Embed Size (px)
Citation preview

Wolfgang Schima
Der weite Gallen- oder Pankreasgang: Sono, CT, EUS oder MRCP Sono, EUS oder MRCP
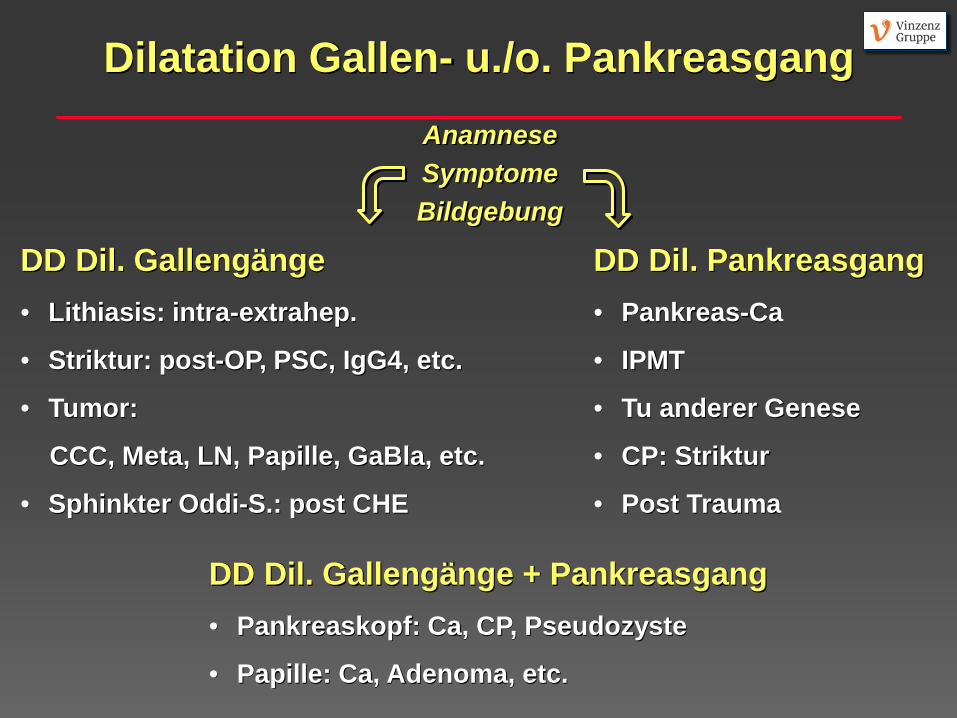
Dilatation Gallen- u./o. Pankreasgang Anamnese Symptome Bildgebung
DD Dil. Gallengänge • Lithiasis: intra-extrahep.
• Striktur: post-OP, PSC, IgG4, etc.
• Tumor:
CCC, Meta, LN, Papille, GaBla, etc.
• Sphinkter Oddi-S.: post CHE
DD Dil. Pankreasgang • Pankreas-Ca
• IPMT
• Tu anderer Genese
• CP: Striktur
• Post Trauma
DD Dil. Gallengänge + Pankreasgang • Pankreaskopf: Ca, CP, Pseudozyste
• Papille: Ca, Adenoma, etc.
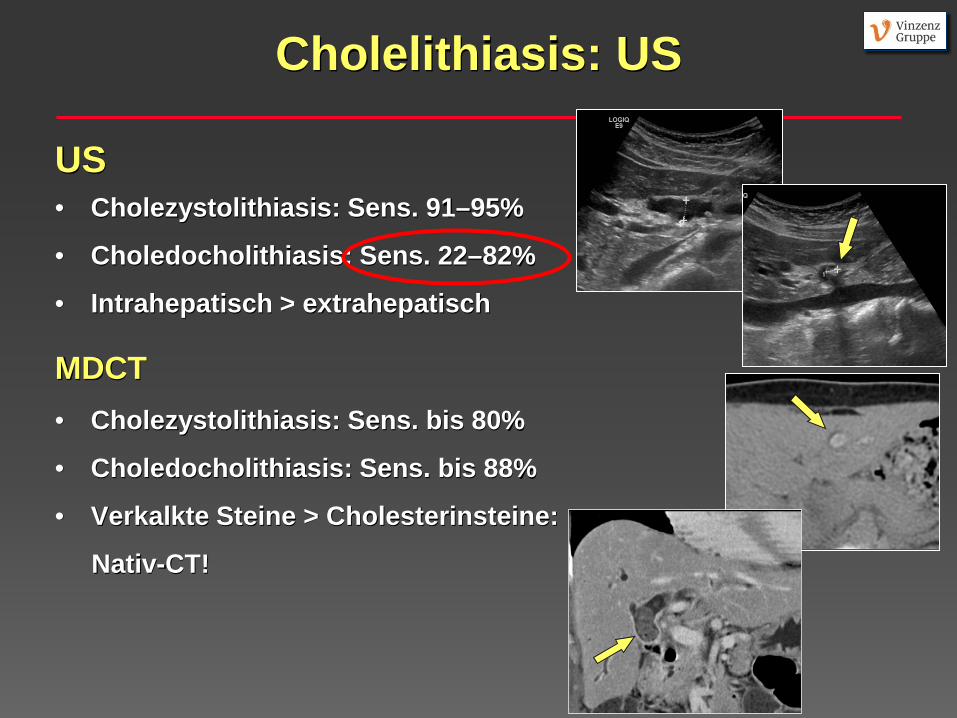
Cholelithiasis: US
US • Cholezystolithiasis: Sens. 91–95%
• Choledocholithiasis: Sens. 22–82%
• Intrahepatisch > extrahepatisch
MDCT • Cholezystolithiasis: Sens. bis 80%
• Choledocholithiasis: Sens. bis 88%
• Verkalkte Steine > Cholesterinsteine:
Nativ-CT!
