Embed Size (px)
Citation preview
Klinik und Surveillance bei
nosokomialen Infektionen auf Intensivstationen
Alexandra Petre
Univ.-Prof. Dr.med.univ. Michael Hiesmayr
Medizinische Universität Wien
Universitätsklinik für Herz-, Thorax- und Gefässchirurgische Anästhesie und
Intensivmedizin, Allgemeines Krankenhaus Wien
nosokomiale Infektionen auf der ICU
15-30% aller Patienten auf ICU
LOS x3
Outcome nach nosokomialer Infektion
höhere Mortalität
nosokomiale Infektionen UND deren Anzahl – stärkste Korrelation
mit einer verlängerten Aufenthaltsdauer (LOS)
• nosokomiale Infektionen auf der ICU – Klinik
klinische Zeichen x Limitierung? Aussagekraft?
Infektionsparameter x Spezifität? Diagnose? Prognose?
Radiologie x Spezifität?
Mikrobiologie x geeignete Therapie?
Prävention
• nosokomiale Infektionen auf der ICU – Surveillance
Surveillance = systematische Einsammlung und Analyse von Daten über
Krankheiten, anschliessende Bewertung der Daten und
Entscheidungsfindung bezüglich der Implementierung
notweniger Massnahmen
Mikrobiologie
Radiologie
Infektionsmarker
klinische Zeichen
Inzidenz der nosokomialen Infektionen, Prävention
→ Beurteilung von Symptomkomplexen
im Sinne einer einheitlichen Festlegung
über das Vorhandensein nosokomialer
Infektionen
• Problemstellung
1) patientenzentriert KLINIK
- erfolgreiche Behandlung
2) stationszentriert SURVEILLANCE
- Qualitätssicherung
- Hygienestandard
- Ökologie der Keime
• Problemdetail
– SURVEILLANCE
Standardisierung und weitgehende Implementierung
einheitlicher Definitionen
under-ascertainment – Fälle werden nicht diagnostiziert
under-reporting – Fälle werden nicht i.R. der Surveillance
erfasst
– KLINIK
Unterbehandlung – schlechtes Outcome
Überbehandlung – Resistenz, Toxizität
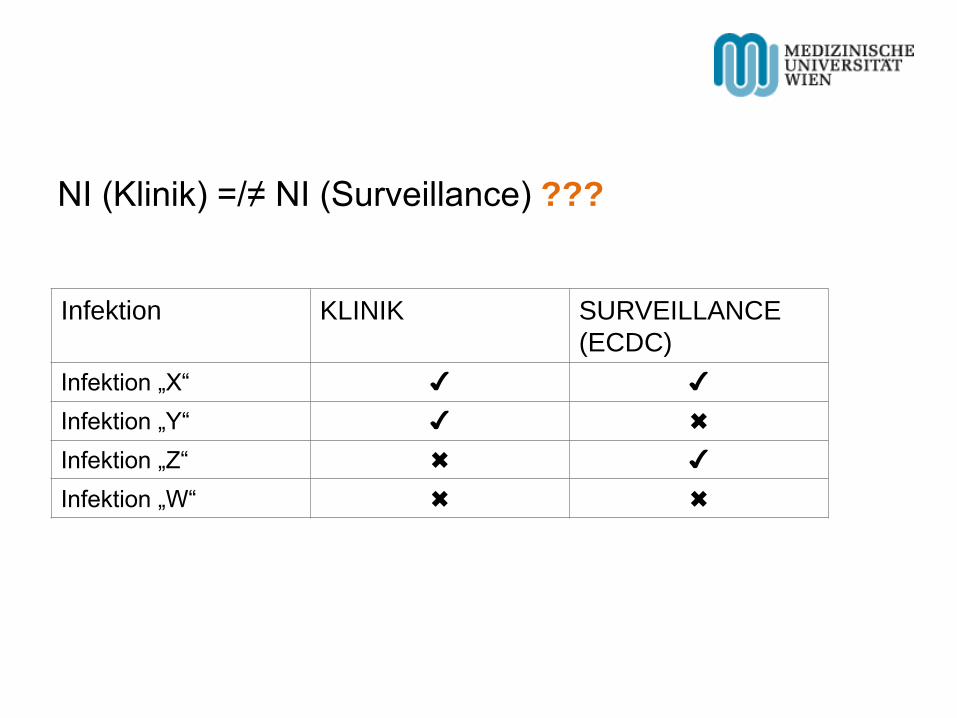
NI (Klinik) =/≠ NI (Surveillance) ???
