Embed Size (px)
Citation preview

Schmerzkurs 2014
Bad Kleinkirchheim Michael Ausserwinkler

Gelenksschmerzen

Weichteilschmerzen


DIFFERENTIALDIAGNOSEN ENTZÜNDLICH RHEUMATISCHER ERKRANKUNGEN
• Rheumatoide Arthritis (1-2%)
• Arthritis psoriatica (0.5-1%)
• Systemischer Lupus
erythematodes • Mischkollagenose • Systemsklerose • CREST-Syndrom • Sjögren Syndrom • Dermato- / Myositis • Anti-Phospholipid-Ak-
Syndrom
• Vaskulitiden (PMR, M. Wegener, PAN)
• Seronegative Spondarthritiden - Morbus Bechterew (-1%)
• Reaktive Arthritis • Virus assoziierte
Arthritiden
• Borreliose • CEDs (Ileitis terminalis, Colitis ulcerosa)
• Paraneoplasien

Diagnostik in Reihenfolge und Wertigkeit
• Anamnese/Krankheitsgeschichte • Untersuchungsbefund • Laborbefunde • Röntgenbefunde • Skelettszintigraphie • Magnetresonanz
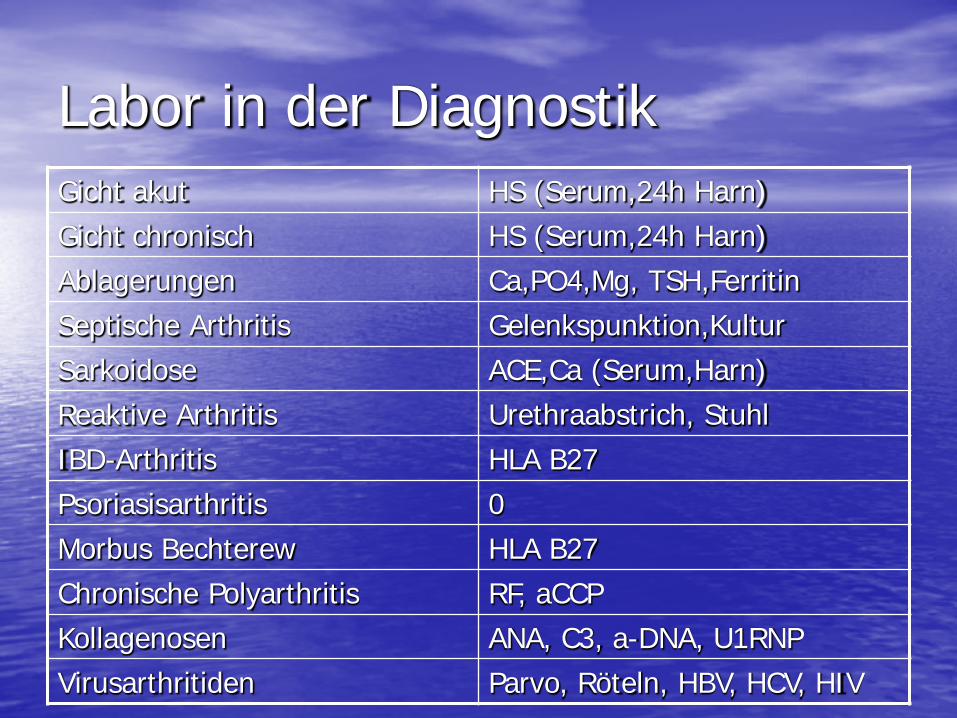
Labor in der Diagnostik Gicht akut HS (Serum,24h Harn) Gicht chronisch HS (Serum,24h Harn) Ablagerungen Ca,PO4,Mg, TSH,Ferritin Septische Arthritis Gelenkspunktion,Kultur Sarkoidose ACE,Ca (Serum,Harn) Reaktive Arthritis Urethraabstrich, Stuhl IBD-Arthritis HLA B27 Psoriasisarthritis 0 Morbus Bechterew HLA B27 Chronische Polyarthritis RF, aCCP Kollagenosen ANA, C3, a-DNA, U1RNP Virusarthritiden Parvo, Röteln, HBV, HCV, HIV

