone does not diagnose CDI because 4% ofhealthy adults may carry this organism in theirnormal intestinal flora and 20% to 25% of C diffi-cile strains may be nontoxigenic. Toxigenic culturetesting from anaerobic culture remains the goldstandard for laboratory diagnosis owing to itshigh sensitivity (94%–100%) and high specificity(99%). While extremely sensitive and specific,the toxigenic culture test is time consuming andlaborious, taking 2 to 5 days.56
Enzyme immunoassays (EIAs) for toxins A and Bhave been a popular laboratory practice because thetests are simple to perform and results are availablewithin 2 to 6 hours. EIAs are relatively inexpensive,easy to perform, and can provide accurate, rapidresults. However, performance of EIAs can varywidely by product and can also be affected byprotocol deviations, improper technique, or spec-imen handling. EIA sensitivity is 63% to 99%, andfalse-negative results can occur.57-60 EIAs should notbe used as an indicator of response to therapy,because results remain positive for extended pe-riods in 25% of successfully treated patients.
A second EIA targets the C difficile common an-tigen, glutamate dehydrogenase (GDH), which issecreted by C difficile into the stool.61 GDH is anenzyme (present in most microbes) that convertsglutamate to a-ketoglutarate. GDH is not specificto C difficile, and its presence does not confirmthe presence of a strain of C difficile containingthe PaLoc locus. However, the absence of GDHfrom stool is strongly predictive of the absence ofC difficile, making it a potential screening assay.GDH-positive specimens are then confirmed using
an assay that specifically detects toxin or the toxingenes (polymerase chain reaction [PCR]).
Nucleic acid amplification (NAAT) is the newestcommercially available method for the diagnosis ofCDI. Current NAATs are formatted in PCR, DNAmicroarray, and loop-mediated isothermal amplifi-cation methods. A result (positive or negative) isreported within 2 hours. NAAT sensitivity rangesfrom 84% to 96% and specificity ranges from 94%to 99% depending on the gold standard used.62,63
The 2010 Society forHealthcareEpidemiology ofAmerica (SHEA) guidelines established specimencollection requirements and recommendations foroptimal C difficile testing based on existing evi-dence.64 The SHEA guidelines recommend that Cdifficile testing only be performed on diarrheal (un-formed) stool, unless ileus due to CDI is suspected.The proper stool specimens should be watery andtake the shape of the collection container. Althoughswab specimens are not considered acceptable,newer molecular probe technology is in develop-ment that will allow swab samples to be analyzed inthe future. Testing of formed stools and asymptom-atic patients is discouraged because a significantproportion of the hospitalized population will becolonized with C difficile.
A recent study has documented that exclusiverelianceonmolecular tests forCDIdiagnosis withouttests for toxin or host response is likely to result inoverdiagnosis, overtreatment, and increased healthcare costs.65When the current SHEAguidelineswerepublished, the optimal method with sufficientevidentiary support for C difficile testing was a 2-stepalgorithm combining GDH with toxin EIA testing.The addition of GDH as a screen increased the sensi-tivity for C difficile but alone was not specific enoughto sufficiently exclude nontoxigenic strains. This ledto the development of the 2-step algorithm whereinGDH-positive specimens are confirmedusing a toxinEIA or C difficile NAAT (Fig 2).
An additional challenge of selecting C difficiletesting is an increasing requirement for public

Fig 2. Recommended C difficile diagnostic testing. Reprinted with permission from Martin et al.22
ARTICLE IN PRESSSurgeryj 2017
6 Napolitano and Edmiston
reporting of C difficile rates. A potential downside ofpublic reporting is a lack of adjustment for case mixand testing methodology.66 Institutions that have im-plemented PCR screening forCdifficilehave reported2- to 3-fold increases in CDI positivity rates. If publicreporting does not allow for rate adjustments basedon testing methodology and population prevalence,
hospitals may be disadvantaged when performingthe most sensitive testing methodologies.
RADIOLOGIC DIAGNOSTIC IMAGING
Diagnostic imaging can assist in making an earlydiagnosis of CDI. Plain radiography of theabdomen can demonstrate polypoid mucosal

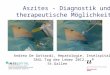
Fig 3. Radiologic diagnostic CT imaging findings in patients with CDI. (A) Accordion sign in 50-year-old woman with Cdifficile colitis. Marked submucosal edema is present in the right colon (“thumbprint” appearance on longitudinal axis,short arrows). Oral contrast material (arrowhead) is trapped within the lumen. Reprinted with permission from Macariet al.67 (B) Target sign in a 65-year-old woman with C difficile infection, with CT through the midabdomen showingdiffusely thickened colonic wall appearing as a “target sign” (concentric circles formed by the layers of bowel wall in in-flammatory disease) on axial imaging (arrow). Reprinted with permission from Ash et al.68 (C) Pneumatosis intestinalisin a 76 year old who underwent esophagectomy and splenectomy for adenocarcinoma and developed ileal C difficile en-teritis requiring small bowel resection, ultimately died. Reprinted with permission from Wee B et al.69
ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 7
thickening, “thumbprinting” (wide transversebands associated with haustral fold thickening),or gaseous distention of the colon (ileus). CT scanimaging is most commonly used to evaluatepatients with CDI to determine the severity ofdisease. Common CT findings include wall thick-ening, low-attenuation mural thickening corre-sponding to mucosal and submucosal edema, the“accordion sign,” the “target sign” (“double halosign”), pericolonic stranding, and ascites (Fig 3).70
Pneumatosis intestinalis (affecting both the smalland large intestine) has also been reported in pa-tients with CDI.71-73 Familiarity with these imagingcharacteristics may allow early diagnosis and treat-ment and prevent progression to more seriouspathologic conditions.
CLINICAL PRESENTATION
Acquisition of C difficile, like most enteric patho-gens, results in a wide spectrum of clinical manifes-tations including intracolonic and extracolonic.The clinical features can vary from asymptomatic
presentation to fulminant colitis and peritonitisdue to perforation of the colon.
Intracolonic disease manifestations. Asymptom-atic carriers. Most individuals who are culture pos-itive for toxin producing C difficile areasymptomatic carriers. Asymptomatic carriage isvery common in hospitalized patients. Symptom-atic disease is less often seen in carriers despitethe observation that most C difficile isolates exhibittoxin production. Asymptomatic carriage can beinfluenced by certain clinical factors, such asrecent antibiotic exposure or previous occurrenceof CDAD.74,75
C difficile diarrhea. This manifests as mild tomoderate diarrhea, often associated with crampsand abdominal pain. Although patients will oftenexhibit malaise and fever, it is not a commoncomponent of disease presentation. Symptomsusually occur during or shortly after antibiotictherapy but sometimes may be delayed for severalweeks. C difficile toxins are normally detected instool samples even though endoscopic and

ARTICLE IN PRESSSurgeryj 2017
8 Napolitano and Edmiston
histologic features may be normal in patients withmild disease.76
C difficile colitis. This is the most commonclinical manifestation of CDI. This is generally amore serious illness, and patients present withmild to moderate abdominal pain, nausea,anorexia, and watery diarrhea. Dehydration, low-grade fever, and systemic polymorphonuclearleukocytosis may occur in selected patients. Anonspecific diffuse or patchy erythematous colitiswithout pseudomembranes may be seen withsigmoidoscopy.77
Pseudomembranous colitis. Symptoms of pseudo-membranous colitis are similar to C difficile colitisbut often more severe. Diarrhea is often profuse,and patients have intense abdominal pain (left orright lower quadrants). Endoscopy will often revealpseudomembranes that appear as raised yellowplaques, measuring about 2 to 10 mm in diameter,scattered over the colorectal mucosa. Most patientswith pseudomembranous colitis have involvementof the rectosigmoid colon, and many will alsohave involvement of the proximal large bowel.There is often marked leukocytosis (white bloodcell count >20,000), and hypoalbuminemia of3.0 g/dL or lower may be observed in severely illpatients.78
Fulminant colitis. Fulminant colitis (FC) is themost feared presentation of CDI and occurs in 2%to 3% of patients. FC accounts for most of theserious CDI complications, including ileus, mega-colon, colonic perforation, and death.79 In somecases, patients presenting with benign symptomswill suddenly and rapidly progress to shock.Contributory factors associated with diseaseseverity and patient death include age, immunestatus, patient comorbidities, microbial virulencefactors, and perhaps antimicrobial resistance.80
Patients with FC complain of severe lowerquadrant or diffuse abdominal pain, distensionand diarrhea, or ileus. Diarrhea is minimum inpatients with ileus, since secretions accumulate inthe dilated atonic colon. FC may lead to toxicmegacolon. The small bowel can also exhibitdilated segments with air-fluid levels simulatingintestinal obstruction or pseudo-obstruction. Thehigh morbidity and mortality associated with FCcan be mitigated by early aggressive diagnosis andtherapy.
Recurrent CDI. Recurrent CDI manifests as reap-pearance of diarrhea/ileus and abdominal symp-toms usually within a few weeks after completion oftreatment for CDI.81 The pathophysiology ofrecurrent CDI has not been well described, but itis likely related to a persistently altered fecal flora
in combination with C difficile sporulation and animpaired host immune response to C difficileand/or its toxin. Recurrent CDI develops inapproximately 5% to 20% of patients treated forCDI. In older patients, acute confusion or alteredmental state may be the first symptom of recurrentCDI. Other nonspecific signs of infection mayinclude weakness and lethargy, frequent falls,anorexia, and loss of physical functional capacity.5
Extracolonic disease manifestations. Extraco-lonic manifestation of CDI in a variety of organsystems includes small bowel infection, bacteremia,reactive arthritis, and other infectious processes(cellulitis, necrotizing fasciitis, and osteomyelitis).Small bowel CDI is often seen after a previousoperation and is associated with high mortality andis also observed in patients with inflammatorybowel disease (IBD) who have undergone totalcolectomy.
Impact of CDI in IBD. Current clinical andepidemiologic findings document a significantincrease in the burden of CDI in the IBD patientpopulation over the last decade. One study re-ported that the rate of CDI-IBD-associated CDI as aproportion of institutional burden increased from7% in 2005 to 16% in 2006 (P < .01). The majorityof patients contracted CDI as outpatients. Anti-biotic exposure in the CDI-IBD patients was foundto be 61%. Univariate and multivariate analysis re-vealed that maintenance immunomodulation andcolonic involvement were independent risk factorsfor CDI.4
In a retrospective study of CDI in IBD patientsover 7 years, there was a doubling of CDI inCrohn’s patients (9.5 to 22.3/1,000 admissions)and a tripling of CDI in ulcerative colitis patients(18.4 to 57.6/1,000 admissions).82 In a study of pa-tients who underwent colectomy for severe ulcera-tive colitis, many developed high-volume ileostomyoutput (clostridial toxin positive), fever, leukocy-tosis, and ileus in the postoperative period.83 Indata obtained from the US Healthcare Cost andUtilization Project Nationwide Inpatient Sample,hospitalized patients with concurrent CDI andIBD had a 4-fold or greater risk of mortality thanpatients admitted for either CDI or IBD alone.CDI-IBD patients also had longer hospital staysand a higher rate of gastrointestinal operationsand endoscopic evaluations than patients withCDI alone.6
IBD patients who acquire CDI share many of therisk factors (environmental acquisition, prior anti-biotic exposure, immunosuppressive therapy, andgastric acid suppressive therapy) associated withnon–IBD patient populations. An interesting

ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 9
epidemiologic finding associated with CDI acqui-sition in IBD patients is that in the majority(>75%) of IBD patients, C difficile acquisition oc-curs in the community.84 This is in direct contrastto many of the CDIs that are acquired within thehospital environment. The reason for this findingis unknown.85
A recent study suggested that a subset of IBDpatients in remission has a higher carriage rate ofC difficile than healthy individuals, and that C diffi-cile carriage appears unrelated to antibiotic expo-sure or immunosuppressive therapy.86 The roleof immunomodulation may be a significant riskfactor in IBD patients because these drugs (azathi-oprine, 6-mercaptopurine, methotrexate, and in-fliximab) have all been associated with anincrease in CDI in IBD patients, with almost 50%of the patients taking 2 immunosuppressive agentsfor maintenance therapy.87
IBD patients may develop C difficile enteritis andC difficile pouchitis. C difficile small bowel enteritis israre but associated mortality is high (60%–83%).83,86 The clinical presentation includes diar-rhea followed by ileus with fluid-filled loops ofsmall bowel and sepsis. C difficile associated pouchi-tis is responsive to medical management.88,89 Po-tential treatment with inhibitory bile acids maybe a future nonantibiotic therapy for CDI pouchi-tis, as the restoration of secondary bile metabolismmay be the key mechanism underlying the successof fecal microbiota transplantation in treatingrecurrent CDI.90 Clinicians should have a high in-dex of suspicion of postoperative CDI in any pa-tient who has a history of IBD, particularly withhistory of CDI prior to colectomy. Most patientswill respond to rapid and aggressive therapy.
MEDICAL TREATMENT STRATEGIES
Initial management of CDI should always bediscontinuation of antimicrobial agents that mayhave led to CDI. Antibiotic treatment of CDI is themainstay of therapy, and specific antibiotic treat-ment guideline recommendations are based onthe severity of CDI disease. Although initial sys-tematic reviews documented that no antimicrobialagent was clearly superior for the initial cure ofCDI,91 additional analyses stratified by diseaseseverity identified that vancomycin providedimproved initial clinical and sustained cure ratesin patients with severe CDI compared with metro-nidazole.92 In a study of quantitative bacterial cul-tures of fecal samples, vancomycin treatmentconsistently reduced C difficile counts to the limitof detection, whereas metronidazole was associated
with C difficile counts 1.5 to 2 log higher at 10 daysof treatment.93 Based on these results, vancomycinis considered first-line therapy for severe andcomplicated CDI (Table III).94
Additional antimicrobials that have potentialefficacy for CDI treatment include rifaximin,tigecycline, ramoplanin, and nitazoxanide.95 Smalltrials of these agents have been encouraging, butadditional studies are warranted.
Fidaxomicin. Fidaxomicin is a member of anew class of antibacterials (macrocycles) and hasbeneficial properties, including in vitro activity 8times greater than vancomycin against clinical Cdifficile isolates,96 minimal systemic absorption,97
and limited activity against the normal gutflora.98 Based on data from 2 phase 3 trials(n = 1,164), clinical cure rates were similar for fi-daxomicin and vancomycin, but CDI recurrence(relative risk [RR] 0.47, 95% confidence interval[CI] 0.34–0.65) was significantly lower and sus-tained cure rates (RR 1.75, 95% CI 1.35–2.27)were significantly higher for fidaxomicin thanvancomycin.99-101 A significant limitation of fidax-omicin compared to other antibiotics for CDI isits high cost.
Intravenous immunoglobulin. Intravenousimmunoglobulin is another potential treatmentstrategy for CDI. Few case reports are available,and current guidelines state the following: “Intra-venous immunoglobulin may be helpful in pa-tients with hypogammaglobulinemia (strongrecommendation, low quality of evidence)”---seeAJG guideline, page 488, right column.102
Monoclonal antibodies. Antibody-based immu-notherapies for CDI are emerging.103 Monoclonalantibodies active against toxins A and B adminis-tered by intravenous (IV) infusion were superiorin reducing rates of recurrent CDI when adminis-tered with antibiotics compared to antibioticsalone (7% vs 25% recurrent CDI) in a phase 2 ran-domized controlled trial that enrolled 200 adultpatients with CDI.104 The mechanistic basis ofthe monoclonal antitoxin antibodies is throughdirect neutralization of the toxins and does notappear to involve host effector functions.105
Bezlotoxumab,106 a fully human monoclonalimmunoglobulin G1/kappa antibody that bindsto and neutralizes C difficile toxin B, was an effica-cious adjunctive therapy for the prevention ofrecurrent CDI. Two global, phase 3, double-blindstudies were conducted to evaluate bezlotoxumab,either alone or in combination with actoxumab (afully human monoclonal antibody against C difficiletoxin A), compared to placebo for the prevention

Table III. Medical treatment recommendations for CDI based on severity of illness
Severity Treatment
Mild/moderate CDI Mild/moderate CDI
Diagnosis of CDI andNone of the criteria in “severe” or “complicated” CDI
Metronidazole 500 mg PO TID for 10–14 days
In patients with metronidazole allergy, pregnant, nursing,
or on warfarin therapy:
Vancomycin 125 mg PO QID for 10–14 days
Severe CDI Severe CDI
WBC $15KCr $ 1.53baselineAge $65 yearsANC #500ALB #2.5 g/dLSOT/BMT <100 daysChronic GVHD (BMT)Treatment of rejection in the preceding 2 months (SOT)Small bowel CDI
Vancomycin 125 mg PO QID for 10–14 days
Complicated CDI Complicated CDI
Septic shock–sepsis with persistent hypotension, requiring
vasopressors to maintain MAP $65 mm Hg and serum
lactate level >2 mmol/L despite adequate fluid
resuscitation
Sepsis–life-threatening organ dysfunction caused by a
dysregulated host response to infection. Suspected or
documented infection and an acute increase of $2
SOFA points
Ileus or bowel obstruction
Toxic Megacolon
Peritonitis
Bowel perforation
Vancomycin 500 mg PO QID
Metronidazole 500 mg IV every 8 hours, and
Vancomycin enema 500 mg in 1,000 mL of normal saline
every 8 hours (in patients with ileus, bowel obstruction
or toxic megacolon).
Consult infectious diseases and surgery to assist in man-
agement including possible surgical intervention.
Operative management strategies for CDI may include
exploratory laparotomy, diverting loop ileostomy with
lavage, total or subtotal abdominal colectomy with end
ileostomy.
ANC, Absolute neutrophil count; ALB, albumin; BMT, bone marrow transplant; Cr, serum creatinine; GVHD, graft versus host disease; MAP, mean arterialpressure; SOFA, sequential organ failure assessment; SOT, solid organ transplant; WBC, white blood cell count.
ARTICLE IN PRESSSurgeryj 2017
10 Napolitano and Edmiston
of recurrent CDI in patients on standard of careantibiotics for a primary or recurrent CDI. TheMODIFY (monoclonal antibodies for C difficiletherapy) I study enrolled 1,452 patients (medianage 65 years) in 19 countries, and the MODIFY IIstudy enrolled 1,203 patients (median age 67 years)in 17 countries. The studies were conducted inboth hospital and outpatient settings, and the pri-mary end point for each study was evaluatedthrough 12 weeks after study drug administration.
In the MODIFY I study, patients receivingstandard-of-care antibiotics for C difficile were ran-domized to receive a single, 1-time infusion ofeither bezlotoxumab (10 mg/kg) (n = 403), actox-umab (10 mg/kg) (n = 242), the combination of
bezlotoxumab and actoxumab (10 mg/kg each)(n = 403), or placebo (n = 404). The actoxumabarm was stopped for efficacy and safety reasons af-ter an interim analysis. In the MODIFY II study, pa-tients receiving standard-of-care antibiotics for Cdifficile were randomized to receive a single, 1-time infusion of either bezlotoxumab (10 mg/kg) (n = 407), bezlotoxumab and actoxumab(10 mg/kg each) (n = 397), or placebo (n = 399).
In both MODIFY I and MODIFY II, the rate ofCDI recurrence through week 12, the primaryefficacy end point, was significantly lower in thebezlotoxumab arms (17.4%, P = .0003) and(15.7%; P = .0003) and the combination bezlotox-umab and actoxumab arms (15.9%, P < .0001) and

ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 11
(14.9%, P < .0001) compared to the placebo arms(27.6%) and (25.7%), respectively. In both studies,the rate of CDI recurrence was lower in the bezlo-toxumab arms compared to the placebo arms inpatient subgroups known to be at high risk forCDI recurrence, including patients with any priorepisodes of CDI within the previous 6 months, pa-tients infected with the BI/NAP1/027 strain, pa-tients with severe CDI (Zar score $2), patients65 years of age or older, and patients with compro-mised immunity.
These subpopulation analyses were prespecifiedin the protocol for each study. Rates of seriousadverse reactions and deaths assessed through12 weeks after infusion were comparable across thetreatment arms. Treatment with the combination ofbezlotoxumabandactoxumabdidnotprovideaddedefficacy over bezlotoxumab alone. Furthermore,actoxumab alone provided no benefit in the preven-tion of CDI recurrence compared with placebo.
Clinical cure of the initial CDI episode, how-ever, was lower for both actoxumab/bezlotoxumab(74.7%; P = .0057) and bezlotoxumab (77.5%;P = .0622) compared with placebo (82.8%) inMODIFY I. In MODIFY II, clinical cure of theinitial CDI episode was numerically lower for ac-toxumab/bezlotoxumab (72.3%) compared withplacebo (77.8%). In contrast, clinical cure wasnumerically higher for bezlotoxumab (82.5%)compared with placebo. Neither of these compari-sons was statistically significant (P = .0801 andP = .0973, respectively).
Based on these results, bezlotoxumab (admin-istered IV as a single dose of 10 mg/kg over1 hour) was recently approved by the Food andDrug Administration (FDA) for the prevention ofCDI recurrence in patients aged 18 years or olderwho are receiving antibacterial drug treatment forCDI.107,108
Vaccines. Despite numerous scientific and oper-ational challenges, there are vaccine candidates inlate-stage clinical development for CDI, and 3 Cdifficile vaccines have progressed to phase 2/3 clin-ical trials.109 Some observations suggest that recur-rent CDI is associated with failure to develop anadequate immune response to C difficile toxins. Im-munization could therefore be beneficial in high-risk patients.
A phase 3 clinical trial with an estimatedprimary completion date of December 2017 isevaluating a vaccine (Cdiffense) that containstoxins A and B for induction of an immuneresponse against toxins A and B.110 The Cdiffensestudy is enrolling 2 patient cohorts: (1) those whohave had at least 2 hospital stays and received
systemic antibiotics in the 12 months prior toenrollment and (2) those scheduled for an inpa-tient hospitalization (>72 hours) for a plannedoperative procedure (kidney, bladder, urinary sys-tem, musculoskeletal system, respiratory system,circulatory system, central nervous system) within60 days of enrollment. Patients will be randomizedto the C difficile vaccine at days 0, 7, 30 or to normalsaline placebo.
TheEuropeanUnion is funding a 3-year initiativeto develop anoral (sublingual)Cdifficile vaccine; theintended strategy is to use harmless bacterial sporesthat carry the antigen and boost immunity by target-ing the protein needed for the infection to takehold.111 The candidate C difficile vaccine has beenwell tolerated by patients. To date, no C difficile–tar-geted vaccine has been approved by the FDA,although an agent is currently under clinical devel-opment by Pfizer Inc (PF-06425090).112,113
NEW AND EMERGING MEDICAL TREATMENTSTRATEGIES
New approaches to CDI prevention and treat-ment are needed (Fig 4). Antibiotics under devel-opment include cadazolid and ridinilazole.Surotomycin has had disappointing phase 3 re-sults. Multiple live biotherapeutics are being devel-oped, including freeze thawed and encapsulatedversions of fecal microbiota transplantation toimprove the practicality of treating patients withrecurrent CDI. Alternatives to fecal microbiotatransplantation that aim to improve safety,including a microbial suspension (RBX2660) anda complex spore formulation (SER-109), have pro-gressed to phase 2 studies. A nontoxigenic C diffi-cile strain has also shown promise to preventrecurrent CDI.114,115
OPERATIVE TREATMENT STRATEGIES
Operative consultation should be consideredearly in the course of severe and complicated CDI(Fig 5), as operative consultation may be benefi-cial.116,117 High mortality rates have been reportedwith operative treatment for CDI, likely related tosignificant delay in operative intervention,118 butoperative therapy for severe CDI can indeed belifesaving. A systematic review of 510 patients withfulminant C difficile colitis reported decreased mor-tality comparing operative treatment with medicaltherapy (RR 0.70, 95% CI 0.49–0.99).119
Subtotal colectomy, end ileostomy with preser-vation of rectum has been a standard recommen-ded operative treatment, particularly for fulminantcolitis. A systematic review of 31 studies (n = 1,442)

