Embed Size (px)
Citation preview

Bedeutung des Schilddrüsenhormonsystems für die Diagnostik und Therapie Affektiver
Störungen
Michael Bauer
Universitätsklinikum Carl Gustav Carus DresdenKlinik und Poliklinik für Psychiatrie und Psychotherapie
E. T. Kocher Dtsch. Z. Chir, 1874
• Erkrankungen der Schilddrüse können zu schweren psychiatrischen Störungen führen 1888 Clinical Society of London - Report on Myxedema
• 1891 Murray (England) - Erfolgreiche Behandlung des Myxödems mit getrockneten Schilddrüsenextrakten (Schaf)
• 1936 Gjessing (Norwegen) - Erfolgreiche Behandlung der Periodischen Katatonie mit Schilddrüsenextrakten (Schaf)
Geschichte
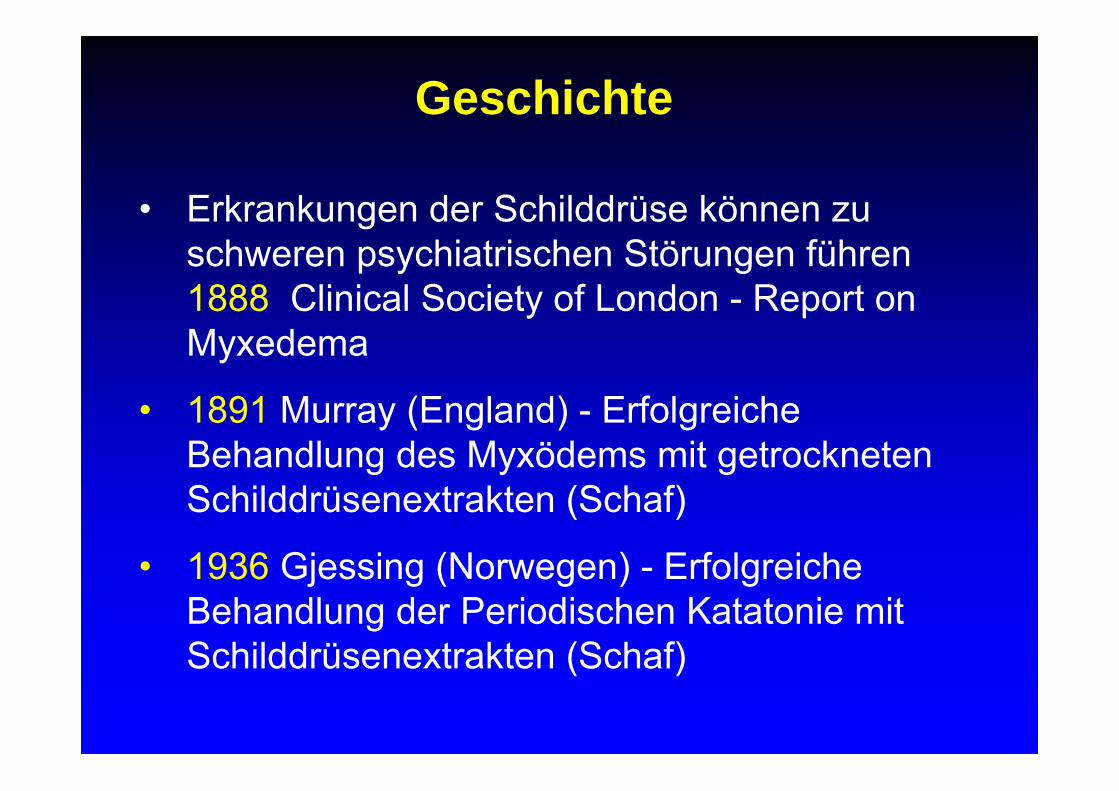
Regelkreis des Schilddrüsensystems: Neuroregulatorischer Negativer Feedback Loop
Schilddrüse
negativeRückkopplung
Hypothalamus
Hypophyse
TRH
TSH
T3, Thyroxin (T4) 1952
1963
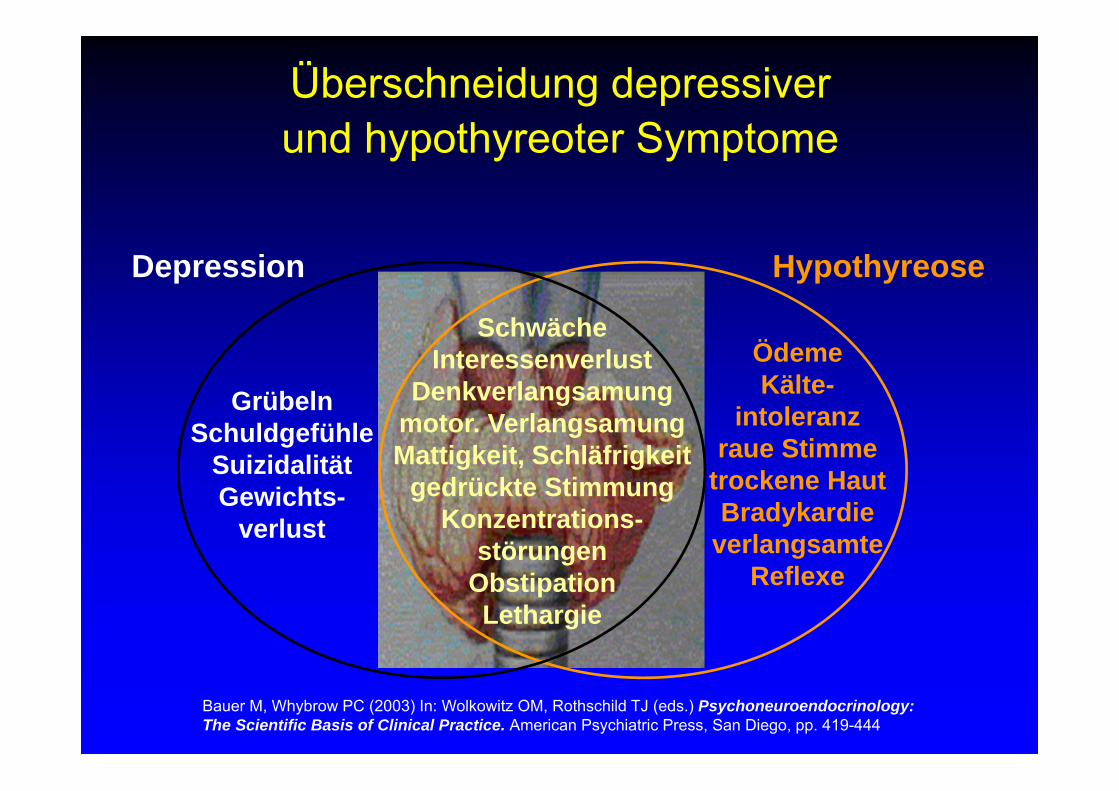
Überschneidung depressiverund hypothyreoter Symptome
HypothyreoseDepression
SchwächeInteressenverlust
Denkverlangsamungmotor. VerlangsamungMattigkeit, Schläfrigkeit
gedrückte Stimmung Konzentrations-
störungenObstipationLethargie
ÖdemeKälte-
intoleranzraue Stimme
trockene HautBradykardie
verlangsamte Reflexe
GrübelnSchuldgefühle
Suizidalität Gewichts-
verlust
Bauer M, Whybrow PC (2003) In: Wolkowitz OM, Rothschild TJ (eds.) Psychoneuroendocrinology: The Scientific Basis of Clinical Practice. American Psychiatric Press, San Diego, pp. 419-444
• T4/T3 essentiell für ZNS-Entwicklung
• Kretinismus, Oligophrenie
• TSH Neugeborenen-Screening
Assoziation des Schilddrüsensystems mit ZNS-Entwicklung
Bauer M, Whybrow PC (2003) In: Wolkowitz OM, Rothschild TJ (eds.) Psychoneuroendocrinology: The Scientific Basis of Clinical Practice. American Psychiatric Press, San Diego, pp. 419-444
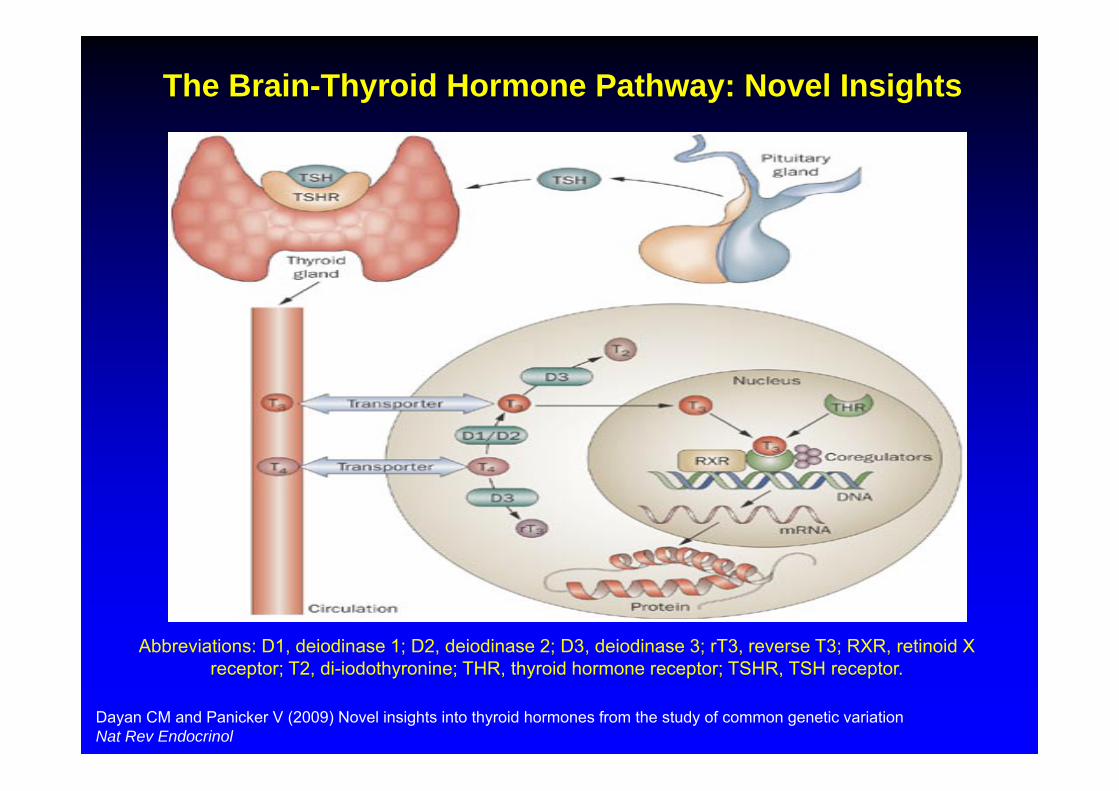
Abbreviations: D1, deiodinase 1; D2, deiodinase 2; D3, deiodinase 3; rT3, reverse T3; RXR, retinoid X receptor; T2, di-iodothyronine; THR, thyroid hormone receptor; TSHR, TSH receptor.
