Embed Size (px)
Citation preview
1
Citratantikoagulation für alle?
Torsten Slowinski
Universitätsklinikum Charité
Campus Mitte
Klinik für Nephrologie
Berlin
2
KDIGO (2012): Empfehlung zur
Citratantikoagulation bei CRRT
www.kdigo.org
Patienten mit CRRT
1. auch ohne erhöhtes Blutungsrisiko und
2. ohne beinträchtigte Blutgerinnung und
3. ohne systemische Antikoagualtion aus anderen Gründen
4. ohne Kontraindikationen für Citrat
-> eher regionale Citratantikoagulation als andere Antikoagulation (2B)
3
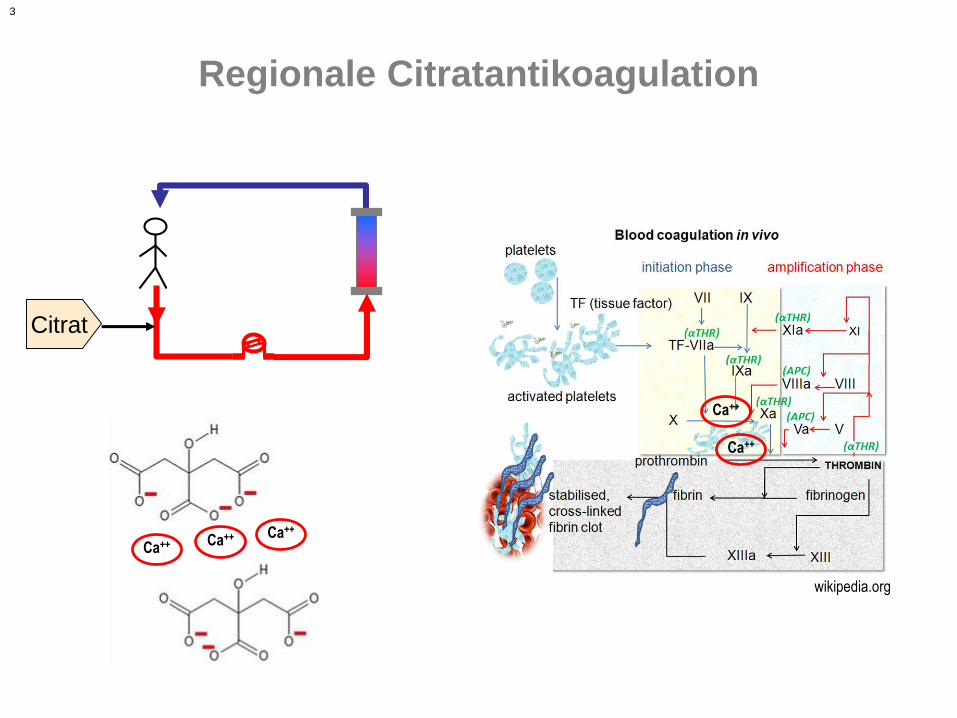
Regionale Citratantikoagulation
Citrat
wikipedia.org
Ca++
Ca++
Ca++ Ca++ Ca++
4
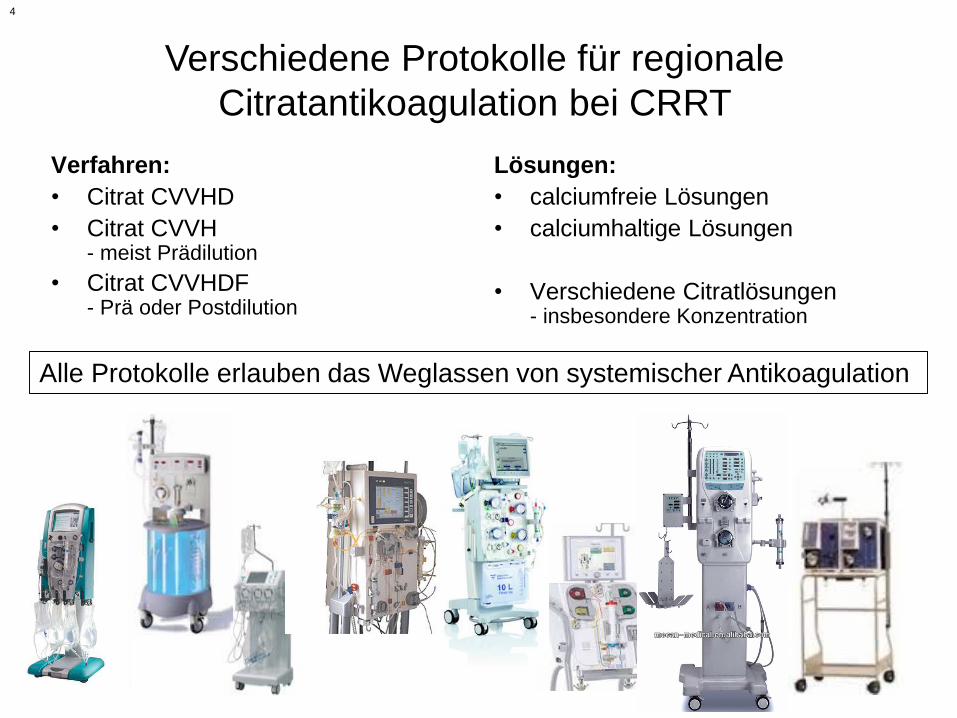
Verfahren:
• Citrat CVVHD
• Citrat CVVH - meist Prädilution
• Citrat CVVHDF- Prä oder Postdilution
Lösungen:
• calciumfreie Lösungen
• calciumhaltige Lösungen
• Verschiedene Citratlösungen- insbesondere Konzentration
Verschiedene Protokolle für regionale
Citratantikoagulation bei CRRT
Alle Protokolle erlauben das Weglassen von systemischer Antikoagulation
5
6
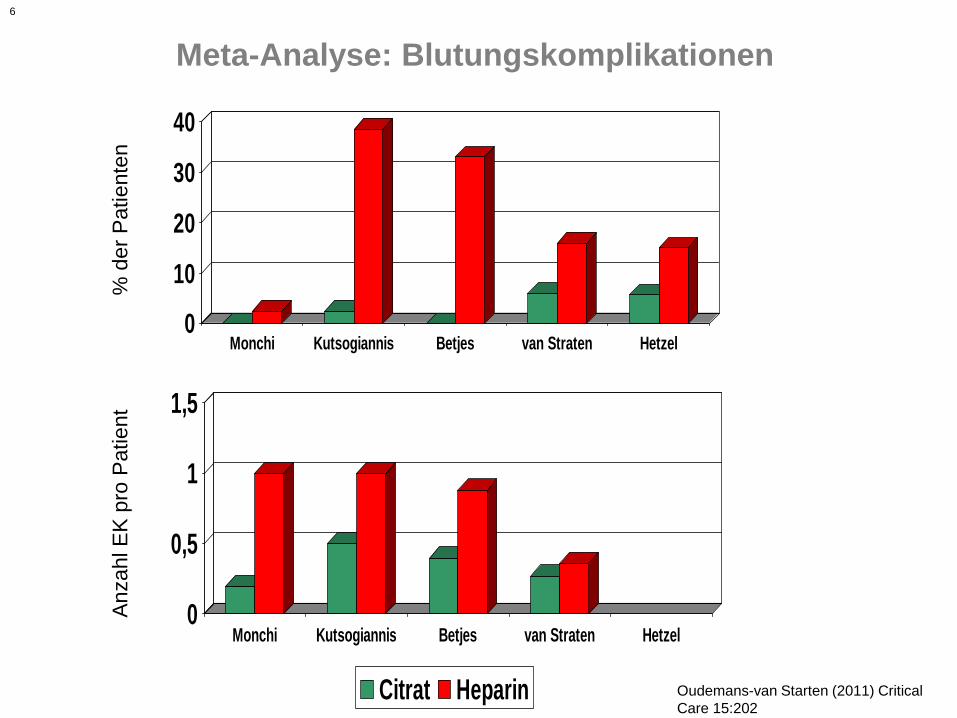
Meta-Analyse: Blutungskomplikationen
0
10
20
30
40
Monchi Kutsogiannis Betjes van Straten Hetzel
Citrat Heparin
Oudemans-van Starten (2011) Critical
Care 15:202
0
0,5
1
1,5
Monchi Kutsogiannis Betjes van Straten Hetzel
Citrat Heparin
% d
er
Pa
tie
nte
nA
nza
hl E
K p
ro P
atie
nt
7
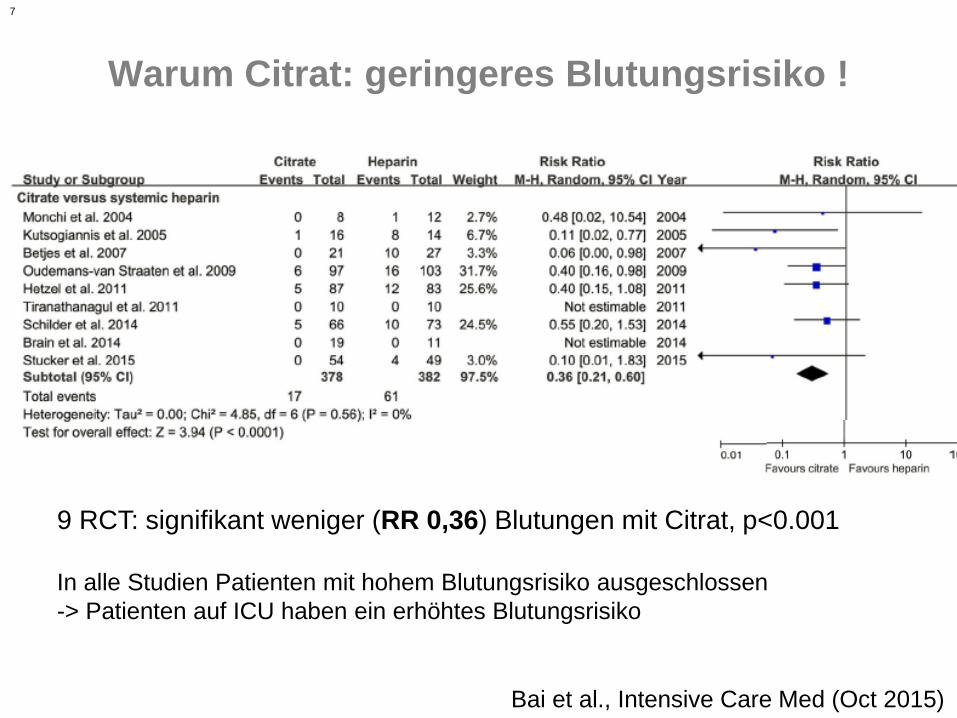
Warum Citrat: geringeres Blutungsrisiko !
