Embed Size (px)
Citation preview
Adipositas und Schwangerschaft S. Seeger
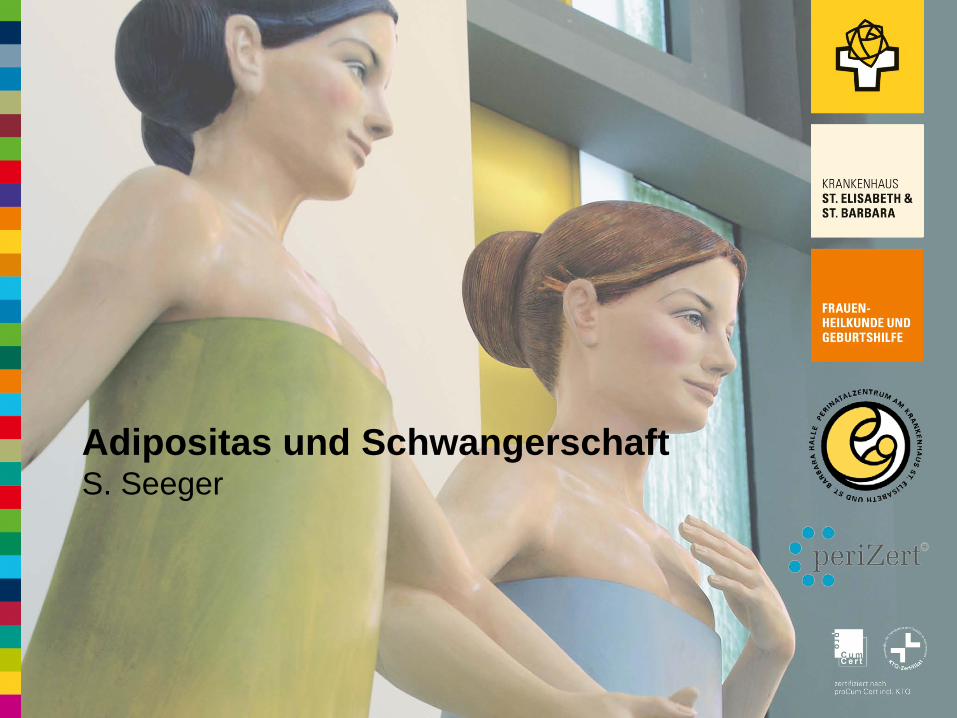
Gewicht bei Schwangeren Sachsen-Anhalt BQS 2013
2
Definition Adipositas in der Schwangerschaft BMI ≥ 30 (mit Beginn der Schwangerschaft)
Erhöhter, aber meist überschätzter Energiemehrbedarf
Gründe für den Energiemehrbedarf: • Wachstum von Kind und Plazenta • Vermehrung und Neubildung von mütterlichem Gewebe • Erhöhter Grundumsatz durch vergrößerte Masse von aktivem Gewebe und erhöhtem Sauerstoff- verbrauch von Plazenta, Uterus und Fetus • Steigende körperliche Belastung
Energiemehrbedarf erst ab II.Trimenon relevant
Energiebedarf in der Schwangerschaft
3
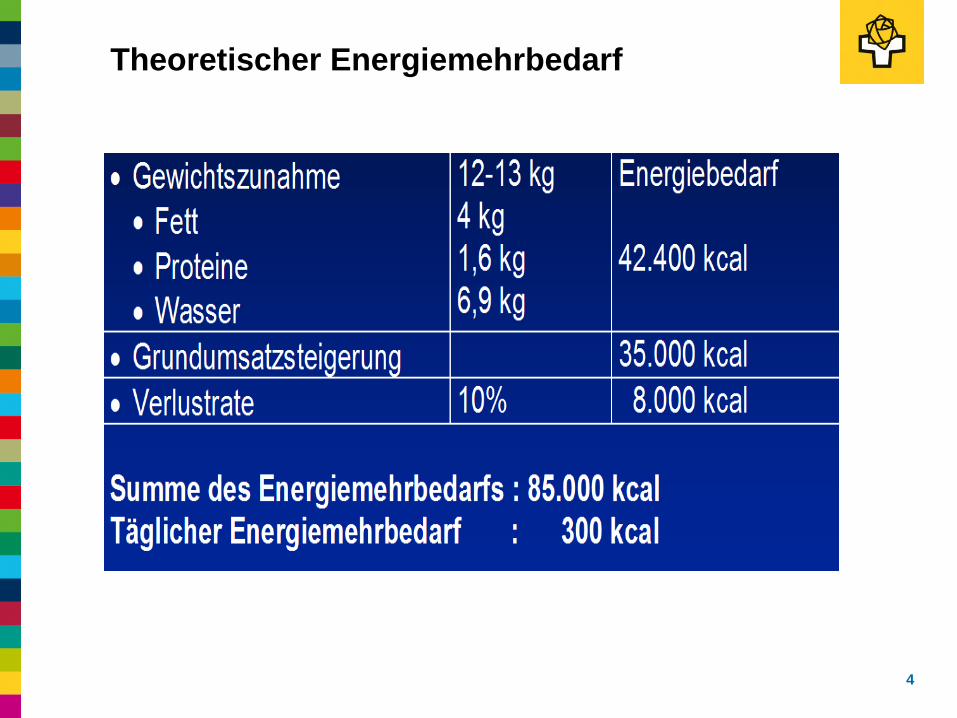
Theoretischer Energiemehrbedarf
4
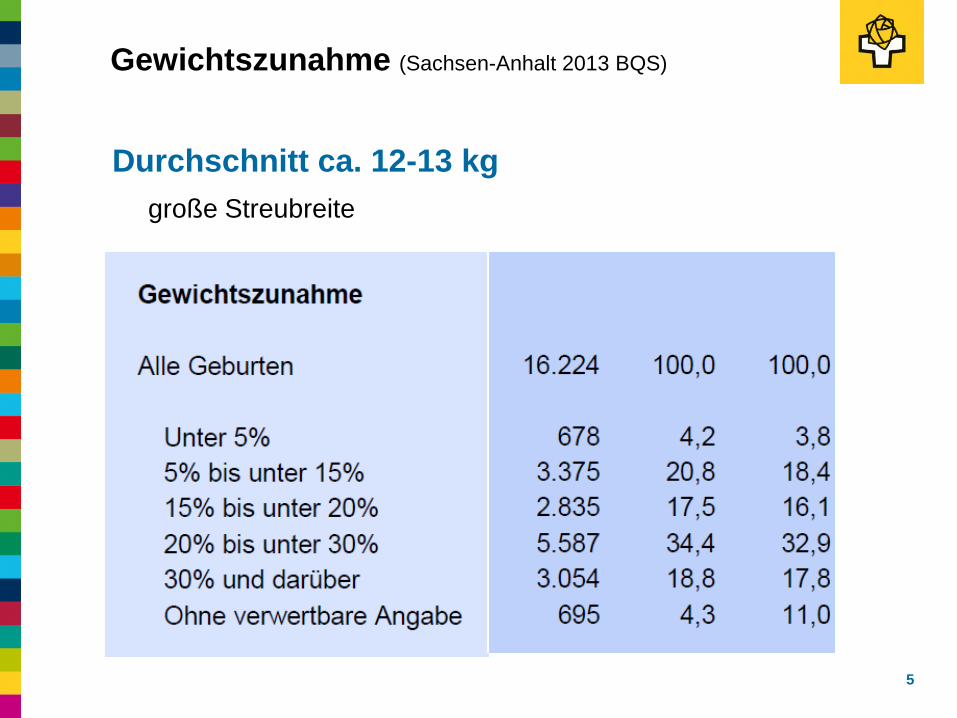
Gewichtszunahme (Sachsen-Anhalt 2013 BQS)
5
Durchschnitt ca. 12-13 kg große Streubreite
