Embed Size (px)
Citation preview

Onkologische Notfälle
Alfred ZippeliusMedizinische Onkologie
• Onkologische Notfälle begegnen nicht nur Onkologen !
• komplexe Situation
• Prävention bzw. frühe Detektion
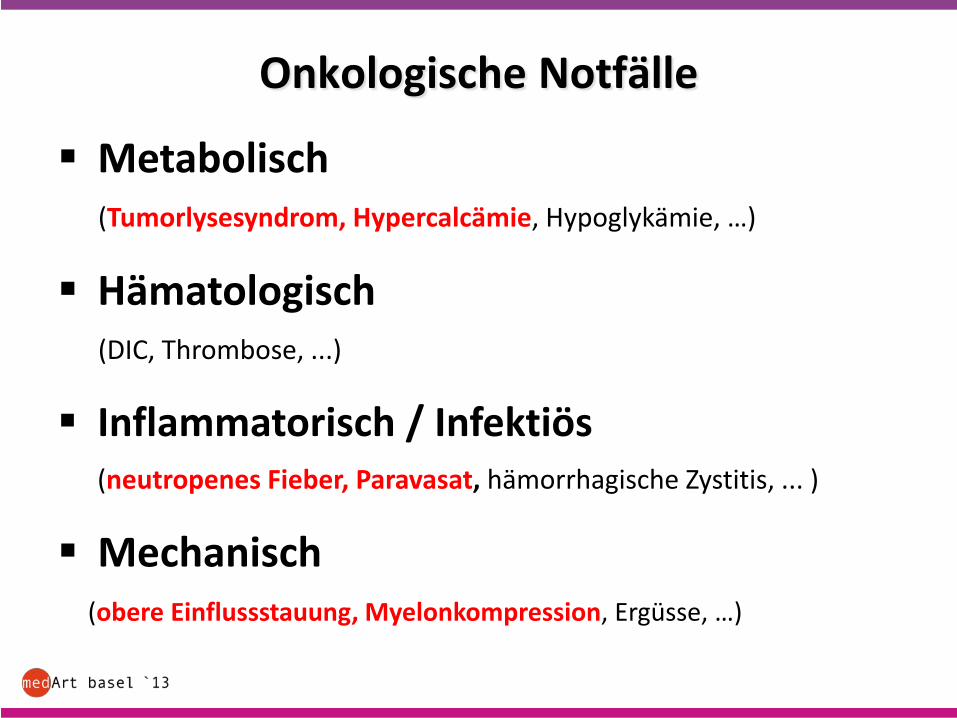
Onkologische Notfälle
Metabolisch(Tumorlysesyndrom, Hypercalcämie, Hypoglykämie, …)
Hämatologisch(DIC, Thrombose, ...)
Inflammatorisch / Infektiös(neutropenes Fieber, Paravasat, hämorrhagische Zystitis, ... )
Mechanisch(obere Einflussstauung, Myelonkompression, Ergüsse, …)
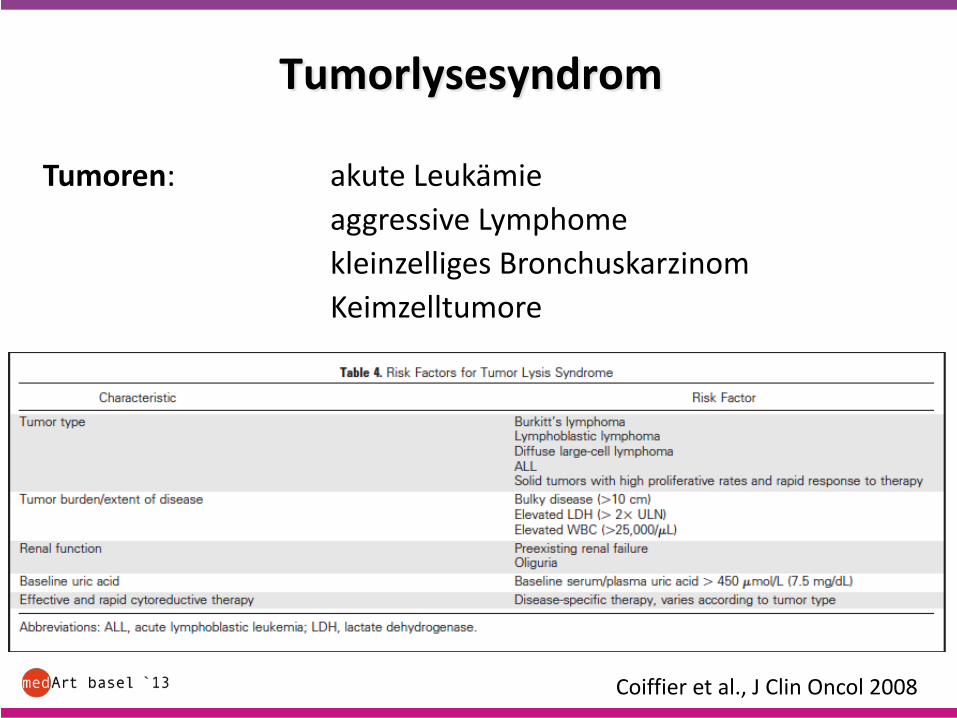
Tumorlysesyndrom
Tumoren: akute Leukämieaggressive Lymphomekleinzelliges BronchuskarzinomKeimzelltumore
Coiffier et al., J Clin Oncol 2008
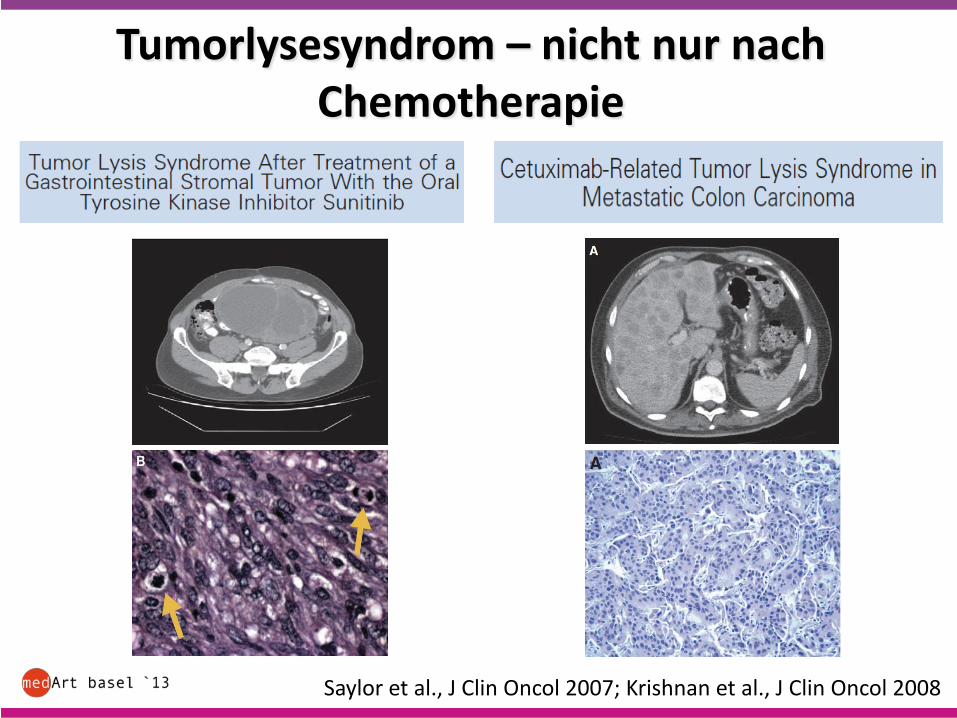
Tumorlysesyndrom – nicht nur nachChemotherapie
Saylor et al., J Clin Oncol 2007; Krishnan et al., J Clin Oncol 2008
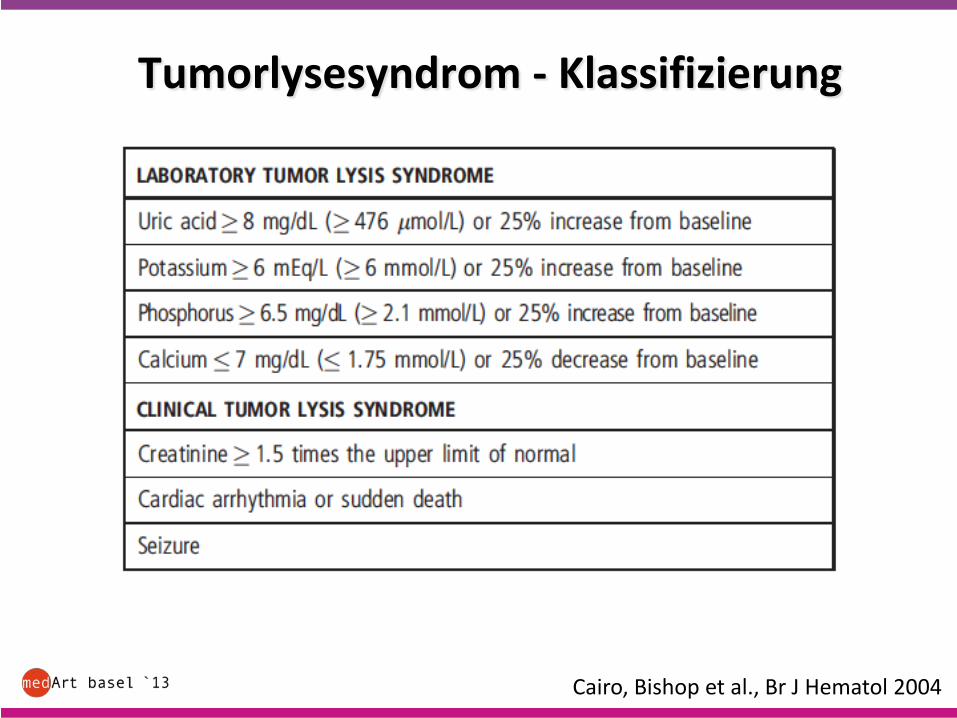
Tumorlysesyndrom - Klassifizierung
