Embed Size (px)
Citation preview


Oligometastatic CRC: What do we know about it, and how to treat it?
Instituto CUF de Oncologia
Lisboa, Portugal
Asklepios Tumorzentrum Hamburg
AK Altona , Abt. Onkologie, Hämatologie und Palliativmedizin
ATZ: Organisationsfelder
„Disease
Track /
Programs“
per Tumorentität
Klinische
„Core
Facilities“
unabhängig von
Tumorentität
QM /
Zertifizierung /
Register
Fortbildung /
Veranstaltung
Studien /
Wissenschaft
Marketing / PR
Klinischer Bereichadministrativer
Bereich
Ergänzende
klinische
Angebote
unabhängig von
Tumorentität

Disclosures Dirk Arnold, 2014-2019
• Participate on Advisory Board with:
Roche, Merck Serono, Amgen, Bayer, Servier, Sanofi, BTG, Lilly
• Speaker and Chairman for educational events with:
Boston Scientific, BTG, Roche, Merck Serono, Bayer, Lilly, Servier, Sanofi
• Investigator and researcher in data generating activities supported and sponsored by
Roche, Mologen, AstraZeneca, Bayer

Metastases in colon cancer
primarily local disease
Prognosis determined by primary
Local treatment
Metastastatic diseasePrognosis determined by metastases
Systemic treatmentdiffuse metastatic diseaseUnfavourable biology, only systemictreatment
Oligometastatic diseasePrognosis „intermediate“ –
because of biology (?) and the optionfor additional (local) treatment
Prognosis
70 yrs „tumour biology“> 120.000 Publicationens
ca. 20 yrs< 50 publications on „biology“
Cure
Palliation
Chronic disease(potentially cure)
→ local (palliative) treatment

Why are pts with few mets. living longer?
• Lower tumour burden?
• better (= „less complicated“) sites?
• Additional use of ablative techniques?

Mathematical-mechanistical hypotheses
Mannsmann UR ASCO GI 2013, abstract no. 427
∆ OS
No tumor shrinkage
PFS
PFS
∆ PFS
Tumor shrinkage
Lethal tumor load
Baseline tumor load
Time under treatment

Time
Cel
lco
un
t
Goldie-Coldman Hypothesis:
less therapy-resistant clones with a smaller number of cells
- Goldie JH et al., Cancer Res. 1984
- Withers HR et al., Sem Radiat Oncol 2006
Cytoreduction: biological hypotheses
Norton-Simon Hypothesis: kinetic resistance - poorer response to chemotherapy in small residualsNorton L et al., Cancer Treat Rep 1986, Oncologist 2005
Chemotherapy
Metastasis 1
Metastasis 2Primary
Subclone
Gerlinger et al., New Engl J Med 2012

Are there really biological characteristicsexisting,
which may help us to distinguish betweenan oligometastatic and a whitespread
pattern of metastasation?

Similar – but (likely) not the same
Local tumour→ oligometastasation→ diffuse mets. → terminal disease
continuum over time?
Paget et al., Lancet 1898; Halstead et al., Ann Surg 1907

Metastasation as an evolutional process: The „SPECTRUM“ hypothesis
Adapted from: Hellman S., Karnofsky Memorial Lecture, J Clin Oncol 1994

Continuum over time?
„new biology“
Local tumour→ oligometastasation→ diffuse mets. → terminal disease
Similar – but (likely) not the same
Paget et al., Lancet 1898; Halstead et al., Ann Surg 1907Hellman et al., 1994

Continuum over time?
„new biology“ Cont. over time?
„new biology“?
Paget et al., Lancet 1898; Halstead et al., Ann Surg 1907Hellman et al., 1994
Local tumour→ oligometastasation→ diffuse mets. → terminal disease
Similar – but (likely) not the same

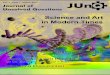
Oligometastatic vs. Disseminated Disease
Adapted from: Reyes et al., Oncotarget 2015