9 RCT: signifikant weniger (RR 0,36) Blutungen mit Citrat, p<0.001
In alle Studien Patienten mit hohem Blutungsrisiko ausgeschlossen
-> Patienten auf ICU haben ein erhöhtes Blutungsrisiko
Bai et al., Intensive Care Med (Oct 2015)
8
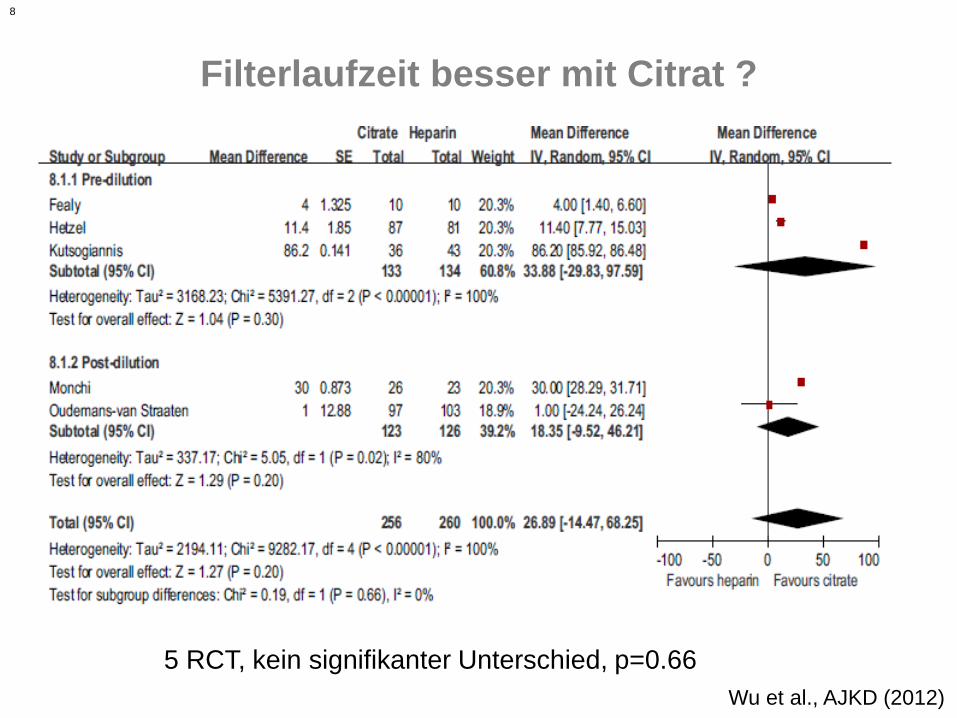
Filterlaufzeit besser mit Citrat ?
Wu et al., AJKD (2012)
5 RCT, kein signifikanter Unterschied, p=0.66
9
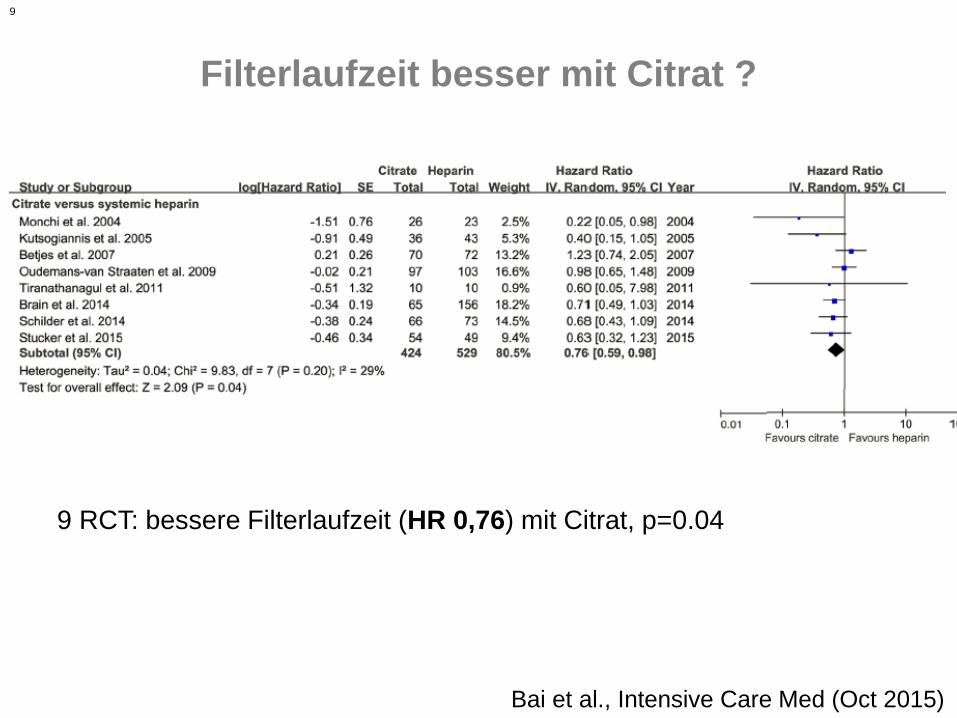
Filterlaufzeit besser mit Citrat ?
9 RCT: bessere Filterlaufzeit (HR 0,76) mit Citrat, p=0.04
Bai et al., Intensive Care Med (Oct 2015)
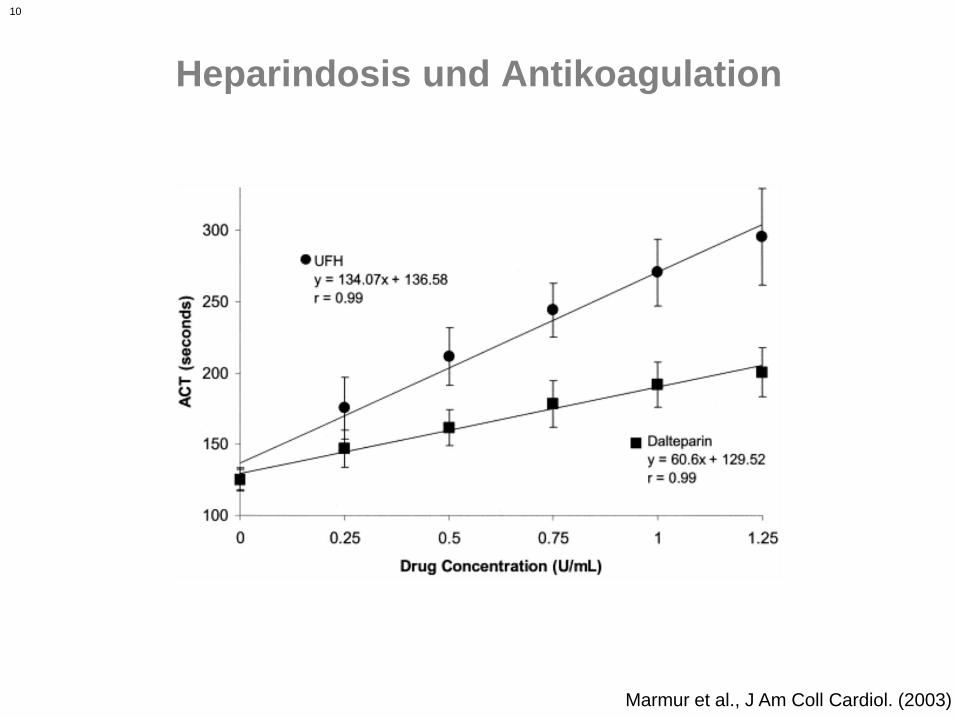
10
Heparindosis und Antikoagulation
Marmur et al., J Am Coll Cardiol. (2003)
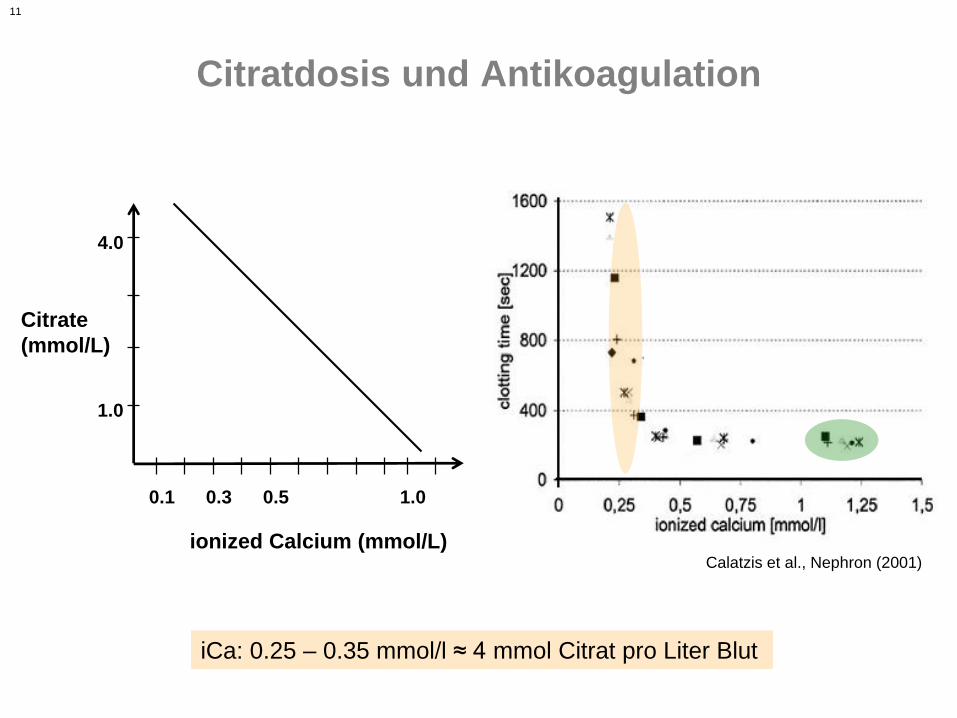
11
Citratdosis und Antikoagulation
iCa: 0.25 – 0.35 mmol/l ≈ 4 mmol Citrat pro Liter Blut
Calatzis et al., Nephron (2001)
ionized Calcium (mmol/L)
Citrate
(mmol/L)
0.1 0.3 0.5 1.0
1.0
4.0
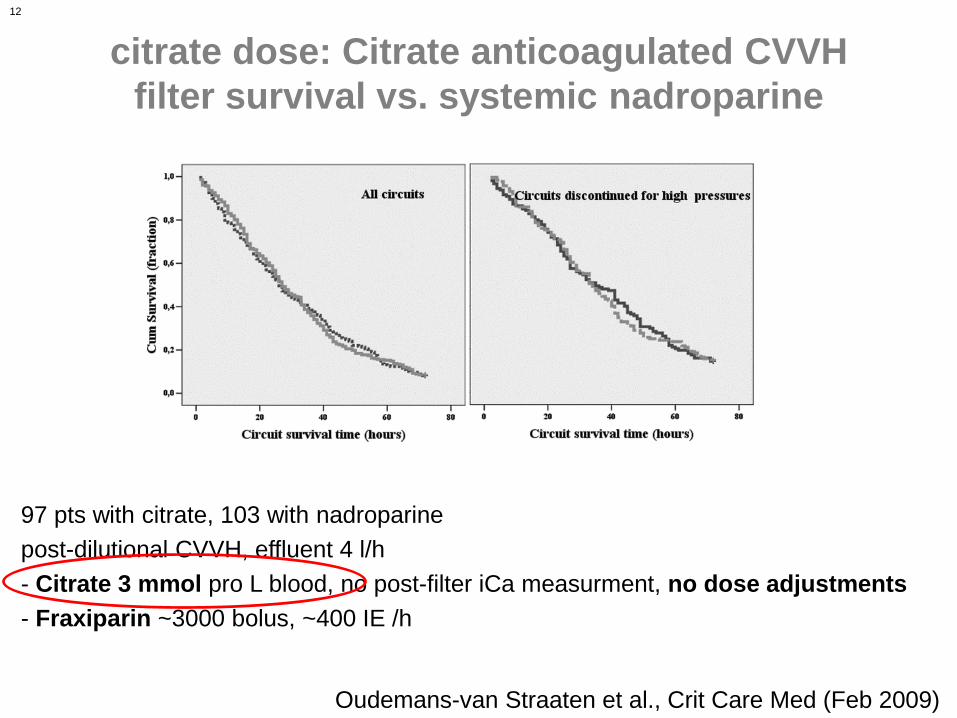
12
