Embed Size (px)
Citation preview

Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 1
Die Internationale Klassifikation der Funktionsfähigkeit, Behinderung und
Gesundheit (ICF)
als Paradigma, Standard und Werkzeug in der Rehabilitation

Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 2
Affiliations Dr. Jan D. Reinhardt
Swiss Paraplegic Research, Nottwil, Switzerland
University of Lucerne, Department of Health Sciences and Health Policy
International Society of Physical and Rehabilitation Medicine, Secretary WHO Liaison Committee, Vice Chair Rehabilitation Disaster Relief Committee
WHO ICF Research Branch of the German WHO CC (DIMDI), Munich, Germany & Nottwil, Switzerland
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Überblick
1. Das ICF Paradigma und Modell
2. Struktur der ICF als Klassifikation
3. ICF Coding
4. Linking Methode und Entwicklung von ICF Core Sets
5. Praktische Anwendung der ICF in der Kinder- und Jugendrehabilitation
6. Ausblick
3
Einführung
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Fragen an das Publikum
Wer hat eines dieser Bücher schon einmal in der Hand gehabt bzw. entsprechende Internetressourcen genutzt?
4
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Fragen an das Publikum
Wer benutzt die ICF oder ICF-CY in der klinischen oder epidemiologischen Forschung?
5
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
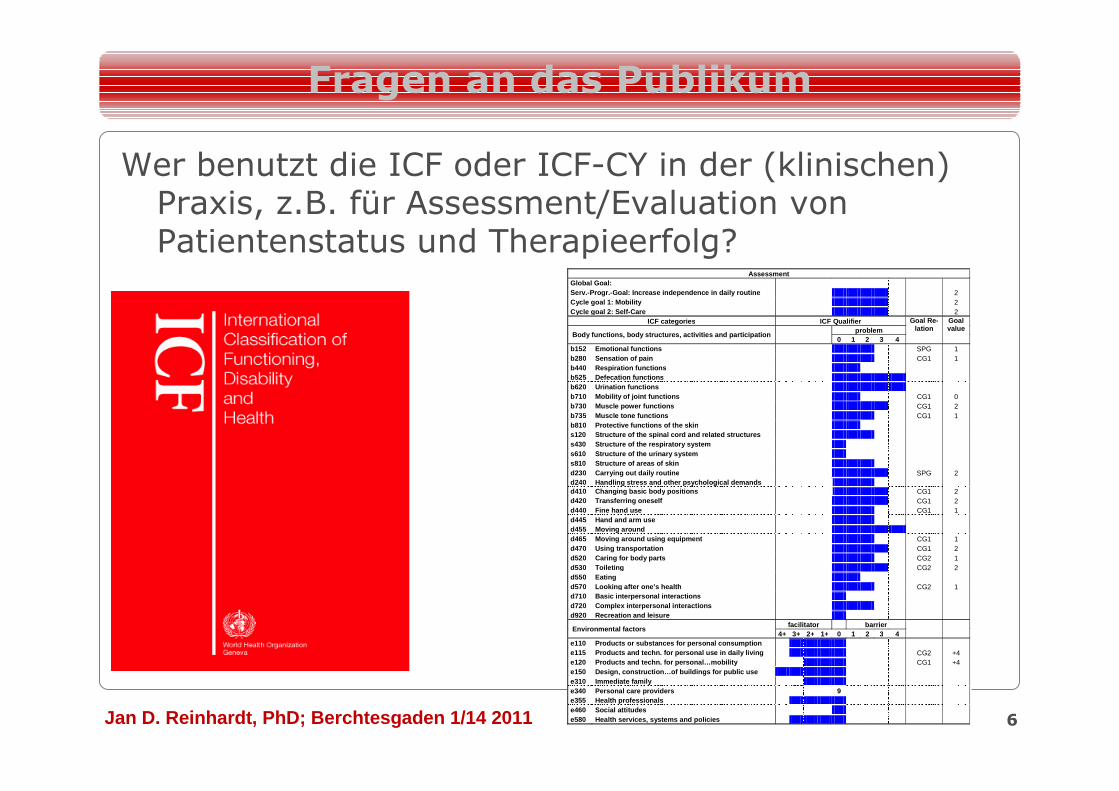
Fragen an das Publikum
Wer benutzt die ICF oder ICF-CY in der (klinischen) Praxis, z.B. für Assessment/Evaluation von Patientenstatus und Therapieerfolg?
6
Assessment Global Goal: Serv.-Progr.-Goal: Increase independence in daily r outine 2 Cycle goal 1: Mobility 2 Cycle goal 2: Self -Care 2
ICF categories ICF Qualifier Goal Re-lation
Goal value
Body functions, body structures, activities and par ticipation
problem 0 1 2 3 4
b152 Emotional function s SPG 1 b280 Sensation of pain CG1 1 b440 Respiration functions b525 Defecation functions b620 Urination functions b710 Mobility of joint functions CG1 0 b730 Muscle power functions CG1 2 b735 Muscle tone functions CG1 1 b810 Protective functions of the skin s120 Structure of the spinal cord and related struc tures s430 Structure of the respiratory system s610 Structure of the urinary system s810 Structure of areas of skin d230 Carrying out daily routine SPG 2 d240 Handling stress and other psychological demand s d410 Changing basic body positions CG1 2 d420 Transferring oneself CG1 2 d440 Fine hand use CG1 1 d445 Hand and arm use d455 Moving around d465 Moving around using equipment CG1 1 d470 Using transportation CG1 2 d520 Caring for bod y parts CG2 1 d530 Toileting CG2 2 d550 Eating d570 Looking after one’s health CG2 1 d710 Basic interpersonal interactions d720 Complex interpersonal interactions d920 Recreation and leisure
Environmental factors facilitator barrier
4+ 3+ 2+ 1+ 0 1 2 3 4 e110 Products or substances for personal consumption e115 Products and techn. for personal use in daily living CG2 +4 e120 Products and techn. for personal…mobility CG1 +4 e150 Design, construction…of buildings for public u se e310 Immediate family e340 Personal care providers 9 e355 Health professionals e460 Social attitudes e580 Health services, systems and policies
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Was ist die ICF?
• Ein Paradigma/eine Theorie/ein Modell
• Eine Klassifikation
• Ein Kommunikationsmedium
• Ein Medium der klinischen und populationsbasierten Forschung
• Ein klinisches Werkzeug?
7
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
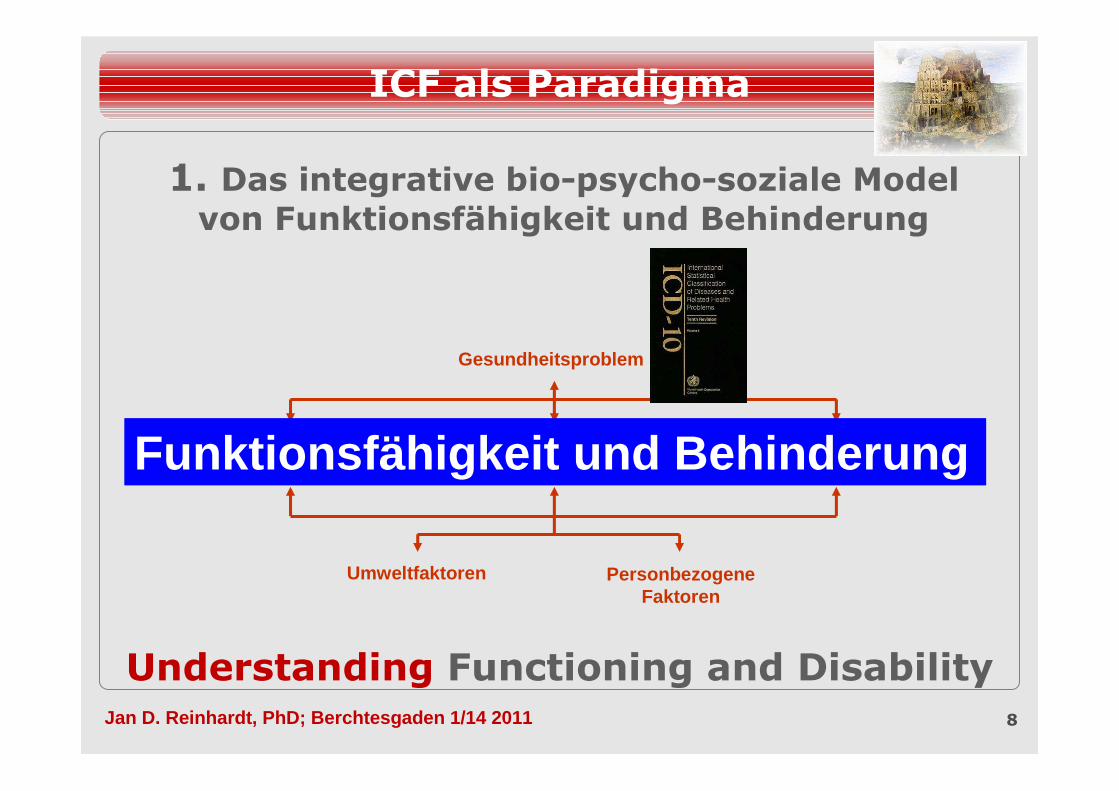
1. Das integrative bio-psycho-soziale Model von Funktionsfähigkeit und Behinderung
8
Gesundheitsproblem
Umweltfaktoren Personbezogene Faktoren
Körperfunktionen/-strukturen
Aktivitäten Partizipation
ICF als Paradigma
Understanding Functioning and Disability
Funktionsfähigkeit und Behinderung
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
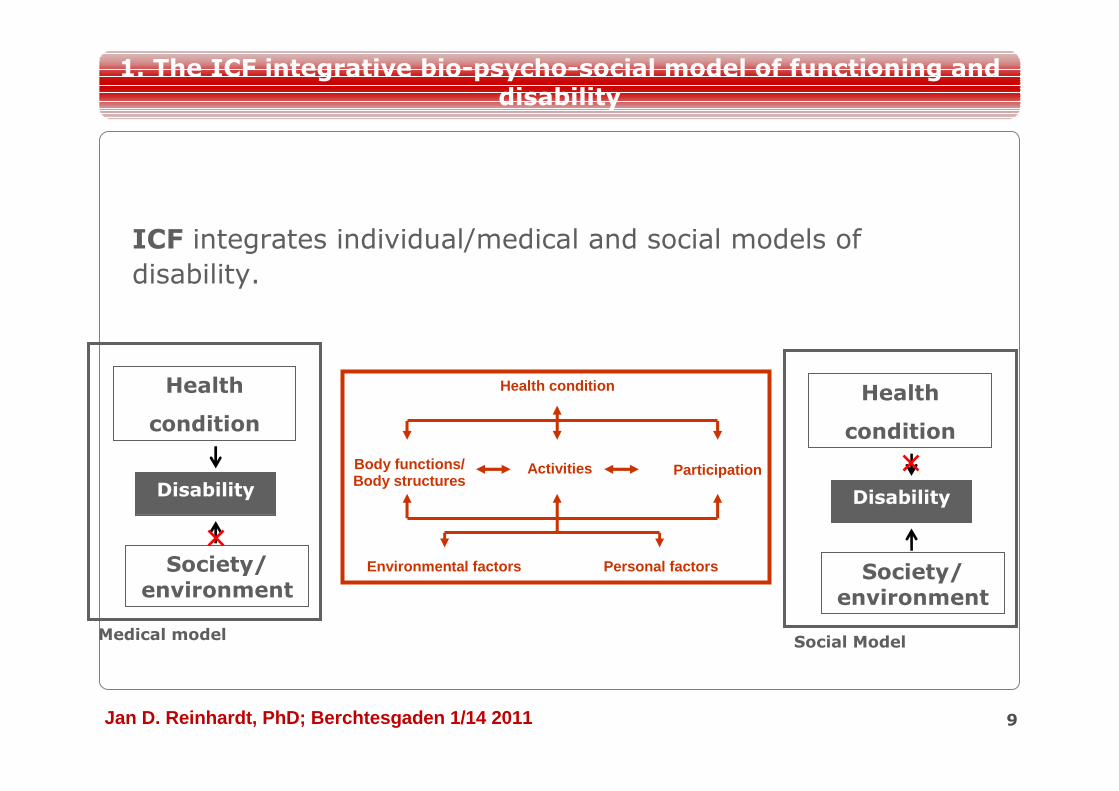
ICF integrates individual/medical and social models of
disability.
9
Disability
Health
condition
Medical model
Health condition
Environmental factors Personal factors
Body functions/ Body structures
Activities Participation
1. The ICF integrative bio-psycho-social model of functioning and disability
Society/environment
Disability
Health
condition
Social Model
Society/environment
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
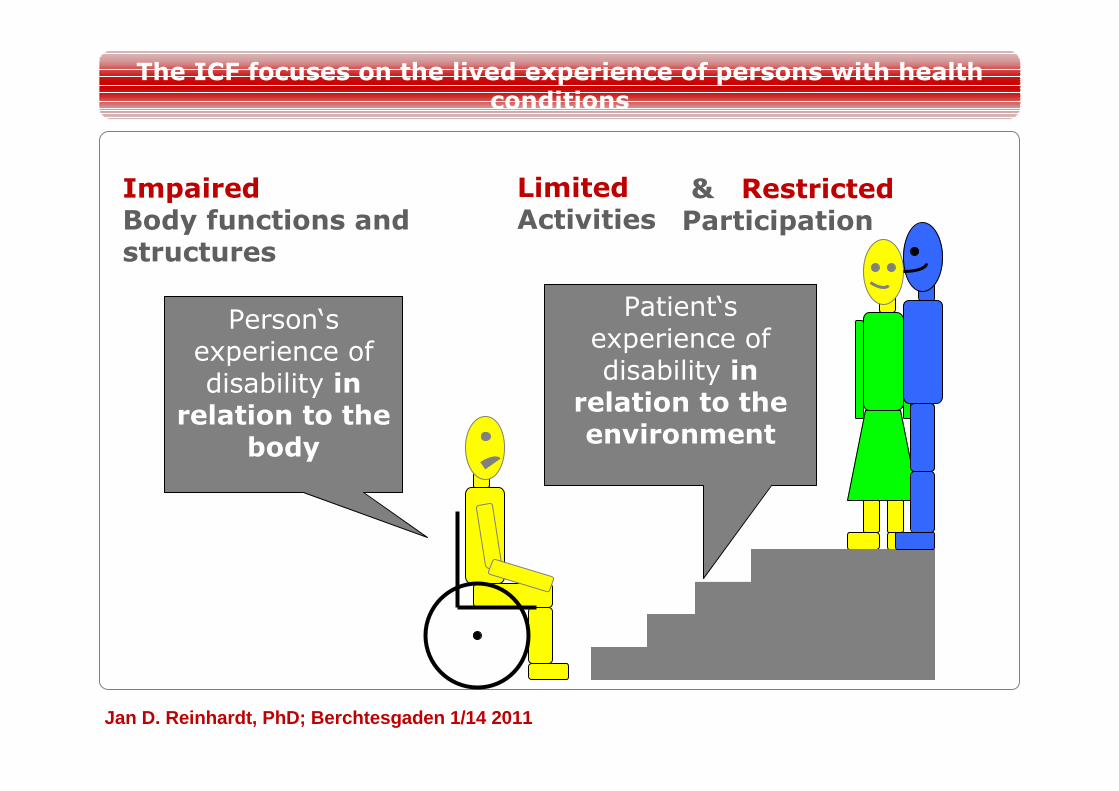
ImpairedBody functions and structures
LimitedActivities
& RestrictedParticipation
Person‘s experience of disability in relation to the
body
Patient‘s experience of disability in relation to the environment
The ICF focuses on the lived experience of persons with health conditions

Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
The lived experience is reflected at the levels of…
11
Body Structures
Activities
Participation
E.g., Joints (hands, fingers)
E.g., Manipulating objects
E.g.,Taking care of others
Body FunctionsE.g., Mobility and stability of joints
1. The ICF integrative bio-psycho-social model of functioning and disability
…in interaction with the environment.
= Functioning and Disability
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
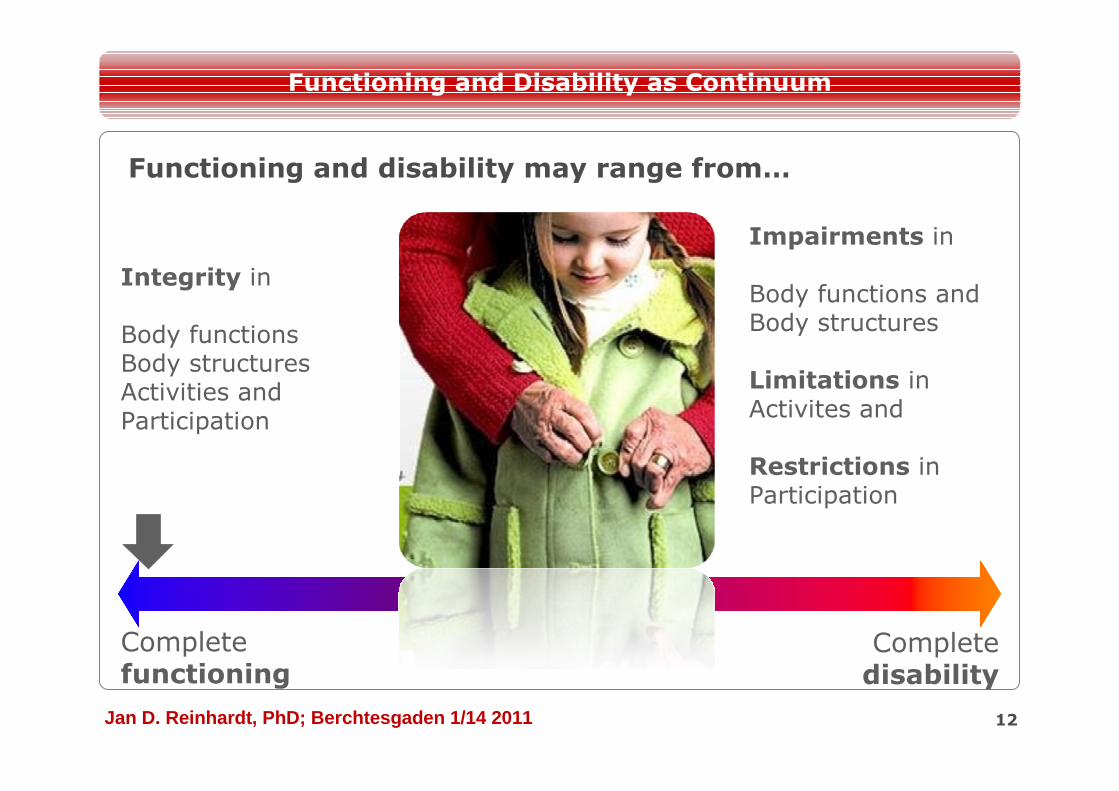
Functioning and disability may range from…
12
Functioning and Disability as Continuum
Complete functioning
Complete disability
Integrity in
Body functionsBody structuresActivities andParticipation
Impairments in
Body functions andBody structures
Limitations inActivites and
Restrictions inParticipation
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 13
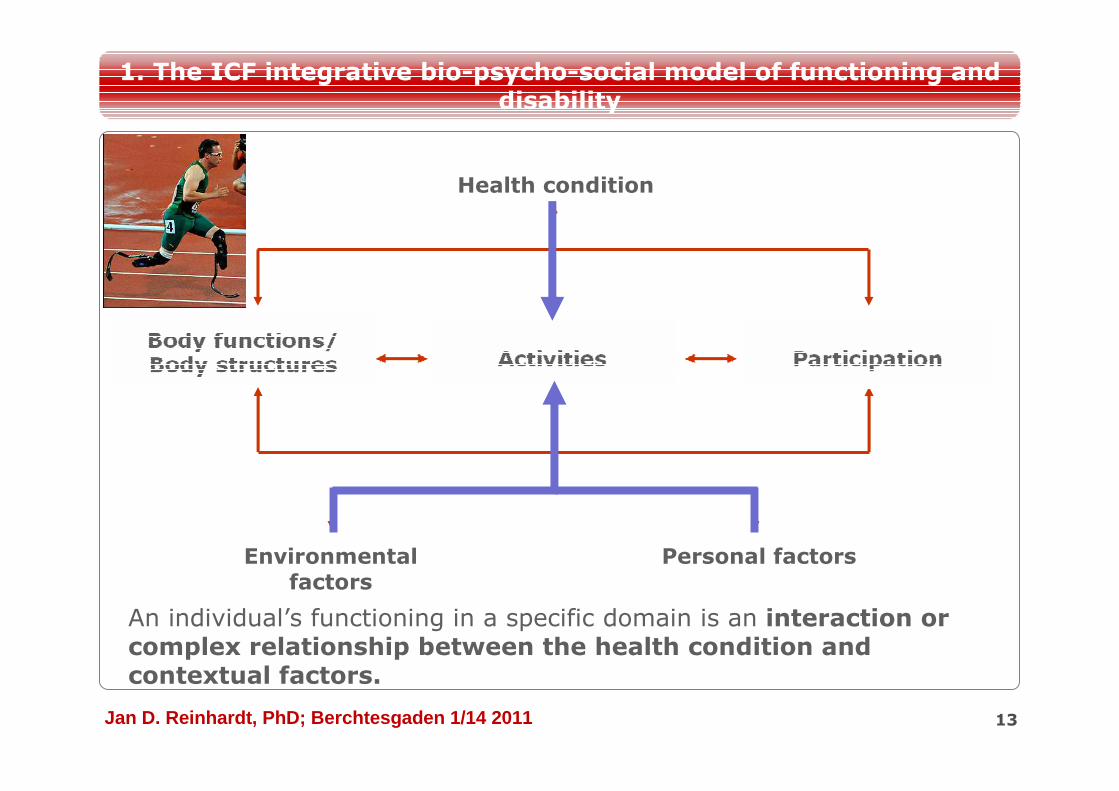
Personal factorsEnvironmental factors
Health condition
1. The ICF integrative bio-psycho-social model of functioning and disability
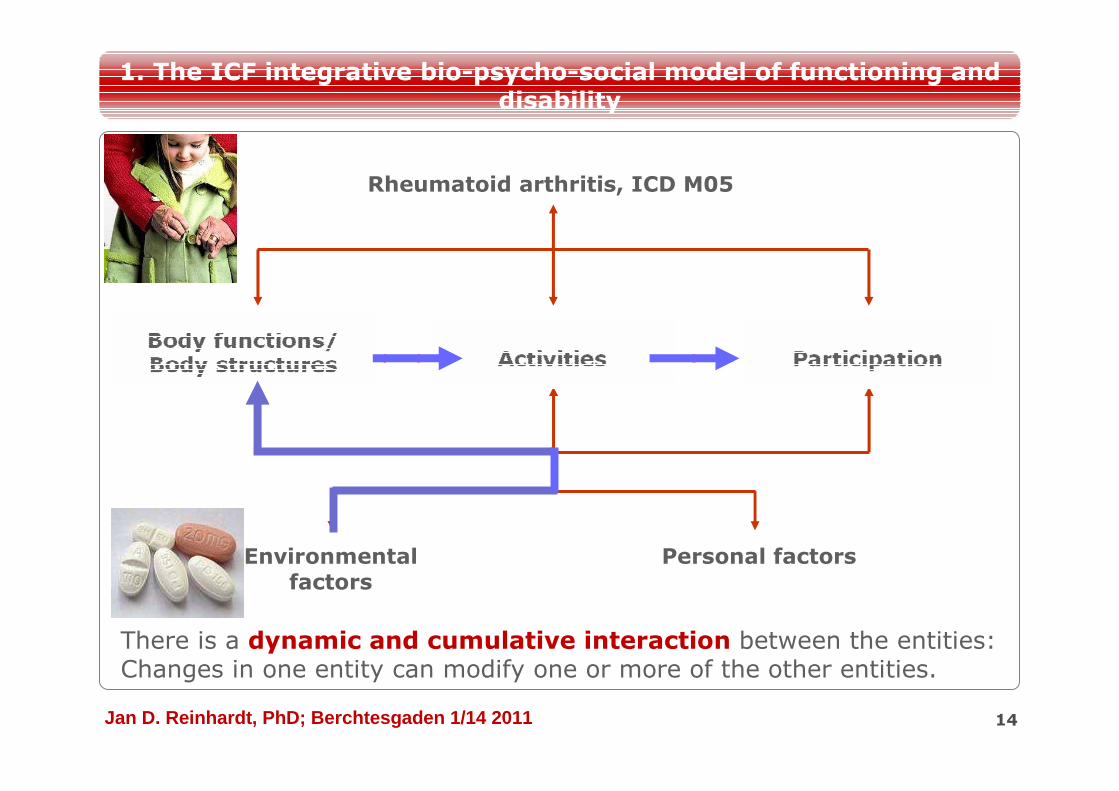
An individual’s functioning in a specific domain is an interaction or complex relationship between the health condition and contextual factors.
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 14
Health condition
Environmental factors
Personal factors
1. The ICF integrative bio-psycho-social model of functioning and disability
There is a dynamic and cumulative interaction between the entities: Changes in one entity can modify one or more of the other entities.