The Brain-Thyroid Hormone Pathway: Novel Insights
Dayan CM and Panicker V (2009) Novel insights into thyroid hormones from the study of common genetic variation Nat Rev Endocrinol
Wegen der Symptomüberschneidung und potentiellen Reversibilität psychiatrischer Symptomatik (Depression, Demenz) der
Hypothyreose ist die Untersuchung des
Schilddrüsensystems von heuristischem Wert fuer die Pathophysiologie psychiatrischer Erkrankungen
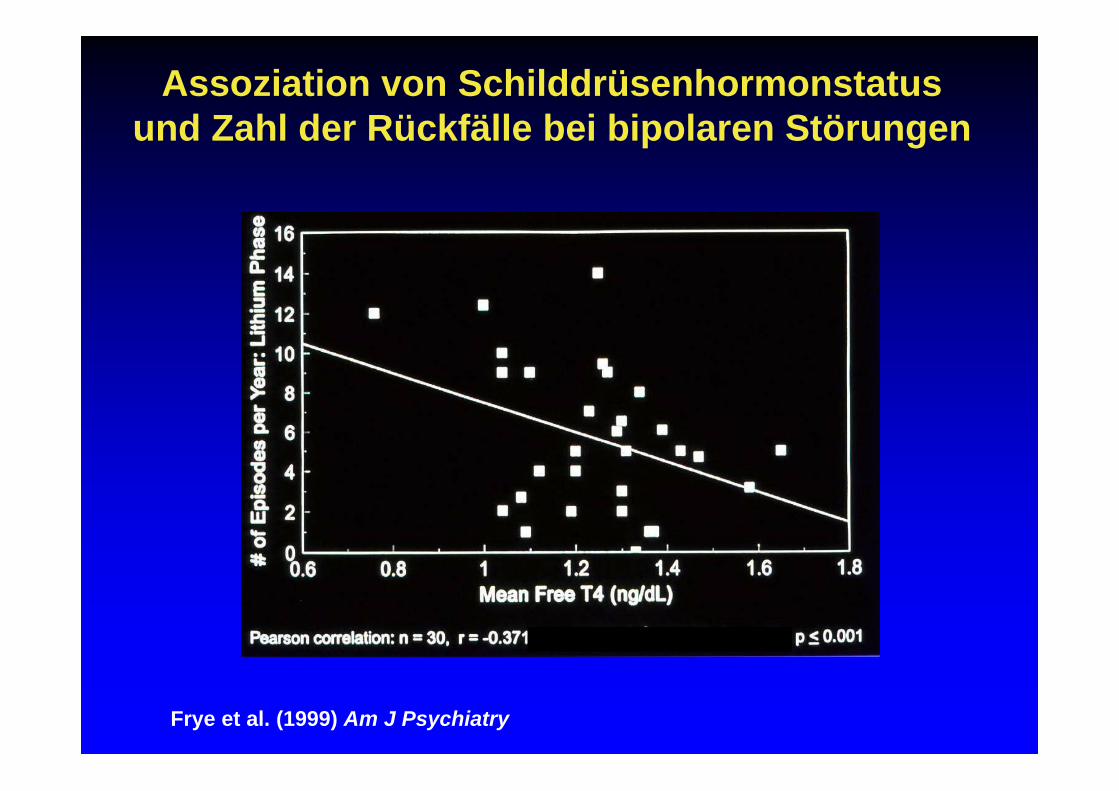
Frye et al. (1999) Am J Psychiatry
Assoziation von Schilddrüsenhormonstatus und Zahl der Rückfälle bei bipolaren Störungen
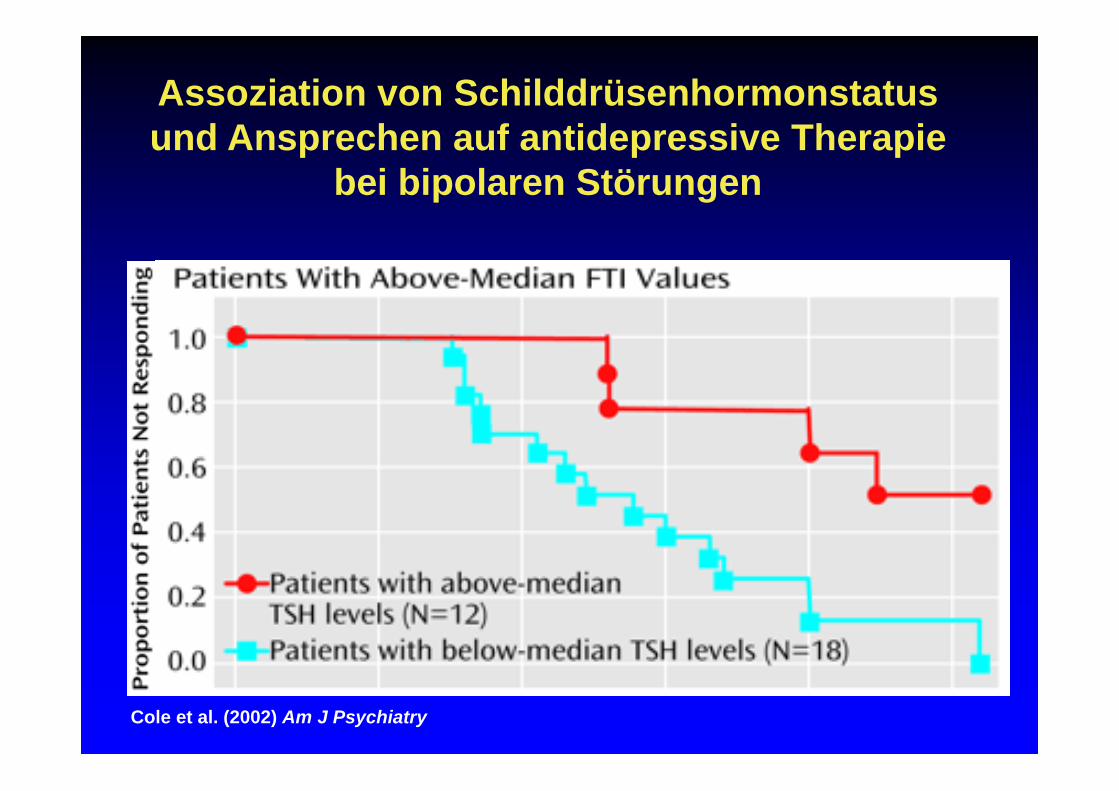
Cole et al. (2002) Am J Psychiatry
Assoziation von Schilddrüsenhormonstatus und Ansprechen auf antidepressive Therapie
bei bipolaren Störungen
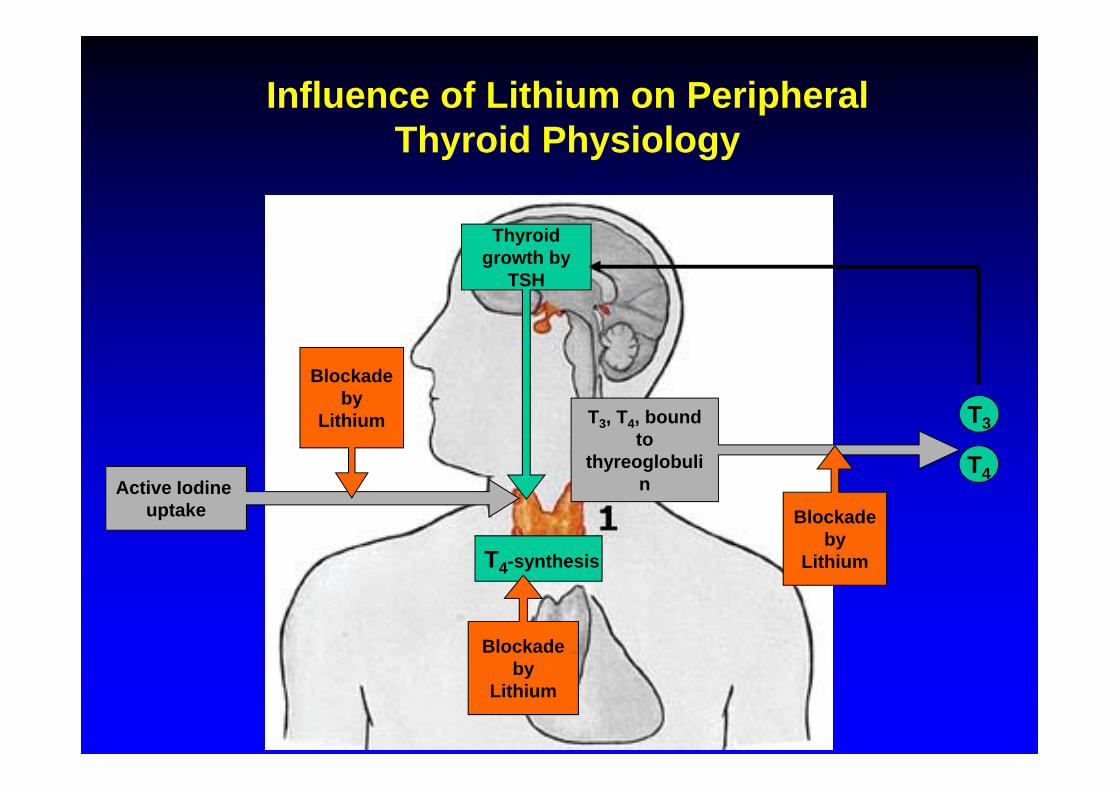
Influence of Lithium on Peripheral Thyroid Physiology
Active Iodine uptake
Blockade by
Lithium T3, T4, bound to
thyreoglobulin
Blockade by
Lithium
T3
T4
T4-synthesis
Blockade by
Lithium
Thyroid growth by
TSH
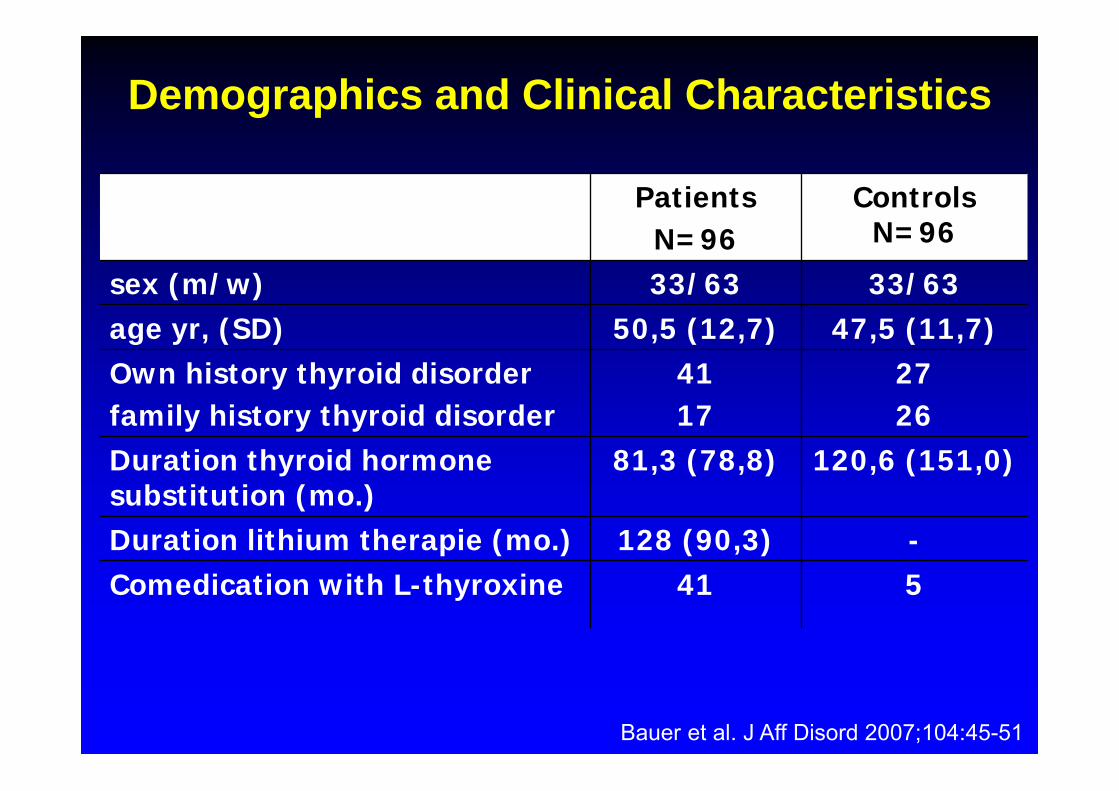
Demographics and Clinical Characteristics
PatientsN=96
Controls N=96
sex (m/w) 33/63 33/63age yr, (SD) 50,5 (12,7) 47,5 (11,7)Own history thyroid disorderfamily history thyroid disorder