Fig 4. Emerging strategies for the prevention and treatment of primary and recurrent CDI. NTCD, Nontoxigenic Clos-tridium difficile. Reprinted with permission from Kociolek et al.114
ARTICLE IN PRESSSurgeryj 2017
12 Napolitano and Edmiston
of patients undergoing emergency operation forCDI documented that 1.1% of all patients withCDI and 29.9% with severe CDI underwent emer-gency operation. The most commonly performedoperation was total colectomy with end ileostomyin 89% of patients. In patients who underwent par-tial colectomy, reoperation to resect additional co-lon was required in 15.9% of patients. The 30-daymortality rate was high (41.3%), and the strongestpredictors of postoperative death were preopera-tive intubation, acute renal failure, multiple organfailure, and shock requiring vasopressors.120
A review of the Nationwide Inpatient Sample2001–2010 documented over 2.7 million dis-charges with a diagnosis of CDI in the UnitedStates over this decade, and colectomy was per-formed in 19,374 cases (0.7%), with an associatedmortality of 30.7%. Predictors of mortality aftercolectomy included coagulopathy, age >60 years,acute renal failure, respiratory failure, sepsis, pe-ripheral vascular disease, and congestive heartfailure. Importantly, operative treatment morethan 3 days after admission was associated withhigher mortality rates.13
Similarly, a review of the American College ofSurgeons National Surgical Quality ImprovementProgram database from 2005–2010 identified 335open colectomies for CDI with an overall mortalityrate of 33% and a median time to death of 8 days.Risk factors for postoperative mortality includedage >80 years, preoperative shock, preoperativedialysis dependence, chronic obstructive pulmo-nary disease, thrombocytopenia, coagulopathy,and renal insufficiency.121
Recent experience with a minimally invasive,colon-preserving approach as an alternative tototal colectomy has proven to be successful inselect patients. Diverting loop ileostomy andcolonic lavage followed by intravenous metronida-zole and vancomycin administered via the efferentlimb of the ileostomy (n = 42) is an accepted alter-native to total colectomy in the treatment of severecomplicated CDI with reduced mortality (19% vs50%) compared to a historical total colectomycohort (n = 42) in a single-institution (Universityof Pittsburgh) report.122
This strategy led to colon preservation in 39/42patients; 3 patients subsequently required total

Fig 5. Surgical consultation and treatment strategies for CDI. (From Brian S. Zuckerbraun MD, University of Pittsburgh.)
ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 13
colectomy, either for abdominal compartment syn-dromeor for continued sepsis. The advantage of thisapproach is that it can be considered early if patientsare failingmedical management, and it can be donelaparoscopically in many patients. This approach,however, should not be considered in patients withabdominal compartment syndrome or concern forcolonic ischemia, necrosis, or perforation (Fig 6).
National and international guidelines recom-mend total abdominal colectomy with endileostomy and preservation of rectum. Diverting
loop ileostomy and colonic lavage followedby intravenous metronidazole and vancomycinadministered via the efferent limb of the ileos-tomy should be considered as an alternative tototal colectomy in selected patients (Table IV).The 2014 Eastern Association for the Surgery ofTrauma practice management guidelines foroperative treatment of CDAD strongly recom-mended that adult patients with CDI undergoearly operative care, before the development ofshock and need for vasopressors, and

Fig 6. Operative management strategy for CDI. (From Brian S. Zuckerbraun MD, University of Pittsburgh.)
ARTICLE IN PRESSSurgeryj 2017
14 Napolitano and Edmiston
conditionally recommended total or subtotal co-lectomy (versus partial colectomy or other opera-tion) as the procedure of choice.
If the diverting loop ileostomy and coloniclavage procedure are planned, it is important tohave an institutional protocol to facilitateprompt performance of this procedure becausethe supplies required may not be readilyavailable in the operating room. We have createda 1-page document that allows our operatingroom staff to obtain all supplies needed andprovides the steps of the operative intervention
in a clear, concise approach to achieve successwith this operative procedure (Fig 7).
SMALL BOWEL CDI
Small bowel involvement in CDI (enteritis) isuncommon; however, increasing case reports andseries have been published, some leading to fataloutcome. Small bowel CDI is more commonlyassociated with abdominal operations and particu-larly among patients with IBD and with totalabdominal colectomy.85 CT imaging features ofCDI of the small bowel include mesenteric or

Table IV. Guideline recommendations for operative management of CDI
Guideline Operative consultation recommended Operative treatment
SHEA/IDSA Guidelines 201066 “Severely ill patient” Subtotal colectomy, end ileostomywith preservation of rectum
American College ofGastroenterology (ACG)Guidelines 2013102
Surgical consultation should besolicited in all severe-complicatedCDI cases with 1 or more of thefollowing: hemodynamic instabilityrequiring vasopressors, clinicalsepsis with organ failure, changesin mental status, extremeleukocytosis ($50,000 cells/mL),elevated lactic acid ($5 mmol/L),or evidence of treatment failureafter 5 days of conservative therapy(strong recommendation,moderate quality evidence).
Subtotal colectomy, end ileostomywith preservation of rectum
Diverting loop ileostomy and coloniclavage followed by intravenousmetronidazole and vancomycinadministered via the efferent limbof the ileostomy; alternative to totalcolectomy in selected patients
European Society of ClinicalMicrobiology and InfectiousDiseases (ESCMID) 2014149
Patients with “systemic inflammationand deteriorating clinical conditiondespite maximal antibiotic therapy(with) toxic megacolon, acuteabdomen, and severe ileus”
Subtotal colectomy, end ileostomywith preservation of rectum.Diverting loop ileostomy andcolonic lavage followed byintravenous metronidazole andvancomycin administered via theefferent limb of the ileostomy;alternative to total colectomy inselected patients
EAST Practice ManagementGuidelines 2014150
No recommendation Subtotal colectomy, end ileostomywith preservation of rectum
WSES Guidelines for Management ofClostridium difficile infection insurgical patients 2015151
18) Patients with severe CDI whoprogress to systemic toxicity shouldundergo early surgical consultationand be evaluated for potentialsurgical intervention(Recommendation 1 C).
“patients with fulminant colitis”
19) Resection of the entire colonshould be considered to treatpatients with fulminant colitis (FC)(Recommendation 1 B).
20) Diverting loop ileostomy withcolonic lavage may be a usefulalternative to resection of entirecolon (Recommendation 2 C).
Practice parameters for themanagement of Clostridium difficileinfection. American Society ofColon and Rectal Surgeons,2015152
“There is no high-grade evidenceregarding the optimal
timing of surgical intervention, but itappears that
surgical consultation early in thecourse of disease may bebeneficial.”
Subtotal colectomy with ileostomy istypically the operative procedure ofchoice for C difficile colitis. Grade ofrecommendation: strongrecommendation based on low-quality evidence, 1C.
Diverting loop ileostomy with coloniclavage may be an alternative to totalabdominal colectomy for thetreatment of severe C difficile colitis.Grade of recommendation: weakrecommendation based on low-quality evidence, 2C.
Australasian Society for InfectiousDiseases (ASID) 2016153,154
Indications for surgery are toxicmegacolon, bowel perforation, orsevere deterioration in spite of first-and second-line medical therapy.
Subtotal colectomy, end ileostomywith preservation of rectum.Diverting loop ileostomy andcolonic lavage followed byintravenous metronidazole andvancomycin administered via theefferent limb of the ileostomy;alternative to total colectomy inselected patients
ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 15

Fig 7. Checklist for preoperative and intraoperative preparation at University of Michigan
ARTICLE IN PRESSSurgeryj 2017
16 Napolitano and Edmiston
retroperitoneal fat stranding, ascites, small boweldistention and mural thickening with the terminalileum being the most affected, pneumatosis intesti-nalis (gas within the wall of the small bowel), andintrahepatic portal venous gas.69
The largest case series of ileal CDI (12 cases in5 years) also included a report of fatal ileal CDI ina 61-year-old man admitted for radical
prostatectomy with lymphadenectomy for prostateadenocarcinoma with no prior antibiotic use. Hewas discharged on postoperative day 4 but wasreadmitted with severe diarrhea; he received oraland intrarectal vancomycin and intravenousmetronidazole for treatment, but died 2 days laterof multiple organ failure. Autopsy confirmed Cdifficile enteritis in the ileum but not in the colon;

ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 17
toxigenic C difficile was isolated from ileal tissue butnot colonic tissue. This case depicts the potentialrapid trajectory of disease in ileal CDI.123 A patientwith possible ileal CDI should be treated with oralvancomycin (not metronidazole) because it resultsin reliable therapeutic concentrations in the smallbowel.124
Recommendations for treatment for smallbowel CDI include IV metronidazole 500 mg IV18 hours, by mouth, orally (PO) vancomycin500 mg every 6 hours (q6h) if evidence of resolu-tion of ileus, and if ileostomy present initiate retro-grade vancomycin flushes (500 mg in 100–500 mLnormal saline q6h) via the ileostomy to reduceluminal toxin. If severe ileus is still present, consid-eration of retrograde polyethylene glycol lavage viathe ileostomy to flush out the intestinal luminaltoxin (similar to the strategy used for loop ileos-tomy and colonic lavage) may be helpful.
RECURRENT CDI TREATMENT
Recurrent CDI affects 15% to 35% of patientswith primary CDI, and additional patients go on todevelop chronic relapsing CDI. Prolonged vanco-mycin oral taper is the initial treatment strategy forrecurrent CDI. For the first recurrence, use ofthe same regimen used in the first episode isrecommended, unless the severity of disease dic-tates a switch from metronidazole to vancomycin.For the second recurrence and all subsequentrecurrences, vancomycin is typically recommendedin tapering and pulsed doses (eg, vancomycin125 mg 4 times a day for 14 days, 125 mg twice dailyfor 7 days, 125 mg daily for 7 days, 125 mg everyother day for 7 days, and 125 mg PO every third dayfor 2–8 weeks).2
Spores are only susceptible to killing by antibi-otics when they are in a fully vegetative form, andby pulsing vancomycin intermittently, spores areallowed to germinate, thus making them suscepti-ble to killing. The repetitive cycle of antibiotic-freeperiods also allows an opportunity for the normalcolonic flora to reestablish itself.
For patients with multiple CDI recurrences whobreak through a tapering/pulsed vancomycintreatment strategy, the use of a fidaxomicin“chaser” (200 mg PO twice a day for 10 days) hasbeen shown to be effective in some patients, butrandomized comparative data are not avail-able.125,126 Bezlotoxumab (administered IV as asingle dose of 10 mg/kg over 1 hour) wasapproved (October 2016) by the FDA for the pre-vention of CDI recurrence in patients aged 18 yearsor older who are receiving antibacterial drug treat-ment for CDI.
Fecal microbiota transplant. In patients withrecurrent CDI, fecal microbiota transplant (FMT)aims to restore the normal composition of the gutmicrobiome and is recommended when antibi-otics fail to resolve CDI. The efficacy of FMT inrecurrent CDI had previously been limited to caseseries and open-label trials.127 The first random-ized controlled double-blind clinical trialenrolled 46 patients who had 3 or more recur-rences of CDI and received a full course of vanco-mycin for their most recent acute episode in 2academic medical centers. FMT with donor orautologous stool was administered by colonos-copy with the primary end point of resolution ofdiarrhea without need for anti-CDI therapy dur-ing the 8-week follow-up. This study demon-strated that donor FMT was more efficacious(90.9% clinical cure) than autologous FMT(62.5% clinical cure) in prevention of additionalCDI episodes.128
Although FMT is a highly effective treatment forrecurrent or refractory CDI, 10% to 20% ofpatients fail to achieve a cure after a single FMT.Risk factors for FMT failure have been identifiedand include severe and severe-complicated indica-tion, inpatient status during FMT, and increasednumber of previous CDI-related hospitalizations. Aprediction model based on these risk factors hadgood discrimination for identification of patientsat high risk of failure after FMT therapy.129 FMT isassociated with primary and secondary cure ratesof 88% and 94% in patients with severe or compli-cated CDI, respectively.130
The National Institute of Allergy and InfectiousDiseases of the National Institutes of Health hasprovided funding to launch the American Gastro-enterological Association Fecal Microbiota Trans-plantation National Registry, the first nationalregistry to track short- and long-term outcomesin patients who have undergone the gut-micro-biome–based therapy. The American Gastroenter-ological Association plans to put a formalinfrastructure into place for physicians and pa-tients to report information that will standardizebest practices for FMT while offering insight intothe gut microbiome and its role in human healthand disease.131
Probiotics. The use of probiotics to restorebalance to colonic microbiota either in the treat-ment or prevention of CDI has been investigated.An updated Cochrane systematic review and meta-analysis of 23 randomized controlled trials,including 4,213 patients (moderate quality evi-dence), suggests that probiotics are both safe andeffective for preventing C difficile–associated

Table V. Prevention strategies for CDI
Handwashing
Contact precautions
Antibiotic stewardship
Chlorhexidine gluconate bathing
Hydrogen peroxide vapor for terminal room cleaning
Pulsed xenon ultraviolet light for terminal room
cleaning
Daily cleaning with hydrogen peroxide disposable wipes
Probiotics
ARTICLE IN PRESSSurgeryj 2017
18 Napolitano and Edmiston
diarrhea.132,133 The SHEA/Infectious Diseases So-ciety of America treatment guidelines do notrecommend probiotics for CDI treatment due tolimited data and potential risk for bloodstreaminfection.
Of the probiotics studied, Saccharomyces boulardiihas the most data as a potential adjunctive treat-ment agent in recurrent CDI in adult pa-tients.134,135 A recent cost-effectiveness analysisconducted in Canada evaluated the impact oforal probiotics on the incidence and cost ofCDAD among hospitalized adult patients. The pre-ventive intervention involved the administration ofone oral dose (capsule) in any formulation withthe course of antibiotics and continuing for5 days after the completion of therapy (the controlgroup received no probiotics). The study docu-mented a reduced risk of CDAD and a cost savingsof $518 per patient treated.120,136
In the operative patient population, a singledose of antibiotic prophylaxis is often sufficient tostimulate the development of CDAD. If we extrap-olate to a population undergoing an operativeprocedure that would most likely require a singleprophylactic antibiotic dose, conservatively esti-mating that number to be 25 million, the pro-jected saving to the US health care system forreducing the risk of CDAD using a probiotic agentwould approach $13 billion. Further studies arewarranted in selective surgical patient populationsto validate the cost-effective and risk-reductionbenefits associated with probiotic prophylaxis forCDI.
INFECTION CONTROL STRATEGIES ANDPREVENTION
The challenges posed by CDI represent one ofthe most difficult patient care issues confrontinghealth care workers and infection control
personnel. All efforts to prevent and control CDIshould be implemented (Table V). Early recogni-tion of patients who are suspected of having orwho are diagnosed with CDI is the primary stepin preventing the spread of this epidemiologicallysignificant organism.49 C difficile can spread bydirect or indirect contact with the patient or his/her environment. CDI patients should be placedin Contact Precautions as recommended by theHealthcare Infection Control Practices AdvisoryCommittee/Centers for Disease Control and Pre-vention guidelines for isolation precautions. Strictadherence to the components of Contact Precau-tions will help to break the chain of infection, mak-ing a significant impact on limiting the spread orcross-contamination of this organism.
The following infection control strategies havedocument efficacy when applied in an appropriatemanner.137-139
(I) Patient placement: Ideally, CDI patients should be
kept in a private room with a bathroom or
commode solely dedicated for their use.
(II) The use of personal protective equipment: Incorporating
effective and consistent barrier precautions is
deemed critical to preventing transmission of
spores from patient to health care providers and
subsequently to other patients. It is important
that personal protective equipment (gown and
gloves) be donned before entering the patient’s
room and discarded before leaving the patient
room. High-touch surfaces like bed railings, door-
knobs, and light switches are often highly contam-
inated with C difficile spores. Consequently, gloves
must be donned before contact with patients or
their environment and throughout the period of
direct or indirect patient care.
(III) Patient transport: Unless it is absolutely necessary,
transport of CDI patients from their rooms should
be limited as much as possible. Individual persons
involved in this transport should be aware of the
patients’ status and use appropriate personal pro-
tective equipment.
(IV) Patient care equipment, instruments, devices, and patient
care environment: C difficile spores will contaminate
patient care equipment and devices through fecal
shedding or through contaminated hands of the
patient or health care providers. C difficile spores
can persist for months within the health care envi-
ronment and be transmitted to patients over a long
period of time (months). Fecal contamination of
surfaces, devices, and materials, such as commodes,
thermometers, and blood pressure equipment may
provide a reservoir for C difficile spores to dissemi-
nate, leading to transmission throughout the

ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 19
health care environment. Disinfectant products
with approved Environmental Protection Agency
registration should be used for daily routine clean-
ing in the health care setting and hypochlorite-
based disinfectants used for environmental surface
disinfection in those patient-care areas where sur-
veillance and epidemiology data indicate ongoing
transmission of C difficile. The Centers for Disease
Control and Prevention currently recommend
that hospital rooms be terminally cleaned with
bleach when patients are discharged or trans-
ferred. The use of selective spectrum ultraviolet
light and hydrogen peroxide vapor have demon-
strated in both laboratory and clinical trials to
reduce (or eliminate) C difficile (vegetative cells
and spores) from inert, contaminated surfaces.140
Hand hygiene. Health care providers’ hands areoften contaminated with C difficile after patient con-tact. After gloves are removed, health care providersshould wash their hands with soap and water rinse.Although alcohol hand gel products are effectiveagainst vegetative cells, they are ineffective againstclostridial spores.141 Numerous studies have docu-mented that judicious compliance with appropriatehand hygiene practice is an effective strategy forreducing the risk of dissemination and acquisitionof C difficile within the health care environment.142
Antibiotic stewardship. Judicious and appro-priate use of antibiotics under an antimicrobialstewardship program plays an important role inprevention strategies for C difficile.143 CDI canoften be linked to prior antibiotic use. Virtuallyall antibiotics produce disruption of the hostnormal colonic flora but differ in their capabilityto cause collateral damage to the patient’s gastro-intestinal flora. There are 2 key considerationswhen evaluating the risk for CDI: (1) the level ofrisk conferred by antibiotics, categorized as low, in-termediate, or high risk; and (2) the number ofdays the patient will be at risk for CDI.
A patient who receives a narrow-spectrum anti-biotic for less than 1 day will be considered to havea low risk and a short duration of risk. Alterna-tively, for a patient who receives operative prophy-laxis with an unnecessary broad-spectrumantibiotic, the level of risk for developing CDIwould move from low to high without any addi-tional clinical benefit from the inappropriatedrug.144
A recent case-controlled clinical trial found thatertapenem operative prophylaxis was significantlyassociated with postoperative CDI (P < .028).145
Furthermore, an analysis of morbidity and mortal-ity outcomes in postoperative CDI in Veterans
Affairs hospitals found that administration of 3or more classes of antibiotics in a 60-day preopera-tive period was one of several significant risk fac-tors.146 Implementation of an effectiveantimicrobial stewardship program would assist inthe development of institutional policies thataddress inappropriate antimicrobial use andlowering the potential for collateral damage.147
In conclusion, C difficile infections are the lead-ing cause of health care–associated infectious diar-rhea, posing a significant risk for both medical andsurgical patients. Because of the significantmorbidity and mortality associated with CDI,knowledge of the epidemiology of C difficile incombination with a high index of suspicion andsusceptible patient populations (including surgi-cal, postcolectomy, and IBD patients) is warranted.
CDI presents with a wide spectrum of disease,ranging from mild diarrhea to fulminant colitis orsmall bowel enteritis and recurrent CDI. Earlyimplementation of medical and operative treat-ment strategies of CDI is imperative for optimalpatient outcomes. National and internationalguidelines recommend early operative consulta-tion and total abdominal colectomy with endileostomy and preservation of rectum. Divertingloop ileostomy and colonic lavage followed byintravenous metronidazole and intracolonic van-comycin administered via the efferent limb of theileostomy should be considered as an alternative tototal colectomy in selected patients.
New and emerging strategies for CDI treatmentinclude monoclonal antibodies, vaccines, probiot-ics, biotherapeutics, and new antibiotics. A suc-cessful C difficile prevention and eradicationprogram requires a multidisciplinary approachthat includes early disease recognition, implemen-tation of guidelines for monitoring adherence toenvironmental control, judicious hand hygiene,evidence-based treatment and management strate-gies, and a focused antibiotic stewardship pro-gram. Surgeons are an important part of theclinical team in management of CDI preventionand treatment.
REFERENCES
1. To KB, Napolitano LM. Clostridium difficile infection: up-date on diagnosis, epidemiology, and treatment strategies.Surg Infect (Larchmt) 2014;15:490-502.
2. Badger VO, Ledeboer NA, Graham MB, Edmiston CE Jr.Clostridium difficile: epidemiology, pathogenesis, manage-ment, and prevention of a recalcitrant healthcare-associ-ated pathogen. JPEN J Parenter Enteral Nutr 2012;36:645-62.
3. Kuehn BM. Scientists seek strategies to prevent Clostridiumdifficile infections. JAMA 2011;306:1849-50.

