Embed Size (px)
Citation preview
257RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
This article is a Directed Reading. To earn continuing education credit for this article, see the instructions on Page 276.
After completing this article, the reader should be able to:�� Describe the anatomical and physiological aspects of swallowing.�� Describe the various phases of deglutition.�� Identify the incidence and causes of dysphagia.�� Summarize the common complications of dysphagia.�� Discuss the modified barium swallow procedure and its role in diagnosing dysphagia.�� Identify postprocedural considerations and treatment options for patients who have dysphagia.
Rebecca Peterson, MSEd, R.T.(R)
Swallowing is part of the process that enables our bodies to receive nutrition. Swallowing difficulties, known as dysphagia,
can have profound adverse effects on patients if left untreated. Fluoroscopic examination is used to help diagnose and treat dysphagia, but radiologic tech-nologists who perform these examina-tions must understand more than the techniques used during evaluation if they are to complete a successful exami-nation; they also must understand the causes of dysphagia and the complica-tions patients face.
Anatomy and Physiology of Swallowing
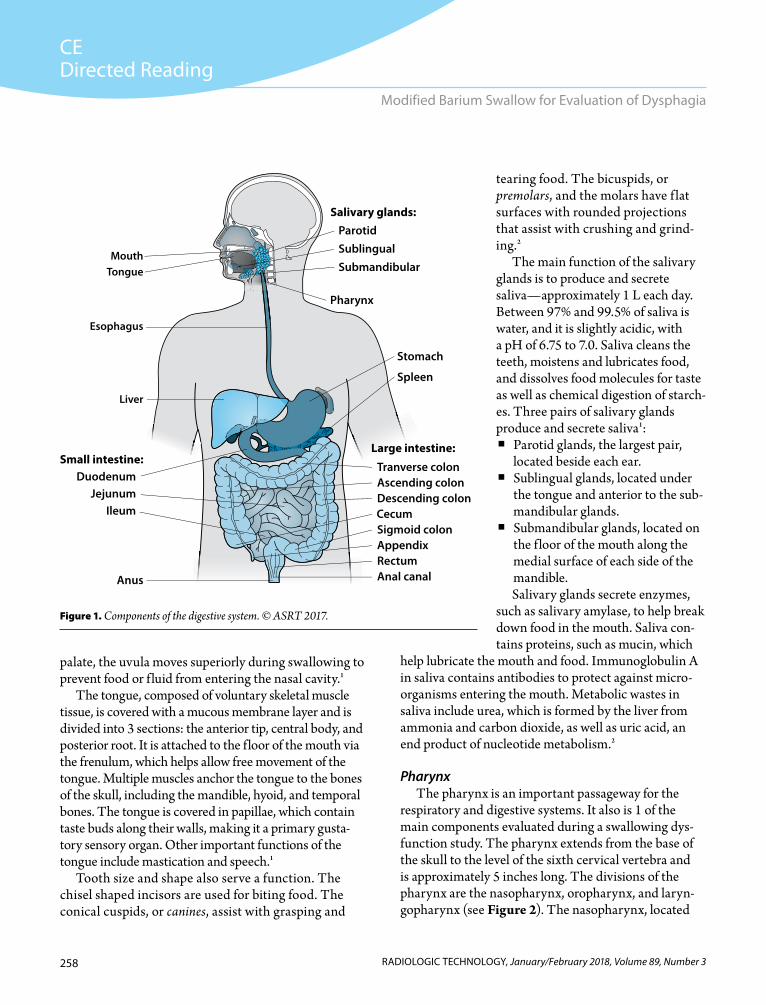
Several anatomical structures are involved in the swallowing process, most of which are part of the aliment-ary canal, or gastrointestinal tract, which begins at the mouth and ends at the anus (see Figure 1). Approximately 30 feet long, the canal’s compo-nents include the mouth, pharynx,
esophagus, stomach, small intestine, large intestine, rectum, and anal canal. The accessory structures involved in eating, drinking, and swallowing are the teeth, tongue, and salivary glands.1 Some respiratory structures also are part of the swallowing process and, therefore, should be evaluated in patients who have dysphagia.
MouthThe components of the mouth—
lips, cheeks, palate, tongue, teeth, and salivary gland ducts—play an important role in the digestive process. Sensory receptors in the lips assess food textures and temperature. The lips and cheeks help food stay in place during chewing and assist in forming words and speaking.1 The palate separates the mouth from the nasal cavity. The ante-rior portion is the hard palate, and the posterior portion is the soft palate. The uvula marks the end of the soft palate, which primarily is composed of soft tissue and muscle. Along with the soft
Modified Barium Swallow for Evaluation of Dysphagia
Deglutition, or the act of swallowing, allows food and fluids to move through the upper gastrointestinal tract. Difficulty swallowing, known as dysphagia, causes a host of complications for patients. Fluoroscopic evaluation of dysphagia enables appropriate diagnosis and treatment. This evaluation commonly is accomplished with a swallowing dysfunction study, also known as a modified barium swallow procedure.
258 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Modified Barium Swallow for Evaluation of Dysphagia
tearing food. The bicuspids, or premolars, and the molars have f lat surfaces with rounded projections that assist with crushing and grind-ing.2
The main function of the salivary glands is to produce and secrete saliva—approximately 1 L each day. Between 97% and 99.5% of saliva is water, and it is slightly acidic, with a pH of 6.75 to 7.0. Saliva cleans the teeth, moistens and lubricates food, and dissolves food molecules for taste as well as chemical digestion of starch-es. Three pairs of salivary glands produce and secrete saliva1:
� Parotid glands, the largest pair, located beside each ear.
� Sublingual glands, located under the tongue and anterior to the sub-mandibular glands.
� Submandibular glands, located on the f loor of the mouth along the medial surface of each side of the mandible.Salivary glands secrete enzymes,
such as salivary amylase, to help break down food in the mouth. Saliva con-tains proteins, such as mucin, which
help lubricate the mouth and food. Immunoglobulin A in saliva contains antibodies to protect against micro-organisms entering the mouth. Metabolic wastes in saliva include urea, which is formed by the liver from ammonia and carbon dioxide, as well as uric acid, an end product of nucleotide metabolism.2
PharynxThe pharynx is an important passageway for the
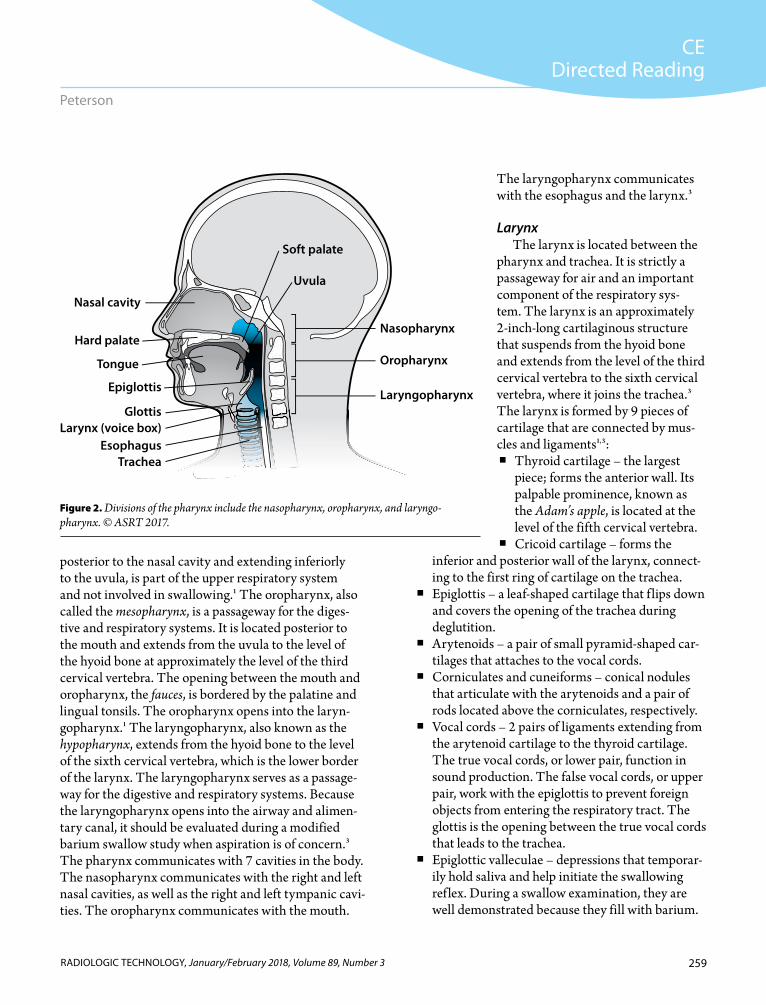
respiratory and digestive systems. It also is 1 of the main components evaluated during a swallowing dys-function study. The pharynx extends from the base of the skull to the level of the sixth cervical vertebra and is approximately 5 inches long. The divisions of the pharynx are the nasopharynx, oropharynx, and laryn-gopharynx (see Figure 2). The nasopharynx, located
palate, the uvula moves superiorly during swallowing to prevent food or f luid from entering the nasal cavity.1
The tongue, composed of voluntary skeletal muscle tissue, is covered with a mucous membrane layer and is divided into 3 sections: the anterior tip, central body, and posterior root. It is attached to the floor of the mouth via the frenulum, which helps allow free movement of the tongue. Multiple muscles anchor the tongue to the bones of the skull, including the mandible, hyoid, and temporal bones. The tongue is covered in papillae, which contain taste buds along their walls, making it a primary gusta-tory sensory organ. Other important functions of the tongue include mastication and speech.1
Tooth size and shape also serve a function. The chisel shaped incisors are used for biting food. The conical cuspids, or canines, assist with grasping and
Fig 1
Cecum
Duodenum
TongueMouth
Liver
Esophagus
Anus
IleumJejunum
Small intestine:Tranverse colonAscending colonDescending colon
Large intestine:
Pharynx
Stomach
Spleen
Submandibular Sublingual Parotid
Salivary glands:
AppendixRectumAnal canal
Sigmoid colon
Figure 1. Components of the digestive system. © ASRT 2017.
259RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Peterson
The laryngopharynx communicates with the esophagus and the larynx.3
LarynxThe larynx is located between the
pharynx and trachea. It is strictly a passageway for air and an important component of the respiratory sys-tem. The larynx is an approximately 2-inch-long cartilaginous structure that suspends from the hyoid bone and extends from the level of the third cervical vertebra to the sixth cervical vertebra, where it joins the trachea.3 The larynx is formed by 9 pieces of cartilage that are connected by mus-cles and ligaments1,3:
� Thyroid cartilage – the largest piece; forms the anterior wall. Its palpable prominence, known as the Adam’s apple, is located at the level of the fifth cervical vertebra.
� Cricoid cartilage – forms theinferior and posterior wall of the larynx, connect-ing to the first ring of cartilage on the trachea.
� Epiglottis – a leaf-shaped cartilage that f lips down and covers the opening of the trachea during deglutition.
� Arytenoids – a pair of small pyramid-shaped car-tilages that attaches to the vocal cords.
� Corniculates and cuneiforms – conical nodules that articulate with the arytenoids and a pair of rods located above the corniculates, respectively.
� Vocal cords – 2 pairs of ligaments extending from the arytenoid cartilage to the thyroid cartilage. The true vocal cords, or lower pair, function in sound production. The false vocal cords, or upper pair, work with the epiglottis to prevent foreign objects from entering the respiratory tract. The glottis is the opening between the true vocal cords that leads to the trachea.
� Epiglottic valleculae – depressions that temporar-ily hold saliva and help initiate the swallowing reflex. During a swallow examination, they are well demonstrated because they fill with barium.
posterior to the nasal cavity and extending inferiorly to the uvula, is part of the upper respiratory system and not involved in swallowing.1 The oropharynx, also called the mesopharynx, is a passageway for the diges-tive and respiratory systems. It is located posterior to the mouth and extends from the uvula to the level of the hyoid bone at approximately the level of the third cervical vertebra. The opening between the mouth and oropharynx, the fauces, is bordered by the palatine and lingual tonsils. The oropharynx opens into the laryn-gopharynx.1 The laryngopharynx, also known as the hypopharynx, extends from the hyoid bone to the level of the sixth cervical vertebra, which is the lower border of the larynx. The laryngopharynx serves as a passage-way for the digestive and respiratory systems. Because the laryngopharynx opens into the airway and alimen-tary canal, it should be evaluated during a modified barium swallow study when aspiration is of concern.3 The pharynx communicates with 7 cavities in the body. The nasopharynx communicates with the right and left nasal cavities, as well as the right and left tympanic cavi-ties. The oropharynx communicates with the mouth.
Figure 2. Divisions of the pharynx include the nasopharynx, oropharynx, and laryngo-pharynx. © ASRT 2017.
Tongue
Larynx (voice box)Glottis
EsophagusTrachea
Epiglottis
Nasopharynx
Oropharynx
Laryngopharynx
Hard palate
Nasal cavity
Soft palate
Uvula
Fig 2
260 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Modified Barium Swallow for Evaluation of Dysphagia
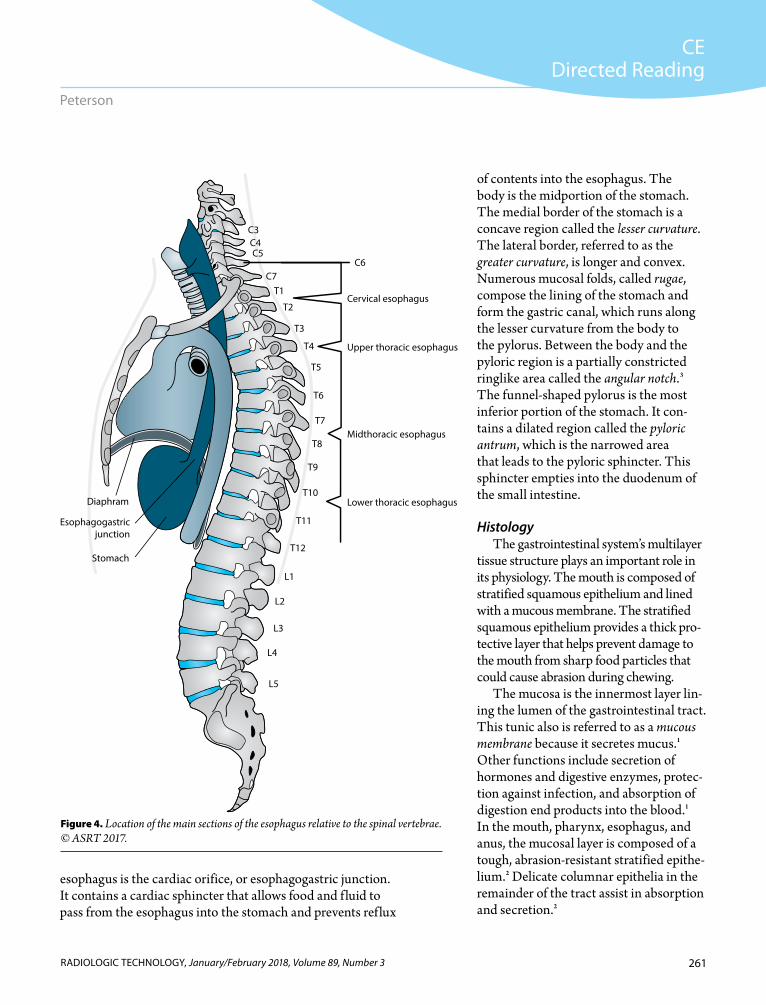
esophagogastric junction.3 It solely is a part of the digestive system and opens during swallowing. Approximately 10 inches long, it extends from the sixth cervical vertebra to the 11th thoracic vertebra (see Figure 4) and is divided into the cervical esophagus, thoracic esophagus, and abdominal esophagus. The laryngopharynx empties into the cervical esophagus at the pharyngoesophageal segment. The esophagus lies posterior to the trachea, larynx, and heart and anterior to the cervical and thoracic spine. Prior to its termina-tion at the junction with the stomach, the esophagus passes through the diaphragm at the level of the tenth thoracic vertebra. The arch of the aorta and the left primary bronchus indentations are located along the length of the esophagus.3
StomachThe widest portion of the alimentary canal is the
stomach, a J-shaped pouch located in the left upper quadrant of the abdominal cavity.3 Superiorly, the esophagus empties into the stomach. Inferiorly, the stomach empties into the first part of the small intes-tine, called the duodenum. The stomach’s 3 main components are the fundus, body, and pylorus. The dome-shaped fundus is the most superior portion of the stomach. The opening between the stomach and
� Piriform sinuses – spaces located on either side of the laryngeal opening that can contain residual food or f luids, even after swallowing.
Trachea and Respiratory TractThe trachea is, roughly, a 4.5-inch-long, 0.75-inch-
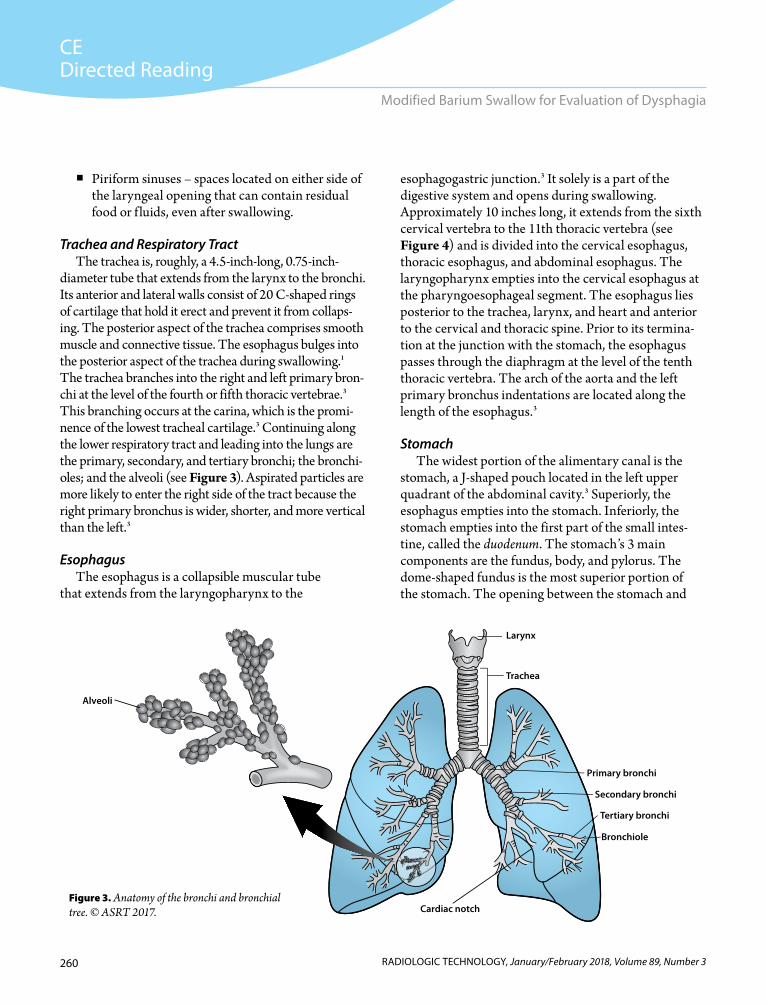
diameter tube that extends from the larynx to the bronchi. Its anterior and lateral walls consist of 20 C-shaped rings of cartilage that hold it erect and prevent it from collaps-ing. The posterior aspect of the trachea comprises smooth muscle and connective tissue. The esophagus bulges into the posterior aspect of the trachea during swallowing.1 The trachea branches into the right and left primary bron-chi at the level of the fourth or fifth thoracic vertebrae.3 This branching occurs at the carina, which is the promi-nence of the lowest tracheal cartilage.3 Continuing along the lower respiratory tract and leading into the lungs are the primary, secondary, and tertiary bronchi; the bronchi-oles; and the alveoli (see Figure 3). Aspirated particles are more likely to enter the right side of the tract because the right primary bronchus is wider, shorter, and more vertical than the left.3
EsophagusThe esophagus is a collapsible muscular tube
that extends from the laryngopharynx to the
Trachea
Primary bronchi
Secondary bronchi
Tertiary bronchi
Bronchiole
Cardiac notch
Larynx
Alveoli
Figure 3. Anatomy of the bronchi and bronchial tree. © ASRT 2017.
261RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Peterson
of contents into the esophagus. The body is the midportion of the stomach. The medial border of the stomach is a concave region called the lesser curvature. The lateral border, referred to as the greater curvature, is longer and convex. Numerous mucosal folds, called rugae, compose the lining of the stomach and form the gastric canal, which runs along the lesser curvature from the body to the pylorus. Between the body and the pyloric region is a partially constricted ringlike area called the angular notch.3 The funnel-shaped pylorus is the most inferior portion of the stomach. It con-tains a dilated region called the pyloric antrum, which is the narrowed area that leads to the pyloric sphincter. This sphincter empties into the duodenum of the small intestine.
HistologyThe gastrointestinal system’s multilayer
tissue structure plays an important role in its physiology. The mouth is composed of stratified squamous epithelium and lined with a mucous membrane. The stratified squamous epithelium provides a thick pro-tective layer that helps prevent damage to the mouth from sharp food particles that could cause abrasion during chewing.
The mucosa is the innermost layer lin-ing the lumen of the gastrointestinal tract. This tunic also is referred to as a mucous membrane because it secretes mucus.1 Other functions include secretion of hormones and digestive enzymes, protec-tion against infection, and absorption of digestion end products into the blood.1 In the mouth, pharynx, esophagus, and anus, the mucosal layer is composed of a tough, abrasion-resistant stratified epithe-lium.2 Delicate columnar epithelia in the remainder of the tract assist in absorption and secretion.2
esophagus is the cardiac orifice, or esophagogastric junction. It contains a cardiac sphincter that allows food and f luid to pass from the esophagus into the stomach and prevents reflux
Midthoracic esophagus
Upper thoracic esophagus
Cervical esophagus
C6
Lower thoracic esophagus
C5C4C3
C7T1
T2
T3
T4
T5
T6
T7
T8
T9
T10
T11
T12
L1
L2
L3
L4
L5
Esophagogastric junction
Stomach
Diaphram
Figure 4. Location of the main sections of the esophagus relative to the spinal vertebrae. © ASRT 2017.

262 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Modified Barium Swallow for Evaluation of Dysphagia
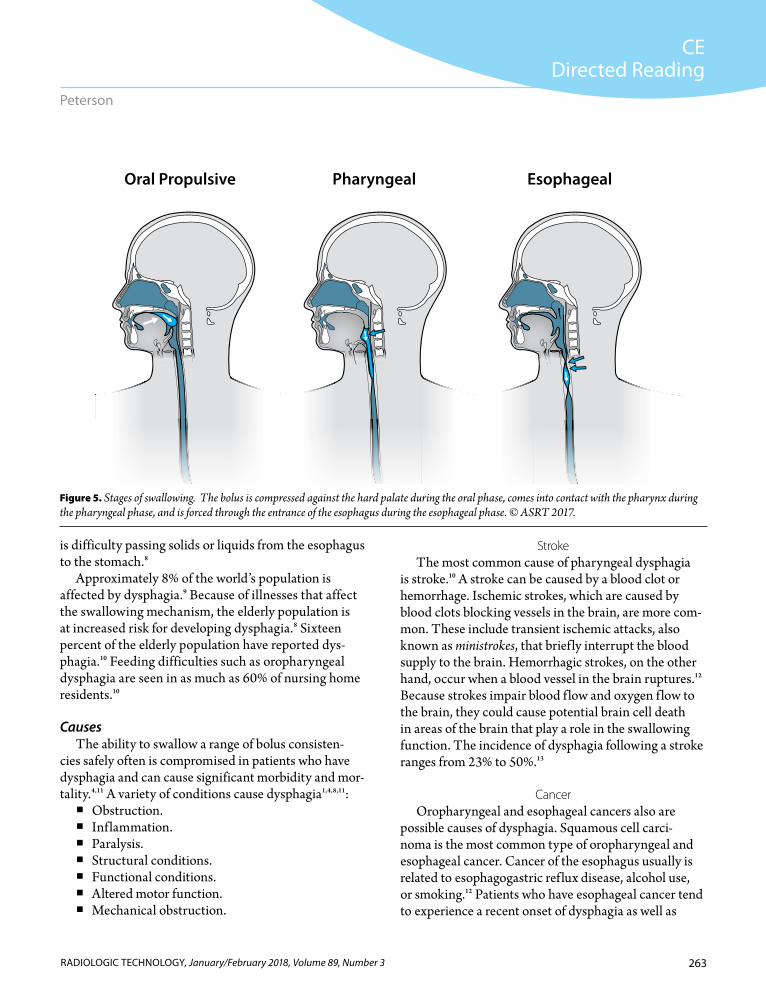
and esophagus.4 The stages of swallowing are oral preparatory, oral propulsive, pharyngeal, and esopha-geal phases (see Figure 5).4 Compression of the bolus against the hard palate occurs during the oral, or buccal, phase. The bolus comes in contact with the pharynx during the pharyngeal phase. Lastly, the bolus is forced through the entrance of the esophagus during the esophageal phase.
During swallowing, food and f luids are forced into the pharynx by the tongue. Sensory receptors initiate an involuntary swallowing reflex. The soft palate and uvula move upward to prevent contents from entering the nasopharynx, and the tongue prevents the contents from re-entering the mouth.3 The epiglottis covers the opening of the larynx to prevent contents from enter-ing the airway. Aspiration also is prevented by the vocal cords closing off the epiglottis.3 Contents are directed into the esophagus by peristalsis, the primary means of propulsion of digestive contents through the alimen-tary canal. Peristalsis results from alternate waves of contraction and relaxation of the muscles found in the walls of the tract. After swallowing, f luids pass to the stomach by gravity and solids pass by gravity and peri-stalsis.3 Unlike deglutition, which is a voluntary type of propulsion, peristalsis is involuntary and normal motil-ity is important.
The motor cortex of the cerebrum sends nerve impulses that regulate voluntary swallowing move-ments. In addition, the deglutition center located in the brainstem controls the involuntary movements involved in swallowing.2
DysphagiaDysphagia is an awareness of difficulty swallowing
or obstruction when a bolus passes from the mouth to the stomach.5 Dysphagia is classified as oropha-ryngeal or esophageal, depending on its location.6 Oropharyngeal dysphagia, or high dysphagia, involves the higher swallowing structures such as the mouth and pharynx.7 It also is referred to as transfer dysphagia because it relates to swallow initiation, which includes the movement of solids or liquids from the pharynx to the esophagus.8 Esophageal dysphagia, or low dysphagia, results from issues in the esophagus.7 In general, it aris-es in the body of the esophagus and occurs when there
The layer external to the mucosa is the submucosa. It is composed of dense connective tissue and has a rich supply of fibers that allows the alimentary canal to stretch. In addition, its nerve plexuses help control movements and secretions along the tract.1 The mus-cularis is a smooth muscle layer divided into an inner circular layer and outer longitudinal layer that contains nerve plexuses that control movements and secretions. Its smooth muscle, also called visceral muscle, is nonstriated and involuntary, and its primary functions are peristalsis and segmentation. The circular layer controls the diame-ter of the lumen by contracting, and the longitudinal layer controls the length of the tube by contracting. Sphincters, which are formed by a thickened inner circular layer, pre-vent backflow along the tract.1
The protective, outermost layer of the gastrointesti-nal tract is known as the serosa if below the diaphragm and adventitia if above the diaphragm. The serosa, also referred to as the serous membrane or visceral peritoneum, is composed of connective tissue with a lining of epithe-lium. It secretes serous f luid for lubrication that helps avoid friction when abdominal organs move against one another. The adventitia is a fibrous connective tissue that binds the esophagus to surrounding structures.1
The respiratory tract is lined with pseudostratified columnar epithelium. This tissue type contains cilia, which help move foreign particles along the tract. It also contains goblet cells, which function in mucus secre-tion. In the lower respiratory tract, alveoli have a single layer of simple squamous epithelium that assists with diffusion and filtration.1
FunctionsThe movement of food and liquids from the mouth
to the stomach involves many functions, specifically mastication, deglutition, and peristalsis. Mastication, or chewing, is a main function of the mouth and involves voluntary movements.2 The tongue manipulates food in the mouth, mixes it with saliva, shapes it into a bolus, and directs it toward the throat for swallowing. Muscles involved in mastication include the temporalis and mas-seter.1 The fifth cranial nerve, or trigeminal nerve, also plays a primary role.
The act of swallowing, also known as deglutition,3 requires coordination of the mouth, pharynx, larynx,
263RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Peterson
StrokeThe most common cause of pharyngeal dysphagia
is stroke.10 A stroke can be caused by a blood clot or hemorrhage. Ischemic strokes, which are caused by blood clots blocking vessels in the brain, are more com-mon. These include transient ischemic attacks, also known as ministrokes, that briefly interrupt the blood supply to the brain. Hemorrhagic strokes, on the other hand, occur when a blood vessel in the brain ruptures.12 Because strokes impair blood f low and oxygen f low to the brain, they could cause potential brain cell death in areas of the brain that play a role in the swallowing function. The incidence of dysphagia following a stroke ranges from 23% to 50%.13
CancerOropharyngeal and esophageal cancers also are
possible causes of dysphagia. Squamous cell carci-noma is the most common type of oropharyngeal and esophageal cancer. Cancer of the esophagus usually is related to esophagogastric reflux disease, alcohol use, or smoking.12 Patients who have esophageal cancer tend to experience a recent onset of dysphagia as well as
is difficulty passing solids or liquids from the esophagus to the stomach.8
Approximately 8% of the world’s population is affected by dysphagia.9 Because of illnesses that affect the swallowing mechanism, the elderly population is at increased risk for developing dysphagia.8 Sixteen percent of the elderly population have reported dys-phagia.10 Feeding difficulties such as oropharyngeal dysphagia are seen in as much as 60% of nursing home residents.10
CausesThe ability to swallow a range of bolus consisten-
cies safely often is compromised in patients who have dysphagia and can cause significant morbidity and mor-tality.4,11 A variety of conditions cause dysphagia1,4,8,11:
� Obstruction. � Inflammation. � Paralysis. � Structural conditions. � Functional conditions. � Altered motor function. � Mechanical obstruction.