Cairo, Bishop et al., Br J Hematol 2004
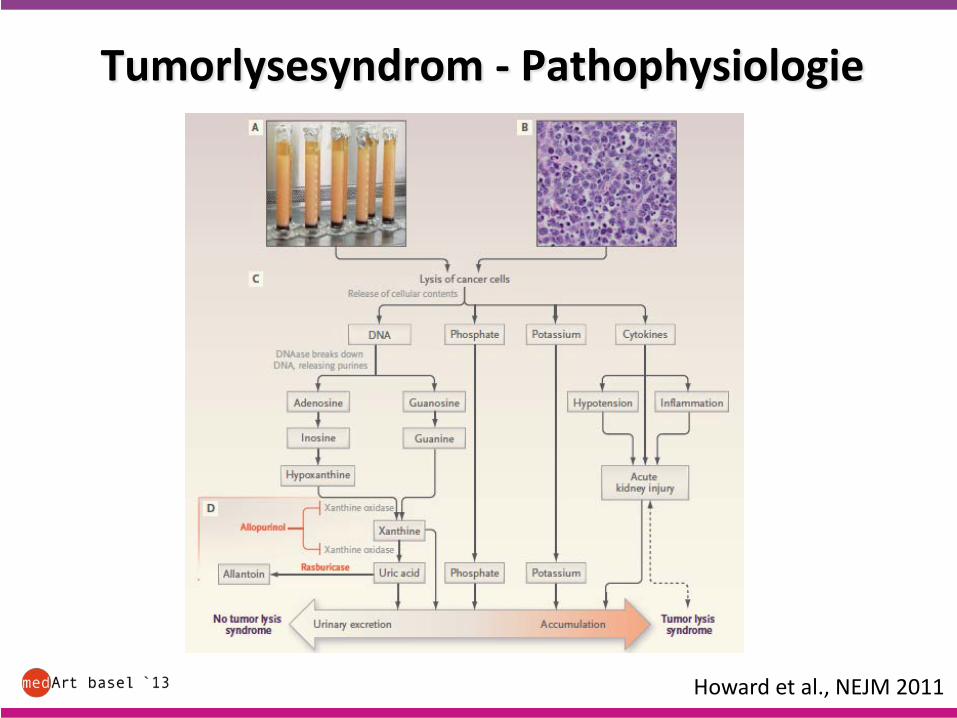
Tumorlysesyndrom - Pathophysiologie
Howard et al., NEJM 2011
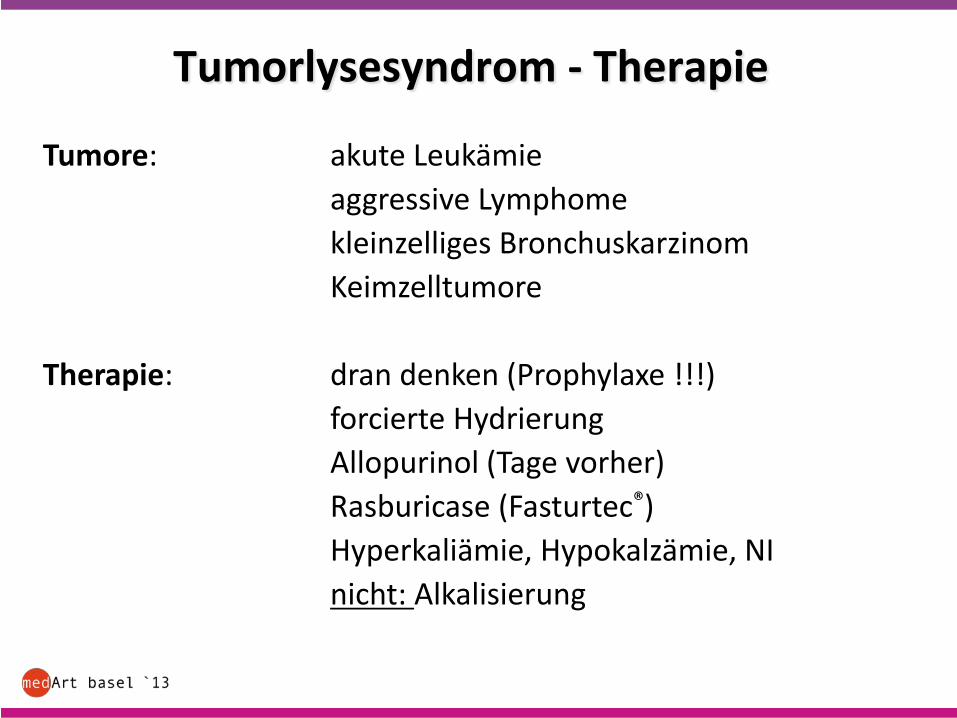
Tumorlysesyndrom - Therapie
Tumore: akute Leukämieaggressive Lymphomekleinzelliges BronchuskarzinomKeimzelltumore
Therapie: dran denken (Prophylaxe !!!)forcierte HydrierungAllopurinol (Tage vorher)Rasburicase (Fasturtec®)Hyperkaliämie, Hypokalzämie, NInicht: Alkalisierung
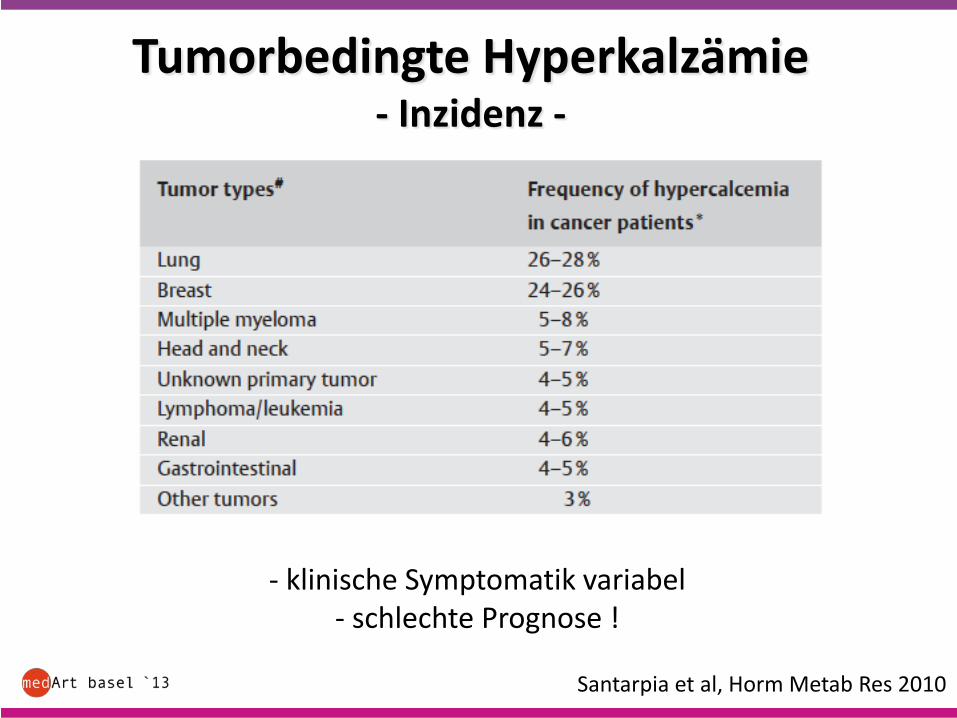
Tumorbedingte Hyperkalzämie- Inzidenz -
Santarpia et al, Horm Metab Res 2010
- klinische Symptomatik variabel- schlechte Prognose !
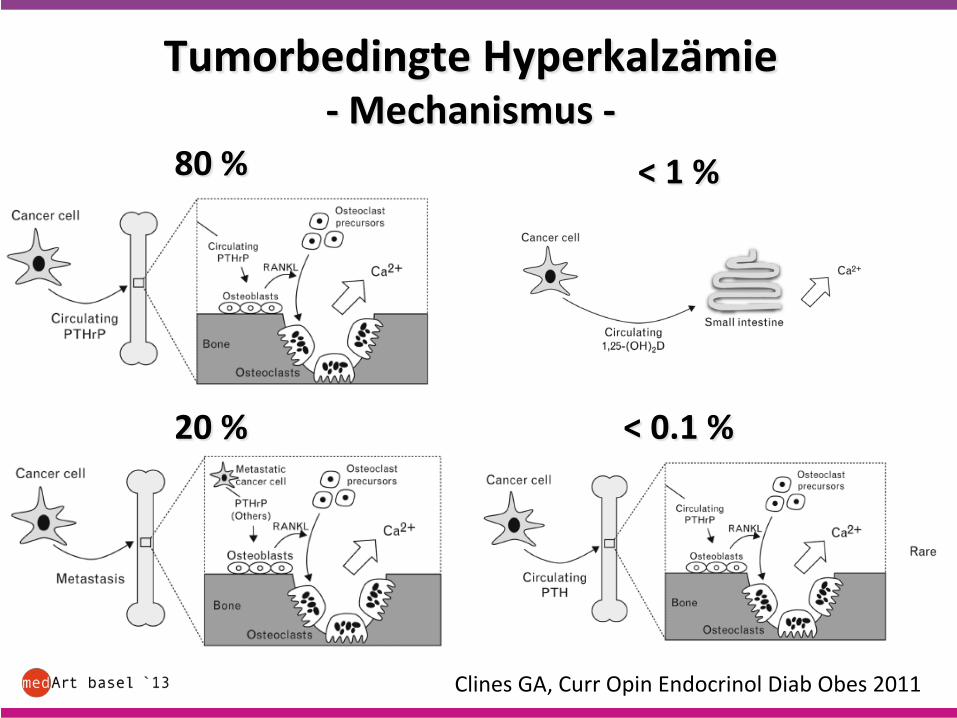
Tumorbedingte Hyperkalzämie- Mechanismus -
80 %
20 %
< 1 %
< 0.1 %
Clines GA, Curr Opin Endocrinol Diab Obes 2011
Hyperkalzämie
Dran denken !!!
• (Re-) Hydrierung
• Lasix ?
• Bisphosphonate (Geduld !, bei PTHrP weniger Effekt)
• Spezifische Tumor-Therapie
• Steroide ?
