Embed Size (px)
Citation preview
1
Katheter-assoziierte Infektionen mit dem SchwerpunktZVK
Walter Popp
Krankenhaushygiene, Universitätsklinikum Essen
Deutsche Anästhesie-Congress, 10. Mai 2009, Leipzig
Interaktiver Workshop Critical Care - facts, news and perspectives,organisiert von Baxter Deutschland GmbH
2
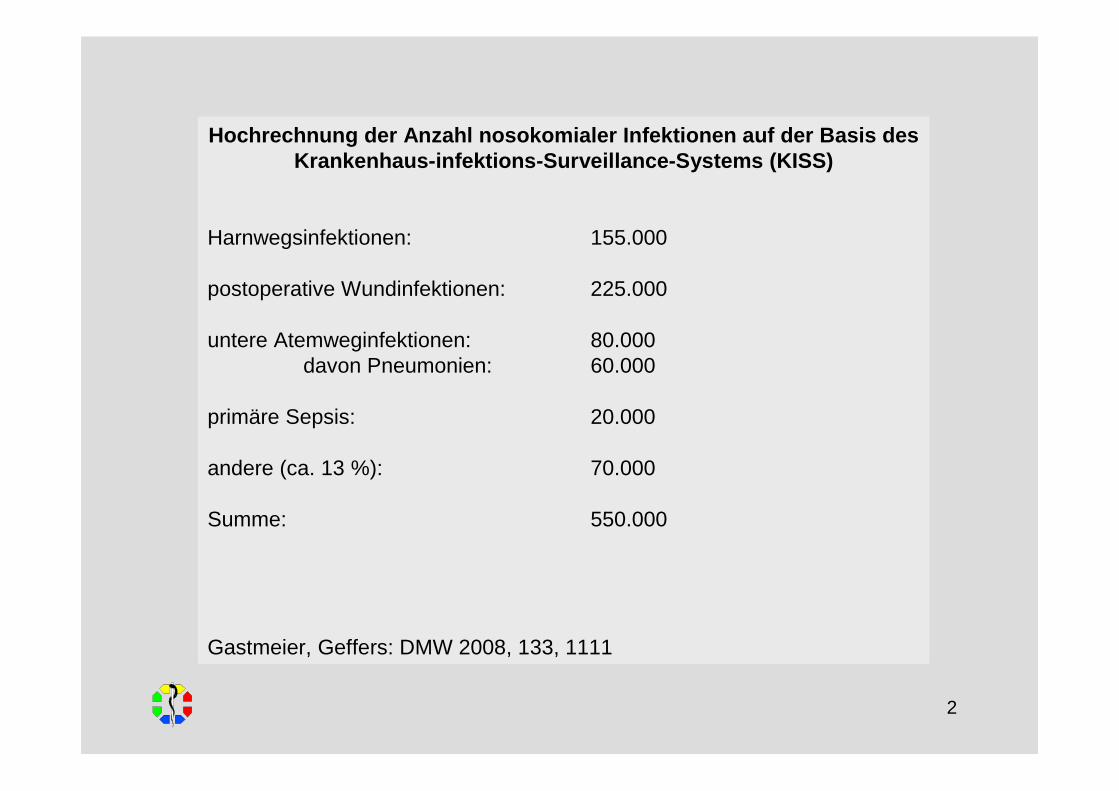
Hochrechnung der Anzahl nosokomialer Infektionen auf der Basis des Krankenhaus-infektions-Surveillance-Systems (KISS)
Harnwegsinfektionen: 155.000
postoperative Wundinfektionen: 225.000
untere Atemweginfektionen: 80.000davon Pneumonien: 60.000
primäre Sepsis: 20.000
andere (ca. 13 %): 70.000
Summe: 550.000
Gastmeier, Geffers: DMW 2008, 133, 1111
3
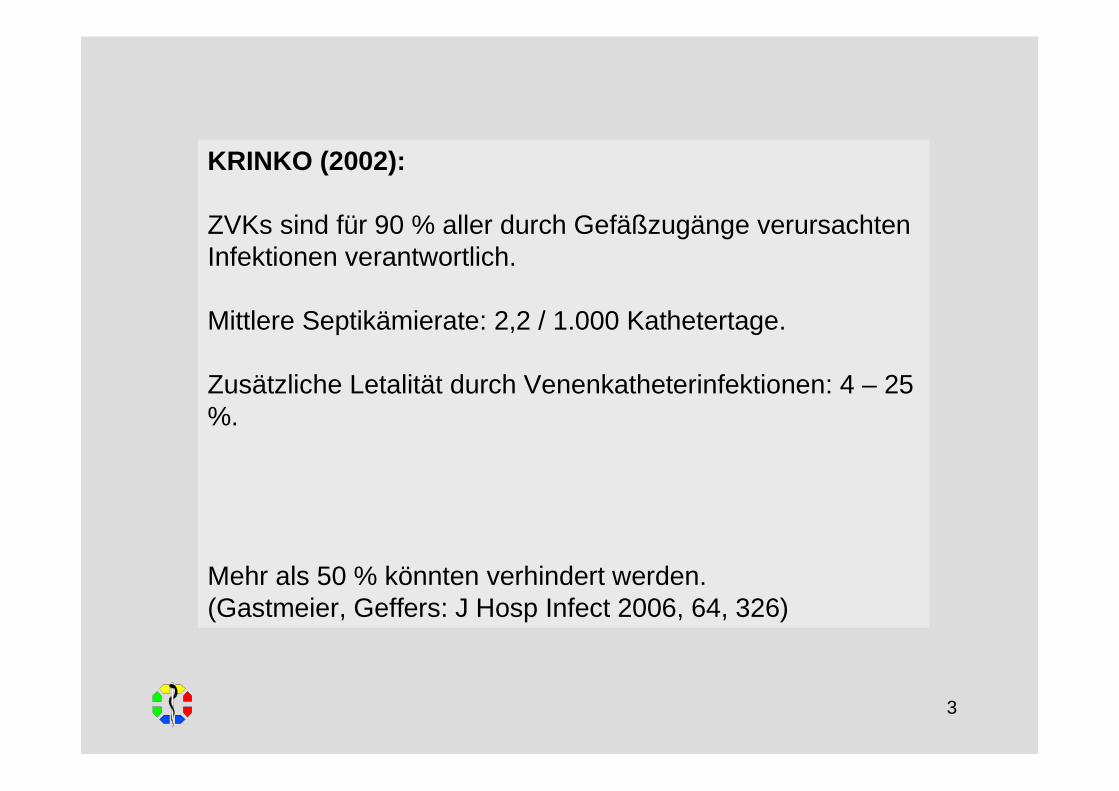
KRINKO (2002):
ZVKs sind für 90 % aller durch Gefäßzugänge verursachten Infektionen verantwortlich.
Mittlere Septikämierate: 2,2 / 1.000 Kathetertage.
Zusätzliche Letalität durch Venenkatheterinfektionen: 4 – 25 %.
Mehr als 50 % könnten verhindert werden.(Gastmeier, Geffers: J Hosp Infect 2006, 64, 326)
4
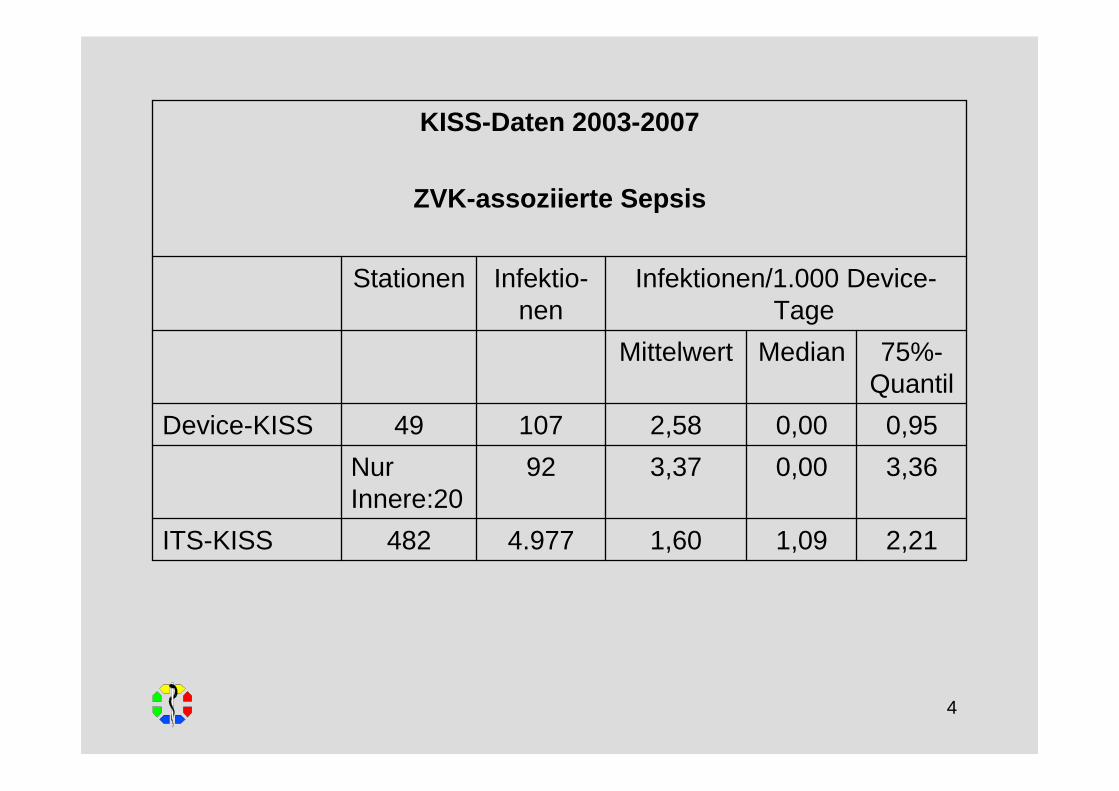
2,211,091,604.977482ITS-KISS
3,360,003,3792NurInnere:20
0,950,002,5810749Device-KISS
75%-Quantil
MedianMittelwert
Infektionen/1.000 Device-Tage
Infektio-nen
Stationen
KISS-Daten 2003-2007
ZVK-assoziierte Sepsis
5
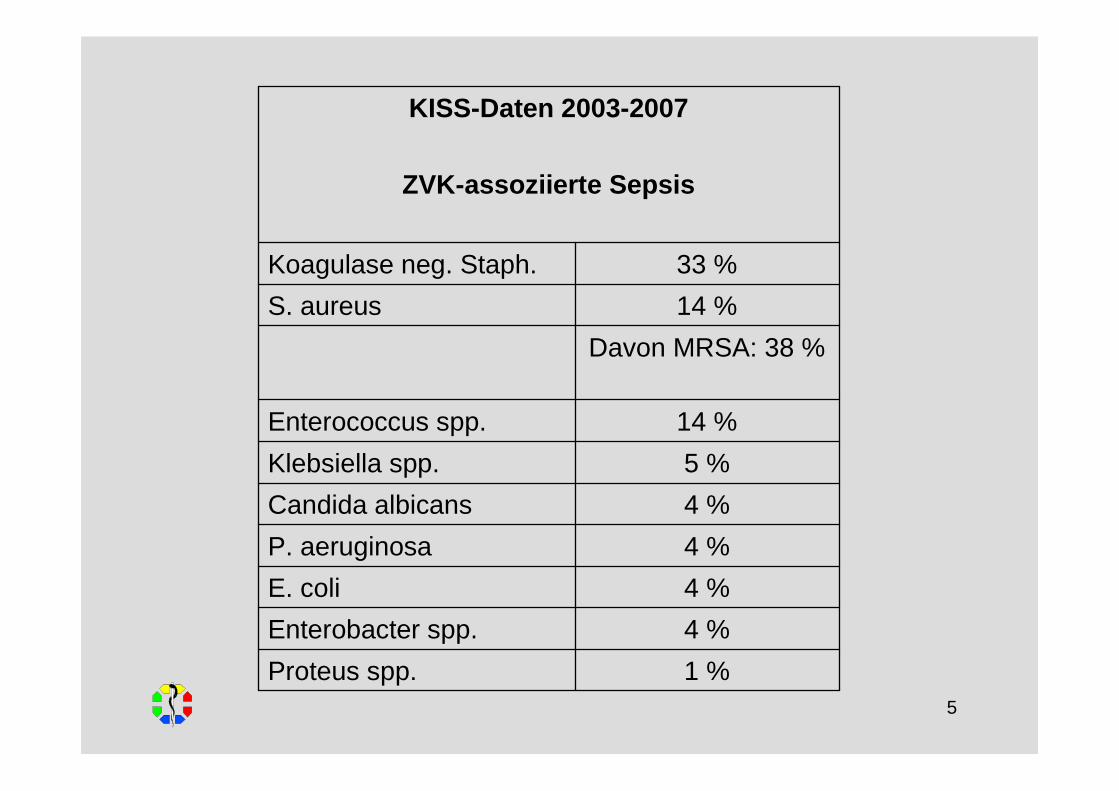
1 %Proteus spp.
