Embed Size (px)
Citation preview

Pro-Contra - Verschluss der SFA > 25 cm:First Line Perkutan
Prof. Dr. T. Zeller
Universitäts-Herz-ZentrumFreiburg-Bad Krozingen
InterdisziplinäresGefäßzentrum
Bad Krozingen
BAD KROZINGENBAD KROZINGEN
Thomas Zeller, MD
For the 12 months preceding this presentation, I disclose thefollowing types of financial relationships:
• Honoraria received from: Abbott Vascular, Bard Peripheral Vascular,Veryan, Biotronik, Boston Scientific Corp., Cook Medical, Gore &Associates, Medtronic, Philips-Spectranetics, TriReme, Veryan, Shockwave,Biotronik
• Consulted for: Boston Scientific Corp., Cook Medical, Gore & Associates,Medtronic, Spectranetics, Veryan
• Research, clinical trial, or drug study funds received from: Biotronik, 480biomedical, Bard Peripheral Vascular, Veryan, Biotronik, Cook Medical,Gore & Associates, Abbott Vascular, Medtronic, Philips, Terumo, TriReme,Veryan, Shockwave
• Common stock: Veryan, QT Medical
2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with ESVS(European Heart Journal 2017; doi:10.1093/eurheartj/ehx095)
www.escardio.org/guidelines
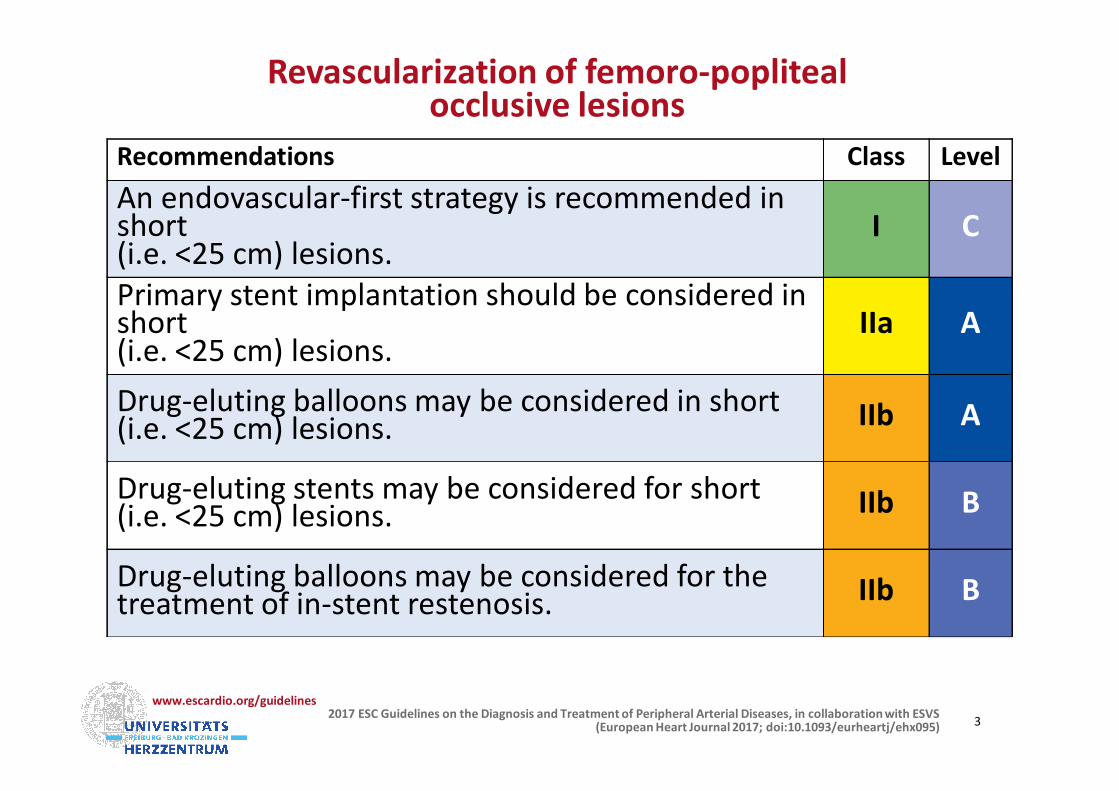
Revascularization of femoro-poplitealocclusive lesions
3
Recommendations Class Level
An endovascular-first strategy is recommended inshort(i.e. <25 cm) lesions.