citrate dose: Citrate anticoagulated CVVH
filter survival vs. systemic nadroparine
Oudemans-van Straaten et al., Crit Care Med (Feb 2009)
97 pts with citrate, 103 with nadroparine
post-dilutional CVVH, effluent 4 l/h
- Citrate 3 mmol pro L blood, no post-filter iCa measurment, no dose adjustments
- Fraxiparin ~3000 bolus, ~400 IE /h
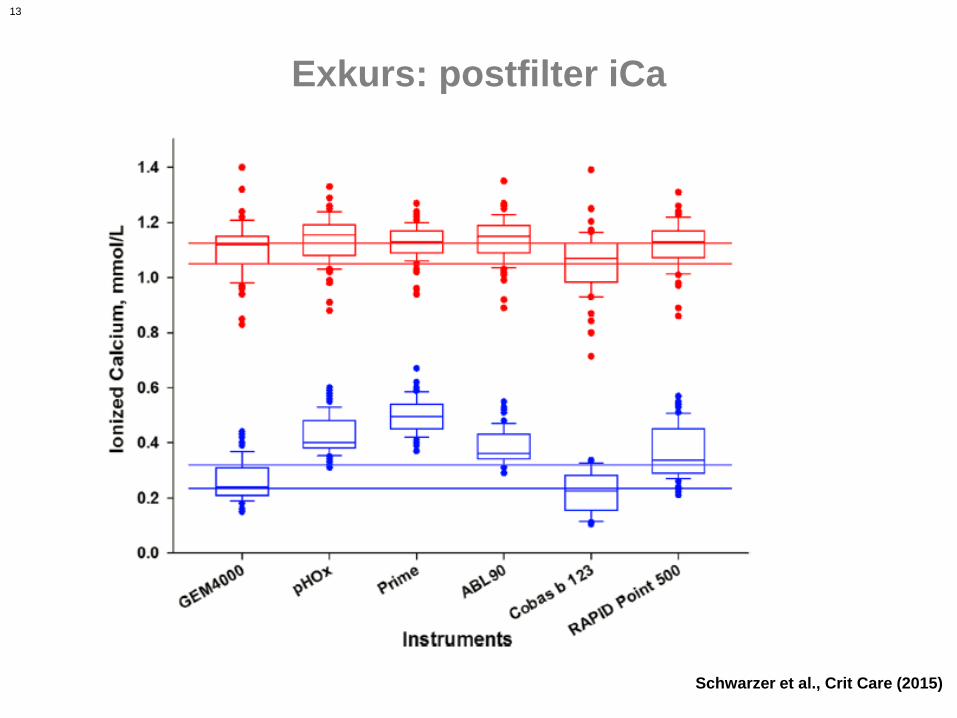
13
Exkurs: postfilter iCa
Schwarzer et al., Crit Care (2015)
14
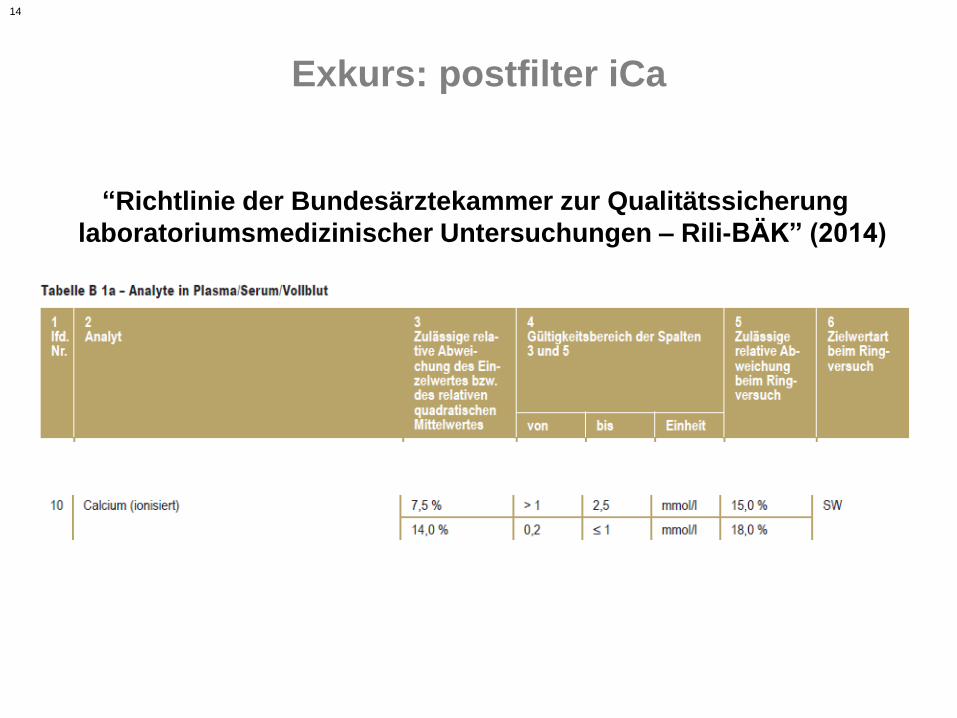
Exkurs: postfilter iCa
“Richtlinie der Bundesärztekammer zur Qualitätssicherung
laboratoriumsmedizinischer Untersuchungen – Rili-BÄK” (2014)
15
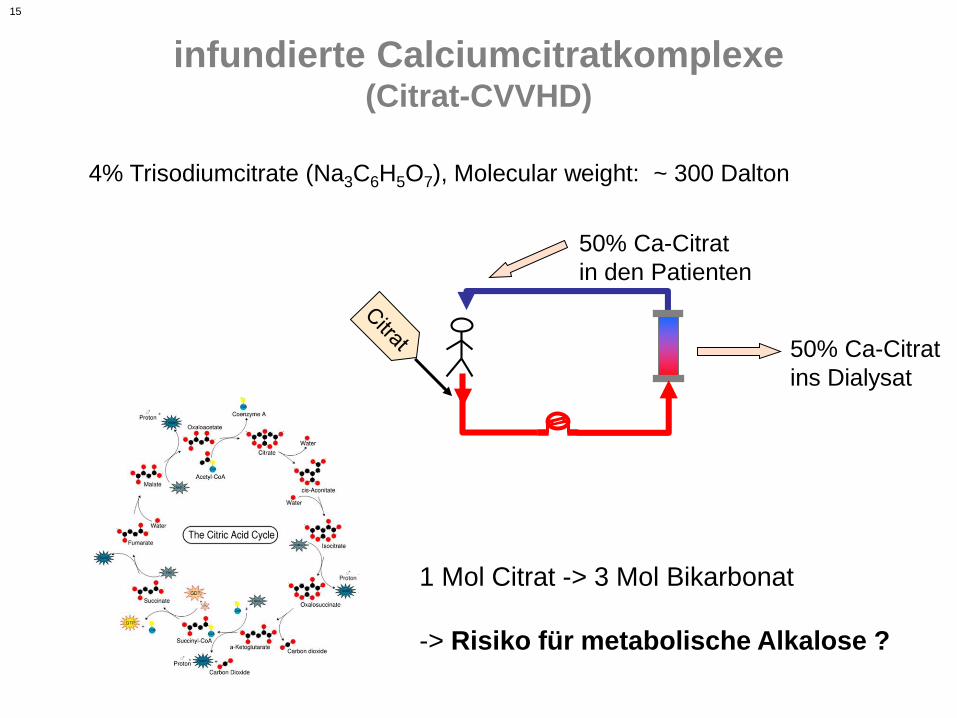
infundierte Calciumcitratkomplexe(Citrat-CVVHD)
4% Trisodiumcitrate (Na3C6H5O7), Molecular weight: ~ 300 Dalton
50% Ca-Citrat
ins Dialysat
50% Ca-Citrat
in den Patienten
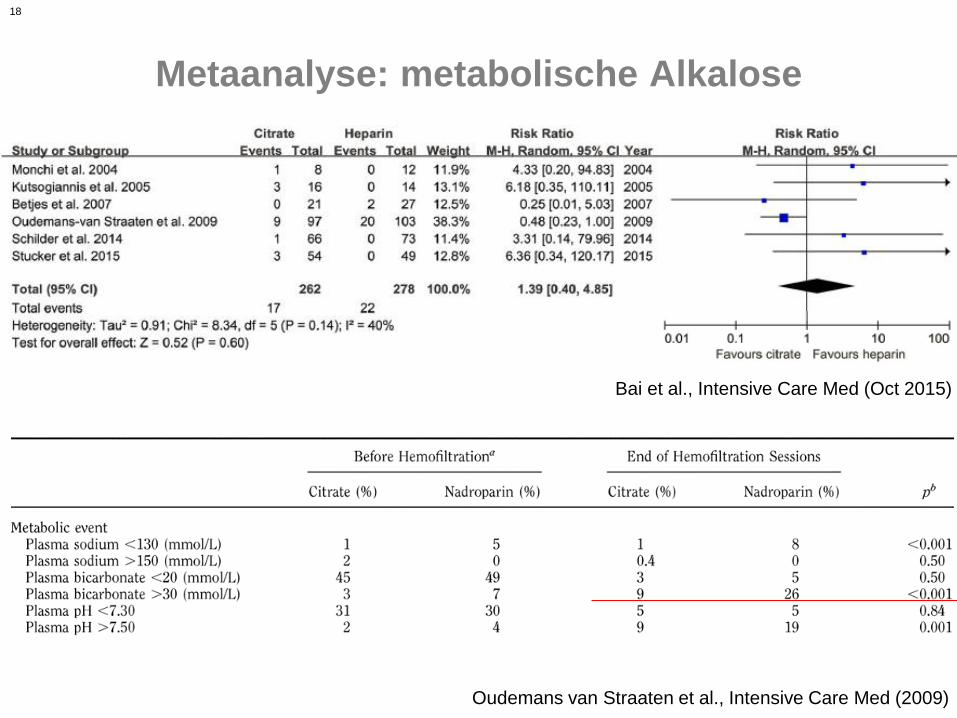
1 Mol Citrat -> 3 Mol Bikarbonat
-> Risiko für metabolische Alkalose ?