4 %Enterobacter spp.
4 %E. coli
4 %P. aeruginosa
4 %Candida albicans
5 %Klebsiella spp.
14 %Enterococcus spp.
Davon MRSA: 38 %
14 %S. aureus
33 %Koagulase neg. Staph.
KISS-Daten 2003-2007
ZVK-assoziierte Sepsis
6
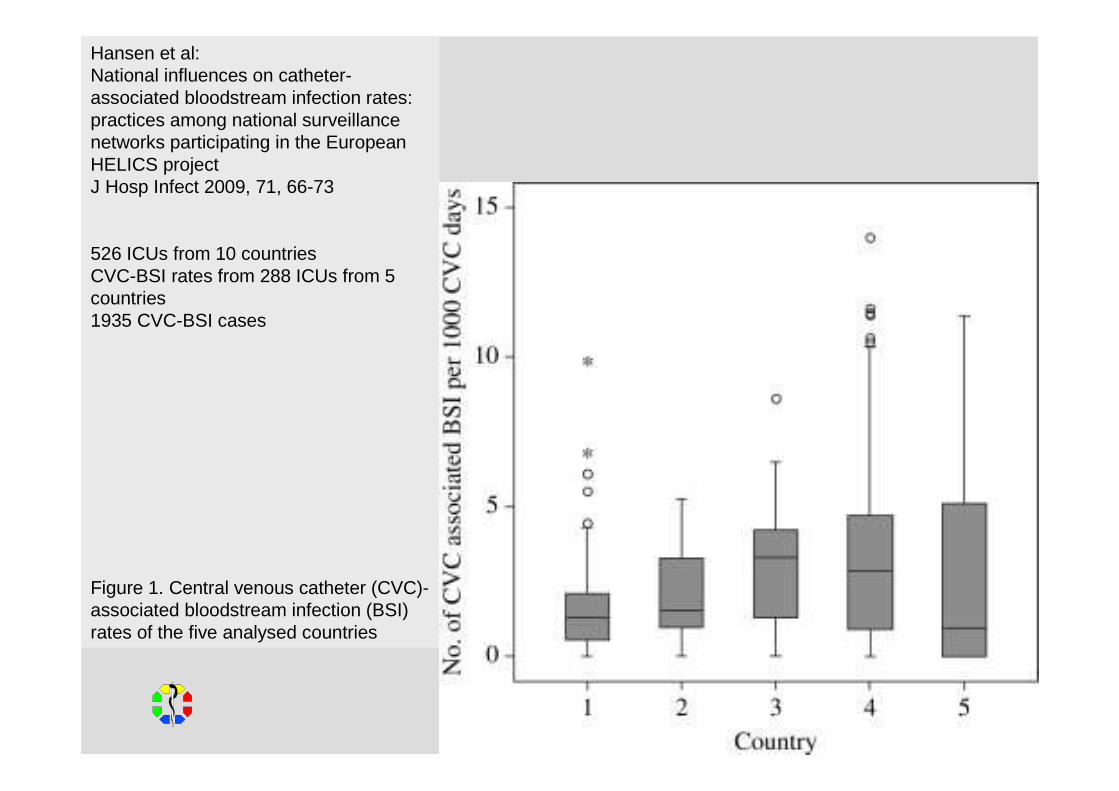
Hansen et al: National influences on catheter-associated bloodstream infection rates: practices among national surveillancenetworks participating in the European HELICS projectJ Hosp Infect 2009, 71, 66-73
526 ICUs from 10 countriesCVC-BSI rates from 288 ICUs from 5 countries1935 CVC-BSI cases
Figure 1. Central venous catheter (CVC)-associated bloodstream infection (BSI) rates of the five analysed countries
7
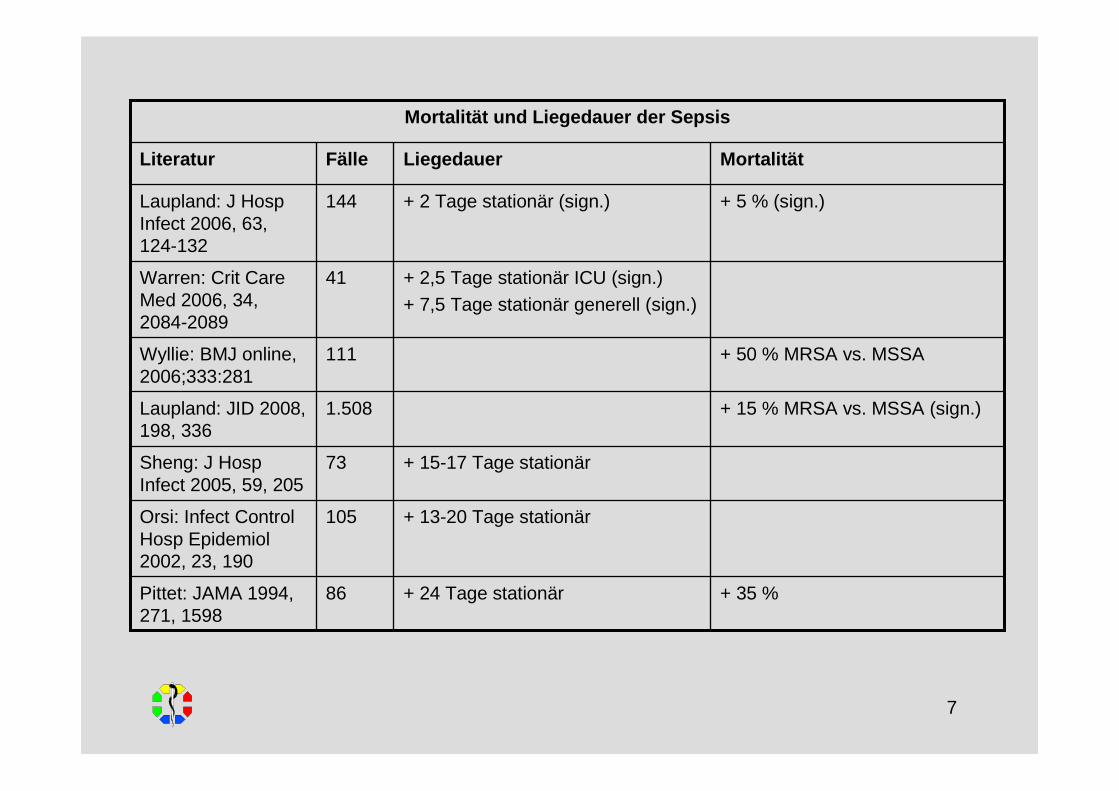
+ 13-20 Tage stationär105Orsi: Infect ControlHosp Epidemiol2002, 23, 190
+ 15-17 Tage stationär73Sheng: J HospInfect 2005, 59, 205
+ 15 % MRSA vs. MSSA (sign.)1.508Laupland: JID 2008, 198, 336
+ 50 % MRSA vs. MSSA111Wyllie: BMJ online, 2006;333:281
+ 2,5 Tage stationär ICU (sign.)+ 7,5 Tage stationär generell (sign.)