DIAGNOSEBAUM LABOR
•BSG
•CrP
•Elpho
•Fe/Ferritin
•etc
•RF
•a-ccP
•HLA B27
•Borrelien
•ANA, dsDNS
•ANCA
•(Parvo B29)
Bildgebung, etc.
ENA



MRT
Szintigraphie

RA, PsA-Komorbiditäten
• Bei der Erstdiagnose leiden 72 % an einer und 50 % an zwei Komorbiditäten
• Je mehr Komorbiditäten umso schlechter das 3-Jahres-Outcome
• Frühere Invalidisierung

VH-Flimmern 60% häufiger bei RA

Kortisontherapie bei rheumatoider Arthritis
• National database of the German Collaborative Arthritis Centers 2009
• 7337 Patienten • 56 % nehmen Kortison • Geringere Dosis

Kortison in UK
• Zunahme der Kortisonkonsumenten • + 34% in den letzten 20a
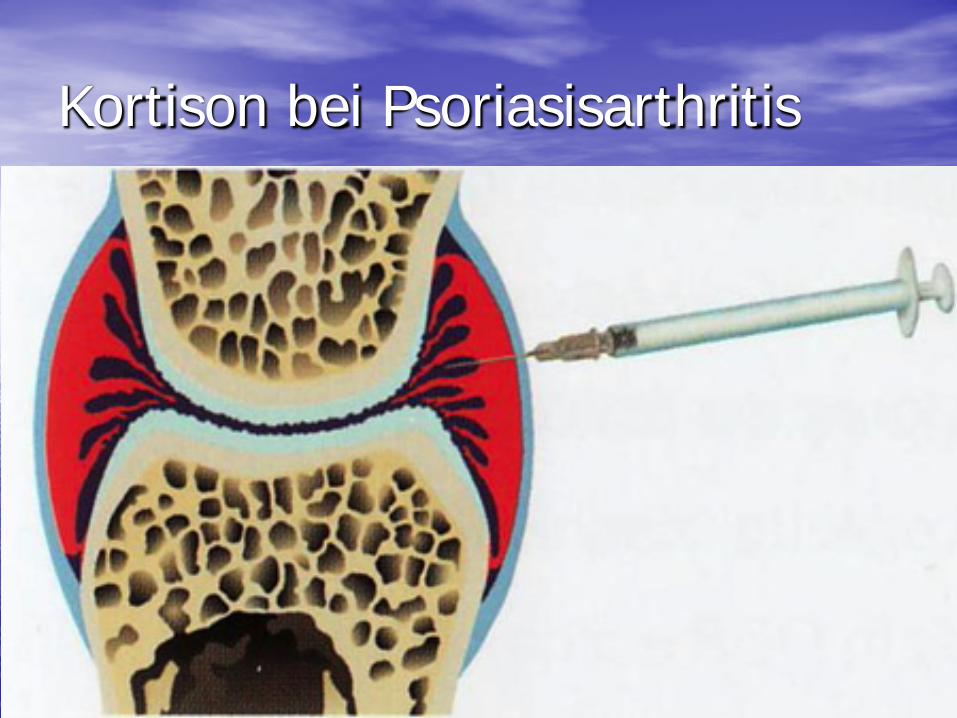
Kortison bei Psoriasisarthritis

