Embed Size (px)
Citation preview
Update über molekulare Tests beim NSCLC
Martin Früh
Onkologie und Hämatologie Kantonsspital St. Gallen
Titel der Präsentation
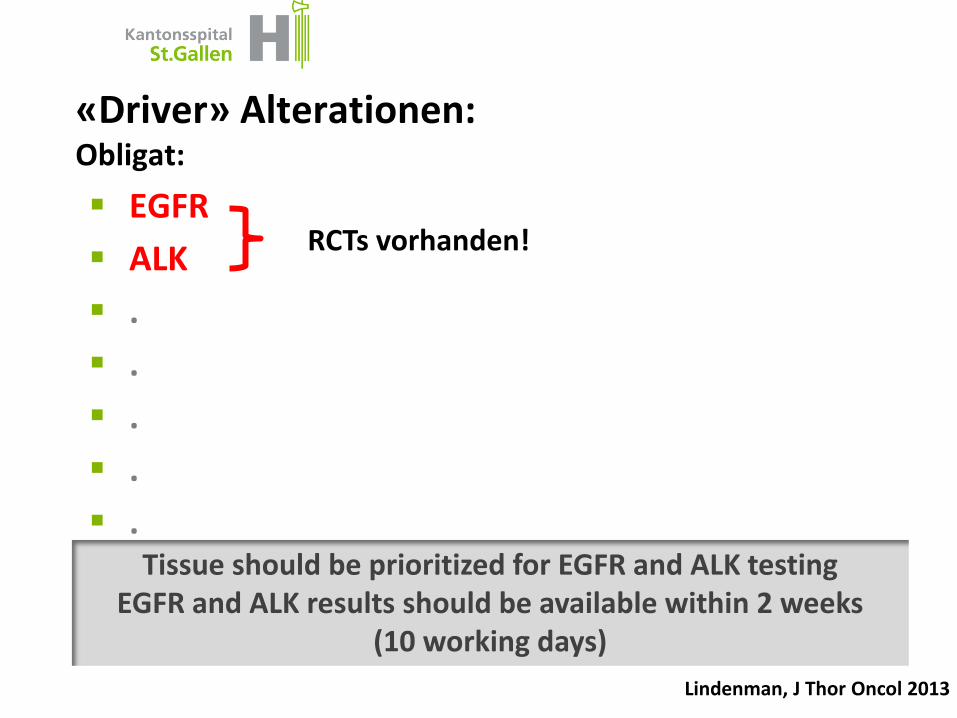
«Driver» Alterationen: Obligat:
EGFR
ALK
.
.
.
.
. Tissue should be prioritized for EGFR and ALK testing
EGFR and ALK results should be available within 2 weeks (10 working days)
Lindenman, J Thor Oncol 2013
RCTs vorhanden!
Titel der Präsentation
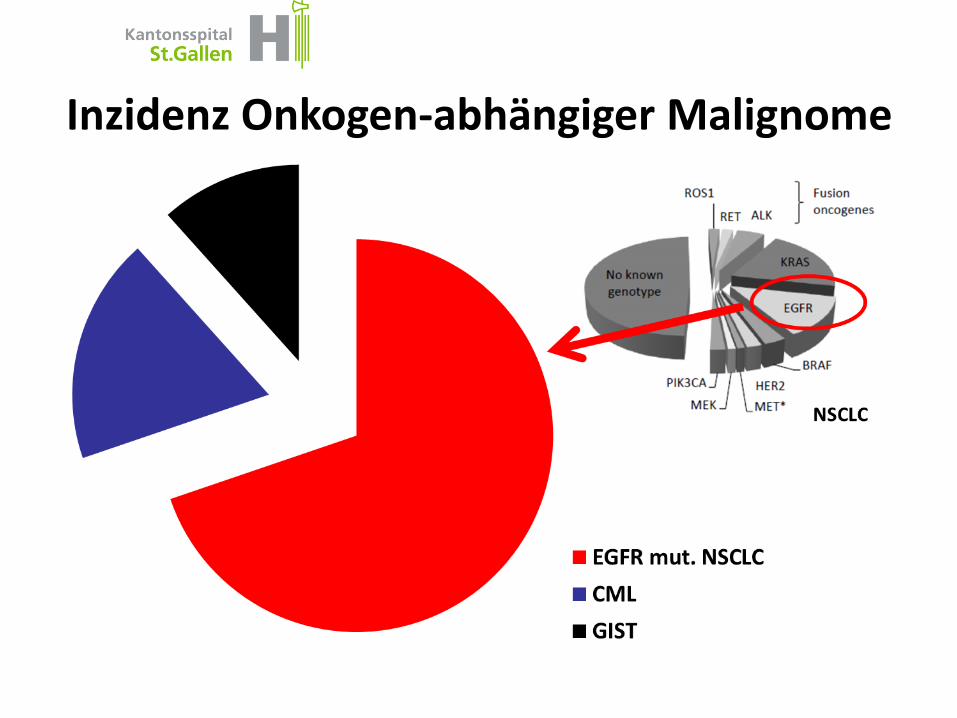
Inzidenz Onkogen-abhängiger Malignome
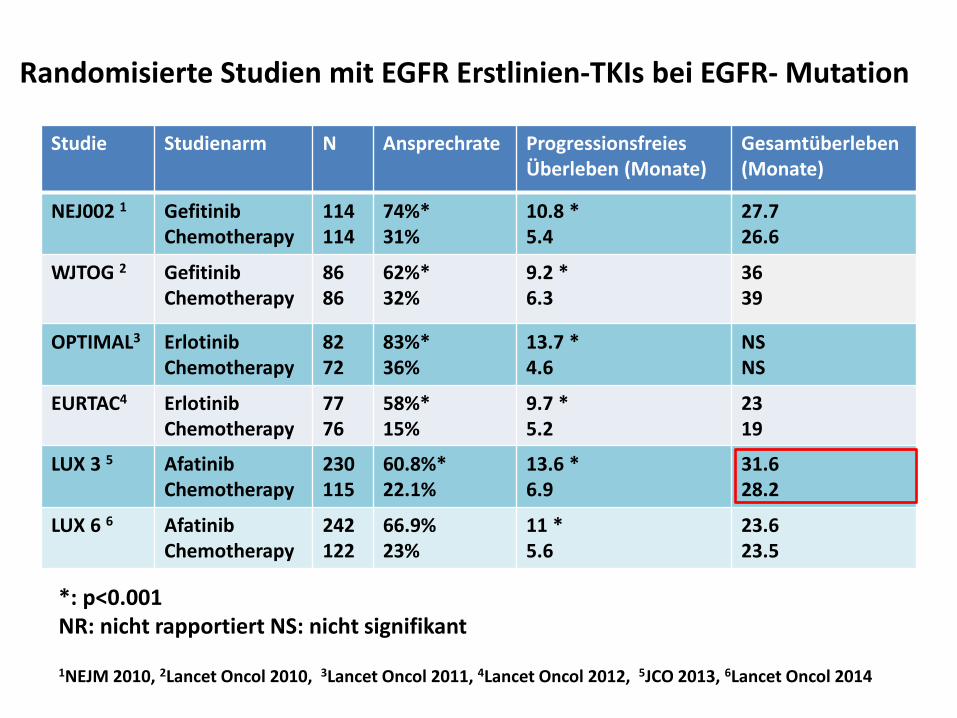
Randomisierte Studien mit EGFR Erstlinien-TKIs bei EGFR- Mutation
Studie Studienarm N Ansprechrate Progressionsfreies Überleben (Monate)
Gesamtüberleben (Monate)
NEJ002 1 Gefitinib Chemotherapy
114 114
74%* 31%
10.8 * 5.4
27.7 26.6
WJTOG 2 Gefitinib Chemotherapy
86 86
62%* 32%
9.2 * 6.3
36 39
OPTIMAL3 Erlotinib Chemotherapy
82 72
83%* 36%
13.7 * 4.6
NS NS
EURTAC4 Erlotinib Chemotherapy
77 76
58%* 15%
9.7 * 5.2
23 19
LUX 3 5 Afatinib Chemotherapy
230 115
60.8%* 22.1%
13.6 * 6.9
31.6 28.2
LUX 6 6 Afatinib Chemotherapy
242 122
66.9% 23%
11 * 5.6
23.6 23.5
1NEJM 2010, 2Lancet Oncol 2010, 3Lancet Oncol 2011, 4Lancet Oncol 2012, 5JCO 2013, 6Lancet Oncol 2014
*: p<0.001 NR: nicht rapportiert NS: nicht signifikant
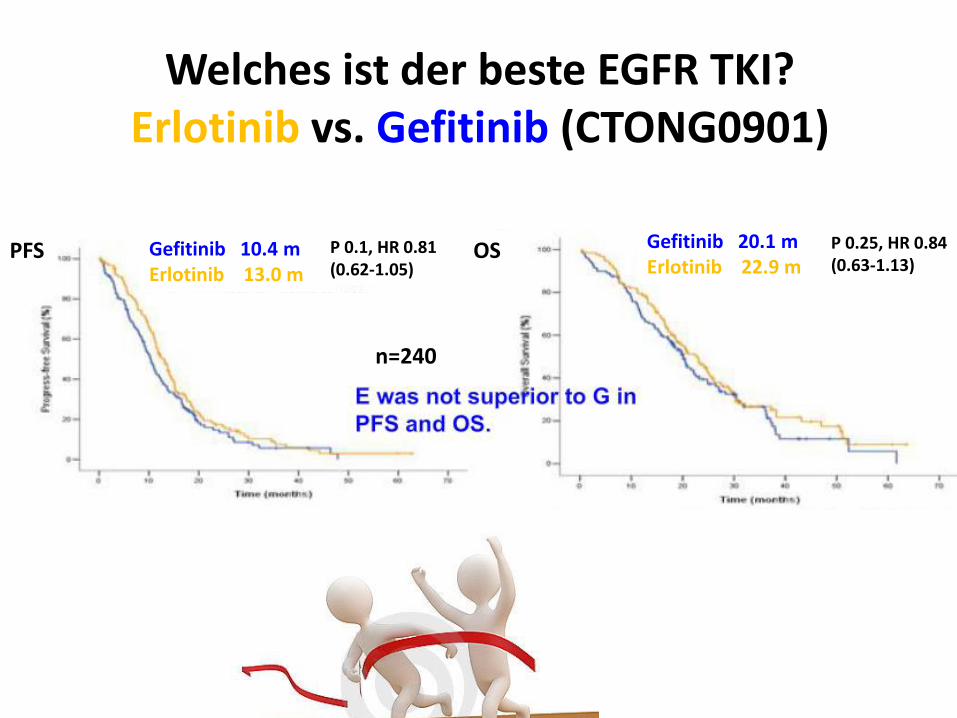
Welches ist der beste EGFR TKI? Erlotinib vs. Gefitinib (CTONG0901)
Yang Abstr 16.13 WCLC 2015
Gefitinib 10.4 m Erlotinib 13.0 m
P 0.1, HR 0.81 (0.62-1.05)
Gefitinib 20.1 m Erlotinib 22.9 m
P 0.25, HR 0.84 (0.63-1.13)
n=240
OS PFS
LUX lung esmo
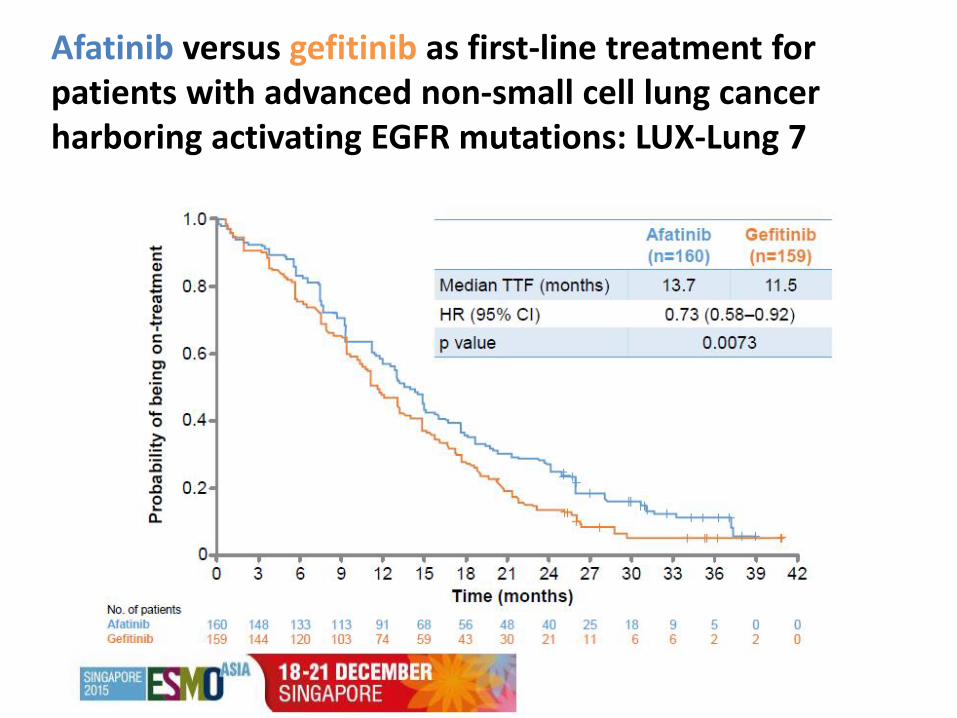
Afatinib versus gefitinib as first-line treatment for patients with advanced non-small cell lung cancer harboring activating EGFR mutations: LUX-Lung 7
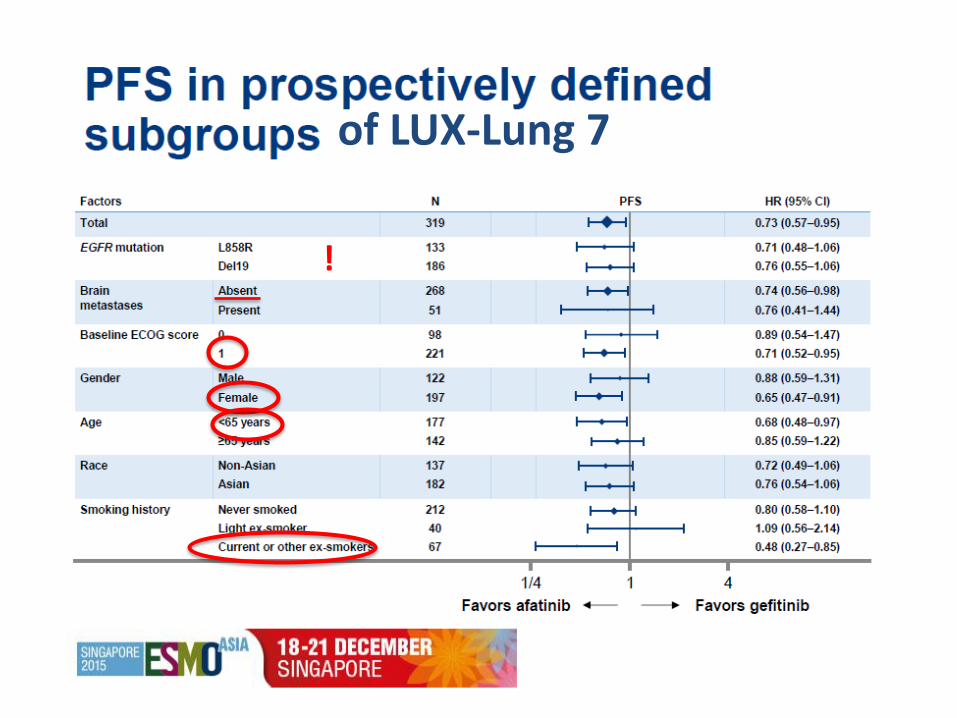
of LUX-Lung 7
!
