Embed Size (px)
Citation preview
DR. KLAUS DIRKS
INTERDISZIPLINÄRE SONOGRAPHIE
REMS-MURR-KLINIKUM WINNENDEN(( (
APPENDIZITIS 2018
RK 17- Abdomen
Part 4 - EFSUMB GIUS Guidelines
Comming soon
accepted
► 18 europ. Experten aus Gastroenterologie, Radiologie und Chirurgie
► 21 Empfehlungen
► > 80% Zustimmung für jede Empfehlung
EFSUMB GIUS Guidelines
Im Druck / Submission:
Part 3: Transrektaler und transperinealer US
Part 4: Appendizitis und Divertikulitis
Sahm M et al. Akute Appendizitis – Wandel in Epidemiologie, Diagnostik und Therapie. Zentralbl Chir 2011:18–24
Bulian D et al: Ergebnisse der bundesweiten Erhebung zur Technik der Appendektomie. BDC online 2013
Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet 2015: 386: 1278–87
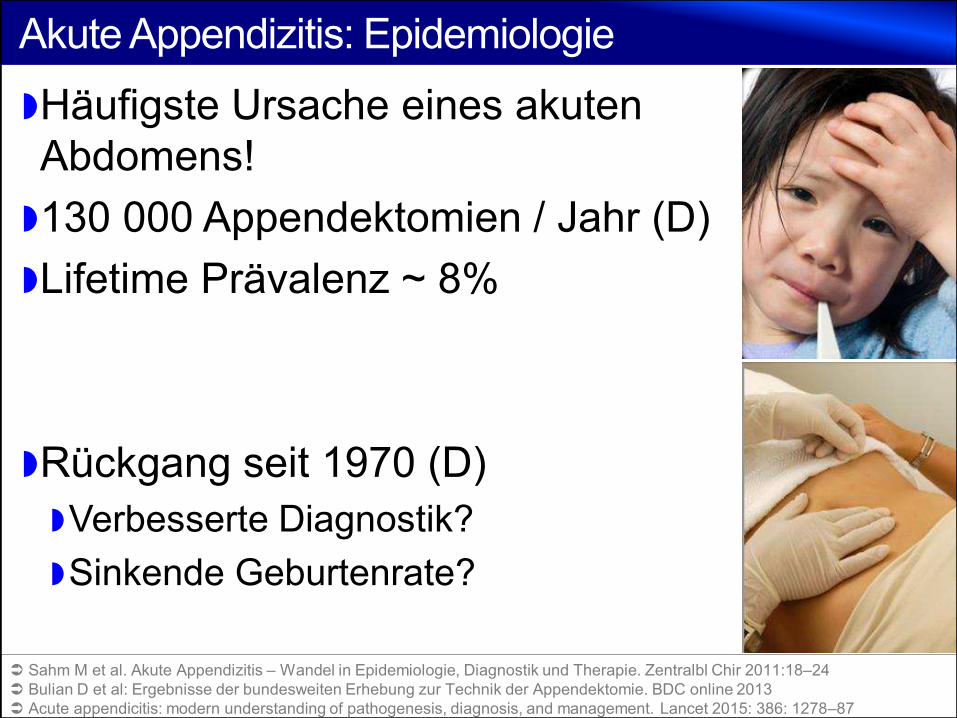
Akute Appendizitis: Epidemiologie
Häufigste Ursache eines akuten
Abdomens!
130 000 Appendektomien / Jahr (D)
Lifetime Prävalenz ~ 8%
Rückgang seit 1970 (D)
Verbesserte Diagnostik?
Sinkende Geburtenrate?
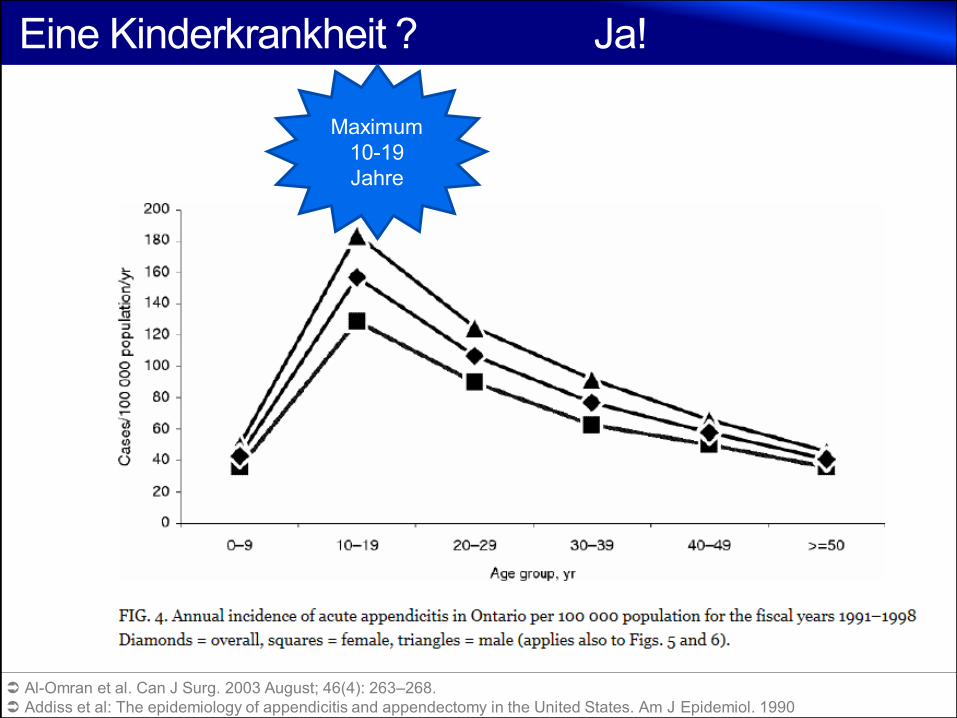
Al-Omran et al. Can J Surg. 2003 August; 46(4): 263–268.
Addiss et al: The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990
Eine Kinderkrankheit ? Ja!
Maximum
10-19
Jahre
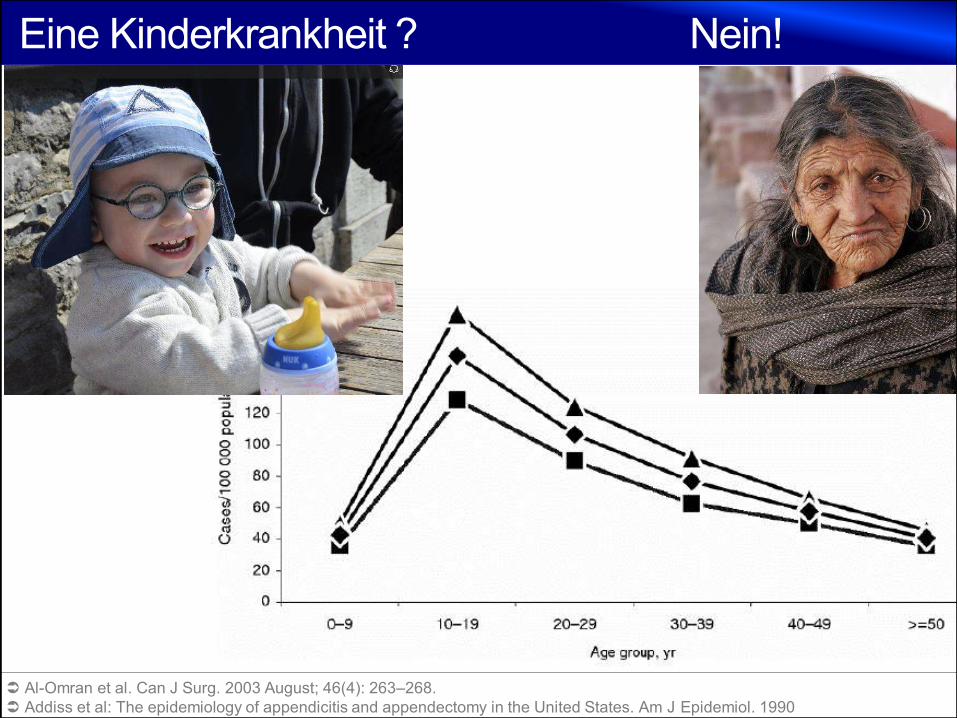
Al-Omran et al. Can J Surg. 2003 August; 46(4): 263–268.
Addiss et al: The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990
Eine Kinderkrankheit ? Nein!
EFSUMB recommendations
Statement 1
The use of ultrasound imaging should be a
routine procedure in every patient with
suspected appendicitis.