4117
2726
Duration thyroid hormone substitution (mo.)
81,3 (78,8) 120,6 (151,0)
Duration lithium therapie (mo.) 128 (90,3) -Comedication with L-thyroxine 41 5
Bauer et al. J Aff Disord 2007;104:45-51
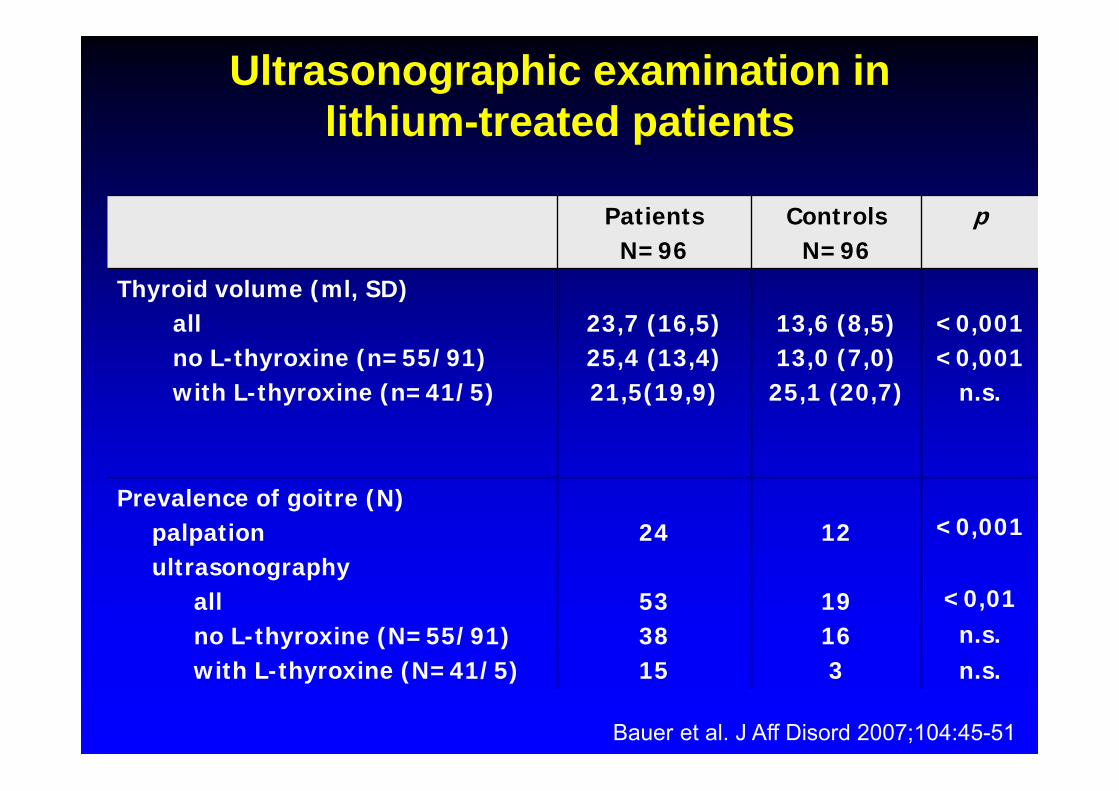
Ultrasonographic examination in lithium-treated patients
PatientsN=96
ControlsN=96
p
Thyroid volume (ml, SD)allno L-thyroxine (n=55/91)with L-thyroxine (n=41/5)
23,7 (16,5)25,4 (13,4)21,5(19,9)
13,6 (8,5)13,0 (7,0)
25,1 (20,7)
<0,001<0,001
n.s.
Prevalence of goitre (N)palpationultrasonography
allno L-thyroxine (N=55/91)with L-thyroxine (N=41/5)
24
533815
12
19163
<0,001
<0,01n.s.n.s.
Bauer et al. J Aff Disord 2007;104:45-51
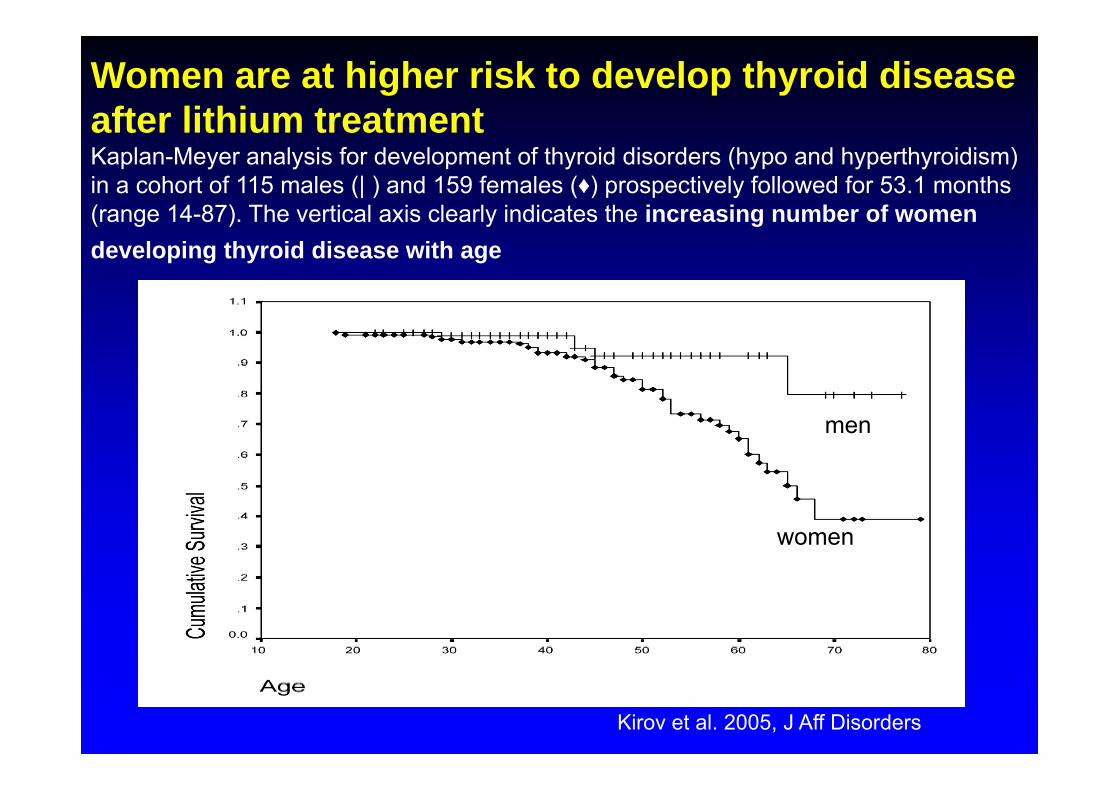
Women are at higher risk to develop thyroid disease after lithium treatment Kaplan-Meyer analysis for development of thyroid disorders (hypo and hyperthyroidism) in a cohort of 115 males (| ) and 159 females (♦) prospectively followed for 53.1 months (range 14-87). The vertical axis clearly indicates the increasing number of women developing thyroid disease with age
Kirov et al. 2005, J Aff Disorders
women
men
• Sind Patienten mit Rapid Cycling Bipolarer Störung sensitiver gegenüber einem Challenge-Test mit Lithium?