41Warren: Crit CareMed 2006, 34, 2084-2089
86
144
Fälle
+ 35 %+ 24 Tage stationärPittet: JAMA 1994, 271, 1598
+ 5 % (sign.)+ 2 Tage stationär (sign.)Laupland: J HospInfect 2006, 63, 124-132
MortalitätLiegedauerLiteratur
Mortalität und Liegedauer der Sepsis
8
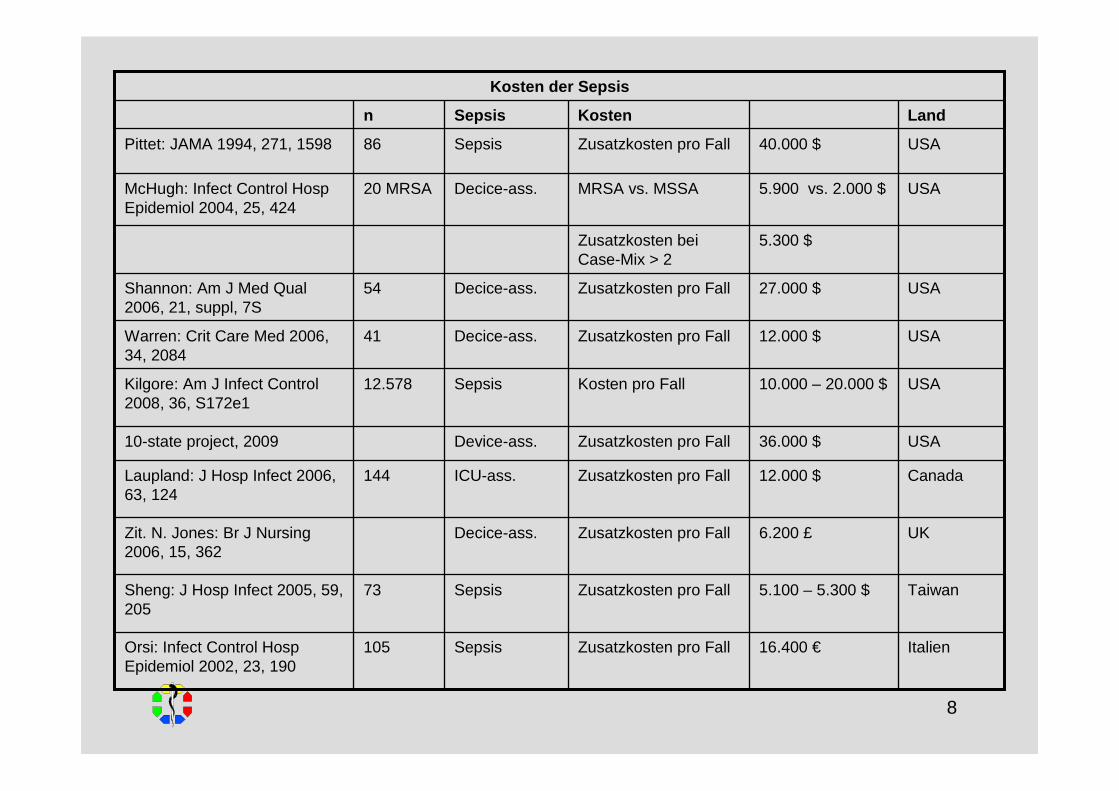
USA40.000 $Zusatzkosten pro FallSepsis86Pittet: JAMA 1994, 271, 1598
USA5.900 vs. 2.000 $MRSA vs. MSSADecice-ass.20 MRSAMcHugh: Infect Control HospEpidemiol 2004, 25, 424
5.300 $Zusatzkosten bei Case-Mix > 2
Canada12.000 $Zusatzkosten pro FallICU-ass.144Laupland: J Hosp Infect 2006, 63, 124
Italien16.400 €Zusatzkosten pro FallSepsis105Orsi: Infect Control HospEpidemiol 2002, 23, 190
Taiwan5.100 – 5.300 $Zusatzkosten pro FallSepsis73Sheng: J Hosp Infect 2005, 59, 205
UK6.200 £Zusatzkosten pro FallDecice-ass.Zit. N. Jones: Br J Nursing2006, 15, 362
USA36.000 $Zusatzkosten pro FallDevice-ass.10-state project, 2009
USA10.000 – 20.000 $Kosten pro FallSepsis12.578Kilgore: Am J Infect Control2008, 36, S172e1
USA27.000 $Zusatzkosten pro FallDecice-ass.54Shannon: Am J Med Qual 2006, 21, suppl, 7S
USA12.000 $Zusatzkosten pro FallDecice-ass.41Warren: Crit Care Med 2006, 34, 2084
LandKostenSepsisn
Kosten der Sepsis
9
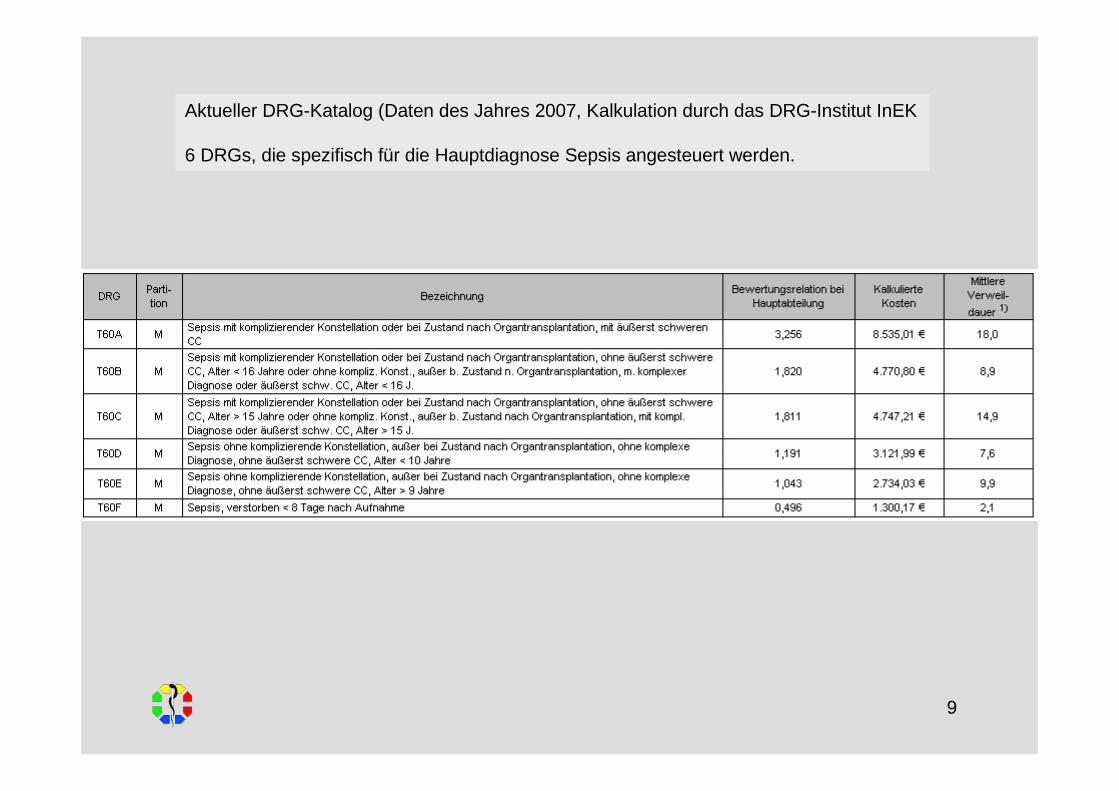
Aktueller DRG-Katalog (Daten des Jahres 2007, Kalkulation durch das DRG-Institut InEK
6 DRGs, die spezifisch für die Hauptdiagnose Sepsis angesteuert werden.
10
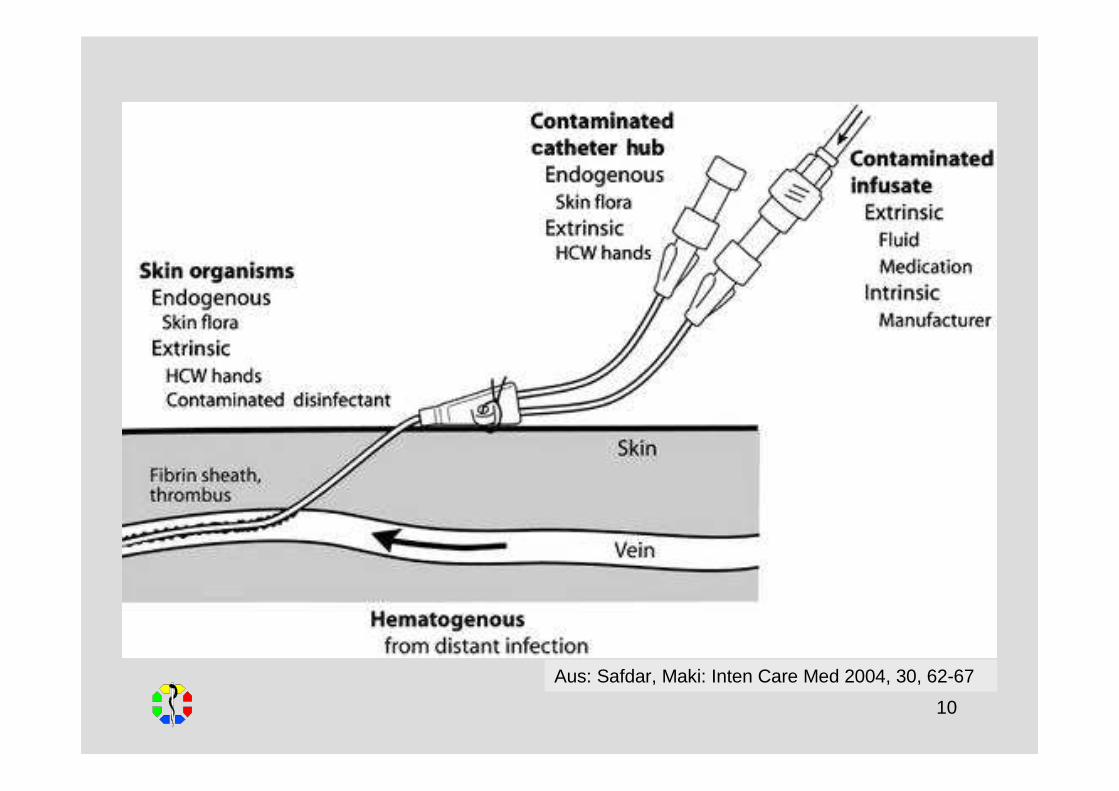
Aus: Safdar, Maki: Inten Care Med 2004, 30, 62-67
11
KRINKO (2002) – ZVK legen
Regelmässige Schulungen (I A).
ZVKs aus Silikon und Polyurethan zu bevorzugen gegenüber PVC und Polyethylen (I A).
Möglichst Single-Lumen-Katheter (I B).
Keine Aussage zu antimikrobiell oder antiseptisch beschichteten Kathetern (III). Keine Aussage zu silberbeschichteten Kollagenmanschetten (III).
V. Subclavia (I B).
Keine Antibiotikaprophylaxe (III).
Hygienische Händedesinfektion vor Anlegen der Schutzkleidung (I A).
MNS, Haube, steriler Kittel, sterile Handschuhe (I A).
Desinfektion der Einstichstelle (I B).
Abdeckung mit grossem sterilen Tuch (I A).
Fixierung, Abdeckung…
12
KRINKO (2002) – ZVK legen
Regelmässige Schulungen (I A).
ZVKs aus Silikon und Polyurethan zu bevorzugen gegenüber PVC und Polyethylen (I A).
Möglichst Single-Lumen-Katheter (I B).
Keine Aussage zu antimikrobiell oder antiseptisch beschichteten Kathetern (III). Keine Aussage zu silberbeschichteten Kollagenmanschetten (III).
V. Subclavia (I B).
Keine Antibiotikaprophylaxe (III).
Hygienische Händedesinfektion vor Anlegen der Schutzkleidung (I A).
MNS, Haube, steriler Kittel, sterile Handschuhe (I A).
Desinfektion der Einstichstelle (I B).
Abdeckung mit grossem sterilen Tuch (I A).
Fixierung, Abdeckung…
Im Jahr 2003 lagen auf 16 % der KISS-Intensivstationen keine schriftlich fixierten Standards für die ZVK-Anlage vor.
Nur 43 % führten alle angeratenen Standards durch.
Vonberg et al: Anaesthesist 2005, 54, 975-982
13
KRINKO (2002) – ZVK legen
Regelmässige Schulungen (I A).
ZVKs aus Silikon und Polyurethan zu bevorzugen gegenüber PVC und Polyethylen (I A).
Möglichst Single-Lumen-Katheter (I B).
