Embed Size (px)
Citation preview

PPI Therapie in der Praxis
Indikationen und InteraktionenH. Leskowschek, LKH Wagna
Samstag, 29. Januar 2011
Samstag, 29. Januar 2011
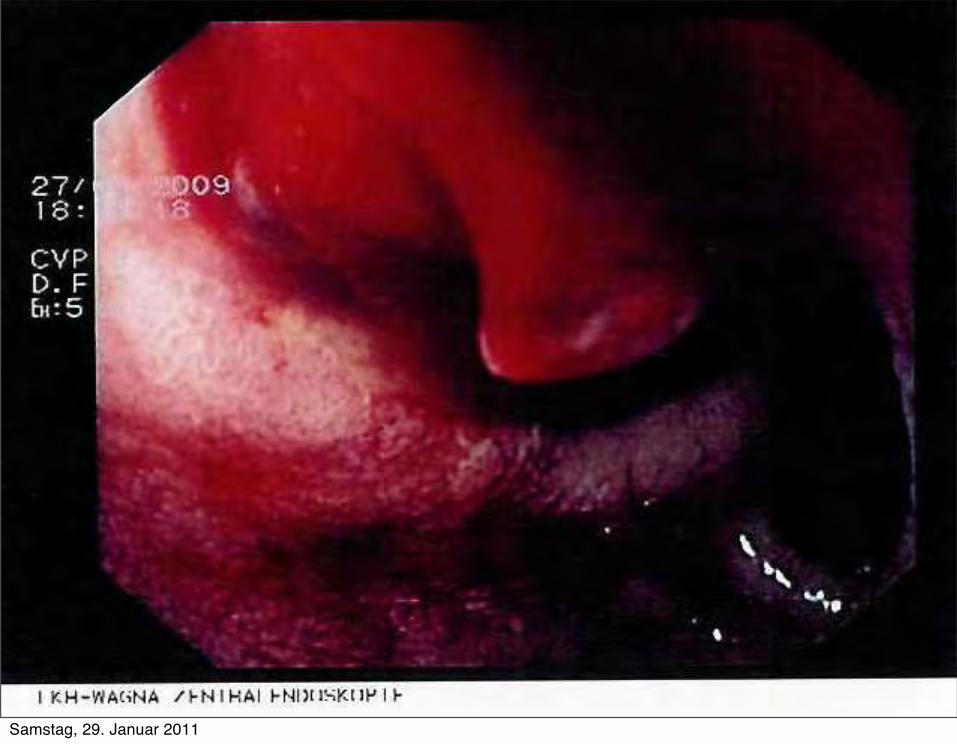
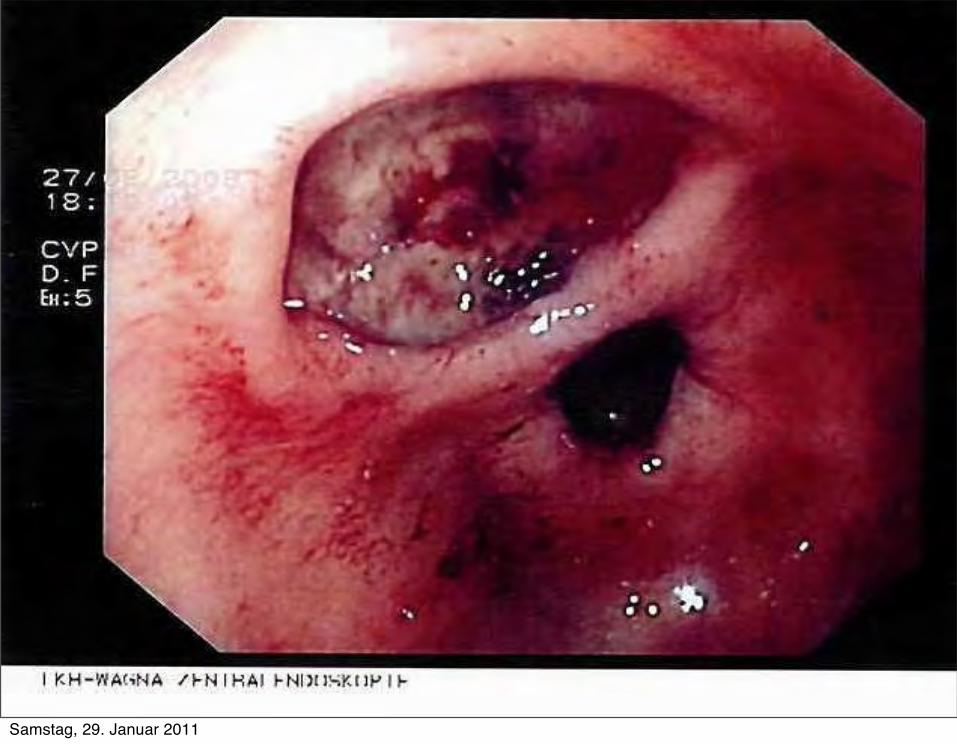
Fallbeispiel
R.R., weiblich, 84a
NAW Zugang wegen Hämatemesis und massiver Meläna
RR 80/50mmHg, tc FLA f=140
Ery 2,40;Hb 6,7; Hkt 20,7; INR 1,25
Samstag, 29. Januar 2011

Samstag, 29. Januar 2011
Samstag, 29. Januar 2011
Samstag, 29. Januar 2011
Samstag, 29. Januar 2011
Lovenox 40mg
Pantoloc 20mg
Hypren 2,5mg 1x1
Hydergin 6mg 1x1
ThromboASS 0/1/0
Betaserc 24mg 1/0/1
Pram 20mg 1/0/0
Aprednislon 25mg 1/0/0
Isomonat 20mg 1/0/0
Dancor ½ /0/ ½
Diclobene 1/0/1
Glurenorm 30 1/0/0 Samstag, 29. Januar 2011
Lovenox 40mg
Pantoloc 20mg
Hypren 2,5mg 1x1
Hydergin 6mg 1x1
ThromboASS 0/1/0
Betaserc 24mg 1/0/1
Pram 20mg 1/0/0
Aprednislon 25mg 1/0/0
Isomonat 20mg 1/0/0
Dancor ½ /0/ ½
Diclobene 1/0/1
Glurenorm 30 1/0/0 Samstag, 29. Januar 2011
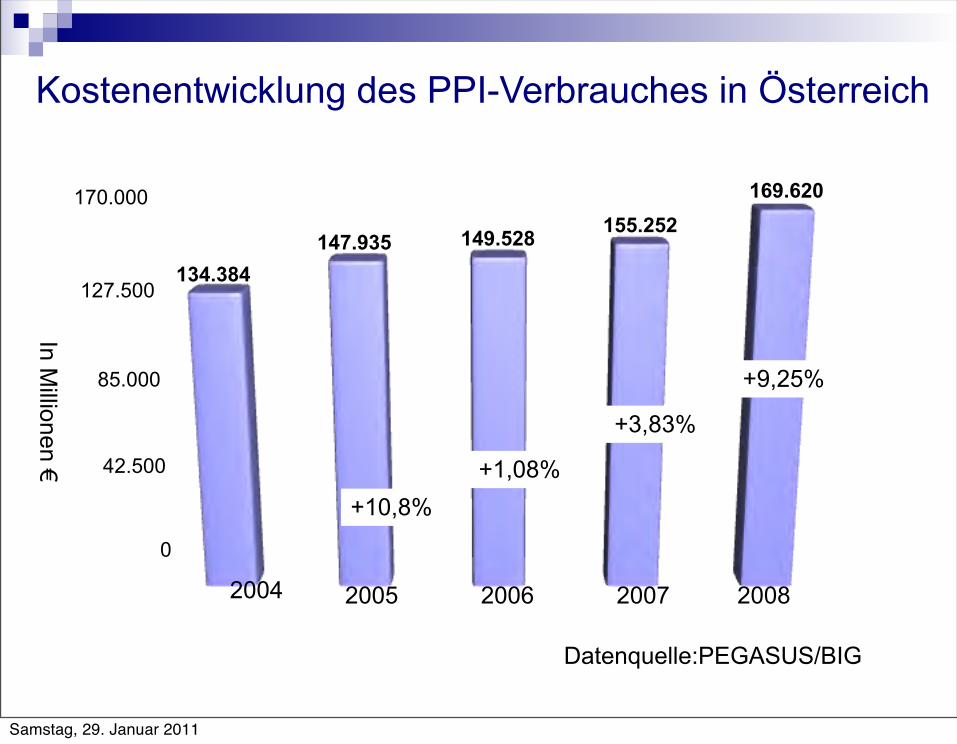
0
42.500
85.000
127.500
170.000
134.384147.935 149.528 155.252
169.620
2004 2005 2006 2007 2008
In Millionen €
Datenquelle:PEGASUS/BIG
Kostenentwicklung des PPI-Verbrauches in Österreich
+9,25%
+3,83%
+1,08%+10,8%
Samstag, 29. Januar 2011
Economic burden of unjustified medicationsat hospital discharge
• Von 577 entlassenen Patienten bei 318 mind. eine ungerechtfertigte Medikation.
