Embed Size (px)
Citation preview

Schweres Asthma & Typ-2-Inflammation
Prof. Dr. Marek Lommatzsch
Abt. Pneumologie, Uniklinik Rostock
27. Juli 2021

Interessenskonflikte
Forschungsunterstützung:
DFG, GSK, Astra Zeneca
Vortrags- und Beratertätigkeit:
ALK, Allergopharma, Astra Zeneca, Bencard,
Berlin-Chemie, Boehringer-Ingelheim, Bosch, Chiesi,
Circassia, GSK, HAL Allergy, Janssen-Cilag, Leti, MSD,
Mundipharma, Novartis, Nycomed/Takeda, Sanofi, TEVA, UCB

Bisherige Definition schweres Asthma (ERS/ATS 2014)
Unter der Therapie mit:- Hochdosis-ICS + mind. 1 zusätzl. Controller (LABA / LTRA /Theophyllin)
oder
- Oralen Glucocorticoiden > 6 Monate / Jahr
trifft mindestens einer der folgenden Punkte zubzw. würde bei Weglassen der Therapie zutreffen:
• ACT < 20 oder ACQ > 1,5
• Mindestens 2 Exazerbationen in den letzten 12 Monaten
• Mindestens 1 Exazerbation mit Krankenhausbehandlung
• oder Beatmungsnotwendigkeit in den letzten 12 Monaten
• FEV1 < 80% (bei FEV1/FVC unterhalb der Altersnorm)
Lommatzsch & Virchow, Dtsch Ärzteblatt 2014

https://ginasthma.org/severeasthma
„Schweres“
AsthmaSchwieriges
AsthmaJa
Mangelnde Asthma-Kontrolle / Rez. Exazerbationen
trotz maximaler inhalativer Therapie
• Stimmt die Diagnose ?
• Inhalationstechnik ok ?
• Inhalation regelmäßig ?
• Optimale Dosis / Med. ?
• Trigger ausgeschaltet?
• Komorbiditäten:
• erkannt & behandelt?
Schweres Asthma: neues Konzept (GINA 2019)

Schweres Asthma: wie häufig ist das?
Schätzung:
3,6 %aller Patienten
mit Asthma
Analyse in den
Niederlanden
Hekking et al., JACI 2015
15.2%
Panel: Pharmacies database
76.50%
40.2%
40.2%
0.6838%
20.50%
74.1%
high intensity treatment
6519
Asthma AND high
intensity treatment
929
Asthma AND high
intensity treatment
2618
Difficult-to-control asthma
688
Severe refractory asthma
141
20.50%
74.1%
Analysed questionaires
2312
Pharmacies Database
500,500
Adults
382,883
76.50%
Panel: Dutch Population
15.2%
0.51%
0.1040%
3.6%
17.4%23.5%
0.6838%
The Netherlands
16,655,799
Adults
12,741,686
Adults with Asthma
370,019
Asthma AND high
intensity treatment
87,133
Difficult-to-control asthma
64,529
Severe refractory asthma
13,248

Asthma-Pathogenese: viele beteiligte Zellen
Barnes, Nat Rev Drug Discovery 2004; 3: 831-844
Epitheldysfunktion
Immundysregulation
(chronische Entzündung)
Neuromuskuläre
Überempfindlichkeit
Vaskuläre Dysfunktion
Bindegewebsumbau
Macrophage/dendritic cell
TH2
Allergen
Mast cell
Neutrophil
Eosinophil
Mucus plugNerve
activation
Epithelial shedding
BronchoconstrictionHypertrophy/hyperplasia
Airwayepithilium
Subepithelialfibrosis
Sensory nerveactivation
Cholinergicreflex
Airwaysmooth muscle
VasodilationNew vessels
(angiogenesis)
MucusHypersecretionHyperplasia
Plasma leakageEdema
Subcutaneous layer