Keine Aussage zu antimikrobiell oder antiseptisch beschichteten Kathetern (III). Keine Aussage zu silberbeschichteten Kollagenmanschetten (III).
V. Subclavia (I B).
Keine Antibiotikaprophylaxe (III).
Hygienische Händedesinfektion vor Anlegen der Schutzkleidung (I A).
MNS, Haube, steriler Kittel, sterile Handschuhe (I A).
Desinfektion der Einstichstelle (I B).
Abdeckung mit grossem sterilen Tuch (I A).
Fixierung, Abdeckung…
Niedrigste Compliance mit Händedesinfektion nach Beobachtung im Rahmen der Aktion Saubere Hände bei aseptischen Tätigkeiten.
Ähnlich auch andere Studien.
Reichardt, Ulmer Symposium Krankenhausinfektionen, April 209
14
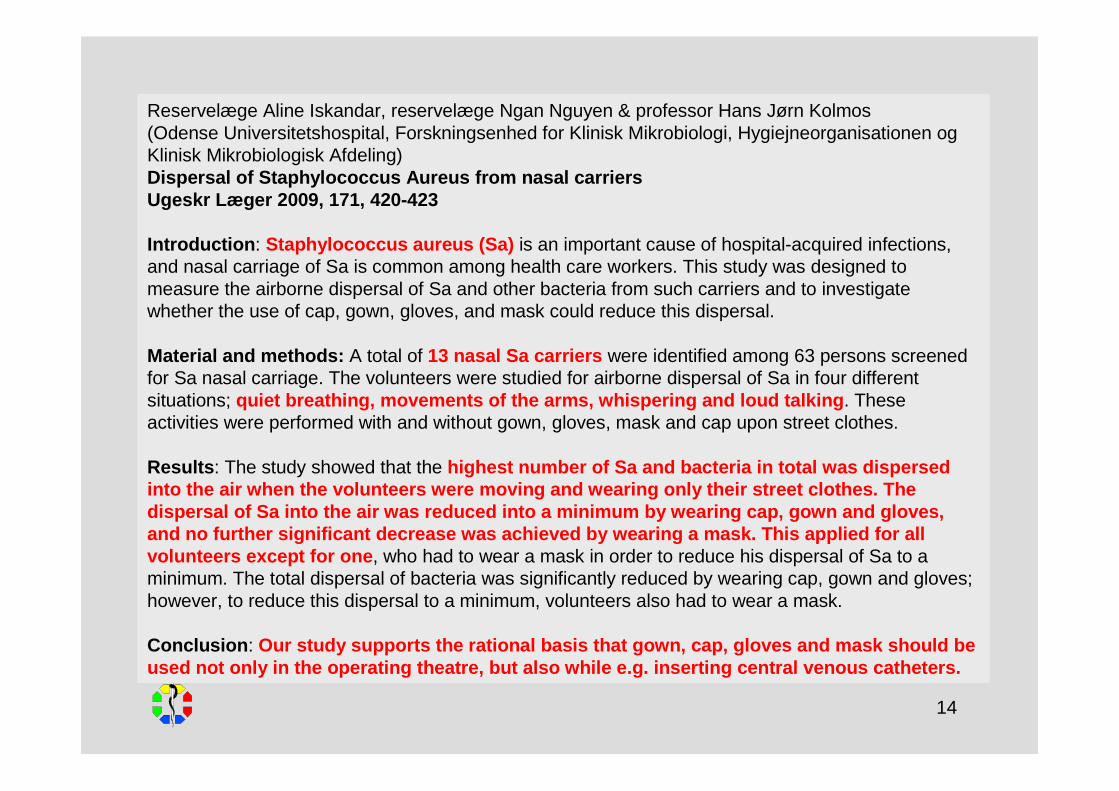
Reservelæge Aline Iskandar, reservelæge Ngan Nguyen & professor Hans Jørn Kolmos(Odense Universitetshospital, Forskningsenhed for Klinisk Mikrobiologi, Hygiejneorganisationen ogKlinisk Mikrobiologisk Afdeling)Dispersal of Staphylococcus Aureus from nasal carriersUgeskr Læger 2009, 171, 420-423
Introduction : Staphylococcus aureus (Sa) is an important cause of hospital-acquired infections, and nasal carriage of Sa is common among health care workers. This study was designed to measure the airborne dispersal of Sa and other bacteria from such carriers and to investigatewhether the use of cap, gown, gloves, and mask could reduce this dispersal.
Material and methods: A total of 13 nasal Sa carriers were identified among 63 persons screenedfor Sa nasal carriage. The volunteers were studied for airborne dispersal of Sa in four different situations; quiet breathing, movements of the arms, whispering and loud talking . These activities were performed with and without gown, gloves, mask and cap upon street clothes.
Results : The study showed that the highest number of Sa and bacteria in total was dispers edinto the air when the volunteers were moving and wearing onl y their street clothes. Thedispersal of Sa into the air was reduced into a minimum by wearing cap, gown and gloves, and no further significant decrease was achieved by wear ing a mask. This applied for all volunteers except for one , who had to wear a mask in order to reduce his dispersal of Sa to a minimum. The total dispersal of bacteria was significantly reduced by wearing cap, gown and gloves; however, to reduce this dispersal to a minimum, volunteers also had to wear a mask.
Conclusion : Our study supports the rational basis that gown, cap, glo ves and mask should beused not only in the operating theatre, but also while e.g . inserting central venous catheters.
15
KRINKO (2002) – ZVK pflegen
Täglich inspizieren, bei Gazeverbänden palpieren (Druckschmerz, Fieber!) (I B).
Täglicher Verbandwechsel von Gazeverbänden bei eingeschränkter Kooperation des Patienten (I B).
Wechsel der Transparentverbände spätestens nach 7 Tagen (I B).
Alkoholische Antiseptika auf Insertionsstelle bei Verbandwechsel (II).
Keine Salben bei Transparentverbänden (I B).
Kein routinemäßiger Wechsel (I A).
Wechsel bei Entzündung bzw. Tunnelinfektion sowie nach Notfallanlage (I B).
Indikation täglich neu prüfen (I B).
Spülung ggfs. mit steriler physiologischer Elektrolylösung (I A).
Keine Aussage zu „antibiotic lock technique“ oderHeparinspülungen (III).
Keine Aussage zum „Ruhen“ (III).
16
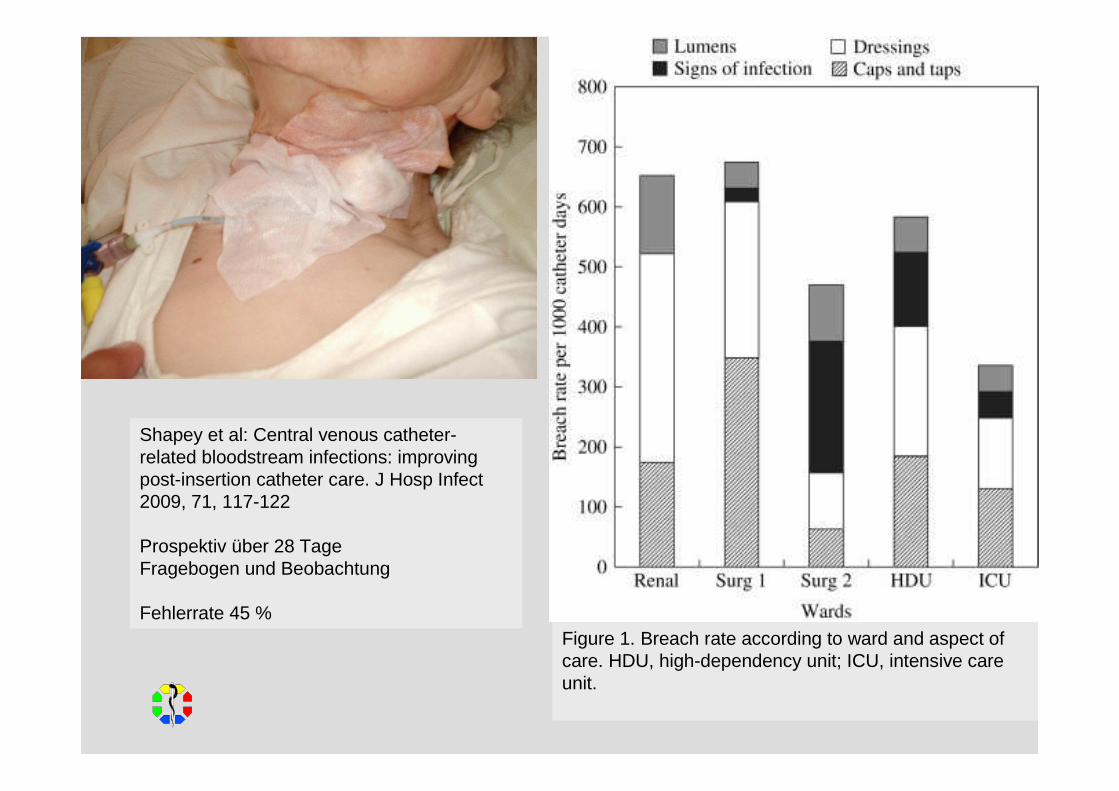
Figure 1. Breach rate according to ward and aspect of care. HDU, high-dependency unit; ICU, intensive careunit.