Consensus levels of agreement: A+ 16/18; A- 2/18
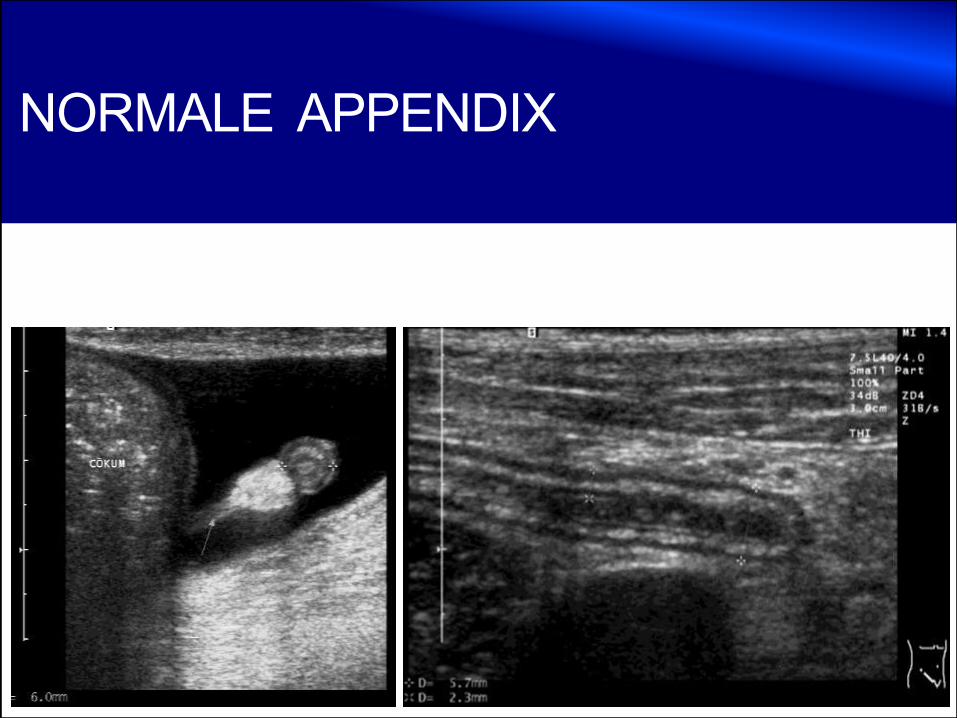
NORMALE APPENDIX
Untersuchungs-Tricks (1)
Schmerz-
maximum?
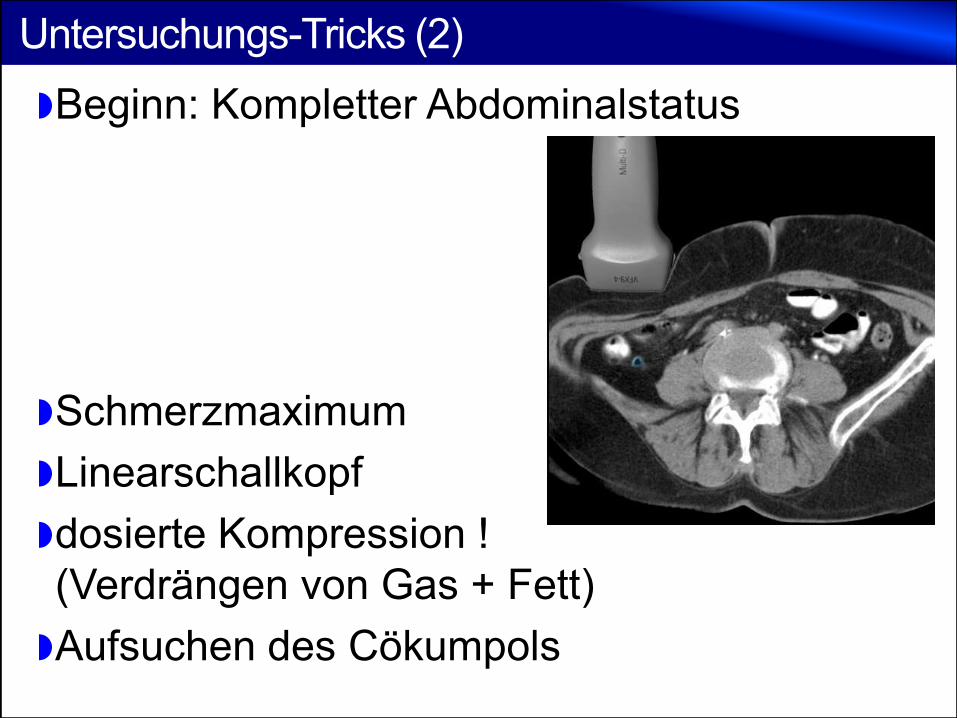
Untersuchungs-Tricks (2)
Beginn: Kompletter Abdominalstatus
Schmerzmaximum
Linearschallkopf
dosierte Kompression !
(Verdrängen von Gas + Fett)
Aufsuchen des Cökumpols
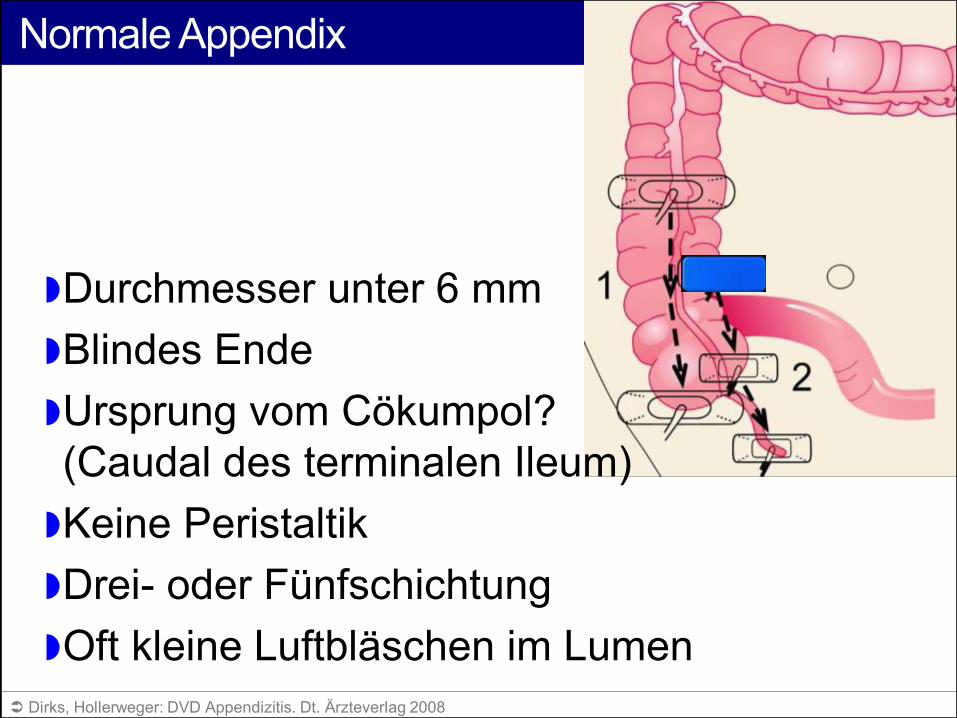
Normale Appendix
Dirks, Hollerweger: DVD Appendizitis. Dt. Ärzteverlag 2008
Durchmesser unter 6 mm
Blindes Ende
Ursprung vom Cökumpol?
(Caudal des terminalen Ileum)
Keine Peristaltik
Drei- oder Fünfschichtung
Oft kleine Luftbläschen im Lumen

Linksseitlage ?
Chang ST et al: Three-step sequential positioning algorithm during sonographic evaluation for appendicitis increases appendiceal
visualization rate and reduces CT use. AJR Am J Roentgenol. 2014 Nov;203(5): 1006-12.