Rheumatoid arthritis, ICD M05
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 15
Health condition
Environmental factors
Personal factors
1. The ICF integrative bio-psycho-social model of functioning and disability
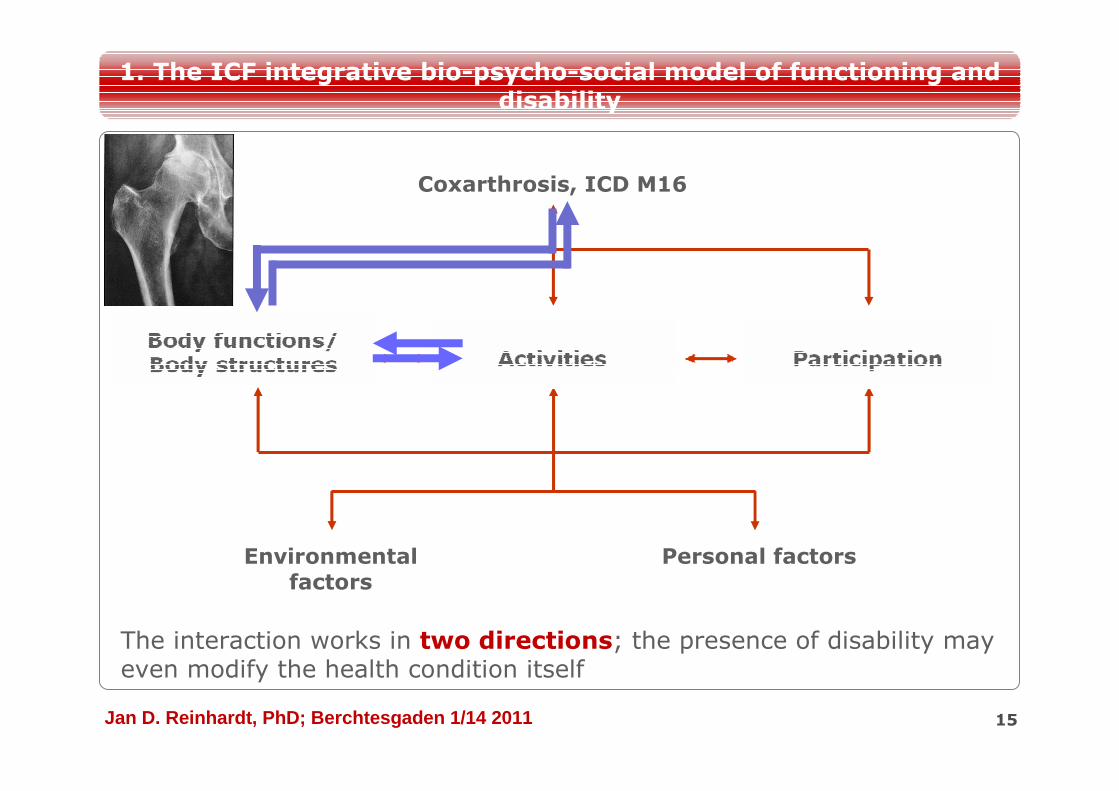
The interaction works in two directions; the presence of disability may even modify the health condition itself
Coxarthrosis, ICD M16
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 16
Health condition
Environmental factors
Personal factors
1. The ICF integrative bio-psycho-social model of functioning and disability
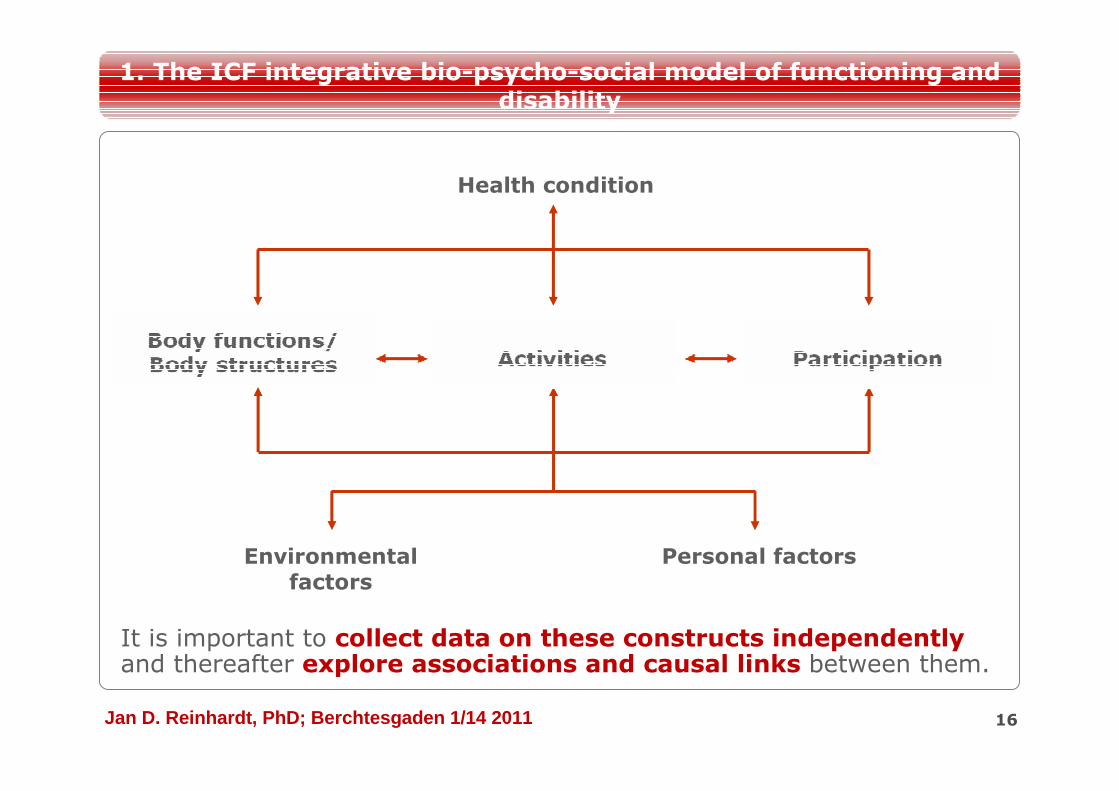
It is important to collect data on these constructs independently and thereafter explore associations and causal links between them.
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 17
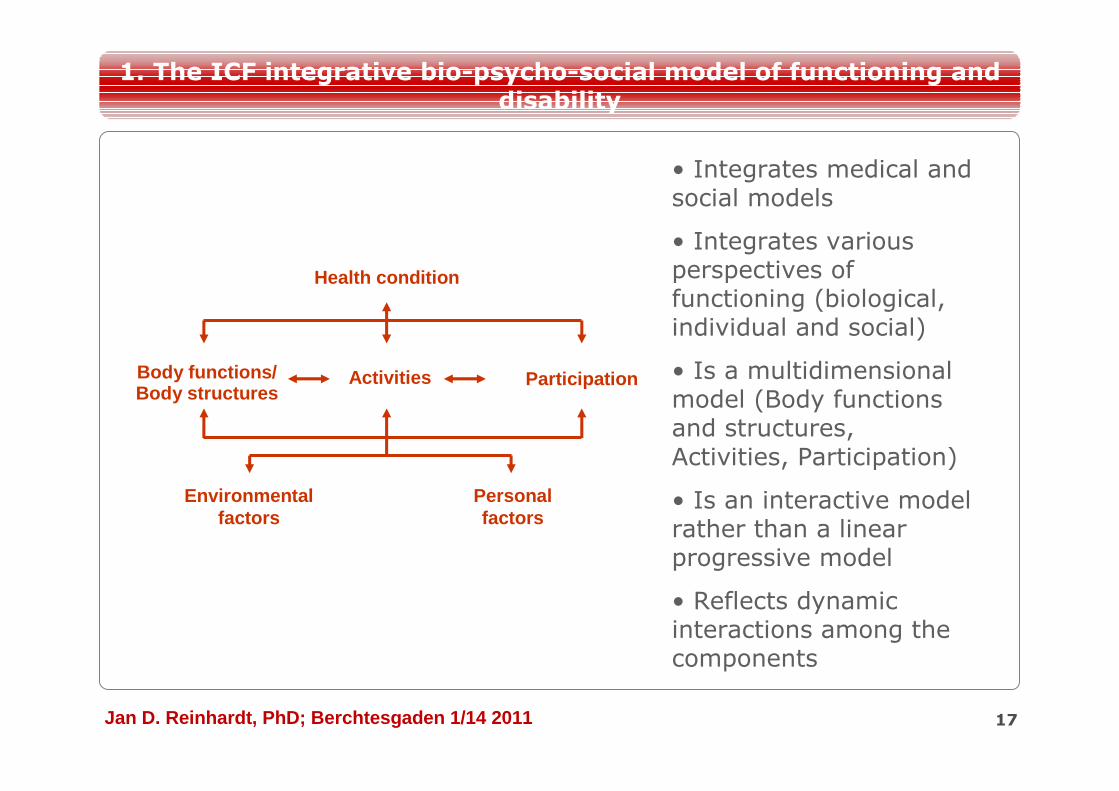
• Integrates medical and social models
• Integrates various perspectives of functioning (biological, individual and social)
• Is a multidimensional model (Body functions and structures, Activities, Participation)
• Is an interactive model rather than a linear progressive model
• Reflects dynamic interactions among the components
Health condition
Environmental factors
Personal factors
Body functions/ Body structures
Activities Participation
1. The ICF integrative bio-psycho-social model of functioning and disability
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
ICF is an universal model and applies to all people irrespective of their culture, health condition, gender, or age.
Instead of making disability a distinguishing mark of a discrete
minority group, the ICF describes all the domains of functioning
and disability that are applicable to everyone.
18
1. The ICF integrative bio-psycho-social model of functioning and disability
?
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
The ICF original version had neglected some aspects important
to children and youth as well as education and pediatric
rehabilitation. Therefore, the ICF-CY was created.
•The ICF-CY is derived classification.
•ICF-CY has additional categories such as play and preschool education.
•ICF-CY has incorporated developmental delay in definition of impairment and activity limitation qualifiers.
• ICF-CY has modified several exclusion and inclusion criteria
for particular categories.
19
1. The ICF integrative bio-psycho-social model of functioning and disability
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 20
2. ICF als Klassifikation
F:\Bilder\Barcelona 09\Barcelona\DSC_0023.JPG
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
ICF as classification
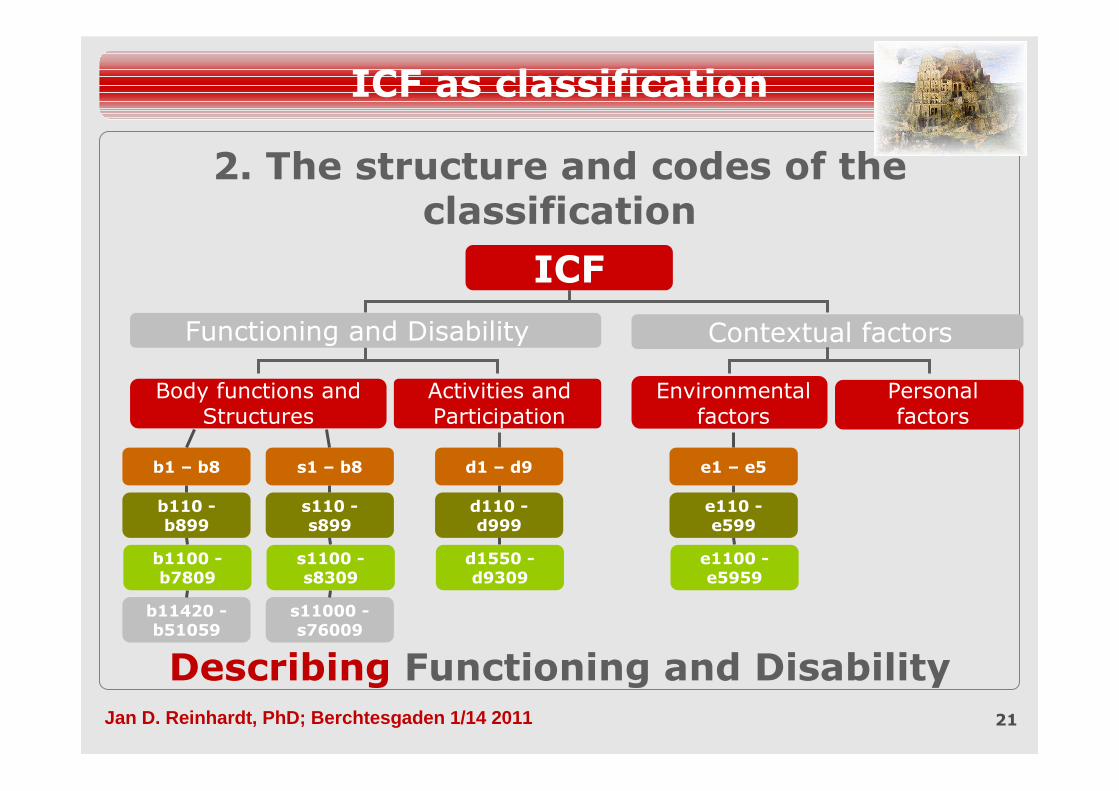
2. The structure and codes of the classification
21
Describing Functioning and Disability
b11420 -b51059
s11000 -s76009
b1100 -b7809
s1100 -s8309
d1550 -d9309
e1100 -e5959
b110 -b899
s110 -s899
d110 -d999
e110 -e599
b1 – b8 s1 – b8 d1 – d9 e1 – e5
ICF
Contextual factors
Body functions and Structures
Activities and Participation
Environmental factors
Personal factors
Functioning and Disability
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Typically, classification is the placing of similar objects into groups
22
2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Hierarchical structure
23
2. The structure and codes of the ICF
Andere Möglichkeiten?
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 24
Health condition
Environmental factors Personal factors
Body functions/ Body structures
Activities Participation
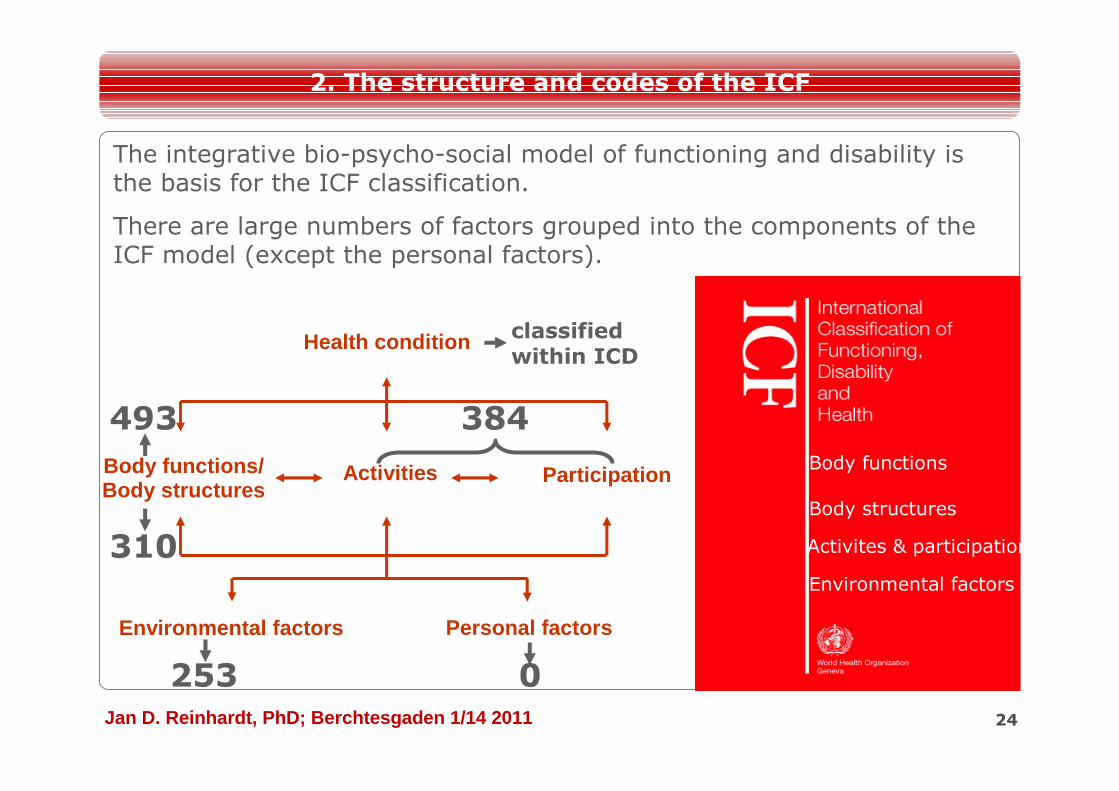
493 384
253
310
0
The integrative bio-psycho-social model of functioning and disability is the basis for the ICF classification.
There are large numbers of factors grouped into the components of the ICF model (except the personal factors).
classified within ICD
Body functions
Body structures
Activites & participation
Environmental factors
2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 25
ICF
Functioning and Disability Contextual factors
Body functions and Structures
Activities and Participation
Environmental factors
Personal factors
Body functions
Body structures
PartsComponents
b11420 -b51059
s11000 -s76009
Fourth-level classification
b1100 -b7809
s1100 -s8309
d1550 -d9309
e1100 -e5959
Third-level classification
b110 -b899
s110 -s899
d110 -d999
e110 -e599
Second-level classification
b1 – b8 s1 – b8 d1 – d9 e1 – e5
Chapters
ICF code = Prefixes + Numeric codes + ICF Qualifiers
bb ss dd ee
Not classified yet!
2. The structure and codes of the ICF
110110 5400254002 44014401 11011101
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 26
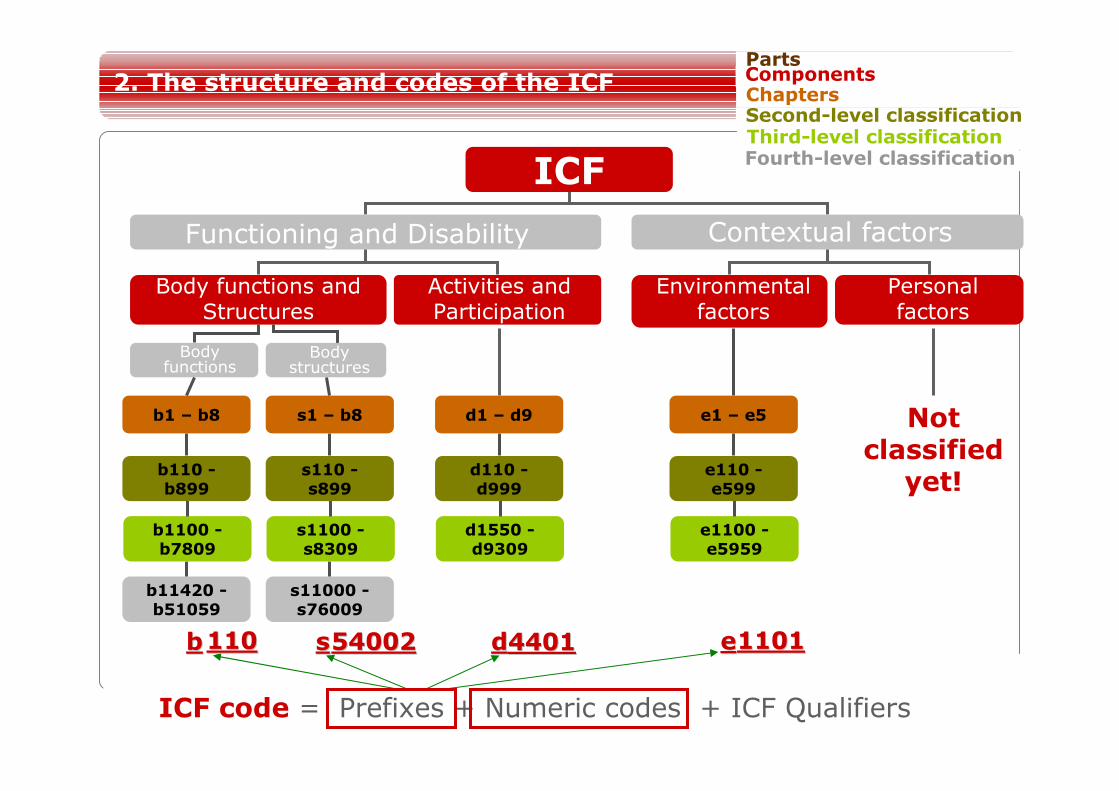
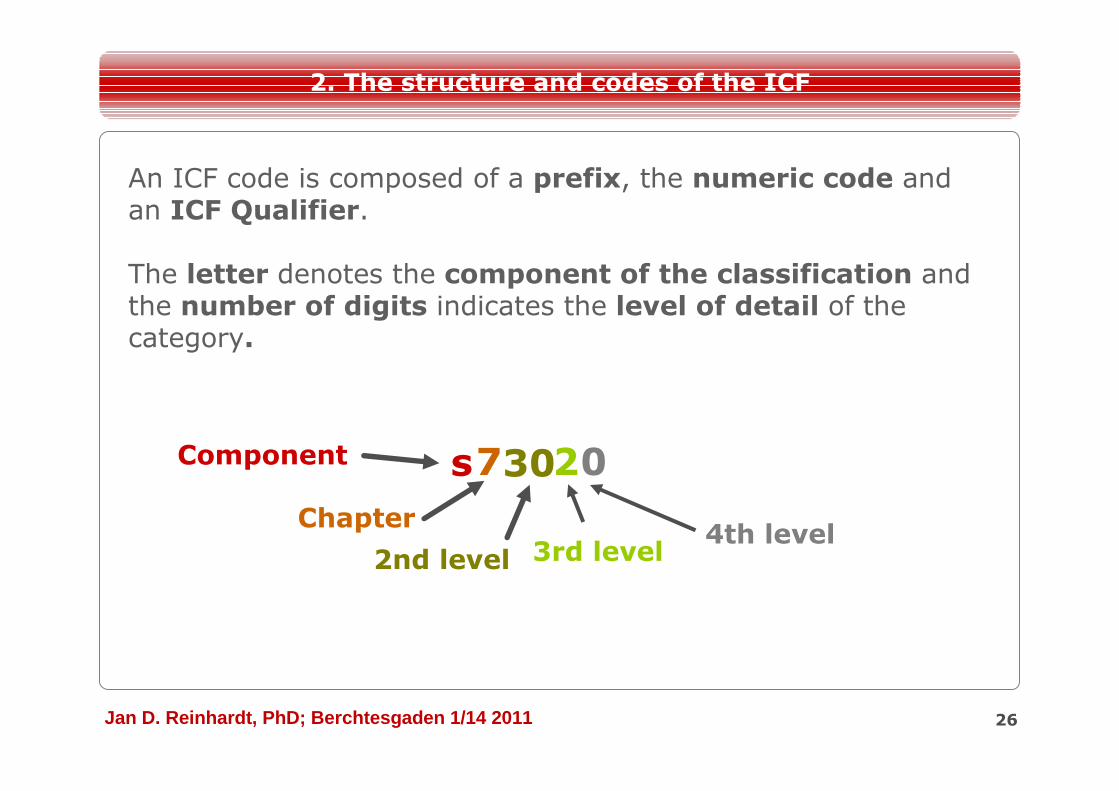
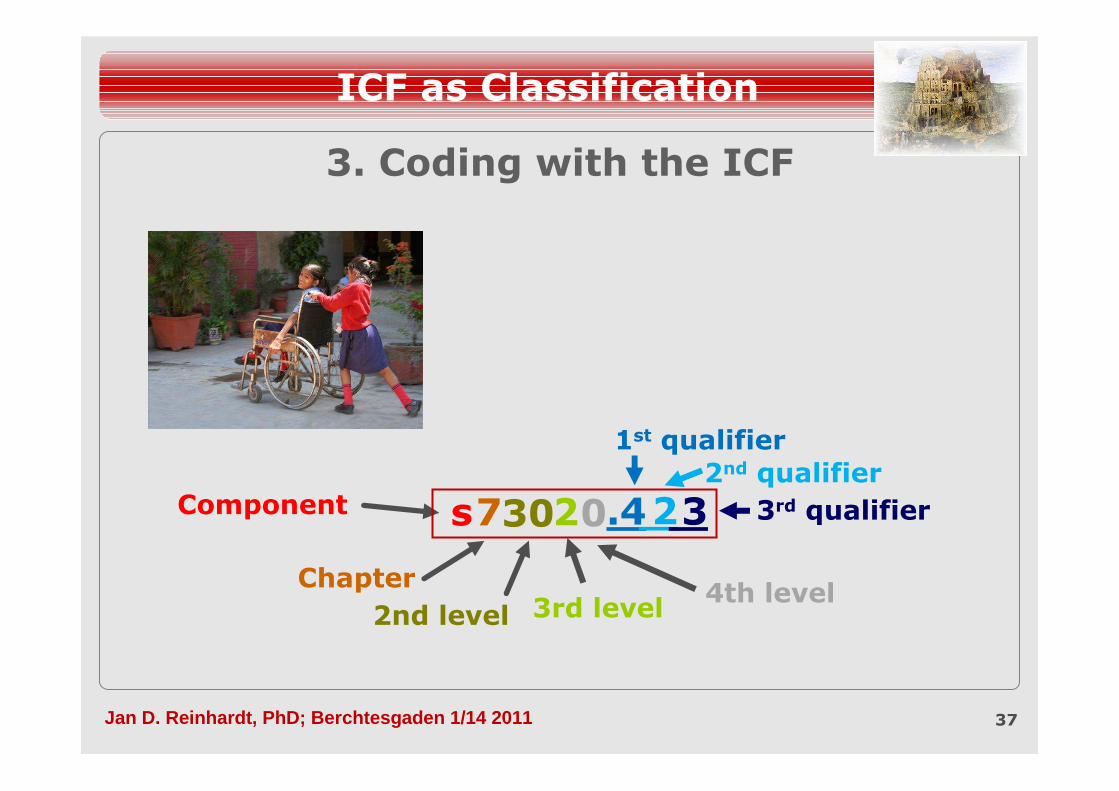
An ICF code is composed of a prefix, the numeric code and an ICF Qualifier.
The letter denotes the component of the classification and the number of digits indicates the level of detail of the category.
