Embed Size (px)
Citation preview

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
18. Summerschool Transplantationsnephrologie, Kiel
Chirurgische Aspekte derNierentransplantation
Dr. med. Jan Henrik Beckmann
Klinik für Allgemeine Chirurgie und ThoraxchirurgieUniversitätsklinikum Schleswig-Holstein
Campus Kiel

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Chirurgie der Nierentransplantation§ Organentnahme
§ Präparation
§ Transplantation
§ PostoperativesManagement

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Mangel an Spenderorganen- Warteliste- Wartezeit um 7 Jahre
- Erweiterung der Spenderkriterien
- zunehmende Anzahl marginaler Organe

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Organentnahme- Kanülierung der abdominellen Aorta, bzw. A. iliaca com.- Klemmen der Aorta oberhalb des Truncus coeliacus- Perfusion mit eisgekühlter Perfusionslösung (HTK)- Anschließend Gewinnung der Organe

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Spendernephrektomie
• Operative Techniken
offen versus laparoskopischtransperitoneal versus extraperitoneal
robotorassistiert

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Spendernephrektomie über pararektale Miniinzision

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Spendernephrektomie über pararektale Miniinzision
Vorteile:- kleine Narbe- wenig Narbenbrüche- extraperitonealer Zugang
Nachteile:- kleiner Zugang- kleines Sichtfeld- technisch schwierig

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
DaVinci

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Probleme der Organentnahme zur NTx
• >95% Fremdentnahme• „Qualität“ unbekannt
– Kapseldefekt– Fett belassen– Beurteilung (Zyste, Tumor ?)– Polarterien abgeschnitten– Inkomplette Perfusion

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Präoperative Phase, Vorbereitung des Empfängers
• Bekannter („unbekannter“) Patient• Unvorhergesehene Risikofaktoren
– Status nach MI, KHK, ACVB, TIA, TVT– Antikoagulation– Gerinnungsstörung– Diabetes– pAVK, Stents– Infekt-Status (CMV)– BMI– Etc., …..

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Präoperative Phase
§pAVK§ Seitenwahl§ Befund aktuell ?§ Fußpulse ?§ Nativ CT Becken/ Abdomen§ Kombiniert TEA ?

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Faktor kalte Ischämie bei NTxEinfluss auf die Primärfunktion

Deutsches Ärzteblatt | Jg. 112 | Heft 6 | 6. Februar 2015 A 235
D ie Organtransplantation ist eine sichere und oft lebens-
rettende medizinische Therapieopti-on bei Organversagen. Fortschritte in Operationstechnik, immunologi-schem Grundverständnis, bei der Abstoßungsprophylaxe und -thera-pie und – nicht zuletzt – auch der Organkonservierung haben den Weg für die Langzeiterfolge in der Transplantationsmedizin geebnet. Der Mangel an Spenderorganen aber ist und bleibt ein zentrales Pro-blem. Außerdem führen eine ver-besserte Gesundheitsversorgung und die längere Lebenserwartung zu ei-ner deutlichen durchschnittlichen Erhöhung des Alters von Organ-spendern.
Große Datenbanken wie das Scientific Registry of Transplant Recipients (SRTR) in den USA be-legen diese Veränderungen ein-drücklich: Während der letzten 20 Jahre stieg der Anteil der Organ-spender > 50 Jahre über 200 Pro-zent, im Gegensatz hierzu fiel der Anteil der Organspender < 50 Jahre um 76 Prozent. Konsequenterweise werden zunehmend marginale Or-
gane verpflanzt, früher als „Expan-ded Criteria Donor“ Organe (ECD) bezeichnet. Diese Definition beruht in erster Linie auf dem erhöhten Al-ter des Spenders, aber auch auf wei-teren Aspekten, die die Funktion im Empfänger beeinflussen können.
Organe älterer Spender sind vulnerabler und immunogenerOrgane von älteren Spendern wei-sen signifikante Besonderheiten hin-sichtlich Vulnerabilität und Immu -nogenität auf, die den Erfolg einer Transplantation gefährden können. Dazu gehören altersbedingt einge-schränkte Reparaturvorgänge, und – damit einhergehend – eine erhöhte Anfälligkeit für sogenannte Ischä-mie-Reperfusionsschäden, die im In-tervall zwischen dem Ende der Durchblutung durch den Spender und dem Wiedereröffnen der Blutge-fäße nach Implantation auftreten. Möglicherweise ist auch eine erhöhte Immunogenität älterer Spenderorga-ne durch zahlreiche molekulare Ver-änderungen wie eine vermehrte Anti-genpräsentation oder eine höhere lo-kale Apoptoserate damit verbunden
(1). Unseren eigenen Untersuchun-gen zufolge ist die Rate der akuten Abstoßungen in älteren und geschä-digten Transplantaten erhöht (2).
Es gibt viele Anstrengungen in den letzten Jahren, um die Organ-qualität zu verbessern. Zu den prin-zipiellen Möglichkeiten gehören Organperfusion und -konservie-rung durch dynamische Flussprin-zipien, meist als pulsatile Perfu -sion. Sie kann zu einer erhebli-chen Verbesserung der Organquali-tät beitragen.
Die ersten klinischen Anwendun-gen der Maschinenperfusion zur Or-gankonservierung gab es schon vor mehr als 60 Jahren (3). Trotzdem blieb der Methode aufgrund des da-mals beträchtlichen Ausmaßes der benötigten Geräte und des damit ver-bundenen logistischen Aufwands ei-ne breite klinische Anwendung ver-wehrt. Gleichzeitig kam es zu einer Verbesserung der Perfusionslösun-gen mit dem Ergebnis einer effekti-veren statischen Konservierung und einer Weiterentwicklung der Immun-suppressiva, so dass der isolierte Ef-fekt der kontinuierlichen Organper-
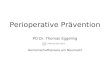
Diese explantierte Niere ist in gutem
Zustand. Standard-versorgung für die Ischämiezeit ist ei-
ne statische Kon-servierung in eisge-
kühlter Lösung.
Foto
: Arn
o M
asse
e/SP
L/Ag
entu
r Foc
us
KONSERVIERUNGSMETHODEN VON ORGANEN FÜR DIE TRANSPLANTATION
Organqualität lässt sich verbessern Die Phase zwischen Ex- und Implantation eines Organs lässt sich zur Vorbeugung von Schäden nutzen. Neue Verfahren sollen mehr Organe transplantabel machen.