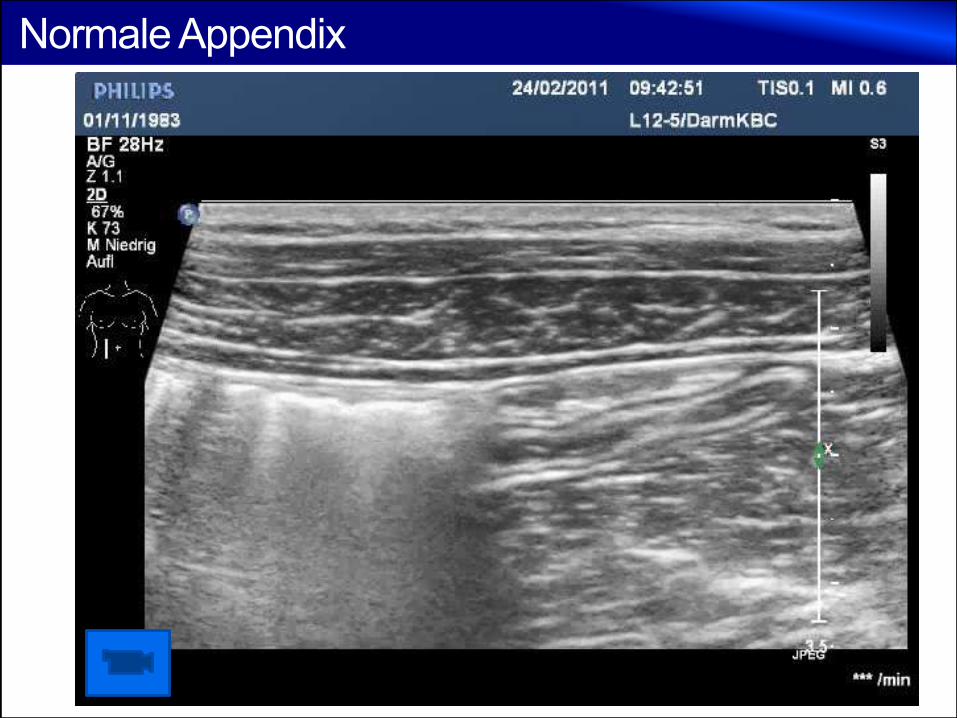
Normale Appendix
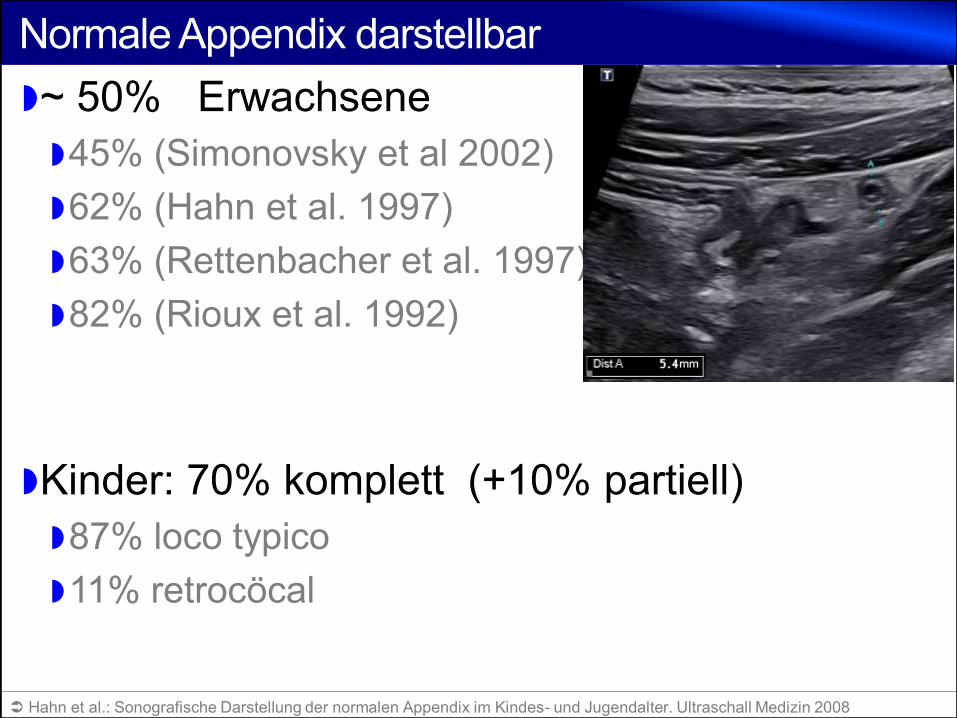
Hahn et al.: Sonografische Darstellung der normalen Appendix im Kindes- und Jugendalter. Ultraschall Medizin 2008
Normale Appendix darstellbar
~ 50% Erwachsene
45% (Simonovsky et al 2002)
62% (Hahn et al. 1997)
63% (Rettenbacher et al. 1997)
82% (Rioux et al. 1992)
Kinder: 70% komplett (+10% partiell)
87% loco typico
11% retrocöcal
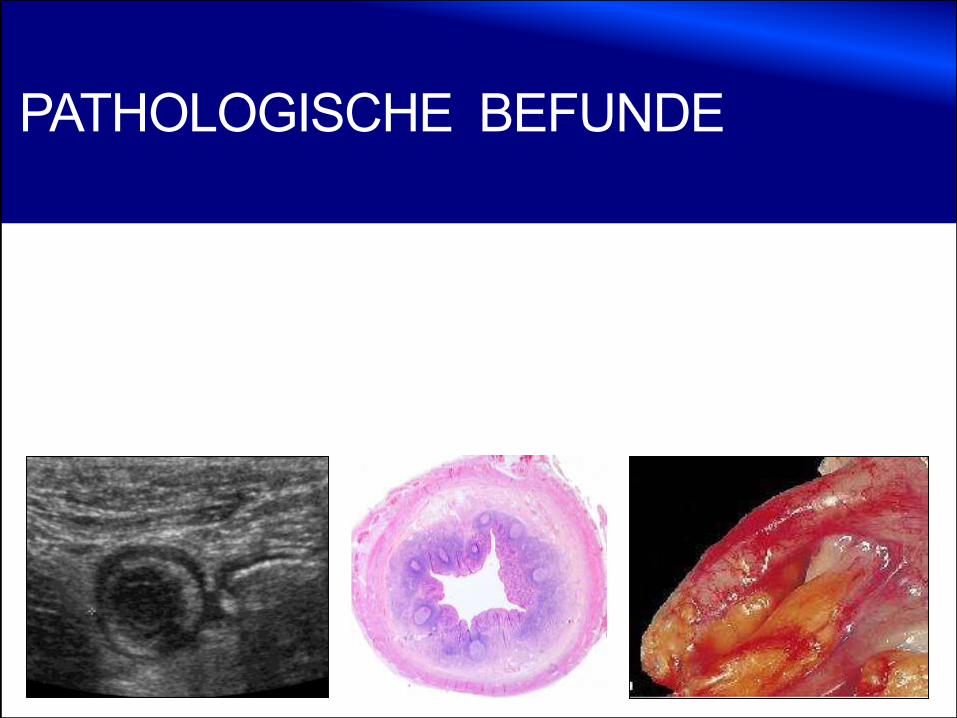
PATHOLOGISCHE BEFUNDE
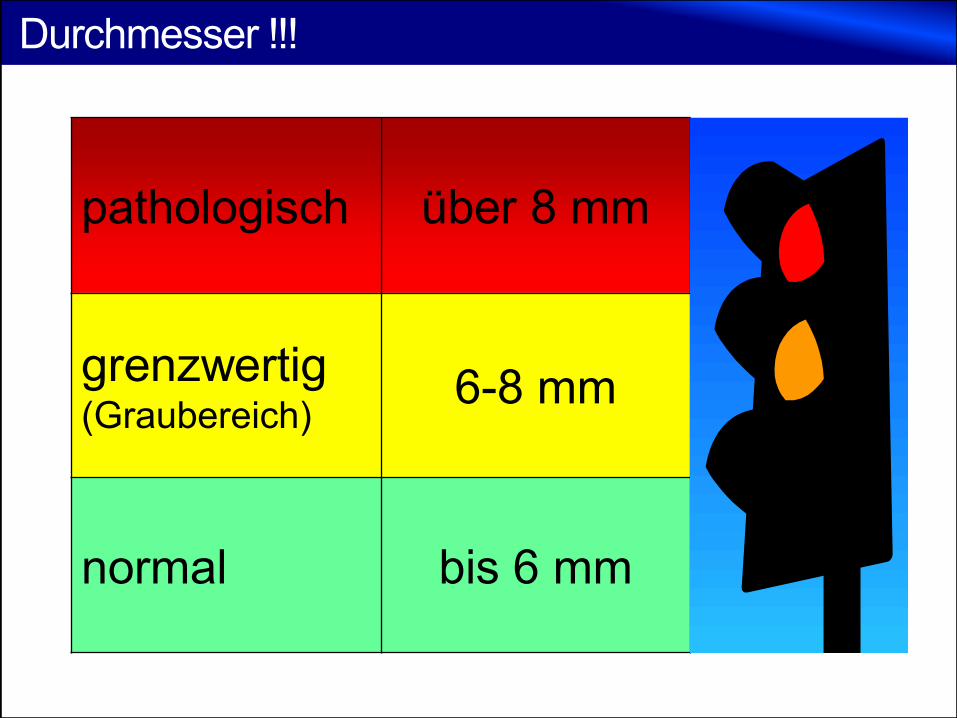
Durchmesser !!!
pathologisch über 8 mm
grenzwertig(Graubereich)
6-8 mm
normal bis 6 mm

… über 8mm pathologisch !