• 619 von 3691 Verordnungen sind ungerechtfertigt (16,8%) 45,8% GI-Präparate (33,8% PPI) 17,7% Kardiovaskuläre Präparate (v.a. Statine) 17,2% Psychopharmaka (Antipsychotika, Benzodiazepine)
• Durchschnittliche Mehrkosten: 32€/Monat/Patient
Andreas Perrena et al; Swiss Med WKLY 2009
Samstag, 29. Januar 2011
Gezielter Einsatz? BMJ 2008:
In hospital inpatients taking proton pump inhibitors in Australia, Ireland, and the UK, 63%, 33%, and 67% of patients did not meet their country’s criteria for taking the drug.
In a series of hospital inpatients in Michigan, USA, 20% of patients were taking a proton pump inhibitor on admission and another 40% were prescribed the drug during their hospital stay (mostly for prophylaxis). At discharge, half the patients were taking a proton pump inhibitor - more than double the number who were taking the drug when admitted. In this study, 90% of patients did not need to take these drugs.
Mat Saad AZ et al. Proton pump inhibitors: a survey of prescribing in an Irish general hospital. Int J Clin Pract 2005;59:31-4Walker NM, McDonald J. An evaluation of the use of proton pump inhibitors. Pharm World Sci 2001;23:116-7Pham CQD et al;Acid suppressive therapy use on an inpatient internal medicine service. Ann Pharmacother 2006;Grant K,Continuation of proton pump inhibitors from hospital to community. Pharm World Sci 2006;28:189-93.
Samstag, 29. Januar 2011
ASS 100mg und PPI• >70a bei Erstverschreibung,
>75a bei bereits laufender Verschreibung
• Ulcusanamnese
• Kombinationstherapie mit
NSAR
Kortikosteroide
Antikoagulantien
andere Thrombozytenfunktionshemmer
SSRI
Konsensusstatement 2008 Thrombozytenaggregationshemmer und Magenschutz: Current Principles in Medicine Vol 1. 2008
Brauser et al;Lancet 2009 (FAMOUS trial)
Samstag, 29. Januar 2011
NSAR –Ulcus Prophylaxe
Konsensusbeschluss der ÖGGH und der Österreichischen Gesellschaft für Rheumatologie 2001 Journal für Gastroenterologische und Hepatologische Erkrankungen , 2004;2(4) 12-15
(Langzeit) NSAR Therapie +
>65a +Corticoide +T-ASS 100mg, Clopidogrel,… +SSRI + Ulcusanamnese <5a
Samstag, 29. Januar 2011
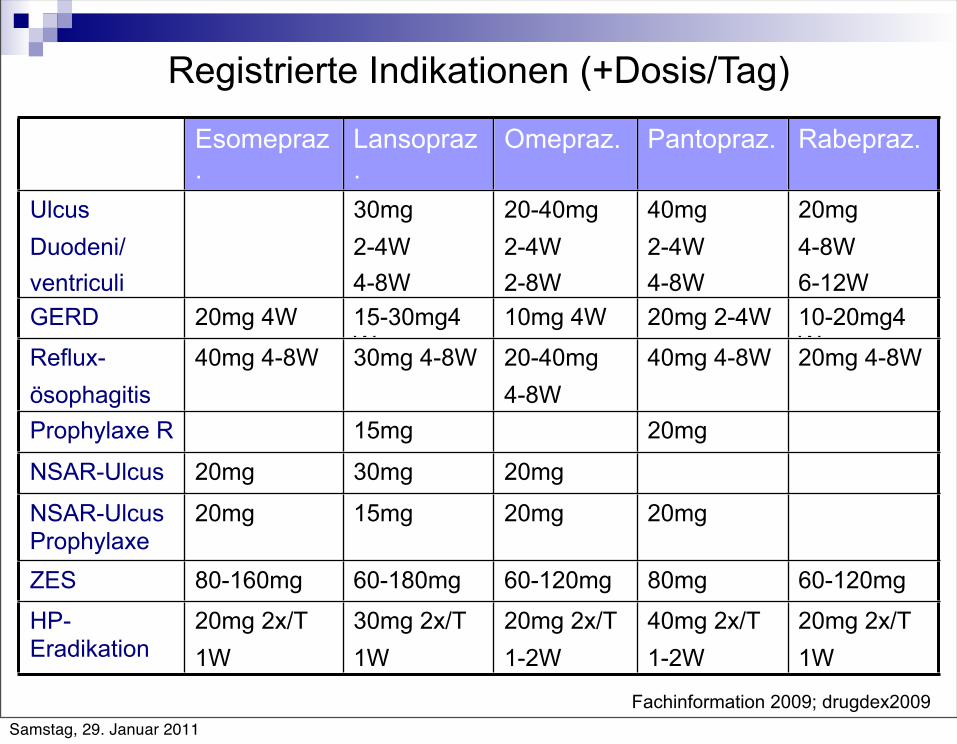
Registrierte Indikationen (+Dosis/Tag)
Esomepraz.
Lansopraz.
Omepraz. Pantopraz. Rabepraz.
Ulcus Duodeni/ventriculi
30mg2-4W4-8W
20-40mg2-4W2-8W
40mg2-4W4-8W
20mg4-8W6-12W
GERD 20mg 4W 15-30mg4W
10mg 4W 20mg 2-4W 10-20mg4WReflux-
ösophagitis40mg 4-8W 30mg 4-8W 20-40mg
4-8W40mg 4-8W 20mg 4-8W
Prophylaxe R 15mg 20mg
NSAR-Ulcus 20mg 30mg 20mg
NSAR-Ulcus Prophylaxe
20mg 15mg 20mg 20mg
ZES 80-160mg 60-180mg 60-120mg 80mg 60-120mg
HP-Eradikation
20mg 2x/T1W
30mg 2x/T1W
20mg 2x/T1-2W
40mg 2x/T1-2W
20mg 2x/T1W
Fachinformation 2009; drugdex2009Samstag, 29. Januar 2011
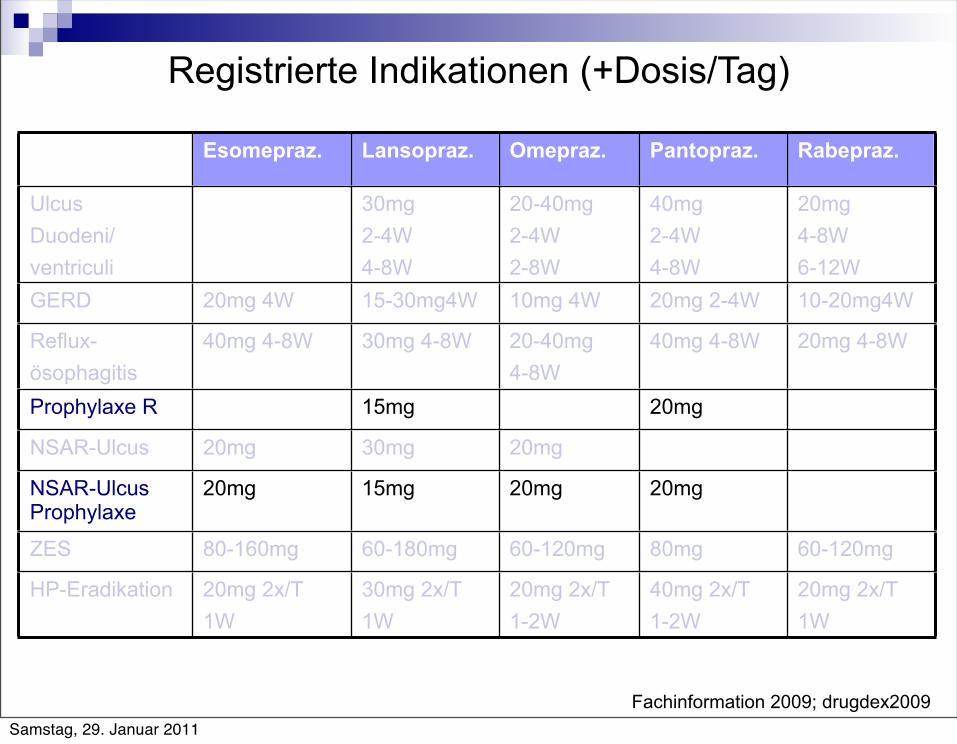
Registrierte Indikationen (+Dosis/Tag)
Esomepraz. Lansopraz. Omepraz. Pantopraz. Rabepraz.
