Embed Size (px)
Citation preview

Enterobacteriaceae
Dr. Bános ZsuzsaDr. Bános Zsuzsa04 04 -- 11 November 200811 November 2008
Normal bakterielle Flora desGastrointestinaltraktes

GRAMNEGATIVE STÄBCHEN
AEROBBordetellaBrucellaFrancisella
PseudomonasAcinetobacterLegionella
FAKULTATIV ANAEROBHaemophilusPasteurella
Familie:EnterobacteriaceaeVibrionaceae
CardiobacteriumEikenellaKingellaActinobacillus
ANAEROBBacteroidesPrevotellaPorphyromonasFusobacterium
MIKROAEROPHILCampylobacterHelicobacter

Normal bakterielleFlora des
Gastrointestinaltraktes
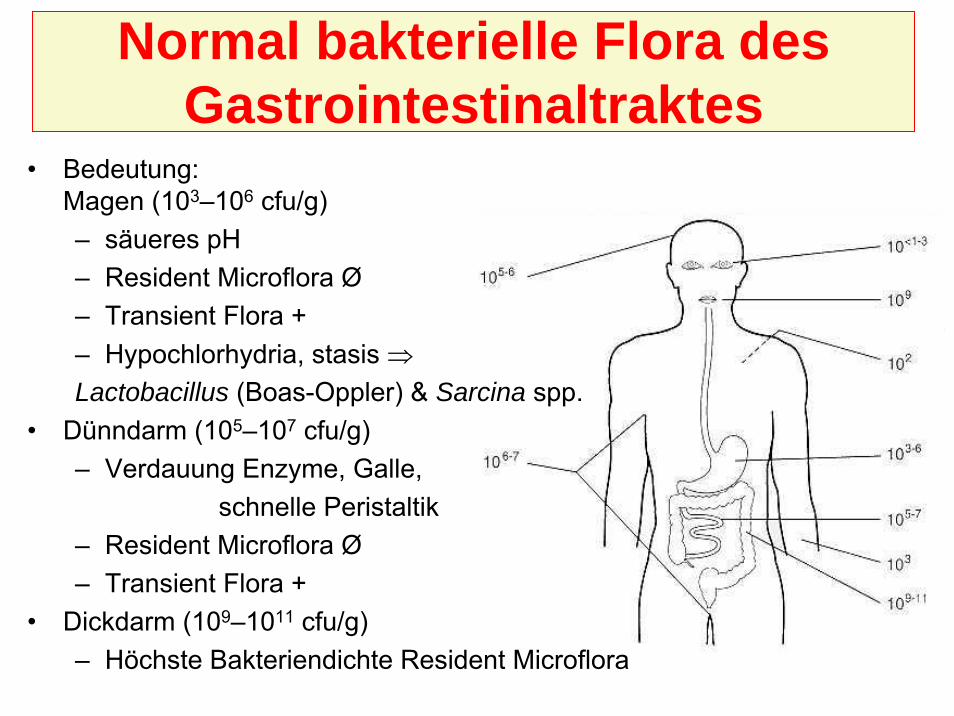
Normal bakterielle Flora desGastrointestinaltraktes
• Bedeutung:Magen (103–106 cfu/g)– säueres pH– Resident Microflora Ø– Transient Flora +– Hypochlorhydria, stasis ⇒Lactobacillus (Boas-Oppler) & Sarcina spp.
• Dünndarm (105–107 cfu/g)– Verdauung Enzyme, Galle,
schnelle Peristaltik– Resident Microflora Ø– Transient Flora +
• Dickdarm (109–1011 cfu/g)– Höchste Bakteriendichte Resident Microflora
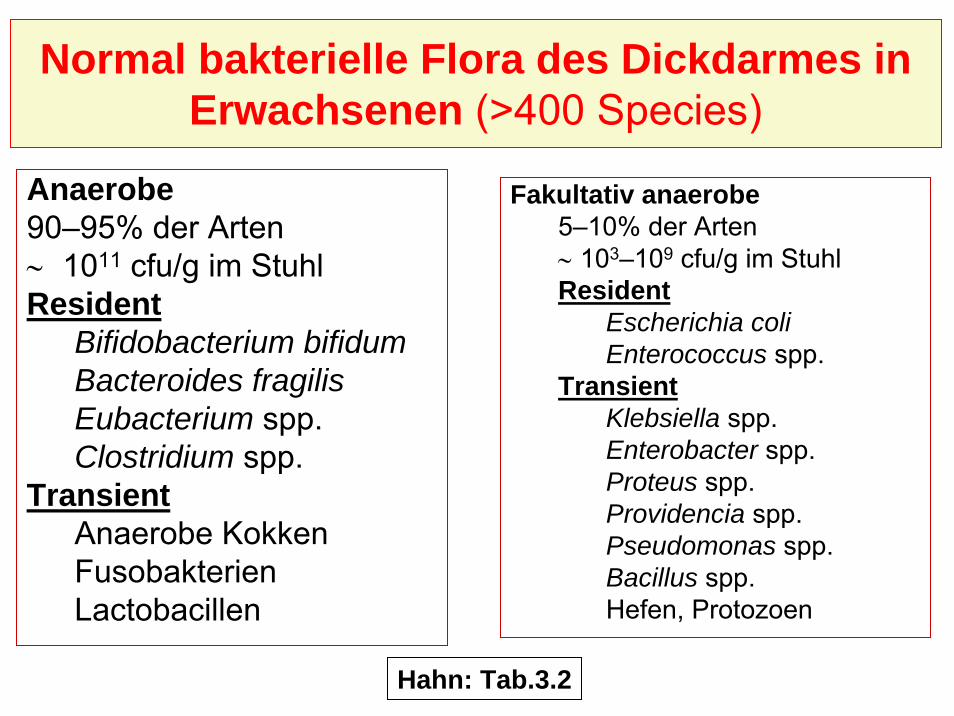
Anaerobe90–95% der Arten∼ 1011 cfu/g im StuhlResident
Bifidobacterium bifidumBacteroides fragilisEubacterium spp.Clostridium spp.
TransientAnaerobe KokkenFusobakterienLactobacillen
Fakultativ anaerobe5–10% der Arten∼ 103–109 cfu/g im StuhlResident
Escherichia coliEnterococcus spp.
TransientKlebsiella spp.Enterobacter spp.Proteus spp.Providencia spp.Pseudomonas spp.Bacillus spp.Hefen, Protozoen
Normal bakterielle Flora des Dickdarmes inErwachsenen (>400 Species)
Hahn: Tab.3.2

• Mit Muttermilch gestillteSäuglinge– Resident
• Bifidobakterien (pH 5,5)– Kolonisierung mit andere Arten ist
gehemmt (Vitamin K Substitution!)• Mischkost
– Erst• Fakultativ anaerobe
– Später• Bacteroides fragilis
Normal bakterielle Flora desDickdarmes der Kinder
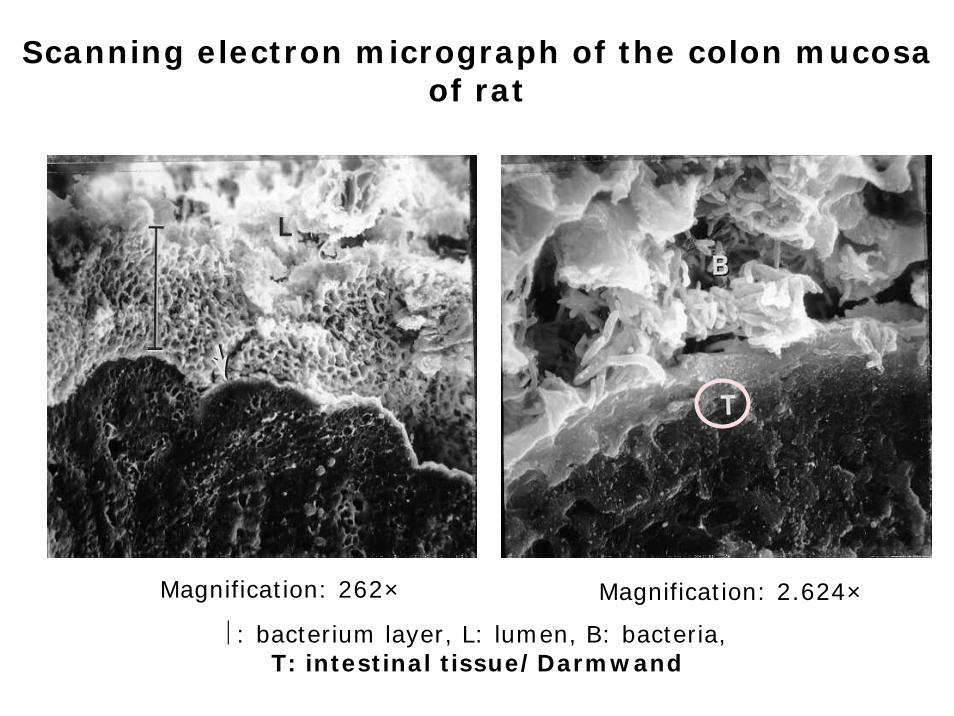
Scanning electron micrograph of the colon mucosa of rat
⎢: bacterium layer, L: lumen, B: bacteria, T: intestinal tissue/Darmwand
Magnification: 262× Magnification: 2.624×

Bedeutung der normal Darmflora
Abbau von NahrungsmittelBildung von Vitaminen: K & B-KomplexGasbildung ⇒ Normal PeristaltikStändige physische & chemische Stimuli ⇒ständige Mukosa TurnoverBiofilmbildung, Blockierung von epithelialenRezeptoren, Rivalität für Nährstoffe ⇒Hemmung von Kolonisation pathogenerBakterienStändige Antigenstimulus ⇒ Entwicklung von ImmunsystemExperimente in keimfreien Tiere

Rolle von normal Bakteriumflora desDickdarmes in pathologischen Prozessen
Extraintestinale InfektionenTranslokation
ImmunmangelzustandObstruktionenShock
KonsequenzenEndotoxaemieBakteriaemieSepsis
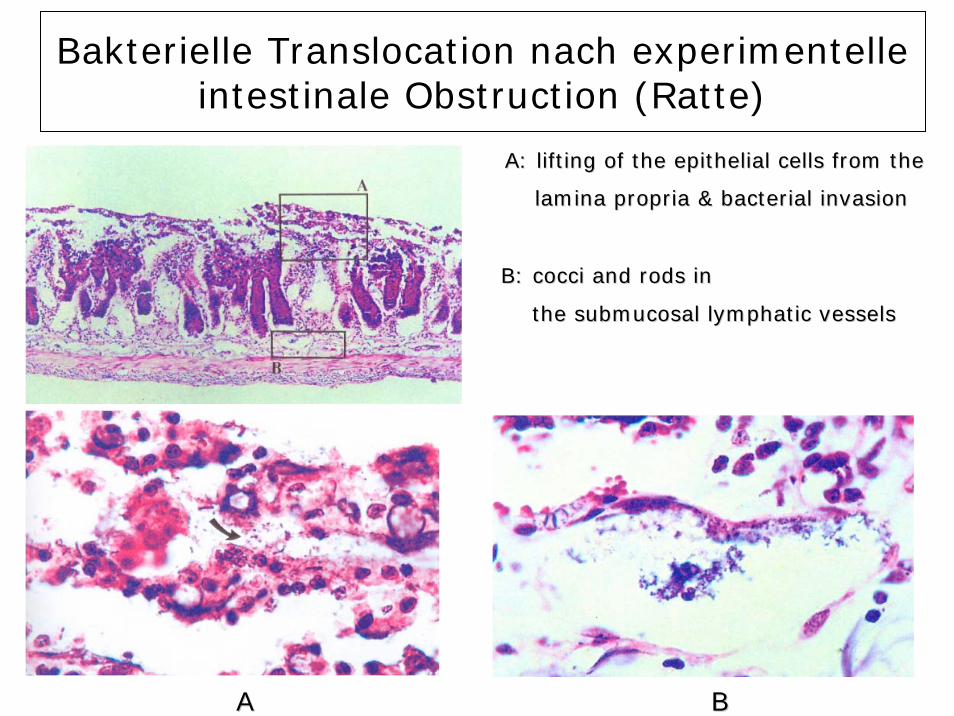
Bakterielle Translocation nach experimentelleintestinale Obstruction (Ratte)
AA BB
A: A: lifting of the epithelial cells from the lifting of the epithelial cells from the
lamina lamina propriapropria & bacterial invasion& bacterial invasion
B: B: coccicocci and rods inand rods in
the the submucosalsubmucosal lymphatic vesselslymphatic vessels

Veränderung von Gleichgewicht dernormal Darmflora
•• UrsacheUrsache– Malnutrition– Breitspektrum (per os) Antibiotika
•• KKonsequenonsequenzzeenn– Maldigestion & Maladsorption, Vitaminmangel– Veränderung von normal Peristaltik, erhöhte
gastrointestinal Gasbildung•• AntibiotiAntibiotikumkumassoassozziiiertiert DDiarrhoeiarrhoe
– Leicht verlaufend: Diarrhoe– Pseudomembranöse Kolitis
(Clostridium difficile)

Pseudomembranöse Kolitis
Thickened wall of the colon Thickened wall of the colon transversumtransversum
Characteristic yellow plaquesCharacteristic yellow plaquesC. difficileC. difficile & & neutrophilsneutrophils

Gramnegative fakultativanaerobe Stäbchen
Enterobacteriaceae

Enterobacteriaceae
Morphologie: - Gram negative Stäbchen- Geißel (Ausnahme: Klebsiella, Shigella)
Züchtung:Einfach, übliche (Agar, Blutagar) MedienDifferenzierung: pathogene-fakultativ pathogene(Biochemische Leistungen)
a) Selektiv-Medienb) Differential-Medienc) Indikator-Medien

Antigene und Virulenzfaktoren:O (Zellwand)H (Flagella)K (Kapsel)Oberflächliche ProteinePiliExotoxineEndotoxine
Enterobacteriaceae