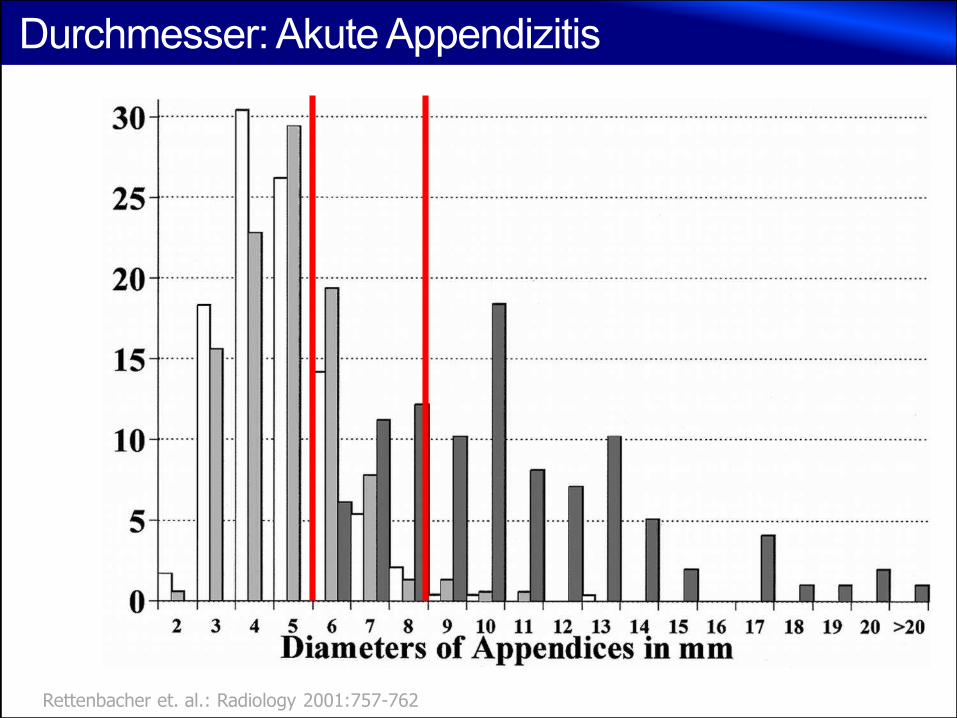
Durchmesser: Akute Appendizitis
Rettenbacher et. al.: Radiology 2001:757-762
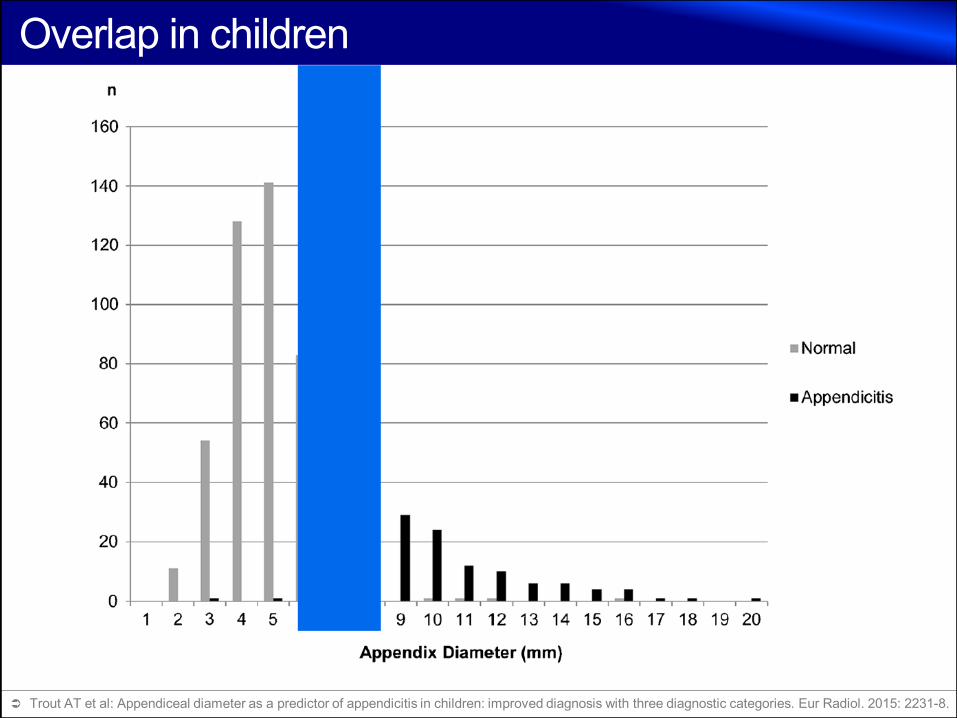
Overlap in children
Trout AT et al: Appendiceal diameter as a predictor of appendicitis in children: improved diagnosis with three diagnostic categories. Eur Radiol. 2015: 2231-8.
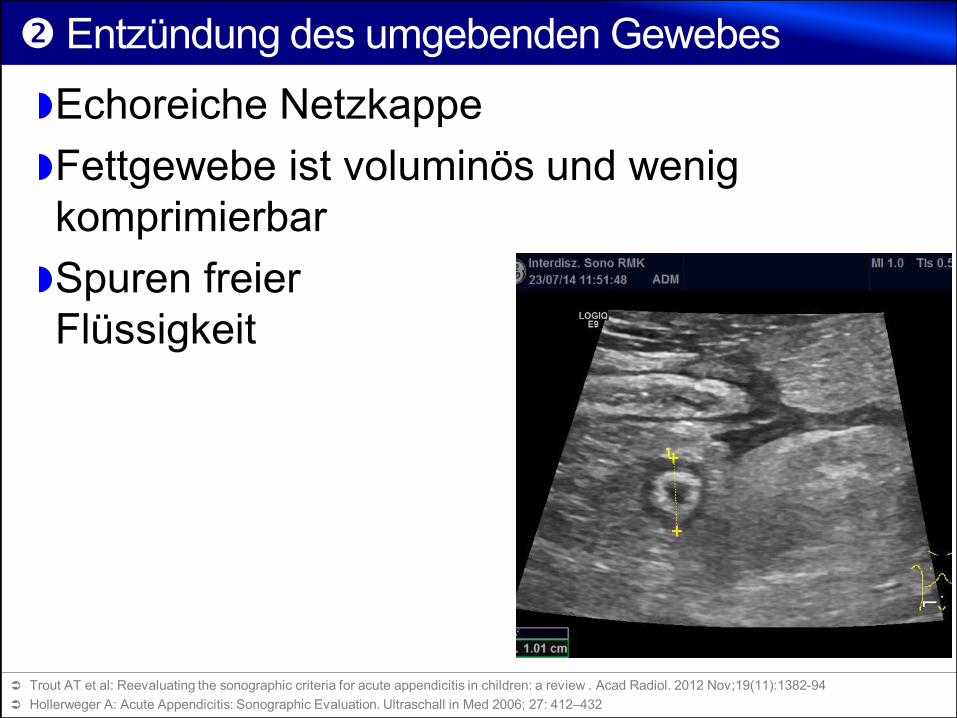
Entzündung des umgebenden Gewebes
Echoreiche Netzkappe
Fettgewebe ist voluminös und wenig
komprimierbar
Spuren freier
Flüssigkeit
Trout AT et al: Reevaluating the sonographic criteria for acute appendicitis in children: a review . Acad Radiol. 2012 Nov;19(11):1382-94
Hollerweger A: Acute Appendicitis: Sonographic Evaluation. Ultraschall in Med 2006; 27: 412–432
EFSUMB recommendations
Statement 5
A thickened appendix at the point of maximum
tenderness and hyperechoic periappendiceal
tissue are the most important signs of
appendicitis.
Consensus levels of agreement: A+ 15/17; A- 2/17
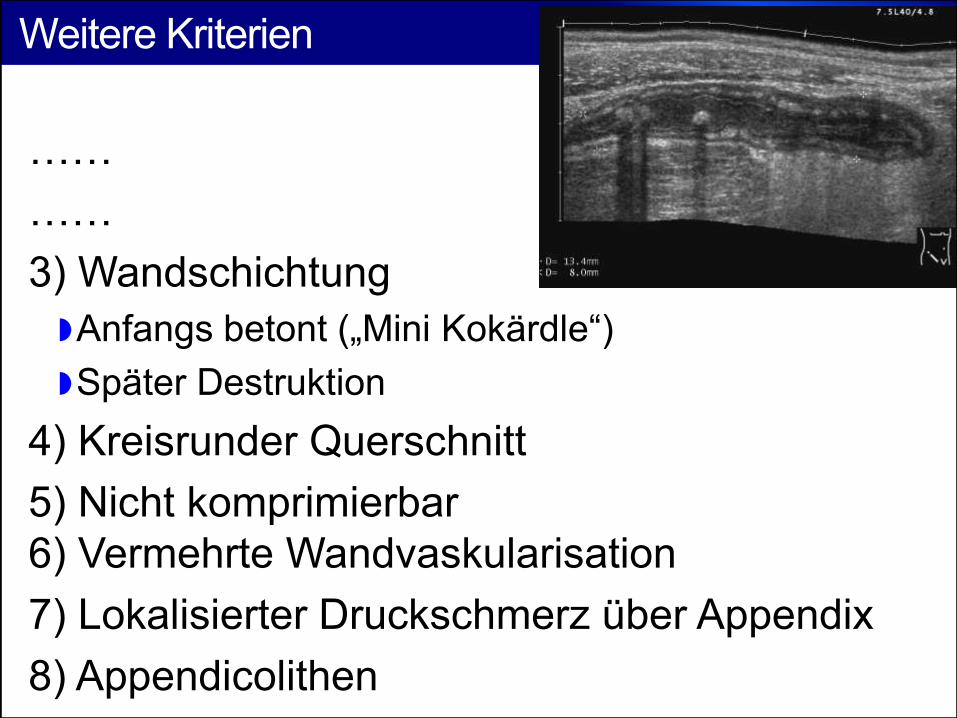
Weitere Kriterien
……
……
3) Wandschichtung