Ulcus Duodeni/ventriculi
30mg2-4W4-8W
20-40mg2-4W2-8W
40mg2-4W4-8W
20mg4-8W6-12W
GERD 20mg 4W 15-30mg4W 10mg 4W 20mg 2-4W 10-20mg4W
Reflux-ösophagitis
40mg 4-8W 30mg 4-8W 20-40mg4-8W
40mg 4-8W 20mg 4-8W
Prophylaxe R 15mg 20mg
NSAR-Ulcus 20mg 30mg 20mg
NSAR-Ulcus Prophylaxe
20mg 15mg 20mg 20mg
ZES 80-160mg 60-180mg 60-120mg 80mg 60-120mg
HP-Eradikation 20mg 2x/T1W
30mg 2x/T1W
20mg 2x/T1-2W
40mg 2x/T1-2W
20mg 2x/T1W
Fachinformation 2009; drugdex2009Samstag, 29. Januar 2011
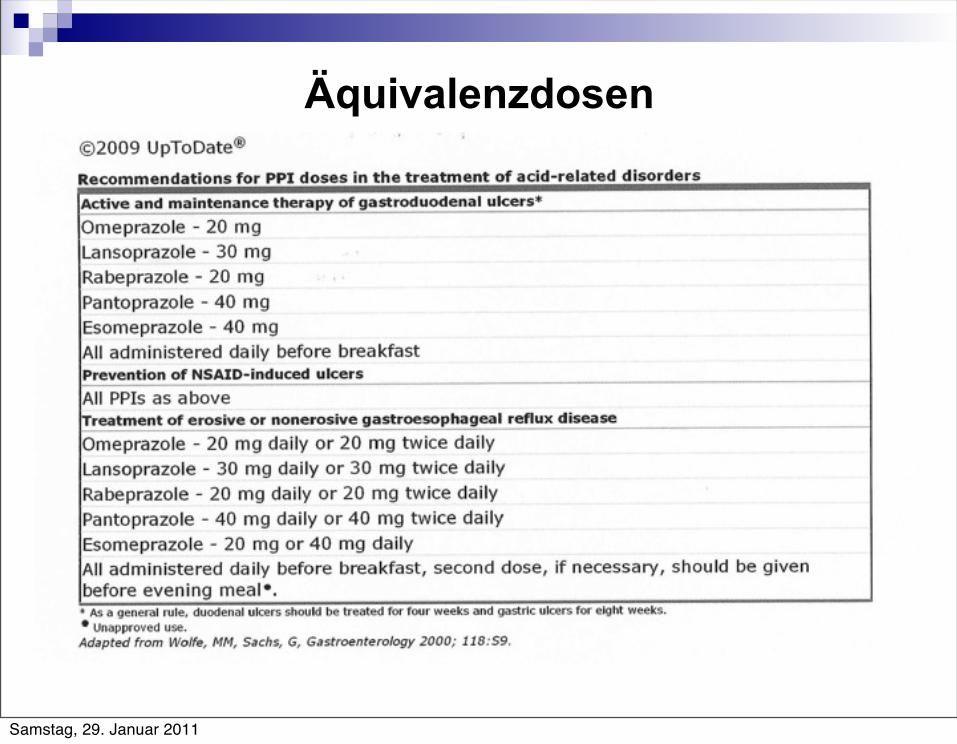
Äquivalenzdosen
Samstag, 29. Januar 2011

PPI Äquivalenzdosen
Esomeprazol 40mg (ER: 20mg)
Lansoprazol 30mg
Omeprazol 20mg
Pantoprazol 40mg
Rhabeprazol 20mg
Samstag, 29. Januar 2011
0
28
55
83
110
1 2 3 4
17
4536
102
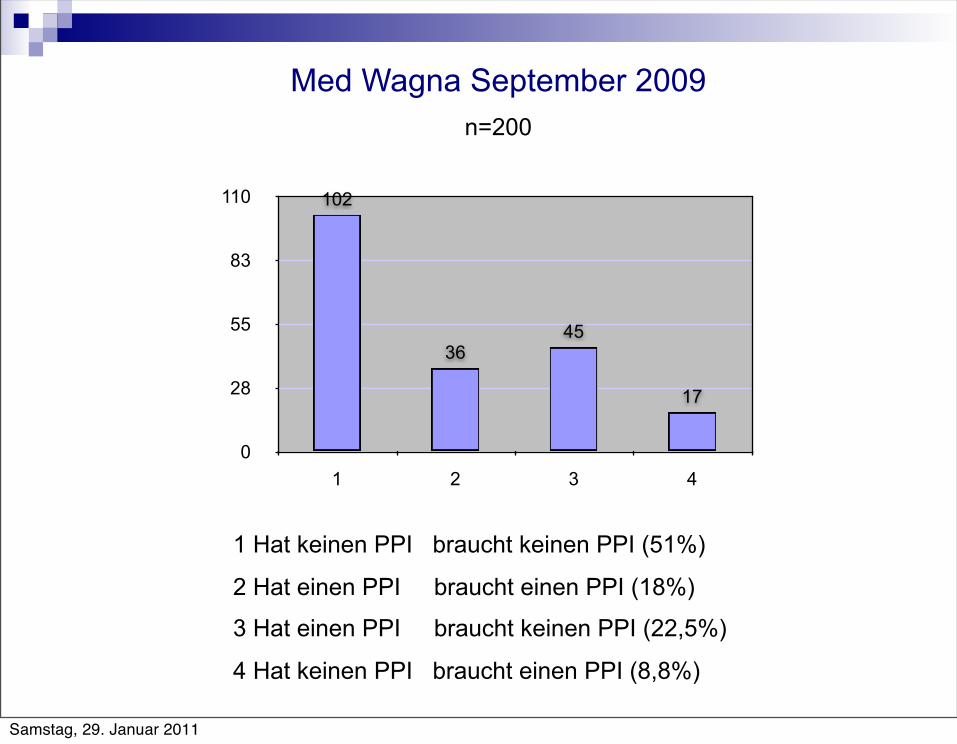
Med Wagna September 2009
n=200
1 Hat keinen PPI braucht keinen PPI (51%)
2 Hat einen PPI braucht einen PPI (18%)
3 Hat einen PPI braucht keinen PPI (22,5%)
4 Hat keinen PPI braucht einen PPI (8,8%)
Samstag, 29. Januar 2011
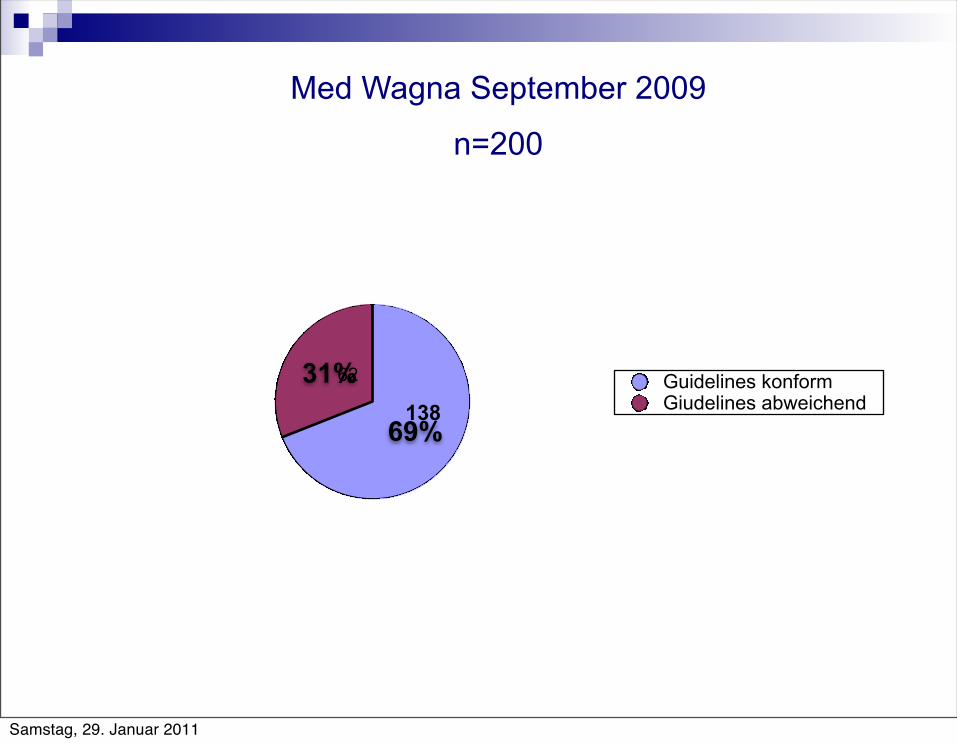
31%
69%
Guidelines konformGiudelines abweichend
62
138
Med Wagna September 2009
n=200
Samstag, 29. Januar 2011
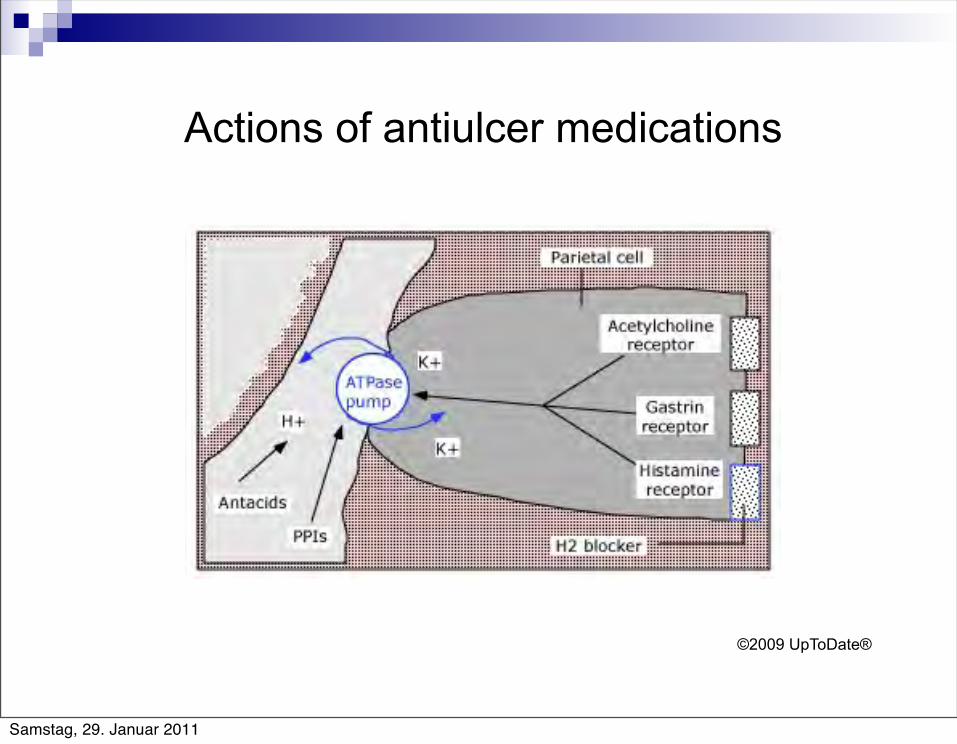
Actions of antiulcer medications
©2009 UpToDate®
Samstag, 29. Januar 2011
Wirkmechanismus
Substituierte Benzimidazole(pro-drug), die in den Parietalzellen bei sauren pH zu Sulfonamiden aktiviert werden, die an Cystein Untereinheiten der Protonenpumpe(H+/K+Adenosintriphosphatase) andocken und die Freisetzung von HCL irreversibel hemmen. Wirkung ist dosisabhängig.
Idealer Einnahmezeitpunkt: 30 Min vor der Mahlzeit, da sie v.a. aktivierte Protonenpumpen hemmen. Nicht teilen!
Per Sonde: Esomeprazol(Nexium) als Granulat oder Tabl.suspendieren; Lansoprazol Kapseln öffnen;