6
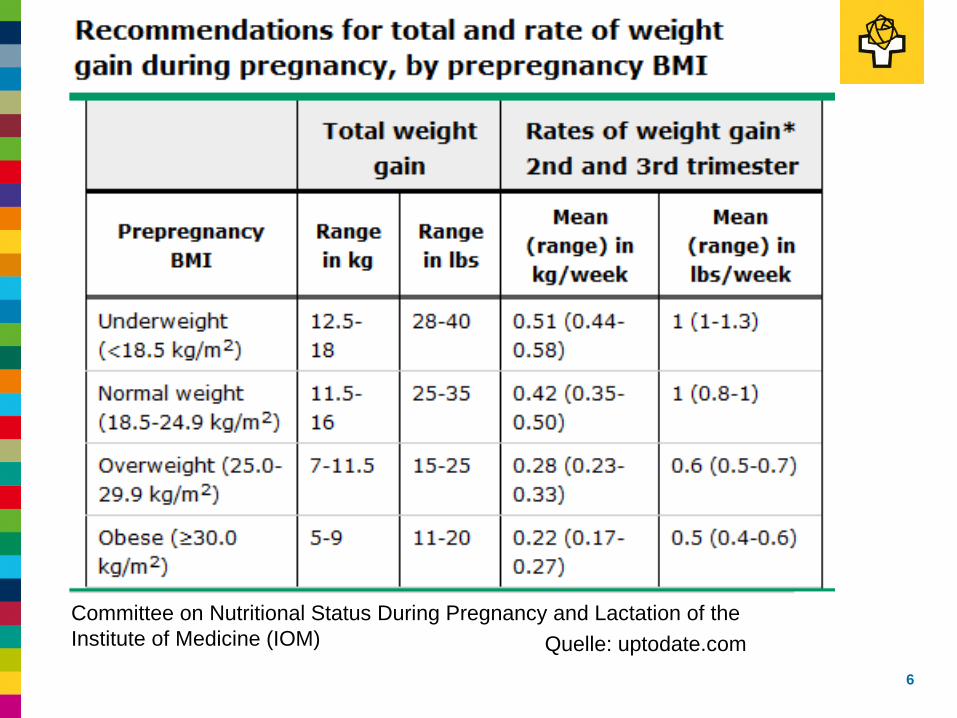
Committee on Nutritional Status During Pregnancy and Lactation of the Institute of Medicine (IOM) Quelle: uptodate.com
Gewichtszunahme / Schwangerschaftsoutcome
7
Hohe Assoziation von maternaler Gewichts-zunahme und Geburtsgewicht des Kindes • (zu) geringe Gewichtszunahme – (zu) geringe Geb.gewicht - > in allen BMI-Gruppen •(zu) hohe Gewichtszunahme – (zu) hohes Geburtsgewicht -> bei unter - oder normgewichtigen Schwangeren
pro kg überdurchschnittlicher mat. Gewichtszunahme 16,7-22,6 g Geburtsgewicht
Intervention während Schwangerschaft verhindert keine fetale Makrosomie
Antenatal lifestyle advice for women who are overweight or obese: LIMIT randomised trial. Dodd JM, Turnbull D, McPhee AJ, Deussen AR, Grivell RM, Yelland LN, Crowther CA, Wittert G, Owens JA, Robinson JS, ;BMJ. 2014;348:g1285.