Anfangs betont („Mini Kokärdle“)
Später Destruktion
4) Kreisrunder Querschnitt
5) Nicht komprimierbar
6) Vermehrte Wandvaskularisation
7) Lokalisierter Druckschmerz über Appendix
8) Appendicolithen

Patholog. Durchmesser (12mm)
➢echoreiche Netzkappe
➢umgebende Flüssigkeit
➢Destruktion der Schichtung

Appendizitis

Appendizitis an der Spitze
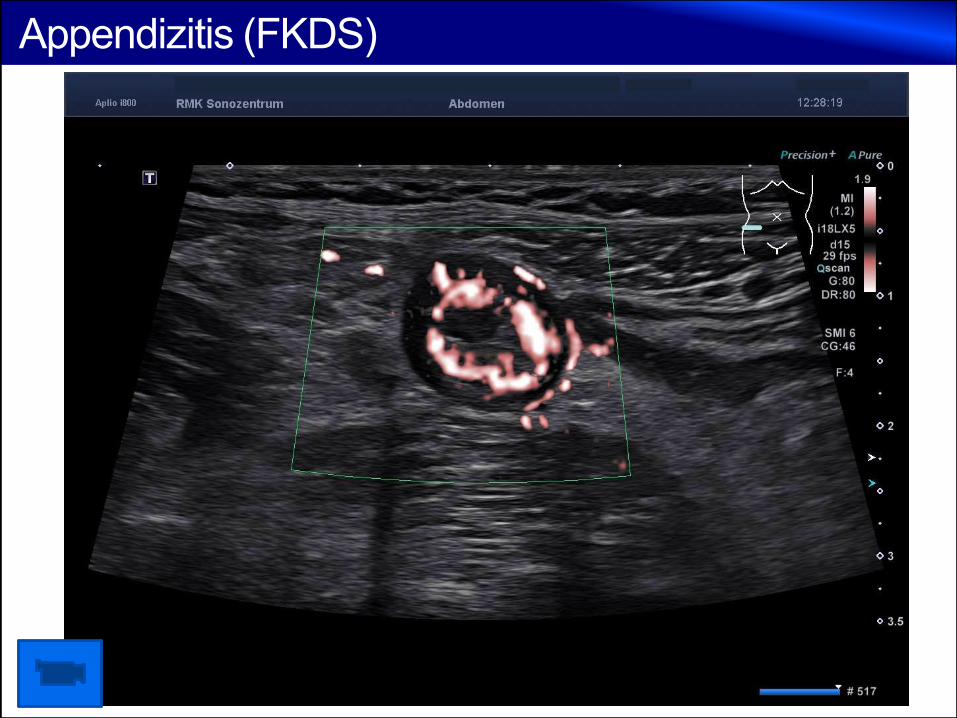
Appendizitis (FKDS)
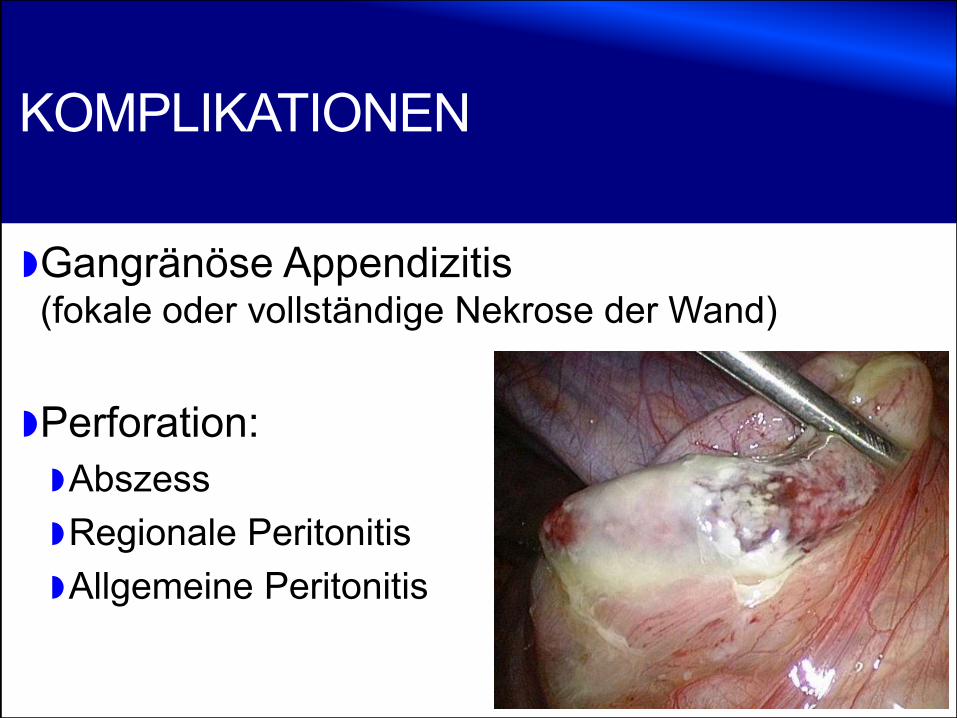
KOMPLIKATIONEN
Gangränöse Appendizitis (fokale oder vollständige Nekrose der Wand)
Perforation:
Abszess
Regionale Peritonitis
Allgemeine Peritonitis
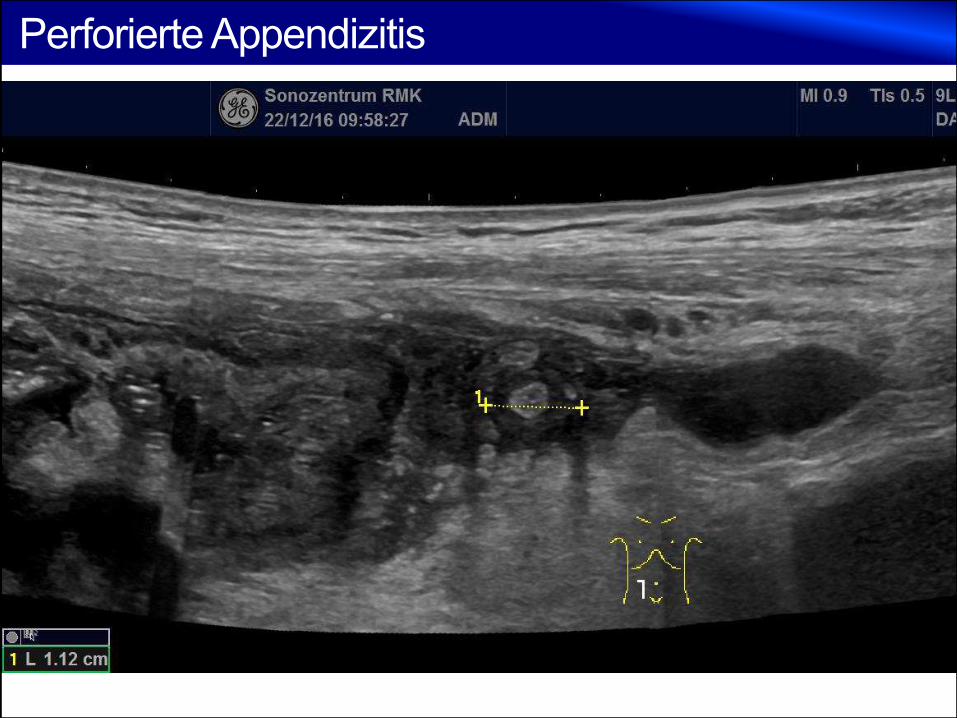
Perforierte Appendizitis
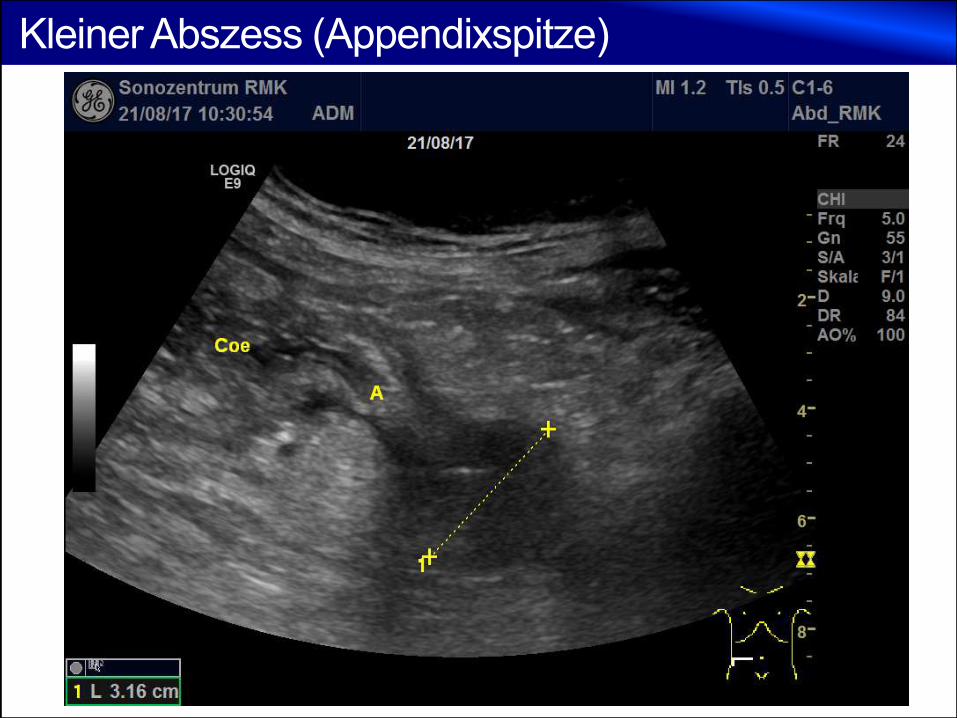
Kleiner Abszess (Appendixspitze)

Perityphlitischer Abszess
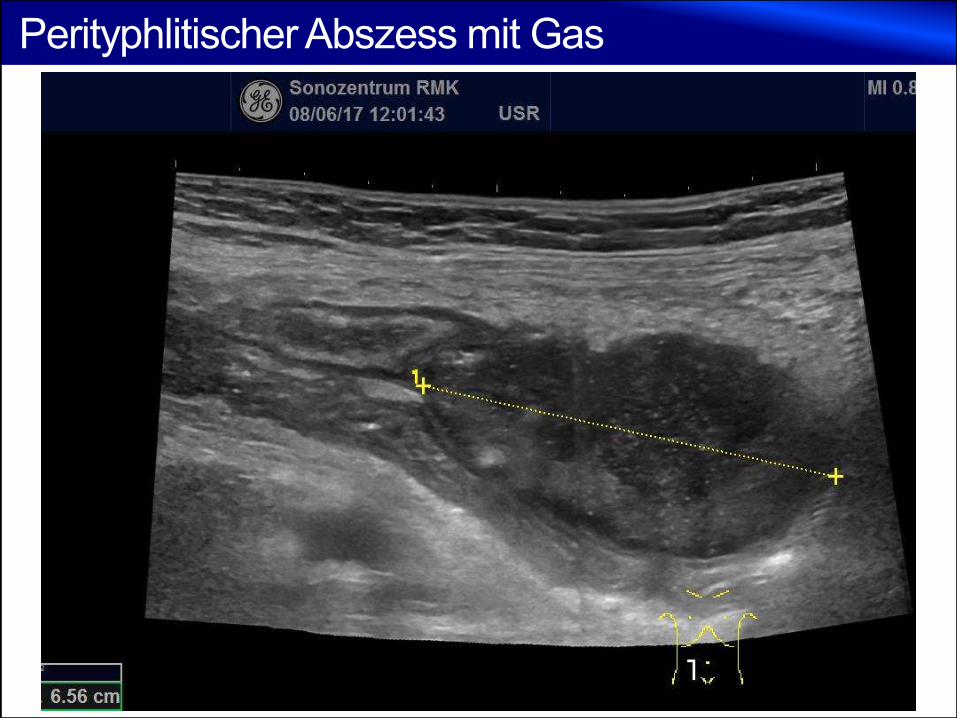
Perityphlitischer Abszess mit Gas

RECHTSSEITIGER UB-SCHMERZEN
KLINISCHES MANAGEMENT
EFSUMB recommendations
Statement 2
Routine sonography in all patients with
suspected appendicitis halves the rate of
unnecessary surgery (negative laparotomy
rate).