Component sChapter
7
2nd level
30
3rd level
2
4th level
0
2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
The classification provides a standard language and a common framework for the description of health and health related domains
“ICF does not classify people, but describes the situation of each person within an array of health or health-related domains.”(WHO 2001:8)
27
2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
b3
b5
b8
b2
b4
b7
b6
b1
28
ICF
Functioning and Disability Contextual factors
Body functions and Structures
Activities and Participation
Environmental factors
Personal factors
Body functions
Body structures
Chapters
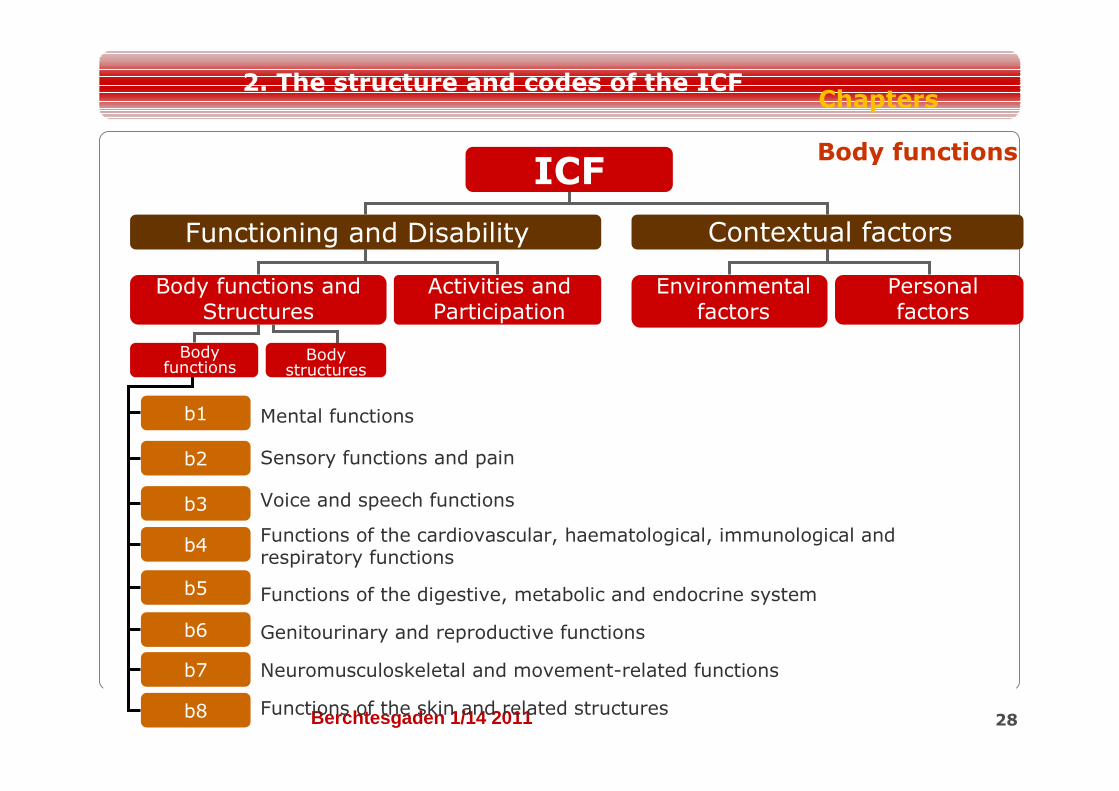
Body functions
Mental functions
Sensory functions and pain
Voice and speech functions
Functions of the cardiovascular, haematological, immunological and respiratory functions
Functions of the digestive, metabolic and endocrine system
Genitourinary and reproductive functions
Neuromusculoskeletal and movement-related functions
Functions of the skin and related structures
2. The structure and codes of the ICF
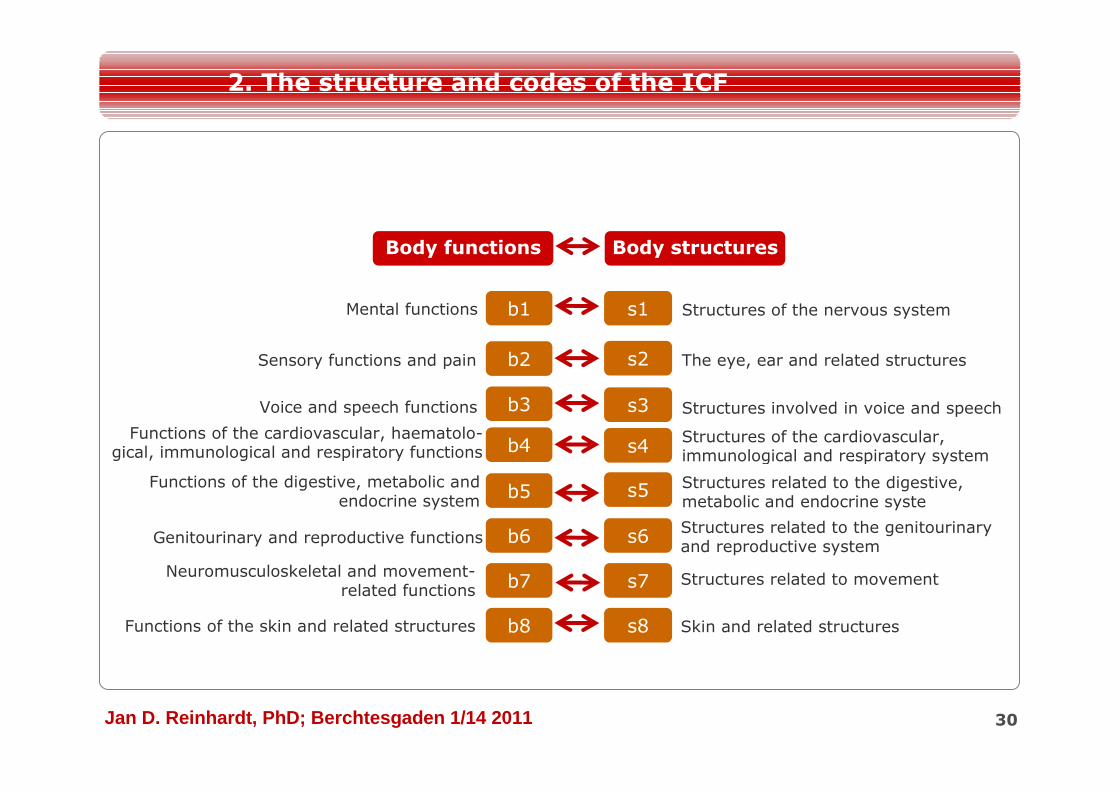
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 29
ICF
s2
s3
s4
s5
s6
s7
s8
s1
Functioning and Disability Contextual factors
Body functions and Structures
Activities and Participation
Environmental factors
Personal factors
Body functions
Body structures
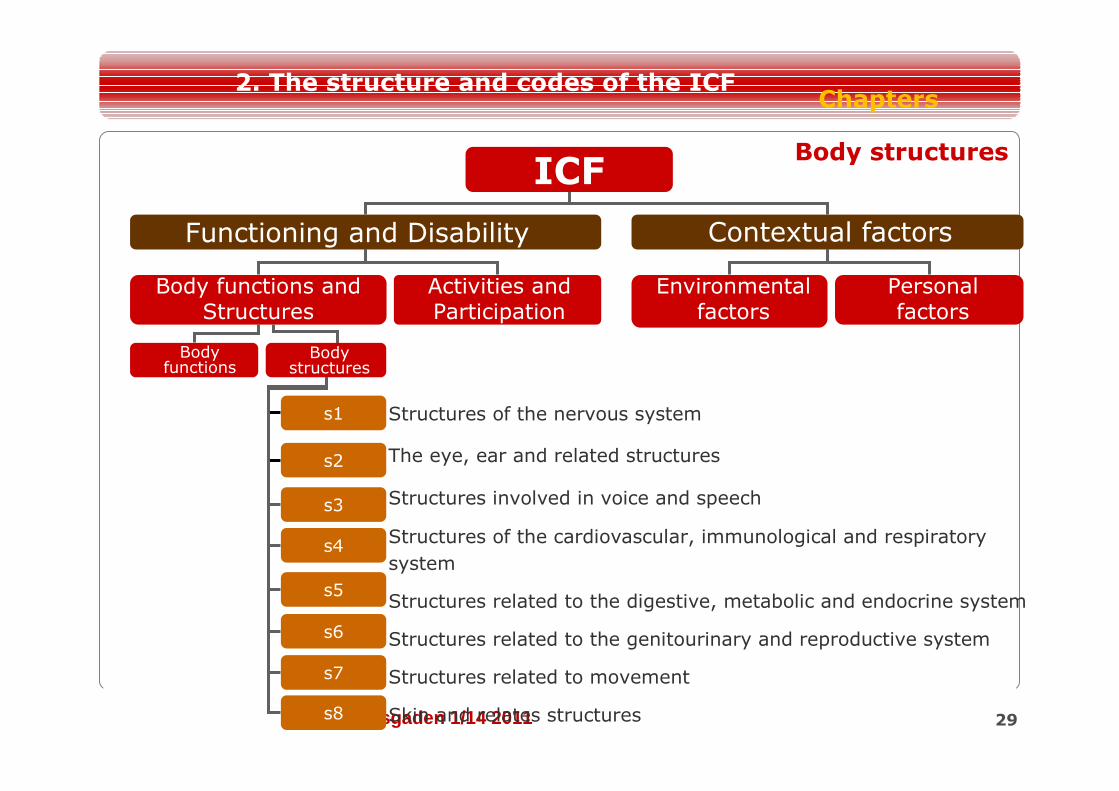
Structures of the nervous system
The eye, ear and related structures
Structures involved in voice and speech
Structures of the cardiovascular, immunological and respiratory
system
Structures related to the digestive, metabolic and endocrine system
Structures related to the genitourinary and reproductive system
Structures related to movement
Skin and relates structures
Body structures
Chapters2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 30
b3
b5
b8
b2
b4
b7
b6
b1Mental functions
s2
s3
s4
s5
s6
s7
s8
s1 Structures of the nervous system
2. The structure and codes of the ICF
Body functions Body structures
The eye, ear and related structures
Structures involved in voice and speech
Structures of the cardiovascular, immunological and respiratory system
Structures related to the digestive, metabolic and endocrine syste
Structures related to the genitourinary and reproductive system
Structures related to movement
Skin and related structures
Sensory functions and pain
Voice and speech functions
Functions of the cardiovascular, haematolo-gical, immunological and respiratory functions
Functions of the digestive, metabolic and endocrine system
Genitourinary and reproductive functions
Neuromusculoskeletal and movement-related functions
Functions of the skin and related structures
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 31
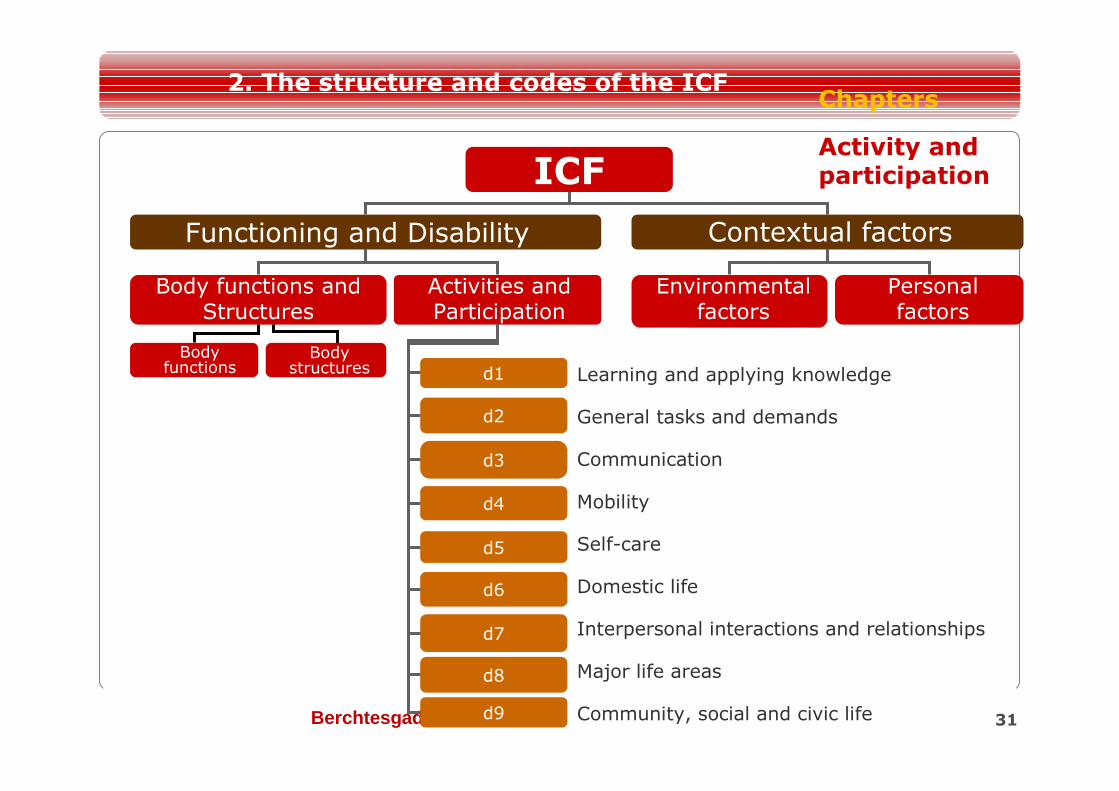
ICF
Functioning and Disability Contextual factors
Body functions and Structures
Activities and Participation
Environmental factors
Personal factors
Body functions
Body structures d1
d2
d3
d4
d5
d6
d7
d8
d9
Learning and applying knowledge
General tasks and demands
Communication
Mobility
Self-care
Domestic life
Interpersonal interactions and relationships
Major life areas
Community, social and civic life
Activity and participation
Chapters2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 32
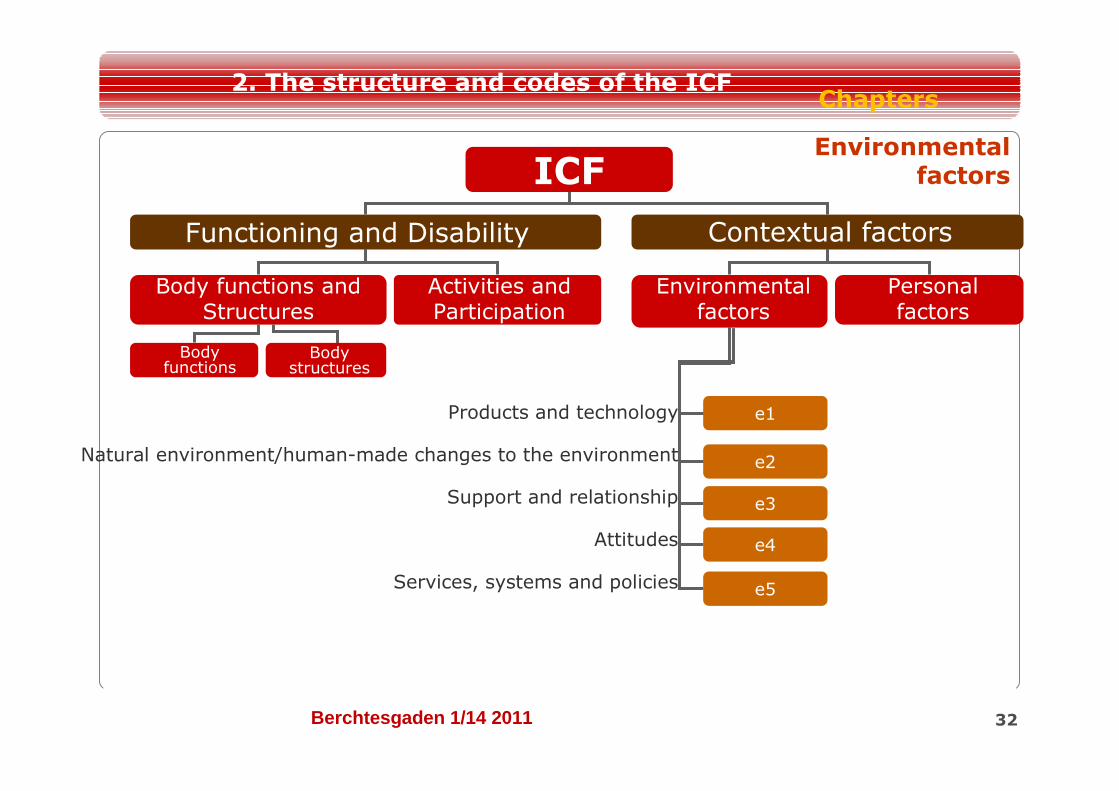
ICF
Functioning and Disability Contextual factors
Body functions and Structures
Activities and Participation
Environmental factors
Personal factors
Body functions
Body structures
e2
e1
e3
e4
e5
Products and technology
Natural environment/human-made changes to the environment
Support and relationship
Attitudes
Services, systems and policies
Environmental factors
Chapters2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
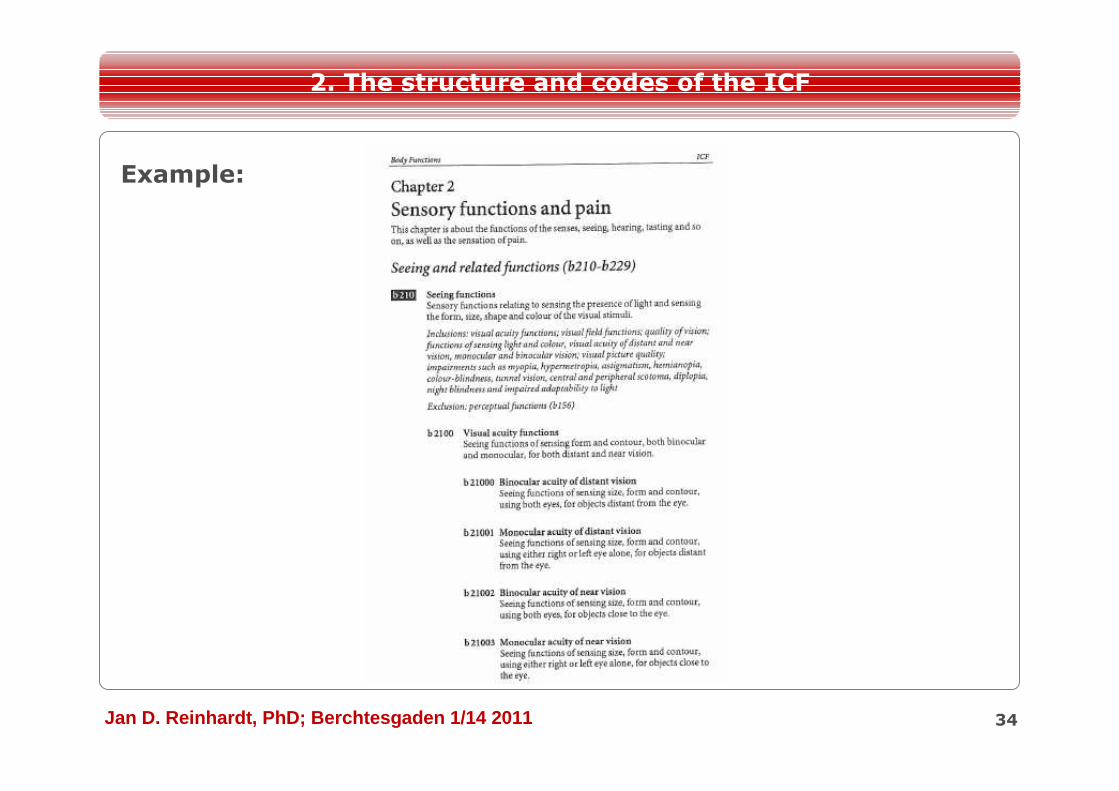
The hierarchical structure of the classification allows either a broader (chapter or 2nd level classification) or a more specific (3rd or 4thlevel classification) description of functioning. Broader categories include the more detailed categories of the parent category.
Within each domain, the specificity of the description of an ICF category increases.
For each category (2nd, 3rd or 4th level) you can find a definition(except in the component of Body structures) together with inclusion and exclusion criteria.
33
2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 34
2. The structure and codes of the ICF
Example:
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 35
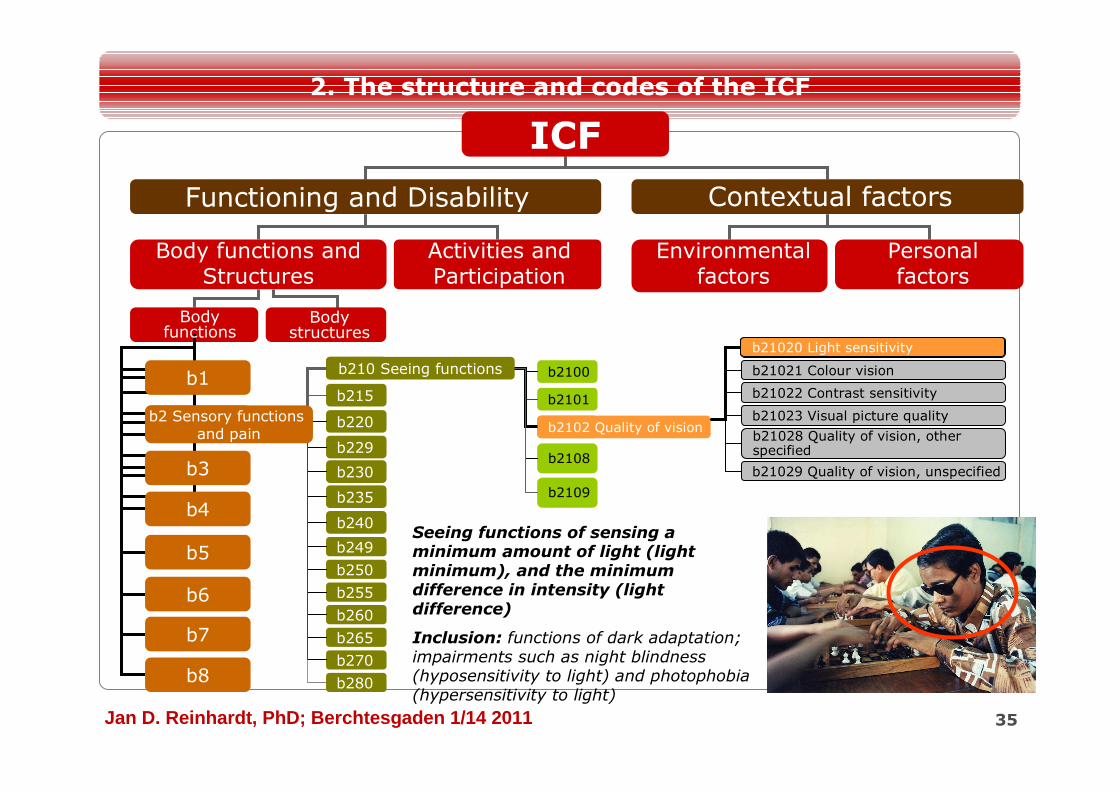
b210b210 Seeing functions
b2102b2102 Quality of vision
b2100
b2101
b2108
b2109
ICF
b3
b5
b8
b2
b4
b7
b6
b1
Functioning and Disability Contextual factors
Body functions and Structures
Activities and Participation
Environmental factors
Personal factors
Body functions
Body structures
b21020 Light sensitivity
b21021 Colour vision
b21022 Contrast sensitivity
b21023 Visual picture quality
b21028 Quality of vision, other specified
b21029 Quality of vision, unspecified
b280
b215
b220
b229
b230
b235
b240
b249
b250
b255
b260
b265
b270
b2 Sensory functions and pain
b21020 Light sensitivity
Seeing functions of sensing a minimum amount of light (light minimum), and the minimum difference in intensity (light difference)
Inclusion: functions of dark adaptation; impairments such as night blindness (hyposensitivity to light) and photophobia (hypersensitivity to light)
2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 36
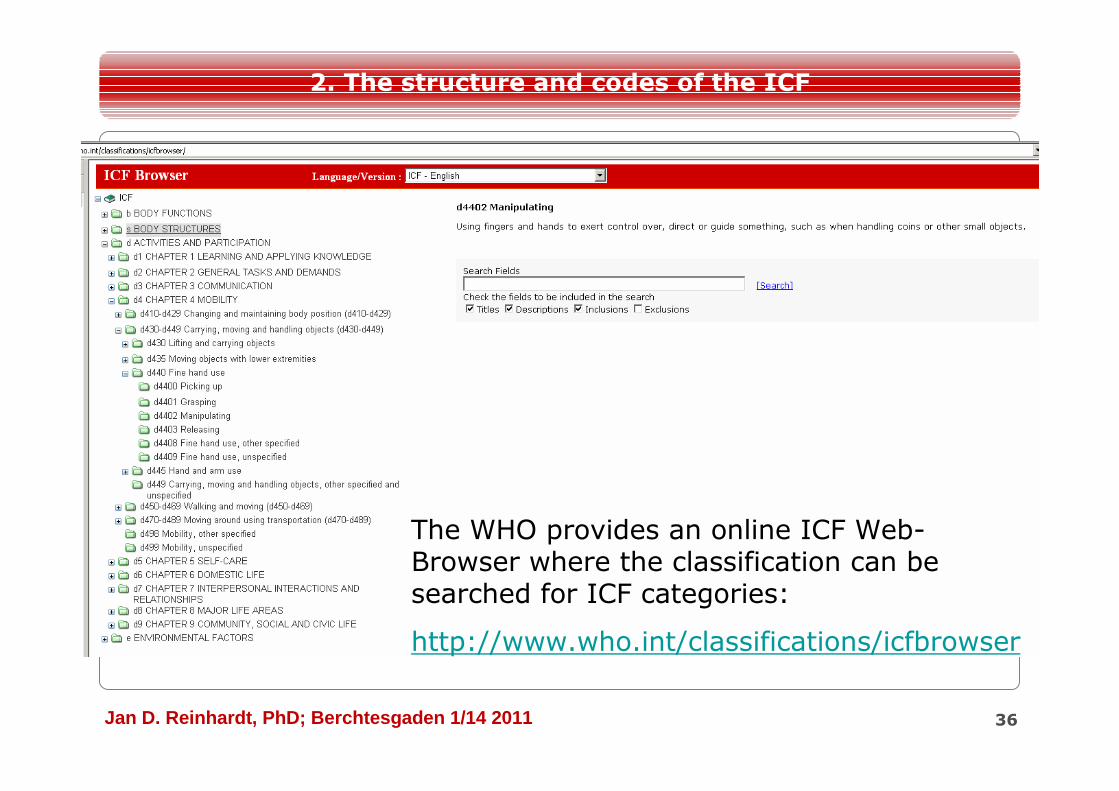
The WHO provides an online ICF Web-Browser where the classification can be searched for ICF categories:
http://www.who.int/classifications/icfbrowser
2. The structure and codes of the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
ICF as Classification
3. Coding with the ICF
37
Component s
Chapter2nd level
30
3rd level
2
4th level
07 .4
1st qualifier
22nd qualifier
3 3rd qualifier
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
3. Coding with ICF qualifiers
38
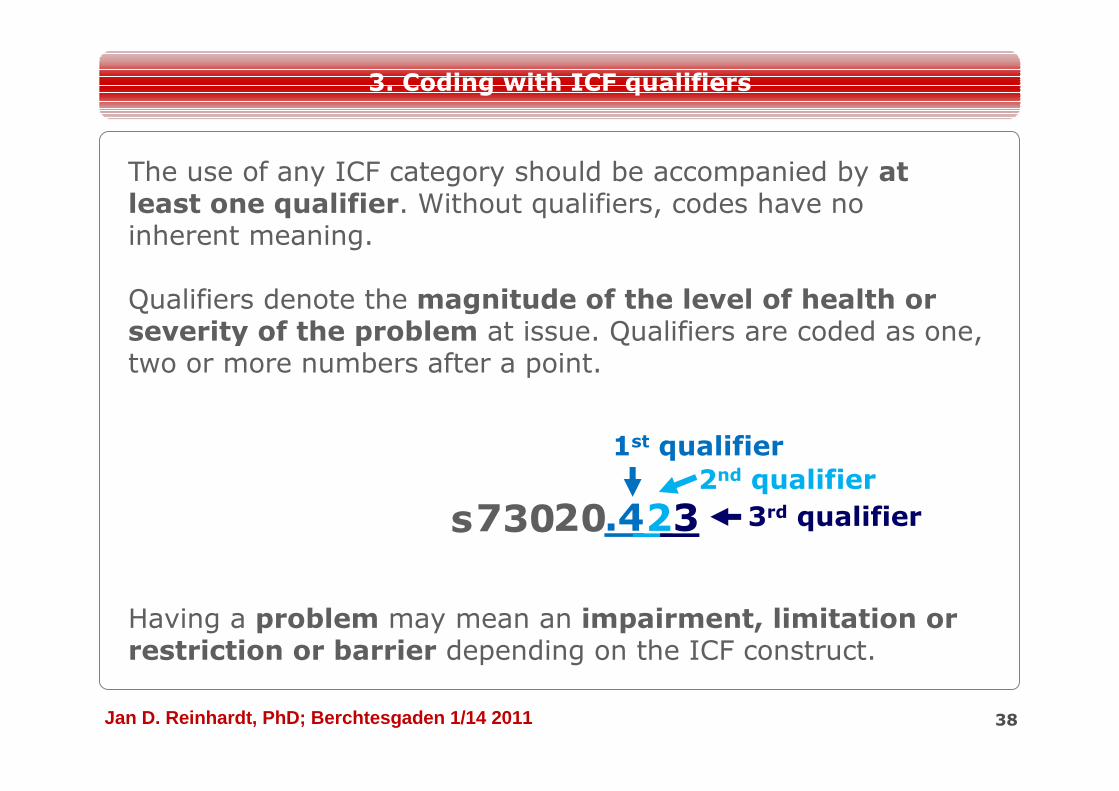
The use of any ICF category should be accompanied by at least one qualifier. Without qualifiers, codes have no inherent meaning.