Oral Propulsive Pharyngeal Esophageal
Fig5
Figure 5. Stages of swallowing. The bolus is compressed against the hard palate during the oral phase, comes into contact with the pharynx during the pharyngeal phase, and is forced through the entrance of the esophagus during the esophageal phase. © ASRT 2017.

264 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Modified Barium Swallow for Evaluation of Dysphagia
� Change in dietary habits. � Unexplained weight loss. � Recurrent pneumonia.
Patients who have oropharyngeal dysphagia typically cannot initiate swallowing, experience nasal regurgita-tion, and have the sensation of food getting stuck in the cervical region.6 The symptoms of esophageal dyspha-gia tend to be retrosternal. Patients who have primary esophageal dysphagia often describe sensations similar to oropharyngeal dysphagia, such as food sticking in the cervical esophagus.6
ComplicationsSwallowing allows nutrition in the form of solids and
liquids to be delivered to the stomach. When difficulty swallowing occurs, swallowed materials might enter the airway and result in complications such as starvation, weight loss, dehydration, and airway obstruction.4,13 Along with malnutrition, aspiration is a significant consequence.13 Aspiration occurs when food or liquids pass through the vocal folds.4 Impaired laryngeal clo-sure often causes aspiration.4 Retained food or liquids in the pharynx or overflow of the contents also causes aspiration.4 People who aspirate have an increased risk of serious respiratory complications, including an increased risk of chest infection.4,13 In addition, swal-lowing disorders can cause aspiration pneumonia—a common cause of death in hospitalized patients.4
The risks of aspiration depend on factors includ-ing the quantity, depth, and physical properties of the aspirate, as well as pulmonary clearance mechanisms.4 Aspirating minute amounts of solids or liquids is nor-mal and results in minimal adverse effects; however, abnormal gross aspiration will cause complications.4 With regard to depth, it is more dangerous for the patient when contents reach the distal airways as opposed to the uppermost portion or trachea.4 Physical properties of the aspirated material also play a role. Aspirated contents that are acidic can damage the pulmonary parenchyma, and aspirated contents that contain large amounts of infectious organisms can cause bacterial pneumonitis.4 Pulmonary clearance mechanisms, such as ciliary action and coughing, are other important factors.4 When aspiration occurs, a strong cough reflex usually is provoked; however, if
associated weight loss.5 If the esophagus is obstructed because of a malignant esophageal neoplasm, progres-sive dysphagia can result, which puts the patient at risk for malnutrition and aspiration pneumonia.14 Cancer treatment with radiation therapy also might result in dysphagia. Patients who receive radiation to the head and neck might suffer damage to structures involved in swallowing. In patients who have stage III and stage IV head and neck cancer, 17% to 81% reported silent aspiration and pneumonia.15 In addition, a common adverse effect of radiation treatment is dry mouth, or xerostomia. Difficulty swallowing can occur as a result of xerostomia because saliva plays a vital role in the pro-cess of deglutition.12
Neurologic DiseaseMany neuromuscular actions are coordinated dur-
ing the act of swallowing.16 Impaired oropharyngeal swallowing can result from diseases that affect the central swallowing network, which includes cortical, subcortical, and brainstem structures.16 Nervous system disorders that can cause dysphagia include multiple sclerosis, Parkinson disease, amyotrophic lateral sclero-sis, and myasthenia gravis.12
Gastroesophageal Reflux DiseaseGastroesophageal reflux disease is a common chron-
ic disease of the digestive system in which acid and stomach contents reflux into the esophagus, causing irritation. Over time, that irritation can lead to esopha-geal cancer or esophageal strictures. The stricture, or narrowing, of the esophagus can result in food getting stuck. Surgery often is required in patients who present with this type of dysphagia.7
Signs and SymptomsThe signs and symptoms of dysphagia often are
specific to the location of the problem. Signs related to oropharyngeal dysphagia include4:
� Coughing while swallowing. � Difficulty initiating swallowing. � Nasal regurgitation. � Change in voice. � Food sticking in the throat. � Drooling.
265RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Peterson
muscle contractions involved in swallowing.17 Endoscopy is another method to evaluate patients who have dysphagia. A fiberoptic endoscopic evaluation of swallowing can identify any pharyngeal retention or aspiration after the patient swallows. However, this examination cannot evaluate a bolus during swallow-ing or the motion of structures.4 The gold standard for evaluating dysphagia is the videofluoroscopic swallow-ing study, which is a f luoroscopy procedure that uses a DVD recording device to capture the entire proce-dure so the study can be played back and evaluated.4
An esophagram, or barium swallow, is a radiographic examination used to evaluate the form and function of the pharynx and esophagus.3 This videofluoro-scopic swallowing examination is useful in evaluating the pathophysiology of swallowing disorders. The procedure also allows therapeutic and compensatory methods to be assessed.4
The Modified Barium SwallowEvery barium swallow is modified based on the
patient’s symptoms, the patient’s ability to perform a barium swallow, and the clinical questions to be answered.18 Modifications include consistency of con-trast agents, swallowing techniques, and equipment setup. Clinical indications include3,19:
� Achalasia (a condition in which the muscles of the lower esophagus fail to relax, which prevents food from passing into the stomach).
� Anatomic anomalies. � Barrett esophagus. � Dysphagia. � Esophageal carcinoma. � Esophageal varices. � Foreign bodies. � Gastroesophageal reflux disease. � Patient choking, drooling, or coughing when
swallowing. � Zenker diverticulum.
ContraindicationsContraindications to swallowing barium sulfate are
suspected perforation or recent surgery of the gastro- intestinal tract, impending abdominal surgery, and risk of barium impaction. A water-soluble agent is
coughing or throat clearing is absent, silent aspira-tion likely is to occur because of impaired sensations.4 Respiratory complications often occur as a result of silent aspiration.4
EvaluationThe cornerstone of clinical practice in most hospitals
for identifying dysphagia is bedside examination.13 Any signs of dysphagia and aspiration are noted after provid-ing the patient with small amounts of food or water.13 These signs include13:
� Facial weakness. � Loss of liquid from the mouth. � Dyspraxia. � Poor muslce coordination. � Coughing. � Throat clearing. � Breathlessness. � Delayed pharyngeal or laryngeal elevation. � Changes in voice.
It is vital to obtain a thorough patient history to diag-nose and treat patients who have dysphagia, especially patients who have silent aspiration and are not aware that they aspirated.4 A thorough history includes rec-ognizing the problem, identifying the anatomic region involved, and detecting clues regarding the etiology of the condition.4 Information needs to be collected about the onset, duration, and severity of the dysphagia, in addition to the presence of other problems that could be linked to the condition.4 A comprehensive physical examination includes evaluating the4:
� Mouth and neck. � Respiratory, neurologic, or connective tissues dis-
orders that affect swallowing. � Oral-motor and laryngeal mechanisms. � Anterior neck for masses. � Gag reflex using a tongue depressor. � Patient swallowing by feeling the jaw and throat.
If an esophageal motility disorder or gastroesopha-geal reflux disease is suspected, manometry can be appropriate. Manometry evaluates the function of the esophagus and the esophagogastric sphincter by placing a tube into the patient’s gastrointestinal tract and measuring the muscles as the patient swallows. The measurements reflect the pressures of esophageal

266 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Modified Barium Swallow for Evaluation of Dysphagia
feet. This position commonly is used for gastroesopha-geal reflux disease evaluation. Shoulder restraints and a sturdy foot board also are required for patient safety.
When setting up the room, the f luoroscopy table should be placed in a 90° upright position. In addi-tion, the Bucky slot cover should be moved to the inferior aspect of the table to avoid image artifacts. If the patient cannot stand safely without assistance but can sit upright, then a videofluoroscopy swallow study stretcher-chair can be used. This also is referred to as a speech therapy procedure chair. When using a chair, the f luoroscopy table foot rest should be removed before tilting the table upright to accommodate space for the chair between the table and the f luoroscopy tower. For patient safety, the technologist should know the weight limits of the examination table, foot rest, and speech therapy chair.
The f luoroscopy equipment must have a system that enables the modified barium swallow examina-tion to be recorded. Recording allows for discussion of the findings during playback and plays a role in the final examination dictation and interpretation by the radiologist. If a recording system is not synced to the f luoroscopy unit to turn it on and off during exposure, then the technologist must remotely control the record and pause options.
Supplies that should be available for the barium swal-low examination include:
� Contrast agents of varying consistency, prepared per protocol.
� Absorbent disposable pads for easy cleanup of contrast material and spills.
� Standard-sized cups, medicine cups, straws, and spoons for contrast administration.
� Cloth or paper towels for patient care purposes. (Because barium sulfate is fairly chalky, a wet cloth is best for cleaning the patient’s lips and face after he or she has ingested contrast.)
� Gloves, gowns, masks, and safety goggles should be used when needed to adhere to standard infec-tion control precautions.
The oral contrast agent of choice for a modified barium swallow is barium sulfate (BaSO4). Barium sulfate agents provide better mucosal detail than do water-soluble agents and are less likely to become
recommended if contrast media might enter the peri-toneal cavity. Barium sulfate entering the peritoneal cavity could result in barium peritonitis. If aspira-tion is of concern in patients who have a suspected perforation, caution should be taken with regard to the osmolality of the water-soluble agent selected.20 A diatrizoate meglumine and diatrizoate sodium solution typically is used for suspected leak studies of the gas-trointestinal tract. Diatrizoate meglumine sodium is an ionic contrast agent with a high osmolality (approxi-mately 1940 mOsm/kg H20).21 This high osmolality can lead to dehydration and severe complications if aspirated into the airway. Therefore, a safer, nonionic, low-osmolar agent such as iopamidol can be used in its place. In addition to these contrast media consider-ations, the patient must be coherent and able to follow instructions during the examination. An upright posi-tion is required for appropriate evaluation. Therefore, if the patient cannot stand, he or she must be able to sit upright in a chair.