Enterobacteriaceae
Fakultativ pathogeneGattungenEscherichia
Klebsiella GruppeEnterobacterEdwardsiellaCitrobacter
Proteus GruppeSerratiaProvidenciaMorganella
Obligat pathogene (Gattungen)E. Coli
ETEC (enterotoxische)EPEC (enteropathogene)EIEC (enteroinvasive)EHEC (enterohemorrhagische)EAggEC (enteroaggregativ)
ShigellaS. dysenteriaeS. flexneriS. boydiiS. sonnei
SalmonellaS. typhiS. paratyphi
YersiniaY. pestisY. pseudotuberculosisY. enterocolitica
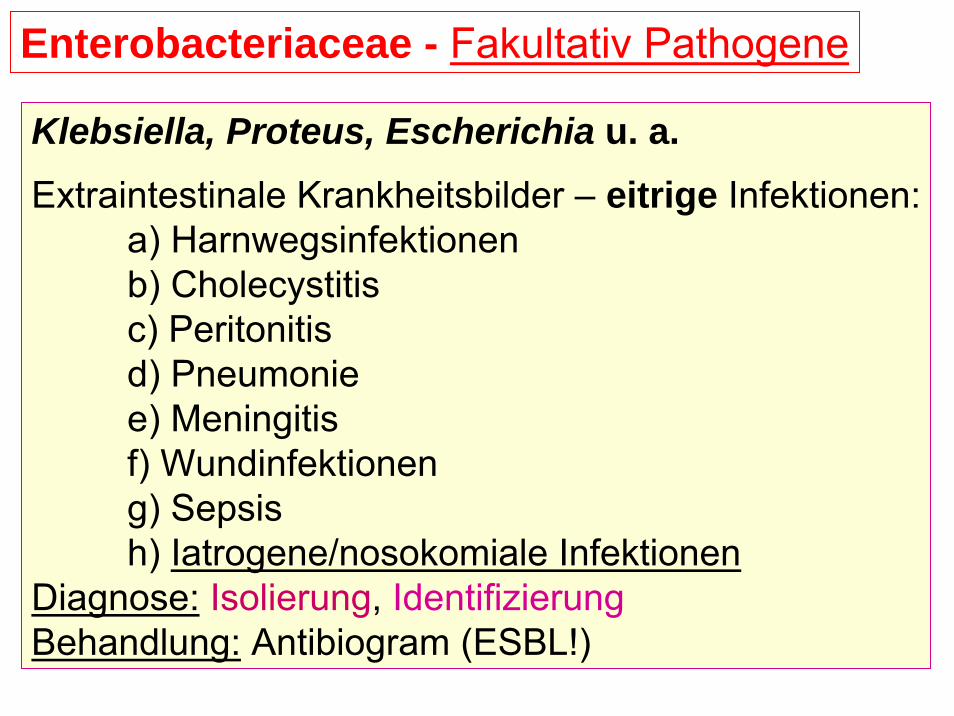
Enterobacteriaceae - Fakultativ Pathogene
Klebsiella, Proteus, Escherichia u. a. Extraintestinale Krankheitsbilder – eitrige Infektionen:
a) Harnwegsinfektionenb) Cholecystitisc) Peritonitisd) Pneumoniee) Meningitisf) Wundinfektioneng) Sepsish) Iatrogene/nosokomiale Infektionen
Diagnose: Isolierung, IdentifizierungBehandlung: Antibiogram (ESBL!)

Serratia marcescens - Serratia marcescens Durch Prodigiosin rotgefärbte Kolonien von Serratia marcescens auf Agargel.
www.biologie.de

pathmicro.med.sc.edu
TSI Medium Identifizierung

Top row, Proteus vulgaris; second row, unidentified enteric bacterium; thirdrow, Klebsiella pneumoniae; bottom row, Vibrio alginolyticus.
helio
s.bt
o.ed
.ac.
ukId
entif
izie
rung
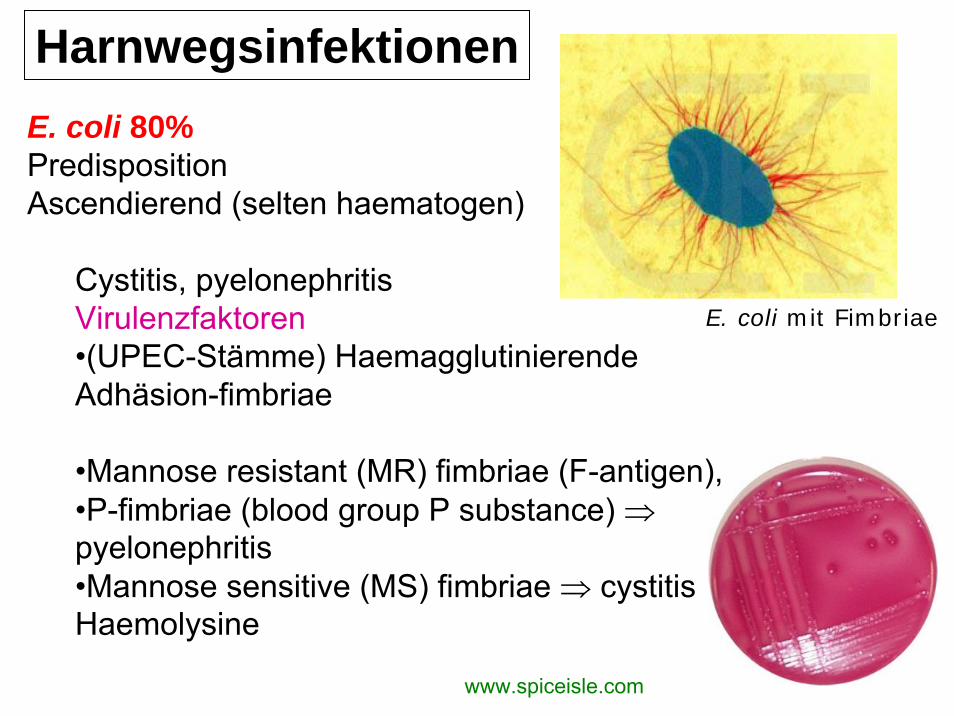
E. coli mit Fimbriae
Harnwegsinfektionen
www.spiceisle.com
E. coli 80%PredispositionAscendierend (selten haematogen)
Cystitis, pyelonephritisVirulenzfaktoren•(UPEC-Stämme) HaemagglutinierendeAdhäsion-fimbriae
•Mannose resistant (MR) fimbriae (F-antigen),•P-fimbriae (blood group P substance) ⇒pyelonephritis•Mannose sensitive (MS) fimbriae ⇒ cystitisHaemolysine
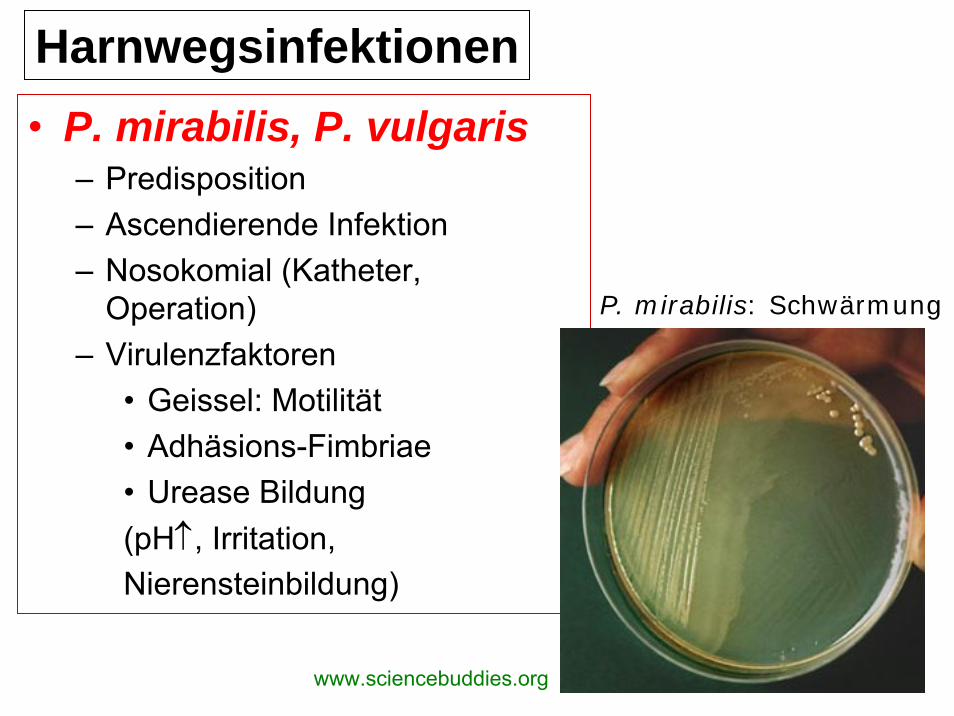
• P. mirabilis, P. vulgaris– Predisposition– Ascendierende Infektion– Nosokomial (Katheter,
Operation)– Virulenzfaktoren
• Geissel: Motilität• Adhäsions-Fimbriae• Urease Bildung(pH↑, Irritation,Nierensteinbildung)
P. mirabilis: Schwärmung
Harnwegsinfektionen
www.sciencebuddies.org
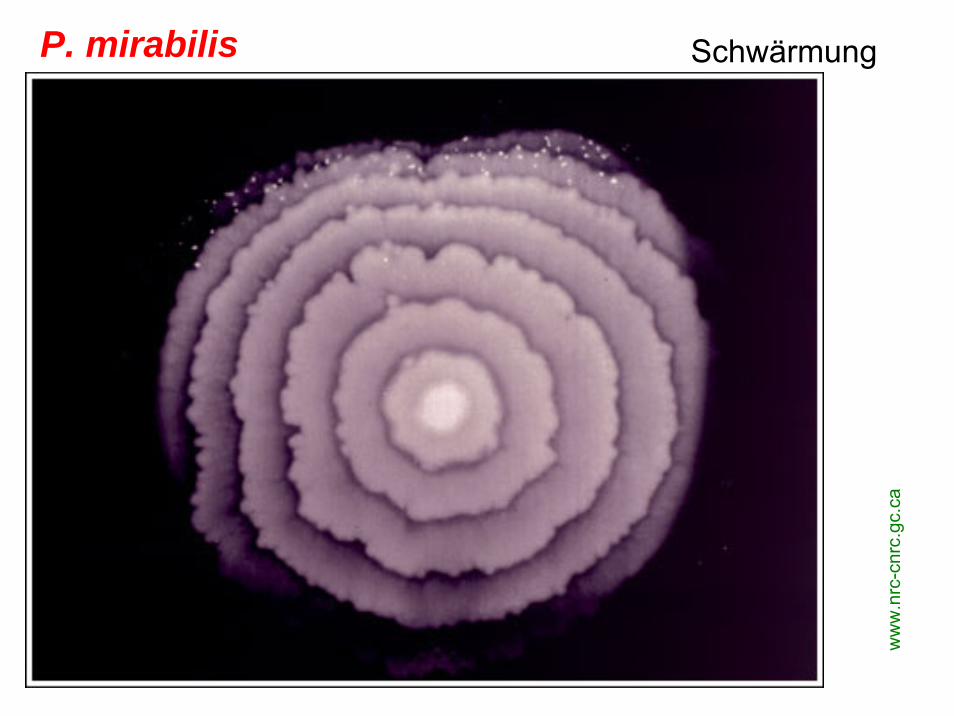
P. mirabilis
ww
w.n
rc-c
nrc.
gc.c
a
Schwärmung

P. mirabilis
Schwärmung- Auf Zellen
www.nrc-cnrc.gc.ca

P. mirabilis
Schwärmung- Auf Zellen
www.nrc-cnrc.gc.ca

biology.clc.uc.edu
Proteus vulgaris Geissel - Färbung

A: Proteus, Providentia – B: Urease Test - / +
helios.bto.ed.ac.uk

Neugeborene Meningitis & Sepsis
E. coli K1(80–85%)
K1-AntigenIdentisch mit Meningococcus B-AgToleranz ⇒ kein Antikörper AntwortTranslokation

Pneumonie
• Nosokomial• Predisposition• Pathogene
E. coli,K. pneumoniae,K. oxytoca, Enterobacter spp. Bronchopneumonie Lobar pneumonie
(Friedländer)K. pneumoniae
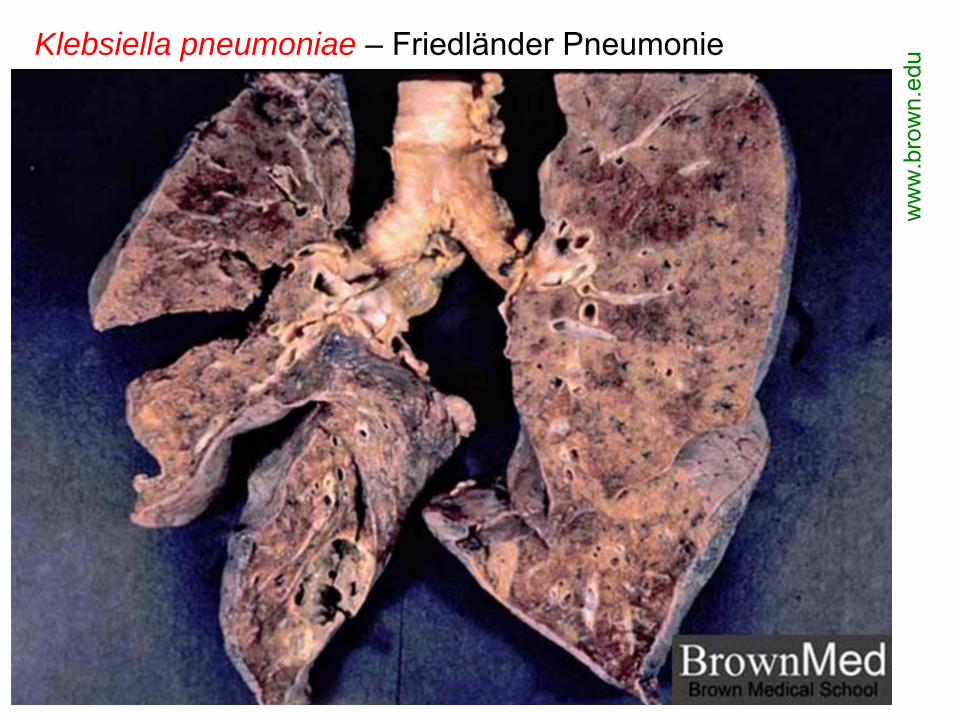
Klebsiella pneumoniae – Friedländer Pneumonie
ww
w.b
row
n.ed
u

www.icbm.de
Klebsiella pneumoniae
Mukoide Kolonien – Kapsel
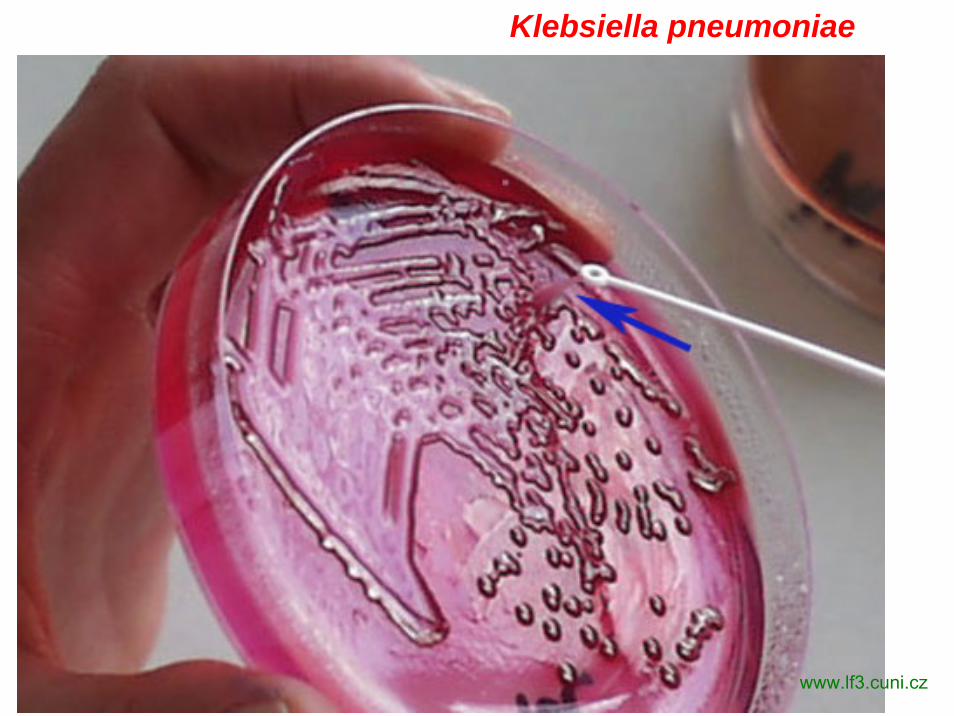
www.lf3.cuni.cz
Klebsiella pneumoniae

