Embed Size (px)
Citation preview

Antikoagulation bei Heparin induzierter Thrombozytopenie
G. R. Hetzel, Düsseldorf
20. Berliner Dialyseseminar 2007
Gemeinschaftspraxis
KarlstraßeGemeinschaftspraxis
Karlstraße
HIT : ein Problem?
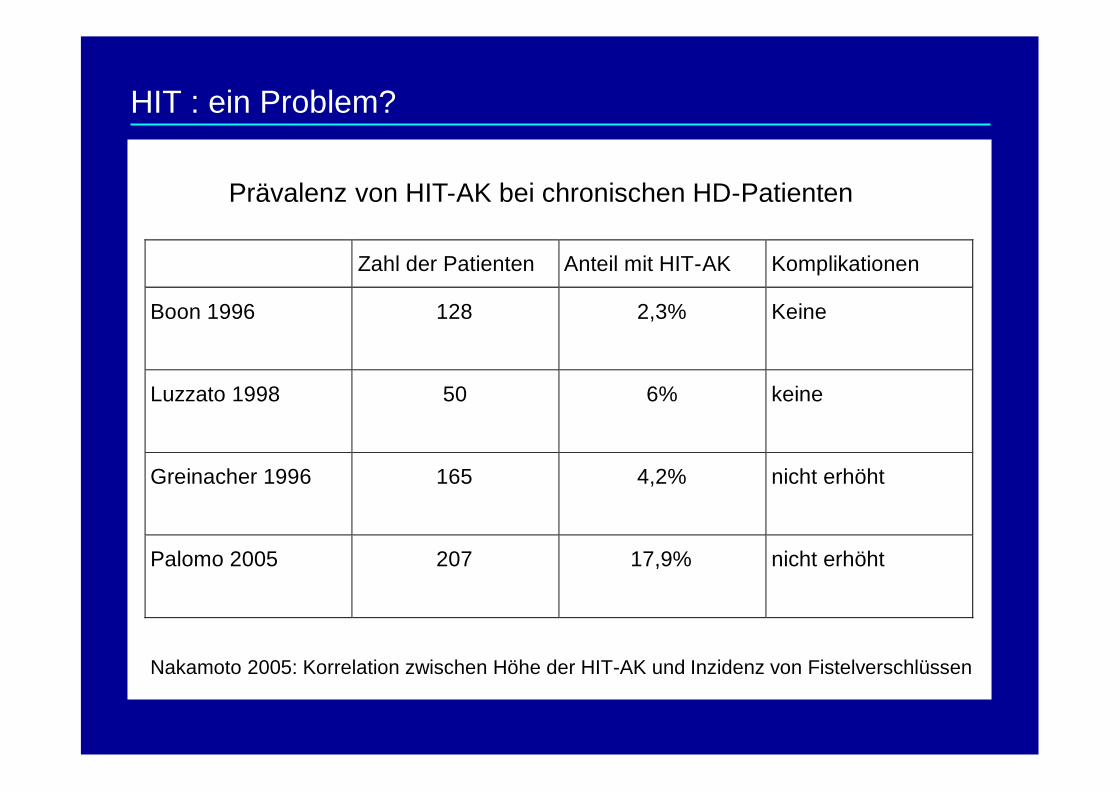
Zahl der Patienten Anteil mit HIT-AK Komplikationen
Boon 1996 128 2,3% Keine
Luzzato 1998 50 6% keine
Greinacher 1996 165 4,2% nicht erhöht
Palomo 2005 207 17,9% nicht erhöht
Nakamoto 2005: Korrelation zwischen Höhe der HIT-AK und Inzidenz von Fistelverschlüssen
HIT : ein Problem?
Prävalenz von HIT-AK bei chronischen HD-Patienten
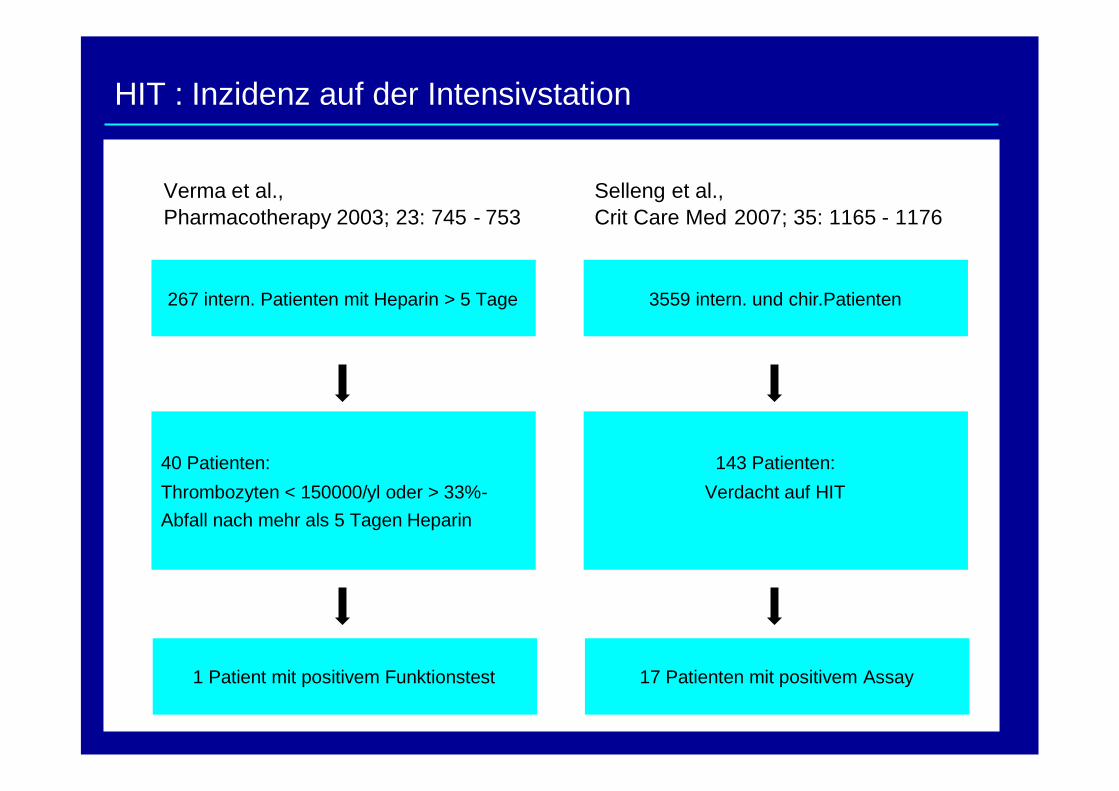
Verma et al.,Pharmacotherapy 2003; 23: 745 - 753
267 intern. Patienten mit Heparin > 5 Tage
40 Patienten:
Thrombozyten < 150000/yl oder > 33%-Abfall nach mehr als 5 Tagen Heparin
1 Patient mit positivem Funktionstest
Selleng et al.,Crit Care Med 2007; 35: 1165 - 1176
3559 intern. und chir.Patienten
143 Patienten:
Verdacht auf HIT
17 Patienten mit positivem Assay
HIT : Inzidenz auf der Intensivstation
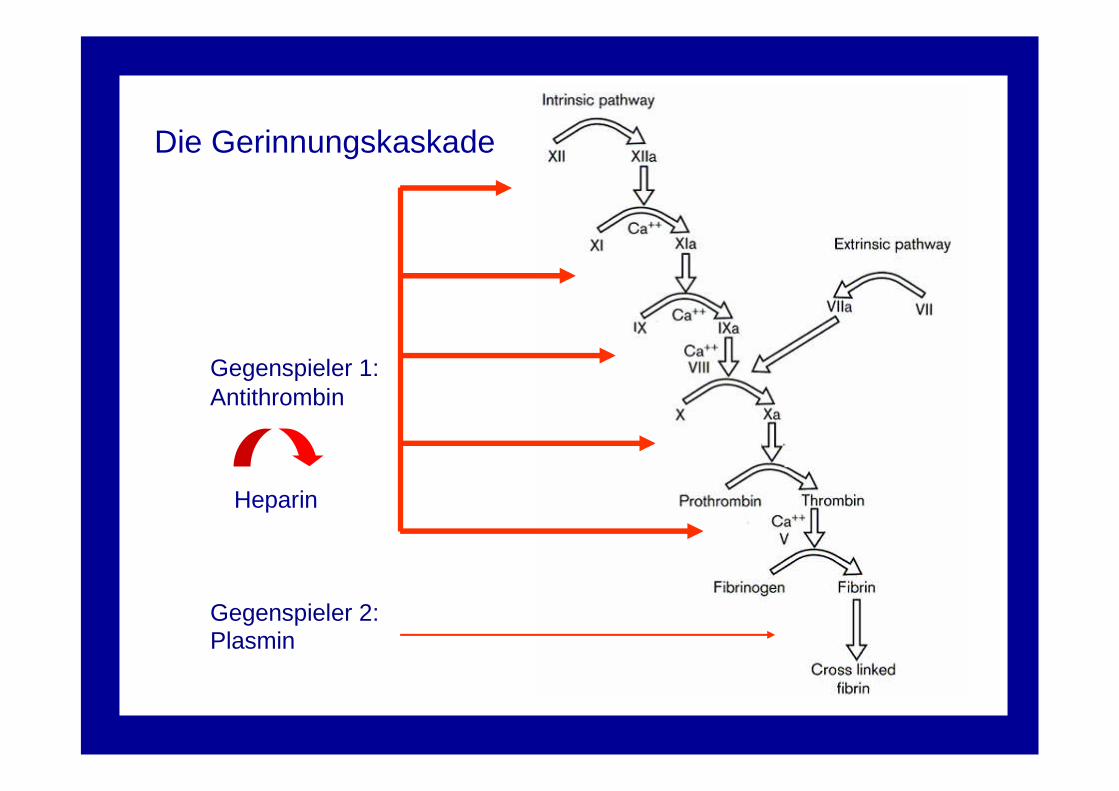
Gegenspieler 1:Antithrombin
Gegenspieler 2:Plasmin
Heparin
Die Gerinnungskaskade
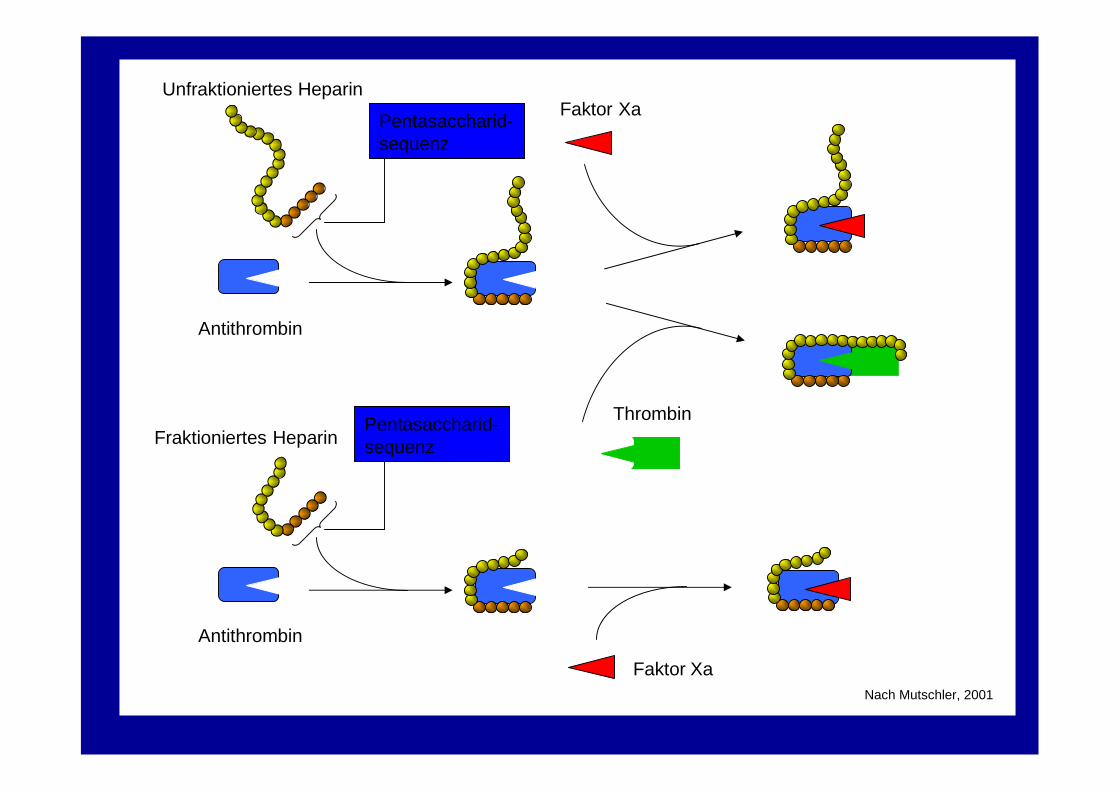
Nach Mutschler, 2001
Faktor Xa
Thrombin
Antithrombin
Unfraktioniertes Heparin
Pentasaccharid-sequenz
Antithrombin
Fraktioniertes HeparinPentasaccharid-sequenz