Infektion KLINIK SURVEILLANCE
(ECDC)
Infektion „X“ ✔ ✔
Infektion „Y“ ✔ ✖
Infektion „Z“ ✖ ✔
Infektion „W“ ✖ ✖
• Population • konsekutive Patienten mit Antibiotika-Therapie und LOS >2d
• drei Intensivstationen (Allgemeines Krankenhaus der Stadt Wien)
• Exposure • „Bloodstream Infection“ (BSI), „Pneumonia“ (PN 1-5), „Urinary Tract
Infection“ (UTI), „Catheter-related Infection“ (CRI1-3), „Skin and Soft
Tissue Infection“ (SST) nach ECDC Definitionen
• Comparison • PN 1-5, BSI, UTI und SSI klinisch diagnostiziert (z.B. AB-
Behandlung/Umstellung, Katheterwechsel, Reoperation)
• Outcome • Konkordanz
• Under-reporting, Under-ascertainment
• Fall 1 – Patient T.E., 54J, 4 Tage LOS
- HTX 14/06
- ICU-Aufnahme 14/06, ICU-Entlassung 17/06
- Tazonam prophylaktisch
KLINIK SURVEILLANCE
Infektion ✖ ✖
• Fall 2 – Patient B.A., 51J, 12 Tage LOS
- MKE am 05/06;
- 12/06: ZVK-Wechsel wegen steigender Entzündungswerte, Fieber