Samstag, 29. Januar 2011
Applikationsschemata
1x tgl. 30 Min vor dem Frühstück
1x tgl abends 30 Min vor einer Mahlzeit (v.a. bei nächtlichen Schmerzen)
Doppelte Standarddosis 2x tgl
2x tgl + H2-Blocker abends
Samstag, 29. Januar 2011
PPIs i.v.
Akute Gastrointestinale Blutung (40mg 2-3x/tgl versus 80mg Bolus+8mg/h
72h)
Zollinger-Ellison-Syndrom
Samstag, 29. Januar 2011
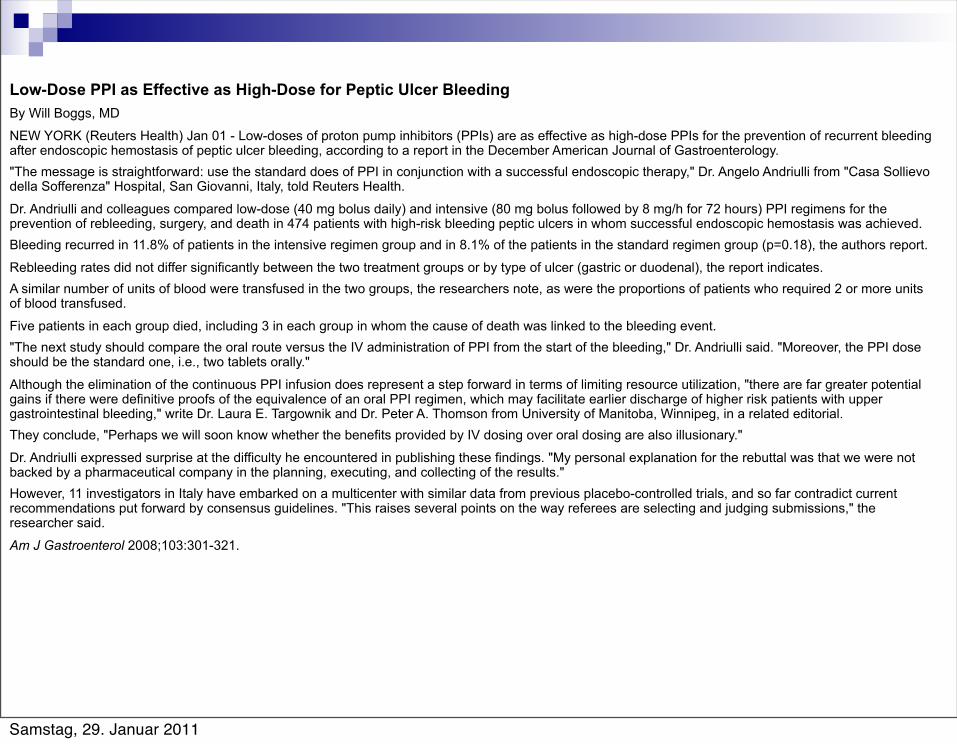
Low-Dose PPI as Effective as High-Dose for Peptic Ulcer BleedingBy Will Boggs, MD
NEW YORK (Reuters Health) Jan 01 - Low-doses of proton pump inhibitors (PPIs) are as effective as high-dose PPIs for the prevention of recurrent bleeding after endoscopic hemostasis of peptic ulcer bleeding, according to a report in the December American Journal of Gastroenterology."The message is straightforward: use the standard does of PPI in conjunction with a successful endoscopic therapy," Dr. Angelo Andriulli from "Casa Sollievo della Sofferenza" Hospital, San Giovanni, Italy, told Reuters Health.
Dr. Andriulli and colleagues compared low-dose (40 mg bolus daily) and intensive (80 mg bolus followed by 8 mg/h for 72 hours) PPI regimens for the prevention of rebleeding, surgery, and death in 474 patients with high-risk bleeding peptic ulcers in whom successful endoscopic hemostasis was achieved.Bleeding recurred in 11.8% of patients in the intensive regimen group and in 8.1% of the patients in the standard regimen group (p=0.18), the authors report.
Rebleeding rates did not differ significantly between the two treatment groups or by type of ulcer (gastric or duodenal), the report indicates.A similar number of units of blood were transfused in the two groups, the researchers note, as were the proportions of patients who required 2 or more units of blood transfused.
