Embed Size (px)
Citation preview
Leitlinien und Empfehlungen
Anaesthesist 2019 · 68 (Suppl 1):S25–S39https://doi.org/10.1007/s00101-017-0376-3Published online: 2 November 2017© Springer Medizin Verlag GmbH 2017
Deutsche Gesellschaft für Anästhesiologie und Intensivmedizin (DGAI)1 ·Deutsche Gesellschaft für Innere Medizin (DGIM)2 · Deutsche Gesellschaft fürChirurgie (DGCH)31 Nuremberg, Germany2Wiesbaden, Germany3 Berlin, Germany
Preoperative evaluation of adultpatients before elective,noncardiothoracic surgeryJoint recommendation of the GermanSociety of Anesthesiology and Intensive CareMedicine, the German Society of Surgery,and the German Society of Internal Medicine
With significant participation from DeutscheGesellschaft für Anästhesiologie und Inten-sivmedizin (DGAI): Götz Geldner, Ludwigsburg;Jörg Karst, Berlin; Frank Wappler, Köln;Bernhard Zwissler, München. DeutscheGesellschaft für Chirurgie (DGCH): Peter Kalbe,Rinteln; Udo Obertacke, Mannheim; WolfgangSchwenk, Hamburg. Deutsche Gesellschaft fürInnere Medizin (DGIM): Matthias Pauschinger,Nürnberg.
Decision of the DGAI Executive Committeefrom 27.3.2017: Simultaneous publication inAnästh Intensivmed,AktivDruck&VerlagGmbH,Ebelsbach; AINS, Thieme Verlag, Stuttgart;and Der Anaesthesist, Springer Medizin VerlagGmbH,Berlin,Heidelberg.
English version of: Deutsche Gesellschaft fürAnästhesiologie und Intensivmedizin (DGAI),Deutsche Gesellschaft für Innere Medizin(DGIM), Deutsche Gesellschaft für Chirurgie(DGCH) (2017) Präoperative Evaluation erwach-sener Patienten vor elektiven, nicht Herz-Tho-raxchirurgischen Eingriffen. GemeinsameEmpfehlung der Deutschen Gesellschaft fürAnästhesiologie und Intensivmedizin, derDeutschen Gesellschaft für Chirurgie und derDeutschen Gesellschaft für Innere Medizin.Anaesthesist 2017·66:442–458https://doi.org/10.1007/s00101-017-0321-5.
Introduction
Theassessment of a patient’s medical his-toryandthephysicalexaminationarerec-ognized standards in preoperative eval-uation. Whether and under which cir-cumstances technical tests can contributeto reduction of the perioperative risk hasnot yet been sufficiently investigated. Thefollowing recommendations on preoper-ative evaluation are thus based not onlyon the available literature, but also on theguidelines of national and internationalspecialist societies, and on expert opin-ions. The recommendations presentedherein are valid for adult patients prior toelective noncardiothoracic surgery. Theyrepresent a revised and updated versionof the guidelines originally published in2010 by the German Society of Anes-thesiology and Intensive Care Medicine(DGAI), the German Society of Inter-nal Medicine (DGIM), and the GermanSociety of Surgery (DGCH) [1], whichhave since gained widespread acceptancein German-speaking counties and terri-tories [2, 3].
In part A, the general principles ofpreoperative evaluation are presented.The procedure in patients with knownor presumed cardiovascular disease is
addressed separately in part B (“Fur-ther cardiac testing”). Finally, the pe-rioperative management of long-termmedication is discussed (part C).
A general principles
Preoperativeevaluationshould takeplacefar enough in advance of the plannedsurgery, since this enables the length ofhospital stay, the number of discontinuedsurgeries, and also costs to be reduced [4,5]. Ideally, the appointments for all nec-essarypreoperative evaluations shouldbescheduled immediately upon establish-ment of the indication for surgery. How-ever, in general, the interval betweenpre-operative evaluation and surgery shouldnot exceed 6 weeks.
A.1 Medical history and physicalexamination
Risk evaluation serves to identifypatientswith a previously unrecognized or insuf-ficiently managed disease with relevancefor the surgery or anesthesia preopera-tively, such that treatment can be opti-mized accordingly. The basis of everypreoperative technical test is a thoroughmedical history including bleeding history
Der Anaesthesist · Suppl 1 · 2019 S25
Leitlinien und Empfehlungen
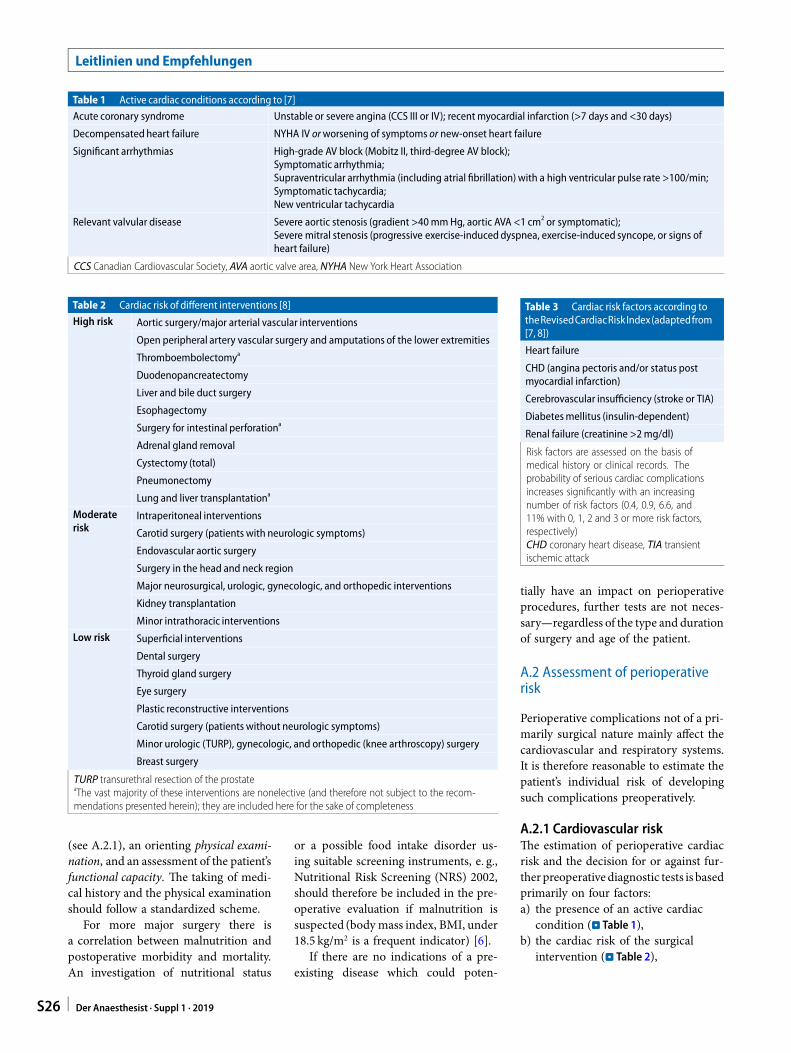
Table 1 Active cardiac conditions according to [7]
Acute coronary syndrome Unstable or severe angina (CCS III or IV); recentmyocardial infarction (>7 days and <30 days)
Decompensated heart failure NYHA IV orworsening of symptoms or new-onset heart failure
Significant arrhythmias High-grade AV block (Mobitz II, third-degree AV block);Symptomatic arrhythmia;Supraventricular arrhythmia (including atrial fibrillation) with a high ventricular pulse rate >100/min;Symptomatic tachycardia;New ventricular tachycardia
Relevant valvular disease Severe aortic stenosis (gradient >40mmHg, aortic AVA <1 cm2 or symptomatic);Severe mitral stenosis (progressive exercise-induced dyspnea, exercise-induced syncope, or signs ofheart failure)
CCS Canadian Cardiovascular Society, AVA aortic valve area, NYHA New York Heart Association
Table 2 Cardiac risk of different interventions [8]
High risk Aortic surgery/major arterial vascular interventions
Open peripheral artery vascular surgery and amputations of the lower extremities
Thromboembolectomya
Duodenopancreatectomy
Liver and bile duct surgery
Esophagectomy
Surgery for intestinal perforationa
Adrenal gland removal
Cystectomy (total)
Pneumonectomy
Lung and liver transplantationa
Moderaterisk
Intraperitoneal interventions
Carotid surgery (patients with neurologic symptoms)
Endovascular aortic surgery
Surgery in the head and neck region
Major neurosurgical, urologic, gynecologic, and orthopedic interventions
Kidney transplantation
Minor intrathoracic interventions
Low risk Superficial interventions
Dental surgery
Thyroid gland surgery
Eye surgery
Plastic reconstructive interventions
Carotid surgery (patients without neurologic symptoms)
Minor urologic (TURP), gynecologic, and orthopedic (knee arthroscopy) surgery
Breast surgery
TURP transurethral resection of the prostateaThe vast majority of these interventions are nonelective (and therefore not subject to the recom-mendations presented herein); they are included here for the sake of completeness
(see A.2.1), an orienting physical exami-nation, and an assessment of the patient’sfunctional capacity. The taking of medi-cal history and the physical examinationshould follow a standardized scheme.
For more major surgery there isa correlation between malnutrition andpostoperative morbidity and mortality.An investigation of nutritional status
or a possible food intake disorder us-ing suitable screening instruments, e. g.,Nutritional Risk Screening (NRS) 2002,should therefore be included in the pre-operative evaluation if malnutrition issuspected (body mass index, BMI, under18.5 kg/m2 is a frequent indicator) [6].
If there are no indications of a pre-existing disease which could poten-
Table 3 Cardiac risk factors according totheRevisedCardiacRiskIndex(adaptedfrom[7, 8])
Heart failure
CHD (angina pectoris and/or status postmyocardial infarction)
Cerebrovascular insufficiency (stroke or TIA)
Diabetesmellitus (insulin-dependent)
Renal failure (creatinine >2mg/dl)
Risk factors are assessed on the basis ofmedical history or clinical records. Theprobability of serious cardiac complicationsincreases significantly with an increasingnumber of risk factors (0.4, 0.9, 6.6, and11% with 0, 1, 2 and 3 or more risk factors,respectively)CHD coronary heart disease, TIA transientischemic attack
tially have an impact on perioperativeprocedures, further tests are not neces-sary—regardless of the type and durationof surgery and age of the patient.
A.2 Assessment of perioperativerisk
Perioperative complications not of a pri-marily surgical nature mainly affect thecardiovascular and respiratory systems.It is therefore reasonable to estimate thepatient’s individual risk of developingsuch complications preoperatively.
A.2.1 Cardiovascular riskThe estimation of perioperative cardiacrisk and the decision for or against fur-therpreoperative diagnostic tests is basedprimarily on four factors:a) the presence of an active cardiac
condition (. Table 1),b) the cardiac risk of the surgical
intervention (. Table 2),
S26 Der Anaesthesist · Suppl 1 · 2019

Abstract · Zusammenfassung
Anaesthesist 2019 · 68 (Suppl 1):S25–S39 https://doi.org/10.1007/s00101-017-0376-3© Springer Medizin Verlag GmbH 2017
Deutsche Gesellschaft für Anästhesiologie und Intensivmedizin (DGAI) · Deutsche Gesellschaft für Innere Medizin (DGIM) · DeutscheGesellschaft für Chirurgie (DGCH)
Preoperative evaluation of adult patients before elective, noncardiothoracic surgery. Jointrecommendation of the German Society of Anesthesiology and Intensive Care Medicine, the GermanSociety of Surgery, and the German Society of Internal Medicine
AbstractEvaluation of the patient’smedical history anda physical examination are the cornerstonesof risk assessment prior to elective surgery,and may help to optimize the patient’spreoperative medical condition and guideperioperative management. Whetherperformance of additional technical tests(e. g., blood chemistry, electrocardiography,spirometry, chest x-ray) can contribute toreduction of the perioperative risk is oftennot well known or controversial. Similarly,there is considerable uncertainty among anes-thesiologists, internists, and surgeons withrespect to perioperativemanagement of thepatient’s long-term medication. Therefore, theGerman Scientific Societies of Anesthesiologyand Intensive Care Medicine (DGAI), InternalMedicine (DGIM), and Surgery (DGCH) havejoined to elaborate recommendations on the
preoperative evaluation of adult patientsprior to elective noncardiothoracic surgerywhich were initially published in 2010. Theserecommendations have now been updatedbased on the current literature and existinginternational guidelines. In the first part, thegeneral principles of preoperative evaluationare described (part A). The current conceptsfor extended evaluation of patients withknown or suspected major cardiovasculardisease are presented in part B. Finally, theperioperativemanagement of patients’ long-term medication is discussed (part C). Theconcepts proposed in these interdisciplinaryrecommendations endorsed by the DGAI,DGIM, and DGCH provide a common basisfor structured preoperative risk assessmentand management. These recommendationsaim to ensure that surgical patients undergo
a rational preoperative assessment and, atthe same time, aim to avoid unnecessary,costly, and potentially dangerous testing. Thejoint recommendations reflect the currentstate-of-the-art knowledge as well as expertopinions, because scientific-based evidence isnot always available. These recommendationswill be subject to regular re-evaluation andupdating when new validated evidencebecomes available.Contribution available free of charge by “FreeAccess”.