Klebsiella pneumoniae

Enterobacter cloacae Klebsiella pneumoniaeMukoide Kolonien
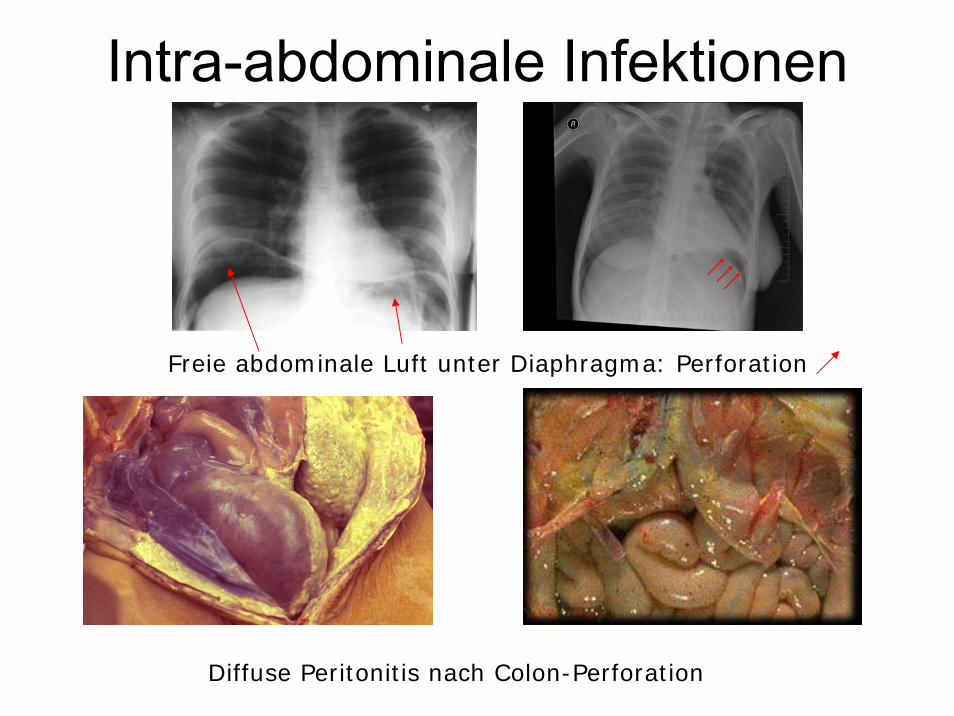
Intra-abdominale Infektionen
Freie abdominale Luft unter Diaphragma: Perforation
Diffuse Peritonitis nach Colon-Perforation

Enterobacteriaceae
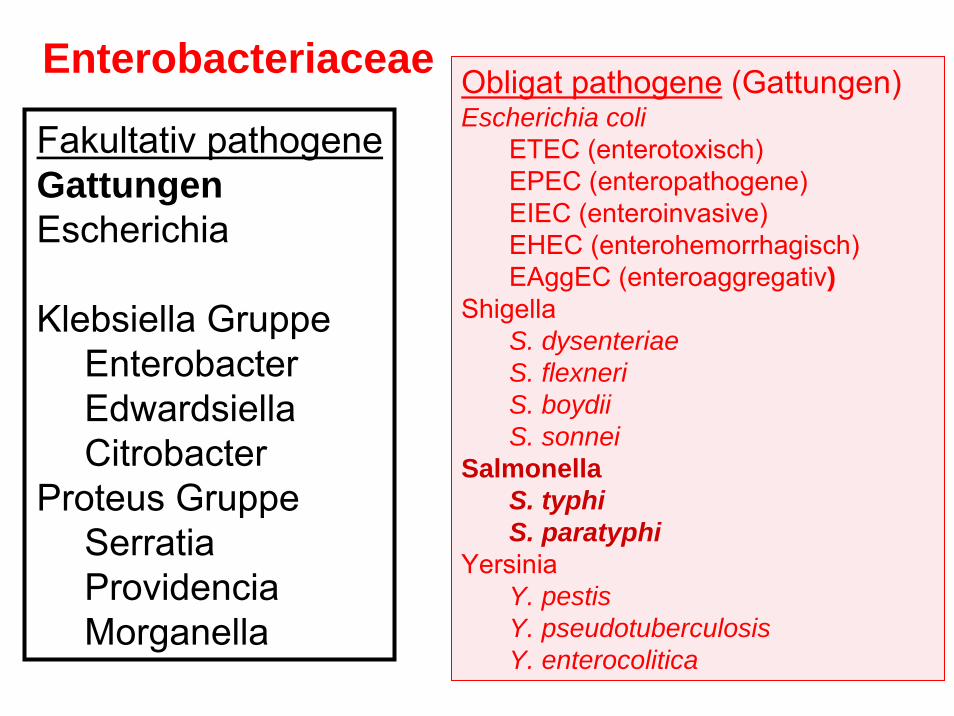
Fakultativ pathogeneGattungenEscherichia
Klebsiella GruppeEnterobacterEdwardsiellaCitrobacter
Proteus GruppeSerratiaProvidenciaMorganella
Obligat pathogene (Gattungen)Escherichia coli
ETEC (enterotoxisch)EPEC (enteropathogene)EIEC (enteroinvasive)EHEC (enterohemorrhagisch)EAggEC (enteroaggregativ)
ShigellaS. dysenteriaeS. flexneriS. boydiiS. sonnei
SalmonellaS. typhiS. paratyphi
YersiniaY. pestisY. pseudotuberculosisY. enterocolitica

FIGURE 25-1 Virulence mechanisms of E coli.
EIEC
ETEC
Medmicro
EAggEC

FIGURE 25-2 Pathogenesis of E. coli diarrheal disease.
Medmicro

Pathogene E. coli Stämme-1
ETEC (enterotoxisch)LT (hitzelabiles) ST (hitzestabiles)
ST Wirkung: ADP-Rybosilierung von GuanilcyklasecGMP Wasser- und Elektrolytverlust
Fimbrien (CFA = colonisation factor antigens)

FIGURE 25-3 Cellular pathogenesis of E coli having CFA pili.
Medmicro
ETEC

Fig.4.26 Enterotoxigenic E. coli infection. Transmission electron micrographshowing bacteria adhering to the brush-border of human intestinal mucosal cells. By courtesy of Dr. S. Knutton
ETEC

FIGURE 25-4 Laboratory methods for isolation andidentification of ETEC.
Medmicro

Fig. 4.14 Bacterial diarrhea. Y1 adrenal cell assay for E. coli LT enterotoxin, showing normal cells (left) and cells after exposure to LT toxin (right). Note disruption of monolayer and rounding up cells. By courtesy of Dr. H.L. DuPont.
ETEC
Pathogene E. coli Stämme-2-3EPEC (enteropathogen) O26; O55; O111; O126…
Adhäsion: Adhärenz Faktor (EAF)Bundle Forming Pilus (BFP)Über das Typ III. Sekretionssystem*: Proteinfilamente (EspA)Tir (translocated intimin receptor)Intimin (eae*) Aktinfasern; Podestbildung, Verlustdes Bürstensaums Zelltod* Chromosom kodiert, im Pathogenitätsinsel
EAggEC (enteroaggregativ)Fimbrien, ST-like, Haemolysin-like Toxin

Fig.4.19 E. coli diarrhea. Electronmicrograph of enteropathogenicE. coli (arrowed) attached tomucosal epithelialcells of ileum. The microvillus borderof the epithelialcells has beenlargely distroyedby bacteria andthe cells show signs of degeneration. X3000 Bycourtesy of Dr. J.R. Cantey
EPEC

Fig.4.27 Enteropathogenic E. coli infection. Electron micrograph showing close, localized adherence of bacteria to human intestinal mucosal cells and localizeddestruction of microvilli. By courtesy of Dr. S. Knutton
EPEC
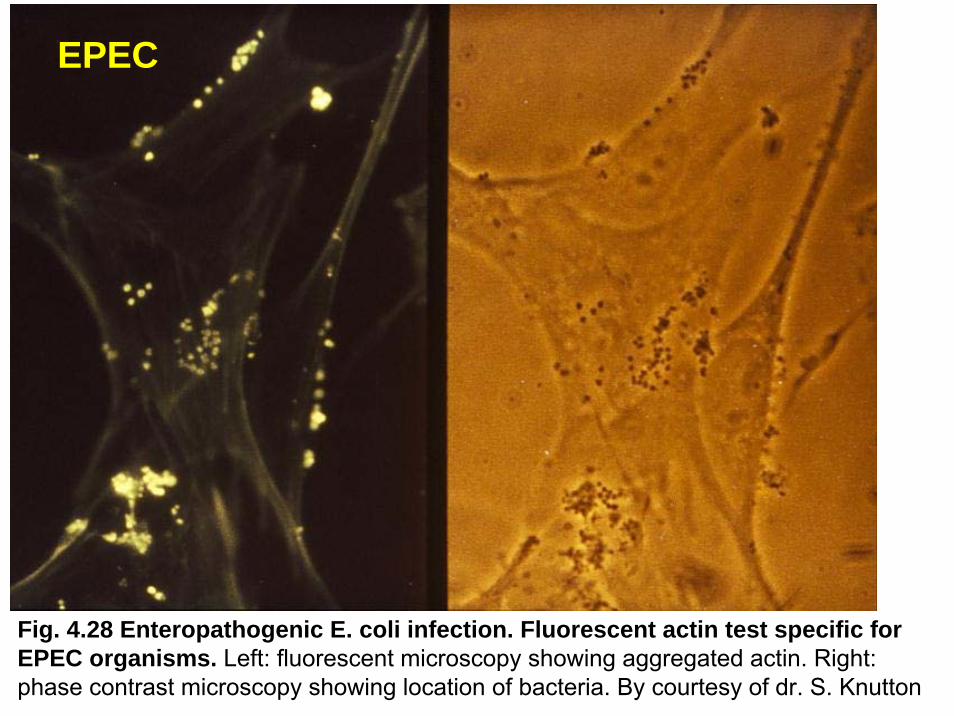
Fig. 4.28 Enteropathogenic E. coli infection. Fluorescent actin test specific forEPEC organisms. Left: fluorescent microscopy showing aggregated actin. Right: phase contrast microscopy showing location of bacteria. By courtesy of dr. S. Knutton
EPEC

Pathogene E. coli Stämme-4
EIEC (enteroinvasive)
O28; O32; O112; O115; O124, O136; O143, O144 u.a.
Pathogenese:s. Shigella ProteinenTyp III. Sekretionssystem

FIGURE 25-5 Cellular pathogenesis of invasive E coli
EIEC

Fig. 4.17 Enteroinvasive E. coli infection. Invasion of mucolsal layer of theintestine by E. coli organisms. There is necrosis of the mucosal layer at the siteof invasion (left). Transmission electron micrograph showing enteroinvasive E. coli organisms within HEp-2 cell (right). By courtesy of Dr. S. Knutton.
EIEC

Fig. 4.31 Enteroinvasive E. coli infection. EIEC organisms invadingHeLa cells in vitro. By courtesy of Dr. S. Knutton.
EIEC

Pathogene E. coli Stämme-5
EHEC (enterohemorrhagisch) = VTEC O157:H7
SLT = Verotoxin = Shiga Toxin (stx1, 2, 2c) Wirkung: hemmt Proteinsynthese zytotoxischHaemolysin
Krankheit:HUS (hämolytische uremisches Syndrom)
Hämolytische AnämieTrombozytopenieakute Niereninsuffizienz
Haemorrhagische Kolitis

Pathogene E. coli Stämme
Transmission electronmicrograph of Escherichia coli O157:H7
pathmicro.med.sc.edu
EHEC(enterohaemorrhagisch)= VTEC O157:H7

EHEC (enterohemorrhagisch) = VTEC O157:H7

Fig. 4.29 Enterohaemorrhagic E. coli infection. Assay for Shiga-like toxin (Verotoxin) produced by EHEC (Serotype O157). Left: Normal monolayer of Verocells. Right: Destruction of Vero cells by the toxin. By courtesy of Dr. S. Knutton
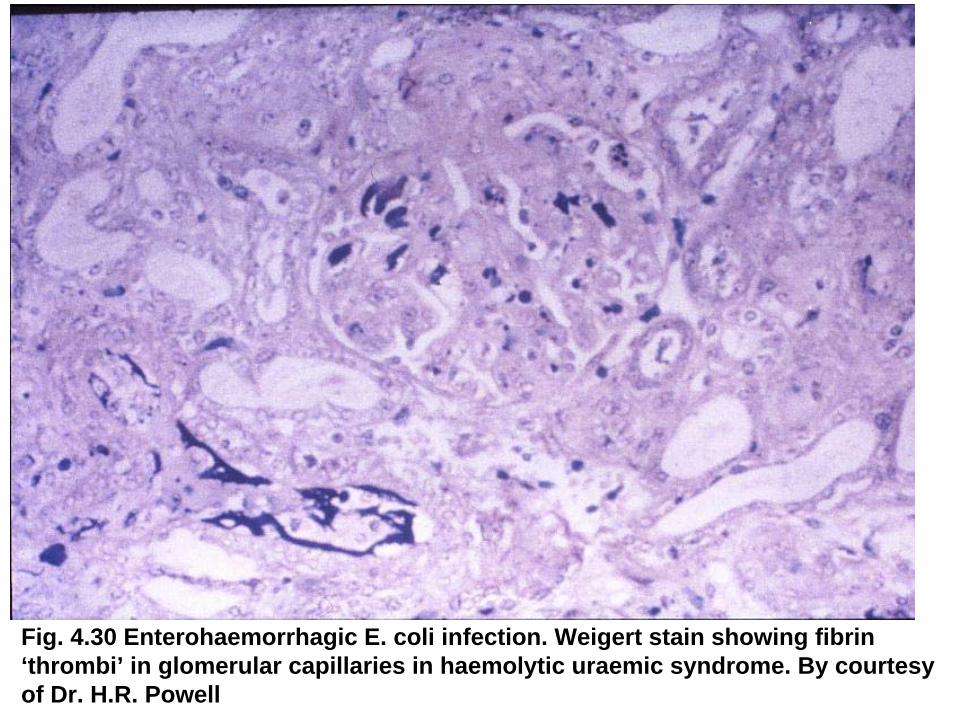
Fig. 4.30 Enterohaemorrhagic E. coli infection. Weigert stain showing fibrin ‘thrombi’ in glomerular capillaries in haemolytic uraemic syndrome. By courtesyof Dr. H.R. Powell
Pathogene E. coli Stämme
DiagnoseErregernachweisSerologische Typisierung
ProphylaxeExpositionsprophylaxe
BehandlungErsatz des WasserverlustesAntibiogram