ARTICLE IN PRESSSurgeryj 2017
20 Napolitano and Edmiston
4. Nguyen GC, Kaplan GG, Harris ML, Brant SR. A nationalsurvey of the prevalence and impact of Clostridium difficileinfection among hospitalized inflammatory bowel diseasepatients. Am J Gastroenterol 2008;103:1443-50.
5. Kelly CP. A 76-year-old man with recurrent Clostridium diffi-cile-associated diarrhea: review of C. difficile infection.JAMA 2009;30:954-62.
6. Ananthakrishnan AN, McGinley EL, Binion DG. Excesshospitalization burden associated with Clostridium difficilein patients with inflammatory bowel disease. Gut 2008;57:205-10.
7. Ananthakrishnan AN, McGinley EL, Saeian K, Binion DG.Temporal trends in disease outcomes related to Clostridiumdifficile infection in patients with inflammatory bowel dis-ease. Inflamm Bowel Dis 2011;17:976-83.
8. Hospital stays involving C. difficile infections leveled after300 percent increase since 1993. AHRQ News andNumbers. Rockville (MD): Agency for HealthcareResearch; 2012. Available from: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed August28 2016.
9. Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK,Dunn JR, et al. Burden of Clostridium difficile infection inthe United States. N Engl J Med 2015;372:825-34.
10. Leffler DA, Lamont JT. Clostridium difficile infection.N Engl J Med 2015;372:1539-48.
11. Hunter JC, Mu Y, Dumyati GK, Farley MM, Winston LG,Johnston HL, et al. Burden of nursing home-onset Clos-tridium difficile infection in the United States: estimates ofincidence and patient outcomes. Open Forum Infect Dis2016;3:ofv196.
12. Zerey M, Paton BL, Lincourt AE, Gersin KS, Kercher KW,Heniford BT. The burden of Clostridium difficile in surgicalpatients in the United States. Surg Infect (Larchmt) 2007;8:557-66.
13. Halabi WJ, Nguyen VQ, Carmichael JC, Pigazzi A,Stamos MJ, Mills S. Clostridium difficile colitis in the UnitedStates: a decade of trends, outcomes, risk factors for colec-tomy, and mortality after colectomy. J Am Coll Surg 2013;217:802-12.
14. Zilberberg MD, Shorr AF, Kollef MH. Increase in adultClostridium difficile-related hospitalizations and case-fatalityrate, United States, 2000–2005. Emerg Infect Dis 2008;14:929-31.
15. Rao K, Erb-Downward JR, Walk ST, Micic D,Falkowski N, Santhosh K, et al. The systemic inflamma-tory response to Clostridium difficile infection. PLoSOne 2014;9:e92578.
16. Hall AJ, Curns AT, McDonald LC, Parashar UD,Lopman BA. The roles of Clostridium difficile and norovirusamong gastroenteritis-associated deaths in the UnitedStates, 1999–2007. Clin Infect Dis 2012;55:216-23.
17. McDonald LC, Killgore GE, Thompson A, Owens RC Jr,Kazakova SV, Sambol SP, et al. An epidemic, toxin gene–variant strain of Clostridium difficile. N Engl J Med 2005;353:2433-41.
18. Akerlund T, Persson I, Unemo M, Nor�en T,Svenungsson B, Wullt M, et al. Increased sporulation rateof epidemic Clostridium difficile type 027/NAP1. J Clin Mi-crobiol 2008;46:1530-3.
19. Loo VG, Poirier L, Miller MA, Oughton M, Libman MD,Michaud S, et al. A predominantly clonal multi-institu-tional outbreak of Clostridium difficile–associated diarrheawith high morbidity and mortality. N Engl J Med 2005;353:2442-9.
20. Warny M, Pepin J, Fang A, Killgore G, Thompson A,Brazier J, et al. Toxin production by an emerging strainof Clostridium difficile associated with outbreaks of severedisease in North America and Europe. Lancet 2005;366:1079-84.
21. See I, Mu Y, Cohen J, Beldavs ZG, Winston LG, Dumyati G,et al. NAP1 strain type predicts outcomes from Clostridiumdifficile infection. Clin Infect Dis 2014;58:1394-400.
22. Martin JS, Monaghan TM, Wilcox MH. Clostridium difficileinfection: epidemiology, diagnosis and understandingtransmission. Nat Rev Gastroenterol Hepatol 2016;13:206-16.
23. Finney JM. Gastro-enterostomy for cicatrizing ulcer of thepylorus. Bull Johns Hopkins Hospital 1893;4:53.
24. Wakefield RD, Sommers SD. Fatal membranous staphylo-coccal enteritis in surgical patients. Ann Surg 1953;138:249.
25. Hummel RP, Altemeier WA, Hill EQ. Iatrogenic staphylo-coccal enterocolitis. Ann Surg 1964;160:551.
26. Tedesco FJ, Barton RW, Alpers DH. Clindamycin-associ-ated colitis: a prospective study. Ann Intern Med 1974;81:429-33.
27. Gerding DN. Clostridium difficile 30 years on: what has, orhas not, changed and why? Int J Antimicrob Agents2009;33:S2-8.
28. Rifkin GD, Fekety FR, Silva J. Antibiotic-induced colitisimplication of a toxin neutralized by Clostridium sordelliantitoxin. Lancet 1977;2:1103-6.
29. Larson HE, Price AB. Pseudomembranous colitis: pres-ence of clostridial toxin. Lancet 1977;2:1312-4.
30. George WL, Sutter VL, Goldstein EJ, Ludwig SL,Finegold SM. Etiology of antimicrobial-agent-associatedcolitis. Lancet 1978;1:802-3.
31. Larson HE, Price AB, Honour P, Borriello SP. Clostridiumdifficile and the etiology of pseudomembranous colitis.Lancet 1978;1:1063-6.
32. Deshpande A, Pasupuleti V, Thota P, Pant C, Rolston DD,Hernandez AV, et al. Risk factors for recurrent Clostridiumdifficile infection: a systematic review and meta-analysis.Infect Control Hosp Epidemiol 2015;36:452-60.
33. Tleyjeh IM, Bin Abdulhak AA, Riaz M, Alasmari FA,Garbati MA, AlGhamdi M, et al. Association between pro-ton pump inhibitor therapy and Clostridium difficile infec-tion: a contemporary systematic review and meta-analysis.PLoS One 2012;7:e50836.
34. Janarthanan S, Ditah I, Adler DG, Ehrinpreis MN. Clos-tridium difficile-associated diarrhea and proton pump inhib-itor therapy: a meta-analysis. Am J Gastroenterol 2012;107:1001-10.
35. Kwok CS, Arthur AK, Anibueze CI, Singh S, Cavallazzi R,Loke YK. Risk of Clostridium difficile infection with acid sup-pressing drugs and antibiotics: meta-analysis. Am J Gastro-enterol 2012;107:1011-9.
36. Shin JH, High KP, Warren CA. Older is not wiser, immuno-logically speaking: effect of aging on host response to Clos-tridium difficile infections. J Gerontol A Biol Sci Med Sci2016;71:916-22.
37. Wijarnpreecha K, Sornprom S, Thongprayoon C,Phatharacharukul P, Cheungpasitporn W, Nakkala K.The risk of Clostridium difficile associated diarrhea in naso-gastric tube insertion: a systematic review and meta-anal-ysis. Dig Liver Dis 2016;48:468-72.
38. Phatharacharukul P, Thongprayoon C,Cheungpasitporn W, Edmonds PJ, Mahaparn P,Bruminhent J. The risks of incident and recurrent

ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 21
Clostridium difficile-associated diarrhea in chronic kidneydisease and end-stage kidney disease patients: a systematicreview and meta-analysis. Dig Dis Sci 2015;60:2913-22.
39. Aquina CT, Probst CP, Becerra AZ, Hensley BJ,Iannuzzi JC, Noyes K, et al. High variability in nosocomialClostridium difficile infection rates across hospitals aftercolorectal resection. Dis Colon Rectum 2016;59:323-31.
40. Donnelly JP, Wang HE, Locke JE, Mannon RB,Safford MM, Baddley JW. Hospital-onset Clostridium difficileinfection among solid organ transplant recipients. Am JTransplant 2015;15:2970-7.
41. Honda H, Dubberke ER. Clostridium difficile infection insolid organ transplant recipients. Curr Opin Infect Dis2014;27:336-41.
42. Eckburg PB, Bik EM, Berstein CN. Diversity of the humanintestinal microbial flora. Science 2005;5728:1635-8.
43. Kelly CP, Pothoulakis C, LaMont JT. Clostridium difficile co-litis. N Eng J Med 1994;330:257-62.
44. Noren T. Clostridium difficile and the disease it causes. In:Mullany P, Roberts AP, editors. Clostridium difficile, methodsin molecular biology. 1st ed. Totowa (NJ): Humana Press;2010. p. 9-35.
45. Leffeler DA, Lamont JT. Treatment of Clostridium difficile-associated disease. Gastroenterology 2009;136:1899-912.
46. Blondeau JM. What have we learned about antimicrobialuse and the risk of Clostridium difficile-associated diarrhea?J Antimicrob Chemother 2009;63:238-42.
47. Carter GP, Rood JI, Lyras D. The role of toxin A and toxinB in the virulence of Clostridium difficile. Trends Microbiol2012;20:21-9.
48. Carroll KC, Bartlett JG. Biology of Clostridium difficile: im-plications for epidemiology and diagnosis. Annu Rev Mi-crobiol 2011;65:501-22.
49. Jank T, Aktories K. Structure and mode of action of clos-tridial glucosylating toxins: the ABCD model. Trends Mi-crobiol 2008;16:222-9.
50. Pothoulakis C. Effects of Clostridium difficile toxins onepithelial cell barrier. Ann NY Acad Sci 2000;915:347.
51. Sebaihia M, Wren BW, Mullany P, Fairweather NF,Minton N. The multidrug resistant pathogen Clostridiumdifficile has a highly mobile mosaic genome. Nat Genet2006;38:779-86.
52. Barbut F, Jones G, Eckert C. Epidemiology and control ofClostridium difficile infections in healthcare settings; an up-date. Curr Opin Infect Dis 2011;24:370-6.
53. Cheknis AK, Sambol SP, Davidson DM. Distribution ofClostridium difficile strains with other strains froma aNorth American, European and Australian trial of treat-ment of C. difficile infections: 2005-2007. Anaerobe 2009;15:230-3.
54. Oka K, Osaki T, Hanawa T, Kurata S, Okazaki M,Manzoku T, et al. Molecular and microbiological charac-terization of Clostridium difficile isolates from single, relapseand reinfection. J Clin Microbiol 2012;50:915-21.
55. Onderdonk AB, Garrett WS. Gas gangrene and otherClostridium-associated diseases. In: Mandell GL, BennettJE, Dolin R, editors. Principles and practices of infec-tious diseases. 7th ed. London: Churchill Livingston;2010. p. 3103-10.
56. Stevens DL, Bryant AE, Berger A, von Eichel-Streiber C.Clostridium. In: Versalovic J, Carroll K, Funke G, Jorgen-sen JH, Landry ML, Warnock DW, editors. Manual of clin-ical microbiology. 10th ed. Washington (DC): ASM Press;2011. p. 834-57.
57. Kyne L, Farrell RJ, Kelly CP. Clostridium difficile. Gastro-enterol Clin North Am 2001;30:753-77.
58. De Girolami PC, Hanff PA, Eichelberger K, Longhi L,Teresa H, Pratt J, et al. Multicenter evaluation of a newenzyme immunoassay for detection of Clostridium difficileenterotoxin A. J Clin Microbiol 1992;30:1085-8.
59. Altaie SS, Meyer P, Dryja D. Comparison of two commer-cially available enzyme immunoassays for detection of Clos-tridium difficile in stool specimens. J Clin Microbiol 1994;32:51-3.
60. Song L, Zhao M, Duffy DC, Hansen J, Shields K,Wungliranirun M, et al. Development and validation ofdirect enzyme-linked immunosorbent assays for ultrasensi-tive detection and quantification of Clostridium difficiletoxin in stool. J Clin Microbiol 2015;53:3204-12.
61. Eastwood K, Else P, Charlett A, Wilcox M. Comparison ofnine commercially available Clostridium difficile toxin detec-tion assays, a real-time PCR assay for C. difficile tcdB, and aglutamate dehydrogenase detection assay to cytotoxintesting and cytotoxigenic culture methods. J Clin Micro-biol 2009;47:3211-7.
62. Ticehurst JR, Aird DZ, Dam LM, Borek AP, Hargrove JT,Carroll KC. Effective detection of toxigenic Clostridiumdifficile by a two-step algorithm including tests for antigenand cytotoxin. J Clin Microbiol 2006;44:1145-9.
63. Stamper PD, Alcabasa R, Aird D, Babiker W, Wehrlin J,Ikpeama I, et al. Comparison of a commercial real-timePCR assay for tcdB detection to a cell culture cytotoxicityassay and toxigenic culture for direct detection of toxin-producing Clostridium difficile in clinical samples. J Clin Mi-crobiol 2009;47:373-8.
64. Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG,McDonald LC, et al. Clinical practice guidelines for Clos-tridium difficile infection in adults: 2010 update by the Soci-ety for Healthcare Epidemiology of America (SHEA) andthe Infectious Diseases Society of America (IDSA). InfectControl Hosp Epidemiol 2010;31:431-55.
65. Polage CR, Gyorke CE, Kennedy MA, Leslie JL, Chin DL,Wang S, et al. Overdiagnosis of Clostridium difficile infectionin the molecular test era. JAMA Int Med 2015;175:1792-801.
66. Fong KS, Fatica C, Hall G, Procop G, Schindler S,Gordon SM, et al. Impact of PCR testing for Clostridiumdifficile on incident rates and potential on public report-ing: is the playing field level? Infect Control Hosp Epide-miol 2011;32:932-3.
67. Macari M, Balthazar EJ, Megibow AJ. The accordion sign atCT: a nonspecific finding in patients with colonic edema.Radiology 1999;211:743-6.
68. Ash L, Baker ME, O’Malley CM Jr, Gordon SM,Delaney CP, Obuchowski NA. Colonic abnormalities onCT in adult hospitalized patients with Clostridium difficilecolitis: prevalence and significance of findings. AJR Am JRoentgenol 2006;186:1393-400.
69. Wee B, Poels JA, McCafferty IJ, Taniere P, Olliff J.A description of CT features of Clostridium difficile infectionof the small bowel in four patients and a review of litera-ture. Br J Radiol 2009;82:890-5.
70. Kawamoto S, Horton KM, Fishman EK. Pseudomembra-nous colitis: spectrum of imaging findings with clinicaland pathologic correlation. Radiographics 1999;19:887-97.
71. Ha D, Tsai CJ. Pneumatosis intestinalis in a patient withrecurrent Clostridium difficile infection. BMJ Case Rep2012;2012:1-4.

ARTICLE IN PRESSSurgeryj 2017
22 Napolitano and Edmiston
72. Kreiss C, Forohar F, Smithline AE, Brandt LJ. Pneumatosisintestinalis complicating C. difficile pseudomembranouscolitis. Am J Gastroenterol 1999;94:2560-1.
73. Schenk P, Madl C, Kramer L, Ratheiser K, Kranz A,Zauner C, et al. Pneumatosis intestinalis with Clostridiumdifficile colitis as a cause of acute abdomen after lung trans-plantation. Dig Dis Sci 1998;43:2455-8.
74. Gerding DN. Global epidemiology of Clostridium difficileinfection in 2010. Infect Control Hosp Epidemiol 2010;31:S32-4.
75. Lo Vecchio A, Zacur GM. Clostridium difficile infection: anupdate on epidemiology, risk factors, and therapeutic op-tions. Curr Opin Gastroenterol 2012;28:1-9.
76. Vaishnavi C. Clostridium difficile infection: clinical spectrumand approach to management. Indian J Gastroenterol2011;30:245-54.
77. Vaishnavi C. Clinical spectrum & pathogenesis of Clos-tridium difficile associated diseases. Indian J Med Res2010;131:487-99.
78. Hookman P, Barkin JS. Clostridium difficile associated infec-tion, diarrhea and colitis. World J Gastroenterol 2009;15:1554-80.
79. Hurley BW, Nguyen CC. The spectrum of pseudomembra-nous enterocolitis and antibiotic-associated diarrhea. ArchIntern Med 2002;162:2177-84.
80. Heinlen L, Ballard JD. Clostridium difficile infection. Am JMed Sci 2010;340:247-52.
81. Kachrimanidou M, Malisiovas N. Clostridium difficile infec-tion: a comprehensive review. Crit Rev Microbiol 2011;37:178-87.
82. Rodemann JF, Dubberke ER, Reske KA, Seo da H,Stone CD. Incidence of Clostridium difficile infection in in-flammatory bowel disease. Clin Gastroenterol Hepatol2007;5:339-44.
83. Lundeen SJ, Otterson MF, Binion DG, Carman ET,Peppard WJ. Clostridium difficile enteritis: an early postoper-ative complication in inflammatory bowel disease patientsafter colectomy. J Gastrointest Surg 2007;11:138-42.
84. Yee HF Jr, Brown RS Jr, Ostroff JW. Fatal Clostridium difficileenteritis after total abdominal colectomy. J Clin Gastroen-terol 1996;22:45-7.
85. Navaneethan U, Venkatesh PG, Shen B. Clostridium difficileinfection and inflammatory bowel disease: Understandingthe evolving relationship. World J Gastroenterol 2010;16:4892-904.
86. Clayton EM, Rea MC, Shanahan F, Quigley EM, Kiely B,Hill C, et al. The vexed relationship between Clostridiumdifficile and inflammatory bowel disease: an assessment ofcarriage in an outpatient setting among patients in remis-sion. Am J Gastroenterol 2009;104:1162-9.
87. Issa M, Vijayapal A, Graham MB, Beaulieu DB,Otterson MF, Lundeen S, et al. Impact of Clostridium diffi-cile on inflammatory bowel disease. Clin GastroenterolHepatol 2007;5:345-51.
88. Seril DN, Shen B. Clostridium difficile infection in patientswith ileal pouches. Am J Gastroenterol 2014;109:941-7.
89. Martinez Ugarte ML, Lightner AL, Colibaseanu D,Khanna S, Pardi DS, Dozois EJ, et al. Clostridium difficileinfection after restorative proctocolectomy and ileal pouchanal anastomosis for ulcerative colitis. Colorectal Dis 2016;18:O154-7.
90. Weingarden AR, Chen C, Zhang N, Graiziger CT, Dosa PI,Steer CJ, et al. Ursodeoxycholic acid inhibits Clostridiumdifficile spore germination and vegetative growth, and
prevents the recurrence of ileal pouchitis associated withthe infection. J Clin Gastroenterol 2016;50:624-30.
91. Drekonja DM, Butler M, MacDonald R, Bliss D, Filice GA,Rector TS, et al. Comparative effectiveness of Clostridiumdifficile treatments: a systematic review. Ann Intern Med2011;155:839-47.
92. Di X, Bai N, Zhang X, Liu B, Ni W, Wang J, et al. A meta-analysis of metronidazole and vancomycin for the treat-ment of Clostridium difficile infection, stratified by diseaseseverity. Braz J Infect Dis 2015;19:339-49.
93. Louie TJ, Byrne B, Emery J, Ward L, Krulicki W, Nguyen D,et al. Differences of the fecal microflora with Clostridiumdifficile therapies. Clin Infect Dis 2015;60(Suppl 2):S91-7.
94. Bagdasarian N, Rao K, Malani PN. Diagnosis and treat-ment of Clostridium difficile in adults: a systematic review.JAMA 2015;313:398-408.
95. Dupont HL. Diagnosis and management of Clostridiumdifficile infection. Clin Gastroenterol Hepatol 2013;11:1216-23; quiz e73.
96. Hecht DW, Galang MA, Sambol SP, Osmolski JR,Johnson S, Gerding DN. In vitro activities of 15 antimicro-bial agents against 110 toxigenic Clostridium difficile clinicalisolates collected from 1983 to 2004. Antimicrobial AgentsChemother 2007;51:2716-9.
97. Shue YK, Sears PS, Shangle S, Walsh RB, Lee C,Gorbach SL, et al. Safety, tolerance, and pharmacokineticstudies of OPT-80 in healthy volunteers following singleand multiple oral doses. Antimicrob Agents Chemother2008;52:1391-5.
98. Louie TJ, Emery J, Krulicki W, Byrne B, Mah M. OPT-80eliminates Clostridium difficile and is sparing of Bacteroidesspecies during treatment of C. difficile infection. Antimi-crob Agents Chemother 2009;53:261-3.
99. Cornely OA, Nathwani D, Ivanescu C, Odufowora-Sita O,Retsa P, Odeyemi IA. Clinical efficacy of fidaxomicincompared with vancomycin and metronidazole in Clos-tridium difficile infections: a meta-analysis and indirecttreatment comparison. J Antimicrob Chemother 2014;69:2892-900.
100. Louie TJ, Miller MA, Mullane KM, Weiss K, Lentnek A,Golan Y, et al. OPT-80-003 Clinical Study Group. Fidaxomi-cin versus vancomycin for Clostridium difficile infection.N Engl J Med 2011;364:422-31.
101. Cornely OA, Crook DW, Esposito R, Poirier A, Somero MS,Weiss K, et al. OPT-80-004 Clinical Study Group. Fidaxomi-cin versus vancomycin for infection with Clostridium difficilein Europe, Canada, and the USA: a double-blind, non-infe-riority, randomised controlled trial. Lancet Infect Dis2012;12:281-9.
102. Surawicz CM, Brandt LJ, Binion DG, Ananthakrishnan AN,Curry SR, Gilligan PH, et al. Guidelines for diagnosis,treatment, and prevention of Clostridium difficile infections.Am J Gastroenterol 2013;108:478-98.
103. Hussack G, Tanha J. An update on antibody-based immu-notherapies for Clostridium difficile infection. Clin Exp Gas-troenterol 2016;9:209-24.
104. Lowy I, Molrine DC, Leav BA, Blair BM, Baxter R,Gerding DN, et al. Treatment with monoclonal antibodiesagainst Clostridium difficile toxins. N Engl J Med 2010;362:197-205.
105. Yang Z, Ramsey J, Hamza T, Zhang Y, Li S, Yfantis HG,et al. Mechanisms of protection against Clostridium difficileinfection by the monoclonal antitoxin antibodies actoxu-mab and bezlotoxumab. Infect Immun 2015;83:822-31.