8
To determine the effect of antenatal dietary and lifestyle interventions on health outcomes in overweight and obese pregnant women. 1.108 women comprehensive dietary and lifestyle intervention delivered by research staff; 1.104 women standard care and received pregnancy care according to local guidelines RESULTS: The risk of the infant being large for gestational age was not significantly different in the two groups (lifestyle advice 203/1075 (19%) v standard care 224/1067 (21%); OR 0.90, 95% CI0.77 to 1.07; P=0.24).
Infants born to women after lifestyle advice were significantly less likely to have birth weight above 4000 g (lifestyle advice 164/1075 (15%) v standard care 201/1067 (19%); (OR 0.82, 0.68 to 0.99; NNT 28, 15 to 263; P=0.04). There were no differences in maternal pregnancy and birth outcomes between the two groups. CONCLUSIONS: For women who were overweight or obese, the antenatal lifestyle advice used in this study did not reduce the risk delivering a baby weighing above the 90th centile for gestational age and sex or improve maternal pregnancy and birth outcomes.
Schwangerschafts- und Geburtsrisiken bei Übergewicht
9
Risiko - Fehlgeburt
10
Frauen mit Übergewicht haben häufiger Fehlgeburten (Dodd et al, 2014)
BMI < 25 10,7 % BMI 25-29 11,8 % OR 1,11 BMI ≥ 30 16,6 % OR 1,31 Zusammenhang zur Kausalität des Übergewichtes z.B. PCO Abortrisiko OR 1,2 – 1,4 z.B. metabol. Syndrom; erhöhte Insulinresistenz
Does obesity increase the risk of miscarriage in spontaneous conception: a systematic review. Boots C, Stephenson MD; Semin Reprod Med. 2011 Nov;29(6):507-13. Epub 2011 Dec 8
11
Method: Data were compared for obese (body mass index [BMI]:≥28 or 30 kg/m (2)), overweight (BMI: 25 to 29 kg/m (2)), and normal-weight (BMI:<25 kg/m (2)) women, with pooled odds ratios (ORs). Six studies met the criteria for a cohort of 28,538 women. Results: Higher miscarriage rate of 13.6% in 3.800 obese versus 10.7% in 17.146 normal-BMI women - OR: 1.31 (95% confidence interval [CI], 1.18 to 1.46). Higher prevalence of recurrent early miscarriage in obese versus normal-BMI women (0.4% versus 0.1%; OR: 3.51 (95% CI, 1.03 to 12.01).
In women with recurrent miscarriage, there was a higher miscarriage rate in the obese versus non obese women (46% versus 43%; OR: 1.71; 95% CI, 1.05). Conclusion: Obesity is associated with a higher miscarriage rate in women who conceive spontaneously. Larger prospective studies are urgently needed to verify these preliminary results.
Does high BMI increase the risk of miscarriage after spontaneous and assisted conception? A meta-analysis of the evidence. Metwally M, Ong KJ, Ledger WL, Li TC; Fertil Steril. 2008;90(3):714.
12
The Academic Unit of Reproductive and Developmental Medicine, The University of Sheffield, United Kingdom. PATIENT(S): Obese and overweight patients who had miscarriage after spontaneous or assisted conception, compared with patients with a normal body mass index. RESULT(S): Sixteen studies were included in the meta-analysis.
Patients with a body mass index of>or =25 kg/m(2) had significantly higher odds of miscarriage, regardless of the method of conception (odds ratio, 1.67; 95% confidence interval, 1.25-2.25). Subgroup analysis from a limited number of studies suggested that this group of women may also have significantly higher odds of miscarriage after oocyte donation (odds ratio, 1.52; 95% confidence interval, 1.10-2.09) and ovulation induction (odds ratio, 5.11; 95% confidence interval, 1.76-14.83). There was no evidence for increased odds of miscarriage after IVF-intracytoplasmic sperm injection. CONCLUSION(S): There is evidence that obesity may increase the general risk of miscarriage. However, there is insufficient evidence to describe the effect of obesity on miscarriage in specific groups such as those conceiving after assisted conception.