NSAR



DMARD Krankheitsmodifizierende
Therapie
Basistherapie

EULAR- guidelines, 2007
• ELAR recommendations for the management of early arthritis: report of a task force of the European Standing Committee for International Clinical Studies Includin Therapeutics (ESCISIT)
• B. Combe et al., AG Smolen
• R1: Patients with arthritis of more than one joint should be referred to and seen by a rheumatologist, ideally within six weeks after the onset of symptoms
• R2: Clinical examinsation is the method of choice for detecting arthritis. … • R3: Exclusion of other diseases than RA requires careful history taking and clinical examination, and ought to
include at least the following laboratory tests: complete blood cell count, urinary analysis, transaminases, and antinuclear antibodies
• R4: the following factors predicting persistent and erosive disease should be measured: Number of swollen and tender joints, ESR/CrP, level of rheumatoid factorand anti-ccP-antibodies, and radiographic erosions
• R5: Patients at risk … should be started with DMARDs as early as possible even if they do not yet fulfill establisher classification criteria …
• R6: Patient information concerning disease and ist treatment and outcome is important. … • R7: NSAIDs have to be considered in symptomatic patients after evaluation of gastrointestinal, renal, and
cardiovascular status • R8: systemic steroids reduce pain and swelling and should be considered as a (mainly temporary) adjunct to the
DMARD strategy. Intraarticular steroids should be considered for the relief of local symptoms of inflammation. • R9:Among the DMARDs, methotrexate ist considered the anchor drug and should be used first in patients at risk
of developping persistent disease. • R10: The main goal of DMARD treatment ist to achieve remission. Regular monitoring of disease activity and
adverse events should guide decisions on choice and changes in treatment strategies (DMARDs including biologic agents)
• AnnRheumDis 2007; 66:34-45

5. Bei Patienten mit einem Risiko für die Entwicklung einer persistierenden und/oder erosiven Erkrankung sollten so früh wie möglich eine DMARD-Therapie begonnen werden, auch wenn die Patienten die ACR-Kriterien nicht erfüllen (Kategorie III)
Combe et al., Ann Rheum Dis 66:34, 2007
EULAR- guidelines, 2007

BASISTHERAPIE - KLASSISCH
• Methotrexat • Leflunomid • Sulfasalazin • Malariamittel (z. B. Chloroquin, Hydroxychloroquin) • Goldsalze (zur Injektion oder oral) • Azathioprin • etc. (selten)
© Welcker, 2006

Biologics

Zulassungen der TNF-Blocker
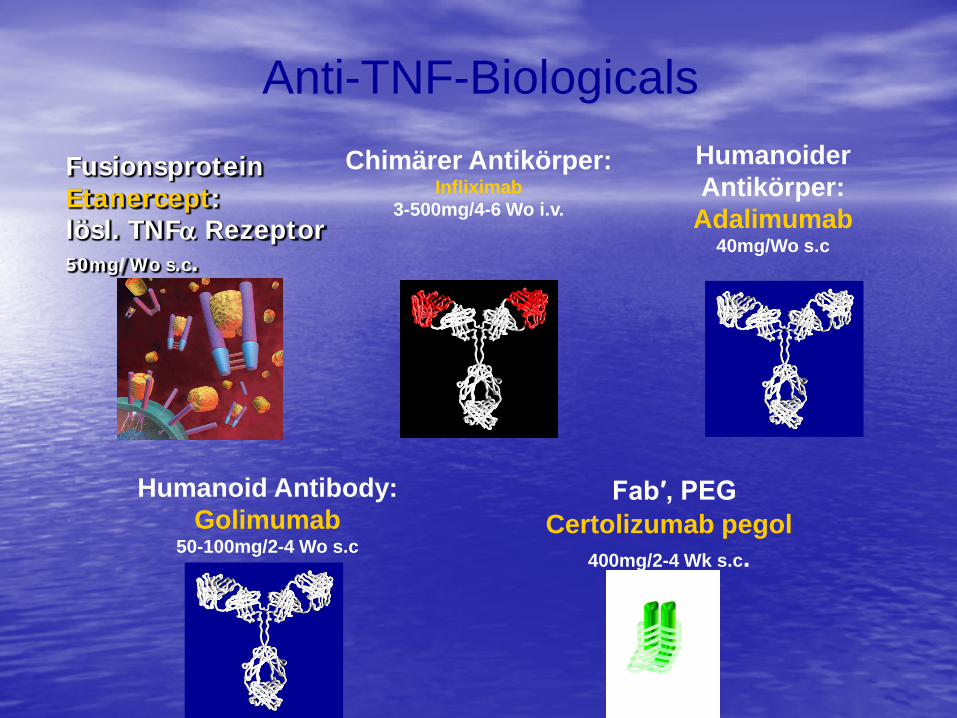
Fusionsprotein Etanercept: lösl. TNFα Rezeptor 50mg/Wo s.c.
Chimärer Antikörper: Infliximab
3-500mg/4-6 Wo i.v.
Humanoider Antikörper:
Adalimumab 40mg/Wo s.c
Anti-TNF-Biologicals
Fab′, PEG Certolizumab pegol
400mg/2-4 Wk s.c.
Humanoid Antibody: Golimumab
50-100mg/2-4 Wo s.c
weitere Biologics