KeywordsPreoperative evaluation · Perioperative risk ·Cardiac risk · Pulmonary risk · Interdisciplinaryrecommendation
Präoperative Evaluation erwachsener Patienten vor elektiven, nicht Herz-Thorax-chirurgischenEingriffen. Gemeinsame Empfehlung der Deutschen Gesellschaft für Anästhesiologie undIntensivmedizin, der Deutschen Gesellschaft für Chirurgie und der Deutschen Gesellschaft für InnereMedizin
ZusammenfassungDie präoperative Anamnese und körperlicheUntersuchung sind anerkannter Standardbei der Risikoevaluation von Patientenvor elektiven chirurgischen Eingriffen. Obund unter welchen Umständen technischeVoruntersuchungen dazu beitragen können,das perioperative Risiko zu reduzieren, istbislang nur unzureichend untersucht. Auchbesteht unter Anästhesisten, Chirurgenund Internisten vielfach Unsicherheit imperioperativen Umgang mit der Dauerme-dikation. Die deutschen wissenschaftlichenFachgesellschaften für Anästhesiologie undIntensivmedizin (DGAI), Chirurgie (DGCH)und Innere Medizin (DGIM) haben daher einegemeinsame Empfehlung zur präoperativenEvaluation erwachsener Patienten vorelektiven, nicht Herz-Thorax-chirurgischen
Eingriffen erarbeitet und erstmals im Jahr2010 publiziert. Die vorliegende Fassungist eine Überarbeitung der Stellungnahmevon 2010 unter Einbeziehung der seitherpublizierten Literatur sowie von aktuellenLeitlinien internationaler Fachgesellschaften.Zunächst werden die allgemeinen Prinzipiender präoperativen Evaluation dargestellt(Teil A). Das Vorgehen bei Patienten mitbekannten oder vermuteten kardiovaskulärenVorerkrankungen wird gesondert betrachtet(Teil B: „Erweiterte kardiale Diagnostik“).Abschließend wird der perioperativeUmgang mit der Dauermedikation diskutiert(Teil C). Die vorgestellten Konzepte stellenfachübergreifende Empfehlungen dar, die einstrukturiertes und gemeinsames Vorgehenermöglichen sollen. Ihr Ziel ist es, durch
transparente und verbindliche Abspracheneine hohe Patientenorientierung unterVermeidung unnötiger Voruntersuchungen zugewährleisten, präoperative Untersuchungs-abläufe zu verkürzen sowie letztlich Kosten zureduzieren. Die gemeinsamen Empfehlungenvon DGAI, DGCH und DGIM spiegeln dengegenwärtigen Kenntnisstand, aber auch dieMeinungen von Experten wider, da nicht fürjede Fragestellung wissenschaftliche Evidenzbesteht. Daher werden eine regelmäßigeÜberprüfung und Aktualisierung derEmpfehlungen erfolgen, sobald gesicherteneue Erkenntnisse vorliegen.
SchlüsselwörterPräoperative Evaluation · PerioperativesRisiko · Kardiales Risiko · Pulmonales Risiko
Der Anaesthesist · Suppl 1 · 2019 S27
Leitlinien und Empfehlungen
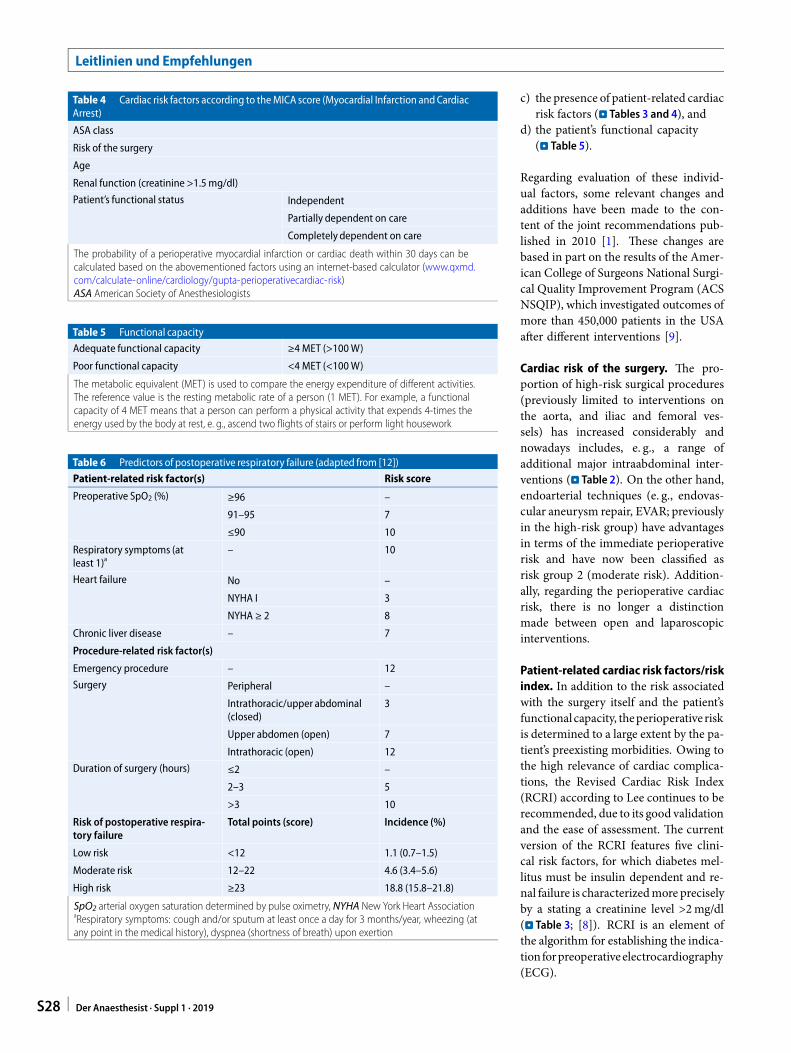
Table 4 Cardiac risk factors according to theMICA score (Myocardial Infarction andCardiacArrest)
ASA class
Risk of the surgery
Age
Renal function (creatinine >1.5mg/dl)
Patient’s functional status Independent
Partially dependent on care
Completely dependent on care
The probability of a perioperative myocardial infarction or cardiac death within 30 days can becalculated based on the abovementioned factors using an internet-based calculator (www.qxmd.com/calculate-online/cardiology/gupta-perioperativecardiac-risk)ASA American Society of Anesthesiologists
Table 5 Functional capacity
Adequate functional capacity ≥4 MET (>100W)
Poor functional capacity <4 MET (<100W)
The metabolic equivalent (MET) is used to compare the energy expenditure of different activities.The reference value is the resting metabolic rate of a person (1 MET). For example, a functionalcapacity of 4 MET means that a person can perform a physical activity that expends 4-times theenergy used by the body at rest, e. g., ascend two flights of stairs or perform light housework
Table 6 Predictors of postoperative respiratory failure (adapted from [12])
Patient-related risk factor(s) Risk score
Preoperative SpO2 (%) ≥96 –
91–95 7
≤90 10
Respiratory symptoms (atleast 1)a
– 10
Heart failure No –
NYHA I 3
NYHA ≥ 2 8
Chronic liver disease – 7
Procedure-related risk factor(s)
Emergency procedure – 12
Surgery Peripheral –
Intrathoracic/upper abdominal(closed)
3
Upper abdomen (open) 7
Intrathoracic (open) 12
Duration of surgery (hours) ≤2 –
2–3 5
>3 10
Risk of postoperative respira-tory failure
Total points (score) Incidence (%)
Low risk <12 1.1 (0.7–1.5)
Moderate risk 12–22 4.6 (3.4–5.6)
High risk ≥23 18.8 (15.8–21.8)
SpO2 arterial oxygen saturation determined by pulse oximetry, NYHA New York Heart AssociationaRespiratory symptoms: cough and/or sputum at least once a day for 3 months/year, wheezing (atany point in the medical history), dyspnea (shortness of breath) upon exertion
c) the presence of patient-related cardiacrisk factors (. Tables 3 and 4), and
d) the patient’s functional capacity(. Table 5).
Regarding evaluation of these individ-ual factors, some relevant changes andadditions have been made to the con-tent of the joint recommendations pub-lished in 2010 [1]. These changes arebased in part on the results of the Amer-ican College of Surgeons National Surgi-cal Quality Improvement Program (ACSNSQIP), which investigated outcomes ofmore than 450,000 patients in the USAafter different interventions [9].
Cardiac risk of the surgery. The pro-portion of high-risk surgical procedures(previously limited to interventions onthe aorta, and iliac and femoral ves-sels) has increased considerably andnowadays includes, e. g., a range ofadditional major intraabdominal inter-ventions (. Table 2). On the other hand,endoarterial techniques (e. g., endovas-cular aneurysm repair, EVAR; previouslyin the high-risk group) have advantagesin terms of the immediate perioperativerisk and have now been classified asrisk group 2 (moderate risk). Addition-ally, regarding the perioperative cardiacrisk, there is no longer a distinctionmade between open and laparoscopicinterventions.
Patient-related cardiac risk factors/riskindex. In addition to the risk associatedwith the surgery itself and the patient’sfunctionalcapacity, theperioperative riskis determined to a large extent by the pa-tient’s preexisting morbidities. Owing tothe high relevance of cardiac complica-tions, the Revised Cardiac Risk Index(RCRI) according to Lee continues to berecommended, due to its good validationand the ease of assessment. The currentversion of the RCRI features five clini-cal risk factors, for which diabetes mel-litus must be insulin dependent and re-nal failure is characterizedmore preciselyby a stating a creatinine level >2mg/dl(. Table 3; [8]). RCRI is an element ofthe algorithm for establishing the indica-tionforpreoperativeelectrocardiography(ECG).