Five patients in each group died, including 3 in each group in whom the cause of death was linked to the bleeding event."The next study should compare the oral route versus the IV administration of PPI from the start of the bleeding," Dr. Andriulli said. "Moreover, the PPI dose should be the standard one, i.e., two tablets orally."
Although the elimination of the continuous PPI infusion does represent a step forward in terms of limiting resource utilization, "there are far greater potential gains if there were definitive proofs of the equivalence of an oral PPI regimen, which may facilitate earlier discharge of higher risk patients with upper gastrointestinal bleeding," write Dr. Laura E. Targownik and Dr. Peter A. Thomson from University of Manitoba, Winnipeg, in a related editorial.They conclude, "Perhaps we will soon know whether the benefits provided by IV dosing over oral dosing are also illusionary."
Dr. Andriulli expressed surprise at the difficulty he encountered in publishing these findings. "My personal explanation for the rebuttal was that we were not backed by a pharmaceutical company in the planning, executing, and collecting of the results."However, 11 investigators in Italy have embarked on a multicenter with similar data from previous placebo-controlled trials, and so far contradict current recommendations put forward by consensus guidelines. "This raises several points on the way referees are selecting and judging submissions," the researcher said.
Am J Gastroenterol 2008;103:301-321.
Samstag, 29. Januar 2011
Low-Dose PPI as Effective as High-Dose for Peptic Ulcer BleedingBy Will Boggs, MDNEW YORK (Reuters Health) Jan 01 - Low-doses of proton pump inhibitors (PPIs) are as effective as high-dose PPIs for the prevention of recurrent bleeding after endoscopic hemostasis of peptic ulcer bleeding, according to a report in the December American Journal of Gastroenterology."The message is straightforward: use the standard does of PPI in conjunction with a successful endoscopic therapy," Dr. Angelo Andriulli from "Casa Sollievo della Sofferenza" Hospital, San Giovanni, Italy, told Reuters Health.Dr. Andriulli and colleagues compared low-dose (40 mg bolus daily) and intensive (80 mg bolus followed by 8 mg/h for 72 hours) PPI regimens for the prevention of rebleeding, surgery, and death in 474 patients with high-risk bleeding peptic ulcers in whom successful endoscopic hemostasis was achieved.Bleeding recurred in 11.8% of patients in the intensive regimen group and in 8.1% of the patients in the standard regimen group (p=0.18), the authors report.Rebleeding rates did not differ significantly between the two treatment groups or by type of ulcer (gastric or duodenal), the report indicates.A similar number of units of blood were transfused in the two groups, the researchers note, as were the proportions of patients who required 2 or more units of blood transfused.Five patients in each group died, including 3 in each group in whom the cause of death was linked to the bleeding event."The next study should compare the oral route versus the IV administration of PPI from the start of the bleeding," Dr. Andriulli said. "Moreover, the PPI dose should be the standard one, i.e., two tablets orally."Although the elimination of the continuous PPI infusion does represent a step forward in terms of limiting resource utilization, "there are far greater potential gains if there were definitive proofs of the equivalence of an oral PPI regimen, which may facilitate earlier discharge of higher risk patients with upper gastrointestinal bleeding," write Dr. Laura E. Targownik and Dr. Peter A. Thomson from University of Manitoba, Winnipeg, in a related editorial.They conclude, "Perhaps we will soon know whether the benefits provided by IV dosing over oral dosing are also illusionary."Dr. Andriulli expressed surprise at the difficulty he encountered in publishing these findings. "My personal explanation for the rebuttal was that we were not backed by a pharmaceutical company in the planning, executing, and collecting of the results."However, 11 investigators in Italy have embarked on a multicenter with similar data from previous placebo-controlled trials, and so far contradict current recommendations put forward by consensus guidelines. "This raises several points on the way referees are selecting and judging submissions," the researcher said.Am J Gastroenterol 2008;103:301-321.
Hochdosis versus Standarddosis: Kein Unterschied bez. Blutungsrezidiv, Verbrauch von Blutkonserven und Mortalität
Hinweis: kein Unterschied bez. i.v. versus p.o. Therapie
Samstag, 29. Januar 2011
Nebenwirkungen der PPIs
Akut(<12W): bis zu 5% Kopfschmerzen,Muskelschwäche,Leukopenie, Diarrhoe, Constipation, Nausea, Hauterscheinungen
Bei Langzeiteinsatz (>5-7a): Risiko für : osteoporotische Frakturen (Hemmung der Freisetzung v. Ca++) Nahrungsmittelallergien (Eiweißaufspaltung vermindert) Risiko für Darm- und Lungeninfektionen
Fachinformation, Drugdex,Vries F 2009;Laine L 2009;
Samstag, 29. Januar 2011
Samstag, 29. Januar 2011
PPIs und Clostridium difficile Infektion
94 Patienten mit C.difficile Diarrhoe:+ PPIs: Odds ratio:3,6 bei Niereninsuffizienz: 5,7
mögliche Ursache: durch pH Anstieg geringere Abtötung der Sporen und Bakterien
Dial et al;JAMA 2005Aseeri et al;Am J Gastroenterol 2008
Samstag, 29. Januar 2011
Kelly CP, Pothoulakis C, & LaMont JT: Clostridium difficile colitis.. N Engl J Med 1994; 330:257-262.
Sehulster L & Chinn RY: Guidelines for environmental infection control in health-care facilities. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee
(HICPAC). MMWR Recomm Rep 2003; 52(RR-10):1-42.
Dial S, Delaney JAC, Barkun AN, et al: Use of gastric acid-suppressive agents and the risk of community-acquired
Clostridium difficile-associated disease. JAMA 2005; 294(23):2989-2995.
Dial S, Alrasadi K, Manoukian C, et al: Risk of Clostridium difficile diarrhea among hospital inpatients prescribed
proton pump inhibitors: cohort and case-control studies. CMAJ 2004; 171(1):33-38.
Cunningham R, Dale B, Undy B, et al: Proton pump inhibitors as a risk factor for Clostridium difficile diarrhoea.
J Hosp Infect 2003; 54(3):243-245.