Oligometasta+c-vs.-Systemic-Disease-
Oncotarget3www.impactjournals.com/oncotarget
Actively migrating
cancer cells
Oligometastatic
Disease Systemic Disease
Hospitable target
organs
Poor primary
tumor conditions
Inhospitable target
organs
Sloughed
cancer cells
Good primary
tumor conditions
s
Figure 1: Oligometastatic disease versus systemic disease. OHIW2 OLJRP HWDVWDWLF GLVHDVH 0 HWDVWDWLF JURZWKSRWHQWLDOLVOLP LWHG
7KLVFRXOGEH D VHFRQGDU\ WRGXHWRHQYLURQP HQWDOFRQGLWLRQVLQWKHSULP DU\ WXP RUIRUHVWDOOLQJ HYROXWLRQDU\ FORQDOSUHVVXUH E FDQFHU
FHOOVWKDWVORXJKRXWRI WKHSULP DU\ WXP RUWKDWGRQRWKDYHWKHSURSHUWLHVQHFHVVDU\ WRVXUYLYHWKHFLUFXODWLRQDQGLQYDGHLQWRWDUJHWRUJDQ
VLWHV DQGRU F WKHFDQFHUFHOOVODQGLQLQKRVSLWDEOHWDUJHWRUJDQV ULJKW6\ VWHP LF GLVHDVH : LGHVSUHDGP HWDVWDWLF JURZWKSRWHQWLDOLV
XQOLP LWHG 7KLVFRXOGEH D VHFRQGDU\ WRGXHWRHQYLURQP HQWDOFRQGLWLRQVLQWKHSULP DU\ WXP RUFUHDWLQJ P DQ\ XQGLIIHUHQWLDWHG DJJUHVVLYH
FORQHV E FDQFHUFHOOVWKDWDFWLYHO\ P LJUDWHRXWRI WKHSULP DU\ WXP RUWKDWKDYHWKHSURSHUWLHVQHFHVVDU\ WR VXUYLYHWKHFLUFXODWLRQDQG
LQYDGHLQWRWDUJHWRUJDQVLWHV DQGRU F WKHFDQFHUFHOOVODQGLQKRVSLWDEOHWDUJHWRUJDQV
Table 1: A comparison of migrants, diaspora, and the spectrum of cancer metastases
Social Demography Cancer Demography
Imperial Diaspora Trading Post Diaspora7UDGLQJ 3RVW' LDVSRUD
Oligometastasis
, P SHULDO' LDVSRUD
Cancer metastasis
/ DUJHSRSXODWLRQVIURP D
VLQJOHKRP HODQG
6P DOOSRSXODWLRQIURP D
VLQJOHKRP HODQG
0 LJUDWHGIURP SULP DU\
FDQFHULQSDVVLYHP DQQHU
' LVSHUVHGIURP DSULP DU\
FDQFHULQDQDFWLYHP DQQHU
6HWWOHP XOWLSOHFRXQWULHVLQ
DJJUHVVLYHP DQQHU
6HWWOHLQIHZ FRXQWULHVZKLOH
DYRLGLQJ XSVHWWLQJ KRVW
FRXQWU\
0 LOGK\ SR[ LDDQGXQOLP LWHG
QXWULHQWV + RP HQLFKH
FRQGLWLRQVGRQRWFDXVH
HYROXWLRQDU\ FORQDOSUHVVXUH
+ \ SR[ LDDQGODFNRI
QXWULHQWVFDXVHSUHVVXUHWR
OHDYHSULP DU\ ( YROYLQJ
KRP HQLFKHFRQGLWLRQVFDXVH
XQGLIIHUHQWLDWHG DJJUHVVLYH
FORQHV
+ RVWFRXQWU\ P D\ RUP D\ QRW
EHUHFHSWLYH
+ RVWFRXQWU\ P D\ RUP D\ QRW
EHUHFHSWLYH
7DUJHWRUJDQP D\ RUP D\ QRW
EHUHFHSWLYH
7DUJHWRUJDQP D\ RUP D\ QRW
EHUHFHSWLYH
* URXS P DLQWDLQVFROOHFWLYH
P HP RU\ RI WKHLUKRP HODQG
DQGFXOWXUH
* URXS P DLQWDLQVFROOHFWLYH
P HP RU\ RI WKHLUKRP HODQG
DQGFXOWXUH
3DWKRORJLVWVFDQLGHQWLI\
ZKHUHDFDQFHUFHOO
RULJLQDWHG
3DWKRORJLVWVFDQLGHQWLI\
ZKHUHDFDQFHUFHOO
RULJLQDWHG
2 IWHQDVVLP LODWHWKHQHZ
KRP HODQG
6XUYLYHDVGLVWLQFW
FRP P XQLWLHV) HZ GLVWLQFWP HWDVWDVHV
0 XOWLSOHP HWDVWDVHVDV
GLVWLQFWP DVVHV
5 HODWLRQVKLS ZLWKKRVW
FRXQWU\ LVXQHDV\ DQG
GHJHQHUDWHVRYHUWLP H
5 HODWLRQVKLS ZLWKKRVW
FRXQWU\ P D\ EHXQHDV\ EXWLV
P DLQWDLQHGRYHUWLP H
,P P XQHV\ VWHP P D\ QRWVHH
DWKUHDW
,P P XQHV\ VWHP WULHVWR
GHVWUR\ WKHFDQFHUFHOOV
7LHGWRWKHKRP HODQGE\
H[ FKDQJHRI UHVRXUFHV
7LHGWRWKHKRP HODQGE\
H[ FKDQJHRI UHVRXUFHV
/ LP LWHGQHHGIRURXWVLGH
UHVRXUFHVIURP KRP HODQG
IHZHUFHOOVWUDI¿FNLQJ
0 XOWLSOHFHOOW\ SHWUDI¿FNLQJ
WUDI¿FNLQJ RI UHVRXUFHVLQIR
7DEOHDGDSWHGIURP 3LHQWDHWDO&OLQ&DQ5 HVHDUFK > @
Adapted'from:'Reyes'et'al.,'Oncotarget'2015'Adapted from: Reyes et al., Oncotarget 2015
Oligometastatic vs. Disseminated Disease