Faktor Xa
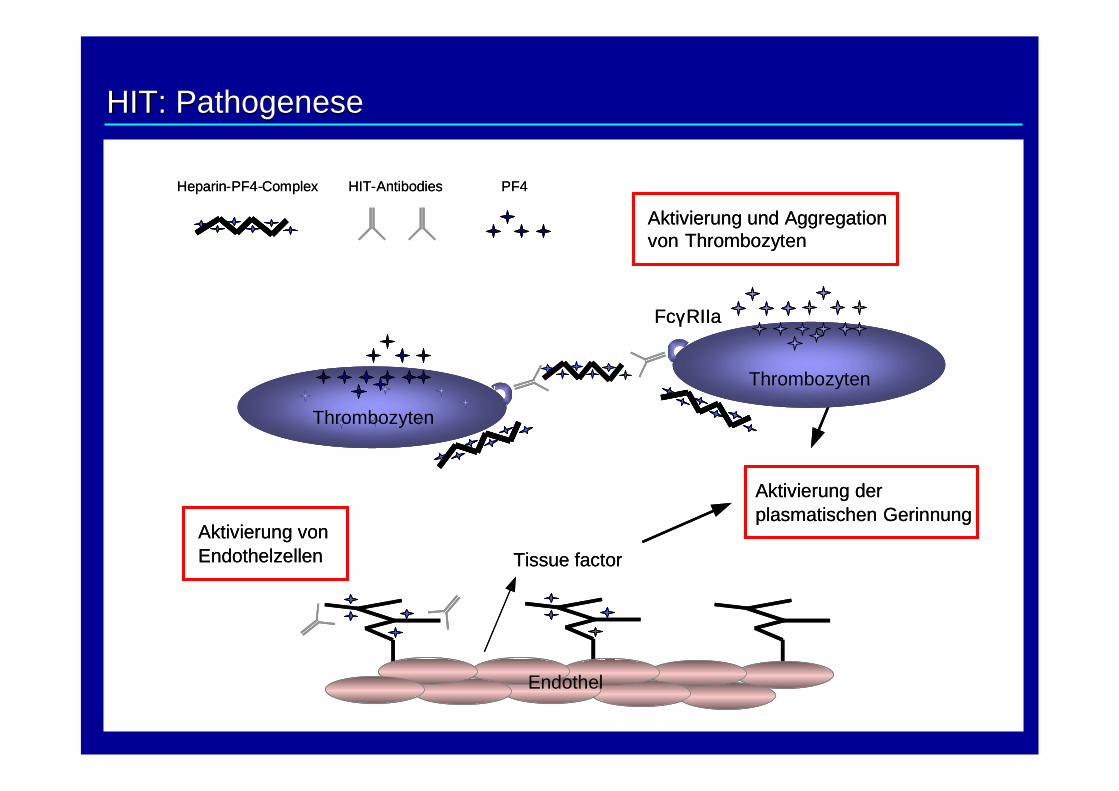
Aktivierung und Aggregationvon Thrombozyten
FcγRIIa
Aktivierung derplasmatischen Gerinnung
Tissue factor
Thrombozyten
Endothel
Heparin-PF4-Complex HIT-Antibodies
Aktivierung vonEndothelzellen
PF4
Thrombozyten
Aktivierung und Aggregationvon Thrombozyten
FcγRIIa
Aktivierung derplasmatischen Gerinnung
Tissue factor
Thrombozyten
Endothel
Heparin-PF4-Complex HIT-Antibodies
Aktivierung vonEndothelzellen
PF4
Thrombozyten
HIT:HIT: PathogenesePathogenese
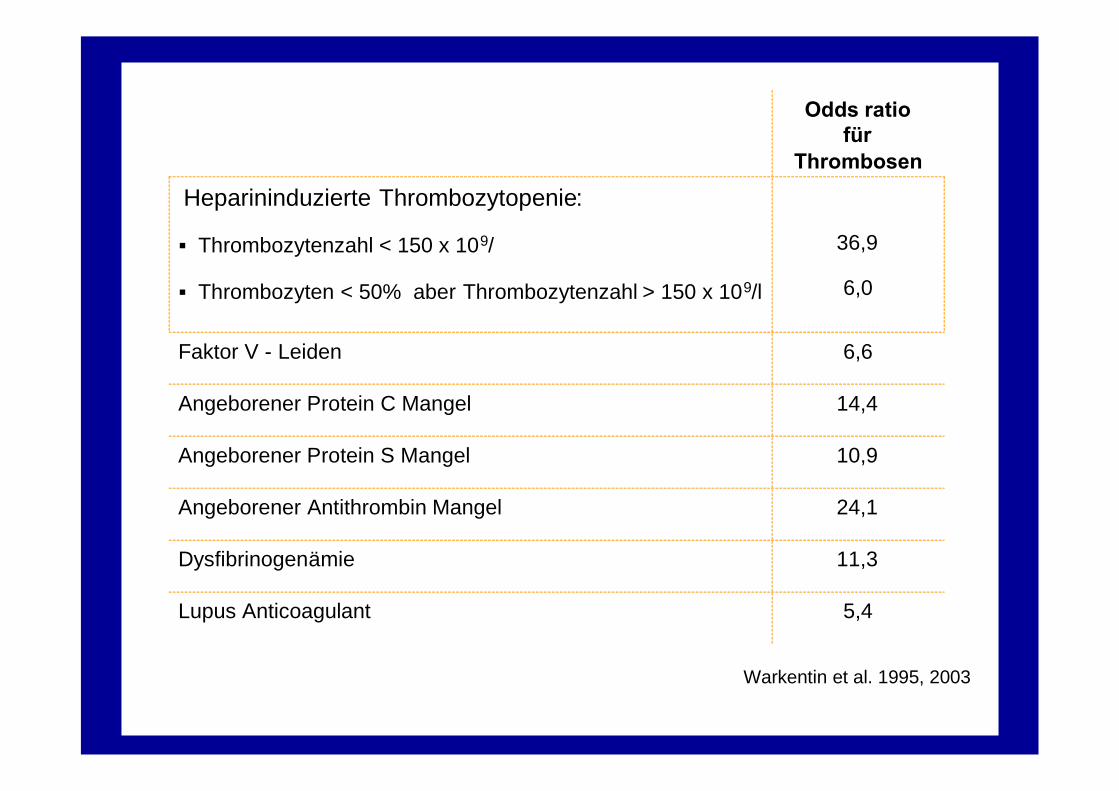
5,4Lupus Anticoagulant
11,3Dysfibrinogenämie
24,1Angeborener Antithrombin Mangel
10,9Angeborener Protein S Mangel
14,4Angeborener Protein C Mangel
6,6Faktor V - Leiden
36,9
6,0
Heparininduzierte Thrombozytopenie:
Thrombozytenzahl < 150 x 109/
Thrombozyten < 50% aber Thrombozytenzahl > 150 x 109/l
Odds ratiofür
Thrombosen
Warkentin et al. 1995, 2003
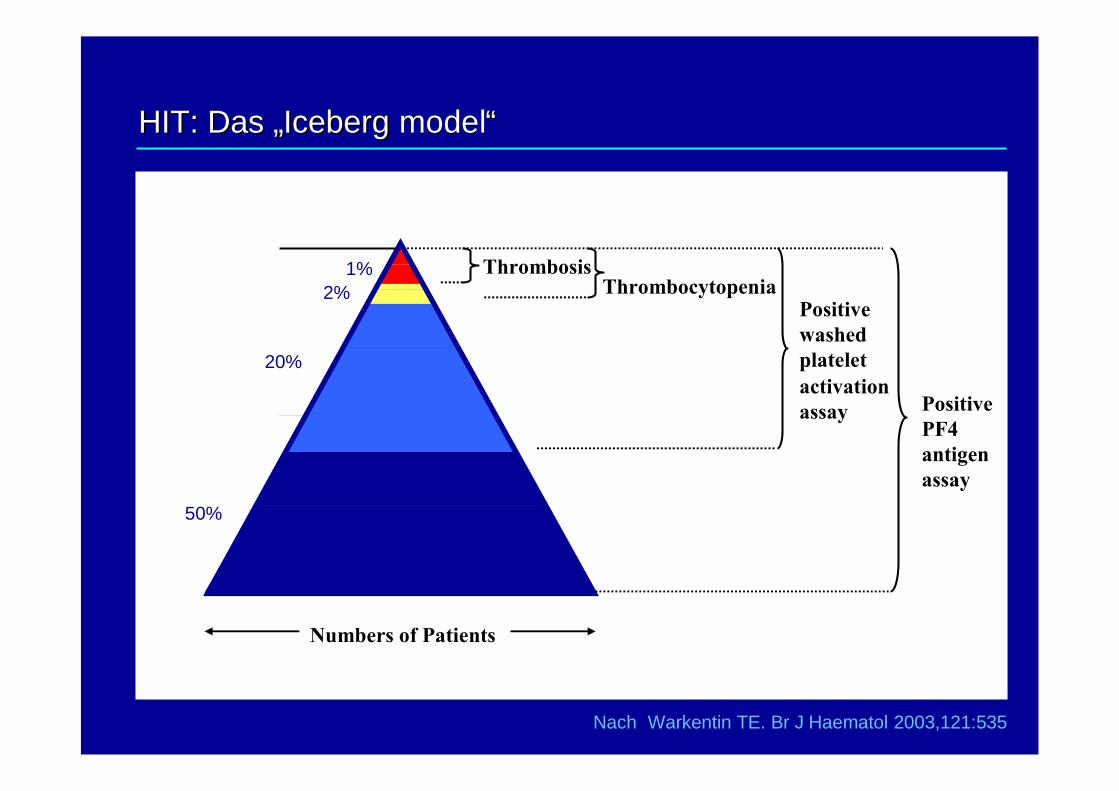
Nach Warkentin TE. Br J Haematol 2003,121:535
ThrombocytopeniaPositivewashedplateletactivationassay Positive
PF4antigenassay
Thrombosis
Numbers of Patients
HIT: Das „HIT: Das „IcebergIceberg modelmodel““
50%
20%
2%1%
HIT : Labortestsysteme
• Antikörpersuchtests:
• überall verfügbar
• detektieren IgG-, IgM- und IgA-Antikörper
• hohe Sensitivität
• rel. geringe Spezifität
• hoher negativ-prädiktiver Wert