• (Calcitonin, Plicamycin, Galliumnitrat)
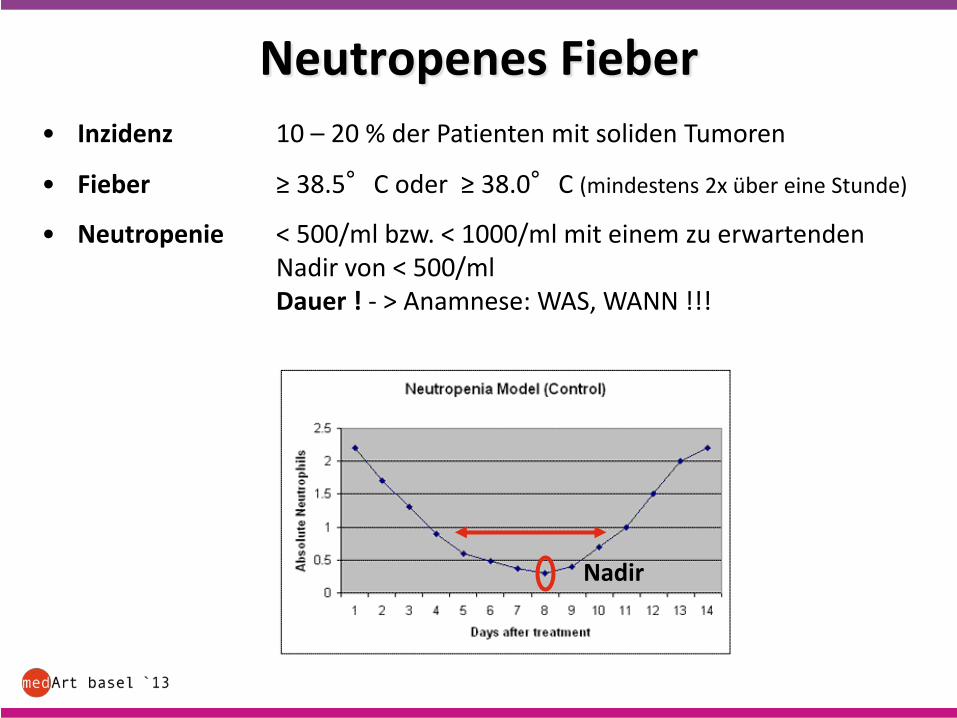
Neutropenes Fieber• Inzidenz 10 – 20 % der Patienten mit soliden Tumoren
• Fieber ≥ 38.5°C oder ≥ 38.0°C (mindestens 2x über eine Stunde)
• Neutropenie < 500/ml bzw. < 1000/ml mit einem zu erwartendenNadir von < 500/mlDauer ! - > Anamnese: WAS, WANN !!!
Nadir
Neutropenes Fieber
• Inzidenz 50% der Patienten mit soliden Tumoren
• Fieber im Ohr ≥ 38.3°C oder 2 x ≥ 38.0°C innert 1 h
• Neutropenie < 500/ml bzw. < 1000/ml mit einem zu erwartendenNadir von < 500/mlDauer ! - > Anamnese: WAS, WANN !!!(Nadir ≈ 7 -12 Tage nach der letzen Chemotherapie)
• Diagnostik BB, CRP, Chemogramm, BK, Thorax-Rx, Urin-Bakt
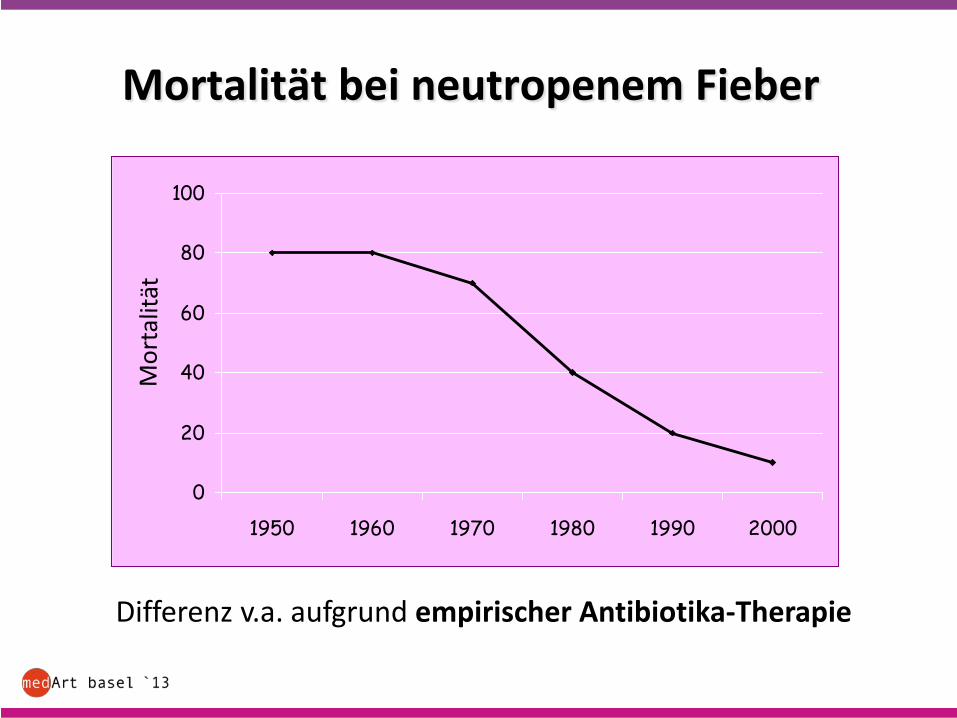
• Mortalität unbehandelt > 70%
• Therapie innert Stunden: empirische Antibiotika
0
20
40
60
80
100
1950 1960 1970 1980 1990 2000
Mortalität bei neutropenem Fieber
Differenz v.a. aufgrund empirischer Antibiotika-Therapie
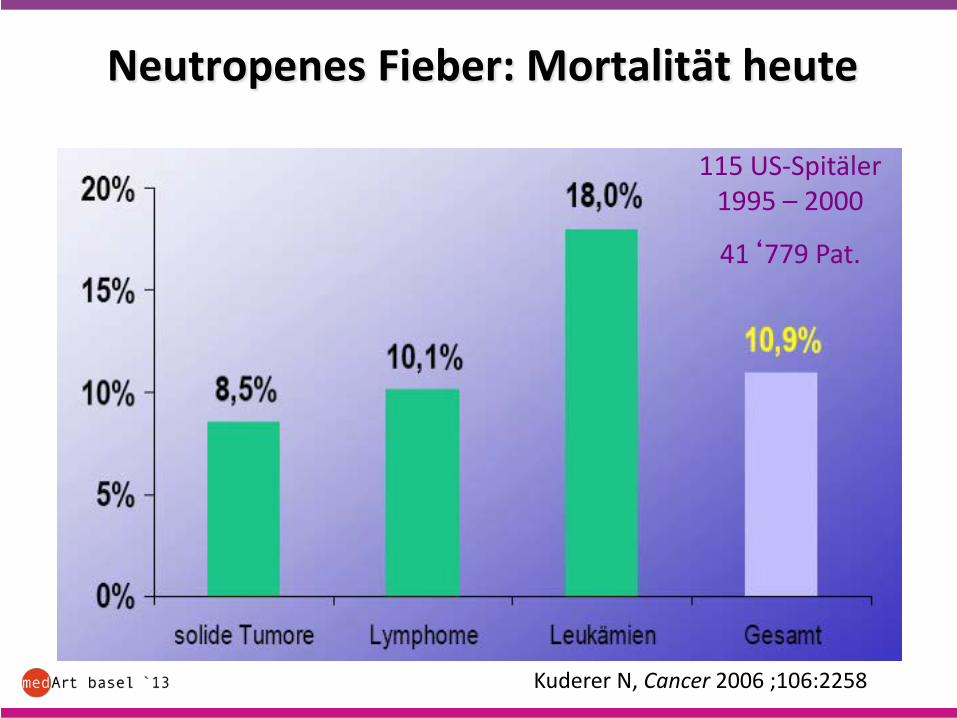
Neutropenes Fieber: Mortalität heute
Kuderer N, Cancer 2006 ;106:2258
115 US-Spitäler1995 – 2000
41‘779 Pat.