ARTICLE IN PRESSSurgeryVolume j, Number j
Napolitano and Edmiston 23
106. Wilcox MH, Gerding DN, Poxton IR, Kelly C, Nathan R,Birch T, et al. MODIFY I and MODIFY II Investigators. Be-zlotoxumab for prevention of recurrent Clostridium difficileinfection. N Engl J Med 2017;376:305-17.
107. Traynor K. Bezlotoxumab approved to prevent Clostridiumdifficile recurrence. Am J Health Syst Pharm 2016;73:1902.
108. Markham A. Bezlotoxumab: first global approval. Drugs2016;76:1793-8.
109. Knisely JM, Liu B, Ranallo RT, Zou L. Vaccines for health-care-associated infections: promise and challenge. ClinInfect Dis 2016;63:657-62.
110. C diffense. Clostridium difficile vaccine trial [Internet].Paris: Sanofi; 2013. Available from: http://www.cdiffense.org/home. Accessed August 28 2016.
111. Goldberg EJ, Bhalodia S, Jacob S, Patel H, Trinh KV,Varghese B, et al. Clostridium difficile infection: a brief up-date on emerging therapies. Am J Health-Syst Pharm2015;72:1007-12.
112. Foglia G, Shah S, Luxemburger C, Pietrobon PJ. Clos-tridium difficile: development of a novel candidate vaccine.Vaccine 2012;30:4307-9.
113. Sheldon E, Kitchin N, Peng Y, Eiden J, Gruber W,Johnson E, et al. A phase 1, placebo-controlled, random-ized study of the safety, tolerability, and immunogenicityof a Clostridium difficile vaccine administered with orwithout aluminum hydroxide in healthy adults. Vaccine2016;34:2082-91.
114. Kociolek LK, Gerding DN. Breakthroughs in the treatmentand prevention of Clostridium difficile infection. Nat RevGastroenterol Hepatol 2016;13:150-60.
115. Martin J, Wilcox M. New and emerging therapies forClostridium difficile infection. Curr Opin Infect Dis 2016;29:546-54.
116. Osman KA, Ahmed MH, Hamad MA, Mathur D. Emer-gency colectomy for fulminant Clostridium difficile colitis:striking the right balance. Scand J Gastroenterol 2011;46:1222-7.
117. Synnott K, Mealy K, Merry C, Kyne L, Keane C, Quill R.Timing of surgery for fulminating pseudomembranous co-litis. Br J Surg 1998;85:229-31.
118. Dudukgian H, Sie E, Gonzalez-Ruiz C, Etzioni DA,Kaiser AM. C. difficile colitis–predictors of fatal outcome.J Gastrointest Surg 2010;14:315-22.
119. Stewart DB, Hollenbeak CS, Wilson MZ. Is colectomy forfulminant Clostridium difficile colitis life saving? A systematicreview. Colorectal Dis 2013;15:798-804.
120. Bhangu A, Nepogodiev D, Gupta A, Torrance A, Singh P.West Midlands Research Collaborative. Systematic reviewand meta-analysis of outcomes following emergency sur-gery for Clostridium difficile colitis. Br J Surg 2012;99:1501-13.
121. Lee DY, Chung EL, Guend H, Whelan RL,Wedderburn RV, Rose KM. Predictors of mortality afteremergency colectomy for Clostridium difficile colitis: ananalysis of ACS-NSQIP. Ann Surg 2014;259:148-56.
122. Neal MD, Alverdy JC, Hall DE, Simmons RL,Zuckerbraun BS. Diverting loop ileostomy and coloniclavage: an alternative to total abdominal colectomy forthe treatment of severe, complicated Clostridium difficileassociated disease. Ann Surg 2011;254:423-7; discussion427-9.
123. Lavall�ee C, Laufer B, P�epin J, Mitchell A, Dub�e S,Labb�e AC. Fatal Clostridium difficile enteritis caused bythe BI/NAP1/027 strain: a case series of ileal C. difficile in-fections. Clin Microbiol Infect 2009;15:1093-9.
124. Pepin J. Vancomycin for the treatment of Clostridium diffi-cile infection: for whom is this expensive bullet reallymagic? Clin Infect Dis 2008;46:1493-8.
125. Johnson S, Gerding DN. Fidaxomicin “chaser” regimenfollowing vancomycin for patients with multiple Clostridiumdifficile recurrences. Clin Infect Dis 2013;56:309-10.
126. Soriano MM, Danziger LH, Gerding DN, Johnson S. Novelfidaxomicin treatment regimens for patients with multipleClostridium difficile infection recurrences that are refractoryto standard therapies. Open Forum Infect Dis 2014;1:ofu069.
127. Drekonja D, Reich J, Gezahegn S, Greer N, Shaukat A,MacDonald R, et al. Fecal microbiota transplantation forClostridium difficile infection: a systematic review. AnnIntern Med 2015;162:630-8.
128. Kelly CR, Khoruts A, Staley C, Sadowsky MJ, Abd M,Alani M, et al. Effect of fecal microbiota transplantationon recurrence in multiply recurrent Clostridium difficileinfection: a randomized trial. Ann Intern Med 2016;165:609-16.
129. Fischer M, Kao D, Mehta SR, Martin T, Dimitry J,Keshteli AH, et al. Predictors of early failure after fecal mi-crobiota transplantation for the therapy of Clostridium diffi-cile infection: a multicenter study. Am J Gastroenterol2016;111:1024-31.
130. Aroniadis OC, Brandt LJ, Greenberg A, Borody T,Kelly CR, Mellow M, et al. Long-term follow-up study offecal microbiota transplantation for severe and/or compli-cated Clostridium difficile infection: a multicenter experi-ence. J Clin Gastroenterol 2016;50:398-402.
131. AGA receives NIH funding for first national FMT registry[Internet]. Thorofare (NJ): SLACK Incorporated; 2017.Available from: http://www.healio.com/gastroenterology/therapeutics-diagnostics/news/online/%7B5f73d4ea-3380-45eb-94c6-f00d5000bb58%7D/aga-receives-nih-funding-for-first-national-fmt-registry?utm_source=maestro&utm_medium=email&utm_campaign=gastroenterology%20news. Ac-cessed August 28 2016.
132. Goldenberg JZ, Ma SS, Saxton JD, Martzen MR,Vandvik PO, Thorlund K, et al. Probiotics for the preven-tion of Clostridium difficile-associated diarrhea in adultsand children. Cochrane Database Syst Rev 2013:CD006095.
133. Pillai A, Nelson RL. Probiotics for treatment of Clostridiumdifficile-associated colitis in adults. Cochrane Database SystRev 2008:CD004611.
134. Griffin AT, Arnold FW. The most effective treatments forClostridium difficile diarrhea: an evidence-based review.Infect Dis Clin Pract 2011;19:171-81.
135. McFarland LV. Systematic review and meta-analysis ofSaccharomyces boulardii in adult patients. World J Gastroen-terol 2010;16:2202-22.
136. Leal JR, Heitman SJ, Conly J, Henderson EA, Manns BJ.Cost-effective analysis of use of priobiotics for the preven-tion of Clostridium difficile-associated diarrhea in a provin-cial healthcare system. Infect Control Hosp Epidemiol2016;37:1079-86.
137. Siegel JD, Rhinehart E, Jackson M, Chiarello L. HealthCare Infection Control Practices Advisory Committee.2007 guideline for isolation precautions: preventing trans-mission of infectious agents in health care settings. Am JInfect Control 2007;35:S65-164.
138. Weber DJ, Rutala WA. The role of the environment intransmission of Clostridium difficile infection in healthcarefacilities. Infect Control Hosp Epidemiol 2011;32:207-9.

ARTICLE IN PRESSSurgeryj 2017
24 Napolitano and Edmiston
139. Gerding DN, Muto CA, Owens RC. Measures to controland prevent Clostridium difficile infection. Clin Infect Dis2008;46:S43-9.
140. Loo VG. Environmental interventions to control Clos-tridium difficile. Infect Dis Clin North Am 2015;29:83-91.
141. Barbut F. How to eradicate Clostridium difficile from theenvironment. J Hosp Infect 2015;89:287-95.
142. Goldstein EJ, Johnson S, Maziade PJ, McFarland LV,Trick W, Dresser L, et al. Pathway to prevention of nosoco-mial Clostridium difficile infection. Clin Infect Dis 2015;60(Suppl 2):S148-58.
143. Bartlett JG. A call to arms: the imperative for antimicrobialstewardship. Clin Infect Dis 2011;53:S4-7.
144. Rebmann T, Carrico RM. Association for Professionals inInfection Control and Epidemiology. Preventing Clos-tridium difficile infections: an executive summary of the as-sociation for professionals in infection control andepidemiology’s elimination guide. Am J Infect Control2011;39:239-42.
145. Lee S, Prasad P, Lin M, Garritson S, Nichols A, Liu C. Er-tapenem prophylaxis associated with increased risk of Clos-tridium difficile infection in surgical patients. Infect ControlHosp Epidemiol 2015;36:1351-4.
146. Li X, Wilson M, Nylander W, Smith T, Lynn M, Gunnar W.Analysis of morbidity and mortality outcomes in postoper-ative Clostridium difficile infection in the Veterans HealthAdministration. JAMA Surg 2016;151:314-22.
147. Bui C, Zhu E, Donnelley MA, Wilson MD, Morita M,Cohen SH, et al. Antimicrobial stewardship programsthat target only high-cost, broad-spectrum antimicrobialsmiss opportunities to reduce Clostridium difficile infections.Am J Infect Control 2016;44:1684-6.
148. Gerding DN, Lessa FC. The epidemiology of Clostridiumdifficile infection inside and outside health care institu-tions. Infect Dis Clin North Am 2015;29:37-50.
149. Debast SB, Bauer MP, Kuijper EJ. European society of clin-ical microbiology and infectious diseases: update of thetreatment guidance document for Clostridium difficile infec-tion. Clin Microbiol Infect 2014;20(Suppl 2):1-26.
150. Ferrada P, Velopulos CG, Sultan S, Haut ER, Johnson E,Praba-Egge A, et al. Timing and type of surgical treat-ment of Clostridium difficile-associated disease: a practicemanagement guideline from the Eastern Associationfor the Surgery of Trauma. J Trauma Acute Care Surg2014;76:1484-93; Erratum in: J Trauma Acute CareSurg 2014;77:186.
151. Sartelli M, Malangoni MA, Abu-Zidan FM, Griffiths EA, DiBella S, McFarland LV, et al. WSES guidelines for manage-ment of Clostridium difficile infection in surgical patients.World J Emerg Surg 2015;10:38.
152. Steele SR, McCormick J, Melton GB, Paquette I,Rivadeneira DE, Stewart D, et al. Practice parameters forthe management of Clostridium difficile infection. Dis ColonRectum 2015;58:10-24.
153. Trubiano JA, Cheng AC, Korman TM, Roder C,Campbell A, May ML, et al. Australasian Society of Infec-tious Diseases updated guidelines for the managementof Clostridium difficile infection in adults and children inAustralia and New Zealand. Intern Med J 2016;46:479-93.
154. Cheng AC, Ferguson JK, Richards MJ, Robson JM,Gilbert GL, McGregor A, et al. Australasian society for in-fectious diseases guidelines for the diagnosis and treat-ment of Clostridium difficile infection. Med J Aust 2011;194:353-8.

MI71CH15-Aktories ARI 16 August 2017 7:31
Annual Review of Microbiology
Clostridium difficileToxin BiologyKlaus Aktories, Carsten Schwan, and Thomas JankInstitute of Experimental and Clinical Pharmacology and Toxicology, University of Freiburg,79104 Freiburg, Germany; email: [email protected],[email protected], [email protected]
Annu. Rev. Microbiol. 2017. 71:281–307
First published as a Review in Advance on June 28,2017
The Annual Review of Microbiology is online atmicro.annualreviews.org
https://doi.org/10.1146/annurev-micro-090816-093458
Copyright c© 2017 by Annual Reviews.All rights reserved
Keywords
Clostridium difficile toxins, glucosylation, toxin receptors, toxin uptake, Rhoproteins, Clostridium difficile infection, Clostridium difficile transferase toxin,CDT, ADP ribosylation, actin, microtubules
Abstract
Clostridium difficile is the cause of antibiotics-associated diarrhea andpseudomembranous colitis. The pathogen produces three protein toxins:C. difficile toxins A (TcdA) and B (TcdB), and C. difficile transferase toxin(CDT). The single-chain toxins TcdA and TcdB are the main virulencefactors. They bind to cell membrane receptors and are internalized. The N-terminal glucosyltransferase and autoprotease domains of the toxins translo-cate from low-pH endosomes into the cytosol. After activation by inositolhexakisphosphate (InsP6), the autoprotease cleaves and releases the gluco-syltransferase domain into the cytosol, where GTP-binding proteins of theRho/Ras family are mono-O-glucosylated and, thereby, inactivated. Inac-tivation of Rho proteins disturbs the organization of the cytoskeleton andaffects multiple Rho-dependent cellular processes, including loss of epithe-lial barrier functions, induction of apoptosis, and inflammation. CDT, thethird C. difficile toxin, is a binary actin-ADP-ribosylating toxin that causesdepolymerization of actin, thereby inducing formation of the microtubule-based protrusions. Recent progress in understanding of the toxins’ actionsinclude insights into the toxin structures, their interaction with host cells,and functional consequences of their actions.
281
Click here to view this article's online features:
• Download figures as PPT slides• Navigate linked references• Download citations• Explore related articles• Search keywords
ANNUAL REVIEWS FurtherA
nnu.
Rev
. Mic
robi
ol. 2
017.
71:2
81-3
07. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
WIB
6221
- K
IZ-A
BT
Lite
ratu
rver
wal
tung
on
04/0
9/18
. For
per
sona
l use
onl
y.