• Funktionstests (z.B. HIPA-Test):
• in speziellen Laboratorien verfügbar
• benötigen Spenderthrombozyten definierter Qualität
• detektieren IgG-Antikörper
• höhere Spezifität als Antikörpersuchtests
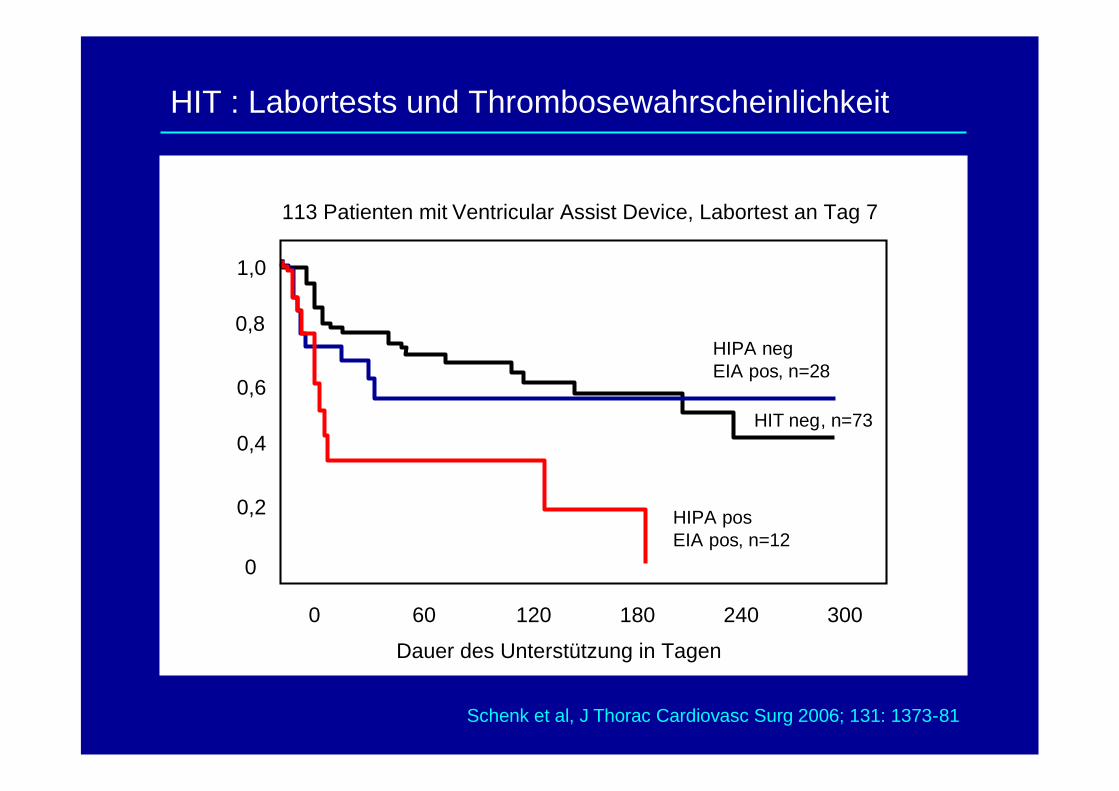
HIPA negEIA pos, n=28
HIT neg, n=73
HIPA posEIA pos, n=12
0
0,2
0,4
0,6
0,8
1,0
0 60 120 180 240 300
Dauer des Unterstützung in Tagen
Schenk et al, J Thorac Cardiovasc Surg 2006; 131: 1373-81
HIT : Labortests und Thrombosewahrscheinlichkeit
113 Patienten mit Ventricular Assist Device, Labortest an Tag 7
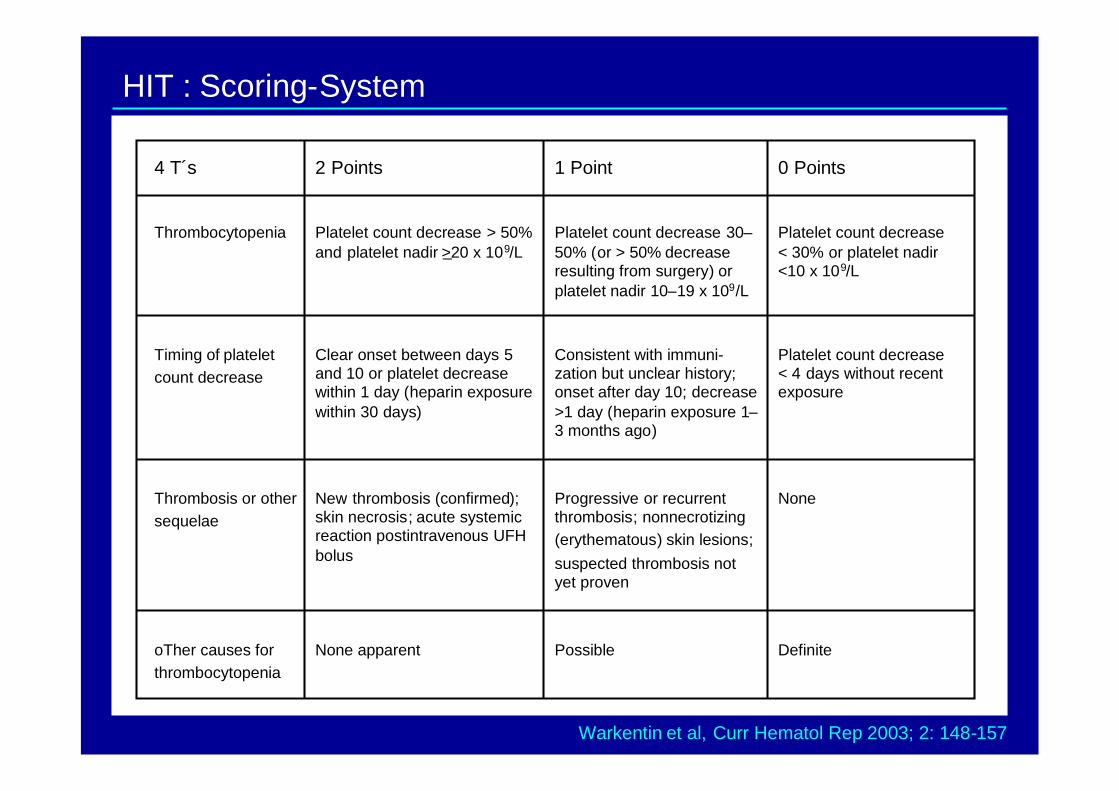
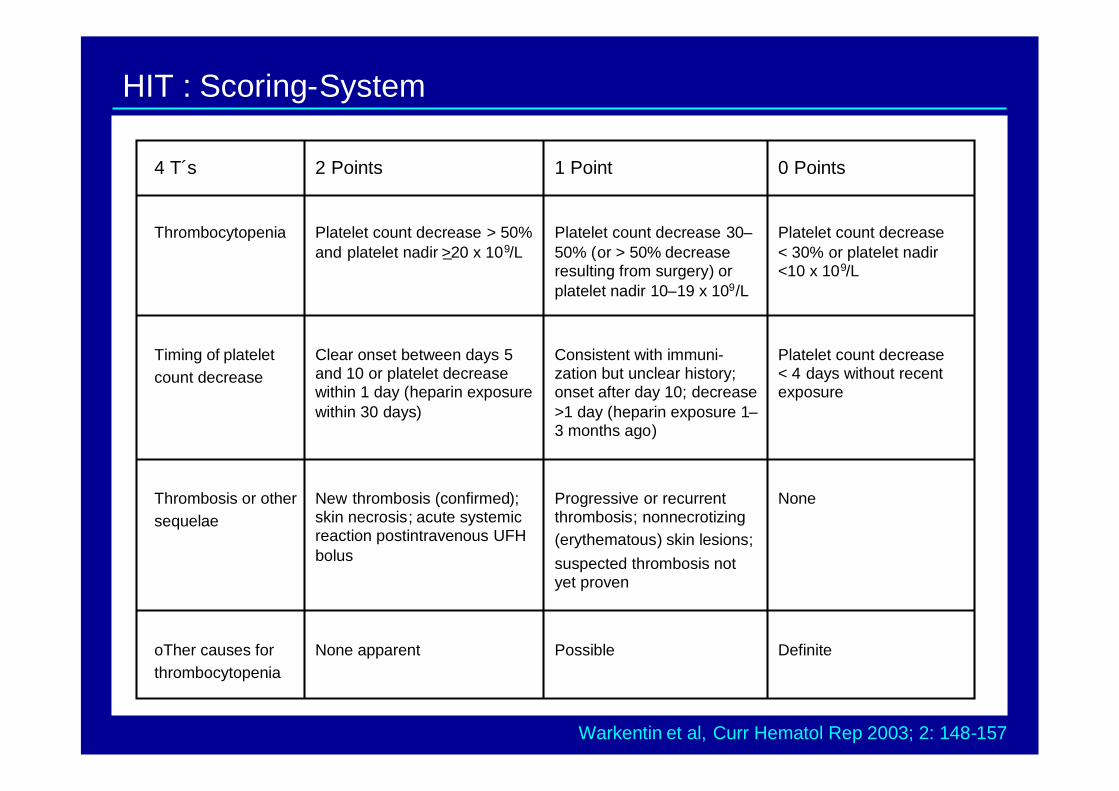
Platelet count decrease< 30% or platelet nadir<10 x 109/L
Platelet count decrease 30–50% (or > 50% decreaseresulting from surgery) orplatelet nadir 10–19 x 109/L
Platelet count decrease > 50%and platelet nadir >20 x 109/L
Thrombocytopenia
DefinitePossibleNone apparentoTher causes forthrombocytopenia
NoneProgressive or recurrentthrombosis; nonnecrotizing(erythematous) skin lesions;suspected thrombosis notyet proven
New thrombosis (confirmed);skin necrosis; acute systemicreaction postintravenous UFHbolus
Thrombosis or othersequelae
Platelet count decrease< 4 days without recentexposure
Consistent with immuni-zation but unclear history;onset after day 10; decrease>1 day (heparin exposure 1–3 months ago)