A comparison of migrants, diaspora, and the spectrum of cancer metastases
adapted from: Pieta et al., Clin Cancer Res 2013
tumor mets capabilities: migration
environmental adverse„pressure“
environmental „hospitality“: tissue
environmental „hospitality“:immunogenicity

Consensus molecular subtypes of CRC

Molecular classification of CRC
31%
26% 19%
24% 56%
10%
27% 7%
51%
15%
31% 3%
Summary of associations
Dienstmann R, et al. WCGIC 2014 (Abstract No. O-0025)
Dienstmann et al., WCGC / ESMO GI 2016

Pitroda et al., Nature Communications 2018

Pitroda et al., Nature Communications 2018

Biology and oligometastasation: What is do we need to know clinically?
• Prognostic information
• How „ambitious“ should our treatment be?
• Predictive information
• E.g. selection of a (primary) local-ablative treatment (e.g. SBRT) vs. systemic tretament
→Biology: not ready for prime time!

Van Cutsem,....et al., Arnold. Ann Oncol 2016

ESMO Consensus: What is seen as „oligometastatic disease“?
Van Cutsem E, Cervantes A, …...Arnold D ESMO Consensus; Ann Oncol 2016

ESMO Consensus: What is seen as „oligometastatic disease“?
Van Cutsem E, Cervantes A, …...Arnold D ESMO Consensus; Ann Oncol 2016

ESMO Consensus: What is seen as „oligometastatic disease“?
Van Cutsem E, Cervantes A, …...Arnold D ESMO Consensus; Ann Oncol 2016

Therapeutic concepts -
What do we know ?