MI71CH15-Aktories ARI 16 August 2017 7:31
Contents
INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 282REGULATION OF TOXIN PRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 283OVERALL TOXIN STRUCTURE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 283RECEPTOR BINDING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284
CROPs Domain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284TcdA Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285Chondroitin Sulfate Proteoglycan 4 Is a Receptor for TcdB. . . . . . . . . . . . . . . . . . . . . . . 285TcdB Binds to the Wnt Receptor Frizzled . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 286
TOXIN UPTAKE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287MEMBRANE TRANSLOCATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
Toxins’ Regions Involved in Translocation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 288PROCESSING OF THE TOXINS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 288
Allosteric Activation by InsP6 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289BIOLOGICAL ACTIVITY OF CLOSTRIDIAL GLUCOSYLATING TOXINS. . . 290
Glucosyltransferase Domain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 290TcdA and TcdB Are Retaining Glycosyltransferases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 290Cosubstrate and Substrate Recognition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 291Rho Proteins as Targets of TcdA and TcdB . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 291Functional Consequences of Rho Modification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292
FROM RHO MODIFICATION TO DISEASE. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 293Cytopathic Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 293Induction of Apoptosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 293Activation of the Inflammasome and Pyroptosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294ROS Production and Effects Not Related to Glucosylation of Rho Proteins . . . . . . . 294
THE BINARY C. DIFFICILE TRANSFERASE TOXIN . . . . . . . . . . . . . . . . . . . . . . . . . . . 296Structure of CDT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296Binding and Uptake of CDT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296CDT ADP-Ribosylates G-Actin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297CDT-Induced ADP Ribosylation of Actin Affects Microtubule Structures . . . . . . . . . 298Functional Roles of CDT-Induced Microtubules . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299
CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299
INTRODUCTION
Increased incidence of and morbidity from infections caused by spore-forming, anaerobic, gram-positive Clostridium difficile bacteria are a major health care problem in most developed countries.The pathogen is the leading cause of nosocomial infection and appears to be responsible for up to29,000 deaths per year in the United States (92). The clinical features of C. difficile infection (CDI)range from mild diarrhea to severe pseudomembranous colitis with complications like megacolonor fulminant infection course (84). In most cases, CDI is the consequence of dysbiosis caused byantibiotic treatment. Antibiotics [e.g., clindamycin > cephalosporins, carbapenems, penicillins,and fluoroquinolones (154)] alter the normal gut microbiome in a way that allows germinationof C. difficile spores with subsequent colonization and proliferation of the bacteria. The diseasestrictly depends on protein toxins produced by C. difficile (84). Three toxins are known: The
282 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
Rho-glucosylating C. difficile toxins A (TcdA) and B (TcdB) are major toxins that are clearlyresponsible for diarrhea and colitis. In addition, 5–30% of clinical C. difficile isolates produce abinary ADP-ribosylating toxin, CDT, that modifies actin (46). However, its role in disease is notclear.
TcdA and TcdB belong to the family of large clostridial glucosylation toxins. Other familymembers are Clostridium sordellii lethal (TcsL) and hemorrhagic (TcsH) toxins, Clostridium novyiα-toxin (TcnA), and Clostridium perfringens toxin TpeL. These single-chain toxins are 26–76%identical. All these toxins share the structural features of the C. difficile toxins and modify Rhoand/or Ras proteins. Several isoforms, especially for TcdA and TcdB, have been described (138).This review describes mainly the prototypes TcdA and TcdB from the high-producer strainC. difficile VPI 10463.
TcdA was called enterotoxin, because initial studies showed that in animal models (hamstersand rabbits) TcdA was more potent in increasing secretion, mucosa damage, and inflammationthan TcdB (94, 107, 162). While in most cell cultures TcdB was much more potent (by a factorof 100 to 1,000) than TcdA, it was named cytotoxin. Later studies revealed that TcdB is evenmore toxic for human colonic epithelium than TcdA (137). The roles of TcdA and TcdB andtheir relative contributions in CDI have recently been extensively discussed (88, 98). It is clearthat both toxins can induce disease; however, TcdB appears to be more important for infectionand innate immune and inflammatory responses (18).
Like many protein toxins that are released from bacteria into the environment to target hostcells by an intracellular mechanism, C. difficile toxins act in a stepwise manner: (a) binding totarget cells, (b) endocytosis of the toxin-receptor complex, (c) toxin translocation across endosomalmembranes into the cytosol, (d ) processing to release the biologically active toxin moiety, and,finally, (e) modification of target proteins of host cells catalyzed by the toxin. Recent findings havelargely increased our knowledge about the regulation, structures, and functions of C. difficile toxins.
REGULATION OF TOXIN PRODUCTION
The encoding genes (tcdA and tcdB) of C. difficile toxins TcdA and TcdB are positioned in apathogenicity locus (PaLoc) of 19.6 kb together with the three additional genes tcdR, tcdE, andtcdC (12, 57). While tcdR encodes an RNA polymerase sigma factor that positively regulates toxinexpression (101), tcdC appears to encode a repressor of toxin expression (103, 164). tcdE is the geneof a bacteriophage holin required for toxin secretion (50, 158). Toxin expression is bidirectionallyregulated by environmental signals. Inhibition of expression occurs by glucose, amino acids (e.g.,proline or cysteine), butanol, and biotin, whereas short-chain fatty acids (e.g., butyrate) and hightemperature (37◦C) stimulate toxin production (11, 82, 83). TcdA and TcdB are expressed whencells enter a stationary phase, likely caused by limitation of nutrients. In nontoxigenic strains,the PaLoc region is usually replaced by a 115-bp sequence. However, PaLoc is also integratedin genomic locations distinct from the classical integration site, indicating horizontal transfer inacquisition (109). Variations in the PaLoc region like deletions, insertions, and mutations result innumerous toxinotypes (>30), which are different from the reference strain VPI 10463 in respectto substrate specificity and activity of their toxins.
OVERALL TOXIN STRUCTURE
TcdA (308 kDa, Acc.Nr. P16154) and TcdB (270 kDa, Acc.Nr. P18177) have 2,710 and 2,366amino acids, respectively, and are 48% identical in their amino acid sequence (Figure 1). Thetoxins consist of at least four major functional domains according to the ABCD model (74). The
www.annualreviews.org • Clostridium difficile Toxins 283
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
1 802543 1,833 2,710
Activity DeliveryCutting Binding
TcdA GTD APD CROPs
A
A
C
C
D
D
B
2,6631,8345441TcdB GTD APD CROPs
799
HP
HP
c
a
CROPs
b
Figure 1Structure of C. difficile toxins A (TcdA) and B (TcdB). (a) Sequences of TcdA and TcdB. Both toxins consistof four domains. Domain A is the glucosyltransferase. Domain B consists of combined repetitiveoligopeptides (CROPs) and is involved in receptor binding. Domain C is an autoprotease domain and isconnected to domain D by a three-helix bundle (dark blue). Domain D is involved in the delivery and also inbinding to host cells. Within domain D is a hydrophobic (HP) sequence (amino acids 958–1,130 in TcdAand 956–1,128 in TcdB) that probably plays a role in toxin translocation. (b) Crystal structure of TcdAdomains A, C, and D. The CROPs domain is missing. From the glucosyltransferase domain the surface viewis given (PDB 4R04) (25). (c) Model of the full-length toxin according to single-particle analysis of theholotoxin (modified from 25). Proposed CROPs domain of TcdA modified from References 51 and 68.
N-terminal, biologically active domain A harbors glucosyltransferase activity that modifies Rhoproteins. The C-terminal part of the toxin (designated domain B) is suggested to be involved inreceptor binding. The C (cutting) domain follows domain A and possesses protease function. TheD domain is probably involved in delivery of the toxin (or part of the toxin) into the cytosol oftarget cells. Whereas various isolated domains of TcdA and TcdB were crystallized some yearsago (51, 68, 127, 129, 136, 151, 180), the full-length toxin still has not been crystallized. However,single-particle analysis of whole toxins (128) and recent crystal structure analyses of N-terminalamino acid residues of TcdA, covering domains A, C, and D (25), allow a nearly complete view ofthese toxins (Figure 1).
RECEPTOR BINDING
CROPs Domain
The B domains of TcdA and TcdB cover residues 1,833–2,710 and 1,834–2,366, respectively, andare characterized by repetitive sequences called combined repetitive peptides (CROPs) (29, 167,
284 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
168) (Figure 1). The isolated domains, as well as antibodies directed against this toxin region,inhibit binding and toxicity, suggesting an important role in receptor binding (37, 93). CROPshave a solenoid fold with 7 long repeats of 30 residues and 31 short repeats of 15–21 residues inTcdA and 7 long repeats of 30 residues and 21 short repeats of 20–23 residues in TcdB (51, 68,111). The repeat units form a hairpin followed by a loop. While TcdA and TcdB CROPs sharethe solenoid fold, they differ in distinct spatial and sequential arrangements of their repeat units.This is in agreement with early findings that the receptors for TcdA and TcdB are different (22).
TcdA Receptors
TcdA binds to α-Gal-(1,3)-β-Gal-(1,4)-β-GlcNAc glycan sequences on rabbit erythro-cytes (87, 163). In the crystal structure, the synthetic sugar α-Gal-(1,3)-β-Gal-(1,4)-β-GlcNAcO(CH2)8CO2CH3 (CD-grease) interacts with each long repeat of the CROPs domain ofTcdA (51). However, this glycan sequence is not the relevant human receptor, because this type ofcarbohydrate is absent in humans. TcdA also binds to GalNAc-(1,3)-β-Gal-(1,4)-β-GlcNAc thatis present on human cells (161). Furthermore, the membrane-bound sucrose-isomaltase has beenidentified as a functional receptor for TcdA in rabbit intestinal epithelial cells (126). However, thisreceptor is not expressed in epithelium cells of human colon. TcdA also binds to Lewis I, X, and Yglycan sequences (155, 163), which are expressed on human intestinal epithelial cells. Moreover, incross-linking experiments, glycoprotein gp96 was identified as a possible receptor for TcdA on thesurface of HT29 human colonic epithelial cells (112). gp96 is a heat shock protein that is presenton human colonocyte apical membranes as well as in the cytoplasm. However, downregulation ofgp96 and anti-gp96 antibody only partially blocks the cytotoxic effects of TcdA (112), suggestingthat gp96 is not the primary receptor and may be a coreceptor. The pathophysiologically relevantreceptor of TcdA is still unknown.
In fact, recent studies indicate that the family of large clostridial glycosylating toxins (includingTcdA and TcdB) uses more than one receptor for cell binding and entry. Moreover, the receptorbinding site of the toxins is clearly not restricted to the C-terminal CROPs domain. Paradigmaticwere studies with C. perfringens toxin TpeL, which is shorter than all other large clostridial glyco-sylating toxins and possesses no CROPs domain but binds to target cells and causes intoxication(4, 53). TpeL binds with its C-terminal part of the D domain to LRP1 (low-density lipoproteinreceptor–related protein 1) (144). Several recent studies on the receptor binding of TcdB supportthe concept of multiple-receptor interaction (89, 90, 159, 177).
Chondroitin Sulfate Proteoglycan 4 Is a Receptor for TcdB
TALEN and CRISPR/Cas9-mediated gene knockout screenings revealed that chondroitin sulfateproteoglycan 4 (CSPG4) functions as a cellular receptor for TcdB (177). CSPG4 mediates bothbinding and internalization of TcdB (Figure 2). Although it has been claimed that CSPG4 bindsto a non-CROPs region of TcdB, recent studies indicate that the binding area is still a part of theCROPs domain, covering residues 1,834–2,366 (119) and not, as first predicted, residues 1,851–2,366 (177). CSPG4 [also named high molecular weight melanoma-associated antigen (HMW-MAA), nerve/glial antigen 2 (NG2), melanoma-associated CSPG, or gp240] is a membrane-bound proteoglycan with a single transmembrane domain (10). The proteoglycan is composedof a short signal peptide (residues 1–29), a very large extracellular domain (residues 30–2,224), ahelical transmembrane domain (amino acids 2,225–2,245), and a short 76–amino acid cytoplasmicdomain (in mouse, rat, and human) (157) (Figure 2). The extracellular domain contains 2 lamininG-type motifs and 15 CSPG repeats potentially involved in glycosaminoglycan interaction (157).
www.annualreviews.org • Clostridium difficile Toxins 285
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
Endosome
TcdB TcdB
Membraneinsertion
Extracellularspace
Cytoplasm
H+ Release of theglucosyltransferase
UDP
+ UDP-glucose
Glucosylation ofRho GTPases
Pathogeniceffects
Autoproteolyticcleavage
GlucoseThr37–OH
Tcd
FZD
CSPG4
Rac Rhoβ-cat
TcdA
Clathrin PACSIN2Dynamin
Receptor withcarbohydrate structure
CRD
Repeats
H+H+H+
H+
H+H+
H+H+
H+
Thr37–O
Rho
InsP6
PRR
PDZ
DvI
H
H+
Rho
Figure 2Binding and uptake of TcdA and TcdB. Both chondroitin sulfate proteoglycan 4 (CSPG4) and Frizzled (FZD) are host cell receptors ofTcdB. FZD is a heptahelical membrane receptor involved in Wnt signaling. TcdB binds with a non–combined repetitive oligopeptides(non-CROPs) region to the cysteine-rich domain (CRD) of FZD. Binding to the single-pass membrane protein CSPG4 occurs withthe CROPs domain of TcdB. After binding, the toxin is endocytosed in a clathrin- and dynamin-dependent manner. Certaincarbohydrate structures (and gp96) are receptors for TcdA. PACSIN2 (also called syndapin-II) and dynamin but not clathrin areinvolved in endocytosis of TcdA. Both toxins reach an acidic endosomal compartment, where they insert into endosomal membranesand translocate into the cytosol at least with the glucosyltransferase (GTD) and the autoprotease domain. Cytosolic inositolhexakisphosphate (InsP6) activates the protease, thereby cleaving the toxin and releasing GTD into the cytosol. GTD translocates tothe cell membrane by its N-terminal, four-helix subdomain. Here, Rho proteins are glucosylated (RhoA at Thr37; Cdc42 and Rac atThr35). Modification of Rho proteins causes pathogenic effects. Signaling of FZD via dishevelled (Dvl), including β-catenin (β-cat),Rac, and Rho signal pathways, is indicated. The proline-rich region (PRR) and the PDZ-binding region (PDZ) of CSPG4 are shown.
CSPG4 is expressed in various progenitor cells, including mesenchymal stem cells, perivascularcells, skeletal myoblasts, chondroblasts, and oligodendrocyte precursor cells, and is overexpressedin several tumors (e.g., melanoma, glioblastoma, and breast cancer). A role of this molecule inproliferation, differentiation, cell migration, and polarity has been suggested (96).
TcdB Binds to the Wnt Receptor Frizzled
Using CRISPR/Cas9-dependent genome-wide screenings, Wnt receptor Frizzled (FZD) proteinswere shown to be involved in binding and cellular uptake of TcdB (159). However, the toxin binds
286 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
to FZD not with the CROPs domain but with a sequence between residues 1,501 and 1,830.Thus, at least two receptors, CSPG4 and FZD, are independently involved in TcdB-bindingand uptake (159). The FZD protein family comprises highly conserved seven-transmembranereceptors, which are distinct from classic G protein–coupled receptors (GPCRs), including 10FZD proteins and the receptor of the hedgehog signaling pathway Smoothened (SMO) (145).FZDs share 20–40% identity. Typical for FZDs is an N-terminal cysteine-rich domain mainlyconsisting of helices, which is probably involved in binding of ligands of the Wnt family. Thisregion is also responsible for the binding of TcdB (159) (Figure 2). FZD1, 2, and 7 bind TcdBwith KD values of 32, 19, and 21 nM.
FZD receptors are essential for Wnt signaling. By controlling cell fate, proliferation, anddifferentiation, Wnt signaling pathways regulate stem cells and progenitor cells, control embryonicdevelopment, and play crucial roles in cancer (86). By interfering with the Wnt-binding site ofFZDs, TcdB blocks Wnt signaling (159). So-called noncanonical Wnt signaling pathways alsoinvolve Rho and Rac proteins (85) (Figure 2). It remains to be seen whether these pathways areespecially targeted by TcdB.
In addition, the protein poliovirus receptor–like 3 (PVRL3) has been reported to functionas a receptor for TcdB-mediated cytotoxicity (89). PVRL3 belongs to a family of four proteins(PVRL1, 2, 3, and 4; also called nectin-1, 2, 3, and 4) (108) that are related to the poliovirus receptor,PVR, and consists of three extracellular immunoglobulin-like domains, a single transmembranehelix, and a short cytoplasmic domain. However, some findings suggest that PVRL3 is not amajor receptor for TcdB: PVRL3 was not found in the CRISPR/Cas9-based screening, and therecombinant ectodomain of PVRL3 does not inhibit cytotoxicity of TcdB, whereas the ectodomainof FZD protects cells (159).
TOXIN UPTAKE
Early studies revealed that the cellular uptake of TcdA and TcdB is mediated by endocytosis (9,64) (Figure 2). The GTPase dynamin, which is involved in pinch-off of endocytic vesicles fromthe plasma membrane (5), is crucial for endocytosis of both toxins (123). However, the toxins differin their uptake pathways. Using Eps15 DN, a dominant-negative inhibitor of clathrin-mediatedendocytosis, or siRNA against the clathrin heavy chain, it was shown that TcdB uptake strictly de-pends on clathrin (123). By contrast, TcdA uptake does not involve clathrin- or caveolae-mediatedendocytosis (19, 47) but PACSIN2/Syndapin-II (19). PACSIN2 is a Bar (Bin/amphiphysin/rvs)-domain-containing protein that interacts with dynamin, regulates the actin cytoskeleton (169),and is involved in receptor-mediated endocytosis (134). Because different receptors are involvedin TcdA binding and TcdB binding, it is not surprising that different endocytic pathways areinvolved in their uptake.
MEMBRANE TRANSLOCATION
Many protein toxins, like diphtheria toxin (99), anthrax toxin (176), and Clostridium botulinumC2 toxin (8), which are translocated into the cytosol from endosomal compartments, depend onthe acidification of endosomal compartments. TcdA and TcdB are so-called short-trip toxins thatenter the cytosol from acidified endosomal compartments (9, 47, 64, 131). In contrast, long-triptoxins, like cholera toxin, Shiga toxin, and Pseudomonas aeruginosa exotoxin A, enter the cytosol af-ter retrograde transport through the Golgi to the endoplasmic reticulum (ER) (140). Accordingly,inhibition of vacuolar H+-ATPase by bafilomycin A blocks the translocation and cytotoxicity ofTcdA and TcdB (9, 131). The low pH of endosomes induces structural changes that force the inser-tion of hydrophobic areas of the toxins into endosomal membranes with subsequent translocation
www.annualreviews.org • Clostridium difficile Toxins 287
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
(9, 131). Therefore, reduction of the pH of extracellular medium allows toxin entry into targetcells without endocytosis (9). The mechanism of toxin translocation is not well understood. Toxin-mediated pore formation might be involved. In artificial membranes, the toxins induce an increasein membrane conductance at pH < 5.6 (9, 49). However, increased membrane conductivity exhibitsrapid fluctuations and not well-defined stepwise pore formation. In agreement with possible poreformation, TcdB and TcdA cause an increase in 86Rb ion release from preloaded cells after decreaseof the pH of the culture medium. 86Rb ion efflux depends on the cholesterol content of membranes.Depletion of cholesterol by methyl-β-cyclodextrin inhibits toxin-induced pore formation (49).
Toxins’ Regions Involved in Translocation
Deletion studies of TcdB revealed that the N-terminal part (amino acids 1–829), including gluco-syltransferase domain A (amino acids 1–543) and the following autoprocessing domain C (aminoacids 544–829), is not involved in pore formation in artificial membranes, lipid vesicles, or nativecell membranes (42). On the other hand, a C-terminal truncation of TcdB resulting in a toxinfragment of amino acids 1–990 is still able to release fluorescence dye from lipid vesicles and toincrease electrical conductance in artificial membranes (42). This leaves a pore-forming regionbetween residues 830 and 990. Moreover, a peptide covering residues 830 to 1,025 of TcdB in-creases electrical conductance at low pH in artificial lipid membranes (42). The crystal structureshows that the equivalent region of TcdA forms a small globular subdomain mainly formed byhelices (Figure 3). However, this small region is not able to translocate the enzyme domains ofthe toxin into the cytosol.
A hydrophobic part (residues 958–1,130 in TcdA and 956–1,128 in TcdB) was suggested to beinvolved in toxin membrane insertion and translocation into the cytosol (6, 167). In TcdA, onepart of this hydrophobic sequence is located in the helical subdomain and another part is stretchedout with 4 helices until the end of the protein (25). Within this α-helical hydrophobic stretch, asmall area has been identified, covering residues L1108–N1111 (Figure 3), that is conserved inmany clostridial glucosylating toxins, including C. sordellii TcsL, C. novyi TcnA, and C. perfringensTpeL (25, 179). Mutations in this region block 86Rb ion efflux and prevent glucosylation of targetproteins in intact cells, suggesting that membrane insertion and/or translocation of the toxin isaffected. Unfortunately, we have no further information about the possible mechanism involvedin translocation of the toxin into the cytosol.
PROCESSING OF THE TOXINS
All clostridial glycosylating toxins are processed by an autoproteolytic mechanism. Seminal werestudies showing that only the glycosyltransferase domain, and not the full-length toxin, reachesthe cytosol (125) and that the toxins are autoproteolytically cleaved depending on inositol hex-akisphosphate (InsP6) (135). All clostridial glycosylating toxins contain cysteine protease activity;the cysteine protease domain is located at the N terminus, following the glycosyltransferase do-main (31, 150) (Figures 1 and 3). Autocleavage occurs behind a highly conserved leucine residue(Leu542 in TcdA and Leu543 in TcdB), thereby releasing the N-terminal glucosyltransferasedomain from the rest of the protein (31, 139).
The autocatalytic cysteine protease domain (APD) covers residues 543–769 in TcdA(Figure 3) and 544–767 in TcdB. The domains, which have been crystallized (25, 127, 151), are56% identical in their amino acid sequences. Proposed active site residues are Cys700, His655,and Asp589 in TcdA (Cys698, His653, and Asp587 in TcdB). Exchange of each of these residuesblocks protease activity (31, 127). The cysteine protease type was deduced from sequence and struc-ture similarities with other cysteine proteases (150). However, recent crystal structure analysis,
288 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
V1109
N1110
N1111
GTD
SGS
APD
Deliverydomain
VNN loopInsP6
β flap
DXD motif
UDP-Glc
Catalytictriad
W101
β flap
N-terminal,4-helix bundle
Figure 3Functions of TcdA domains. The glucosyltransferase domain (GTD, residues 1–542): Trp101 (W101) andDXD motif (Asp285-X-Asp287) are involved in UDP-glucose (UDP-Glc) binding. The N-terminal, 4-helixbundle is involved in membrane binding of GTD. The autoprotease domain (APD) harbors the catalytictriad residues Cys700, His653, and Asp587. The back side shows the binding site of inositolhexakisphosphate (InsP6), with seven lysine residues ( yellow) important for binding. The β flap separates thecatalytic triad from the InsP6-binding side. Conformational changes of the β flap upon InsP6 bindingtransduce activation of the protease. A small globular subdomain (SGS, residues 850–1,025) includes part ofthe hydrophobic sequences (958–1,130) of the delivery domain. The rest of the hydrophobic sequences( green) are distributed down to the end of the protein structure. VNN loop: These small hydrophobicsequences (VNN loop, Val1109, Asn1110, and Asn1111) within the delivery domain are essential for toxintranslocation. Nonhydrophobic parts of the delivery domain are in yellow (PDB 4R04).
obtained with full-length TcdA without the C-terminal CROPs domain, surprisingly challengedthis view, showing the presence of a zinc ion at the active site (25). Moreover, chelation of zincby TPEN [N,N,N′,N′-tetrakis(2-pyridylmethyl)ethylenediamine] caused loss of autoprocessingactivity. Thus, the molecular mechanism of autoproteolysis is not clear.
Allosteric Activation by InsP6
The autoproteolytic activity of all clostridial glucosylating toxins is largely increased by InsP6
(31, 54, 135, 151). Isothermal titration calorimetry revealed a KD value of ∼2.5 μM for InsP6
binding to TcdB and a stoichiometry of 1:1 (30). InsP6 is a highly negatively charged molecule
www.annualreviews.org • Clostridium difficile Toxins 289
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
and binds at the back side of the APD in a pocket that contains several positively charged residues(Figure 3). The apo-APD of TcdA possesses four lysine residues (K602, K649, K754, and K777)at this site (25) that are all conserved within the toxin family. Binding of InsP6 causes majorstructural changes and thereby increases the number of interacting residues to seven lysines andone arginine. Therefore, binding affinity is in the low micromolar range. Thus, at the typicalcytosolic concentration of 10–100 μM InsP6, most translocated toxin molecules are activated byInsP6 binding. InsP6-mediated toxin activation is an allosteric mechanism. The binding side ofthe APD for InsP6 is completely separated from the catalytic side by a three-stranded β sheet(residues 746–765), called a β flap (127). InsP6 binding induces major conformational changes inthis β flap (151), which is probably propagated to the active site. Interestingly, the cysteine residueinvolved in toxin processing is the target of endogenous nitrosylation (142). Attachment of NOonto this residue decreases processing and, thereby, the activity of the toxin.
BIOLOGICAL ACTIVITY OF CLOSTRIDIAL GLUCOSYLATING TOXINS
Glucosyltransferase Domain
TcdA and TcdB are glucosyltransferases that attach glucose onto Rho proteins utilizing UDP-glucose as a cosubstrate (79, 80). In general, three structural types of glycosyltransferases exist:GT-A, GT-B, and GT-C. Clostridial glucosylating toxins belong to the GT-A family of gly-cosyltransferases. Typical for the GT-A-type structure is an α/β/α sandwich (Rossmann-likefold) of a seven-stranded β sheet with a 3214657 topology. According to CAZy nomenclature(http://www.cazy.org/), clostridial toxin glucosyltransferases form the unique glycosyltransferasefamily 44. This family now has >518 genes; in addition to clostridial glycosylating toxins, genesfrom Escherichia coli, Chlamydia spp., Pseudomonas spp., and Serratia spp. belong to this family.
The glucosyltransferase domain covers amino acids 1 to 543 in TcdB (1–542 in TcdA)(Figure 3). The enzymatic core of the glucosyltransferase of TcdB is represented by 234 residues,which mainly form parallel β strands (136). The 309 additional residues are peripheral and formmainly helices. A four-helix bundle (amino acid 1–90 in TcdB) that is located at the very N-terminal end of the glucosyltransferase domain, containing several basic amino acid residues, isprobably involved in plasma membrane binding of the glucosyltransferase domain (41).
Clostridial glucosyltransferases share many highly conserved amino acid residues that are es-sential for catalysis and typical for the whole group of GT-A-type glycosyltransferases. Of specialimportance is the DXD motif (D285/D287 in TcdA and D286/D288 in TcdB) that is essential forbinding of Mn2+ and the cosubstrate UDP-glucose. Whereas D286 binds Mn2+ directly, D288coordinates Mn2+ through a water molecule. A tryptophan residue (W101 in TcdA and W102 inTcdB) is involved in binding of the uracil of UDP-glucose by aromatic π-π stacking. Exchange ofthe above-mentioned residues inhibits the enzyme activity of the toxins (15, 16, 136). Such mutanttoxins are frequently used as controls in cell biology experiments or for vaccination. However,for complete blockade of enzyme activity, multiple mutations are necessary. Typical for GT-A-type glycosyltransferases is a flexible loop that defines an open and closed conformation of theenzymes (129, 132, 136, 180). This loop covers residues 516–522 in TcdA and 517–523 in TcdBand undergoes major conformational changes (>10 A) upon UDP-glucose binding.
TcdA and TcdB Are Retaining Glycosyltransferases
TcdA and TcdB glucosylate Rho proteins at threonine 35/37. This glucosylation reaction retainsthe α-glycosidic configuration of the donor substrate UDP-glucose in modified Rho proteins.Therefore, TcdA and TcdB (and all other clostridial glycosyltransferases) are assigned as retaining
290 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
Table 1 Protein substrates of TcdA and TcdBa
Toxin Targets Minor substrates
TcdA RhoA/B/C, Rac1, Cdc42, Rap2 TC10, Rap1, Ral, Ras, RhoG
TcdB RhoA/B/C, Rac1, Cdc42, TC10, TCL, RhoG Rap1/2, Ras
aData mainly based on References 44 and 178.
enzymes. This is important for the stability of the glucose-threonine bond in target cells. Thetoxin-catalyzed glucosylation is quasi-irreversible, because humans do not possess glucosidases inthe cytoplasm, which are able to cleave α-anomeric linkages.
Cosubstrate and Substrate Recognition
Whereas TcdA and TcdB transfer glucose onto Rho proteins, other clostridial glucosyltrans-ferases, like TcnA and TpeL, catalyze the attachment of N-acetylglucosamine (GlcNAc) ontotarget protein using UDP-GlcNAc (53, 113, 149). Donor sugar specificity is defined by only twoamino acids in TcdB. Thus, the Ile383Ser/Gln385Ala mutated TcdB accepts UDP-GlcNAc as acosubstrate (76).
Main protein substrates of TcdA and TcdB are Rho family proteins, including the prominentfamily members RhoA, B, and C; Rac; and Cdc42 (79, 80). Several studies have indicated thatdifferences in protein substrates exist between TcdA and TcdB (20, 129). Rap2 and R-Ras2 areminor substrates of TcdA but not of TcdB. Recently, the substrate specificity was studied in moredetail by means of extensive in vitro glucosylation analysis (44) and in vivo shotgun proteomicsanalysis (178); results of these studies are summarized in Table 1. Notably, assignment of substratespecificity is complicated by the existence of several isoforms of TcdA and TcdB. In addition, onehas to consider that most small GTPases are posttranslationally modified by isoprenylation. Invitro studies usually employ nonisoprenylated proteins. This might affect the substrate specificity.
No crystal structure of the complex of glucosyltransferase domain with its protein substrates isavailable. However, mutagenesis studies and alanine scanning reveal that residues Arg455, Asp461,Lys463, and Glu472 and amino acids of helix α17 of the glucosyltransferase domain of TcdB areessential for protein substrate recognition (75).
Rho Proteins as Targets of TcdA and TcdB
Rho proteins, the main substrates of TcdA and TcdB, are small 21–25 kDa GTP-binding proteinsthat belong to the Ras superfamily (1, 14, 17, 56, 73). About 20 Rho family members exist with thekey representatives RhoA, B, and C; Rac1 and 2; and Cdc42. Rho proteins are molecular switchesthat are involved in numerous signal processes (14, 17, 60). They are master regulators of thecytoskeleton and control motile processes like migration, phagocytosis, and intracellular traffic.Prototypical effects on the actin cytoskeleton are formation of stress fiber by RhoA, lamellipodiaby Rac, and filopodia by Cdc42 (56). Moreover, Rho proteins regulate transcription, cell cycleprogression, and apoptosis (73).