16
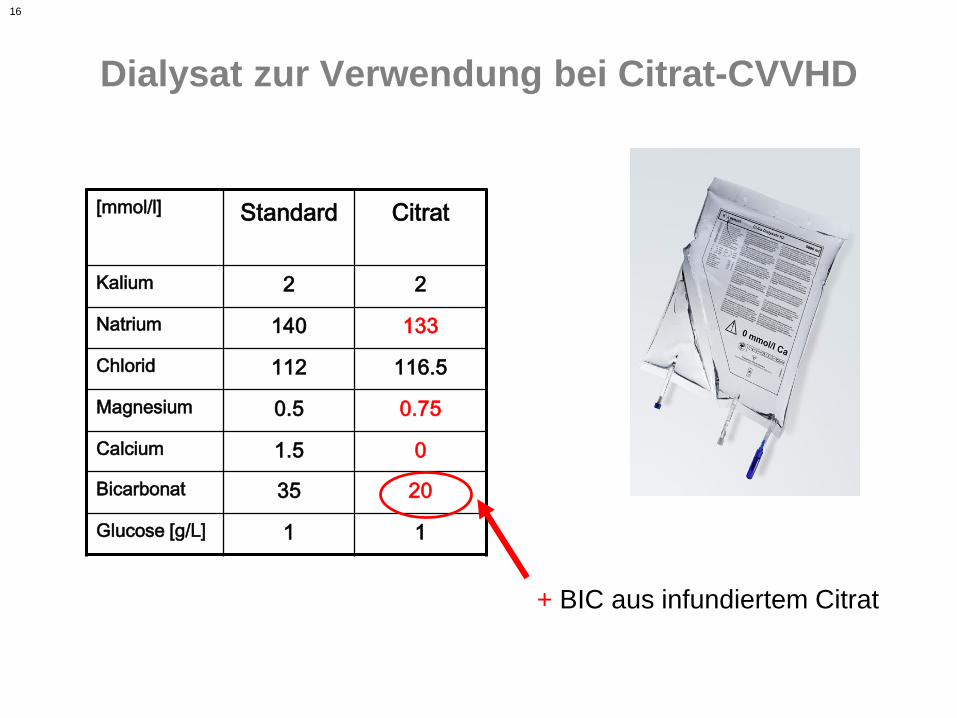
Dialysat zur Verwendung bei Citrat-CVVHD
[mmol/l] Standard Citrat
Kalium 2 2
Natrium 140 133
Chlorid 112 116.5
Magnesium 0.5 0.75
Calcium 1.5 0
Bicarbonat 35 20
Glucose [g/L] 1 1
+ BIC aus infundiertem Citrat
17
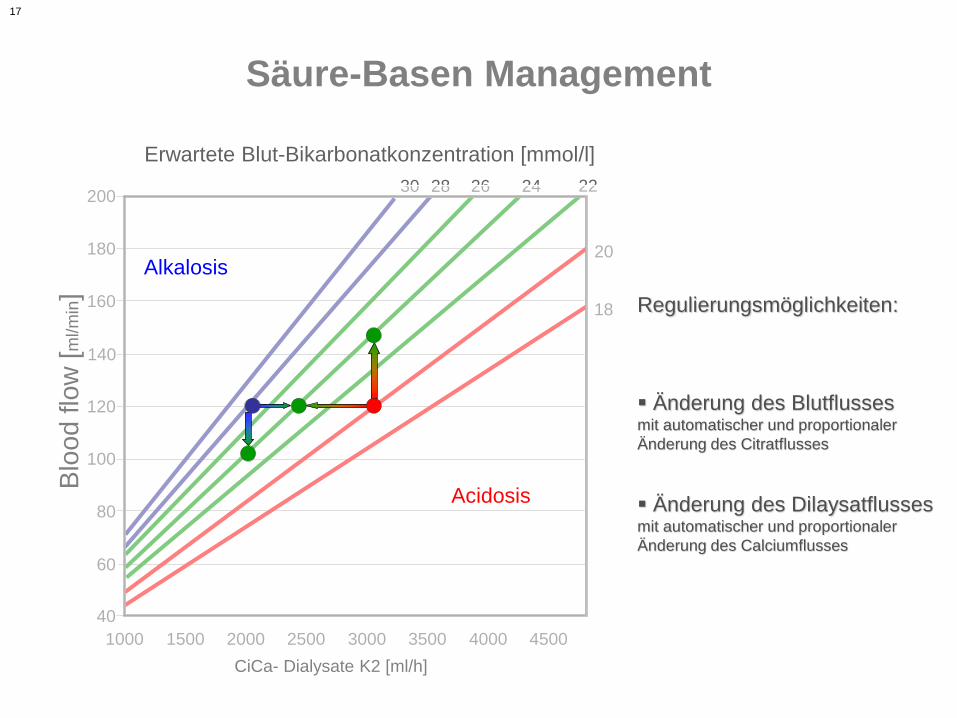
Säure-Basen Management
Änderung des Blutflussesmit automatischer und proportionaler
Änderung des Citratflusses
Regulierungsmöglichkeiten:
Erwartete Blut-Bikarbonatkonzentration [mmol/l]
Blo
od
flo
w [
ml/m
in]
40
60
80
100
120
140
160
180
200
CiCa- Dialysate K2 [ml/h]
30 242628
18
20
22
1000 1500 2000 2500 3000 3500 4000 4500
Alkalosis
Acidosis Änderung des Dilaysatflussesmit automatischer und proportionaler
Änderung des Calciumflusses
18
Metaanalyse: metabolische Alkalose
Bai et al., Intensive Care Med (Oct 2015)
Oudemans van Straaten et al., Intensive Care Med (2009)
19
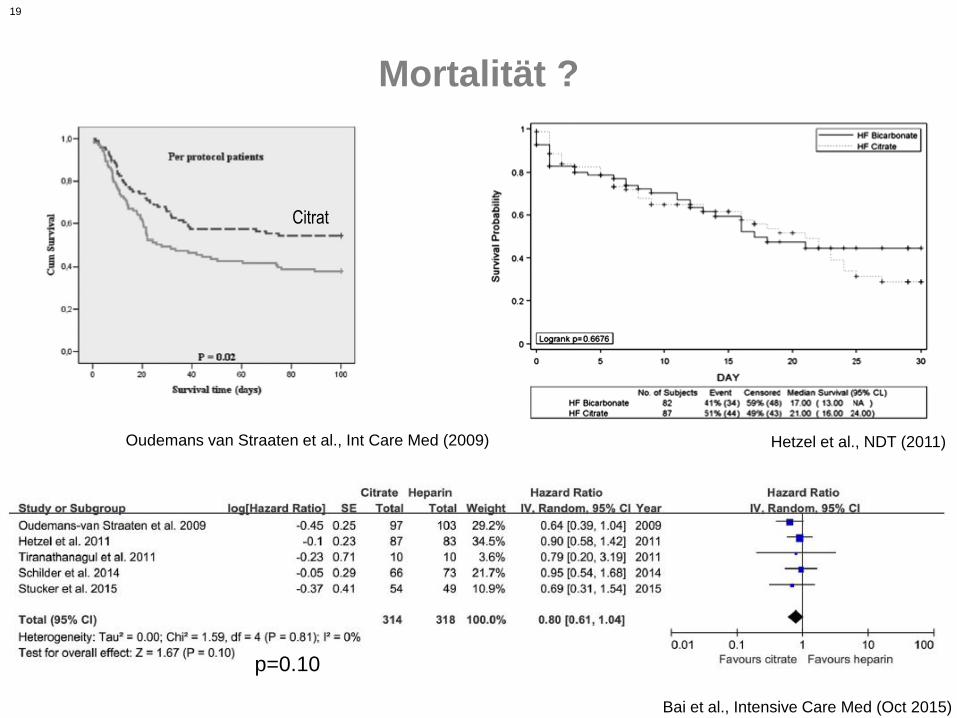
Mortalität ?
Bai et al., Intensive Care Med (Oct 2015)
Hetzel et al., NDT (2011)Oudemans van Straaten et al., Int Care Med (2009)
p=0.10
Citrat
20
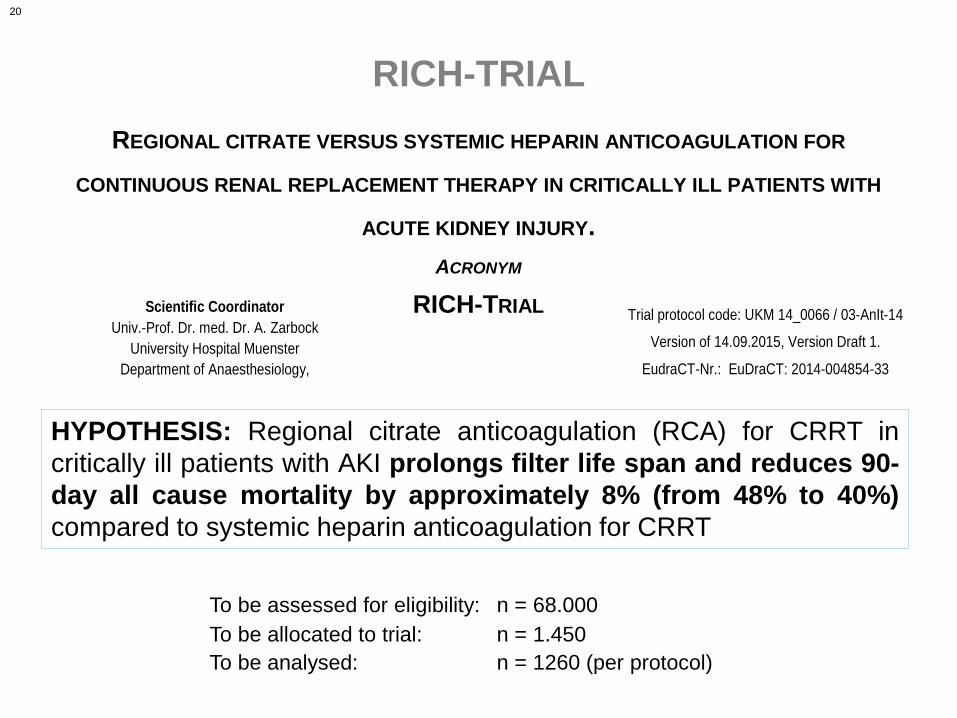
RICH-TRIAL
REGIONAL CITRATE VERSUS SYSTEMIC HEPARIN ANTICOAGULATION FOR
CONTINUOUS RENAL REPLACEMENT THERAPY IN CRITICALLY ILL PATIENTS WITH
ACUTE KIDNEY INJURY.
ACRONYM
RICH-TRIAL Scientific Coordinator
Univ.-Prof. Dr. med. Dr. A. Zarbock
University Hospital Muenster
Department of Anaesthesiology,
Trial protocol code: UKM 14_0066 / 03-AnIt-14
Version of 14.09.2015, Version Draft 1.