S28 Der Anaesthesist · Suppl 1 · 2019
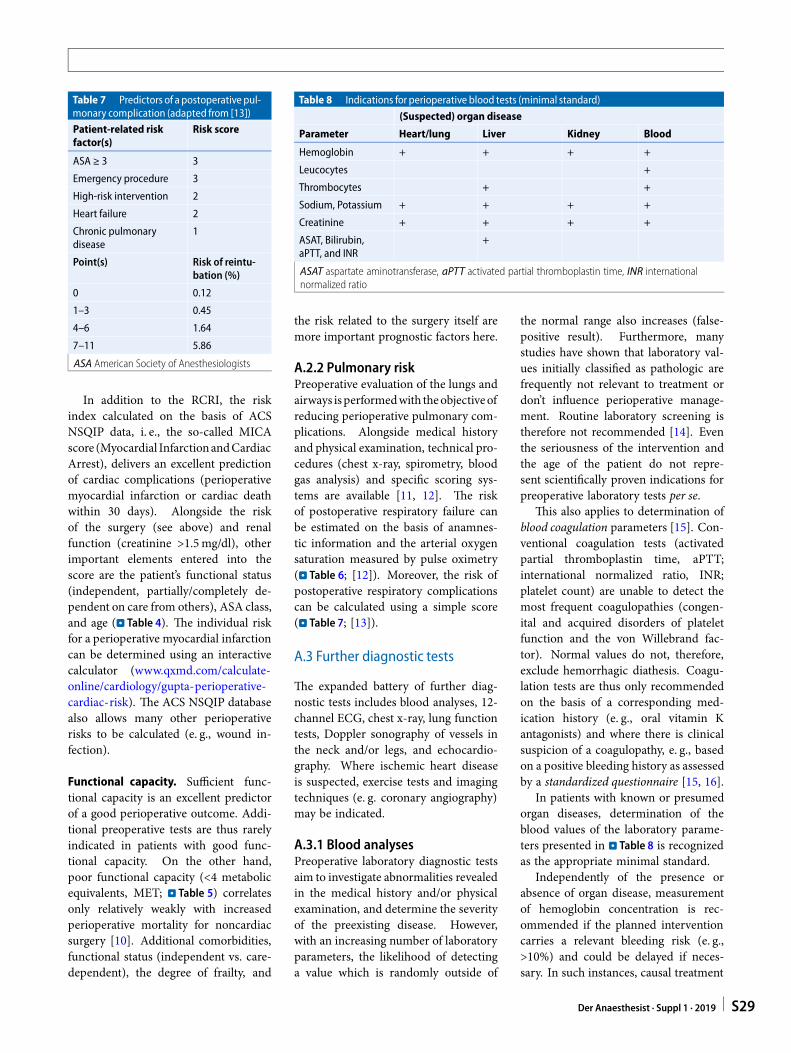
Table 7 Predictors of a postoperative pul-monary complication (adapted from [13])
Patient-related riskfactor(s)
Risk score
ASA ≥ 3 3
Emergency procedure 3
High-risk intervention 2
Heart failure 2
Chronic pulmonarydisease
1
Point(s) Risk of reintu-bation (%)
0 0.12
1–3 0.45
4–6 1.64
7–11 5.86
ASA American Society of Anesthesiologists
In addition to the RCRI, the riskindex calculated on the basis of ACSNSQIP data, i. e., the so-called MICAscore (Myocardial InfarctionandCardiacArrest), delivers an excellent predictionof cardiac complications (perioperativemyocardial infarction or cardiac deathwithin 30 days). Alongside the riskof the surgery (see above) and renalfunction (creatinine >1.5mg/dl), otherimportant elements entered into thescore are the patient’s functional status(independent, partially/completely de-pendent on care from others), ASA class,and age (. Table 4). The individual riskfor a perioperative myocardial infarctioncan be determined using an interactivecalculator (www.qxmd.com/calculate-online/cardiology/gupta-perioperative-cardiac-risk). The ACS NSQIP databasealso allows many other perioperativerisks to be calculated (e. g., wound in-fection).
Functional capacity. Sufficient func-tional capacity is an excellent predictorof a good perioperative outcome. Addi-tional preoperative tests are thus rarelyindicated in patients with good func-tional capacity. On the other hand,poor functional capacity (<4 metabolicequivalents, MET; . Table 5) correlatesonly relatively weakly with increasedperioperative mortality for noncardiacsurgery [10]. Additional comorbidities,functional status (independent vs. care-dependent), the degree of frailty, and
Table 8 Indications for perioperative blood tests (minimal standard)
(Suspected) organ disease
Parameter Heart/lung Liver Kidney Blood
Hemoglobin + + + +
Leucocytes +
Thrombocytes + +
Sodium, Potassium + + + +
Creatinine + + + +
ASAT, Bilirubin,aPTT, and INR
+
ASAT aspartate aminotransferase, aPTT activated partial thromboplastin time, INR internationalnormalized ratio
the risk related to the surgery itself aremore important prognostic factors here.
A.2.2 Pulmonary riskPreoperative evaluation of the lungs andairways isperformedwith theobjectiveofreducing perioperative pulmonary com-plications. Alongside medical historyand physical examination, technical pro-cedures (chest x-ray, spirometry, bloodgas analysis) and specific scoring sys-tems are available [11, 12]. The riskof postoperative respiratory failure canbe estimated on the basis of anamnes-tic information and the arterial oxygensaturation measured by pulse oximetry(. Table 6; [12]). Moreover, the risk ofpostoperative respiratory complicationscan be calculated using a simple score(. Table 7; [13]).
A.3 Further diagnostic tests
The expanded battery of further diag-nostic tests includes blood analyses, 12-channel ECG, chest x-ray, lung functiontests, Doppler sonography of vessels inthe neck and/or legs, and echocardio-graphy. Where ischemic heart diseaseis suspected, exercise tests and imagingtechniques (e. g. coronary angiography)may be indicated.
A.3.1 Blood analysesPreoperative laboratory diagnostic testsaim to investigate abnormalities revealedin the medical history and/or physicalexamination, and determine the severityof the preexisting disease. However,with an increasing number of laboratoryparameters, the likelihood of detectinga value which is randomly outside of
the normal range also increases (false-positive result). Furthermore, manystudies have shown that laboratory val-ues initially classified as pathologic arefrequently not relevant to treatment ordon’t influence perioperative manage-ment. Routine laboratory screening istherefore not recommended [14]. Eventhe seriousness of the intervention andthe age of the patient do not repre-sent scientifically proven indications forpreoperative laboratory tests per se.
This also applies to determination ofblood coagulation parameters [15]. Con-ventional coagulation tests (activatedpartial thromboplastin time, aPTT;international normalized ratio, INR;platelet count) are unable to detect themost frequent coagulopathies (congen-ital and acquired disorders of plateletfunction and the von Willebrand fac-tor). Normal values do not, therefore,exclude hemorrhagic diathesis. Coagu-lation tests are thus only recommendedon the basis of a corresponding med-ication history (e. g., oral vitamin Kantagonists) and where there is clinicalsuspicion of a coagulopathy, e. g., basedon a positive bleeding history as assessedby a standardized questionnaire [15, 16].
In patients with known or presumedorgan diseases, determination of theblood values of the laboratory parame-ters presented in . Table 8 is recognizedas the appropriate minimal standard.
Independently of the presence orabsence of organ disease, measurementof hemoglobin concentration is rec-ommended if the planned interventioncarries a relevant bleeding risk (e. g.,>10%) and could be delayed if neces-sary. In such instances, causal treatment
Der Anaesthesist · Suppl 1 · 2019 S29
Leitlinien und Empfehlungen
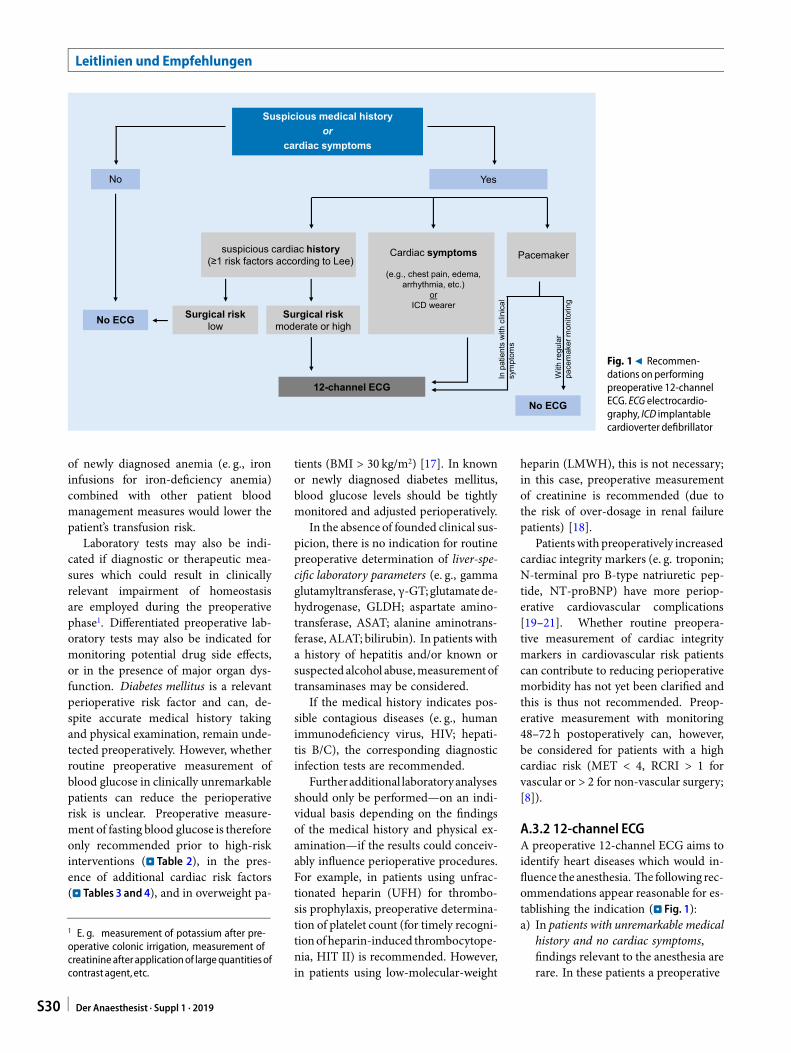
suspicious cardiac history(≥1 risk factors according to Lee)
No Yes
Suspicious medical historyor
cardiac symptoms
12-channel ECG
Cardiac symptoms
(e.g., chest pain, edema, arrhythmia, etc.)
orICD wearer
Pacemaker
In p
atie
nts
with
clin
ical
sym
ptom
s
No ECG Surgical riskmoderate or high
Surgical risklow
With
regu
lar
pace
mak
er m
onito
ring
No ECG
Fig. 19 Recommen-dations on performingpreoperative 12-channelECG. ECG electrocardio-graphy, ICD implantablecardioverter defibrillator
of newly diagnosed anemia (e. g., ironinfusions for iron-deficiency anemia)combined with other patient bloodmanagement measures would lower thepatient’s transfusion risk.
Laboratory tests may also be indi-cated if diagnostic or therapeutic mea-sures which could result in clinicallyrelevant impairment of homeostasisare employed during the preoperativephase1. Differentiated preoperative lab-oratory tests may also be indicated formonitoring potential drug side effects,or in the presence of major organ dys-function. Diabetes mellitus is a relevantperioperative risk factor and can, de-spite accurate medical history takingand physical examination, remain unde-tected preoperatively. However, whetherroutine preoperative measurement ofblood glucose in clinically unremarkablepatients can reduce the perioperativerisk is unclear. Preoperative measure-ment of fasting blood glucose is thereforeonly recommended prior to high-riskinterventions (. Table 2), in the pres-ence of additional cardiac risk factors(. Tables 3 and 4), and in overweight pa-
1 E. g. measurement of potassium after pre-operative colonic irrigation, measurement ofcreatinine after applicationof largequantitiesofcontrastagent,etc.
tients (BMI > 30 kg/m2) [17]. In knownor newly diagnosed diabetes mellitus,blood glucose levels should be tightlymonitored and adjusted perioperatively.
In the absence of founded clinical sus-picion, there is no indication for routinepreoperative determination of liver-spe-cific laboratory parameters (e. g., gammaglutamyltransferase, γ-GT;glutamatede-hydrogenase, GLDH; aspartate amino-transferase, ASAT; alanine aminotrans-ferase, ALAT; bilirubin). In patients witha history of hepatitis and/or known orsuspected alcohol abuse,measurementoftransaminases may be considered.
If the medical history indicates pos-sible contagious diseases (e. g., humanimmunodeficiency virus, HIV; hepati-tis B/C), the corresponding diagnosticinfection tests are recommended.
Furtheradditional laboratoryanalysesshould only be performed—on an indi-vidual basis depending on the findingsof the medical history and physical ex-amination—if the results could conceiv-ably influence perioperative procedures.For example, in patients using unfrac-tionated heparin (UFH) for thrombo-sis prophylaxis, preoperative determina-tion of platelet count (for timely recogni-tionofheparin-induced thrombocytope-nia, HIT II) is recommended. However,in patients using low-molecular-weight
heparin (LMWH), this is not necessary;in this case, preoperative measurementof creatinine is recommended (due tothe risk of over-dosage in renal failurepatients) [18].
Patientswith preoperatively increasedcardiac integrity markers (e. g. troponin;N-terminal pro B-type natriuretic pep-tide, NT-proBNP) have more periop-erative cardiovascular complications[19–21]. Whether routine preopera-tive measurement of cardiac integritymarkers in cardiovascular risk patientscan contribute to reducing perioperativemorbidity has not yet been clarified andthis is thus not recommended. Preop-erative measurement with monitoring48–72 h postoperatively can, however,be considered for patients with a highcardiac risk (MET < 4, RCRI > 1 forvascular or > 2 for non-vascular surgery;[8]).