bis 38,5°C; kurze hämodynamische Instabilität
Septifast, Blutkultur, Tazonam Start
- 13/06: Septifast negativ
- 14/06: BK + nach 20 Stunden – Staph. epidermidis
- 18/06: ZVK Spitze – Staph. epidermidis und haemolyticus >100KBE
KLINIK: „Cavasepsis“ ≈ SURVEILLANCE: „CRI-3“
KLINIK SURVEILLANCE
Infektion ✔ ✔
• Fall 3 – Patient N.G., 62J, 13 Tage LOS
– Übernahme zur prä-operativen Evaluierung für LVAD;
– Tazonam prophylaktisch
– Fieber, CRP, Noradrenalin, Beatmungsaufwand
– 2xReanimation, ECMO-Implantation
– BAL – H. influenzae, Streptococcus pneumoniae, E.coli, Candida
tropicalis jeweils 10E4KBE/ml
– BK und ZVK-Spitze – kein Wachstum
– C/P kein Hinweis auf Infiltrat
KLINIK: Pneumonie SURVEILLANCE: ≠ Pneumonie
KLINIK SURVEILLANCE
Infektion ✔ ✖
• Fall 4
– Intensivpatient – Symptome schwer beurteilbar
– UTI-A
KLINIK SURVEILLANCE
Infektion ✖ ✔