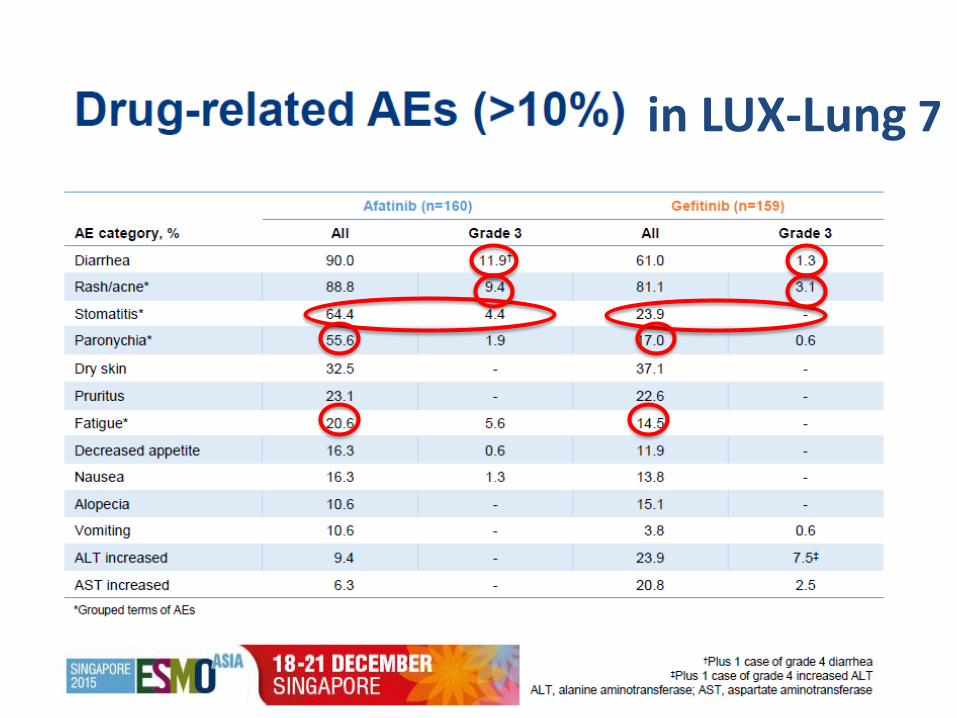
in LUX-Lung 7
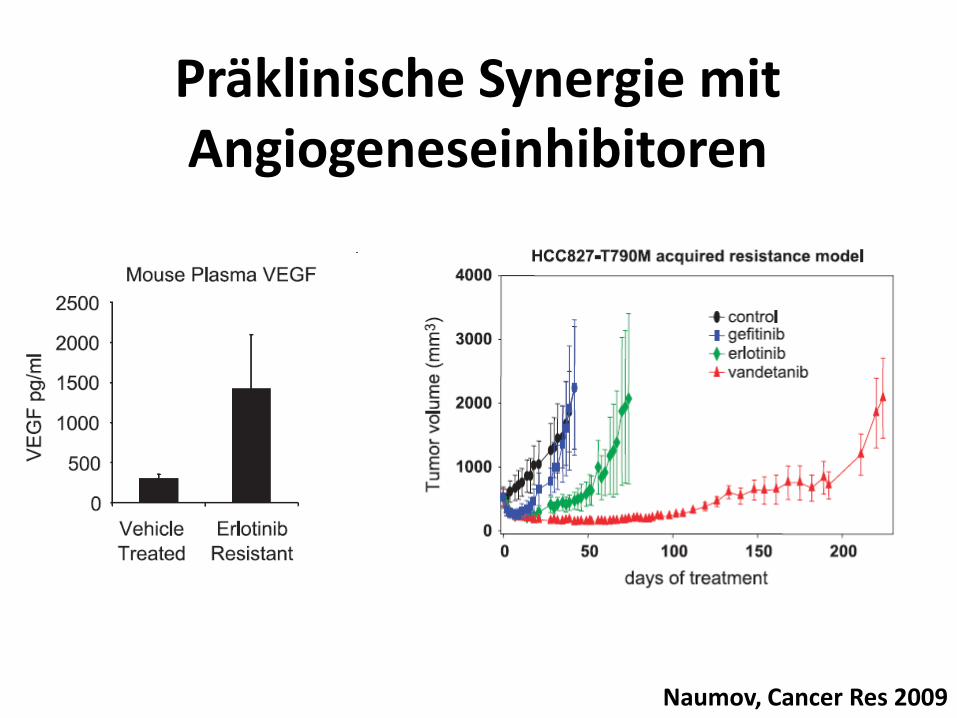
Präklinische Synergie mit Angiogeneseinhibitoren
Naumov, Cancer Res 2009
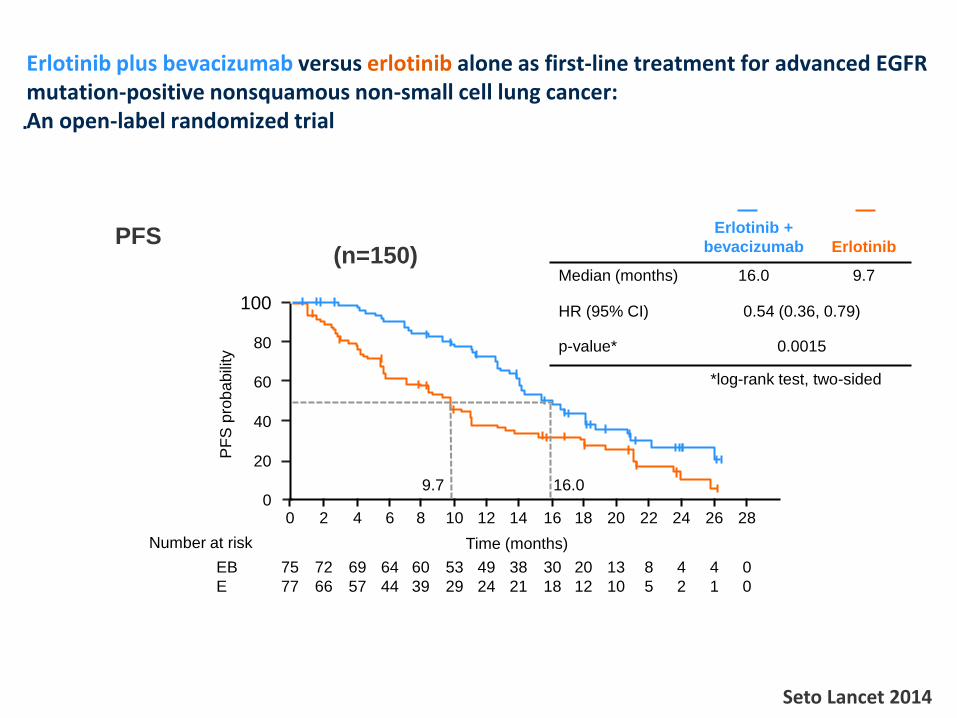
Erlotinib plus bevacizumab versus erlotinib alone as first-line treatment for advanced EGFR mutation-positive nonsquamous non-small cell lung cancer: An open-label randomized trial
Seto Lancet 2014
PFS P
FS
pro
ba
bili
ty
100
80
60
40
20
0 0 2 4 6 8 10 12 14 16 18
Time (months)
20 22 24 26 28
Erlotinib +
bevacizumab Erlotinib
Median (months) 16.0 9.7
HR (95% CI) 0.54 (0.36, 0.79)
p-value* 0.0015
*log-rank test, two-sided
Number at risk
EB
E
75
77
72
66
69
57
64
44
60
39
53
29
49
24
38
21
30
18
20
12
13
10
8
5
4
2
4
1
0
0
9.7 16.0
(n=150)
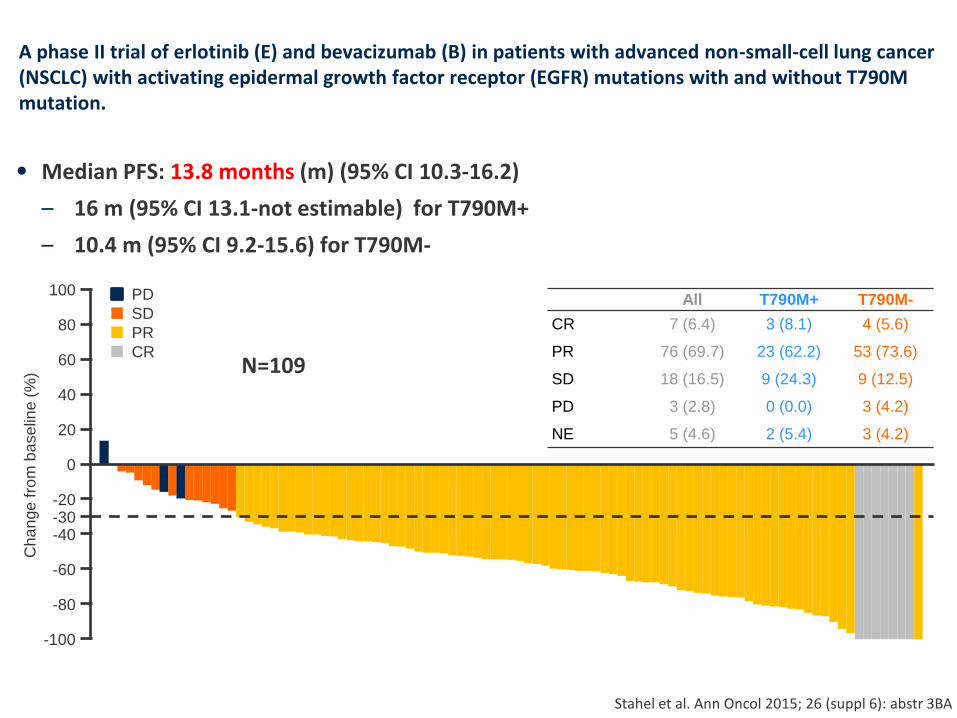
A phase II trial of erlotinib (E) and bevacizumab (B) in patients with advanced non-small-cell lung cancer (NSCLC) with activating epidermal growth factor receptor (EGFR) mutations with and without T790M mutation.