• 20 unmedizierte Patienten mit RC-BD vs. 20 (gematcht für Alter und Geschlecht)
• 4 Wochen Lithium-Therapie (> 0.5 mmol/L)
• SD-Funktionstests, TRH Stimulationstest
Lithium Challenge Studie
Gyulai, Bauer, Whybrow et al. (2003) Biol Psychiatry 53:899-905
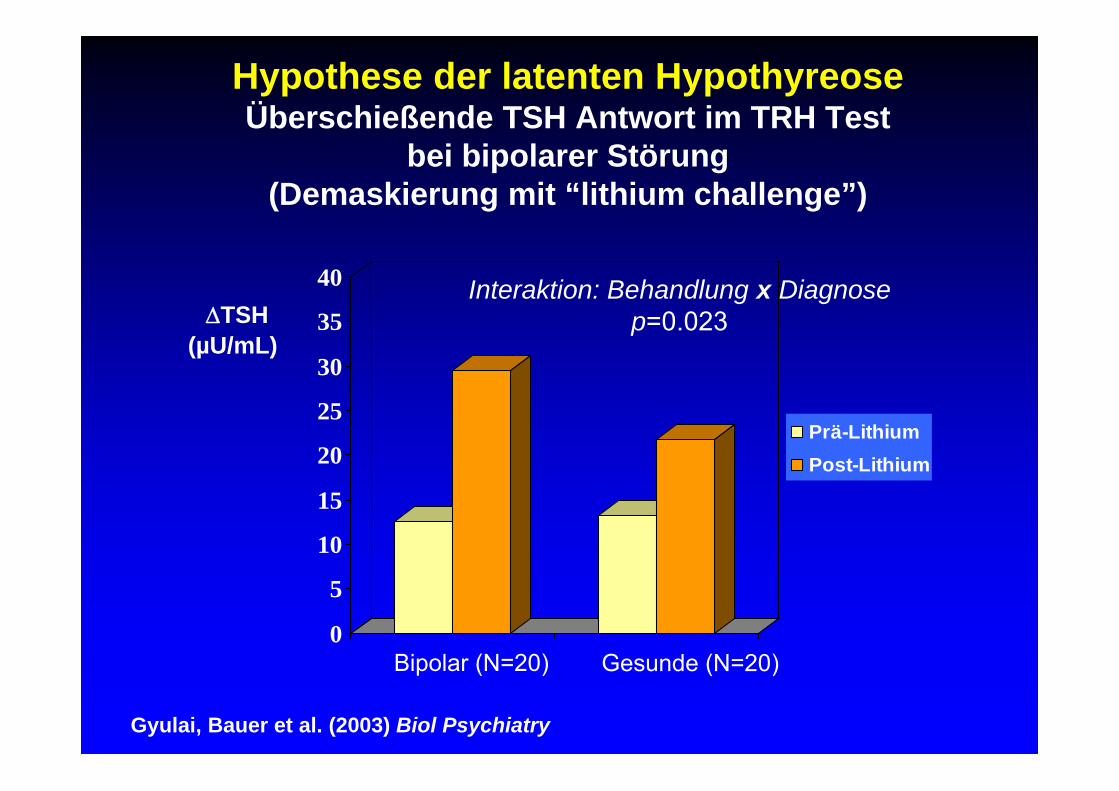
Hypothese der latenten HypothyreoseÜberschießende TSH Antwort im TRH Test
bei bipolarer Störung (Demaskierung mit “lithium challenge”)
0
5
10
15
20
25
30
35
40
Prä-LithiumPost-Lithium
TSH(µU/mL)
Bipolar (N=20) Gesunde (N=20)
Interaktion: Behandlung x Diagnose p=0.023
Gyulai, Bauer et al. (2003) Biol Psychiatry
• Accelerationsbehandlung (T3) (Wirkungsbeschleunigung AD, Akuttherapie)
• Augmentation (T3, L-T4)(Wirkungsverstärkung AD, Akuttherapie)
• Adjuvante Phasenprophylaxe (L-T4) (Wirkungsverstärkung Mood Stabilizer)
Schilddrüsenhormone als Stimmungsmodulatoren
Bauer M, Whybrow PC (2002) Thyroid Hormone, Brain and Behavior. In: Pfaff DW et al. (eds.) Hormones, Brain and Behavior. Academic Press, San Diego, pp. 239-264
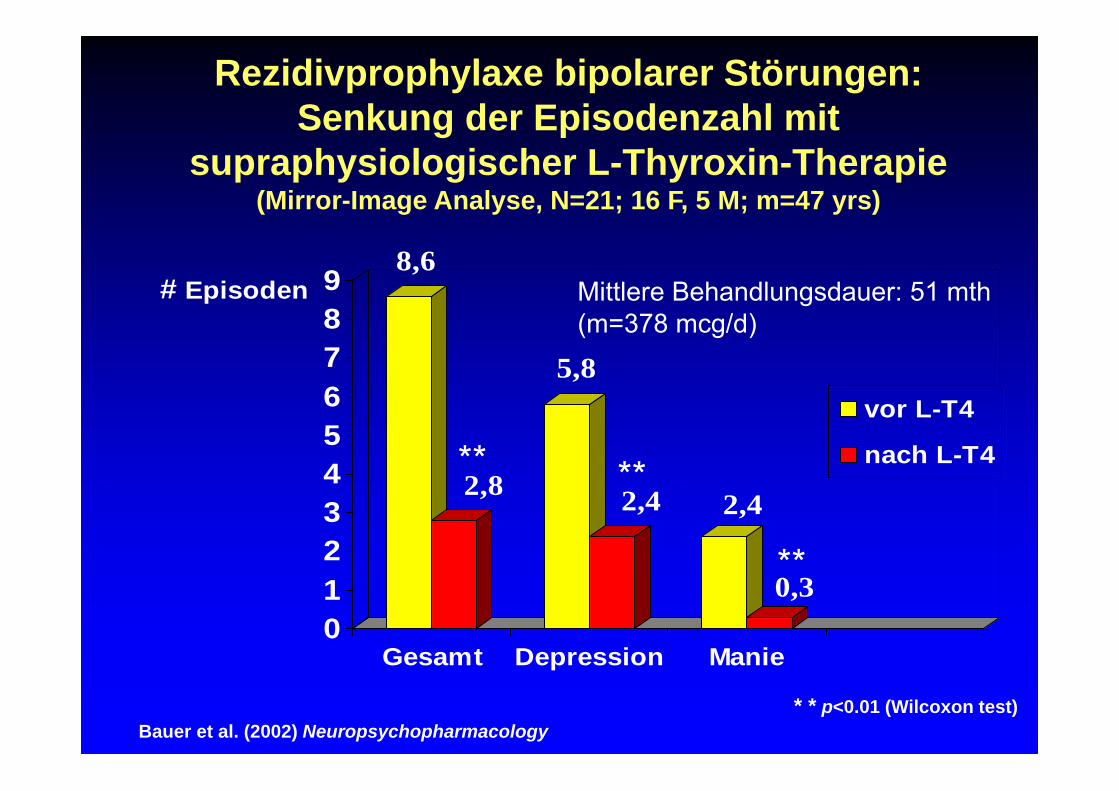
8,6
2,8
5,8
2,4 2,4
0,30123456789# Episoden
Gesamt Depression Manie
vor L-T4
nach L-T4
* * p<0.01 (Wilcoxon test)