Asthma-Pathogenese: viele beteiligte Zellen
Holgate, Nat Med 2012
Epitheldysfunktion
als wichtiger
pathogenetischer
Faktor bei Asthma
Mucosalepithelium
Bacteria
PollutantVirus Allergen
Damagedepithilium
InnatePRRs
CCR6
Bone marrow
Activated EC
CD34+mDC
CCL20CCL27
CLL19
CCR10
CCR7
IL-33TSLPIL-25
GM-CSFIL-1βTFN-α
DCmigration
Traffickingof DCs
Antigen uptakeand processing
MHC-II
Processedallergen
IL-33IL-25 CCL5
CCL17CCL22
CX3CL1
CCR4
TH2
TH2
TH2
TH2
TH2
TN
TN
Locallymph node
T celldiffentiation
Antigen presentation
TH2 expansionAnd memoryresponse
TH2 maturationand migration

FeNO: Signal aus dem erkrankten Epithel
Busse et al., Lancet Respir Med 2021
Macrophage/dendritic cell
TH2
Allergen
Mast cell
Neutrophil
Eosinophil
Mucus plugNerve
activation
Epithelial shedding
BronchoconstrictionHypertrophy/hyperplasia
Airwayepithilium
Subepithelialfibrosis
Sensory nerveactivation
Cholinergicreflex
Airwaysmooth muscle
VasodilationNew vessels
(angiogenesis)
MucusHypersecretionHyperplasia
Plasma leakageEdema
Subcutaneous layer
FeNO
NO-Produktion:Vor allem getriggert durch
Interleukin-13 (IL-13)
Biomarker für:- Diagnose Asthma
- Neigung zu Exazerbationen
- Ansprechen auf Steroide
- Ansprechen auf bestimmte Biologika
FeNO
Barnes, Nat Rev Drug Discovery 2004; 3: 831-844

Asthma-Immunpathologie
Lambrecht & Hammad, Nat Immunol 2015
Allergen
Airway
epithelium
IL-33
IL-25
TSLP
Goblet
cells
Pollutant, microbes,
glycolipids
Alternatively
activated
macrophages
YM1
IL-33
TSLPR
NKT cells
IL-25R IL-33R
PGD2
CRTH2
Lipoxin A4
Naive
T cell
MHC-II
TCRMast cells
DCs
TH2
GATA-3
ILC2
GATA-3
RORα
Allergic eosinophilic airway inflammation
B cells
Nonallergic eosinophilic airway inflammation
IL-9
IL-5
IL-13
Eosinophils
IL-13
IL-5
IL-9
IL-4
IL-13
Bronchial hyperreactivity
AllergischesAsthma:
Th2-Zellen
IntrinsischesAsthma:
ILC2-Zellen
Ähnliches Zytokin-Muster
In der Endstrecke
Konzept: Typ-2-Inflammation

Konzept: Typ-2-Inflammation
Lambrecht & Hammad, Nat Immunol 2015
Allergen
Airway
epithelium
IL-33
IL-25
TSLP
Goblet
cells
Pollutant, microbes,
glycolipids
Alternatively
activated
macrophages
YM1
IL-33
TSLPR
NKT cells
IL-25R IL-33R
PGD2
CRTH2
Lipoxin A4
Naive
T cell
MHC-II
TCRMast cells
DCs
TH2
GATA-3
ILC2
GATA-3
RORα
Allergic eosinophilic airway inflammation
B cells
Nonallergic eosinophilic airway inflammation
IL-9
IL-5
IL-13
Eosinophils
IL-13
IL-5
IL-9
IL-4
IL-13
Bronchial hyperreactivity
Klinische Bio-Marker:
Blut-Eosinophile
FeNO
Allergien
Korrelieren
nicht immer miteinander:
Individuelle Wichtung