CLM: Surgery and retrospective seriesInitially non-resectable liver metastases
Adam et al., J Clin Oncol 2009

Vatandoust et al., World J Gastroenterol 2017
CRC: Single organ metastases

Perioperative treatment strategywith liver metastases
Van Cutsem E, Cervantes A, …...Arnold D. ESMO Consensus; Ann Oncol 2016

Perioperative treatment strategywith liver metastases
Van Cutsem E, Cervantes A, …...Arnold D. ESMO Consensus; Ann Oncol 2016

Retrospective blinded evaluation of (potential) resectabilityof 448 pat. @ baseline and best response
Independent assesent by 8 surgeons and 3 oncologists

Fig. 1
22%
Modest et al., Eur J Cancer 2018

Fig. 1
53%
Modest et al., Eur J Cancer 2018

Fig. 3
European Journal of Cancer 2018 88, 77-86DOI: (10.1016/j.ejca.2017.10.028) Modest et al., Eur J Cancer 2018

Fig. 3
European Journal of Cancer 2018 88, 77-86DOI: (10.1016/j.ejca.2017.10.028) Modest et al., Eur J Cancer 2018

Perioperative treatment strategywith liver metastases
Van Cutsem E, Cervantes A, …...Arnold D. ESMO Consensus; Ann Oncol 2016

ABSTRACT #3509
PHASE II TRIAL DESIGN
mCRCUnresectable
1st-line
WT RAS**
Age ≥ 18yrs
ECOG PS 0-1
N = 96
Randomization:
6/2011 - 1/2017
R
Treatment until PD, resectability,
or to maximum 12 cycles
mFOLFOXIRI +
panitumumab 6 mg/kg
Q2W
N = 63Irinotecan 150 mg/m2, oxaliplatin 85 mg/m2,
LV 200 mg/m2, 5-FU 3000 mg/m2 CIV;
Planned safety analysis after 10 patients
treated in panitumumab arm
FOLFOXIRI Q2W
N = 33
2:1
If resectable:
Surgery, then
protocol treatment to
maximum 12 cycles
If CR/PR/SD after 12 cycles:
re-induction
(same combination)
recommended on PD
Strata:
Cohort 1: histologically confirmed and definitively inoperable or unresectable
Cohort 2: chance of secondary resection with curative intent (* pretreatment liver/tumor biopsy)
**amendment in 11/2013 to include all RAS wild-type only
*
*
• 21 active centers in Germany
1 cycle FOLFOXIRI
prior R was allowed
.Geissler et al., ASCO 2018 #3509
VOLFI trial: FOLFOXIRI +/- panitumumabin RAS WT mCRC

PRIMARY ENDPOINT: OBJECTIVE RESPONSE RATEFINAL DATA AFTER EXTERNAL MONITORING
mFOLFOXIRI +
panitumumab
N = 63
FOLFOXIRI
N = 33
% 95%-CI % 95%-CI Odds ratio p
87.3 76.5 – 94.4 60.6 42.1 – 77.14.469
(1.614-12.376)0.004
p: Exact test of Fisher (2-sided, alpha = 0.05)
Geissler et al., ESMO 2018
VOLFI trial: FOLFOXIRI +/- panitumumabin RAS WT mCRC

Patient #1
• 64 y/o lawyer, active, no relevant comorbidity
• C. transversum adenocarcinoma, 4y ago stage II, R0, no adjuvant
• Now, at follow-up: 3 peripheral hepatic lesions: „segmental resection possible“
• CEA 23

Patient #2
• 59 y/o, female, shop assistant, no relevant comorbidity
• Sigmoid colon adenocarcinoma, stage III (N1), R0, just finished adjuvant FOLFOX
• Now, at follow-up: 3 peripheral hepatic lesions: „segmental resection possible“
• CEA 78


Perioperative treatment strategywith liver metastases
Van Cutsem E, Cervantes A, …...Arnold D. ESMO Consensus; Ann Oncol 2016

Perioperative treatment strategywith liver metastases
Van Cutsem E, Cervantes A, …...Arnold D. ESMO Consensus; Ann Oncol 2016

Perioperative treatment strategywith liver metastases
„best systemic therapy“ (if appropriate)
Van Cutsem E, Cervantes A, …...Arnold D. ESMO Consensus; Ann Oncol 2016


Patient #3
• 74 y/o, former mayor, hypertension
• Left colon adenocarcinoma , 11 months ago, stage II, RAS wt, BRAF w, R0
• Started adjuvant capecitabine for 6 months
• Now, after 3 months: 3 peripheral hepatic lesions: „segmental resection possible“
• CEA 239

What to do, if resectability isunclear?