Qualifiers denote the magnitude of the level of health or severity of the problem at issue. Qualifiers are coded as one, two or more numbers after a point.
Having a problem may mean an impairment, limitation or restriction or barrier depending on the ICF construct.
s73020.4
1st qualifier
22nd qualifier
3 3rd qualifier
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 39
ICF
Functioning and Disability
Body functions and Structures
Activities and Participation
Body functions
Body structures
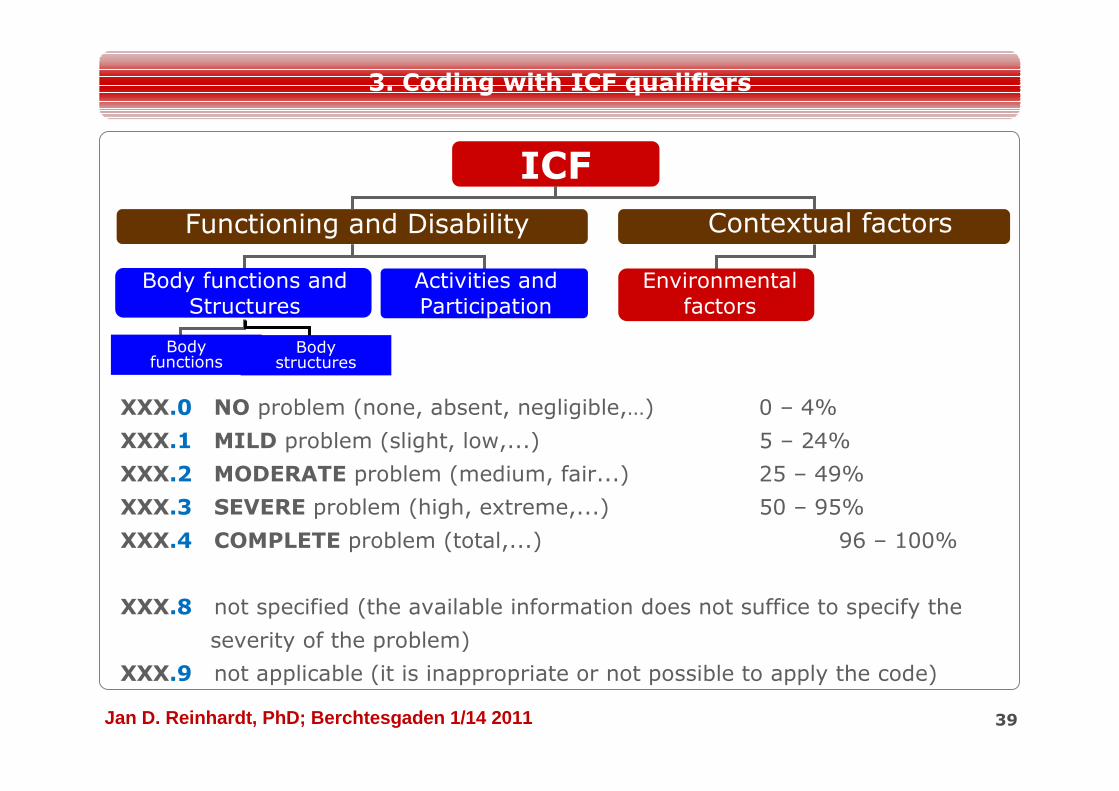
XXX.0 NO problem (none, absent, negligible,…) 0 – 4%
XXX.1 MILD problem (slight, low,...) 5 – 24%
XXX.2 MODERATE problem (medium, fair...) 25 – 49%
XXX.3 SEVERE problem (high, extreme,...) 50 – 95%
XXX.4 COMPLETE problem (total,...) 96 – 100%
XXX.8 not specified (the available information does not suffice to specify the
severity of the problem)
XXX.9 not applicable (it is inappropriate or not possible to apply the code)
Contextual factors
Environmental factors
3. Coding with ICF qualifiers
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 40
ICF
Functioning and Disability Contextual factors
Body functions and structures
Activities and Participation
Environmental factors
Body functions
Body structures
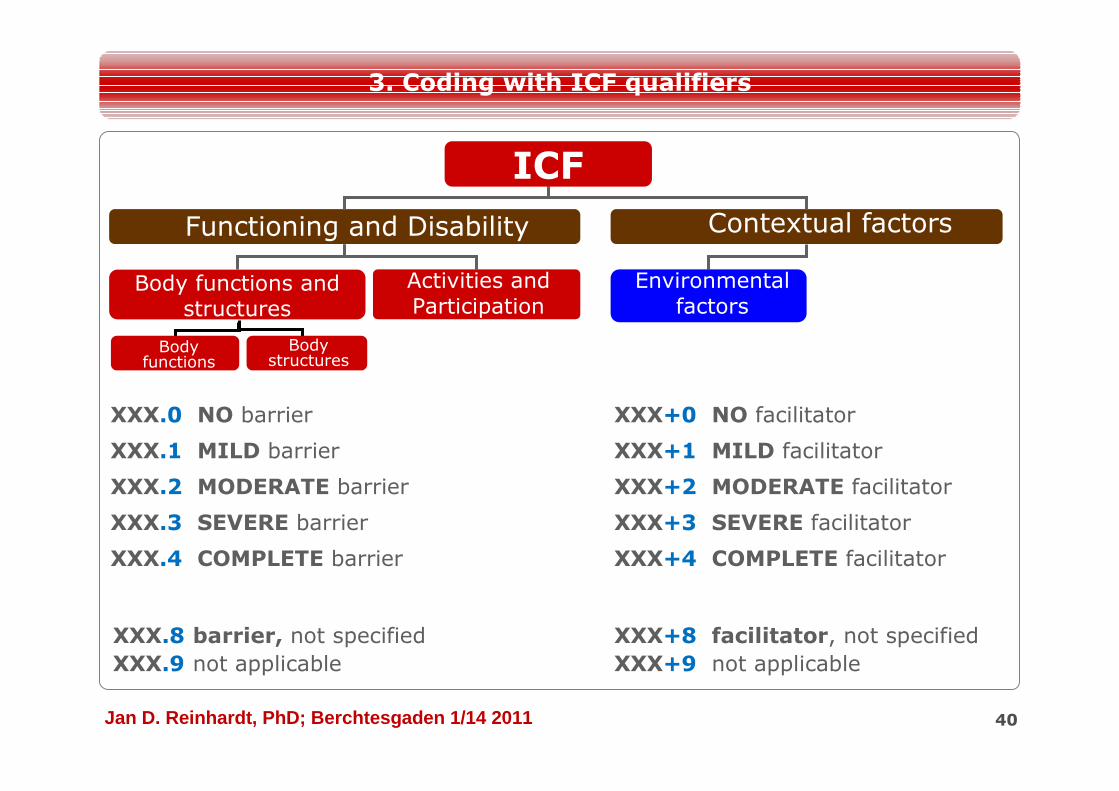
XXX.0 NO barrier
XXX.1 MILD barrier
XXX.2 MODERATE barrier
XXX.3 SEVERE barrier
XXX.4 COMPLETE barrier
XXX+0 NO facilitator
XXX+1 MILD facilitator
XXX+2 MODERATE facilitator
XXX+3 SEVERE facilitator
XXX+4 COMPLETE facilitator
XXX.8 barrier, not specified XXX+8 facilitator, not specifiedXXX.9 not applicable XXX+9 not applicable
3. Coding with ICF qualifiers
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
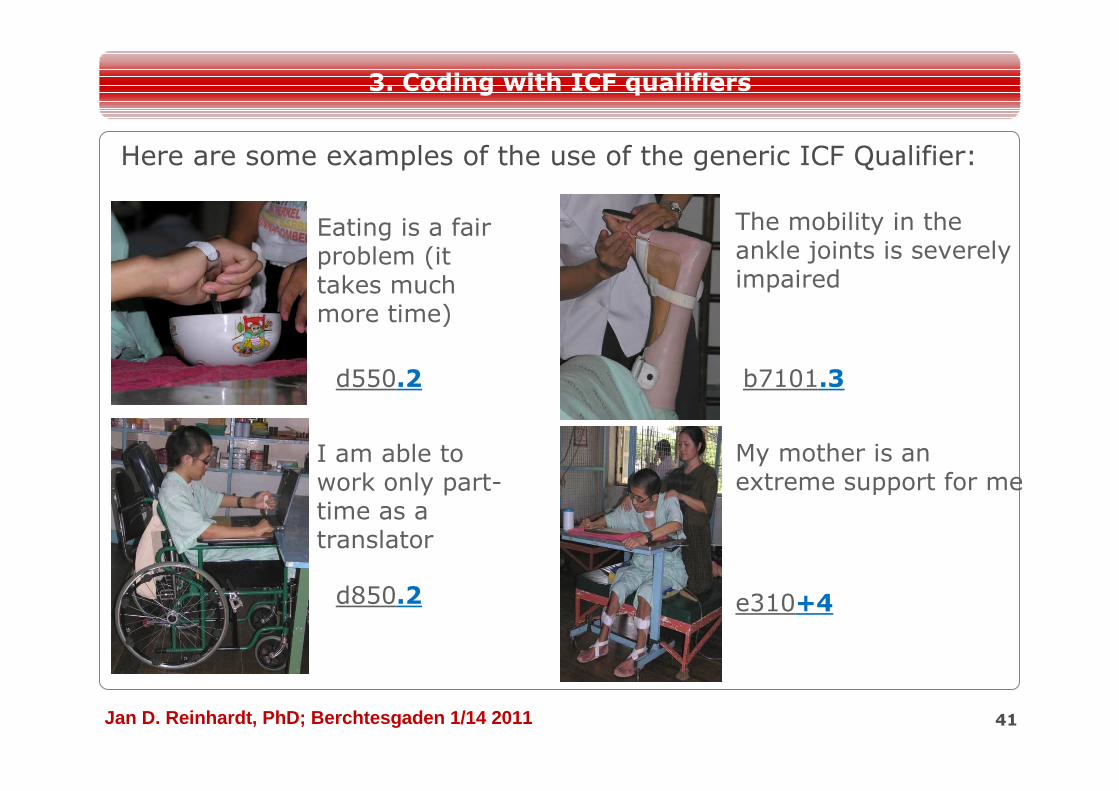
Here are some examples of the use of the generic ICF Qualifier:
41
Eating is a fair problem (it takes much more time)
My mother is an extreme support for me
The mobility in the ankle joints is severely impaired
I am able to work only part-time as a translator
d550.2 b7101.3
d850.2 e310+4
3. Coding with ICF qualifiers
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 42
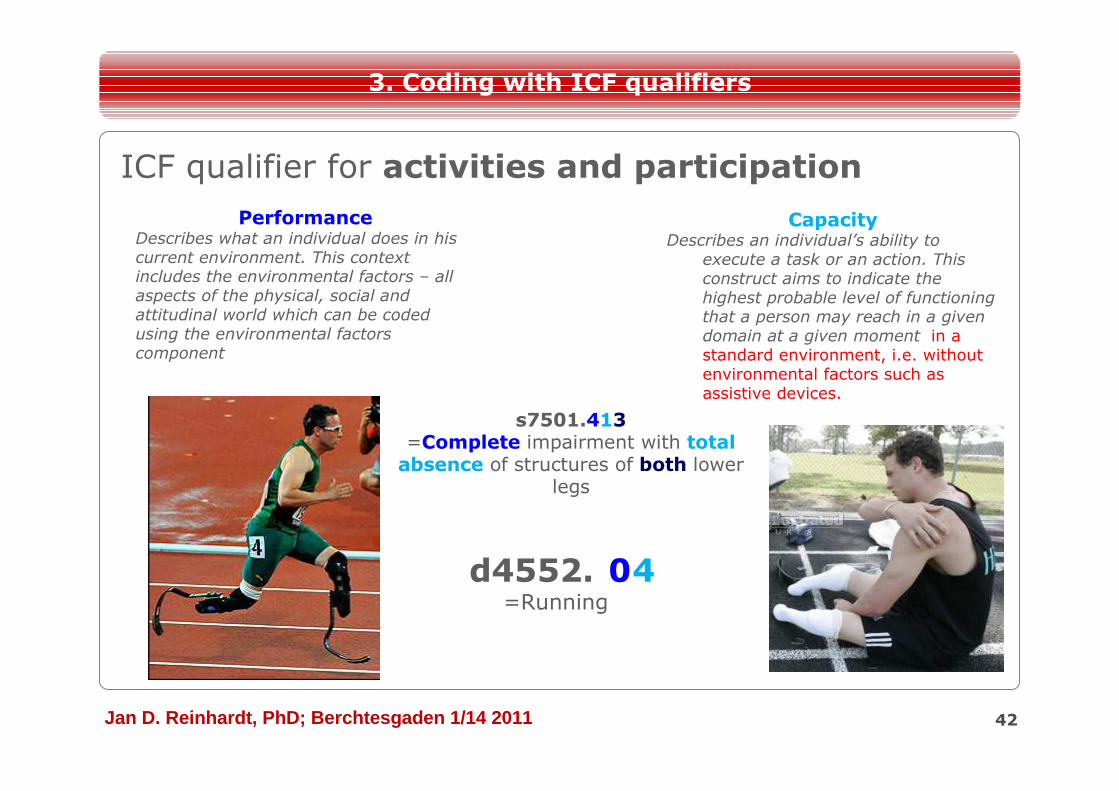
3. Coding with ICF qualifiers
ICF qualifier for activities and participation
PerformanceDescribes what an individual does in his current environment. This context includes the environmental factors – all aspects of the physical, social and attitudinal world which can be coded using the environmental factors component
CapacityDescribes an individual’s ability to
execute a task or an action. This construct aims to indicate the highest probable level of functioning that a person may reach in a given domain at a given moment in a standard environment, i.e. without environmental factors such as assistive devices.
d4552.XX=Running
s7501.413=Complete impairment with total absence of structures of both lower
legs
40
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 43
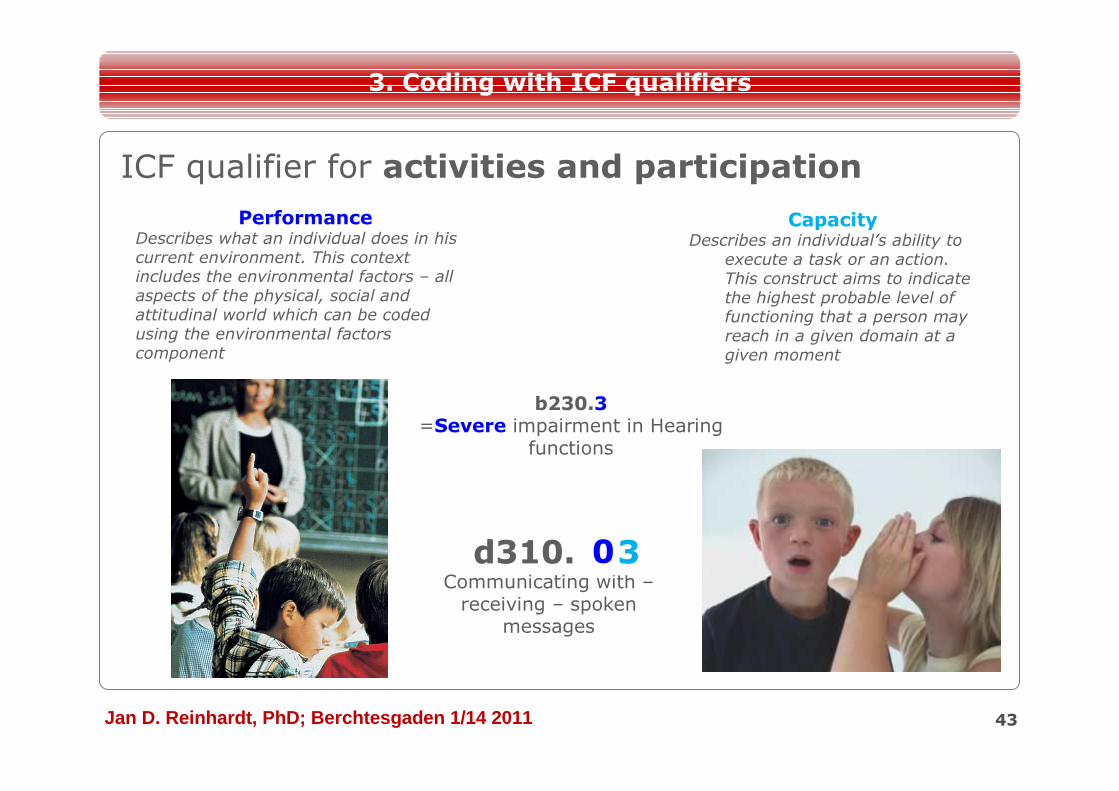
3. Coding with ICF qualifiers
ICF qualifier for activities and participation
PerformanceDescribes what an individual does in his current environment. This context includes the environmental factors – all aspects of the physical, social and attitudinal world which can be coded using the environmental factors component
CapacityDescribes an individual’s ability to
execute a task or an action. This construct aims to indicate the highest probable level of functioning that a person may reach in a given domain at a given moment
d310.XXCommunicating with –receiving – spoken
messages
b230.3=Severe impairment in Hearing
functions
30
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
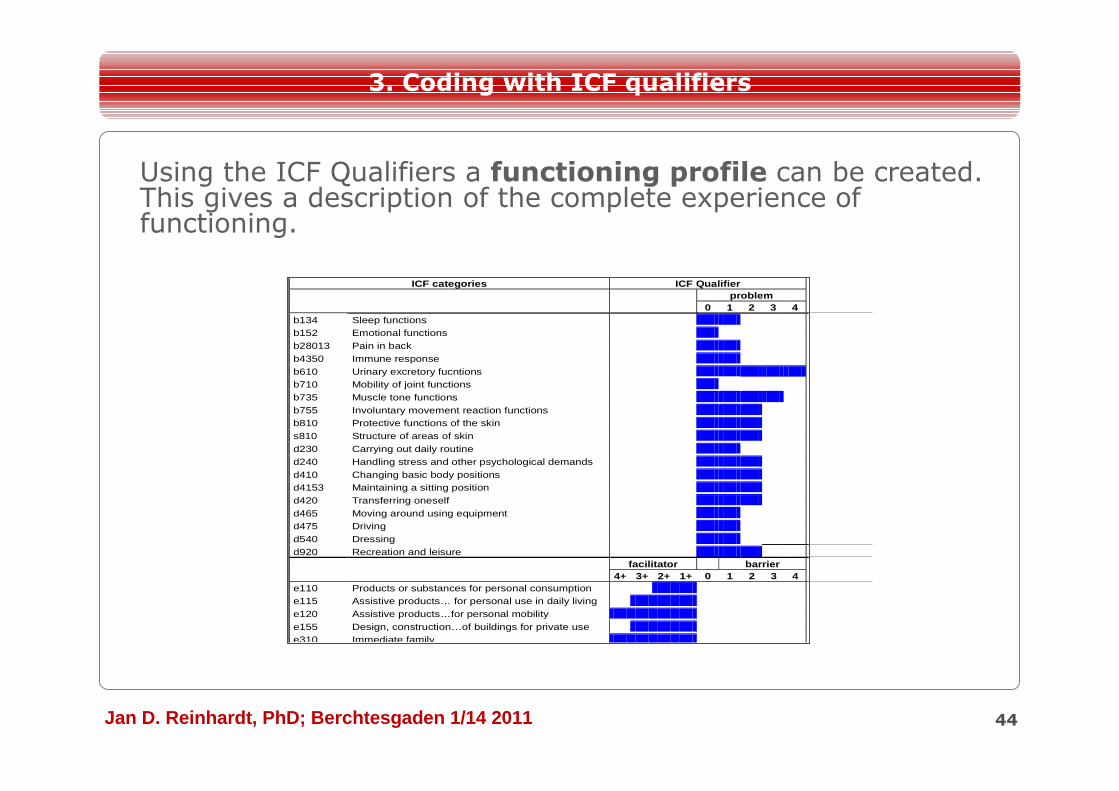
Using the ICF Qualifiers a functioning profile can be created. This gives a description of the complete experience of functioning.
ICF categories ICF Qualifier problem
0 1 2 3 4 b134 Sleep functions b152 Emotional functions b28013 Pain in back b4350 Immune response b610 Urinary excretory fucntions b710 Mobility of joint functions b735 Muscle tone functions b755 Involuntary movement reaction functions b810 Protective functions of the skin s810 Structure of areas of skin d230 Carrying out daily routine d240 Handling stress and other psychological demands d410 Changing basic body positions d4153 Maintaining a sitting position d420 Transferring oneself d465 Moving around using equipment d475 Driving d540 Dressing d920 Recreation and leisure
facilitator barrier 4+ 3+ 2+ 1+ 0 1 2 3 4 e110 Products or substances for personal consumption e115 Assistive products… for personal use in daily living e120 Assistive products…for personal mobility e155 Design, construction…of buildings for private use e310 Immediate family
44
3. Coding with ICF qualifiers
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 45
The linking methodology allows the use the ICF
standard vocabulary to facilitate
• understanding the meaning of health and health
related information
• comparsion of information from different
sources
4.1 Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
J Rehabil Med 2002~ 34: 205-210
SPECIAL REPORT
LINKING HEALTH-STATUS MEASUREMENTS TO THE INTERNATIONALCLASSIFICATION OF FUNCTIONING, DISABILITY AND HEALTH
Alarcos Cieza, Thomas Brockow , Thomas Ewert, Edda Amman, Barbara Kollerits,Somnath Chatterj , T. Berdihan Üstün and Gerold Stucki
From the Department of Physical Medicine and Rehabilitation, University of Munich, Munich, Spa Medicine ResearchInstitute, Bad Elster, Germany and Classification, Assessment, Surveys and Terminology Team, World Health Organization,
Switzerland.
With the approval of the International Classification of Functioning, Disability and Health by the World Health Assembly in May 2001,the concurrent use of both healthstatus measures and the International Classification of Functioning, Disability and Health is expected.It is therefore important to understand the relationship between these two concepts. The objective of this paper is to provide asystematic and standardized approach when linking healthstatus measures to the International Classification of Functioning, Disabilityand Health. The specific aims are to develop rules, to test their reliability and to illustrate these rules with examples. Ten linking rulesand an example of their use are presented in this paper. The percentage agreement between two health professionals for 8 healthstatusinstruments tested is also presented. A high level of agreement between the health professionals reflects that the linking rulesestablished in this study allow the sound linking of items from health-status measures to the International Classification of Functioning,Disability and Health.
Keywords: ICF, health-status measures, linking rules.
J Rehabil Med 2002; 34: 205-210Correspondence address: Alarcos Cieza, Department of Physical Medicine and Rehabilitation, Ludwig-Maximilians Universit , Munich,Germany E-mail: Alarcos.Cieza @ phys.med.uni-muenchen.deSubmitted June 18, 2002; Accepted June 20, 2002
© 2002 Taylor & Francis. ISSN 10-50-/977J Rehabil Med 34
Taylor&Francishealthsciences
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
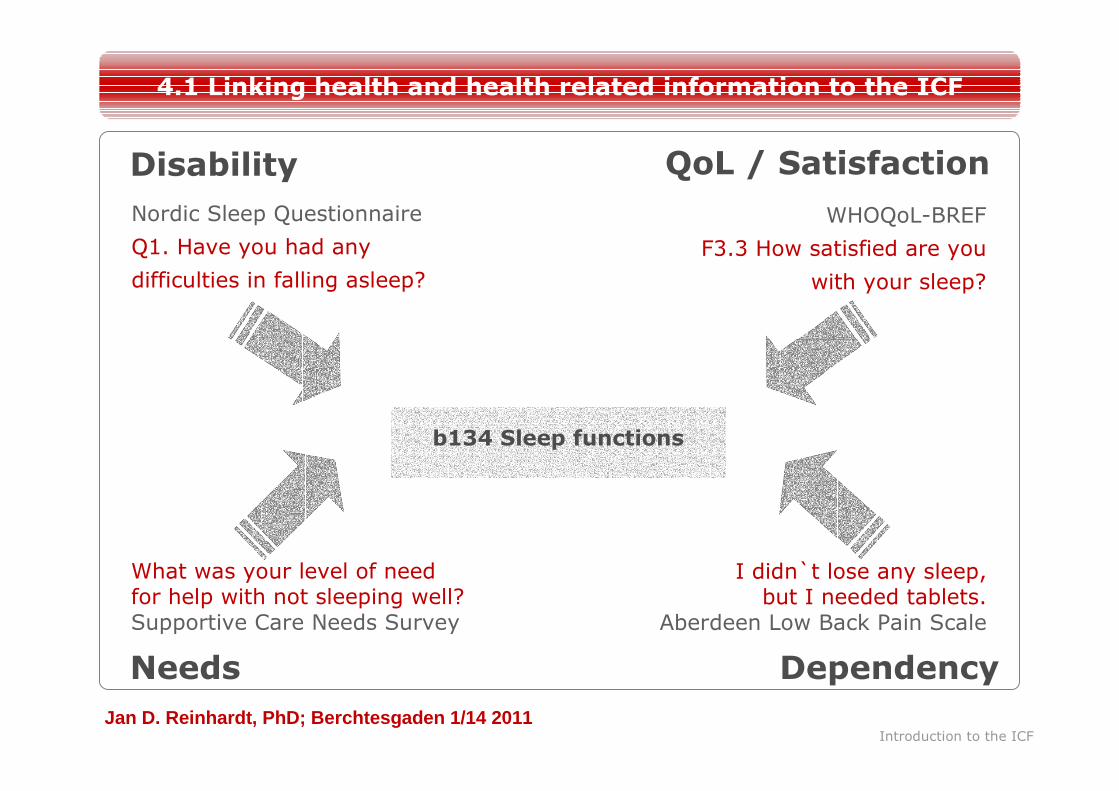
b134 Sleep functions
Disability QoL / Satisfaction
Needs Dependency
Nordic Sleep Questionnaire
Q1. Have you had any
difficulties in falling asleep?