Definitionen Typ-2-Inflammation
Lommatzsch et al., Allergy 2021
FeNO ≥ 20 ppb
Bluteosinophile ≥ 150/µl
„Asthma is clinically allergen-driven“
und/oderGINA-Definition:
Presence of
Type-2-Infammation
in severe asthma
FeNO ≥ 25 ppb
Bluteosinophile ≥ 150/µl
UKSAR-Definition:
Type-2-High
FeNO < 25 ppb
Bluteosinophile < 150/µl
und
UKSAR-Definition:
Type-2-Low
UKSAR: United Kingdom Severe Asthma Registry
und/oder
und
und
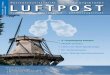
„Adult-onset Asthma“ vs. „Early-Onset Asthma“:Alter bei Erkrankungsbeginn als wichtige klinische Information
Pavord et al., Lancet 2018
Transient Asthma/Wheezing
„Early-onset asthma“
"Adult-onset Asthma"

Schweres Asthma: Typ-2-Marker je nach Erkrankungsbeginn
Lommatzsch et al., Allergy 2021
Erkrankungsbeginn
im Kindes- oder
Jugendalter:
Erhöhte Typ-2-Marker
Erkrankungsbeginn
im Erwachsenen-Alter:
Stark erhöhte
Typ-2-Marker
FeNO & Eosinophile
teils unabhängig
von IgE/Allergien

Schweres Asthma: Typ-2-Marker je nach Erkrankungsbeginn
Lommatzsch et al., Allergy 2021
Type-2-Hoch-Phänotyp:
bei Erkrankungsbeginn im
Erwachsenen-Alter häufiger
Erkrankungsbeginn
im Erwachsenen-Alter:
generell Neigung zu
schwereren Verläufen
Niedrige Type-2-Marker:
Weniger als 10 %
aller Patienten
mit schwerem Asthma