PPIs und Clostridium difficile Infektion
Samstag, 29. Januar 2011
PPI und im KH erworbene Pneumonie
Herzig SJ, Howell MD, Ngo LH. Marcantonio ER: Acid-Suppressive Medication Use and the Risk for Hospital-Acquired Pneumonia. JAMA.2009: 301(20):2120-8
Kohn LT, Corrigan JM, Donaldson MS: To err is human – Building a safer health system
n=32 922: Personen, die im KH säureunterdrückende Medikamente erhalten haben
83%: PPI, restliche Personen v.a. H2 Blocker
2219 Patienten erkrankten im KH an einer Pneumonie
Statistisch unbereinigt: 4,9% Pneumonie + PPI – 2,0% Pneumonie ohne PPI
Statistisch bereinigt: Mit PPI Pneumonierisiko um 30%> (nicht bei H2 Blocker)
USA: 180 000 durch PPI Gabe erworbene Pneumonie im KH
33 000 dadurch bedingte Todesfälle
Samstag, 29. Januar 2011
Interaktionen von PPIs
Erhöhung des pH-Werts im Magen
Beeinflussung des P-Glykoproteins
Beeinflussung des Cytochrom P450 Systems
Samstag, 29. Januar 2011
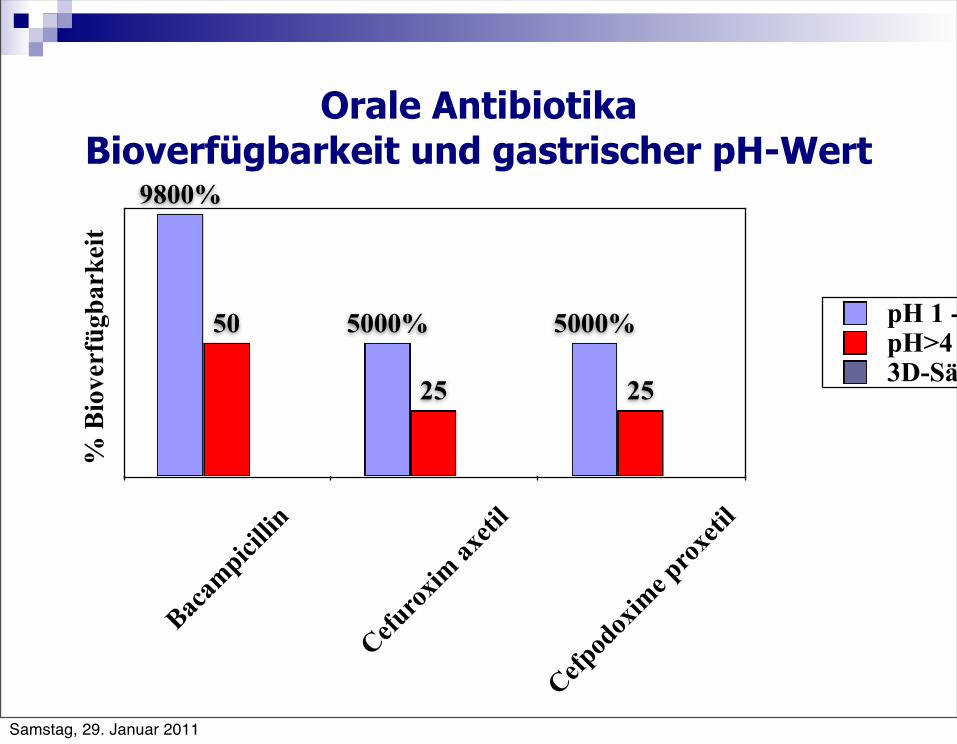
Orale Antibiotika Bioverfügbarkeit und gastrischer pH-Wert
Bacam
picillin
Cefurox
im ax
etil
Cefpod
oxim
e prox
etil
2525
50 5000%5000%
9800%
% B
iove
rfüg
bark
eit
pH 1 - 2pH>43D-Säule 3
Samstag, 29. Januar 2011
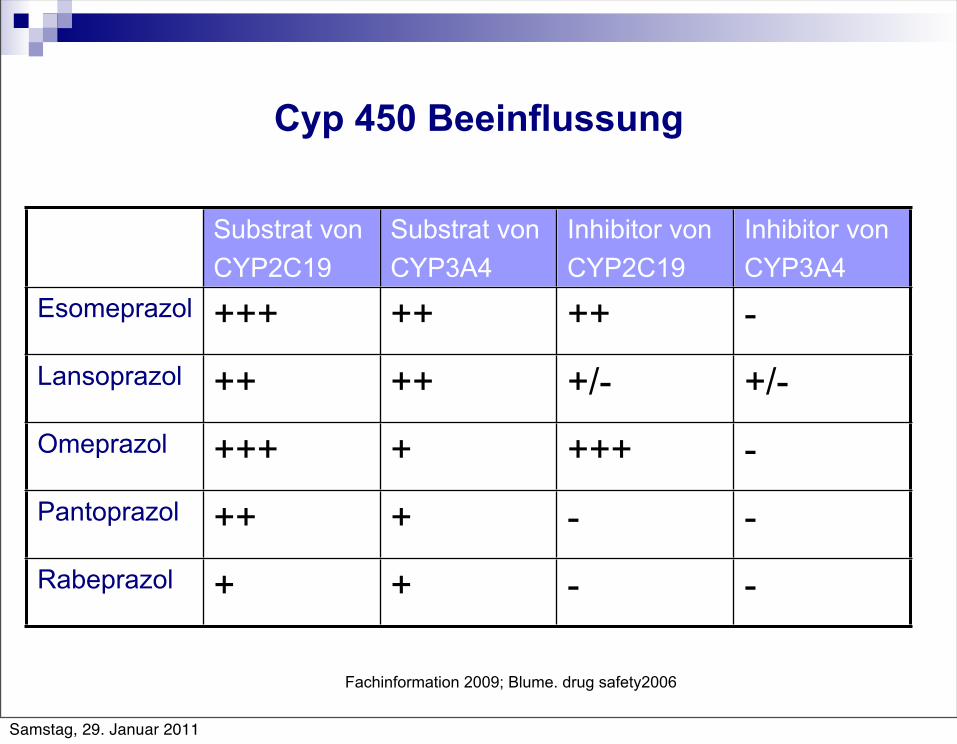
Cyp 450 Beeinflussung
Substrat vonCYP2C19
Substrat vonCYP3A4
Inhibitor vonCYP2C19
Inhibitor vonCYP3A4
Esomeprazol +++ ++ ++ -Lansoprazol ++ ++ +/- +/-Omeprazol +++ + +++ -Pantoprazol ++ + - -Rabeprazol + + - -
Fachinformation 2009; Blume. drug safety2006
Samstag, 29. Januar 2011
Empfehlung der FDA
Healthcare providers should continue to prescribe and patients should continue to take clopidogrel as directed, because clopidogrel has demonstrated benefits in preventing blood clots that could lead to a heart attack or stroke.
Healthcare providers should re-evaluate the need for starting or continuing treatment with a PPI, including Prilosec OTC, in patients taking clopidogrel.
Patients taking clopidogrel should consult with their healthcare provider if they are currently taking or considering taking a PPI, including Prilosec OTC.(January 26, 2009 - Early Communication about an Ongoing Safety Review – FDA www.fda.gov/medwatch/report.htm)
Samstag, 29. Januar 2011
Die Arzneimittelkommission der deutschen Ärzteschaft(AKdÄ) hat aufgrund der Studienergebnisse folgende vorläufigen Empfehlungen ausgesprochen:
● Eine routinemäßige Verordnung von Protonenpumpeninhibitoren bei Patienten, die Clopidogrel erhalten, sollte unterbleiben.
● Bei einer dualen Hemmung der Thrombozytenaggregation mit ASS und Clopidogrel wird eine begleitende PPI-Gabe empfohlen, da durch die gleichzeitige Einnahme von ASS und Clopidogrel das Risiko für eine gastroduodenale Blutung von 1,8 auf 7,1 erhöht wird.
● Um die Folgen der beschriebenen Interaktion zu vermeiden, sollte bei Indikation für die Gabe eines Protonenpumpeninhibitors Pantoprazol verordnet werden.
● Alternativ kommen H2-Rezeptorantagonisten (z.B. Ranitidin,Famotidin) zur Prophylaxe gastrointestinaler Komplikationen in Betracht.
Quelle:Arzneimittelkommission der deutschen Ärzteschaft: Drug Safety Mail 2009 vom 24. April 2009
Samstag, 29. Januar 2011
Bundesamt für Sicherheit im Gesundheitswesen 14.08.2009
Bitte beachten Sie eine mögliche WW zwischen Clopidogrel und PPIs oder Wirkstoffen die CYP 2C19 hemmen, was zu einer möglichen Verringerung der klinischen Aktivität von Clopidogrel führt.
Patienten sollen Plavix/Iscover weiterhin wie empfohlen einnehmen
PPIs und Substanzen die CYP 2C19 hemmen, sollten bei Patienten, die clopidogrelhaltige Arzneispezialitäten anwenden, vermieden werden, außer diese Kombination ist absolut notwendig. Wenn der Bedarf an einem gastroprotektiven Wirkstoff besteht sollte berücksichtigt werden, dass es keinen Hinweis dafür gibt, dass andere Wirkstoffe, die die Magensäure reduzieren, wie z.B. H2-Blocker oder Antacida, mit der thromozytenhemmenden Wirkung interagieren.
