Embed Size (px)
Citation preview
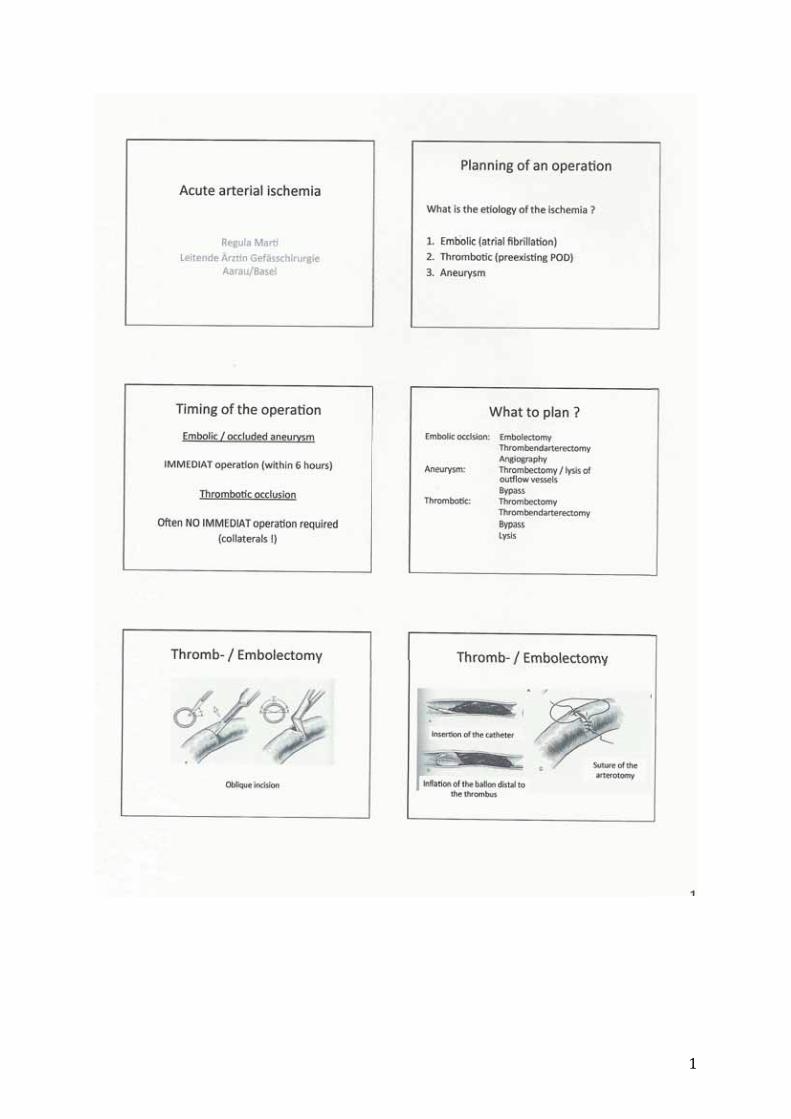
„How I do it 6“ Weiterbildungstagung Forum Junger Chirurgen SGC Journée de formation du Forum des Jeunes Chirurgiens SSC Baar/Zug 20. April 2013/ 20 avril 2013
Programm/Programme Vorsitz Vor- bzw. Nachmittagssitzung Modération séance du matin/après-midi André Rotzer, Andreas Rindlisbacher ab 08.00h Registration, Kaffee/Gipfeli/ dès 08.00h inscription, petit déjeuner 08.45h Begrüssung/Accueil: FJC Vorstandsmitglieder/membres du comité du FJC 09.00-09.30h Analfistel/Fistule anale Stephan Bischofberger 09.30-10.00h Laparotomie... und –Verschluss!/ Annette Ringger Laparotomie... et la fermeture de l`abdomen 10.00-10.30h Darm-Anastomosen/Anastomoses intestinales Renata Jori 10.30-11.00h Kaffeepause/Pause café 11.00-11.30h Freie Luft im Abdomen, und jetzt?/ Hervé Probst Air libre dans l’abdomen, que faire? 11.30-12.00h Akuter arterieller Verschluss/ Regula Marti Occlusion arterielle aïgue 12.00-12.30h Urologie für Allgemeinchirurgen/ Patrick Maurer L’urologie pour les chirurgiens généralistes 12.30-13.00h Forum Junger Chirurgen : Ziele und Aktivitäten FJC Forum des Jeunes Chirurgiens: objectifs et activités 13.00-14.00h Lunch 14.00-14.30 Materialschlacht: DC, LC-DC, LISS... was ist was? / Jörg Winkler La lutte du matériel: DC, LC-DC, LISS... lequel sert à quoi? 14.30-15.00h Fixateur externe/fixateur externe Philipp Stillhard 15.00-15.30h Luxationen und ihre Reposition/ Luxations et leur reduction Gian Melcher 15.30-16.00h Versorgung der pertrochantären Femurfraktur/ Thomas Beck Le traitement de la fracture pertrochantérienne ab 16.00h Abschiedsapéro/dès 16.00h Apéritif de clôture
Thema/Sujet: How I do it Datum/ Date: 20 April 2013/ 20 avril 2013 Ort/Lieu: Hörsaal, Kantonsspital Zug, Baar/ Auditorium de l’Hôpital Cantonal de Zug, Baar Kosten/Tarif : Bei Anmeldung bis 14.04.13: 50.00 sFr.
bar zu bezahlen bei Registrierung/ Jusqu’au 14.04.13: 50 CHF à payer en espèces lors de l’inscription Vor Ort: 70 sFr. bar zu bezahlen bei Registrierung/ Sur place: 70 CHF à payer en espèces lors de l’inscription
Anmeldung/Inscription: per E-mail an Alexandra Nagy, Vorstand FJC
[email protected] par e-mail à Alexandra Nagy, Comité FJC [email protected] Registrierung/Enregistrement: am Morgen des Fortbildungstages vor Ort le matin, sur le site de la journée de formation Akkreditierung/Accréditation: 6 Credits/6 crédits Teilnehmer/Participation: Für alle Chirurgen in Ausbildung S’adresse à tous les chirurgiens en formation Auskunft/Renseignements: [email protected] oder/ou
Beschreibung: Die Veranstaltung steht unter dem Motto „How I do it“ und wird aus Kurzreferaten à jeweils 30 min. (inkl. Diskussion) über häufige chirurgische Eingriffe bestehen. Es geht nicht darum, etwas über Krankheitsbilder im klassischen Sinne mit Diagnostik, Indikation usw. zu erfahren. Vielmehr wird Schritt für Schritt beschrieben, wie ein bestimmter Eingriff zu erfolgen hat und natürlich auch was zu vermeiden ist („pit-falls“). Also ganz pragmatisch – das Handwerk der Chirurgie. Den Besuchern dieser Fortbildung wird am Ende zu jedem Referat ein Hand-out abgegeben auf dem die Referenten ihre Schritt-für-Schritt-Anweisungen festgehalten haben.
Description: La journée de formation s’articule autour du thème „How I do
it“. Elle est constituée d’exposés de 30 minutes (incluant la discussion) portant sur des interventions chirurgicales courantes. Ni la théorie pertinente aux diverses pathologies, ni les indications opératoires ne seront discutées. L’exécution des interventions sera décrite étape par étape, et les pièges à éviter seront présentés. Il s’agira donc d’exposés pragmatiques portant sur les aspects purement techniques de la chirurgie. A la fin des exposés, un document sera remis aux participants avec les instructions étape par étape des opérateurs.
Organisation: Forum Junger Chirurgen SGC/ Forum des Jeunes Chirurgiens SSC
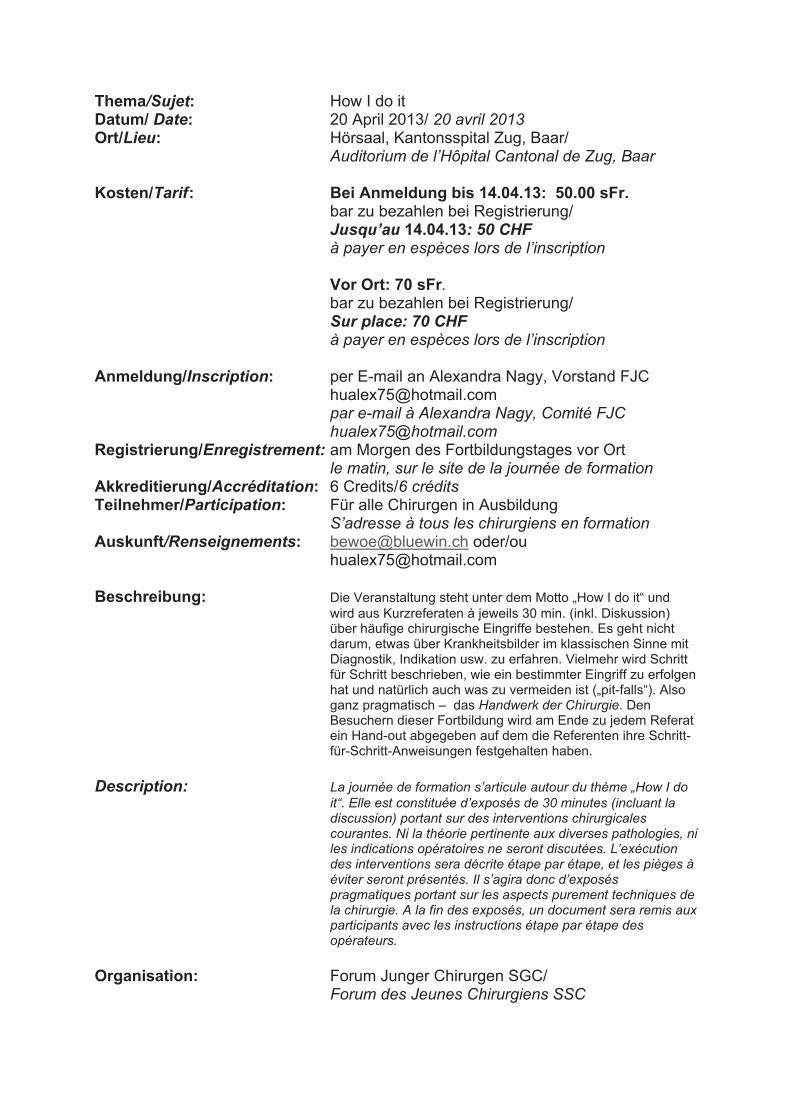
Anreise Bus: ZVB-Linie 3 Oberwil-Baar (Haltestelle Bahnhof Baar, 5 Minuten zu Fuss) ZVB-Linie 8 Rotkreuz-Cham-Steinhausen-Kantonsspital-Bahnhof Baar Verschiedene ZVB- und Postauto-Linien (Haltestelle Bahnhof Baar) Bahn: Stadtbahn Zug S1 Luzern-Rotkreuz-Zug-Baar (Bahnhof Baar, 5 Minuten zu Fuss) Schnellzüge Luzern-Zug-Zürich mit stündlichem Halt in Baar
Directions Avec les transports publics: ZVB bus ligne 3 Oberwil-Baar, arrète gare Baar ZVB ligne 8 Rotkreuz-Cham-Steinhausen-Kantonsspital-Bahnhof Baar En train: train S1 Lucerne-Rotkreuz-Baar
Sponsoren: siehe Industrieausstellung im Vorraum Commenditaires: voir les exposants dans la pièce attenante

Hauptsitz Medartis AG | Hochbergerstrasse 60E | CH-4057 Basel
Medartis GmbH | Am Gansacker 10 | D-79224 Umkirch
Medartis GmbH | Impulszentrum Fabrik I Rheinstrasse 26-27 I A-6890 Lustenau
www.medartis.com
Medartis ist einer der führenden Hersteller von medizinischen Produkten für die Osteosynthese im Bereich des Gesichtsschädels und der Extremitäten. Medartis hat sich zum Wohle des Patienten verp� ichtet, Chirurgen und OP-Personal mit den innovativsten Titanimplantaten und Instrumenten zu versorgen und den besten Service zu bieten.