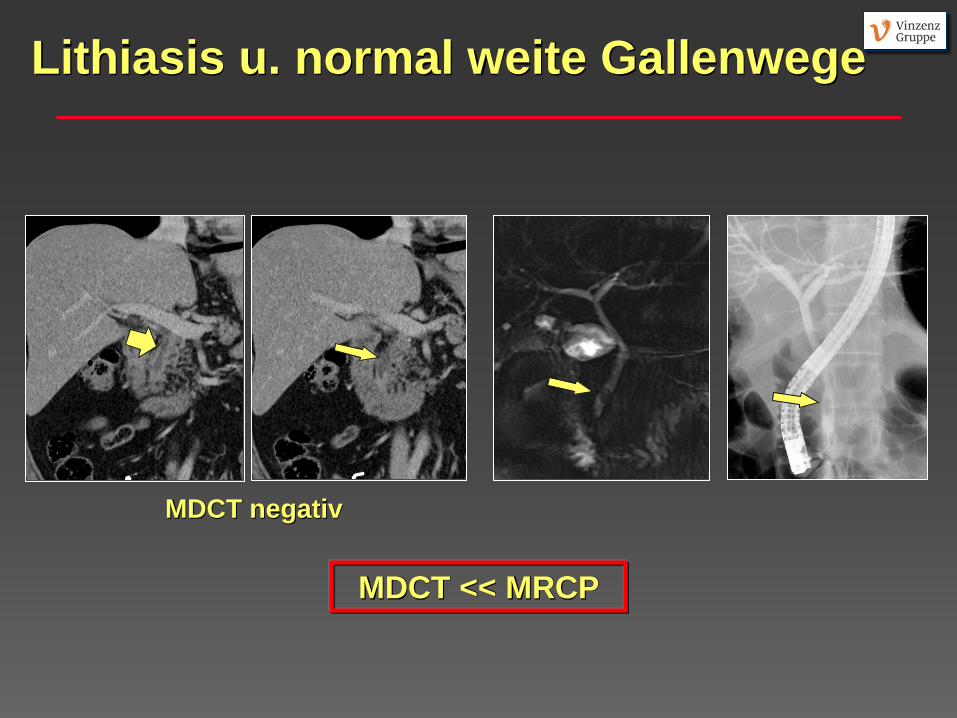
Lithiasis u. normal weite Gallenwege
MDCT << MRCP
MDCT negativ
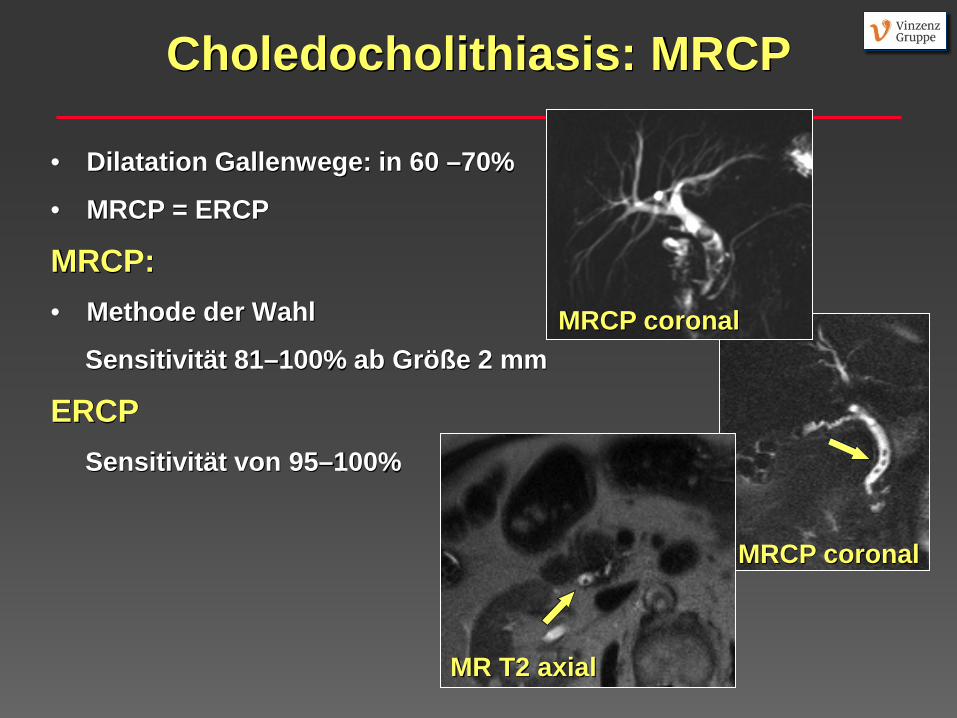
Choledocholithiasis: MRCP
• Dilatation Gallenwege: in 60 –70%
• MRCP = ERCP
MRCP: • Methode der Wahl
Sensitivität 81–100% ab Größe 2 mm
ERCP Sensitivität von 95–100%
MR T2 axial
MRCP coronal
MRCP coronal
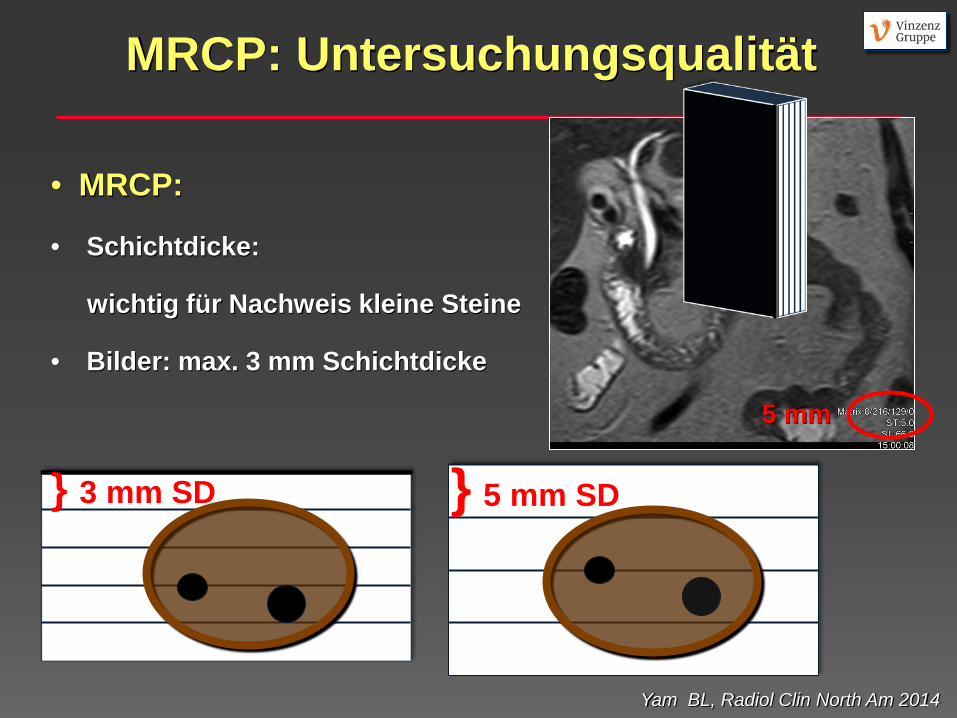
• MRCP:
• Schichtdicke:
wichtig für Nachweis kleine Steine
• Bilder: max. 3 mm Schichtdicke
5 mm
} 3 mm SD } 5 mm SD
Yam BL, Radiol Clin North Am 2014
MRCP: Untersuchungsqualität
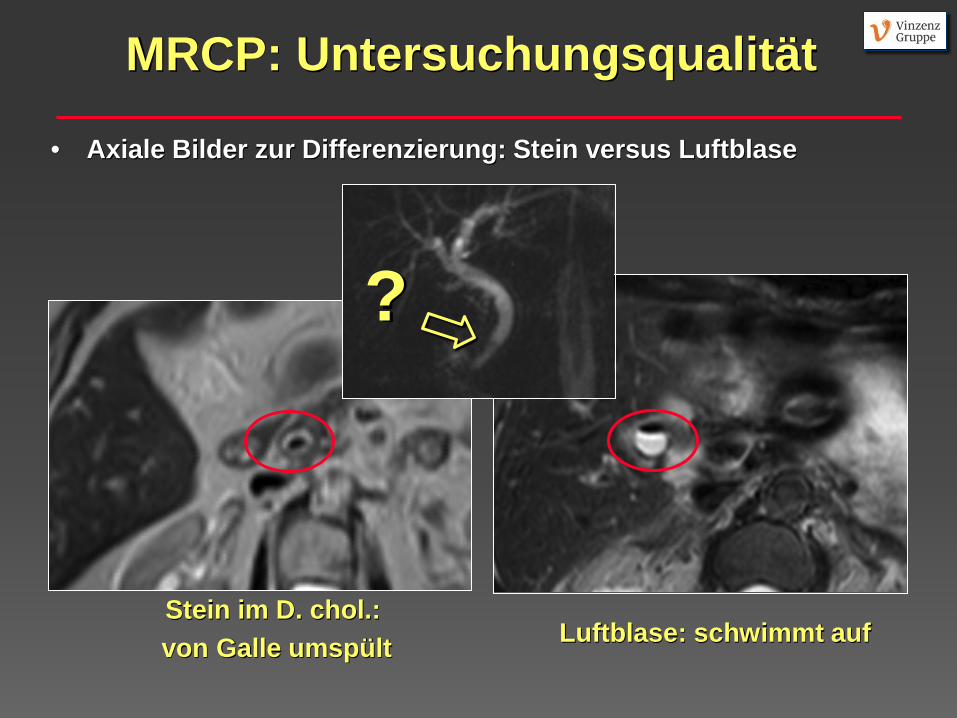
• Axiale Bilder zur Differenzierung: Stein versus Luftblase
Stein im D. chol.: von Galle umspült Luftblase: schwimmt auf
?