Shapey et al: Central venous catheter-related bloodstream infections: improvingpost-insertion catheter care. J Hosp Infect2009, 71, 117-122
Prospektiv über 28 TageFragebogen und Beobachtung
Fehlerrate 45 %
17
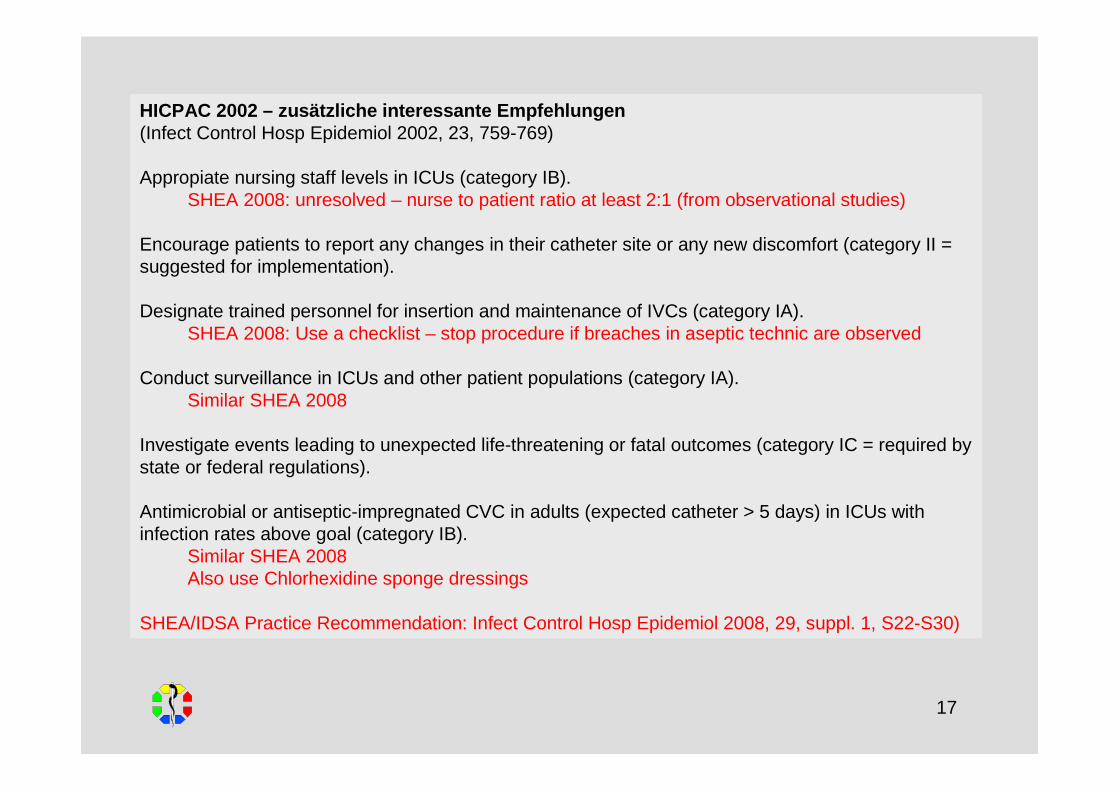
HICPAC 2002 – zusätzliche interessante Empfehlungen(Infect Control Hosp Epidemiol 2002, 23, 759-769)
Appropiate nursing staff levels in ICUs (category IB).SHEA 2008: unresolved – nurse to patient ratio at least 2:1 (from observational studies)
Encourage patients to report any changes in their catheter site or any new discomfort (category II = suggested for implementation).
Designate trained personnel for insertion and maintenance of IVCs (category IA).SHEA 2008: Use a checklist – stop procedure if breaches in aseptic technic are observed
Conduct surveillance in ICUs and other patient populations (category IA).Similar SHEA 2008
Investigate events leading to unexpected life-threatening or fatal outcomes (category IC = required bystate or federal regulations).
Antimicrobial or antiseptic-impregnated CVC in adults (expected catheter > 5 days) in ICUs withinfection rates above goal (category IB).
Similar SHEA 2008Also use Chlorhexidine sponge dressings
SHEA/IDSA Practice Recommendation: Infect Control Hosp Epidemiol 2008, 29, suppl. 1, S22-S30)
18
Pronovost et al: An intervention to decrease catheter-relatedbloodstream infections in the ICU. N Engl J Med 355, 2006, 2725-2732
103 ICUs, vorwiegend in Michigan
Bundle, u.a.Ein Arzt und ein Pflegekraft als Team-Leader,Kenntnisse verbreiten,Telefonkonferenzen jede Woche,Schulung durch Projektleitung,zentrale Treffen zweimal im Jahr.
19
Pronovost et al: An intervention to decrease catheter-relatedbloodstream infections in the ICU. N Engl J Med 355, 2006, 2725-2732
103 ICUs in Michigan
Bundle, u.a.Ein Arzt und ein Pflegekraft als Team-Leader,Kenntnisse verbreiten,Telefonkonferenzen jede Woche,Schulung durch Projektleitung,Zentrale Treffen zweimal im Jahr.
20
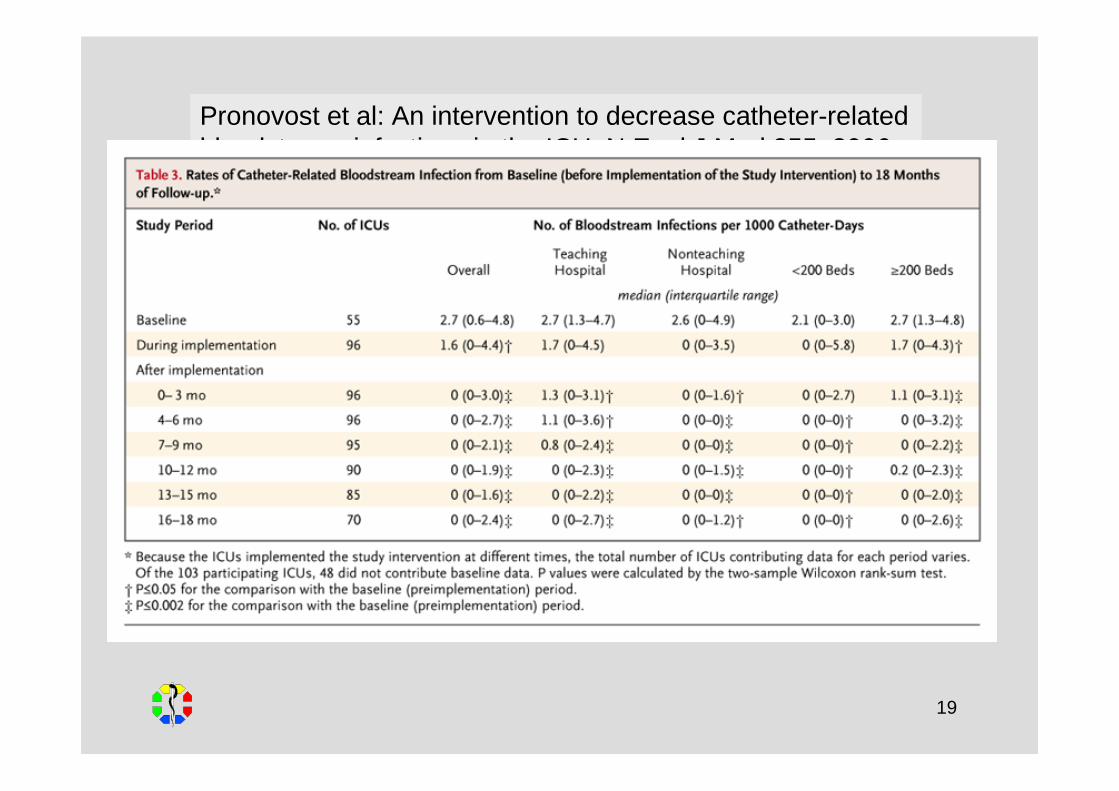
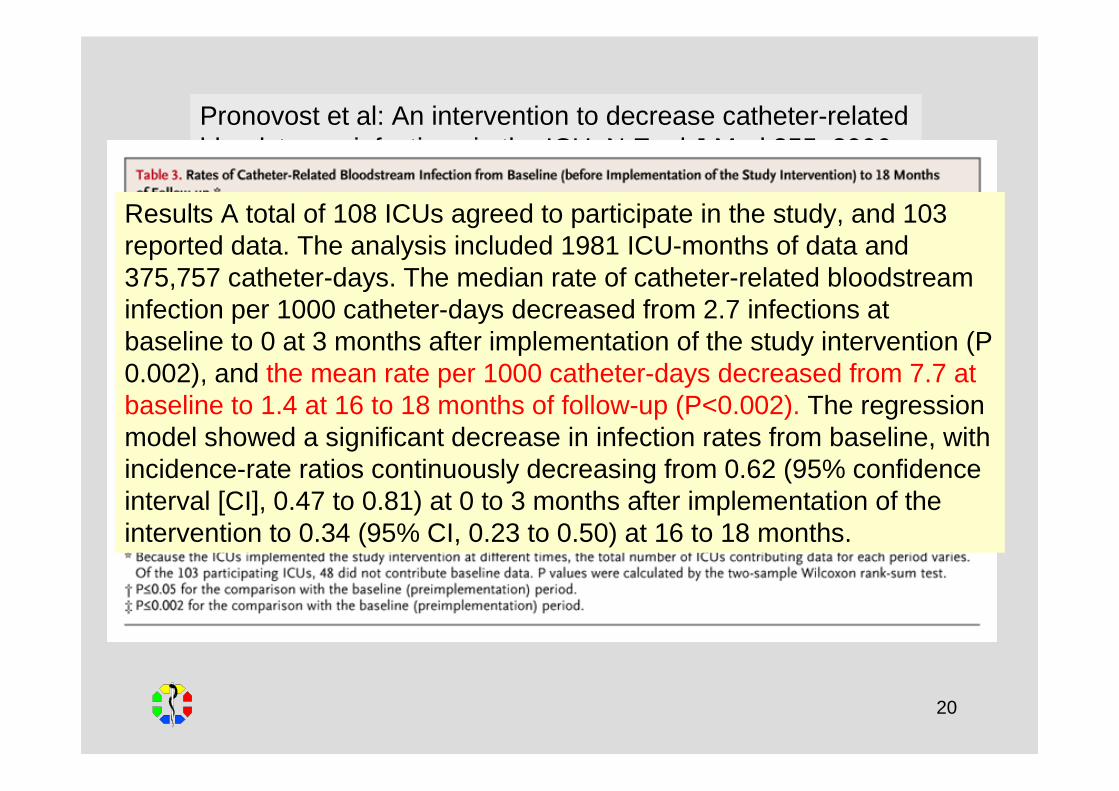
Pronovost et al: An intervention to decrease catheter-relatedbloodstream infections in the ICU. N Engl J Med 355, 2006, 2725-2732
103 ICUs in Michigan
Bundle, u.a.Ein Arzt und ein Pflegekraft als Team-Leader,Kenntnisse verbreiten,Telefonkonferenzen jede Woche,Schulung durch Projektleitung,Zentrale Treffen zweimal im Jahr.
Results A total of 108 ICUs agreed to participate in the study, and 103 reported data. The analysis included 1981 ICU-months of data and 375,757 catheter-days. The median rate of catheter-related bloodstreaminfection per 1000 catheter-days decreased from 2.7 infections at baseline to 0 at 3 months after implementation of the study intervention (P 0.002), and the mean rate per 1000 catheter-days decreased from 7.7 at baseline to 1.4 at 16 to 18 months of follow-up (P<0.002). The regressionmodel showed a significant decrease in infection rates from baseline, withincidence-rate ratios continuously decreasing from 0.62 (95% confidenceinterval [CI], 0.47 to 0.81) at 0 to 3 months after implementation of theintervention to 0.34 (95% CI, 0.23 to 0.50) at 16 to 18 months.
21
Copyright ©2006 BMJ Publishing Group Ltd.
Warren et al: The Effect of an Education Program on the Incidence of Central VenousCatheter-Associated Bloodstream Infection in a Medical ICU. Chest 2004, 126, 1612-1618
Setting: The 19-bed medical ICU in a 1,400-bed university-affiliated urban teaching hospital.
Intervention: A mandatory education program directed toward ICU nurses and physicians was developed by a multidisciplinary task force to highlight correct practices for theprevention of catheter-associated bloodstream infection. The program consisted of a 10-page self-study module on risk factors and practice modifications involved in catheter-related bloodstream infections and in-services at scheduled staff meetings. Eachparticipant was required to complete a pretest before reviewing the study module and an identical test after completion of the study module. Fact sheets and posters reinforcingthe information in the study module were also posted throughout the ICU.