As molecular switches, Rho proteins are controlled by a GTPase cycle (Figure 4). They areinactive in the GDP-bound form and active after GTP binding (24). Numerous guanine nucleotideexchange proteins (GEFs) mediate GDP/GTP exchange and activate Rho (40). In the active form,Rho proteins interact with numerous effectors (14). The active GTP-bound state is terminatedby GTP hydrolysis, which is stimulated by various GTPase-activating proteins (GAPs) (24, 160).
www.annualreviews.org • Clostridium difficile Toxins 291
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
Epithelialbarrier
Migration
Phagocytosis
Cytokineproduction
Immune cellsignaling
O2–
production
Inflammasomeactivation
Signal
GEF
GAP
hoRhoGDP
RhoGTP
Inactive
Pi
Glucose
TcdATcdB
Effector
Figure 4GTPase cycle and inhibition by TcdA and TcdB. Rho GTPases are inactive in the GDP-bound state andactive with GTP bound. Guanine nucleotide exchange factors (GEFs) activate Rho proteins by GDP/GTPexchange. GTPase-activating proteins (GAPs) facilitate GTP hydrolysis and inhibit the active state of Rhoproteins. Active Rho proteins interact with multiple effectors to control fundamental cellular functions.Glucosylation of RhoA at Thr37 (Rac and Cdc42 at Thr35) blocks the interaction with effectors; severalsignal pathways and cellular functions are thereby affected that are crucial for host-pathogen interaction(e.g., epithelial barrier functions, migration, phagocytosis, cytokine production, immune cell signaling, andO2
− production). On the other hand, inactivation of RhoA by glucosylation activates the inflammasome.
Rho functions require posttranslational modification by isoprenylation and membrane association.Here, another regulatory principle comes into play: Guanine dissociation inhibitors (GDIs) keepRho in its inactive GDP-bound state in the cytosol and control Rho functions (38).
Functional Consequences of Rho Modification
Glucosylation of Rho proteins by TcdA and TcdB occurs in Thr35/37 (Rac, Cdc42 in Thr35;RhoA, B, and C in Thr37) (79, 80). This threonine residue is highly conserved in Rho/Ras proteinsand involved in coordination of the magnesium ion that is essential for nucleotide binding (69, 171).Moreover, Thr35/37 is located in the switch I-region of Rho proteins. The switch I- and switchII-regions (covering amino acids 29–42 and 62–68, respectively) undergo major conformationalchanges upon activation by GTP-binding and interact with Rho effectors for signal transmission.Therefore, the main effect of glucosylation of Rho proteins in Thr35/37 by TcdA and TcdB isthe blockade of the interaction of Rho proteins with their effectors, which may occur by sterichindrance (79). However, additional toxin effects have been identified: (a) Glucosylation inhibitsthe activation of Rho GTPases by GEF proteins and completely blocks the interaction with GAPs(148). (b) Toxin-induced glucosylation keeps Rho/Ras proteins in their inactive conformations(166). (c) Modified inactive Rho proteins remain attached to the cell membrane and are notextracted from membranes by GDI proteins (43).
292 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
FROM RHO MODIFICATION TO DISEASE
Rho proteins as main targets of TcdA and TcdB control numerous cellular functions. Therefore,key clinical features of CDIs, like diarrhea, inflammation, and enterocolitis, depend on differentpathogenic pathways. To address these topics mechanistically, we discuss toxin-induced cytopathiceffects, apoptosis, inflammasome activation, and reactive oxygen species (ROS) production.
Cytopathic Effects
Typical cytopathic features caused by TcdA and TcdB are changes in cell morphology, redistri-bution of the actin cytoskeleton with loss of stress fibers, and major shrinking of the cell withremaining irregular neurite-like extensions (36, 120). Redistribution of actin microfilaments (of-ten with no major increase in G-actin) precedes gross changes in cell shape and occurs when nochanges in microtubule or intermediate filament networks are observed (120). In fibroblasts, majorcytopathic effects of C. difficile toxins on the cytoskeleton have been preferentially attributed toglucosylation of Rac (55). The mutated RacQ61L protein, which is a poor substrate for toxin-catalyzed glucosylation, prevents cytopathic effects by TcdB. Moreover, the toxin isoform TcdBF(C. difficile strain 1470) and the related C. sordellii toxin TcsL, which modify Rac but not RhoA,cause similar cytopathic effects as TcdB (21). Early toxin effects cause disturbances of cell-cellcontacts and cell adhesion, resulting in loss of barrier functions and integrity of the intestinalepithelial cells (23, 61, 62, 77, 117, 118). Increase in paracellular permeability appears to occurmainly by alteration of tight junction functions, which are controlled by Rho proteins and actin(67, 117). Here, toxins cause dissociation of occludin, ZO-1, and ZO-2 from lipid-rich membranemicrodomains at tight junctions (118). Because similar effects are observed with TcsL, which doesnot modify RhoA, these effects have also been assigned to Rac glucosylation (45). However, reg-ulation of the cytoskeleton and of most actin-dependent processes, including cell-cell contacts,depends on a dynamic balance of Rho, Rac, and Cdc42 (104). Thus, toxin effects (dependingon time, toxin concentration, and cellular context) on one type of Rho proteins alter the RhoGTPase balance, with major consequences for the cytoskeletal organization (110). Therefore, asingle primary target of C. difficile toxins in cytopathic effects is not established.
Induction of Apoptosis
Both TcdA and TcdB induce apoptosis. This was shown in intestinal epithelium cell lines (13, 34,100, 130); primary epithelial cells (100); and human intestinal tissue, xenografted subcutaneouslyinto the scid mice model (141). Most studies showed that induction of apoptosis depends strictlyon the glucosyltransferase activity of the toxins (13, 48). Thus, the enzyme-deficient TcdA DXDmutant (D285N/D287N) is not able to trigger apoptosis in these cell models. In human colonadenocarcinoma HT-29 cells, TcdA induces activation of caspase-3, 8, and 9 and thereby triggersapoptotic cell death (48). Importantly, latrunculin B, which causes depolymerization of actinfilaments, does not induce apoptosis under the same conditions, showing that the toxin effect is notcaused merely by redistribution of the actin cytoskeleton. Activation of the executioner caspase-3correlates with glucosylation of Rac1 (48). However, a role of other Rho proteins cannot beexcluded. Dependent on cell type, Rho proteins have apoptotic or antiapoptotic effects (35). As inintestinal epithelium cells, TcdB induces apoptosis in endothelial cells (66). However, this effectof TcdB appears to depend on inactivation of RhoA. TcdBF, which glucosylates Rac1 and Cdc42but not RhoA, is not able to induce apoptotic death in these cells, whereas inactivation of RhoA bythe Rho-specific C3 ADP-ribosyltransferase causes apoptosis (66). Neuronal cells are also highly
www.annualreviews.org • Clostridium difficile Toxins 293
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
susceptible to TcdB-induced apoptosis (91, 156). Here, inactivation of Rac by TcdB is essential totrigger apoptosis. However, analysis of the apoptotic pathways revealed that the consequences ofselective inhibition of Rac (e.g., by the compound NSC23766, which prevents Rac activation) aredifferent from those of global Rho protein inhibition induced by TcdB (156). Thus, TcdB leadsto decreased degradation and enhanced transcription of Bim, whereas NSC23766 inhibition ofRac causes dephosphorylation and induction of Bad (156). These findings suggest that GTPasesother than Rac are involved in induction of apoptosis by TcdB.
Activation of the Inflammasome and Pyroptosis
Ng and coworkers (115) showed that TcdA and TcdB trigger inflammasome activation in an ASC[apoptosis-associated speck-like protein with a caspase recruitment domain (CARD)]-dependentmanner and cause release of interleukin-1β (IL-1β) (Figure 5). In a seminal study, the Shao groupidentified pyrin (also termed TRIM20 and marenostrin), the product of the Mediterranean fevergene MEFV, as an intracellular sensor for toxin-modified RhoA inflammasome activation (173).Similar to other cytoplasmic pattern recognition receptors, pyrin interacts with its PYD domainwith the adaptor protein ASC, which recruits and activates procaspase-1 (97). This interaction isapparently regulated by phosphorylation. Phosphorylation of Ser205 and Ser241 of mouse pyrinprevents interaction with ASC and favors binding to 14-3-3 proteins (39). Similarly, human pyrinis phosphorylated by the Rho effector protein kinase N (PKN) at Ser208 and Ser248, resultingin binding to 14-3-3 proteins and inhibition of inflammasome activation (124). A phosphataseinvolved in this regulation has not been identified. However, one can conclude that Rho inacti-vation by toxin-induced glucosylation (or by any other toxin-mediated Rho inhibition, e.g., byADP ribosylation, deamidation, or AMPylation), which decreases activation of the Rho effectorPKN, results in decreased phosphorylation of pyrin and an increase in inflammasome activity withcaspase-1 activation.
Caspase-1 is a key enzyme of innate immune defense and activates IL-1β and IL-18. Thesecytokines can, among other things, induce release of IL-6, interferon-γ (IFN-γ), and IL-8, re-spectively. This is in agreement with well-known findings that C. difficile toxins strongly activatethe release of IL-8 and IFN-γ (71, 72, 95, 100). IL-8 is a most potent attractant of neutrophils.Strong neutrophil invasion into colon mucosa is typical for CDI and is probably responsible formucosal damage and for control of infection.
Moreover, TcdB-induced activation of the pyrin inflammasome is a strong trigger for pyropto-sis. This is a cellular defense mechanism mainly against intracellular bacterial infection that aimsat removal of the replicative niche of the pathogen (78, 106). Pyroptosis is characterized by cellswelling and cell lysis with gross release of cellular content, which induces strong inflammation.This effect depends on pore formation of target cells caused by caspase-1-dependent activationof gasdermin D (caspase-4, -5, and -11 also activate gasdermin D; however, this is initiated bycytosolic lipopolysaccharide) (27, 143, 152, 153). Caspase-1 triggers pyroptosis by cleavage of thetwo-domain gasdermin D, thereby releasing the N-terminal part (gasdermin-N) from autoinhi-bition. Upon contact with lipid membranes, gasdermin-N oligomerizes, forms pores, and causespyroptosis. Gasdermin-N appears also to be involved in the release of inflammatory cytokines likeIL-1β (152).
ROS Production and Effects Not Related to Glucosylation of Rho Proteins
The participation of ROS in TcdA-induced enteritis in rats was first suggested by LaMont andcolleagues (133). Later, the Lacy group reported that TcdB at high concentrations (>100 pM)
294 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
Procaspase-1
Pyrininflammasome
(human pyrin)
Active caspase-1Gasdermin D
Pyroptosis
IL-1β/IL-18
Pro-IL-1β
Cytokine release
Microtubules
dephosphorylation
Phosphorylation/Rho
ASC
CARD
PYD
Pyrin inactive
PYD
B30.2domain
CC
PP
B
14-314-3-3
Glucose
Extracellular space
Cytoplasm
TcdB
FZD
Figure 5Effects of Rho glucosylation on activation of the inflammasome and on pyroptosis. Inactivation of Rhoproteins by glucosylation activates the pyrin inflammasome. Pyrin, which consists of the N-terminal pyrindomain (PYD), the B-box domain (B), the coiled-coil (CC) domain, and the B30.2 domain, is inactive afterphosphorylation by interaction with 14-3-3 proteins. Modification of Rho causes dephosphorylation of pyrin,which then forms an active inflammasome complex with ASC [apoptosis-associated speck-like protein with acaspase recruitment domain (CARD)] and procaspase-1. Interaction occurs through PYD and CARD domains.Formation of the active pyrin inflammasome depends on microtubules. Formed active caspase-1 cleavesand activates interleukin-1β (IL-1β) and IL-18. Moreover, gasdermin D is activated by proteolytic cleavageresulting in pore formation and pyroptosis. Gasdermin pores may also be involved in interleukin release.
induces ROS production by activation of epithelial cell NADPH oxidase (NOX), with necroticeffects, and rapid ATP depletion, lactate dehydrogenase (LDH) release, and loss of membraneintegrity but without caspase-3/7 activation (33). Surprisingly, these effects are independent of theglucosyltransferase activity of TcdB (33). Similar results were reported by Gerhard and cowork-ers (172), who found pyknotic cell death with chromatin condensation and cell cycle arrest andballooning of the nuclear envelope. These effects occurred at toxin concentrations 5,000 timesgreater than necessary for Rho protein glucosylation. Effects not only depended on ROS pro-duction and occurred with glucosyltransferase-inactive TcdB mutants, but also depended on thepresence of the glucosyltransferase domain (172). Donald et al. reported on residual cytotoxicityof high concentrations (8,000- to 10,000-fold greater than necessary for cytopathic effects of wild-type toxin) of TcdA and TcdB mutants lacking glucosyltransferase and autoproteolytic processing
www.annualreviews.org • Clostridium difficile Toxins 295
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
activities (28). The mechanism of cytotoxicity and significance of the effects of very high toxinconcentrations remain to be clarified.
THE BINARY C. DIFFICILE TRANSFERASE TOXIN
Five to thirty percent of C. difficile strains produce C. difficile transferase toxin (CDT) (46). Thistoxin has gained increasing attention, because it is frequently produced by so-called hypervirulentstrains of C. difficile (e.g., ribotype BI/NAP1/027), which cause increased morbidity and mortality(46). CDT belongs to the family of binary actin ADP-ribosylating toxins, which also includesC. botulinum C2 toxin, C. perfringens iota toxin and binary enterotoxin, Clostridium spiroforme toxin(CST), and the Bacillus cereus/Bacillus thuringiensis vegetative insecticidal proteins (VIPs) (7). Allthese toxins consist of two separated components. One component is involved in receptor bindingand toxin uptake. The other component is an enzyme and possesses ADP-ribosyltransferaseactivity (52).
Structure of CDT
The mature enzyme component CDTa (48 kDa, strain CD196) consists of two identically foldeddomains, suggesting evolution by gene duplication (58) (Figure 6). The N-terminal part is in-volved in the interaction with the binding component CDTb, and the C-terminal part harbors theADP-ribosyltransferase activity (residues 1–215 and 224–420, respectively, of the mature enzymeafter cleavage of a signal peptide of 42 amino acids). The binding component CDTb (98.8 kDa,876 amino acids), which is related to the protective antigen (PA) of anthrax toxin, is divided intofour domains. The N-terminal 257 residues form activation domain I. Domain II (residues 258–480) is involved in membrane insertion and pore formation. Domain III (amino acids 481–591)participates in oligomerization, and the C-terminal domain IV (amino acids 592–876) is involvedin receptor binding. The binding component CDTb is activated by proteolytic cleavage of theN-terminal domain I and release of an ∼20-kDa fragment. This cleavage allows oligomerizationand formation of heptamers. This process might occur in solution or on the surface of target cellsafter receptor binding (7).
Binding and Uptake of CDT
CDT binds to the lipolysis-stimulated lipoprotein receptor (LSR) (121) (Figure 7). LSR is a typeI single-pass transmembrane protein of 581 amino acids. It has an extracellular immunoglobulin-like domain and a long intracellular part. LSR is highly expressed in liver and many other tissues,like intestine, lung, and kidney (105). Notably, LSR is also the receptor for C. perfringens iota toxinand CST (121). LSR is involved in lipoprotein clearance (174, 175). The receptor is suggestedto participate in uptake and removal of apoB- and apoE-containing triglyceride-rich lipoproteinsand in clearance of low-density lipoprotein (LDL) by an LDL receptor–independent pathway.Remarkably, LSR is also involved in formation of tricellular tight junctions (102), which functionat the site of cell contact of three epithelial cells. It recruits the tricellular tight junction proteintricellulin, which is related to occludin (70). LSR belongs to a family of immunoglobulin-likedomain-containing receptors (ILDRs), which also have tight junction functions similar to thoseof LSR (65). However, only LSR functions as a receptor for CDT.
The activated binding component of CDT interacts with LSR, followed by accumulation inlipid rafts, oligomerization, and binding of the enzyme component (63, 114, 122). The toxin-receptor complex is endocytosed to reach a low pH compartment. Here, CDT inserts into thevesicle membrane to form a 14-strand transmembrane β-barrel channel, just as PA does (176).Translocation of CDT and refolding in the cytosol depend on intracellular folding helper proteins,
296 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
8761 258 481 592
Proteolyticactivation
CDT binding component (CDTb)
7×
ca
215 224
ADP-ribosyltransferase
4201
Adaptor
CDT enzymatic component (CDTa)
ART
ADP-ribosyltransferase
Adaptor
b
I II III IV
Figure 6(a) CDT consists of two separate components: CDTa (PDB 2WN7) is an ADP-ribosyltransferase thatmodifies actin, and CDTb is the binding component. (c) After proteolytic activation, CDTb formsheptamers. (b) CDTa consists of two domains. Both domains have the same ADP-ribosyltransferase fold.The N-terminal domain acts as an adaptor and interacts with the binding component, whereas theC-terminal domain possesses ADP-ribosyltransferase activity. The cosubstrate NAD+ is indicated. TheCDT binding component consists of four domains. Domain I is activated by proteolytic cleavage and thenforms heptamers. The structure of the heptameric binding component of CDT is deduced from the relatedstructure of Clostridium botulinum C2 toxin (PDB 2J42).
including Hsp90, peptidyl-prolyl cis-/trans-isomerase cyclophilin A, and FK506-binding protein51 (32, 59, 81).
CDT ADP-Ribosylates G-Actin
In the cytosol, CDTa ADP-ribosylates monomeric G-actin at Arg177 (52), thereby inhibitingactin polymerization (Figure 7). The same residue of actin is also modified by all other binaryactin ADP-ribosylating toxins, including iota toxin, CST, VIP, and C2 toxin (2, 165). ADP-ribosylated actin acts as a capping protein that binds to the barbed (fast-polymerizing) ends ofactin filaments. This inhibits polymerization of nonmodified actin (170). Because the pointedends of actin filaments remain free, actin still depolymerizes, eventually resulting in completedepolymerization of the actin cytoskeleton (3). This induces major changes in cell morphol-ogy, loss of barrier functions of epithelial cells, and alteration of numerous cellular functionsthat depend on the polymerizability of actin, like migration, phagocytosis, endocytosis, andsecretion.
www.annualreviews.org • Clostridium difficile Toxins 297
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
Integrin
Microtubule-basedprotrusions
C. difficileBa
sal
Api
cal
Rab5
Ca2+
Shortrecycling
Rab5Ca2+
Rab5
Longrecycling
Shortrecycling
Longrecycling
Rab5
Septins
Cdc42 Borg
F-actin
F-actin
Fibronectin
LSR
CDTb
Proteolyticactivation
HSP
NAD+
Microtubules
CDTa
Oligomer-
ization
Binding
H+
H+H+
CDT
Rab11
Rab4
Rab11
Rab5
Rab5
Rab4
Rab11
Ca2+
ADP-R
ADP-RADP-R
ADP-R
ADP-R
ADP-R
ADP-R
ADP-R
ADP-R
ADP-R
Figure 7Action of the binary toxin CDT on actin, microtubules, and vesicle traffic. Clostridium difficile releases the two components CDTa andCDTb of the binary toxin CDT. The monomeric binding component CDTb or the oligomer binds to its membrane receptor,lipolysis-stimulated lipoprotein receptor (LSR). Thereafter, the enzyme component CDTa binds to CDTb. The toxin-receptorcomplex is endocytosed and reaches low-pH endosomes. Here, the CDT heptamer inserts into membranes and forms a central porethrough which the enzyme component is translocated into the cytosol. Translocation and refolding of CDTa is facilitated bychaperones, including HSP90 (HSP) and cyclophilins. In the cytosol G-actin is ADP-ribosylated. ADP-ribosylated actin is unable topolymerize. Moreover, ADP-ribosylated actin acts as a capping protein to prevent polymerization of nonmodified actin. Numerousactin-dependent functions are thereby altered. Depolymerization of actin affects the microtubule system and induces microtubule-basedprotrusions. Formation of the protrusions depends on septins, which translocate to the plasma membrane; their translocation dependson Cdc42 and its effector protein Borg. Moreover, CDT-induced depolymerization of F-actin alters integrin-dependent endocytosisand recycling of extracellular matrix proteins like fibronectin. Fibronectin-containing Rab11-associated vesicles are rerouted to theapical membrane along microtubules. Microtubule-based protrusions and fibronectin interact with clostridia.
CDT-Induced ADP Ribosylation of Actin Affects Microtubule Structures
ADP-ribosylation of actin by CDT changes the organization and dynamics of microtubules. Mi-crotubules are long intracellular filaments that consist of α-/β-tubulin heterodimers. They havea polarized structure with a fast-growing “plus” end and a slow-growing “minus” end. Polymer-ization and growth of microtubules toward the cell membrane is usually stopped by contact withthe layer of cortical actin that is beneath the cell membrane, a process that is called capture ofmicrotubules. Treatment of epithelial cells with CDT (or other actin-depolymerizing toxins) dis-turbs the capture function of cortical actin by local actin depolymerization. At these sites, long
298 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
membrane protrusions develop, formed by growth of microtubule plus ends. The microtubule-based protrusions are 0.05–0.5 μm in diameter, with a length of up to several hundreds of microm-eters. The precise mechanism of CDT-induced protrusion formation is not clear. Recent studiessuggest a pivotal role of septins that are regulated by the small GTPase Cdc42 and its effectorprotein Borg (binder of Rho GTPases) (116) (Figure 7).
Functional Roles of CDT-Induced Microtubules
CDT-induced microtubule-based protrusions form a network on the surface of epithelial cells thatappears to increase the adherence of bacteria (147) (Figure 7). Moreover, the protrusions containvesicles, exhibiting anterograde and retrograde trafficking (146). Remarkably, the cell protrusionsalso contain tubules of ER (146), which connect to the distal tips of microtubules via the ERmembrane protein Stim1. In the protrusions, Stim1 can couple to Orai proteins, which functionas channels in store-operated calcium entry (SOCE). Thus, it has been suggested that the CDT-induced protrusions are capable of specific signaling (147). Another consequence of CDT-inducedF-actin depolymerization is the rerouting of fibronectin and of other extracellular matrix proteins,from the basolateral membrane of epithelial cells to the apical side, where they facilitate bindingof clostridia (146). Extracellular matrix proteins (e.g., fibronectin) interact with integrin receptorsat the basolateral side of epithelial cells, where they are endocytosed via integrin receptors andreach Rab5- and Rab11-associated vesicles. Usually, the vesicles are recycled and incorporatedwith the integrins into the basolateral membrane, a process that is involved in cell movementand motility. CDT-induced partial depolymerization of actin alters recycling of vesicles. By usingmicrotubules as tracks, the vesicles translocate to the apical membrane, where fibronectin andother extracellular membrane proteins are released (Figure 7). Thus, adherence of bacteria maybe increased by formation of the microtubule-based, tentacle-like web and by accumulation ofadhesive glycoproteins at the apical surface of cells, which exhibits increased affinity for clostridia.
CONCLUSIONS
Studies from recent years have largely increased our knowledge about the three C. difficile toxinsTcdA, TcdB, and CDT. Crystal structure analysis of TcdA has provided novel insights into thestructure of the translocation domain of clostridial glucosylating toxins (25), revealing a completenew fold for toxin translocation. The findings suggest that TcdA and probably all other clostridialglucosylating toxins use a novel, unknown molecular mechanism for cytosol translocation. Theidentification of FZD (159) and of CSPG4 (177) as membrane receptors for TcdB might be aprerequisite for development of novel antitoxin strategies. It is an exciting hypothesis that theWnt signaling pathway plays a role in TcdB pathogenesis, because it is essential for self-renewaland repair of the colonic epithelium (159). Also, the recent identification of RhoA as a sensor foractivation of the pyrin inflammasome and of pyroptosis is a major step forward in the understandingof the pathogenicity of CDI (173). Although we have obtained exciting new information aboutthe action of CDT on target cells, its relevance in CDI pathology is still unclear. While CDIsolely induced by CDT appears to be extremely rare, the binary toxin might be relevant as anenhancing factor for TcdA and TcdB pathogenicity. Recently, it was reported that CDT selectivelyinduces apoptosis of protective colonic eosinophils in a TLR2-dependent manner and therebyenhances C. difficile virulence (26). However, the precise pathway is not known. CDT acts notonly on the actin cytoskeleton but also on the microtubule system (146, 147), which appears toresult in an increase in Clostridia adhesion, colonization, and colonic inflammation. Notably, theactivation of the pyrin inflammasome depends on microtubule polymerization (e.g., colchicine
www.annualreviews.org • Clostridium difficile Toxins 299
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
depolymerizes microtubules and inhibits the pyrin inflammasome in Mediterranean fever) (seealso Figure 5). CDT enhances microtubule formation; thus, it would be of interest to studywhether CDT enhances TcdA- and TcdB-induced inflammasome activation. Many questionsremain. Concerning structure-function relationships and modes of action of toxins, progress inthe understanding of the membrane translocation of TcdA and TcdB is one of the most importantobjectives for future studies.
DISCLOSURE STATEMENT
The authors are not aware of any affiliations, memberships, funding, or financial holdings thatmight be perceived as affecting the objectivity of this review.
LITERATURE CITED
1. Aktories K. 2011. Bacterial protein toxins that modify host regulatory GTPases. Nat. Rev. Microbiol.9:487–98
2. Aktories K, Barmann M, Ohishi I, Tsuyama S, Jakobs KH, Habermann E. 1986. Botulinum C2 toxinADP-ribosylates actin. Nature 322:390–92
3. Aktories K, Wegner A. 1989. ADP-ribosylation of actin by clostridial toxins. J. Cell Biol. 109:1385–874. Amimoto K, Noro T, Oishi E, Shimizu M. 2007. A novel toxin homologous to large clostridial cytotoxins
found in culture supernatant of Clostridium perfringens type C. Microbiology 153:1198–2065. Antonny B, Burd C, De Camilli P, Chen E, Daumke O, et al. 2016. Membrane fission by dynamin: what
we know and what we need to know. EMBO J. 35:2270–846. Barroso LA, Moncrief JS, Lyerly DM, Wilkins TD. 1994. Mutagenesis of the Clostridium difficile toxin
B gene and effect on cytotoxic activity. Microb. Pathog. 16:297–3037. Barth H, Aktories K, Popoff MR, Stiles BG. 2004. Binary bacterial toxins: biochemistry, biology, and
applications of common Clostridium and Bacillus proteins. Microbiol. Mol. Biol. Rev. 68:373–4028. Barth H, Blocker D, Behlke J, Bergsma-Schutter W, Brisson A, et al. 2000. Cellular uptake of Clostridium
botulinum C2 toxin requires oligomerization and acidification. J. Biol. Chem. 275:18704–119. Barth H, Pfeifer G, Hofmann F, Maier E, Benz R, Aktories K. 2001. Low pH-induced formation of ion
channels by Clostridium difficile toxin B in target cells. J. Biol. Chem. 276:10670–7610. Biname F. 2014. Transduction of extracellular cues into cell polarity: the role of the transmembrane
proteoglycan NG2. Mol. Neurobiol. 50:482–9311. Bouillaut L, Dubois T, Sonenshein AL, Dupuy B. 2015. Integration of metabolism and virulence in
Clostridium difficile. Res. Microbiol. 166:375–8312. Braun V, Hundsberger T, Leukel P, Sauerborn M, Von Eichel-Streiber C. 1996. Definition of the single
integration site of the pathogenicity locus in Clostridium difficile. Gene 181:29–3813. Brito GAC, Fujji J, Carneiro-Filho BA, Lima AAM, Obrig T, Guerrant RL. 2002. Mechanism of Clostrid-
ium difficile toxin A—induced apoptosis in T84 cells. J. Infect. Dis. 186:1438–4714. Burridge K, Wennerberg K. 2004. Rho and Rac take center stage. Cell 116:167–7915. Busch C, Hofmann F, Gerhard R, Aktories K. 2000. Involvement of a conserved tryptophan residue in
the UDP-glucose binding of large clostridial cytotoxin glycosyltransferases. J. Biol. Chem. 275:13228–3416. Busch C, Hofmann F, Selzer J, Munro J, Jeckel D, Aktories K. 1998. A common motif of eukaryotic
glycosyltransferases is essential for the enzyme activity of large clostridial cytotoxins. J. Biol. Chem.273:19566–72
17. Bustelo XR, Sauzeau V, Berenjeno IM. 2007. GTP-binding proteins of the Rho/Rac family: regulation,effectors and functions in vivo. BioEssays 29:356–70
18. Carter GP, Chakravorty A, Pham Nguyen TA, Mileto S, Schreiber F, et al. 2015. Defining the rolesof TcdA and TcdB in localized gastrointestinal disease, systemic organ damage, and the host responseduring Clostridium difficile infections. mBio 6:e00551
19. Chandrasekaran R, Kenworthy AK, Lacy DB. 2016. Clostridium difficile toxin A undergoes clathrin-independent, PACSIN2-dependent endocytosis. PLOS Pathog. 12:e1006070
300 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
20. Chaves-Olarte E, Freer E, Parra A, Guzman-Verri C, Moreno E, Thelestam M. 2003. R-Ras glucosy-lation and transient RhoA activation determine the cytopathic effect produced by toxin B variants fromtoxin A-negative strains of Clostridium difficile. J. Biol. Chem. 278:7956–63
21. Chaves-Olarte E, Low P, Freer E, Norlin T, Weidmann M, et al. 1999. A novel cytotoxin from Clostridiumdifficile serogroup F is a functional hybrid between two other large clostridial cytotoxins. J. Biol. Chem.274:11046–52
22. Chaves-Olarte E, Weidmann M, Von Eichel-Streiber C, Thelestam M. 1997. Toxins A and B fromClostridium difficile differ with respect to enzymatic potencies, cellular substrate specificities, and surfacebinding to cultured cells. J. Clin. Investig.100:1734–41
23. Chen ML, Pothoulakis C, LaMont JT. 2002. Protein kinase C signaling regulates ZO-1 translocationand increased paracellular flux of T84 colonocytes exposed to Clostridium difficile toxin A. J. Biol. Chem.277:4247–54
24. Cherfils J, Zeghouf M. 2013. Regulation of small GTPases by GEFs, GAPs, and GDIs. Physiol. Rev.93:269–309
25. Chumbler NM, Rutherford SA, Zhang Z, Farrow MA, Lisher JP, et al. 2016. Crystal structure ofClostridium difficile toxin A. Nat. Microbiol. 1:15002
26. Cowardin CA, Buonomo EL, Saleh MM, Wilson MG, Burgess SL, et al. 2016. The binary toxin CDTenhances Clostridium difficile virulence by suppressing protective colonic eosinophilia. Nat. Microbiol.1:16108
27. Ding J, Wang K, Liu W, She Y, Sun Q, et al. 2016. Pore-forming activity and structural autoinhibitionof the gasdermin family. Nature 535:111–16
28. Donald RG, Flint M, Kalyan N, Johnson E, Witko SE, et al. 2013. A novel approach to generate arecombinant toxoid vaccine against Clostridium difficile. Microbiology 159:1254–66
29. Dove CH, Wang SZ, Price SB, Phelps CJ, Lyerly DM, et al. 1990. Molecular characterization of theClostridium difficile toxin A gene. Infect. Immun. 58:480–88
30. Egerer M, Giesemann T, Herrmann C, Aktories K. 2009. Autocatalytic processing of Clostridium difficiletoxin B: binding of inositol hexakisphosphate. J. Biol. Chem. 284:3389–95
31. Egerer M, Giesemann T, Jank T, Satchell KJ, Aktories K. 2007. Auto-catalytic cleavage of Clostridiumdifficile toxins A and B depends on a cysteine protease activity. J. Biol. Chem. 282:25314–21