MODUS TriLockk k k 2.0/0/0/0/0/22222.333/2.5
• TriLock - multidirektional UND wwwwwiiiininkelstaaabibibibibilllll
• Anatomische Plattendesigns
• HexaDrive - die neue Schraubengeneration
• Erhöhte Primärstabilität
• Keine Schraubenlockerung und Dislokation
• Weniger Implantatmaterial notwendig
• Verkürzte Operationszeit

How You do it Korrekte Vorbereitung auf eine Operation
Vortag: Allgemeinzustand? Relevante Nebendiagnosen? Spezielle Anamnese / Status
- Voroperationen? - OP – Region untersuchen: Narben? Lokaler Infekt? Auffälligkeiten in der
Umgebung (z.B. Hauttumore: gleichzeitige Exzision?, Nabelhernie bei Laparoskopie), periphere Pulse +Sensibilität vorhanden (vor Osteosynthesen)
- Gerinnungscheck: Aspirin?, Plavix?, Marcoumar?, Sintrom? Thromboembolierisiko?
- stimmt OP-Indikation? (Eingriff bei diesem Pat. Zu diesem Zeitpunkt gerechtfertigt?
Vorbereitungen :
- OP-Aufklärung - Seite markieren - Präoperative Antibiotikaprophylaxe festlegen - Thromboembolieprophylaxe festlegen - Aktuelle Röntgenbilder da? - Labor in Ordnung? (Gerinnung, Tc, Hb, Elektrolyte, Krea, andere für diese OP
relevanten Werte) - Korrektes Narkoseverfahren organisiert? (z.B. ist der Eingriff in LA möglich?) - Gedanken zur Lagerung und Abdeckung machen
Vorbereitung am Abend - Anatomie repetieren - Zugangsweg kennen - Operationstechnik lesen (vgl. Literaturtips)
OP-Tag
- pünktlich im OP sein !! - Lagerung kontrollieren - Korrekte Seite? - Falls nötig: DK gelegt? - Präoperative Antibiotikaprophylaxe gegeben? (1/2 h vor Schnitt!) - Benötigte Implantate (z.B. Platte, Netz, Port usw.) vorhanden - Röntgenschurz angezogen? (z.B. auch bei intraoperativer Cholangiographie!) - unbedingt steril bleiben ☺
Postoperativ:
- Redons offen? - Verordnungen (leserlich) schreiben:
Drainagenzug wann, Kostaufbau, Mobilisation,Physiotherapie, postoperative Antibiose, Thromboembolieprophylaxe, Fadenentfernung am XX postoperativen Tag, Sprechstundenkontrolle, Spezielles
- Falls nötig: Helfen beim Umlagern, auf Lagerung und Drainagen achten - Angehörige informieren - Patienten visitieren
- Histologie oder Bakteriologie: Zettel korrekt ausgefüllt? Literaturtips: Operationsatlas Chirurgie/Atlas of General Surgery – Schumpelick; Thieme Verlag Checkliste Chirurgie – Largiader, Saeger; Thieme Verlag Standardverfahren in der Orthopädie und Unfallchirurgie – Ewerbeck; Thieme Verlag Hernien – Schumpelick; Thieme Verlag Chirurgische Operationslehre – Breitner; DVD Sonderausgabe Urban & Fischer Techniques chirurgicales- les fiches Tome I- Lacaine F. ; Masson EMC: Encyclopédie Médico-chirurgicale-Elsevier Masson Oxford Handbook of Operative Surgery- McLatchie G.R.-Oxford University Press Surgical Exposures in Orthopaedics : The Anatomic Approach- Hoppenfeld S. ; Lippincott Williams & Wilkins Netter - Farbatlanten der Medizin; Thieme Verlag Sobotta - Atlas der Anatomie des Menschen; Urban & Fischer Rouvière - Anatomie humaine (3 tomes) Grant - Atlas of Anatomy
How You do it La préparation adéquate à une intervention chirurgicale
La veille: Anamnèse et status
- Antécédents chirurgicaux? - Examen clinique du site à opérer: cicatrices? Infection locale? - Anomalies environnantes (p.ex. tumeurs cutanées: excision simultanée?
Hernie ombilicale au cours d’une laparoscopie), pouls périphériques et sensibilité actuelle (avant ostéosynthèse)
- Hémostase: Aspirine? Plavix? Sintrom? Marcoumar? Risque thrombo-embolique?
Préparatopms:: - Explication de l‘intervention - Marquage du site opératoire - Etablissement de l’antibioprophylaxie préopératoire - Etablissement de la prophylaxie thrombo-embolique - Imagerie récente disponible sur place? - Labo préop en ordre? (Crase, formule sanguine, groupe sanguin, électrolytes,
urée, créatinine) - La narcose adéquate a-t-elle été organisée? (ex. l’intervention est-elle
réalisable sous anesthésie locale?) - Réfléchir à l’installation et au champage
Préparations du soir - Révision de l‘anatomie - Connaissance de la voie d‘abord - Lecture des aspects techniques (c.f. conseils de lecture)
Le jour opératoire
- Arrivée ponctuelle en salle d’opération!! - Contrôler l‘installation - Vérification du côté à opérer - Si nécessaire: sonde urinaire en place? - La prophylaxie antibiotique a-t-elle été administrée? (1/2 heure avant
l’incision) - Le matériel nécessaire est-il préparé? (ex. plaques, filets, trocarts, etc.) - Les tabliers de plomb sont-ils portés? - Eviter les fautres de stérilité ☺
Période postopératoire
- Les redons sont-ils ouverts? - Ordres postop écrits lisiblement:
Délai d’ablation des redons, réalimentation postop, mobilisation, physiothérapie, antibiothérapie postop, prophylaxie anti-thrombotique, ablation des fils à X jours, consultation de contrôle, autres.
- Aider au transfert du patient en veillant aux champs et aux drains - Informer la famille - Aller revoir le patient - Suivre les résultats histologiques et de bactériologie

How You do it come prepararsi correttamente ad un’operazione
Giornata preoperatoria: Anamnesi / stato clinico
- operazioni precedenti? - visita della regione operatoria: cicatrici? infezione locale? particolarità nelle
vicinanze (p.es. tumori cutanei: resezione contemporanea?, ernia umbilicale in caso di laparoscopia), polsi periferici e sensibilità intatti (prima di osteosintesi)
- controllo della coagulazione: Aspirina?, Plavix?, Marcoumar?, Sintrom? rischio tromboembolico?
Preparativi : - informazione e consenso scritto del paziente - contrassegnare il lato - stabilire la profilassi antibiotica preoperativa - stabilire la profilassi tromboembolica - esami radiologici attuali a disposizione? - esami di laboratorio in ordine? (coagulazione, Tc, Hb, elettroliti, creatinina) - organizzare un’anestesia adeguata (p.es. operazione possibile in anestesia
locale?) - pianificare la posizione del paziente e la copertura del campo operatorio
Preparativi alla sera - ripetizione dell’anatomia - conoscenza della via d’accesso - studio della tecnica operatoria (cfr. Literaturtips)
Giornata operatoria:
- arrivare puntuali in sala operatoria !! - controllare il posizionamento del paziente - lato corretto? - se necessario: catetere vescicale posizionato? - profilassi antibiotica applicata? (mezz’ora prima dell’incisione!) - impianti necessari a disposizione? (p.es. placca, rete, Port-a-Cath, ecc.) - vestiti di protezione dai raggi indossati? (p.es. in caso di colangiografia
intraoperatoria!) - assolutamente restare sterili ☺
Fase postoperatoria:
- drenaggi funzionanti? - prescrizioni postoperatorie (leggibili):
estrazione dei drenaggi, alimentazione, mobilizzazione, fisioterapia, antibiosi postoperativa, profilassi tromboembolica,stabilire quando togliere i punti, controlli in ambulatorio, particolarità
- aiutare nel riposizionare il paziente, prestando attenzione alla posizione e ai drenaggi
- informazione dei parenti - visita del paziente - controllo dei risultati istologici o batteriologici

Literaturtips: Operationsatlas Chirurgie – Schumpelick; Thieme Verlag Checkliste Chirurgie – Largiader, Saeger; Thieme Verlag Standardverfahren in der Orthopädie und Unfallchirurgie – Ewerbeck; Thieme Verlag Hernien – Schumpelick; Thieme Verlag Chirurgische Operationslehre – Breitner; DVD Sonderausgabe Urban & Fischer Netter - Farbatlanten der Medizin; Thieme Verlag Sobotta – Atlas der Anatomie des Menschen; Urban & Fischer
Hauptsitz Medartis AG | Hochbergerstrasse 60E | CH-4057 Basel Medartis GmbH | Am Gansacker 10 | D-79224 UmkirchMedartis GmbH | Impulszentrum Fabrik I Rheinstrasse 26-27 I A-6890 Lustenau www.medartis.com
Medartis ist einer der führenden Hersteller von medizinischen Produkten für die Mund-, Kiefer- und Gesichtschirurgie, die Hand- und Plastische sowie die orthopädische Traumachirurgie. Medartis hat sich zum Wohle des Patienten verp� ichtet, Chirurgen und OP-Personal mit den innovativsten Titanimplantaten und Instrumenten zu versorgen und den besten Service zu bieten.