Clear onset between days 5and 10 or platelet decreasewithin 1 day (heparin exposurewithin 30 days)
Timing of plateletcount decrease
0 Points1 Point2 Points4 T´s
HIT : Scoring-System
Warkentin et al, Curr Hematol Rep 2003; 2: 148-157
30-
20-
10-
40-
0-
5 10 15 20 30 50 70 100 150 200 300 500
Pat
ient
enm
itH
IT
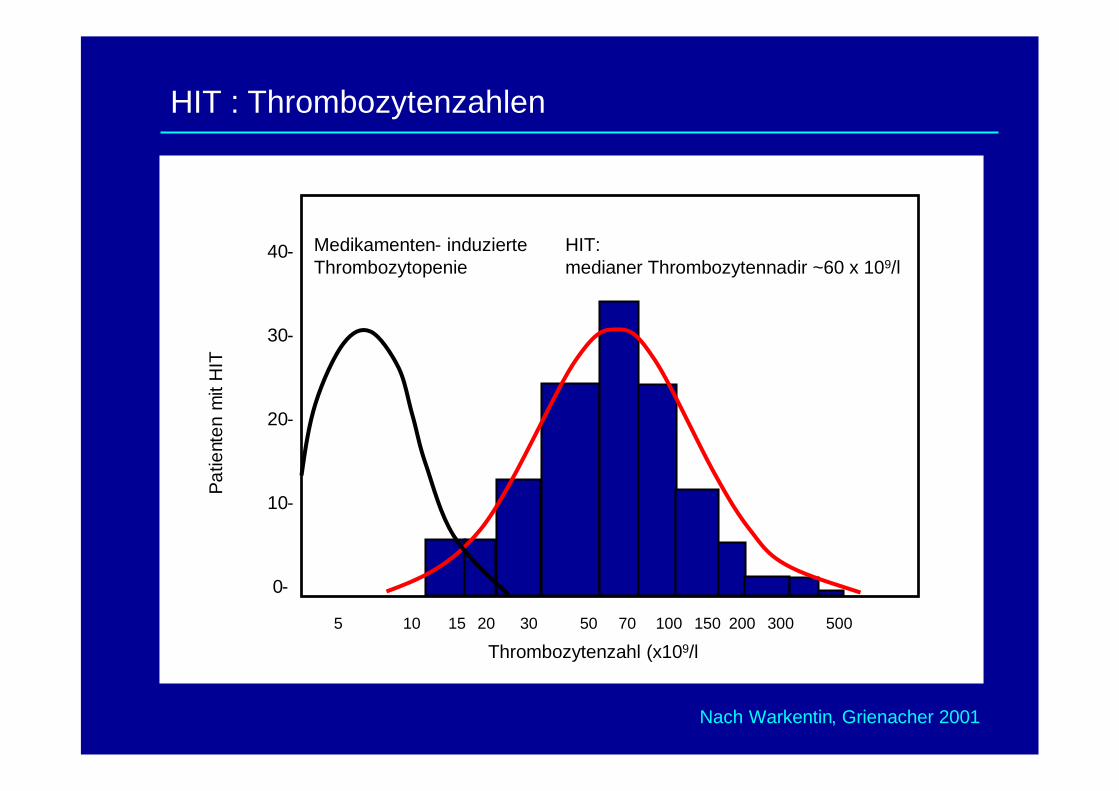
Thrombozytenzahl (x109/l
HIT:medianer Thrombozytennadir ~60 x 109/l
Medikamenten- induzierteThrombozytopenie
HIT : Thrombozytenzahlen
Nach Warkentin, Grienacher 2001
Platelet count decrease< 30% or platelet nadir<10 x 109/L
Platelet count decrease 30–50% (or > 50% decreaseresulting from surgery) orplatelet nadir 10–19 x 109/L
Platelet count decrease > 50%and platelet nadir >20 x 109/L
Thrombocytopenia
DefinitePossibleNone apparentoTher causes forthrombocytopenia
NoneProgressive or recurrentthrombosis; nonnecrotizing(erythematous) skin lesions;suspected thrombosis notyet proven
New thrombosis (confirmed);skin necrosis; acute systemicreaction postintravenous UFHbolus
Thrombosis or othersequelae
Platelet count decrease< 4 days without recentexposure
Consistent with immuni-zation but unclear history;onset after day 10; decrease>1 day (heparin exposure 1–3 months ago)
Clear onset between days 5and 10 or platelet decreasewithin 1 day (heparin exposurewithin 30 days)
Timing of plateletcount decrease
0 Points1 Point2 Points4 T´s