MRCP: Untersuchungsqualität
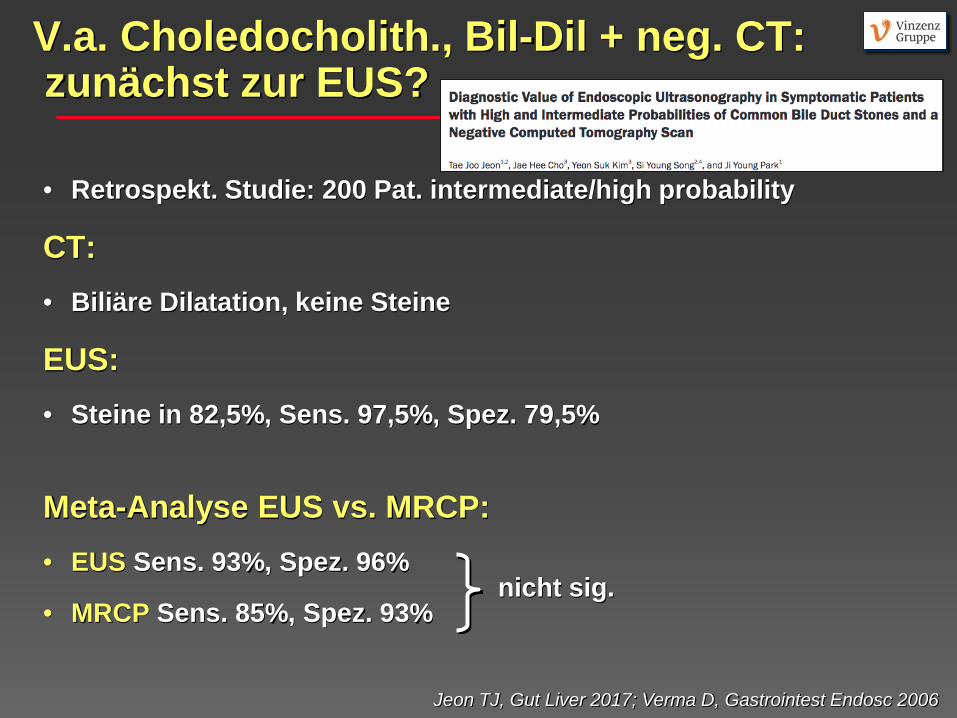
V.a. Choledocholith., Bil-Dil + neg. CT: zunächst zur EUS?
• Retrospekt. Studie: 200 Pat. intermediate/high probability
CT: • Biliäre Dilatation, keine Steine
EUS: • Steine in 82,5%, Sens. 97,5%, Spez. 79,5%
Meta-Analyse EUS vs. MRCP: • EUS Sens. 93%, Spez. 96%
• MRCP Sens. 85%, Spez. 93%
Jeon TJ, Gut Liver 2017; Verma D, Gastrointest Endosc 2006
nicht sig.
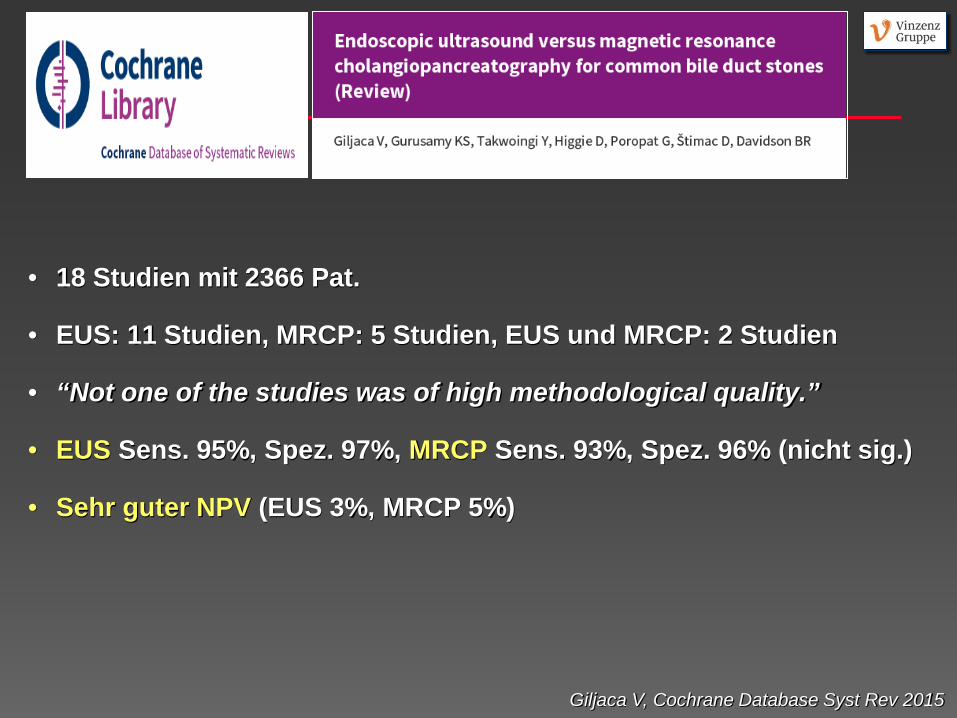
• 18 Studien mit 2366 Pat.
• EUS: 11 Studien, MRCP: 5 Studien, EUS und MRCP: 2 Studien
• “Not one of the studies was of high methodological quality.”
• EUS Sens. 95%, Spez. 97%, MRCP Sens. 93%, Spez. 96% (nicht sig.)
• Sehr guter NPV (EUS 3%, MRCP 5%)
Giljaca V, Cochrane Database Syst Rev 2015
Conclusion: • “People with neg. EUS or MRCP do not need further invasive tests.”
• “The two tests are similar in terms of diagnostic accuracy and the choice of which test will be informed by availability and contra-indications to each test.”