Risiko Gestationsdiabetes / Typ II Diabetes
13
Frauen mit Übergewicht haben eine höhere Wahr- scheinlichkeit für einen Gestationsdiabetes • Bei Übergewicht steigt die Wahrscheinlichkeit um 0,92% pro BMI Punkt
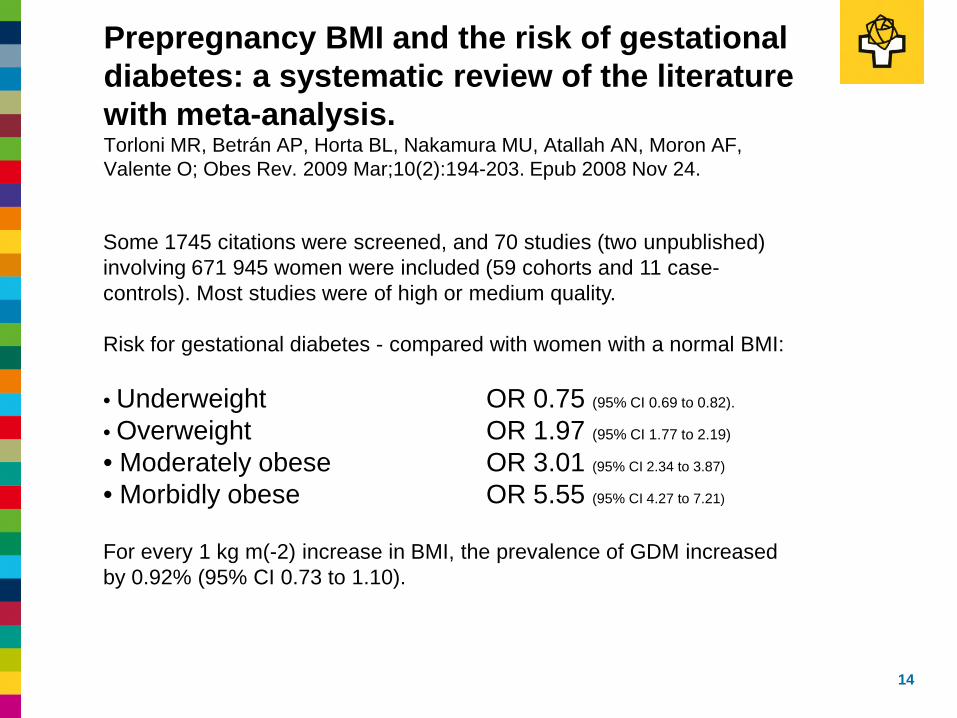
Prepregnancy BMI and the risk of gestational diabetes: a systematic review of the literature with meta-analysis. Torloni MR, Betrán AP, Horta BL, Nakamura MU, Atallah AN, Moron AF, Valente O; Obes Rev. 2009 Mar;10(2):194-203. Epub 2008 Nov 24.
14
Some 1745 citations were screened, and 70 studies (two unpublished) involving 671 945 women were included (59 cohorts and 11 case-controls). Most studies were of high or medium quality. Risk for gestational diabetes - compared with women with a normal BMI: • Underweight OR 0.75 (95% CI 0.69 to 0.82).
• Overweight OR 1.97 (95% CI 1.77 to 2.19)
• Moderately obese OR 3.01 (95% CI 2.34 to 3.87)
• Morbidly obese OR 5.55 (95% CI 4.27 to 7.21)
For every 1 kg m(-2) increase in BMI, the prevalence of GDM increased by 0.92% (95% CI 0.73 to 1.10).
Gestationsdiabetes
Definition GDM : Glucosetoleranzstörung in der Schwangerschaft Klare Abgrenzung vom manifesten Diabetes BZ > 11,1 mmol/l (200mg/dl) im 50g-Screening oder im 2 Std. Wert nach 75g oGTT
GDM-Inzidenz: lt. BQS 2011: 4,4% (28.200 Fälle) Geschätzte Inzidenz des GDM ca. 6% (2-20%) weiter hohe Dunkelziffer (mind. 25-50%) OR 2,8 (95% CI 2,54-3,08)
16
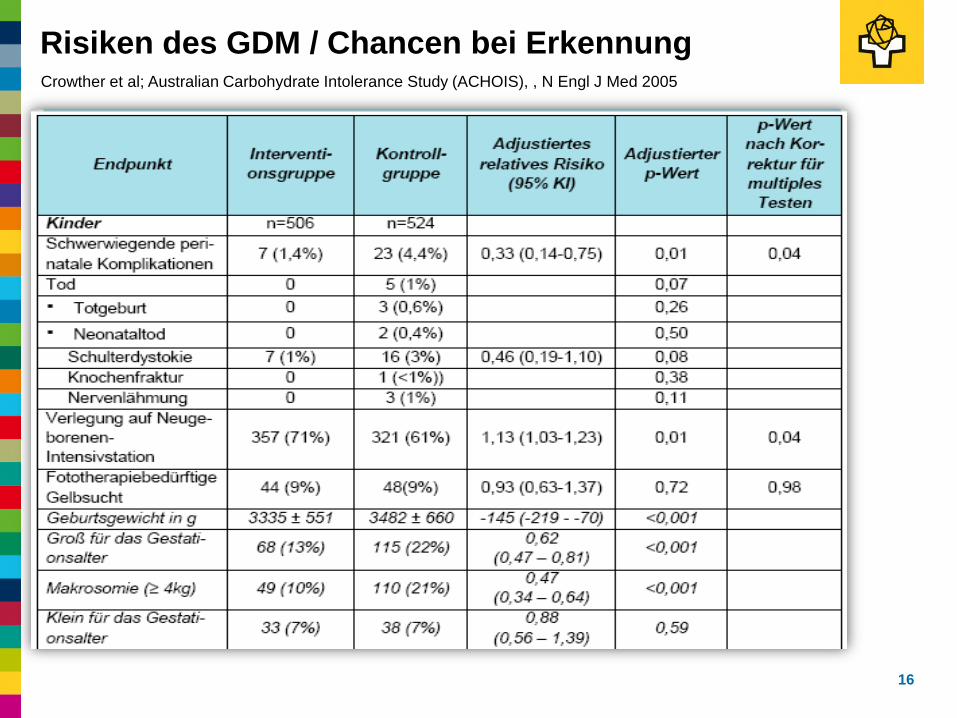
Risiken des GDM / Chancen bei Erkennung Crowther et al; Australian Carbohydrate Intolerance Study (ACHOIS), , N Engl J Med 2005
17
Screening im Nichtrisikokollektiv!