I C
Primary stent implantation should be considered inshort(i.e. <25 cm) lesions.
IIa A
Drug-eluting balloons may be considered in short(i.e. <25 cm) lesions. IIb A
Drug-eluting stents may be considered for short(i.e. <25 cm) lesions. IIb B
Drug-eluting balloons may be considered for thetreatment of in-stent restenosis. IIb B
2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with ESVS(European Heart Journal 2017; doi:10.1093/eurheartj/ehx095)
www.escardio.org/guidelines
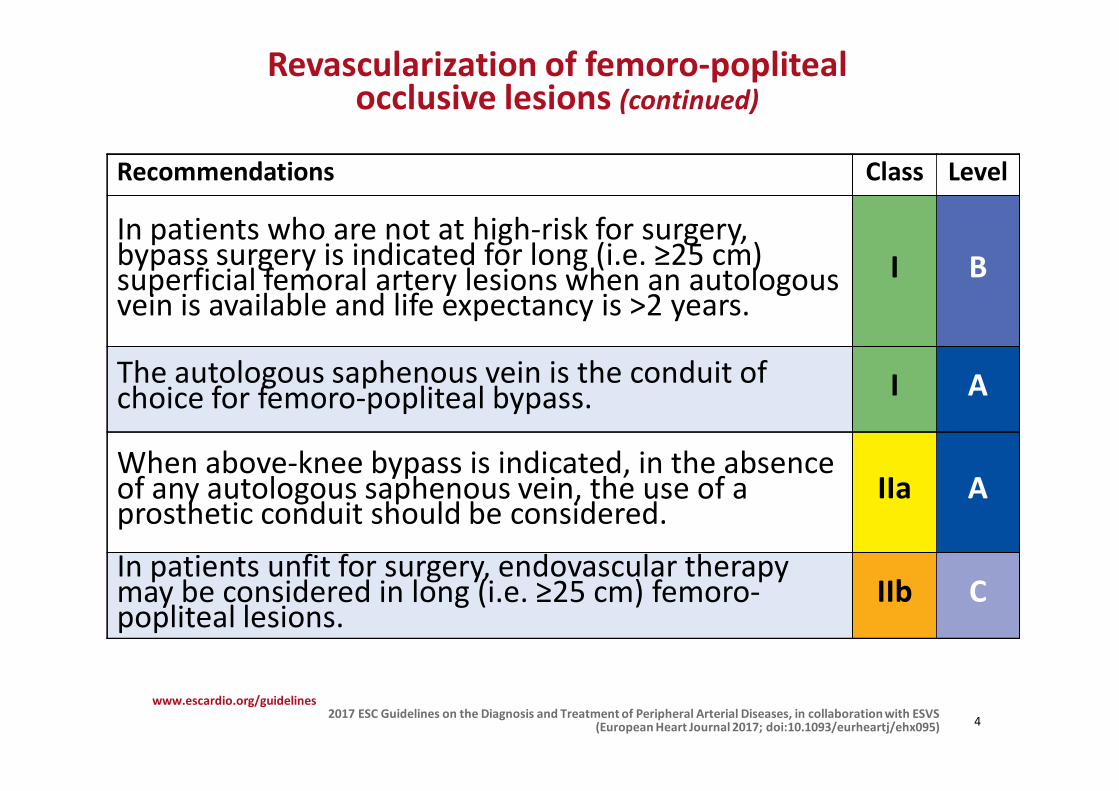
Revascularization of femoro-poplitealocclusive lesions (continued)
4
Recommendations Class Level
In patients who are not at high-risk for surgery,bypass surgery is indicated for long (i.e. ≥25 cm) superficial femoral artery lesions when an autologousvein is available and life expectancy is >2 years.
I B
The autologous saphenous vein is the conduit ofchoice for femoro-popliteal bypass. I A
When above-knee bypass is indicated, in the absenceof any autologous saphenous vein, the use of aprosthetic conduit should be considered.
IIa A
In patients unfit for surgery, endovascular therapymay be considered in long (i.e. ≥25 cm) femoro-popliteal lesions.
IIb C
What are the arguments of the promotors ofsurgery first?
Old fashioned, outdated and underpowered!!
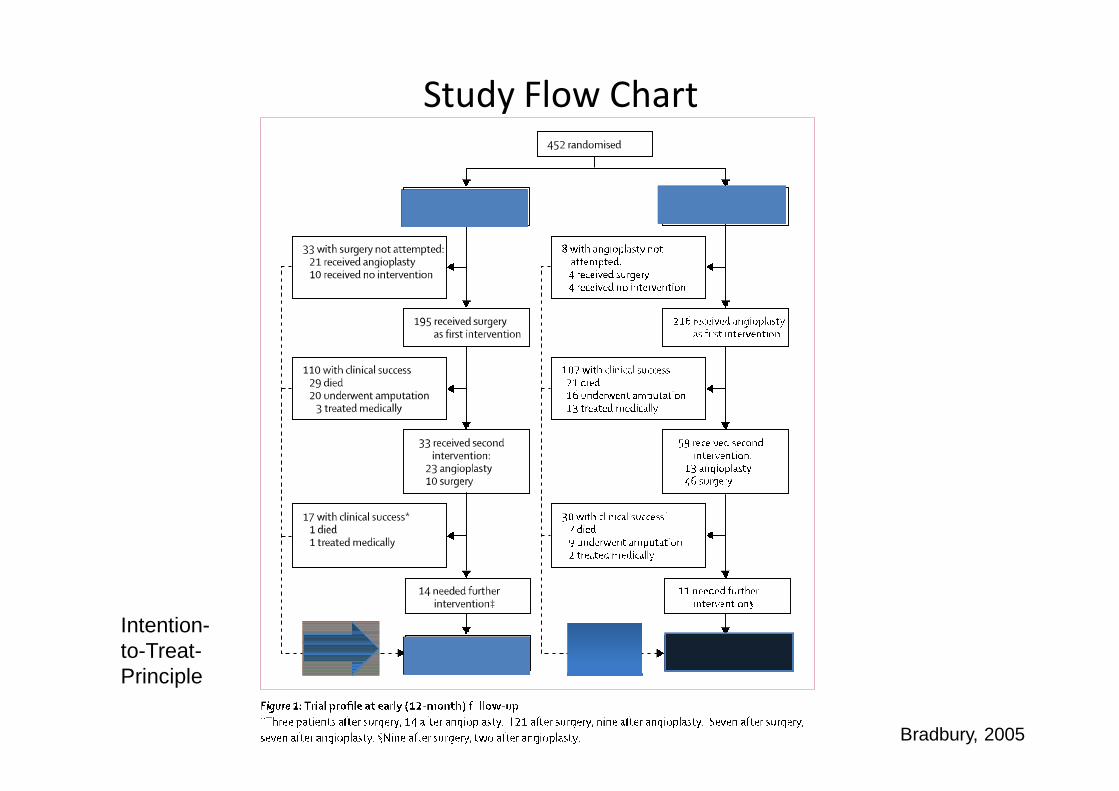