WHOQoL-BREF
F3.3 How satisfied are you
with your sleep?
What was your level of needfor help with not sleeping well?Supportive Care Needs Survey
I didn`t lose any sleep, but I needed tablets.
Aberdeen Low Back Pain Scale
Introduction to the ICF
4.1 Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
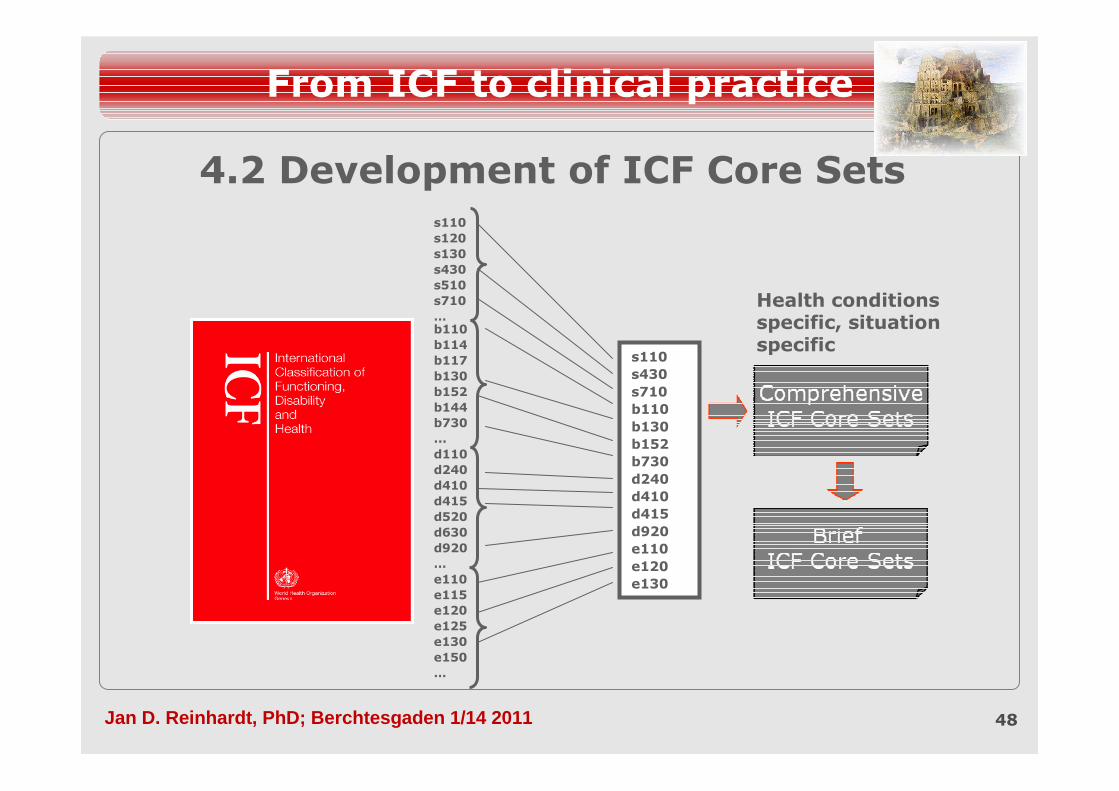
4.2 Development of ICF Core Sets
48
From ICF to clinical practice
s110s120s130s430s510s710…b110b114b117b130b152b144b730...d110d240d410d415d520d630d920…e110e115e120e125e130e150…
s110s430s710b110b130b152b730d240d410d415d920e110e120e130
Health conditions specific, situation specific
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
ICF Core Sets
Ein ICF Core Set ist eine Liste von ICF Kategorien, die so wenig Kategorien wie möglich, jedoch so viele wie nötig umfasst, um alle relevanten Aspekte der Funktionsfähigkeit von Menschen mit einer spezifischen Gesundheitstörung und in einem spezifischen Kontext für ein umfassendes und multidisziplinäres Assessment zu beschreiben.
Entwicklung von ICF Core Sets
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
ClinicalPerspective
Researchers’Perspective
Patients’Perspective
Health professionals’
Perspective
What problems of persons with the
health condition are measured and
reported in the literature?
What problems of persons with the
health condition are found in clinical
practice?
What are the problems that persons
with the health condition experience
from their perspective?
What problems of persons with the health condition are considered relevant by the health professionals that treat them?
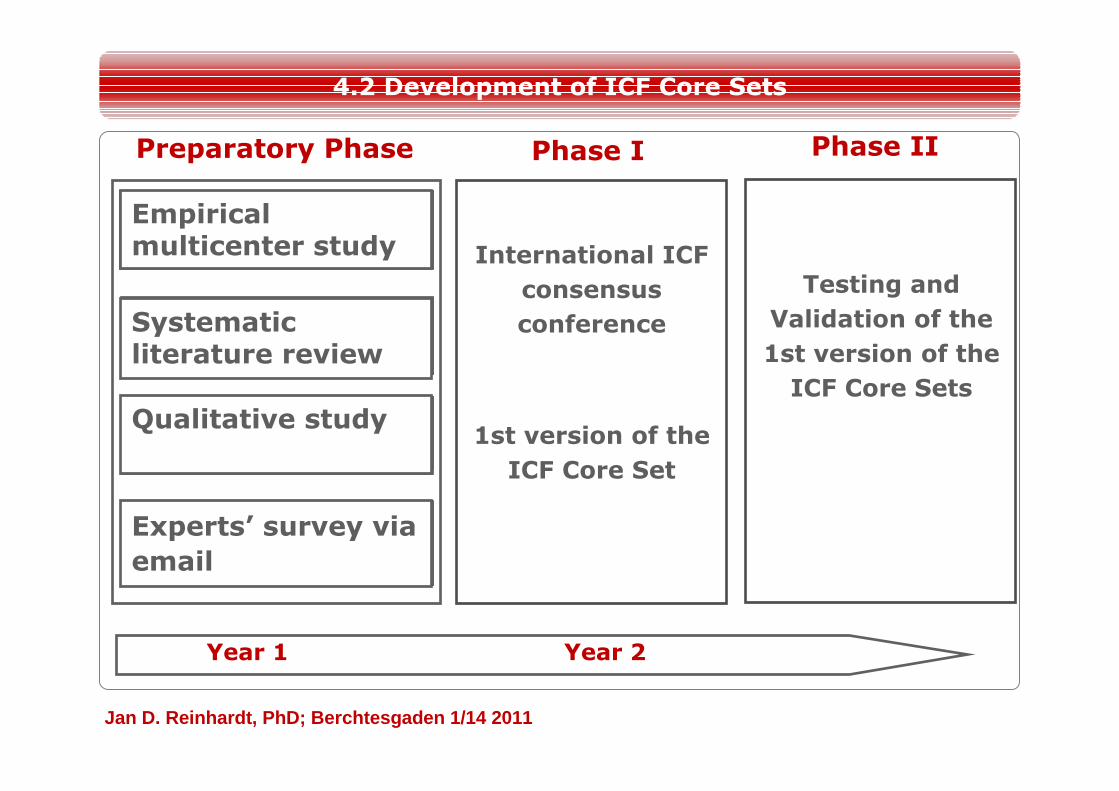
Empirical multicenter study
Systematic literature review
Qualitative study
Experts’ survey via email
International ICF
consensus
conference
1st version of the
ICF Core Set
Phase I Phase IIPreparatory Phase
Year 1 Year 2
Testing and
Validation of the
1st version of the
ICF Core Sets
4.2 Development of ICF Core Sets
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
�
nkylosing spondylitis�
reast cancer�
hronic ischemic heart disease�
hronic widespread pain�
epression�
iabetes�
and conditions�
ead and Neck Cancer�
ow back pain�
ultiple sclerosis�
Health conditions
4.2 Development of ICF Core Sets
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
� Amputees� Bipolar disorders� Burns� Cerebral Palsy� Inflammatory bowel Diseases� Traumatic Brain Injury� Vocational Rehabilitation
Current developments
4.2 Development of ICF Core Sets
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
List of ICF categories that includes as few categories as possible to be practical, but as many as necessary to describe the aspects of functioning relevant to persons with a specific condition in a comprehensive, multi-disciplinary assessment
• Comprehensive ICF Core Set
4.2 Development of ICF Core Sets
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
List of ICF categories that serves as the minimal standard for reporting the functioning of persons with a specific health condition along the continuum of care (ranging from the acute hospital to rehabilitation facilities and community) and across sectors (health, education, labour and social affairs)
• Brief ICF Core Set
4.2 Development of ICF Core Sets
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 55
…What to measure
and not
…How to measure
Keep in mind:
ICF Core Sets define…
4.2 Development of ICF Core Sets
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Value of ICF Core Sets
• Guide for clinical assessment
– Minimum functioning catalogue:What to assess?
– What are the patient’s problems?
• Basis for improving communication
– Among professionals
– Between settings
4.2 Development of ICF Core Sets
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
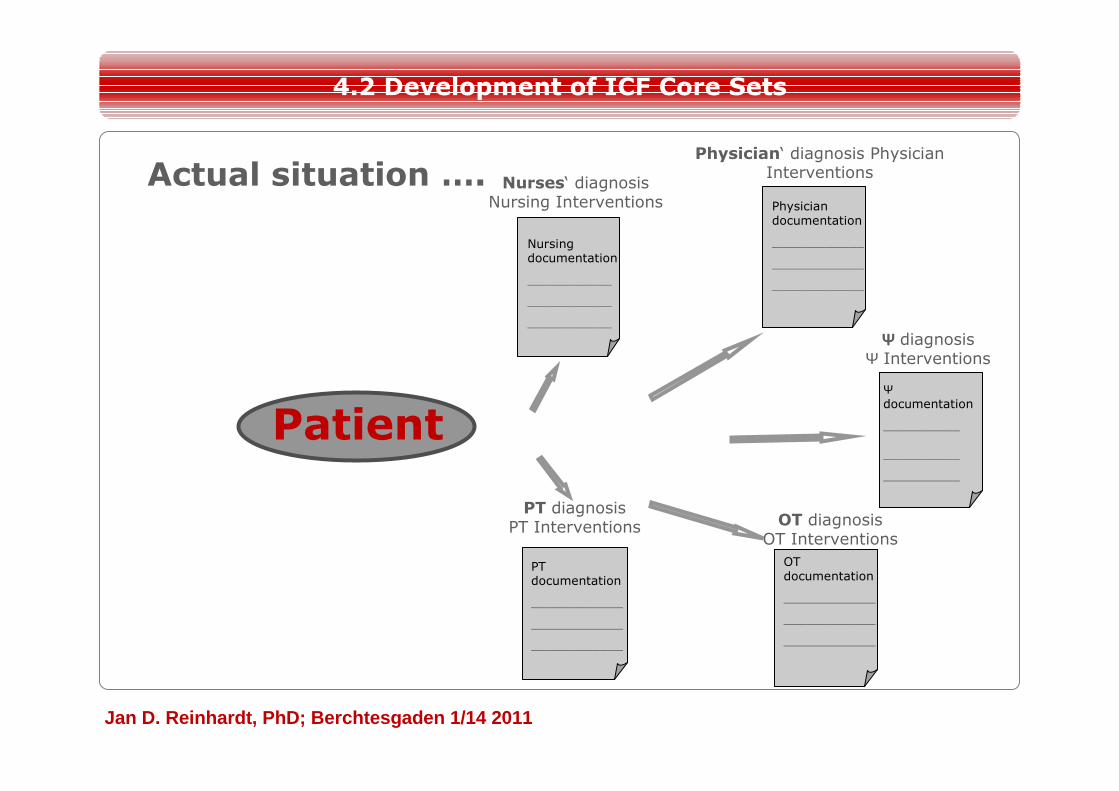
ΨΨΨΨ diagnosisΨ Interventions
Ψdocumentation
__________
__________
__________
Physician‘ diagnosis Physician Interventions
Physician documentation
____________
____________
____________
Nurses‘ diagnosisNursing Interventions
Nursing documentation
___________
___________
___________
OT diagnosis OT Interventions
OTdocumentation
____________
____________
____________
PT diagnosisPT Interventions
PTdocumentation
____________
____________
____________
Patient
4.2 Development of ICF Core Sets
Actual situation ….
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
ΨΨΨΨ diagnosisΨ Interventions
Ψdocumentation
__________
__________
__________
Physician‘ diagnosis Physician Interventions
Physician documentation
____________
____________
____________
Nurses‘ diagnosisNursing Interventions
Nursing documentation
___________
___________
___________
OT diagnosis OT Interventions
OTdocumentation
____________
____________
____________
PT diagnosisPT Interventions
PTdocumentation
____________
____________
____________
Patient
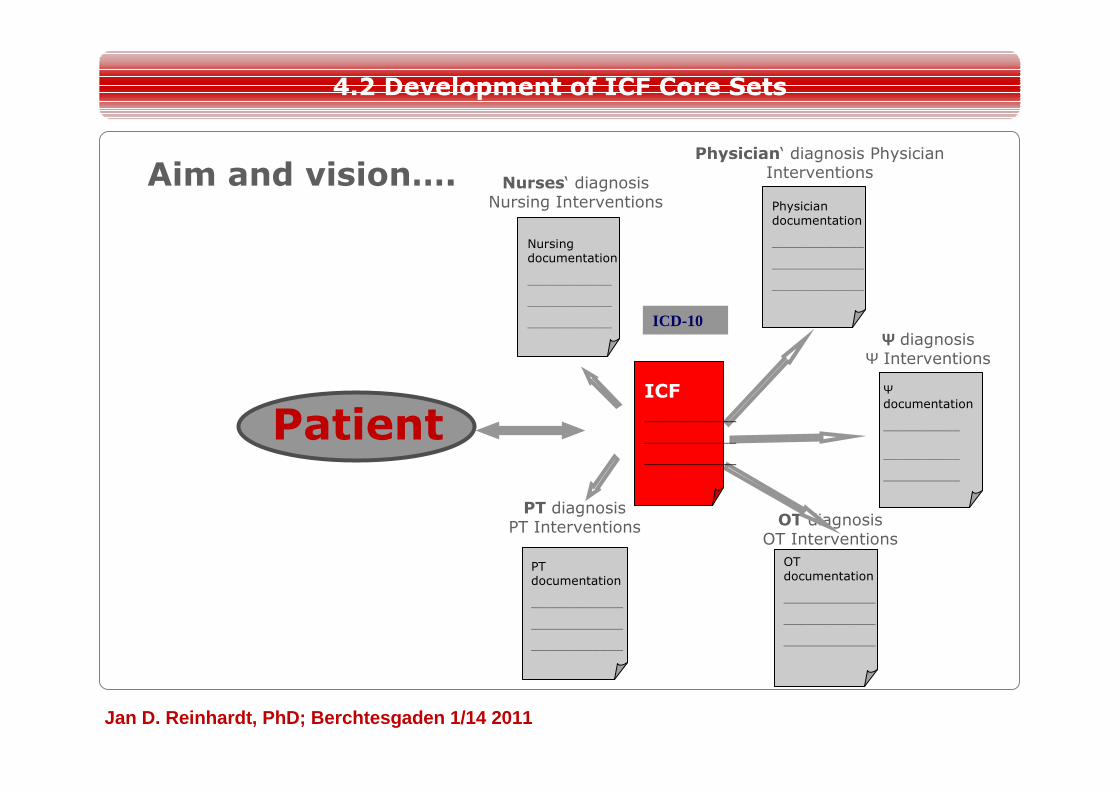
4.2 Development of ICF Core Sets
Aim and vision….
ICF____________
____________
____________
ICD-10
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
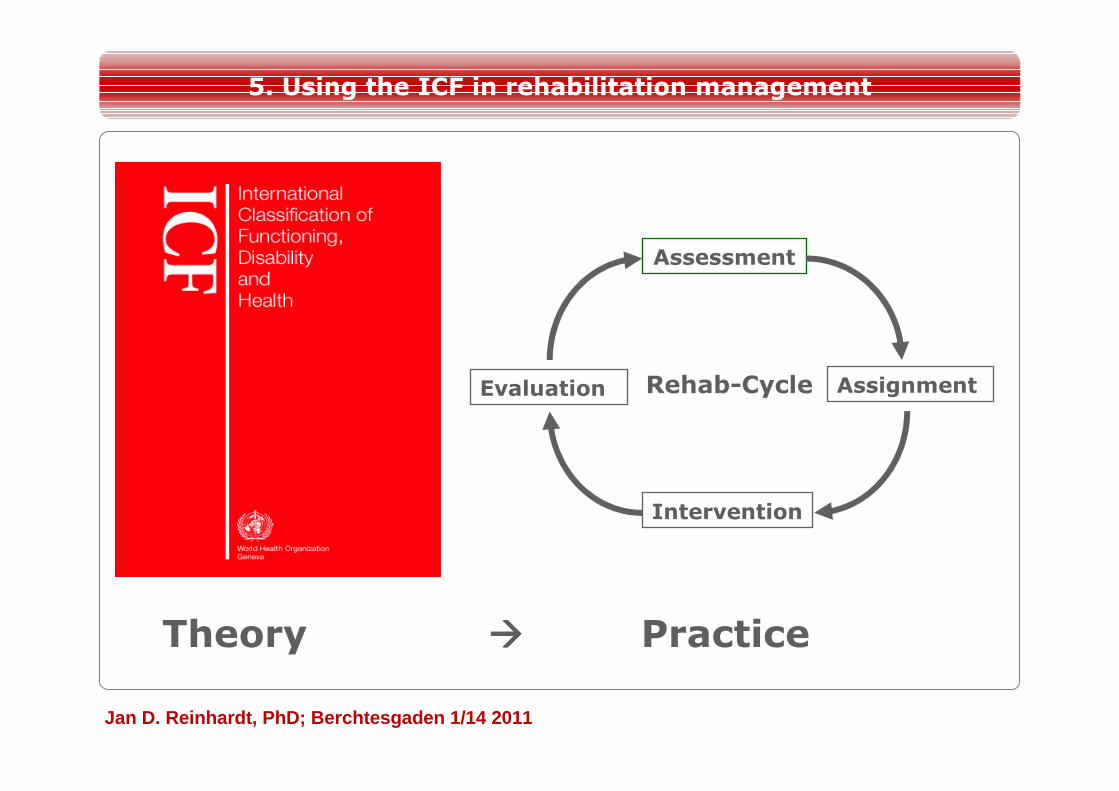
Theory ���� Practice
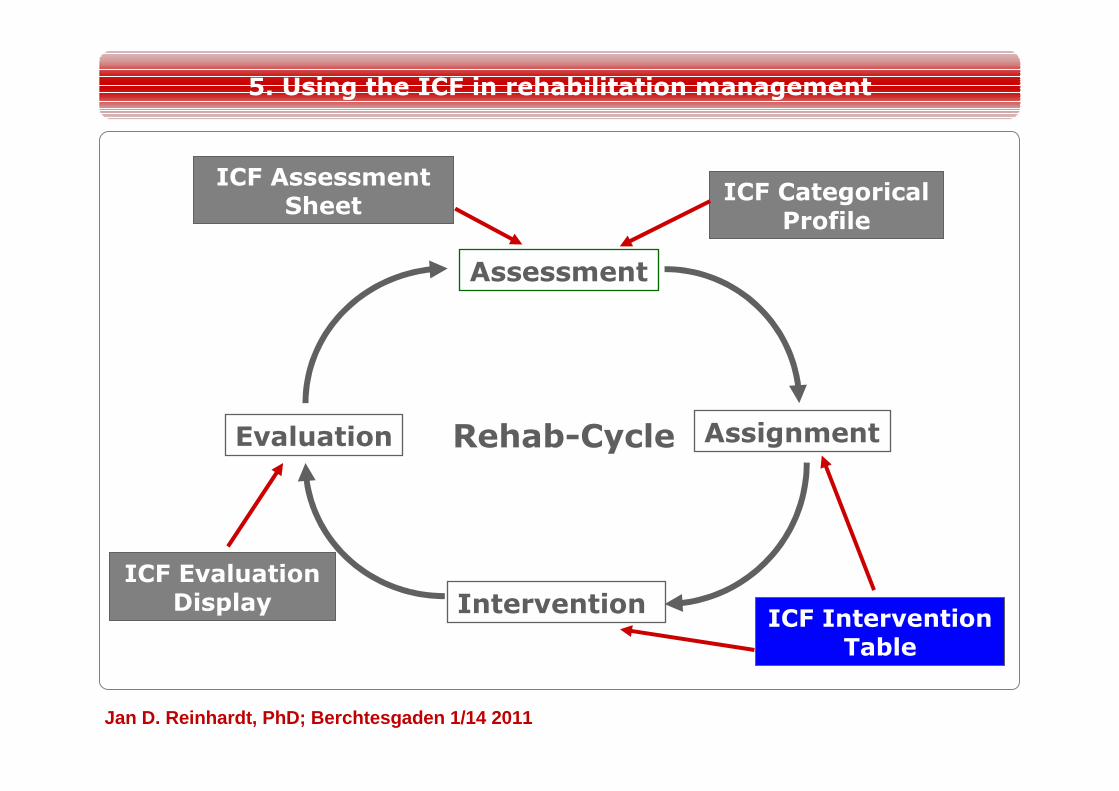
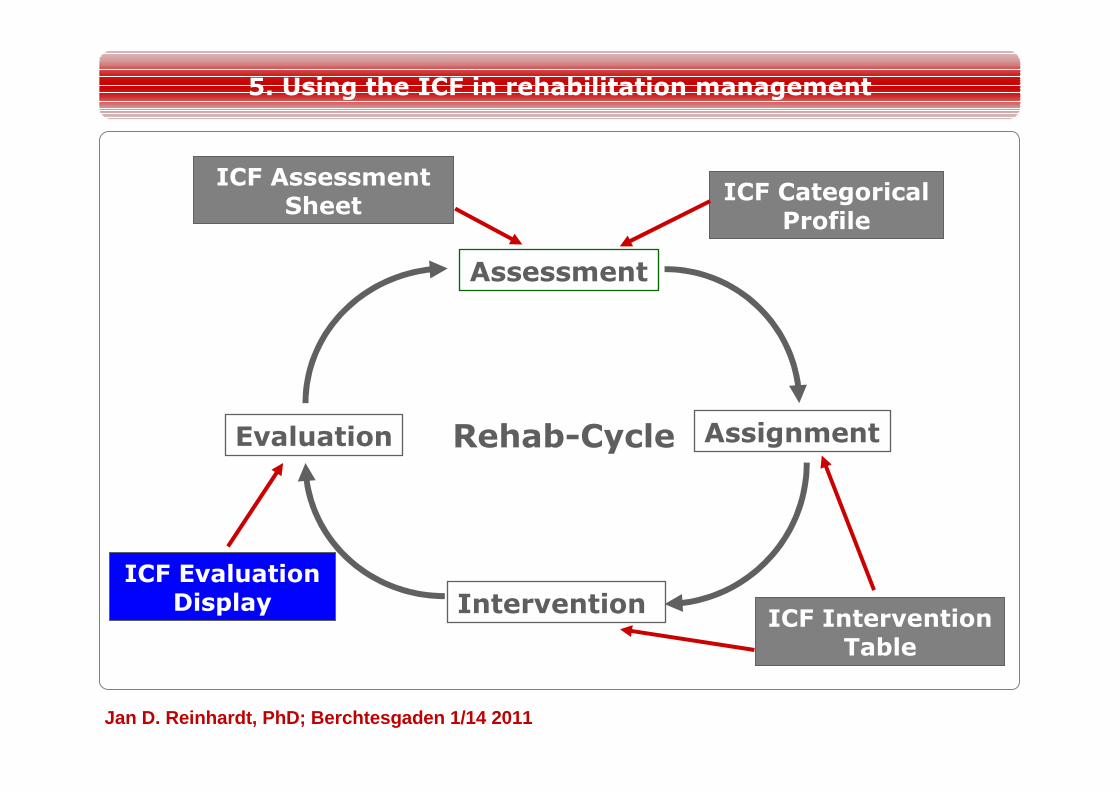
5. Using the ICF in rehabilitation management
Assessment
Assignment
Intervention
Evaluation Rehab-Cycle
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
At the core of rehabilitation care provision are the evolving problems and needs of individuals in relation to functioning.
5. Using the ICF in rehabilitation management
To achieve or maintain optimal function a multidisciplinary approach is required. Hence, rehabilitation integrates medical approaches labor, educational, social, architectural etc. approaches through cooperation and professionals across sectors.