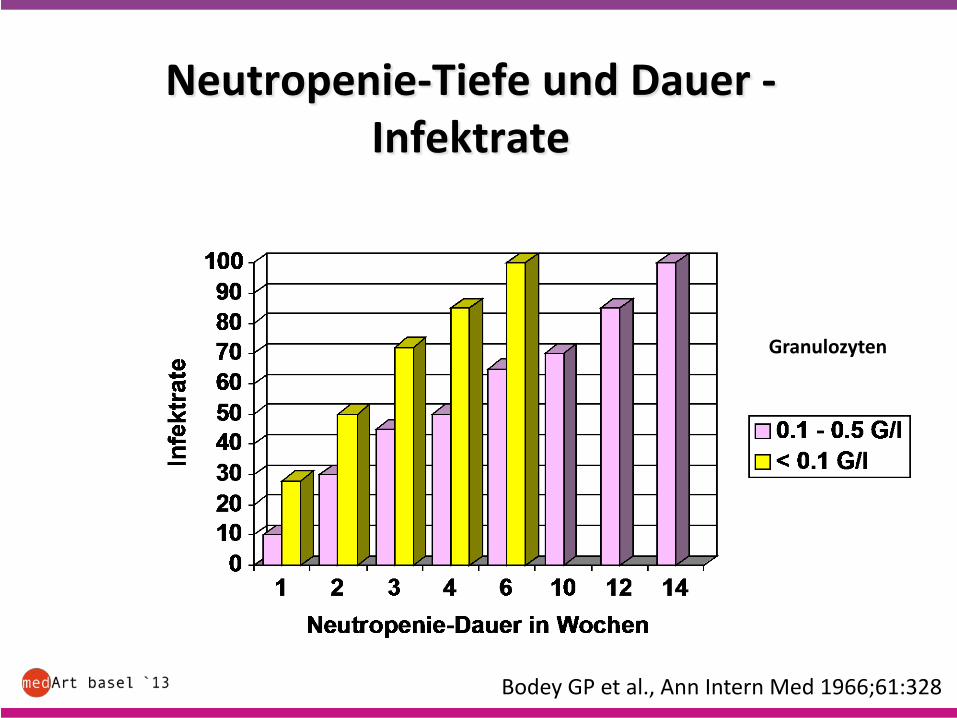
Neutropenie-Tiefe und Dauer -Infektrate
Bodey GP et al., Ann Intern Med 1966;61:328
Granulozyten
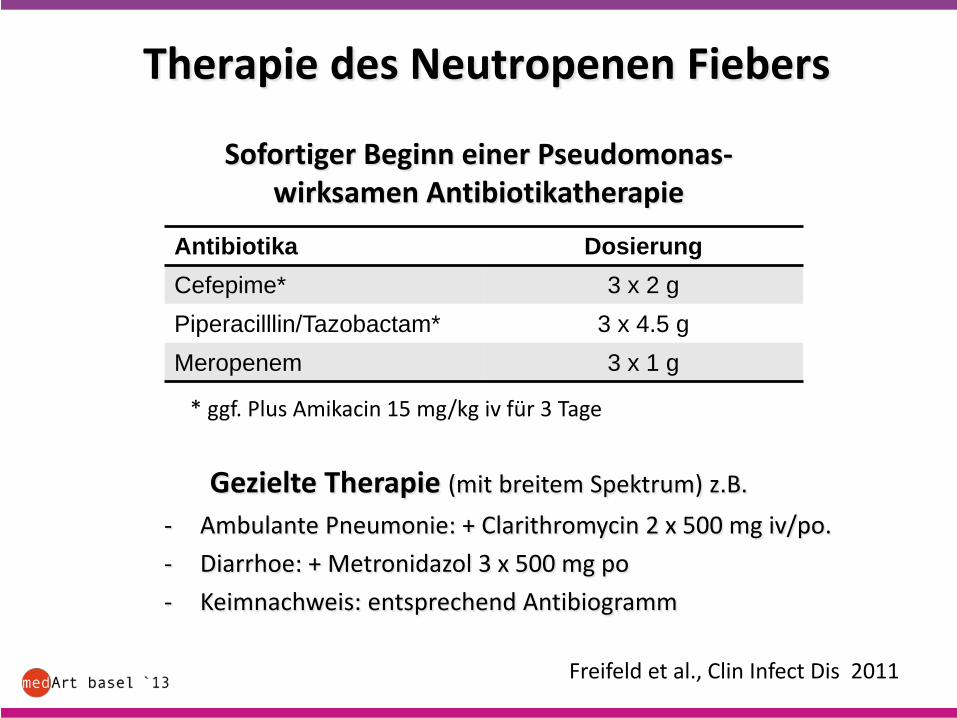
Therapie des Neutropenen Fiebers
Freifeld et al., Clin Infect Dis 2011
Antibiotika DosierungCefepime* 3 x 2 gPiperacilllin/Tazobactam* 3 x 4.5 gMeropenem 3 x 1 g
Sofortiger Beginn einer Pseudomonas-wirksamen Antibiotikatherapie
Gezielte Therapie (mit breitem Spektrum) z.B.- Ambulante Pneumonie: + Clarithromycin 2 x 500 mg iv/po.- Diarrhoe: + Metronidazol 3 x 500 mg po- Keimnachweis: entsprechend Antibiogramm
* ggf. Plus Amikacin 15 mg/kg iv für 3 Tage
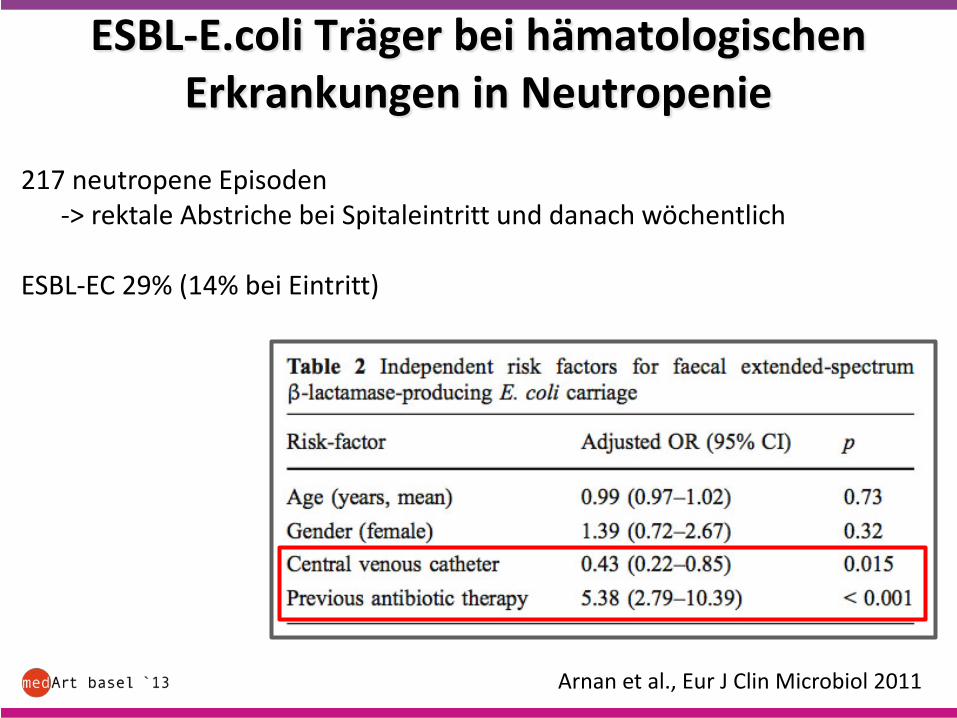
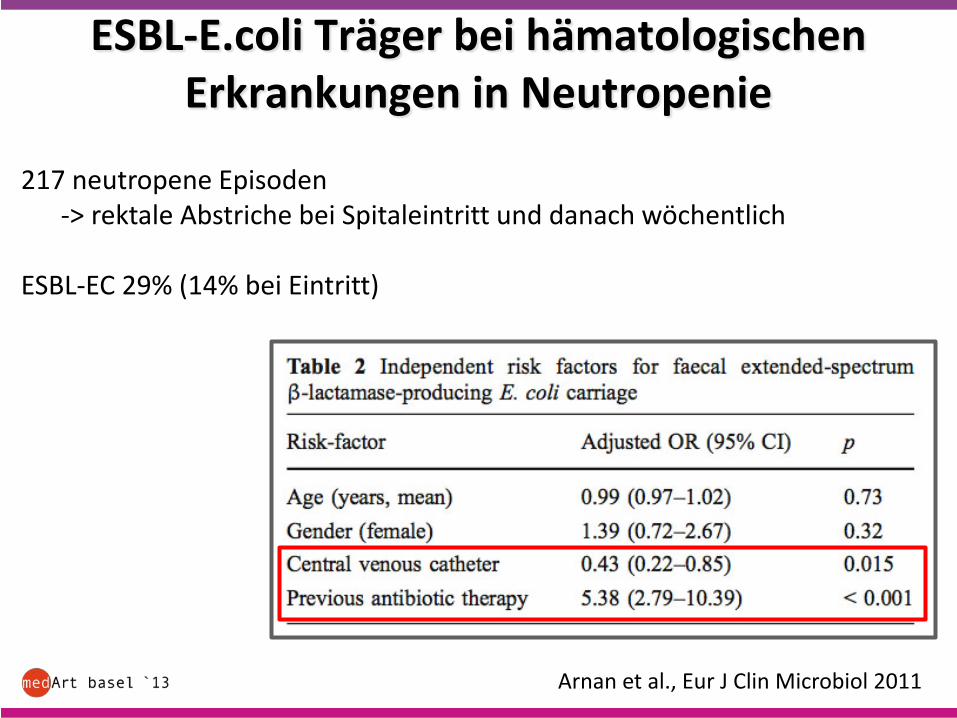
ESBL-E.coli Träger bei hämatologischen Erkrankungen in Neutropenie
Arnan et al., Eur J Clin Microbiol 2011
217 neutropene Episoden-> rektale Abstriche bei Spitaleintritt und danach wöchentlich
ESBL-EC 29% (14% bei Eintritt)
ESBL-E.coli Träger bei hämatologischen Erkrankungen in Neutropenie
Arnan et al., Eur J Clin Microbiol 2011
217 neutropene Episoden-> rektale Abstriche bei Spitaleintritt und danach wöchentlich
ESBL-EC 29% (14% bei Eintritt)
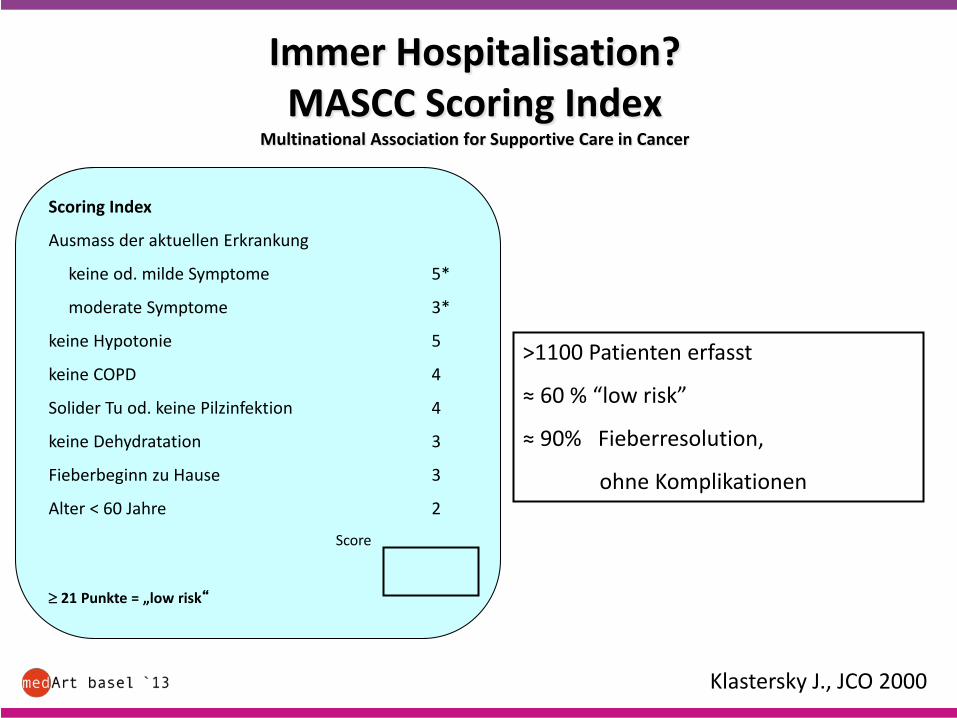
Immer Hospitalisation?MASCC Scoring Index
Multinational Association for Supportive Care in Cancer
Scoring Index
Ausmass der aktuellen Erkrankung
keine od. milde Symptome 5*
moderate Symptome 3*
keine Hypotonie 5
keine COPD 4
Solider Tu od. keine Pilzinfektion 4
keine Dehydratation 3
Fieberbeginn zu Hause 3
Alter < 60 Jahre 2
Score
≥ 21 Punkte = „low risk“
>1100 Patienten erfasst
≈ 60 % “low risk”
≈ 90% Fieberresolution,
ohne Komplikationen
Klastersky J., JCO 2000
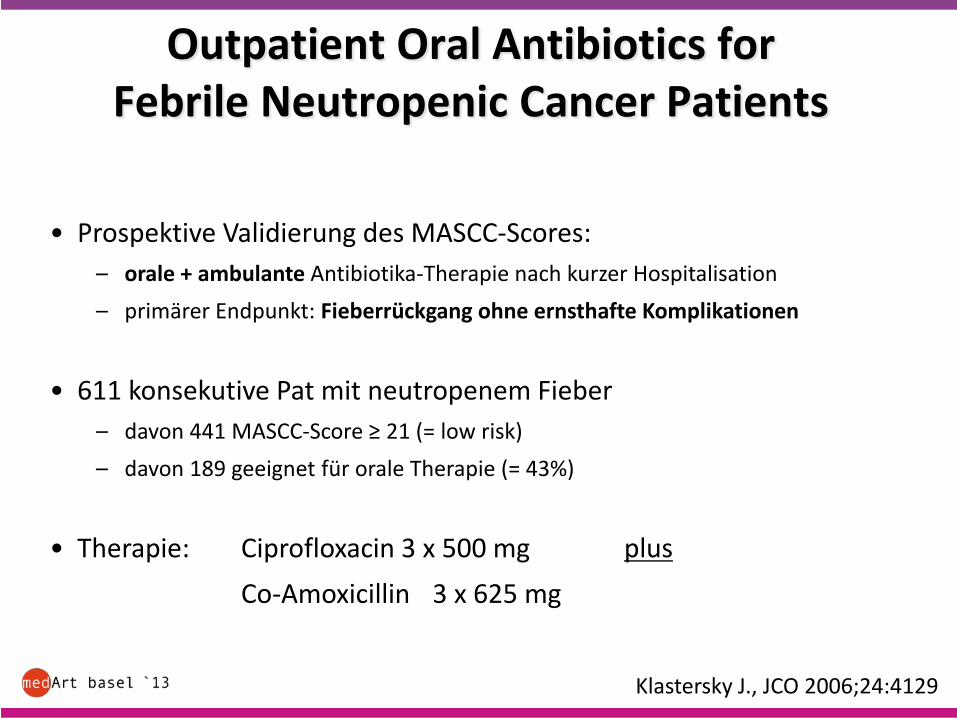
Outpatient Oral Antibiotics forFebrile Neutropenic Cancer Patients
• Prospektive Validierung des MASCC-Scores:– orale + ambulante Antibiotika-Therapie nach kurzer Hospitalisation– primärer Endpunkt: Fieberrückgang ohne ernsthafte Komplikationen