EudraCT-Nr.: EuDraCT: 2014-004854-33
To be assessed for eligibility: n = 68.000
To be allocated to trial: n = 1.450
To be analysed: n = 1260 (per protocol)
HYPOTHESIS: Regional citrate anticoagulation (RCA) for CRRT in
critically ill patients with AKI prolongs filter life span and reduces 90-
day all cause mortality by approximately 8% (from 48% to 40%)
compared to systemic heparin anticoagulation for CRRT
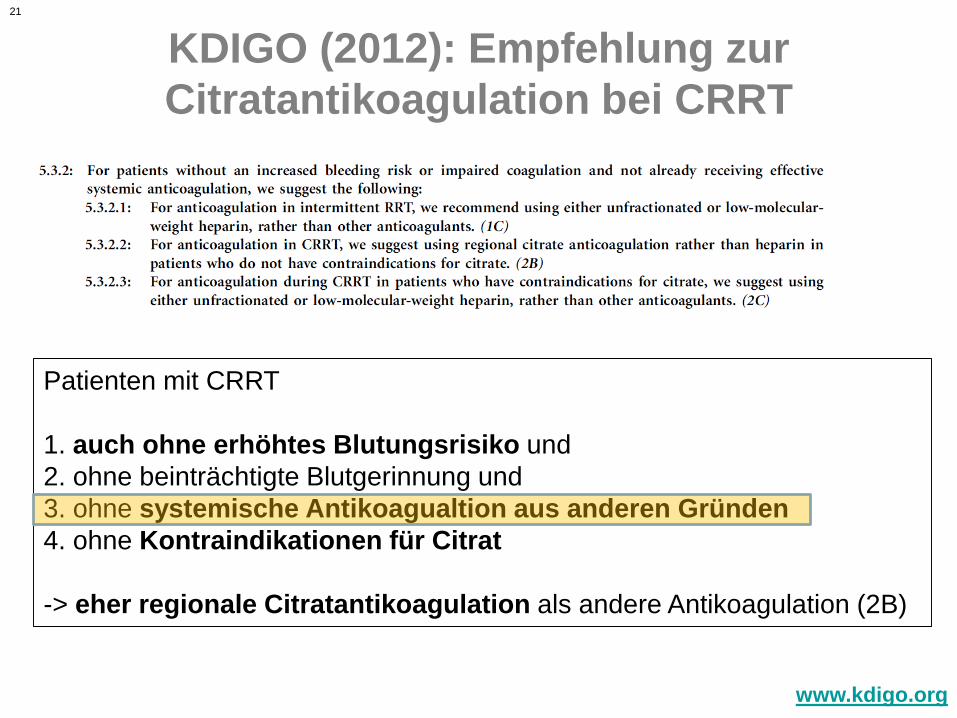
21
KDIGO (2012): Empfehlung zur
Citratantikoagulation bei CRRT
www.kdigo.org
Patienten mit CRRT
1. auch ohne erhöhtes Blutungsrisiko und
2. ohne beinträchtigte Blutgerinnung und
3. ohne systemische Antikoagualtion aus anderen Gründen
4. ohne Kontraindikationen für Citrat
-> eher regionale Citratantikoagulation als andere Antikoagulation (2B)
22
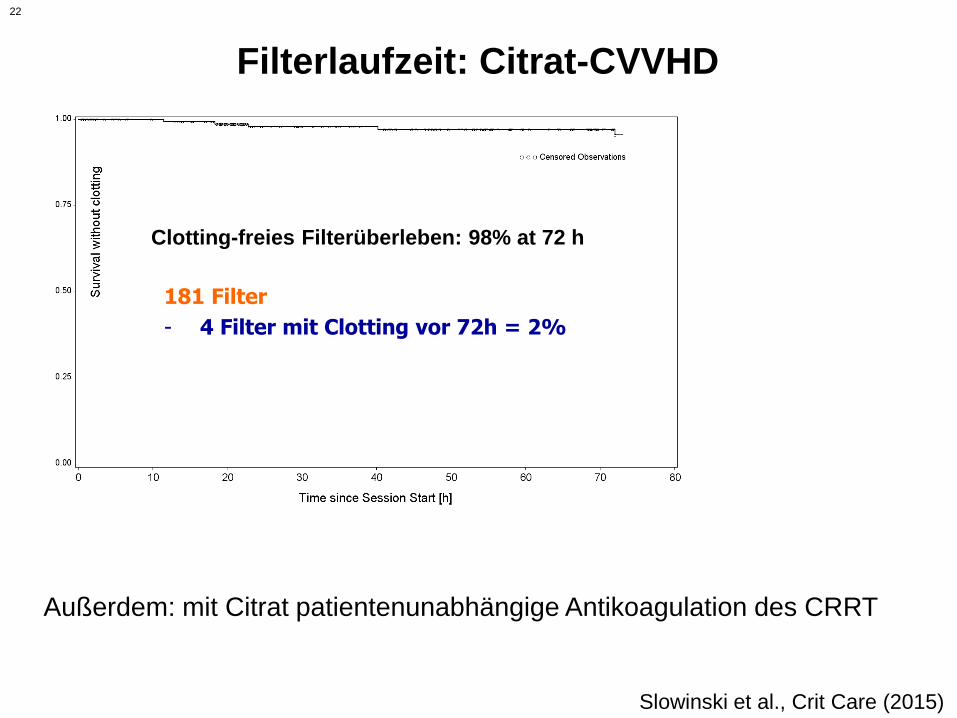
Filterlaufzeit: Citrat-CVVHD
181 Filter
- 4 Filter mit Clotting vor 72h = 2%
Clotting-freies Filterüberleben: 98% at 72 h
Außerdem: mit Citrat patientenunabhängige Antikoagulation des CRRT
Slowinski et al., Crit Care (2015)
23
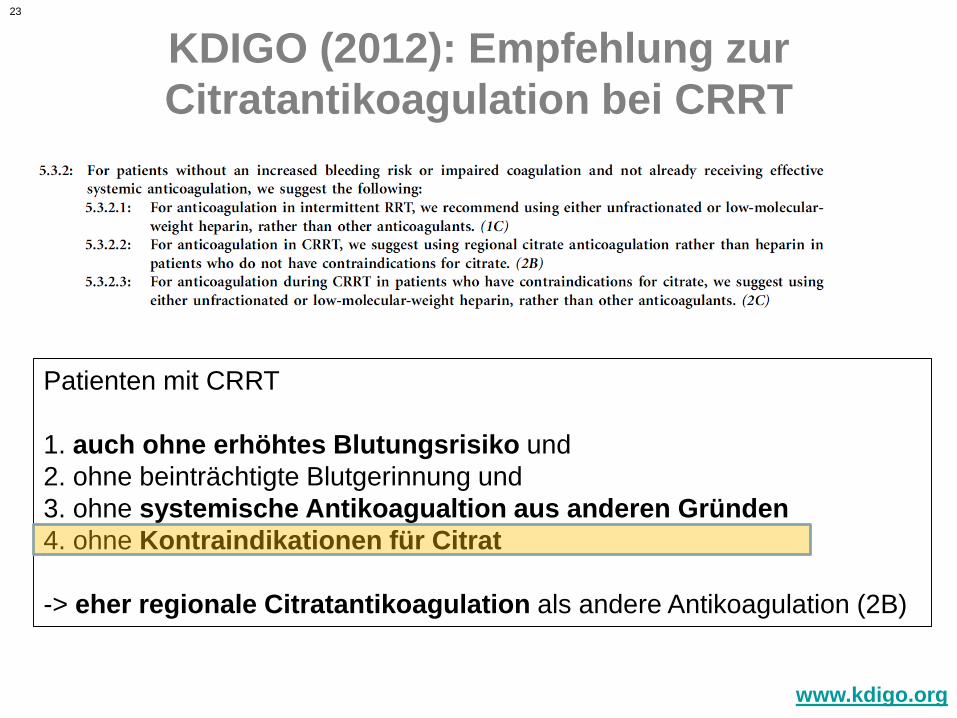
KDIGO (2012): Empfehlung zur
Citratantikoagulation bei CRRT
www.kdigo.org
Patienten mit CRRT
1. auch ohne erhöhtes Blutungsrisiko und
2. ohne beinträchtigte Blutgerinnung und
3. ohne systemische Antikoagualtion aus anderen Gründen
4. ohne Kontraindikationen für Citrat
-> eher regionale Citratantikoagulation als andere Antikoagulation (2B)
24
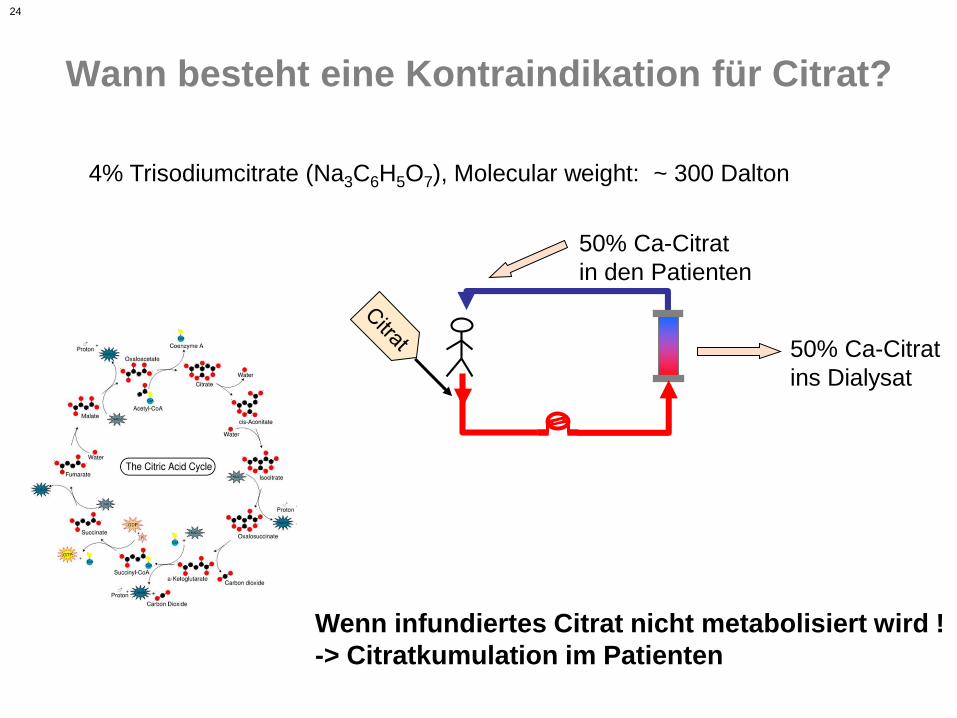
Wann besteht eine Kontraindikation für Citrat?
4% Trisodiumcitrate (Na3C6H5O7), Molecular weight: ~ 300 Dalton
50% Ca-Citrat
ins Dialysat
50% Ca-Citrat
in den Patienten
Wenn infundiertes Citrat nicht metabolisiert wird !
-> Citratkumulation im Patienten
25
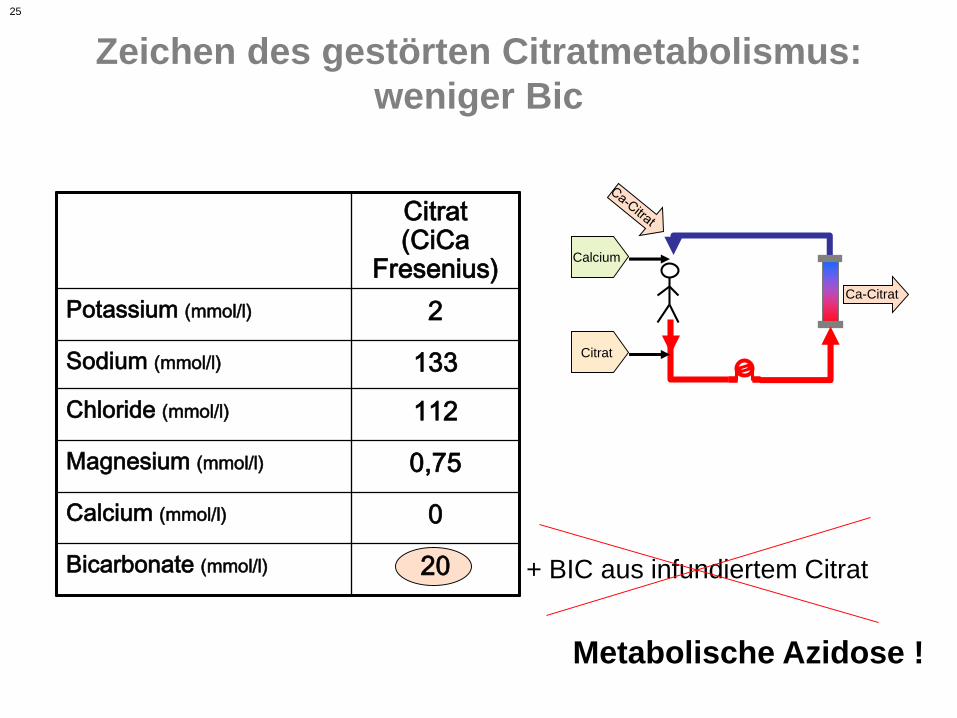
Zeichen des gestörten Citratmetabolismus:
weniger Bic
Citrat(CiCa
Fresenius)
Potassium (mmol/l) 2
Sodium (mmol/l) 133
Chloride (mmol/l) 112
Magnesium (mmol/l) 0,75
Calcium (mmol/l) 0
Bicarbonate (mmol/l) 20
Metabolische Azidose !