Study Flow Chart
Intention-to-Treat-Principle
Bradbury, 2005
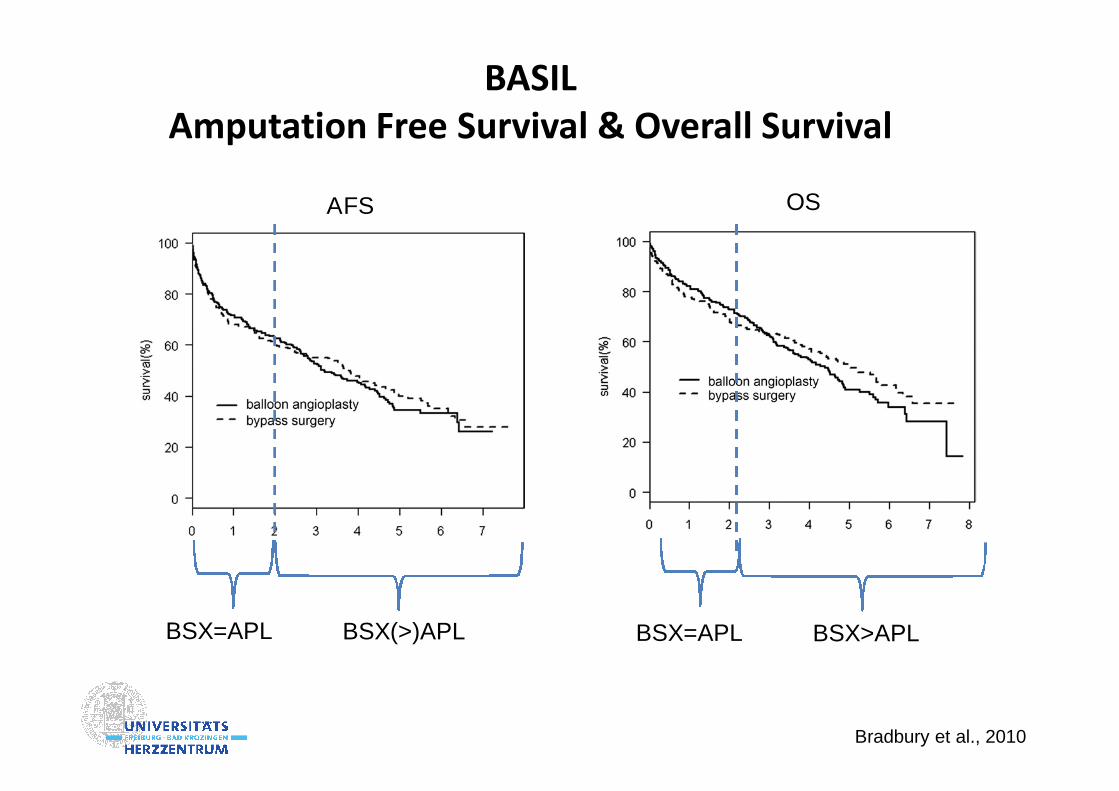
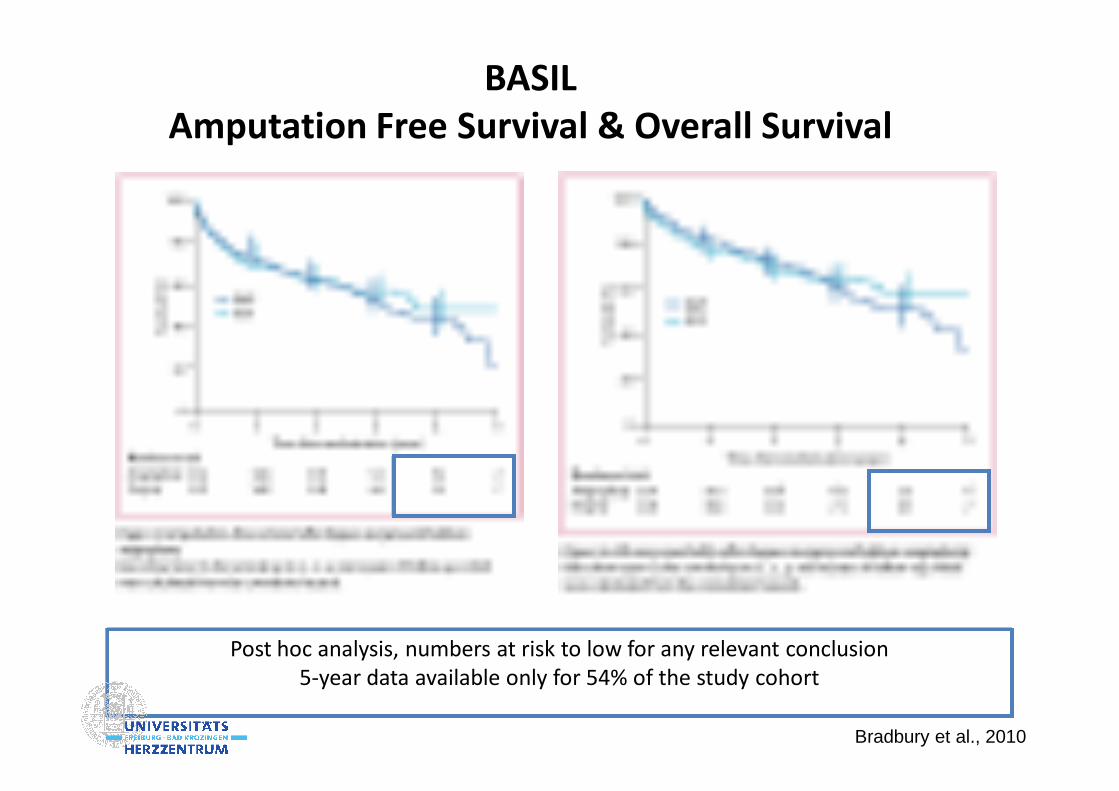
BASILAmputation Free Survival & Overall Survival
BSX=APL BSX(>)APL BSX=APL BSX>APL
AFS OS
Bradbury et al., 2010
BASILAmputation Free Survival & Overall Survival
Bradbury et al., 2010
Post hoc analysis, numbers at risk to low for any relevant conclusion5-year data available only for 54% of the study cohort
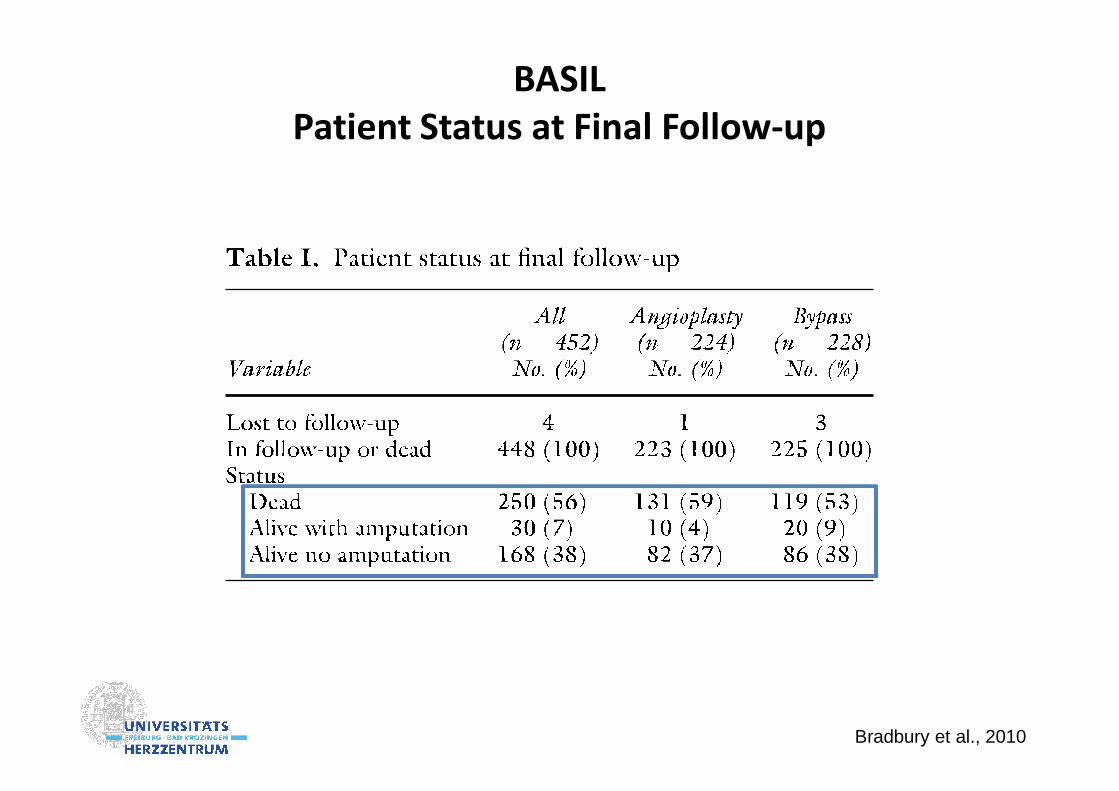
BASILPatient Status at Final Follow-up
Bradbury et al., 2010
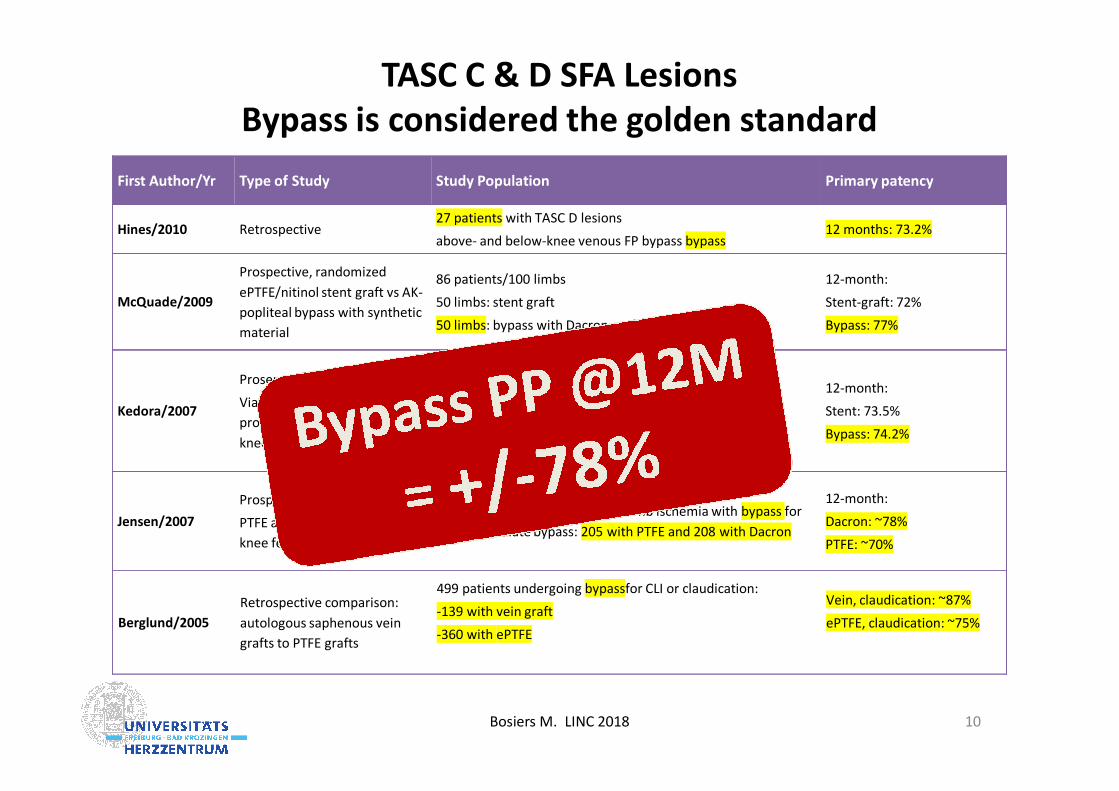
TASC C & D SFA LesionsBypass is considered the golden standard
Bosiers M. LINC 2018
First Author/Yr Type of Study Study Population Primary patency
Hines/2010 Retrospective27 patients with TASC D lesions
above- and below-knee venous FP bypass bypass12 months: 73.2%
McQuade/2009
Prospective, randomized
ePTFE/nitinol stent graft vs AK-
popliteal bypass with synthetic
material
86 patients/100 limbs
50 limbs: stent graft
50 limbs: bypass with Dacron graft or ePTFE
12-month:
Stent-graft: 72%
Bypass: 77%
Kedora/2007
Prosepctive,Randomized
Viabahn stent grafts vs
prosthetic femoro-(above-
knee) popliteal bypass
86 patients with femoro-popliteal artery occlusive disease
50 limbs treated with angio and stent