**
Bauer et al. (2002) Neuropsychopharmacology
Rezidivprophylaxe bipolarer Störungen:Senkung der Episodenzahl mit
supraphysiologischer L-Thyroxin-Therapie(Mirror-Image Analyse, N=21; 16 F, 5 M; m=47 yrs)
Mittlere Behandlungsdauer: 51 mth (m=378 mcg/d)
**
**
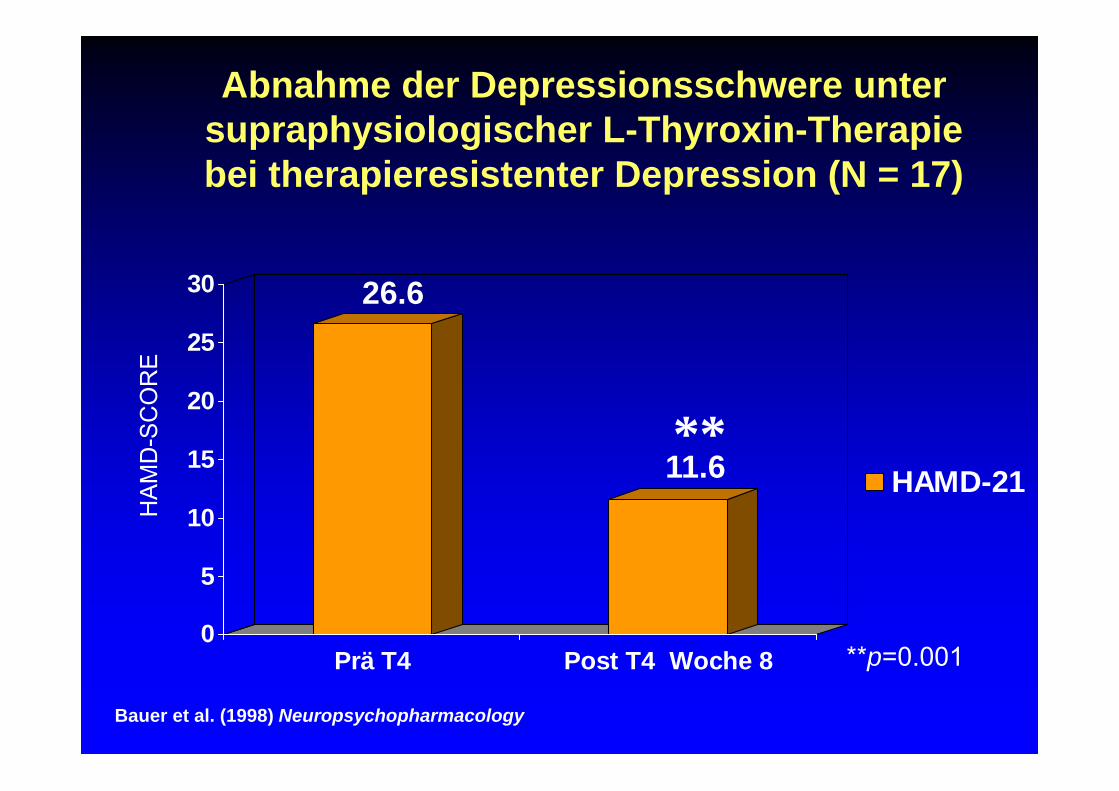
Abnahme der Depressionsschwere unter supraphysiologischer L-Thyroxin-Therapiebei therapieresistenter Depression (N = 17)
0
5
10
15
20
25
30
Prä T4 Post T4 Woche 8
HAMD-21
HA
MD
-SC
OR
E
**
**p=0.001
26.6
11.6
Bauer et al. (1998) Neuropsychopharmacology
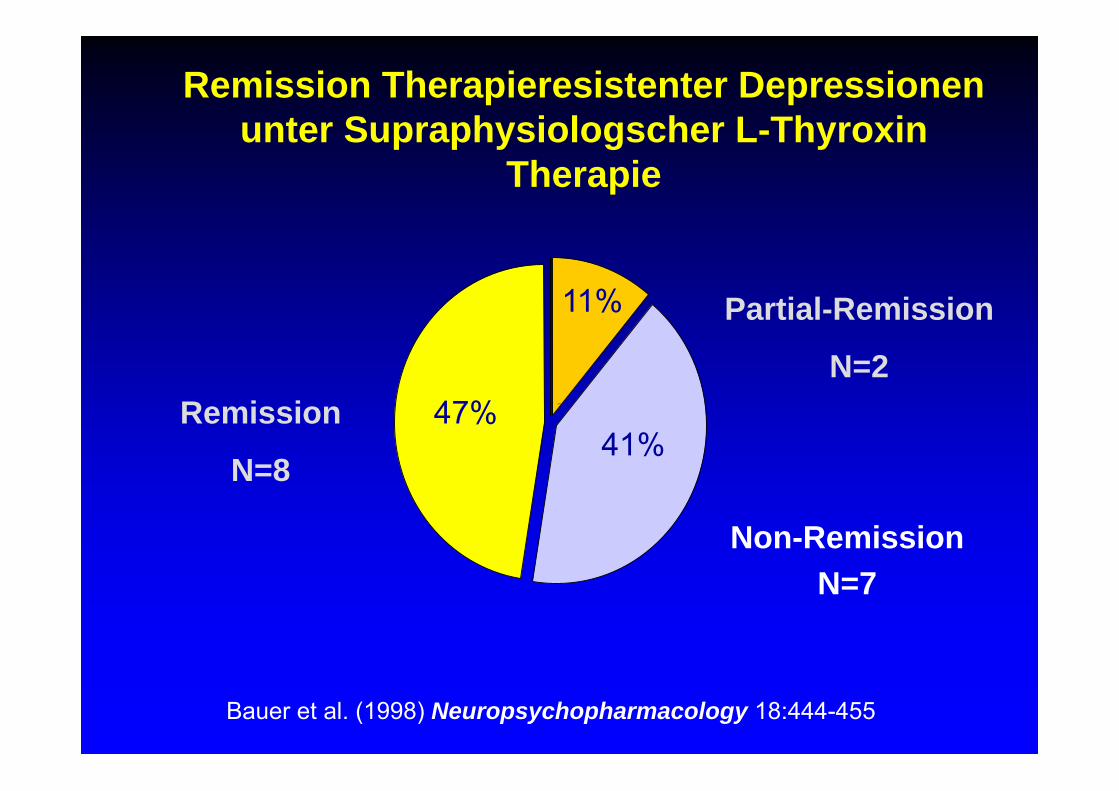
Remission
N=8
Partial-Remission
N=2
Non-RemissionN=7
47%
11%
41%Post T$
Remission Therapieresistenter Depressionen unter Supraphysiologscher L-Thyroxin
Therapie
Bauer et al. (1998) Neuropsychopharmacology 18:444-455
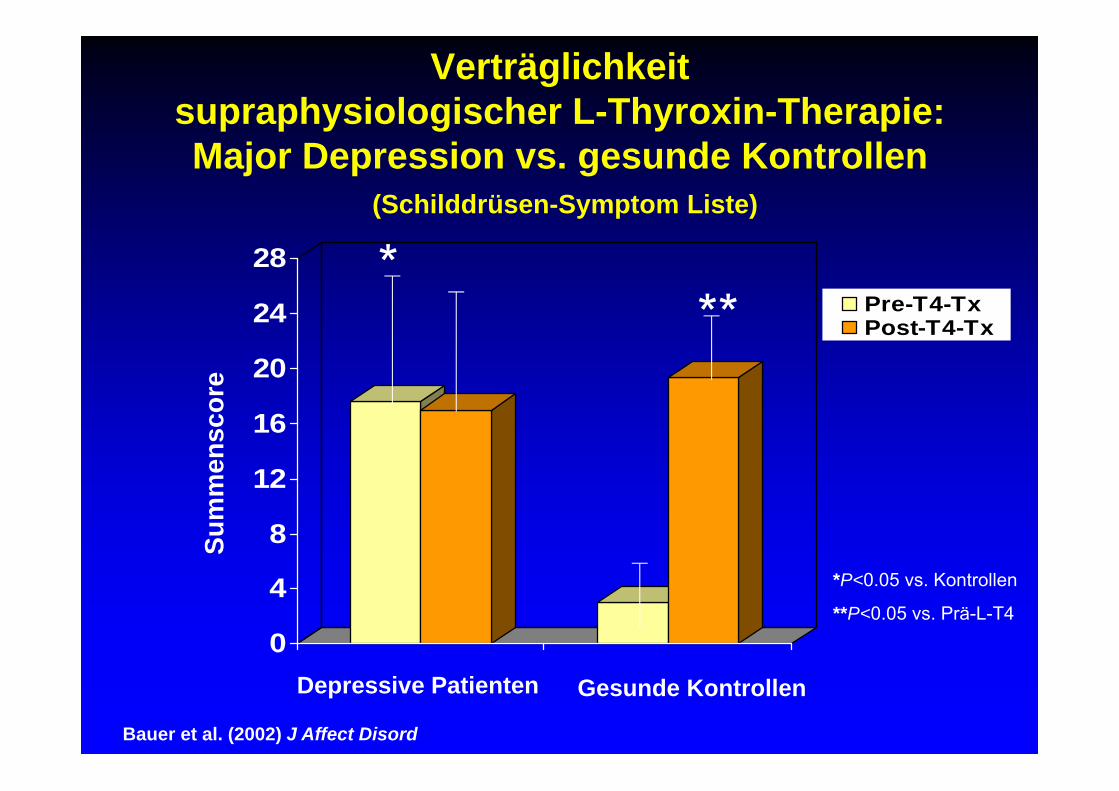
Verträglichkeitsupraphysiologischer L-Thyroxin-Therapie:Major Depression vs. gesunde Kontrollen
(Schilddrüsen-Symptom Liste)
0
4
8
12
16
20
24
28Pre-T4-TxPost-T4-Tx
Sum
men
scor
e
**
*P<0.05 vs. Kontrollen
**P<0.05 vs. Prä-L-T4
*
Depressive Patienten Gesunde Kontrollen
Bauer et al. (2002) J Affect Disord
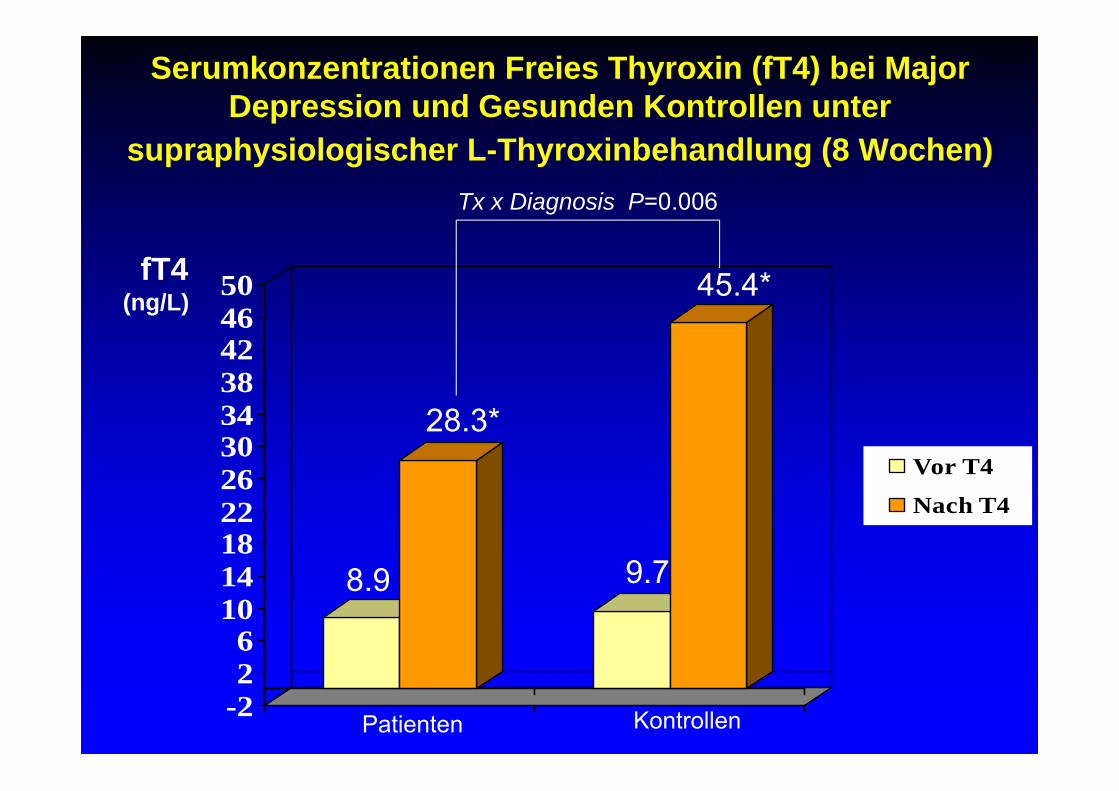