Analyse (ECDC) nach Mikrobiologie (390 Patienten)
(≈ 3000 Datensätze)
- 27 x Pneumonia
- 42 x Bloodstream Infection
- 60 x Catheter-related Infection
- 14 x Urinary Tract Infection
143 Infektepisoden
Sample: 112 Patienten
- 68 männlich, 44 weiblich (61% bzw. 39%)
- 60 Patienten auf chir. ICU, 52 Patienten auf kard. ICU
(54% bzw. 46%)
- Alter (mean) ≈ 65a, SD 15a
- LOS (mean) 12d, SD 14d
- LOS pre-ICU 9d, SD 15d
Sample: 112 Patienten (2)
- Herkunft:
52% Aufwachraum
31% Station
6% andere ICU
11% andere
- Aufnahmegrund (chir./intern.):
50% chirurgisch (elektiv)
30% internistisch
20% chirurgisch (Notfall)
Sample: 112 Patienten (3)
- Aufnahmegrund
83% kardial
11% respiratorisch
6% andere (z.B. neurologisch, septisch)
- Operation
67% Herz-OP (ausser CABG)
16% Herz: CABG und andere
8% vaskulär
7% CABG
2% andere
Sample: 112 Patienten (4)
- Komorbiditäten
49 Patienten (44%):
46 Patienten: Herzversagen (NYHA IV)