22
Copyright ©2006 BMJ Publishing Group Ltd.
Warren et al: The Effect of an Education Program on the Incidence of Central VenousCatheter-Associated Bloodstream Infection in a Medical ICU. Chest 2004, 126, 1612-1618
Setting: The 19-bed medical ICU in a 1,400-bed university-affiliated urban teaching hospital.
Intervention: A mandatory education program directed toward ICU nurses and physicians was developed by a multidisciplinary task force to highlight correct practices for theprevention of catheter-associated bloodstream infection. The program consisted of a 10-page self-study module on risk factors and practice modifications involved in catheter-related bloodstream infections and in-services at scheduled staff meetings. Eachparticipant was required to complete a pretest before reviewing the study module and an identical test after completion of the study module. Fact sheets and posters reinforcingthe information in the study module were also posted throughout the ICU.
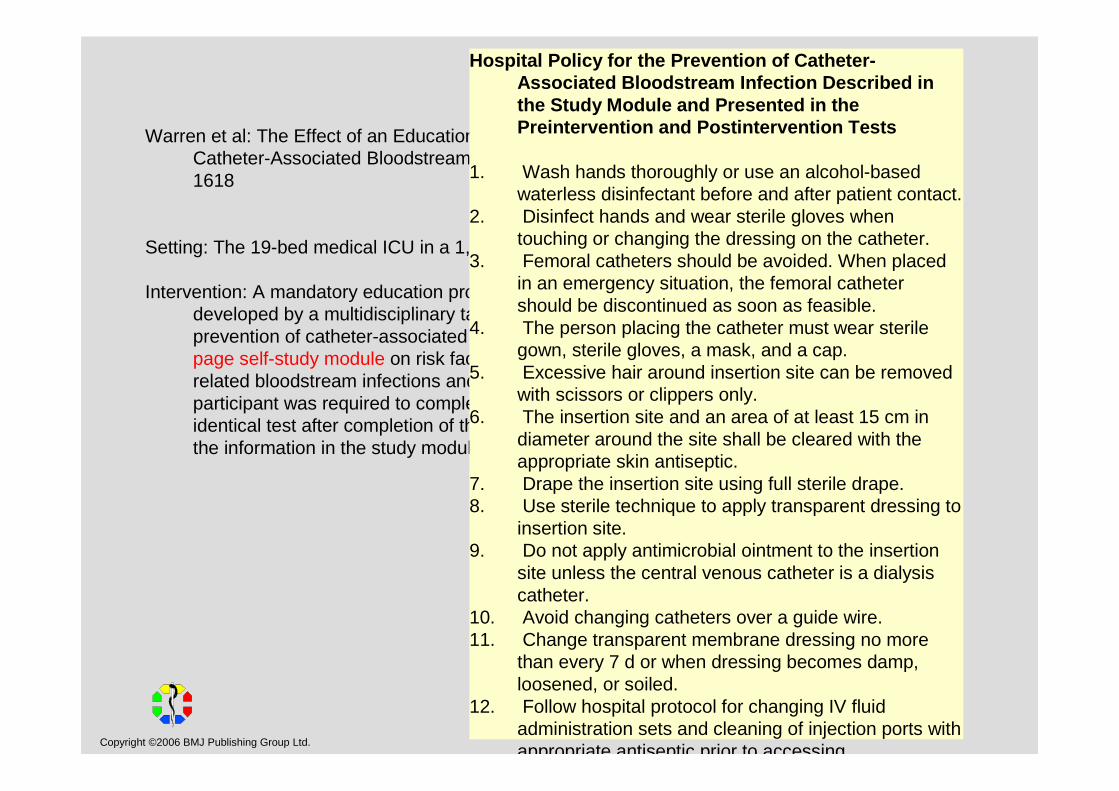
Hospital Policy for the Prevention of Catheter-Associated Bloodstream Infection Described in the Study Module and Presented in thePreintervention and Postintervention Tests
1. Wash hands thoroughly or use an alcohol-basedwaterless disinfectant before and after patient contact.
2. Disinfect hands and wear sterile gloves whentouching or changing the dressing on the catheter.
3. Femoral catheters should be avoided. When placedin an emergency situation, the femoral cathetershould be discontinued as soon as feasible.
4. The person placing the catheter must wear sterile gown, sterile gloves, a mask, and a cap.
5. Excessive hair around insertion site can be removedwith scissors or clippers only.
6. The insertion site and an area of at least 15 cm in diameter around the site shall be cleared with theappropriate skin antiseptic.
7. Drape the insertion site using full sterile drape.8. Use sterile technique to apply transparent dressing to
insertion site.9. Do not apply antimicrobial ointment to the insertion
site unless the central venous catheter is a dialysiscatheter.
10. Avoid changing catheters over a guide wire.11. Change transparent membrane dressing no more
than every 7 d or when dressing becomes damp, loosened, or soiled.
12. Follow hospital protocol for changing IV fluidadministration sets and cleaning of injection ports withappropriate antiseptic prior to accessing.
23
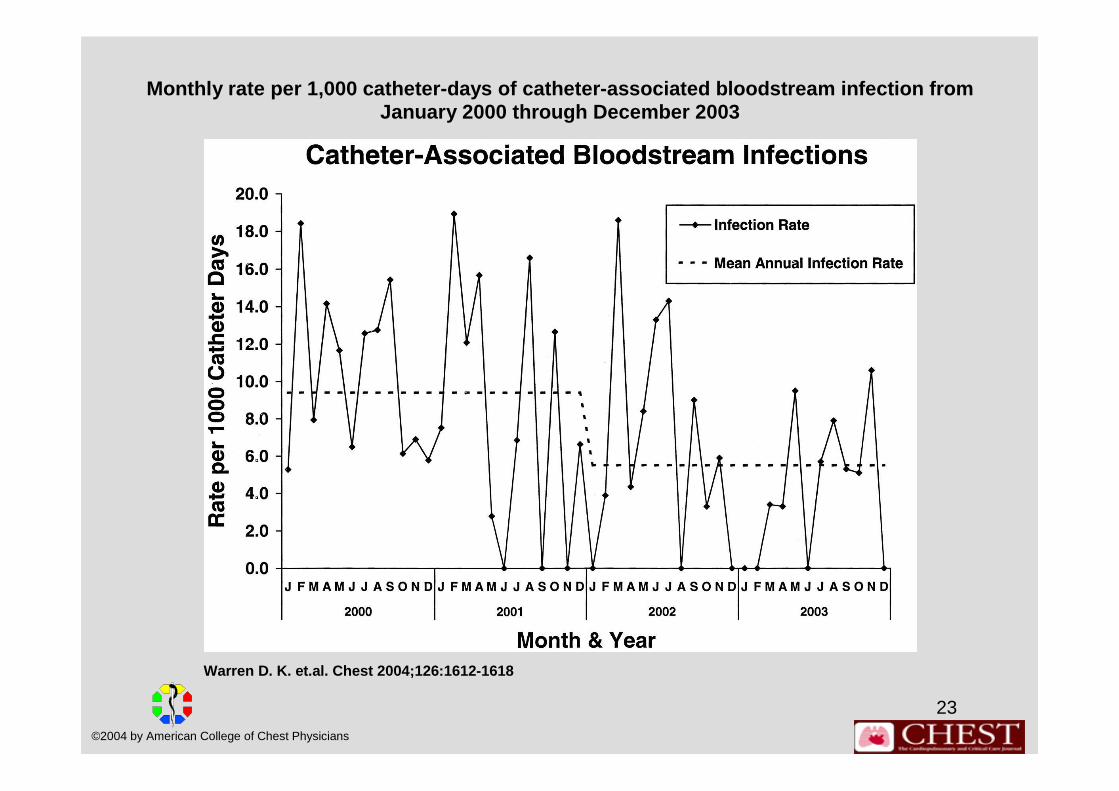
Monthly rate per 1,000 catheter-days of catheter-as sociated bloodstream infection from January 2000 through December 2003
Warren D. K. et.al. Chest 2004;126:1612-1618
©2004 by American College of Chest Physicians
24
Copyright ©2006 BMJ Publishing Group Ltd.
Warren et al: The Effect of an Education Program on the Incidence of Central VenousCatheter-Associated Bloodstream Infection in a Medical ICU. Chest 2004, 126, 1612-1618
Setting: The 19-bed medical ICU in a 1,400-bed university-affiliated urban teaching hospital.
Intervention: A mandatory education program directed toward ICU nurses and physicians was developed by a multidisciplinary task force to highlight correct practices for theprevention of catheter-associated bloodstream infection. The program consisted of a 10-page self-study module on risk factors and practice modifications involved in catheter-related bloodstream infections and in-services at scheduled staff meetings. Eachparticipant was required to complete a pretest before reviewing the study module and an identical test after completion of the study module. Fact sheets and posters reinforcingthe information in the study module were also posted throughout the ICU.
Measurements and main results: Seventy-four episodes of catheter-associated bloodstreaminfection occurred in 7,879 catheter-days (9.4 per 1,000 catheter-days) in the 24 monthsbefore the introduction of the education program. Following implementation of theintervention, the rate of catheter-associated bloodstream infection decreased to 41 episodes in 7,455 catheter days (5.5 per 1,000 catheter-days) [p = 0.019]. The estimatedcost savings secondary to the decreased rate of catheter-associated bloodstreaminfection for the 24 months following introduction of the education program was between$103,600 and $1,573,000.
25
Copyright ©2006 BMJ Publishing Group Ltd.