„Einstufenkonzept“: primär 75g-oGTT
„Zweistufenkonzept“: initial 50g-Glucose-Screening wenn BZ > 7,5 mmol/l (135g/dl) sekundär 75g-oGTT(27%)
Zeitraum 24+0 bis 27+6 SSW
Leitlinie Diagnostik und Therapie des Gestationsdiabetes der DGGG mit Empfehlung zum generellen Screening (Stand 2008)
18
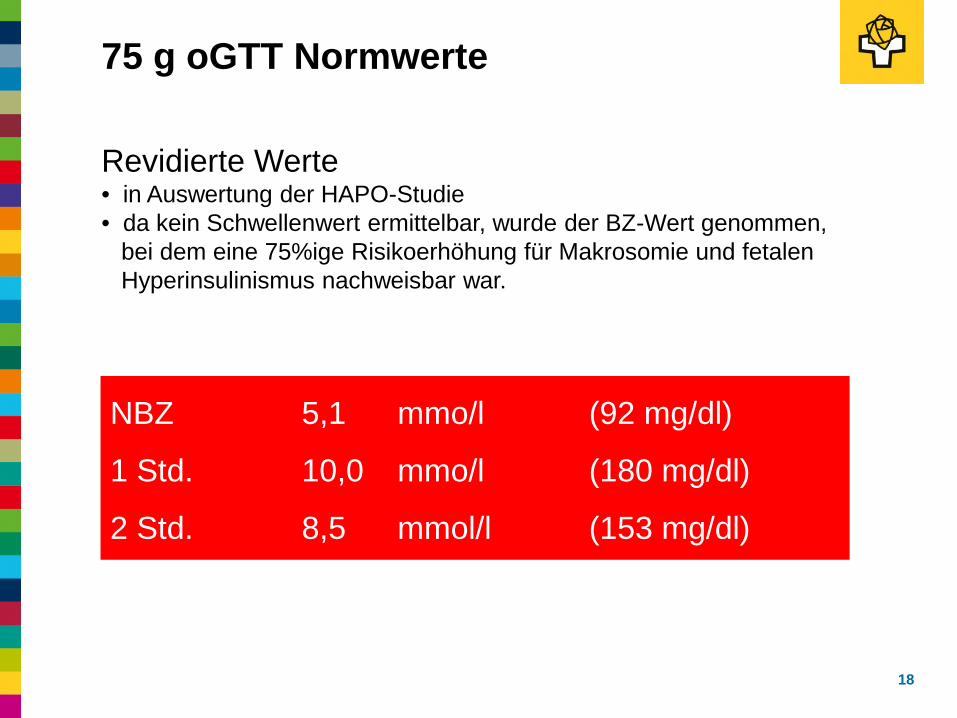
75 g oGTT Normwerte
Revidierte Werte • in Auswertung der HAPO-Studie • da kein Schwellenwert ermittelbar, wurde der BZ-Wert genommen, bei dem eine 75%ige Risikoerhöhung für Makrosomie und fetalen Hyperinsulinismus nachweisbar war.