Consensus levels of agreement: A+ 14/18; A- 4/18
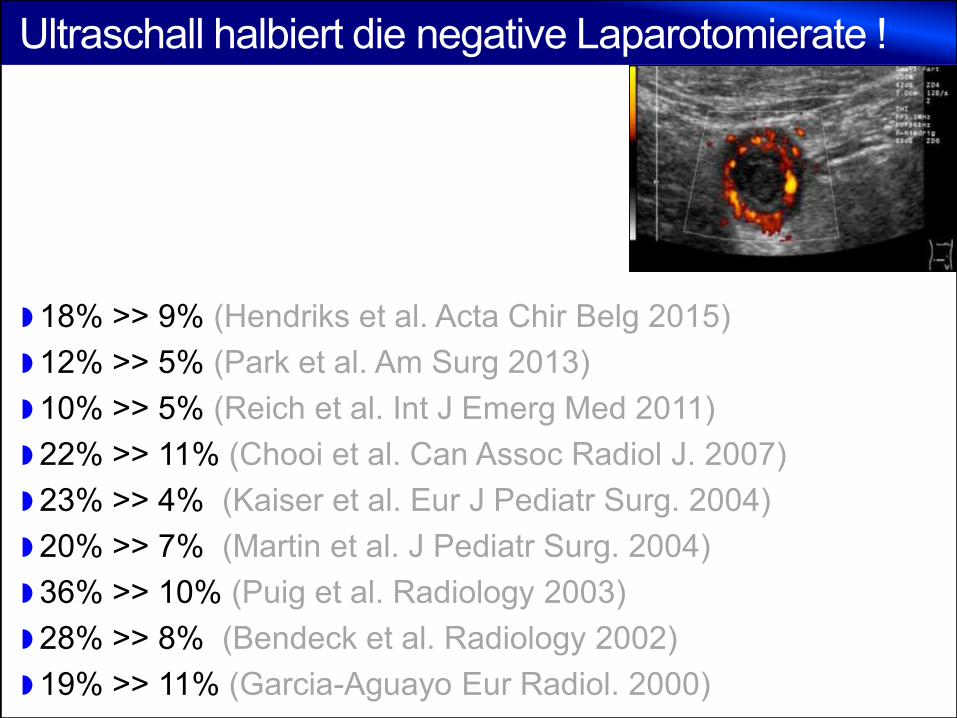
Ultraschall halbiert die negative Laparotomierate !
18% >> 9% (Hendriks et al. Acta Chir Belg 2015)
12% >> 5% (Park et al. Am Surg 2013)
10% >> 5% (Reich et al. Int J Emerg Med 2011)
22% >> 11% (Chooi et al. Can Assoc Radiol J. 2007)
23% >> 4% (Kaiser et al. Eur J Pediatr Surg. 2004)
20% >> 7% (Martin et al. J Pediatr Surg. 2004)
36% >> 10% (Puig et al. Radiology 2003)
28% >> 8% (Bendeck et al. Radiology 2002)
19% >> 11% (Garcia-Aguayo Eur Radiol. 2000)
EFSUMB recommendations
Statement 8
Systematic search for signs that suggest
differential diagnoses of appendicitis should be
implemented.
Consensus levels of agreement: A+ 17/18; A- 1/18
Immer komplette Sono: Differentialdiagnosen!
Bei18-31% der Patienten, die mit dringendem
Appendizitisverdacht aufgenommen wurden,
fand sich eine andere Schmerzursache
Auch wenn ein erfahrender Chirurg die
Anamnese und die körperliche Untersuchung
durchführte
Enteritis, rechtsseitige Divertikulitis,
mesenteriale Lymphadenitis, ...
Rettenbacher et al: Should Diagnostic Imaging Be Performed if the Clinical Presentation Is Highly Suggestive of the Disease? Radiology 2002
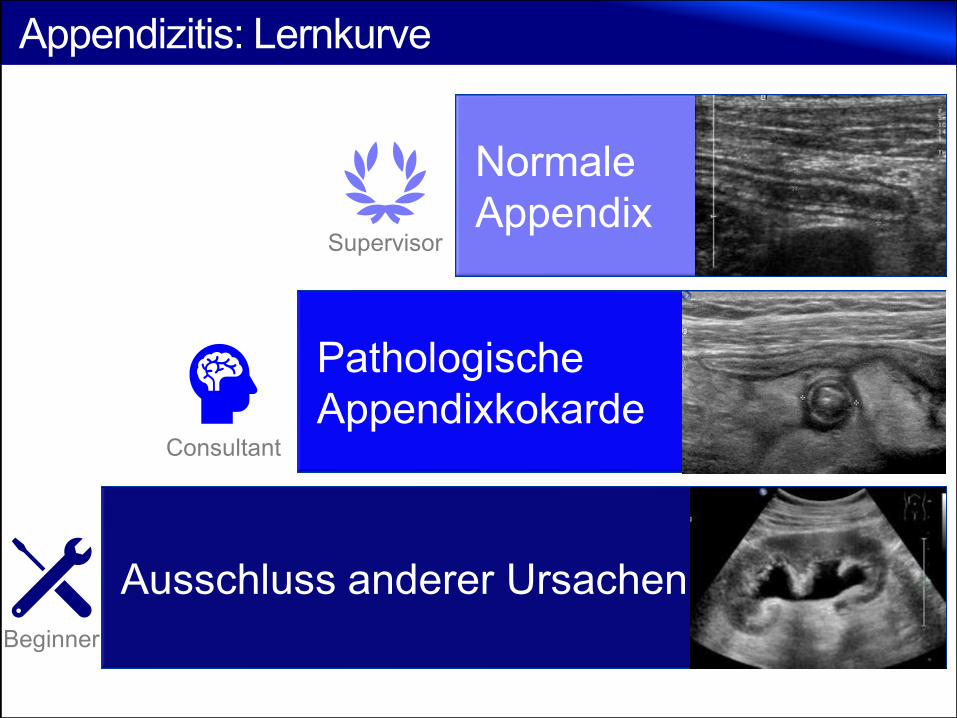
Appendizitis: Lernkurve
Ausschluss anderer Ursachen
Pathologische
Appendixkokarde
Normale
AppendixSupervisor
Consultant
Beginner
Falsch positive Sonographie
1) Verwechselung mit term. Ileum
2) Andere tubuläre Struktur re. UnterbauchMeckel Divertikulitis
Rechtsseitige Colon-Divertikulitis
dilatierte Tube
Ovarialvenen Thrombose
Faserbündel des M. psoas
3) Appendixverdickung durch andere
ErkrankungenM. Crohn: Appendix beteiligt in 20-25%
Infektiöse Enterocolitis
Zökumkarzinom
Appendix-Tumore (Cystadenom, Mucocele oder Karzinoid)
EFSUMB recommendations
Statement 6
Adequate training is a precondition for
sonographic diagnosis of acute appendicitis.
Consensus levels of agreement: A+ 18/18
Die Konkurrenz …
Sensitivität + Treffsicherheit gleich (90%)
aber weniger untersucherabhängig
Kosten, meist KM notwendig
Strahlenbelastung (Ovar !)Erwachsene: 1 Krebsfall auf 1000 CTs
Kinder: 1 Krebsfall auf 550 CTs
EFSUMB recommendations
Statement 9
In the hands of well-trained operators and
adequate equipment sensitivity and specificity
of ultrasound in acute appendicitis is similar to
CT or MRI.
Consensus levels of agreement: A+ 15/18; A- 2/18; I 1/18
Vergleich mit anderen Methoden
Die diagnostische Genauigkeit der High-End-
Sono bei Appendizitis hat sich in den letzten
Jahrzehnten deutlich verbessert.
GIUS ist ein stark Untersucherabhängig
Patientenmerkmale (z.B. Adipositas)
Institutionen, die Sono regelmäßig nutzen,
haben
eine höhere Sensibilität
Häufigere Darstellbarkeit der Appendix
EFSUMB recommendations
Statement 10
In any case of suspected appendicitis an
“ultrasound-first” strategy should be used in
both children and adults.