Neue NVL Asthma
Lommatzsch et al., Dt. Ärzteblatt, 2020
Biologika:
Mittel der 1. Wahl
Orale Steroide:nur noch in
begründeten Fällen
bei Versagen von Biologika
Zusatz-Optionen
in Stufe 5
Langzeittherapie:
ICS in Höchstdosis
+ LABA + LABA
Bedarfstherapie:
SABA
oder
ICS/Formoterol
Langzeittherapie:
ICS mittel- bis
hochdosiert
+ LABA (bevorzugt)
oder
ICS mittel- bis
hochdosiert
+ LABA + LAMA
Bedarfstherapie:
SABA
oder
ICS/Formoterol
Langzeittherapie:
ICS niedrigdosiert
+ LABA (bevorzugt)
oder
ICS mitteldosiert
Bedarfstherapie:
SABA
oder
ICS/Formoterol
ICS mittel- bis
hochdosiert
+ LABA + LTRA
ICS mittel- bis
hochdosiert
+ LAMA
Stufe 1
ICS niedrigdosiert
als Langzeittherapie
+ SABA
als Bedarfstherapie
LTRA als
Langzeittherapie
+ SABA
Als Bedarfstherapie
ICS niedrigdosiert
+ LAMA
ICS niedrigdosiert
+LTRA
OCS
(zusätzlich
oder alternativ)
Alternativen in begründeten Fällen:
Langzeittherapie:
ICS niedrigdosiert
+ SABA bei Bedarf
oder
Bedarfstherapie:
ICS/Formoterol
Bedarfstherapie:
ICS/Formoterol
oder
SABA
Stufe 2
Stufe 3
Stufe 4
Biologika:
Anti-IgE-Antikörper
oder
Anti-IL-5-(R)-
Antikörper
oder
Anti-IL-4-(R)-
Antikörper
Stufe 5
Generell:
- Asthma-Schulung, Allergie-/Umweltkontrolle, Beachtung von Komorbiditäten
- Allergen-Immuntherapie (bei gegebener Indikation)
Update 2020
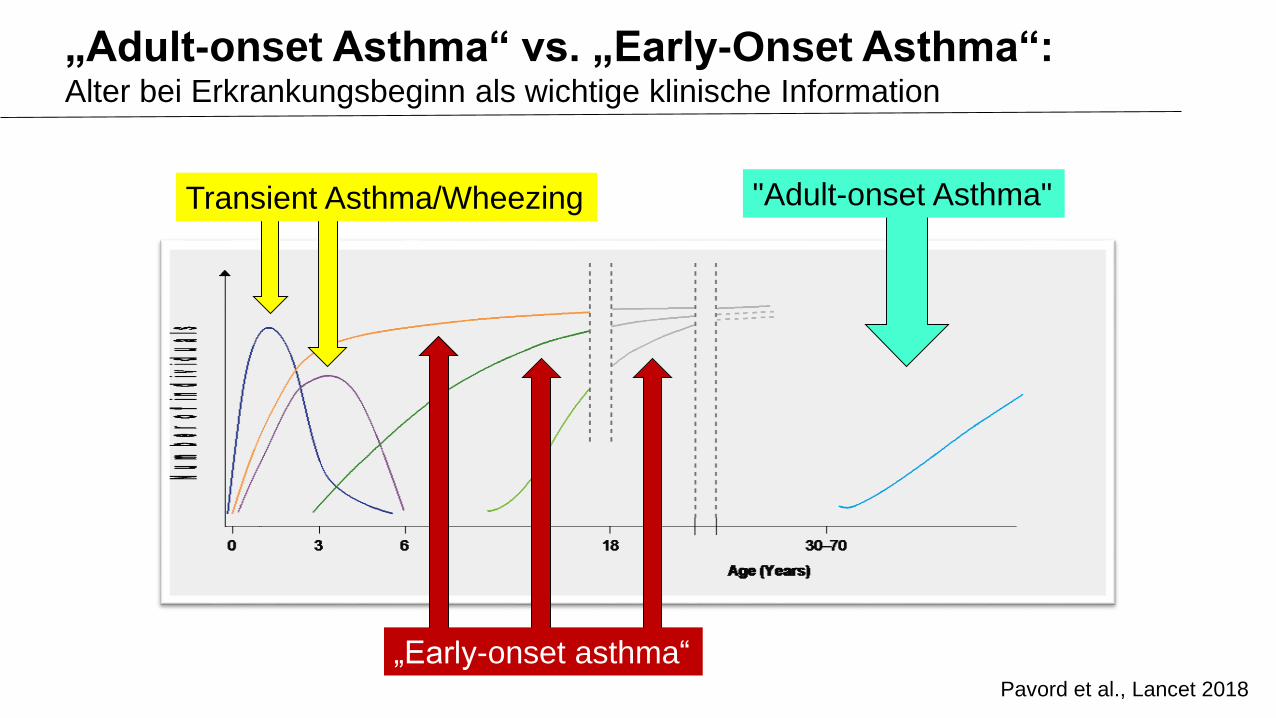
Biologika: Zielgenauer Eingriff in die Entzündung
Lambrecht & Hammad, Nat Immunol 2015
Allergen
Airway
epithelium
IL-33
IL-25
TSLP
Goblet
cells
Pollutant, microbes,
glycolipids
Alternatively
activated
macrophages
YM1
IL-33
TSLPR
NKT cells
IL-25R IL-33R
PGD2
CRTH2
Lipoxin A4
Naive
T cell
MHC-II
TCRMast cells
DCs
TH2
GATA-3
ILC2
GATA-3
RORα
Allergic eosinophilic airway inflammation
B cells
Nonallergic eosinophilic airway inflammation
IL-9
IL-5
IL-13
Eosinophils
IL-13
IL-5
IL-9
IL-4
IL-13
Bronchial hyperreactivity
Anti-IgE
Omalizumab
Prädiktoren des Ansprechens:
Early-Onset Asthma
Allergien
IgE-Erhöhung