Yoshino et al., Ann Oncol 2018 (online since Nov 2017)

ESMO Asia Consensus Guidelines 2018
Yoshino et al., Ann Oncol 2018 (online since Nov 2017)

Management of OMD
Van Cutsem E, Cervantes A, …...Arnold D. ESMO Consensus; Ann Oncol 2016

Ruers et al., JNCI 2017
EORTCCAO (ALM)NCRI CCCG

Median follow-up 9.7 yrs
OSHR 0.58p = 0.01
PFSHR 0.57p < 0.01
Ruers et al., JNCI 2017

Management of OMD
Van Cutsem,.....Arnold. ESMO Consensus Guidelines mCRC., Ann Oncol 2016

Management of OMD
Van Cutsem,.....Arnold. ESMO Consensus Guidelines mCRC., Ann Oncol 2016

Induction
Best systemictreatment
Best maintenance
De-escalation ?
pause ?
other compound?
Best ablation
resection
„ablation toolbox“
severalmanifeststions,
„palliative“
Oligometastastaticdisease
„ablative“
post induction
where ?response?
Metastatic CRC: Main principles

Example for (too?) early integration: The SIRFLOX trial
Treatment arm: FOLFOX + SIRT ( delayed start of bevacizumab/cetuximab)
Work up for
SIRT
Preparation
On day -14 to -3
Control arm: FOLFOX ( bevacizumab/cetuximab from Cycle 1)
Cycle 1
Bev/Cet
OX = 85
mg/m2
Cycle 2 Cycle 3 Cycle ≥4
FOLFOXOX = 85
mg/m2
OX = 85
mg/m2
OX = 85
mg/m2
OX = 60
mg/m2
OX = 60
mg/m2
Bev/Cet
OX = 85
mg/m2
SIRT(Cycle 1 or 2)
On day 3 or 4
FOLFOX
Bev/Cet
FOLFOX
Bev/Cet
FOLFOX
Bev/Cet
Cycle 1
FOLFOX
Cycle 2
FOLFOX
Cycle 3
FOLFOXOX = 60
mg/m2
Cycle ≥4
FOLFOX
Bev, bevacizumab; Cet, cetuximab
Sharma et al., ASCO 2017

Liver-failure free survival Progression free survival
Sharma et al., J Clin Oncol 2018
Example for (too?) early integration: The SIRFLOX trial

Where are our limitations...?

Tanis et al., Eur J Cancer 2014

6%
Tanis et al., Eur J Cancer 2014

Tanis et al., Eur J Cancer 2014
6%
25-30%

CELIM trial: Initially irresectable liver mets
··· Disease free survival after
resection
All patients
< 5 metastases
5-10 metastases
> 10 metastases
DFS 9.9 [95% CI: 5.8-14.0] months
Comparison between groups:
p < 0.001
Pro
ba
bilit
y o
f s
urv
iva
l
Folprecht et al, Ann Oncol 2014

··· Progression free survival
▬ Overall survival
R0 resected patients
R1 resection / ablation
Not resected patients
OS R0 resected 53.9 mo. [95% CI: 35.9-71.9]
not resected 21.9 mo. [95% CI: 17.1-26.7]
HR 0.29 [0.17-0.50], p <0.001
PFS R0 resected 15.4 mo. [95% CI: 11.4-19.5]
not resected 6.9 mo. [95% CI: 5.9-8.0]
HR 0.31 [0.19-0.50]p <0.001
46.2% [29.5-62.9%]
R0 resection vs. no resection:
HR 0.42 [95% CI: 0.21-0.86], p=0.021
Patients with PR/CR,
only
Folprecht et al, ASCO 2013
CELIM trial: Initially irresectable liver mets

Do we need a „proof of concept“ –
in randomised trials?