A.3.2 12-channel ECGA preoperative 12-channel ECG aims toidentify heart diseases which would in-fluence the anesthesia. The following rec-ommendations appear reasonable for es-tablishing the indication (. Fig. 1):a) In patients with unremarkable medical
history and no cardiac symptoms,findings relevant to the anesthesia arerare. In these patients a preoperative
S30 Der Anaesthesist · Suppl 1 · 2019
Known/stable disease• e.g., COPD, asthma
No Yes
Suspicious medical historyor
pulmonary symptoms
New-onset pulmonary symptoms
• e.g., dyspnea• e.g., coughing, wheezing,
sputum• e.g., hypoxemia (pulse
oximetry)
Suspected finding with relevance for
surgery/anesthesia
• e.g., goiter• e.g., thorax deformities,
etc.Major
abdominal surgery
Chest x-ray (p.-a.)
Lung function tests* (optionally)
No
No further testsChest x-ray (p.-a.)
*e.g., pulse oximetry, spirometry, blood gas analysis
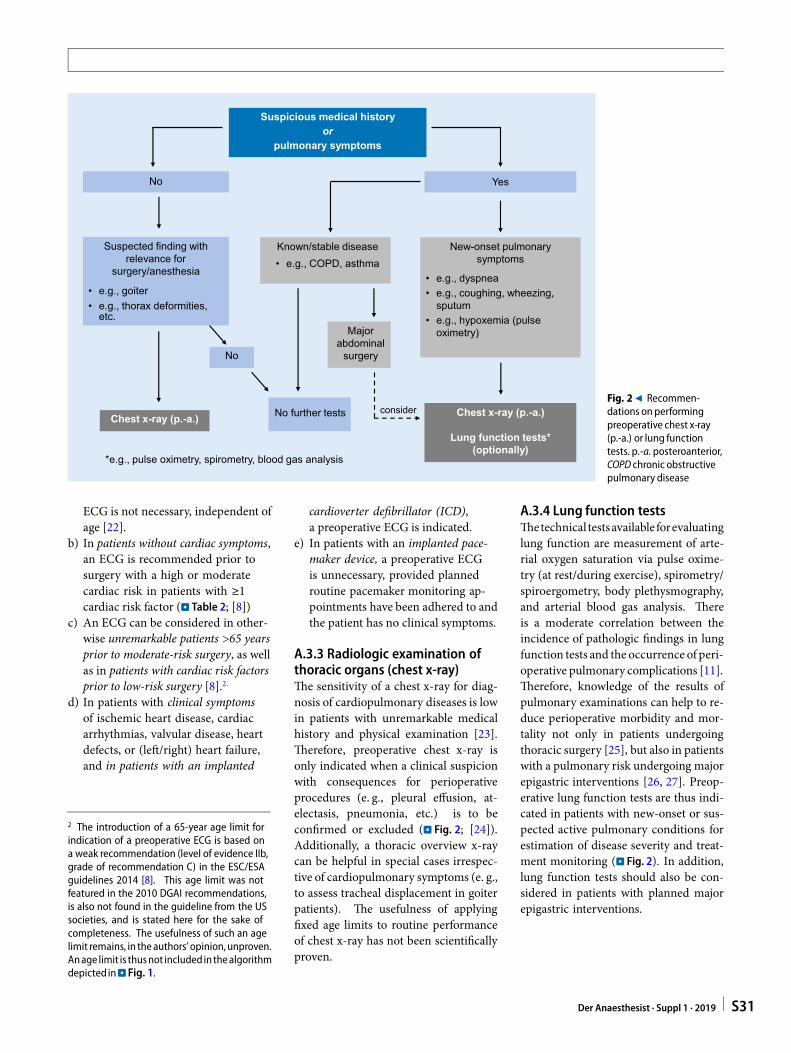
considerFig. 29 Recommen-dations on performingpreoperative chest x-ray(p.-a.) or lung functiontests. p.-a. posteroanterior,COPD chronic obstructivepulmonary disease
ECG is not necessary, independent ofage [22].
b) In patients without cardiac symptoms,an ECG is recommended prior tosurgery with a high or moderatecardiac risk in patients with ≥1cardiac risk factor (. Table 2; [8])
c) An ECG can be considered in other-wise unremarkable patients >65 yearsprior to moderate-risk surgery, as wellas in patients with cardiac risk factorsprior to low-risk surgery [8].2.
d) In patients with clinical symptomsof ischemic heart disease, cardiacarrhythmias, valvular disease, heartdefects, or (left/right) heart failure,and in patients with an implanted
2 The introduction of a 65-year age limit forindication of a preoperative ECG is based ona weak recommendation (level of evidence IIb,grade of recommendation C) in the ESC/ESAguidelines 2014 [8]. This age limit was notfeatured in the 2010 DGAI recommendations,is also not found in the guideline from the USsocieties, and is stated here for the sake ofcompleteness. The usefulness of such an agelimit remains, in theauthors’ opinion,unproven.Anage limit is thusnot included in thealgorithmdepicted in.Fig. 1.
cardioverter defibrillator (ICD),a preoperative ECG is indicated.
e) In patients with an implanted pace-maker device, a preoperative ECGis unnecessary, provided plannedroutine pacemaker monitoring ap-pointments have been adhered to andthe patient has no clinical symptoms.
A.3.3 Radiologic examination ofthoracic organs (chest x-ray)The sensitivity of a chest x-ray for diag-nosis of cardiopulmonary diseases is lowin patients with unremarkable medicalhistory and physical examination [23].Therefore, preoperative chest x-ray isonly indicated when a clinical suspicionwith consequences for perioperativeprocedures (e. g., pleural effusion, at-electasis, pneumonia, etc.) is to beconfirmed or excluded (. Fig. 2; [24]).Additionally, a thoracic overview x-raycan be helpful in special cases irrespec-tive of cardiopulmonary symptoms (e. g.,to assess tracheal displacement in goiterpatients). The usefulness of applyingfixed age limits to routine performanceof chest x-ray has not been scientificallyproven.
A.3.4 Lung function testsThetechnical testsavailable forevaluatinglung function are measurement of arte-rial oxygen saturation via pulse oxime-try (at rest/during exercise), spirometry/spiroergometry, body plethysmography,and arterial blood gas analysis. Thereis a moderate correlation between theincidence of pathologic findings in lungfunction tests and the occurrence of peri-operative pulmonary complications [11].Therefore, knowledge of the results ofpulmonary examinations can help to re-duce perioperative morbidity and mor-tality not only in patients undergoingthoracic surgery [25], but also in patientswith a pulmonary risk undergoing majorepigastric interventions [26, 27]. Preop-erative lung function tests are thus indi-cated in patients with new-onset or sus-pected active pulmonary conditions forestimation of disease severity and treat-ment monitoring (. Fig. 2). In addition,lung function tests should also be con-sidered in patients with planned majorepigastric interventions.
Der Anaesthesist · Suppl 1 · 2019 S31
Leitlinien und Empfehlungen
With successful intervention
No Yes (TIA, stroke) <6 months
Medical history suspicious fordiseases of the cervical vessels
No sonography
Sonography
Patents prior to major arterial vascular surgery, surgery in the head and neck region, and surgery
in a sitting position
Following TIA/stroke, elective interventions should only be performed after an interval of 6 months
With intervention but returning symptoms
Without intervention
May be appropriate in some cases
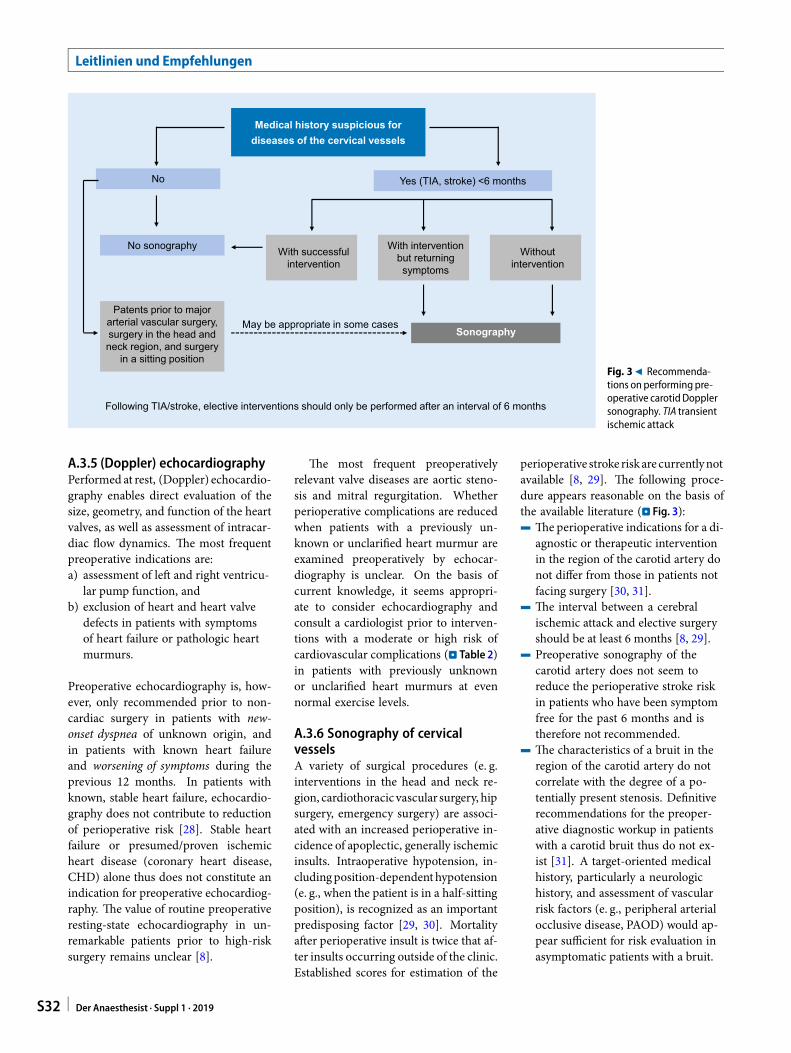
Fig. 39 Recommenda-tions on performing pre-operative carotidDopplersonography. TIA transientischemic attack
A.3.5 (Doppler) echocardiographyPerformed at rest, (Doppler) echocardio-graphy enables direct evaluation of thesize, geometry, and function of the heartvalves, as well as assessment of intracar-diac flow dynamics. The most frequentpreoperative indications are:a) assessment of left and right ventricu-
lar pump function, andb) exclusion of heart and heart valve
defects in patients with symptomsof heart failure or pathologic heartmurmurs.
Preoperative echocardiography is, how-ever, only recommended prior to non-cardiac surgery in patients with new-onset dyspnea of unknown origin, andin patients with known heart failureand worsening of symptoms during theprevious 12 months. In patients withknown, stable heart failure, echocardio-graphy does not contribute to reductionof perioperative risk [28]. Stable heartfailure or presumed/proven ischemicheart disease (coronary heart disease,CHD) alone thus does not constitute anindication for preoperative echocardiog-raphy. The value of routine preoperativeresting-state echocardiography in un-remarkable patients prior to high-risksurgery remains unclear [8].
The most frequent preoperativelyrelevant valve diseases are aortic steno-sis and mitral regurgitation. Whetherperioperative complications are reducedwhen patients with a previously un-known or unclarified heart murmur areexamined preoperatively by echocar-diography is unclear. On the basis ofcurrent knowledge, it seems appropri-ate to consider echocardiography andconsult a cardiologist prior to interven-tions with a moderate or high risk ofcardiovascular complications (. Table 2)in patients with previously unknownor unclarified heart murmurs at evennormal exercise levels.
A.3.6 Sonography of cervicalvesselsA variety of surgical procedures (e. g.interventions in the head and neck re-gion, cardiothoracic vascular surgery, hipsurgery, emergency surgery) are associ-ated with an increased perioperative in-cidence of apoplectic, generally ischemicinsults. Intraoperative hypotension, in-cludingposition-dependenthypotension(e. g., when the patient is in a half-sittingposition), is recognized as an importantpredisposing factor [29, 30]. Mortalityafter perioperative insult is twice that af-ter insults occurring outside of the clinic.Established scores for estimation of the
perioperative stroke riskare currentlynotavailable [8, 29]. The following proce-dure appears reasonable on the basis ofthe available literature (. Fig. 3):4 Theperioperative indications for a di-
agnostic or therapeutic interventionin the region of the carotid artery donot differ from those in patients notfacing surgery [30, 31].