• 611 konsekutive Pat mit neutropenem Fieber– davon 441 MASCC-Score ≥ 21 (= low risk)– davon 189 geeignet für orale Therapie (= 43%)
• Therapie: Ciprofloxacin 3 x 500 mg plusCo-Amoxicillin 3 x 625 mg
Klastersky J., JCO 2006;24:4129
Outpatient oral antibiotics for NF
• 5% ernsthafte Komplikationen
– früh entlassene (n = 79): • 0% ernsthafte Komplikationen• 4% Wiedereintritte (Stomatitis, Schüttelfrost, pers. Fieber)
– spät entlassene (n = 99):• 9% ernsthafte Komplikationen (2% )
Hypotonie, Konfusion, Sepsis, ANV, Resp. Insuffizienz
Klastersky J., JCO 2006
Ambulante Therapie für neutropenes Fieber: Ja, aber:
• nur für ausgewählte low-risk Patienten (MASCC ≥ 21 Punkte)
• Nach 24 Std. stationärer Beobachtung• klin. Kontrolle + BE min. alle 2 Tage, dazw. Telefon-Kontakt• genaue Instruktion bezüglich Verhalten bei Fieber oder
Komplikationen mit sofortiger Re-Hospitalisation• Antibiotika:
– Augmentin 3 x 625mg– Ciproxin 2 x 750mg
G-CSF?
Primäre Prophylaxe:
• Reduktion der Inzidenz, Länge und Schwere
• Reduktion der Mortalität (early + infection – related)
• Steigerung der Chemotherapie-Dosis
-> Empfehlung: bei ≥ 20% Risiko (kurativ, ≥ 10% mit RF)
Clark et al, J Clin Oncol 2005; Kuderer et al, J Clin Oncol 2007Clinical Practive Guidelines of the Infectious Diseases Society of America 2010
Neutropenes Fieber:
• Verkürzung der Neutropeniedauer sowie Hospitalisation
• kein Einfluss auf Mortalität (early + infection – related)
-> keine Empfehlung
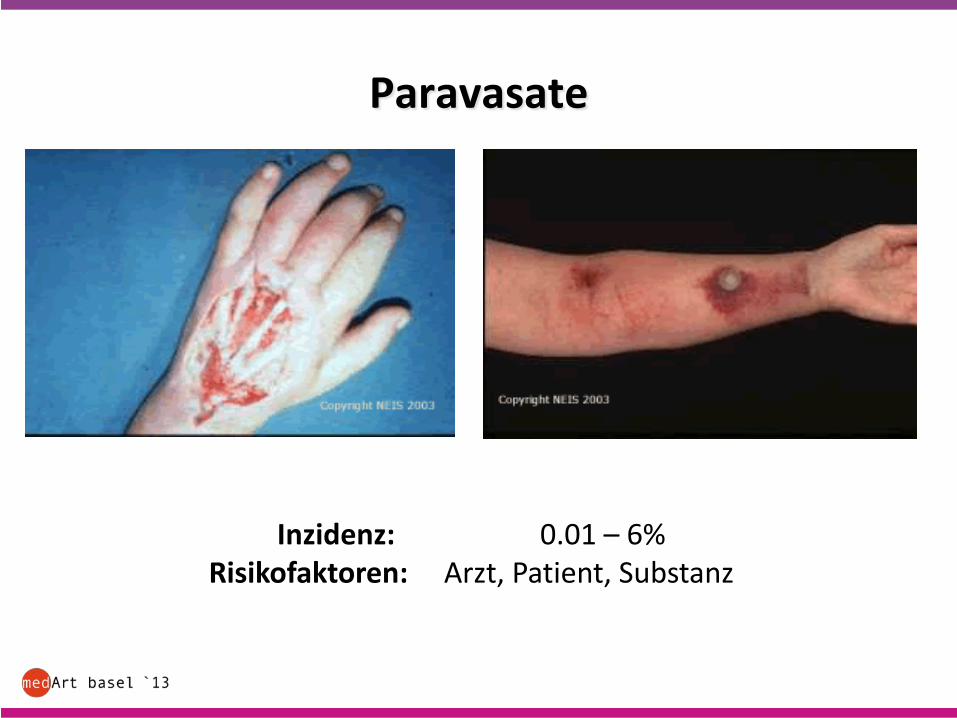
Paravasate
Inzidenz: 0.01 – 6%Risikofaktoren: Arzt, Patient, Substanz
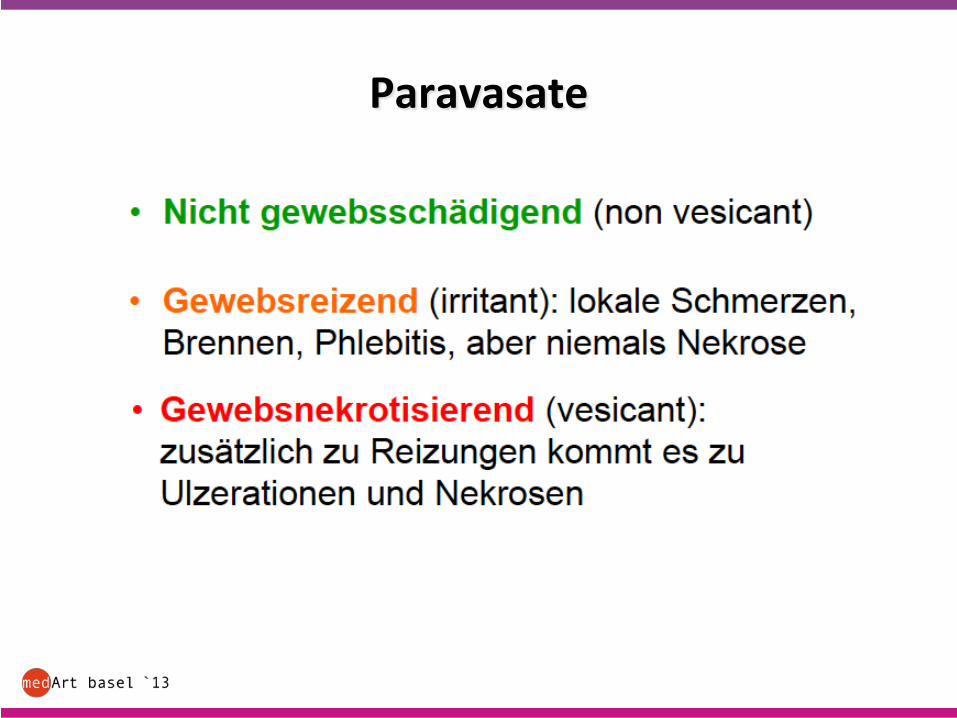
Paravasate
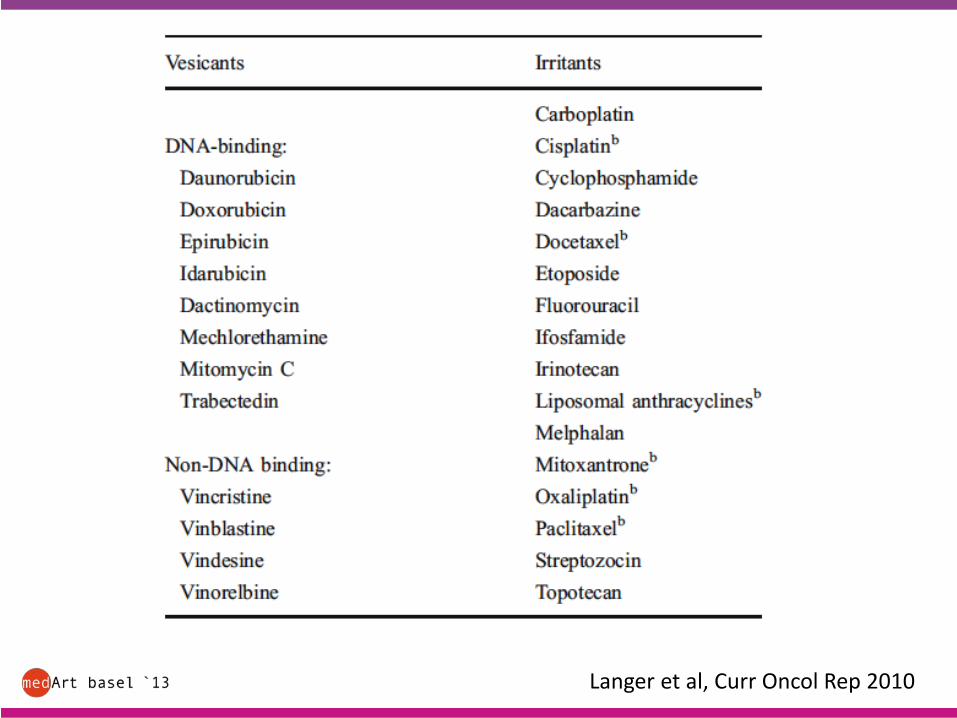
Langer et al, Curr Oncol Rep 2010
Paravasate: Erste Massnahmen
• Infusion STOP
• Nadel belassen/nicht spülen
• Arm hoch lagern
• Aspiration aus Nadel/Subcutis
• Kein Druck
• Spezifische Massnahmen
• Dokumentieren!!!