Patient PreparationAlthough bowel prep is not required for a modi-
fied barium swallow, the patient should not eat, drink, smoke, chew gum, or suck on mints or candy for at least 8 hours prior to the examination because these actions increase saliva secretions and affect barium coating properties. The patient should change into a gown and remove all items that could cause artifacts, such as a bra, jewelry, dentures, eyeglasses, and piercings. Special attention also should be paid to any objects on the patient’s gown that might cause artifacts, such as snaps.
EquipmentBoth static and dynamic imaging can be accom-
plished with f luoroscopy equipment. Equipment used for modified barium swallow examinations must meet state and federal radiation standards and must be capable of providing and recording images of diagnos-tic quality.19 The equipment also must produce at least 100 kVp.19 A radiographic/fluoroscopic unit with table tilt capabilities of 90°/45° generally is used for barium swallow studies. The table tilt allows the patient to be evaluated in the full upright position, as well as the Trendelenburg position with the head lower than the
267RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Peterson
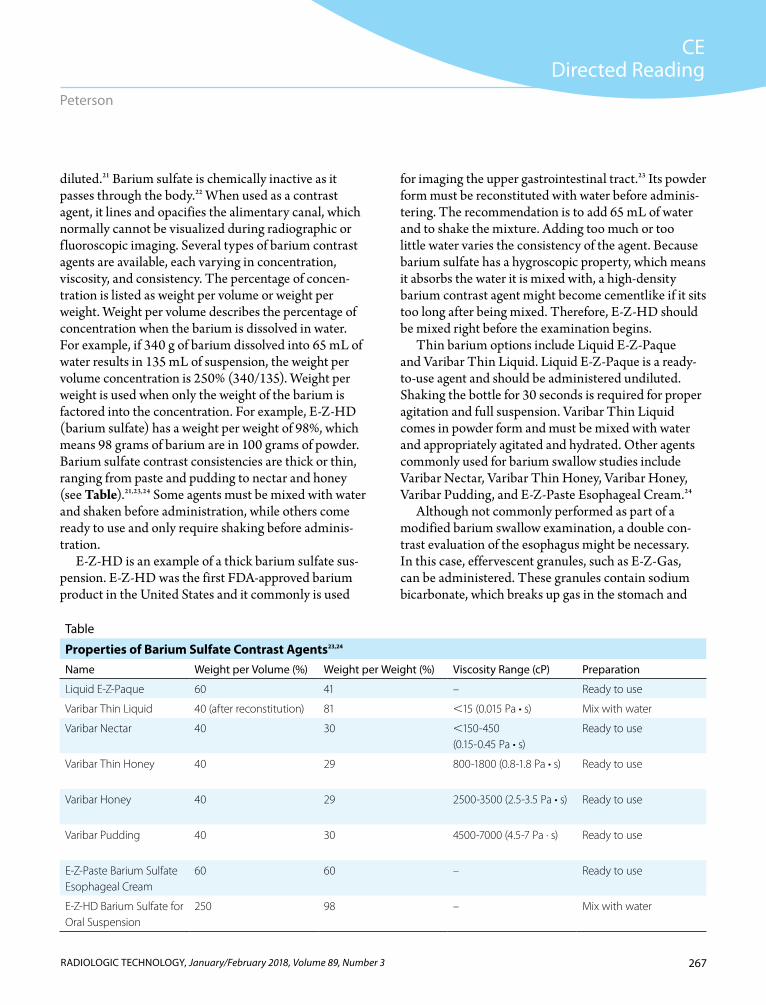
for imaging the upper gastrointestinal tract.23 Its powder form must be reconstituted with water before adminis-tering. The recommendation is to add 65 mL of water and to shake the mixture. Adding too much or too little water varies the consistency of the agent. Because barium sulfate has a hygroscopic property, which means it absorbs the water it is mixed with, a high-density barium contrast agent might become cementlike if it sits too long after being mixed. Therefore, E-Z-HD should be mixed right before the examination begins.
Thin barium options include Liquid E-Z-Paque and Varibar Thin Liquid. Liquid E-Z-Paque is a ready-to-use agent and should be administered undiluted. Shaking the bottle for 30 seconds is required for proper agitation and full suspension. Varibar Thin Liquid comes in powder form and must be mixed with water and appropriately agitated and hydrated. Other agents commonly used for barium swallow studies include Varibar Nectar, Varibar Thin Honey, Varibar Honey, Varibar Pudding, and E-Z-Paste Esophageal Cream.24
Although not commonly performed as part of a modified barium swallow examination, a double con-trast evaluation of the esophagus might be necessary. In this case, effervescent granules, such as E-Z-Gas, can be administered. These granules contain sodium bicarbonate, which breaks up gas in the stomach and
diluted.21 Barium sulfate is chemically inactive as it passes through the body.22 When used as a contrast agent, it lines and opacifies the alimentary canal, which normally cannot be visualized during radiographic or f luoroscopic imaging. Several types of barium contrast agents are available, each varying in concentration, viscosity, and consistency. The percentage of concen-tration is listed as weight per volume or weight per weight. Weight per volume describes the percentage of concentration when the barium is dissolved in water. For example, if 340 g of barium dissolved into 65 mL of water results in 135 mL of suspension, the weight per volume concentration is 250% (340/135). Weight per weight is used when only the weight of the barium is factored into the concentration. For example, E-Z-HD (barium sulfate) has a weight per weight of 98%, which means 98 grams of barium are in 100 grams of powder. Barium sulfate contrast consistencies are thick or thin, ranging from paste and pudding to nectar and honey (see Table).21,23,24 Some agents must be mixed with water and shaken before administration, while others come ready to use and only require shaking before adminis-tration.
E-Z-HD is an example of a thick barium sulfate sus-pension. E-Z-HD was the first FDA-approved barium product in the United States and it commonly is used
Table
Properties of Barium Sulfate Contrast Agents23,24
Name Weight per Volume (%) Weight per Weight (%) Viscosity Range (cP) Preparation
Liquid E-Z-Paque 60 41 – Ready to use
Varibar Thin Liquid 40 (after reconstitution) 81 ,15 (0.015 Pa • s) Mix with water
Varibar Nectar 40 30 ,150-450 (0.15-0.45 Pa • s)
Ready to use
Varibar Thin Honey 40 29 800-1800 (0.8-1.8 Pa • s) Ready to use
Varibar Honey 40 29 2500-3500 (2.5-3.5 Pa • s) Ready to use
Varibar Pudding 40 30 4500-7000 (4.5-7 Pa · s) Ready to use
E-Z-Paste Barium Sulfate Esophageal Cream
60 60 – Ready to use
E-Z-HD Barium Sulfate for Oral Suspension
250 98 – Mix with water

268 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Modified Barium Swallow for Evaluation of Dysphagia
demonstrate incomplete openings and strictures of the pharynx or esophagus. A patient can be seated in a videof luoroscopy swallow study stretcher-chair if he or she cannot stand. This approach allows for upright imaging, which is required for proper evaluation of the oral and pharyngeal phases.18 Patients who can-not stand or sit safely in a videof luoroscopy swallow study stretcher-chair can be positioned right lateral recumbent on the table.18 Before contrast administra-tion, a f luoroscopic spot image might be recorded to identify patient artifacts, obvious pathology, or surgi-cal clips. Anteroposterior and lateral scout images commonly are obtained.
All members of the examination team must acknowl-edge the start and end points of swallowing. Swallowing begins at the lips and is complete once the bolus reaches the gastric cardia.18 Thorough evaluation of swallowing function includes many aspects (see Box).26 It is easier to evaluate the esophageal aspects of swallowing as opposed to the events involved in the oropharyngeal phase because the events in the esophageal body and lower esophageal sphincter occur more slowly than do events in the mouth and pharynx.27 This also explains why visual recording of the f luoroscopic evaluation is important: Valuable diagnostic information might be
makes its elimination easier. Two medicine cups are required to administer this contrast agent. The granules are poured into a cup, and 15 mL of water is poured into another. Too much water will dilute the effect. The patient pours the granules onto the back of the tongue, followed immediately by a water chaser. The patient should swallow often and avoid burping to ensure the gas remains in the alimentary canal; otherwise, the double-contrast effect will be unsuccessful. If the patient burps, another dose of granules and water can be given. E-Z-Disk, a 700-mg, half-inch barium tablet, also is available for swallow examinations to evaluate esophageal strictures.25
All barium contrast agents should be stored at a controlled room temperature of 68°F to 77°F, not in the refrigerator or freezer. Target viscosity is based on mea-surements at 30 seconds to 1 minute at 77°F.24
Imaging TeamTeam members involved in a modified barium swal-
low examination include a board-certified radiologist, radiology resident, and a registered radiologist assistant, as well as a radiologic technologist who is trained in gas-trointestinal radiography.19 The radiologist or radiology resident operates the f luoroscopic equipment during the procedure and is responsible for dictation and inter-pretation of the resultant images, whereas the radiologic technologist prepares the examination room and the contrast media and assists the f luoroscopy operator during the examination. It also is common for a speech-language pathologist or speech therapist to participate in the examination to direct the patient’s compensa-tory and therapeutic maneuvers.18 This person should be educated and trained in modified barium swallow performance and understand the indications for these examinations.19
ProcedureBoth anteroposterior and lateral projections
are important during a modified barium swallow examination. The procedure usually begins with the patient in the erect lateral position.18 As com-pared with a frontal erect position, it is easier to see barium penetrating the laryngeal vestibule with the patient positioned laterally.18 It also is necessary to
Box
Components of Swallowing Evaluated During a Modified Barium Swallow26
Lip closureMasticationBolus preparationTongue control and motionBolus transportOral residuePharyngeal swallow initiationElevation of soft palate and larynxAnterior hyoid excursionEpiglottic movementVestibular closure of larynxPharyngeal contraction and stripping waveOpening of the pharyngoesophageal segmentTongue base retractionPharyngeal residueClearance of the esophagus

269RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Peterson
Videofluoroscopy is used throughout the f luoros-copy examination. Spot or last image hold images also can be obtained in the anteroposterior and lateral projections. Rapid sequence imaging of 3 or 4 frames per second also is common. The technologist should be knowledgeable about control panel setting options to ensure the rapid sequence is selected and unselected when required by the f luoroscopy operator.