• Median PFS: 13.8 months (m) (95% CI 10.3-16.2)
– 16 m (95% CI 13.1-not estimable) for T790M+
– 10.4 m (95% CI 9.2-15.6) for T790M-
Stahel et al. Ann Oncol 2015; 26 (suppl 6): abstr 3BA
All T790M+ T790M-
CR 7 (6.4) 3 (8.1) 4 (5.6)
PR 76 (69.7) 23 (62.2) 53 (73.6)
SD 18 (16.5) 9 (24.3) 9 (12.5)
PD 3 (2.8) 0 (0.0) 3 (4.2)
NE 5 (4.6) 2 (5.4) 3 (4.2)
Ch
an
ge
fro
m b
ase
line (
%)
100
80
60
40
20
0
PD
SD
PR
CR
-100
-80
-60
-40
-20 -30
N=109
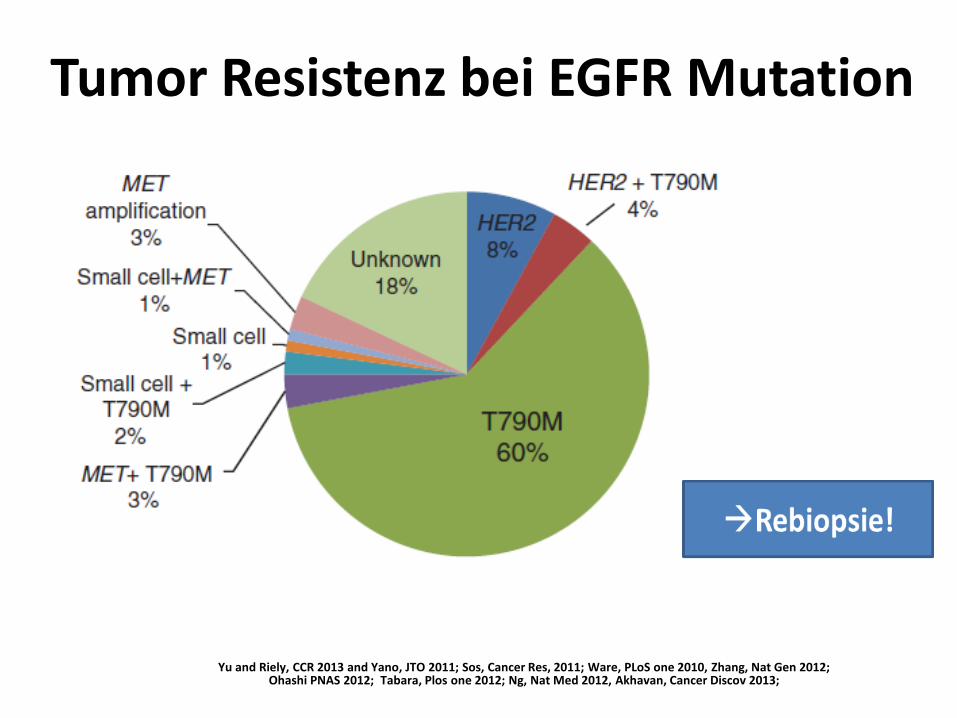
Yu and Riely, CCR 2013 and Yano, JTO 2011; Sos, Cancer Res, 2011; Ware, PLoS one 2010, Zhang, Nat Gen 2012; Ohashi PNAS 2012; Tabara, Plos one 2012; Ng, Nat Med 2012, Akhavan, Cancer Discov 2013;
Tumor Resistenz bei EGFR Mutation
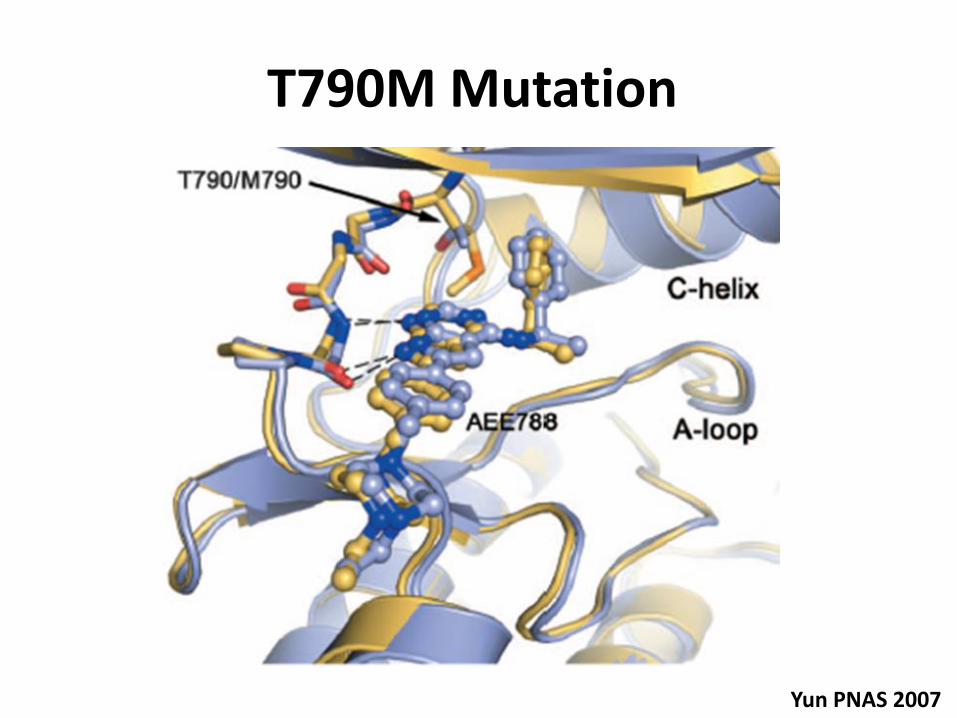
T790M Mutation
Yun PNAS 2007
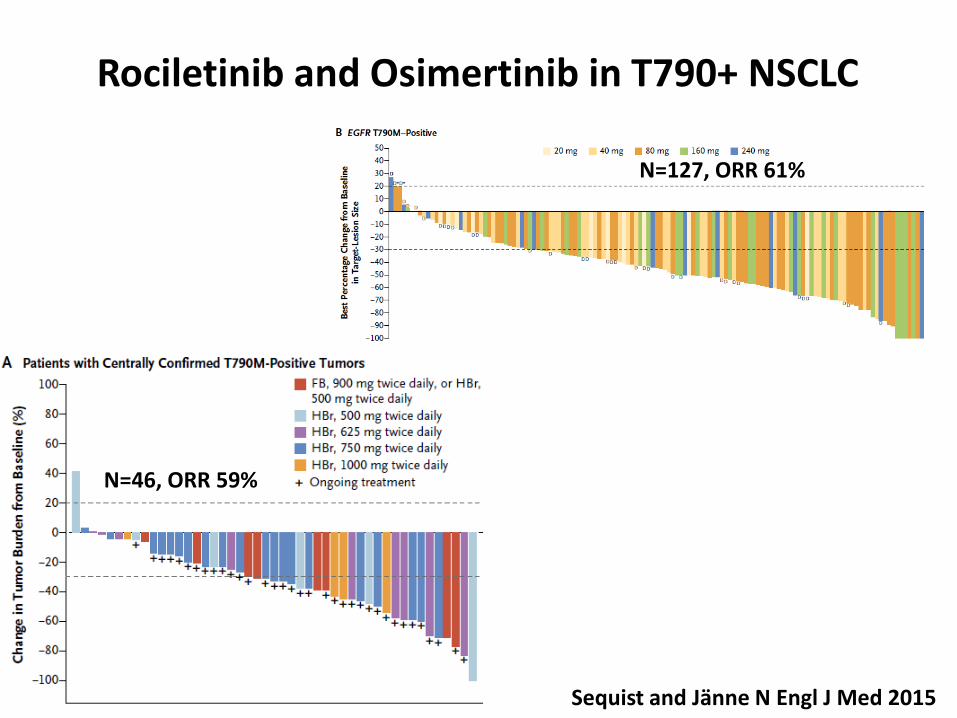
Rociletinib and Osimertinib in T790+ NSCLC
Sequist and Jänne N Engl J Med 2015
N=127, ORR 61%
N=46, ORR 59%
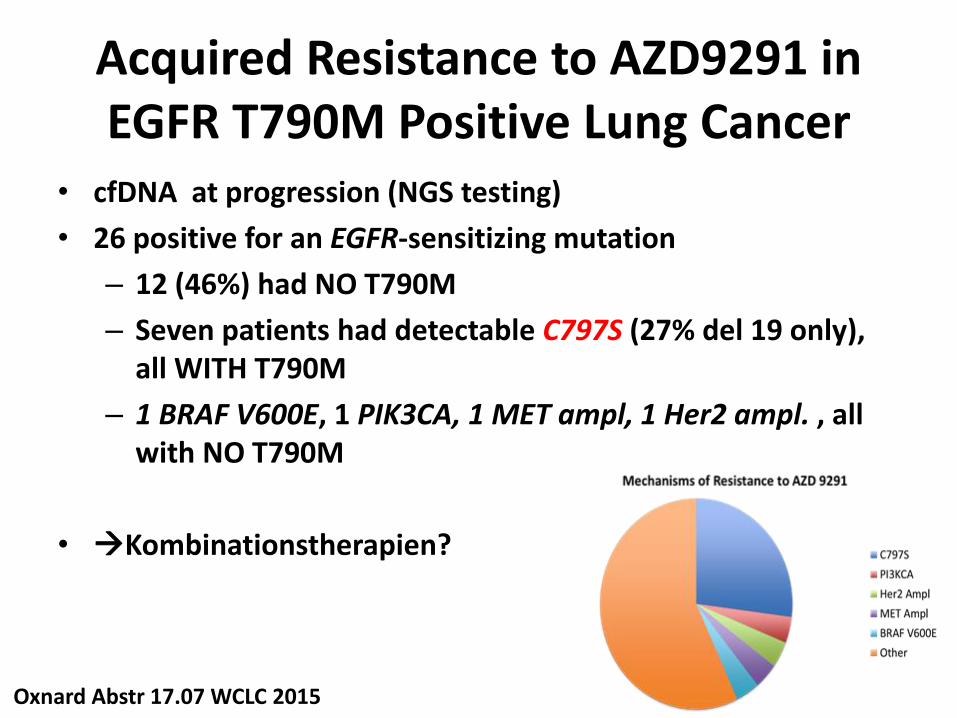
Acquired Resistance to AZD9291 in EGFR T790M Positive Lung Cancer
• cfDNA at progression (NGS testing)
• 26 positive for an EGFR-sensitizing mutation
– 12 (46%) had NO T790M
– Seven patients had detectable C797S (27% del 19 only), all WITH T790M
– 1 BRAF V600E, 1 PIK3CA, 1 MET ampl, 1 Her2 ampl. , all with NO T790M
• Kombinationstherapien?
Oxnard Abstr 17.07 WCLC 2015
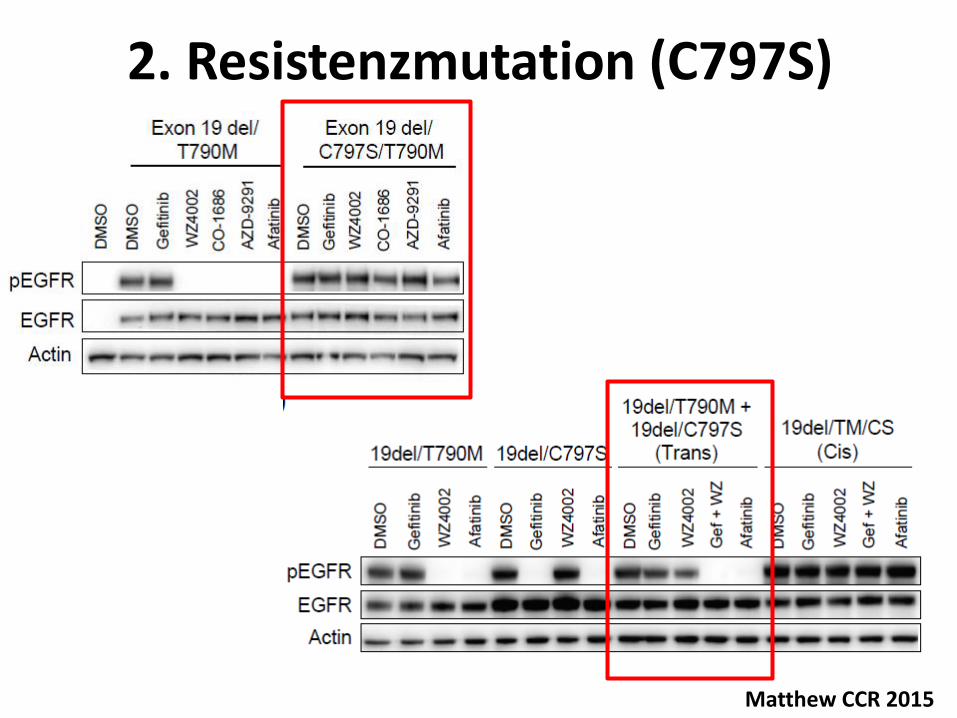
2. Resistenzmutation (C797S)
Matthew CCR 2015
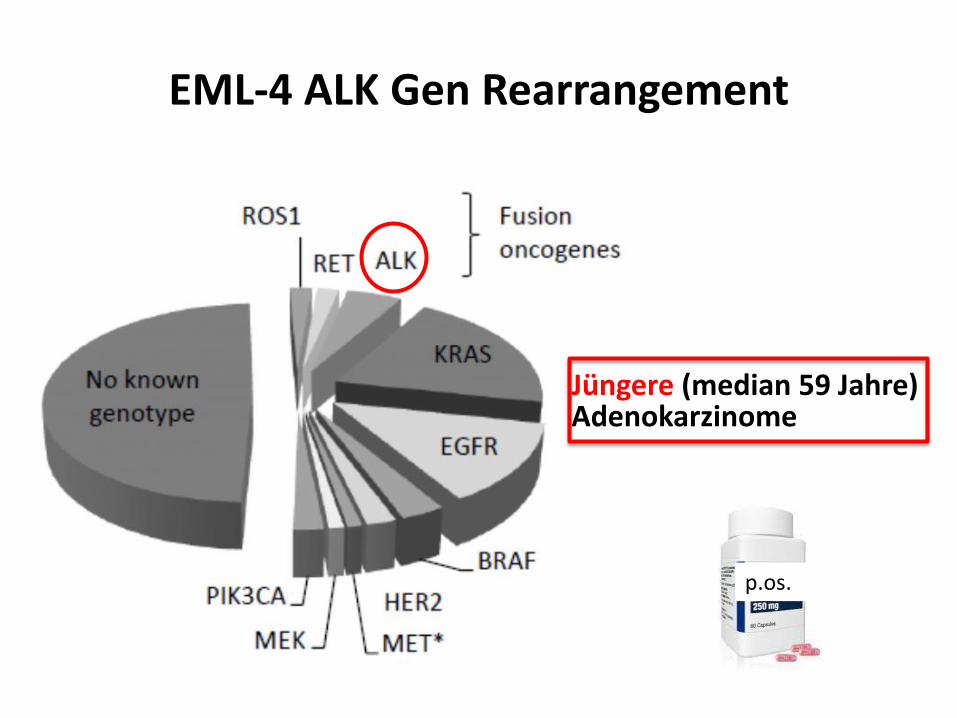
EML-4 ALK Gen Rearrangement
Jüngere (median 59 Jahre) Adenokarzinome
p.os.
Titel der Präsentation
18
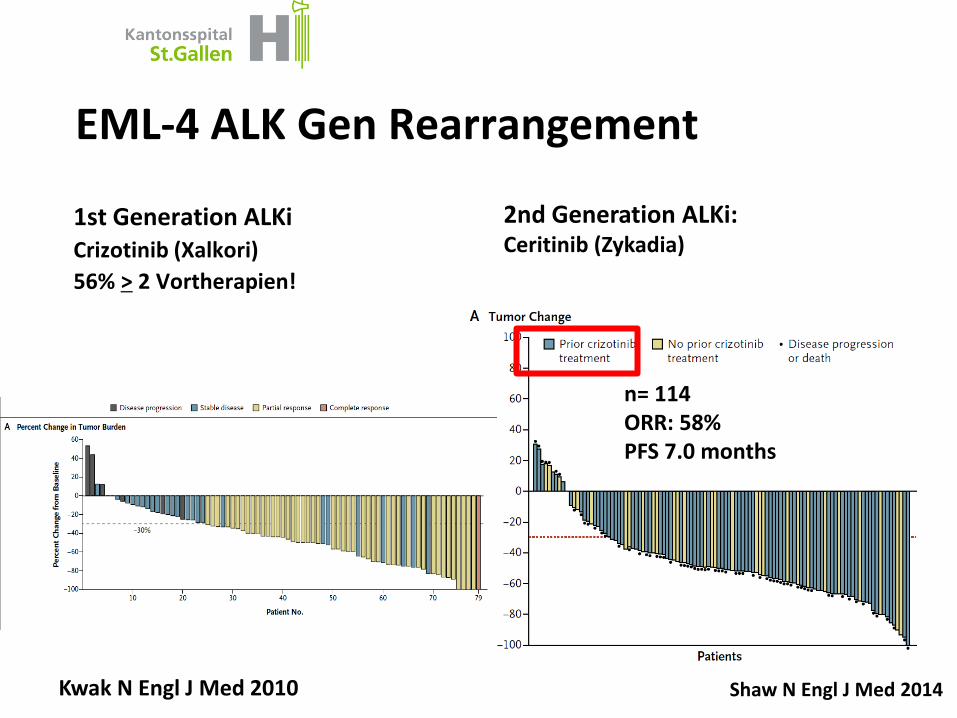
EML-4 ALK Gen Rearrangement
Shaw N Engl J Med 2014
n= 114 ORR: 58% PFS 7.0 months
2nd Generation ALKi: Ceritinib (Zykadia)
Kwak N Engl J Med 2010
1st Generation ALKi Crizotinib (Xalkori)
56% > 2 Vortherapien!