Serumkonzentrationen Freies Thyroxin (fT4) bei Major Depression und Gesunden Kontrollen unter
supraphysiologischer L-Thyroxinbehandlung (8 Wochen)
-226
1014182226303438424650
Vor T4
Nach T4
fT4(ng/L)
Patienten Kontrollen
Tx x Diagnosis P=0.006
28.3*
45.4*
8.9 9.7
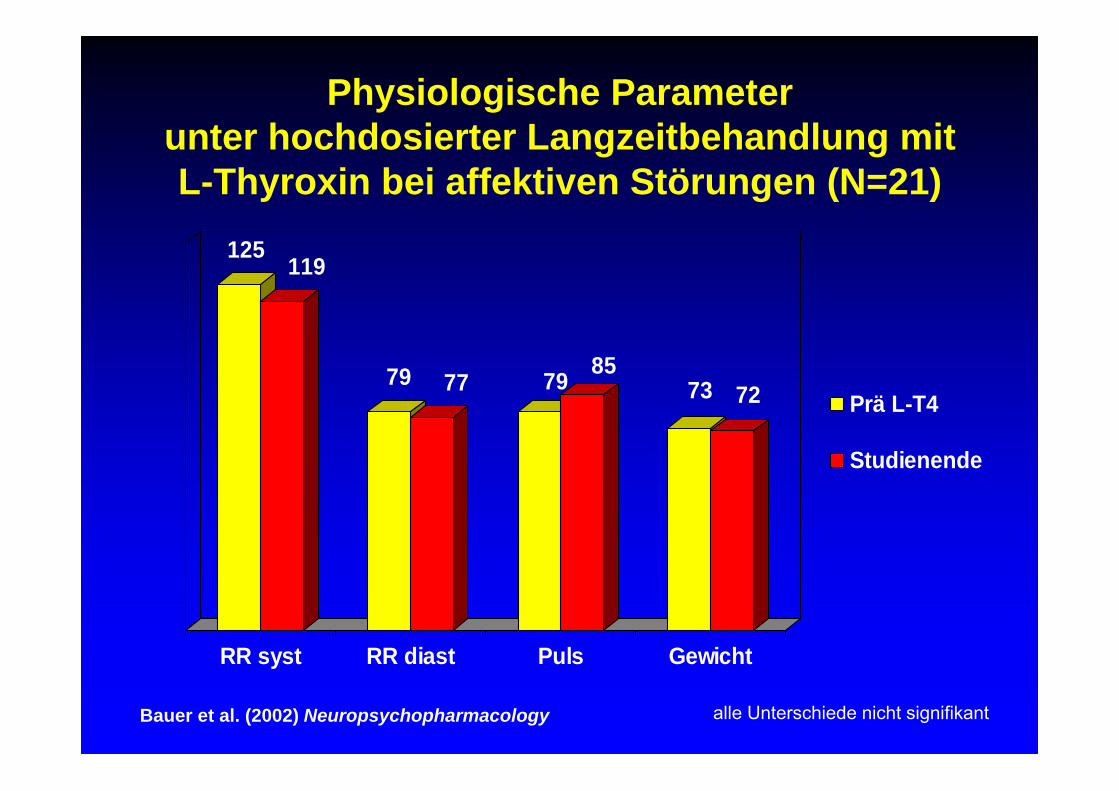
125119
79 77 79 8573 72
RR syst RR diast Puls Gewicht
Prä L-T4
Studienende
alle Unterschiede nicht signifikantBauer et al. (2002) Neuropsychopharmacology
Physiologische Parameterunter hochdosierter Langzeitbehandlung mitL-Thyroxin bei affektiven Störungen (N=21)
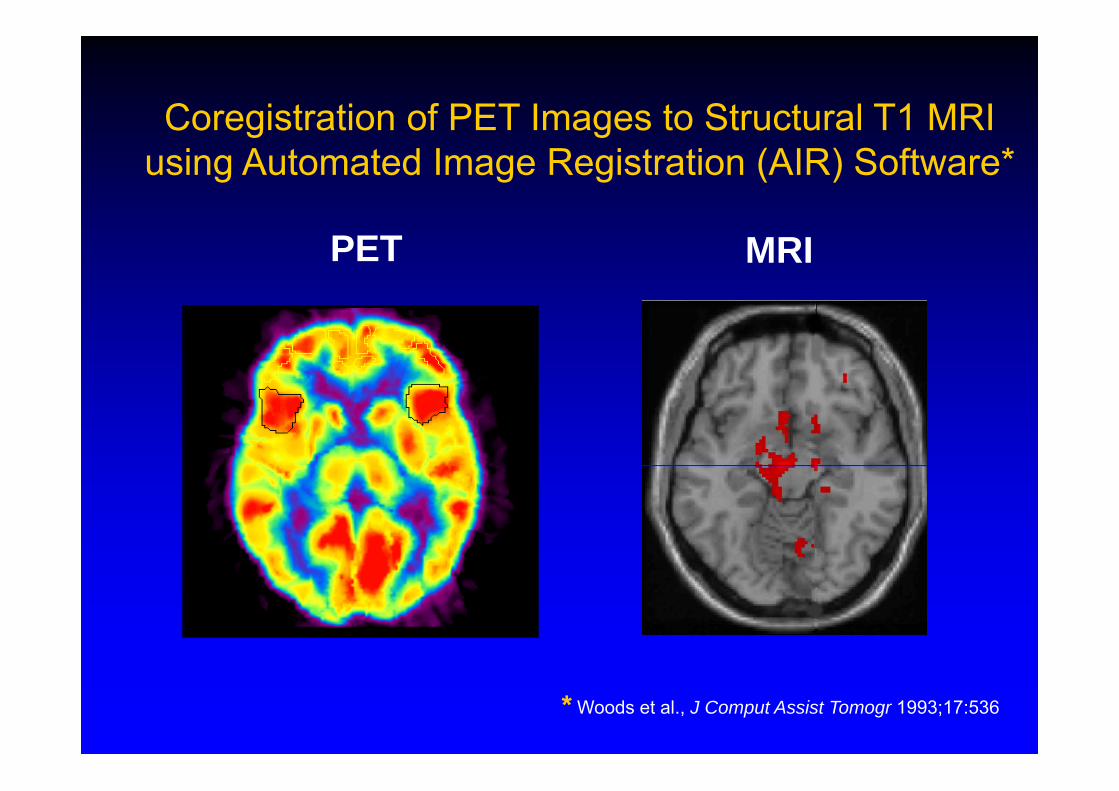
Coregistration of PET Images to Structural T1 MRI using Automated Image Registration (AIR) Software*
PET MRI
* Woods et al., J Comput Assist Tomogr 1993;17:536
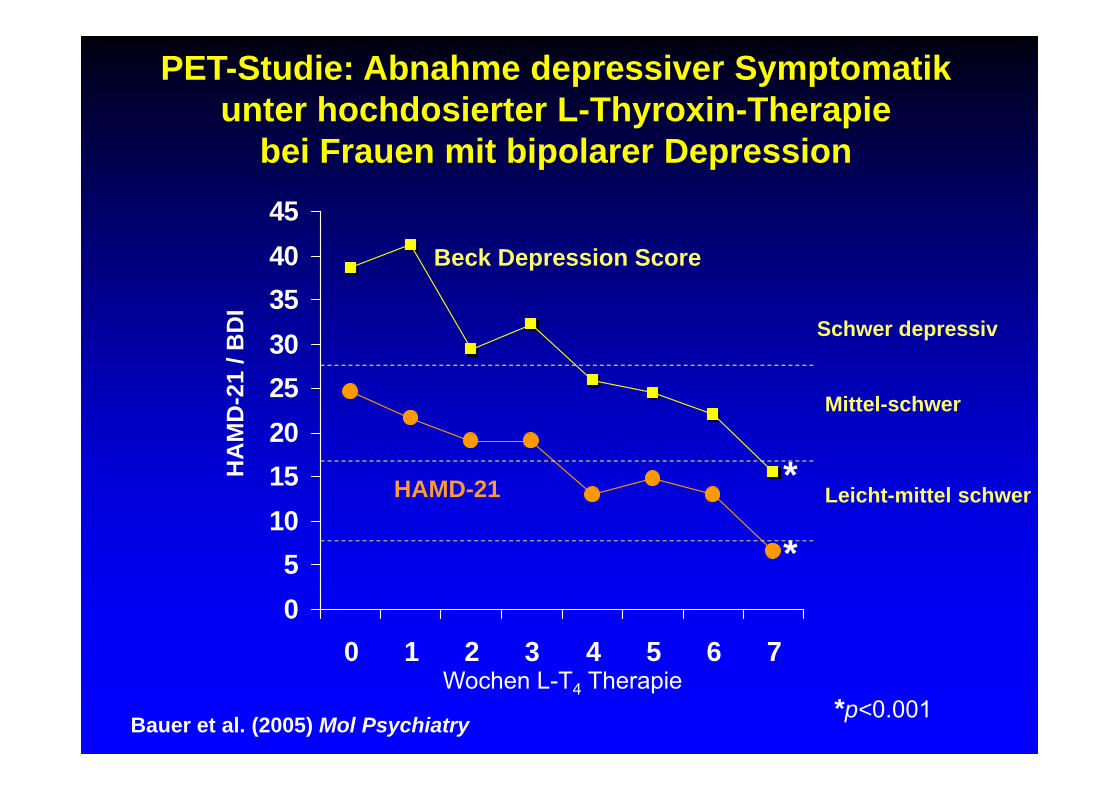
PET-Studie: Abnahme depressiver Symptomatikunter hochdosierter L-Thyroxin-Therapie
bei Frauen mit bipolarer Depression
05
1015202530354045
0 1 2 3 4 5 6 7Wochen L-T4 Therapie
HA
MD
-21
/ BD
I
HAMD-21
Beck Depression Score
Schwer depressiv
Mittel-schwer
Leicht-mittel schwer
*p<0.001
*
*
Bauer et al. (2005) Mol Psychiatry
• [18F] Fluorodeoxyglucose PET
• Aufmerksamkeitstest (Auditory Cont. Performance Task, CPT)