APTUS® Ellenbogensystem 2.0, 2.8
Sichere und stabile Osteosynthese komplexer Ellenbogenfrrrraaaakkkkktttuuuuurrrrreeeeennnnn
• Multidirektionale und winkelstabile TriLock® Verblockungs-technologie (±15°)
• Anatomisches Plattendesign und niedriges Plattenpro� l zzzzuuuurur VVVVVerererrrreree mememememememememeidididididididi unng g gvon Weichteilirritationen
• Neuartiges Implantatsortiment für Zug- und Doppppepepepelllplpppppplalalalaaaatttttttt enenenennnntetetetetttt chhninikkkk

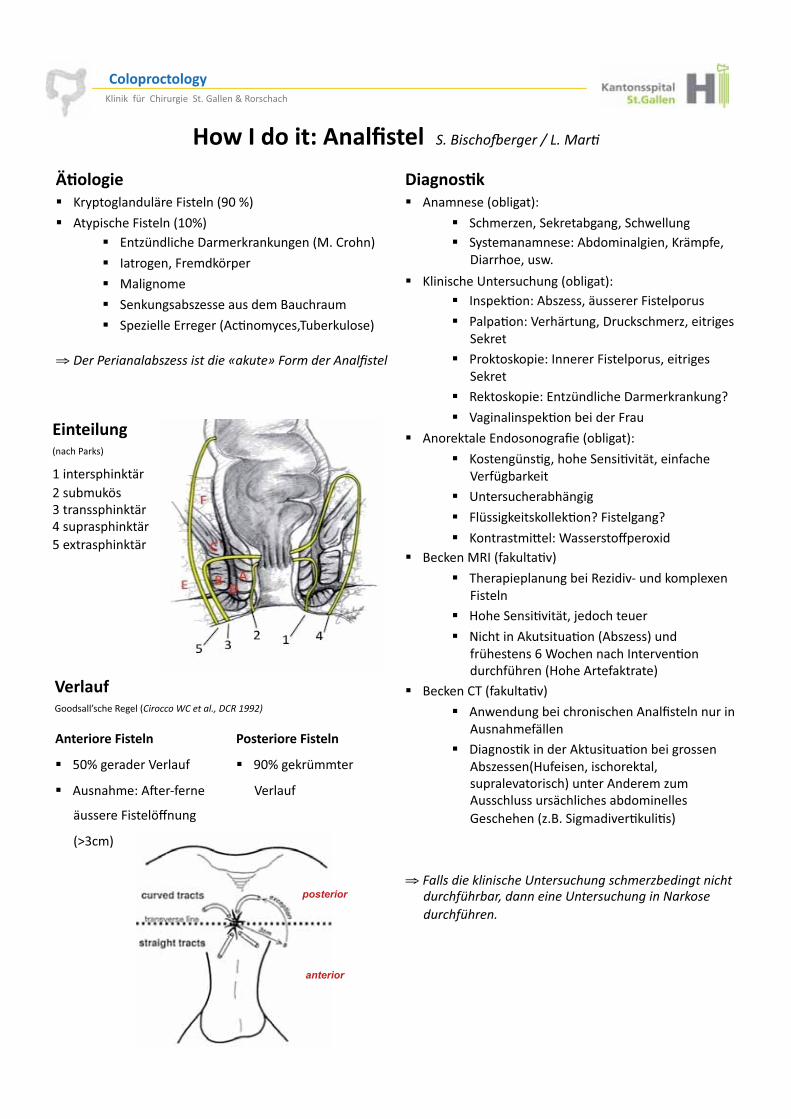
������������� ���������������� �� �������� ��
���������������������������� ���������������������������
����������������������
��������������� �� !" �#��$��������������%�� �����������&��'�����������
���� ������(����)�������������� �������������������������
posterior
anterior
�� �������� *��"�������!������+��
� ���"�,��-�������!����-����.��� ���� �/���"���"����+�*!(�"��������-���"���-�
0�����-� �.��
� ����������1���� �� �����!������+�� 2�����3��+�*!�,���-�� �����4������� ���
� �����3��+�5���� ��-�0 �����"�,-���������������
� �����������+�2�����4������� �-���������������
� �����������+�6��,�(������0�"����� ��7�
� 5������������3���!���(��4� �
� *���������6�(�������8����!������+�
� ���������3�-�����������39����-����������5���!������
� 1���� ����!�������
� 4����������������3��7�4���������7�
� �������"�:��+�;�������<���'�(�� =������>�2����� ���39��
� ?���������� ���!�����,�(�9@� �(���"���'���4�������
� A���������39����-�B�(������ ��
� C��������*� ���� �3����*!�,����� �(����������D�;�����������2���9��3���( ��������A����*�����������
� =�������?����� ���39��
� *�.��( ���!��������������*���8������� ����* ����"���������
� 0������3�����(��*�� ��� �3���!����������*!�,������A ������-�����������-�� ����9��������� ����*�(��"�, "�* ����� ��� ������������!(�"�������������������,�=�����"�(�9�3� ��3���
⇒ ������ ���!��"�����#"�� �$�$"����%� &'� �"���"���� $ �() '� �� �""���"��#"�� �$�$"���"�*� !��� $ �() �"��
���������� �/�������( ����4��������EF�G��
� *�/�������4���������FG��� 6��,�(������0�"����� ������>��������
� 2������-�4�"(�#���
� >������"���
� ���� ����!�,������ ��(�"�=� ��� "�
� ���,������6�����*�3��"/���-? !�� ������
⇒ �� �+� ��"���'�&�������� ���,�!$��-�� %� � �."��/�����
��������� ������
� &FG����(��5��� ��
� * ����"�+�*H�@�����
� �����4�����#<� ���
�I$�"��
!��������� ������
� EFG����""���
5��� ��
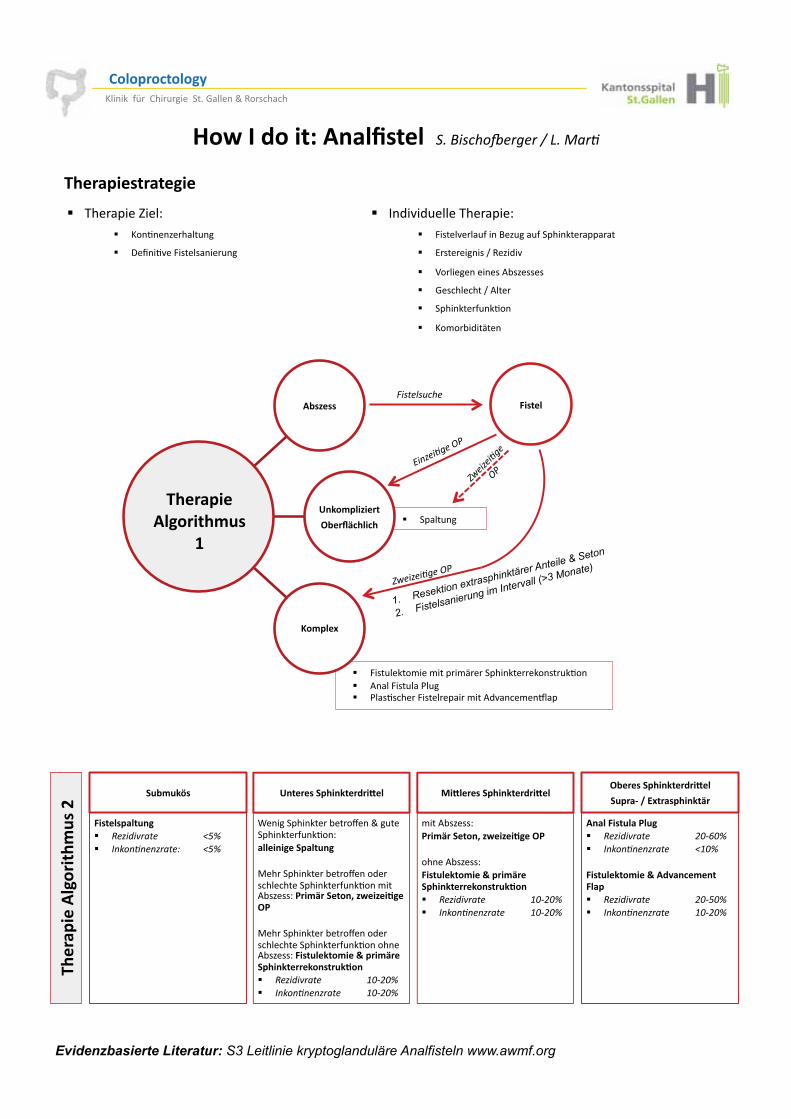
�"�#����
$���%���#����
&"��'(�)���)�
*�%���+�
�������$���
� ����� ���
� 4��� �����"���"�����"����������������� �3���� *����4��� ����� ��� ����3�����4����������"���*(9����"��J����
�����
01��&������2
+��
1. Resektion extrasphinktärer Anteile & Seton
2. Fistelsanierung im Intervall (>3 Monate)
,)�� ����������)%���
-�
,)�� ����� �����
������������� ���������������� �� �������� ��
��������������
� 2�(�9�( �����?������+�� 4�����9��� �����=�, ��� �����������������
� 6����������K���,�(�9�
� 5��������������*!�,������
� �����������K�*����
� ��������� ��3���
� ��"�!�(�������
� ?�������L���+�� ���3���,����� ���
� 0�8��39��4���������� ���
.�"%��/��
������ ������ ��&� �3 ���� � �456�� 7"!"�"�"& ���8 �456�
$������.�)��������0�� ��
;��������������!���<������ ������������ ��3��+�� ���������.� �����
>������������!���<����(��������������������� ��3���"���*!�,���+�!��%(��.���1�#���#������&!�
>������������!���<����(��������������������� ��3��������*!�,���+� �������%���2����%(���.�)������������������� ��&� �3 ���� � ��9:�96�� 7"!"�"�"& ���� ��9:�96�
3�0������.�)��������0���
"���*!�,���+��!��%(��.���1�#���#������&!�
�����*!�,���+�� �������%���2����%(���.�)������������������� ��&� �3 ���� � ��9:�96�� 7"!"�"�"& ���� ��9:�96�
&"�����.�)��������0���
.��� 4�5��+� ��)���(��
�� �� ���� �!����� ��&� �3 ���� � ��9:;96�� 7"!"�"�"& ���� �4�96�
�������%���2���6 ���%��� � ��� ��&� �3 ���� � ��9:596�� 7"!"�"�"& ���� ��9:�96�
,)�� �
���������)%
���7�
�������������� ���������������������������
Evidenzbasierte Literatur: S3 Leitlinie kryptoglanduläre Analfisteln www.awmf.org
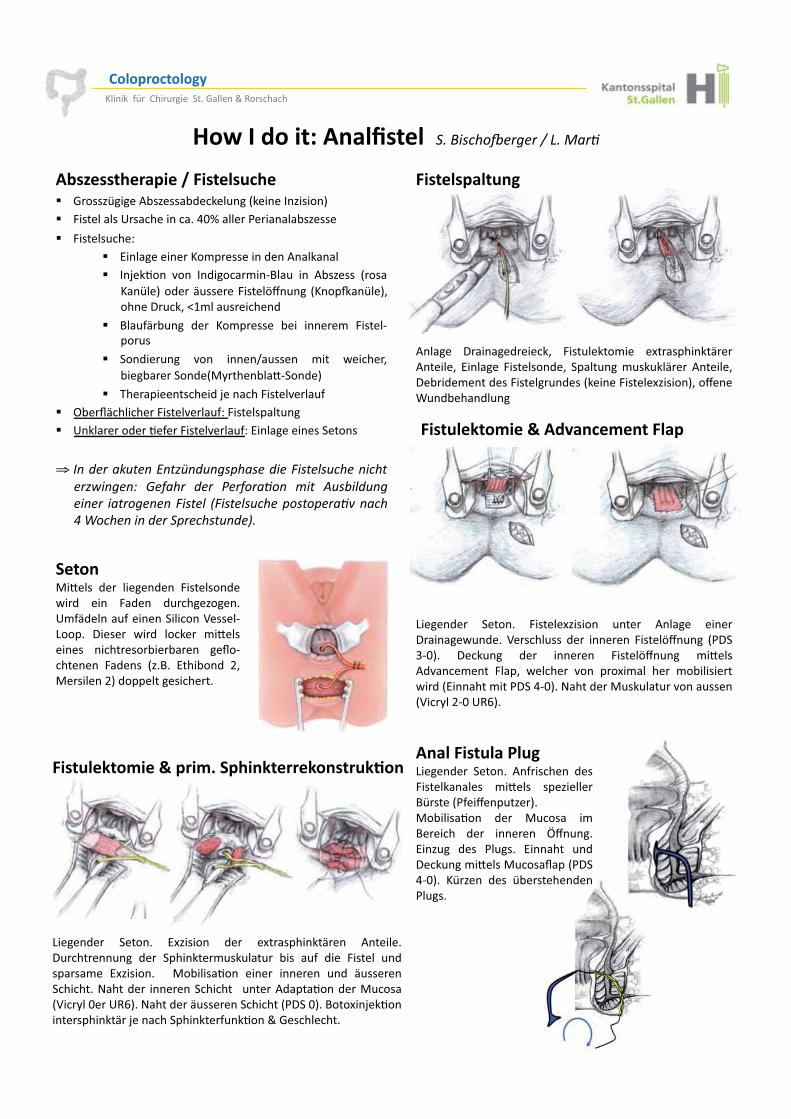
������������� ���������������� �� �������� ��
��������������
�"�#���)�� ����5� �������)��� ����,�����*!�,����!(����� ����������2�,�������� 4����������1�������������%FG��������������!�,�����
� 4������ ���+�� 6��������������"���������(���*���������� 2�B��3��� 9��� 2�(�����"��@=�� � ��� *!�,���� �����
��������(��� �����4�����#<� ��� �����M�����-������0 ��-�N�"��� �������(�
� =�� ��! ��� (�� ��"������ !��� �����"� 4�����@�� ��
� ���(�� ��� 9��� �����K� ����� "��� .�����-�!���!������(��>/����!��:@���(���
� ?��������������(�B�������4�����9��� ��� O!�P���������4�����9��� �+�4���������� ���� 1�������(��3����4�����9��� �+�6��������������������
⇒ 7"� � ��!$��"�<"�&)" $"��=���� ����������$���"����� &1�"��"8� >�(� � � � +� ( ��"� %��� .$�'�� $"����"� � ��� ��"�"�������� ?�������$���=��=� ��3�"���@����"��"� � ��= ����$" ����
������ �����
*������ 0������(�����-� 4��� �����"��� �'������������*������-� 6������� 4��������(�-� ����� ���" �� ����� *������-�0�!�(�"����(���4������ �(����������4������',������-��<����; �(!����(� ���
�������%���2���6 ���%��� � ��
Q�����(�� ������� 4������',������ ���� *������ �����0������. �(��� 5����� ��� (�� ������� 4�����#<� ��� ��0��$@F��� 0��� ��� (�� ������� 4�����#<� ��� "�:����*(9����"���� 4���-� .������ 9��� ��'�"��� ��� "�!��������.�(��6�������"����0��%@F���C����(��> �� ��� �9���� ������5��/�� @F�1�D���
.����>�:���� (�� ������(��� 4��������(��.�(� ���� 4�(��� ( ����,������1"��(����� ����������������5�����@Q����� 0����� .�(� ������ "�:���������� ��������!��!���� ��P�@�������� 4�(���� �,�=�� 6���!��(� -�>������� ��(�����������������
�������%���2����%8�.�)������������������
Q�����(�� ������� 6',������ (�� �'������������� *��������0 ������ ��� (�� ��������" �� ��� � !��� � �� (��� 4������ �(������"�� 6',������� � >�!�����3��� ����� ������� �(� � ���������������C����(�� ��������������� � ����*(����3���(��> ������5��/��F��1�D���C����(��� ����������������0��F���=���'��B��3����������������B���������������� ��3�����������������
Q�����(�� ������� *��������� (���4������������� "�:���� ���,������=���������<��� �,����>�!�����3��� (�� > ����� �"�=������ (�� ������� R<� ����6��, �� (��� �� ���� 6������� �(�0��� ���"�:����> ����P�����0��%@F��� �,��� (��� !�������(����� ����
�� �� ���� �!����
�������������� ���������������������������

MODUS®
und Unterkiefer
• Trauma• Orthognaththieiee• Rekonsnsttrukktitionon
Hauptsitz Medartis AG | Hochbergerstrasse 60E | CH-4057 Basel
Medartis GmbH | Am Gansacker 10 | D-79224 Umkirch
Medartis GmbH | Impulszentrum Fabrik I Rheinstrasse 26-27 I A-6890 Lustenau
www.medartis.com
Medartis ist einer der führenden Hersteller von medizinischen Produkten für die Osteosynthese im Bereich des Gesichtsschädels und der Extremitäten. Medartis hat sich zum Wohle des Patienten verp� ichtet, Chirurgen und OP-Personal mit den innovativsten Titanimplantaten und Instrumenten zu versorgen und den besten Service zu bieten.