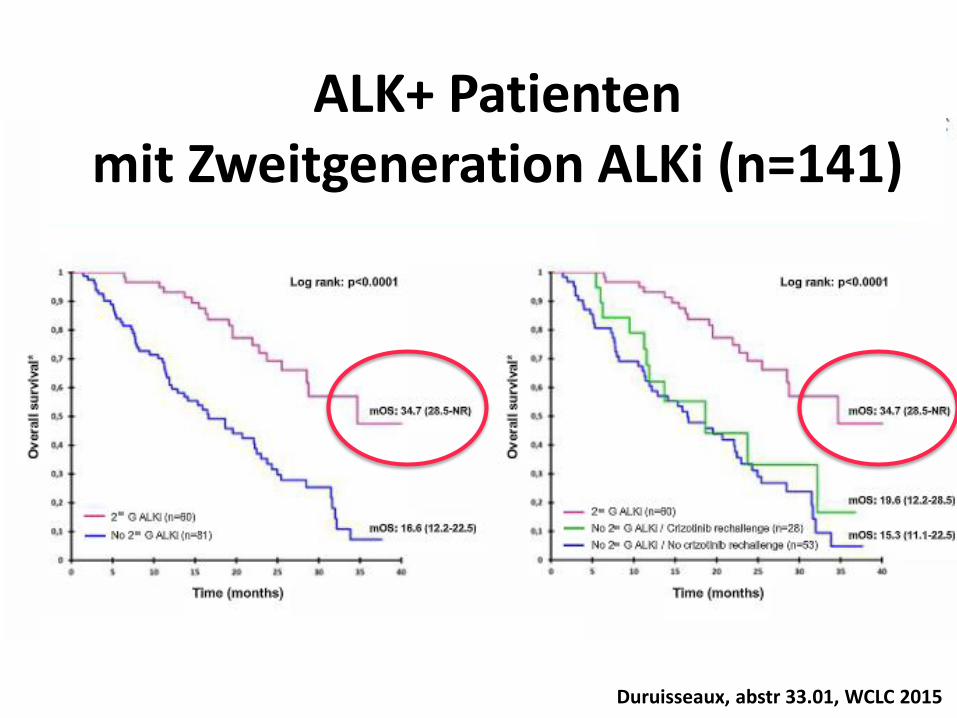
Duruisseaux, abstr 33.01, WCLC 2015
ALK+ Patienten mit Zweitgeneration ALKi (n=141)
Titel der Präsentation
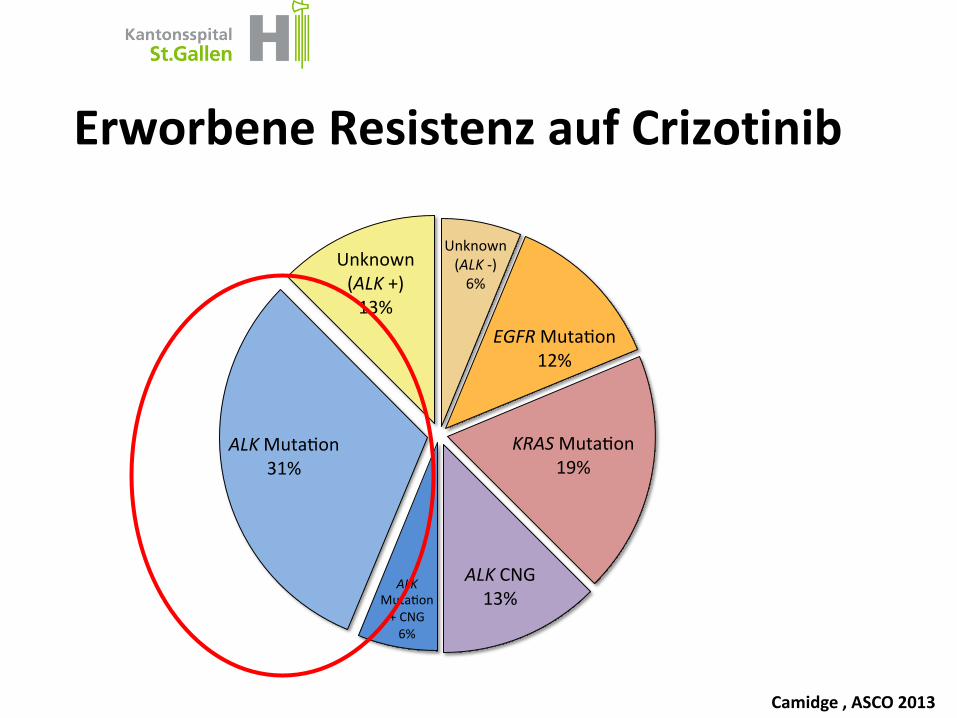
Erworbene Resistenz auf Crizotinib
Unknown(ALK-)6%
EGFRMuta on12%
KRASMuta on19%
ALKCNG13%
ALKMuta on+CNG6%
ALKMuta on31%
Unknown(ALK+)13%
Camidge , ASCO 2013
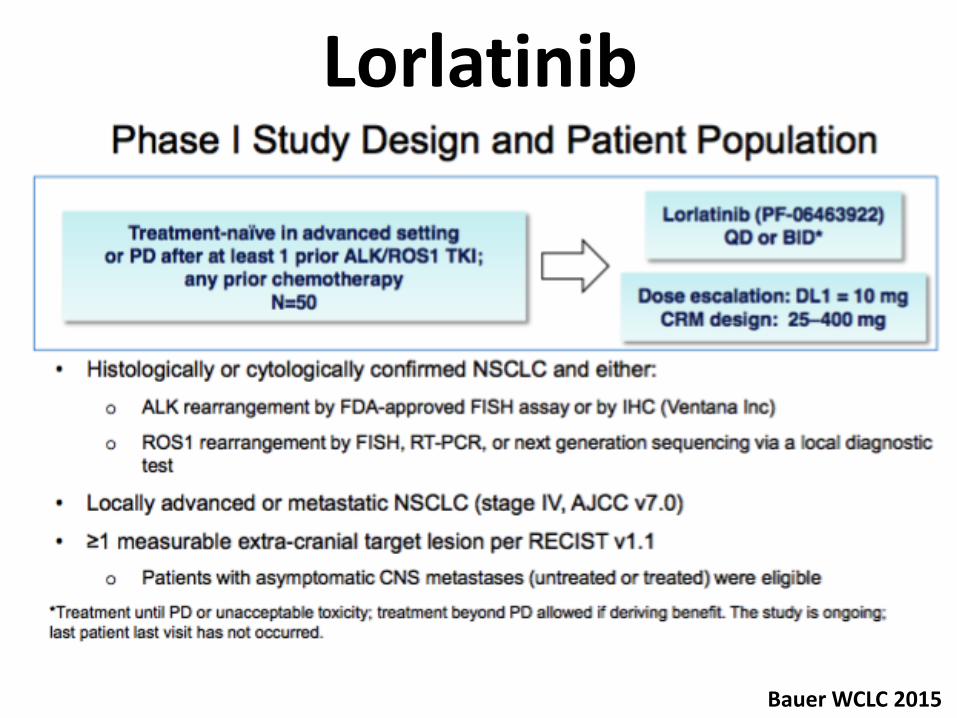
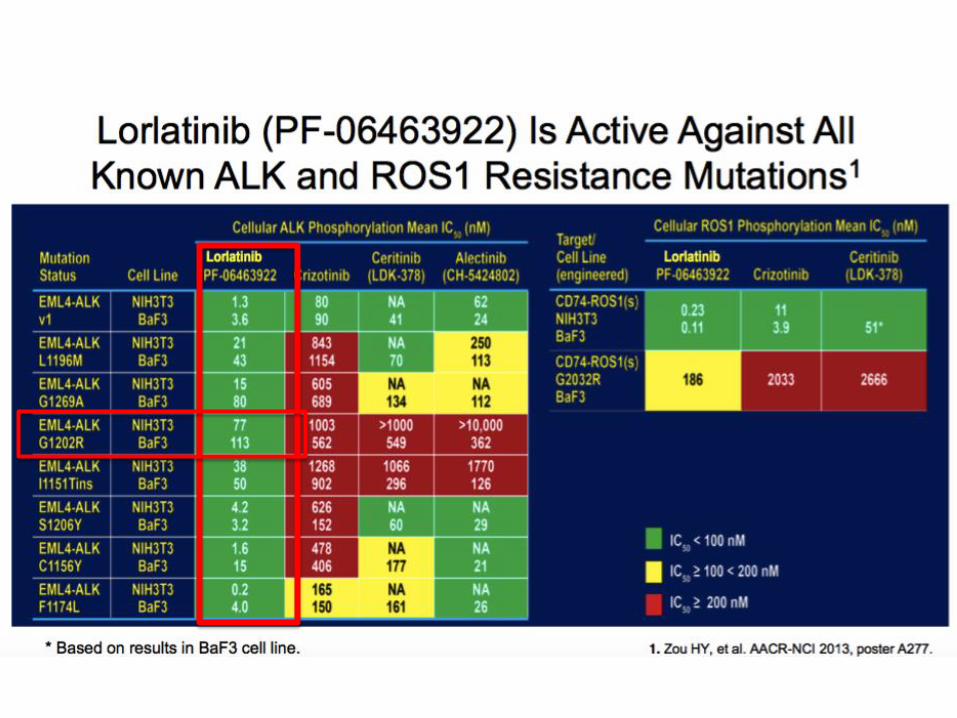
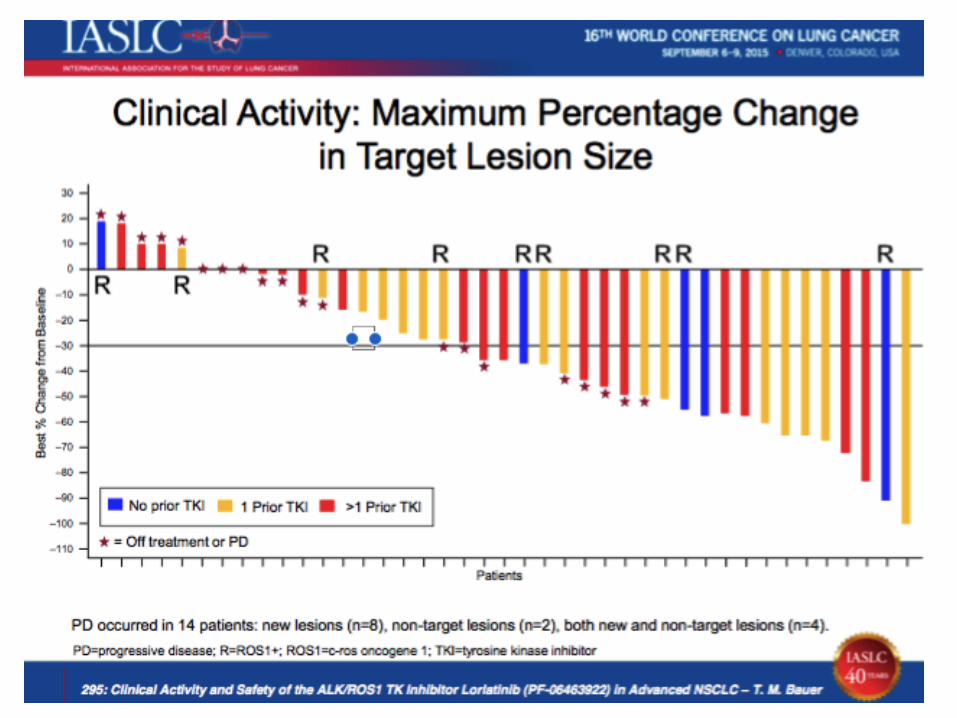
Lorlatinib
Bauer WCLC 2015
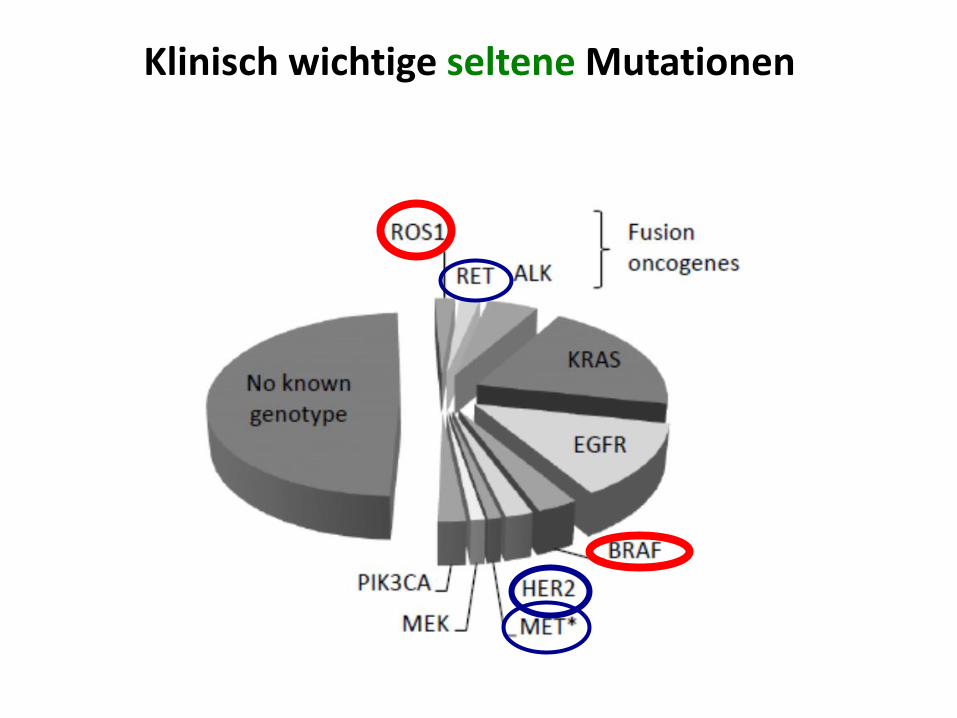
Klinisch wichtige seltene Mutationen
24
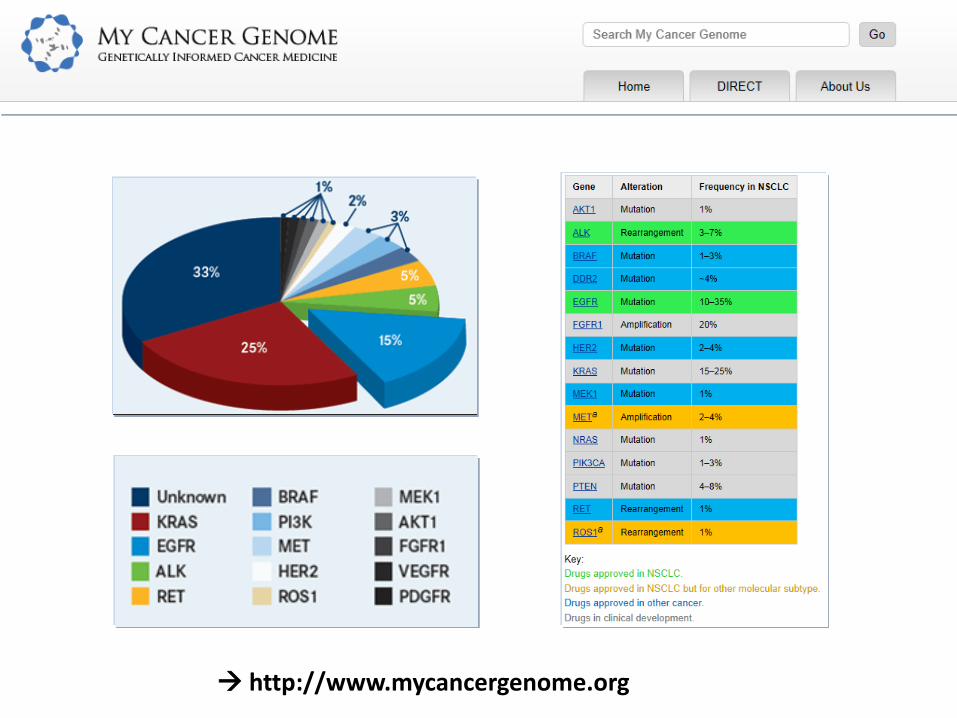
http://www.mycancergenome.org