Gramnegative fakultativanaerobe Stäbchen
Enterobacteriaceae II.
Dr. Bános ZsuzsaDr. Bános Zsuzsa04 04 -- 11 November 200811 November 2008

BAKTERIELLE DARMINFEKTIONENI. TypEnterotoxinHypersekretionDünndarm
wäßriger Durchfall
Vibrio choleraeEscherichia coli(ETEC)
II. TypInflammationInvasion in MucosaDickdarm
Eiter, Blut, Schleim im Stuhl
ShigellaE. coli (EIEC) (EPEC, EHEC)SalmonellaYersinia enterocoliticaCampylobacter jejuniAeromonas sp.Vibrio parahaemolyticus
Clostridium difficileClostridium perfringens
III. TypPenetration,GeneralisationErreger intrazellulärIleum
Typhus, Sepsis
Salmonella typhiS. paratyphi A, BYersinia enterocoliticaY. pseudotuberculosisCampylobacter fetus
Exogene, perorale Infektion, fäkal–orale Übertragungsweise
Enterobacteriaceae
Fakultativ pathogeneGattungenEscherichia
Klebsiella GruppeEnterobacterEdwardsiellaCitrobacter
Proteus GruppeSerratiaProvidenciaMorganella
Obligat pathogene (Gattungen)Escherichia coli
ETEC (enterotoxisch)EPEC (enteropathogene)EIEC (enteroinvasive)EHEC (enterohemorrhagisch)EAggEC (enteroaggregativ)
ShigellaS. dysenteriaeS. flexneriS. boydiiS. sonnei
SalmonellaS. typhiS. paratyphi
YersiniaY. pestisY. pseudotuberculosisY. enterocolitica

www.ltsa.frwww.about-salmonella.com
Salmonella sp.

Salmonella typhi, S. paratyphi A, B, C
Antigenstruktur von Salmonella typhigripsdb.dimdi.de
Menschenpathogene Arten
AntigeneOH (Geissel)Oberflächliches Vi Ag

Salmonella typhi, S. paratyphi A, B, C
PathogeneseInfektionsquelleKranke, Ausscheider; Kontaminierte Lebensmittel, TrinkwasserEintrittspforteMund Darm Blut Organen: Milz, Leber, Gallenwege, Knochenmark, Nieren, GehirnIleum: geschwüre (Blutungen, Perforation)
Krankheitsbilder:Typhus abdominalisParatyphus

Salmonella typhi, S. paratyphi A, B, C
Figure 2. Flagellar stain of a SalmonellaTyphi. Like E. coli, Salmonella are motileby means of peritrichous flagella. A closerelative that causes enteric infections is the bacterium Shigella. Shigella is notmotile, and therefore it can be differentiated from Salmonella on the baisof a motility test or a flagellar stain. (CDC)
Figure 1. Salmonella typhi, the agentof typhoid. Gram stain. (CDC)
www.textbookofbacteriology.net
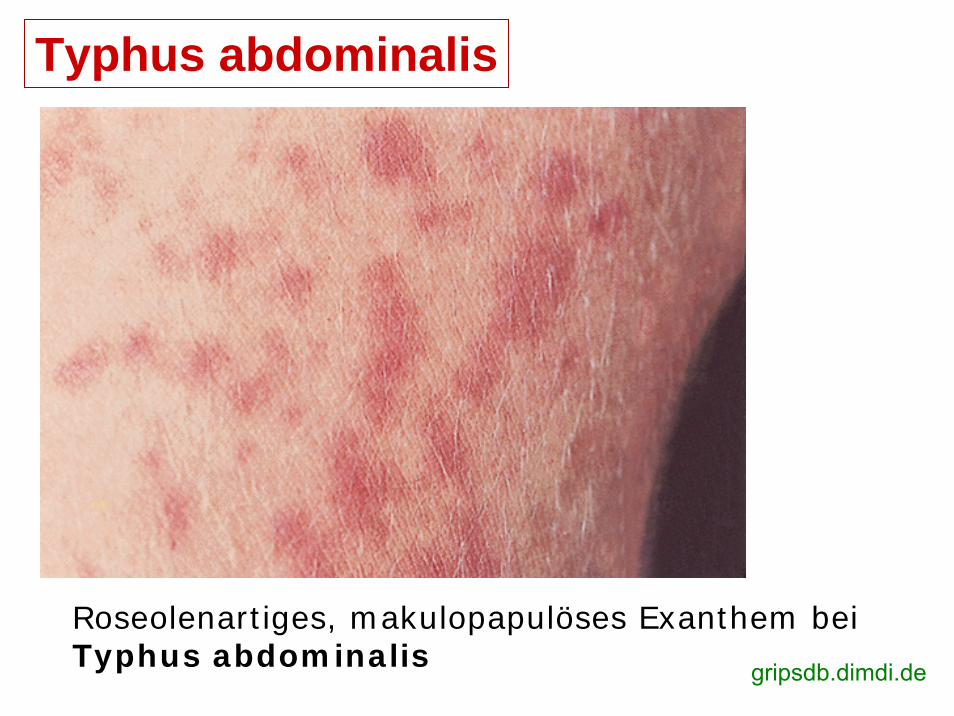
Typhus abdominalis
Roseolenartiges, makulopapulöses Exanthem beiTyphus abdominalis gripsdb.dimdi.de

www.wrongdiagnosis.comRose spots on abdomen of a patient with typhoid feverdue to the bacterium Salmonella typhi.

Rose spots on the chest of a patient with typhoid feverdue to the bacterium Salmonella typhi. www.wrongdiagnosis.com
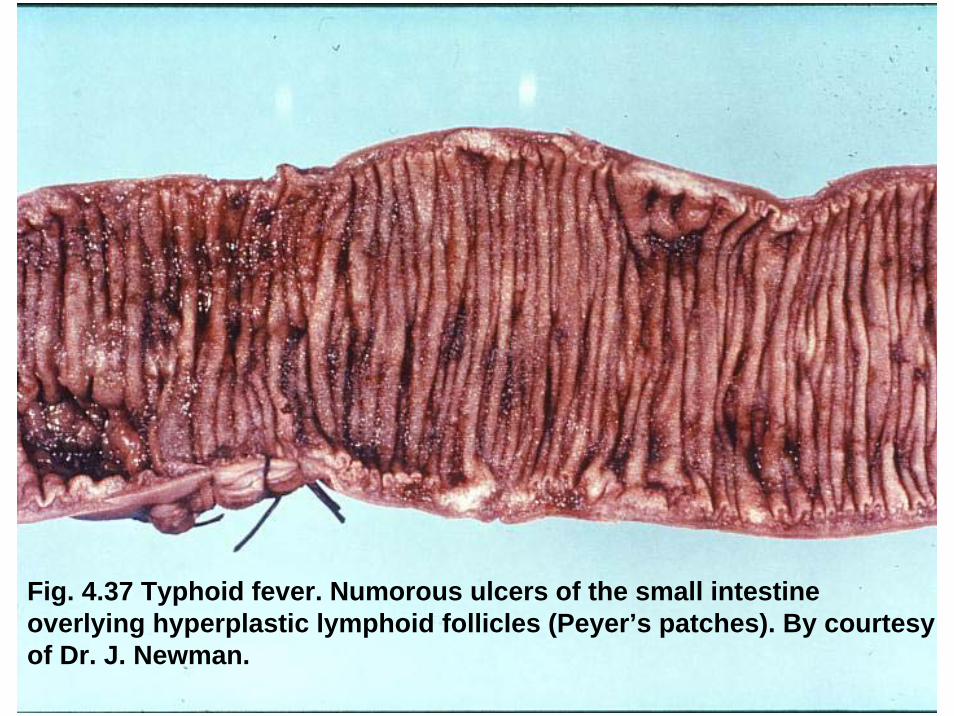
Fig. 4.37 Typhoid fever. Numorous ulcers of the small intestineoverlying hyperplastic lymphoid follicles (Peyer’s patches). By courtesyof Dr. J. Newman.

Fig. 4.39 Typhoid fever. Mononuclear cells and red blood cells in thestool. Trichrome stain. By courtesy of Dr. H.L. DuPont.
Typhus abdominalis
DiagnoseErregernachweis (Blut, Stuhl, Urine)SelektivmedienAntikörpernachweis (Agglutination)
ProphylaxeExpositionsprophylaxeImmunprophylaxe:1) Aktive orale Immunisierung mit
Ty21, einem apathogenen, abgeschwächten Stamm
2) Parenterale Impfung mit ViKapselpolysaccharidS. typhi-Stamm Typ-2
TherapieAmpicillinTrimethoprimChloramphenikol
Sanierung derDauerausscheider!
„Typhoid Mary”
www.spiceisle.com

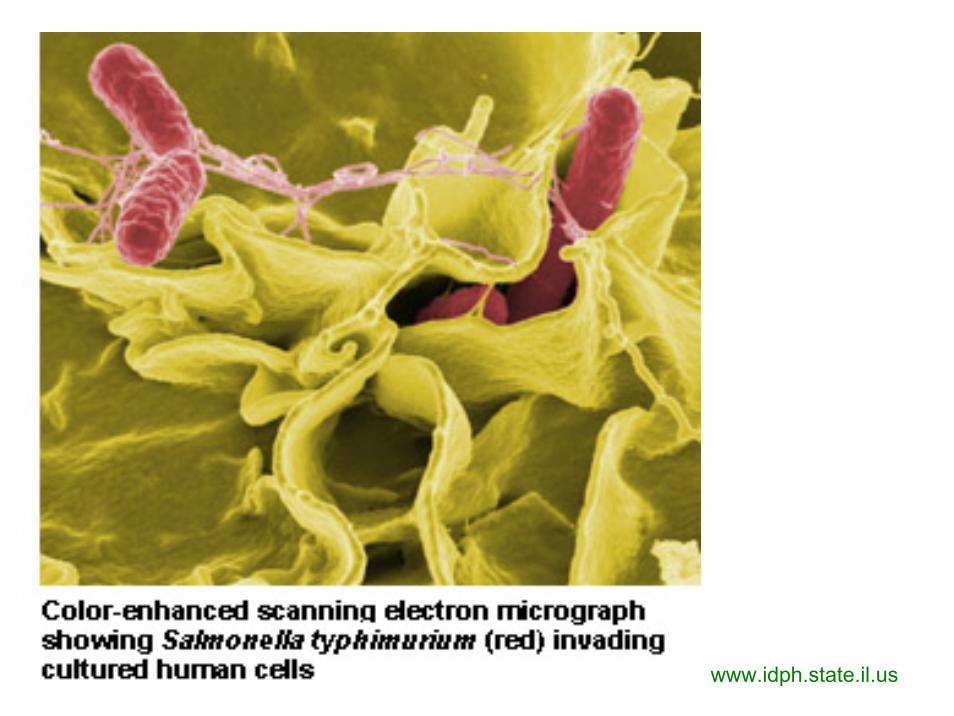
Salmonella - SalmonellosisUbiquitär S. typhimurium, S. enteritidis u.a
Pathogen für Geflügel, Eier, Schwein, Rind, Mäuse, Ratte und Menschen
PathogeneseInfektionsquelle: Infizierte tierische, kontaminierte LebensmittelBakterien vermehren sich im Lebensmittel Endotoxin wird frei
Krankheitsbild: (Gastro)Enteritis – Endotoxin WirkungKeimausscheidung ist kurz
Diagnose: Erregernachweis (Stuhl, Speiseresten)Prophylaxe: Lebensmittel und Küchenhygiene

Figure 21-3 Invasion of intestinal mucosa by Salmonella.
medmicro
www.idph.state.il.us


spacescience.comSalmonella sp.

www2.nphs.wales.nhs.uk
Salmonella enterica
www.textbookofbacteriology.net

Figure 3. Salmonella sp. after24 hours growth onXLD agar.
www.textbookofbacteriology.net

www.textbookofbacteriology.net
Figure 4. Colonial growth Salmonella choleraesuissubsp. arizonae bacteria grown on a blood agar culture plate. Also known as Salmonella Arizonae, itis a zoonotic bacterium that can infect humans, birds, reptiles, and other animals. (CDC)

www.chromagar.com
Rambach™ Agar For detection of Salmonella spp. •Salmonella - red•other bacteria - blue, violet, colourless, or inhibited.
wqc
.ariz
ona.
edu
Isolation of Salmonellafrom EnvironmentalSamples

pathmicro.med.sc.edu
TSI Medium Identifizierung

www.textbookofbacteriology.netSalmonella typhimurium HE agar

Enterobacteriaceae
Fakultativ pathogeneGattungenEscherichia
Klebsiella GruppeEnterobacterEdwardsiellaCitrobacter
Proteus GruppeSerratiaProvidenciaMorganella
Obligat pathogene (Gattungen)Escherichia coli
ETEC (enterotoxisch)EPEC (enteropathogene)EIEC (enteroinvasive)EHEC (enterohemorrhagisch)EAggEC (enteroaggregativ)
ShigellaS. dysenteriaeS. flexneriS. boydiiS. sonnei
SalmonellaS. typhiS. paratyphi
YersiniaY. pestisY. pseudotuberculosisY. enterocolitica