Consensus levels of agreement: A+ 18/18
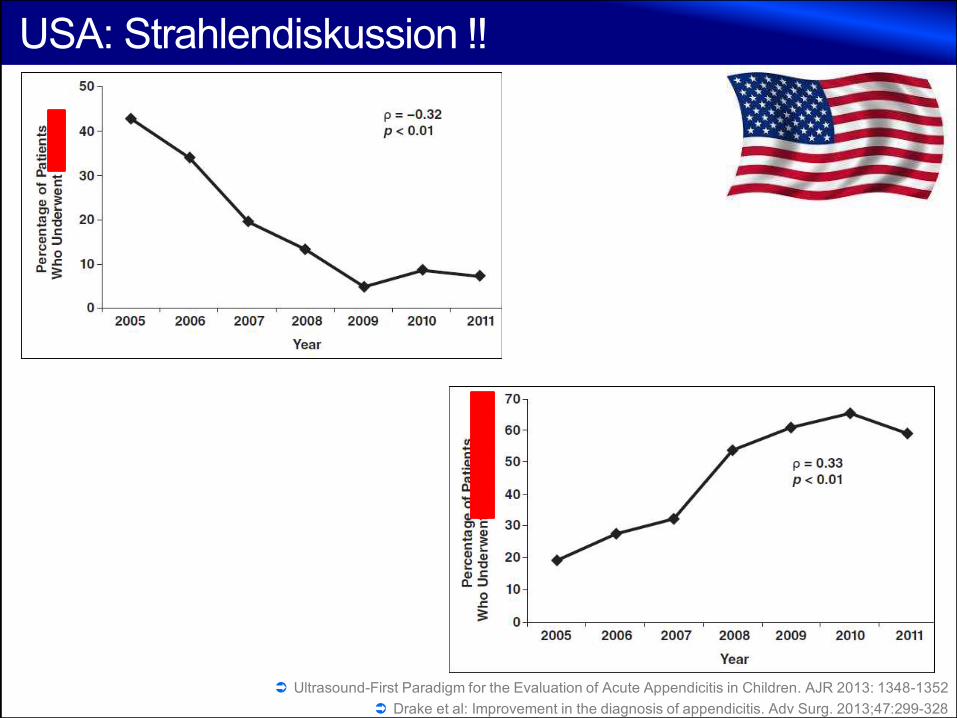
USA: Strahlendiskussion !!
Ultrasound-First Paradigm for the Evaluation of Acute Appendicitis in Children. AJR 2013: 1348-1352
Drake et al: Improvement in the diagnosis of appendicitis. Adv Surg. 2013;47:299-328
EFSUMB recommendations
Statement 11
Complementary CT or MRI should be limited to inconclusive findings and difficult conditions, e.g. in very obese patients or in pregnant women (MRI).
Consensus levels of agreement: A+ 14/18; A- 3/18; I 2/18; D- 1/18

It´s so easy ….
EDUCATION / TRAINING
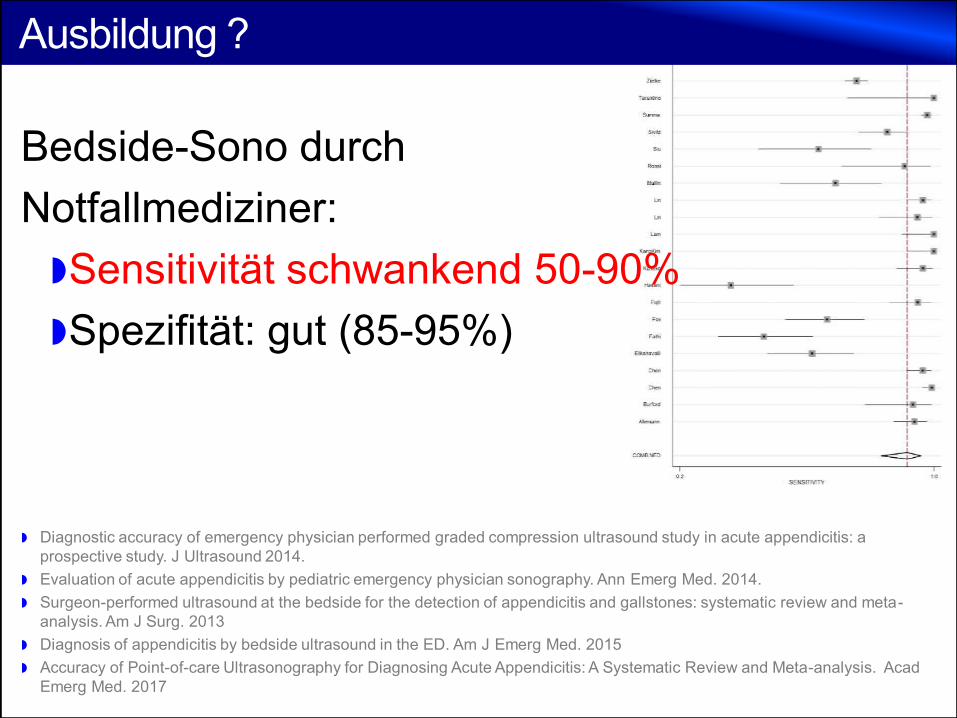
Ausbildung ?
Bedside-Sono durch
Notfallmediziner:
Sensitivität schwankend 50-90%
Spezifität: gut (85-95%)
Diagnostic accuracy of emergency physician performed graded compression ultrasound study in acute appendicitis: a
prospective study. J Ultrasound 2014.
Evaluation of acute appendicitis by pediatric emergency physician sonography. Ann Emerg Med. 2014.
Surgeon-performed ultrasound at the bedside for the detection of appendicitis and gallstones: systematic review and meta-
analysis. Am J Surg. 2013
Diagnosis of appendicitis by bedside ultrasound in the ED. Am J Emerg Med. 2015
Accuracy of Point-of-care Ultrasonography for Diagnosing Acute Appendicitis: A Systematic Review and Meta-analysis. Acad
Emerg Med. 2017
Surgeon-performed ultrasound
Accuracy of surgeon-performed gallbladder ultrasound in identification of acute cholecystitis. J Invest Surg. 2013 Apr;26(2):85-8
Surgeon-performed ultrasound at the bedside for detection of appendicitis and gallstones: American Journal of Surgery, Vol 205, No 1, January 2013
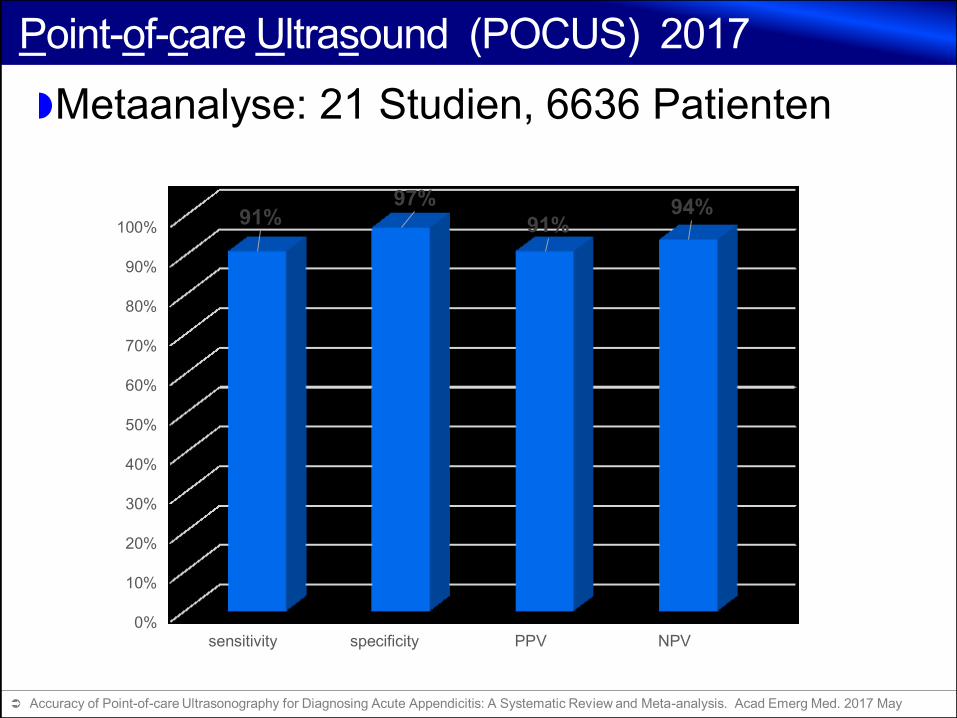
Point-of-care Ultrasound (POCUS) 2017
Metaanalyse: 21 Studien, 6636 Patienten
Accuracy of Point-of-care Ultrasonography for Diagnosing Acute Appendicitis: A Systematic Review and Meta-analysis. Acad Emerg Med. 2017 May
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
sensitivity specificity PPV NPV
91%97%
91%94%
Ausbildung und Qualitäts-Management
Problem: Sog. “non-diagnostic ultrasound”
(v.a. bei unerfahrenen Untersuchern)
Der nicht-diagnostische Ultraschall resultiert
aus:
Grenzwertigen App-Durchmesser (6-8mm)
Fehlende Auffindbarkeit der Appendix
Standardisiertes Untersuchungspotokoll
Reduktion “nicht diagnostischer” Sonos: 48% 0,1%
CT-Rate: 44% 14%
Appendix Appendix darstellbar ?
diameter?