NBZ 5,1 mmo/l (92 mg/dl)
1 Std. 10,0 mmo/l (180 mg/dl)
2 Std. 8,5 mmol/l (153 mg/dl)
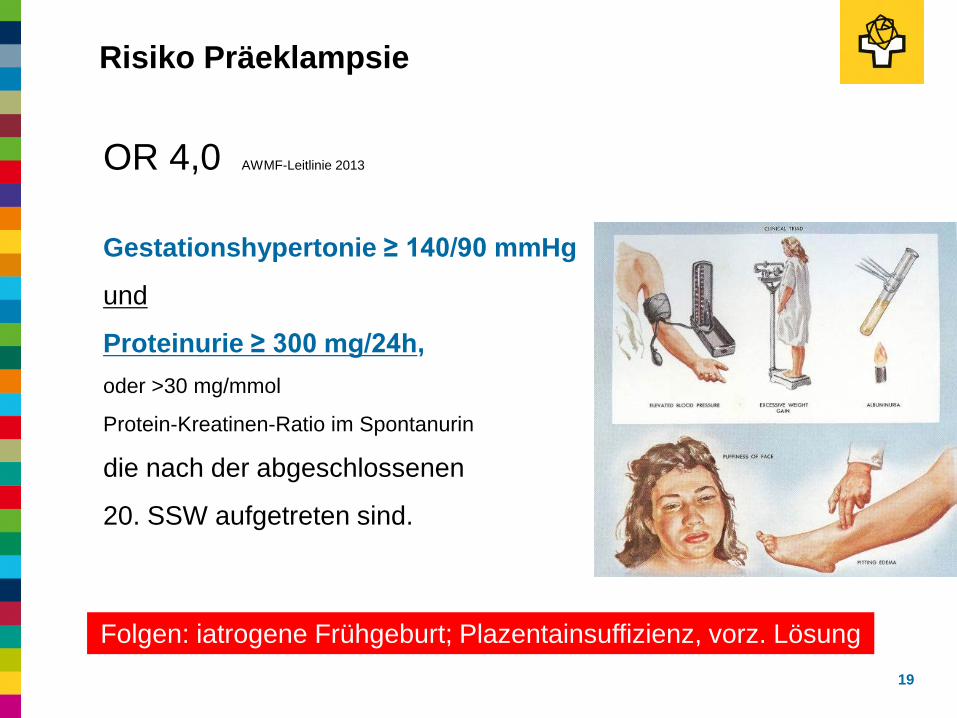
Risiko Präeklampsie
19
Gestationshypertonie ≥ 140/90 mmHg
und
Proteinurie ≥ 300 mg/24h, oder >30 mg/mmol
Protein-Kreatinen-Ratio im Spontanurin
die nach der abgeschlossenen
20. SSW aufgetreten sind.
OR 4,0 AWMF-Leitlinie 2013
Folgen: iatrogene Frühgeburt; Plazentainsuffizienz, vorz. Lösung
Risiko iatrogener Frühgeburt OR 1,30 (95% CI 1,23-1,37) Mc Donald et. Al ; BMJ. 2010;341:c3428.
• in Folge von Schwangerschaftskomplikationen (PE, Diabetes)
Risiko spontaner Frühgeburt • in Folge von sozioökonomischer Unterschiede
(Schwangerenvorsorge; Harnwegsinfektionen (OR 1,42) …
• bei BMI < 35 ist Risiko für Geburt <37. SSW nicht erhöht: OR 0,87 (95% CI 0,74-1,04) aber für Risiko früher und sehr früher Frühgeburt
Risiko Frühgeburt
20
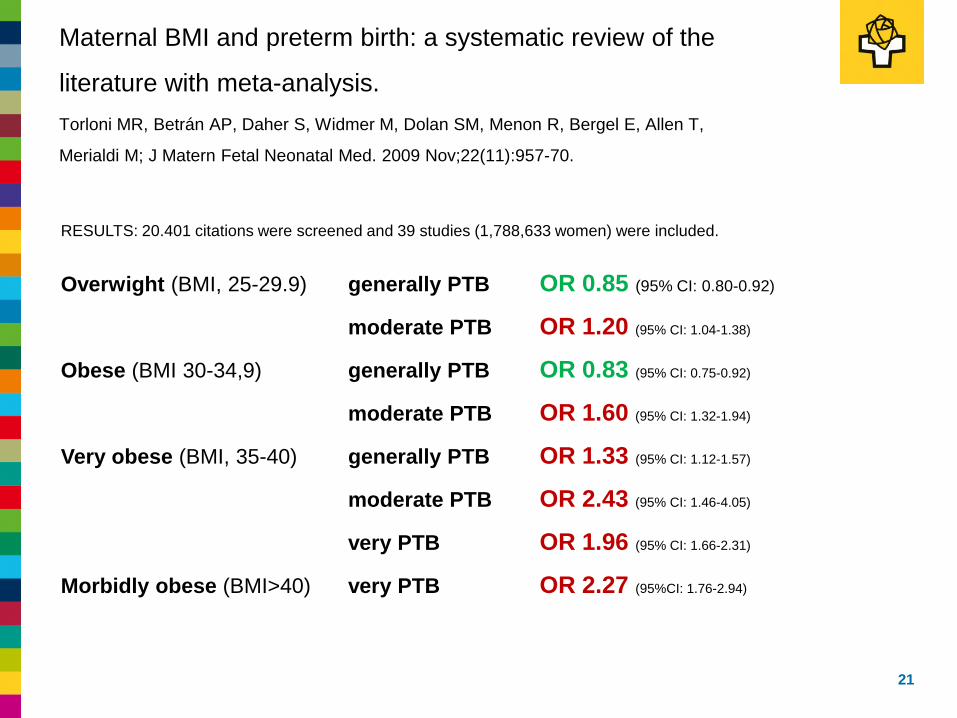
Maternal BMI and preterm birth: a systematic review of the
literature with meta-analysis. Torloni MR, Betrán AP, Daher S, Widmer M, Dolan SM, Menon R, Bergel E, Allen T,
Merialdi M; J Matern Fetal Neonatal Med. 2009 Nov;22(11):957-70.
21
RESULTS: 20.401 citations were screened and 39 studies (1,788,633 women) were included.