Citrat
Calcium
Ca-Citrat
+ BIC aus infundiertem Citrat
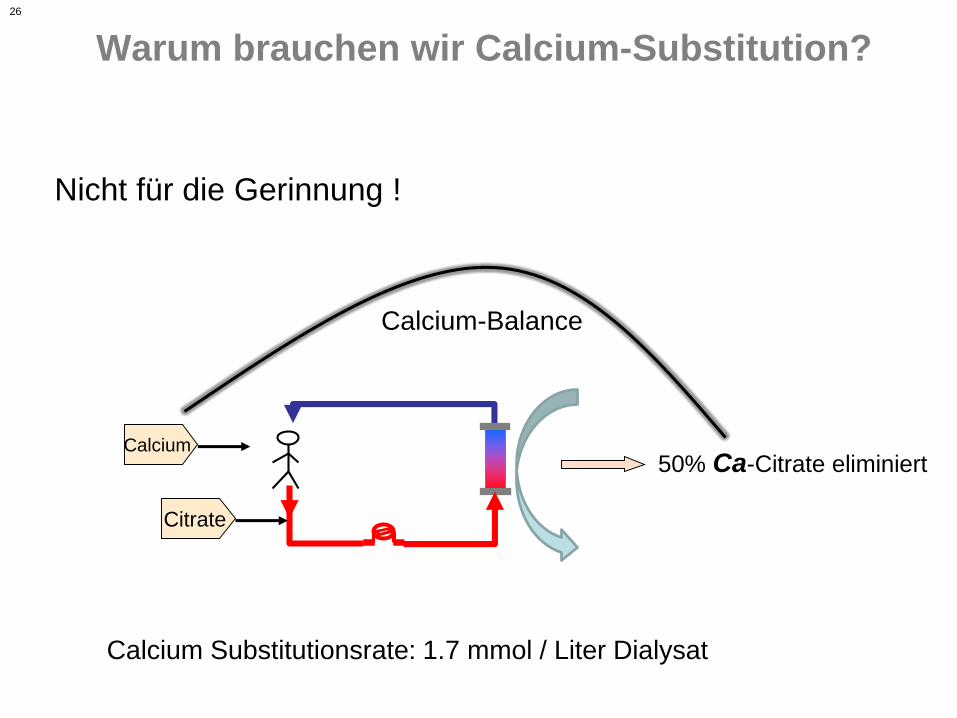
26
Warum brauchen wir Calcium-Substitution?
Citrate
50% Ca-Citrate eliminiertCalcium
Nicht für die Gerinnung !
Calcium-Balance
Calcium Substitutionsrate: 1.7 mmol / Liter Dialysat
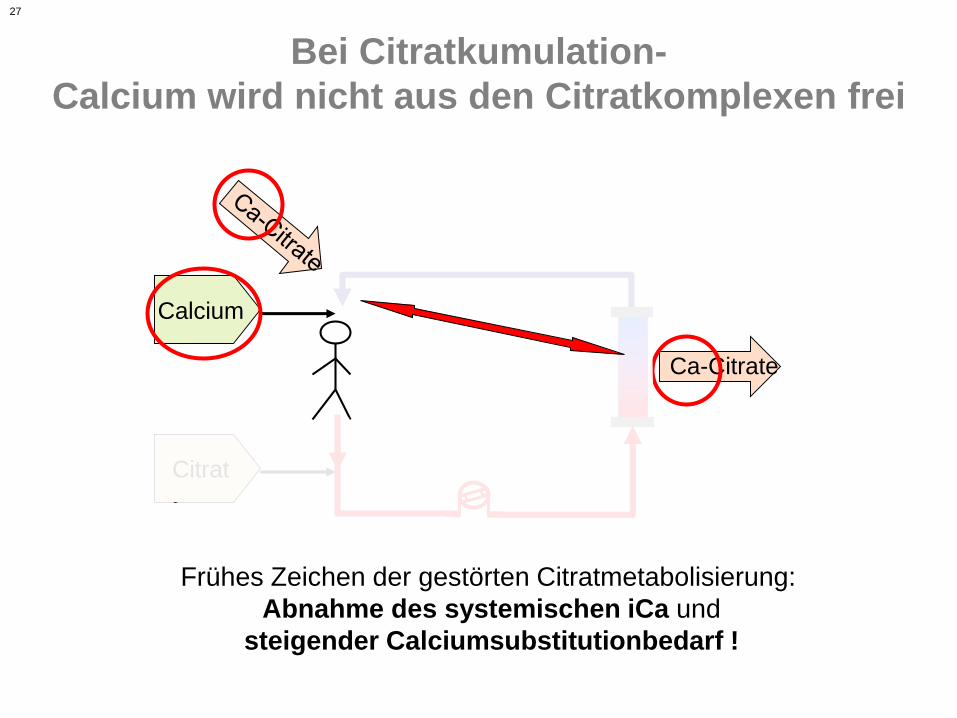
27
Bei Citratkumulation-
Calcium wird nicht aus den Citratkomplexen frei
Citrat
Calcium
Ca-Citrate
Frühes Zeichen der gestörten Citratmetabolisierung:
Abnahme des systemischen iCa und
steigender Calciumsubstitutionbedarf !
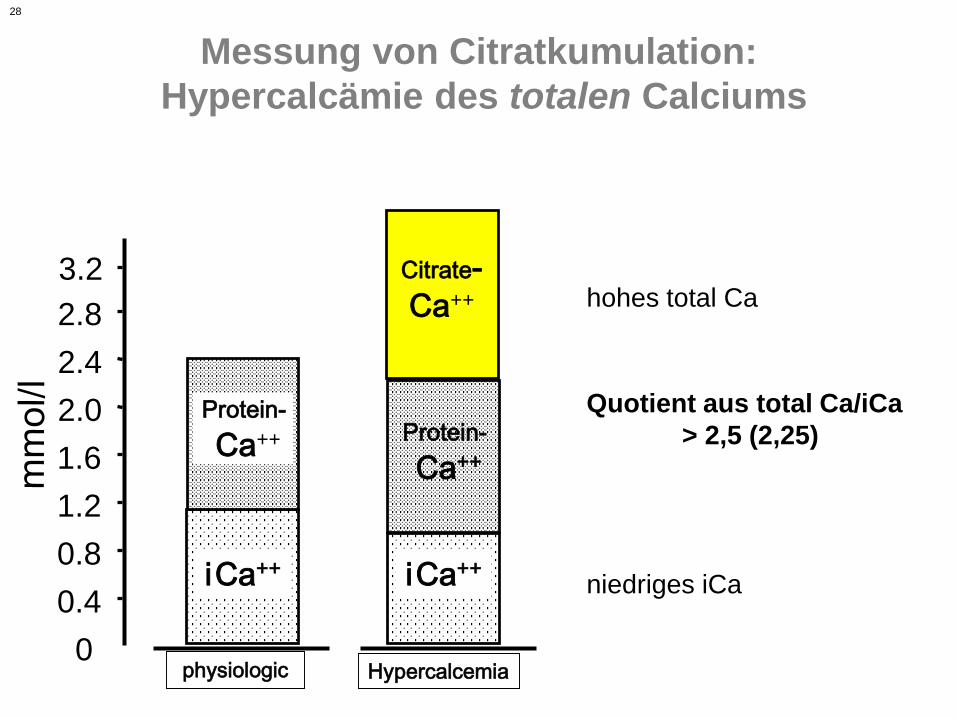
28
Messung von Citratkumulation:
Hypercalcämie des totalen Calciums
0
0.4
0.8
1.2
1.6
2.0
2.4
2.8
3.2
iCa++
Protein-
Ca++
physiologic
Citrate-
Ca++
iCa++
Protein-
Ca++
Hypercalcemia
niedriges iCa
hohes total Ca
Quotient aus total Ca/iCa
> 2,5 (2,25)
29
Zeichen der Citratkumulation
• Metabolische Azidose
• Niedriges ionisiertes Calcium
• total-Ca/iCa > 2,5
• (erweiterte Anionenlücke)
30
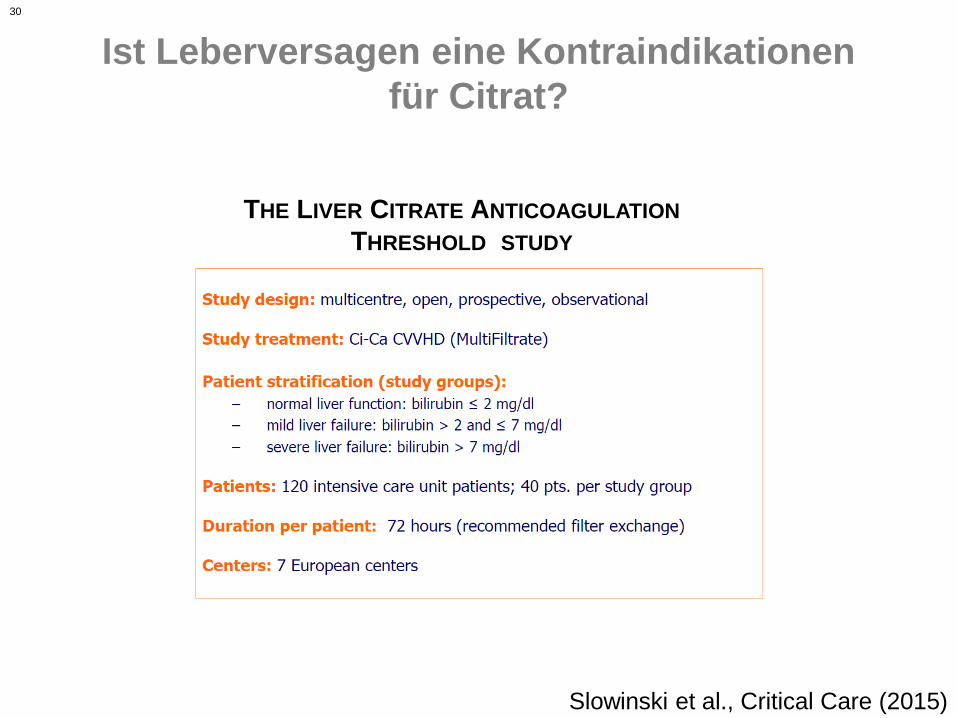
Ist Leberversagen eine Kontraindikationen
für Citrat?