50 limbs treated with bypass with synthetic Dacron or PTFE
grafts
12-month:
Stent: 73.5%
Bypass: 74.2%
Jensen/2007
Prospective, Randomized:
PTFE and Dacron for above the
knee femoropopliteal bypass
427 patients with chronic lower limb ischemia with bypass for
suprageniculate bypass: 205 with PTFE and 208 with Dacron
12-month:
Dacron: ~78%
PTFE: ~70%
Berglund/2005
Retrospective comparison:
autologous saphenous vein
grafts to PTFE grafts
499 patients undergoing bypassfor CLI or claudication:
-139 with vein graft
-360 with ePTFE
Vein, claudication: ~87%
ePTFE, claudication: ~75%
10
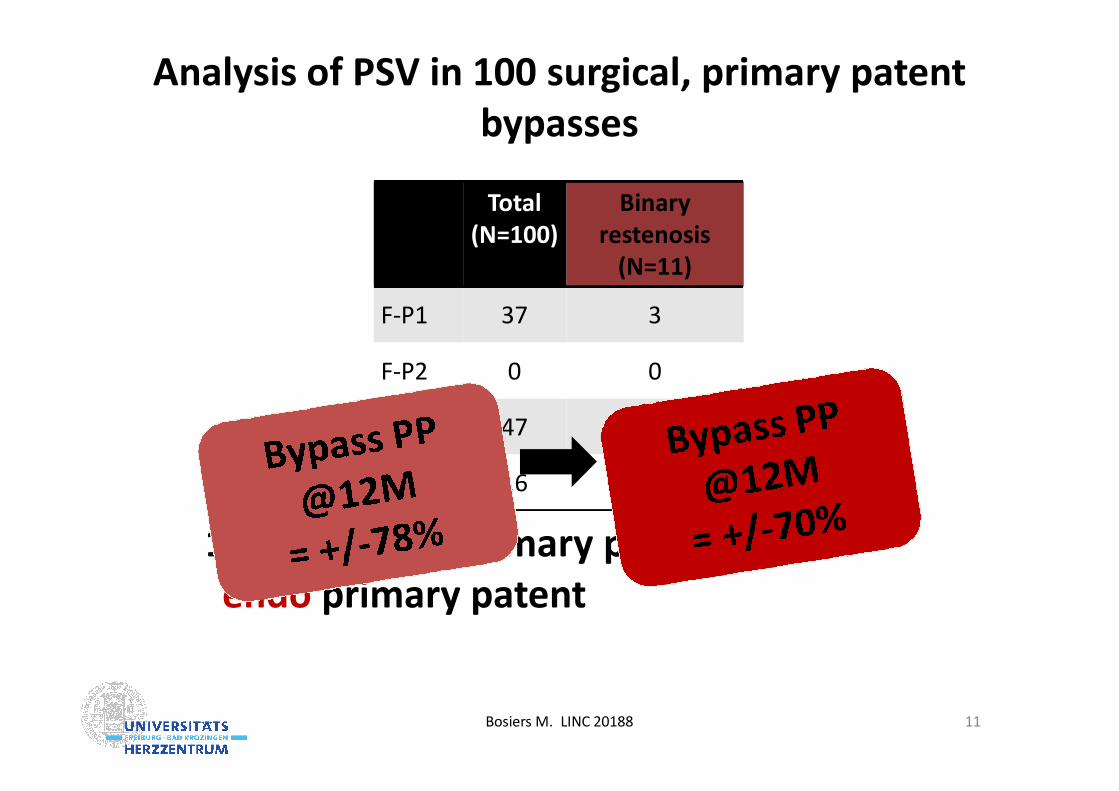
Analysis of PSV in 100 surgical, primary patentbypasses
Bosiers M. LINC 20188
Total(N=100)
Binaryrestenosis
(N=11)
F-P1 37 3
F-P2 0 0
F-P3 47 6
F-tibial 16 2
100% surgical primary patent = 89%endo primary patent
11
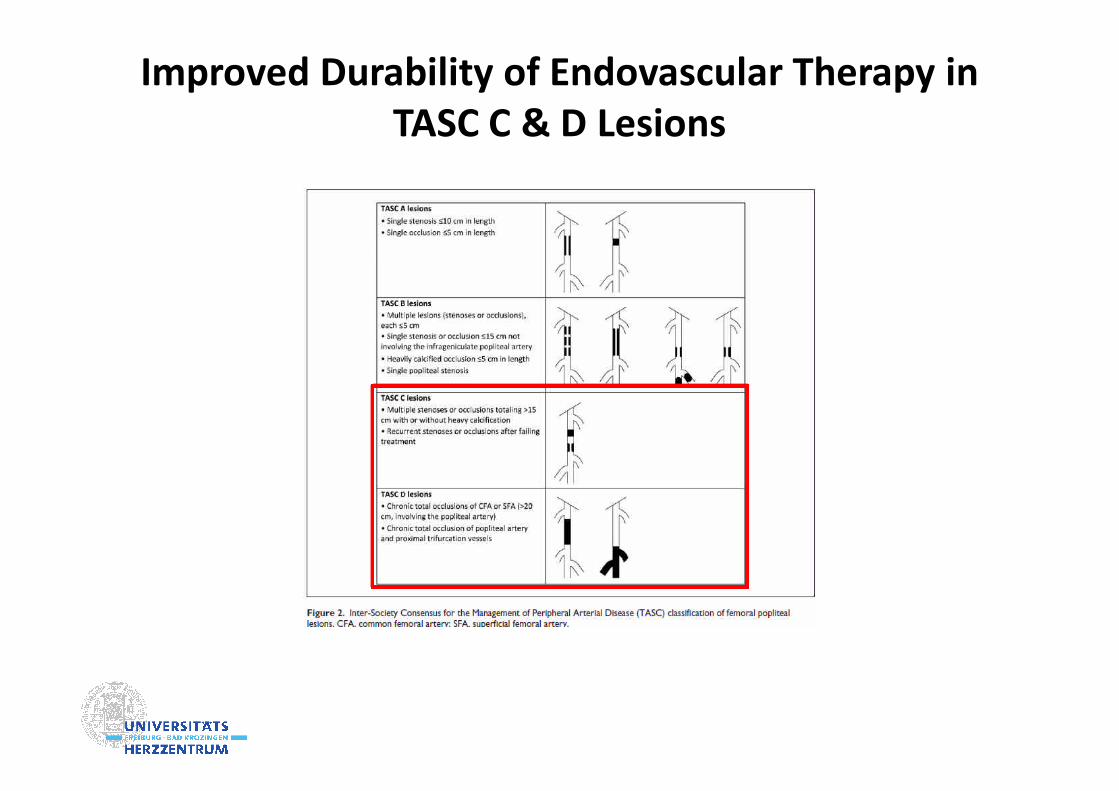
Improved Durability of Endovascular Therapy inTASC C & D Lesions
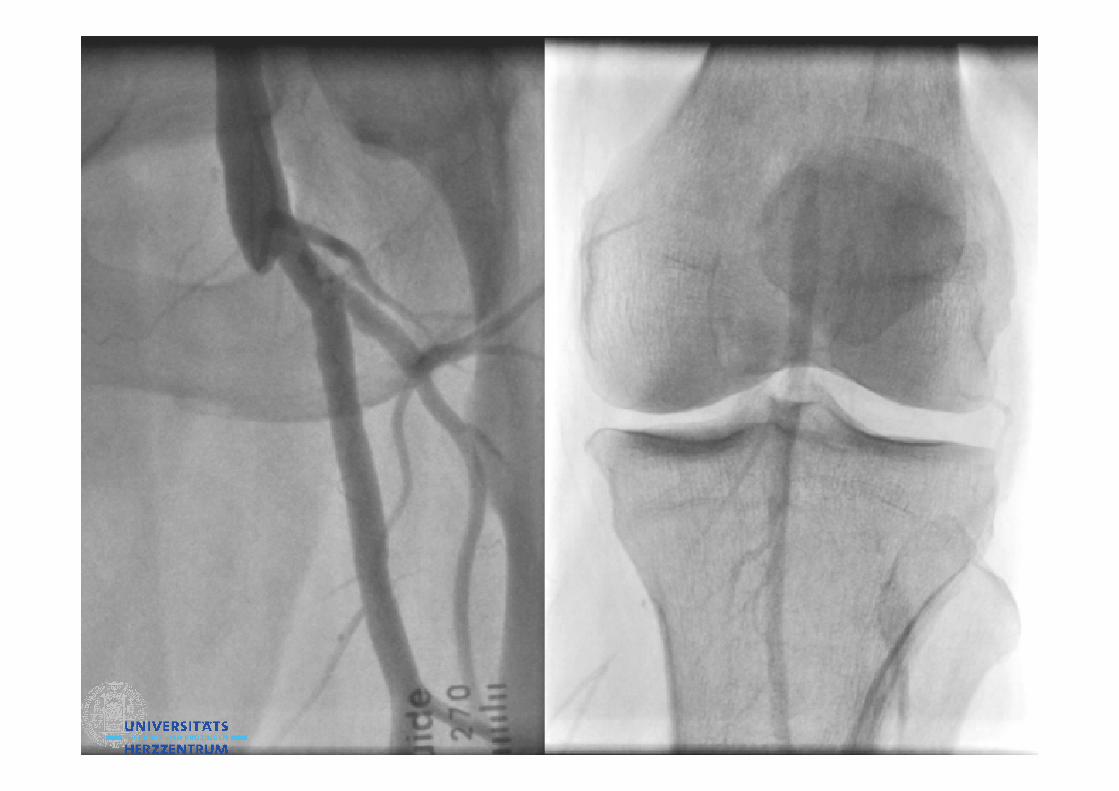

4.4.11
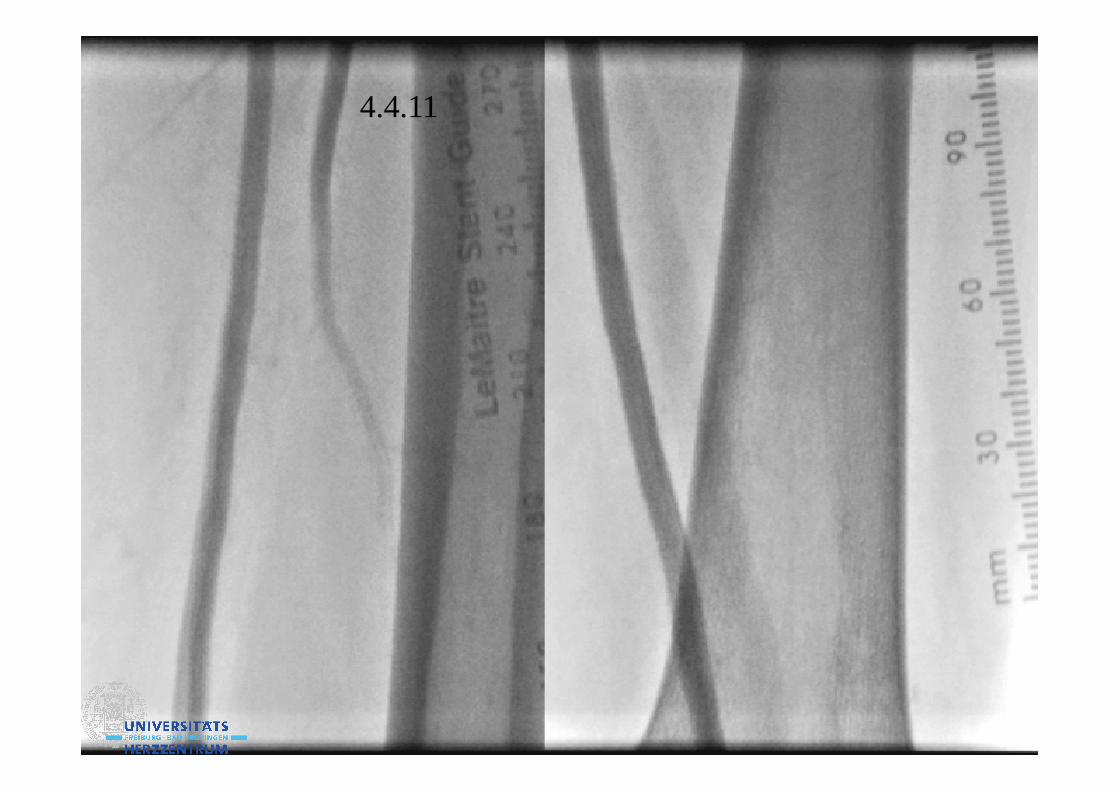
4.4.11
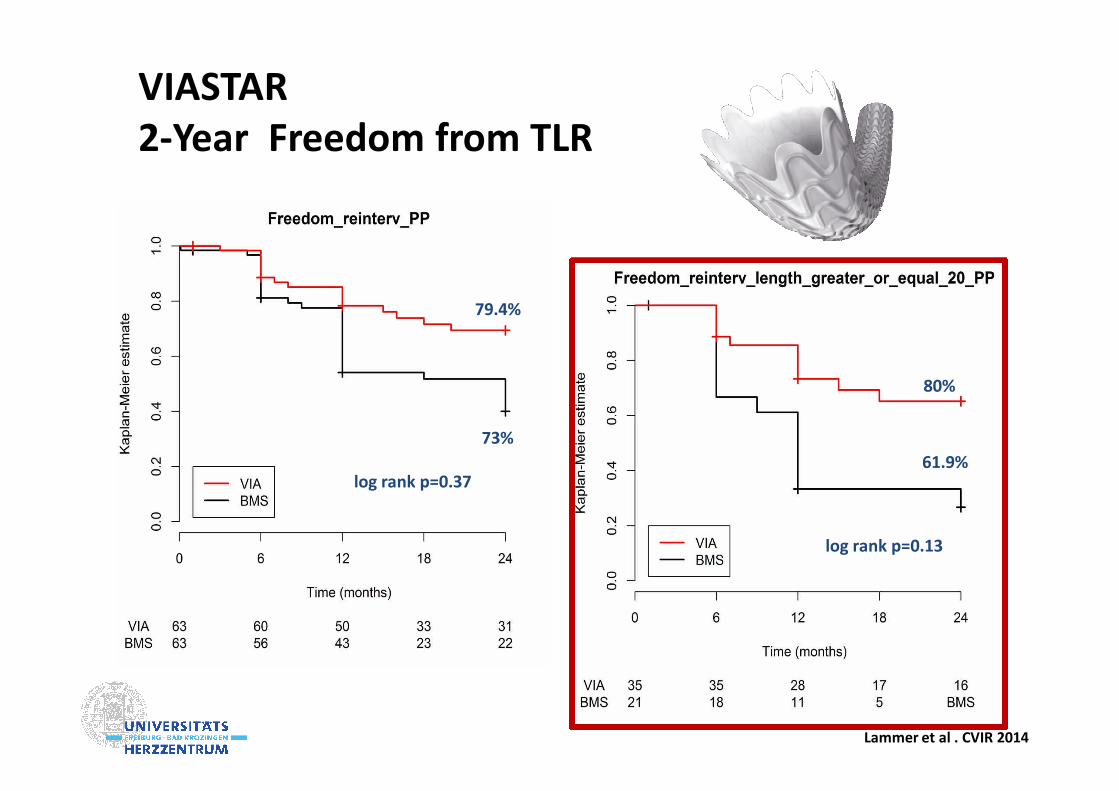
VIASTAR2-Year Freedom from TLR
79.4%
73%
log rank p=0.37
80%
61.9%
log rank p=0.13
Lammer et al . CVIR 2014
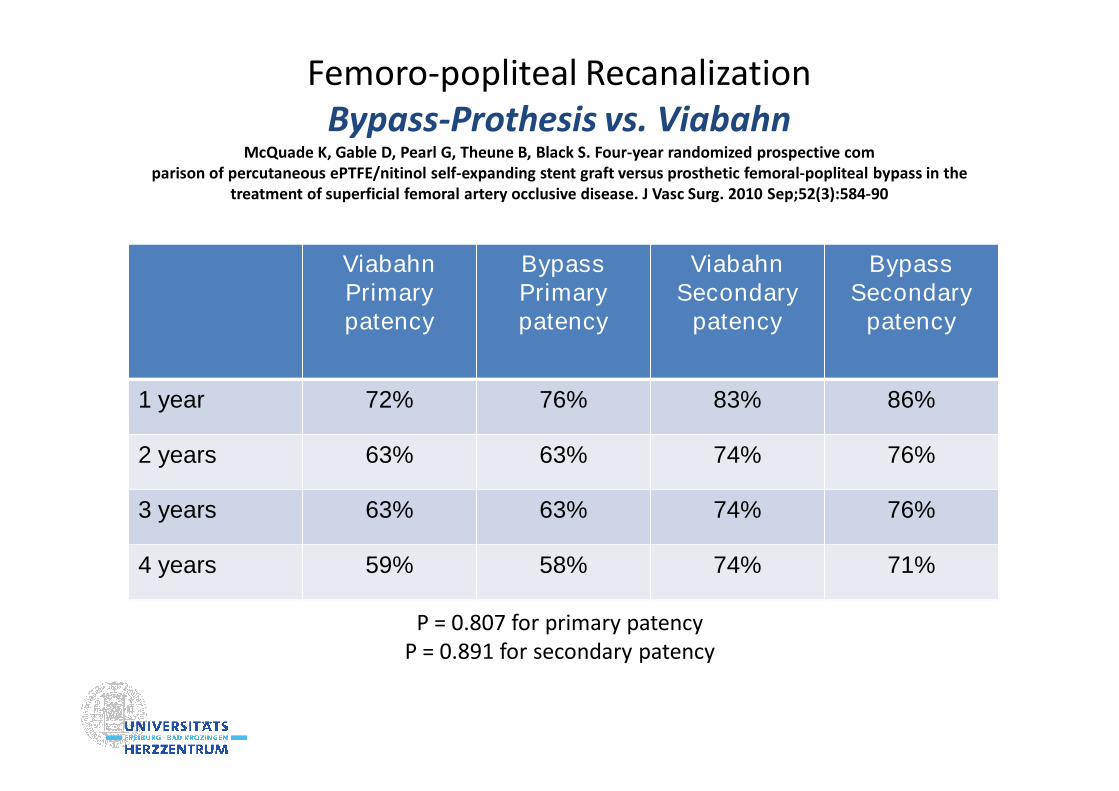
Femoro-popliteal RecanalizationBypass-Prothesis vs. Viabahn