weitere Biologics
• B-Zell-Antikörper – Rituximab (Mabthera)
• T-Zell-Antikörper – Abatacept (Orencia)
• Anti-Zytokine – Anti-IL6-Rez.Antikörper (RoActemra)
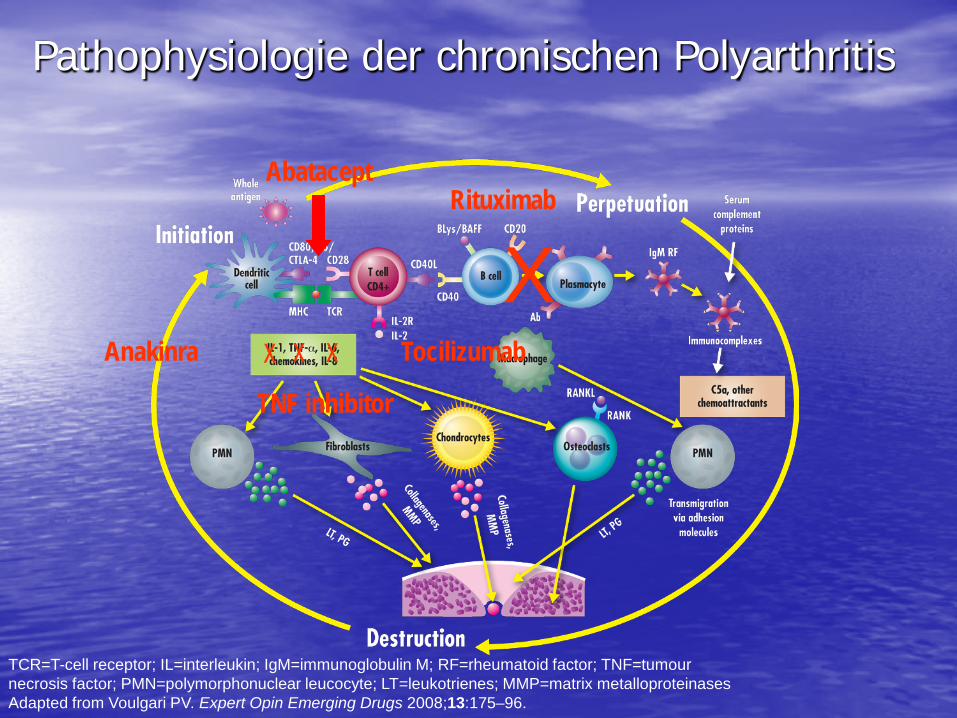
TCR=T-cell receptor; IL=interleukin; IgM=immunoglobulin M; RF=rheumatoid factor; TNF=tumour necrosis factor; PMN=polymorphonuclear leucocyte; LT=leukotrienes; MMP=matrix metalloproteinases Adapted from Voulgari PV. Expert Opin Emerging Drugs 2008;13:175–96.
TNF inhibitor
X Anakinra X
Rituximab
X Abatacept
X Tocilizumab
Pathophysiologie der chronischen Polyarthritis