Giljaca V, Cochrane Database Syst Rev 2015
Dilatation D. chol. und/oder D. panc., normale LFP
Retrospektiv, 83 Pat.: 1. Dilatation D. chol. und/oder D. panc. 2. Normale LFP Signifikante Findings in EUS:
• Bei Dilatation D. chol.: 20%
• Bei Dilatation D. panc.: 60%
• Bei Dilatation D. chol. + d. panc.: 13% (kausal aber nur in 2.6%)
Oppong KW Scand J Gastroenterol 2014
• Isolierte Dilatation D. chol. nach CHE: assoz. mit neg. EUS • “EUS should ideally follow review of original cross-sectional imaging by a specialist radiologist”
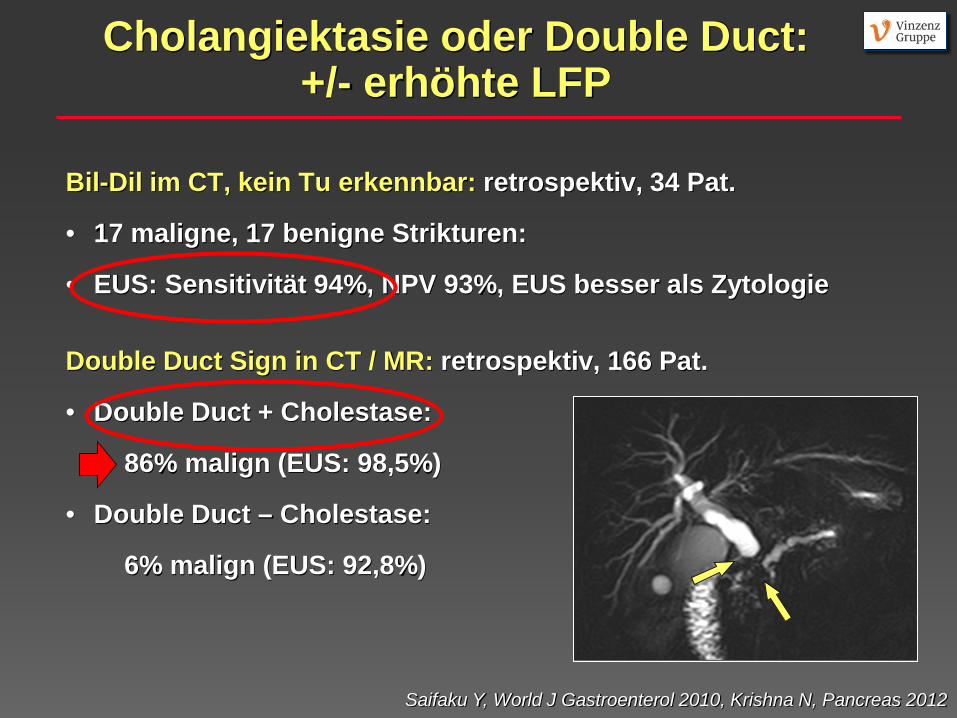
Cholangiektasie oder Double Duct: +/- erhöhte LFP
Bil-Dil im CT, kein Tu erkennbar: retrospektiv, 34 Pat.
• 17 maligne, 17 benigne Strikturen:
• EUS: Sensitivität 94%, NPV 93%, EUS besser als Zytologie
Double Duct Sign in CT / MR: retrospektiv, 166 Pat.
• Double Duct + Cholestase:
86% malign (EUS: 98,5%)
• Double Duct – Cholestase:
6% malign (EUS: 92,8%)
Saifaku Y, World J Gastroenterol 2010, Krishna N, Pancreas 2012
Zufällig entdeckte Dilatation D. chol.: Systematischer Review
• Insgesamt 9 Studien
• Vermischung Pat. mit erhöhten und normalen LFP
• EUS pos. bei erhöhten LFP 53%, normalen LFP 6%
Smith I, J Clin Gastroenterol 2015
• “The best diagnostic approach for patients with
incidental CBD dilatation is unknown.”
• “The truly asymptomatic patient with normal liver tests
in whom bile duct dilatation is found incidentally should be
followed closely with clinical and laboratory follow-up ...”
Dilatation D. chol bei normalen LFP: keine weitere Bildgebung
Schmerzloser Ikterus: Was tun bei V. a. Gallengangsstenose?
1. Optimiertes MDCT-Protokoll:
• Auswärtige CT kritisch evaluieren (Befund und Bilder!)
• MDCT: 2019 CT- Standard definiert von ÖRG + BURA
hinsichtlich Schichtdicke, KM-Menge, 3D-Rekonstruktionen 2. MRCP + KM-verstärkte MRT
• MRCP allein reicht nicht: Gangabbruch ja, Ursache nein 3. EUS +/- Biopsie
• Nach Verfügbarkeit und lokaler Expertise
http://www.oerg.at/tl_files/banner/00News%200419/OERG%20CT%20Protokolle%20A2_rz.pdf
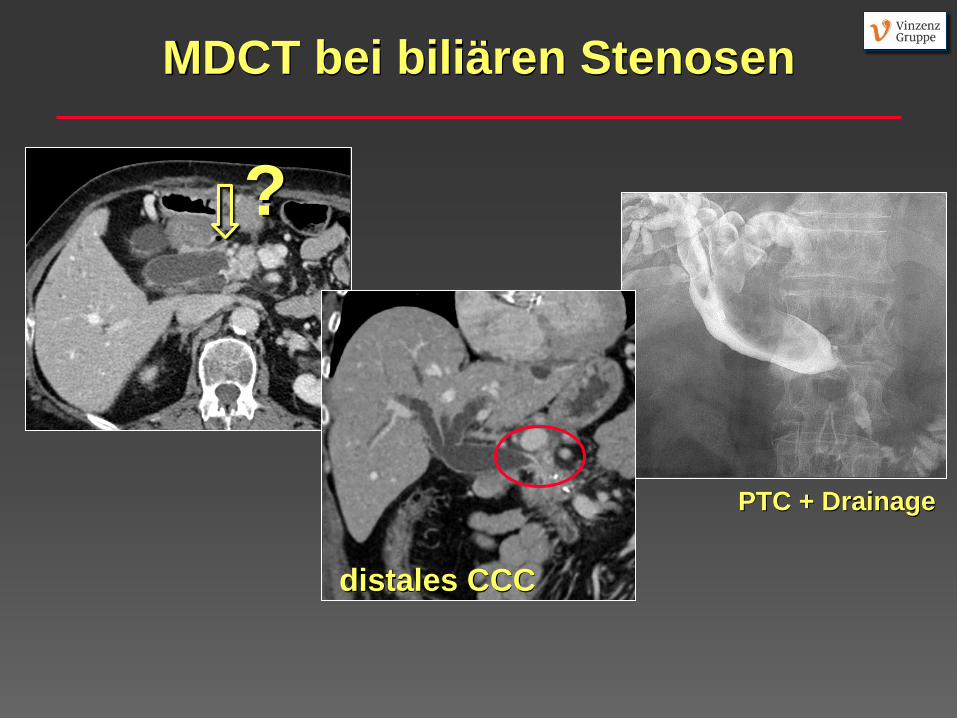
MDCT bei biliären Stenosen
?
PTC + Drainage
distales CCC
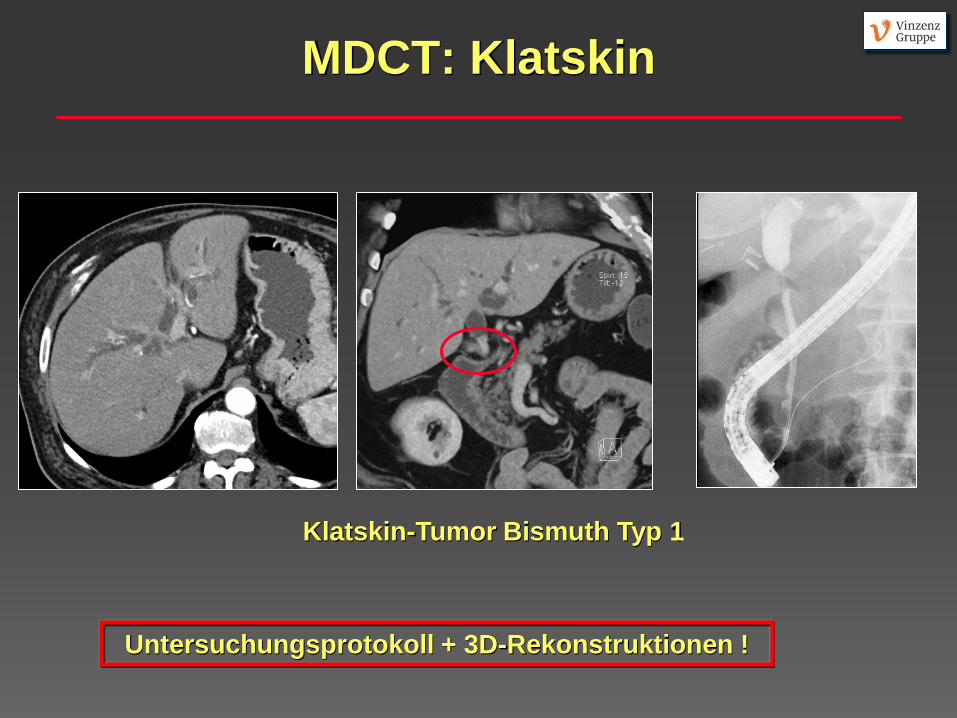
MDCT: Klatskin
Untersuchungsprotokoll + 3D-Rekonstruktionen !