Hypothermic machine perfusion in kidney transplantationDe Deken, Julie; Kocabayoglu, Peri; Moers, Cyril, 2016

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Ablauf der Nierentransplantation
-Hautschnitt-Präparation der Fossa iliaca-Darstellung der Beckenstrombahn-Präparation der Gefäße-Klemmen der Arterie-arterielle Anastomose-Freigabe der Arterie, Ausklemmen der Tx Arterie-Venöse Anastomose-Reperfusion-Ureteranastomose-Drainage-Bauchdeckenverschluss

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Nierentransplantation
Arteria iliacaexterna
Arteria iliacacom.
Vena iliacaexterna

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Transplantation in die Fossa iliaca
Beckmann, Allgemein und Viszeralchirurgie up2date 2009

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Nierentransplantation
Arteria iliaca externa
Arteria iliacacom.
Vena iliaca externa

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Multiple Nierenarterien, sequentielle Anastomose
Kein signifikanter Unterschied in der Inzidenzvon Komplikationen,allenfalls erhöhte Rate an Lymphozelen

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Implantation und Reperfusion

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
DaVinci Nierentransplantation
• minimal invasive Nierentransplantation• bisher 2 Zentren in Deutschland• bisher < 50 Eingriffe europaweit• Kiel ab 2017• Trainingscenter Anatomie CAU