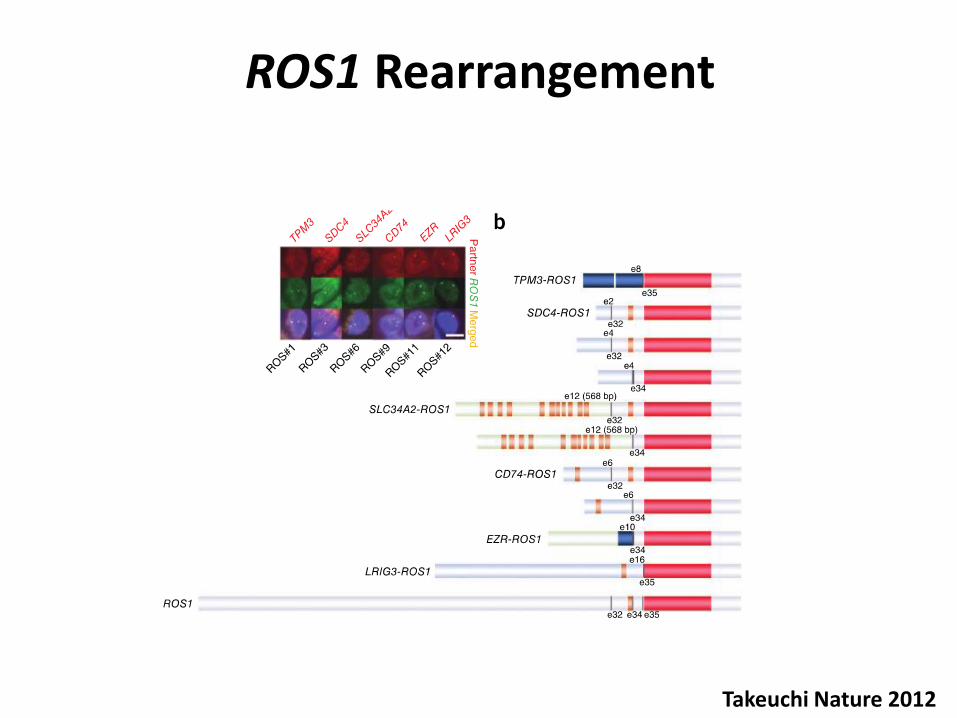
ROS1 Rearrangement
Takeuchi Nature 2012
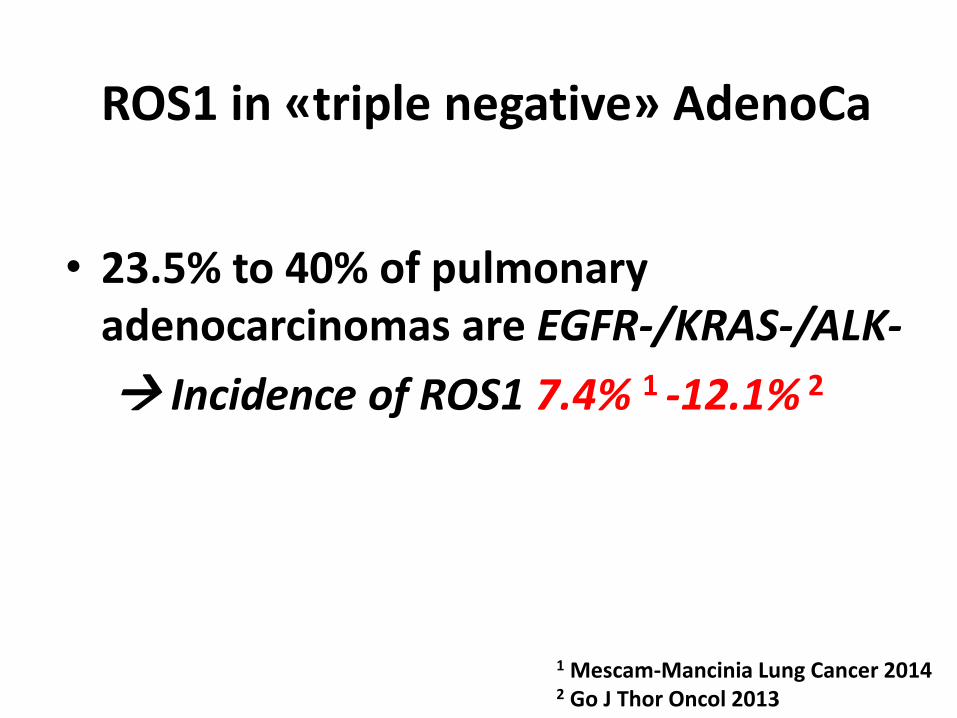
ROS1 in «triple negative» AdenoCa
• 23.5% to 40% of pulmonary adenocarcinomas are EGFR-/KRAS-/ALK-
Incidence of ROS1 7.4% 1 -12.1% 2
1 Mescam-Mancinia Lung Cancer 2014 2 Go J Thor Oncol 2013
Titel der Präsentation
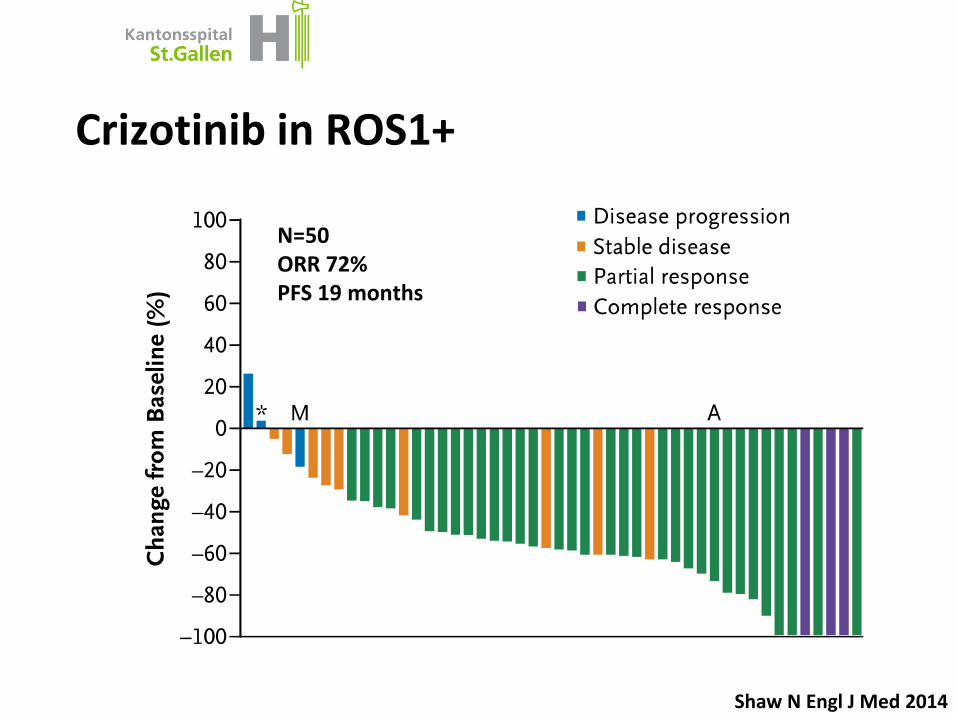
Crizotinib in ROS1+
Shaw N Engl J Med 2014
28
N=50 ORR 72% PFS 19 months
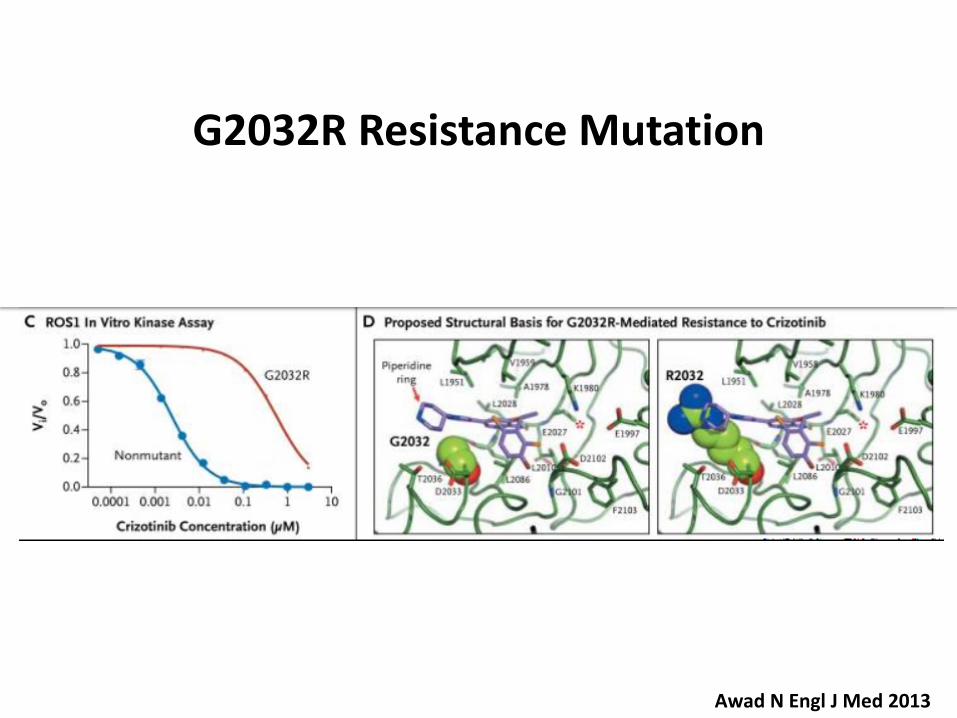
Awad N Engl J Med 2013
G2032R Resistance Mutation
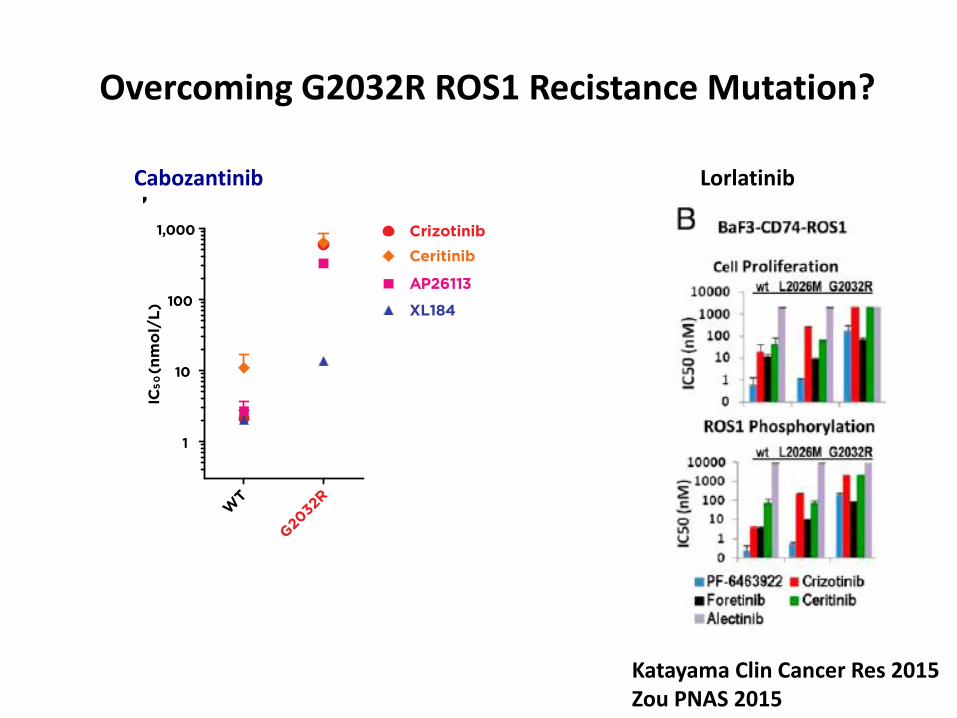
Overcoming G2032R ROS1 Recistance Mutation?