McQuade K, Gable D, Pearl G, Theune B, Black S. Four-year randomized prospective comparison of percutaneous ePTFE/nitinol self-expanding stent graft versus prosthetic femoral-popliteal bypass in the
treatment of superficial femoral artery occlusive disease. J Vasc Surg. 2010 Sep;52(3):584-90
ViabahnPrimarypatency
BypassPrimarypatency
ViabahnSecondary
patency
BypassSecondary
patency
1 year 72% 76% 83% 86%
2 years 63% 63% 74% 76%
3 years 63% 63% 74% 76%
4 years 59% 58% 74% 71%
P = 0.807 for primary patencyP = 0.891 for secondary patency
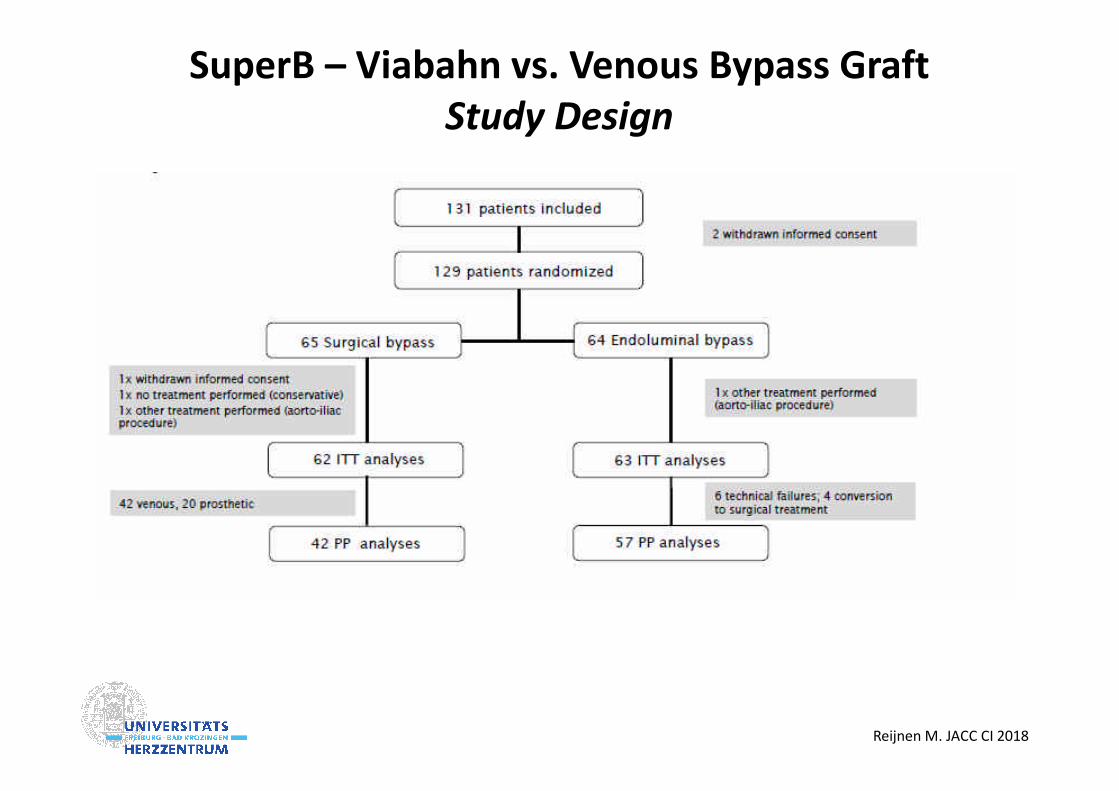
SuperB – Viabahn vs. Venous Bypass GraftStudy Design
Reijnen M. JACC CI 2018
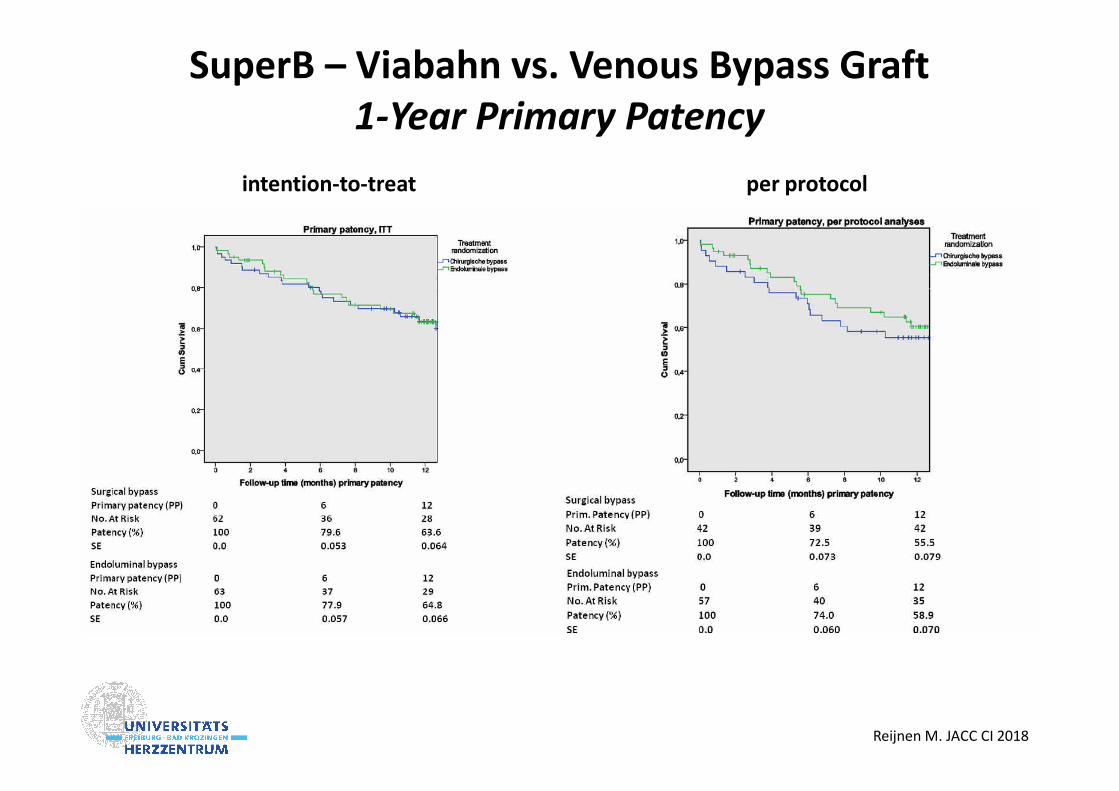
SuperB – Viabahn vs. Venous Bypass Graft1-Year Primary Patency
intention-to-treat per protocol
Reijnen M. JACC CI 2018
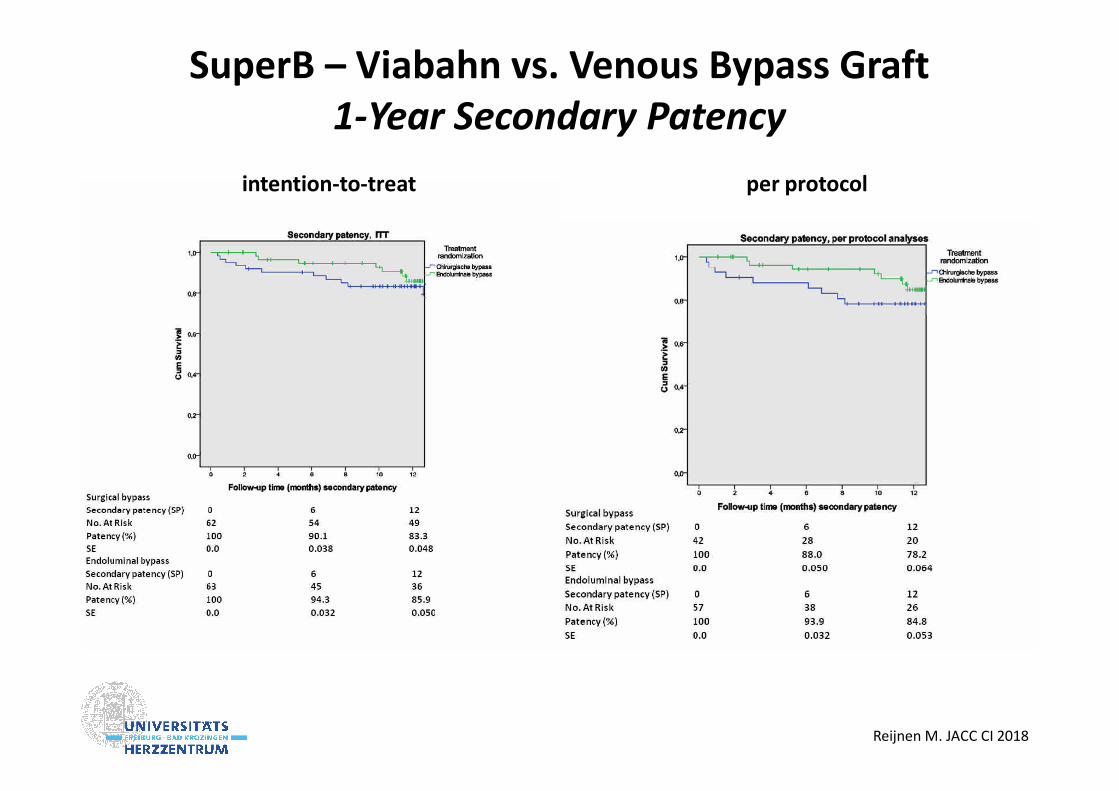
SuperB – Viabahn vs. Venous Bypass Graft1-Year Secondary Patency
intention-to-treat per protocol
Reijnen M. JACC CI 2018
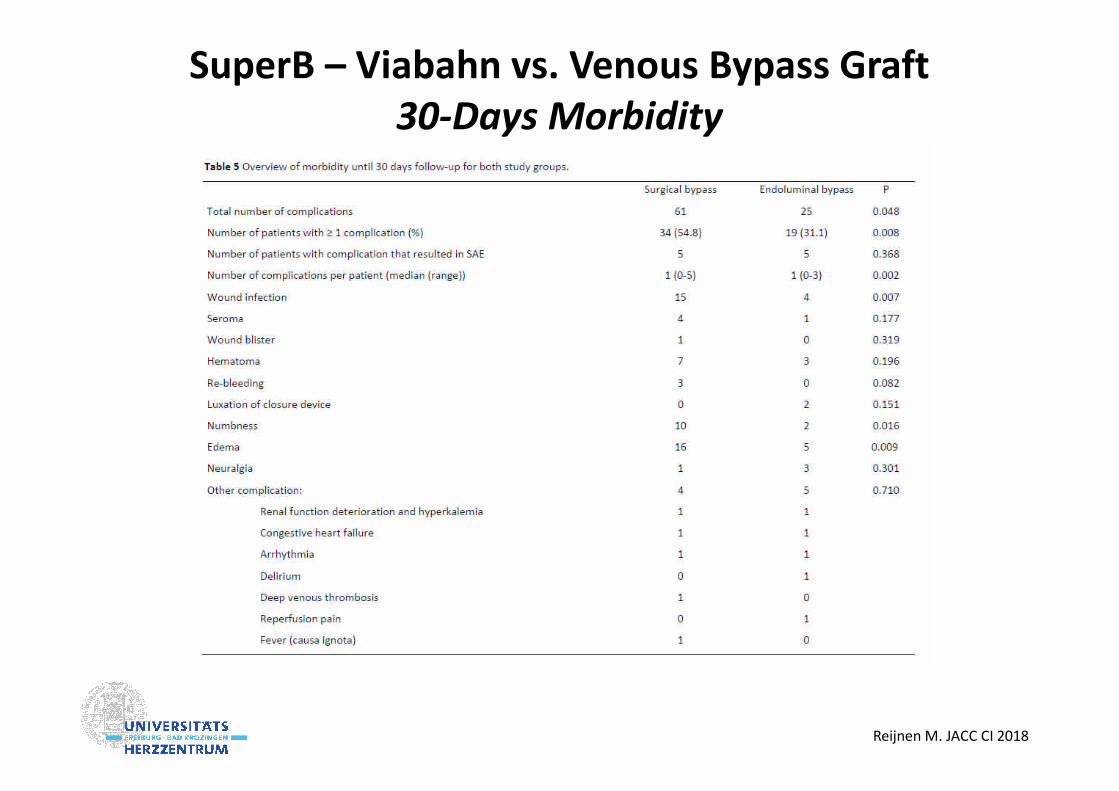
SuperB – Viabahn vs. Venous Bypass Graft30-Days Morbidity
Reijnen M. JACC CI 2018
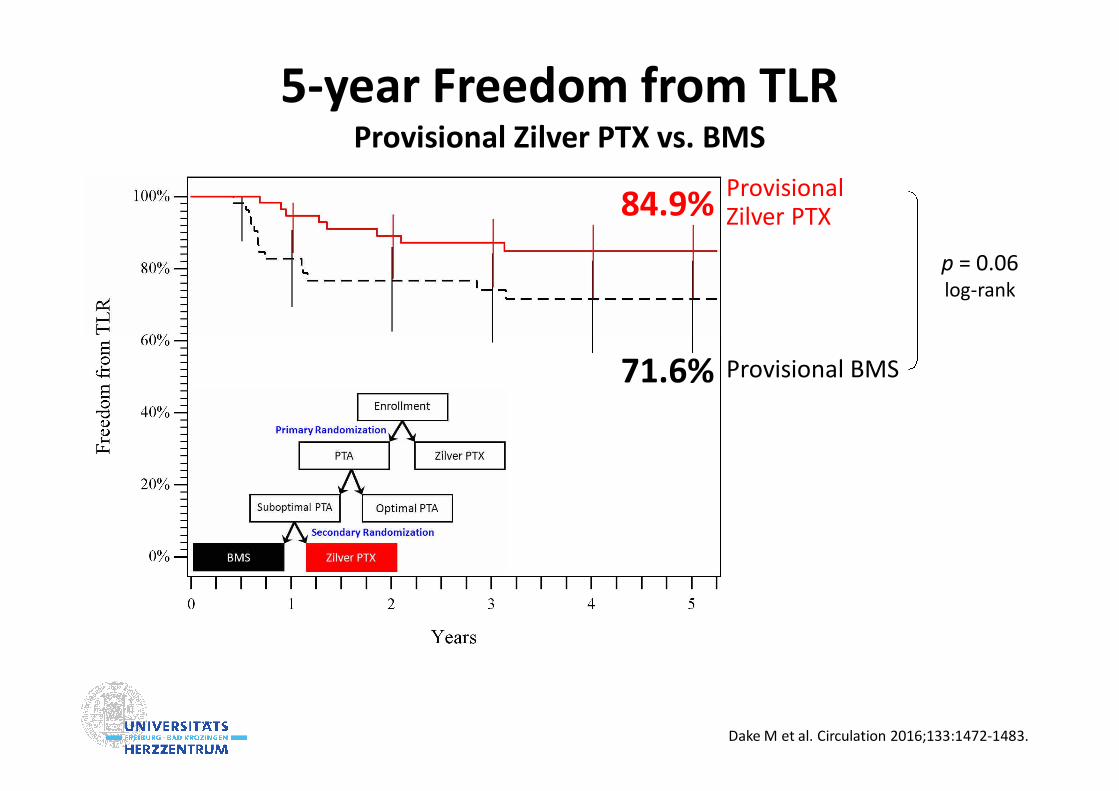
5-year Freedom from TLRProvisional Zilver PTX vs. BMS
Provisional BMS
ProvisionalZilver PTX84.9%
71.6%
p = 0.06log-rank
Dake M et al. Circulation 2016;133:1472-1483.