Psoriasisarthritis Zulassung September 2013

Stelara versus Enbrel
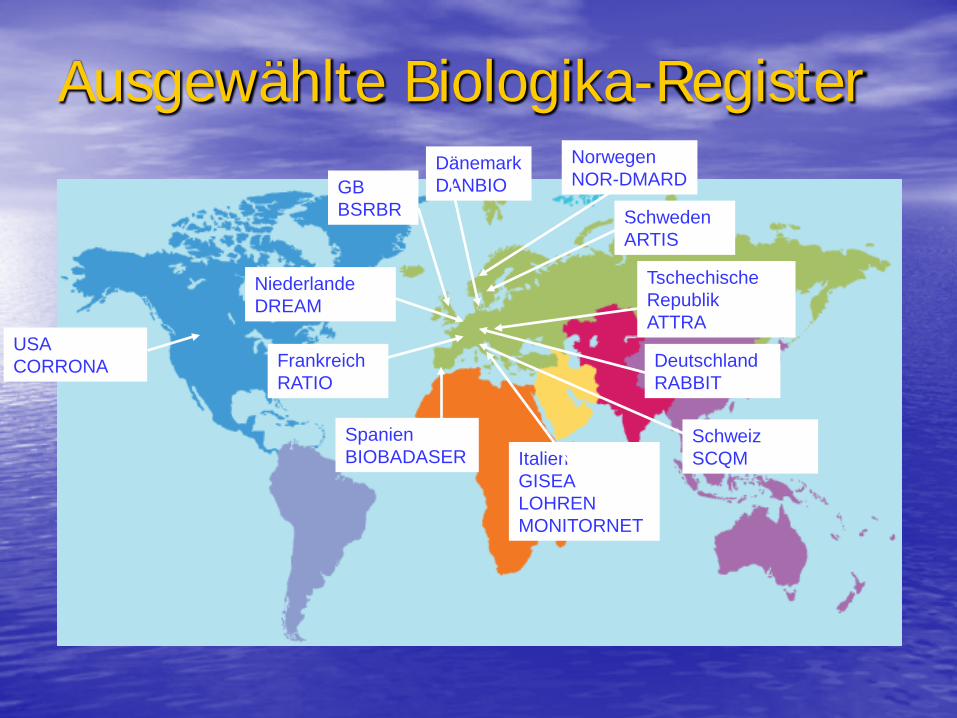
Ausgewählte Biologika-Register Dänemark DANBIO GB
BSRBR
Frankreich RATIO
Deutschland RABBIT
Niederlande DREAM
Italien GISEA LOHREN MONITORNET
Spanien BIOBADASER
Schweden ARTIS
Norwegen NOR-DMARD
Tschechische Republik ATTRA
Schweiz SCQM
USA CORRONA