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie

Vol.:(0123456789)1 3
World J Urol (2017) 35:1507–1515 DOI 10.1007/s00345-017-2006-8
ORIGINAL ARTICLE
Robotic kidney transplantation: one year after the beginningAlberto Breda1 · Angelo Territo1 · Lluis Gausa1 · Oscar Rodríguez-Faba1 · Jorge Caffaratti1 · Javier Ponce de León1 · Lluis Guirado2 · Carme Facundo2 · Marco Guazzieri1 · Andrea Guttilla1,3 · Humberto Villavicencio1
Received: 20 December 2016 / Accepted: 11 January 2017 / Published online: 22 February 2017 © Springer-Verlag Berlin Heidelberg 2017
and one case of intraperitoneal hematoma. No anastomosis revision and wounds infections occurred.Conclusion RAKT with regional hypothermia appears to be a safe surgical procedure in a properly selected group of patients. The potential advantages of RAKT are related to the quality of the vascular anastomosis, the possible lower complication rate and the shorter recovery of the recipients.
Keywords Kidney transplantation · Regional hypothermia · Robot-assisted kidney transplantation · Robotic surgery · Vascular anastomosis
AbbreviationsBMI Body mass indexdVSS® Da Vinci surgical system®
DGF Delayed graft functionESRD End-stage renal diseaseGFR Glomerular filtration rateKT Kidney transplantationPKD Polycystic kidney diseasePOD Post-operative dayRAKT Robotic-assisted kidney transplantationVAS Visual analog scale
Introduction
End-stage renal disease (ESRD) is defined as GFR <15 mL/min/1.73 m2 with the necessity for renal replace-ment therapy. This condition is associated with high mor-bidity and mortality [1, 2]. Replacement therapy consists of dialysis (hemodialysis and peritoneal dialysis) or kidney transplantation (KT). Hemodialysis and peritoneal dialysis can lead to long-term survival and can serve as a bridge for patients who need KT. If it is compared with long-term
Abstract Introduction Kidney transplantation (KT) is the preferred treatment for patients with end-stage renal disease (ESRD). To reduce the morbidity of the open surgery, a robotic-assisted approach has been recently introduced. Our aim is to evaluate surgical and functional results on 17 cases of robotic-assisted kidney transplantation (RAKT) performed at the same institution.Materials and methods From July 2015 to June 2016, we performed 17 cases of RAKT from living donors in pre-emptive patients, who underwent laparoscopic nephrec-tomy. A prospective pilot study was made at Fundació Puigvert (Barcelona), evaluating functional and surgi-cal outcomes. In this series, we considered the functional results, surgical outcomes and complications rates.Results Seventeen patients successfully underwent RAKT, in particular surgical console time was 181 min (150–200) with vascular suture time 42 min (32–48), and estimated blood loss <70 ml. Overall ischemia time was 98.9 min (84–140). No patient was converted to open trans-plantation. No major surgical intra-operative complications were observed. The mean post-operative serum creatinine level 160 μmol/L (81–479). We reported a case of delayed graft function (DGF), one case of graft arterial thrombosis
* Alberto Breda [email protected] Department of Urology, Fundació Puigvert, Autonoma
University of Barcelona, Barcelona, Spain2 Department of Nephrology, Fundació Puigvert, Autonoma
University of Barcelona, Barcelona, Spain3 Department of Urology, U.L.S.S. 15 “Alta Padovana”,
Camposampiero Hospital, Camposampiero, Padua, Italy

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Zystureteroneostomie
Häufig Einlage einer Ureterschiene.Cave: Dokumentation und Entfernung 6 Wochen postOP

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Frühpostoperative Procedere• Dauerkatheter 5 Tage belassen• frühzeitige Mobilisation, Aufstehen am OP Tag• frei trinken am OP Tag, zügiger Kostaufbau• Immunsuppression• Bilanz +500ml, tgl. wiegen, 3kg über TG• Prophylaxen: PCP, Thrombose, Ulkus, Osteoporose, CMV,
Soor• Drainagen entfernen• regelmäßige Sonographie, Laborkontrolle
• Ureterschiene im Intervall entfernen• 6 Wochen keine schweren körperlichen Belastungen

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Komplikationen nach NTx

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Routine Diagnostik zur Erkennung von Komplikationen
Duplex Sonographie !!!

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Postoperative Blutung, Auslöser-Anastomoseninsuffizienz
-Spenderseitige Blutungsquelle Hilus / Kapsel / Ureter
-Empfängerseitige Quelleretroperitoneal / Muskulatur / subkutan / Blase
-„entgleiste“ Gerinnungheparininduziert, ggf. Dialyse postoperativMarcumarisierungASS, Plavix
-IatrogenBiopsie

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Komplikationen nach NTxGefäßkomplikationen, Thrombose / Stenose
Arterieller Pendelfluss venöser Thrombose à Notfall OP !

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Komplikationen nach NTxInterventionelle Therapie der Transplantatarterienstenose
vor Dilatation nach Dilatation

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Urologische Komplikationen
Whang, Transplantation Proceedings 2011

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Urologische KomplikationenUrinleckage
Revisionsoperation mit Neuanlage, ggf. Eigenureteranschluss
Urinleck drei Wochen nach NTx

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Lymphozele

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Lymphozele
19.10.2005 / 36 Developments and Innovationsin Medicine Oman 2011
Sigma
A. Iliac
a exte
rna
Laparoskopische Lymphozelenfensterung

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Komplikationen nach NTx
Chirurgische Komplikationenbrauchen
chirurgische Lösungen

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Routine Diagnostik zur Erkennung von Komplikationen
Duplex Sonographie !!!

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
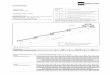
Komplikationsloser postoperativer Verlauf
0
100
200
300
400
500
600
700
800
23.09. 24.09. 25.09.
Kreatinin µmol/lHarnstoff µmol/l

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Vorbereitung morbid adipöser Patienten
Erhöhtes Risiko durch:
- Narkose- Erhöhter Schwierigkeitsgrad- Wundinfektionen- Durchblutungsstörungen
Bariatrische OP vor NTx sinnvoll?