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
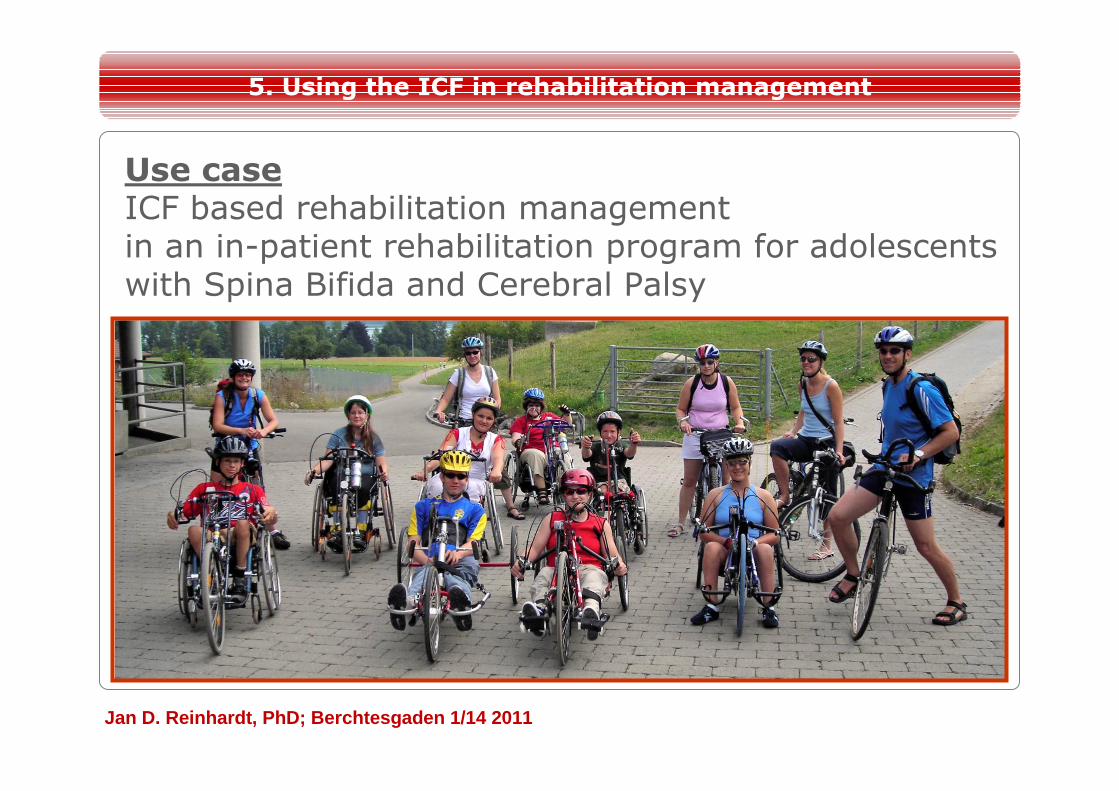
Use case ICF based rehabilitation management in an in-patient rehabilitation program for adolescents with Spina Bifida and Cerebral Palsy
5. Using the ICF in rehabilitation management
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Assessment of a patient‘s functioning status within the ICF Categorical Profile: A case example
62
5. Using the ICF in rehabilitation management
A person with Spina Bifida
• 17 year old adolescent
• Living with his family
• Visiting regular school
• Hobbies: Impassioned panpipe-player, reading, listen to music, computer
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 63
6.2. Using the ICF in rehabilitation management
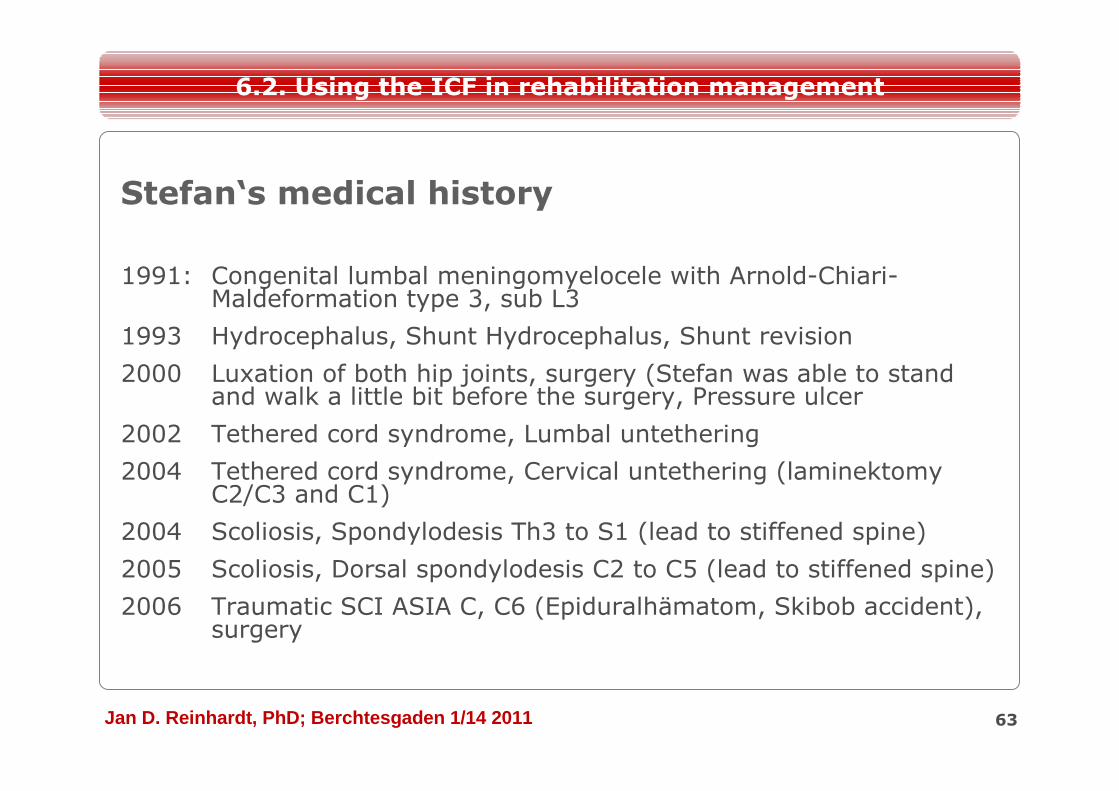
1991: Congenital lumbal meningomyelocele with Arnold-Chiari-Maldeformation type 3, sub L3
1993 Hydrocephalus, Shunt Hydrocephalus, Shunt revision
2000 Luxation of both hip joints, surgery (Stefan was able to stand and walk a little bit before the surgery, Pressure ulcer
2002 Tethered cord syndrome, Lumbal untethering
2004 Tethered cord syndrome, Cervical untethering (laminektomy C2/C3 and C1)
2004 Scoliosis, Spondylodesis Th3 to S1 (lead to stiffened spine)
2005 Scoliosis, Dorsal spondylodesis C2 to C5 (lead to stiffened spine)
2006 Traumatic SCI ASIA C, C6 (Epiduralhämatom, Skibob accident), surgery
Stefan‘s medical history
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
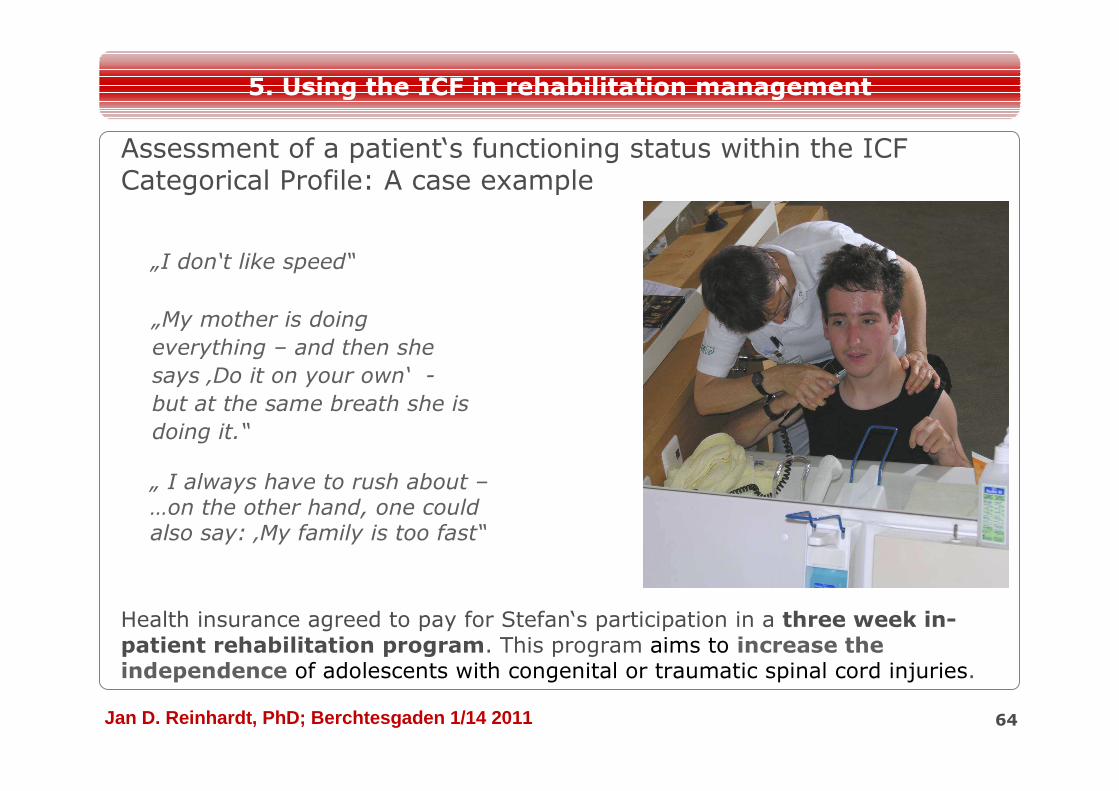
Assessment of a patient‘s functioning status within the ICF Categorical Profile: A case example
Health insurance agreed to pay for Stefan‘s participation in a three week in-patient rehabilitation program. This program aims to increase the independence of adolescents with congenital or traumatic spinal cord injuries.
64
5. Using the ICF in rehabilitation management
„I don‘t like speed“
„My mother is doing
everything – and then she
says ‚Do it on your own‘ -
but at the same breath she is
doing it.“
„ I always have to rush about –…on the other hand, one could also say: ‚My family is too fast“
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Assessment Global Goal: Service-Program-Goal: Cycle goal 1: Cycle goal 2:
ICF categories ICF Qualifier Goal Re-lation
Goal value
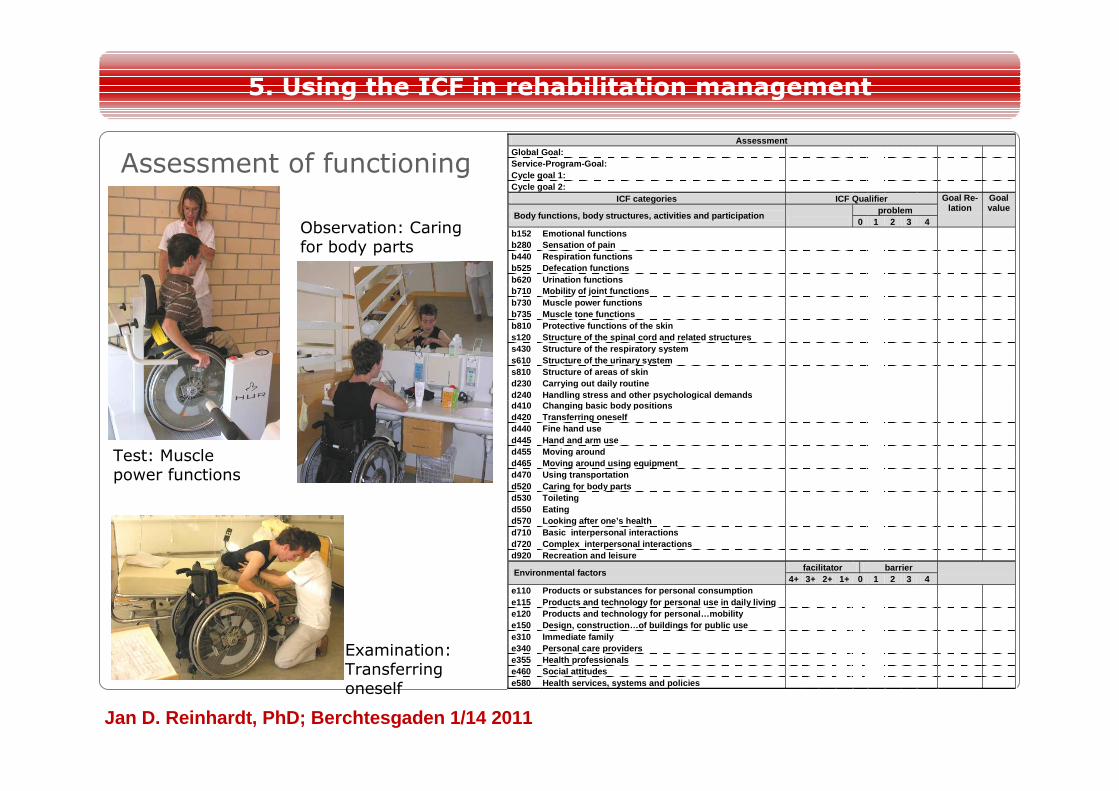
Body functions, body structures, activities and pa rticipation
problem 0 1 2 3 4
b152 Emotional functions b280 Sensation of pain b440 Respiration functions b525 Defecation functions b620 Urination functions b710 Mobility of joint functions b730 Muscle power functions b735 Muscle tone functions b810 Protective functions of the skin s120 Structure of the spinal cord and related struc tures s430 Structure of the respiratory system s610 Structure of the urinary system s810 Structure of areas of skin d230 Carrying out daily routine d240 Handling stress and other psychological demand s d410 Changing basic body positions d420 Transferring oneself d440 Fine hand use d445 Hand and arm use d455 Moving around d465 Moving around using equipment d470 Using transportation d520 Caring for body parts d530 Toileting d550 Eating d570 Looking after one’s health d710 Basic interpersonal interactions d720 Complex interpersonal interactions d920 Recreation and leisure
Environmental factors facilitator barrier 4+ 3+ 2+ 1+ 0 1 2 3 4
e110 Products or substances for personal consumptio n e115 Products and technology for personal use in da ily living e120 Products and technology for personal…mobility e150 Design, construction…of buildings for public u se e310 Immediate family e340 Personal care providers e355 Health professionals e460 Social attitudes e580 Health services, systems and policies
5. Using the ICF in rehabilitation management
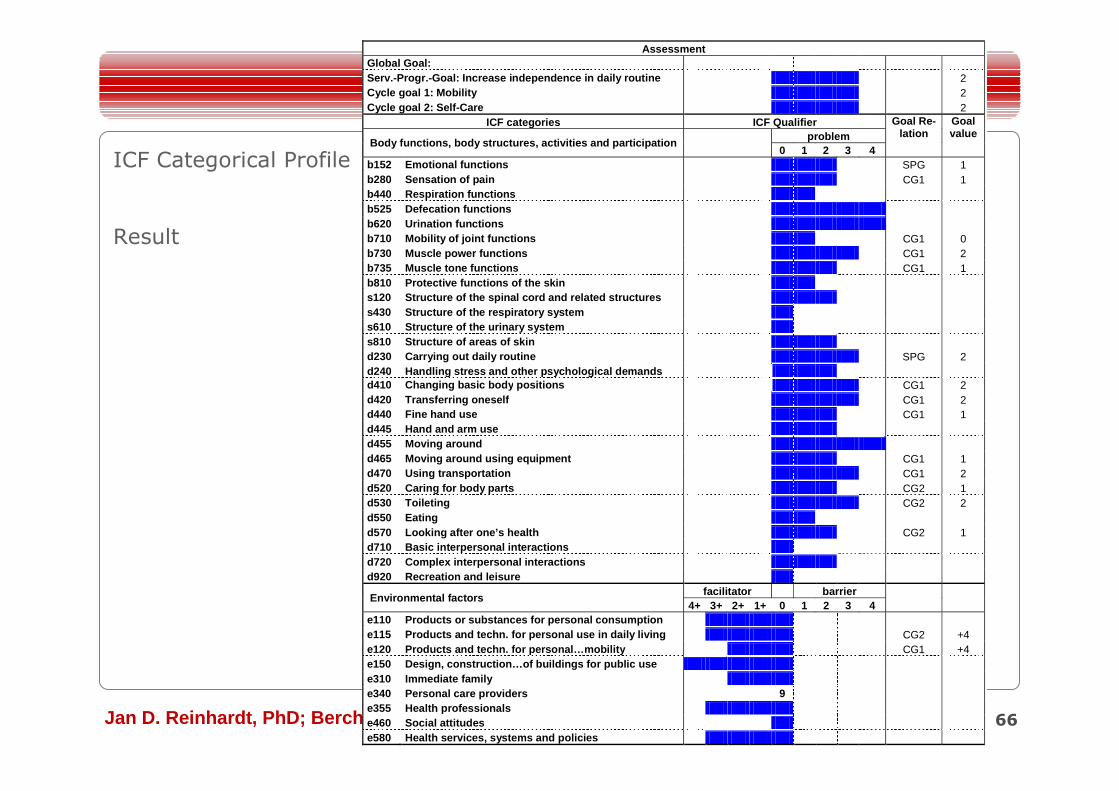
Assessment of functioning
Test: Muscle power functions
Observation: Caring for body parts
Examination: Transferring oneself
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 66
Assessment Global Goal: Serv.-Progr.-Goal: Increase independence in daily r outine 2 Cycle goal 1: Mobility 2 Cycle goal 2: Self-Care 2
ICF categories ICF Qualifier Goal Re-lation
Goal value
Body functions, body structures, activities and par ticipation
problem 0 1 2 3 4
b152 Emotional functions SPG 1 b280 Sensation of pain CG1 1 b440 Respiration functions b525 Defecation functions b620 Urination functions b710 Mobility of joint functions CG1 0 b730 Muscle power functions CG1 2 b735 Muscle tone functions CG1 1 b810 Protective functions of the skin s120 Structure of the spinal cord and related struc tures s430 Structure of the respiratory system s610 Structure of the urinary system s810 Structure of areas of skin d230 Carrying out daily routine SPG 2 d240 Handling stress and other psychological demand s d410 Changing basic body positions CG1 2 d420 Transferring oneself CG1 2 d440 Fine hand use CG1 1 d445 Hand and arm use d455 Moving around d465 Moving around using equipment CG1 1 d470 Using transportation CG1 2 d520 Caring for body parts CG2 1 d530 Toileting CG2 2 d550 Eating d570 Looking after one’s health CG2 1 d710 Basic interpersonal interactions d720 Complex interpersonal interactions d920 Recreation and leisure
Environmental factors facilitator barrier
4+ 3+ 2+ 1+ 0 1 2 3 4 e110 Products or substances for personal consumptio n e115 Products and techn. for personal use in daily living CG2 +4 e120 Products and techn. for personal…mobility CG1 +4 e150 Design, construction…of buildings for public u se e310 Immediate family e340 Personal care providers 9 e355 Health professionals e460 Social attitudes e580 Health services, systems and policies
ICF Categorical Profile
Result
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Assessment
Assignment
Intervention
Evaluation Rehab-Cycle
ICF Categorical Profile
ICF Assessment Sheet
ICF Intervention Table
ICF Evaluation Display
5. Using the ICF in rehabilitation management
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
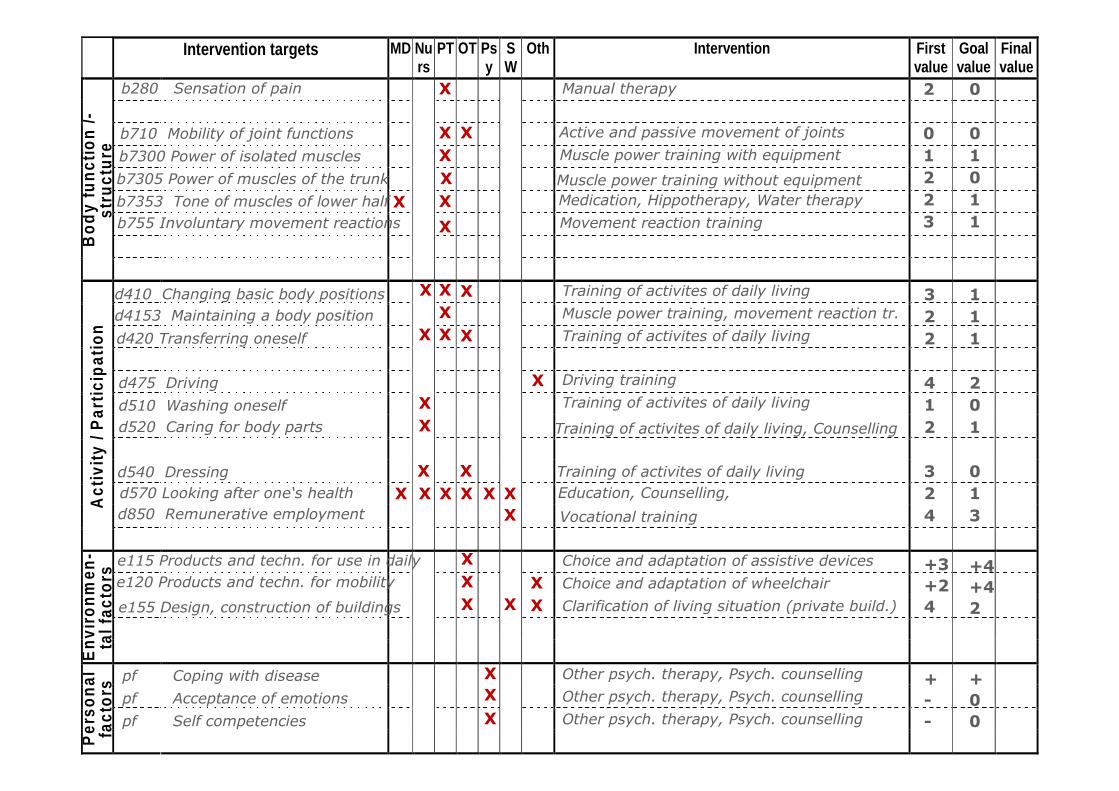
Intervention targets MD Nurs
PT OT Psy
SW
Oth Intervention First value
Goal value
Final value
B
ody
func
tion
/-
stru
ctur
e
Act
ivity
/ P
artic
ipat
ion
Env
ironm
en-
tal f
acto
rs
Per
sona
l fa
ctor
s
b280 Sensation of pain
b710 Mobility of joint functions
b7300 Power of isolated muscles
b7305 Power of muscles of the trunk
b7353 Tone of muscles of lower half
b755 Involuntary movement reactions
d410 Changing basic body positions
d4153 Maintaining a body position
d420 Transferring oneself
d475 Driving
d510 Washing oneself
d520 Caring for body parts
d540 Dressing
d850 Remunerative employment
e115 Products and techn. for use in daily
e120 Products and techn. for mobility
e155 Design, construction of buildings
pf Coping with disease
pf Acceptance of emotions
pf Self competencies
Manual therapy
Active and passive movement of joints
Muscle power training with equipment
Muscle power training without equipment
Medication, Hippotherapy, Water therapy
Movement reaction training
Training of activites of daily living
Muscle power training, movement reaction tr.
Training of activites of daily living
Driving training
Training of activites of daily living
d570 Looking after one‘s health
Training of activites of daily living, Counselling
Training of activites of daily living
Education, Counselling,
Vocational training
Choice and adaptation of assistive devices
Choice and adaptation of wheelchair
Clarification of living situation (private build.)
Other psych. therapy, Psych. counselling
Other psych. therapy, Psych. counselling
Other psych. therapy, Psych. counselling
XX
X
X
X
X XX
X
X X
X
XXX
XX
XXX
X XX X X X
X
XX XX XX
XX
X
2
01223
322
412
324
+3+24
+--
0
01011
111
201
013
+4+42
+00
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 69
1… provides an overview of the assignment of interventions to intervention targets and to the different health professionals.