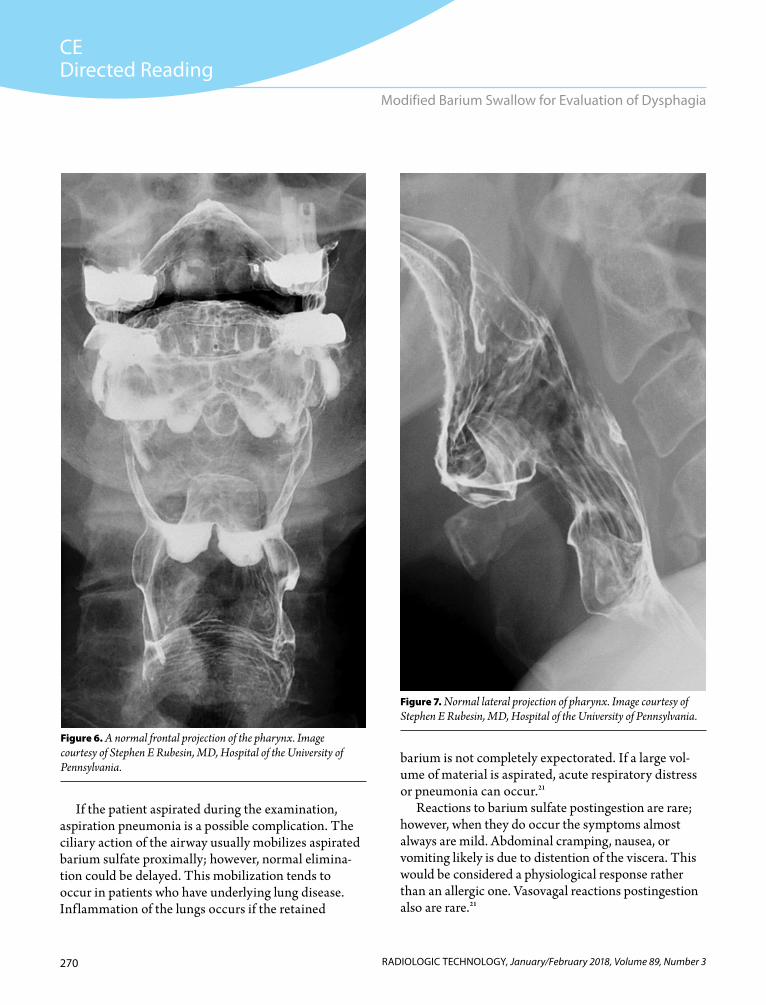
FindingsA normal frontal projection of the pharynx demon-
strates barium-coated midline and lateral structures such as the hard palate, epiglottis, epiglottic valleculae, and piriform sinuses (see Figure 6). A normal lateral projection demonstrates the relationship between anterior and posterior structures as well as superior and inferior structures, which include the oropharynx, layrngopharynx, soft palate, epiglottic tip, overlapping right and left valleculae, hyoid bone, overlapping piri-form sinuses, pharyngoesophageal segment, posterior pharyngeal wall, and spine (see Figure 7). Laryngeal vestibule closure also can be demonstrated in the lateral projection as the contrast moves through to the esopha-gus (see Figure 8).
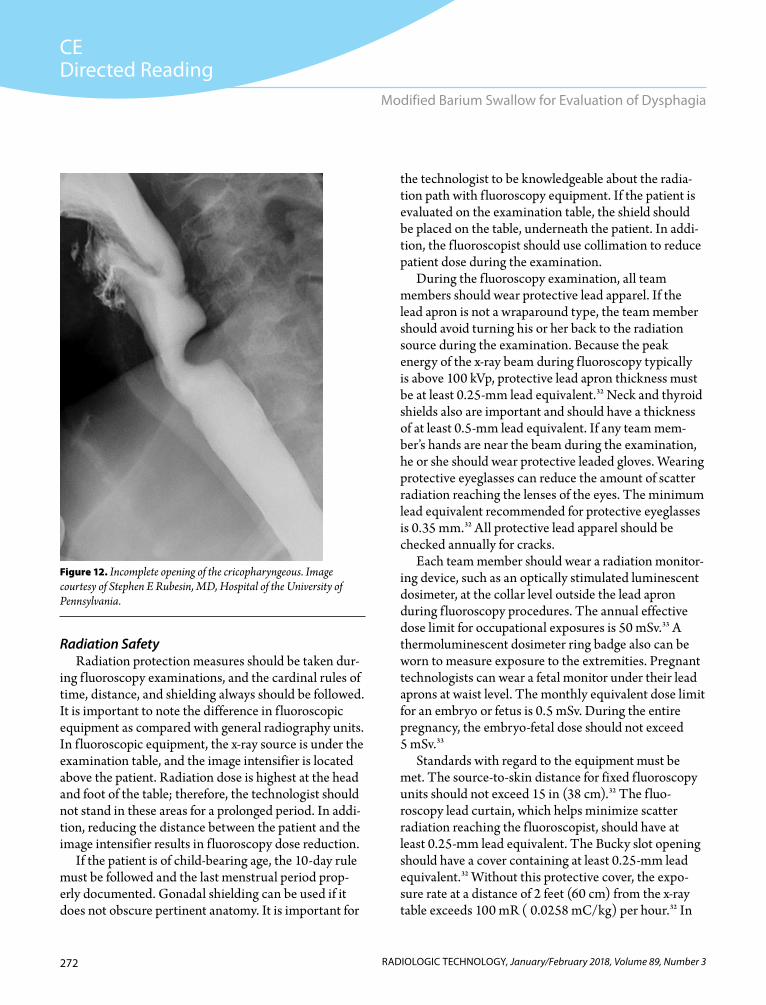
Abnormal findings can be apparent on imaging. Epiglottic tilt to the right or left is well visualized on a frontal image. If this occurs, barium will enter the larynx and cause aspiration (see Figure 9). In patients who have oropharyngeal dysphagia, penetration-aspiration is the most serious factor.31 Aspiration is well demonstrated on a lateral image, as it shows the relationship between anterior and posterior structures (see Figure 10). Filling defects and irregular lining of the mucosa sometimes are present in cases such as supraglottic squamous cell carcinoma (see Figure 11). A lateral image can demonstrate incomplete opening of the pharyngoesophageal segment (see Figure 12).
Postprocedural ConsiderationsBecause barium sulfate is an inert inorganic salt, it is
not absorbed by the gastrointestinal tract. The patient should be advised to resume a normal diet and drink plenty of f luids following the examination. Passing of white in the stools is normal. If constipation occurs, the patient can take a mild over-the-counter laxative.
missed with delayed spot image capture during swal-lowing.
Barium agents of varying consistency should be on hand for the examination. Determining the effects of food consistency on swallowing can be tested using liquids and solids of different consistencies.4 Solid foods can be mixed with barium to make them appear radiopaque on the radiographic images.4 For example, a graham cracker topped with barium pudding might be given to the patient. Liquids also can be mixed with the barium agents; mixing apple juice with the nectar-consistency agent, for example.
Upon administration of contrast to the patient, the patient usually is instructed to hold the bolus in the mouth. When prompted, the patient swallows the bolus all at once.28 Asking the patient to not swallow again allows the team to evaluate normal vs abnormal motil-ity. The amount of time it takes a patient to swallow the bolus varies based on the concentration and consistency of the barium agent.29
Less aspiration occurs with thick liquids than with thin liquids in patients who have poor bolus con-trol.4 For example, a patient is less likely to aspirate a nectar-consistency liquid than water or apple juice. If aspiration is a concern, the examination should begin with a high-density barium or thick agent because thin liquids penetrate the airway more easily.
The effectiveness of compensatory maneuvers can be tested during a modified barium swallow examina-tion. Commonly used strategies include chin down, chin tuck, head rotation, head tilt, and supraglottic swallowing.30 Supraglottic swallowing involves hold-ing a bolus in the mouth during the Valsalva maneuver. Altering head position, modifying feeding methods, and having the patient voluntarily contract muscles dur-ing swallowing are examples of techniques used.4 These maneuvers reduce the possibility of aspiration, open the upper esophageal sphincter, and improve pharyngeal clearance.4 For example, if a patient has unilateral pha-ryngeal weakness, a compensatory maneuver of turning the head toward the weak side deflects the bolus to the strong side and improves pharyngeal clearance of the bolus.4 Another commonly used technique is the Mendelsohn maneuver, which is when the patient vol-untarily prolongs hyolaryngeal elevation.30
270 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Modified Barium Swallow for Evaluation of Dysphagia
barium is not completely expectorated. If a large vol-ume of material is aspirated, acute respiratory distress or pneumonia can occur.21
Reactions to barium sulfate postingestion are rare; however, when they do occur the symptoms almost always are mild. Abdominal cramping, nausea, or vomiting likely is due to distention of the viscera. This would be considered a physiological response rather than an allergic one. Vasovagal reactions postingestion also are rare.21
If the patient aspirated during the examination, aspiration pneumonia is a possible complication. The ciliary action of the airway usually mobilizes aspirated barium sulfate proximally; however, normal elimina-tion could be delayed. This mobilization tends to occur in patients who have underlying lung disease. Inf lammation of the lungs occurs if the retained
Figure 7. Normal lateral projection of pharynx. Image courtesy of Stephen E Rubesin, MD, Hospital of the University of Pennsylvania.
Figure 6. A normal frontal projection of the pharynx. Image courtesy of Stephen E Rubesin, MD, Hospital of the University of Pennsylvania.

271RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Peterson
Figure 8. Lateral projection during swallowing with contractile wave pro-gressing and showing laryngeal vestibule closure, epiglottic tilt, and normal opening cricopharyngeus opposite redundant mucosa in postcricoid region.Image courtesy of Stephen E Rubesin, MD, Hospital of the University of Pennsylvania.
Figure 9. Abnormal epiglottic tilt on left (importance of frontal pro-jection recorded as part of fluoroscopic study). This patient also has a left-sided lateral pharyngeal pouch. Image courtesy of Stephen E Rubesin, MD, Hospital of the University of Pennsylvania.
Figure 10. Laryngeal penetration. Image courtesy of Stephen E Rubesin, MD, Hospital of the University of Pennsylvania.
Figure 11. Supraglottic squamous cell carcinoma. Image courtesy of Stephen E Rubesin, MD, Hospital of the University of Pennsylvania.
272 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Modified Barium Swallow for Evaluation of Dysphagia
the technologist to be knowledgeable about the radia-tion path with f luoroscopy equipment. If the patient is evaluated on the examination table, the shield should be placed on the table, underneath the patient. In addi-tion, the f luoroscopist should use collimation to reduce patient dose during the examination.
During the f luoroscopy examination, all team members should wear protective lead apparel. If the lead apron is not a wraparound type, the team member should avoid turning his or her back to the radiation source during the examination. Because the peak energy of the x-ray beam during f luoroscopy typically is above 100 kVp, protective lead apron thickness must be at least 0.25-mm lead equivalent.32 Neck and thyroid shields also are important and should have a thickness of at least 0.5-mm lead equivalent. If any team mem-ber’s hands are near the beam during the examination, he or she should wear protective leaded gloves. Wearing protective eyeglasses can reduce the amount of scatter radiation reaching the lenses of the eyes. The minimum lead equivalent recommended for protective eyeglasses is 0.35 mm.32 All protective lead apparel should be checked annually for cracks.
Each team member should wear a radiation monitor-ing device, such as an optically stimulated luminescent dosimeter, at the collar level outside the lead apron during f luoroscopy procedures. The annual effective dose limit for occupational exposures is 50 mSv.33 A thermoluminescent dosimeter ring badge also can be worn to measure exposure to the extremities. Pregnant technologists can wear a fetal monitor under their lead aprons at waist level. The monthly equivalent dose limit for an embryo or fetus is 0.5 mSv. During the entire pregnancy, the embryo-fetal dose should not exceed 5 mSv.33
Standards with regard to the equipment must be met. The source-to-skin distance for fixed f luoroscopy units should not exceed 15 in (38 cm).32 The f luo-roscopy lead curtain, which helps minimize scatter radiation reaching the f luoroscopist, should have at least 0.25-mm lead equivalent. The Bucky slot opening should have a cover containing at least 0.25-mm lead equivalent.32 Without this protective cover, the expo-sure rate at a distance of 2 feet (60 cm) from the x-ray table exceeds 100 mR ( 0.0258 mC/kg) per hour.32 In
Radiation SafetyRadiation protection measures should be taken dur-
ing f luoroscopy examinations, and the cardinal rules of time, distance, and shielding always should be followed. It is important to note the difference in f luoroscopic equipment as compared with general radiography units. In f luoroscopic equipment, the x-ray source is under the examination table, and the image intensifier is located above the patient. Radiation dose is highest at the head and foot of the table; therefore, the technologist should not stand in these areas for a prolonged period. In addi-tion, reducing the distance between the patient and the image intensifier results in f luoroscopy dose reduction.
If the patient is of child-bearing age, the 10-day rule must be followed and the last menstrual period prop-erly documented. Gonadal shielding can be used if it does not obscure pertinent anatomy. It is important for
Figure 12. Incomplete opening of the cricopharyngeous. Image courtesy of Stephen E Rubesin, MD, Hospital of the University of Pennsylvania.

273RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Peterson
barium swallow allow for the design of an individu-alized patient diet that includes foods that can be swallowed safely.4 Reducing aspiration is the goal of dysphagia therapy because reduced aspiration improves the patient’s ability to eat, drink, and swallow and optimizes his or her nutritional status.4 The mortality associated with aspiration-related chest infections also is reduced.13 Overall, proper management of swallowing disorders allows the patient to have an improved quality of life.13
Reducing the risks of aspiration or choking com-monly is accomplished by introducing thickened drinks and texture-modified foods.9 Rehabilitative measures such as postural maneuvers, exercises to strengthen muscles used in swallowing, and exercises during the act of swallowing usually improve oral and pharyngeal swallowing disorders.4 Compensatory techniques to improve pharyngeal clearance and reduce aspiration are required to maintain oral feeding.4
Although surgery rarely is indicated, in severe cases enteral or parenteral nutrition might be necessary to bypass the mouth and pharynx. Cricopharyngeal myotomy, the most common sur-gery performed for dysphagia, involves modifying the cricopharyngeus muscle to reduce pharyngeal outf low tract resistance.4
ConclusionDysphagia is a frequent diagnosis that stems from a
number of factors. A modified barium swallow proce-dure is an excellent method for evaluating swallowing dysfunction. Barium sulfate contrast agents of varying concentrations, consistencies, and viscosities are used to evaluate different stages of swallowing. Modification of the examination depends on the patient’s condition and history. Based on diagnosis, individualized treat-ment plans can be prepared for each patient.
Rebecca Peterson, MSEd, R.T.(R), is director of the Diagnostic Medical Imaging program at the Community College of Philadelphia in Pennsylvania. Before becoming a full-time educator, she worked as a staff technologist in the Gastrointestinal/Genitourinary Radiology Department at the Hospital of the University of Pennsylvania.
addition, leakage radiation must not exceed 0.1 cGy per hour when measured at a distance of 1 m from the radiation source.34 Exposure standards must be met for all f luoroscopic equipment. Kilovoltage peak set-tings usually are 100 because of the need for barium sulfate penetration, whereas milliamperes tend to be low (eg, , 5) during gastrointestinal f luoroscopic imaging. The f luoroscopy operator must be able to see the kilovoltage peak and milliampere settings. The air kerma rate should not exceed 5 cGy per minute. In addition, when cinef luorography (rapid sequence imaging) is used, the air kerma rate should not exceed 0.3 µGy per frame.34
Fluoroscopy time should be kept to a minimum to ensure low dose to the patient and imaging team members. Fluoroscopy time continuously must be displayed in minutes and tenths of minutes at the f luo-roscopy operator’s working position.35 Intermittent or pulsed f luoroscopy should be used as much as possible. Magnification mode should be used minimally. The last image hold option can reduce overall exposure as opposed to taking f luoroscopic spot images. Modified barium swallow examinations generally have f luo-roscopy times of less than 5 minutes; however, the f luoroscopy cumulative timer should alarm after 5 min-utes of exposure and continue to sound until the timer is reset manually.35 In addition, a dead man’s exposure switch should be applied to the equipment to ensure exposure is terminated appropriately.34
Benefits and RisksThe main benefit of a modified barium swallow exam-
ination is that it is noninvasive. It assists in determining which solids and liquids are safe for the patient to eat or drink based on evaluation of different consistencies. Radiation dose is low for this examination (ie, within the typical diagnostic range). Allergic reactions to barium are rare; usually they occur because of the flavorings added, such as vanilla, citrus, and strawberry.36
TreatmentDetermining the effect of behavioral and sensory
interventions on the function of the swallowing mechanism is a primary purpose of a swallowing dysfunction examination.27 Results of a modified

274 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Modified Barium Swallow for Evaluation of Dysphagia
13. Singh S, Hamdy S. Dysphagia in stroke patients. Postgrad Med J. 2006;82(968):383-391. doi:10.1136/pgmj.2005 .043281.
14. Fujita T, Tanabe M, Shimizu K, Iida E, Matsunaga N. Radiological image-guided placement of covered Niti-S stent for palliation of dysphagia in patients with cervi-cal esophageal cancer. Dysphagia. 2013;28(2):253-259. doi:10.1007/s00455-013-9446-0.
15. Lee SY, Kim BH, Park YH. Analysis of dysphagia pat-terns using a modified barium swallowing test follow-ing treatment of head and neck cancer. Yonsei Med J. 2015;56(5):1221-1226. doi:10.3349/ymj.2015.56.5.1221.
16. Dziewas R, Beck AM, Clave P, et al. Recognizing the impor-tance of dysphagia: stumbling blocks and stepping stones in the twenty-first century. Dysphagia. 2017;32(1):78-82. doi:10.1007/s00455-016-9746-2.
17. Esophageal manometry. Medline Plus website. https://med lineplus.gov/ency/article/003884.htm. Reviewed August 14, 2015. Accessed July 22, 2017.
18. Levine MS, Ramchandani P, Rubesin SE. Pharynx. In: Practical Fluoroscopy of the GI and GU Tracts. Cambridge, NY: Cambridge University Press; 2012:1-21.
19. ACR practice parameter for the performance of the modi-fied barium swallow. American College of Radiology website. https://www.acr.org/~/media/ACR/Documents /PGTS/guidelines/Modified_Barium_Swallow.pdf. Revised 2017. Accessed July 22, 2017.
20. Bell DJ, Jones J. Barium swallow. Radiopaedia website. https://radiopaedia.org/articles/barium-swallow. Accessed July 22, 2017.
21. ACR manual on contrast media, v10.3. American College of Radiology website. Published 2017. Accessed November 1, 2017.
22. Jensen SC, Peppers MP. Classification, chemistry, and phar-macology of contrast agents. In: Pharmacology and Drug Administration for Imaging Technologists. 2nd ed. St Louis, MO: Mosby; 2006:64-90.
23. E-Z-HD. Imaging Bracco website. http://imaging.bracco.com/us-en/products/fluoroscopy/e-z-hd. Accessed July 27, 2017.
24. Varibar. Imaging Bracco website. http://imaging.bracco .com/us-en/products/fluoroscopy/varibar. Accessed July 27, 2017.