Klatskin-Tumor Bismuth Typ 1
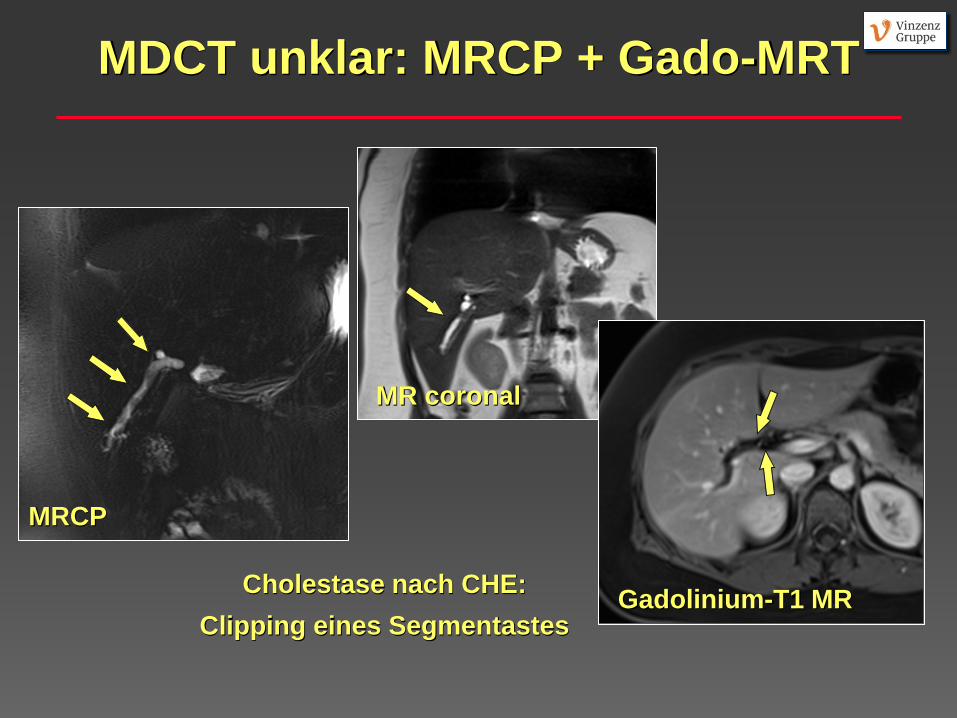
MDCT unklar: MRCP + Gado-MRT
Cholestase nach CHE: Clipping eines Segmentastes
MRCP
MR coronal
Gadolinium-T1 MR
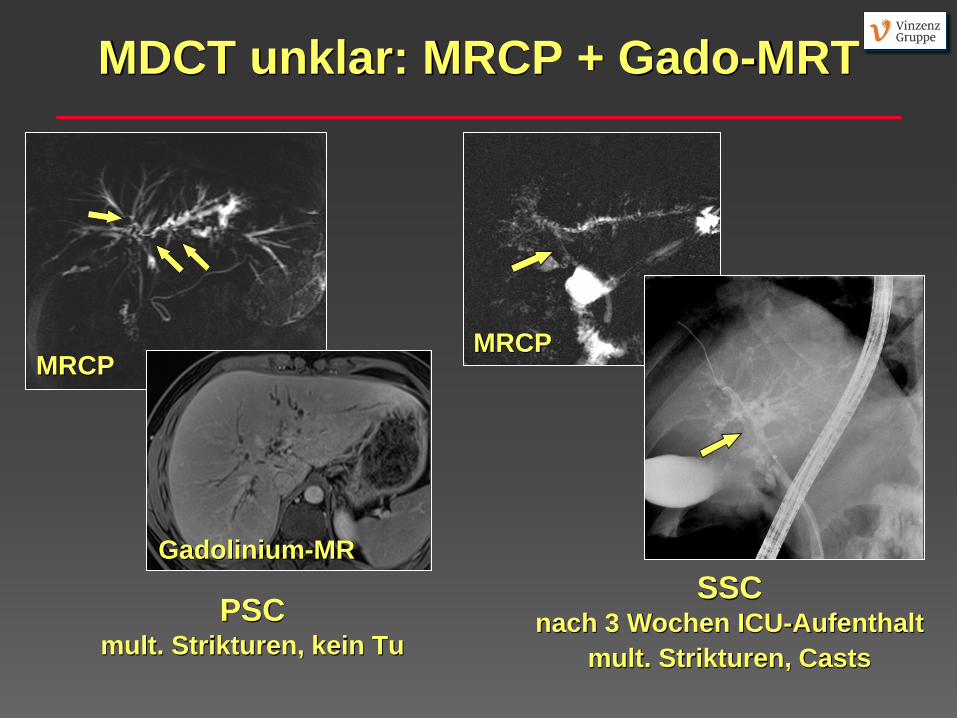
MDCT unklar: MRCP + Gado-MRT
PSC mult. Strikturen, kein Tu
SSC nach 3 Wochen ICU-Aufenthalt
mult. Strikturen, Casts
MRCP MRCP
Gadolinium-MR
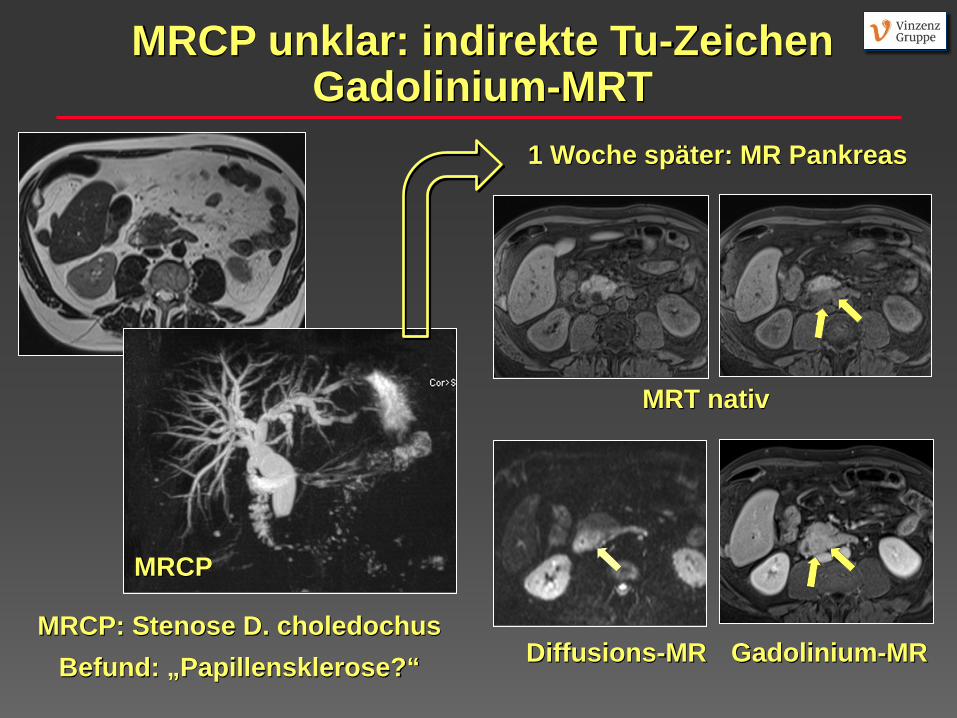
MRCP: Stenose D. choledochus Befund: „Papillensklerose?“
MRT nativ
Gadolinium-MR Diffusions-MR
1 Woche später: MR Pankreas
MRCP unklar: indirekte Tu-Zeichen Gadolinium-MRT
MRCP
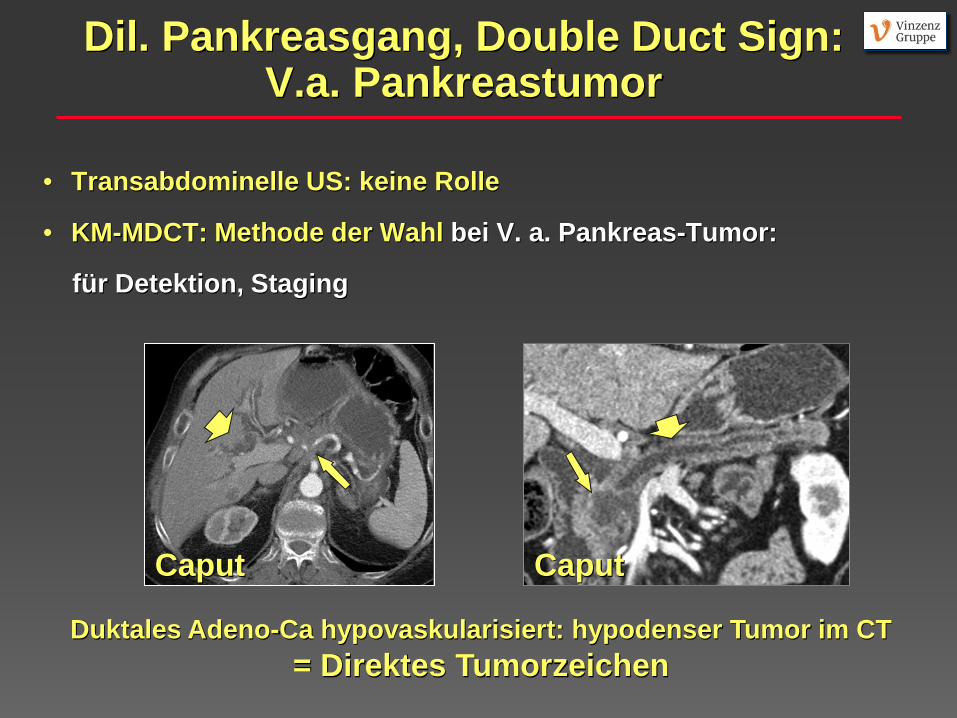
Dil. Pankreasgang, Double Duct Sign: V.a. Pankreastumor