Samstag, 29. Januar 2011
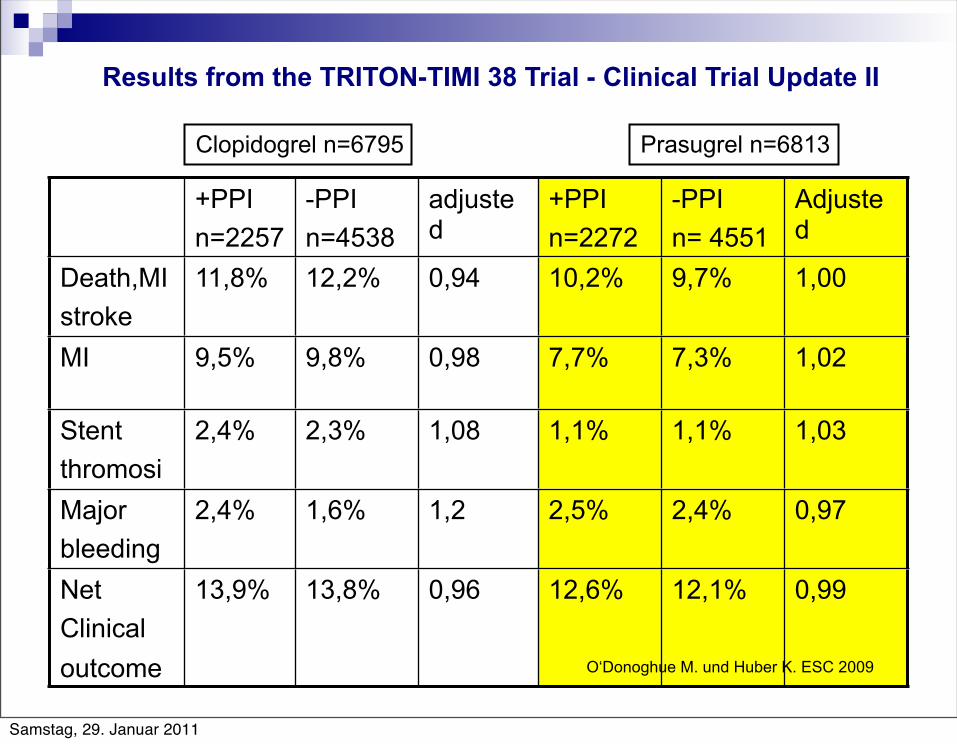
+PPIn=2257
-PPIn=4538
adjustedHR
+PPIn=2272
-PPIn= 4551
AdjustedHRDeath,MI
stroke11,8% 12,2% 0,94 10,2% 9,7% 1,00
MI 9,5% 9,8% 0,98 7,7% 7,3% 1,02
Stentthromosis
2,4% 2,3% 1,08 1,1% 1,1% 1,03
Majorbleeding
2,4% 1,6% 1,2 2,5% 2,4% 0,97
Net Clinicaloutcome
13,9% 13,8% 0,96 12,6% 12,1% 0,99
Clopidogrel n=6795 Prasugrel n=6813
O‘Donoghue M. und Huber K. ESC 2009
Results from the TRITON-TIMI 38 Trial - Clinical Trial Update II
Samstag, 29. Januar 2011
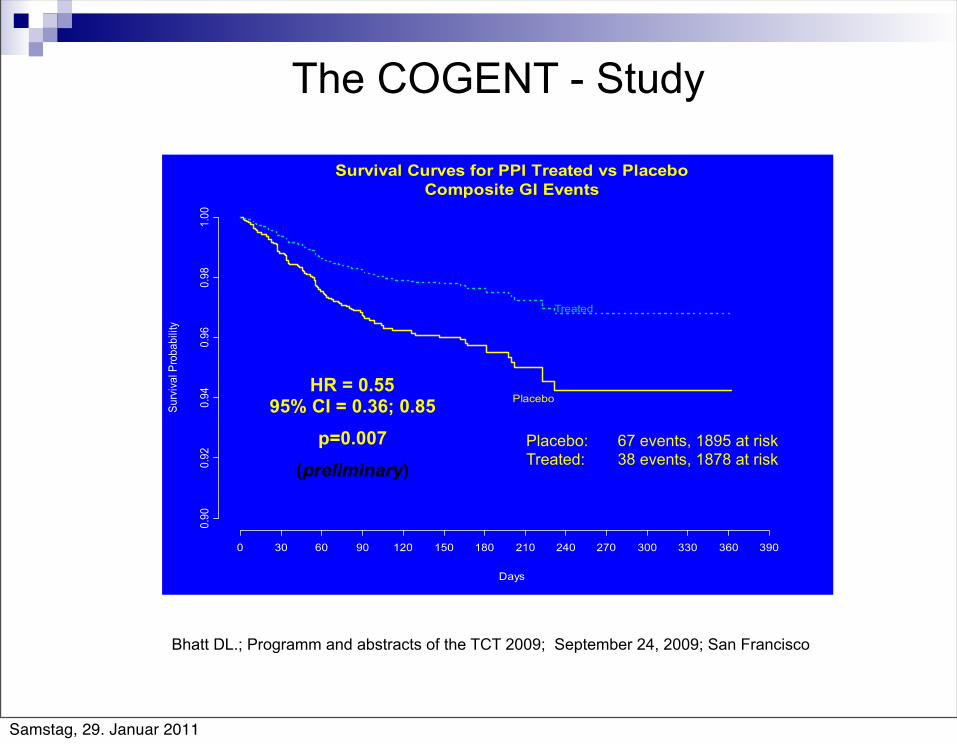
HR = 0.5595% CI = 0.36; 0.85
p=0.007(preliminary)
Placebo: 67 events, 1895 at riskTreated: 38 events, 1878 at risk
The COGENT - Study
Bhatt DL.; Programm and abstracts of the TCT 2009; September 24, 2009; San Francisco
Samstag, 29. Januar 2011
Mögliche Alternativen
H2 Blocker: Famotidin, Ranitidin 2x/tgl Misoprostol: 3-4x 200mcg/Tag Antacida:bis zu 4x/Tag nüchtern Sucralfat: 2-4x/Tag (ev.vor dem PPI) Unterlegen gegenüber PPI
Samstag, 29. Januar 2011
Duale Plättchenhemmung essentiell bei ACS und nach coronaren Stents Interaktion von Clopidogrel mit PPI gesichert Blutungsrisiko bei dualer Plättchenhemmung um 7-8 x erhöht PPIs: einzige gesicherte Prophylaxe einer (Rezidiv-) GI Blutung
Samstag, 29. Januar 2011
DGVS 09 2010
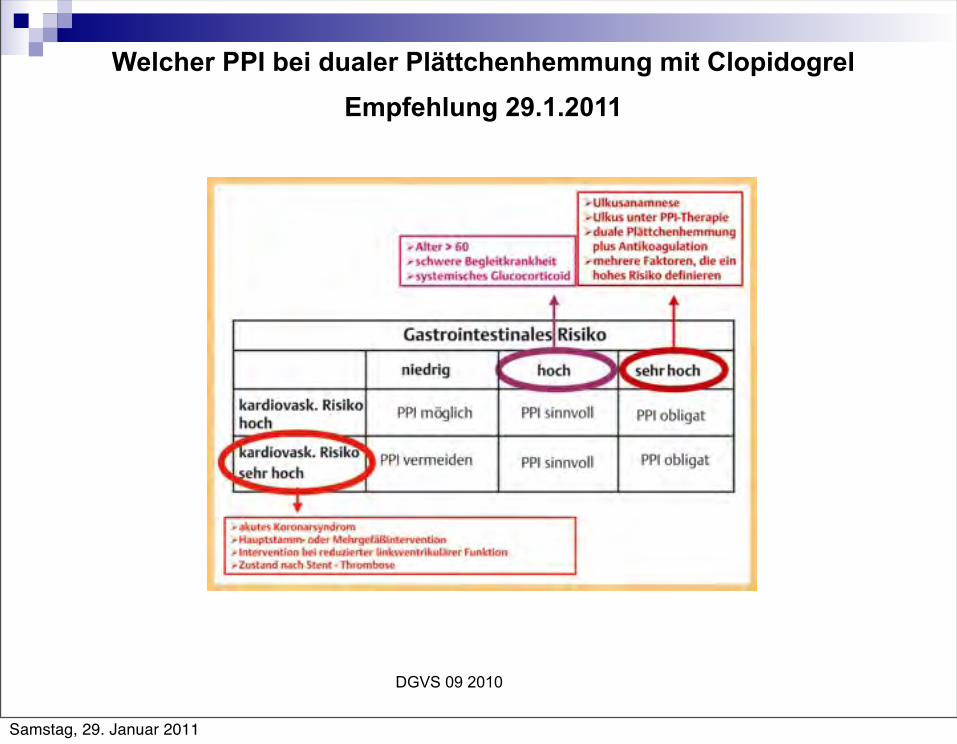
Empfehlung 29.1.2011Welcher PPI bei dualer Plättchenhemmung mit Clopidogrel
Samstag, 29. Januar 2011
DGVS 09 2010
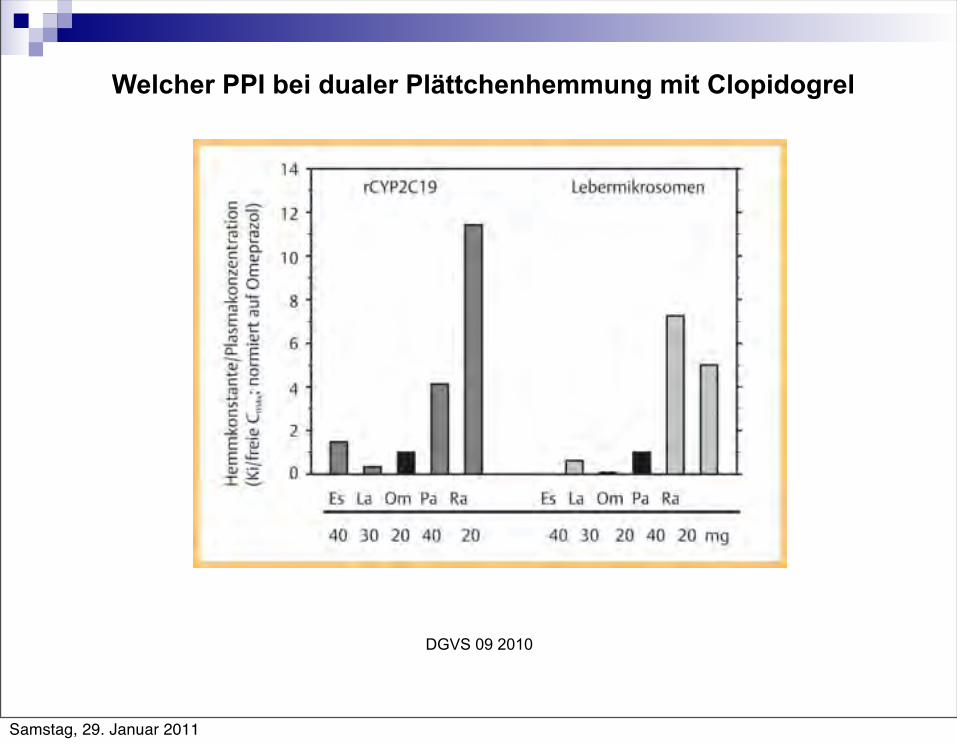
Welcher PPI bei dualer Plättchenhemmung mit Clopidogrel
Samstag, 29. Januar 2011
DGVS 09 2010
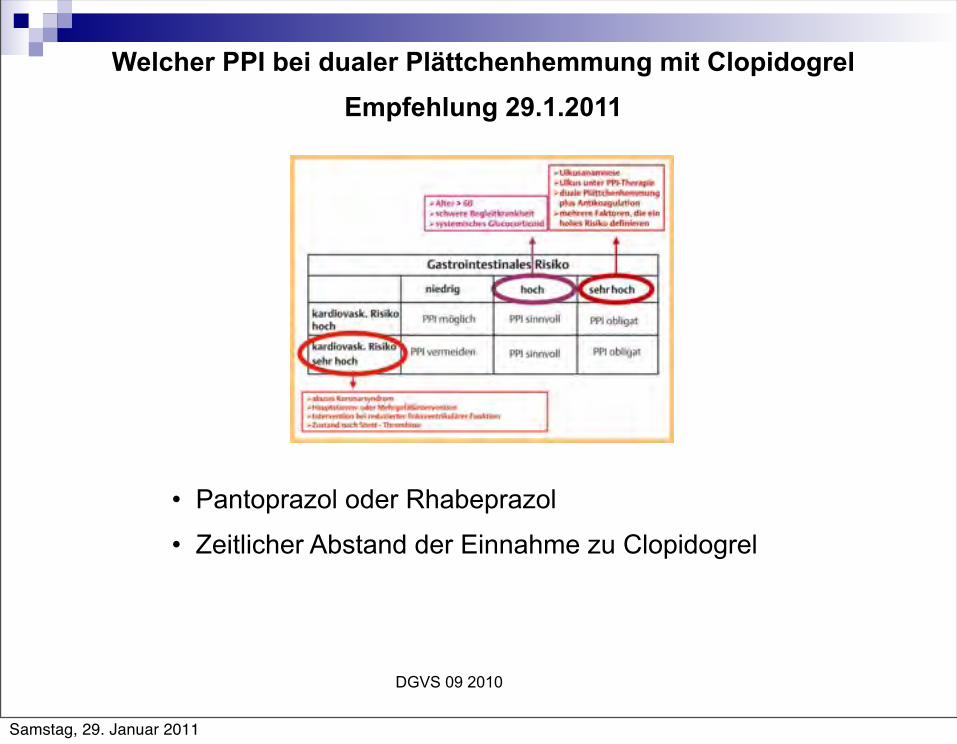
Empfehlung 29.1.2011Welcher PPI bei dualer Plättchenhemmung mit Clopidogrel
• Pantoprazol oder Rhabeprazol
• Zeitlicher Abstand der Einnahme zu Clopidogrel
Samstag, 29. Januar 2011
•PPI und Schwangerschaft
•PPI und rebound nach Langzeittherapie
•PPI und Asthma
•PPI und Dyspepsie
•PPI und Reisediarrhoe
•Welcher PPI?
...was noch zu sagen wäre
Samstag, 29. Januar 2011

Medline ® Abstract for Reference 32 of 'Overview and comparison of the proton pump inhibitors for the treatment of acid-related disorders' 32 TIDirect comparative trials of the efficacy of proton pump inhibitors in the management of gastro-oesophageal reflux disease and peptic ulcer disease. AUVakil N; Fennerty MB SOAliment Pharmacol Ther 2003 Sep 15;18(6):559-68. BACKGROUND: Five proton pump inhibitors are now available for use in North America. Claims of differences in the clinical efficacy of different strengths and/or agents have been made. AIM: To identify any consistent evidence of differences in outcomes between agents or doses within this class of drugs. METHODS: A search of the medical literature was performed in two electronic databases, and randomized controlled trials of higher quality were included in the assessment. RESULTS AND CONCLUSIONS: Thirty-two trials met our criteria. No convincing data were found to indicate that low doses of proton pump inhibitors are as effective as standard doses of proton pump inhibitors in the healing of erosive oesophagitis or in the relief of symptoms of