THE LIVER CITRATE ANTICOAGULATION
THRESHOLD STUDY
Slowinski et al., Critical Care (2015)
31
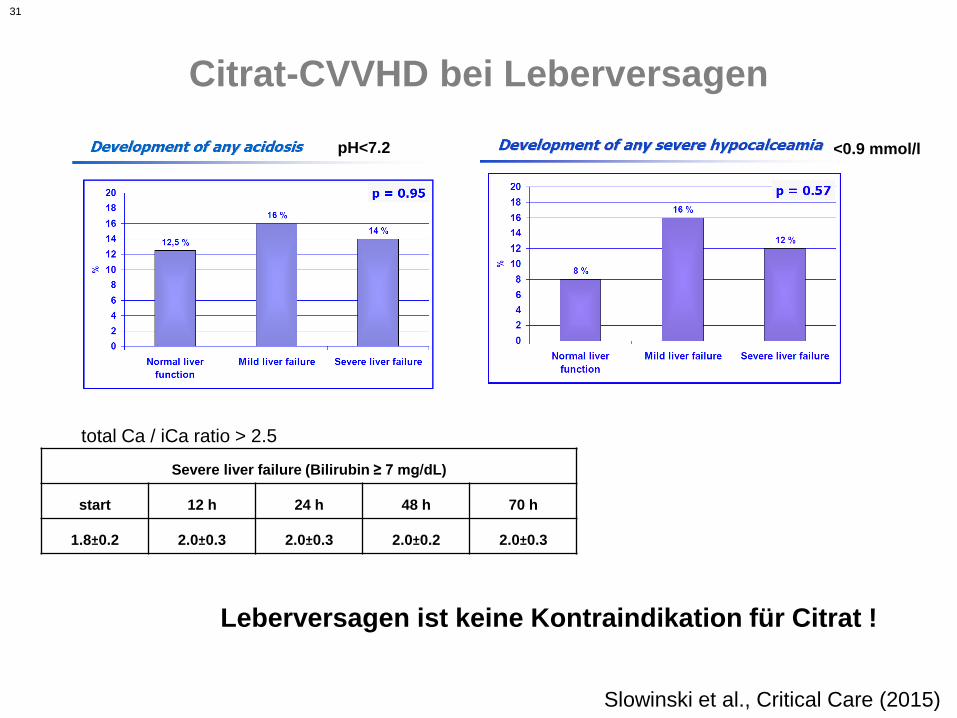
Citrat-CVVHD bei Leberversagen
Severe liver failure (Bilirubin ≥ 7 mg/dL)
start 12 h 24 h 48 h 70 h
1.8±0.2 2.0±0.3 2.0±0.3 2.0±0.2 2.0±0.3
total Ca / iCa ratio > 2.5
Leberversagen ist keine Kontraindikation für Citrat !
pH<7.2 <0.9 mmol/l
Slowinski et al., Critical Care (2015)
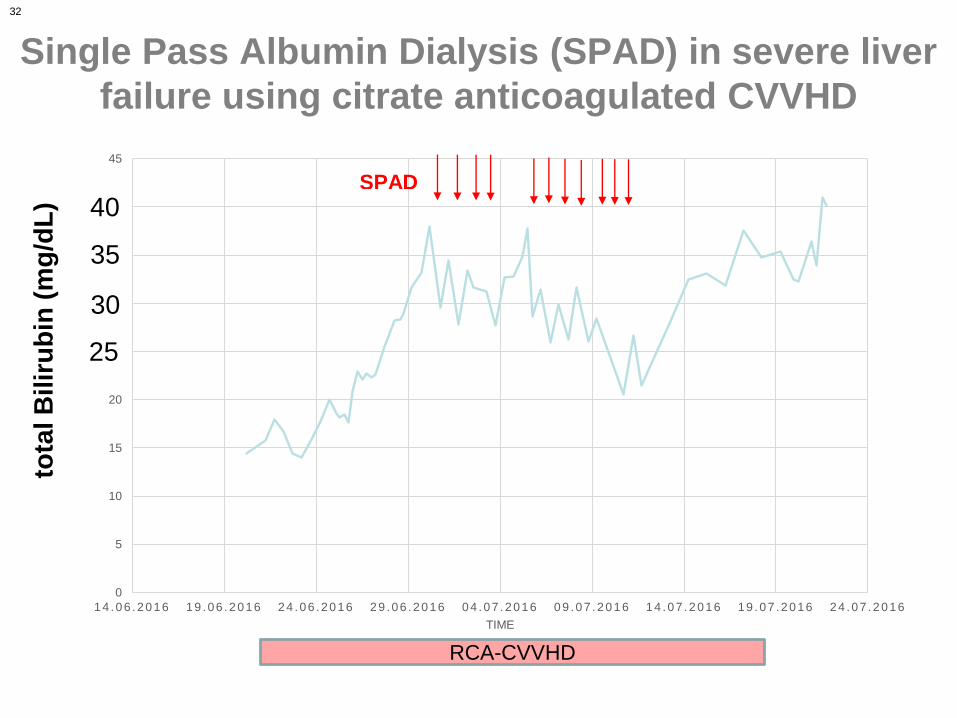
32
Single Pass Albumin Dialysis (SPAD) in severe liver
failure using citrate anticoagulated CVVHD
0
5
10
15
20
25
30
35
40
45
14 .06 .2016 19 .06 .2016 24 .06 .2016 29 .06 .2016 04 .07 .2016 09 .07 .2016 14 .07 .2016 19 .07 .2016 24 .07 .2016
TIME
SPAD
RCA-CVVHD
tota
l B
ilir
ub
in (
mg
/dL
)
30
35
40
25
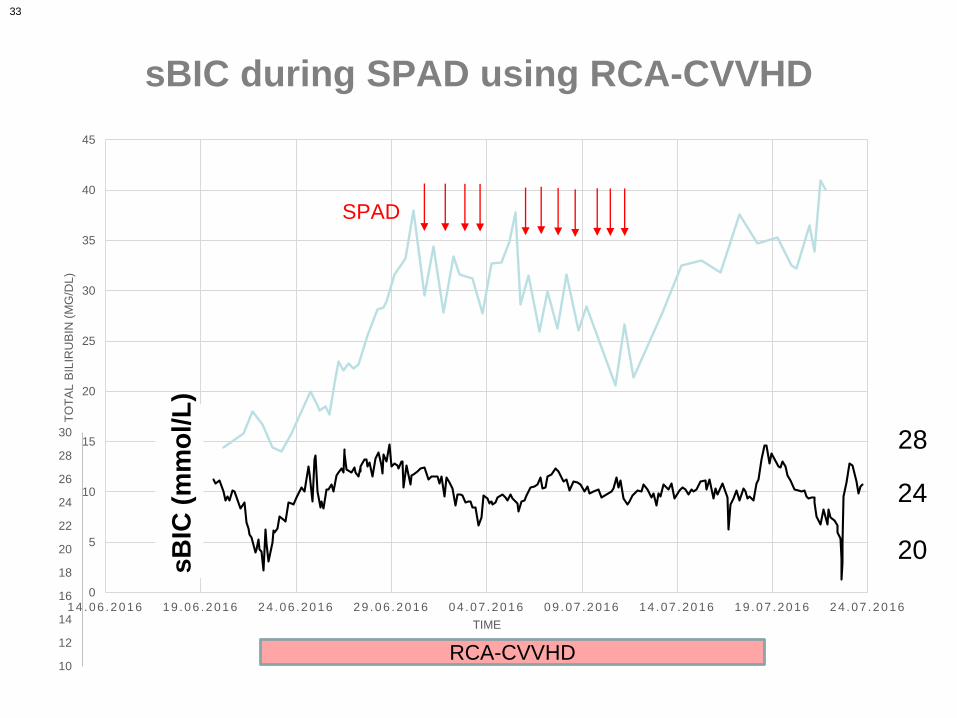
33
0
5
10
15
20
25
30
35
40
45
14 .06 .2016 19 .06 .2016 24 .06 .2016 29 .06 .2016 04 .07 .2016 09 .07 .2016 14 .07 .2016 19 .07 .2016 24 .07 .2016
TO
TA
L B
ILIR
UB
IN (
MG
/DL
)
TIME
SPAD
10
12
14
16
18
20
22
24
26
28
30
sB
IC (
mm
ol/L)
252520
24
28
RCA-CVVHD
sB
IC(m
mo
l/L
)
sBIC during SPAD using RCA-CVVHD
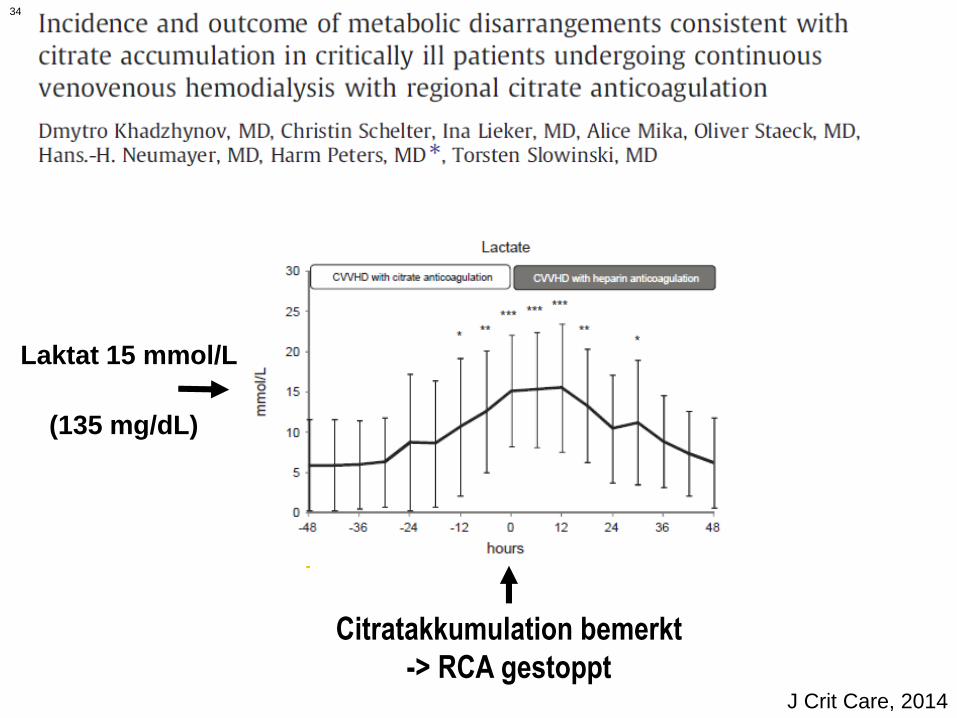
34
Citratakkumulation bemerkt
-> RCA gestopptJ Crit Care, 2014
Laktat 15 mmol/L
(135 mg/dL)
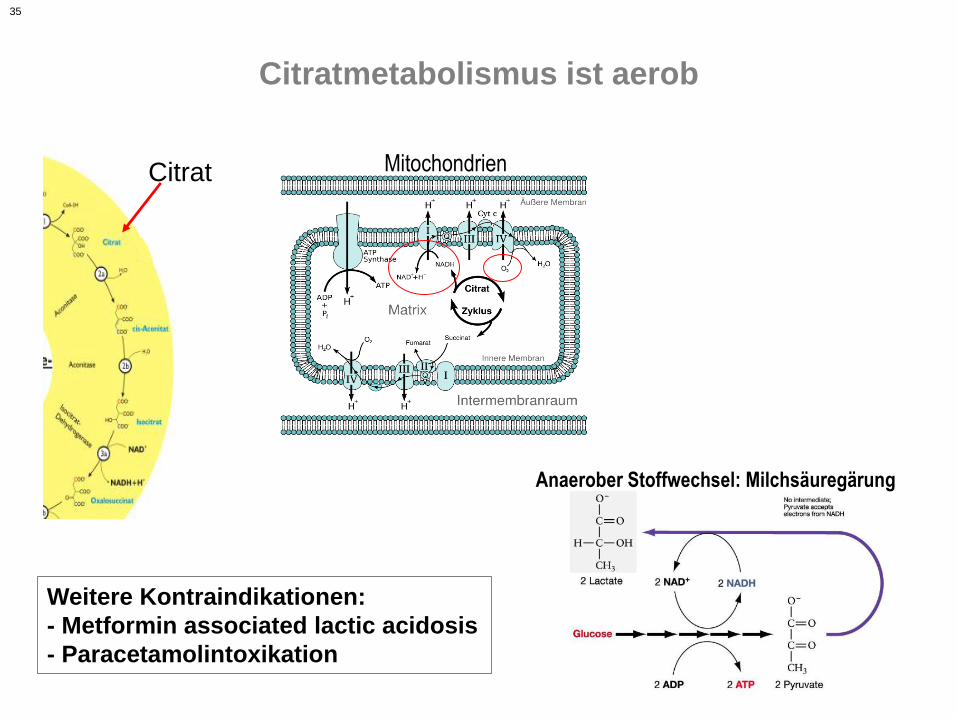
35
Citratmetabolismus ist aerob
Citrat Mitochondrien
Anaerober Stoffwechsel: Milchsäuregärung
Weitere Kontraindikationen:
- Metformin associated lactic acidosis
- Paracetamolintoxikation
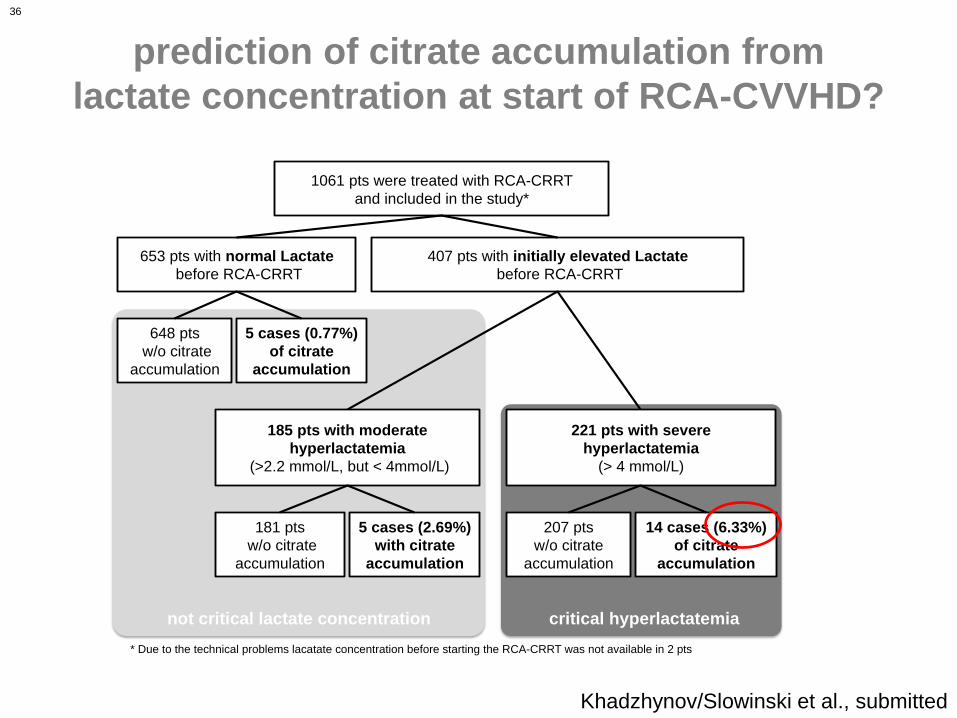
36
prediction of citrate accumulation from
lactate concentration at start of RCA-CVVHD?
1061 pts were treated with RCA-CRRT
and included in the study*
653 pts with normal Lactate
before RCA-CRRT
407 pts with initially elevated Lactate
before RCA-CRRT
648 pts
w/o citrate
accumulation
5 cases (0.77%)
of citrate
accumulation
185 pts with moderate
hyperlactatemia
(>2.2 mmol/L, but < 4mmol/L)