32. Ernst K, Langer S, Kaiser E, Osseforth C, Michaelis J, et al. 2015. Cyclophilin-facilitated membranetranslocation as pharmacological target to prevent intoxication of mammalian cells by binary clostridialactin ADP-ribosylated toxins. J. Mol. Biol. 427:1224–38
33. Farrow MA, Chumbler NM, Lapierre LA, Franklin JL, Rutherford SA, et al. 2013. Clostridium diffi-cile toxin B-induced necrosis is mediated by the host epithelial cell NADPH oxidase complex. PNAS110:18674–79
34. Fiorentini C, Fabbri A, Falzano L, Fattorossi A, Matarrese P, et al. 1998. Clostridium difficile toxin Binduces apoptosis in intestinal cultured cells. Infect. Immun. 66:2660–65
35. Fiorentini C, Falzano L, Travaglione S, Fabbri A. 2003. Hijacking Rho GTPases by protein toxins andapoptosis: molecular strategies of pathogenic bacteria. Cell Death Differ. 10:147–52
36. Fiorentini C, Thelestam M. 1991. Clostridium difficile toxin A and its effects on cells. Toxicon 29:543–6737. Frey SM, Wilkins TD. 1992. Localization of two epitopes recognized by monoclonal antibody PCG-4
on Clostridium difficile toxin A. Infect. Immun. 60:2488–9238. Fukumoto Y, Kaibuchi K, Hori Y, Fujioka H, Araki S, et al. 1990. Molecular cloning and characterization
of a novel type of regulatory protein (GDI) for the rho proteins, ras p21-like small GTP-binding proteins.Oncogene 5:1321–28
39. Gao W, Yang J, Liu W, Wang Y, Shao F. 2016. Site-specific phosphorylation and microtubule dynamicscontrol Pyrin inflammasome activation. PNAS 113:E4857–66
40. Garcia-Mata R, Burridge K. 2007. Catching a GEF by its tail. Trends Cell Biol. 17:36–4341. Geissler B, Tungekar R, Satchell KJ. 2010. Identification of a conserved membrane localization domain
within numerous large bacterial protein toxins. PNAS 107:5581–8642. Genisyuerek S, Papatheodorou P, Guttenberg G, Schubert R, Benz R, Aktories K. 2011. Structural
determinants for membrane insertion, pore formation and translocation of Clostridium difficile toxin B.Mol. Microbiol. 79:1643–54
www.annualreviews.org • Clostridium difficile Toxins 301
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
43. Genth H, Aktories K, Just I. 1999. Monoglucosylation of RhoA at threonine-37 blocks cytosol-membranecycling. J. Biol. Chem. 274:29050–56
44. Genth H, Pauillac S, Schelle I, Bouvet P, Bouchier C, et al. 2014. Haemorrhagic toxin and lethal toxinfrom Clostridium sordellii strain vpi9048: molecular characterization and comparative analysis of substratespecificity of the large clostridial glucosylating toxins. Cell. Microbiol.16:1706–21
45. Geny B, Grassart A, Manich M, Chicanne G, Payrastre B, et al. 2010. Rac1 inactivation by lethal toxinfrom Clostridium sordellii modifies focal adhesions upstream of actin depolymerization. Cell. Microbiol.12:217–32
46. Gerding DN, Johnson S, Rupnik M, Aktories K. 2014. Clostridium difficile binary toxin CDT: mechanism,epidemiology, and potential clinical importance. Gut Microbes 5:15–27
47. Gerhard R, Frenzel E, Goy S, Olling A. 2013. Cellular uptake of Clostridium difficile TcdA and truncatedTcdA lacking the receptor binding domain. J. Med. Microbiol. 62:1414–22
48. Gerhard R, Nottrott S, Schoentaube J, Tatge H, Olling A, Just I. 2008. Glucosylation of Rho GTPasesby Clostridium difficile toxin A triggers apoptosis in intestinal epithelial cells. J. Med. Microbiol. 57:765–70
49. Giesemann T, Jank T, Gerhard R, Maier E, Just I, et al. 2006. Cholesterol-dependent pore formationof Clostridium difficile toxin A. J. Biol. Chem. 281:10808–15
50. Govind R, Dupuy B. 2012. Secretion of Clostridium difficile toxins A and B requires the holin-like proteinTcdE. PLOS Pathog. 8:e1002727
51. Greco A, Ho JG, Lin SJ, Palcic MM, Rupnik M, Ng KK. 2006. Carbohydrate recognition by Clostridiumdifficile toxin A. Nat. Struct. Mol. Biol. 13:460–1
52. Gulke I, Pfeifer G, Liese J, Fritz M, Hofmann F, et al. 2001. Characterization of the enzymatic componentof the ADP-ribosyltransferase toxin CDTa from Clostridium difficile. Infect. Immun. 69:6004–11
53. Guttenberg G, Hornei S, Jank T, Schwan C, Lu W, et al. 2012. Molecular characteristics of Clostridiumperfringens TpeL toxin and consequences of mono-O-GlcNAcylation of Ras in living cells. J. Biol. Chem.287:24929–40
54. Guttenberg G, Papatheodorou P, Genisyuerek S, Lu W, Jank T, et al. 2011. Inositol hexakisphosphate-dependent processing of Clostridium sordellii lethal toxin and Clostridium novyi α-toxin. J. Biol. Chem.286:14779–86
55. Halabi-Cabezon I, Huelsenbeck J, May M, Ladwein M, Rottner K, et al. 2008. Prevention of the cyto-pathic effect induced by Clostridium difficile toxin B by active Rac1. FEBS Lett. 582:3751–56
56. Hall A. 1994. Small GTP-binding proteins and the regulation of the actin cytoskeleton. Annu. Rev. CellBiol. 10:31–54
57. Hammond GA, Johnson JL. 1995. The toxigenic element of Clostridium difficile strain VPI 10463. Microb.Pathog. 19:203–13
58. Han S, Craig JA, Putnam CD, Carozzi NB, Tainer JA. 1999. Evolution and mechanism from structuresof an ADP-ribosylating toxin and NAD complex. Nat. Struct. Biol. 6:932–36
59. Haug G, Leemhuis J, Tiemann D, Meyer DK, Aktories K, Barth H. 2003. The host cell chaperoneHsp90 is essential for translocation of the binary Clostridium botulinum C2 toxin into the cytosol. J. Biol.Chem. 274:32266–74
60. Heasman SJ, Ridley AJ. 2008. Mammalian Rho GTPases: new insights into their functions from in vivostudies. Nat. Rev. Mol. Cell Biol. 9:690–701
61. Hecht G, Koutsouris A, Pothoulakis C, LaMont JT, Madara JL. 1992. Clostridium difficile toxin B disruptsthe barrier function of T84 monolayers. Gastroenterology 102:416–23
62. Hecht G, Pothoulakis C, LaMont JT, Madara JL. 1988. Clostridium difficile toxin A perturbs cytoskeletalstructure and tight junction permeability of cultured human intestinal epithelial monolayers. J. Clin.Investig. 82:1516–24
63. Hemmasi S, Czulkies BA, Schorch B, Veit A, Aktories K, Papatheodorou P. 2015. Interaction of theClostridium difficile binary toxin CDT and its host cell receptor, lipolysis-stimulated lipoprotein receptor(LSR). J. Biol. Chem. 290:14031–44
64. Henriques B, Florin I, Thelestam M. 1987. Cellular internalisation of Clostridium difficile toxin A. Microb.Pathogen. 2:455–63
302 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
65. Higashi T, Tokuda S, Kitajiri SI, Masuda S, Nakamura H, et al. 2012. Analysis of the angulin familyconsisting of LSR, ILDR1 and ILDR2: tricellulin recruitment, epithelial barrier function and implicationin deafness pathogenesis. J. Cell Sci. 126:966–77
66. Hippenstiel S, Schmeck B, N’Guessan PD, Seybold J, Krull M, et al. 2002. Rho protein inactivationinduced apoptosis of cultured human endothelial cells. Am. J. Physiol. Lung Cell. Mol. Physiol. 283:L830–38
67. Hirase T, Kawashima S, Wong EY, Ueyama T, Rikitake Y, et al. 2001. Regulation of tight junctionpermeability and occludin phosphorylation by Rhoa-p160ROCK-dependent and -independent mecha-nisms. J. Biol. Chem. 276:10423–31
68. Ho JG, Greco A, Rupnik M, Ng KK. 2005. Crystal structure of receptor-binding C-terminal repeatsfrom Clostridium difficile toxin A. PNAS 102:18373–78
69. Ihara K, Muraguchi S, Kato M, Shimizu T, Shirakawa M, et al. 1998. Crystal structure of human RhoAin a dominantly active form complexed with a GTP analogue. J. Biol. Chem. 273:9656–66
70. Ikenouchi J, Furuse M, Furuse K, Sasaki H, Tsukita S, Tsukita S. 2005. Tricellulin constitutes a novelbarrier at tricellular contacts of epithelial cells. J. Cell Biol. 171:939–45
71. Ishida Y, Maegawa T, Kondo T, Kimura A, Iwakura Y, et al. 2004. Essential involvement of IFN-gammain Clostridium difficile toxin A-induced enteritis. J. Immunol. 172:3018–25
72. Jafari NV, Kuehne SA, Bryant CE, Elawad M, Wren BW, et al. 2013. Clostridium difficile modulates hostinnate immunity via toxin-independent and dependent mechanism(s). PLOS ONE 8:e69846
73. Jaffe AB, Hall A. 2005. Rho GTPases: biochemistry and biology. Annu. Rev. Cell Dev. Biol. 21:247–6974. Jank T, Aktories K. 2008. Structure and mode of action of clostridial glucosylating toxins: the ABCD
model. Trends Microbiol. 16:222–2975. Jank T, Giesemann T, Aktories K. 2007. Clostridium difficile glucosyltransferase toxin B-essential amino
acids for substrate binding. J. Biol. Chem. 282:35222–3176. Jank T, Reinert DJ, Giesemann T, Schulz GE, Aktories K. 2005. Change of the donor substrate specificity
of Clostridium difficile toxin B by site-directed mutagenesis. J. Biol. Chem. 280:37833–3877. Johal SS, Solomon K, Dodson S, Borriello SP, Mahida YR. 2004. Differential effects of varying concen-
trations of Clostridium difficile toxin A on epithelial barrier function and expression of cytokines. J. Infect.Dis. 189:2110–19
78. Jorgensen I, Miao EA. 2015. Pyroptotic cell death defends against intracellular pathogens. Immunol. Rev.265:130–42
79. Just I, Selzer J, Wilm M, Von Eichel-Streiber C, Mann M, Aktories K. 1995. Glucosylation of Rhoproteins by Clostridium difficile toxin B. Nature 375:500–3
80. Just I, Wilm M, Selzer J, Rex G, Von Eichel-Streiber C, et al. 1995. The enterotoxin from Clostridiumdifficile (ToxA) monoglucosylates the Rho proteins. J. Biol. Chem. 270:13932–36
81. Kaiser E, Bohm N, Ernst K, Langer S, Schwan C, et al. 2012. FK506-binding protein 51 interacts withClostridium botulinum C2 toxin and FK506 inhibits membrane translocation of the toxin in mammaliancells. Cell Microbiol. 14:1193–205
82. Karlsson S, Burman LG, Akerlund T. 1999. Suppression of toxin production in Clostridium difficile VPI10463 by amino acids. Microbiology 145(Part 7):1683–93
83. Karlsson S, Lindberg A, Norin E, Burman LG, Akerlund T. 2000. Toxins, butyric acid, and other short-chain fatty acids are coordinately expressed and down-regulated by cysteine in Clostridium difficile. Infect.Immun. 68:5881–88
84. Kelly CP, LaMont JT. 2008. Clostridium difficile—more difficult than ever. N. Engl. J. Med. 359:1932–4085. Kishida S, Yamamoto H, Kikuchi A. 2004. Wnt-3a and Dvl induce neurite retraction by activating
Rho-associated kinase. Mol. Cell. Biol. 24:4487–50186. Klaus A, Birchmeier W. 2008. Wnt signalling and its impact on development and cancer. Nat. Rev.
Cancer 8:387–9887. Krivan HC, Clark GF, Smith DF, Wilkins TD. 1986. Cell surface binding site for Clostridium difficile
enterotoxin: evidence for a glycoconjugate containing the sequence Gal α1-3Galβ1-4GlcNAc. Infect.Immun. 53:573–81
88. Kuehne SA, Cartman ST, Heap JT, Kelly ML, Cockayne A, Minton NP. 2010. The role of toxin A andtoxin B in Clostridium difficile infection. Nature 467:711–13
www.annualreviews.org • Clostridium difficile Toxins 303
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
89. LaFrance ME, Farrow MA, Chandrasekaran R, Sheng J, Rubin DH, Lacy DB. 2015. Identification of anepithelial cell receptor responsible for Clostridium difficile TcdB-induced cytotoxicity. PNAS 112:7073–78
90. Lambert GS, Baldwin MR. 2016. Evidence for dual receptor-binding sites in Clostridium difficile toxinA. FEBS Lett. 590:4550–63
91. Le SS, Loucks FA, Udo H, Richardson-Burns S, Phelps RA, et al. 2005. Inhibition of Rac GTPasetriggers a c-Jun- and Bim-dependent mitochondrial apoptotic cascade in cerebellar granule neurons.J. Neurochem. 94:1025–39
92. Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK, et al. 2015. Burden of Clostridium difficileinfection in the United States. N. Engl. J. Med. 372:825–34
93. Leuzzi R, Spencer J, Buckley A, Brettoni C, Martinelli M, et al. 2013. Protective efficacy induced byrecombinant Clostridium difficile toxin fragments. Infect. Immun. 81:2851–60
94. Lima AAM, Lyerly DM, Wilkins TD, Innes DJ, Guerrant RL. 1988. Effects of Clostridium difficiletoxins A and B in rabbit small and large intestine in vivo and on cultured cells in vitro. Infect. Immun.56:582–88
95. Linevsky JK, Pothoulakis C, Keates S, Warny M, Keates AC, et al. 1997. IL-8 release and neutrophilactivation by Clostridium difficile toxin-exposed human monocytes. Am. J. Physiol. 273:G1333–40
96. Lord MS, Whitelock JM. 2013. Recombinant production of proteoglycans and their bioactive domains.FEBS J. 280:2490–510
97. Lu A, Wu H. 2015. Structural mechanisms of inflammasome assembly. FEBS J. 282:435–4498. Lyras D, O’Connor JR, Howarth PM, Sambol SP, Carter GP, et al. 2009. Toxin B is essential for
virulence of Clostridium difficile. Nature 458(7242):1176–7999. Madshus IH, Stenmark H, Sandvig K, Olsnes S. 1991. Entry of diphtheria toxin-protein A chimeras into
cells. J. Biol. Chem. 266:17446–53100. Mahida YR, Makh S, Hyde S, Gray T, Borriello SP. 1996. Effect of Clostridium difficile toxin A on human
intestinal epithelial cells: induction of interleukin 8 production and apoptosis after cell detachment. Gut38:337–47
101. Mani N, Dupuy B. 2001. Regulation of toxin synthesis in Clostridium difficile by an alternative RNApolymerase sigma factor. PNAS 98:5844–49
102. Masuda S, Oda Y, Sasaki H, Ikenouchi J, Higashi T, et al. 2011. LSR defines cell corners for tricellulartight junction formation in epithelial cells. J. Cell Sci. 124:548–55
103. Matamouros S, England P, Dupuy B. 2007. Clostridium difficile toxin expression is inhibited by the novelregulator TcdC. Mol. Microbiol. 64:1274–88
104. McCormack J, Welsh NJ, Braga VM. 2013. Cycling around cell-cell adhesion with Rho GTPase regu-lators. J. Cell. Sci. 126:379–91
105. Mesli S, Javorschi S, Berard AM, Landry M, Priddle H, et al. 2004. Distribution of the lipolysis stimulatedreceptor in adult and embryonic murine tissues and lethality of LSR−/− embryos at 12.5 to 14.5 days ofgestation. Eur. J. Biochem. 271:3103–14
106. Miao EA, Leaf IA, Treuting PM, Mao DP, Dors M, et al. 2010. Caspase-1-induced pyroptosis is aninnate immune effector mechanism against intracellular bacteria. Nat. Immunol. 11:1136–42
107. Mitchell TJ, Ketley JM, Haslam SC, Stephen J, Burdon DW, et al. 1986. Effect of toxin A and B ofClostridium difficile on rabbit ileum and colon. Gut 27:78–85
108. Miyoshi J, Takai Y. 2007. Nectin and nectin-like molecules: biology and pathology. Am. J. Nephrol.27:590–604
109. Monot M, Eckert C, Lemire A, Hamiot A, Dubois T, et al. 2015. Clostridium difficile: new insights intothe evolution of the pathogenicity locus. Sci. Rep. 5:15023
110. Moorman JP, Luu D, Wickham J, Bobak DA, Hahn CS. 1999. A balance of signaling by Rho family smallGTPases RhoA, Rac1 and Cdc42 coordinates cytoskeletal morphology but not cell survival. Oncogene18:47–57
111. Murase T, Eugenio L, Schorr M, Hussack G, Tanha J, et al. 2014. Structural basis for antibody recogni-tion in the receptor-binding domains of toxins A and B from Clostridium difficile. J. Biol. Chem. 289:2331–43
112. Na X, Kim H, Moyer MP, Pothoulakis C, LaMont JT. 2008. gp96 is a human colonocyte plasmamembrane binding protein for Clostridium difficile toxin A. Infect. Immun. 76:2862–71
304 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
113. Nagahama M, Ohkubo A, Oda M, Kobayashi K, Amimoto K, et al. 2011. Clostridium perfringens TpeLglycosylates the Rac and Ras subfamily proteins. Infect. Immun. 79(2):905–10
114. Nagahama M, Yamaguchi A, Hagiyama T, Ohkubo N, Kobayashi K, Sakurai J. 2004. Binding andinternalization of Clostridium perfringens iota-toxin in lipid rafts. Infect. Immun. 72:3267–75
115. Ng J, Hirota SA, Gross O, Li Y, Ulke-Lemee A, et al. 2010. Clostridium difficile toxin-induced inflam-mation and intestinal injury are mediated by the inflammasome. Gastroenterology 139:542–52.e3
116. Nolke T, Schwan C, Lehmann F, Ostevold K, Pertz O, Aktories K. 2016. Septins guide microtubuleprotrusions induced by actin-depolymerizing toxins like Clostridium difficile transferase (CDT). PNAS113:7870–75
117. Nusrat A, Giry M, Turner JR, Colgan SP, Parkos CA, et al. 1995. Rho protein regulates tight junctionsand perijunctional actin organization in polarized epithelia. PNAS 92:10629–33
118. Nusrat A, Von Eichel-Streiber C, Turner JR, Verkade P, Madara JL, Parkos CA. 2001. Clostridiumdifficile toxins disrupt epithelial barrier function by altering membrane microdomain localization of tightjunction proteins. Infect. Immun. 69:1329–36
119. Orth P, Xiao L, Hernandez LD, Reichert P, Sheth PR, et al. 2014. Mechanism of action and epitopesof Clostridium difficile toxin B-neutralizing antibody bezlotoxumab revealed by X-ray crystallography.J. Biol. Chem. 289:18008–21
120. Ottlinger ME, Lin S. 1988. Clostridium difficile toxin B induces reorganization of actin, vinculin, and talinin cultures cells. Exp. Cell. Res. 174:215–29
121. Papatheodorou P, Carette JE, Bell GW, Schwan C, Guttenberg G, et al. 2011. Lipolysis-stimulatedlipoprotein receptor (LSR) is the host receptor for the binary toxin Clostridium difficile transferase (CDT).PNAS 108:16422–27
122. Papatheodorou P, Hornuss D, Nolke T, Hemmasi S, Castonguay J, et al. 2013. Clostridium difficilebinary toxin CDT induces clustering of the lipolysis-stimulated lipoprotein receptor into lipid rafts.mBio 4:e00244-13
123. Papatheodorou P, Zamboglou C, Genisyuerek S, Guttenberg G, Aktories K. 2010. Clostridial glucosy-lating toxins enter cells via clathrin-mediated endocytosis. PLOS ONE 5:e10673
124. Park YH, Wood G, Kastner DL, Chae JJ. 2016. Pyrin inflammasome activation and RhoA signaling inthe autoinflammatory diseases FMF and HIDS. Nat. Immunol. 17:914–21
125. Pfeifer G, Schirmer J, Leemhuis J, Busch C, Meyer DK, et al. 2003. Cellular uptake of Clostridiumdifficile toxin B: translocation of the N-terminal catalytic domain into the cytosol of eukaryotic cells.J. Biol. Chem. 278:44535–41
126. Pothoulakis C, Gilbert RJ, Cladaras C, Castagliuolo I, Semenza G, et al. 1996. Rabbit sucrase-isomaltasecontains a functional intestinal receptor for Clostridium difficile toxin A. J. Clin. Investig. 98:641–49
127. Pruitt RN, Chagot B, Cover M, Chazin WJ, Spiller B, Lacy DB. 2009. Structure-function analysis of inos-itol hexakisphosphate-induced autoprocessing in Clostridium difficile toxin A. J. Biol. Chem. 284:21934–40
128. Pruitt RN, Chambers MG, Ng KK, Ohi MD, Lacy DB. 2010. Structural organization of the functionaldomains of Clostridium difficile toxins A and B. PNAS 107:13467–72
129. Pruitt RN, Chumbler NM, Rutherford SA, Farrow MA, Friedman DB, et al. 2012. Structural determi-nants of Clostridium difficile toxin A glucosyltransferase activity. J. Biol. Chem. 287:8013–20
130. Qa’Dan M, Christensen KA, Zhang L, Roberts TM, Collier RJ. 2005. Membrane insertion by anthraxprotective antigen in cultured cells. Mol. Cell. Biol. 25:5492–98
131. Qa’Dan M, Spyres LM, Ballard JD. 2000. pH-induced conformational changes in Clostridium difficiletoxin B. Infect. Immun. 68:2470–74
132. Qasba PK, Ramakrishnan B, Boeggeman E. 2005. Substrate-induced conformational changes in glyco-syltransferases. Trends Biochem. Sci. 30:53–62
133. Qiu B, Pothoulakis C, Castagliuolo I, Nikulasson S, LaMont JT. 1999. Participation of reactive oxygenmetabolites in Clostridium difficile toxin A-induced enteritis in rats. Am. J. Physiol. 276:G485–90
134. Qualmann B, Kelly RB. 2000. Syndapin isoforms participate in receptor-mediated endocytosis and actinorganization. J. Cell Biol. 148:1047–62
135. Reineke J, Tenzer S, Rupnik M, Koschinski A, Hasselmayer O, et al. 2007. Autocatalytic cleavage ofClostridium difficile toxin B. Nature 446:415–19
www.annualreviews.org • Clostridium difficile Toxins 305
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
136. Reinert DJ, Jank T, Aktories K, Schulz GE. 2005. Structural basis for the function of Clostridium difficiletoxin B. J. Mol. Biol. 351:973–81
137. Riegler M, Sedivy R, Pothoulakis C, Hamilton G, Zacheri J, et al. 1995. Clostridium difficile toxin B ismore potent than toxin A in damaging human colonic epithelium in vitro. J. Clin. Investig. 95:2004–11
138. Rupnik M, Janezic S. 2016. An update on Clostridium difficile toxinotyping. J. Clin. Microbiol. 54:13–18139. Rupnik M, Pabst S, Rupnik M, Von Eichel-Streiber C, Urlaub H, Soling HD. 2005. Characterization
of the cleavage site and function of resulting cleavage fragments after limited proteolysis of Clostridiumdifficile toxin B (TcdB) by host cells. Microbiology 151:199–208
140. Sandvig K, Skotland T, van Deurs B, Klokk TI. 2013. Retrograde transport of protein toxins throughthe Golgi apparatus. Histochem. Cell. Biol. 140:317–26
141. Savidge TC, Pan W-H, Newman P, O’Brien M, Anton PM, Pothoulakis C. 2003. Clostridium difficiletoxin B is an inflammatory enterotoxin in human intestine. Gastroenterology 125:413–20
142. Savidge TC, Urvil P, Oezguen N, Ali K, Choudhury A, et al. 2011. Host S-nitrosylation inhibitsclostridial small molecule-activated glucosylating toxins. Nat. Med. 17:1136–41
143. Sborgi L, Ruhl S, Mulvihill E, Pipercevic J, Heilig R, et al. 2016. GSDMD membrane pore formationconstitutes the mechanism of pyroptotic cell death. EMBO J. 35:1766–78
144. Schorch B, Song S, van Diemen FR, Bock HH, May P, et al. 2014. LRP1 is a receptor for Clostrid-ium perfringens TpeL toxin indicating a two-receptor model of clostridial glycosylating toxins. PNAS111:6431–36
145. Schulte G. 2010. International Union of Basic and Clinical Pharmacology: LXXX. The class Frizzledreceptors. Pharmacol. Rev. 62:632–67
146. Schwan C, Kruppke AS, Nolke T, Schumacher L, Koch-Nolte F, et al. 2014. Clostridium difficile toxinCDT hijacks microtubule organization and reroutes vesicle traffic to increase pathogen adherence. PNAS111:2313–18
147. Schwan C, Stecher B, Tzivelekidis T, van Ham M, Rohde M, et al. 2009. Clostridium difficile toxin CDTinduces formation of microtubule-based protrusions and increases adherence of bacteria. PLOS Pathog.5:e1000626
148. Sehr P, Joseph G, Genth H, Just I, Pick E, Aktories K. 1998. Glucosylation and ADP ribosylation of Rhoproteins: effects on nucleotide binding, GTPase activity, and effector coupling. Biochemistry 37:5296–304
149. Selzer J, Hofmann F, Rex G, Wilm M, Mann M, et al. 1996. Clostridium novyi α-toxin-catalyzed incor-poration of GlcNAc into Rho subfamily proteins. J. Biol. Chem. 271:25173–77
150. Sheahan K-L, Cordero CL, Fullner Satchell KJ. 2007. Autoprocessing of the Vibrio cholerae RTX toxinby the cysteine protease domain. EMBO J. 26:2552–61
151. Shen A, Lupardus PJ, Gersch MM, Puri AW, Albrow VE, et al. 2011. Defining an allosteric circuit inthe cysteine protease domain of Clostridium difficile toxins. Nat. Struct. Mol. Biol. 18:364–71
152. Shi J, Gao W, Shao F. 2017. Pyroptosis: gasdermin-mediated programmed necrotic cell death. TrendsBiochem. Sci. 42:245–54
153. Shi J, Zhao Y, Wang K, Shi X, Wang Y, et al. 2015. Cleavage of GSDMD by inflammatory caspasesdetermines pyroptotic cell death. Nature 526:660–65
154. Slimings C, Riley TV. 2014. Antibiotics and hospital-acquired Clostridium difficile infection: update ofsystematic review and meta-analysis. J. Antimicrob. Chemother. 69:881–91
155. Smith JA, Cooke DL, Hyde S, Borriello SP, Long RG. 1997. Clostridium difficile toxin A binding tohuman intestinal epithelial cells. J. Med. Microbiol. 46:953–58
156. Stankiewicz TR, Ramaswami SA, Bouchard RJ, Aktories K, Linseman DA. 2015. Neuronal apoptosisinduced by selective inhibition of Rac GTPase versus global suppression of Rho family GTPases ismediated by alterations in distinct mitogen-activated protein kinase signaling cascades. J. Biol. Chem.290(15):9363–76
157. Staub E, Hinzmann B, Rosenthal A. 2002. A novel repeat in the melanoma-associated chondroitin sulfateproteoglycan defines a new protein family. FEBS Lett. 527:114–18
158. Tan KS, Wee BY, Song KP. 2001. Evidence for holin function of tcdE gene in the pathogenicity ofClostridium difficile. J. Med. Microbiol. 50:613–19
159. Tao L, Zhang J, Meraner P, Tovaglieri A, Wu X, et al. 2016. Frizzled proteins are colonic epithelialreceptors for C. difficile toxin B. Nature 538:350–55
306 Aktories · Schwan · Jank
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71CH15-Aktories ARI 16 August 2017 7:31
160. Tcherkezian J, Lamarche-Vane N. 2007. Current knowledge of the large RhoGAP family of proteins.Biol. Cell 99:67–86
161. Teneberg S, Lonnroth I, Lopez JFT, Galili U, Halvarsson MO, et al. 1996. Molecular mimicry in therecognition of glycosphingolipids by Galα3Galβ4GlcNAcβ-binding Clostridium difficile toxin A, humannatural anti α-galactosyl IgG and the monoclonal antibody Gal-13: characterization of a binding-activehuman glycosphingolipid, non-identical with the animal receptor. Glycobiology 6:599–609
162. Triadafilopoulos G, Pothoulakis C, O’Brien MJ, LaMont JT. 1987. Differential effects of Clostridiumdifficile toxins A and B on rabbit ileum. Gastroenterology 93:273–79
163. Tucker KD, Wilkins TD. 1991. Toxin A of Clostridium difficile binds to the human carbohydrate anti-gens I, X, and Y. Infect. Immun. 59:73–78
164. van Leeuwen HC, Bakker D, Steindel P, Kuijper EJ, Corver J. 2013. Clostridium difficile TcdC proteinbinds four-stranded G-quadruplex structures. Nucleic Acids Res. 41:2382–93
165. Vandekerckhove J, Schering B, Barmann M, Aktories K. 1988. Botulinum C2 toxin ADP-ribosylatescytoplasmic β/γ-actin in arginine 177. J. Biol. Chem. 263:696–700
166. Vetter IR, Hofmann F, Wohlgemuth S, Herrmann C, Just I. 2000. Structural consequences of mono-glucosylation of Ha-Ras by Clostridium sordellii lethal toxin. J. Mol. Biol. 301:1091–95
167. Von Eichel-Streiber C, Laufenberg-Feldmann R, Sartingen S, Schulze J, Sauerborn M. 1992. Compar-ative sequence analysis of the Clostridium difficile toxins A and B. Mol. Gen. Genet. 233:260–68
168. Von Eichel-Streiber C, Sauerborn M. 1990. Clostridium difficile toxin A carries a C-terminal repetitivestructure homologous to the carbohydrate binding region of streptococcal glycosyltransferases. Gene96:107–13
169. Wang Q, Navarro MV, Peng G, Molinelli E, Goh SL, et al. 2009. Molecular mechanism of membraneconstriction and tubulation mediated by the F-BAR protein Pacsin/Syndapin. PNAS 106:12700–5
170. Wegner A, Aktories K. 1988. ADP-ribosylated actin caps the barbed ends of actin filaments. J. Biol.Chem. 263:13739–42
171. Wei Y, Zhang Y, Derewenda U, Liu X, Minor W, et al. 1997. Crystal structure of RhoA-GDP and itsfunctional implications. Nat. Struct. Biol. 4:699–703
172. Wohlan K, Goy S, Olling A, Srivaratharajan S, Tatge H, et al. 2014. Pyknotic cell death induced byClostridium difficile TcdB: Chromatin condensation and nuclear blister are induced independently of theglucosyltransferase activity. Cell. Microbiol. 16:1678–92
173. Xu H, Yang J, Gao W, Li L, Li P, et al. 2014. Innate immune sensing of bacterial modifications of RhoGTPases by the pyrin inflammasome. Nature 513:237–41
174. Yen FT, Mann CJ, Guermani LM, Hannouche NF, Hubert N, et al. 1994. Identification of a lipolysis-stimulated receptor that is distinct from the LDL receptor and the LDL receptor-related protein.Biochemistry 33:1172–80
175. Yen FT, Roitel O, Bonnard L, Notet V, Pratte D, et al. 2008. Lipolysis stimulated lipoprotein receptor:a novel molecular link between hyperlipidemia, weight gain, and atherosclerosis in mice. J. Biol. Chem.283:25650–59
176. Young JA, Collier RJ. 2007. Anthrax toxin: receptor binding, internalization, pore formation, and translo-cation. Annu. Rev. Biochem. 76:243–65
177. Yuan P, Zhang H, Cai C, Zhu S, Zhou Y, et al. 2015. Chondroitin sulfate proteoglycan 4 functions asthe cellular receptor for Clostridium difficile toxin B. Cell Res. 25:157–68
178. Zeiser J, Gerhard R, Just I, Pich A. 2013. Substrate specificity of clostridial glucosylating toxins and theirfunction on colonocytes analyzed by proteomics techniques. J. Proteome Res. 12:1604–18
179. Zhang Z, Park M, Tam J, Auger A, Beilhartz GL, et al. 2014. Translocation domain mutations affectingcellular toxicity identify the Clostridium difficile toxin B pore. PNAS 111:3721–26
180. Ziegler MO, Jank T, Aktories K, Schulz GE. 2008. Conformational changes and reaction of clostridialglycosylating toxins. J. Mol. Biol. 377:1346–56
www.annualreviews.org • Clostridium difficile Toxins 307
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71-FrontMatter ARI 16 August 2017 7:4
Annual Review ofMicrobiology
Volume 71, 2017 Contents
A Life in Bacillus subtilis Signal TransductionJames A. Hoch � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 1
Metabolic Diversity and Novelties in the OomycetesHoward S. Judelson � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �21
Early Diverging Fungi: Diversity and Impact at the Dawnof Terrestrial LifeMary L. Berbee, Timothy Y. James, and Christine Strullu-Derrien � � � � � � � � � � � � � � � � � � � � � � �41
Regulation of Cell Polarity in Motility and Cell Divisionin Myxococcus xanthusDominik Schumacher and Lotte Søgaard-Andersen � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �61
Assembly and Function of the Bacillus anthracis S-LayerDominique Missiakas and Olaf Schneewind � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �79
The Cell Wall of the Human Fungal Pathogen Aspergillus fumigatus:Biosynthesis, Organization, Immune Response, and VirulenceJean-Paul Latge, Anne Beauvais, and Georgios Chamilos � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �99
Elongation Factor P and the Control of Translation ElongationAndrei Rajkovic and Michael Ibba � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 117
Genetics and Epigenetics of Mating Type Determination inParamecium and TetrahymenaEduardo Orias, Deepankar Pratap Singh, and Eric Meyer � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 133
Microbiota-Based Therapies for Clostridium difficile andAntibiotic-Resistant Enteric InfectionsBrittany B. Lewis and Eric G. Pamer � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 157
A Symphony of Cyclases: Specificity in Diguanylate Cyclase SignalingKurt M. Dahlstrom and George A. O’Toole � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 179
Evolution of Mating in the SaccharomycotinaKenneth H. Wolfe and Geraldine Butler � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 197
“Fleaing” the Plague: Adaptations of Yersinia pestis to Its Insect VectorThat Lead to TransmissionB. Joseph Hinnebusch, Clayton O. Jarrett, and David M. Bland � � � � � � � � � � � � � � � � � � � � � � � � 215
viii
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71-FrontMatter ARI 16 August 2017 7:4
Evolutionary Genomics of Defense Systems in Archaea and BacteriaEugene V. Koonin, Kira S. Makarova, and Yuri I. Wolf � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 233
Regulating Bacterial Virulence with RNAJuan J. Quereda and Pascale Cossart � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 263
Clostridium difficile Toxin BiologyKlaus Aktories, Carsten Schwan, and Thomas Jank � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 281
Lessons from the Environmental Antibiotic ResistomeMatthew D. Surette and Gerard D. Wright � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 309
Evolutionary Origins of Two-Barrel RNA Polymerasesand Site-Specific Transcription InitiationThomas Fouqueau, Fabian Blombach, and Finn Werner � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 331
The Critical Roles of Polysaccharides in Gut Microbial Ecologyand PhysiologyNathan T. Porter and Eric C. Martens � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 349
The RNAi Universe in Fungi: A Varied Landscape of Small RNAsand Biological FunctionsSantiago Torres-Martınez and Rosa M. Ruiz-Vazquez � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 371
Bacterial Cell Division: Nonmodels Poised to Take the SpotlightPrahathees J. Eswara and Kumaran S. Ramamurthi � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 393
Histone Methylation by SET Domain Proteins in FungiMichael Freitag � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 413
Predator Versus Pathogen: How Does Predatory Bdellovibriobacteriovorus Interface with the Challenges of Killing Gram-NegativePathogens in a Host Setting?David Negus, Chris Moore, Michelle Baker, Dhaarini Raghunathan,
Jess Tyson, and R. Elizabeth Sockett � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 441
Germination of Spores of the Orders Bacillales and ClostridialesPeter Setlow, Shiwei Wang, and Yong-Qing Li � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 459
Microbial ExpansinsDaniel J. Cosgrove � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 479
Bacterial Cell Size: Multifactorial and MultifacetedCorey S. Westfall and Petra Anne Levin � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 499
Bacterial Membranes: Structure, Domains, and FunctionHenrik Strahl and Jeff Errington � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 519
Outer Membrane BiogenesisAnna Konovalova, Daniel E. Kahne, and Thomas J. Silhavy � � � � � � � � � � � � � � � � � � � � � � � � � � � � 539
Contents ix
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.