HIT : Scoring-System
Warkentin et al, Curr Hematol Rep 2003; 2: 148-157
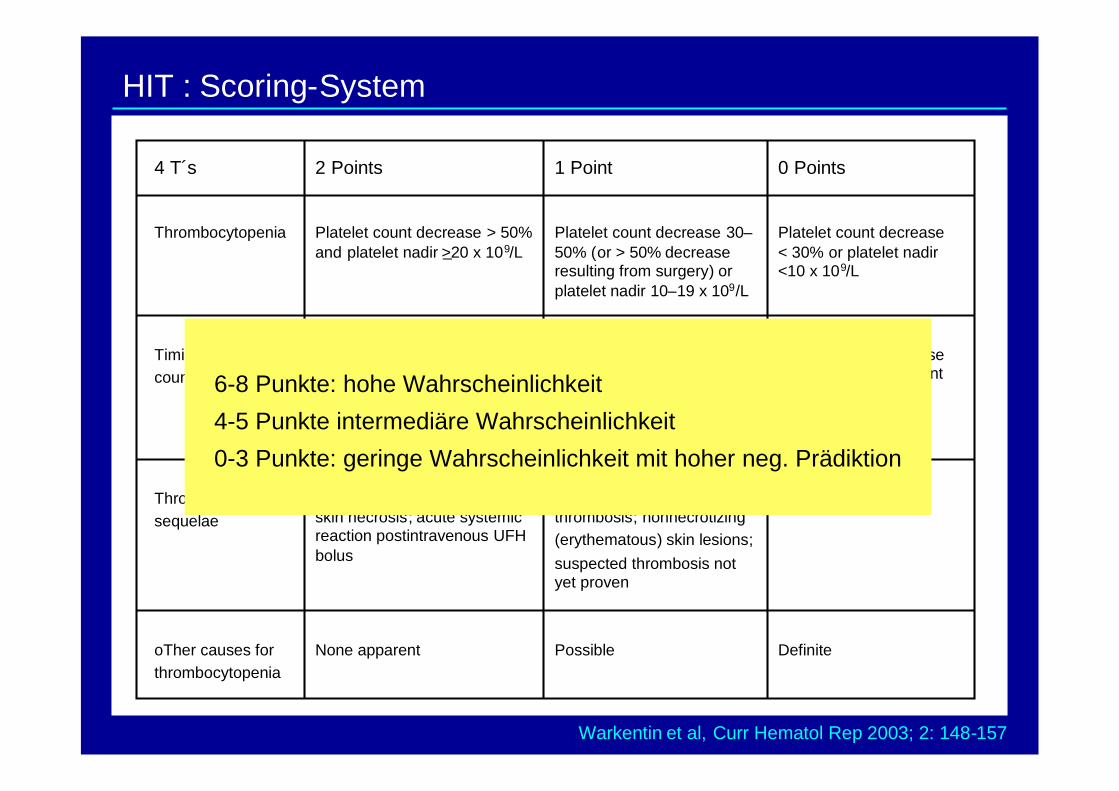
Platelet count decrease< 30% or platelet nadir<10 x 109/L
Platelet count decrease 30–50% (or > 50% decreaseresulting from surgery) orplatelet nadir 10–19 x 109/L
Platelet count decrease > 50%and platelet nadir >20 x 109/L
Thrombocytopenia
DefinitePossibleNone apparentoTher causes forthrombocytopenia
NoneProgressive or recurrentthrombosis; nonnecrotizing(erythematous) skin lesions;suspected thrombosis notyet proven
New thrombosis (confirmed);skin necrosis; acute systemicreaction postintravenous UFHbolus
Thrombosis or othersequelae
Platelet count decrease< 4 days without recentexposure
Consistent with immuni-zation but unclear history;onset after day 10; decrease>1 day (heparin exposure 1–3 months ago)
Clear onset between days 5and 10 or platelet decreasewithin 1 day (heparin exposurewithin 30 days)
Timing of plateletcount decrease
0 Points1 Point2 Points4 T´s
HIT : Scoring-System
6-8 Punkte: hohe Wahrscheinlichkeit
4-5 Punkte intermediäre Wahrscheinlichkeit
0-3 Punkte: geringe Wahrscheinlichkeit mit hoher neg. Prädiktion
Warkentin et al, Curr Hematol Rep 2003; 2: 148-157
HIT : Labortestsysteme
• Antikörpersuchtests:
• überall verfügbar
• detektieren IgG-, IgM- und IgA-Antikörper
• hohe Sensitivität
• rel. geringe Spezifität