• “Volumes of Interest (VOI)” Analyse
• “Statistical Parametric Mapping (SPM 99)”Identifizierung regionaler Aktivierungen und Deaktivierungen im gesamten Gehirn
Vergleich der PET Bilder zwischen Prä- und Post T4 Therapie (“voxel-by-voxel method”)
PET Acquisition & Bild Analyse
Bauer et al. (2005) Mol Psychiatry
• 10 Frauen mit Bipolarer Depression
• Bipolar Type I n=9, Type II n=1
• Euthyreoter SD Status baseline (TSH and fT4)
• Alter: 39.3 + 7.8
• Jahre krank: 20.4 + 7.0
• 10 Gesunde Kontrollen, 35.9 + 9.3
Studienteilnehmer
• Woche 1: 100 mcg/d
• Woche 2: 200 mcg/d
• Woche 3: 300 mcg/d
• Woche 4: 400 mcg/d, bei non-suppression von TSH
Methoden L-T4 Dosierungsschema
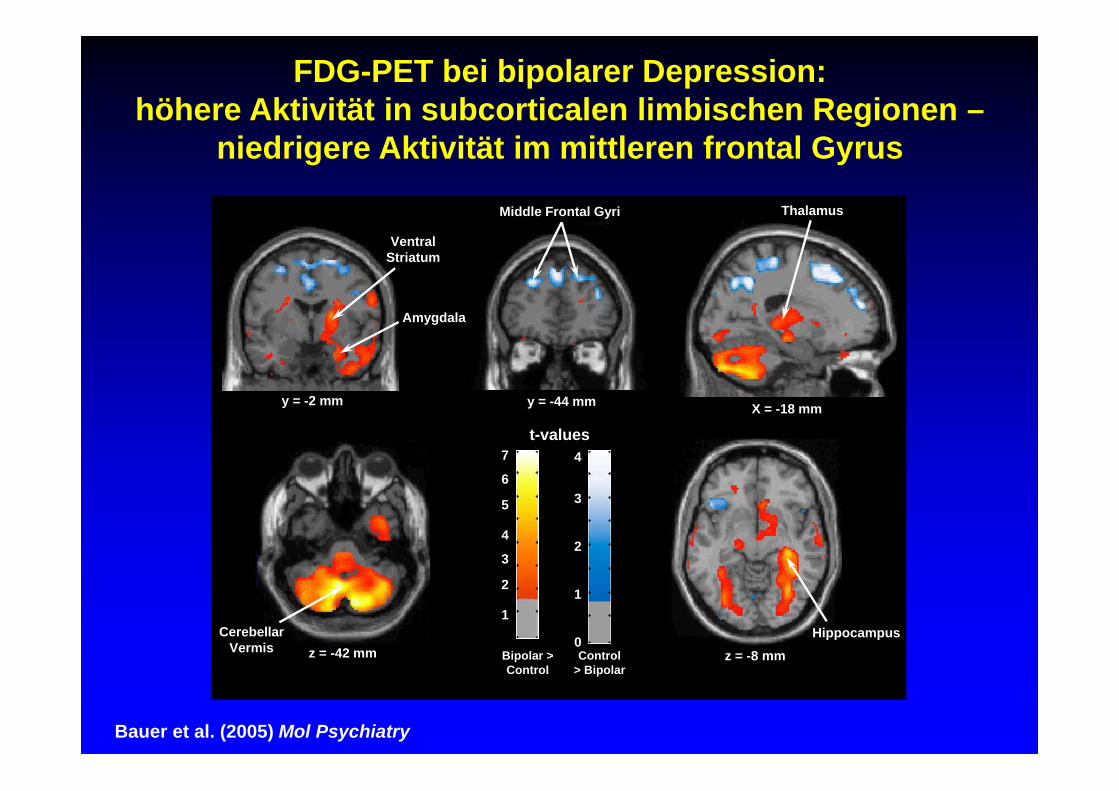
z = -42 mmCerebellar
VermisHippocampus
z = -8 mm
t-values
Control> Bipolar
3
1
2
4
0Bipolar > Control
5
3
2
4
6
7
1
y = -44 mm
Middle Frontal Gyri
y = -2 mm
Amygdala
VentralStriatum
X = -18 mm
Thalamus
FDG-PET bei bipolarer Depression:höhere Aktivität in subcorticalen limbischen Regionen –
niedrigere Aktivität im mittleren frontal Gyrus
Bauer et al. (2005) Mol Psychiatry
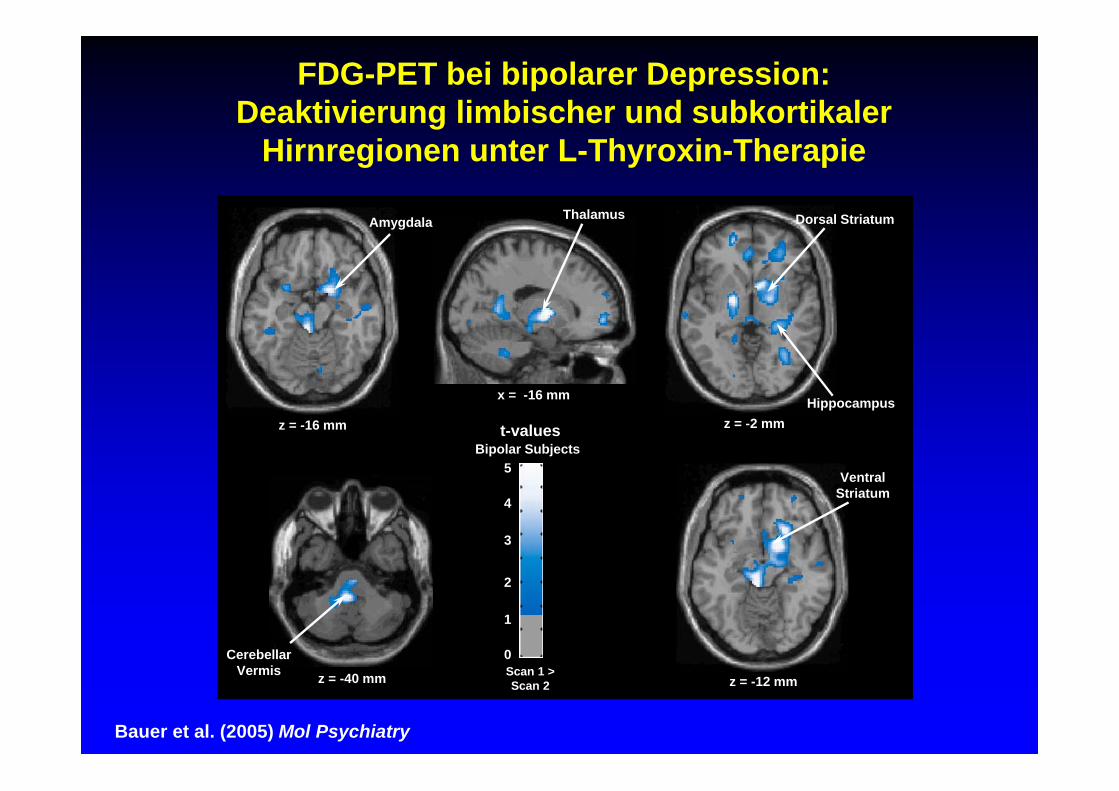
Hippocampusz = -2 mm
Dorsal Striatum
z = -16 mm
Amygdala