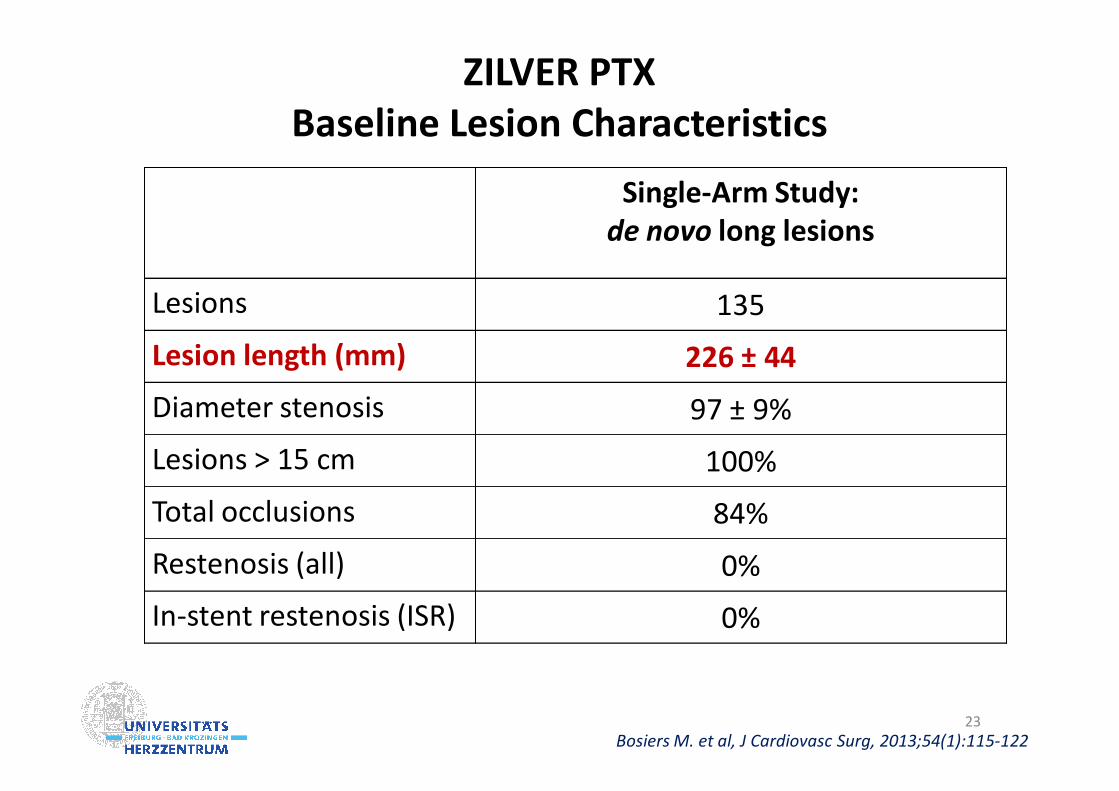
ZILVER PTXBaseline Lesion Characteristics
Single-Arm Study:de novo long lesions
Lesions 135
Lesion length (mm) 226 ± 44
Diameter stenosis 97 ± 9%
Lesions > 15 cm 100%
Total occlusions 84%
Restenosis (all) 0%
In-stent restenosis (ISR) 0%
23
Bosiers M. et al, J Cardiovasc Surg, 2013;54(1):115-122
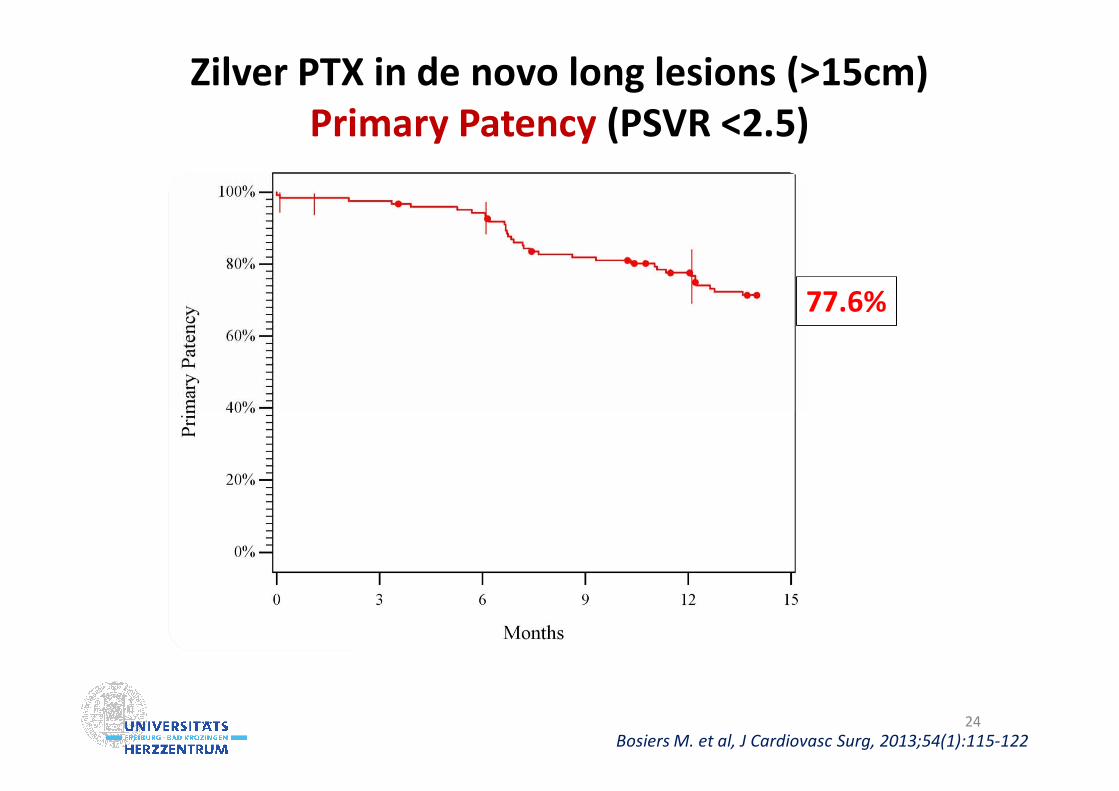
Zilver PTX in de novo long lesions (>15cm)Primary Patency (PSVR <2.5)
77.6%
24
Bosiers M. et al, J Cardiovasc Surg, 2013;54(1):115-122
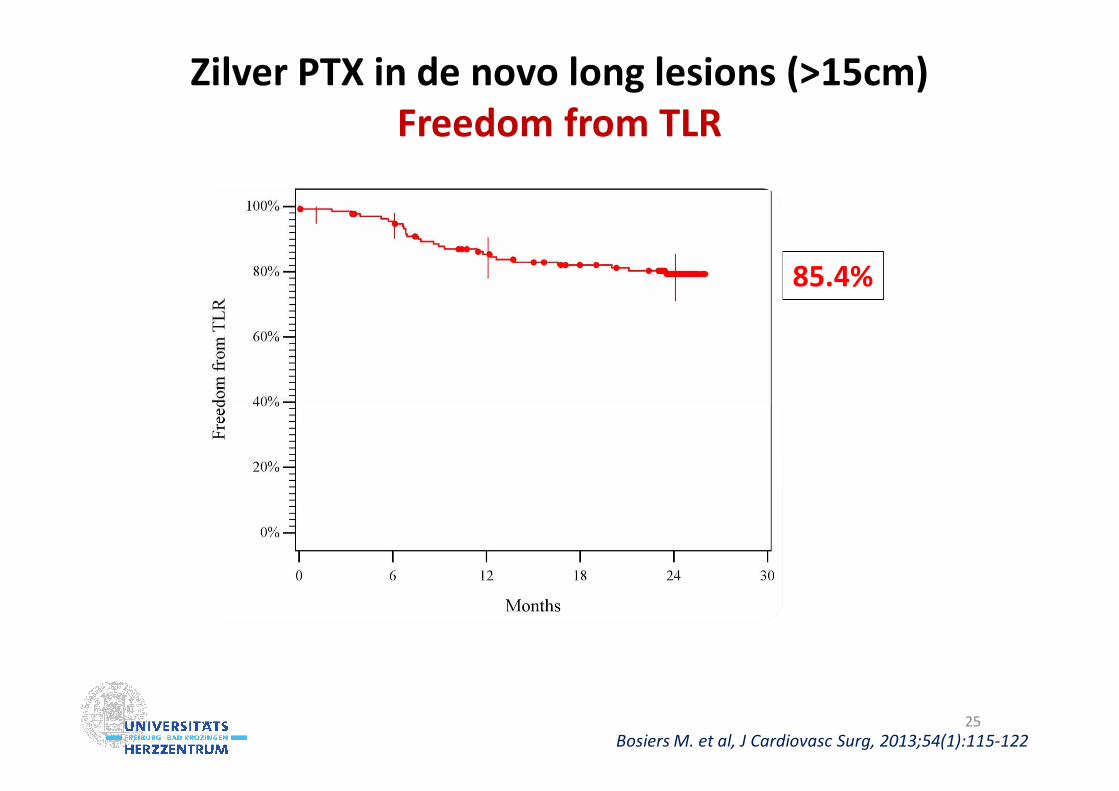
Zilver PTX in de novo long lesions (>15cm)Freedom from TLR
85.4%
25
Bosiers M. et al, J Cardiovasc Surg, 2013;54(1):115-122
ZILVERPASS study
The Cook Zilver PTX drug-eluting stent
versusbypass surgery
for the treatment offemoropopliteal TASC C&D
lesions.
26
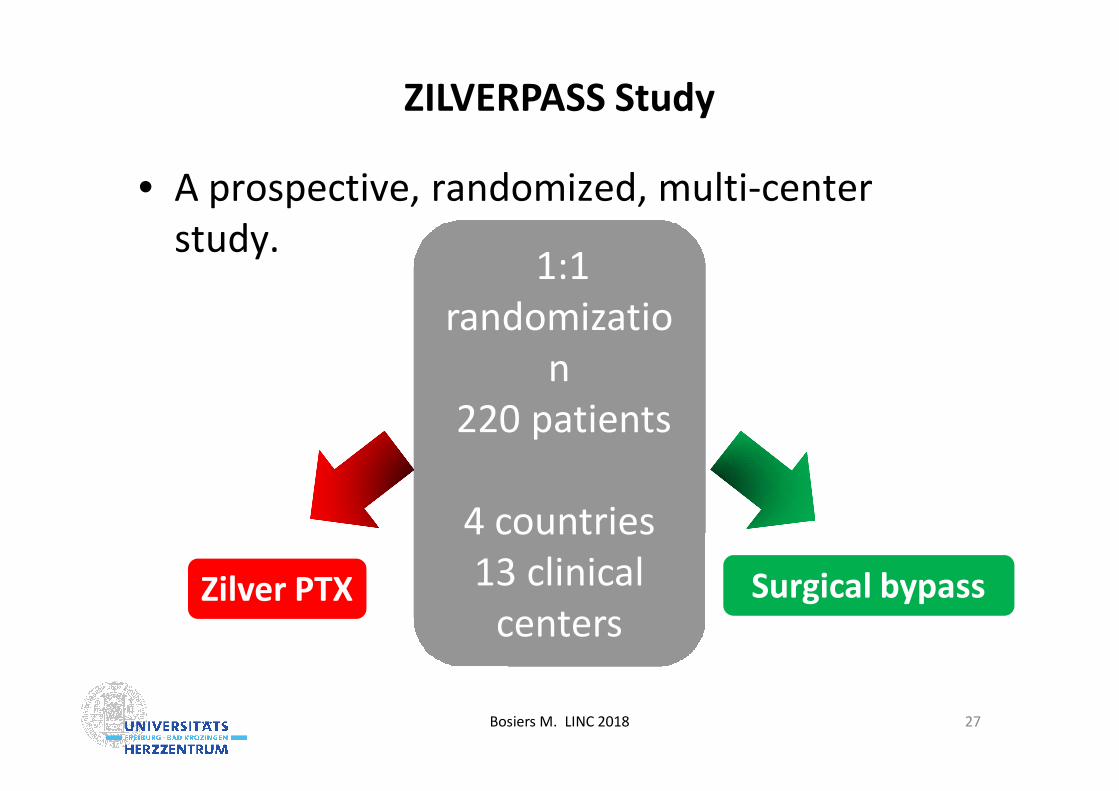
ZILVERPASS Study
• A prospective, randomized, multi-centerstudy.
Zilver PTX Surgical bypass
1:1randomizatio
n220 patients
4 countries13 clinical
centers
27Bosiers M. LINC 2018
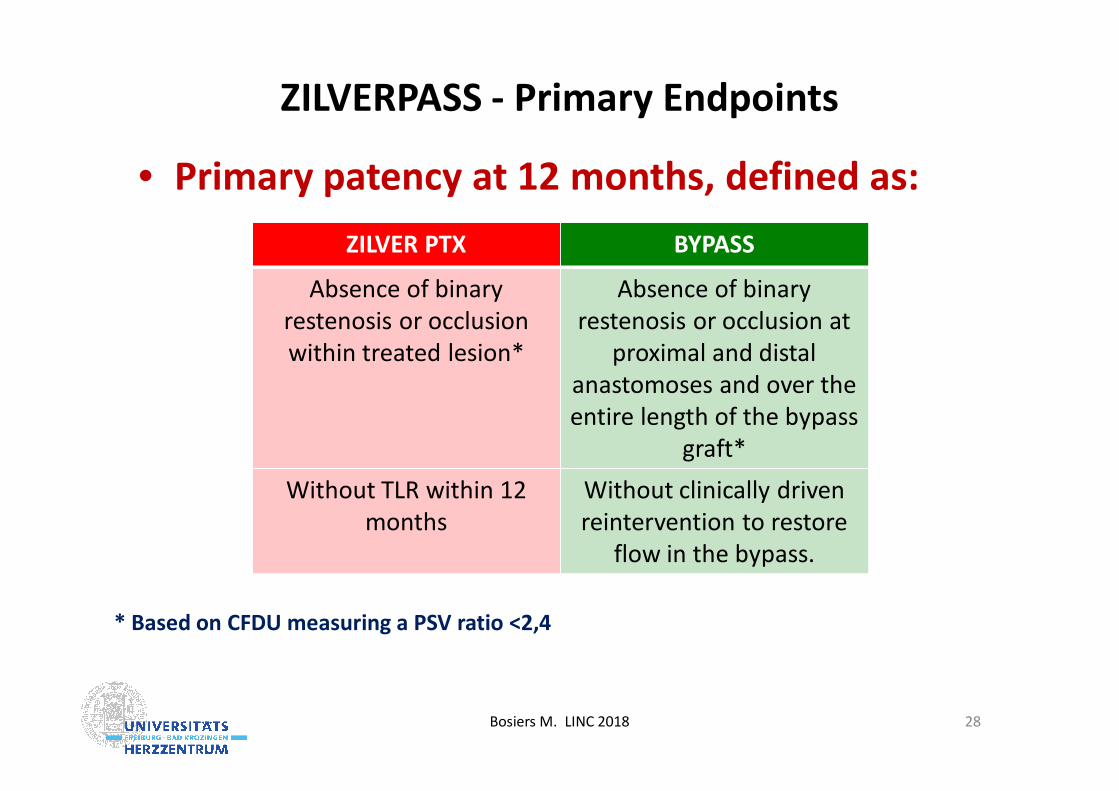
ZILVERPASS - Primary Endpoints
• Primary patency at 12 months, defined as:
ZILVER PTX BYPASS
Absence of binaryrestenosis or occlusionwithin treated lesion*
Absence of binaryrestenosis or occlusion at
proximal and distalanastomoses and over theentire length of the bypass
graft*
Without TLR within 12months
Without clinically drivenreintervention to restore
flow in the bypass.