Shigella
S. dysenteriae* 10 SerotypS. flexneri* 6 SerotypS. boydii 15 SerotypS. sonnei
AntigeneO
* Toxinbilder
Shigella sonnei
Shigella
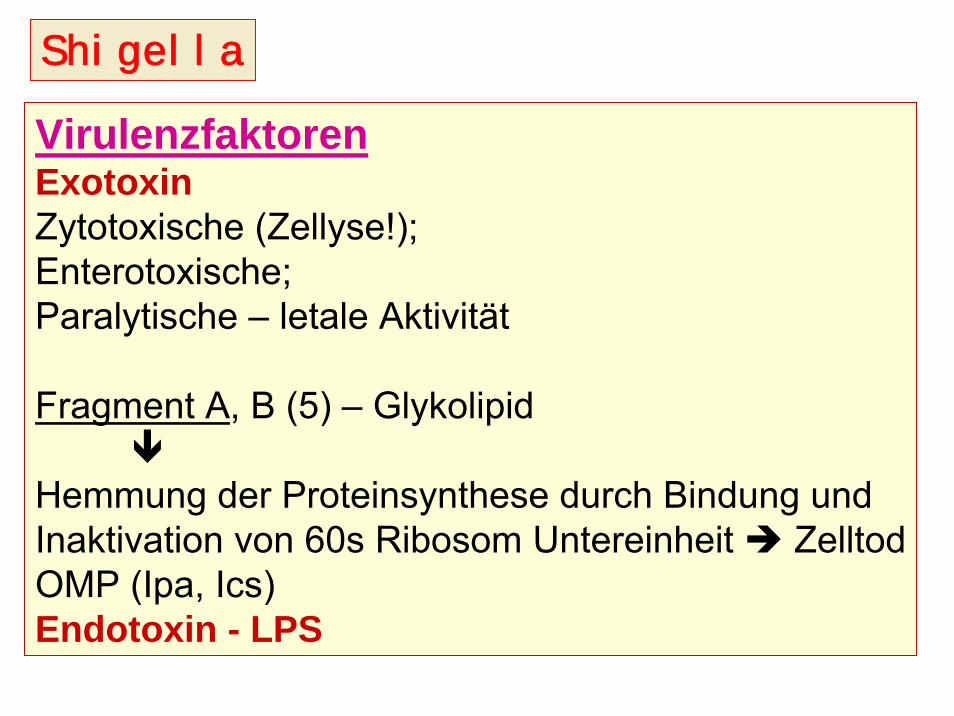
VirulenzfaktorenExotoxinZytotoxische (Zellyse!);Enterotoxische;Paralytische – letale Aktivität
Fragment A, B (5) – Glykolipid
Hemmung der Proteinsynthese durch Bindung und Inaktivation von 60s Ribosom Untereinheit ZelltodOMP (Ipa, Ics)Endotoxin - LPS

Pathogenität – ID50: 100-200 BakterienEindringen und Vermehrung in Epithelzellen:Invasion Plasmid Antigens – IpaIntercellular Spread – Ics
Pathogenese, KrankheitsbilderLokale InfektionEpithelnekrose, GeschwürbildungHemmung von AbsorptionHUS!
Shigella

Medmicro
Shigella
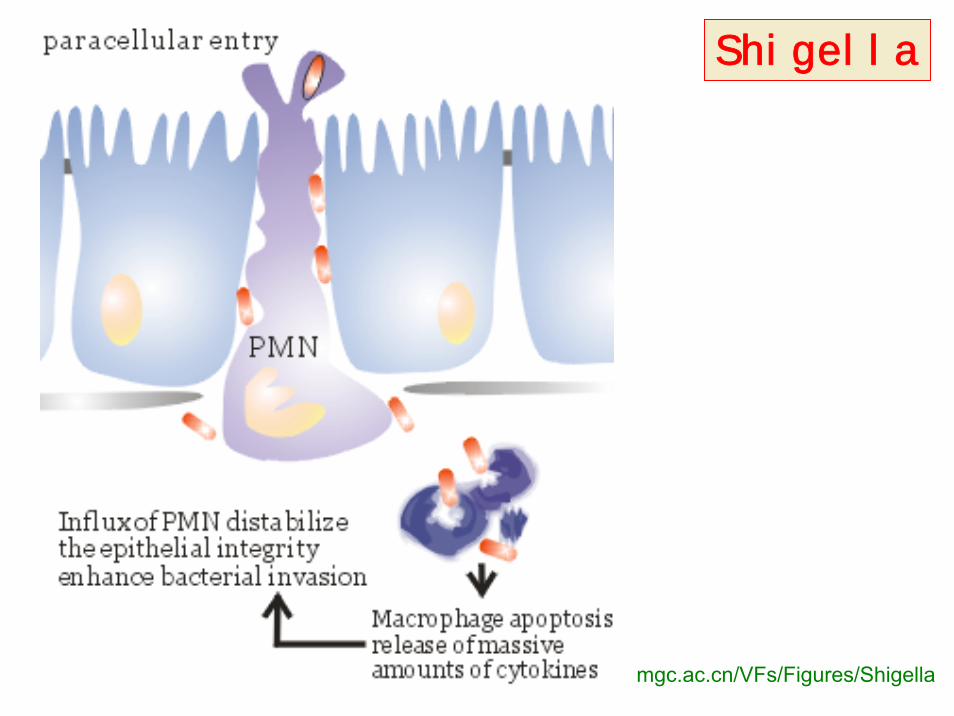
mgc.ac.cn/VFs/Figures/Shigella
Shigella

Fig. 2: Shigella Passing Through theMucous Membrane and …
… Invading MucosalEpithelial Cells
facu
lty.c
cbcm
d.ed
u

Fig. 4.33 Shigellosis. Sigmoidiscopic view of colonicmucosa in a mild case of infectiondue to S. flexneri. Note the thinwhitish exsudate, which is made upof fibrin and polymorphonuclearleucocytes. By courtesy of Dr. R.H. Gilman.
Fig. 4.34 Shigellosis. Sigmoidiscopic view of colonicmucosa in a fatal case of infection with S. dysenteriaetype 1 showing extensivepseudomembranous colitis. Bycourtesy of Dr. R.H. Gilmanand Dr. F. Koster.
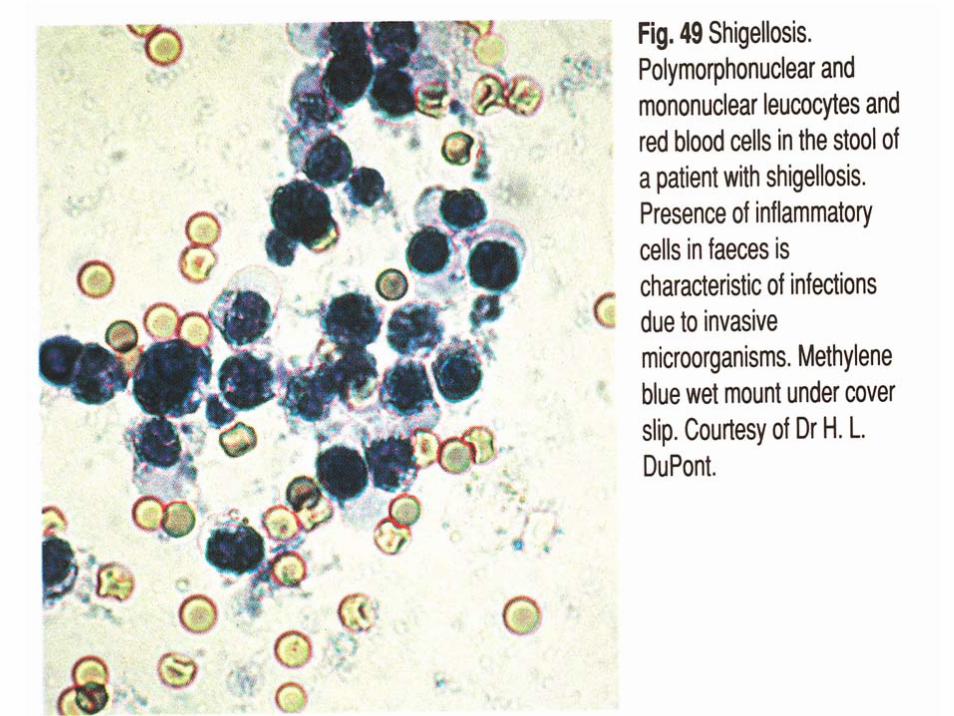

Fig. 4.18 Positive Serény test. Keratoconjunctivitis in the rabbit produced by the instillation of shigella microorganism. By courtesy of Dr. H.L. DuPont.

www.textbookofbacteriology.net
Shigella
DiagnoseErregernachweis(aus dem Stuhl)
Differenzierung –SelektivMedien
IdentifizierungSerotypisierung
pathmicro.med.sc.edu
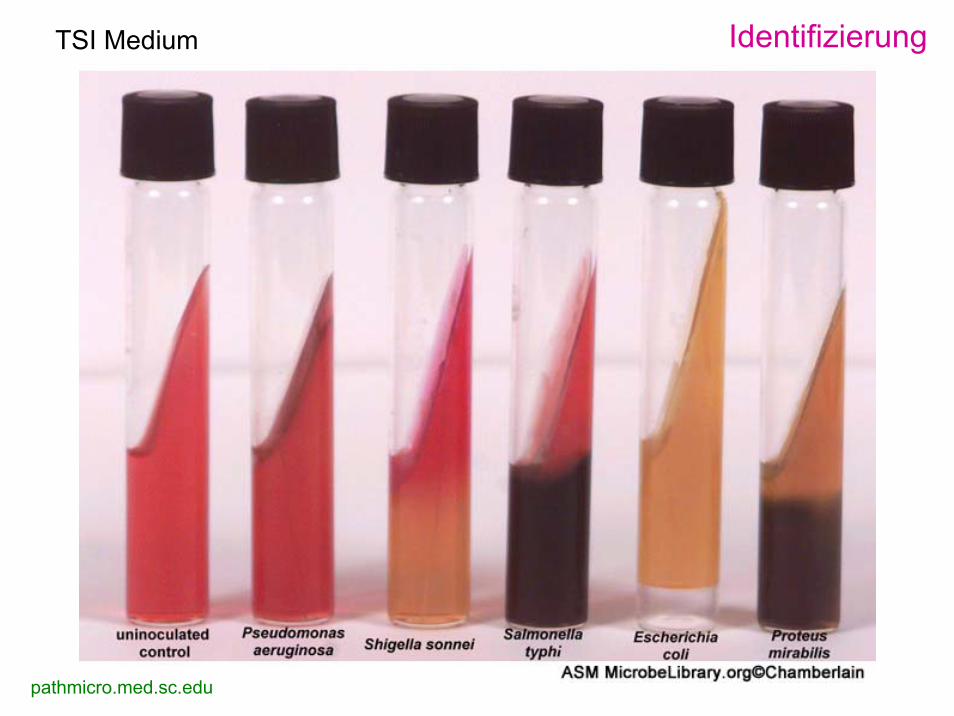
TSI Medium Identifizierung

Shigella boydii Kolonien auf Blutagar
www.biologie.de

Appearance of Colonies on Salmonella-Shigella Agar
ww
w.rc
i.rut
gers
.edu
A. Klebsiella pneumoniae B. Escherichia coliKlebsiella pneumoniae & Escherichia coli are positive for acid production fromfermentation of thecarbohydrate(s) present.
C: Salmonella sp.
D: Proteus mirabilis
Both Salmonella sp. & Proteus mirabilis producthydrogen sulfide. E: Pseudomona aeruginosa
The
Pse
udom
onas
colo
nies
are
near
lyco
lorle
ss.
Shigella
ProphylaxeExpositionsprophylaxe – Verbesserung der Hygiene
TherapieAntibiogramTetracylin, Ampicillin, Chloramphenicol, Sumetrolim

Enterobacteriaceae
Fakultativ pathogeneGattungenEscherichia
Klebsiella GruppeEnterobacterEdwardsiellaCitrobacter
Proteus GruppeSerratiaProvidenciaMorganella
Obligat pathogene (Gattungen)Escherichia coli
ETEC (enterotoxisch)EPEC (enteropathogene)EIEC (enteroinvasive)EHEC (enterohemorrhagisch)EAggEC (enteroaggregativ)
ShigellaS. dysenteriaeS. flexneriS. boydiiS. sonnei
SalmonellaS. typhiS. paratyphi
YersiniaY. pestisY. pseudotuberculosisY. enterocolitica
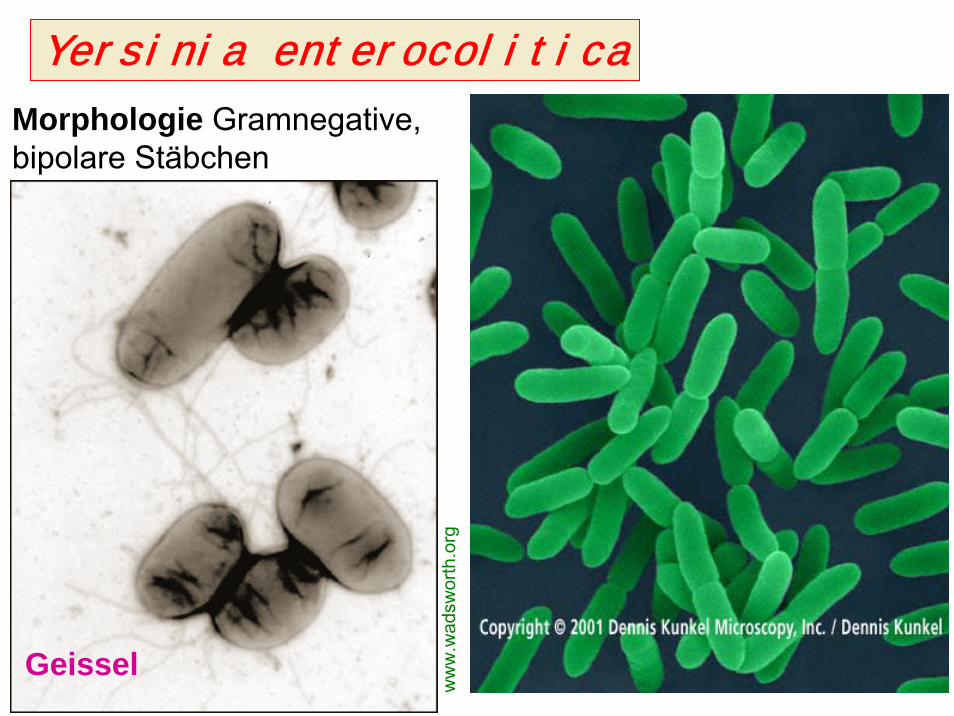
Yersinia enterocolitica
Morphologie Gramnegative,bipolare Stäbchen
Geissel
ww
w.w
adsw
orth
.org

Yersinia enterocolitica www.ktl.fi
KulturWachstumoptimum 28°C, Beweglich auch bei 28°C
Y. enterocoliticaO:5,27 CIN-ag
www.szu.czBlutagar
AntigeneO und H