• Transabdominelle US: keine Rolle
• KM-MDCT: Methode der Wahl bei V. a. Pankreas-Tumor:
für Detektion, Staging
Caput
Duktales Adeno-Ca hypovaskularisiert: hypodenser Tumor im CT = Direktes Tumorzeichen
Caput
Prokesch R, Radiology 2002; Takeshita K, Br J Radiol 2010
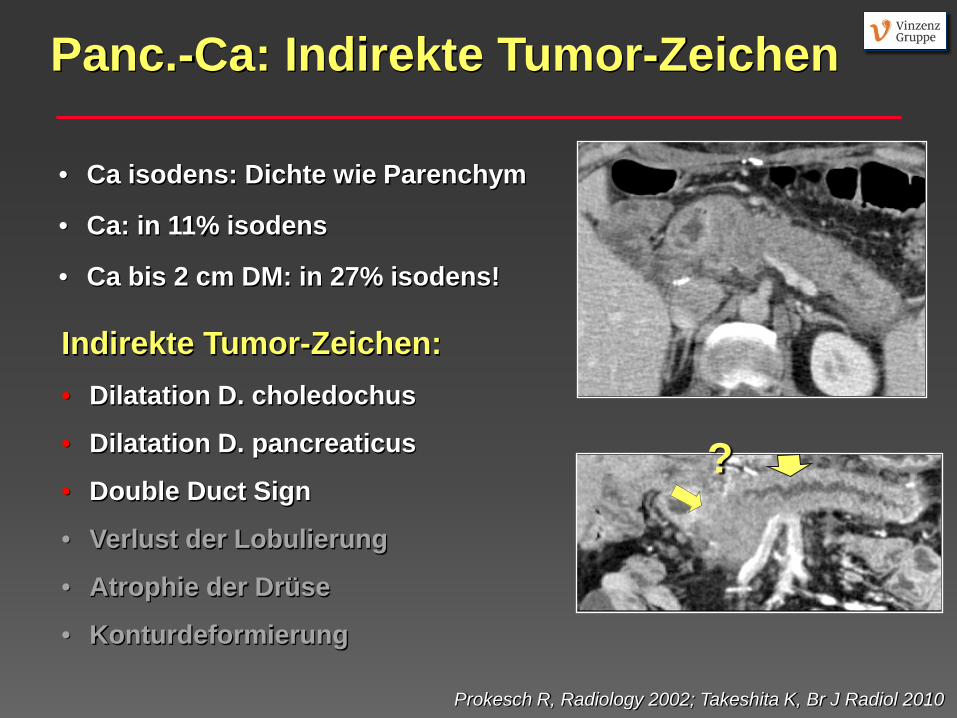
Indirekte Tumor-Zeichen: • Dilatation D. choledochus
• Dilatation D. pancreaticus
• Double Duct Sign
• Verlust der Lobulierung
• Atrophie der Drüse
• Konturdeformierung
• Ca isodens: Dichte wie Parenchym
• Ca: in 11% isodens
• Ca bis 2 cm DM: in 27% isodens!
Panc.-Ca: Indirekte Tumor-Zeichen
?
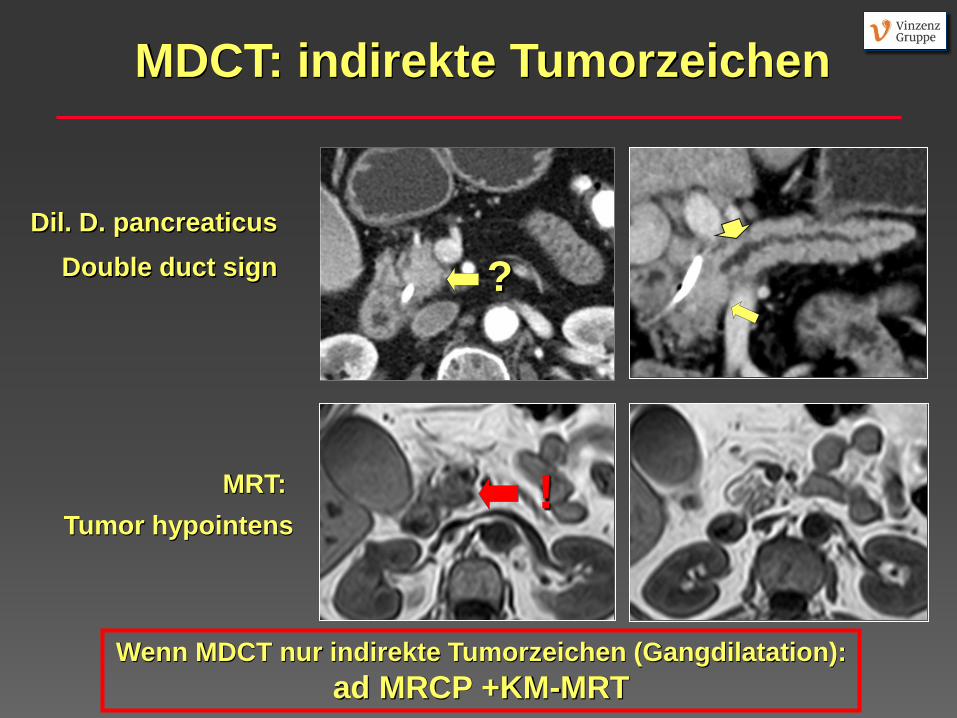
? Dil. D. pancreaticus
Double duct sign
MRT: Tumor hypointens
!