Nächtliche Schmerzen
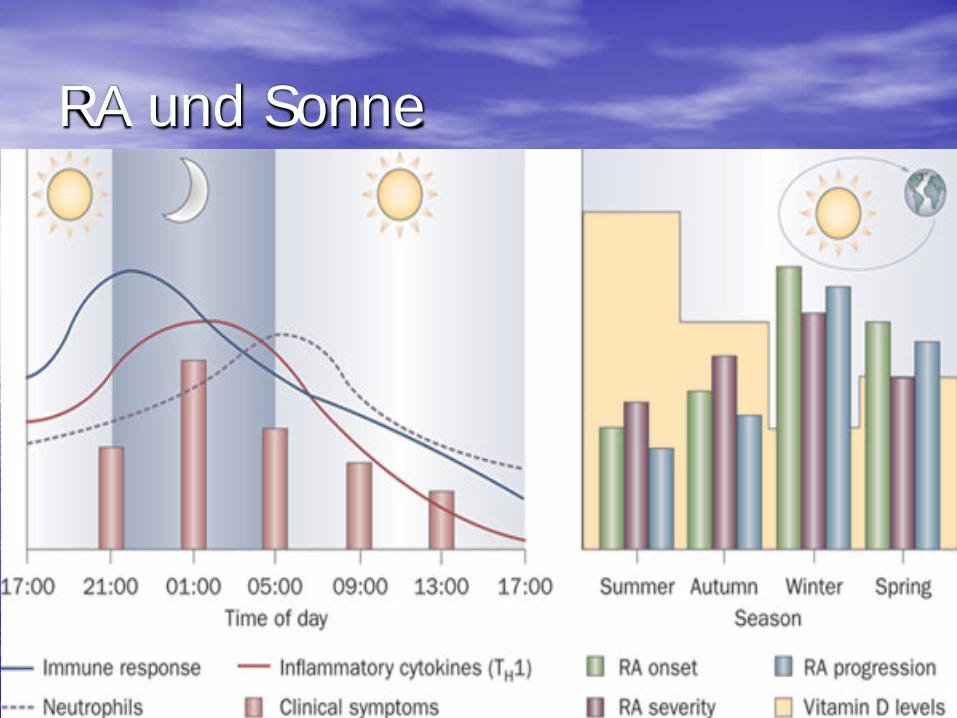
RA und Sonne



Vitamin D
• Oleovit D Tropfen
• Bei Nierenkranken: Rocaltrol, Etalpha

Hippocrates
• Lass die Nahrung deine Medizin sein und die Medizin deine Nahrung

Spondylarthritis Therapie
Altes Ägypten : Zum Erweichen Natron, Bohnen, Behenöl,
Nilpferdöl, Krokodilöl, Öl des Silurusfisches, Öl der Meeräsche, Weihrauch, süße Myme, Honig.
John Barns,
London 2003


Fasten
• Erhöht die die körpereigene Glukokortikoidproduktion
• Erhöht die Endorphinspiegel
• Nur bei übergewichtigen Patienten

Fasten oder mediterane Kost bei Patienten mit RA und FMS Michalsen A. et al. BMC Complement Altern Med 2005 Dec 22;5:22
• Mediterane Kost • N=22 • Alter 50.9a
• 8 Tage Fasten • N=30 • Allter 53.7

Fasten oder mediterane Kost
Vegetarische Kost für Patienten mit rheumatoider Arthritis
• Abfall der Thrombocyten • Weniger Leukocyten • Weniger Calprotectin • Geringere Konzentration des IgG und IgM
Rheumafaktors
Changes in laboratory variables in RA during a trial of fasting and one year vegetarian diet.
Kjeldsen-Kragh J. et al. Scand J Rheumatol.1995;24(2):85-93

Gluten freie Kost bei rheumatoider Arthritis Elkan AC et al. Arthritis Res Ther 2008
• Glutenfrei vegan n=38 • Mittleres Alter 50a • BMI tiefer • Cholesterin tiefer • LDL tiefer • oxLDL tiefer
• Ausgewogene Kost n=28
• Mittleres Alter 50,8a

Vorteile der vegetarischen Kost
• Weinger gesättigte Fettsäuren • Weniger Cholesterin • Mehr Kohlehydrate • Mehr Faserstoffe • Mehr Magnesium • Mehr Folsäure • Mehr Vitamin A,C,E

Nachteile der vegetarischen Kost
• Weniger Proteine • Weniger Eisen • Weniger Zink • Weniger Kalzium • Weniger Vitamin B 12 • Weniger Jod
Abhängig vom sozioökonomischen Status

Kaffee
• Bis 3 Tassen unbedenklich

Arthrose - Osteoarthritis

Fettgewebe und Entzündung

Osteoarthritis
• Erwärmung positiv

Osteoarthritis
• Kühle negativ

Erwärmende Nahrungsmittel
• Ingwer • Chili

Soja • IIsoflavone (Phytoöstrogene) Genistein Diazein Biochanin
Knoblauch
• Enthält Diallyl Disulfid
• Reduziert die Expression von matrixdegradierenden Proteasen

Zwillingsstudie
• 1086 weiblich ( 46-77a ) • Röntgenbilder • Matrix-degradierende Proteasen
Dietary garlic and hip osteoarthritis. Frances MK Williams, et al. BMC Musculoskelet Disord 2010;11:280
Ernährung und Hüftosteoarthritis
• Positiver Einfluss von Obst und Gemüse
• Nicht-Citrus-Früchte (p=0,015) und Alliums hatten den größten positiven Effekt

Gicht bestätigte Verursacher

Gicht-jahrelang verdächtigt, jetzt freigesprochen

Allgemeine Empfehlungen
• Langsamer Abbau von Übergewicht • Täglich Vollkornprodukte, Obst, Gemüse • Milchprodukte • 2x pro Woche Fisch • Selten Fleisch • Wenig tierische Fette • Vitamin D, C, E