• hoher negativ-prädiktiver Wert
• Funktionstests (z.B. HIPA-Test):
• in speziellen Laboratorien verfügbar
• benötigen Spenderthrombozyten definierter Qualität
• detektieren IgG-Antikörper
• höhere Spezifität als Antikörpersuchtests
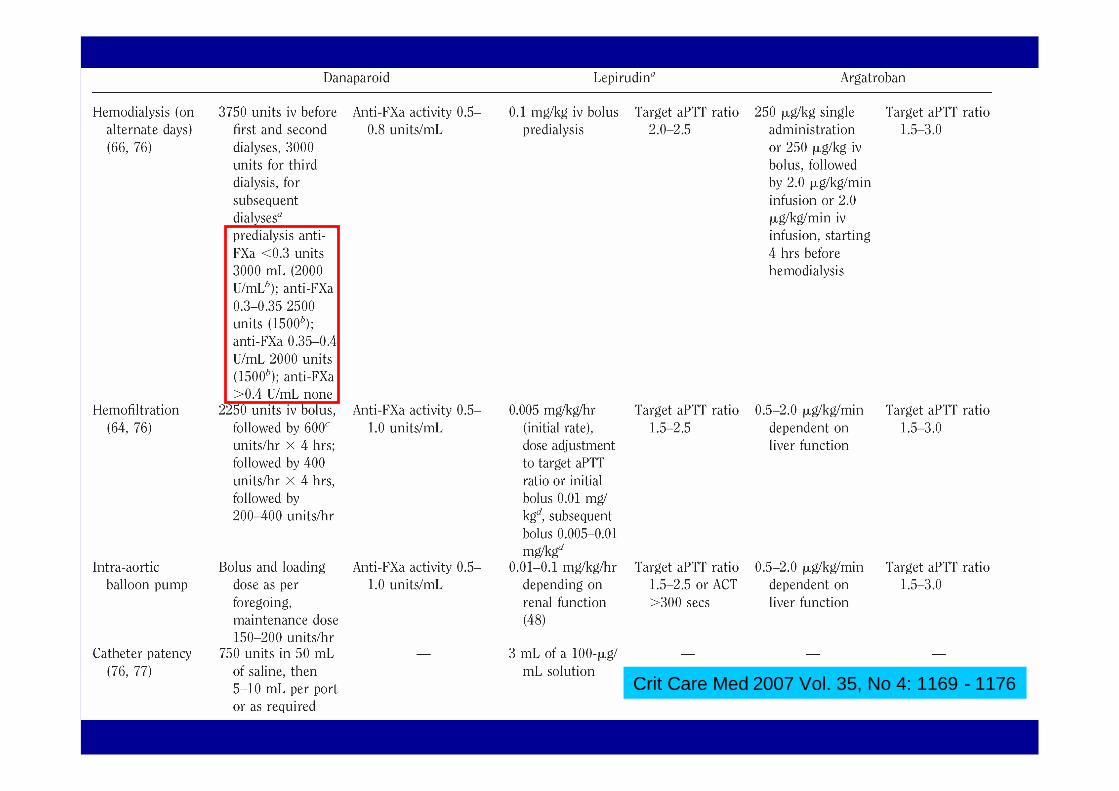
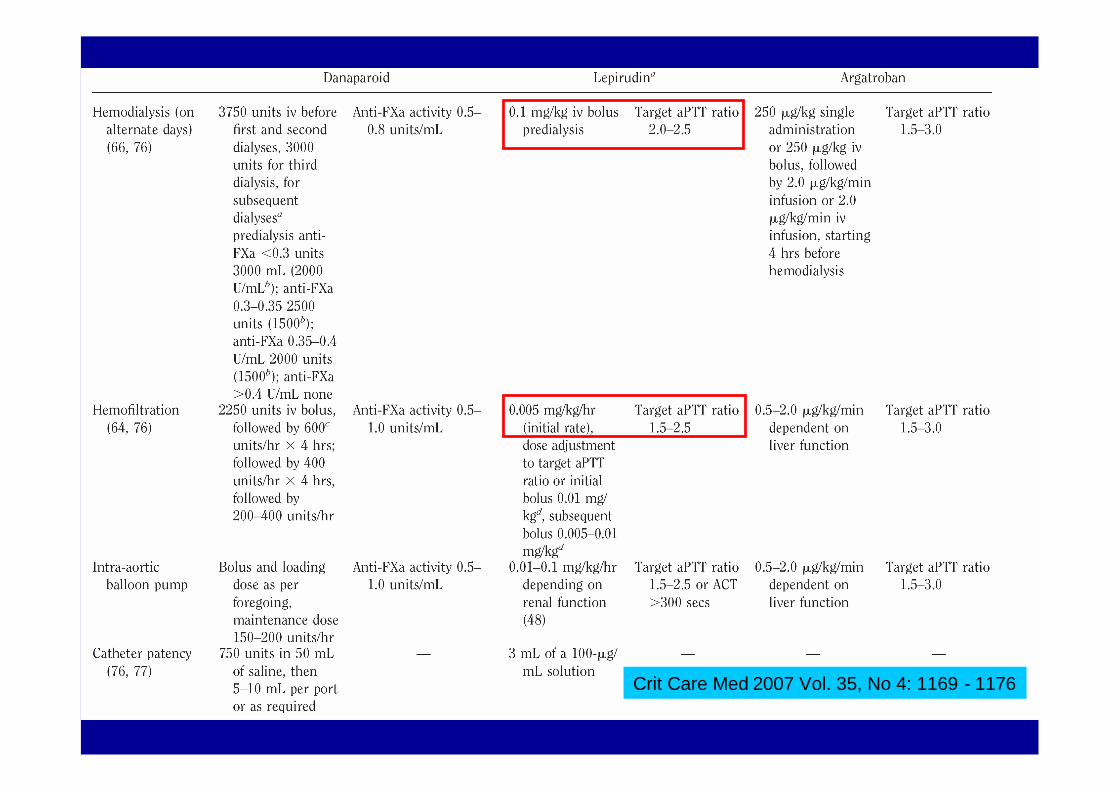
Crit Care Med 2007 Vol. 35, No 4: 1169 - 1176
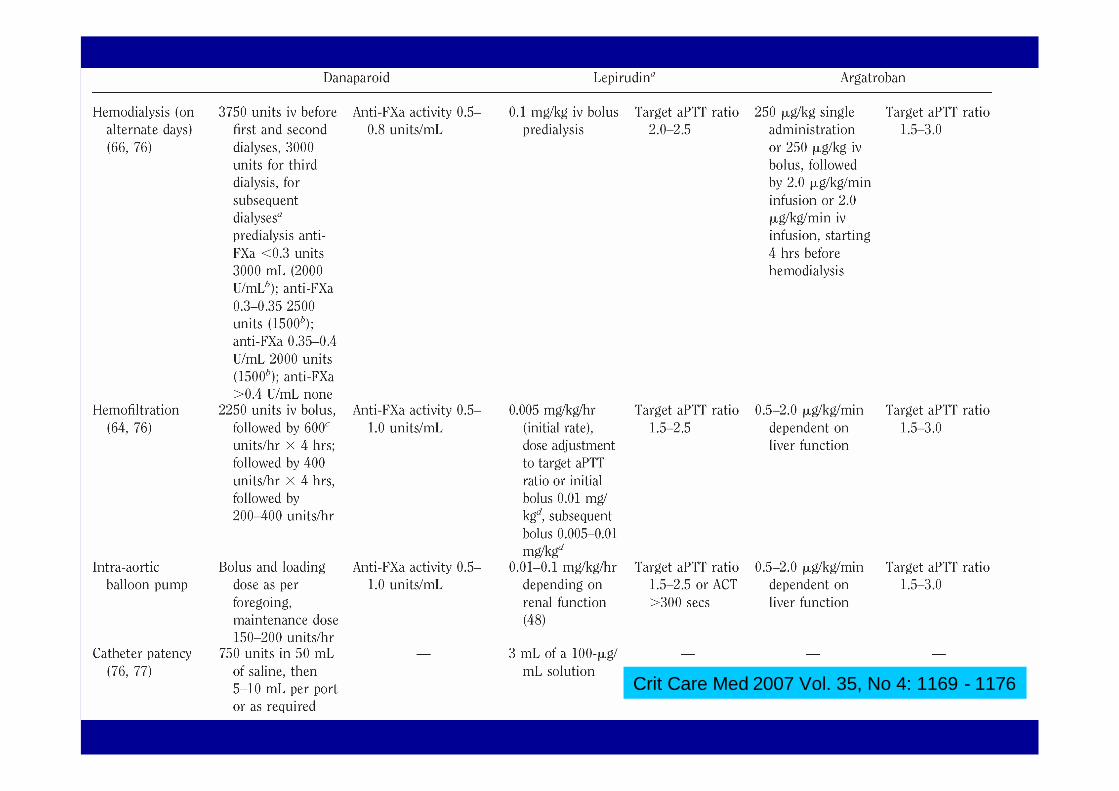
Crit Care Med 2007 Vol. 35, No 4: 1169 - 1176
HeparinoidHeparinoid:: DalteparinDalteparin ((OrgaranOrgaran))
Gemisch aus Glykosaminoglykanen, überwiegend
Heparansulfat
Bindet an Antithrombin III
Anti-Xa/Anti-IIa-Ratio 28 : 1
Kreuzreaktion bei HIT in 5 – 10 %
Lange Eliminationshalbwertszeit 25 h
Kein Antagonist, ggf. Plasmapherese
Crit Care Med 2007 Vol. 35, No 4: 1169 - 1176
Aus Hirudo medicinalisgewonnen
Polypeptid aus 65 AS
R-Hirudin: Lepirudin(Refludan) und Desirudin(Revasc)
Renale Elimination
HWZ 60 – 100 min, beiterminaler NI 1.5 – 50 h
Kein Antidot
Direkter Thrombin-Antagonist,sowohl freies als auch fibrin-gebundenes
HirudinHirudin als direkterals direkter ThrombinantagonistThrombinantagonist
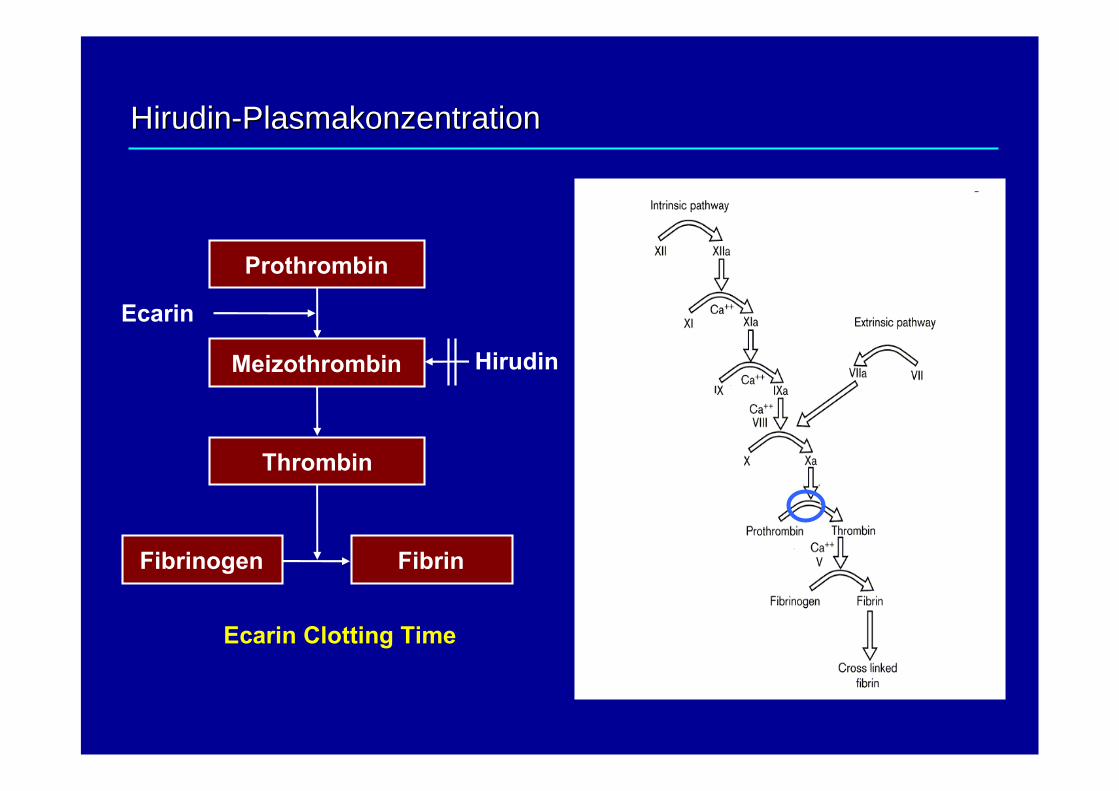
Ecarin
Hirudin
Fibrinogen Fibrin
Meizothrombin
Prothrombin
Thrombin
Ecarin Clotting Time
HirudinHirudin--PlasmakonzentrationPlasmakonzentration
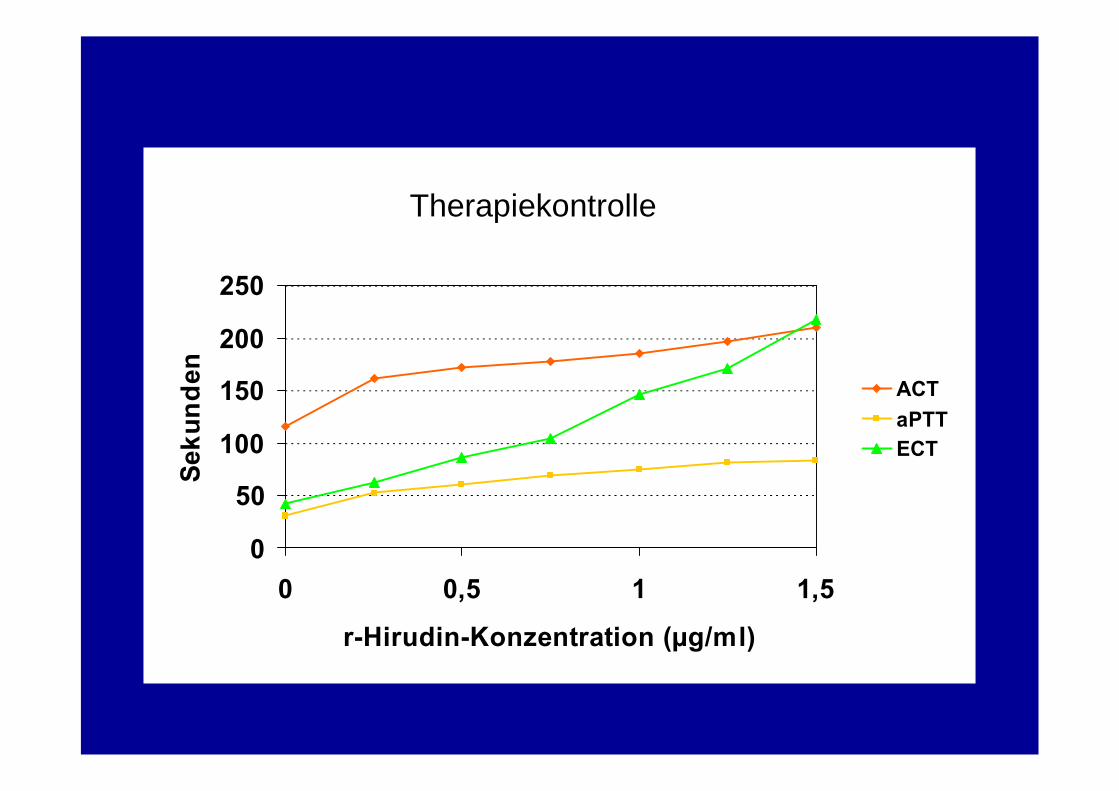
0
50
100
150
200
250