25. E-Z-Disk. Imaging Bracco website. http://imaging.bracco .com/us-en/products/fluoroscopy/e-z-disk. Accessed July 27, 2017.
26. Modified barium swallow study: gold standard or old news? Dysphagia ramblings website. https://dysphagiaramblings
Reprint requests may be mailed to the American Society of Radiologic Technologists, Publications Department, 15000 Central Ave NE, Albuquerque, NM 87123-3909, or emailed to [email protected].
© 2018 American Society of Radiologic Technologists
References1. Applegate E. Digestive system. In: The Anatomy &
Physiology Learning System. 4th ed. St Louis, MO: WB Saunders; 2011:351-376.
2. Thibodeau G, Patton K. The digestive system. In: Structure & Function of the Body. 14th ed. St Louis, MO: Elsevier; 2012:350-376.
3. Bontrager KL, Lampignano JP. Biliary tract and upper gas-trointestinal system. In: Textbook of Radiographic Positioning and Related Anatomy. 8th ed. St Louis, MO: Mosby; 2014: 450-486.
4. Palmer JB, Drennan JC, Baba M. Evaluation and treat-ment of swallowing impairments. Am Fam Physician. 2000;61(8):2453-2462.
5. Carucci LR, Turner MA. Dysphagia revisited: common and unusual causes. Radiographics. 2015;35(1):105-122. doi:10.1148/rg.351130150.
6. Allen BC, Baker ME, Falk GW. Role of barium esopha-gography in evaluating dysphagia. Cleve Clin J Med. 2009;76(2):105-111. doi:10.3949/ccjm.76a.08032.
7. Nordqvist C. Dysphagia: symptoms, diagnosis, and treat-ment. Medical News Today website: http://www.medical newstoday.com/articles/177473.php. Updated November 25, 2016. Accessed July 22, 2017.
8. Aslam M, Vaezi MF. Dysphagia in the elderly. Gastroenterol Hepatol (N Y). 2013;9(12):784-795.
9. Cichero JAY, Lam P, Steele CM, et al. Development of inter-national terminology and definitions for texture-modified foods and thickened fluids used in dysphagia management: the IDDSI Framework. Dysphagia. 2017;32(2):293-314. doi:10.1007/s00455-016-9758-y.
10. Cook IJ. Diagnostic evaluation of dysphagia. Nat Clin Pract Gastroenterol Hepatol. 2008;5(7):393-403. doi:10.1038 /ncpgasthep1153.
11. Popa Nita S, Murith M, Chisholm H, Engmann J. Matching the rheological properties of videofluoroscopic contrast agents and thickened liquid prescriptions. Dysphagia. 2013;28(2):245-252. doi:10.1007/s00455-012-9441-x.
12. Stroke. Medline Plus website. https://medlineplus.gov /stroke.html. Reviewed August 19, 2015. Accessed July 22, 2017.
CEDirected Reading
275RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
CEDirected Reading
Peterson
.net/2017/01/11/modified-barium-swallow-study-gold -standard-or-old-news/. Published January 11, 2017. Accessed July 22, 2017.
27. Martin-Harris B, Jones B. The videofluorographic swallow-ing study. Phys Med Rehabil Clin N Am. 2008;19(4):769-785, viii. doi:10.1016/j.pmr.2008.06.004.
28. Long BW, Rollins JH, Smith BJ. Anterior part of neck. In: Merrill’s Atlas of Radiographic Positioning & Procedures. 13th ed. Volume 2. St Louis, MO: Mosby; 2016:74.
29. Stokely SL, Molfenter SM, Steele CM. Effects of barium concentration on oropharyngeal swallow timing measures. Dysphagia. 2014;29(1):78-82. doi:10.1007/s00455-013 -9485-6.
30. Leigh JH, Oh BM, Seo HG, et al. Influence of the chin-down and chin-tuck maneuver on the swallowing kinematics of healthy adults. Dysphagia. 2015;30(1):89-98. doi:10.1007 /s00455-014-9580-3.
31. Steele CM, Cichero JAY. Physiological factors related to aspiration risk: a systematic review. Dysphagia. 2014;29(3):295-304. doi:10.1007/s00455-014-9516-y.
32. Statkiewicz Sherer MA, Visconti PJ, Ritenour ER, Haynes KW. Management of imaging personnel radiation dose during diagnostic x-ray procedures. In: Radiation Protection in Medical Radiography. 7th ed. Maryland Heights, MO: Mosby; 2014:306-336.
33. Report No NCRP. 116. Limitation of exposure to ionizing radiation. National Council on Radiation Protection & Measurements website. http://www.ncrppublications.org /index.cfm?fm=Product.AddToCart&pid=9143114606. Published 1993. Accessed April 4, 2017.
34. Report No NCRP. 102. Medical x-ray, electron beam, and gamma-ray protection for energies up to 50 MeV (equip-ment design, performance and use). National Council on Radiation Protection & Measurements website. http://www.ncrppublications.org/Reports/102. Published 1989. Accessed April 4, 2017.
35. Performance standard for diagnostic x-ray systems and their major components. U.S. Food and Drug Administra- tion website. https://www.fda.gov/downoads/Radiation -EmittingProducts/RadiationEmittingProductsand Procedures/MedicalImaging/MedicalX-Rays/UCM2031 06.pdf. Published June 10, 2005. Accessed April 4, 2017.
36. Video fluoroscopic swallowing exam (VFSE). Radiology Info.org website: https://www.radiologyinfo.org/en/info .cfm?pg=modbariumswallow. Reviewed April 1, 2017. Accessed April 4, 2017.
276 RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
Directed Reading Quiz
continued on next page
Read the preceding Directed Reading and choose the answer that is most correct based on the article.
To earn continuing education credit: Take this Directed Reading quiz online at asrt.org/drquiz. Enter the Quiz ID XXXXX-XX into the search bar. Or, transfer your responses to the answer sheet following the quiz and mail it in for grading.
* Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date. Some quizzes are renewed and the expiration date extended. Check online at asrt.org/drquiz or call Member Services at 800-444-2778.
To earn continuing education credit: Take this Directed Reading quiz online at asrt.org/drquiz. Enter the Quiz ID 18801-01 into the search bar. Or, transfer your responses to the answer sheet following the quiz and mail it in for grading.
* Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date. Some quizzes are renewed and the expiration date extended. Check online at asrt.org/drquiz or call Member Services at 800-444-2778.
1.5 Category A+ creditsExpires February 28, 2021*
QUIZ ID: 18801-01
Modified Barium Swallow for Evaluation of Dysphagia
4. The act of swallowing also is known as:a. mastication.b. peristalsis.c. deglutition.d. segmentation.
5. Oropharyngeal dysphagia typically involves which of the following?a. nose and mouthb. mouth and pharynxc. pharynx and esophagusd. esophagus and stomach
6. What percentage of the world’s population is estimated to be affected by dysphagia?a. 8b. 16c. 30d. 60
1. Dysphagia is also known as:a. aspiration.b. esophagogastric reflux.c. difficulty speaking.d. difficulty swallowing.
2. The esophagus lies ______ to the trachea.a. superiorb. inferiorc. posteriord. anterior
3. Which of the following describes the innermost layer lining the lumen of the gastrointestinal tract?a. serosab. mucosac. submucosad. muscularis
277RADIOLOGIC TECHNOLOGY, January/February 2018, Volume 89, Number 3
Directed Reading Quiz
12. Therapy for dysphagia can:1. reduce aspiration.2. improve nutrition and quality of life.3. reduce mortality associated with chest
infections.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
7. The most common type of oropharyngeal and esophageal cancer is:a. squamous cell carcinoma.b. adenocarcinoma.c. goblet cell carcinoma.d. eosinophilic granuloma.
8. Contraindications to swallowing barium sulfate include which of the following?a. aspirationb. perforationc. aphasiad. achalasia
9. A modified barium swallow usually begins with the patient in which of the following positions because of its ability to demonstrate barium penetrating the laryngeal vestibule?a. ventral recumbentb. recumbent right anterior obliquec. erect laterald. erect left posterior oblique
10. All of the following are true with regard to barium sulfate except:a. It is an inert inorganic salt.b. It can result in white stools.c. It can result in constipation.d. It is absorbed by the gastrointestinal tract.
11. Which of the following describes the proper location for a radiation monitoring device measuring occupational exposure during fluoroscopy?a. at waist level, under the lead apronb. at waist level, outside the lead apronc. at collar level, under the lead aprond. at collar level, outside the lead apron
✁
Carefully cut or tear here.
Modified Barium Swallow for Evaluation of Dysphagia
Expiration Date: February 28, 2021*Approved for 1.5 Category A+ credits1 8 8 0 1 - 0 1
-- A passing score is 75% or better.-- Take the quiz online at asrt.org/drquiz for immediate results and your CE certificate.-- Or, mail the original answer sheet to Processing Center 2908 Stewart Creek Blvd., Charlotte, NC 28216.-- ASRT must receive this answer sheet before the quiz expires and before the end of the CE biennium for which
you want credit.-- To see a list of the Directed Readings available to you, visit asrt.org/drquiz.-- To evaluate this Directed Reading, visit asrt.org/dreval.
CE Answers Section2
1 A B C D
2 A B C D
3 A B C D
4 A B C D
5 A B C D
6 A B C D
7 A B C D
8 A B C D
Note: For true/false questions, A=true, B=false.
USE A BLACK INK PEN. Completely fill in the circles.
Get immediate Directed Reading quiz results and CE credit when you take your test online at asrt.org/drquiz.
*Some quizzes are renewed and the expiration date extended. Check online at asrt.org/drquiz or call Member Services at 800-444-2778.
2 We need your ASRT Member ID and your two-digit BirthMonth to track your CE credits. Be sure to use yourASRT Member ID and not your ARRT Registry Number.
Birth Month
ASRT Member ID
3 9 3 8 6 1
2 To ensure proper credit, please print the following information.
Identification Section Member Information Section
Name
City
State
9 A B C D
10 A B C D
11 A B C D
12 A B C D
0252408281





