Keep in mind:
The ICF Intervention Table…
5. Using the ICF in rehabilitation management
2… illustrates the required resources
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Assessment
Assignment
Intervention
Evaluation Rehab-Cycle
ICF Categorical Profile
ICF Assessment Sheet
ICF Intervention Table
ICF Evaluation Display
5. Using the ICF in rehabilitation management
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
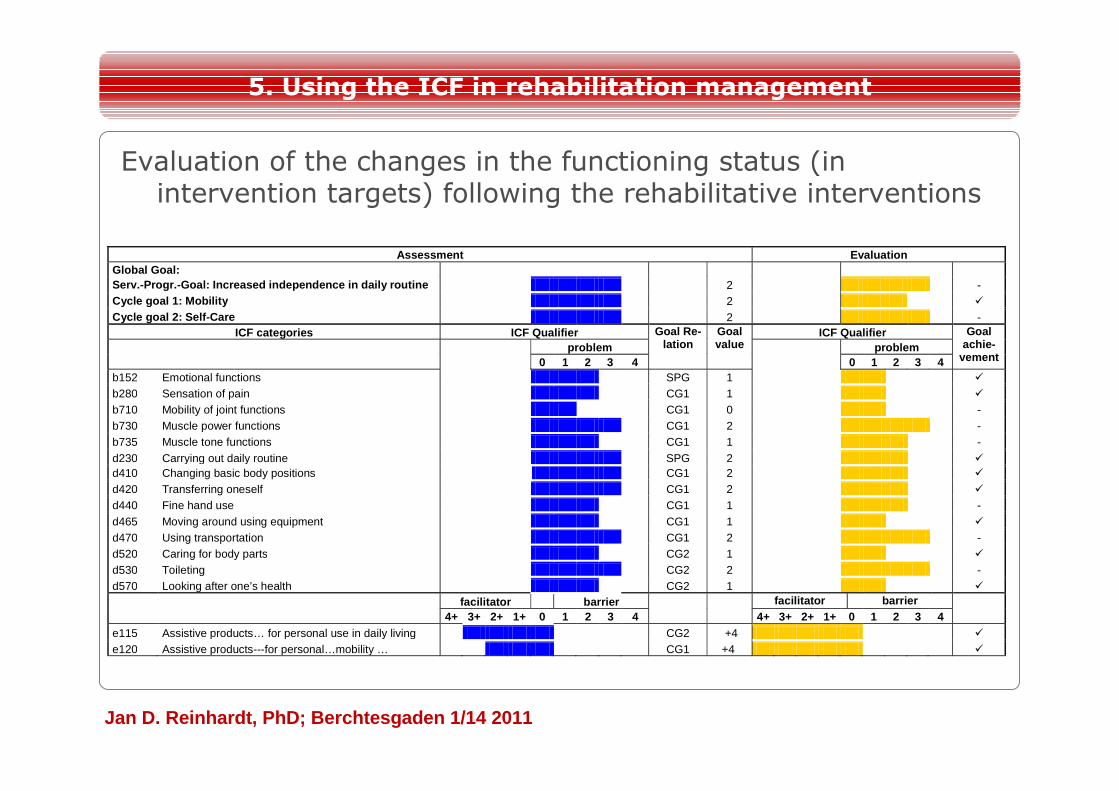
5. Using the ICF in rehabilitation management
Evaluation of the changes in the functioning status (in intervention targets) following the rehabilitative interventions
Assessment Evaluation Global Goal:
Serv.-Progr.-Goal: Increased independence in daily routine 2 - Cycle goal 1: Mobility 2 � Cycle goal 2: Self-Care 2 -
ICF categories ICF Qualifier Goal Re-lation
Goal value
ICF Qualifier Goal achie-
vement
problem
problem 0 1 2 3 4 0 1 2 3 4
b152 Emotional functions SPG 1 � b280 Sensation of pain CG1 1 � b710 Mobility of joint functions CG1 0 - b730 Muscle power functions CG1 2 - b735 Muscle tone functions CG1 1 - d230 Carrying out daily routine SPG 2 � d410 Changing basic body positions CG1 2 � d420 Transferring oneself CG1 2 � d440 Fine hand use CG1 1 - d465 Moving around using equipment CG1 1 � d470 Using transportation CG1 2 - d520 Caring for body parts CG2 1 � d530 Toileting CG2 2 - d570 Looking after one’s health CG2 1 �
facilitator barrier
facilitator barrier 4+ 3+ 2+ 1+ 0 1 2 3 4 4+ 3+ 2+ 1+ 0 1 2 3 4
e115 Assistive products… for personal use in daily living CG2 +4 � e120 Assistive products---for personal…mobility … CG1 +4 �
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011 72
1… depicts the changes in a patient’s functioning status and goal achievement
Keep in mind:
The ICF Evaluation Display…
5. Using the ICF in rehabilitation management
2… provides information for further rehabilitation planning
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
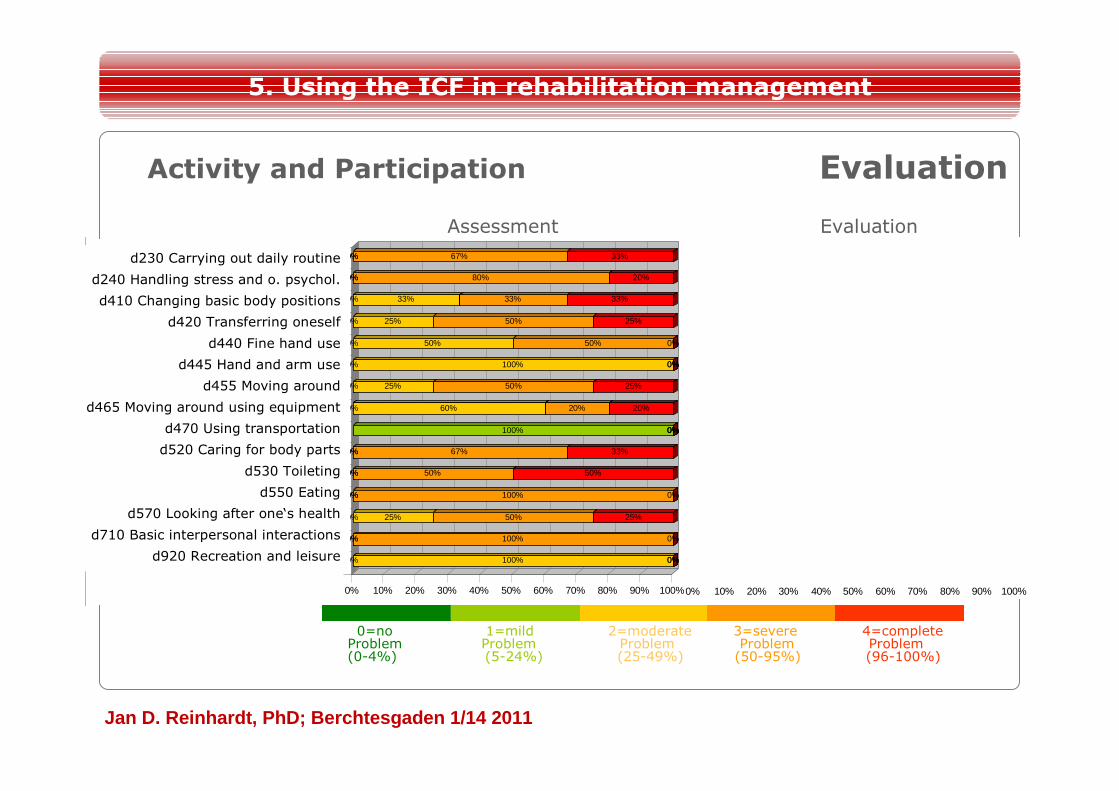
Activity and Participation
Assessment Evaluation
0% 100% 0%0%
0%0% 100% 0%
0% 25% 50% 25%
0%0% 100% 0%
0%0% 50% 50%
0%0% 67% 33%
100% 0%0%0%
0% 60% 20% 20%
0% 25% 50% 25%
0% 100% 0%0%
0% 50% 50% 0%
0% 25% 50% 25%
0% 33% 33% 33%
0%0% 80% 20%
0%0% 67% 33%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Die tägliche Routine durchführen d230 (9)
Mit Stress u. a. psych. Anforderungen umgehen d240 (5)
Eine elementare Körperposition wechseln d410 (6)
Sich verlagern d420 (4)
Feinmotorischer Handgebrauch d440 (2)
Hand- und Armgebrauch d445 (2)
Sich auf andere Weise fortbewegen d455 (4)
Sich unter Verwendung von Geräten fortbewegen d465 (5)
Transportmittel benutzen d470 (1)
Seine Körperteile pflegen d520 (6)
Die Toilette benutzen d530 (6)
Essen d550 (3)
Auf seine Gesundheit achten d570 (4)
Elementare interpersonelle Aktivitäten d710 (3)
Erholung und Freizeit d920 (3) 33% 67% 0%0%
0% 33% 67% 0%
25% 25% 50% 0%
0% 33% 67% 0%
17% 17% 33% 33%
17% 17% 33% 33%
100% 0%0%0%
20% 40% 40% 0%
25% 0% 25% 50%
100% 0%0%0%
50% 0% 50% 0%
25% 25% 50% 0%
33% 33% 17% 17%
0% 20% 60% 20%
11% 33% 44% 11%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
d230 Carrying out daily routine
d240 Handling stress and o. psychol.
d410 Changing basic body positions
d420 Transferring oneself
d440 Fine hand use
d445 Hand and arm use
d455 Moving around
d465 Moving around using equipment
d470 Using transportation
d520 Caring for body parts
d530 Toileting
d550 Eating
d570 Looking after one‘s health
d710 Basic interpersonal interactions
d920 Recreation and leisure
5. Using the ICF in rehabilitation management
Evaluation
0=no 1=mild 2=moderate 3=severe 4=complete Problem Problem Problem Problem Problem(0-4%) (5-24%) (25-49%) (50-95%) (96-100%)
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Practicability of the ICF Categorical Profile
The use of the ICF Categorical Profile• facilitated a clear depiction of a patient‘s functioning status and allowed the documentation of rehabilitation goals and intervention targets
• contributed rehabilitation management by increasing communication and common goal-setting
• increased time consumption for documentation
5. Using the ICF in rehabilitation management
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Practicability of the ICF Categorical Profile
Challenges:• ICF categories were experienced too less comprehensive and specific
• Definition of ICF categories were experienced sometimes too less precise and sometimes overlapping
• Rating within ICF Qualifiers was experienced too less objective
• ICF Qualifiers are too less sensitive for illustrating changes in the functioning states
• Ambivalent EF cannot be coded.
5. Using the ICF in rehabilitation management
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
6. Ausblick
• Das ICF Modell und Klassifikation (ICF-CY) bieten eine umfassende und dynamische Perspektive für die Rehabilitation von Kindern und Jugendlichen
• Weiterentwicklungen in Forschung und Praxis sind aber unabdingbar:
– Noch keine diagnosespezifischen Core Sets für Kinder und Jugendliche -> Differentielle Core Sets für unterschiedliche Entwicklungsstufen
– Klinische ICF Tools sind am Anfang ihrer Entwicklung und weisen noch einige Schwächen auf
76
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
6. Ausblick
• Kaum systematische Evaluationsstudien bzgl. clinical effectiveness
• Mittelfristig muss eine Erhöhung des Dokumentationsaufwands durch ICF vermieden werden, z.B.
– die Entwicklung ICF-basierter Outcome Instrumente
– durch integrierte, elektronische ICF-basierte Dokumentationssysteme
– Algorhythmen zur Umrechnung klinischer Testergebnisse in ICF Qualifier
• Klärung des Verhältnisses zur ICD: – Symptome und Functioning?
– Risk factors und Umweltfaktoren?
77
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Danke für Ihre Aufmerksamkeit!
78
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Training Material der ICF Research Branch
79
ICFresearch branch
The use of the ICF Core Sets in clinical practice and research
Training VideoICF Research Branch of WHO CC FIC (DIMDI)
Swiss Paraplegic ResearchLudwig-Maximilians-University
Ressourcen
http://p.ideaday.de/104.2/icf/http://www.icf-research-branch.org/aboutus/services.htm
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Backup – ICF Linking
80
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Targets for ICF linking:
• standardized patient-orientedoutcomes
• clinical assessments, also thoserequiring an specialized apparatus
• interventions targets
• qualitative data
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
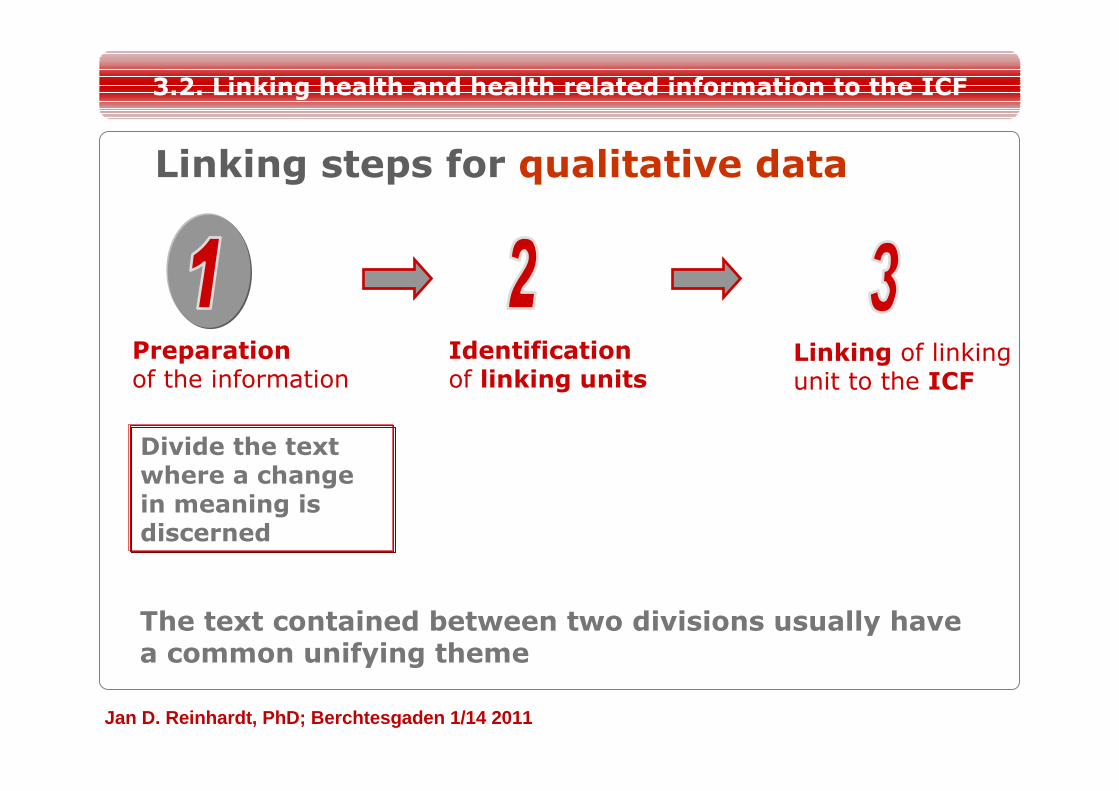
Linking steps for qualitative data
Identification of linking units
Linking of linking unit to the ICF
Preparation of the information
Divide the text where a change in meaning is discerned
3.2. Linking health and health related information to the ICF
The text contained between two divisions usually have a common unifying theme
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
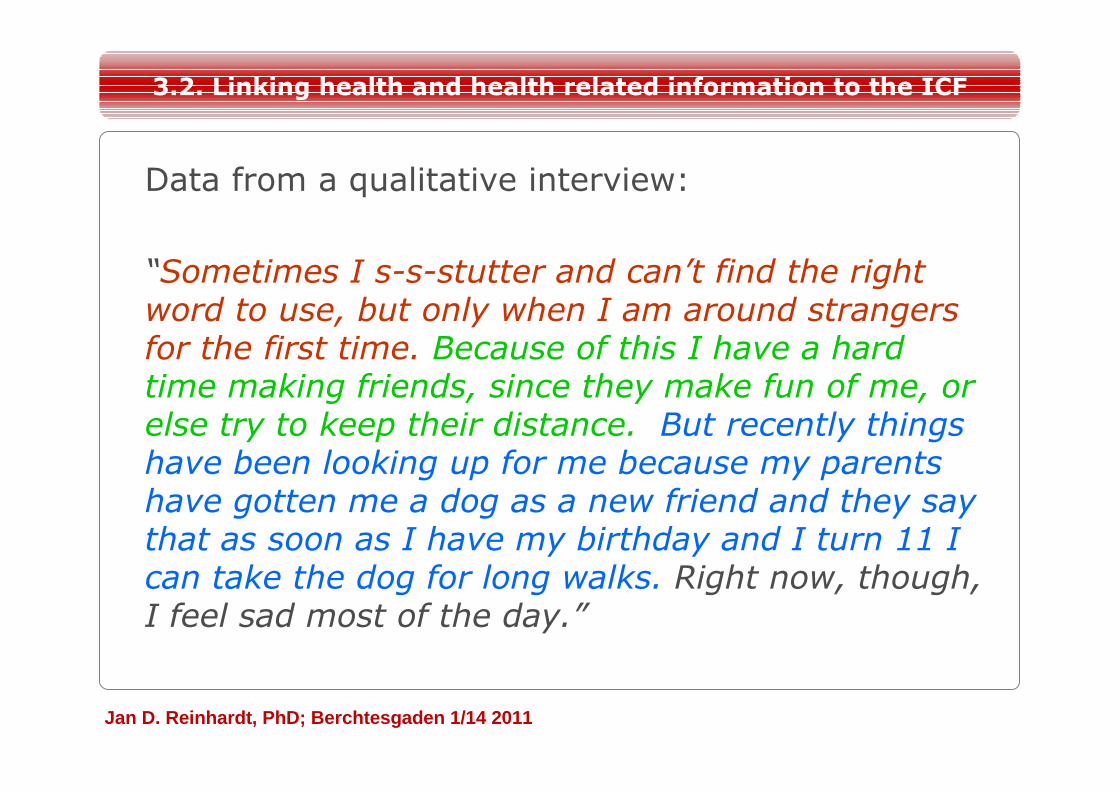
Data from a qualitative interview:
“Sometimes I s-s-stutter and can’t find the right word to use, but only when I am around strangers for the first time. Because of this I have a hard time making friends, since they make fun of me, or else try to keep their distance. But recently things have been looking up for me because my parents have gotten me a dog as a new friend and they say that as soon as I have my birthday and I turn 11 I can take the dog for long walks. Right now, though, I feel sad most of the day.”
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
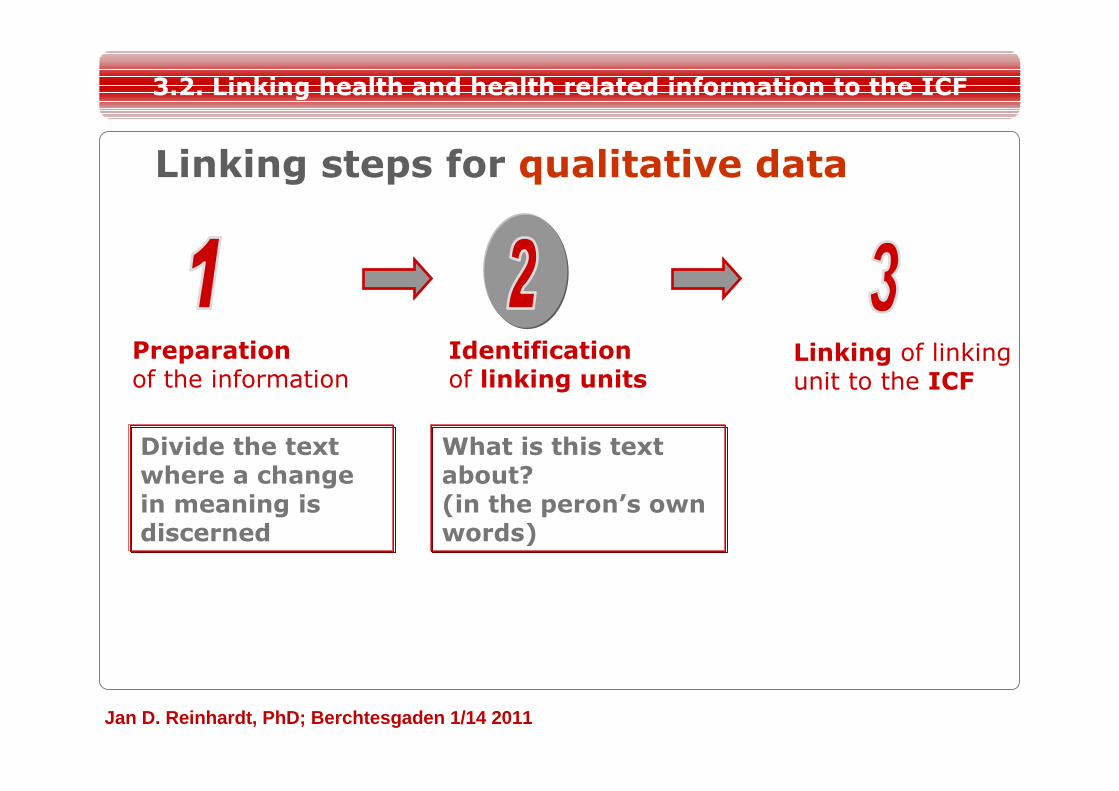
Linking steps for qualitative data
Identification of linking units
Linking of linking unit to the ICF
Preparation of the information
Divide the text where a change in meaning is discerned
3.2. Linking health and health related information to the ICF
What is this text about?(in the peron’s own words)
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
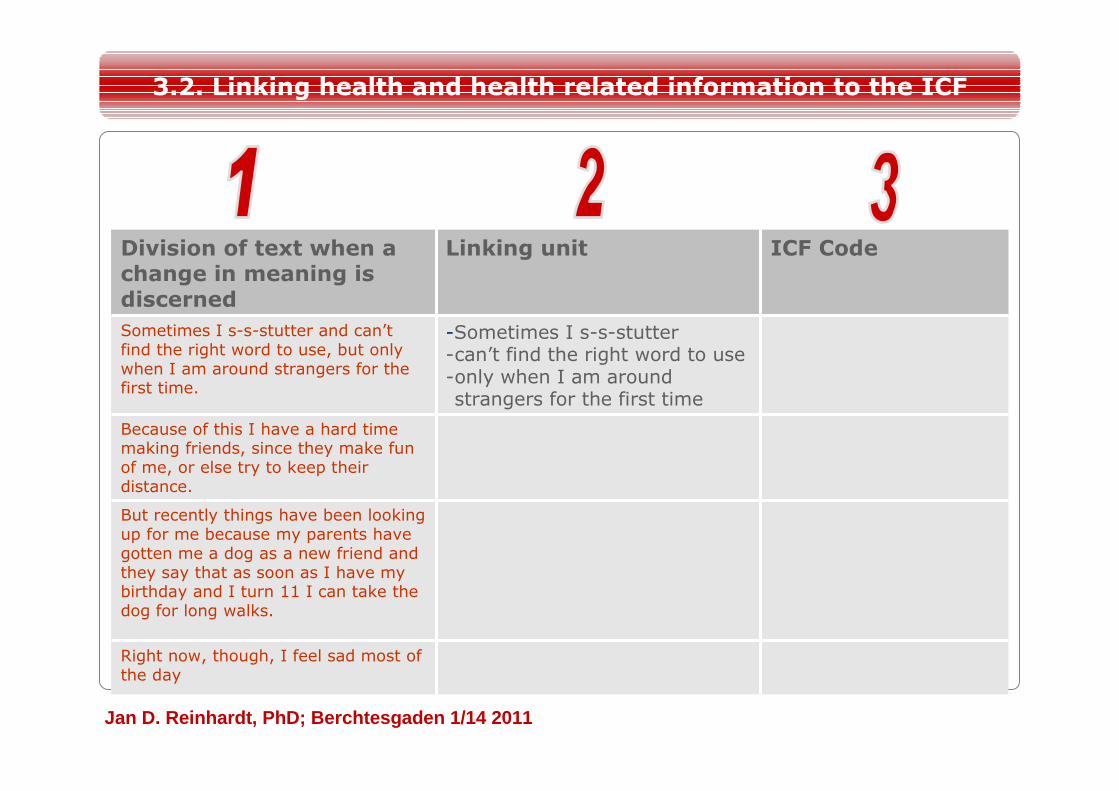
Division of text when a change in meaning is discerned
Linking unit ICF Code
Sometimes I s-s-stutter and can’t find the right word to use, but only when I am around strangers for the first time.
-Sometimes I s-s-stutter-can’t find the right word to use-only when I am around strangers for the first time
Because of this I have a hard time making friends, since they make fun of me, or else try to keep their distance.
But recently things have been looking up for me because my parents have gotten me a dog as a new friend and they say that as soon as I have my birthday and I turn 11 I can take the dog for long walks.
Right now, though, I feel sad most of the day
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
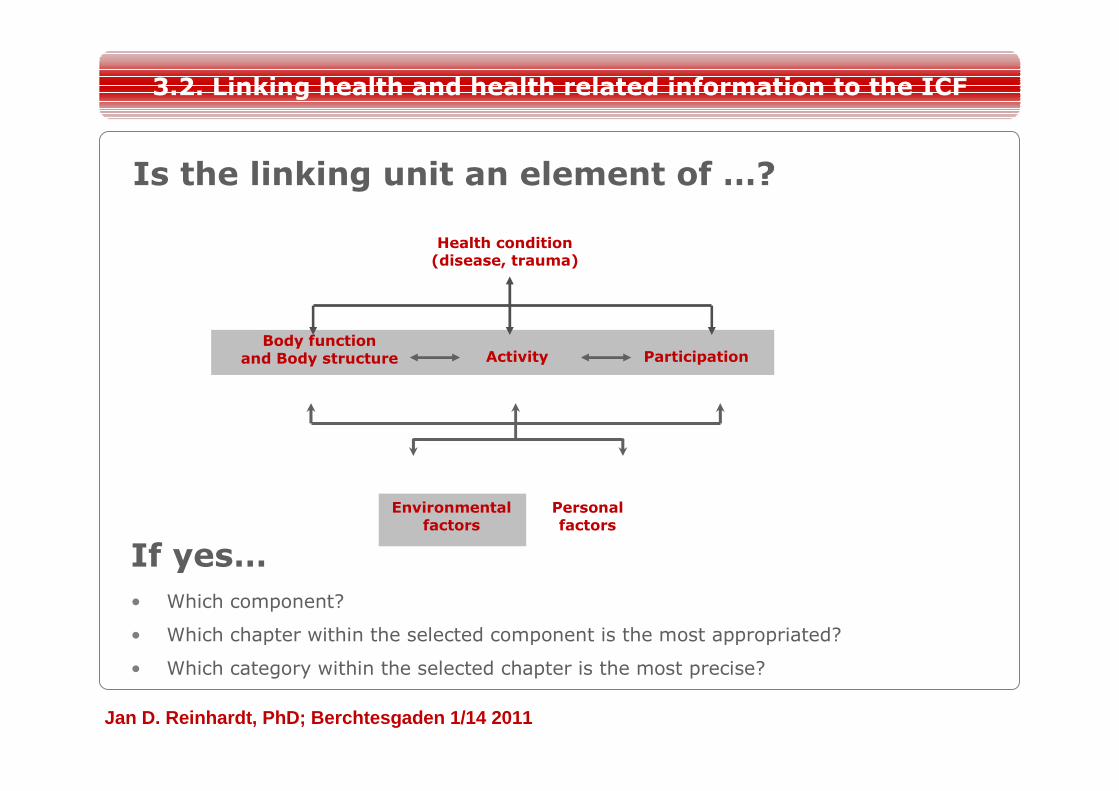
If yes…• Which component?
• Which chapter within the selected component is the most appropriated?
• Which category within the selected chapter is the most precise?
Health condition(disease, trauma)
Environmentalfactors
Personalfactors
Activity ParticipationParticipationBody function
and Body structure
Is the linking unit an element of …?