Overwight (BMI, 25-29.9) generally PTB OR 0.85 (95% CI: 0.80-0.92)
moderate PTB OR 1.20 (95% CI: 1.04-1.38)
Obese (BMI 30-34,9) generally PTB OR 0.83 (95% CI: 0.75-0.92)
moderate PTB OR 1.60 (95% CI: 1.32-1.94)
Very obese (BMI, 35-40) generally PTB OR 1.33 (95% CI: 1.12-1.57)
moderate PTB OR 2.43 (95% CI: 1.46-4.05)
very PTB OR 1.96 (95% CI: 1.66-2.31)
Morbidly obese (BMI>40) very PTB OR 2.27 (95%CI: 1.76-2.94)
Wahrscheinlichkeit für Übertragungen OR 1,2 - 1,7
Übertragungen
22
Kausalität unklar: • Verrechnungen (schlechte US-Sicht; verlängerter Zyklus … • hormonale Geburtsauslösung verzögert ?
Adipositas per se keine Sectioindikation, aber: • Erschwerte fetale Überwachung
• Längere Eröffnungsperiode
(BM I <26: 6,2 h – BM I 26-29: 7,5h – BMI >29: 7,9 h) Vahratian et al., Maternal prepregnancy overweight and obesity and the pattern of labor progression in term nulliparous women.; Obstet Gynecol. 2004;104(5 Pt 1):943.
• Schulterdystokie OR 1,51 (95% CI 1,33-1,74)
• Möglichst keine dringliche (Not-) Sectio
Entbindungsmodus
23
Wenn Kaiserschnitt, dann • Längere Vorbereitung
(Spezial-Tisch; Instrumente …) • Größeres Team • Anästhesieprobleme:
SPA/PDA; periphere Zugänge; Probleme Maskenbeatmung …
• Längere OP-Dauer • Längere E-E-Zeit bei Not-Sectio • Mehr Blutverlust >1.000 ml
(OR 1,44; 95% CI 1,30-1,60), Sebire et al. 2001
• p.o. Probleme: Wundinfektionen; Endometritis; Thrombembolie
Entbindungsmodus
24
• Stillen • Späterer Laktationsbeginn, kürzere Stilldauer ?
• Venöse Thrombembolien • Wundinfektionen • Postpartale Blutungen
Probleme post partum
25
Erschwerte Pränataldiagnostik
26
„Synchrone (Weiter)Entwicklung von Ultraschalltechnik und BMI“
Detektionsrate mind. 20% geringer (uptodate 2015)
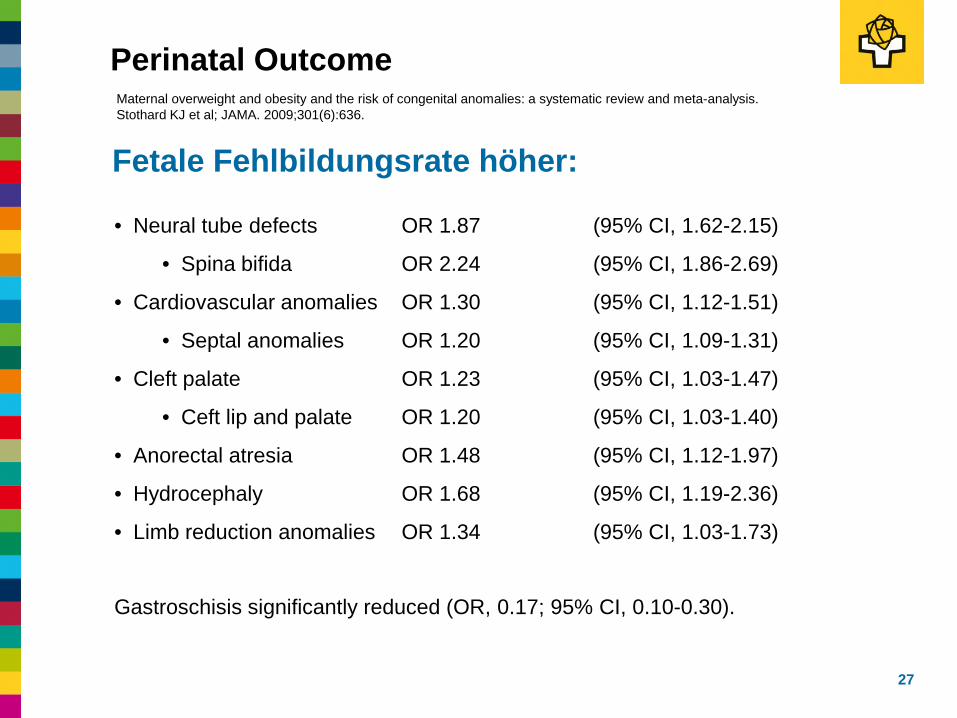
Fetale Fehlbildungsrate höher:
Perinatal Outcome
27
• Neural tube defects OR 1.87 (95% CI, 1.62-2.15)
• Spina bifida OR 2.24 (95% CI, 1.86-2.69)
• Cardiovascular anomalies OR 1.30 (95% CI, 1.12-1.51)
• Septal anomalies OR 1.20 (95% CI, 1.09-1.31)
• Cleft palate OR 1.23 (95% CI, 1.03-1.47)
• Ceft lip and palate OR 1.20 (95% CI, 1.03-1.40)
• Anorectal atresia OR 1.48 (95% CI, 1.12-1.97)
• Hydrocephaly OR 1.68 (95% CI, 1.19-2.36)
• Limb reduction anomalies OR 1.34 (95% CI, 1.03-1.73) Gastroschisis significantly reduced (OR, 0.17; 95% CI, 0.10-0.30).