Katayama Clin Cancer Res 2015 Zou PNAS 2015
Lorlatinib Cabozantinib
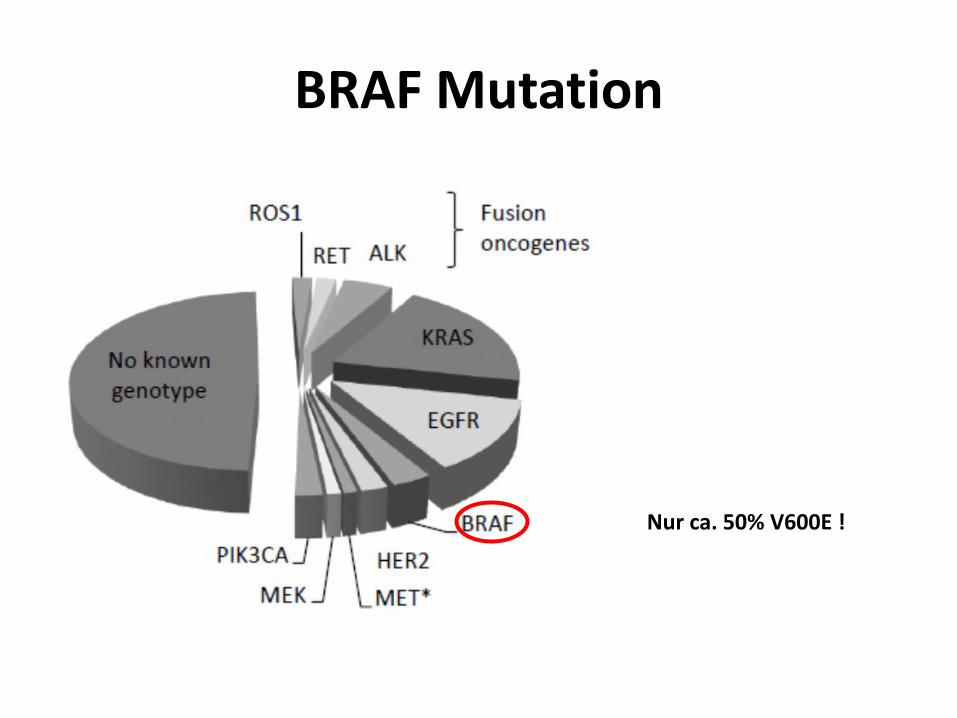
BRAF Mutation
Nur ca. 50% V600E !
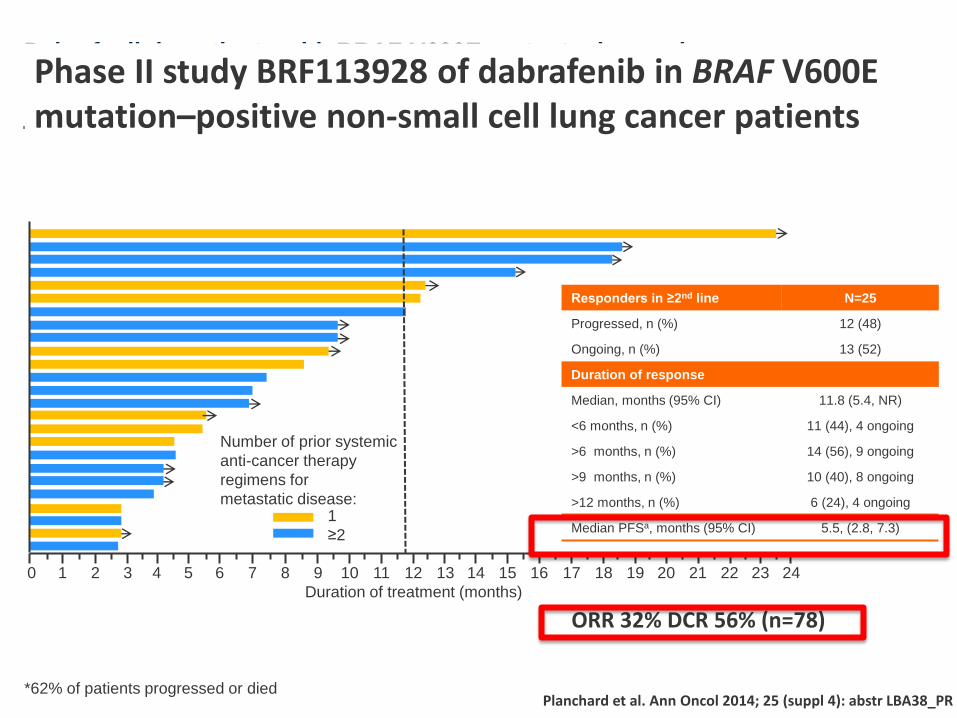
Dabrafenib in patients with BRAF V600E-mutant advanced
non-small cell lung cancer (NSCLC): A multicenter, open-label, phase II trial
(BRF113928)
Planchard et al. Ann Oncol 2014; 25 (suppl 4): abstr LBA38_PR *62% of patients progressed or died
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Number of prior systemic
anti-cancer therapy
regimens for
metastatic disease: 1
≥2
Duration of treatment (months)
Responders in ≥2nd line N=25
Progressed, n (%) 12 (48)
Ongoing, n (%) 13 (52)
Duration of response
Median, months (95% CI) 11.8 (5.4, NR)
<6 months, n (%) 11 (44), 4 ongoing
>6 months, n (%) 14 (56), 9 ongoing
>9 months, n (%) 10 (40), 8 ongoing
>12 months, n (%) 6 (24), 4 ongoing
Median PFSa, months (95% CI) 5.5, (2.8, 7.3)
ORR 32% DCR 56% (n=78)
Phase II study BRF113928 of dabrafenib in BRAF V600E mutation–positive non-small cell lung cancer patients
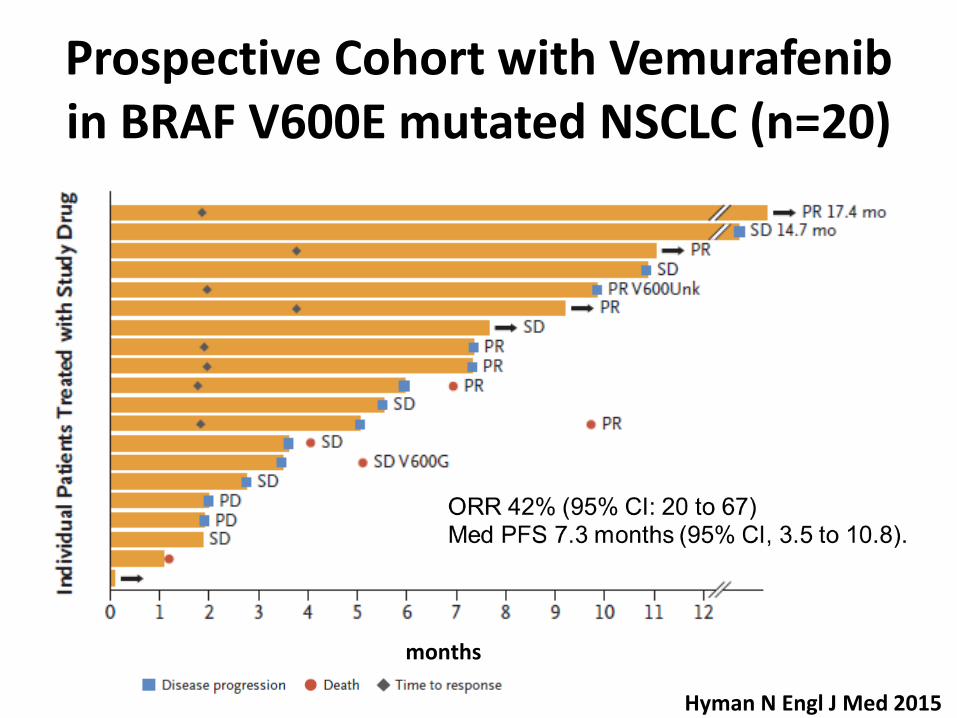
Prospective Cohort with Vemurafenib in BRAF V600E mutated NSCLC (n=20)
Hyman N Engl J Med 2015
months
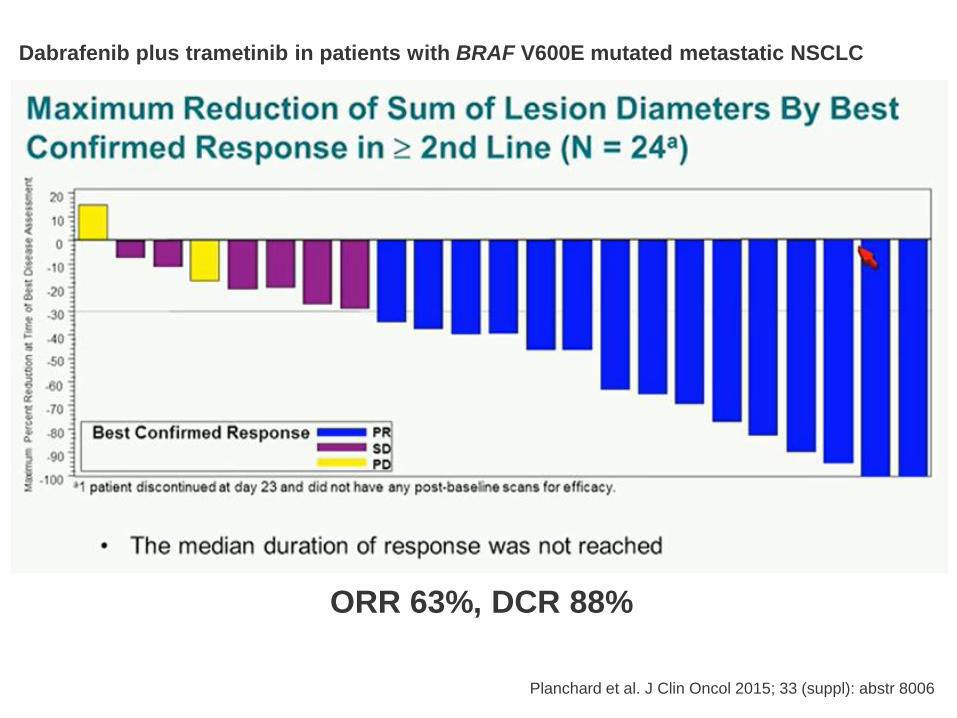
Dabrafenib plus trametinib in patients with BRAF V600E mutated metastatic NSCLC
ORR 63%, DCR 88%
Planchard et al. J Clin Oncol 2015; 33 (suppl): abstr 8006
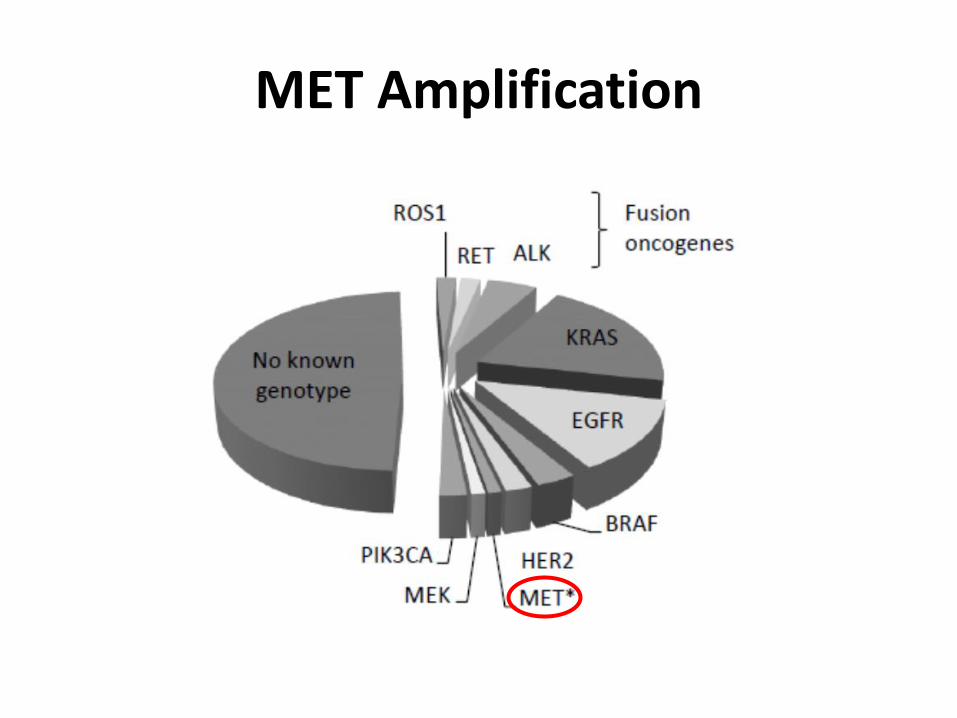
MET Amplification
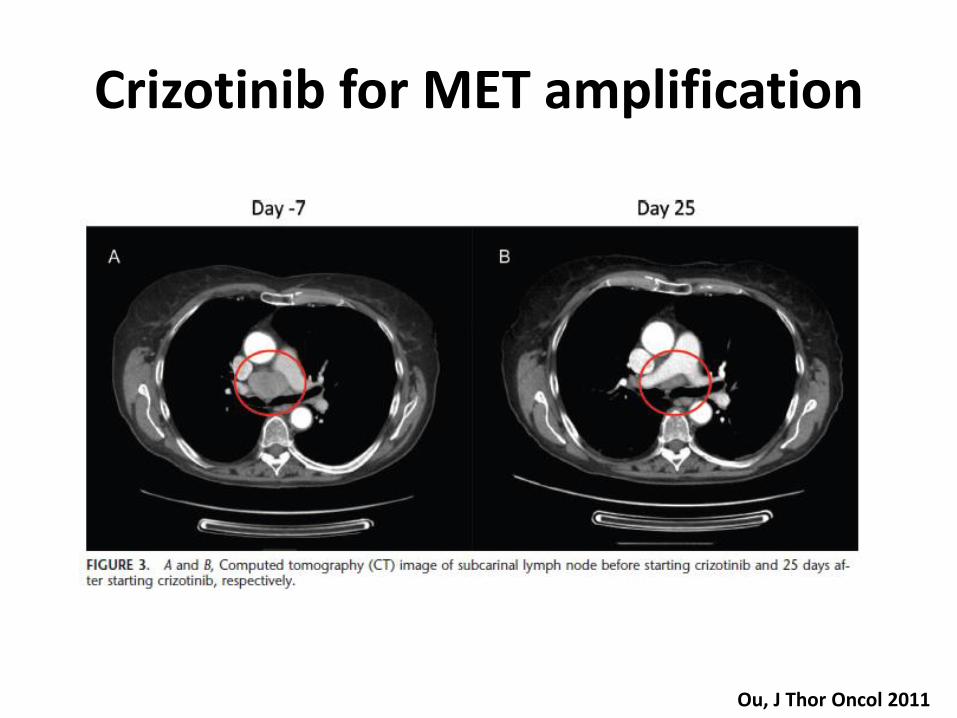
Crizotinib for MET amplification
Ou, J Thor Oncol 2011
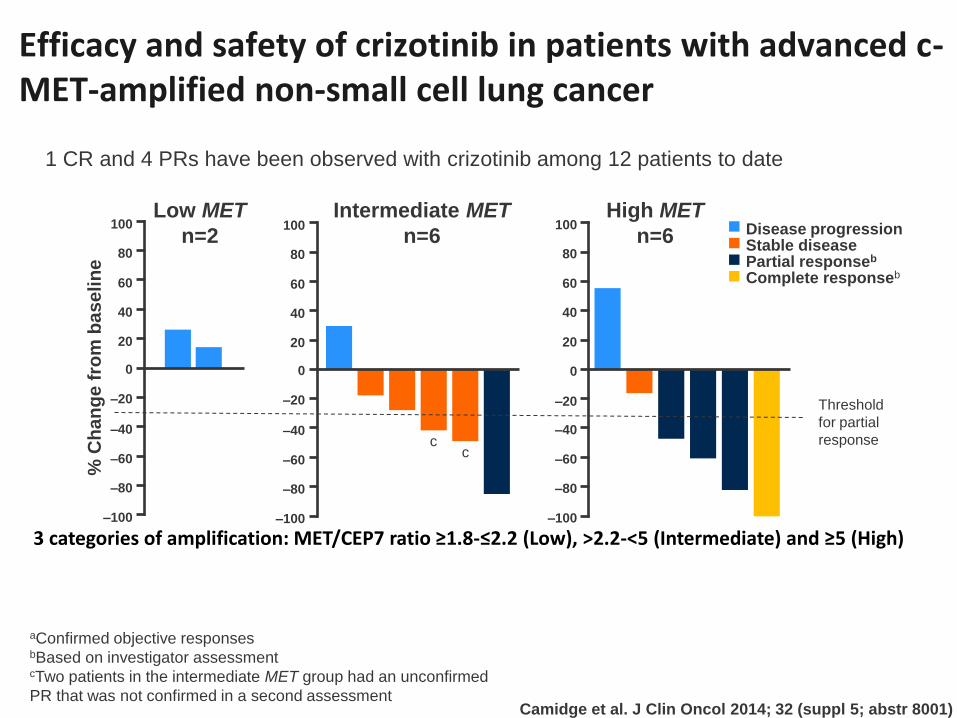
Efficacy and safety of crizotinib in patients with advanced c-MET-amplified non-small cell lung cancer
1 CR and 4 PRs have been observed with crizotinib among 12 patients to date
3 categories of amplification: MET/CEP7 ratio ≥1.8-≤2.2 (Low), >2.2-<5 (Intermediate) and ≥5 (High)
Camidge et al. J Clin Oncol 2014; 32 (suppl 5; abstr 8001)
Low MET
n=2
Intermediate MET
n=6
High MET
n=6 100
80
60
40
20
0
–20
–40
–60
–80
–100
100
80
60
40
20
0
–20
–40
–60
–80
–100