gastro-oesophageal reflux disease; however, they may be as effective as maintenance therapy for gastro-oesophageal reflux disease and peptic ulcer disease. Differences were found between the standard doses of proton pump inhibitors with regard to the onset of symptom relief in gastro-oesophageal reflux disease (lansoprazole was faster than omeprazole, and esomeprazole was faster than both lansoprazole and omeprazole) and the healing of oesophagitis (esomeprazole was superior to both omeprazole and lansoprazole). Despite these differences, there are as yet insufficient data to establish the superiority of any one agent over all others across all disease states treated with these agents. ADDepartments of Medicine, Sections of Gastroenterology, University of Wisconsin, Milwaukee, WI, USA. PMID12969082
Samstag, 29. Januar 2011
Medline ® Abstract for Reference 32 of 'Overview and comparison of the proton pump inhibitors for the treatment of acid-related disorders' 32 TIDirect comparative trials of the efficacy of proton pump inhibitors in the management of gastro-oesophageal reflux disease and peptic ulcer disease. AUVakil N; Fennerty MB SOAliment Pharmacol Ther 2003 Sep 15;18(6):559-68. BACKGROUND: Five proton pump inhibitors are now available for use in North America. Claims of differences in the clinical efficacy of different strengths and/or agents have been made. AIM: To identify any consistent evidence of differences in outcomes between agents or doses within this class of drugs. METHODS: A search of the medical literature was performed in two electronic databases, and randomized controlled trials of higher quality were included in the assessment. RESULTS AND CONCLUSIONS: Thirty-two trials met our criteria. No convincing data were found to indicate that low doses of proton pump inhibitors are as effective as standard doses of proton pump inhibitors in the healing of erosive oesophagitis or in the relief of symptoms of gastro-oesophageal reflux disease; however, they may be as effective as maintenance therapy for gastro-oesophageal reflux disease and peptic ulcer disease. Differences were found between the standard doses of proton pump inhibitors with regard to the onset of symptom relief in gastro-oesophageal reflux disease (lansoprazole was faster than omeprazole, and esomeprazole was faster than both lansoprazole and omeprazole) and the healing of oesophagitis (esomeprazole was superior to both omeprazole and lansoprazole). Despite these differences, there are as yet insufficient data to establish the superiority of any one agent over all others across all disease states treated with these agents. ADDepartments of Medicine, Sections of Gastroenterology, University of Wisconsin, Milwaukee, WI, USA. PMID12969082
Egal welcher PPI – Alle gleich gut
Samstag, 29. Januar 2011
Take Home Message
Wichtige Substanzgruppe
Richtige Anwendung Leitlinien Dosierung Applikationszeitpunkt Therapiedauer / no switch
NW und Interaktionen: Ph - Erhöhung: Resorptionsstörungen CYP 2C19 Hemmung: Plavix, Marcoumar,Diazepam P-GP Interaktion
Samstag, 29. Januar 2011
Samstag, 29. Januar 2011