VentralStriatum
z = -12 mm
x = -16 mm
Thalamus
CerebellarVermis z = -40 mm Scan 1 >
Scan 2
t-values
5
3
2
4
1
0
Bipolar Subjects
FDG-PET bei bipolarer Depression:Deaktivierung limbischer und subkortikaler
Hirnregionen unter L-Thyroxin-Therapie
Bauer et al. (2005) Mol Psychiatry
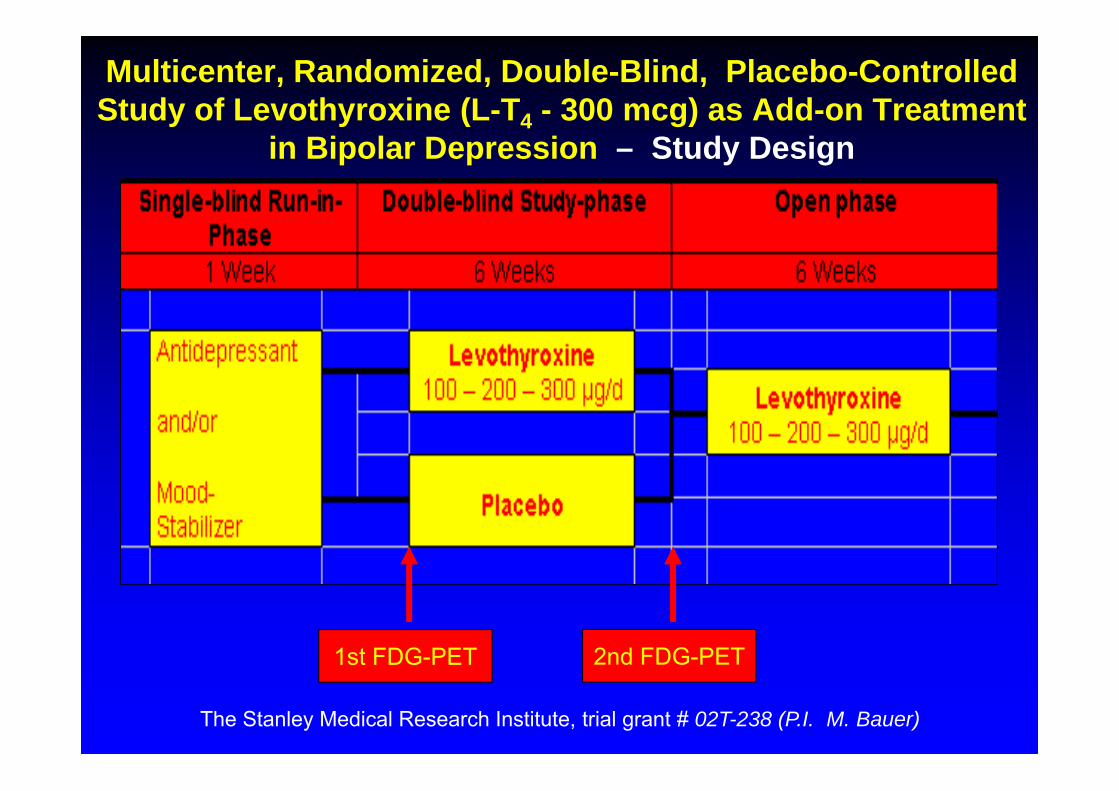
Multicenter, Randomized, Double-Blind, Placebo-Controlled Study of Levothyroxine (L-T4 - 300 mcg) as Add-on Treatment
in Bipolar Depression – Study Design
1st FDG-PET 2nd FDG-PET
The Stanley Medical Research Institute, trial grant # 02T-238 (P.I. M. Bauer)
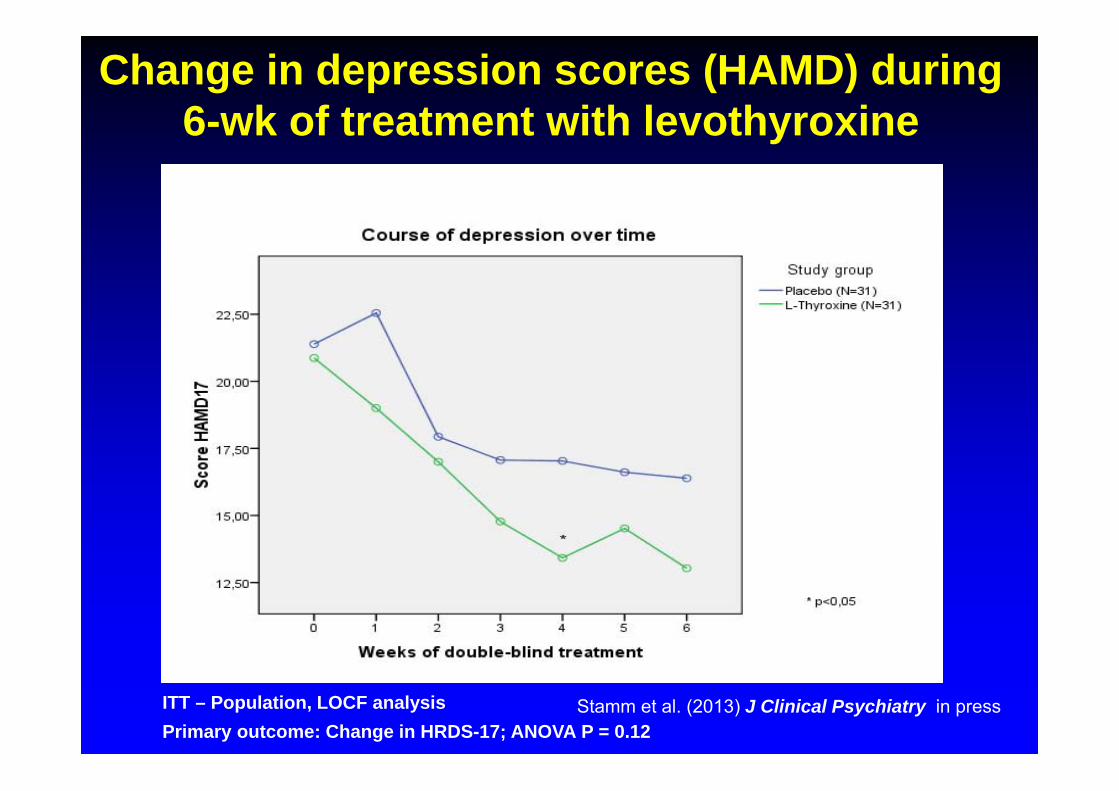
Change in depression scores (HAMD) during 6-wk of treatment with levothyroxine
ITT – Population, LOCF analysisPrimary outcome: Change in HRDS-17; ANOVA P = 0.12
Stamm et al. (2013) J Clinical Psychiatry in press
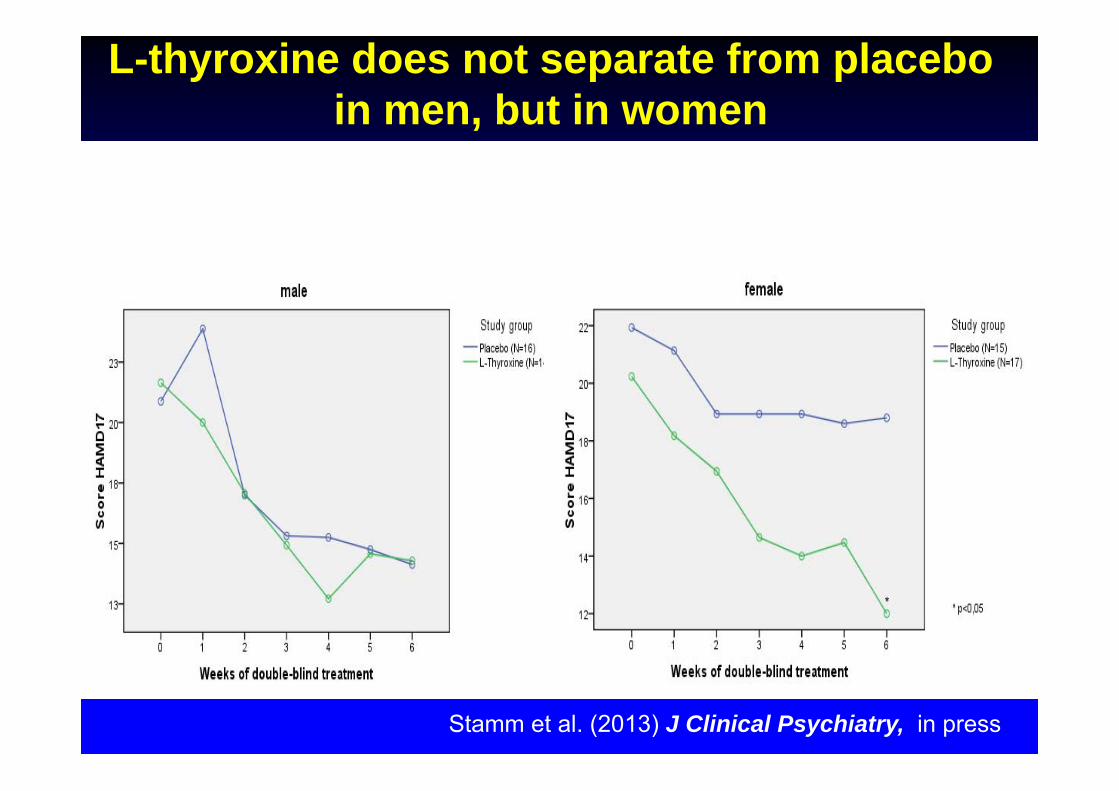
L-thyroxine does not separate from placebo in men, but in women
Stamm et al. (2013) J Clinical Psychiatry, in press
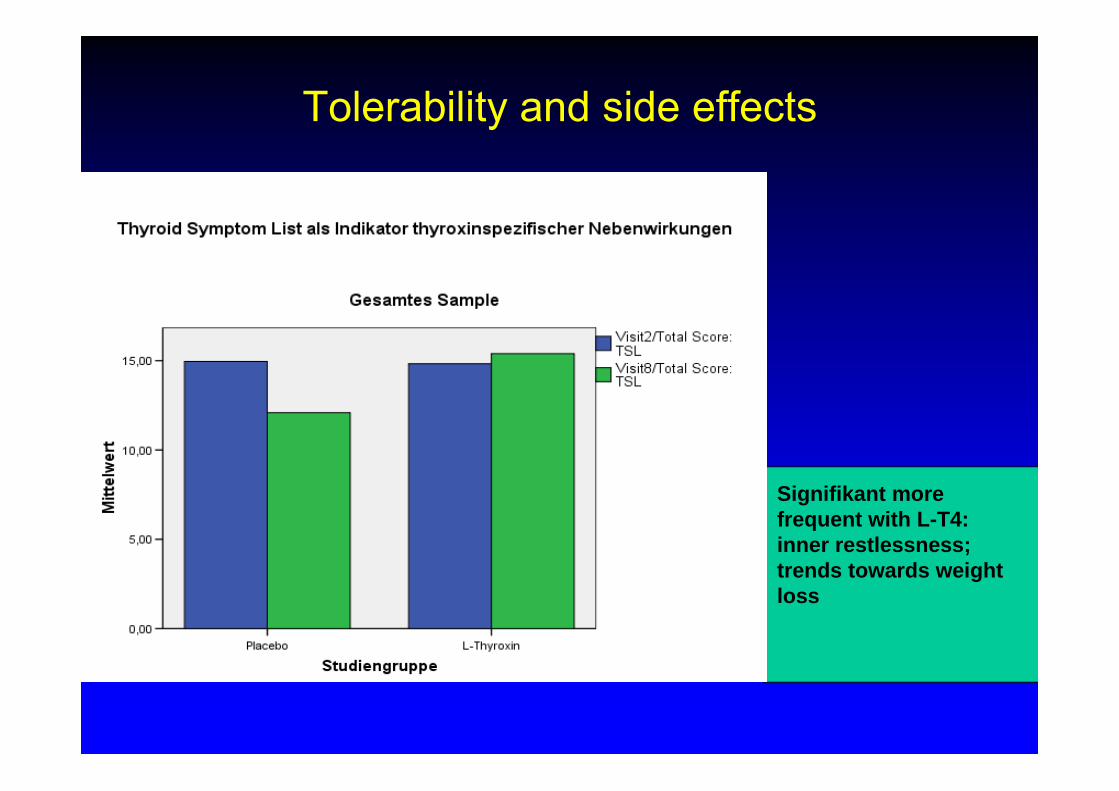
Tolerability and side effects
Signifikant more frequent with L-T4: inner restlessness; trends towards weight loss
T3, T4Schilddrüsen-hormonsystem Affektive Störungen