Y. enterocoliticade.wikipedia.org

Figure 29-7 Pathogenesis of Y. enterocolitica.
KrankheitsbilderEnterocolitisLymphadenitis mesenterica
DiagnoseErregernachweisSerologieSerotypisierung
TherapieTetracyclinChloramphenicolSumetrolim
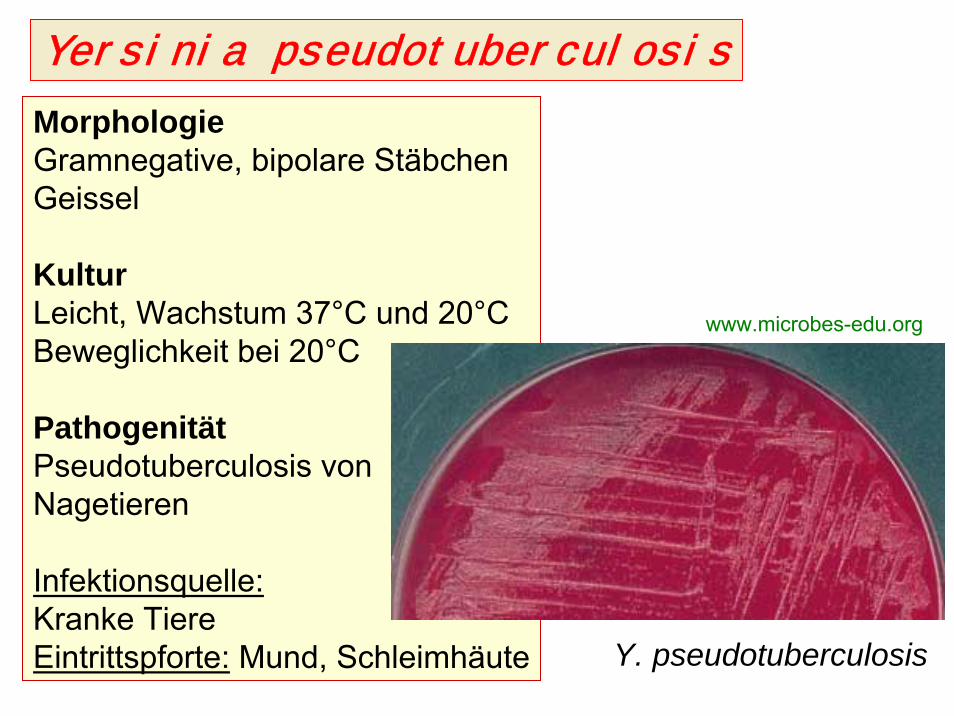
Yersinia pseudotuberculosis
MorphologieGramnegative, bipolare StäbchenGeissel
KulturLeicht, Wachstum 37°C und 20°CBeweglichkeit bei 20°C
PathogenitätPseudotuberculosis vonNagetieren
Infektionsquelle:Kranke TiereEintrittspforte: Mund, Schleimhäute Y. pseudotuberculosis
www.microbes-edu.org

Yersinia pseudotuberculosis
KrankheitsbilderLymphadenitis mesentericaSeptische-typhöse FormEnteritis
DiagnoseErregernachweisSerotypisierung – AgglutinationSerologie
TherapieTetracyclin

Fig. 4.50 Yersinia infection. Gross specimen of ileum, showing superficial necrosis of theintestinal musosa with several weel-defined deep and superficial ulcers.

www.llnl.gov
Y. pseudotuberculosis

Gramnegativefakultative anaerobe
Stäbchen
Vibrionaceae

GRAMNEGATIVE STÄBCHEN
AEROBBordetellaBrucellaFrancisella
PseudomonasAcinetobacterLegionella
FAKULTATIV ANAEROBHaemophilusPasteurella
Familie:EnterobacteriaceaeVibrionaceae
CardiobacteriumEikenellaKingellaActinobacillus
ANAEROBBacteroidesPrevotellaPorphyromonasFusobacterium
MIKROAEROPHILCampylobacterHelicobacter

BAKTERIELLE DARMINFEKTIONENI. TypEnterotoxinHypersekretionDünndarm
wäßriger Durchfall
Vibrio choleraeEscherichia coli(ETEC)
II. TypInflammationInvasion in MucosaDickdarm
Eiter, Blut, Schleim im Stuhl
ShigellaE. coli (EIEC) (EPEC, EHEC)SalmonellaYersinia enterocoliticaCampylobacter jejuniAeromonas sp.Vibrio parahaemolyticus
Clostridium difficileClostridium perfringens
III. TypPenetration,GeneralisationErreger intrazellulärIleum
Typhus, Sepsis
Salmonella typhiS. paratyphi A, BYersinia enterocoliticaY. pseudotuberculosisCampylobacter fetus
Exogene, perorale Infektion, fäkal–orale Übertragungsweise

Gramnegative fakultativ anaerobe Stäbchen(Positive Glucose fermentation)
Oxidase positive Oxidase negative
Vibrionaceae Aeromonadaceae
Vibrio Aeromonas
Enterobacteriaceae
EscherichiaKlebsiella
EnterobacterProteusSerratia
ProvidenciaMorganella
EdwardsiellaCitrobacter
Hafnia
SalmonellaShigellaYersinia
Facultativepathogenic
Obligatepathogenic
Plesiomonas
V. choleraeV. parahaemolyticusV. vulnificus
P. shigelloides A. hydrophila

VibrionaceaeSpecies Krankheiten
V. cholerae O1klassische & El Tor Cholera
V. cholerae O139 Cholera
V. parahaemolyticus Gastroenteritis
V. vulnificus Wundinfektion, Sepsis
Non-agglutinable(NAG) vibrios Gastroenteritis
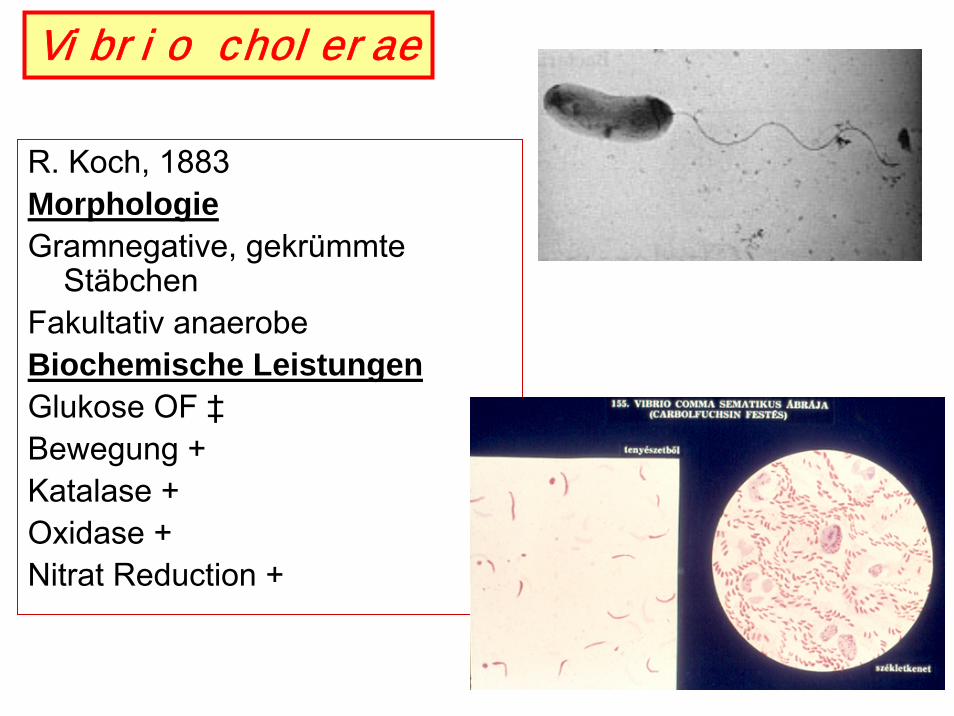
R. Koch, 1883MorphologieGramnegative, gekrümmte
StäbchenFakultativ anaerobeBiochemische LeistungenGlukose OF ‡Bewegung +Katalase +Oxidase +Nitrat Reduction +
Vibrio cholerae

bepast.org
V. cholerae

AntigenstrukturO (Zellwand) - 138O1 & O139H Geissel (gemeinsam)Fimbriae: A, B, CO1: Bio und Serotypen
V. cholerae

Vibrio cholerae. Leifson flagella stain (digitally colorized). CDC/Dr. William A. Clark
pathmicro.med.sc.edu
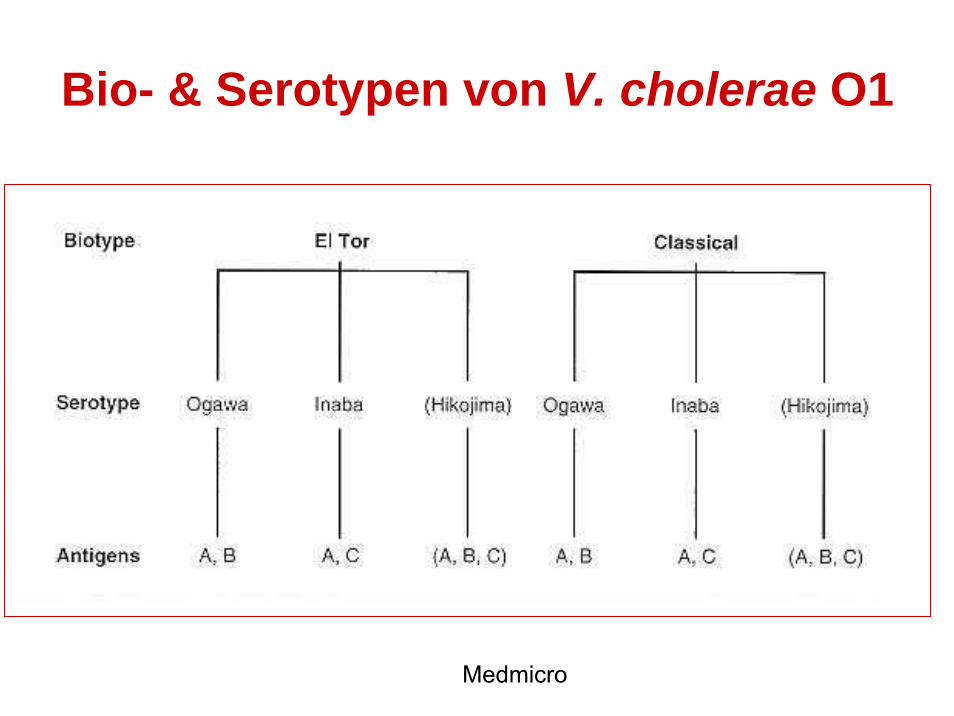
Bio- & Serotypen von V. cholerae O1
Medmicro

Virulenzfaktoren
Virulenzfaktor Biologische Effekt
Choleratoxin (Enterotoxin) Hypersekretion von Wasser und Elektrolyten
Fimbrien Adhäsion – Mucus Membran
Accessory colonisation factor(ACF) Adhäsion – Mucus Membran
Haemagglutination Protease(Mucinase) Schleim Hydrolyse
Neuraminidase Überregulation von Toxin-Rezeptor
V. cholerae
Pathogenese – Obligat MenschenpathogenInfektionsquelle: 1. Kranke Menschen und Ausscheider(Inkubations-, Dauerausscheider und Rekonvalenscente– durch Stuhl! – Fliege!)2. Kontaminierte Lebensmittel (Seespeise!) und TrinkwasserReservoir: Algen, Muscheln, PlaktonÜbertragung: Perorale InfektionEintrittspforte: Magen-Darmtrakt
Toxinbildung in DünndarmKeine Ausbreitung!Krankheit: Kolera – durch Choleratoxin
Immunität: lokal IgA (IgG im Blut)

Adhäsion von V. cholerae

Medmicro ch 24
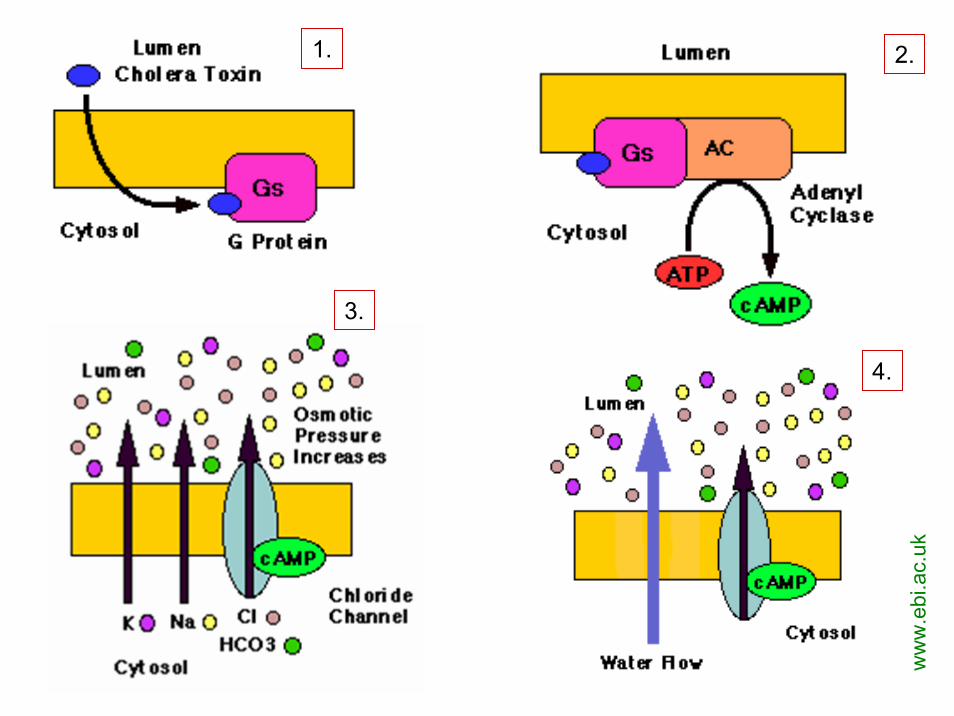
FIGURE 24-1 Pathophysiology of cholera.
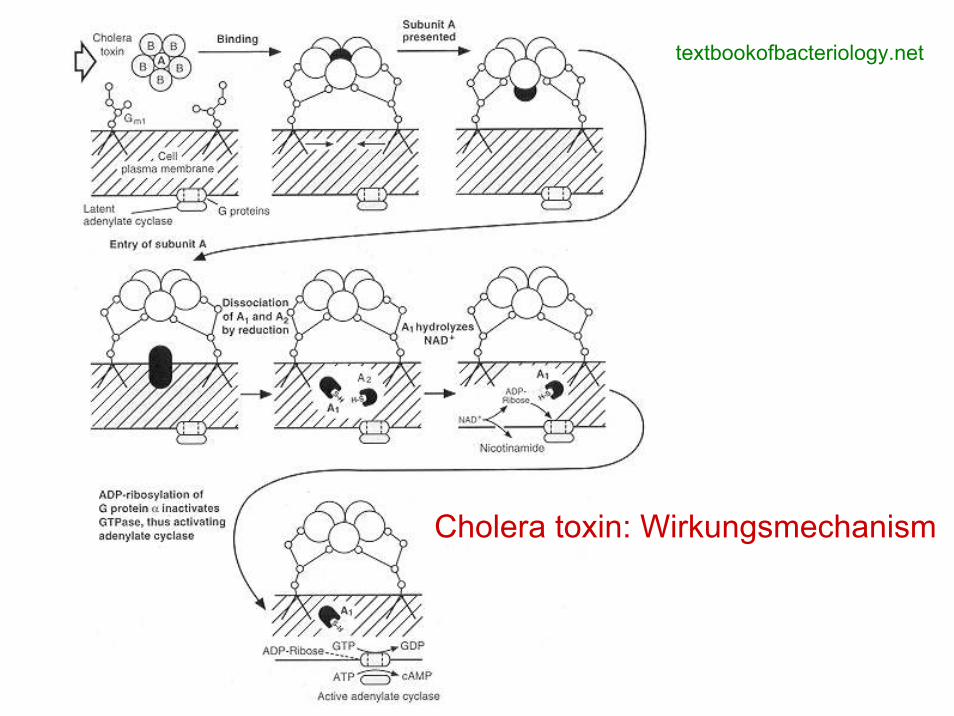
textbookofbacteriology.net
Cholera toxin: Wirkungsmechanism
ww
w.e
bi.a
c.uk
1. 2.
3.
4.