Disease progression Stable disease Partial responseb
Complete responseb
% C
ha
ng
e f
rom
ba
se
lin
e
100
80
60
40
20
0
–20
–40
–60
–80
–100
Threshold
for partial
response c
c
aConfirmed objective responses bBased on investigator assessment cTwo patients in the intermediate MET group had an unconfirmed
PR that was not confirmed in a second assessment
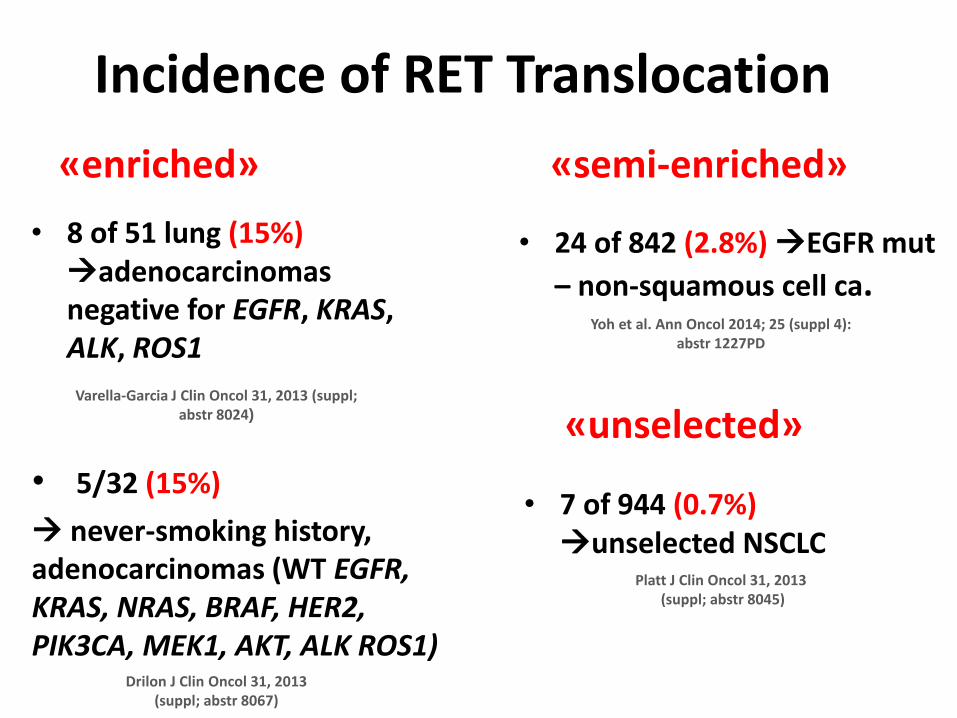
Incidence of RET Translocation
• 7 of 944 (0.7%) unselected NSCLC
• 8 of 51 lung (15%) adenocarcinomas negative for EGFR, KRAS, ALK, ROS1
Varella-Garcia J Clin Oncol 31, 2013 (suppl; abstr 8024)
Platt J Clin Oncol 31, 2013 (suppl; abstr 8045)
• 5/32 (15%)
never-smoking history, adenocarcinomas (WT EGFR, KRAS, NRAS, BRAF, HER2, PIK3CA, MEK1, AKT, ALK ROS1)
Drilon J Clin Oncol 31, 2013 (suppl; abstr 8067)
«enriched»
«unselected»
• 24 of 842 (2.8%) EGFR mut
– non-squamous cell ca. Yoh et al. Ann Oncol 2014; 25 (suppl 4):
abstr 1227PD
«semi-enriched»
Clinical response of RET+ patients
– Vandetanib: 3/3 SD (2 shrinkages) 1
– Vandetanib: 2/2 SD, Sunitinib: 2/2 PD 2
– Cabozantinib: 2/3 PR 3
39
Platt J Clin Oncol, 2013 (suppl; abstr 8045)1, Varella-Garcia J Clin Oncol, 2013 (suppl; abstr 8024)2, Drilon Cancer Discovery 20133
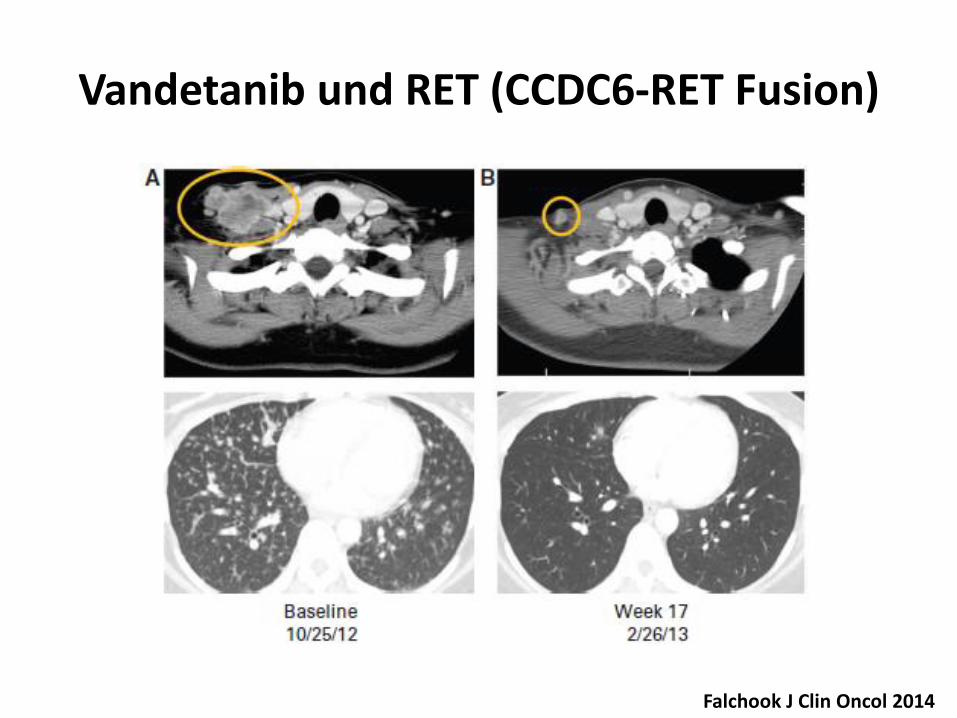
Vandetanib und RET (CCDC6-RET Fusion)
Falchook J Clin Oncol 2014
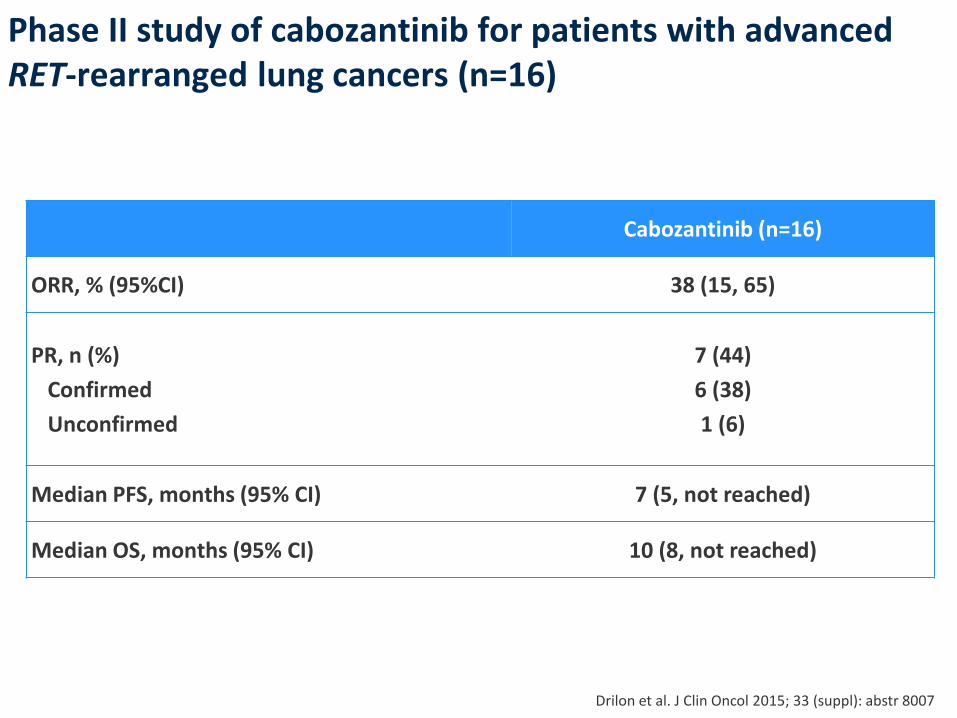
Phase II study of cabozantinib for patients with advanced RET-rearranged lung cancers (n=16)
Drilon et al. J Clin Oncol 2015; 33 (suppl): abstr 8007
Cabozantinib (n=16)
ORR, % (95%CI) 38 (15, 65)
PR, n (%)
Confirmed
Unconfirmed
7 (44)
6 (38)
1 (6)
Median PFS, months (95% CI) 7 (5, not reached)
Median OS, months (95% CI) 10 (8, not reached)
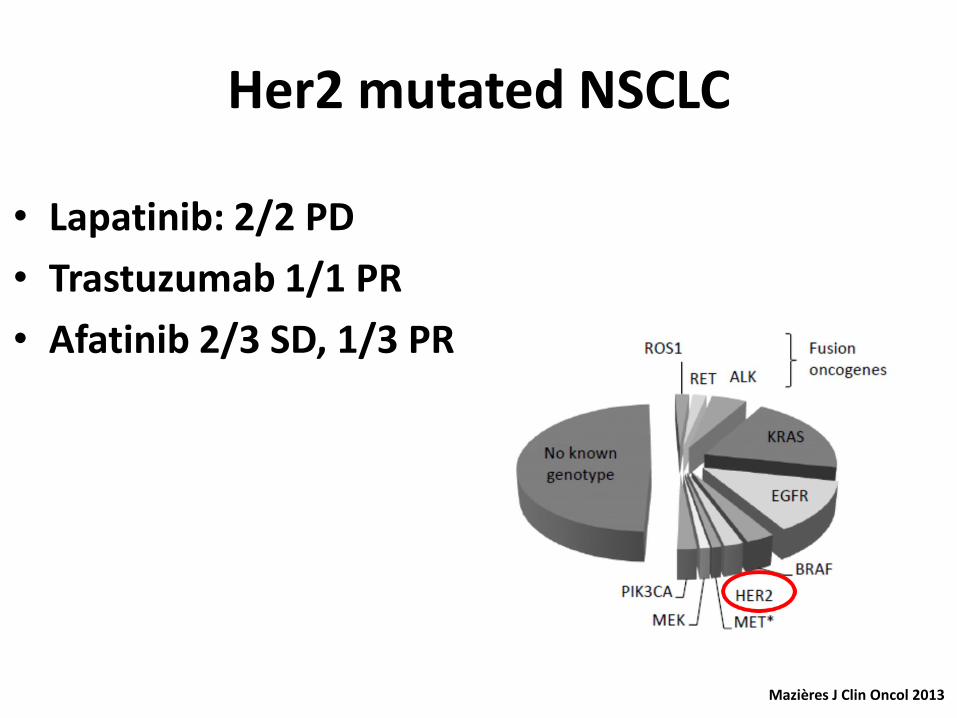
Her2 mutated NSCLC
Mazières J Clin Oncol 2013
• Lapatinib: 2/2 PD
• Trastuzumab 1/1 PR
• Afatinib 2/3 SD, 1/3 PR
26-30 September 2014, Madrid, Spain
esmo.org
esmo.org
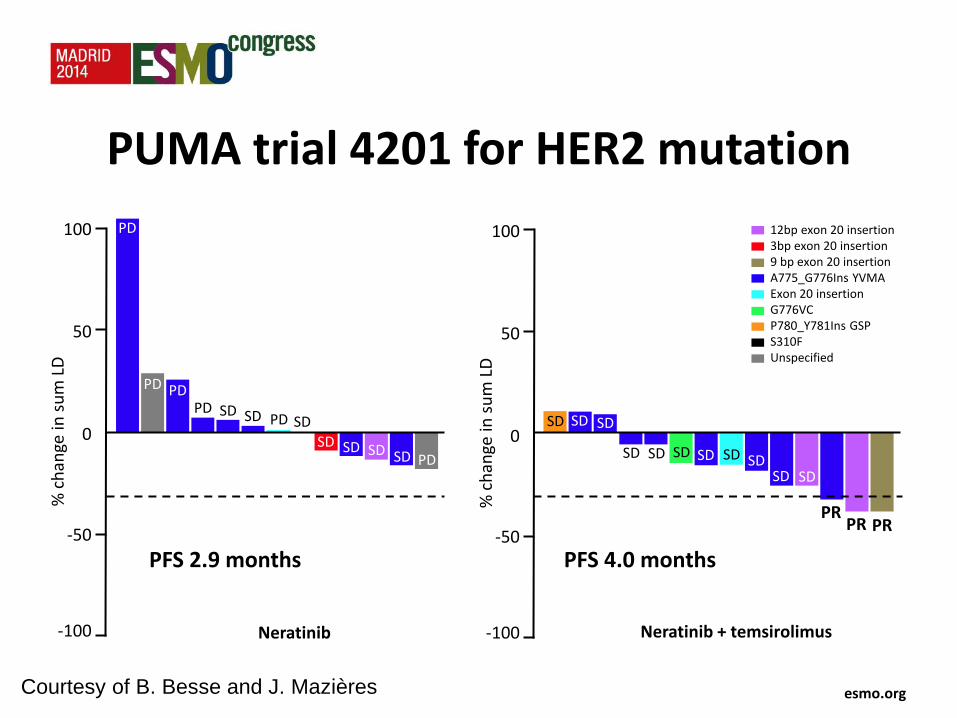
PUMA trial 4201 for HER2 mutation
100
0
-50
-100
50
% c
han
ge in
su
m L
D
PD