Adipositas und Nierentransplantation
ORIGINAL SCIENTIFIC REPORT
Kidney Transplant Outcomes in the Super Obese: A NationalStudy From the UNOS Dataset
Pooja Kanthawar1 • Xiaonan Mei1 • Michael F. Daily1 • Jyotin Chandarana1 •
Malay Shah1 • Jonathan Berger1 • Ana Lia Castellanos1 • Francesc Marti1 •
Roberto Gedaly1,2
Published online: 22 June 2016! Societe Internationale de Chirurgie 2016
AbstractBackground We evaluated outcomes of super-obese patients (BMI[50) undergoing kidney transplantation in the US.
Methods We performed a review of 190 super-obese patients undergoing kidney transplantation from 1988 through
2013 using the UNOS dataset.Results Super-obese patients had a mean age of 45.7 years (21–75 years) and 111 (58.4 %) were female. The mean
BMI of the super-obese group was 56 (range 50.0–74.2). A subgroup analysis demonstrated that patients with
BMI[ 50 had worse survival compared to any other BMI class. The 30-day perioperative mortality and length ofstay was 3.7 % and 10.09 days compared to 0.8 % and 7.34 days in nonsuper-obese group. On multivariable
analysis, BMI[ 50 was an independent predictor of 30-day mortality, with a 4.6-fold increased risk of perioperative
death. BMI[ 50 increased the risk of delayed graft function and the length of stay by twofold. The multivariableanalysis of survival showed a 78 % increased risk of death in this group. Overall patient survival for super-obese
transplant recipients at 1, 3, and 5 years was 88, 82, and 76 %, compared to 96, 91, 86 % on patients transplanted
with BMI\ 50. A propensity score adjusted analysis further demonstrates significant worse survival rates in super-obese patients undergoing kidney transplantation.
Conclusion Super-obese patients had prolonged LOS and worse DGF rates. Perioperative mortality was increased
4.6-fold compared to patients with BMI\ 50. In a subgroup analysis, super-obese patients who underwent kidneytransplantation had significantly worse graft and patient survival compared to underweight, normal weight, and
obesity class I, II, and III (BMI 40–50) patients.
AbbreviationsBMI Body mass index
LOS Length of stay
DGF Delayed graft functionESRD End-stage renal disease
UNOS United network for organ sharing
SO Super obese
US United States of AmericaUNK Unknown
F Female
M Male
Introduction
Obesity has grown in prevalence in the United States (US)
with more than two-thirds of adults (68.8 %) considered
overweight or obese [1]. Although, obesity is a significant
& Roberto [email protected]
1 Transplant Center, University of Kentucky College ofMedicine, Lexington, KY, USA
2 University of Kentucky Transplant Center, 800 Rose Street,C451, Lexington, KY 40536-0293, USA
123
World J Surg (2016) 40:2808–2815
DOI 10.1007/s00268-016-3615-x
à BMI > 50 erhöht das Mortalitätsrisiko um den Faktor 4,6

• verlängerte Operationszeit + 0,77h• Verlängerter stationärer Aufenthalt + 2,3d• Erhöhte Komplikationsraten (Wundinfekte und allgemeine
Komplikationen) 3 x• Erhöhtes Risiko für einen T2D post Tx 2,2 x• Reduziertes Organ- und Patientenüberleben ?
BMI > 30 bei Nierentransplantation
Potentielle Nierentransplantatempfänger sollten vorher das Gewicht reduzieren.Lafranca et al. BMC Medicine (2015) 13:111