Cholera Toxin und Pertussis Toxin

Cholera Pandemien• Indien, Mündung von Ganges• Interkontinentale Reisen, Handelsverkehr, Kriege⇒ 7 Pandemien ab 1817
• Jetzt: 7. Pandemie, V. EL Tor– 1961: Asien– 70’s–80’s: Afrika, Europa, Oceania– 1991: Süd-Amerika
• 1992 : V. cholerae O139 „Bengal”– Schnelle Ausbreitung (Asien, Europa, USA)– Keine Kreuzimmunität mit O1-Stämme– 8. Pandemie?

7. Cholera Pandemie 1961

Cholera Erkrankungen, WHO: 2000–2001

Cholera Ausbruch
Cholera camp in Mozambique
Cholera clinic in Mozambique

Cholera: Klinik• Wässrige Durchfall
(25 L/day)• Dehydration• Haemokoncentration• Blut pH • Serum K+ , Na+
• Serum Glucose ↑• Shock• Letalität
– Unbehandelte• Klassisch: 60%• El Tor: 15–30%
– Behandelte: 1%
Rice-water diarrhoea ; Reiswasser Stühle
Vor und nachRehydration
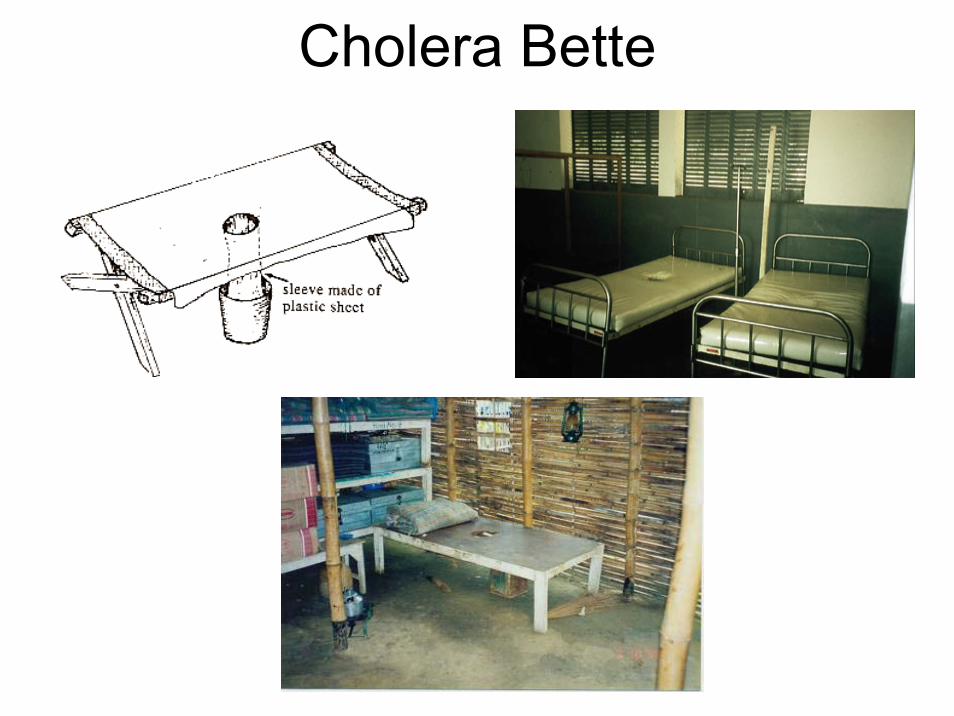
Cholera Bette
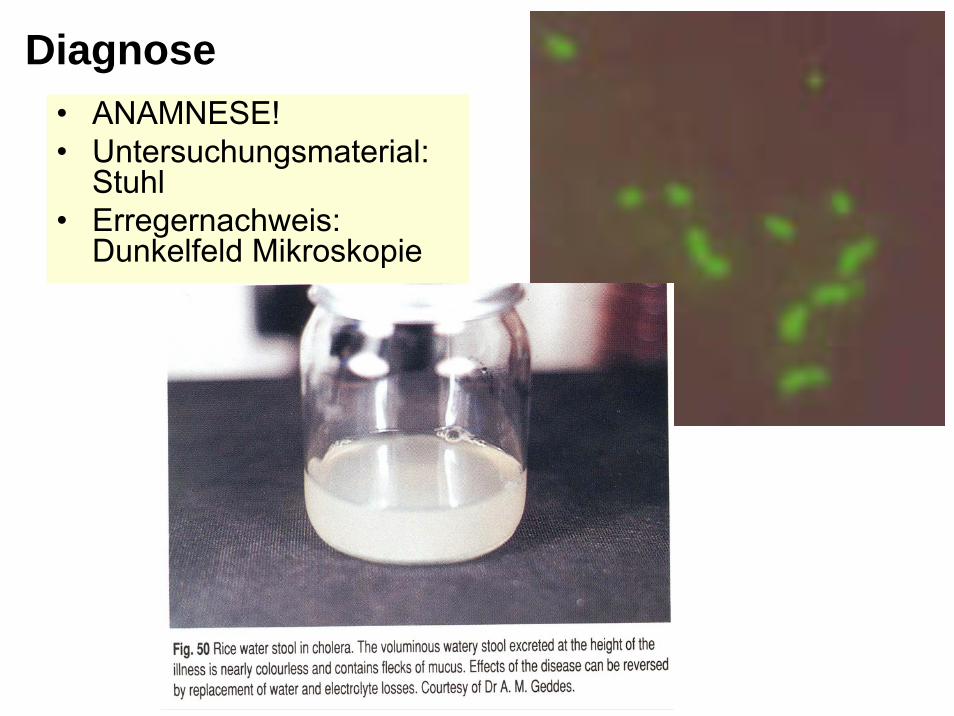
• ANAMNESE!• Untersuchungsmaterial:
Stuhl• Erregernachweis:
Dunkelfeld Mikroskopie
Diagnose

Transport: Alkalische PeptonwasserKultur: TCBS Nährmedium
Diagnose

IdentifizierungBiochemische Reaktionen
Serotypisierung (O1, O139)
Antibiogram
Diagnose
V. cholerae
Prophylaxe von Kolera
ExpositionsprophylaxeVerbesserung der Trinkwasser– und Lebensmittelhygiene und der AbwasserbeseitigungMassenerziehung von hygienischen MassnahmenIsolierung; QuarantäneAusheilung, DesinfektionAbkochen des WassersKontrolle der AusscheiderWHO Meldepfilcht

• ImmunprophylaxeVaccination
– Schutzimpfung (nur gegen O1)• Inaktivierte Bakterien, parenterale• Inaktivierte Bakterien + B-subunit Toxoid per os• Genmanipulierte, attenuierte V. cholerae per os
– Immunität dauert 3–6 Monate, Effektivität 50–60%
– Reisende– WHO: falsches Sicherheitsgefühl (!)
Massenerziehung von hygienischenMassnahmen

Therapie von Cholera
Salt-sticks
Coke

Therapie von Cholera
• Ersatz von Wasser und Elektrolyte– Intravenös– Per os Oral Rehydration Fluid
ORF• Glucose 20g/l• NaHCO3: 2,5 g/l• NaCl: 3,5 g/l• KCl: 1,5 g/l
• Antibiotika– Ciprofloxacin– Doxycycline
Peru
Bangladesh

Vibrio parahaemolyticus
www.city.niigata.niigata.jp
www.fehd.gov.hk
Gastroenteritis

Fig. 10.20 Cellulitis. Severe infection with bullous lesions due to V. vulnificus infection following immersion of leg in brackish water.
V. vulnificus

V. vulnificus
Fig. 10.21 Vibrio cellulitis. Haemorrhagic, bullous lesions of V. vulnificus sepsis. Bycourtesy of Dr. J.R. Cantey

A. hydrophila P. shigelloides
Cellulitis Myonecrosis
A. hydrophila infection in fish
Gastroenteritis
Sea food
Natural water sources
web.umr.edu

Aeromonas hydrophila
www.buddycom.com

www.buddycom.comweb.umr.edu
Aeromonas hydrophila
Plesiomonas shigelloideshttp://www.vetmed.wisc.edu

Aeromonas hydrophila

Aeromonas hydrophila
I.Gramnegative spiralförmige
und gekrümmte Stäbchen
Gramnegative anaerobeStäbchen
Dr. Bános ZsuzsaDr. Bános Zsuzsa04 04 -- 11 November 200811 November 2008

1. Microaerophile –Campylobacter und
Helicobacter

BAKTERIELLE DARMINFEKTIONENI. TypEnterotoxinHypersekretionDünndarm
wäßriger Durchfall
Vibrio choleraeEscherichia coli(ETEC)
II. TypInflammationInvasion in MucosaDickdarm
Eiter, Blut, Schleim im Stuhl
ShigellaE. coli (EIEC) (EPEC, EHEC)SalmonellaYersinia enterocoliticaCampylobacter jejuniAeromonas sp.Vibrio parahaemolyticus
Clostridium difficileClostridium perfringens
III. TypPenetration,GeneralisationErreger intrazellulärIleum
Typhus, Sepsis
Salmonella typhiS. paratyphi A, BYersinia enterocoliticaY. pseudotuberculosisCampylobacter fetus
Exogene, perorale Infektion, fäkal–orale Übertragungsweise

Spiral formed & curvedGram-negative bacteria
Spirillaceae
Campylobacter Helicobacter Spirillum
C. jejuni H. pylori S. minus

Wichtigste Arten von Campylobacter
Species Reservoir Krankheit Häufigkeit
C. jejuniGeflügel, Schwein, Rind, Hase
Gastroenteritis, Sepsis, Meningitis, Guillan-Barré
Häufig
C. coliGeflügel, Schwein, Rind, Schaf
Sepsis, Gastroenteritis, Meningitis
Selten
C. fetus Rind, SchafSepsis, Gastroenteritis, Meningitis
Selten
C. lariGeflügel, Schwein, Katze, Affe, Pferd
Gastroenteritis, Sepsis Selten
C. upsalensis Hund, Katze Gastroenteritis, Sepsis, Abszess ?

Campylobacter
MorphologieGramnegativegekrümmte Stäbchen(0,3–0,6 μm)
Campylobacter
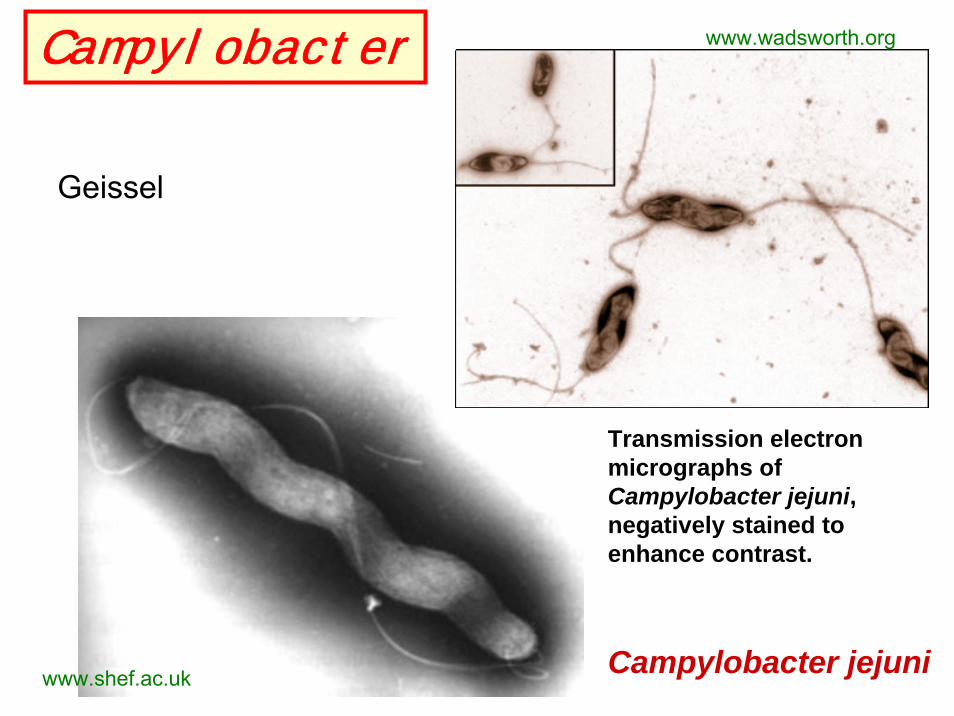
Geissel
Transmission electronmicrographs of Campylobacter jejuni, negatively stained toenhance contrast.
www.wadsworth.org
www.shef.ac.uk Campylobacter jejuni