Biologika: Zielgenauer Eingriff in die Entzündung
Lambrecht & Hammad, Nat Immunol 2015
Allergen
Airway
epithelium
IL-33
IL-25
TSLP
Goblet
cells
Pollutant, microbes,
glycolipids
Alternatively
activated
macrophages
YM1
IL-33
TSLPR
NKT cells
IL-25R IL-33R
PGD2
CRTH2
Lipoxin A4
Naive
T cell
MHC-II
TCRMast cells
DCs
TH2
GATA-3
ILC2
GATA-3
RORα
Allergic eosinophilic airway inflammation
B cells
Nonallergic eosinophilic airway inflammation
IL-9
IL-5
IL-13
Eosinophils
IL-13
IL-5
IL-9
IL-4
IL-13
Bronchial hyperreactivity
Anti-IL-5-(R)
Mepolizumab
Reslizumab
Benralizumab
Prädiktoren des Ansprechens:
Adult-Onset Asthma
Bluteosinophile > 150 Zellen/ µl
(> 300 Zellen / µl)

Biologika: Zielgenauer Eingriff in die Entzündung
Lambrecht & Hammad, Nat Immunol 2015
Allergen
Airway
epithelium
IL-33
IL-25
TSLP
Goblet
cells
Pollutant, microbes,
glycolipids
Alternatively
activated
macrophages
YM1
IL-33
TSLPR
NKT cells
IL-25R IL-33R
PGD2