4 The interval between a cerebralischemic attack and elective surgeryshould be at least 6 months [8, 29].
4 Preoperative sonography of thecarotid artery does not seem toreduce the perioperative stroke riskin patients who have been symptomfree for the past 6 months and istherefore not recommended.
4 The characteristics of a bruit in theregion of the carotid artery do notcorrelate with the degree of a po-tentially present stenosis. Definitiverecommendations for the preoper-ative diagnostic workup in patientswith a carotid bruit thus do not ex-ist [31]. A target-oriented medicalhistory, particularly a neurologichistory, and assessment of vascularrisk factors (e. g., peripheral arterialocclusive disease, PAOD) would ap-pear sufficient for risk evaluation inasymptomatic patients with a bruit.
S32 Der Anaesthesist · Suppl 1 · 2019

4 Patients who have experiencedsymptoms indicating carotid arterystenosis within the past 6 monthsshould undergo preoperative diag-nostic tests (generally sonography)and, if necessary, treatment [8, 32].
Previously symptomatic patients as wellasthosewithpriorsurgical/interventionaltreatments generally receive dual an-tiplatelet therapy, normally for a limitedduration. Provided justifiable in termsof the bleeding risk, these prophylactictreatments should not be interruptedperioperatively. In this case, patientmanagement—including the indicationto delay surgery—follows the treatmentconcepts for cardiac patients on dualantiplatelet therapy (see chapter C.6)[29, 31].
B Further cardiac testing
In patients with known or presumedpre-existent cardiovascular disease, preoper-ative cardiac differential diagnostic testsmay be necessary. However, due to theoften unclear benefit of preoperative car-diologic or cardiosurgical interventionsin terms of perioperative morbidity andmortality, strict criteria shouldbe appliedwhen establishing the indication for suchtests. Rational evaluation of the periop-erative cardiovascular risk as well as thedecision for or against extended diag-nostic testing is based upon the factorsdescribed in section A.2.1.
In patients with an active cardiac con-dition (e. g. ST elevation myocardial in-farction, STEMI), the surgery—with theexception of emergencies—must be de-layed, and the cardiac situation clarifiedand treated preoperatively [7]. This is,in principle, also valid for patients withnon-STEMI (NSTEMI); however, in thiscase the urgency of the surgery mustbe weighed up against the urgency ofthe coronary diagnostics and treatment.Upon evidence of relevantmyocardial is-chemia and significant clinical symptoms(Canadian Cardiovascular Society, CCS,grade III–IV), diagnostic invasive coro-nary angiography should be performedif drug-based treatment of myocardialischemia is unsuccessful.
Before elective high-risk surgery, pa-tients with known CHD or a high is-chemia risk shouldbeevaluatedbyamul-tidisciplinary treatment team comprisedof a surgeon, an anesthetist, and cardiol-ogists [8]. The extent of the cardiac riskcan contribute to determining the typeof intervention.
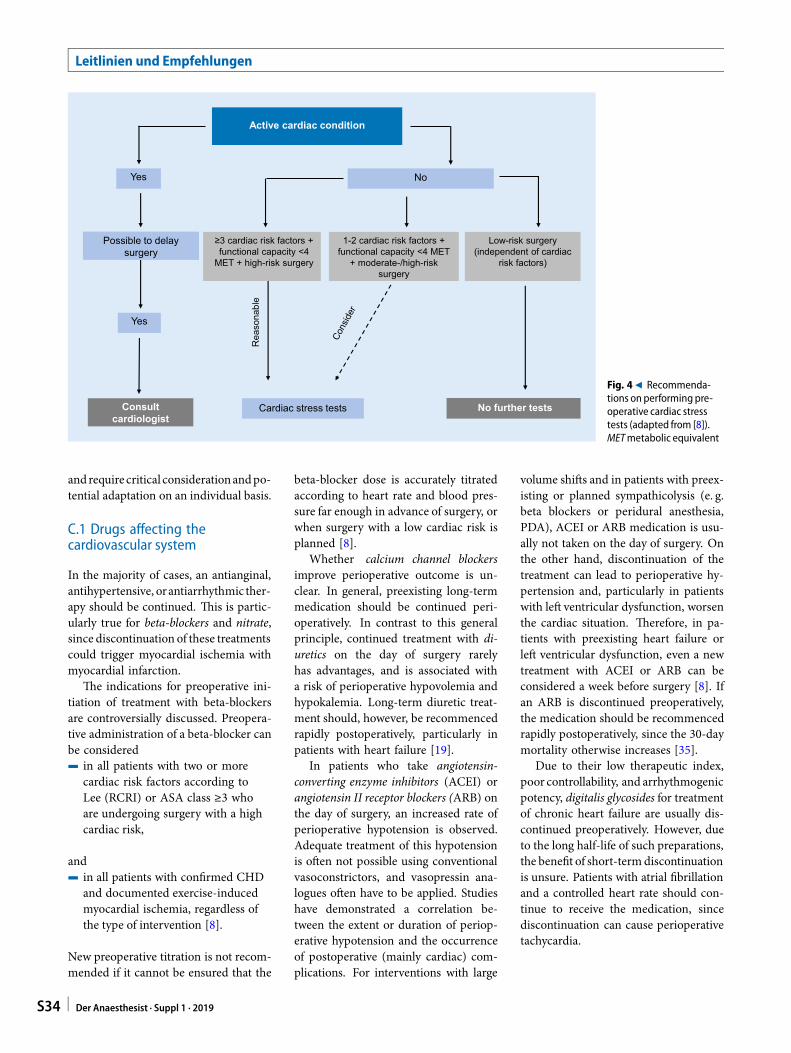
On the basis of current understand-ing, performance of noninvasive cardiacstress tests3 would only seem appropriate(. Fig. 4)4 in patients with ≥3 clinical risk factors
and impaired (<4 MET) or unknownfunctional capacity prior to high-risksurgery [8]
and can be considered4 in patients with 1–2 clinical risk
factors and impaired (<4 MET) orunknown functional capacity priorto surgery with a moderate or highcardiac risk [8]. 4.
There is currently no indication for fur-ther cardiac testing4 in patients facing surgery with a low
cardiac risk (. Table 2), independent
3 The type and extent of diagnostic testing isdeterminedby the consultant cardiologist. Themethod currently usedmost often for ischemiadiagnosis isergometry (exerciseECG).Ergometryenables evaluationof functional capacity, bloodpressure, and frequency response, as wellas detection of typical ischemic ST segmentchanges. A capacity of 100W correspondsto about 4 MET (. Table 5). The diagnosticvalue of ergometry is limited when, due toinsufficient physical fitness or comorbidities(e. g., arthrosis; PAOD; chronic obstructivepulmonary disease, COPD), no maximumheart rate is reached. Therefore, dobutaminestress echocardiography (DSE) and myocardialscintigraphy are recommended alternatives,particularly in older patients with limitedphysical capacity. Myocardial scintigraphy iswell suitedforpreoperativepredictionofcardiaccomplications, although its specificity is low.All things considered, DSE is currently viewedas the best diagnostic method for predictingperioperative cardiac events. Ultimately, theselection of the method has to be basedon availability and investigator-dependentexperiences at the particular location. In thecase of positive stress test findings, coronaryangiography isgenerally thenperformed.4 Provided it is expected that the resultsof corresponding investigations would alsoinfluence furtherperioperativemanagement.
of the presence of cardiac risk factors[8]
The indication for invasive coronary di-agnostic testing (cardiac catheterization)for estimationof perioperative risk is rareprior to noncardiac surgery. In general,the indication corresponds to that forcoronary angiography or percutaneouscoronary intervention (PCI) irrespectiveof the scheduled surgery.
Preoperative coronary angiography iscurrently only recommended in patientswith confirmedmyocardial ischemia andin patients with chest pain refractory topharmacologic treatment, provided theintervention can be postponed [8].
However, in an as-yet unconfirmedstudy, routine coronary angiographyand potential subsequent revascular-ization in patients with two or morecardiac risk factors prior to major ar-terial vascular interventions improvedperioperative outcome [33]. In anotherinvestigation, clinically stable patients(normal ECG, normal echo, no signsof CHD) were examined routinely withcoronary angiography prior to carotidthromboendarterectomy (TEA) and sig-nificant coronary stenosis was found in31% [34]. Subsequent revascularizationreduced the incidence of severe cardiaccomplications significantly, from 4.2 to0%. It is therefore possible that patientsfacing carotid TEA and patients witha high cardiac risk facing major vascularsurgerywouldbenefit fromprior invasivediagnostic and therapeutic procedures[8]. There are currently no studies avail-able on the indications for and valueof cardiac magnetic resonance imaging(MRI) and cardiac computed tomogra-phy (CT) for preoperative evaluation.
C Preoperative management oflong-termmedication
Theassessment of the individual patient’slong-term medication is an importantpart of the preoperative evaluation. Thequestion of whether it is medically jus-tifiable to continue a preoperative drugperioperatively or to initiate a new drug-based treatmentprior to surgeryhasbeeninadequately investigated. The followingrecommendations are thus only a guide
Der Anaesthesist · Suppl 1 · 2019 S33
Leitlinien und Empfehlungen
≥3 cardiac risk factors + functional capacity <4
MET + high-risk surgery
Yes No
Active cardiac condition
1-2 cardiac risk factors + functional capacity <4 MET
+ moderate-/high-risk surgery
Possible to delay surgery
No further tests
Yes
Cardiac stress testsConsult cardiologist
Rea
sona
ble
Low-risk surgery (independent of cardiac
risk factors)
Fig. 49 Recommenda-tions on performing pre-operative cardiac stresstests (adapted from [8]).METmetabolic equivalent
andrequire critical considerationandpo-tential adaptation on an individual basis.
C.1 Drugs affecting thecardiovascular system
In the majority of cases, an antianginal,antihypertensive, orantiarrhythmic ther-apy should be continued. This is partic-ularly true for beta-blockers and nitrate,since discontinuation of these treatmentscould trigger myocardial ischemia withmyocardial infarction.
The indications for preoperative ini-tiation of treatment with beta-blockersare controversially discussed. Preopera-tive administration of a beta-blocker canbe considered4 in all patients with two or more
cardiac risk factors according toLee (RCRI) or ASA class ≥3 whoare undergoing surgery with a highcardiac risk,
and4 in all patients with confirmed CHD
and documented exercise-inducedmyocardial ischemia, regardless ofthe type of intervention [8].
New preoperative titration is not recom-mended if it cannot be ensured that the
beta-blocker dose is accurately titratedaccording to heart rate and blood pres-sure far enough in advance of surgery, orwhen surgery with a low cardiac risk isplanned [8].
Whether calcium channel blockersimprove perioperative outcome is un-clear. In general, preexisting long-termmedication should be continued peri-operatively. In contrast to this generalprinciple, continued treatment with di-uretics on the day of surgery rarelyhas advantages, and is associated witha risk of perioperative hypovolemia andhypokalemia. Long-term diuretic treat-ment should, however, be recommencedrapidly postoperatively, particularly inpatients with heart failure [19].
In patients who take angiotensin-converting enzyme inhibitors (ACEI) orangiotensin II receptor blockers (ARB) onthe day of surgery, an increased rate ofperioperative hypotension is observed.Adequate treatment of this hypotensionis often not possible using conventionalvasoconstrictors, and vasopressin ana-logues often have to be applied. Studieshave demonstrated a correlation be-tween the extent or duration of periop-erative hypotension and the occurrenceof postoperative (mainly cardiac) com-plications. For interventions with large
volume shifts and in patients with preex-isting or planned sympathicolysis (e. g.beta blockers or peridural anesthesia,PDA), ACEI or ARB medication is usu-ally not taken on the day of surgery. Onthe other hand, discontinuation of thetreatment can lead to perioperative hy-pertension and, particularly in patientswith left ventricular dysfunction, worsenthe cardiac situation. Therefore, in pa-tients with preexisting heart failure orleft ventricular dysfunction, even a newtreatment with ACEI or ARB can beconsidered a week before surgery [8]. Ifan ARB is discontinued preoperatively,the medication should be recommencedrapidly postoperatively, since the 30-daymortality otherwise increases [35].