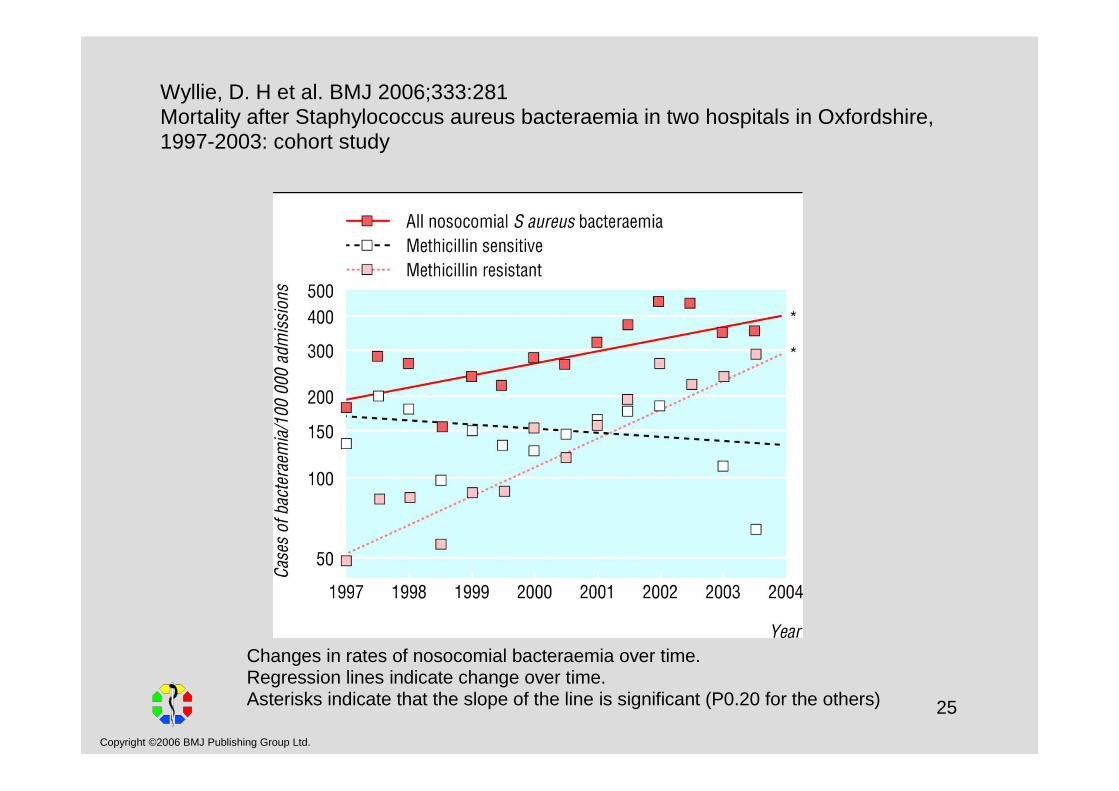
Wyllie, D. H et al. BMJ 2006;333:281Mortality after Staphylococcus aureus bacteraemia in two hospitals in Oxfordshire, 1997-2003: cohort study
Changes in rates of nosocomial bacteraemia over time.Regression lines indicate change over time.Asterisks indicate that the slope of the line is significant (P0.20 for the others)
26
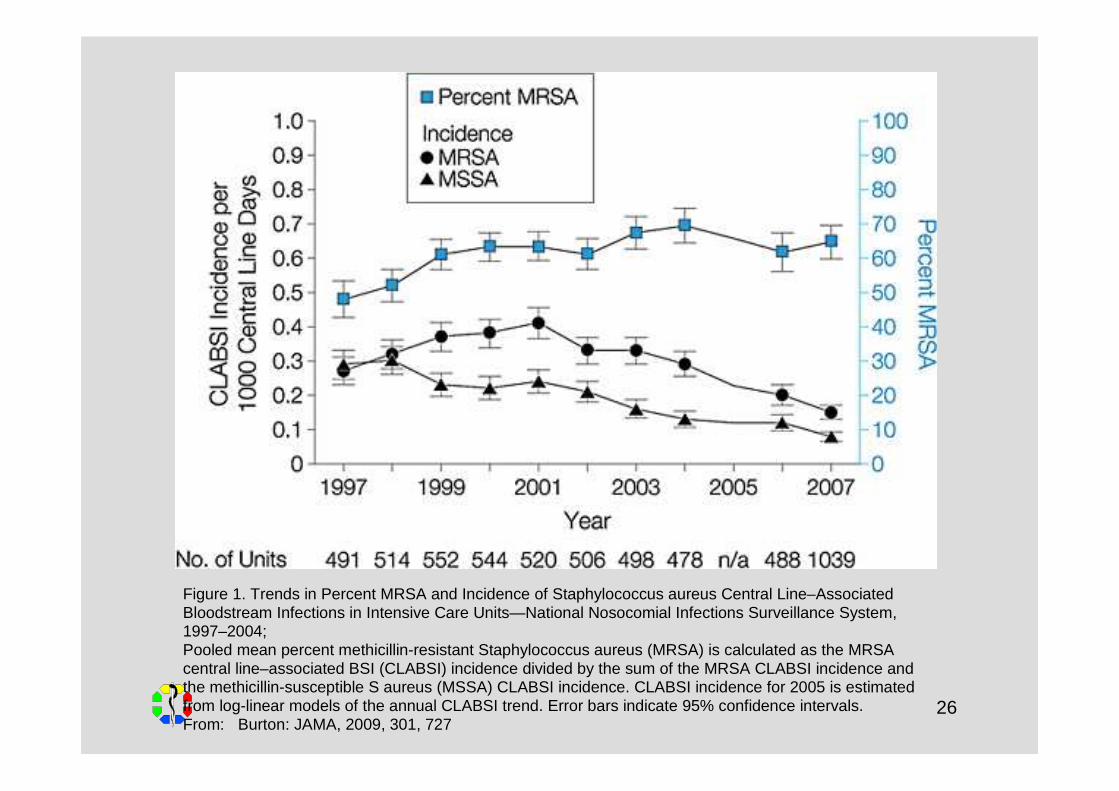
Figure 1. Trends in Percent MRSA and Incidence of Staphylococcus aureus Central Line–AssociatedBloodstream Infections in Intensive Care Units—National Nosocomial Infections Surveillance System, 1997–2004; Pooled mean percent methicillin-resistant Staphylococcus aureus (MRSA) is calculated as the MRSA central line–associated BSI (CLABSI) incidence divided by the sum of the MRSA CLABSI incidence and the methicillin-susceptible S aureus (MSSA) CLABSI incidence. CLABSI incidence for 2005 is estimatedfrom log-linear models of the annual CLABSI trend. Error bars indicate 95% confidence intervals. From: Burton: JAMA, 2009, 301, 727
27
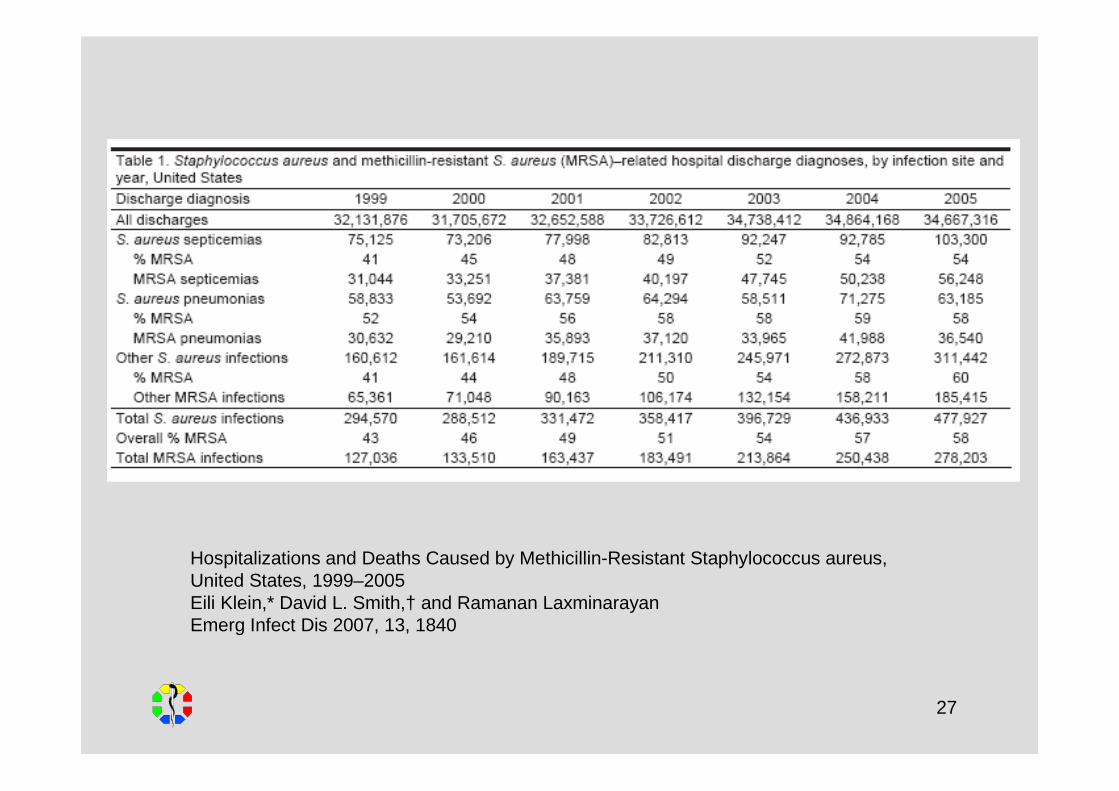
Hospitalizations and Deaths Caused by Methicillin-Resistant Staphylococcus aureus, United States, 1999–2005Eili Klein,* David L. Smith,† and Ramanan LaxminarayanEmerg Infect Dis 2007, 13, 1840
28
Copyright ©2006 BMJ Publishing Group Ltd.
Perencevich, Pittet:Preventing catheter-related bloodstream infections. Th inking outside the checklist. Editorial.JAMA 2009, 301, 1285-1287
Approximately 80.000 catheter-related bloodstream infections occur annually in US intensive care units (ICUs) and are associated with as many as 24 000 patient deaths.Each of these infections is estimated to have a mean attributable cost of $18 000 and an associated excess hospital stay of 12 days per episode.…To counteract this, since October 2008, the Centers for Medicare & Medicaid Services will no longer reimburse hospitals for expenses associated with catheter-related bloodstreaminfections. Similar strategies have been proposed in some countries in Europe and elsewhere.…starting in January 2010 the Joint Commission's Hospital Accreditation Program National Patient Safety Goals will require the use of a catheter checklist and a standardized protocolfor central venous catheter (CVC) insertion, along with other measures.
The most frequently cited bundle of interventions includes appropriate hand hygiene, use of chlorhexidine for skin antisepsis, use of maximal sterile barrier precautions (mask, sterile gown, sterile gloves, and large sterile drapes) during catheter insertion, avoidance of thefemoral vein, and prompt removal of unnecessary catheters. Adherence to these basicinfection control practices was tracked using a checklist and was associated with a 66% reduction in catheter-related bloodstream infections in a quasi-experimental study.
29
Copyright ©2006 BMJ Publishing Group Ltd.
The Joint CommissionAccreditation Program: HospitalNational patient safety goals2008
Goal 7: Reduce the risk of health care associated infections.NPSG.07.04.01Implement best practices or evidence-based guidelines to preventcentral line-associated bloodstream infections
Beginn in 2009,Tests (milestones) in 3-Monats-Abständen,Volle Implementierung 2010, u.a.:
Schulung benannter Mitarbeiter,Unterrichtung der Patienten und ihrer Angehörigen,periodische Erfassung von Infektionen und Compliance,Standardprotokoll beim Legen und Checkliste,routinemäßige tägliche Evaluation der Notwendigkeit des Liegens.

30
Institute for Healthcare Improvement, 2007Central line bundle elements
1. Hand hygiene2. Maximal barrier precautions3. Chlorhexidine skin antisepsis4. Optimal catheter site selection, with avoidance of
using the femoral vein for central venous access in adult patients
5. Daily review of line necessity with prompt removal of unnecessary lines
31
Key Change: Central Line Checklist
• Have the nurse document compliance with the insertion criteria at the time of insertion.