CRTH2
Lipoxin A4
Naive
T cell
MHC-II
TCRMast cells
DCs
TH2
GATA-3
ILC2
GATA-3
RORα
Allergic eosinophilic airway inflammation
B cells
Nonallergic eosinophilic airway inflammation
IL-9
IL-5
IL-13
Eosinophils
IL-13
IL-5
IL-9
IL-4
IL-13
Bronchial hyperreactivity
Anti-IL-4/13
Dupilumab
Prädiktoren des Ansprechens:
FeNO > 25 ppb
Bluteosinophilie > 150 Zellen/µl
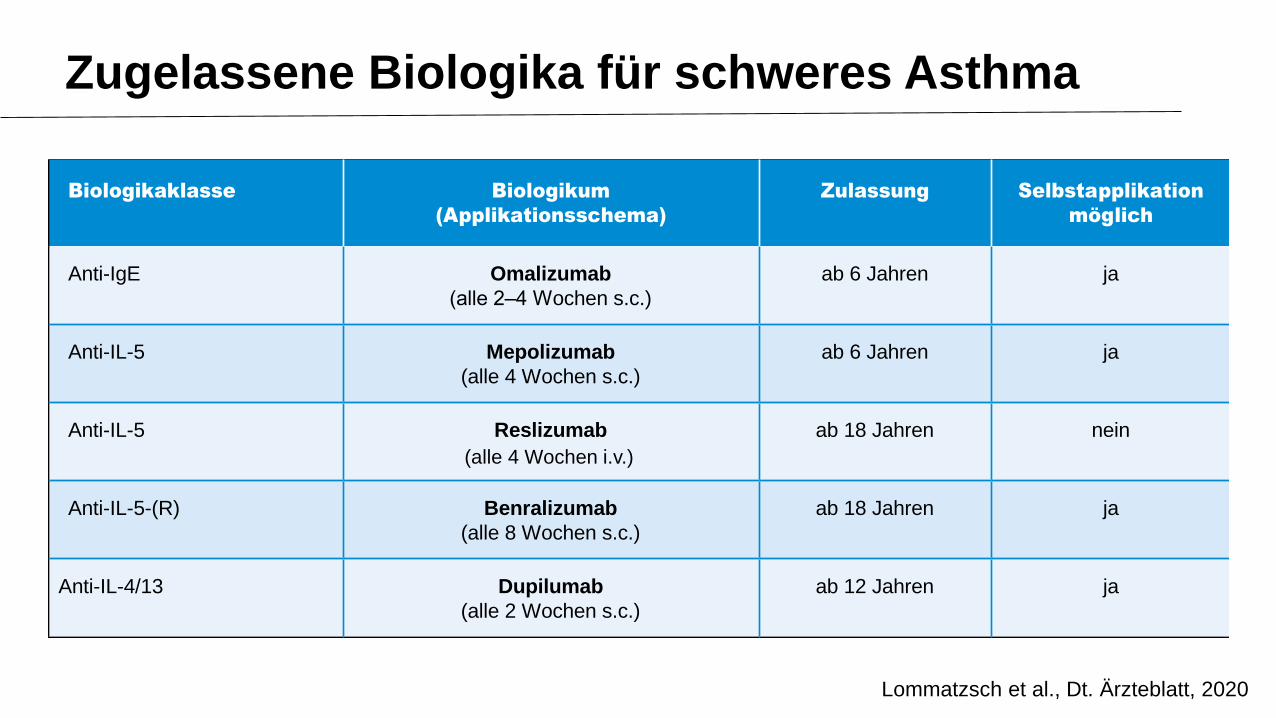
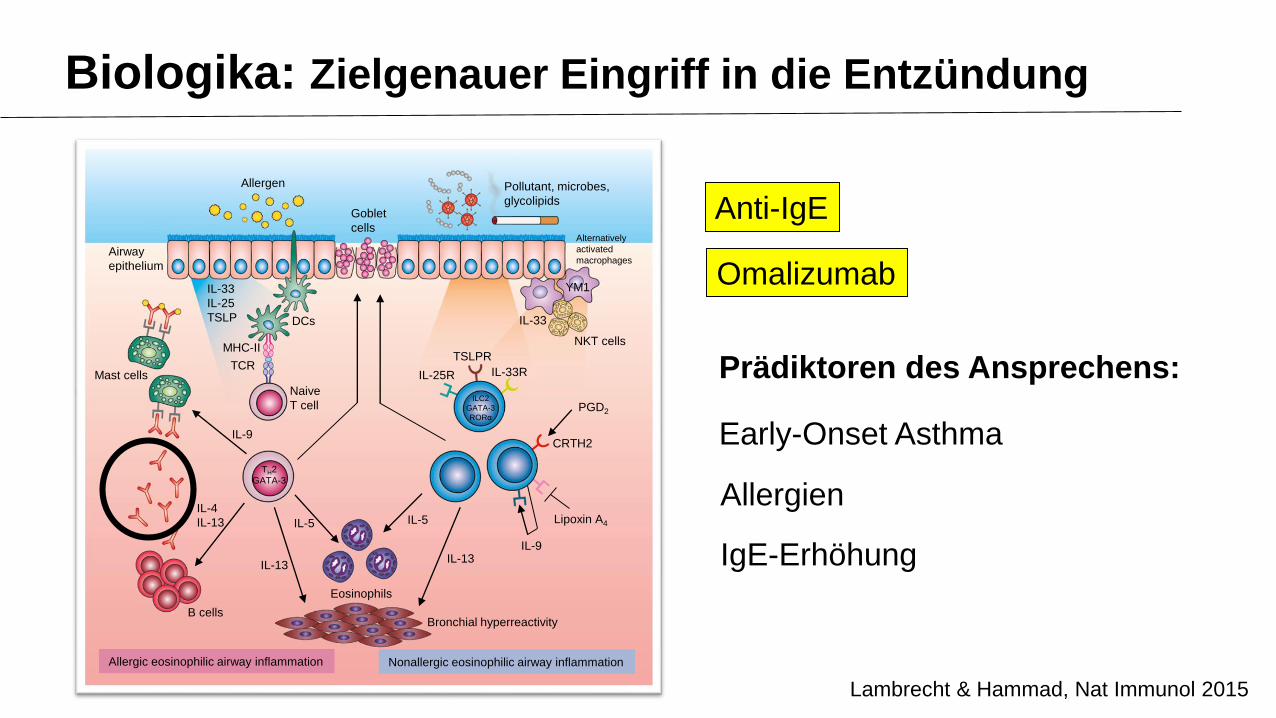
Zugelassene Biologika für schweres Asthma
Lommatzsch et al., Dt. Ärzteblatt, 2020
Biologikaklasse Biologikum
(Applikationsschema)
Zulassung Selbstapplikation
möglich
Anti-IgE Omalizumab
(alle 2–4 Wochen s.c.)
ab 6 Jahren ja
Anti-IL-5 Mepolizumab
(alle 4 Wochen s.c.)
ab 6 Jahren ja
Anti-IL-5 Reslizumab
(alle 4 Wochen s.c.)
ab 18 Jahren nein
Anti-IL-5-(R) Benralizumab
(alle 8 Wochen s.c.)
ab 18 Jahren ja
Anti-IL-4/13 Dupilumab
(alle 2 Wochen s.c.)
ab 12 Jahren ja
(alle 4 Wochen i.v.)