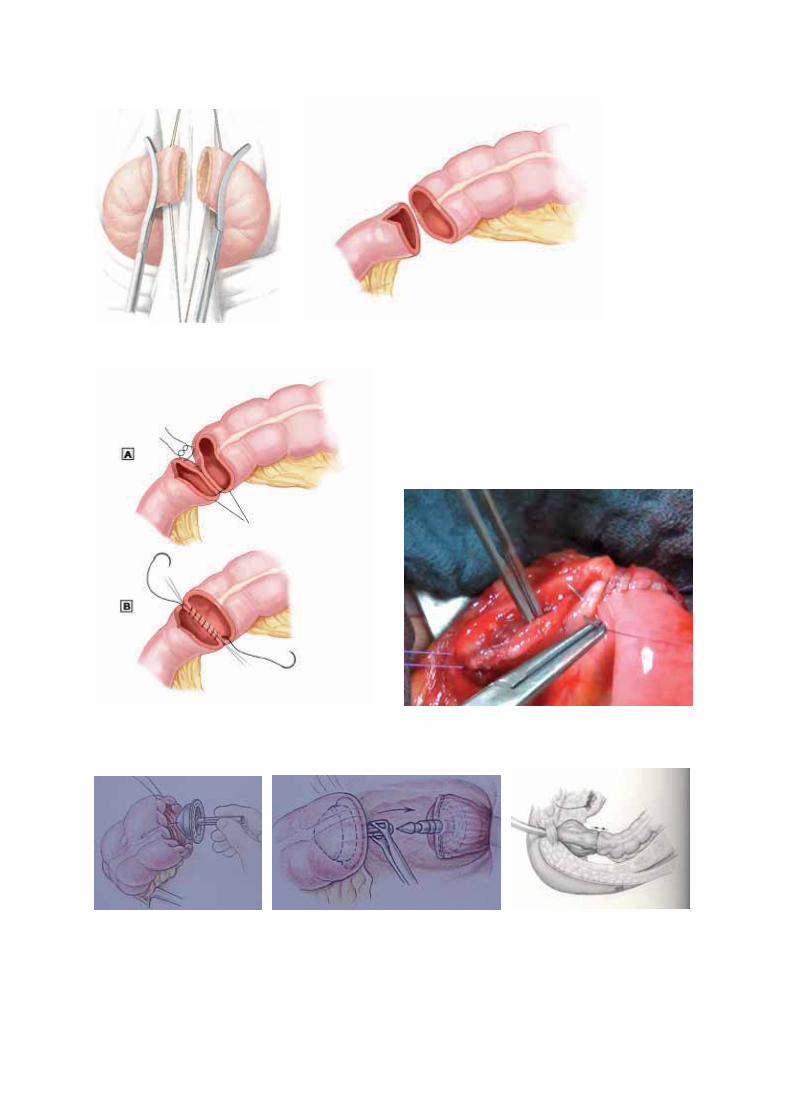
INTESTINALE ANASTOMOSEN grundsätzlich
• keine Darmlavage, ausser für laparoskopische Eingriffe, damit der Darm nicht so schwer und voluminös ist
• Antibiotika-Prophylaxe single shot • Darmstümpfe müssen gut durchblutet sein • offene Darmenden desinfizieren (keine alkoholhaltigen Tinkturen) • Mesolücke verschliessen (nicht laparoskopisch) • postoperativ sofort Normalkost (ausser oberer GI-Trakt), kauen aktiviert den Darm
Handanastomose
• Darmenden ergonomisch ausrichten, Übersichtlichkeit schaffen • Haltefäden nach Bedarf • resobierbarer monofiler Faden 4-0 • Naht i.d.R. extramukös fortlaufend • Hinterwand im Zweifelsfall Vollwandstiche • an der unübersichtlichsten Stelle beginnen, z. B. antimesenterial
o Stichabstand 2-3 mm o Abstand von der Schnittkante konstant halten o senkrecht zur Schnittkante stechen o Naht so fest anziehen, dass die Darmenden sich aneinander schmiegen aber
nicht pressen o Mukosa einstülpen und Faden sauber legen beim Anziehen der Naht
• Lumenunterschiede ausgleichen: Schrägschnitt des kleineren Lumens, Darmwandinzision antimesenterial oder auch End-zu-Seit / Seit-zu-Seit, Stichweite einseitig ändern
• visuelle Kontrolle ob Naht durchgehend regelmässig dicht • digital Lumen prüfen ob es durchgängig ist
Stapleranastomose (Kolon/Rektum)
• Darmenden denudieren, damit nicht zu viel Material in die Naht zu liegen kommt, aber doch so wenig als möglich
• Absetzen distal mit dem Endo-GIA, Rektum muss gestreckt sein, evtl. mit dem Bougie austesten, damit keine Falte das Vorschieben bis in den Apex behindert
• Durchmesser des circular Stapler dem Darmlumen anpassen (i.d.R. 31 mm, selten 28 mm), evt. zur Relaxation des Darms von der Anästhesie 1 Ampulle Buscopan geben lassen. bei Unsicherheit mit den Bougies ausmessen
• proximal Einnähen des Staplerkopfs mit einer kräftigen monofilen Tabaksbeutelnaht (Hand oder maschinell); drohen Divertikel in die Naht zu kommen, diese mit einem Stich, z.B. Vicryl 3-0, hochbinden
• Kontrolle der richtigen Lage des Kolons • Anal digitales Austasten, Stapler sorgfältig der Krümmung des Sakrums entlang
einführen und Rektumstumpf sanft aufspannen, Dorn idealerweise dorsal der Staplerlinie ausfahren
• spannungsfrei anastomosieren • Dichteprüfung mit transanaler Luftinsufflation (Veloschlauchtest), Ringe auf
Vollständigkeit kontrollieren
••
• Annnatatatatttaaa omomoomisssischchchcheeeee PlllPlPlPlatatatatatatata teteteteteeetettendndndndndesessigigigigigignsnsnsnsnsns
•
• Modulareee SSSSSSSSysyysyy teteeemkmkmkkmkoomomommmommmmpppoponenten
Medartis ist einer der führenden Hersteller von medizinischen Produkten für die Osteosynthese im Bereich des Gesichtsschädels und der Extremitäten. Medartis hat sich zum Wohle des Patienten verp� ichtet, Chirurgen und OP-Personal mit den innovativsten Titanimplantaten und Instrumenten zu versorgen und den besten Service zu bieten.
Hauptsitz Medartis AG | Hochbergerstrasse 60E | CH-4057 Basel
Medartis GmbH | Impulszentrum Fabrik I Rheinstrasse 26-27 I A-6890 Lustenau
Medartis GmbH | Am Gansacker 10 | D-79224 Umkirch
www.medartis.com

� ��
� ��
� ��
� ��

� ��
�

ddie koompplettte LLösuung füür daas HHanndgeelennk
2.0/2.3, 2.5 winkelstabile Implantate für die Teilil- ododerer
Totalarthrodese am Handgelenk
• Speziell entwickelte Platten für die Four Corner Fusion ((4CF) und diee FFusiosion n von Skaphoid, Trapezium und Trapezoideum (STT))
• Speziell entwickelte Platten für die Fusion vonn RRadRadius, Skapaphoiiddund Lunatum (RSL)
• Anatomische Total Wrist Fusion (TWF) PlPlatten mitt und ohnene VeVerststr eife ung der CMC Gelenklinie
• TriLock – multidirektionale und winknkelstabile (±( 15°515 ) V) Verbbllockunkungstechechnolnologiogiee
Hauptsitz Medartis AG | Hochbergerstrasse 60E | CH-4057 Basel
Medartis GmbH | Impulszentrum Fabrik I Rheinstrasse 26-27 I A-6890 Lustenau
Medartis GmbH | Am Gansacker 10 | D-79224 Umkirch
www.medartis.com
Medartis ist einer der führenden Hersteller von medizinischen Produkten für die Osteosynthese im Bereich des Gesichtsschädels und der Extremitäten. Medartis hat sich zum Wohle des Patienten verp� ichtet, Chirurgen und OP-Personal mit den innovativsten Titanimplantaten und Instrumenten zu versorgen und den besten Service zu bieten.