0 0,5 1 1,5
r-Hirudin-Konzentration (µg/ml)
Sek
und
en ACTaPTTECT
Therapiekontrolle
Crit Care Med 2007 Vol. 35, No 4: 1169 - 1176
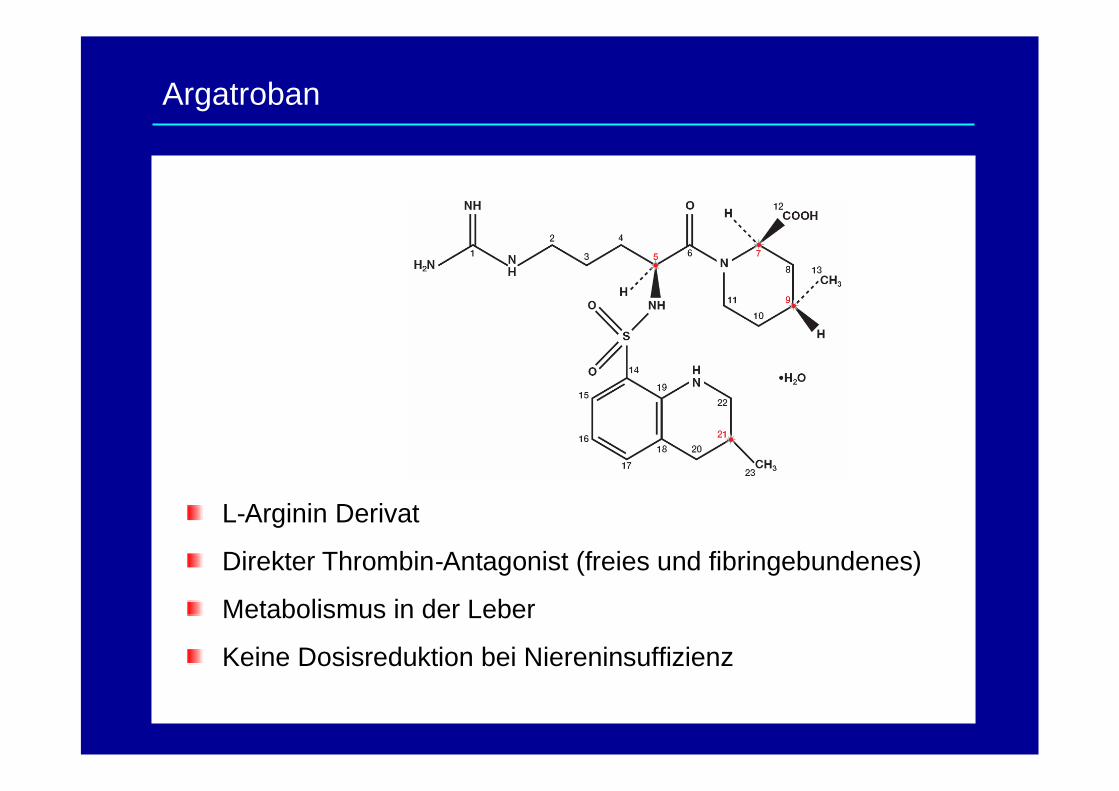
L-Arginin Derivat
Direkter Thrombin-Antagonist (freies und fibringebundenes)
Metabolismus in der Leber
Keine Dosisreduktion bei Niereninsuffizienz
Argatroban
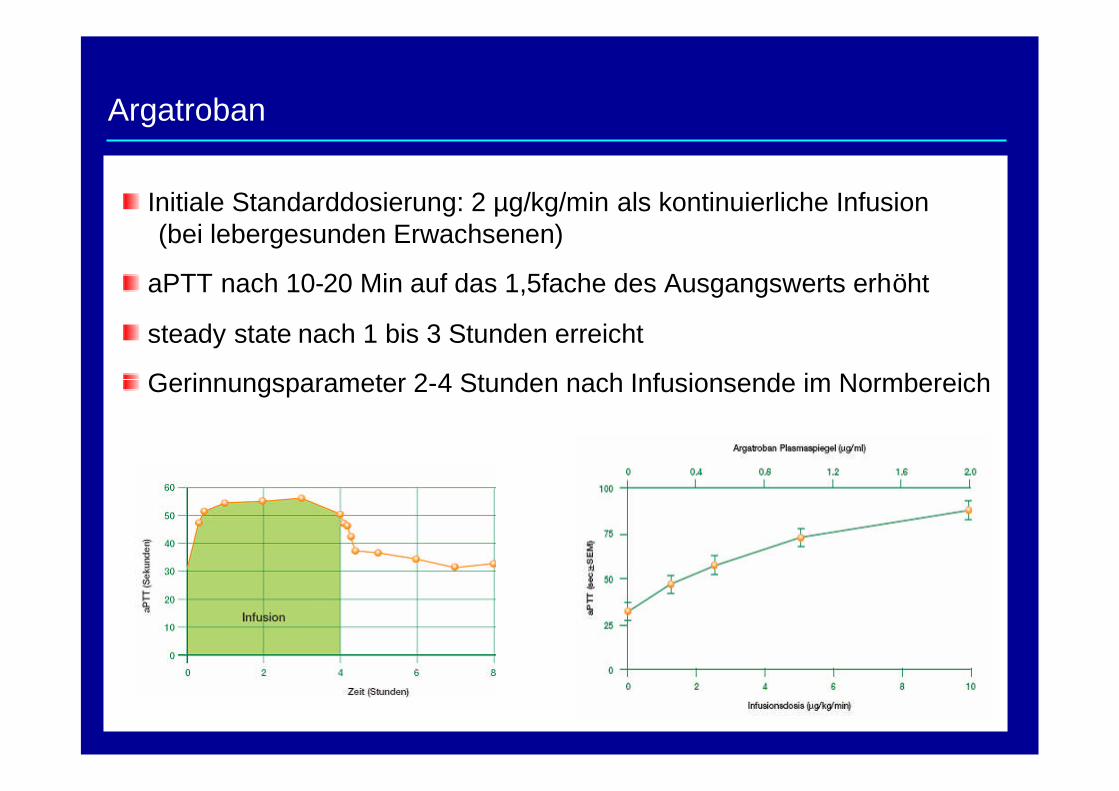
Argatroban
Initiale Standarddosierung: 2 µg/kg/min als kontinuierliche Infusion(bei lebergesunden Erwachsenen)
aPTT nach 10-20 Min auf das 1,5fache des Ausgangswerts erhöht
steady state nach 1 bis 3 Stunden erreicht
Gerinnungsparameter 2-4 Stunden nach Infusionsende im Normbereich
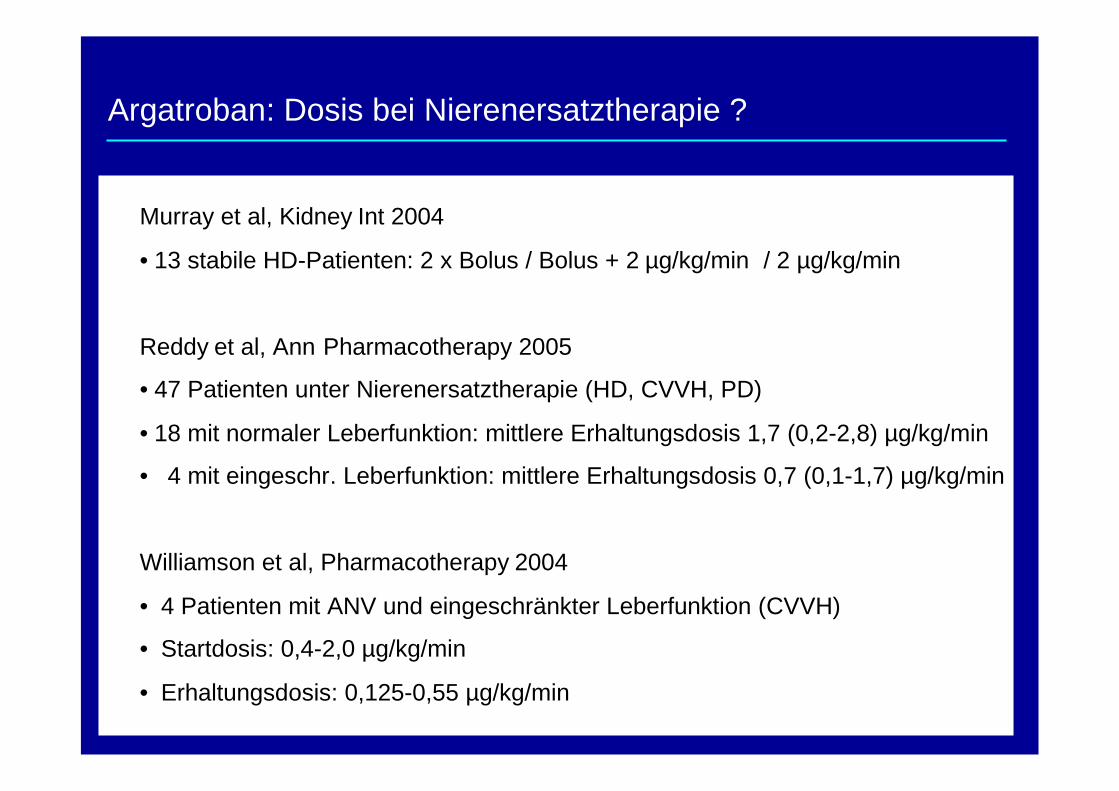
Argatroban: Dosis bei Nierenersatztherapie ?
Murray et al, Kidney Int 2004
• 13 stabile HD-Patienten: 2 x Bolus / Bolus + 2 µg/kg/min / 2 µg/kg/min
Reddy et al, Ann Pharmacotherapy 2005
• 47 Patienten unter Nierenersatztherapie (HD, CVVH, PD)
• 18 mit normaler Leberfunktion: mittlere Erhaltungsdosis 1,7 (0,2-2,8) µg/kg/min
• 4 mit eingeschr. Leberfunktion: mittlere Erhaltungsdosis 0,7 (0,1-1,7) µg/kg/min
Williamson et al, Pharmacotherapy 2004
• 4 Patienten mit ANV und eingeschränkter Leberfunktion (CVVH)
• Startdosis: 0,4-2,0 µg/kg/min
• Erhaltungsdosis: 0,125-0,55 µg/kg/min
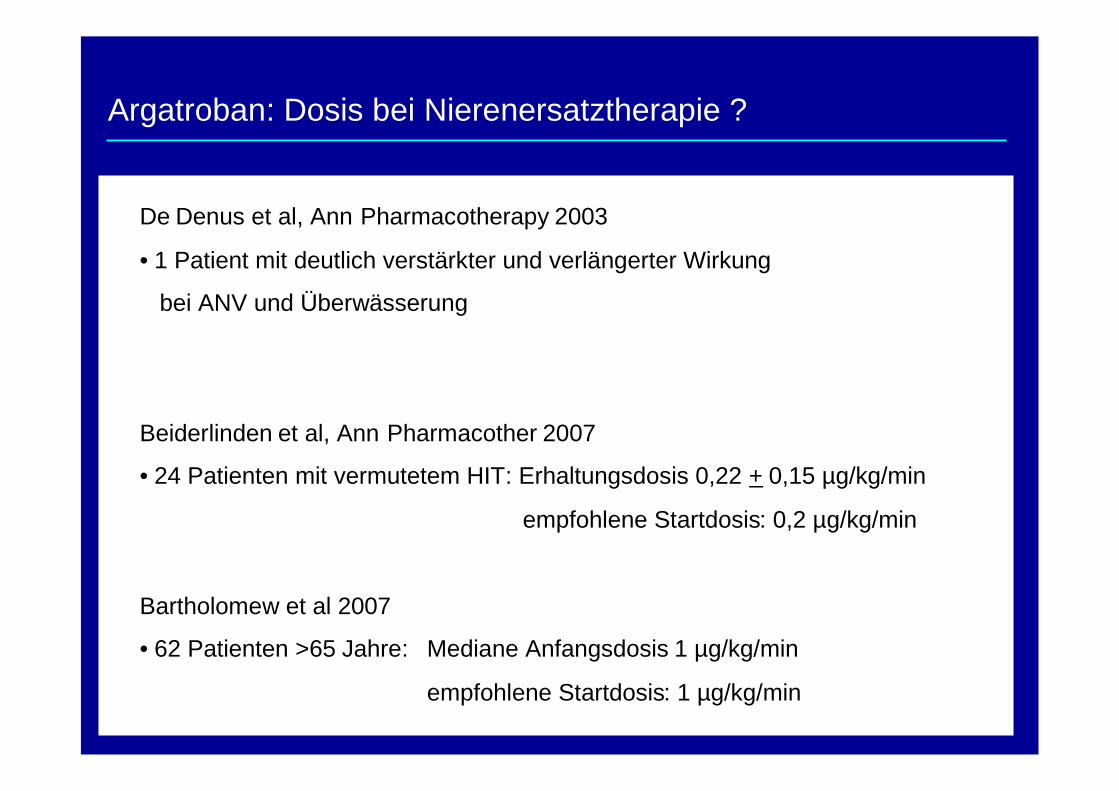
Argatroban: Dosis bei Nierenersatztherapie ?