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
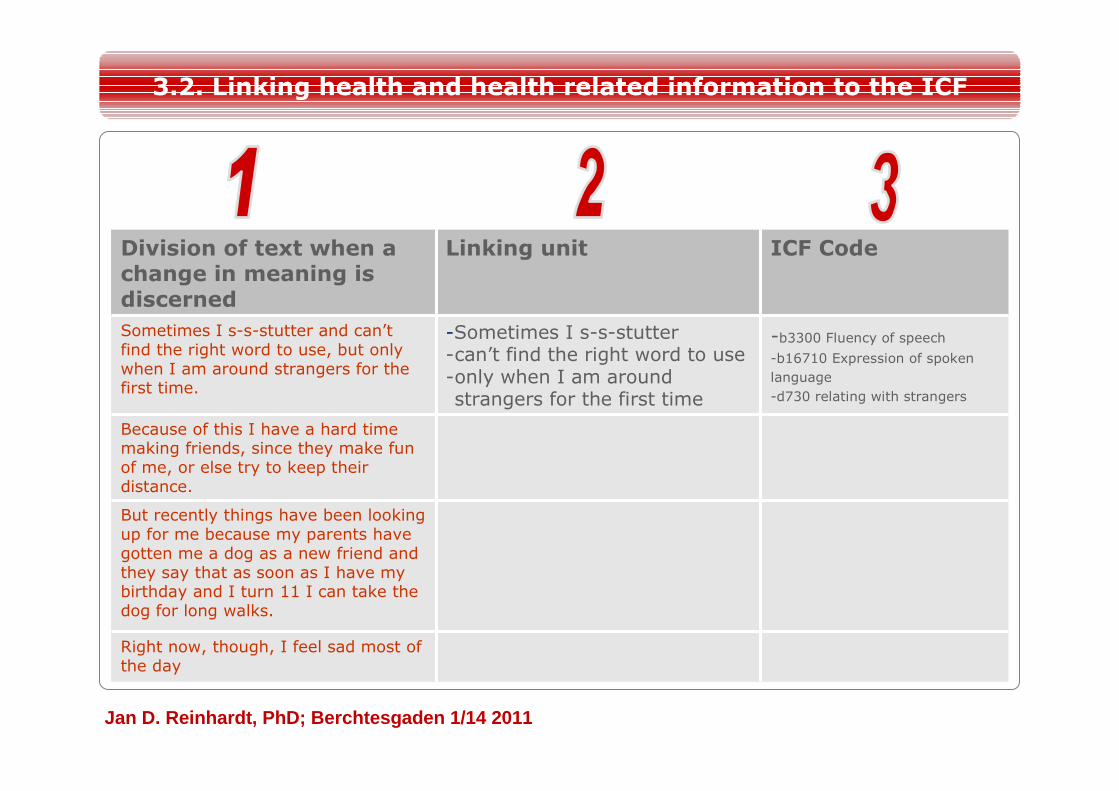
Division of text when a change in meaning is discerned
Linking unit ICF Code
Sometimes I s-s-stutter and can’t find the right word to use, but only when I am around strangers for the first time.
-Sometimes I s-s-stutter-can’t find the right word to use-only when I am around strangers for the first time
-b3300 Fluency of speech-b16710 Expression of spoken
language
-d730 relating with strangers
Because of this I have a hard time making friends, since they make fun of me, or else try to keep their distance.
But recently things have been looking up for me because my parents have gotten me a dog as a new friend and they say that as soon as I have my birthday and I turn 11 I can take the dog for long walks.
Right now, though, I feel sad most of the day
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
Linking Methodology
Uses and advantages
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
The health and health-related information for linking may be derived from:
• standardized patient-orientedoutcomes
• clinical assessments, also thoserequiring an specialized apparatus
• interventions targets
• qualitative data
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
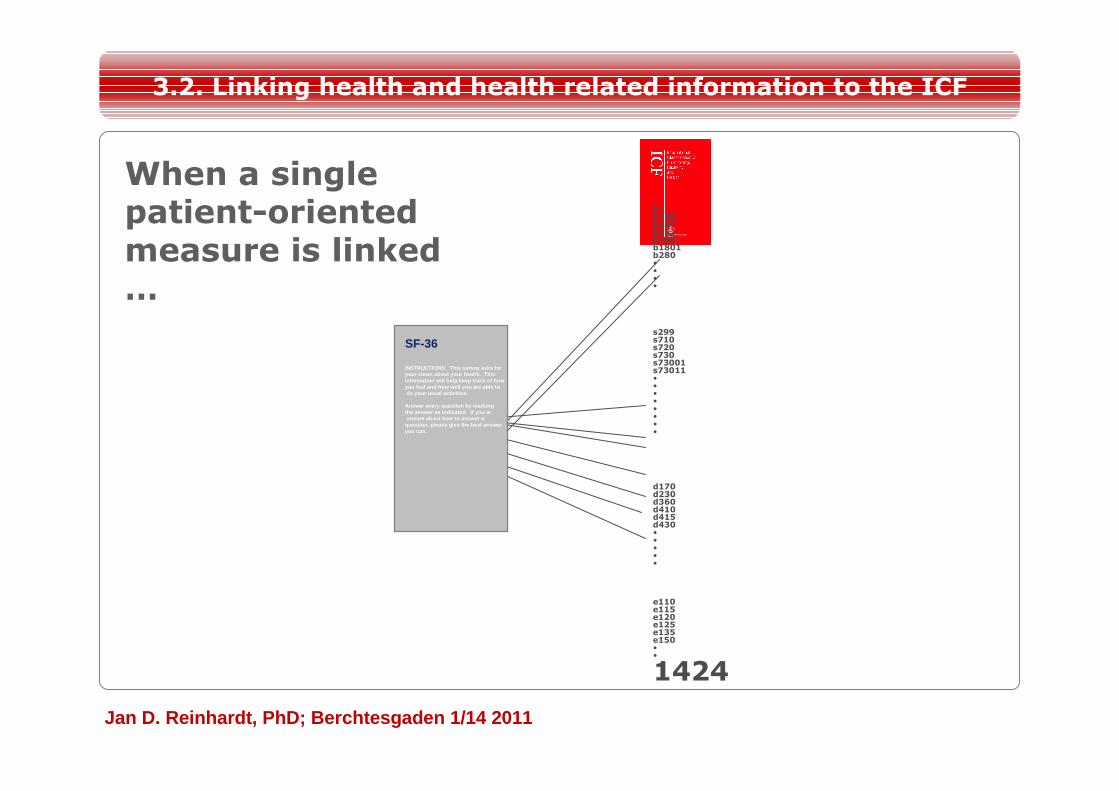
SF-36
INSTRUCTIONS: This survey asks foryour views about your health. Thisinformation will help keep track of howyou feel and how well you are able todo your usual activities.
Answer every question by markingthe answer as indicated. If you arunsure about how to answer aquestion, please give the best answer you can.
b1b130b134b152b180b1801b280••••
s299s710s720 s730s73001s73011••••••••
d170d230d360d410 d415d430•••••
e110e115e120e125e135e150••
1424
3.2. Linking health and health related information to the ICF
When a single patient-oriented measure is linked …
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
… its content validity can be studied
– breadth of coverage– repetition of content area
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
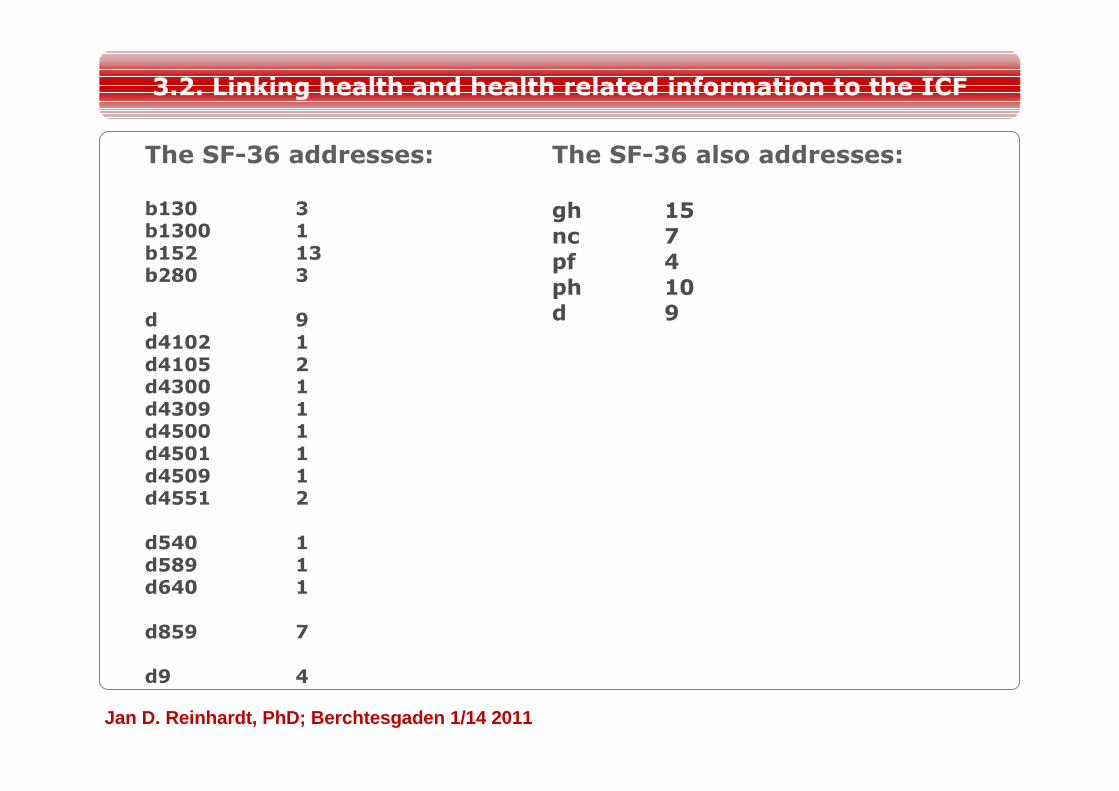
The SF-36 addresses:
b130 3b1300 1b152 13b280 3
d 9d4102 1d4105 2d4300 1d4309 1d4500 1d4501 1d4509 1d4551 2
d540 1d589 1d640 1
d859 7
d9 4
3.2. Linking health and health related information to the ICF
The SF-36 also addresses:
gh 15nc 7pf 4ph 10d 9
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
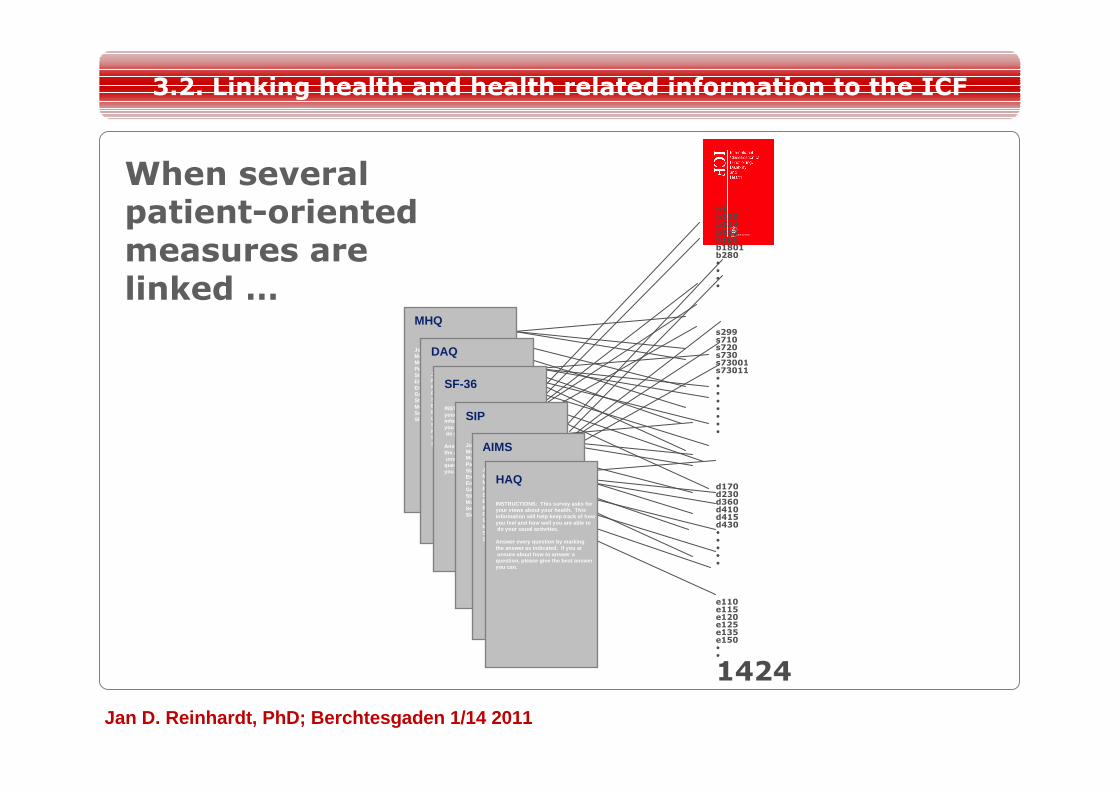
MHQ
Joint mobilityMobility (general)Muscle power / StrengthPainStability of jointsEmotional functionEngergy & Drive functionsGait / AmbulationStiffnessMuscle enduranceSexual functionsSleep
DAQ
Joint mobilityMobility (general)Muscle power / StrengthPainStability of jointsEmotional functionEngergy & Drive functionsGait / AmbulationStiffnessMuscle enduranceSexual functionsSleep
SF-36
INSTRUCTIONS: This survey asks foryour views about your health. Thisinformation will help keep track of howyou feel and how well you are able todo your usual activities.
Answer every question by markingthe answer as indicated. If you arunsure about how to answer aquestion, please give the best answer you can.
SIP
Joint mobilityMobility (general)Muscle power / StrengthPainStability of jointsEmotional functionEngergy & Drive functionsGait / AmbulationStiffnessMuscle enduranceSexual functionsSleep
AIMS
Joint mobilityMobility (general)Muscle power / StrengthPainStability of jointsEmotional functionEngergy & Drive functionsGait / AmbulationStiffnessMuscle enduranceSexual functionsSleep
HAQ
INSTRUCTIONS: This survey asks foryour views about your health. Thisinformation will help keep track of howyou feel and how well you are able todo your usual activities.
Answer every question by markingthe answer as indicated. If you arunsure about how to answer aquestion, please give the best answer you can.
b1b130b134b152b180b1801b280••••
s299s710s720 s730s73001s73011••••••••
d170d230d360d410 d415d430•••••
e110e115e120e125e135e150••
1424
3.2. Linking health and health related information to the ICF
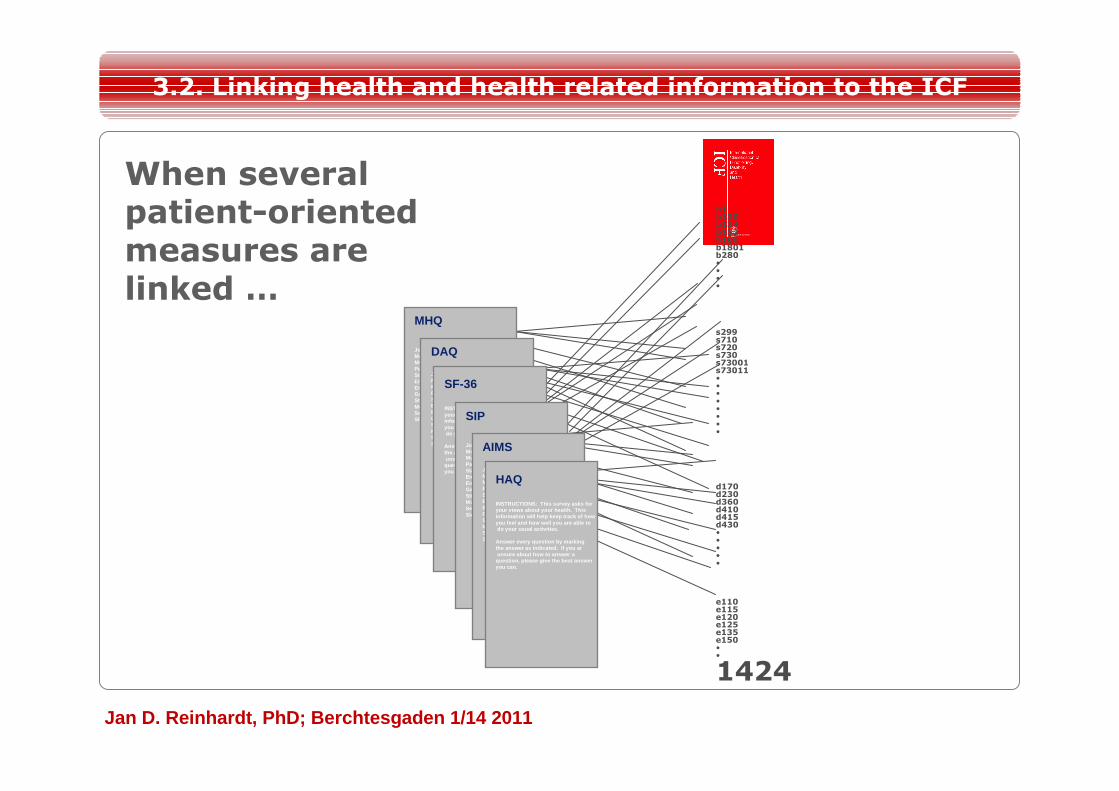
When several patient-oriented measures are linked …
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
… their content can be compared and the most appropriate measure to address the person’s needs can be selected
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
MHQ
Joint mobilityMobility (general)Muscle power / StrengthPainStability of jointsEmotional functionEngergy & Drive functionsGait / AmbulationStiffnessMuscle enduranceSexual functionsSleep
DAQ
Joint mobilityMobility (general)Muscle power / StrengthPainStability of jointsEmotional functionEngergy & Drive functionsGait / AmbulationStiffnessMuscle enduranceSexual functionsSleep
SF-36
INSTRUCTIONS: This survey asks foryour views about your health. Thisinformation will help keep track of howyou feel and how well you are able todo your usual activities.
Answer every question by markingthe answer as indicated. If you arunsure about how to answer aquestion, please give the best answer you can.
SIP
Joint mobilityMobility (general)Muscle power / StrengthPainStability of jointsEmotional functionEngergy & Drive functionsGait / AmbulationStiffnessMuscle enduranceSexual functionsSleep
AIMS
Joint mobilityMobility (general)Muscle power / StrengthPainStability of jointsEmotional functionEngergy & Drive functionsGait / AmbulationStiffnessMuscle enduranceSexual functionsSleep
HAQ
INSTRUCTIONS: This survey asks foryour views about your health. Thisinformation will help keep track of howyou feel and how well you are able todo your usual activities.
Answer every question by markingthe answer as indicated. If you arunsure about how to answer aquestion, please give the best answer you can.
b1b130b134b152b180b1801b280••••
s299s710s720 s730s73001s73011••••••••
d170d230d360d410 d415d430•••••
e110e115e120e125e135e150••
1424
3.2. Linking health and health related information to the ICF
When several patient-oriented measures are linked …
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
… the basis for categories-specific item banks can be created
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
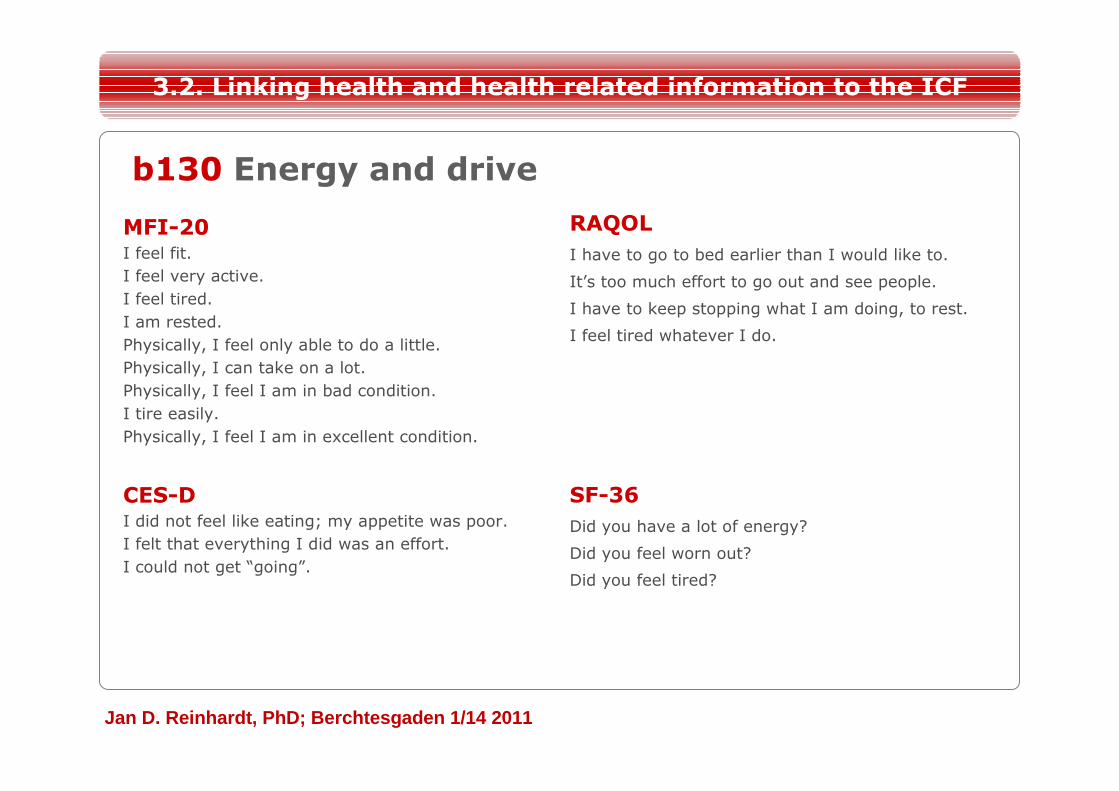
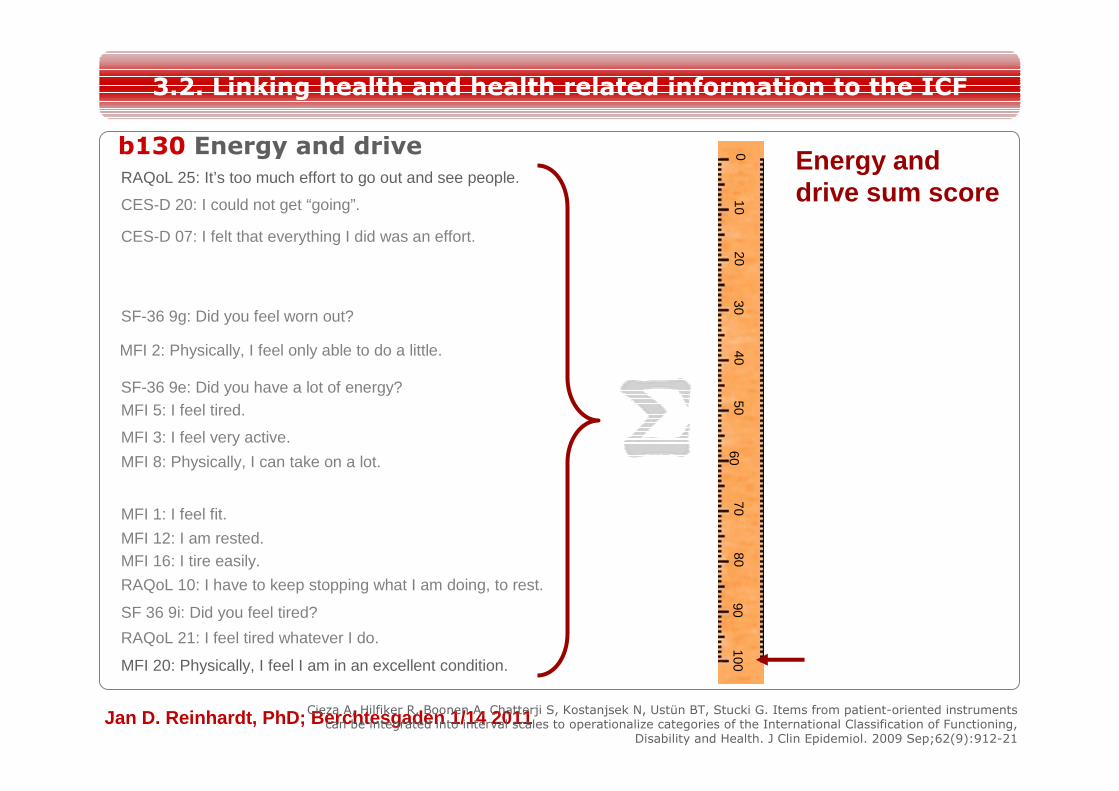
b130 Energy and drive
MFI-20I feel fit.
I feel very active.
I feel tired.
I am rested.
Physically, I feel only able to do a little.
Physically, I can take on a lot.
Physically, I feel I am in bad condition.
I tire easily.
Physically, I feel I am in excellent condition.
CES-DI did not feel like eating; my appetite was poor.
I felt that everything I did was an effort.
I could not get “going”.
RAQOLI have to go to bed earlier than I would like to.
It’s too much effort to go out and see people.
I have to keep stopping what I am doing, to rest.
I feel tired whatever I do.
SF-36Did you have a lot of energy?
Did you feel worn out?
Did you feel tired?
3.2. Linking health and health related information to the ICF
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
9080
010
2030
4050
6070
100
RAQoL 25: It’s too much effort to go out and see people.
CES-D 07: I felt that everything I did was an effort.
CES-D 20: I could not get “going”.
SF-36 9g: Did you feel worn out?
MFI 2: Physically, I feel only able to do a little.
SF-36 9e: Did you have a lot of energy?MFI 5: I feel tired.
MFI 3: I feel very active.
MFI 8: Physically, I can take on a lot.
MFI 1: I feel fit.
MFI 12: I am rested.MFI 16: I tire easily.
RAQoL 10: I have to keep stopping what I am doing, to rest.
SF 36 9i: Did you feel tired?
RAQoL 21: I feel tired whatever I do.
MFI 20: Physically, I feel I am in an excellent condition.
b130 Energy and drive
3.2. Linking health and health related information to the ICF
Cieza A, Hilfiker R, Boonen A, Chatterji S, Kostanjsek N, Ustün BT, Stucki G. Items from patient-oriented instrumentscan be integrated into interval scales to operationalize categories of the International Classification of Functioning,
Disability and Health. J Clin Epidemiol. 2009 Sep;62(9):912-21
Energy and drive sum score
Jan D. Reinhardt, PhD; Berchtesgaden 1/14 2011
The use of the linking methodology in qualitative data obtained from patients is useful for:
• identifying patients’ needs and for comparing these needs among different groups of patients
• evaluating the content validity of instruments
– Do the existing instruments address what is relevant to patients?
• evaluating interventions and studies
– Do the existing interventions and the studies being performed address what is relevant to patients?
3.2. Linking health and health related information to the ICF









![DIE IntErnatIonalE KlassIfIKatIon DEr funKtIonsfähIgKEIt ...08 Sozialpolitik und Rehabilitation gen zu klären, bevor eine internationale Entwicklung initiiert werden kann [13]. Kodierung](https://img.pdfslide.org/doc/110x75/6091c3f04caa47344158c9f0/die-internationale-klassifikation-der-funktionsfhigkeit-08-sozialpolitik-und.jpg)