MDCT: indirekte Tumorzeichen
Wenn MDCT nur indirekte Tumorzeichen (Gangdilatation): ad MRCP +KM-MRT
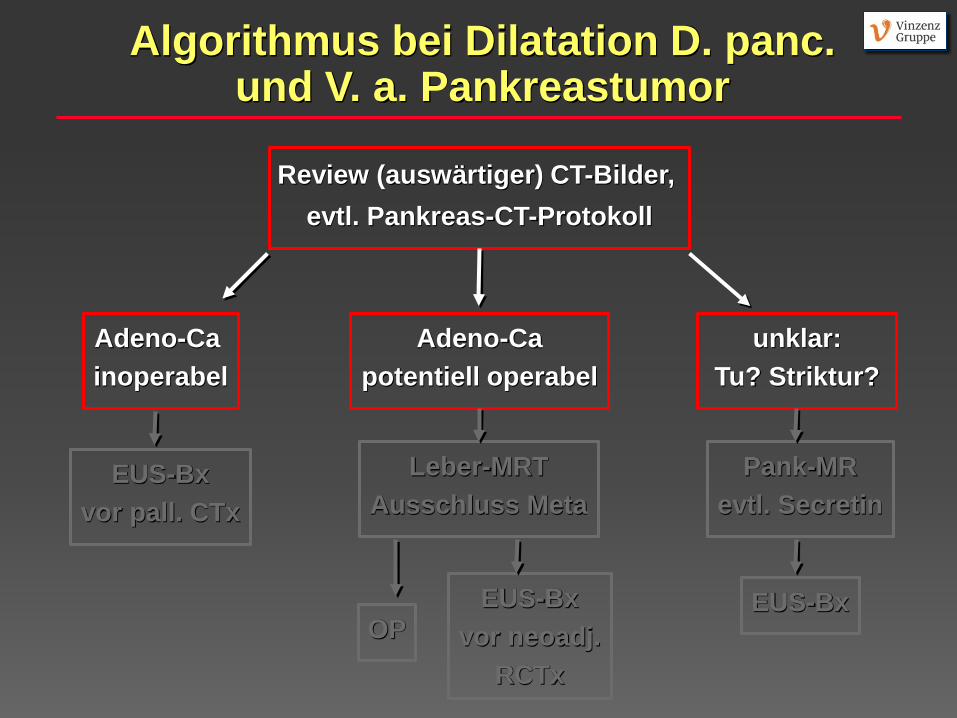
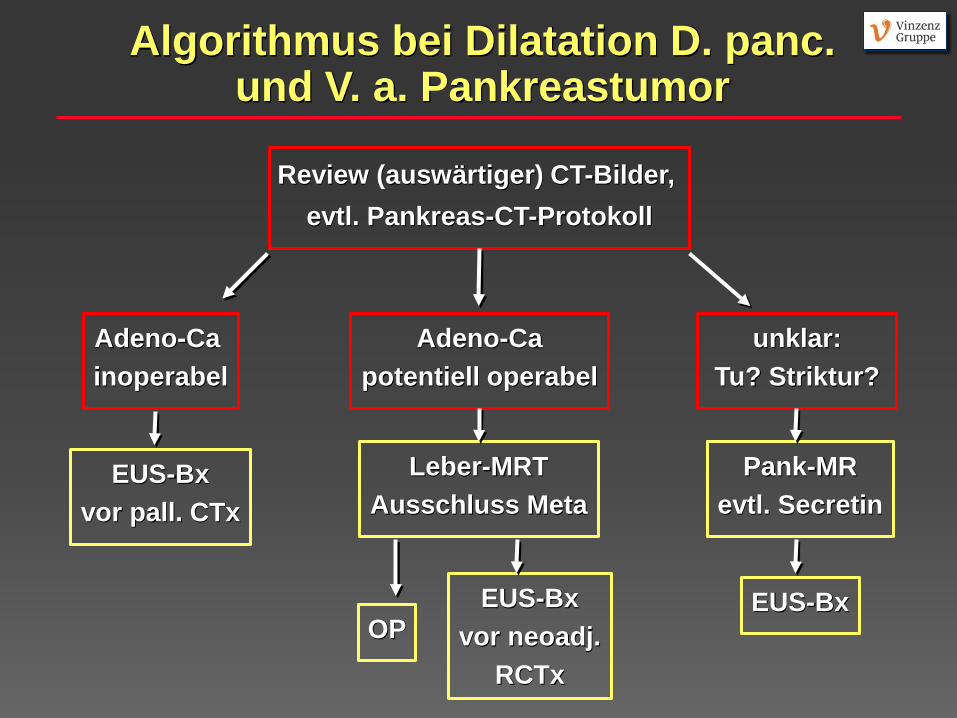
Algorithmus bei Dilatation D. panc. und V. a. Pankreastumor
Review (auswärtiger) CT-Bilder, evtl. Pankreas-CT-Protokoll
Adeno-Ca inoperabel
Adeno-Ca potentiell operabel
unklar: Tu? Striktur?
EUS-Bx vor pall. CTx
Leber-MRT Ausschluss Meta
OP EUS-Bx
vor neoadj. RCTx
Pank-MR evtl. Secretin
EUS-Bx
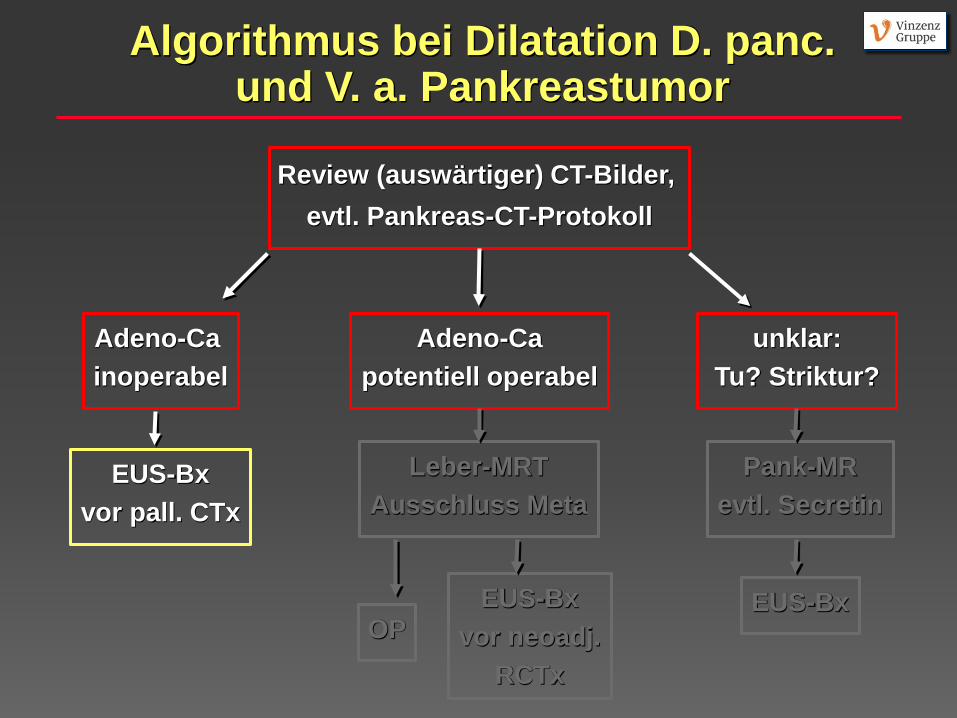
Algorithmus bei Dilatation D. panc. und V. a. Pankreastumor
Review (auswärtiger) CT-Bilder, evtl. Pankreas-CT-Protokoll
Adeno-Ca inoperabel
Adeno-Ca potentiell operabel
unklar: Tu? Striktur?