Maternal overweight and obesity and the risk of congenital anomalies: a systematic review and meta-analysis. Stothard KJ et al; JAMA. 2009;301(6):636.
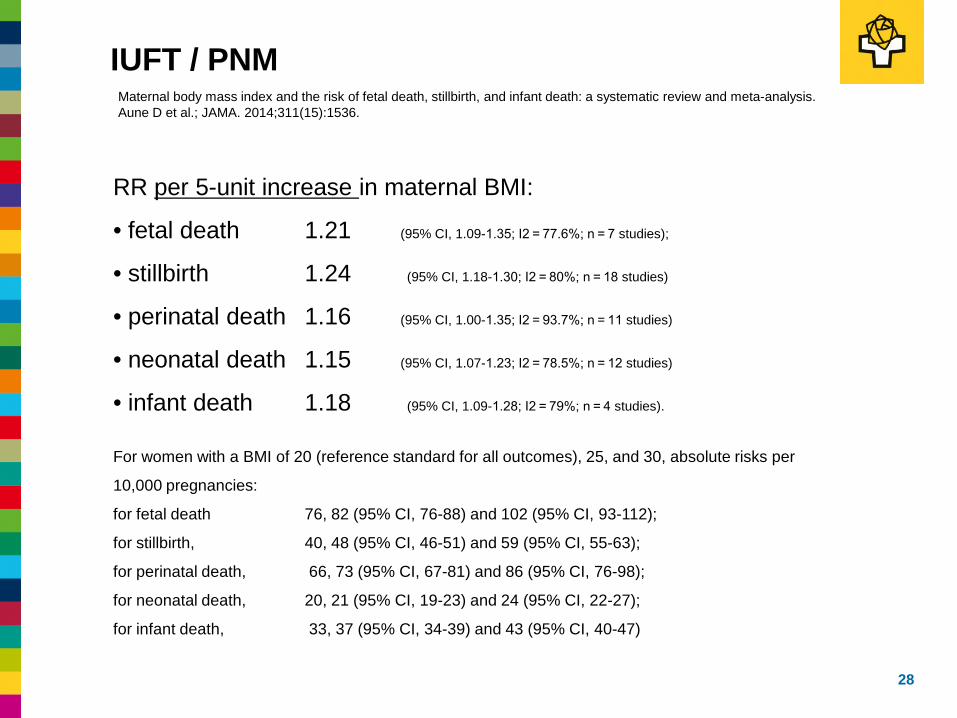
IUFT / PNM
28
Maternal body mass index and the risk of fetal death, stillbirth, and infant death: a systematic review and meta-analysis. Aune D et al.; JAMA. 2014;311(15):1536.
RR per 5-unit increase in maternal BMI:
• fetal death 1.21 (95% CI, 1.09-1.35; I2 = 77.6%; n = 7 studies);
• stillbirth 1.24 (95% CI, 1.18-1.30; I2 = 80%; n = 18 studies)
• perinatal death 1.16 (95% CI, 1.00-1.35; I2 = 93.7%; n = 11 studies)
• neonatal death 1.15 (95% CI, 1.07-1.23; I2 = 78.5%; n = 12 studies)
• infant death 1.18 (95% CI, 1.09-1.28; I2 = 79%; n = 4 studies).
For women with a BMI of 20 (reference standard for all outcomes), 25, and 30, absolute risks per
10,000 pregnancies:
for fetal death 76, 82 (95% CI, 76-88) and 102 (95% CI, 93-112);
for stillbirth, 40, 48 (95% CI, 46-51) and 59 (95% CI, 55-63);
for perinatal death, 66, 73 (95% CI, 67-81) and 86 (95% CI, 76-98);
for neonatal death, 20, 21 (95% CI, 19-23) and 24 (95% CI, 22-27);
for infant death, 33, 37 (95% CI, 34-39) and 43 (95% CI, 40-47)
• Adipositas: BMI ≥30 bei Schwangerschaftsbeginn • Fett ist endokrines Organ. Höhere Insulinresistenz ist
assoziiert mit Fertilitäts- und Reproduktions- problemen • Im Vergleich zu normgewichtigen Frauen kommen relevante
Schwangerschaftskomplikationen häufiger vor: • Fehlgeburt / Totgeburt / Neonatale Mortalität • Diabetes mellitus / Gestationsdiabetes / Präeklampsie • Geburtskomplikationen: Schulterdystokie, Sectiorate
• Eine Gewichtsreduktion vor Schwanger führt zu reduziert diese Probleme, eine Reduktion in der Schwangerschaft jedoch nicht
• Bei LGA Kindern sind Langzeiteffekte durch „fetale Programmierung“ bekannt
• Kardiovaskul. Risiko; Atopien; Diabetes; Adipositas
Zusammenfassung
29

30
„Den Schritt ins Leben kompetent und zugewandt begleiten“