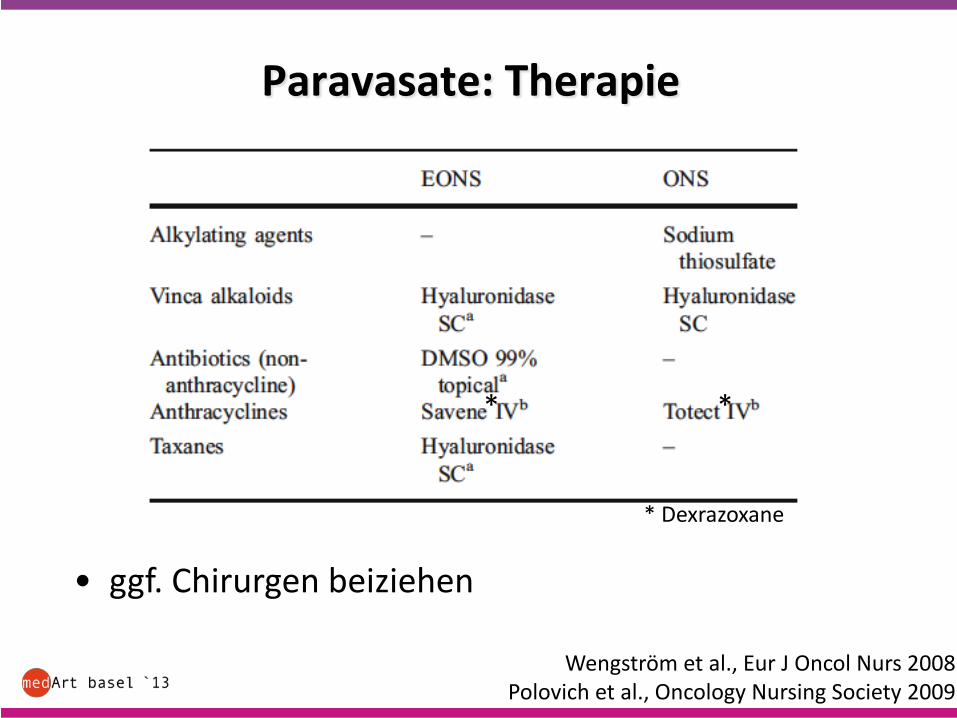
Paravasate: Therapie
• ggf. Chirurgen beiziehen
Wengström et al., Eur J Oncol Nurs 2008Polovich et al., Oncology Nursing Society 2009
* *
* Dexrazoxane
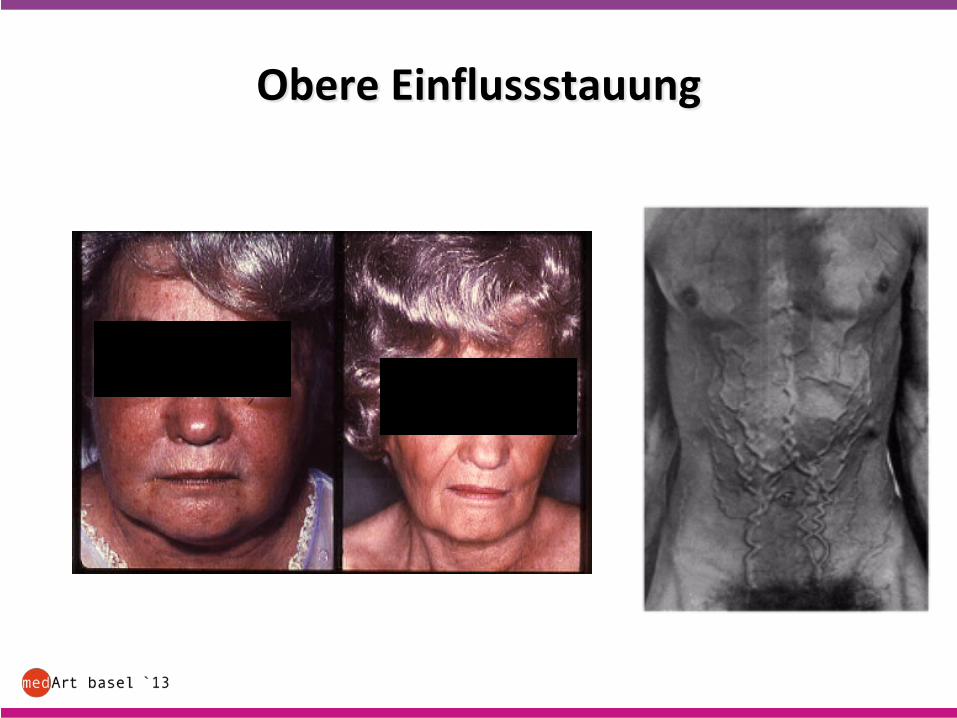
Obere Einflussstauung
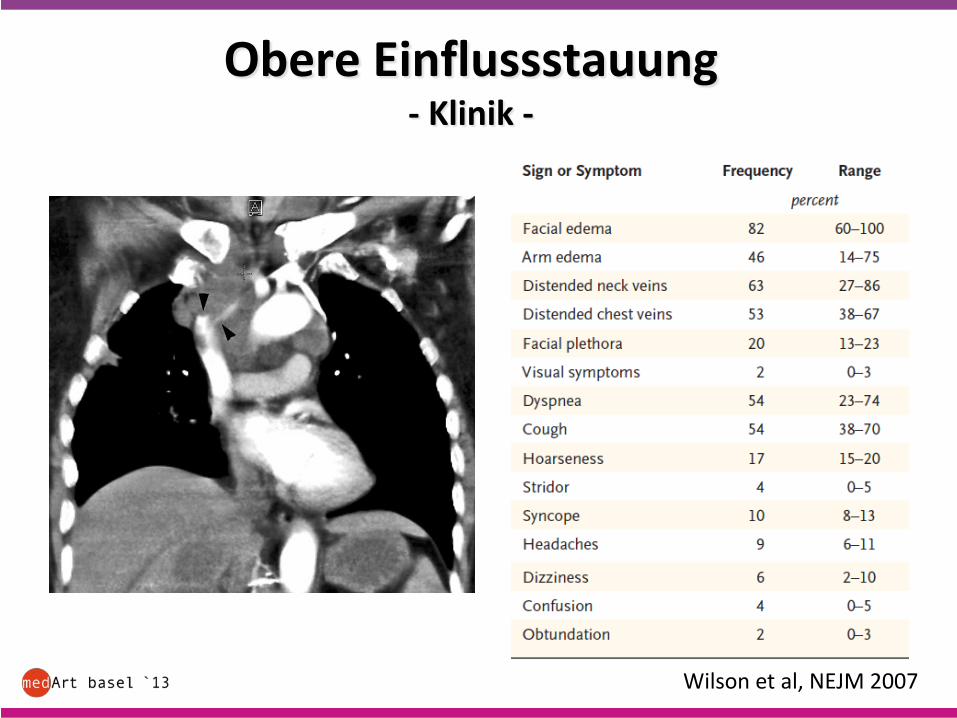
Obere Einflussstauung- Klinik -
Wilson et al, NEJM 2007
Wilson et al, NEJM 2007
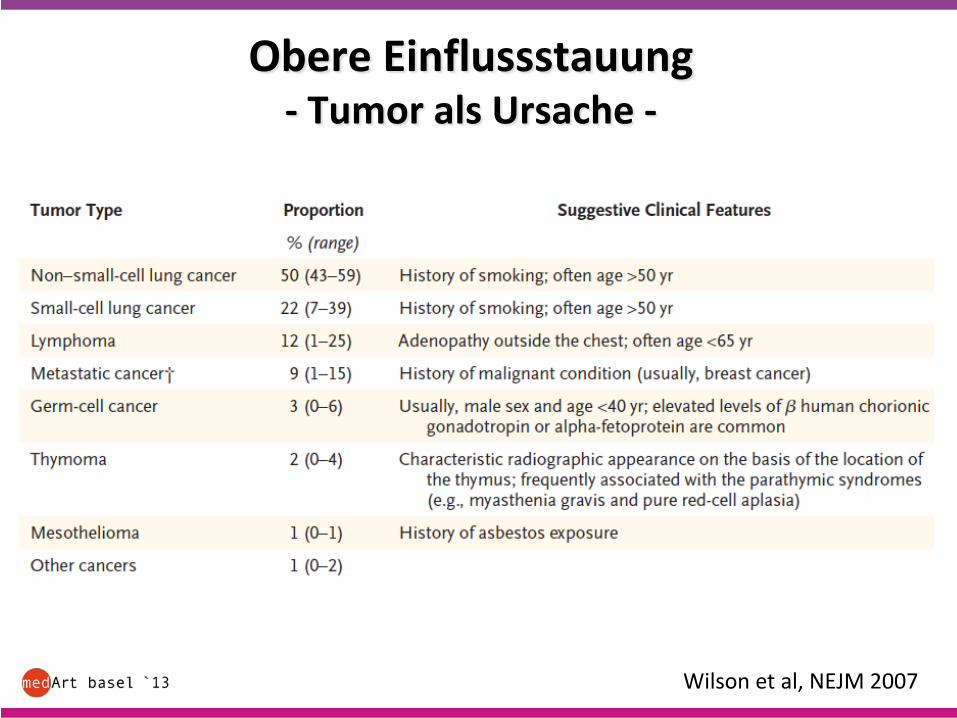
Obere Einflussstauung- Tumor als Ursache -
Wilson et al, NEJM 2007
Obere Einflussstauung- Therapie -
• Diagnostik
• Supportive Therapie (Steroide ?)