Due to their low therapeutic index,poor controllability, and arrhythmogenicpotency, digitalis glycosides for treatmentof chronic heart failure are usually dis-continued preoperatively. However, dueto the long half-life of such preparations,the benefit of short-termdiscontinuationis unsure. Patients with atrial fibrillationand a controlled heart rate should con-tinue to receive the medication, sincediscontinuation can cause perioperativetachycardia.
S34 Der Anaesthesist · Suppl 1 · 2019

C.2 Antidiabetic drugs
Primarily oral antidiabetic drugs areused to treat type 2 diabetes mellitus.These include sulfonylureas (e. g., gliben-clamide), biguanide (metformin), andglinides (e. g. repaglinide), as well asalpha-glucosidase inhibitors (e. g., acar-bose), glitazones (e. g., pioglitazon), andgliptins (e. g., sitagliptin). In animalexperiments, sulfonylureas prevent is-chemia- and volatile anesthesia-inducedpreconditioning, particularly myocar-dial preconditioning, and thus enlargethe necrotic area of the myocardiumafter ischemia. Whether similar effectsalso occur in humans is unclear; it istherefore also currently unclear whethersulfonylureas should be discontinuedpreoperatively. Glitazones increase thesensitivity of various tissues to insulinand are used increasingly for glucosemanagement in patients with type 2 di-abetes mellitus. There are case studies inthe literature describing acute heart fail-ure in connection with glitazones. Therelevance of these findings for perioper-ative management is unclear. The actionof gliptins corresponds to the action ofthe endogenous hormone incretin, andlowers blood glucose via increased in-sulin release from β cells and increasedglucagon synthesis in pancreatic α cells.Hypoglycemia generally does not occurwith gliptin monotherapy. In rare cases,metformin accumulation (e. g., in pa-tients with renal failure) can lead to life-threatening lactic acidosis, and a recom-mendation for its discontinuation 48 hbefore the intervention can be found inthe prescribing information. However,risk of lactic acidosis during the directperioperative period appears to be verylow [36]. Continuation of metforminmedication up until the evening beforesurgery can thus be justified on the basisof an individual risk-benefit assessment.The British National Health Service(NHS) and the Society of AmbulatoryAnaesthesia (SAMBA) even recommendcontinuation of metformin treatment inpatients with healthy kidneys, in partbecause of results indicating a better out-come with this scheme [37]. However,if application of an intravenous contrastagent is planned, metformin treatment
should be paused 24–48 h in advance ofthe procedure [38]. Overall, the decisionon whether to continue or discontinueoral antidiabetic drugs should be basedprimarily on blood glucose managementand less on potential adverse effects.
Insulins are the standard treatmentfor type 1 diabetes as well as for ad-vanced-stage type 2 diabetes refractoryto oral antidiabetic drugs. Conventionalinsulin therapy is distinguished from in-tensive insulin therapy (with a combina-tion of a long-acting basal insulin doseand a short-acting bolus dose at meal-times) and insulin pump therapy. Pre-operative fasting and the postaggressionmetabolism resulting from the particu-lar type and extent of surgery combineto increase the risk or hypoglycemia ifinsulin therapy is continued. For shortinterventions in patients with preoper-ative intensive insulin therapy, only thebasal insulin should be administered onthemorning of surgery; the bolus shouldbe omitted. In contrast, in patients withconventional insulin therapy undergoinga short surgical intervention, only 50%of the normal insulin dose should beapplied in a long-acting form. Postop-erative insulin therapy can be continuedas normal. Tight monitoring and cor-rection of blood sugar is indispensableduring the entire perioperative period.
C.3 HMG-CoA reductase inhibitors(statins)
Lipid-lowering HMG-CoA reductaseinhibitors (statins) stabilize vulnerableplaques, have anti-inflammatory effects,inhibit thrombosis formation, and canreduce the incidence of perioperativeischemia, (re)infarction, and mortal-ity in patients with coronary risk [39,40]. Long-term statin therapy shouldtherefore not be interrupted periop-eratively. In vascular surgery patientswithout previous statin medication, ac-tive commencement of prophylaxis atleast 2 weeks prior to surgery in recom-mended [8].
C.4 Vitamin K antagonists
Anticoagulation therapy with vitamin Kantagonists (usually phenprocoumon) is
obligatory in patients with mechanicalheart valves and is generally also receivedby patients with biological heart valvesduring the first 3 months after implan-tation. Depending on the type of valueand its localization, an international nor-malized ratio (INR) of 2.0–3.0 should bestrived for. Other important clinical in-dications for vitamin K antagonists arepostthrombotic treatment and atrial fib-rillation.
The risk of thromboembolism re-sulting from perioperative interruptionof anticoagulants should be weighedagainst the perioperative bleeding riskon an individual basis. In instances ofdiscontinuation, treatment is stopped3–5 days (preferably 5–8 days for phen-procoumon) preoperatively, with dailyINR monitoring (target for surgery:<1.5). Preoperative bridging withLMWH, which was long recommended,did not reduce the incidence of arterialthromboembolisms in atrial fibrillationpatients, but did increase the risk ofmajor bleeding (from 1.3 to 3.2%) [41].
In agreement with this, a prospectiveregistry study also found an increasedbleeding rate, a worse cardiac outcome,and increased mortality in patients withbridging [42]. The indication for bridg-ingwithLMWHafterdiscontinuingvita-minKantagonists is thus tobeestablishedincreasinglycritically. Sincepatientswithmechanical heart valves were excludedfrom the study by Douketis et al. [41],no definitive conclusions can currentlybe drawn for this patient collective. Inpatientswith ahigh thromboembolic risk(CHA2DS2-VASc score of 4 or more, me-chanical valves, freshly implantedbiolog-ical heart valves,mitral heart valve recon-struction <3 months previously, throm-bophilia), bridging with LMWHor UFHis generally still considered to be indi-cated. The last dose of LMWH should beadministered at least 12 h before surgery(a longer interval is necessary in patientswith impaired renal function). The deci-sion forUFHorLMWHforperioperativeprophylaxisofvenous thromboembolismis not affected by these considerations[18].
Der Anaesthesist · Suppl 1 · 2019 S35
Leitlinien und Empfehlungen
Table 9 Time required for NOAC elimination
Preparation Target factor Elimination time
Rivaroxaban Xa 24–36 h
Apixaban Xa 24–36 h
Edoxaban Xa 24–36 h
Dabigatrana IIa 24–72 hb
NOAC novel oral anticoagulantaInhibitor: idarucizumabbLonger in patients with renal failure
C.5 Direct oral anticoagulants(DOAC)
The acronyms NOAC (novel oral an-ticoagulants) and DOAC (directly act-ing oral anticoagulants) are used syn-onymously for a group of orally/enterallyadministered factor IIa or factor Xa in-hibitors which have been available for5–10years (NOAK“neueoraleAntikoag-ulanzien” is also used in theGerman-lan-guage literature). Thecurrent indicationsare prophylaxis of stroke and systemicembolisms in non-valvular atrial fibril-lation, treatment and secondary prophy-laxis of deep vein thrombosis and lungembolisms, and thromboembolic pro-phylaxis in patients with elective hip andknee joint surgery.
NOACs (half-life 9–14 h) are elimi-nated via a number of routes (with theexception of dabigatran, which is elim-inated primarily via the kidneys). Inthe context of elective surgery in adultswith a moderate bleeding risk, the min-imum elimination time intervals statedin the following section (correspondingto at least 2–3 half-lives [8]) should beobserved before surgery after discontin-uation of the corresponding substance(. Table 9; [43, 44]).
The time interval to be waited beforesurgery depends on renal function. Inclinical routine, 48 h represents a safeinterval, except for the situation of dabi-gatran application in patients with renalfailure. In emergency situations, applica-tionof25–50IU/kgbodymassprothrom-bin complex concentrate (PCC) can beconsidered. Idarucizumab is an availabledabigatran antidote, whereas an antidoteto factor Xa inhibitors is currently underclinical investigation.
Whether a NOAC should remain un-changed preoperatively, be discontinued
long enough in advance of surgery (in de-pendenceof theeliminationtime; prema-ture discontinuation must be avoided),or be exchanged for heparin depends onthe type of surgery and the associatedbleeding risk, as well as the original in-dication for anticoagulant therapy. Thedecision should be made in close collab-oration between the involved specialistdisciplines (usually surgery, anesthesia,and internal medicine).
Postoperatively, anticoagulation ther-apy should be recommenced as soon aspossible, although the current bleedingrisk must be taken into consideration. Inpatients with atrial fibrillation or throm-bosis/embolism, it may be necessary tobridge several postoperative days withheparin (LMWH or NMH) or fonda-parinux, until a switch back to NOACis possible. In contrast to the procedurewith vitamin K antagonists, the switchback to NOAC is made without overlap-ping, i. e., the first tablet is taken 12 hafter LMWH or fondaparinux.
Specific requirements covering thehandling of NOACs (and platelet aggre-gation inhibitors) exist for spinal anes-thesia, and these should be observed[45].
C.6 Platelet aggregation inhibitors
Patients with CHD generally receivelong-term medication with aspirin andoften also with a P2Y12 inhibitor (e. g.,clopidogrel). For patients after surgicalor interventional coronary revascular-ization (e. g., stenting), but also forpatients with acute coronary syndrome,the benefit of temporary (see below) dualantiplatelet therapy has been proven. Inthese high-risk patients, the periopera-tive bleeding risk is outweighed by therisk of myocardial infarction as a con-
sequence of medication discontinuation(reviewed in [46]).
Therefore, on the basis of current un-derstanding, only before major surgeryassociated with a high bleeding riskshould P2Y12 inhibitors be stopped5 (clopidogrel/ticagrelor) or 7 days (pra-sugrel) preoperatively. In patients witha high risk of an ischemic myocar-dial event after stent implantation, thisdecision must be made in consulta-tion with the treating cardiologist onan individual basis. Discontinuationis mandatory prior to interventions insealed cavities (posterior chamber ofthe eye, intraspinal and intracerebralinterventions) as well as before regionalspinal anesthesia. Perioperative man-agement of aspirin therapy also proceedson an individual basis. In patients witha high coronary risk (recurrent anginapectoris; status after acute coronarysyndrome; status after coronary inter-vention with a bare metal stent, BMS, ora drug eluting stent, DES), aspirin med-ication (e. g., 100mg/day) should onlybe interrupted perioperatively in thepresence of absolute contraindications(e. g., neurosurgical intervention; reviewin [46]).