Addressing Morbid Obesity as a Barrier toRenal Transplantation With LaparoscopicSleeve Gastrectomy
C. M. Freeman1, E. S. Woodle1, J. Shi2,J. W. Alexander1, P. L. Leggett3, S. A. Shah1,F. Paterno1, M. C. Cuffy1, A. Govil4,G. Mogilishetty4, R. R. Alloway4, D. Hanseman1,M. Cardi5 and T. S. Diwan1,*
1Department of Surgery, Division of Transplantation,University of Cincinnati College of Medicine, Cincinnati, OH2University of Cincinnati College of Medicine, Cincinnati, OH3Department of Surgery, University of Texas-HoustonHealth Science Center, Houston, TX4Department of Medicine, Division of Nephrology,University of Cincinnati College of Medicine, Cincinnati, OH5Department of Medicine, Division of Nephrology, TheChrist Hospital, Cincinnati, OH!Corresponding author: Tayyab S. Diwan,[email protected]
Morbid obesity is a barrier to renal transplantation andis inadequately addressed by medical therapy. Wepresent results of a prospective evaluation of laparo-scopic sleeve gastrectomy (LSG) for patients failing toachieve significant weight loss with medical therapy.Over a 25-month period, 52 obese renal transplantcandidates meeting NIH guidelines for metabolicsurgery underwent LSG. Mean age was 50.0 "10.0 years with an average preoperative BMI of43.0 " 5.4 kg/m2 (range 35.8–67.7 kg/m2). Follow-upafter LSG was 220 " 152 days (range 26–733 days)with last BMI of 36.3 " 5.3 kg/m2 (range 29.2–49.8 kg/m2) with 29 (55.8%) patients achieving goal BMIof<35 kg/m2 at 92 " 92 days (range 13–420 days). Themean percentage of excess weight loss (%EWL) was32.1 " 17.6% (range 6.7–93.8%). A segmented regres-sion model was used to compare medical therapyversus LSG. This revealed a statistically significantincrease in the BMI reduction rate (0.3 kg/m2/monthversus 1.1 kg/m2/month, p< 0.0001). Patients alsoexperienced a 40.9% decrease in anti-hypertensivemedications (p< 0.001) and a 49.7% decrease in totaldaily insulin dose (p< 0.001). LSG is a safe and effectivemeans for addressing obesity in kidney transplantcandidates in the context of a multidisciplinaryapproach.
Abbreviations: BMI, body mass index; CKD, chronickidney disease; ESRD, end stage renal disease; %EWL,percent excess weight loss; HD, hemodialysis; ICU,
intensive care unit; LSG, laparoscopic sleevegastrectomy
Received 09 July 2014, revised 20 October 2014 andaccepted for publication 16 November 2014
Introduction
Obesity is a rising pandemic that is most pronounced indeveloping countries (1). It has been estimated that by2030,more than 50%of the U.S. populationwill have a BMI>30 kg/m2 (2). The proportion of patients undergoing renaltransplantation who are obese (BMI # 30 kg/m2) at the timeof transplant is currently 60% (3).
Obesity is also an important risk factor for complicationsfollowing renal transplantation (3–6). Recent reviews andsingle center experiences have shown that morbid obesityis associated with increased delayed graft function, woundcomplications, prolonged hospitalization, new onset diabe-tes mellitus, acute biopsy proven rejection and reducedgraft survival (4–13,36). Higher mortality rates in obeserenal transplant recipients are thought to be due toincreased rates of postoperative cardiovascular complica-tions including atrial fibrillation and congestive heartfailure (14–16). Recognition of these associated complica-tions has led to obesity becoming a relative contraindicationto renal transplantation with many centers using a BMI of35–40 kg/m2 as an upper limit for transplant candidacy. Ofnote, patients with obesity (class I–III) have a reportedlower likelihood of transplantation when compared to anormal BMI patient (17).
Kidney transplant programs often require that obesetransplant candidates meet specified BMI and/or weightloss criteria prior to being approved as a transplantcandidate for living donor transplantation or approved foractive status on the deceased donor waitlist. Recent SRTRdata has shown that obesity is the third leading cause ofbeing inactive on the kidney transplant waitlist (18). Formost obese transplant candidates, medical weight loss hastraditionally been the primary approach for achieving pre-transplant weight loss. However, medical weight lossregimens have historically had poor short and long-termsuccess rates (19). Similarly, we have foundmedical weight
American Journal of Transplantation 2015; 15: 1360–1368Wiley Periodicals Inc.
$C Copyright 2015 The American Society of Transplantationand the American Society of Transplant Surgeons
doi: 10.1111/ajt.13116
1360
Laparoscopic sleeve gastrectomy in patients with ESRD is
safeefficacioussuperior to medical weight loss managementcan increase access to transplantation

Adipositas und terminale NiereninsuffizienzEmpfehlungen
BMI > 30 konservative Therapie
BMI > 35 und Nebenerkrankungen multidisziplinärer Ansatz, MMK undbzw. BMI > 40 Sleevegastrektomie
kein genereller Ausschluss von der Nierentransplantation aufgrund einer Adipositas!

Klinik für Allgemeine-, Viszeral-, Transplantations-,Thorax- und Kinderchirurgie
Klinik für Allgemeine-, Viszeral-, Transplantations-, Thorax- und Kinderchirurgie
Bariatrische Chirurgie
Sleevegastrektomie Magenbypass
- laparoskopisches Vorgehen - standardisiertes Procedere - 5 Tage stationärer Aufenthalt - zur erwartender Gewichtsverlust 70% des Übergewichts
innerhalb von 24 Monaten