Resumefor
total of 6
months
Optimal LAAT
(to be determined)non progressive,
non resectable,
oligometastatic
(up to 3 sites/5
lesions) after
any chemo
for 3-6 monthsvtr
ialin
clu
sio
n
Do we need a randomised „strategy“ trialto proof the principle?
Continuation of CT until PD
Rand
Pro
gre
ssio
n

How can we improve this principle?

Consensus molecular subtypes of CRC

0
100
200
300
400
500
600
700
800
900C
EA (
ng/
ml)
CEA
Response by RECIST (CT scan)
Tumor burden (CT-scan)
1 32 4 5 6 7
Montagut, Siravegna & Bardelli . Ann Oncol 2015
cycles of chemotherapy
Consensus molecular subtypes of CRC

0
10
20
30
40
50
60
0
100
200
300
400
500
600
700
800
900
Mu
tate
d a
llele
s (%
)
CEA
(n
g/m
l)
CEA
ctDNA mutation in plasma
Molecular response by liquid
biopsy
Blood draws (ctDNA)
Tumor burden
1 32 4 5 6 7
Response by RECIST (CT scan)
cycles of chemotherapy
Consensus molecular subtypes of CRC
Montagut, Siravegna & Bardelli . Ann Oncol 2015

Methods / Concepts Issues Goals
2008 Liver surgery Technical limitations 5% selected→ „cure“ for about 20%
The spectrum of metastases in CRC: Consequences

Methods / Concepts Issues Goals
2008 Liver surgery Technical limitations 5% selected→ „cure“ for about 20%
2012 Liver surgeryTumour BoardSystemic treatment
Technical improvementPrognosticalconsiderations
20% selected→ „cure“ for about 30%
The spectrum of metastases in CRC: Consequences

Methods / Concepts Issues Goals
2008 Liver surgery Technical limitations 5% selected→ „cure“ for about 20%
2012 Liver surgeryTumour BoardSystemic treatment
Technical improvementPrognosticalconsiderations
20% selected→ „cure“ for about 30%
2016 Concept of oligometastaticdiseaseIntegration of ablativetreatments
New methods / multidisciplinarityNew strategic goals
25% liver mets onlyAbout 60% with „anyoligometastatic disease“
The spectrum of metastases in CRC: Consequences

Methods / Concepts Issues Goals
2008 Liver surgery Technical limitations 5% selected→ „cure“ for about 20%
2012 Liver surgeryTumour BoardSystemic treatment
Technical improvementPrognosticalconsiderations
20% selected→ „cure“ for about 30%
2016 Concept of oligometastaticdiseaseIntegration of ablativetreatments
New methods / multidisciplinarityNew strategic goals
25% liver mets onlyAbout 60% with „anyoligometastatic disease“
>2018 Broad acceptance of the currentconcept – to save lives!
The spectrum of metastases in CRC: Consequences

Methods / Concepts Issues Goals
2008 Liver surgery Technical limitations 5% selected→ „cure“ for about 20%
2012 Liver surgeryTumour BoardSystemic treatment
Technical improvementPrognosticalconsiderations
20% selected→ „cure“ for about 30%
2016 Concept of oligometastaticdiseaseIntegration of ablativetreatments
New methods / multidisciplinarityNew strategic goals
25% liver mets onlyAbout 60% with „anyoligometastatic disease“
>2018 Molecular determination ofpattern of mets.?Tumor → stroma, Immunotherapy?
Broad acceptance of the currentconcept – to save lives!
The spectrum of metastases in CRC: Consequences

Dirk Arnold
Asklepios Tumorzentrum Hamburg
Instituto CUF de Oncologia, Lissabon
Statine
vor und während der Systemtherapie wirken protektiv!
Seicean et al., JACC 2012.