* Based on CFDU measuring a PSV ratio <2,4
28Bosiers M. LINC 2018
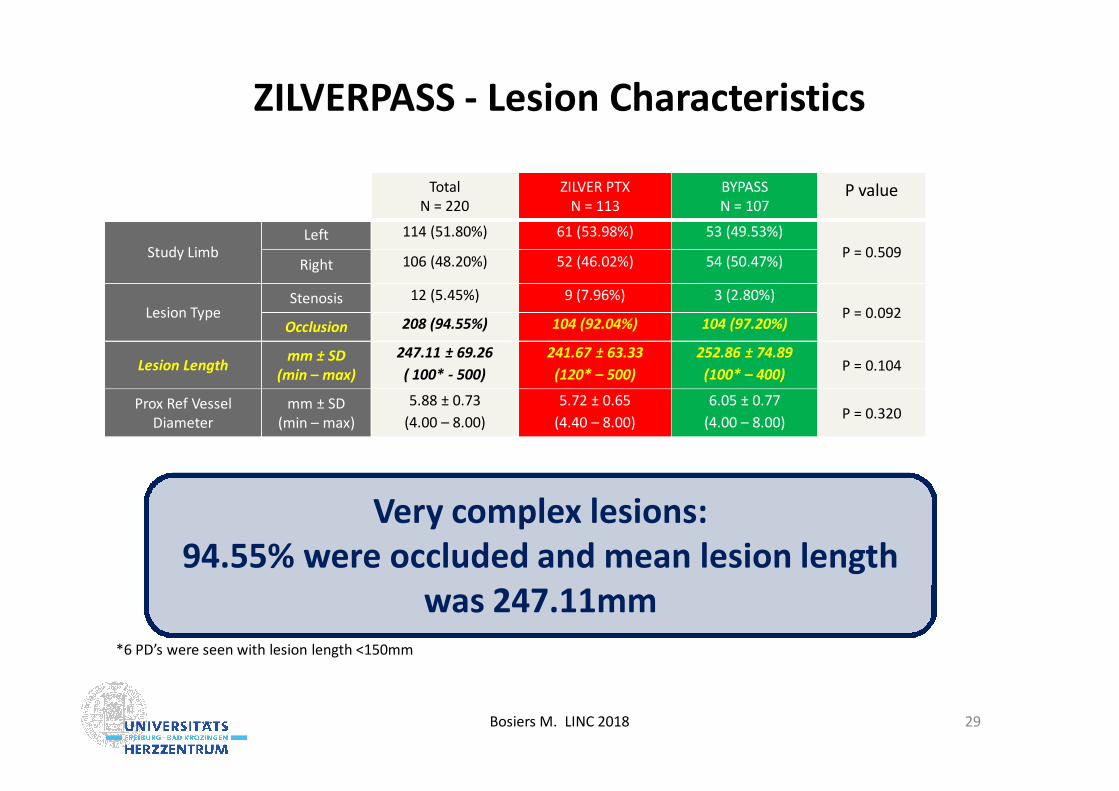
ZILVERPASS - Lesion Characteristics
TotalN = 220
ZILVER PTXN = 113
BYPASSN = 107
P value
Study LimbLeft 114 (51.80%) 61 (53.98%) 53 (49.53%)
P = 0.509Right 106 (48.20%) 52 (46.02%) 54 (50.47%)
Lesion TypeStenosis 12 (5.45%) 9 (7.96%) 3 (2.80%)
P = 0.092Occlusion 208 (94.55%) 104 (92.04%) 104 (97.20%)
Lesion Lengthmm ± SD
(min – max)
247.11 ± 69.26
( 100* - 500)
241.67 ± 63.33
(120* – 500)
252.86 ± 74.89
(100* – 400)P = 0.104
Prox Ref VesselDiameter
mm ± SD(min – max)
5.88 ± 0.73
(4.00 – 8.00)
5.72 ± 0.65
(4.40 – 8.00)
6.05 ± 0.77
(4.00 – 8.00)P = 0.320
*6 PD’s were seen with lesion length <150mm
Very complex lesions:94.55% were occluded and mean lesion length
was 247.11mm
29Bosiers M. LINC 2018
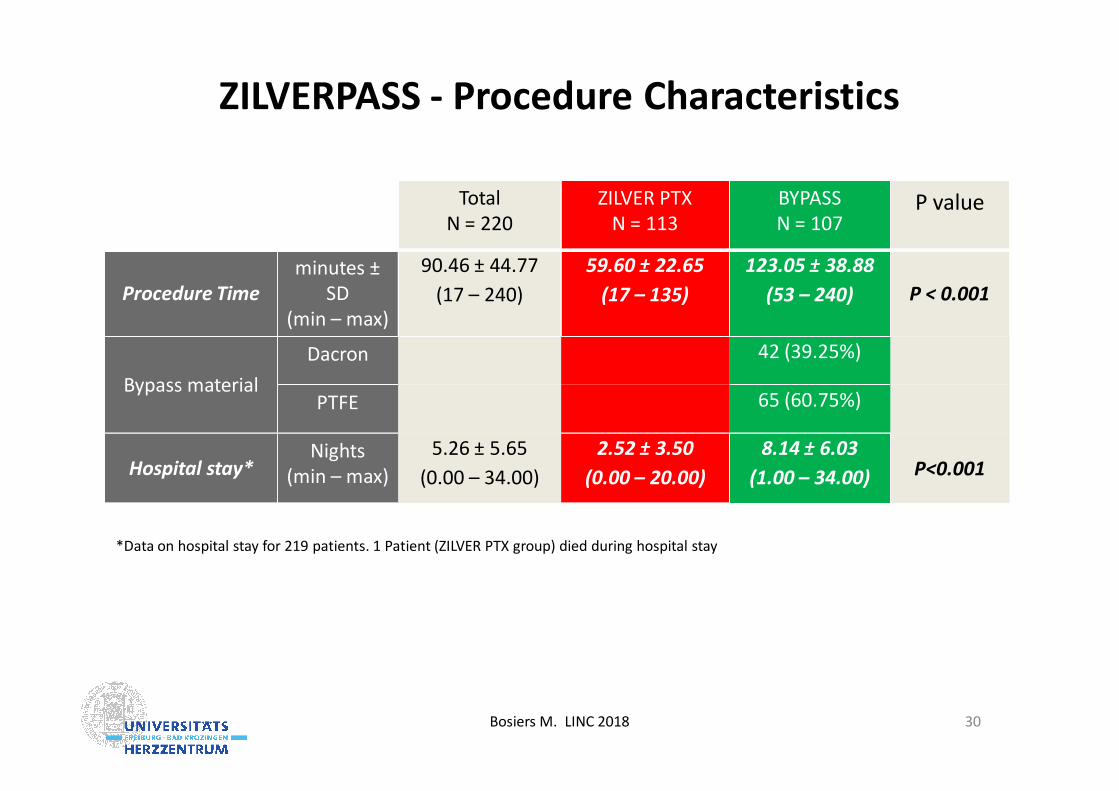
ZILVERPASS - Procedure Characteristics
TotalN = 220
ZILVER PTXN = 113
BYPASSN = 107
P value
Procedure Timeminutes ±
SD(min – max)
90.46 ± 44.77
(17 – 240)
59.60 ± 22.65
(17 – 135)
123.05 ± 38.88
(53 – 240) P < 0.001
Bypass material
Dacron 42 (39.25%)
PTFE 65 (60.75%)
Hospital stay*Nights
(min – max)
5.26 ± 5.65
(0.00 – 34.00)
2.52 ± 3.50
(0.00 – 20.00)
8.14 ± 6.03
(1.00 – 34.00) P<0.001
*Data on hospital stay for 219 patients. 1 Patient (ZILVER PTX group) died during hospital stay
30Bosiers M. LINC 2018
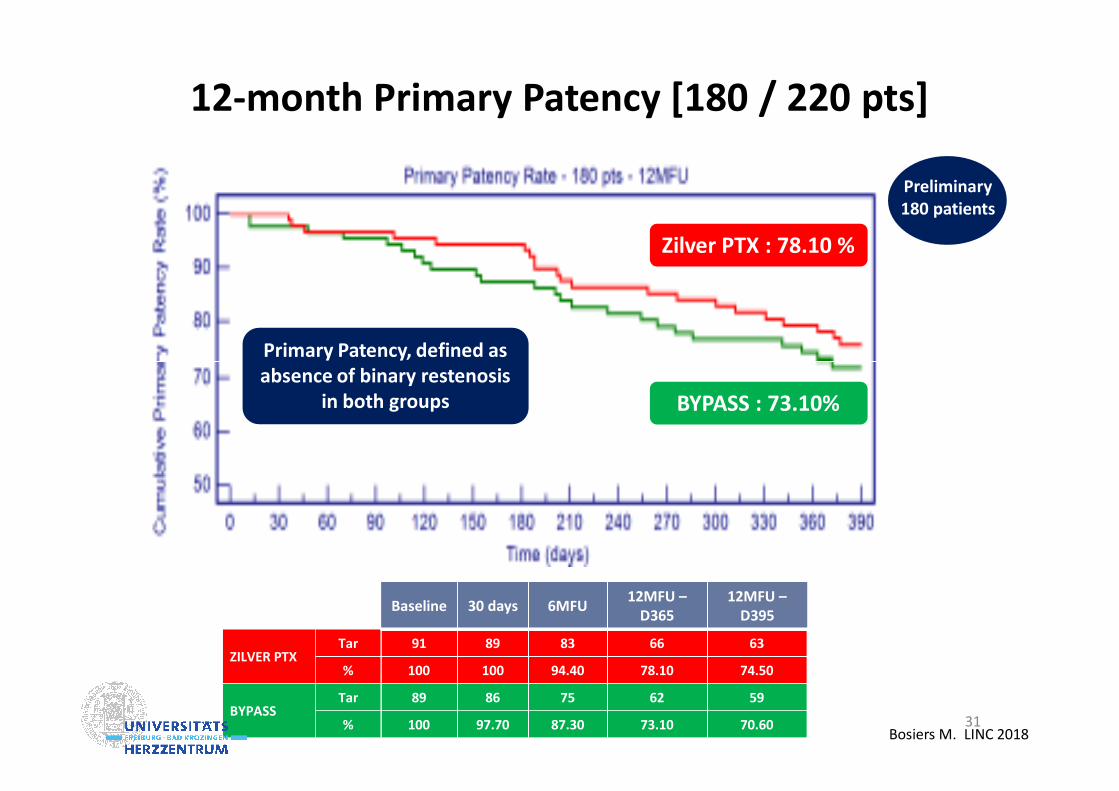
12-month Primary Patency [180 / 220 pts]
FMRP - 2018
Baseline 30 days 6MFU12MFU –
D36512MFU –
D395
ZILVER PTXTar 91 89 83 66 63
% 100 100 94.40 78.10 74.50
BYPASSTar 89 86 75 62 59
% 100 97.70 87.30 73.10 70.60
Preliminary180 patients
Zilver PTX : 78.10 %
BYPASS : 73.10%
Primary Patency, defined asabsence of binary restenosis
in both groups