EUS-Bx vor pall. CTx
Leber-MRT Ausschluss Meta
OP EUS-Bx
vor neoadj. RCTx
Pank-MR evtl. Secretin
EUS-Bx
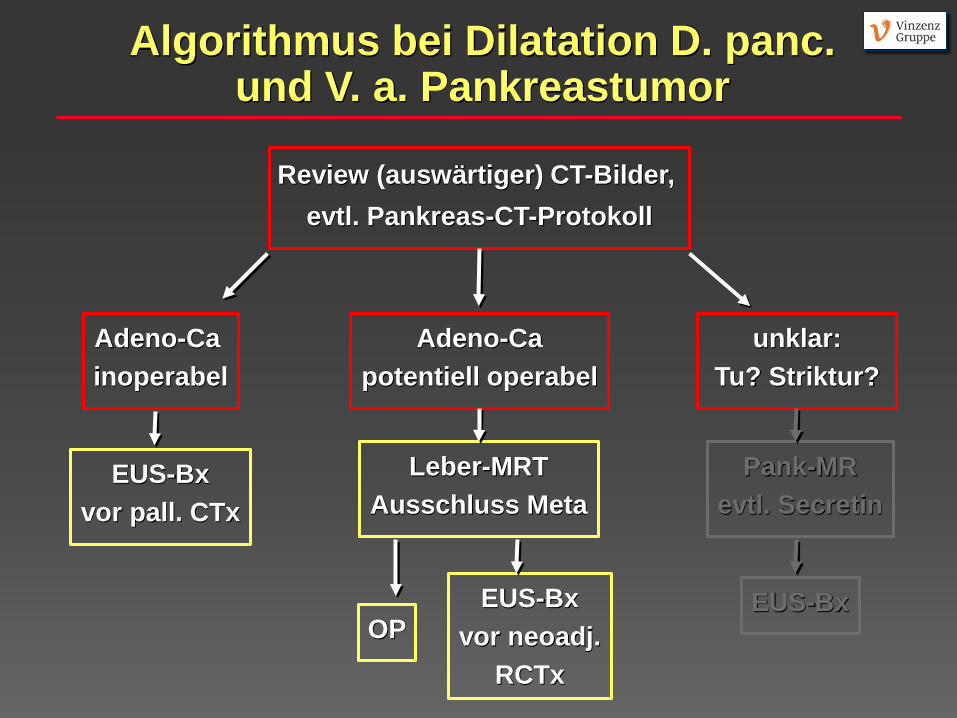
Algorithmus bei Dilatation D. panc. und V. a. Pankreastumor
Review (auswärtiger) CT-Bilder, evtl. Pankreas-CT-Protokoll
Adeno-Ca inoperabel
Adeno-Ca potentiell operabel
unklar: Tu? Striktur?
EUS-Bx vor pall. CTx
Leber-MRT Ausschluss Meta
OP EUS-Bx
vor neoadj. RCTx
Pank-MR evtl. Secretin
EUS-Bx
Algorithmus bei Dilatation D. panc. und V. a. Pankreastumor
Review (auswärtiger) CT-Bilder, evtl. Pankreas-CT-Protokoll
Adeno-Ca inoperabel
Adeno-Ca potentiell operabel
unklar: Tu? Striktur?
EUS-Bx vor pall. CTx
Leber-MRT Ausschluss Meta
OP EUS-Bx
vor neoadj. RCTx
Pank-MR evtl. Secretin
EUS-Bx
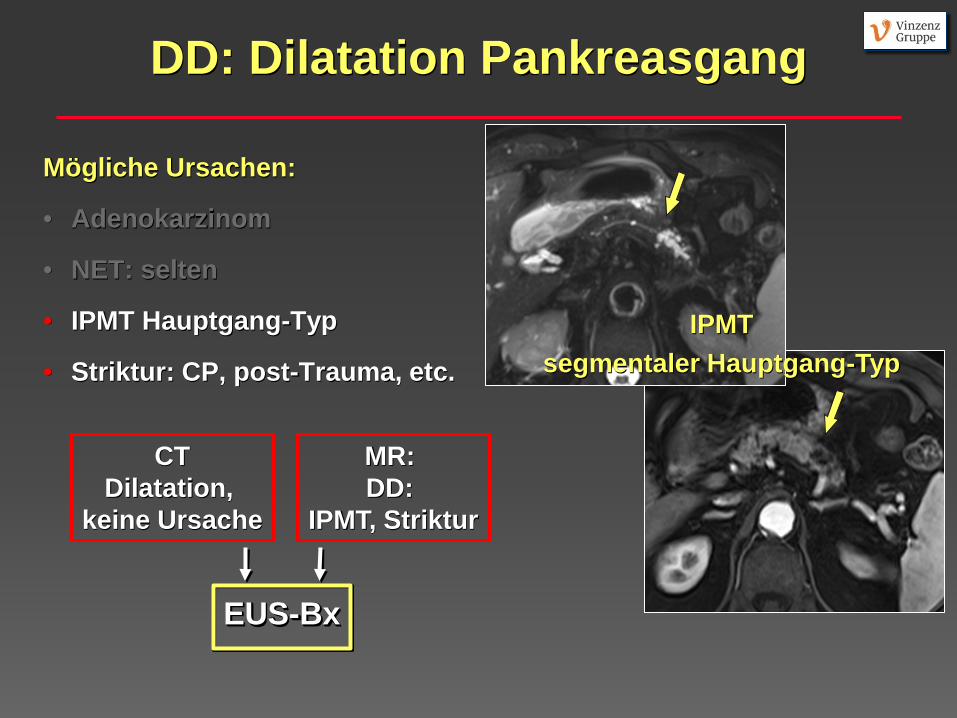
DD: Dilatation Pankreasgang
Mögliche Ursachen:
• Adenokarzinom
• NET: selten
• IPMT Hauptgang-Typ
• Striktur: CP, post-Trauma, etc. IPMT
segmentaler Hauptgang-Typ
CT Dilatation,
keine Ursache
MR: DD:
IPMT, Striktur
EUS-Bx
Zusammenfassung:
V. a. Cholangiolithiasis: • MRCP oder EUS: nach neg. Test keine weitere Abklärung Isolierte Dilation D. choledochus ohne Cholestase: • Geringer Zusatznutzen der EUS, keine Bildgebung Dil. Gallenwege (o. Double Duct) + schmerzloser Ikterus: • Keine gute Evidenz: MDCT, wenn unklar: MRCP+KM-MR, EUS
Dilatation Pankreasgang: • Eine Herausforderung! EUS oft notwendig




















![Personalisierung von EUS für Entscheidungsprozesse von Experten · 2012-12-21 · Abb. 3: Ablauf der Critical Decision Method (aufbauend auf [HoCS98, S. 272-274]) Zur Aufbereitung](https://img.pdfslide.org/doc/110x75/5f04a1157e708231d40eeb1c/personalisierung-von-eus-fr-entscheidungsprozesse-von-experten-2012-12-21-abb.jpg)