![5 D E D WWH I¾ U . X Q G H Q...7 JFMN FI SLP N N UFTE BSBV GBO TJFJO UFM MJH FO U [V H FTUBMUFO ) JFS[V FJO JH F 7 P S TDI MÅH F 8 P VD W]E H ]R J H Q H 5 D E D WWH & JO FSTUFS"](https://img.pdfslide.org/doc/110x75/5f2aa6b4cd627279f329e37a/5-d-e-d-wwh-i-u-x-q-g-h-q-7-jfmn-fi-slp-n-n-ufte-bsbv-gbo-tjfjo-ufm-mjh.jpg)
![,FK OLHE H ' $ 1 · ,fk olhe h d ovr e lq lfk ,fk e hnhq q h ,fk k d e h j holhe w ' $ 1 . (: lu g d q nhq yr q j d q ]hp + hu]hq iÙu g lh : r uwh g hv 0 lwj hiÙk ov xq g g hu +](https://img.pdfslide.org/doc/110x75/6059abda6395da47bd6ccd78/fk-olhe-h-1-fk-olhe-h-d-ovr-e-lq-lfk-fk-e-hnhq-q-h-fk-k-d-e-h-j-holhe-w.jpg)




![Ostsee 2020 - yaban-travel.de3&*4&5&3.*/& 'sbvfo 8pdifofoef bo efs 0tutff.r p p h p lw x q v i u h lq h q h uk r ovdp h q .x u] x uodx e dq g lh 2 vwvh h = x * dvw lp * uh livz dog](https://img.pdfslide.org/doc/110x75/5e3a0958c1e59b1d8f42bfcd/ostsee-2020-yaban-3453-sbvfo-8pdifofoef-bo-efs-0tutffr.jpg)


![Blaettle 2 2015 · 2019-08-06 · ]>>*q dw\ q*:y 5' ah @] q \dd3 *:y* z 9 h9(ro(0 9x5 2h40( (493 io r"8(iir90 9&(h oroo3 0 ho(h oh 1(48 2hqy=. ]2 *q @= rr]@5 (*r :@:ry*q:]>r](https://img.pdfslide.org/doc/110x75/5f4c495cbf9da5317272970d/blaettle-2-2015-2019-08-06-q-dw-qy-5-ah-q-dd3-y-z-9-h9ro0.jpg)

![R L `R R - Florida State Universityxyuan/paper/98dissertation.pdf · ike]\ z#m1s+iuw&mocgbae q q q q qtq q q q q q qtq q q q q q q qtq q q q q q qtq q q q q q qtq q q q q a iyiyi](https://img.pdfslide.org/doc/110x75/5e7ee2d94f9cb4604b1e970c/r-l-r-r-florida-state-xyuanpaper98dissertationpdf-ike-zm1siuwmocgbae.jpg)

![q Einladung - kinderklinik-datteln.de · R R S H U D W LR Q I U 7 U DQ VS D UH Q ] XQ G 4 XD OLW W LP * H V X Q G K H L W V Z H V H Q e Dienstag, 19. Februar 2019 Seminar 10.30 -](https://img.pdfslide.org/doc/110x75/5d617bf188c993d6258b470b/q-einladung-kinderklinik-r-r-s-h-u-d-w-lr-q-i-u-7-u-dq-vs-d-uh-q-xq-g-4.jpg)






![Z Z Z MX J H Q G LQ IR N a F K e in e r % e a r b e it u n J s ] e it Y R … · 2018-07-05 · Q R H D W MX J H Q G N D U WH K R O V LH G LU ] u m D R Z n OR a d ] u r 9 e r f ü](https://img.pdfslide.org/doc/110x75/5e98cc265dea4f1e3a23bc42/z-z-z-mx-j-h-q-g-lq-ir-n-a-f-k-e-in-e-r-e-a-r-b-e-it-u-n-j-s-e-it-y-r-2018-07-05.jpg)