2 Patienten: Chemotherapie
1 Patient: Leukämie
- Immunsuppression:
20 Patienten (18%)
- antimikrobielle Therapie bei Aufnahme
92% ≥1 Antibiotika
8% kein Antibiotikum
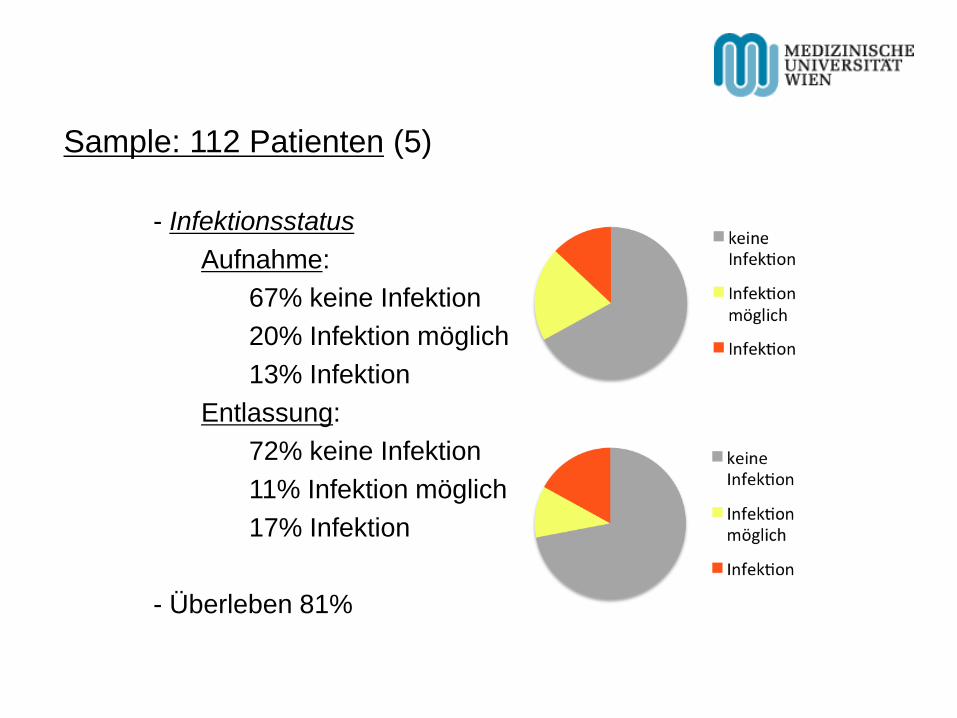
Sample: 112 Patienten (5)
- Infektionsstatus
Aufnahme:
67% keine Infektion
20% Infektion möglich
13% Infektion
Entlassung:
72% keine Infektion
11% Infektion möglich
17% Infektion
- Überleben 81%
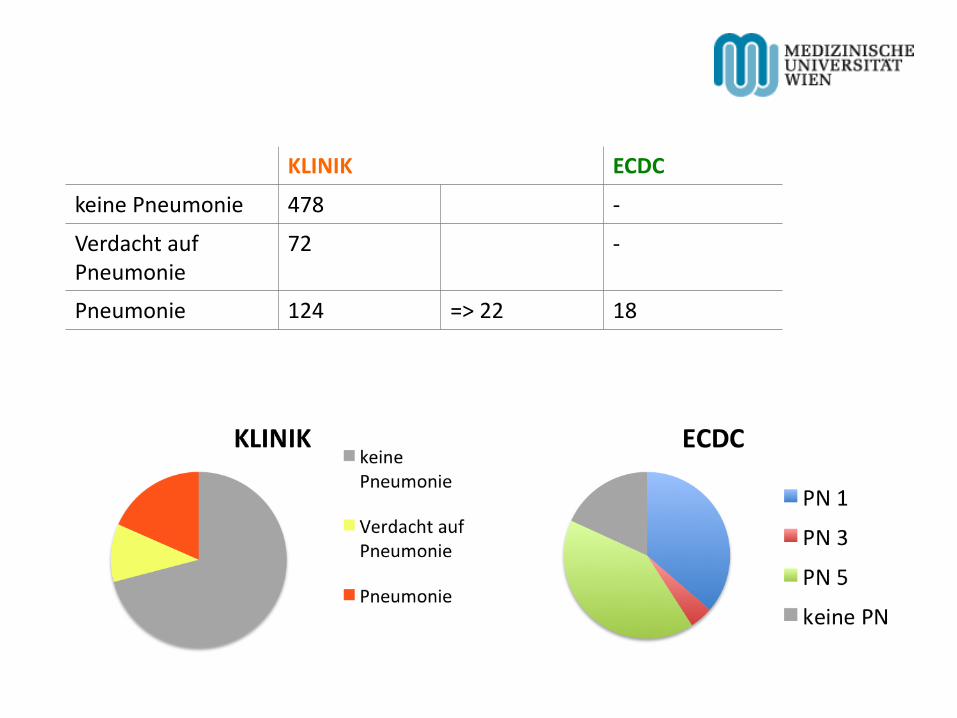
KLINIK ECDC
keine Pneumonie 478 -
Verdacht auf Pneumonie
72 -
Pneumonie 124 => 22 18
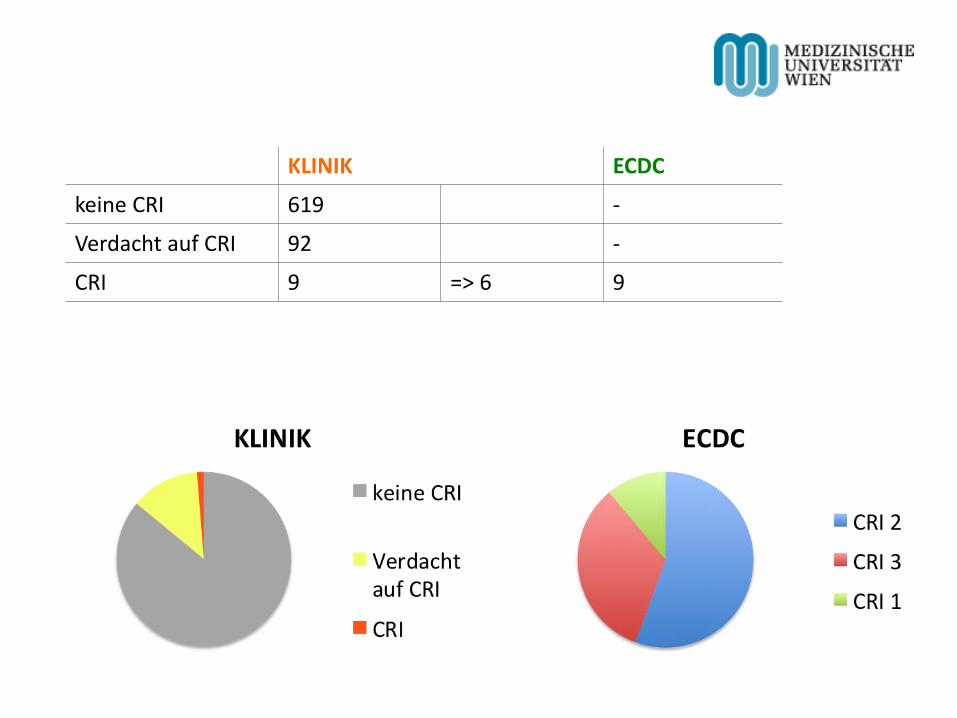
KLINIK ECDC
keine CRI 619 -
Verdacht auf CRI 92 -
CRI 9 => 6 9
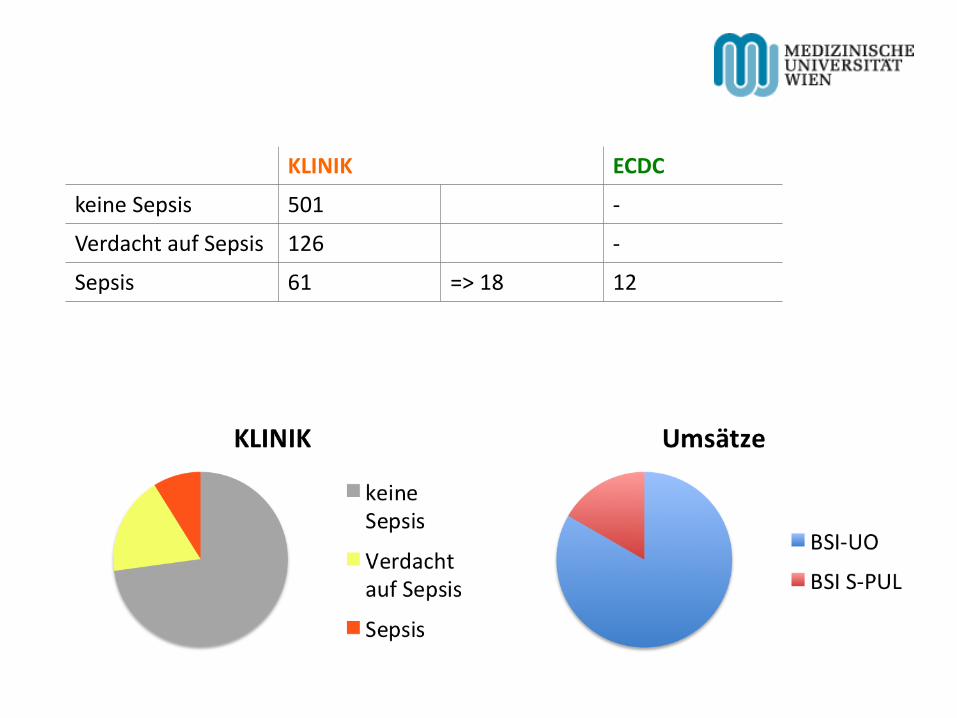
KLINIK ECDC
keine Sepsis 501 -
Verdacht auf Sepsis 126 -
Sepsis 61 => 18 12
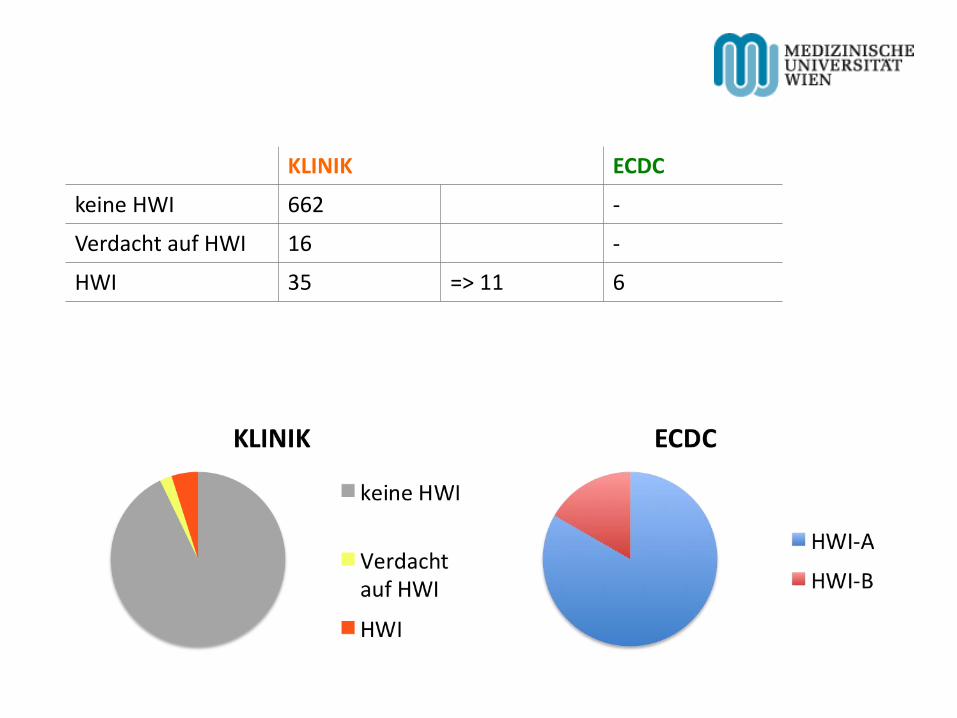
KLINIK ECDC
keine HWI 662 -
Verdacht auf HWI 16 -
HWI 35 => 11 6
Vielen Dank für Ihre Aufmerksamkeit!