PD PD PD SD SD PD SD
SD SD SD SD PD SD
SD SD SD SD SD SD
SD SD SD
PR PR PR
SD
12bp exon 20 insertion 3bp exon 20 insertion 9 bp exon 20 insertion A775_G776Ins YVMA Exon 20 insertion G776VC P780_Y781Ins GSP S310F Unspecified
100
0
-50
-100
50
% c
han
ge in
su
m L
D
Neratinib Neratinib + temsirolimus
Courtesy of B. Besse and J. Mazières
PFS 2.9 months PFS 4.0 months
26-30 September 2014, Madrid, Spain
esmo.org
esmo.org
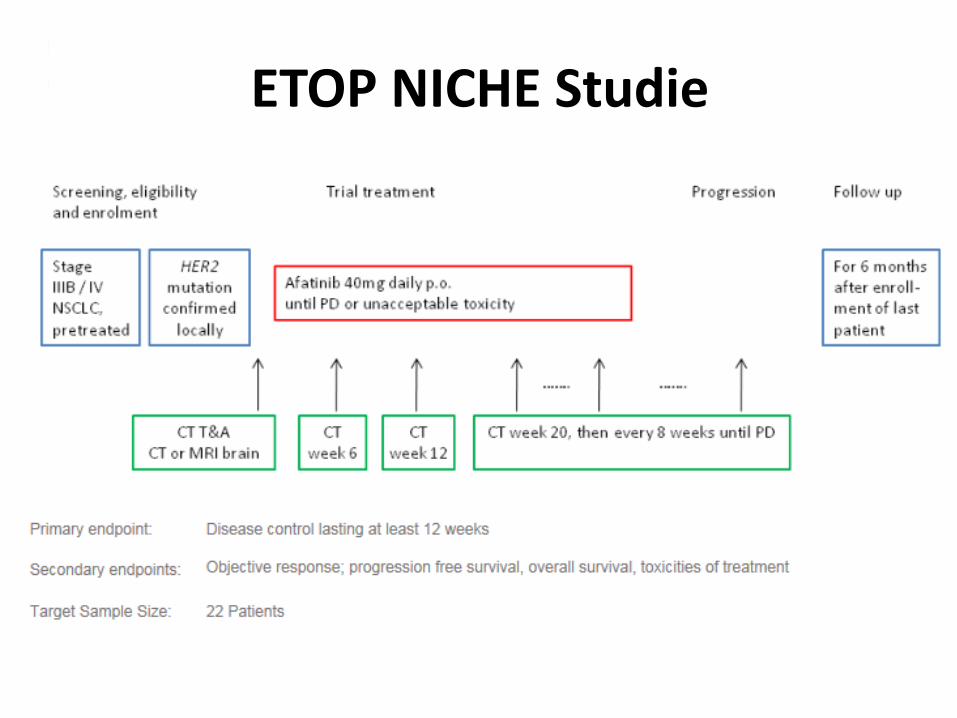
ETOP NICHE Studie
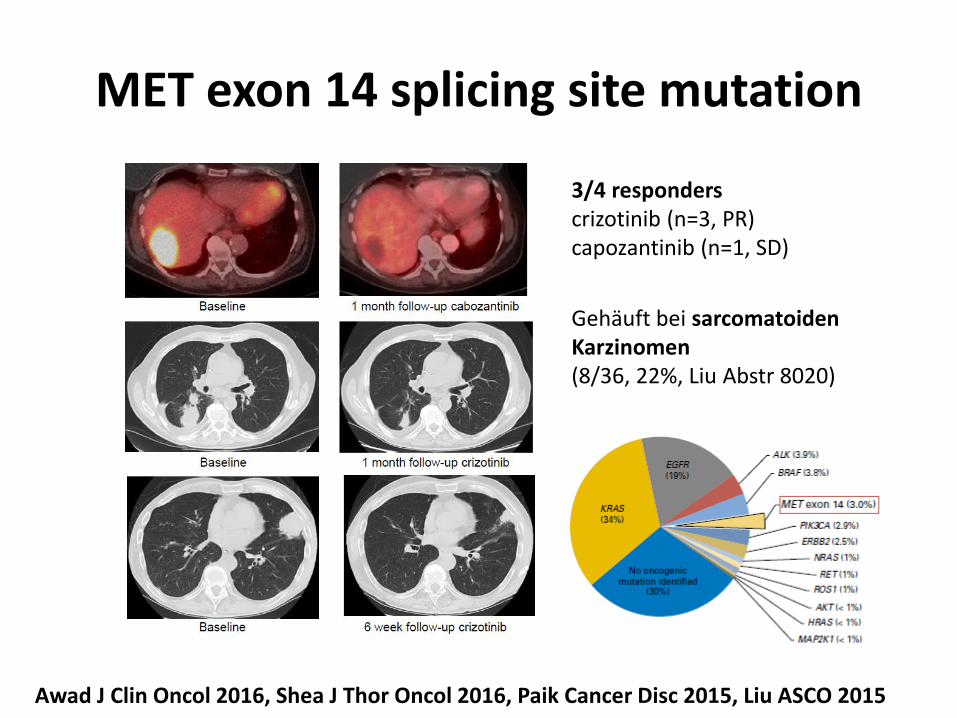
MET exon 14 splicing site mutation
3/4 responders crizotinib (n=3, PR) capozantinib (n=1, SD)
Awad J Clin Oncol 2016, Shea J Thor Oncol 2016, Paik Cancer Disc 2015, Liu ASCO 2015
Gehäuft bei sarcomatoiden Karzinomen (8/36, 22%, Liu Abstr 8020)
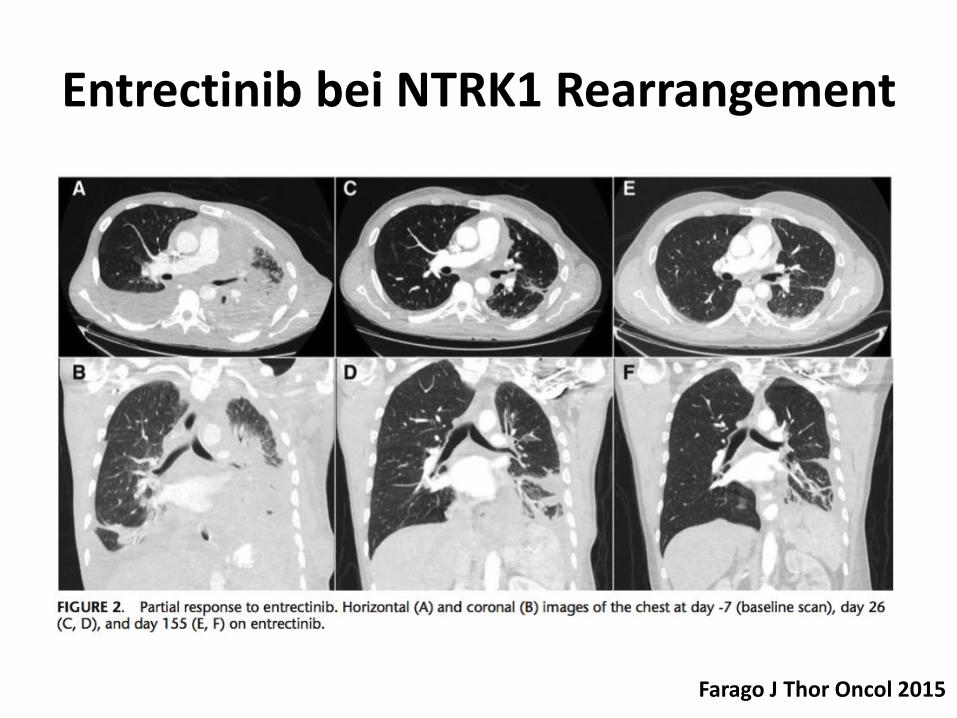
Entrectinib bei NTRK1 Rearrangement
Farago J Thor Oncol 2015
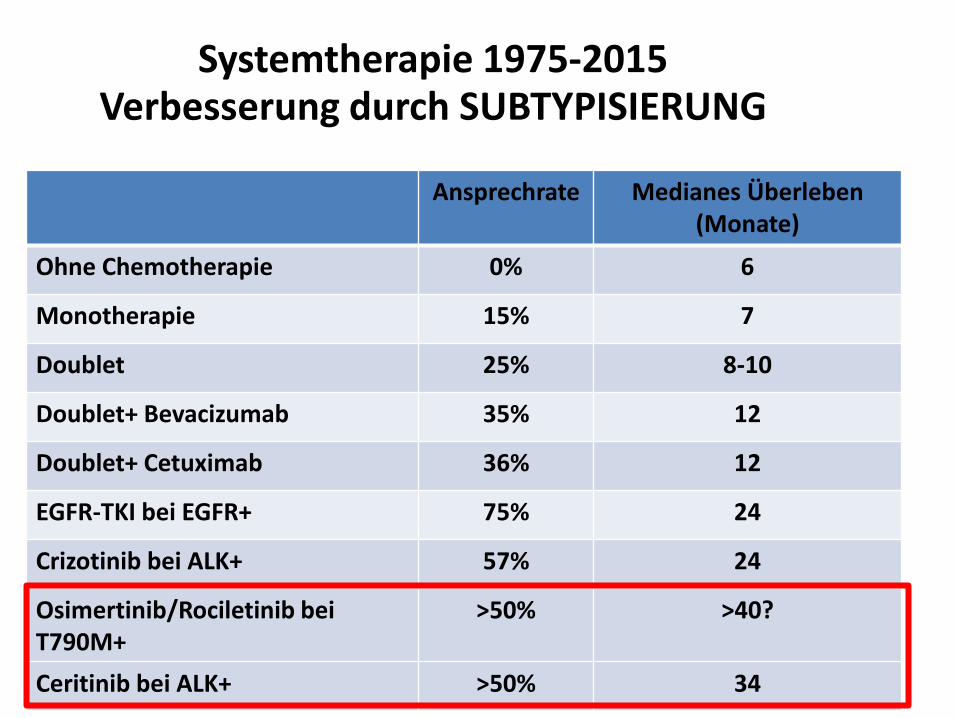
Systemtherapie 1975-2015 Verbesserung durch SUBTYPISIERUNG
47
Ansprechrate Medianes Überleben (Monate)
Ohne Chemotherapie 0% 6
Monotherapie 15% 7
Doublet 25% 8-10
Doublet+ Bevacizumab 35% 12
Doublet+ Cetuximab 36% 12
EGFR-TKI bei EGFR+ 75% 24
Crizotinib bei ALK+ 57% 24
Osimertinib/Rociletinib bei T790M+
>50% >40?
Ceritinib bei ALK+ >50% 34
Titel der Präsentation
Zusammenfassung 30-40% der nicht-plattenepitehlialen NSCLC besitzen eine
potentiell onkogene «Driver» Mutation
Randomisierte Studien zeigen einen Benefit bezüglich ORR, PFS und QoL bei EGFR und ALK
Identifikation weiterer «selteneren» molekularen Mutation und Einschluss in Studienprotokolle ist entscheidend
Erneute molekulare Testung bei Progression ermöglicht die Behandlung mit neuen wirksamen Substanzen (z. B. 790M)
















![Molekulare Biotechnologie, BSc · Studiengang Molekulare Biotechnologie Universität Heidelberg, Fakultät für Biowissenschaften [1] MODULHANDBUCH Molekulare Biotechnologie, BSc](https://img.pdfslide.org/doc/110x75/5e1dc9b208ba112f8f2362ad/molekulare-biotechnologie-studiengang-molekulare-biotechnologie-universitt-heidelberg.jpg)