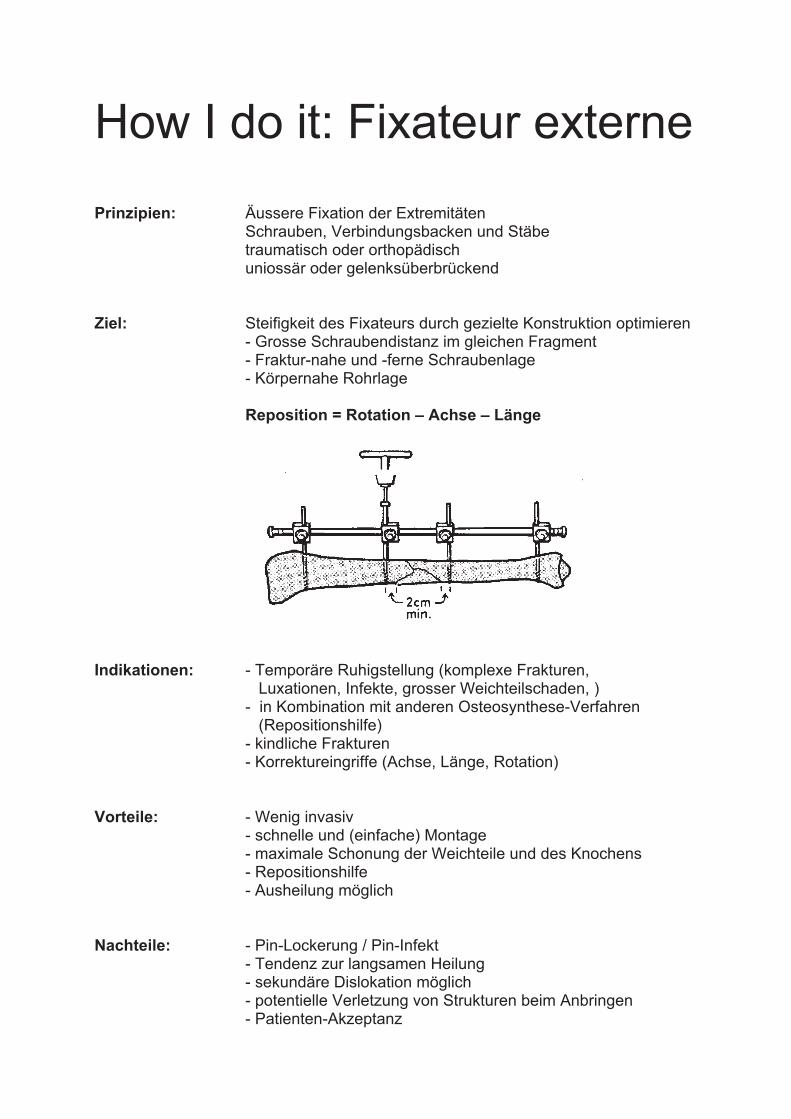
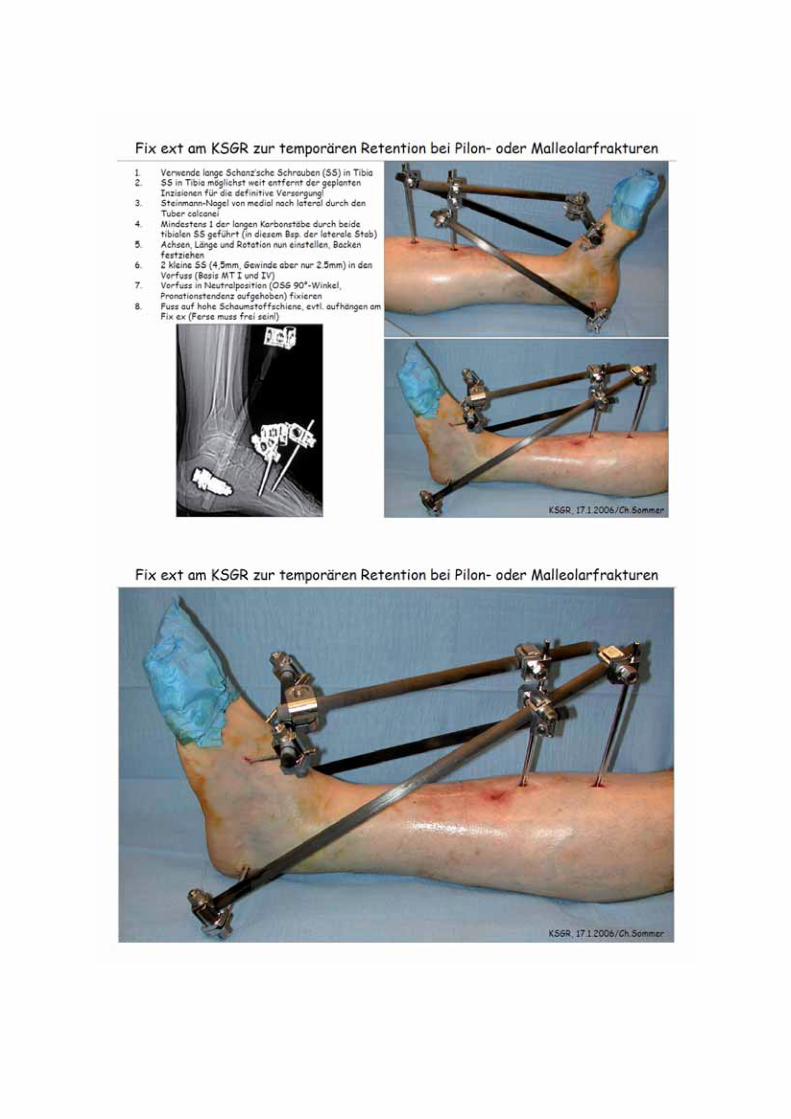
How I do it: Fixateur externe Prinzipien: Äussere Fixation der Extremitäten Schrauben, Verbindungsbacken und Stäbe
traumatisch oder orthopädisch uniossär oder gelenksüberbrückend
Ziel: Steifigkeit des Fixateurs durch gezielte Konstruktion optimieren - Grosse Schraubendistanz im gleichen Fragment - Fraktur-nahe und -ferne Schraubenlage - Körpernahe Rohrlage Reposition = Rotation – Achse – Länge
Indikationen: - Temporäre Ruhigstellung (komplexe Frakturen, Luxationen, Infekte, grosser Weichteilschaden, )
- in Kombination mit anderen Osteosynthese-Verfahren (Repositionshilfe) - kindliche Frakturen
- Korrektureingriffe (Achse, Länge, Rotation) Vorteile: - Wenig invasiv
- schnelle und (einfache) Montage - maximale Schonung der Weichteile und des Knochens - Repositionshilfe - Ausheilung möglich
Nachteile: - Pin-Lockerung / Pin-Infekt
- Tendenz zur langsamen Heilung - sekundäre Dislokation möglich - potentielle Verletzung von Strukturen beim Anbringen - Patienten-Akzeptanz
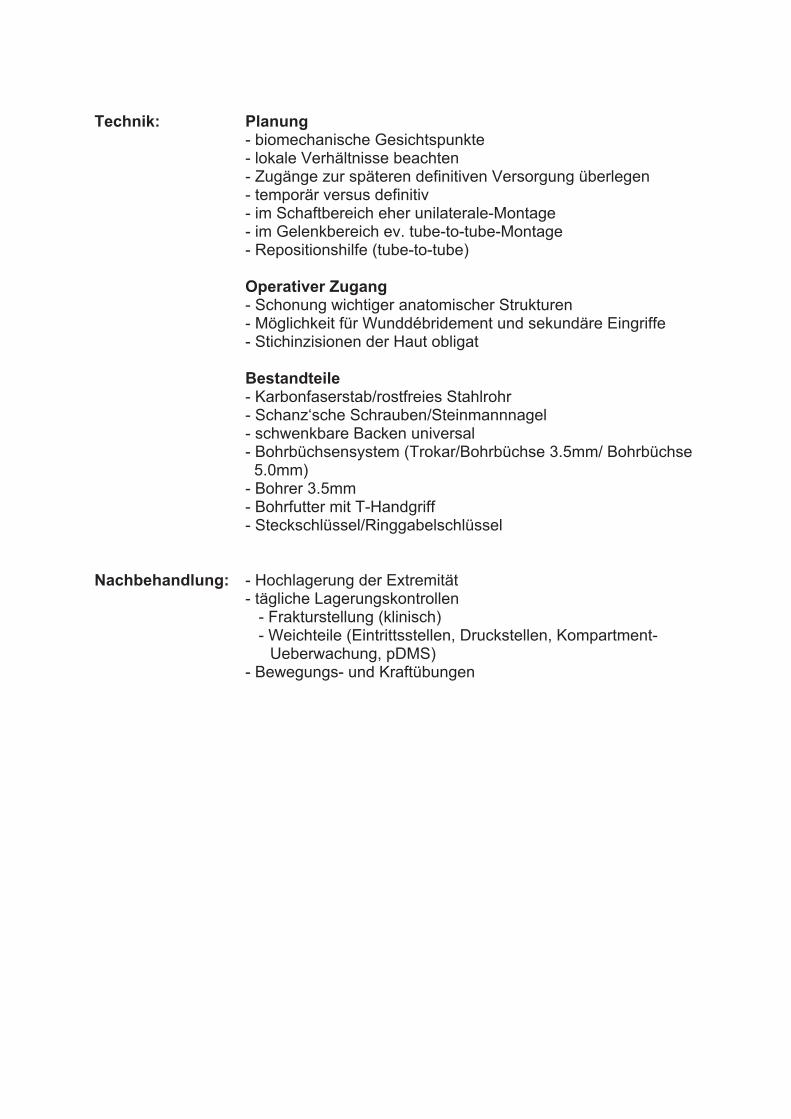
Technik: Planung
- biomechanische Gesichtspunkte - lokale Verhältnisse beachten - Zugänge zur späteren definitiven Versorgung überlegen - temporär versus definitiv - im Schaftbereich eher unilaterale-Montage - im Gelenkbereich ev. tube-to-tube-Montage - Repositionshilfe (tube-to-tube)
Operativer Zugang
- Schonung wichtiger anatomischer Strukturen - Möglichkeit für Wunddébridement und sekundäre Eingriffe - Stichinzisionen der Haut obligat
Bestandteile
- Karbonfaserstab/rostfreies Stahlrohr - Schanz‘sche Schrauben/Steinmannnagel - schwenkbare Backen universal - Bohrbüchsensystem (Trokar/Bohrbüchse 3.5mm/ Bohrbüchse 5.0mm) - Bohrer 3.5mm - Bohrfutter mit T-Handgriff - Steckschlüssel/Ringgabelschlüssel
Nachbehandlung: - Hochlagerung der Extremität
- tägliche Lagerungskontrollen - Frakturstellung (klinisch) - Weichteile (Eintrittsstellen, Druckstellen, Kompartment- Ueberwachung, pDMS)
- Bewegungs- und Kraftübungen

How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 1
How I do it Joint Luxations (diagnosis and therapy)
Dr. J. Schäfli und Christina Graf Oberärztinnen Prof. Dr. G. Melcher, Chefarzt
Chirurgische Klinik Spital Uster
1. Shoulder dislocation Epidemiology
- The most frequent luxation in adulthood, second in childhood
- Incidence 10-20/100‘000/year, 95% antero-inferior
Anatomy
- Dynamic components: rotator cuff → cavity compression; capsular tension; muscular balance
- Stiff components: configuration of humeral head and glenoid; labrum glenoidale; joint capsule;
glenohumeral ligaments
Classifications
- Matsen, Gerber, Ian Bayley, etc. etc.