31Bosiers M. LINC 2018
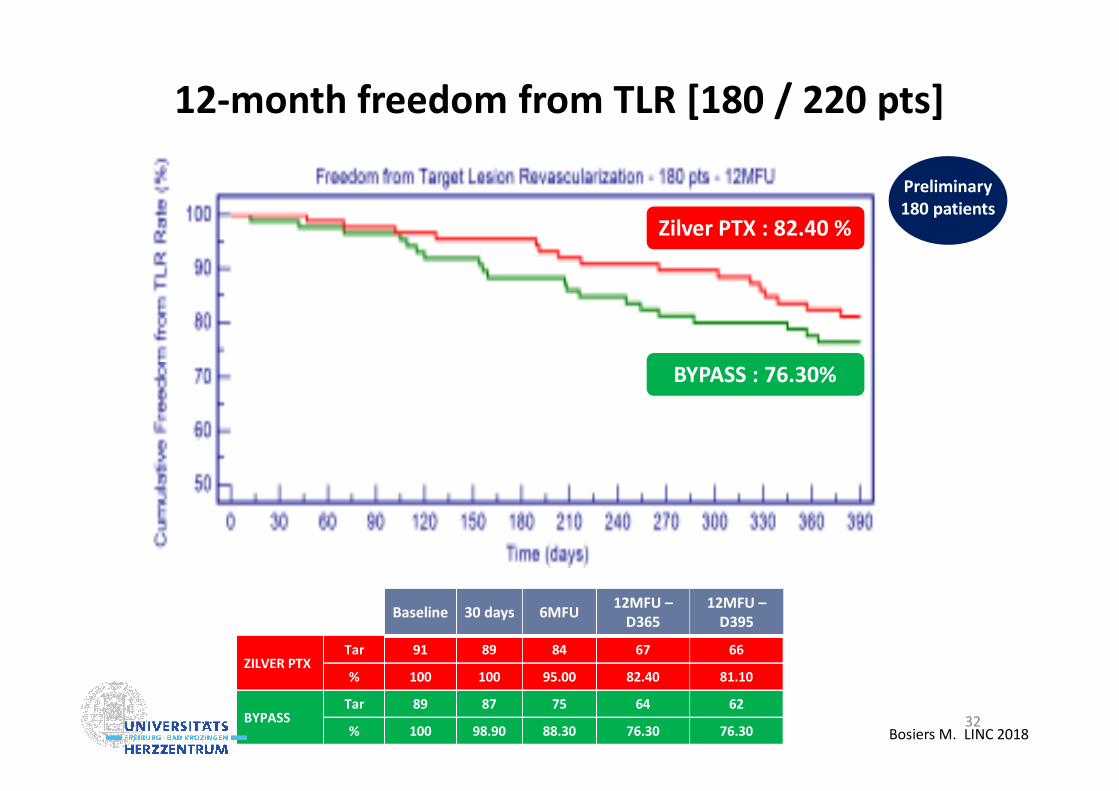
12-month freedom from TLR [180 / 220 pts]
FMRP - 2018
Baseline 30 days 6MFU12MFU –
D36512MFU –
D395
ZILVER PTXTar 91 89 84 67 66
% 100 100 95.00 82.40 81.10
BYPASSTar 89 87 75 64 62
% 100 98.90 88.30 76.30 76.30
Preliminary180 patients
Zilver PTX : 82.40 %
BYPASS : 76.30%
32Bosiers M. LINC 2018
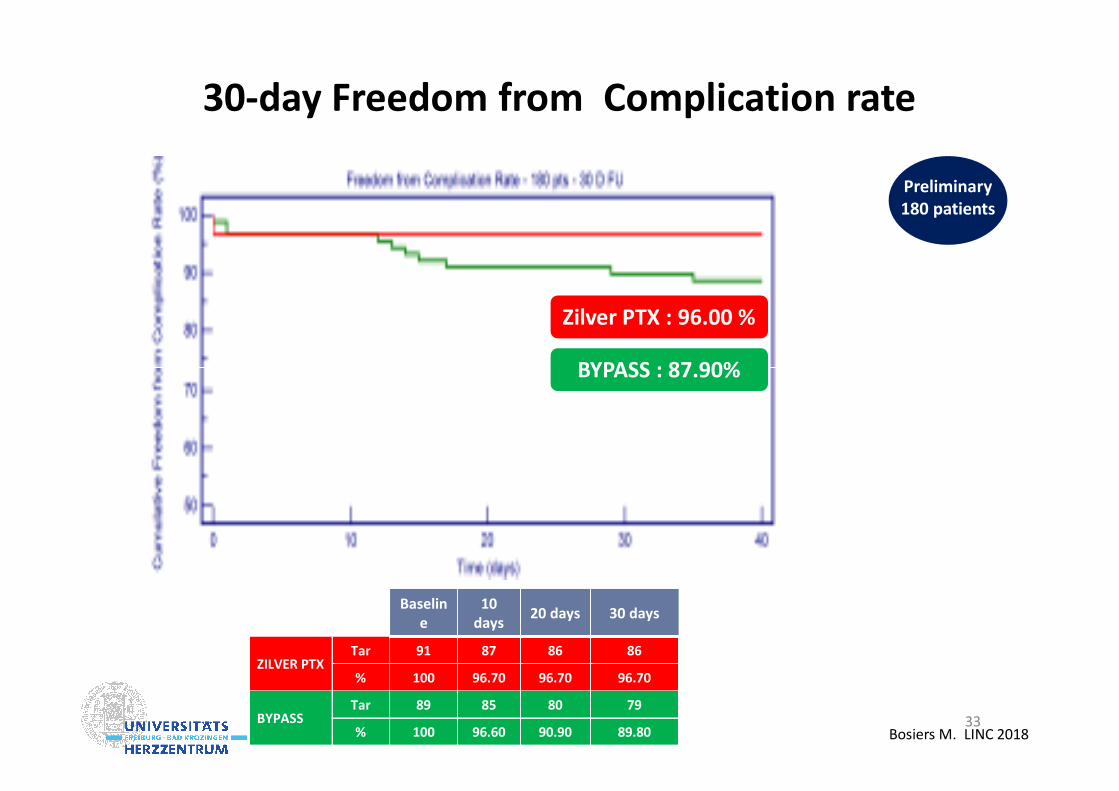
30-day Freedom from Complication rate
FMRP - 2018
Baseline
10days
20 days 30 days
ZILVER PTXTar 91 87 86 86
% 100 96.70 96.70 96.70
BYPASSTar 89 85 80 79
% 100 96.60 90.90 89.80
Preliminary180 patients
Zilver PTX : 96.00 %
BYPASS : 87.90%
33Bosiers M. LINC 2018
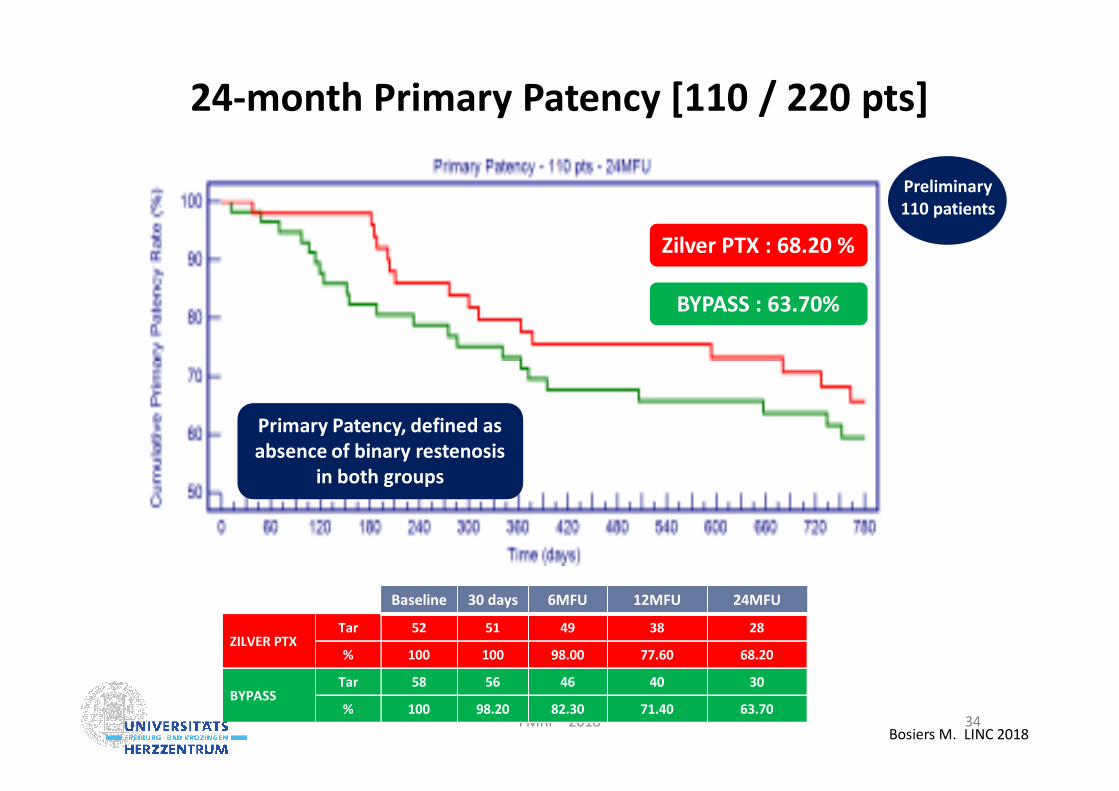
24-month Primary Patency [110 / 220 pts]
FMRP - 2018
Baseline 30 days 6MFU 12MFU 24MFU
ZILVER PTXTar 52 51 49 38 28
% 100 100 98.00 77.60 68.20
BYPASSTar 58 56 46 40 30
% 100 98.20 82.30 71.40 63.70
Preliminary110 patients
Zilver PTX : 68.20 %
BYPASS : 63.70%
Primary Patency, defined asabsence of binary restenosis
in both groups
34Bosiers M. LINC 2018
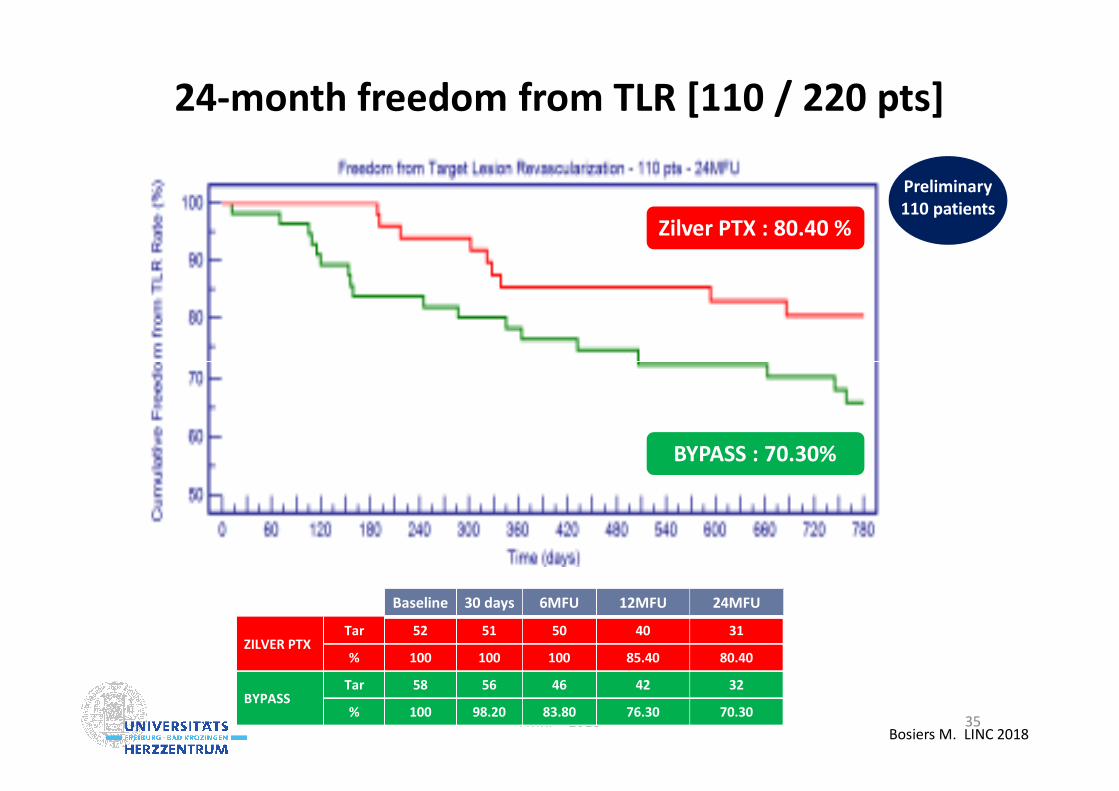
24-month freedom from TLR [110 / 220 pts]
FMRP - 2018
Baseline 30 days 6MFU 12MFU 24MFU
ZILVER PTXTar 52 51 50 40 31
% 100 100 100 85.40 80.40
BYPASSTar 58 56 46 42 32
% 100 98.20 83.80 76.30 70.30
Preliminary110 patients
Zilver PTX : 80.40 %
BYPASS : 70.30%
35Bosiers M. LINC 2018
Femoro-popliteale Verschlüsse – Ist die endo-vaskuläre Therapie der neue Goldstandard?
Ja!
• Die Morbidität der endovaskulären Techniken istsignifikant niedriger als die der Bypass Operation
• Selbst die Ergebnisse der VENÖSEN Bypassanlagesind nicht besser als die endovaskuläre Therapie!
• Die aktuellen Leitlinien berücksichtigen nicht denaktuellen Stand der klinischen Forschung.
36