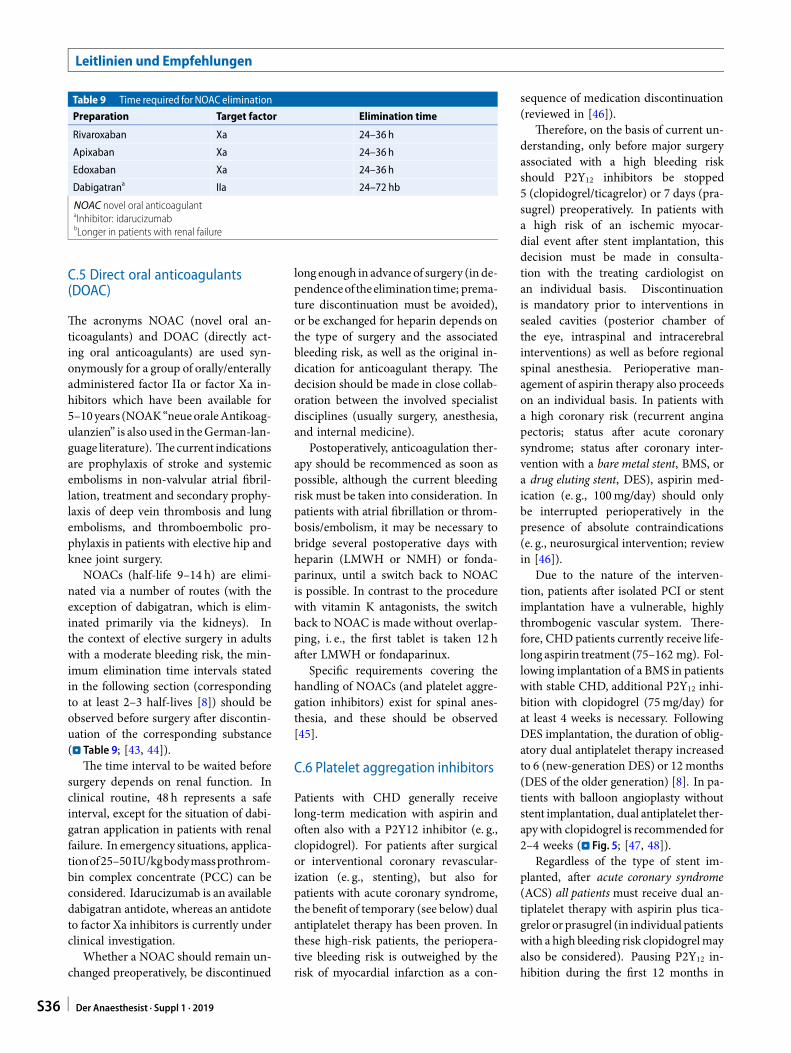
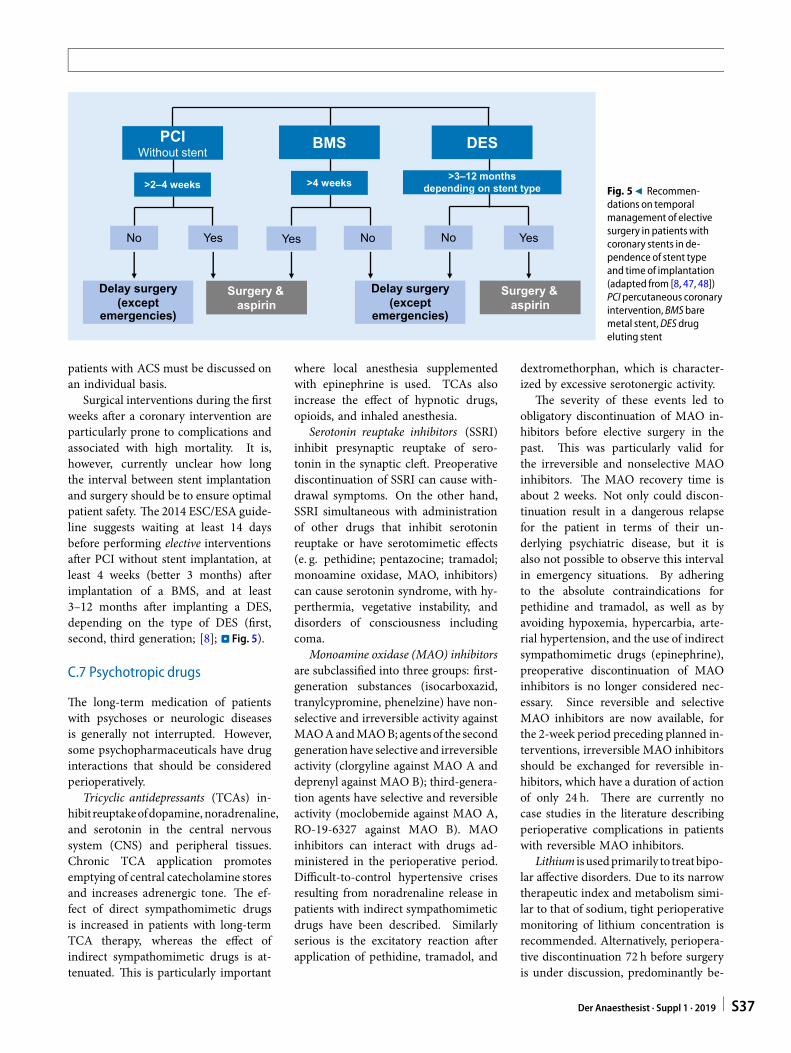
Due to the nature of the interven-tion, patients after isolated PCI or stentimplantation have a vulnerable, highlythrombogenic vascular system. There-fore, CHD patients currently receive life-long aspirin treatment (75–162 mg). Fol-lowing implantation of a BMS in patientswith stable CHD, additional P2Y12 inhi-bition with clopidogrel (75mg/day) forat least 4 weeks is necessary. FollowingDES implantation, the duration of oblig-atory dual antiplatelet therapy increasedto 6 (new-generation DES) or 12 months(DES of the older generation) [8]. In pa-tients with balloon angioplasty withoutstent implantation, dual antiplatelet ther-apywith clopidogrel is recommended for2–4 weeks (. Fig. 5; [47, 48]).
Regardless of the type of stent im-planted, after acute coronary syndrome(ACS) all patientsmust receive dual an-tiplatelet therapy with aspirin plus tica-grelor or prasugrel (in individual patientswith a high bleeding risk clopidogrelmayalso be considered). Pausing P2Y12 in-hibition during the first 12 months in
S36 Der Anaesthesist · Suppl 1 · 2019
No
Surgery & aspirin
PCIWithout stent
Yes
>3–12 monthsdepending on stent type>4 weeks>2–4 weeks
Delay surgery (except
emergencies)
Yes No
Delay surgery (except
emergencies)
No
Surgery & aspirin
Yes
BMS DES
Fig. 59 Recommen-dations on temporalmanagement of electivesurgery in patients withcoronary stents in de-pendence of stent typeand time of implantation(adapted from [8, 47, 48])PCI percutaneous coronaryintervention, BMSbaremetal stent,DESdrugeluting stent
patients with ACS must be discussed onan individual basis.
Surgical interventions during the firstweeks after a coronary intervention areparticularly prone to complications andassociated with high mortality. It is,however, currently unclear how longthe interval between stent implantationand surgery should be to ensure optimalpatient safety. The 2014 ESC/ESA guide-line suggests waiting at least 14 daysbefore performing elective interventionsafter PCI without stent implantation, atleast 4 weeks (better 3 months) afterimplantation of a BMS, and at least3–12 months after implanting a DES,depending on the type of DES (first,second, third generation; [8]; . Fig. 5).
C.7 Psychotropic drugs
The long-term medication of patientswith psychoses or neurologic diseasesis generally not interrupted. However,some psychopharmaceuticals have druginteractions that should be consideredperioperatively.
Tricyclic antidepressants (TCAs) in-hibitreuptakeofdopamine, noradrenaline,and serotonin in the central nervoussystem (CNS) and peripheral tissues.Chronic TCA application promotesemptying of central catecholamine storesand increases adrenergic tone. The ef-fect of direct sympathomimetic drugsis increased in patients with long-termTCA therapy, whereas the effect ofindirect sympathomimetic drugs is at-tenuated. This is particularly important
where local anesthesia supplementedwith epinephrine is used. TCAs alsoincrease the effect of hypnotic drugs,opioids, and inhaled anesthesia.
Serotonin reuptake inhibitors (SSRI)inhibit presynaptic reuptake of sero-tonin in the synaptic cleft. Preoperativediscontinuation of SSRI can cause with-drawal symptoms. On the other hand,SSRI simultaneous with administrationof other drugs that inhibit serotoninreuptake or have serotomimetic effects(e. g. pethidine; pentazocine; tramadol;monoamine oxidase, MAO, inhibitors)can cause serotonin syndrome, with hy-perthermia, vegetative instability, anddisorders of consciousness includingcoma.
Monoamine oxidase (MAO) inhibitorsare subclassified into three groups: first-generation substances (isocarboxazid,tranylcypromine, phenelzine) have non-selective and irreversible activity againstMAOAandMAOB; agents of the secondgeneration have selective and irreversibleactivity (clorgyline against MAO A anddeprenyl against MAO B); third-genera-tion agents have selective and reversibleactivity (moclobemide against MAO A,RO-19-6327 against MAO B). MAOinhibitors can interact with drugs ad-ministered in the perioperative period.Difficult-to-control hypertensive crisesresulting from noradrenaline release inpatients with indirect sympathomimeticdrugs have been described. Similarlyserious is the excitatory reaction afterapplication of pethidine, tramadol, and
dextromethorphan, which is character-ized by excessive serotonergic activity.
The severity of these events led toobligatory discontinuation of MAO in-hibitors before elective surgery in thepast. This was particularly valid forthe irreversible and nonselective MAOinhibitors. The MAO recovery time isabout 2 weeks. Not only could discon-tinuation result in a dangerous relapsefor the patient in terms of their un-derlying psychiatric disease, but it isalso not possible to observe this intervalin emergency situations. By adheringto the absolute contraindications forpethidine and tramadol, as well as byavoiding hypoxemia, hypercarbia, arte-rial hypertension, and the use of indirectsympathomimetic drugs (epinephrine),preoperative discontinuation of MAOinhibitors is no longer considered nec-essary. Since reversible and selectiveMAO inhibitors are now available, forthe 2-week period preceding planned in-terventions, irreversible MAO inhibitorsshould be exchanged for reversible in-hibitors, which have a duration of actionof only 24 h. There are currently nocase studies in the literature describingperioperative complications in patientswith reversible MAO inhibitors.
Lithium isusedprimarily to treatbipo-lar affective disorders. Due to its narrowtherapeutic index and metabolism simi-lar to that of sodium, tight perioperativemonitoring of lithium concentration isrecommended. Alternatively, periopera-tive discontinuation 72 h before surgeryis under discussion, predominantly be-
Der Anaesthesist · Suppl 1 · 2019 S37

Leitlinien und Empfehlungen
cause no withdrawal symptoms are tobe expected; however, the risk of intox-ication in the instance of perioperativehemodynamic instability or impaired re-nal function (lithium is excreted via thekidneys) is high. Treatment should berecommenced rapidly postoperatively ina stable electrolyte situation.
Neuroleptic agents are a highly het-erogeneous group of psychotropic drugswith sedative and antipsychotic prop-erties. They are mainly used to treatdelusions and hallucinations in patientswithschizophreniaandbipolardisorders.Owing to the risk of psychotic episodesreturning and on the basis of an in-creased rate of postoperative confusion,neuroleptic agents should be continuedperioperatively.
Antiepileptic drugs should be contin-ued perioperatively. The requirement foropioids and relaxants may be increasedin these patients.
Methylphenidate is an amphetaminederivative used to treat attention deficithyperactivity disorder (ADHD) andnarcolepsy. Methylphenidate can in-crease anesthetic requirements. Due toits short half-life (2–4 h in unretarded,up to 12 h in retarded tablet form),methylphenidate can be continued up topremedication.
C.8 Antiparkinsonmedication
The symptoms experienced by Parkinsondisease patients are caused by dopaminedeficit in the region of the substantianigra. Long-term therapy in Parkinsonpatients thus primarily comprises sub-stances which increase the concentra-tion or effect of dopamine in the brain,e. g. via exogenous supply of dopamine(L-DOPA) and dopamine agonists (e. g.bromocriptine), by slowing the degrada-tionofendogenousdopamineviaMAOBinhibitors (e. g. selegiline), or by in-creasing dopamine release via N-methylD-aspartate (NMDA) receptor antago-nists (e. g. amantadine). The effect ofL-DOPAmonotherapy is superior to thatof all other antiparkinson medications,and this is therefore the most commontreatment. The half-life of L-DOPA isshort and a 6–12-hour interruption oftherapy can cause severe muscle rigidity
or aParkinsoncrisiswith life-threateningsymptoms such as dysphagia and respi-ratory dysfunction. Therefore, oral med-ication with L-DOPA and also with allother antiparkinson medications shouldbecontinueduntil themorningofsurgeryand recommenced immediately postop-eratively. In cases where oral medica-tion is not possible postoperatively, thepossibility of preoperative conversion toa transdermallyabsorbabledopamineag-onist (e. g. rotigotine plaster) should bediscussed with a neurologist.
Dopamine antagonists (e. g. meto-clopramide) and medications associatedwith a risk of extrapyramidal symptoms(e. g. droperidolHT3 antagonists) shouldbe avoided. In the case of an akineticParkinson crisis titrated intravenous ap-plication of amantadine (e. g. 1–2-times200mg i. v. over 3 h is recommended).
C.9 Corticosteroids
Independent of dose (above or belowthe Cushing’s threshold) and methodof application (systemic or topical), pa-tients with long-term steroid medication(>5days) are at riskof inadequate cortisolproduction [49]. Case studies indicatea correlation between cortisol deficiencyand intraoperative hypotensionor shock,although this has not yet been unequiv-ocally proven [49, 50]. Therefore, ingeneral, patients should not interrupttheir long-term steroid medication inthe perioperative phase and take this asnormal on the morning of surgery.