MI71-FrontMatter ARI 16 August 2017 7:4
Rewriting the Genetic CodeTakahito Mukai, Marc J. Lajoie, Markus Englert, and Dieter Soll � � � � � � � � � � � � � � � � � � � � � 557
Evolutionary Trajectories to Antibiotic ResistanceDiarmaid Hughes and Dan I. Andersson � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 579
Copper Acquisition and Utilization in FungiAaron D. Smith, Brandon L. Logeman, and Dennis J. Thiele � � � � � � � � � � � � � � � � � � � � � � � � � � � 597
Variant Gene Expression and Antigenic Variation by Malaria ParasitesKirk W. Deitsch and Ron Dzikowski � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 625
Syntrophy Goes Electric: Direct Interspecies Electron TransferDerek R. Lovley � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 643
Neisseria gonorrhoeae: Drug Resistance, Mouse Models,and Vaccine DevelopmentPeter A. Rice, William M. Shafer, Sanjay Ram, and Ann E. Jerse � � � � � � � � � � � � � � � � � � � � � � 665
Rho Protein: Roles and MechanismsPallabi Mitra, Gairika Ghosh, Md. Hafeezunnisa, and Ranjan Sen � � � � � � � � � � � � � � � � � � � � 687
Present and Future of Culturing BacteriaJorg Overmann, Birte Abt, and Johannes Sikorski � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 711
The Colorful World of Extracellular Electron ShuttlesNathaniel R. Glasser, Scott H. Saunders, and Dianne K. Newman � � � � � � � � � � � � � � � � � � � � � � 731
Molecular Evolution of Antifungal Drug ResistanceNicole Robbins, Tavia Caplan, and Leah E. Cowen � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 753
Indexes
Cumulative Index of Contributing Authors, Volumes 67–71 � � � � � � � � � � � � � � � � � � � � � � � � � � � 777
Errata
An online log of corrections to Annual Review of Microbiology articles may be found athttp://www.annualreviews.org/errata/micro
x Contents
Ann
u. R
ev. M
icro
biol
. 201
7.71
:281
-307
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
g A
cces
s pr
ovid
ed b
y W
IB62
21 -
KIZ
-AB
T L
itera
turv
erw
altu
ng o
n 04
/09/
18. F
or p
erso
nal u
se o
nly.