www.indigo.com
Campylobacter jejuni

KulturMicroaerophil
5–7% O25–10% CO2Thermophil: 42ºC
Campylobacter
Campy-blood-agarmedinfo.ufl.edu
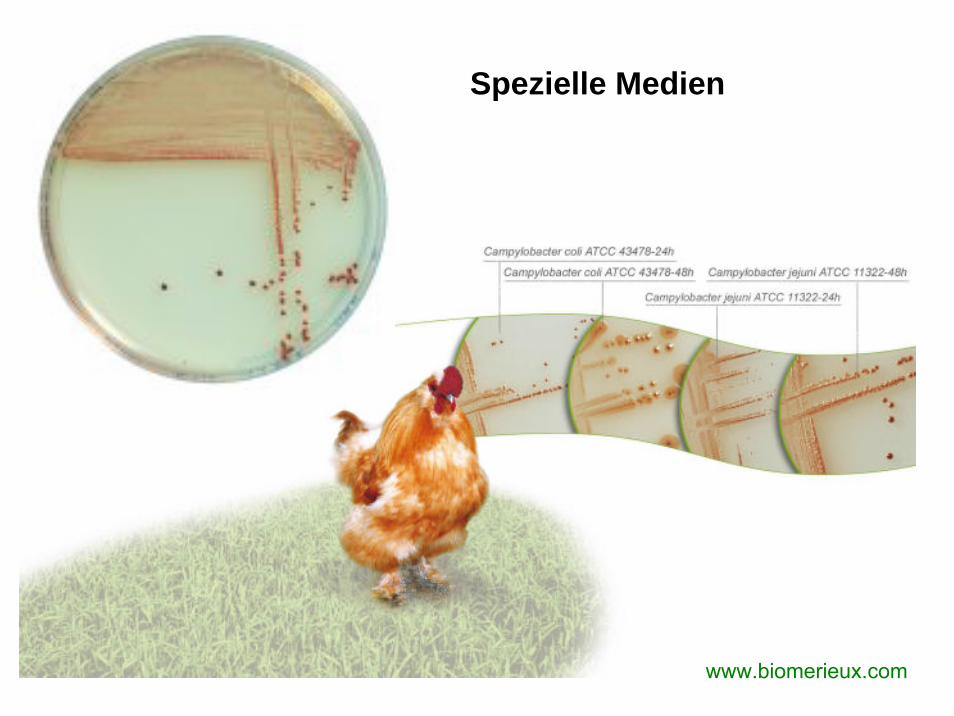
www.biomerieux.com
Spezielle Medien
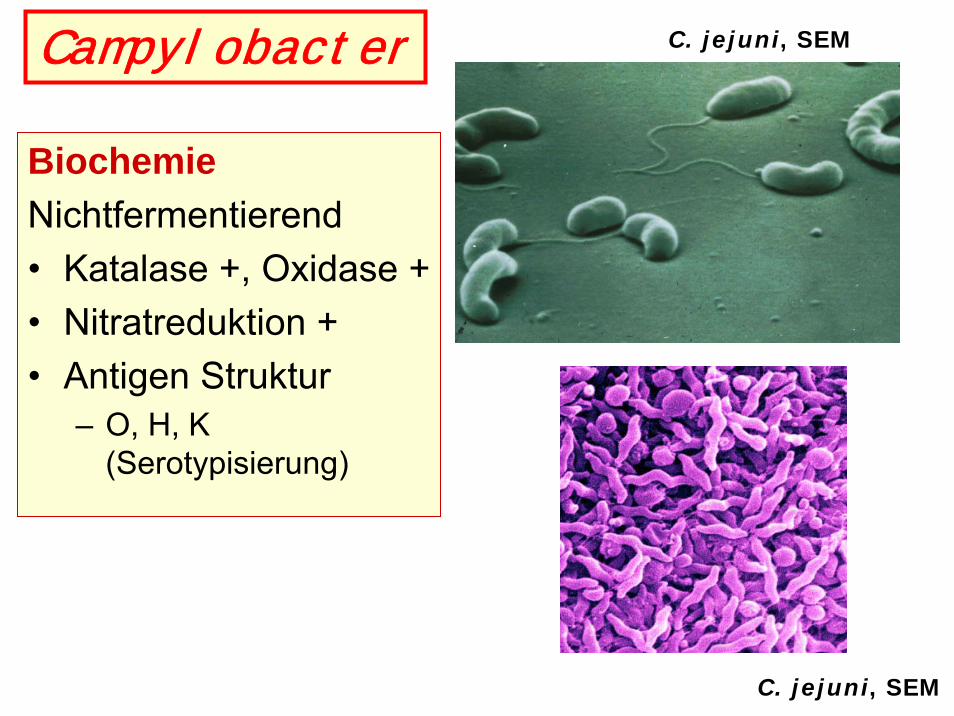
Campylobacter C. jejuni, SEM
C. jejuni, SEM
BiochemieNichtfermentierend• Katalase +, Oxidase +• Nitratreduktion +• Antigen Struktur
– O, H, K(Serotypisierung)

Virulenzfaktoren• Geissel ⇒ Bewegung• Adhäsion Faktoren• Invasion Faktoren (?)• Zytotoxin• C. fetus: S-Proteinhülle ⇒ Hemmung von C3b Bindung
⇒ Antiphagozytose• LPS
Komplikation:• Guillan-Barré SyndromStrukturähnlichkeit: Kernoligosaccharide des LPS mit
Gangliosiden im Nervensystem (GM1, GM2) ⇒Antikörper gegen GM1 ⇒ Autoimmunprozess ⇒Demyelinisierung
Campylobacter

C. coli & Guillan-Barré syndrome

Epidemiologie
• Zoonose!• Infektionsquelle:
Kontaminierte Lebensmittel & Wasser
• Mensch zu Mensch: Fäkal-oral Übertragung (Kinder). Selten
• ID: 500• Häufig in tropischen,
subtropischen Ländern (80%)
Campylobacteriosis: Klinik• Inkubation: 1–2 Tage• Blutige Durchfälle• Fieber• Abdominale Schmerzen,
Krämpfe• Spontan Ausheilung:
1–7 Tage• Komplikationen
– Protahierte Verlauf– Systemische Infektion– Reaktiv Arthritis– Guillan-Barré Syndrome
(Polyneuropathie)

Diagnose von Campylobacter Infektionen
• Untersuchungsmaterial– Stuhl– Blutkultur, Liquor– Lebensmittel
• Kultur(Mikroaerophil!, Thermophil!)
• Identifizierung• Antibiogram
Campylo-agarculture
Biochemical identification

Therapie & Prevention von Campylobacter Infektionen
• Wasser und Elektrolytsubstitution• Antibiotika
– Gastroenteritis• Erythromycin, Doxycycline, Ciprofloxacin,
Amoxicillin/Klavulansäure– Systemische Infektionen
• Carbapenem, Aminoglycoside, Chloramphenicol
• Prevention: Lebensmittelhygiene
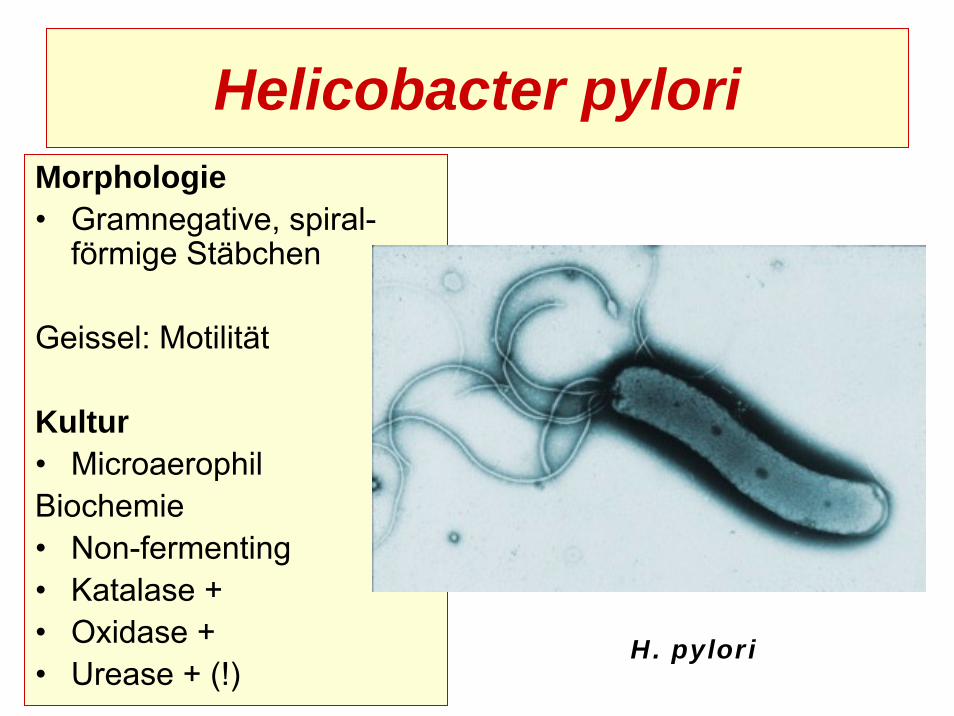
Helicobacter pyloriMorphologie• Gramnegative, spiral-
förmige Stäbchen
Geissel: Motilität
Kultur• MicroaerophilBiochemie• Non-fermenting• Katalase +• Oxidase +• Urease + (!)
H. pylori

Virulenzfaktoren von H. pylori• Adhäsine (HOP)• Flagella (Motilität)
• Urease Aktivität• Vacuolisierendes Zytotoxin• Protein CagA
Translokation durchTyp IV. SekretionssystemVeränderung von ZytoskeletIl-8, Il-1, TNFα Stimulation
Urease positiv
Cytotoxic effect in HeLa cells

Epidemiologie und Klinik vonH. pylori Infektionen
Epidemiologie• Weltweit verbreitet• Reservoir: Mensch• Übertragung
– Fäkal-oral– Oro-oral (Speichel)– Endoskop!
KlinikAkut GastritisChronisch-aktive GastritisGastroduodenale UlcuskrankheitTumorbildung
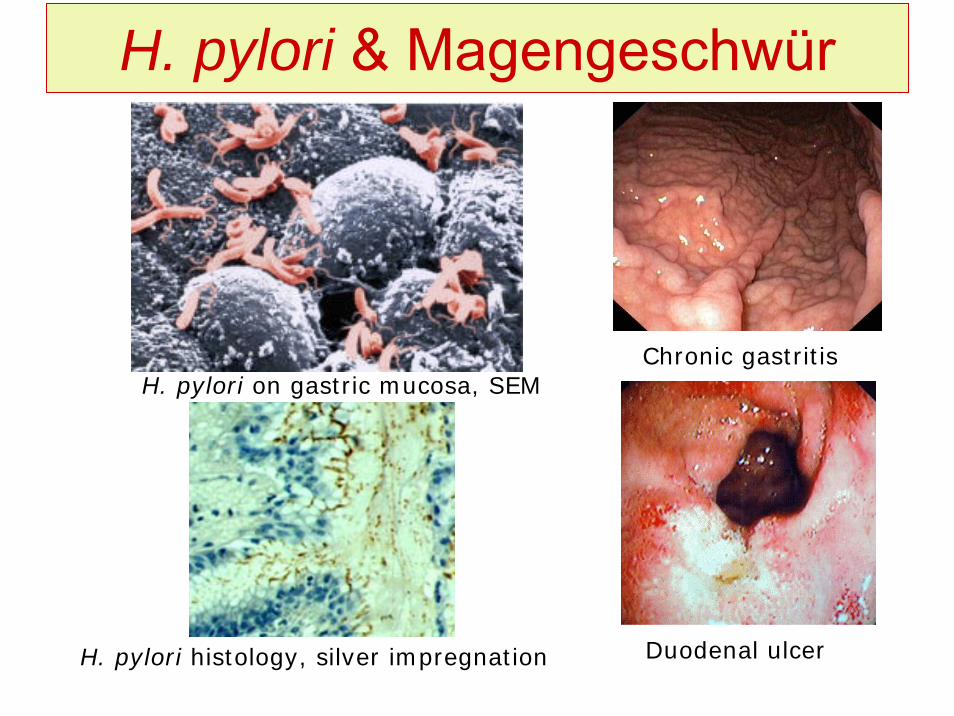
H. pylori & Magengeschwür
Chronic gastritis
Duodenal ulcer
H. pylori on gastric mucosa, SEM
H. pylori histology, silver impregnation

H. pylori & Tumorbildung
Antral adenocarcinomagastroscopic finding
Gastric adenocarcinoma withliver metastasis & ascites

Diagnose von H. pylori
• Nachweis von Helicobacter Antigen im Stuhl• Magenbiopsie: Histopathologischer, kultureller, molekulargenetischer Nachweis• Radioaktiv Urea Atemtest (Urease Nachweis)• Antikörper Nachweis

Radioaktiv Urea Atemtest
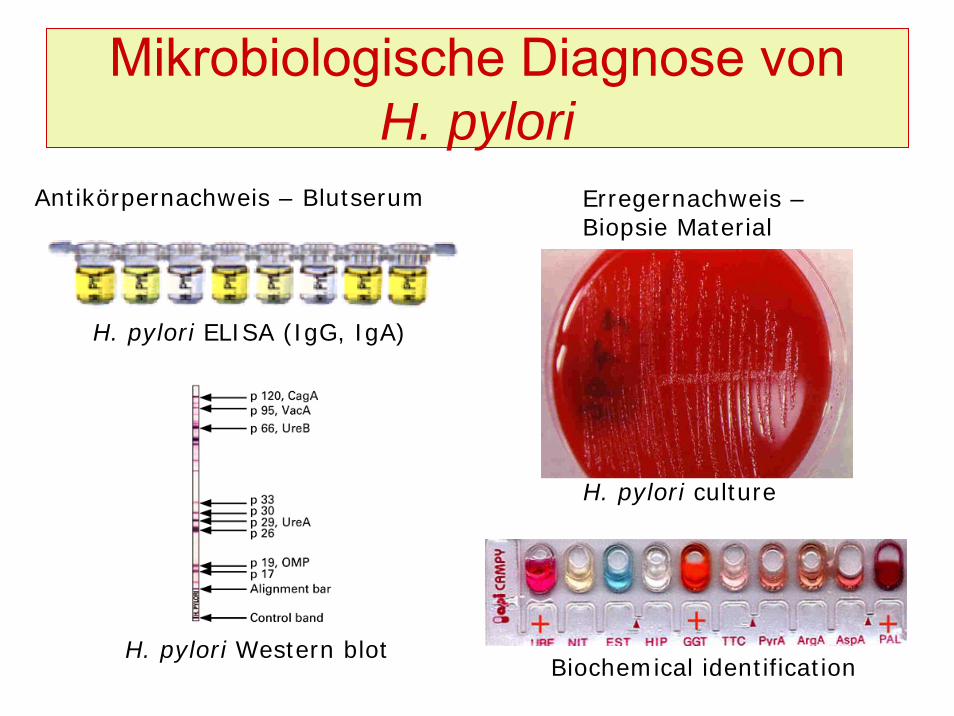
Mikrobiologische Diagnose von H. pylori
H. pylori culture
Biochemical identification
H. pylori ELISA (IgG, IgA)
H. pylori Western blot
Erregernachweis –Biopsie Material
Antikörpernachweis – Blutserum

H. pylori Eradikation
• Kombinations - Therapie mit– Protonenpumpenhemmer– Antibiotika
• Clarithromycin + Metronidazole• Amoxicillin + Metronidazole• Doxycycline + Metronidazole
– Eradikation: 90% der Fälle

ENDE
Zakynthos, 2004