- In the daily business: distinguish between anteroinferior and posterior shoulder dislocation
Pathomechanism
- Abduction – external rotation
- Signs of traumatic shoulder luxation:
- adequate trauma
- reposition by another person
- Hill-Sachs lesion
- no hyperlaxity
Pathoanatomy
- Labrum-ligament complex (LLC): Bankart lesion, Perthes lesion
- Rotator cuff
- Gleoid cavity --> Bankart fracture
- Humeral head --> Hill-Sachs lesion
Diagnosis
- Inspection (Epaulettenphänomen)
- Palpation (empty joint cavity)
- Nerves and vessels (A. radialis, Nn. Ulnaris, medianus, radialis, axillaris)
- Radiography: true-a.-p., Y-view/Neer → distinguish anterior vs. posterior luxation
Pitfall Posterior dislocation: missed in 50% → Look for elliptoid overlay
Therapy
- Closed reduction
- Clinic (nerves and vessels) and radiologic control post-repositionem
- Open reduction
- Indications
- Unsuccessful closed reduction
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 2
- Luxation with associated fracture
Closed reduction
- Preparation: O2 via nasal prongs or mask, O2 saturation monitoring
- Analgosedation:
- Dormicum® (Midazolam):
- i.v. boli a 1mg (max. 3.5-7.5mg) for adults < 60y
- i.v. boli a 0.5mg (max. <3.5mg) for adults > 60y
- Effect starts after 2‘, maximal effect after 5-10‘, t1/2 1.5-3.5h (CAVE >60y
t1/2 can be 4 times longer)
- Overdose: Anexate® (Flumazenil): 0.2mg i.v. over 15‘‘, repeat with 0.1mg
every 60‘‘, max. 1mg; CAVE t1/2 1h
- Morphin HCL Amino® (Morphini hydrochloridum):
- i.v. boli a 1mg
- Effect starts almost immediately, maximal effect after 20‘, t1/2 2.5-3h
(elderly: t1/2 can be longer)
- Overdose: Naloxon® (Naloxonhydrochlorid): 0.4-2mg i.v., repeat after 2-3‘,
max. 10mg; CAVE t1/2 60-90‘
Pitfall: Neglect to monitor the patient post-repositionem
- Entonox® (Lachgas, O2 and N2O2 ):
- Reduces pain, induces euphoric status
- CI: facial trauma, brain trauma, increased ICP, facial infections (otitis media etc.),
Trauma of the thorax (Pneumo-/Hematothorax…), ileus, ocular operation during the
previous 2 months, cardial dysfunction, reduced cognitive function, other drugs
- General Anaesthesia
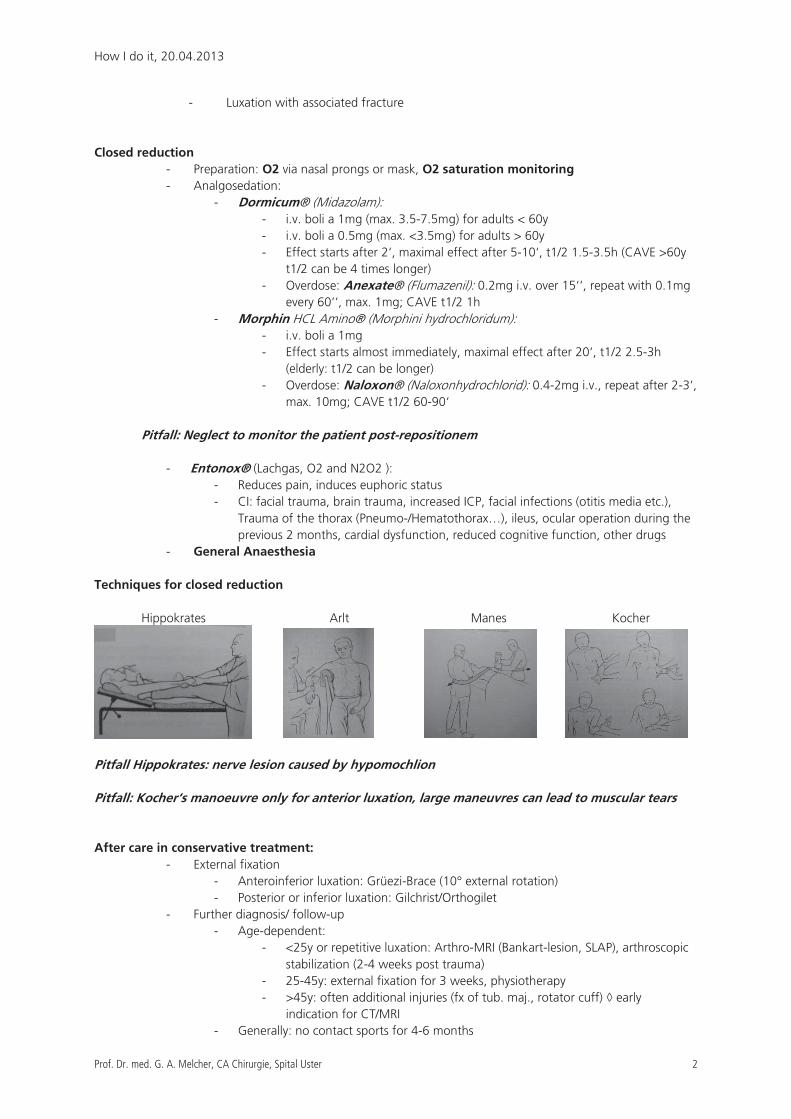
Techniques for closed reduction
Hippokrates Arlt Manes Kocher
Pitfall Hippokrates: nerve lesion caused by hypomochlion
Pitfall: Kocher‘s manoeuvre only for anterior luxation, large maneuvres can lead to muscular tears
After care in conservative treatment:
- External fixation
- Anteroinferior luxation: Grüezi-Brace (10° external rotation)
- Posterior or inferior luxation: Gilchrist/Orthogilet
- Further diagnosis/ follow-up
- Age-dependent:
- <25y or repetitive luxation: Arthro-MRI (Bankart-lesion, SLAP), arthroscopic
stabilization (2-4 weeks post trauma)
- 25-45y: external fixation for 3 weeks, physiotherapy
- >45y: often additional injuries (fx of tub. maj., rotator cuff) � early
indication for CT/MRI
- Generally: no contact sports for 4-6 months
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 3
2. Luxation of the elbow Epidemiology
- The most frequent luxation in childhood, second in adulthood
- Incidence 6-13/100‘000/year, m>w, 60% adominant upper extremity
- Predisposing factors: anatomical variant, previous injury, sport of casting with chronic instability
Anatomy
- Medial + lateral collateral ligaments
- Anterior capsule
- Head of the radius
- Dynamic stabilizers:
M. triceps, M. biceps, M. brachioradialis, M. anconeus
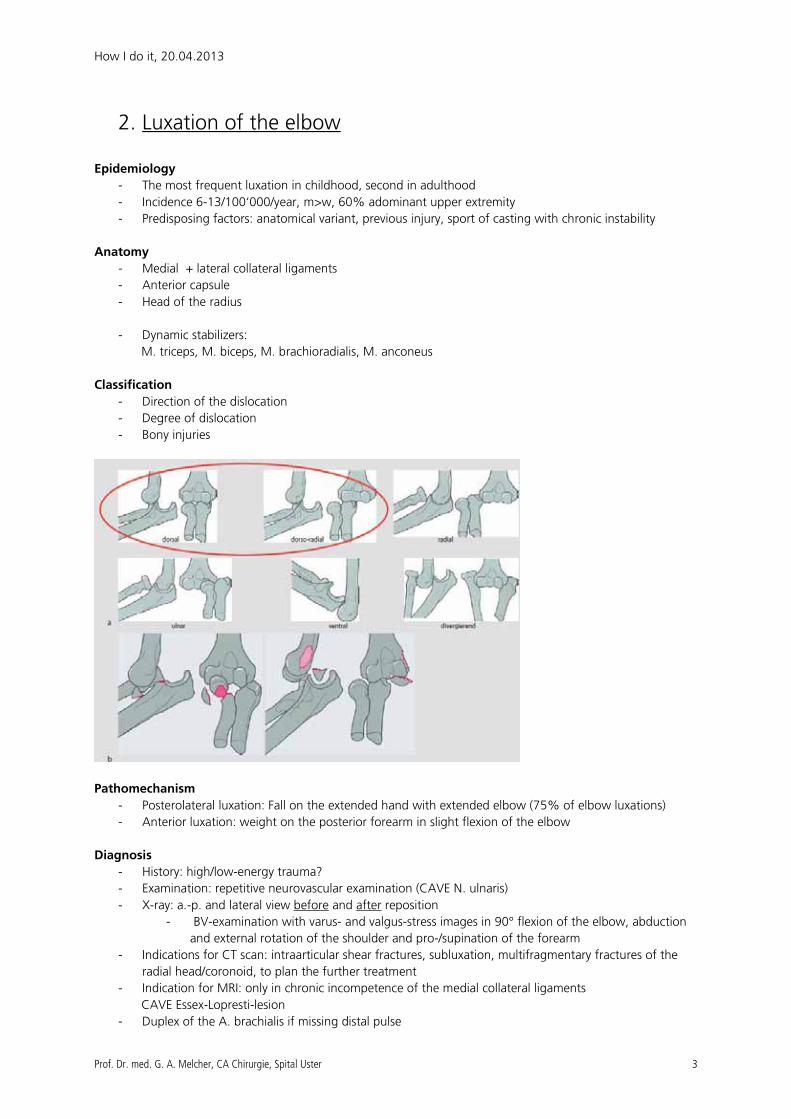
Classification
- Direction of the dislocation
- Degree of dislocation
- Bony injuries
Pathomechanism
- Posterolateral luxation: Fall on the extended hand with extended elbow (75% of elbow luxations)
- Anterior luxation: weight on the posterior forearm in slight flexion of the elbow
Diagnosis
- History: high/low-energy trauma?