• Chirurgie
• Chemotherapie
• Radiotherapie
• Stent
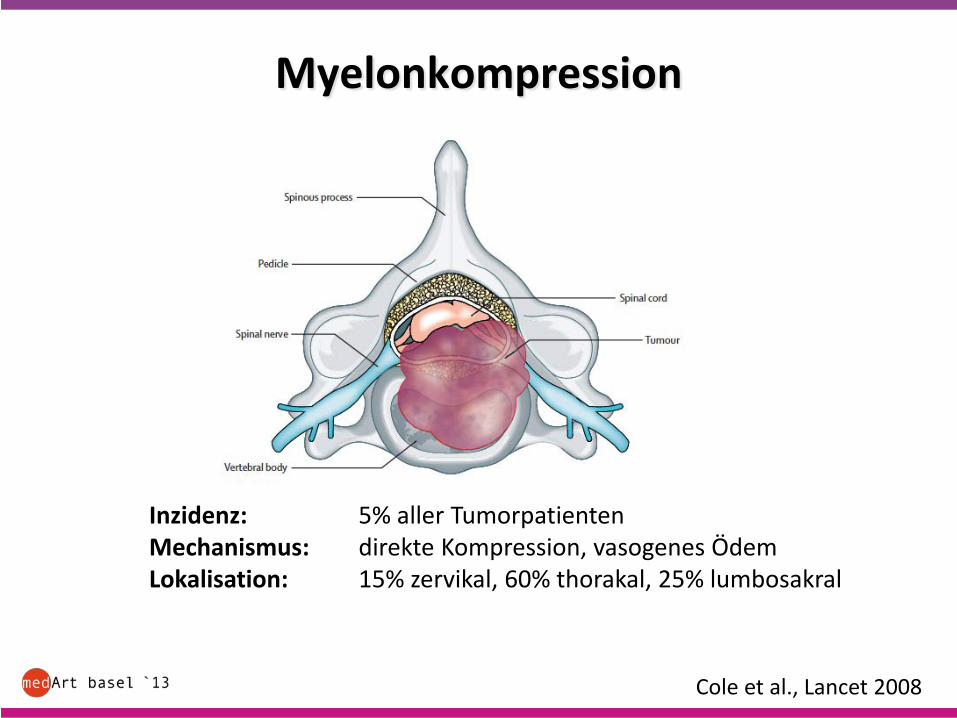
Myelonkompression
Cole et al., Lancet 2008
Inzidenz: 5% aller TumorpatientenMechanismus: direkte Kompression, vasogenes ÖdemLokalisation: 15% zervikal, 60% thorakal, 25% lumbosakral
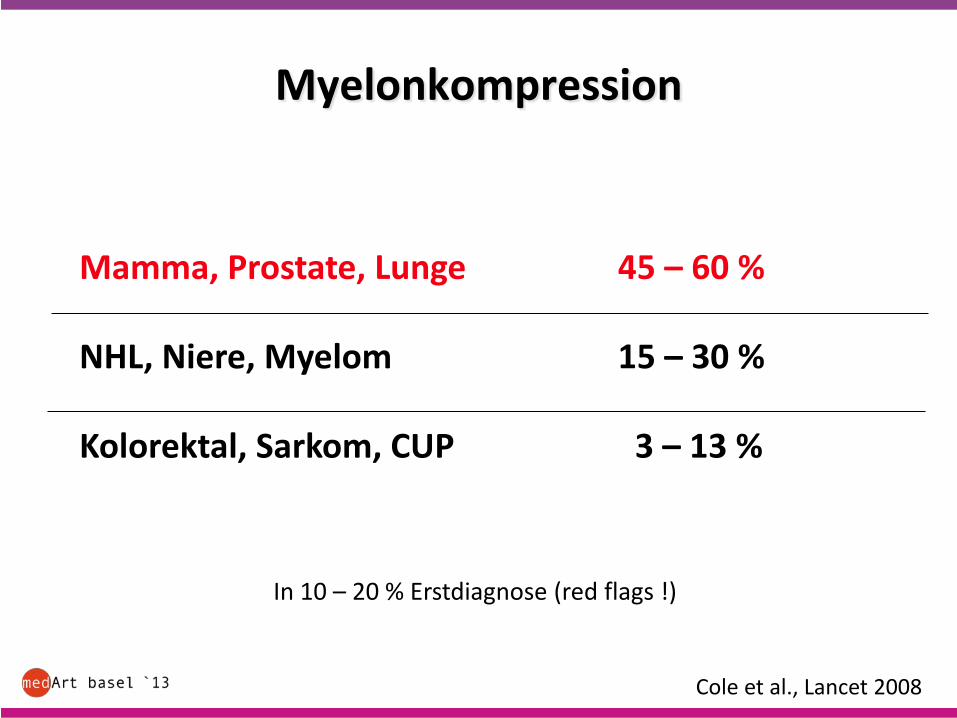
Myelonkompression
Cole et al., Lancet 2008
Mamma, Prostate, Lunge 45 – 60 %
NHL, Niere, Myelom 15 – 30 %
Kolorektal, Sarkom, CUP 3 – 13 %
In 10 – 20 % Erstdiagnose (red flags !)
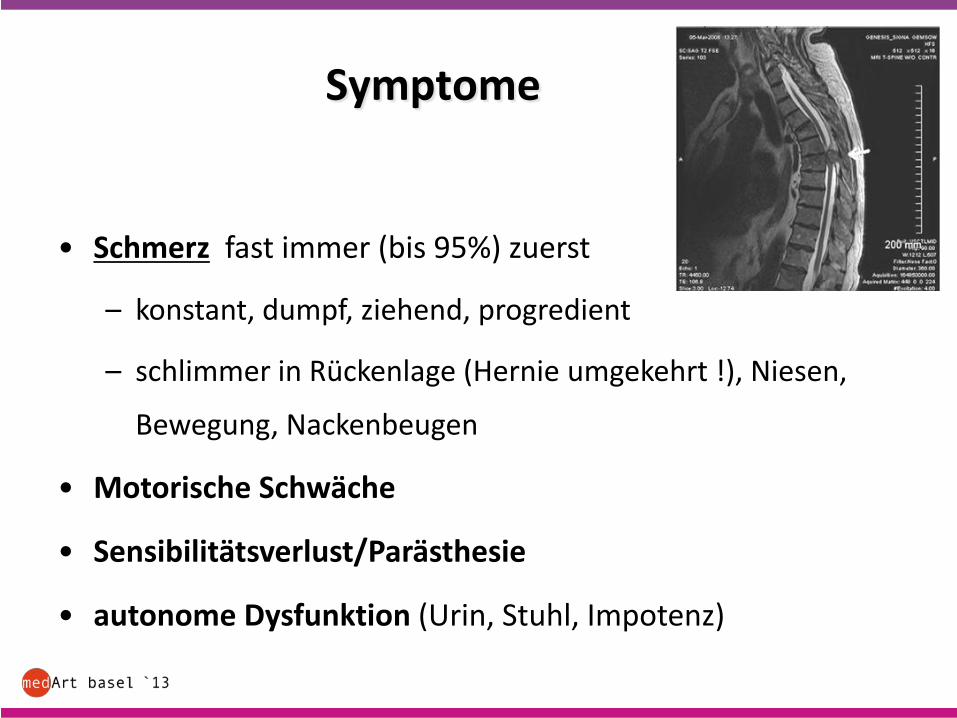
Symptome
• Schmerz fast immer (bis 95%) zuerst
– konstant, dumpf, ziehend, progredient
– schlimmer in Rückenlage (Hernie umgekehrt !), Niesen,
Bewegung, Nackenbeugen
• Motorische Schwäche
• Sensibilitätsverlust/Parästhesie
• autonome Dysfunktion (Urin, Stuhl, Impotenz)
Behandlung
• Dexamethason
>10 mg i.v., dann 4-8 mg alle 6 Std.wenn stabil, alle 4 Tage Dosisreduktion
• Multidisziplinär:
– Chemotherapie
– Radiotherapie
– Chirurgie
Radiotherapie
• wichtigste Therapieform
• radiosensitive Tumoren ohne spinale Instabilität oder knöcherne Kompression des Myelons
• Dosis und Fraktionierung unklar
Chirurgie
Chirurgische Dekompression:
• rasche neurologische Progression
• spinale Instabilität oder knöcherne Kompression des Myelon(Wirbel-Hinterwand)
• kein Ansprechen auf Radiotherapie
aber: individuelle Entscheidung für den einzelnen Patienten !