Secondary signs: Echoreiche Umgebungsreaktion?
Freie Flüssigkeit?
Abszess?
Kotstein in Appendix? ……
Reducing computed tomography scans for appendicitis by introduction of a standardized and validated ultrasonography report template. J Pediatr Surg. 2015.
Improving ultrasound for appendicitis through standardized reporting of secondary signs. J Pediatr Surg. 2017 Aug;52(8):1273-1279.
Improving ultrasound quality to reduce computed tomography use in pediatric appendicitis: the Safe and Sound campaign. American J Surgery 2015
EFSUMB recommendations
Statement 12
Structured training programs, quality controls
and the use of standardized ultrasound
reporting templates should be integrated in the
training of emergency physicians for point-of-
care-ultrasound (POCUS) of appendicitis.
Consensus levels of agreement: A+ 15/18; A- 2/18; I 1/18
AUSBLICK 2018:
KONSERVATIVE THERAPIE ???
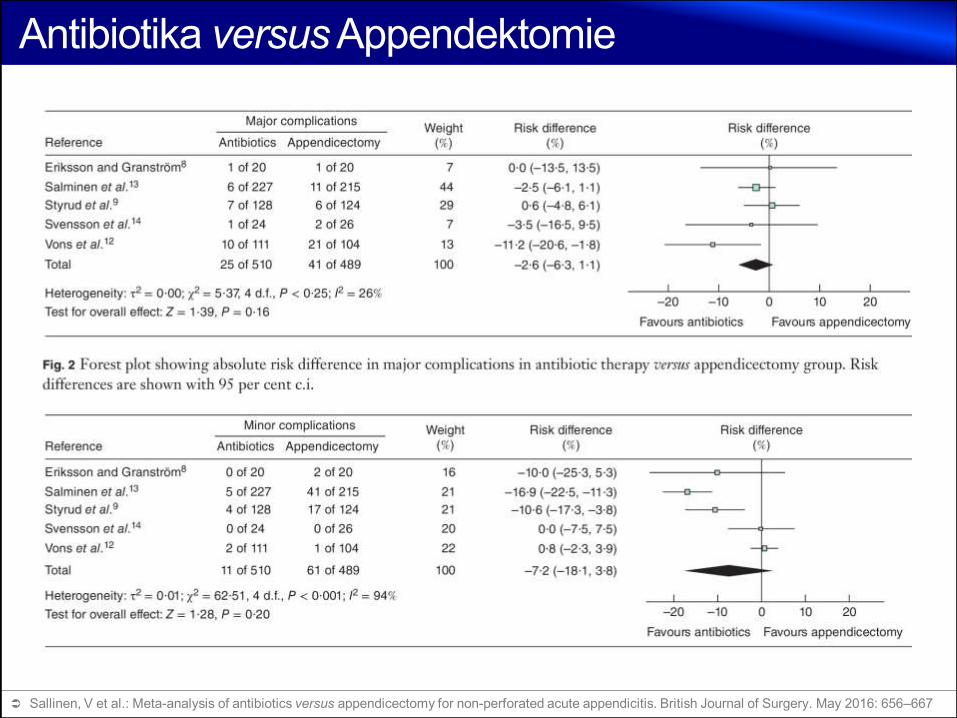
Antibiotika versus Appendektomie
Sallinen, V et al.: Meta-analysis of antibiotics versus appendicectomy for non-perforated acute appendicitis. British Journal of Surgery. May 2016: 656–667
Scoring Systeme ?!
Komplizierte
Appendizitis:
Operation
Gangränös
Perforiert
oder diffuse
Peritonitis
Unkomplizierte
Appendizitis:
Antibiotika
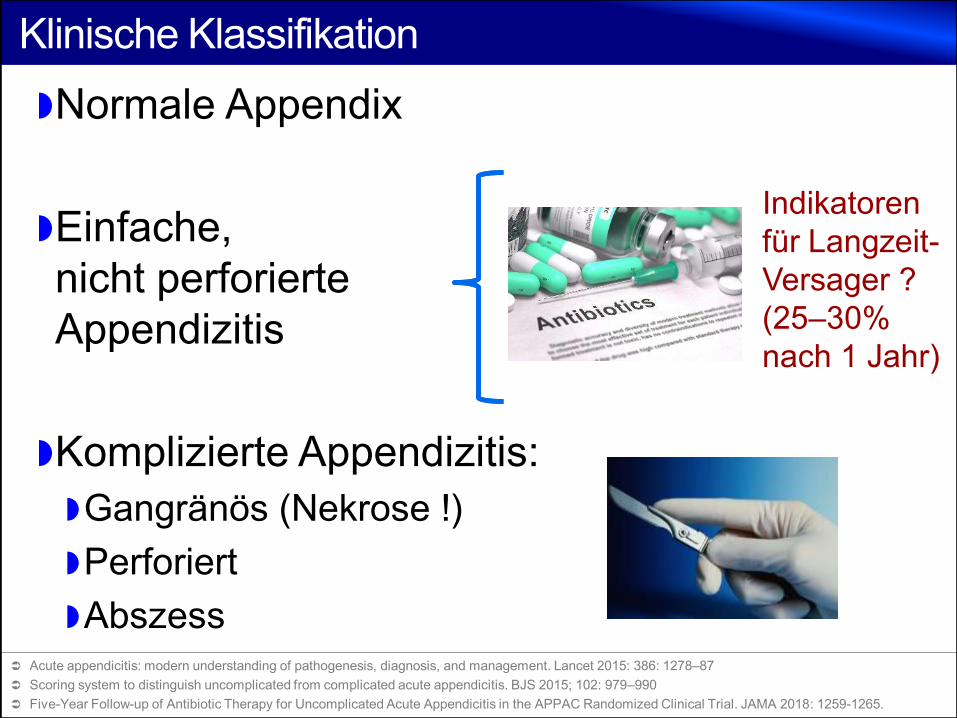
Klinische Klassifikation
Normale Appendix
Einfache,
nicht perforierte
Appendizitis
Komplizierte Appendizitis:
Gangränös (Nekrose !)
Perforiert
Abszess Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet 2015: 386: 1278–87
Scoring system to distinguish uncomplicated from complicated acute appendicitis. BJS 2015; 102: 979–990
Five-Year Follow-up of Antibiotic Therapy for Uncomplicated Acute Appendicitis in the APPAC Randomized Clinical Trial. JAMA 2018: 1259-1265.
Indikatoren
für Langzeit-
Versager ?
(25–30%
nach 1 Jahr)
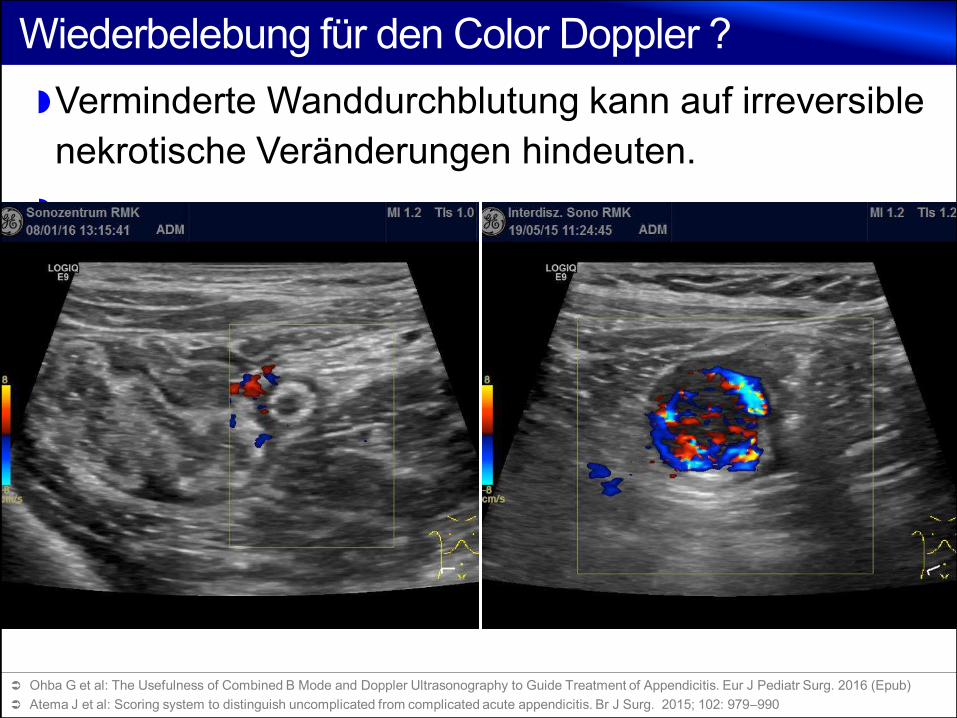
Wiederbelebung für den Color Doppler ?
Verminderte Wanddurchblutung kann auf irreversible
nekrotische Veränderungen hindeuten.
Ohba G et al: The Usefulness of Combined B Mode and Doppler Ultrasonography to Guide Treatment of Appendicitis. Eur J Pediatr Surg. 2016 (Epub)
Atema J et al: Scoring system to distinguish uncomplicated from complicated acute appendicitis. Br J Surg. 2015; 102: 979–990

2020:
Bestätigung der Verdachtsdiagnose Appendizitis
+
Unkomplizierte Appendizitis ohne Kotstein?