221 pts with severe
hyperlactatemia
(> 4 mmol/L)
181 pts
w/o citrate
accumulation
5 cases (2.69%)
with citrate
accumulation
207 pts
w/o citrate
accumulation
14 cases (6.33%)
of citrate
accumulation
Figure.1
not critical lactate concentration critical hyperlactatemia
* Due to the technical problems lacatate concentration before starting the RCA-CRRT was not available in 2 pts
Khadzhynov/Slowinski et al., submitted
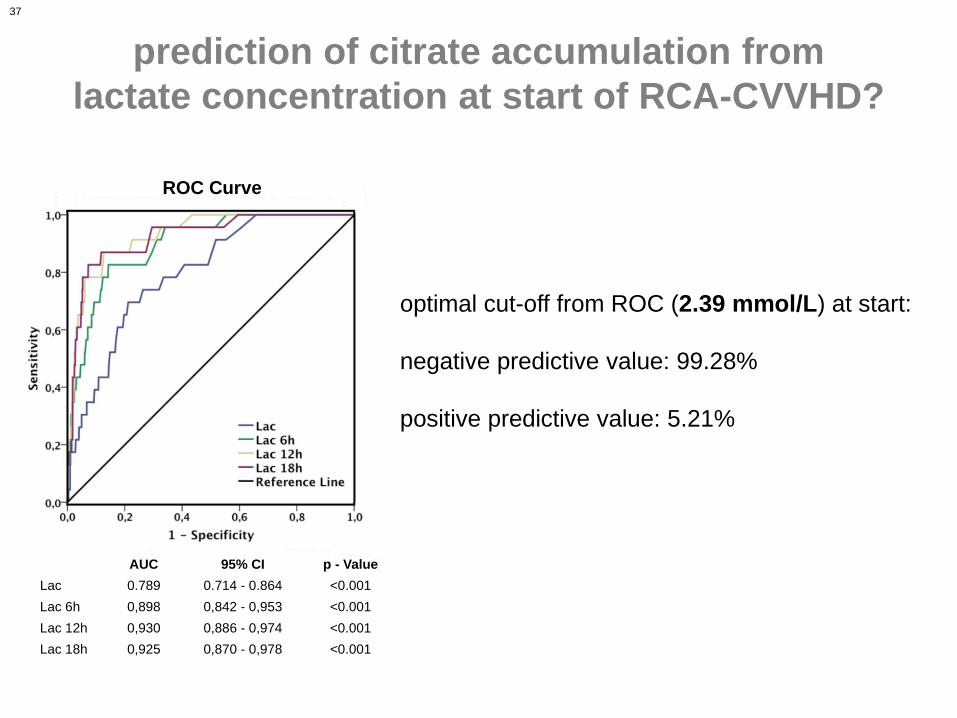
37
prediction of citrate accumulation from
lactate concentration at start of RCA-CVVHD?
ROC Curve
Fig. 2
AUC 95% CI p - Value
Lac 0.789 0.714 - 0.864 <0.001
Lac 6h 0,898 0,842 - 0,953 <0.001
Lac 12h 0,930 0,886 - 0,974 <0.001
Lac 18h 0,925 0,870 - 0,978 <0.001
optimal cut-off from ROC (2.39 mmol/L) at start:
negative predictive value: 99.28%
positive predictive value: 5.21%
38
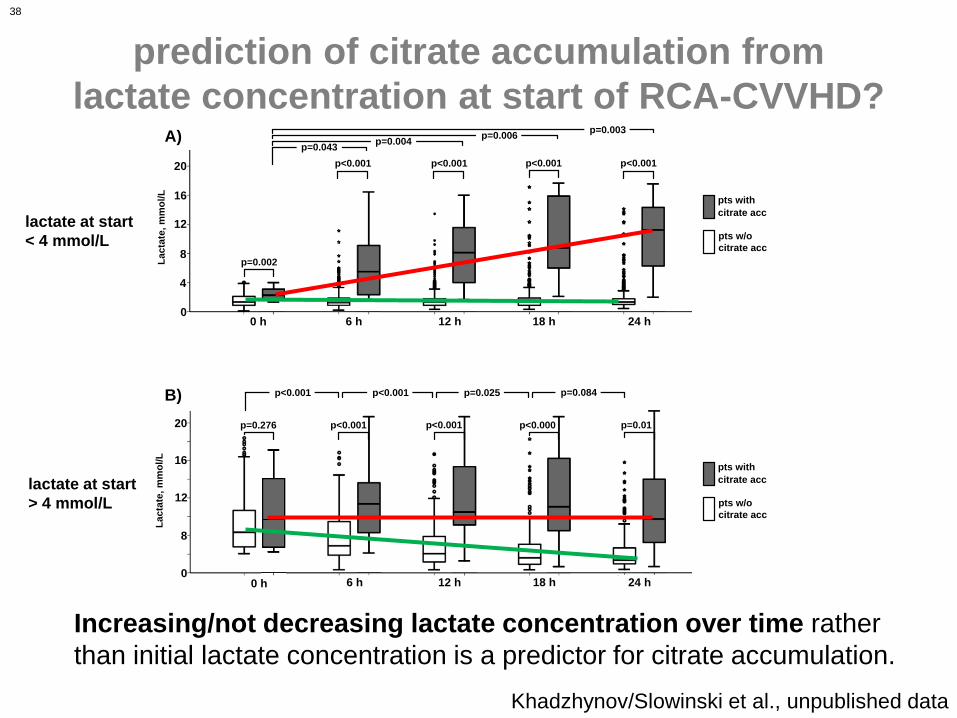
p=0.276
0 h 6 h 12 h 18 h 24 h0
8
12
16
20 p<0.001 p<0.001 p<0.000 p=0.01
p<0.001 p<0.001 p=0.025 p=0.084
Lac
tate
,m
mo
l/L
0
4
8
12
20
16
0 h 6 h 12 h 18 h 24 h
p=0.002
p<0.001 p<0.001 p<0.001 p<0.001
p=0.043p=0.004
p=0.006p=0.003
Lac
tate
,m
mo
l/L
A)
B)
pts with
citrate acc
pts w/o
citrate acc
pts with
citrate acc
pts w/o
citrate acc
prediction of citrate accumulation from
lactate concentration at start of RCA-CVVHD?
Khadzhynov/Slowinski et al., unpublished data
Increasing/not decreasing lactate concentration over time rather
than initial lactate concentration is a predictor for citrate accumulation.
lactate at start
< 4 mmol/L
lactate at start
> 4 mmol/L
39
Citratantikoagulation für alle?
- Geringeres Blutungsrisiko auch bei nicht-Risikopatienten
- Patientenunabhängige Antikoagulation der CRRT
- Bessere metabolische Kontrolle ist möglich
- Bessere Filterlaufzeit ist möglich
- Leberversagen alleine ist keine Kontraindikation für Citrat
- Vorsicht bei sehr hohem und
insbesondere bei steigendem Laktat