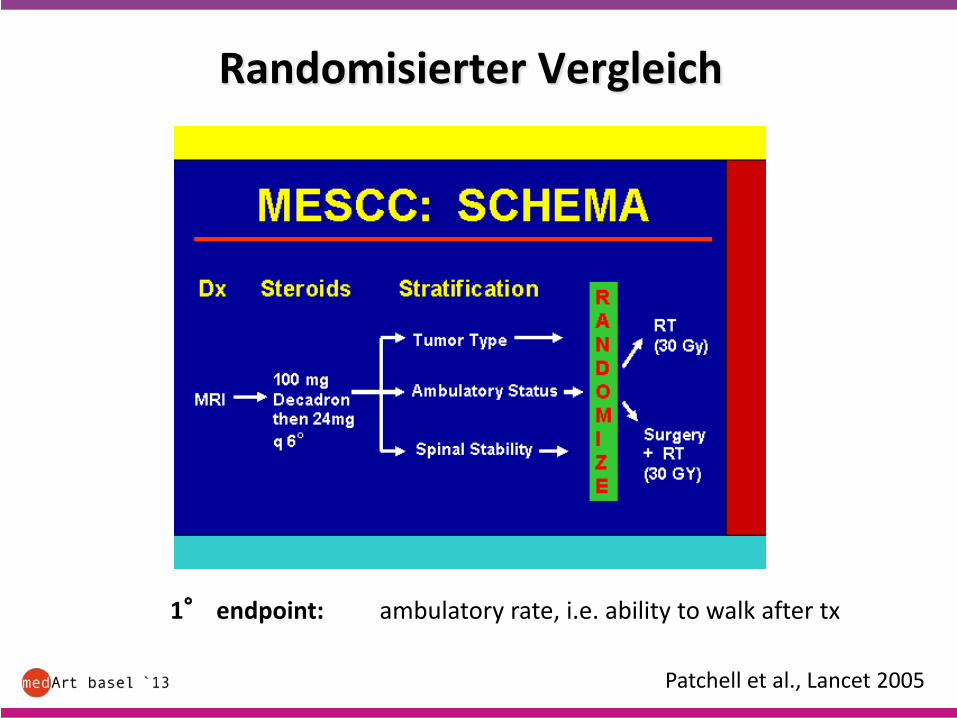
Randomisierter Vergleich
Patchell et al., Lancet 2005
1° endpoint: ambulatory rate, i.e. ability to walk after tx
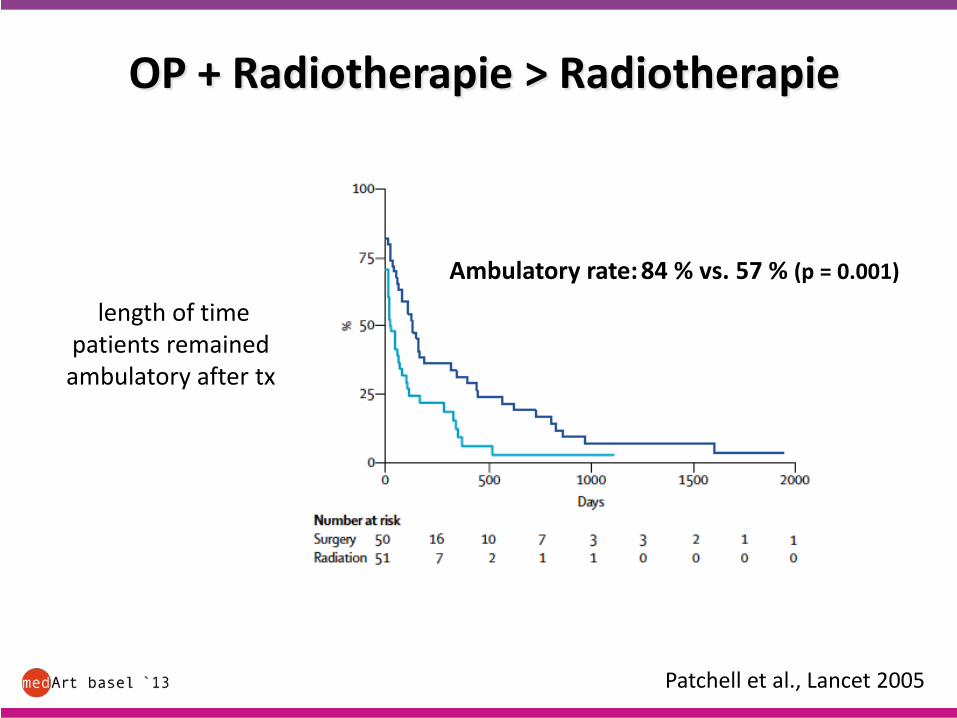
Patchell et al., Lancet 2005
length of timepatients remained ambulatory after tx
OP + Radiotherapie > Radiotherapie
Ambulatory rate: 84 % vs. 57 % (p = 0.001)
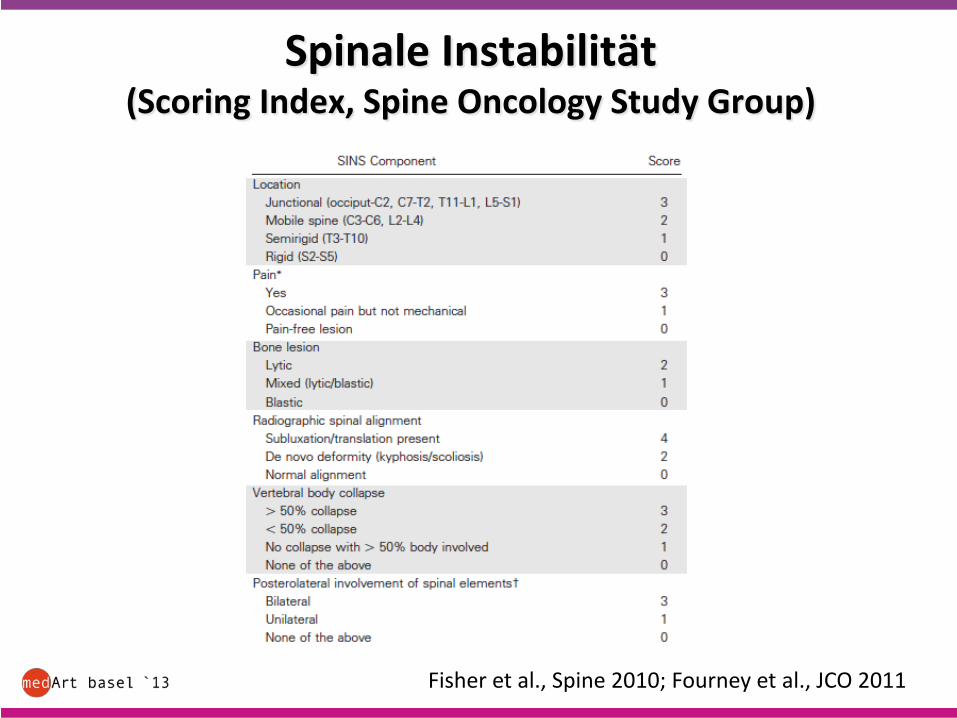
Spinale Instabilität(Scoring Index, Spine Oncology Study Group)
Fisher et al., Spine 2010; Fourney et al., JCO 2011
Myelonkompression„Take Home Messages“
Wenn immer möglich, die drei Fachdisziplinen Chirurgie, Radiotherapie, Onkologie gleichzeitig am Patientenbett
Geschwindigkeit entscheidend !!!(ca. 80% können später gehen, wenn noch keine Paralyse bei Therapiebeginn - sonst ca. 10%)
Literatur zu Referat „Onkologische Notfälle“, A. Zippelius:
1. Howard SC, Jones DP, Pui C-H The tumor lysis syndrome. New England J.
Medicine 2011; 364: 1844-1854
2. Clines GA Mechanisms and treatment of hyercalcemia of malignancy. Curr
Opin Endocrinol Diabetes Obes 2011; 18: 339-346
3. Bennett CL, Djulbegovic B, Norris LB, Armitage JO. Colony-stimulating
factors for febrile neutropenia during cancer therapy. N Engl J Med 2013;
368: 1131-1139.
4. Flowers CR, Seidenfeld J, Bow EJ, Karten C, Gleason C, Hawley DK,
Kuderer NM, Langston AA, Marr KA, Rolston KV, Ramsey SD. Antimicrobial
prophylaxis and outpatient management of fever and neutropenia in adults
treated for malignancy: American Society of Clinical Oncology clinical practice
guideline. J Clin Oncology 2013; 31: 794-810
5. Wilson LD, Detterbeck FC, Yahalom J. Superior Vena cava sysndrome with
malignant causes. New England J Medicine 2007; 356:1862-1869
6. Cole JS, Patchell RA. Metastatic epidural spinal cord compression. Lancet
Neurol 2008; 7:459-466
7. McCurdy MT, Shanholtz CB. Oncologic emergencies. Crit Care Med 2012;
40:2212-2222
8. Morgan C, Tillett T, Braybrooke J, Ajithkumar T. Management of uncommon
chemotherapy-induced emergencies. Lancet Oncol 2011; 12:806-814
















![Mund- und Zahnpflege - Klinikum-Passau · 2] Seite Mundschleimhaut und Onkologie 5 Veränderungen der Mundschleimhaut Stomatitis 6 Soor 7 Xerostomie 8 Blutungsneigung 10 Pflege des](https://img.pdfslide.org/doc/110x75/5d55e9f788c993b51c8b7df8/mund-und-zahnpflege-klinikum-passau-2-seite-mundschleimhaut-und-onkologie.jpg)







![Pflegerische Interventionen in der letzten Lebensphase ... · Stomatitis oder Soorbefall [5]. Die Ansiedlung der Mikroorganismen erfolgt durch den Kontakt des Menschen mit seiner](https://img.pdfslide.org/doc/110x75/5b09374d7f8b9af0438d5c4e/pflegerische-interventionen-in-der-letzten-lebensphase-oder-soorbefall-5.jpg)
![KL 2 Otitis Stomatitis Tonsillitis [Kompatibilitätsmodus] · 6fkxo]hqwuxp 6slh] 1266 03$ .udqnkhlwvohkuh 2wlwlv 6wrpdwlwlv 7rqvloolwlv 2wlwlv phgld 6\pswrph yhujo %xfk 7khudslh](https://img.pdfslide.org/doc/110x75/6078cf1fb715d5605b30d214/kl-2-otitis-stomatitis-tonsillitis-kompatibilitftsmodus-6fkxohqwuxp-6slh.jpg)