De Denus et al, Ann Pharmacotherapy 2003
• 1 Patient mit deutlich verstärkter und verlängerter Wirkung
bei ANV und Überwässerung
Beiderlinden et al, Ann Pharmacother 2007
• 24 Patienten mit vermutetem HIT: Erhaltungsdosis 0,22 + 0,15 µg/kg/min
empfohlene Startdosis: 0,2 µg/kg/min
Bartholomew et al 2007
• 62 Patienten >65 Jahre: Mediane Anfangsdosis 1 µg/kg/min
empfohlene Startdosis: 1 µg/kg/min

Crit Care Med 2007 Vol. 35, No 4: 1169 - 1176
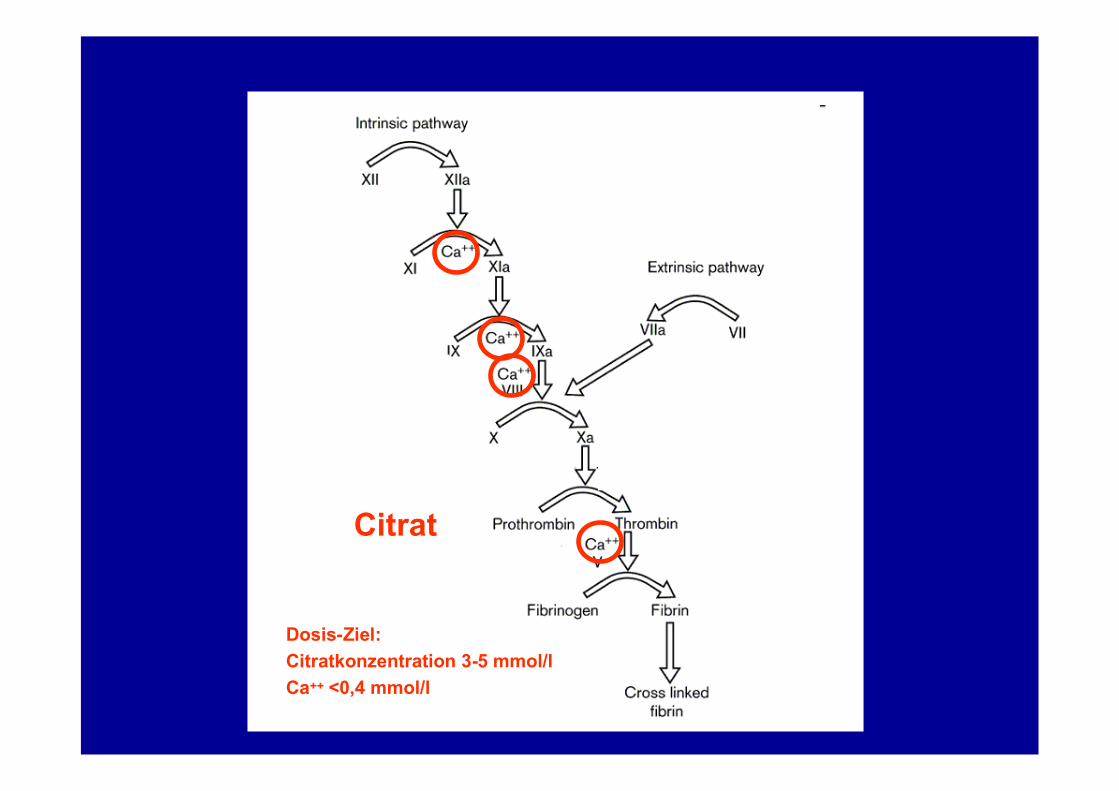
Citrat
Dosis-Ziel:Citratkonzentration 3-5 mmol/lCa++ <0,4 mmol/l
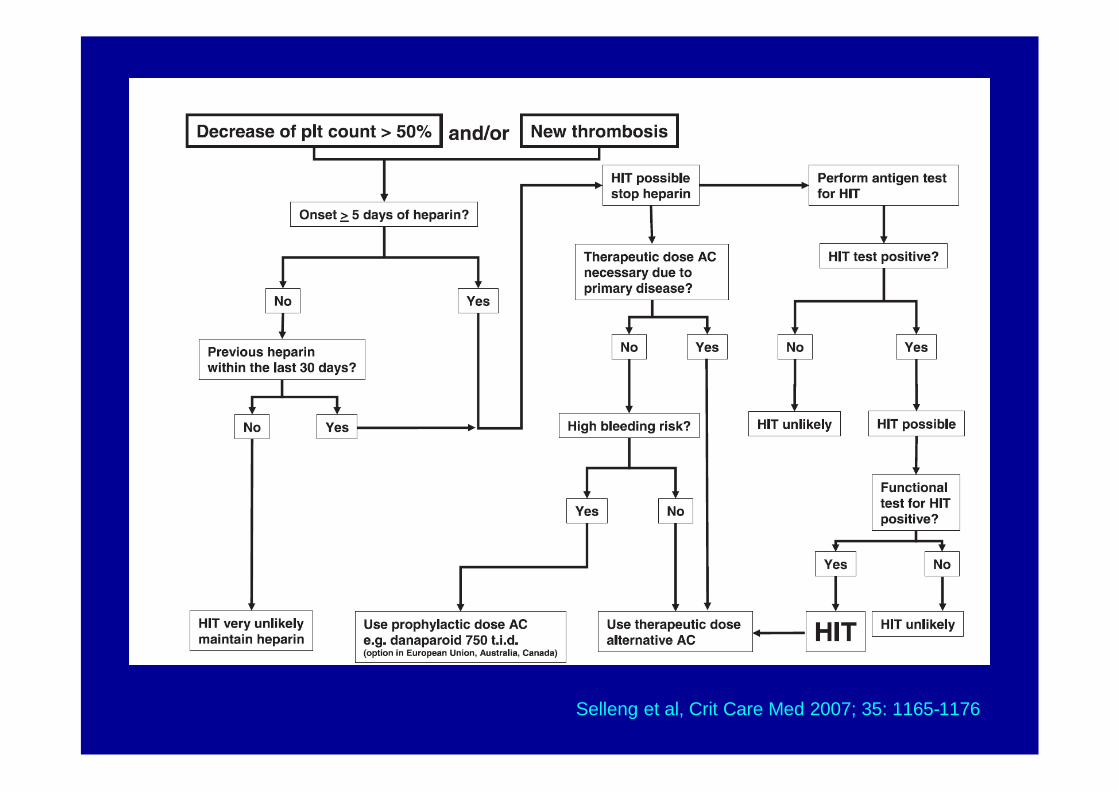
Selleng et al, Crit Care Med 2007; 35: 1165-1176
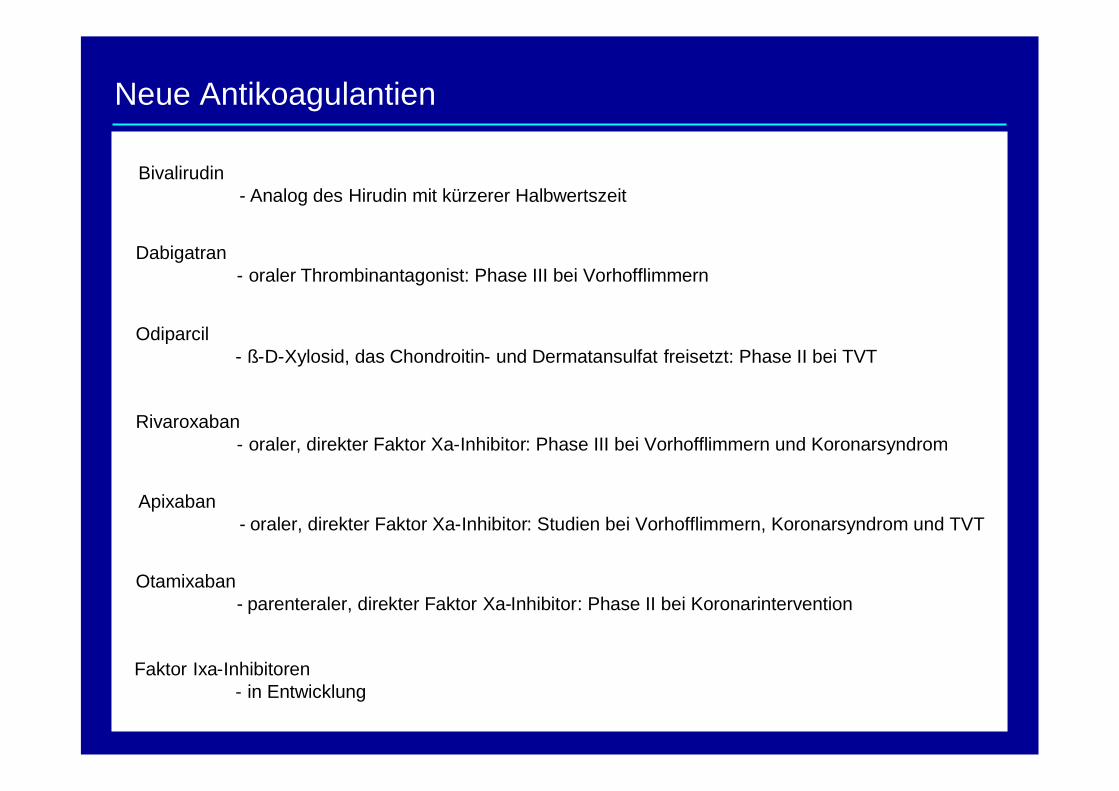
Neue Antikoagulantien
Dabigatran- oraler Thrombinantagonist: Phase III bei Vorhofflimmern
Bivalirudin- Analog des Hirudin mit kürzerer Halbwertszeit
Odiparcil- ß-D-Xylosid, das Chondroitin- und Dermatansulfat freisetzt: Phase II bei TVT
Rivaroxaban- oraler, direkter Faktor Xa-Inhibitor: Phase III bei Vorhofflimmern und Koronarsyndrom
Apixaban- oraler, direkter Faktor Xa-Inhibitor: Studien bei Vorhofflimmern, Koronarsyndrom und TVT
Otamixaban- parenteraler, direkter Faktor Xa-Inhibitor: Phase II bei Koronarintervention
Faktor Ixa-Inhibitoren- in Entwicklung

Antikoagulation bei Heparin induzierter Thrombozytopenie
20. Berliner Dialyseseminar 2007
