It is unclear whether patients withlong-term steroid medication belowthe Cushing’s threshold benefit fromadditional perioperative steroid admin-istration [51]. Due to the individualand highly variable reactions to surgicaltrauma, as well as differing suppres-sion of endogenous cortisol synthesis byexogenous steroids, the following proce-dure can be considered on the basis ofexpert opinion:4 Minor surgery (e. g. endoscopic
surgery, herniotomy, thyroid glandremoval) → application of 25mghydrocortisone at the start of surgery.
4 Medium-sized surgery (e. g., ab-dominal surgery) → application of100mg hydrocortisone over 24 h,
recommencement of normal steroidmedication the next day.
4 Major surgery with a risk of postoper-ative systemic inflammatory responsesyndrome (SIRS) → application of100mg hydrocortisone over 24 h(e. g. 4mg/h) on the day of surgery,50mg over 24 h the day after surgery,and 25mg hydrocortisone on the sec-ond postoperative day (also possibleorally).
D Conclusion
The concepts presented herein for pre-operative evaluation of adult patientsprior to elective noncardiothoracicsurgery represent multidisciplinary rec-ommendations that enable structuredand concerted patient management, andshould improve the quality of treatment.Through transparent and binding agree-ments, these recommendations aim toensure highly patient-oriented clinicalmanagement with avoidance of unnec-essary preoperative tests, thus reducingpreoperative examination times and, ul-timately, costs. A corollary of this is thatfor some individual patients, individualconcepts have to be generated.
Thepresented joint recommendationsfrom the DGAI, DGCH, and DGIM re-flect the current state of knowledge butalso expert opinions, since scientific ev-idence does not exist for every scenario.Therefore, these guidelines will be reg-ularly reviewed and updated as soon asnew findings become available.
Corresponding address
Prof. Dr. B. ZwisslerDepartment of Anesthesiology, UniversityHospital, LMUMunichMarchioninistr. 15, 81377Munich, [email protected]
Compliance with ethicalguidelines
Conflict of interest. G. Geldner, J. Karst, F.Wappler,B. Zwissler, P. Kalbe, U. Obertacke, andM. Pauschingerdeclare that theyhave no competing interests.W. Schwenk receives consulting fees fromBayer fora decision tool for perioperative use ofNOACs, butabstained fromvotingon the correspondingpassages.
S38 Der Anaesthesist · Suppl 1 · 2019

This article does not contain any studieswith humanparticipants or animals performedby anyof the au-thors
References
1. Deutsche Gesellschaft für Anästhesiologie undIntensivmedizin, - (2010) Preoperative evaluationof adult patients prior to elective, non-cardiacsurgery: joint recommendations of GermanSociety of Anesthesiology and Intensive CareMedicine, German Society of Surgery andGermanSociety of Internal Medicine. Anaesthesist59(11):1041–1050
2. BöhmerABetal (2014)Preoperativeriskevaluationof adult patients prior to elective non-cardiacsurgery: follow-upsurveyoftherecommendationspublished in2010. Anaesthesist63(3):198–208
3. BöhmerABetal (2012)Preoperativeriskevaluationof adult patients for elective, noncardiac surgicalinterventions. Results of an on-line survey on thestatus inGermany. Anaesthesist61(5):407–419
4. Wijeysundera DN et al (2009) A population-based study of anesthesia consultation beforemajor noncardiac surgery. Arch Intern Med169(6):595–602
5. Ferschl MB et al (2005) Preoperative clinic visitsreduce operating room cancellations and delays.Anesthesiology103(4):855–859
6. WeimannAetal (2014)Clinicalnutritioninsurgery.Guidelines of the German Society for NutritionalMedicine. Chirurg85(4):320–326
7. Fleisher LA et al (2007) ACC/AHA 2007 Guidelineson perioperative cardiovascular evaluation andcare for noncardiac surgery: executive summary:a report of the American College of Cardiology/AmericanHeart Association Task Force onPracticeGuidelines. Circulation116(17):1971–1996
8. KristensenSDetal (2014)2014ESC/ESAGuidelineson non-cardiac surgery: cardiovascular assess-ment and management: The Joint Task Forceon non-cardiac surgery: cardiovascular assess-ment and management of the European Societyof Cardiology (ESC) and the European Societyof Anaesthesiology (ESA). Eur J Anaesthesiol31(10):517–573
9. Gupta PKet al (2011)Development and validationofa riskcalculator forpredictionofcardiac riskaftersurgery. Circulation124(4):381–387
10. Wiklund RA, Stein HD, Rosenbaum SH (2001)Activities of daily living and cardiovascularcomplications following elective, noncardiacsurgery. Yale JBiolMed74(2):75–87
11. Canet J et al (2010) Prediction of postoperativepulmonary complications in a population-basedsurgicalcohort. Anesthesiology113(6):1338–1350
12. Canet J et al (2015)Developmentandvalidationofa score topredict postoperative respiratory failurein a multicentre European cohort: a prospec-tive, observational study. Eur J Anaesthesiol32(7):458–470
13. Brueckmann B et al (2013) Development andvalidationofascoreforpredictionofpostoperativerespiratory complications. Anesthesiology118(6):1276–1285
14. Smetana GW, Macpherson DS (2003) The caseagainst routine preoperative laboratory testing.MedClinNorthAm87(1):7–40
15. Chee YL et al (2008)Guidelines on the assessmentof bleeding risk prior to surgery or invasiveprocedures. British Committee for Standards inHaematology. Br JHaematol140(5):496–504
16. Pfanner G et al (2007) Preoperative evaluation ofthe bleeding history. Recommendations of theworking group on perioperative coagulation oftheAustrianSociety forAnaesthesia,Resuscitationand IntensiveCare. Anaesthesist56(6):604–611
17. KernerW,Brückel J (2008)Definition,Klassifikationund Diagnostik des Diabetes mellitus. DiabetolStoffwechs3(Suppl2):131–133
18. S3-Leitlinie Prophylaxe der venösen Throm-boembolie (VTE). 2015: http://www.awmf.org/uploads/tx_szleitlinien/003-001l_S3_VTE-Prophylaxa:2015-12.pdf. Zugegriffen: 12.05.2017
19. Poldermans D et al (2009) Guidelines for pre-op-erative cardiac risk assessment and perioperativecardiac management in non-cardiac surgery. EurHeart J30(22):2769–2812
20. Choi JH et al (2010) Preoperative NT-proBNP andCRP predict perioperative major cardiovascularevents innon-cardiacsurgery. Heart96(1):56–62
21. Potgieter D et al (2015) N-terminal pro-B-typenatriuretic peptides’ prognostic utility is over-estimated in meta-analyses using study-specificoptimal diagnostic thresholds. Anesthesiology123(2):264–271
22. Liu LL, Dzankic S, Leung JM (2002) Preoper-ative electrocardiogram abnormalities do notpredict postoperative cardiac complications ingeriatric surgical patients. J Am Geriatr Soc50(7):1186–1191
23. FritschGetal (2012)Abnormalpre-operative tests,pathologic findings of medical history, and theirpredictive value for perioperative complications.ActaAnaesthesiolScand56(3):339–350
24. Feely MA et al (2013) Preoperative testing beforenoncardiac surgery: guidelines and recommenda-tions. AmFamPhysician87(6):414–418
25. ArozullahAM, CondeMV, Lawrence VA (2003) Pre-operative evaluation forpostoperativepulmonarycomplications.MedClinNorthAm87(1):153–173
26. Ohrlander T, Dencker M, Acosta S (2012) Preop-erative spirometry results as a determinant forlong-termmortality after EVAR for AAA. Eur J VascEndovascSurg43(1):43–47
27. Jeong O, Ryu SY, Park YK (2013) The value ofpreoperative lung spirometry test for predictingthe operative risk in patients undergoing gastriccancer surgery. JKoreanSurgSoc84(1):18–26
28. Halm EA et al (1996) Echocardiography forassessingcardiacriskinpatientshavingnoncardiacsurgery. Studyof Perioperative Ischemia ResearchGroup. Ann InternMed125(6):433–441
29. Jorgensen ME et al (2014) Time elapsed afterischemic stroke and risk of adverse cardiovasculareventsandmortalityfollowingelectivenoncardiacsurgery. JAMA312(3):269–277
30. Mashour GA, Woodrum DT, Avidan MS (2015)Neurological complications of surgery andanaesthesia. Br JAnaesth114(2):194–203
31. Mashour GA et al (2014) Perioperative care ofpatients at high risk for stroke during or afternon-cardiac, non-neurologic surgery: consensusstatement from the Society for Neuroscience inAnesthesiology and Critical Care. J NeurosurgAnesthesiol26(4):273–285
32. De Hert S et al (2011) Preoperative evaluation oftheadultpatientundergoingnon-cardiac surgery:guidelinesfromtheEuropeanSocietyofAnaesthe-siology. Eur JAnaesthesiol28(10):684–722
33. Monaco M et al (2009) Systematic strategy ofprophylactic coronary angiography improveslong-term outcome after major vascular surgeryin medium- to high-risk patients: a prospec-tive, randomized study. J Am Coll Cardiol54(11):989–996
34. Illuminati G et al (2010) Systematic preoperativecoronary angiography and stenting improvespostoperative results of carotid endarterectomyin patients with asymptomatic coronary arterydisease: a randomised controlled trial. Eur J VascEndovascSurg39(2):139–145
35. LeeSM,TakemotoS,WallaceAW(2015)Associationbetween withholding angiotensin receptorblockers in the early postoperative period and30-day mortality: a cohort study of the VeteransAffairs Healthcare System. Anesthesiology123(2):288–306
36. DuncanAIet al (2007)Recentmetformin ingestiondoes not increase in-hospital morbidity ormortality after cardiac surgery. Anesth Analg104(1):42–50
37. AldamP,LevyN,HallGM(2014)Perioperativeman-agement of diabetic patients: new controversies.Br JAnaesth113(6):906–909
38. Joshi GP et al (2010) Society for AmbulatoryAnesthesia consensus statementonperioperativeblood glucose management in diabetic patientsundergoing ambulatory surgery. Anesth Analg111(6):1378–1387
39. Schouten O et al (2009) Fluvastatin and periop-erative events in patients undergoing vascularsurgery. NEngl JMed361(10):980–989
40. Berwanger O et al (2016) Association betweenpre-operative statin use andmajor cardiovascularcomplications among patients undergoing non-cardiac surgery: the VISION study. Eur Heart J37(2):177–185
41. Douketis JD et al (2015) Perioperative bridginganticoagulation in patients with atrial fibrillation.NEngl JMed373(9):823–833
42. Steinberg BA et al (2015) Use and outcomesassociated with bridging during anticoagulationinterruptions in patients with atrial fibrillation:findings from the Outcomes Registry for BetterInformed Treatment of Atrial Fibrillation (ORBIT-AF).Circulation131(5):488–494
43. Kovacs RJ et al (2015) Practical management ofanticoagulation in patients with atrial fibrillation.JAmCollCardiol65(13):1340–1360
44. Heidbuchel H et al (2015) Updated EuropeanHeart Rhythm Association practical guide on theuse of non-vitamin K antagonist anticoagulantsin patients with non-valvular atrial fibrillation.Europace17(10):1467–1507
45. Waurick K (2016) Antikoagulanzien und Region-alanästhesie. Anästh Intensivmed57:506–521
46. Jambor C, Spannagl M, Zwissler B (2009) Periop-erative management of patients with coronarystents in non-cardiac surgery. Anaesthesist58(10):971–985
47. GawazM, Geisler T (2012)Update orale Plättchen-hemmer. Positionspapier der deutschenGesellschaftfürKardiologie. Kardiologe6:195–209
48. Windecker S et al (2015) 2014 ESC/EACTSguidelines on myocardial revascularization.EuroIntervention10(9):1024–1094
49. Schlaghecke R et al (1992) The effect of long-term glucocorticoid therapy on pituitary-adrenalresponses to exogenous corticotropin-releasinghormone. NEngl JMed326(4):226–230
50. FraserCG, Preuss FS, BigfordWD(1952)Adrenal at-rophyand irreversible shockassociatedwith corti-sonetherapy. JAmMedAssoc149(17):1542–1543
51. Young SL, Marik P, EspositoM, Coulthard P (2009)Supplemental perioperative steroids for surgicalpatients with adrenal insufficiency. CochraneDatabaseSystRev2009:CD5367
Der Anaesthesist · Suppl 1 · 2019 S39