Biomarker unter Biologika-Therapie
Lommatzsch, Der Pneumologe, 2017
Anti-IL-5 Anti-IL-4/13
FeNO
Eos
IgE
Anti-IgETemporäre Erhöhung der Eosinophilen
unter Dupilumab-Therapie,
meist ohne Symptome:
Kontrolle des Differential-Blutbildes
4 Wochen nach Therapie-Beginn empfohlen
(Lommatzsch et al. Allergy 2021)

Zugelassene Biologika für schweres Asthma
Lommatzsch et al., Dt. Ärzteblatt, 2020
Biologikaklasse Biologikum
(Applikationsschema)
Zulassung Selbstapplikation
möglich
Anti-IgE Omalizumab
(alle 2–4 Wochen s.c.)
ab 6 Jahren ja
Anti-IL-5 Mepolizumab
(alle 4 Wochen s.c.)
ab 6 Jahren ja
Anti-IL-5 Reslizumab
(alle 4 Wochen s.c.)
ab 18 Jahren nein
Anti-IL-5-(R) Benralizumab
(alle 8 Wochen s.c.)
ab 18 Jahren ja
Anti-IL-4/13 Dupilumab
(alle 2 Wochen s.c.)
ab 12 Jahren ja
Kollaterale Wirksamkeit bei Ko-MorbiditätenHohe Wirksamkeit, selten Nebenwirkungen
(alle 4 Wochen i.v.)

Biologika-Therapie bei Asthma:Positiv beeinflusste Ko-Morbiditäten (*separate Zulassungen)
Anti-IL5Mepolizumab, Reslizumab,
Benralizumab
Anti-IgEOmalizumab
Anti-IL4/13Dupilumab Neurodermitis*
Simpson et al., NEJM 2016 | Blauvelt et al., Lancet 2017
Churg-Strauss-SyndromKim et al., JACI 2010 | Wechsler et al., NEJM 2017
„Hypereosinophilie“Roufosse et al., JACI 2013
Chronische Rhinosinusitis mit Polyposis (CRSwNP)*Bachert et al., Lancet 2019
Chronische Rhinosinusitis mit Polyposis (CRSwNP)Tversky et al., CEA 2021
Chronische Rhinosinusitis mit Polyposis (CRSwNP)*Gevaert et al., JACI 2020
Urtikaria *Allergien ABPAMaurer et al., NEJM 2013 | Voskamp et al., JACI-P 2015

Zusammenfassung:
• Schweres Asthma: in den aktuellen Leitlinien klar definiert
• Typ-2-Inflammation: zentrale Rolle bei schwerem Asthma
• Typ-2-Biomarker-Expression: individuell unterschiedlich
(u.a. abhängig vom Alter bei Erkrankungsbeginn)
• Gezielte Hemmung der Inflammation durch Biologika:
zentrales Therapie-Konzept bei schwerem Asthma
(+ Behandlung von Komorbiditäten)
Schweres Asthma & Typ-2-Inflammation

Vielen Dank für Ihre Aufmerksamkeit!
Transparenzinformation
Diese CME wird Ihnen mit freundlicher Unterstützung von Sanofi-
Aventis auf cme.medlearning.de angeboten (€ 12.750,00).