- Examination: repetitive neurovascular examination (CAVE N. ulnaris)
- X-ray: a.-p. and lateral view before and after reposition
- BV-examination with varus- and valgus-stress images in 90° flexion of the elbow, abduction
and external rotation of the shoulder and pro-/supination of the forearm
- Indications for CT scan: intraarticular shear fractures, subluxation, multifragmentary fractures of the
radial head/coronoid, to plan the further treatment
- Indication for MRI: only in chronic incompetence of the medial collateral ligaments
CAVE Essex-Lopresti-lesion
- Duplex of the A. brachialis if missing distal pulse
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 4
Therapy
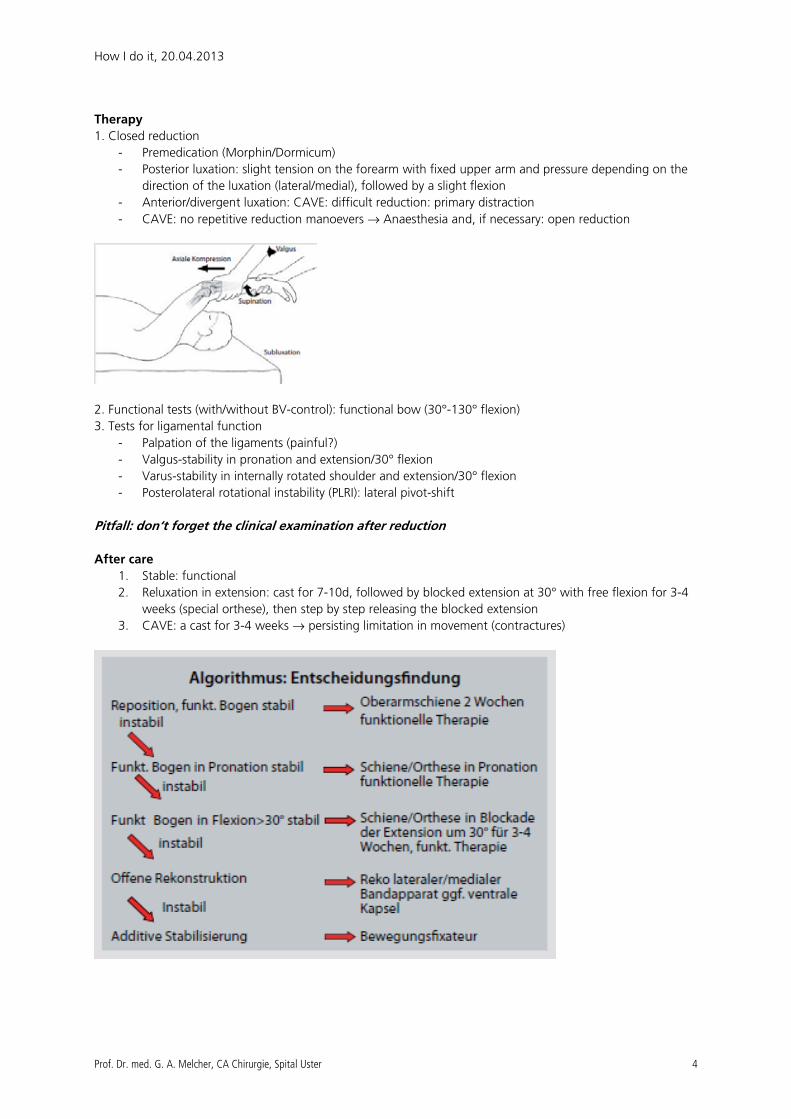
1. Closed reduction
- Premedication (Morphin/Dormicum)
- Posterior luxation: slight tension on the forearm with fixed upper arm and pressure depending on the
direction of the luxation (lateral/medial), followed by a slight flexion
- Anterior/divergent luxation: CAVE: difficult reduction: primary distraction
- CAVE: no repetitive reduction manoevers → Anaesthesia and, if necessary: open reduction
2. Functional tests (with/without BV-control): functional bow (30°-130° flexion)
3. Tests for ligamental function
- Palpation of the ligaments (painful?)
- Valgus-stability in pronation and extension/30° flexion
- Varus-stability in internally rotated shoulder and extension/30° flexion
- Posterolateral rotational instability (PLRI): lateral pivot-shift
Pitfall: don‘t forget the clinical examination after reduction
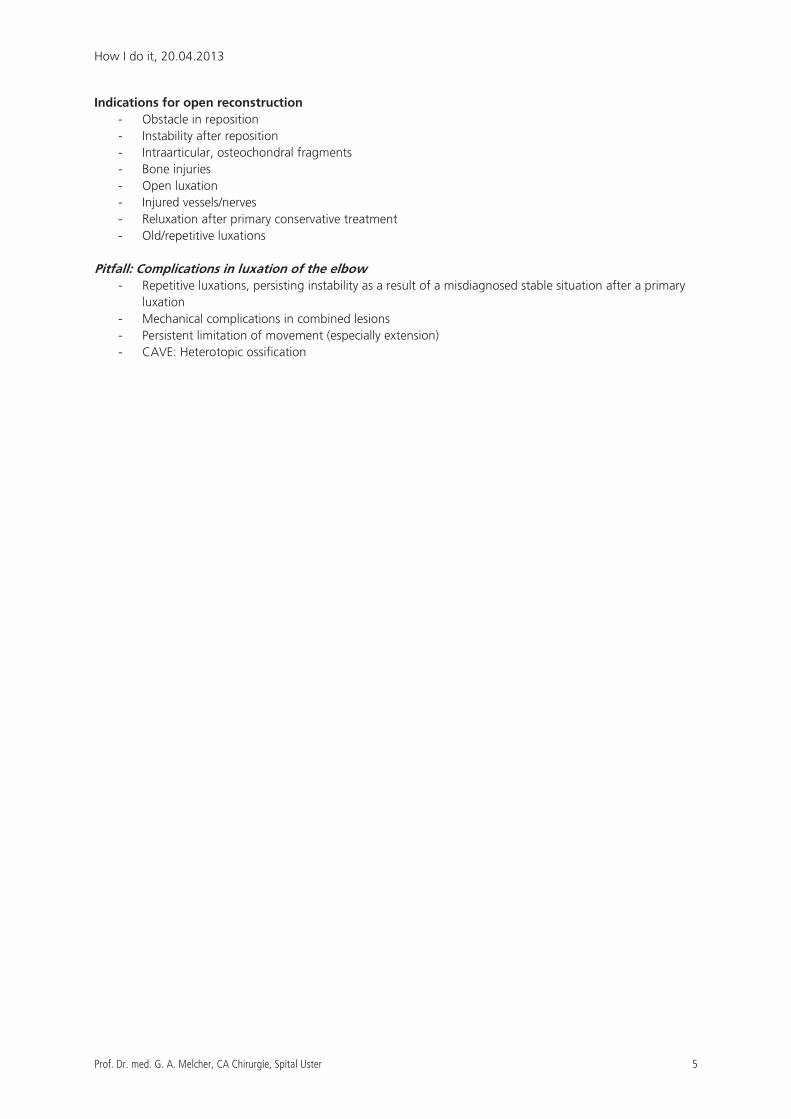
After care
1. Stable: functional
2. Reluxation in extension: cast for 7-10d, followed by blocked extension at 30° with free flexion for 3-4
weeks (special orthese), then step by step releasing the blocked extension
3. CAVE: a cast for 3-4 weeks → persisting limitation in movement (contractures)
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 5
Indications for open reconstruction
- Obstacle in reposition
- Instability after reposition
- Intraarticular, osteochondral fragments
- Bone injuries
- Open luxation
- Injured vessels/nerves
- Reluxation after primary conservative treatment
- Old/repetitive luxations
Pitfall: Complications in luxation of the elbow
- Repetitive luxations, persisting instability as a result of a misdiagnosed stable situation after a primary
luxation
- Mechanical complications in combined lesions
- Persistent limitation of movement (especially extension)
- CAVE: Heterotopic ossification
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 6
3. Hip dislocation Epidemiology:
- High-energy trauma, typically in motor vehicle accidents (dashboard-injury)
Pathomechanism: - Dashboard injury
- Anterior dislocation occurs in abduction and external rotation of the femoral head
Symptoms: - Posterior dislocation (90%): hip and leg in slight flexion, adduction, and internal rotation
- Anterior dislocation (10%): hip and leg in flexion, abduction, and external rotation
Diagnosis:
- X-ray of the pelvis (ap) : shows typically posterior luxation (head size, Tr. minor rotation)
- CT scan: gives you 3D information on the luxation
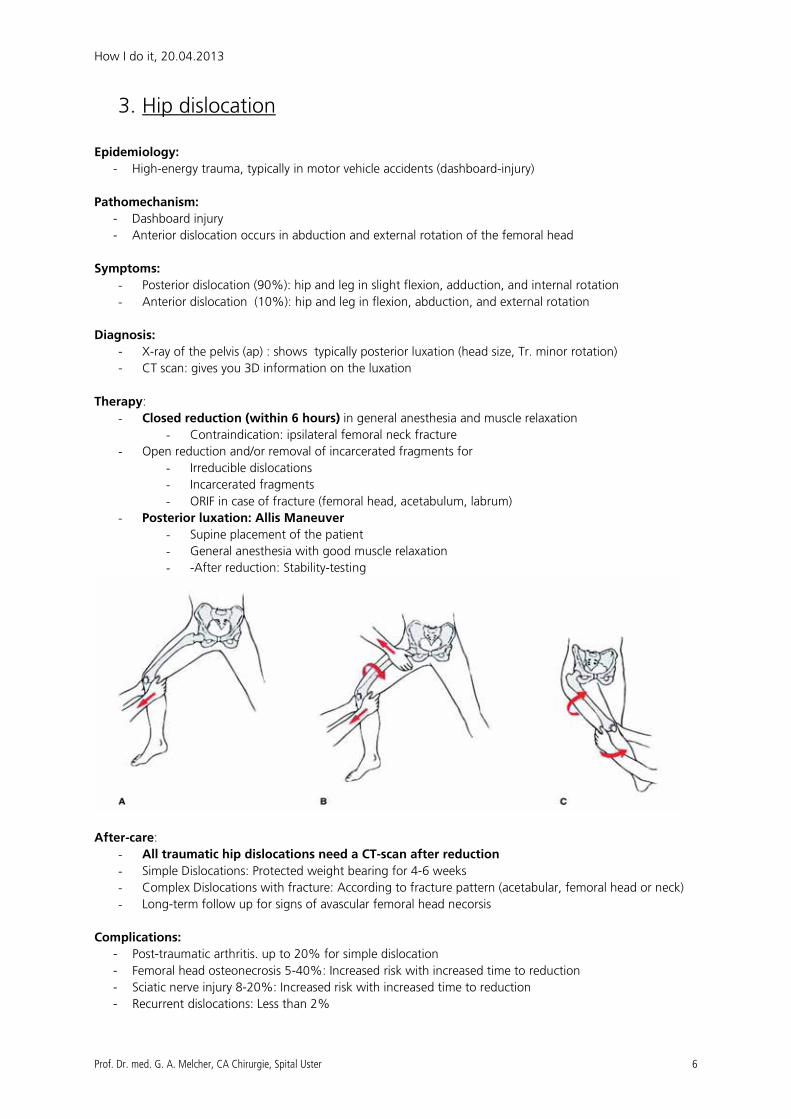
Therapy:
- Closed reduction (within 6 hours) in general anesthesia and muscle relaxation
- Contraindication: ipsilateral femoral neck fracture
- Open reduction and/or removal of incarcerated fragments for
- Irreducible dislocations
- Incarcerated fragments
- ORIF in case of fracture (femoral head, acetabulum, labrum)
- Posterior luxation: Allis Maneuver
- Supine placement of the patient
- General anesthesia with good muscle relaxation
- -After reduction: Stability-testing
After-care:
- All traumatic hip dislocations need a CT-scan after reduction
- Simple Dislocations: Protected weight bearing for 4-6 weeks
- Complex Dislocations with fracture: According to fracture pattern (acetabular, femoral head or neck)
- Long-term follow up for signs of avascular femoral head necorsis
Complications:
- Post-traumatic arthritis. up to 20% for simple dislocation
- Femoral head osteonecrosis 5-40%: Increased risk with increased time to reduction
- Sciatic nerve injury 8-20%: Increased risk with increased time to reduction
- Recurrent dislocations: Less than 2%
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 7
4. Patellar dislocation Epidemiology:
- Acute dislocation occurs equally by gender
- Recurrent dislocation occurs more in women
- Most commonly in the 2nd to 3rd decades of life
- Risk factors:
- Soft tissue disorders (e.g. Ehlers-Danlos syndrome)
- Disorders of the bone structures (e.g. patella alta, trochlear dysplasia)
- Genu valgum
Pathomechanism: - External rotation with the knee extended and foot externally rotated
- Direct fall onto the knee
-
Symptoms:
- Anterior knee pain
- Large hemarthros
- Medial sided tenderness
- Medial Patellofemoral Ligament
Diagnosis:
- X-Ray: Knee ap/lat and Patella ax.
- Loose body and fracture
- Patella alta
- Trochlear dysplasia
- MRI: Osteochondral lesion? / Tear of Medial Patellofemoral Ligament?