• Create a culture of safety and prevention:
☺ empower nurses to stop line placement if improper techniques are used
• Instruct nurses in use of critical communication strategies to facilitate important exchanges.
� e.g. “the sterile field has been contaminated,” rather than “YouYou contaminated the catheter!”
32
Copyright ©2006 BMJ Publishing Group Ltd.
How patients and family members can help:
Watch the hospital staff to make sure they wash their handsbefore and after working with the patient. Do not be afraid to remind them to wash their hands!
Ask the doctors and nurses lots of questions before you agreeto a line.Questions can include: Which vein will you use to put in theline? How will you clean the skin when the line goes in? Whatsteps are you taking to lower the risk of infection?
Make sure the doctors and nurses check the line every day forsigns of infection. They should only replace the line whenneeded and not on a schedule.
(Infoflyer für Patienten)
33
Copyright ©2006 BMJ Publishing Group Ltd.
Erfolge in Frankreich
Nationales Programm 1999-2004:Krankenhaushygienische Struktur: 1 Facharzt für 800 Betten, eineFachkraft für 400 Betten.Empfehlungen bekanntmachen.Surveillance in allen Häusern alle 5 Jahre und Meldung ernster NI an zentrale Institution.Patienten und Öffentlichkeit besser informieren.
Nationales Programm 2005-2008:Punktesystem für Erfüllung krankenhaushygienischer Anforderungen.Erfassung von Wundinfektionen.Erfassung Händedesinfektionsmittelverbrauch.MRSA/1.000 Patiententage.Antibiotikaverbrauch/1.000 Patiententage.
Hajjar: J Hosp Infect 2008, 70, 17-21
34
Copyright ©2006 BMJ Publishing Group Ltd.
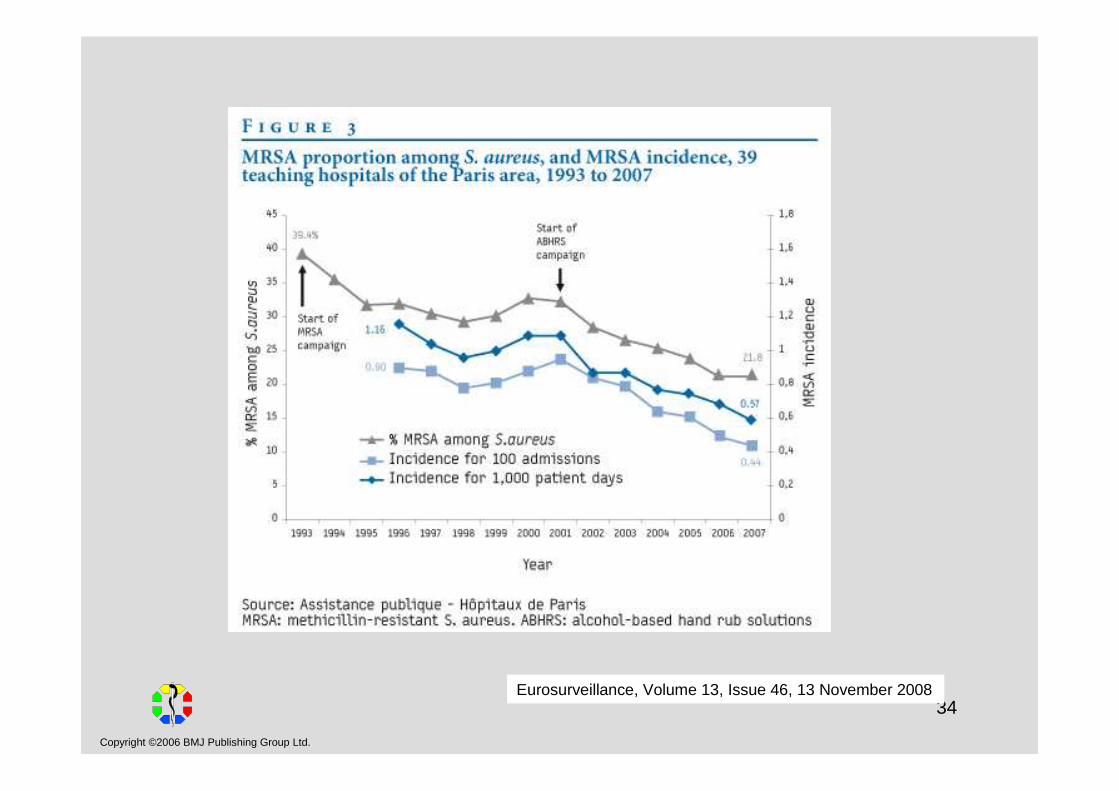
Eurosurveillance, Volume 13, Issue 46, 13 November 2008
35
Copyright ©2006 BMJ Publishing Group Ltd.
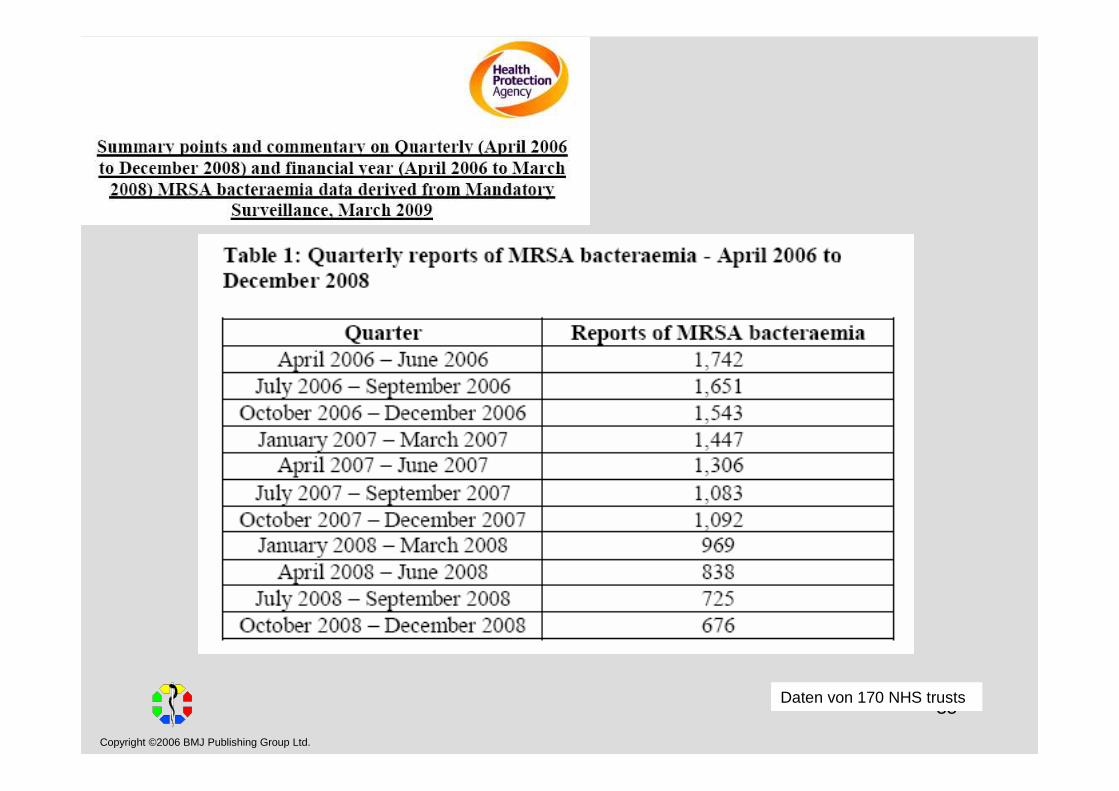
Daten von 170 NHS trusts
36
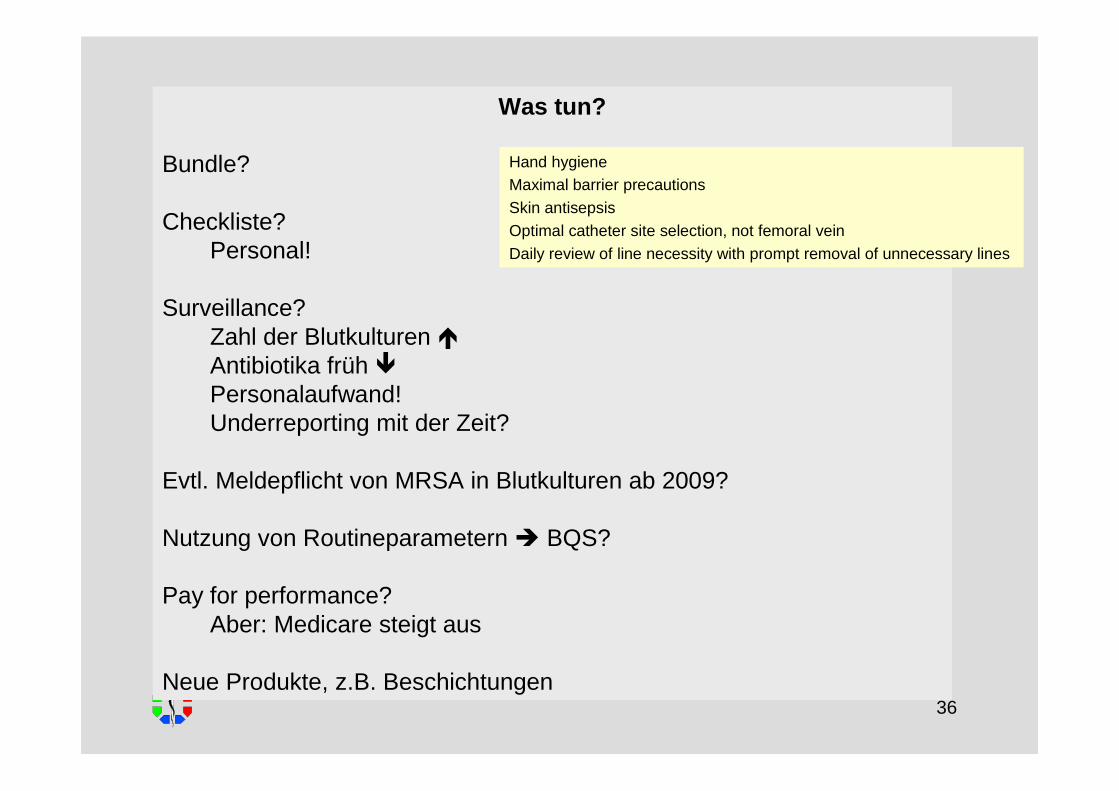
Was tun?
Bundle?
Checkliste?Personal!
Surveillance?Zahl der Blutkulturen �Antibiotika früh �Personalaufwand!Underreporting mit der Zeit?
Evtl. Meldepflicht von MRSA in Blutkulturen ab 2009?
Nutzung von Routineparametern � BQS?
Pay for performance?Aber: Medicare steigt aus
Neue Produkte, z.B. Beschichtungen
Hand hygieneMaximal barrier precautionsSkin antisepsisOptimal catheter site selection, not femoral veinDaily review of line necessity with prompt removal of unnecessary lines