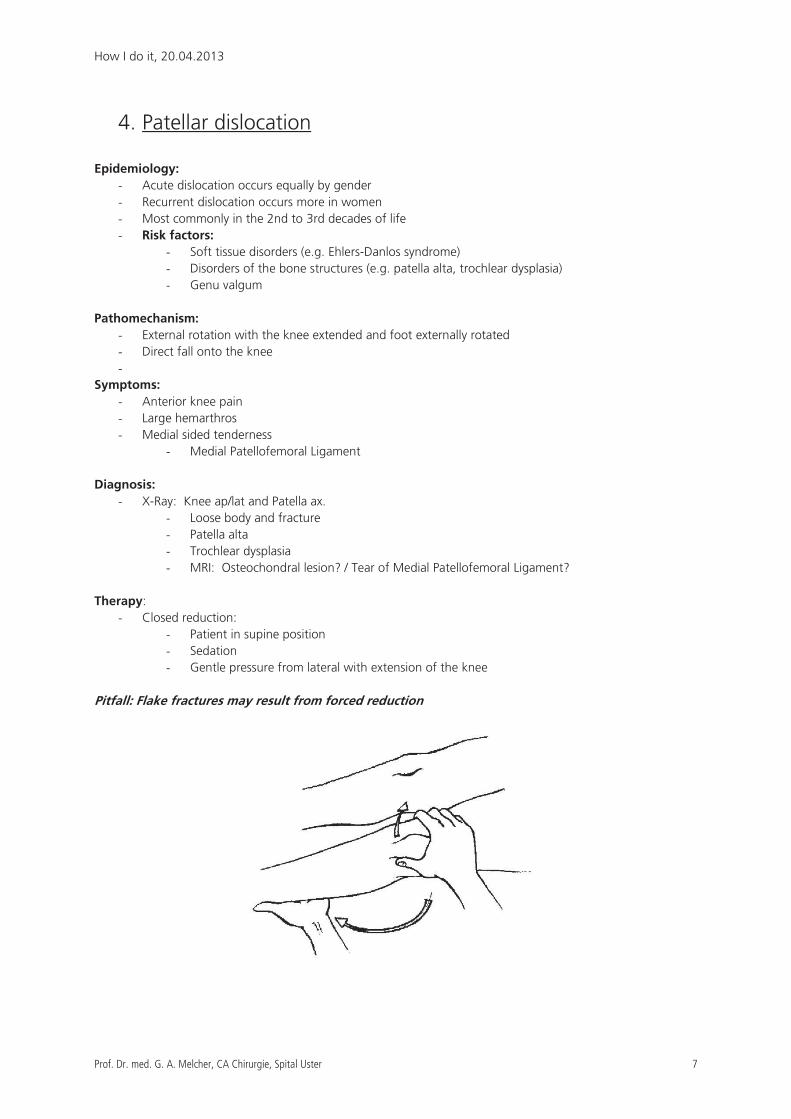
Therapy:
- Closed reduction:
- Patient in supine position
- Sedation
- Gentle pressure from lateral with extension of the knee
Pitfall: Flake fractures may result from forced reduction
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 8
After-care:
- MRI of the knee to rule out osteochondral defect and/or loose bodies
- Conservative:
- Treatment of choice for first time dislocation without loose bodies or intraarticular
damage
- Short term immobilization, patellar stabilizing sleeve, NSAID
- Physical therapy, Controlled motion
- Operative
- Arthroscopic debridement in cases with intraarticular damage
- Trochleoplasty or different orthopedic procedure in cases of chronic patellar instability
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 9
5. Luxation of the ankle joint Epidemiology:
- Mostly associated with malleolar fracture
Classification:
- Open vs. Closed : difficult to assess in ER, better intraoperative
- Gustillo-Anderson-Classification
- CAVE: Secondary skin necrosis
Pathomechanism: - Rotational traumata with low and high energy
- The position of the foot and the direction of the force applied result in specific fracture pattern
Symptoms: - visible deviation : no X-Ray !!!
Therapy:
- In cases of visible deviation: primary reduction with axial traction and fixation in cast or Vacoped
- Assess neurovascular status prior to and after reduction
- open fractures: cover wounds (Bethadine) and start antibiotic treatment
Diagnosis:
- X-Ray: OSG ap/lat (Sufficient reduction? Classification?)
- CT
After-care:
- Operative fracture treatment
- T< 6-8 h, good soft tissue, closed Frakture : ORIF
- T > 8 h, swollen soft tissue, open frakture: Fix-Ex.
Pitfall : In case of any doubt: Fix-Ex. and postprimary internal fixation
Complications:
- Wound problems (5%)
- Post-traumatic arthritis
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 10
6. Hindfoot dislocations and fractures Epidemiology:
- Rare injury (<1%)
Pitfall: Often missed fracture (approx. 20% of all fractures are missed on initial x-ray)
→→→→ Serious consequences after missed fractures and dislocations (Arthritis, chronic instability)
Pathomechanism: - High energy force in motor vehicle accidents or falls
- Lower energy trauma in twisting falls
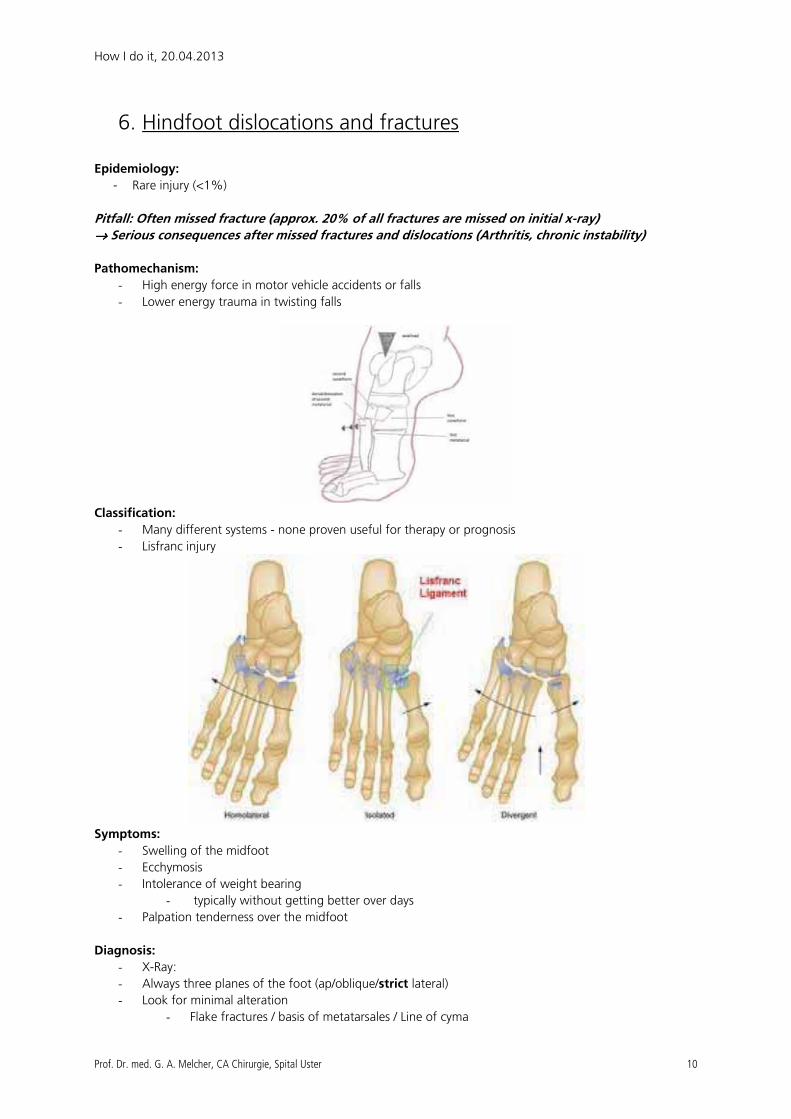
Classification:
- Many different systems - none proven useful for therapy or prognosis
- Lisfranc injury
Symptoms:
- Swelling of the midfoot
- Ecchymosis
- Intolerance of weight bearing
- typically without getting better over days
- Palpation tenderness over the midfoot
Diagnosis:
- X-Ray:
- Always three planes of the foot (ap/oblique/strict lateral)
- Look for minimal alteration
- Flake fractures / basis of metatarsales / Line of cyma
How I do it, 20.04.2013
Prof. Dr. med. G. A. Melcher, CA Chirurgie, Spital Uster 11
Pitfall: CT in any suspicious case!!!
Therapy:
- Conservative:
- Cast immobilisation for 8 weeks (no displacement, no bony injury)
- Patient unfit for surgery or low demand
- Operative
- Timing of surgery: delayed!
- Emergency only, if: compartment syndrome, open fx, irreducible and critical
skin
- Soft tissue management
- Temporary arthrodesis (K-wires, screws)
After-care:
- Protected weight bearing for 6-8 weeks
- Prophylaxis of thromboembolism
- Removal of screw arthrodesis 8-12 weeks post trauma
References:
M. Walz „Eine schonende Methode zur Reposition der vorderen Schulterluxation, Unfallchirurg 2006 ·
109:551–555
T.Mittlmeier „Luxation des Ellenbogengelenks des Erwachsenen“ Unfallchirurg 2009 112:487-505
Engelhardt Lexikon Orthopädie und Unfallchirurgie
www.orthobullets.com
www.wheelessonline.com

Pertrochantere Femurfrakturen „How I do it“Forum junger Chirurgen, Kantonsspital Zug, 20. April 2013
Thomas Beck, Spitalzentrum Oberwallis, Visp
Präoperative Überlegungen
- Unfallmechanismus: High energy / low energy - Röntgenbild lesen:
o Frakturstabilität / Klassifikation o CCD Winkel o Markkanalweite o Andere Implantate
- Zeitpunkt der Operation o „Schwierige pertrochantere Frakturen bleiben schwierig“
- Implantatwahl o Intramedullärer Kraftträger (Typ PFN, gamma-Nagel etc.) o Platte (DHS, Klingenplatte, Trochanterplatte etc.) o Implantatmanual lesen und Instrumentarium kennen
Peri- und intraoperatives Vorgehen:
- Patientenlagerung o Extensionstisch o „Bananenposition“ o BV Positionierung (evtl. 2 BV)
- Geschlossene Reposition o Extension, leichte Innenrotation o „Petite geste de valgisation“ o Abdecken (Vertikalfolie) nach Reposition o Eine ungenügende Reposition verlangt ein (zumindest partiell) offenes
Vorgehen - Repositionshilfen:
o Steinmann-Pins o Einzinkerhaken o (Koaxiale) Repositionszangen o (Kabel) Cerclagen
- Nageleintrittspunkt o Trochanterspitze (je nach Nagel), no stress !!! o In 2 Ebenen kontrollieren o Draht mit T- Handgriff o Dislozierten Trochanter mitauffädeln.
- Aufbohren des proximalen Femurs o Hochtourig, ohne Druck o Ansonsten: Auseinanderdrängen der Fraktur (Varusdislokation) ohne
Auffräsen des Trochantermassivs. o Evtl. Aufbohren des Markkanals notwendig (1.5 mm über Nageldicke)
- Klingenposition o Führungsdrahtsposition (je nach Implantat)
� Kontrolle in zwei Ebenen o Kontrolle unter BV während dem Aufbohren über den KD
(Dislokationsgefahr ins kleine Becken) o Durchschwenken des BV bei ungenügender Sicht
- Distale Verriegelung o Unter ap BV Einstellung o Zug komplett lösen (erste Sinterung möglich) o Vorher: Zielbügel nochmals festziehen
Notausgang - Extramedullärer Kraftträger mit zusätzlicher Trochanterabstützplatte
o Nachteil: Fraktursinterung und Off-set Verlust
Zusammenfassung:
- „Schwierige pertrochantere Frakturen bleiben schwierig“
- Eine korrekte Reposition ist essentiell
- Die meisten Komplikationen entstehen durch einen technischen Fehler (meist resultierend aus einer nicht korrekten Reposition).





























