Embed Size (px)
Citation preview
27.07.2017 - 13:30 – 13:50
Hepatitis B/D: Wofür braucht der ÖGD ein Hepatologisches Labor
an einer Universitätsklinik?
Heinz Zoller
Universitätsklinik für Innere Medizin I
Leiter Prof. Herbert Tilg
Medizinische Universität - Tirol Kliniken
Warum Hepatitis B?
JAMA. 1965 Feb 15;191:541-6. A "NEW" ANTIGEN IN LEUKEMIA SERA. BLUMBERG BS, ALTER HJ, VISNICH S.
1960: ca. 30 % der Bluttransfusionen Transfusionsreaktion (Fieber, Schüttelfrost, Ikterus,…) 1965: Erweiterung der Blutgruppenserologie durch Immunologische Untersuchungen 1965: Identifikation einer Kreuzreaktion zwischen Hämophilie Patienten aus New York und Aboriginee Häufung des neuen ‚red Anitgens‘ ‚Australia Antigen‘ ‚HBs Antigen‘ bei Trisomie 21 Patienten, Hämophilen & Leukämiepatienten (10 % vs. 0,1%) 1968: Elektronenmikroskopische Identifikation des Dane Partikels & Beschreibung des Hepatitis B Virus

Electron Micrograph of HBV. Both from Linda Stannard, Department of Medical Microbiology, University of Cape Town. http://web.uct.ac.za/depts/mmi/stannard/hepb.html.
Hepatitis B - Übertragungswege
MTC
IVD
MSM BTx
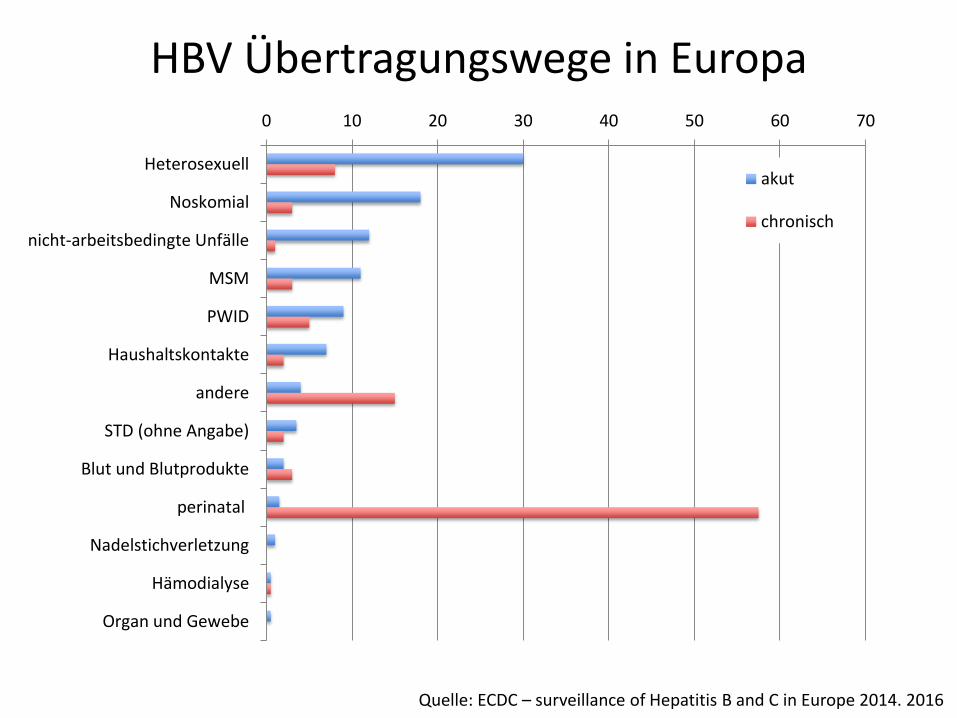
HBV Übertragungswege in Europa 0 10 20 30 40 50 60 70
Heterosexuell
Noskomial
nicht-arbeitsbedingte Unfälle
MSM
PWID
Haushaltskontakte
andere
STD (ohne Angabe)
Blut und Blutprodukte
perinatal
Nadelstichverletzung
Hämodialyse
Organ und Gewebe
akut
chronisch
Quelle: ECDC – surveillance of Hepatitis B and C in Europe 2014. 2016
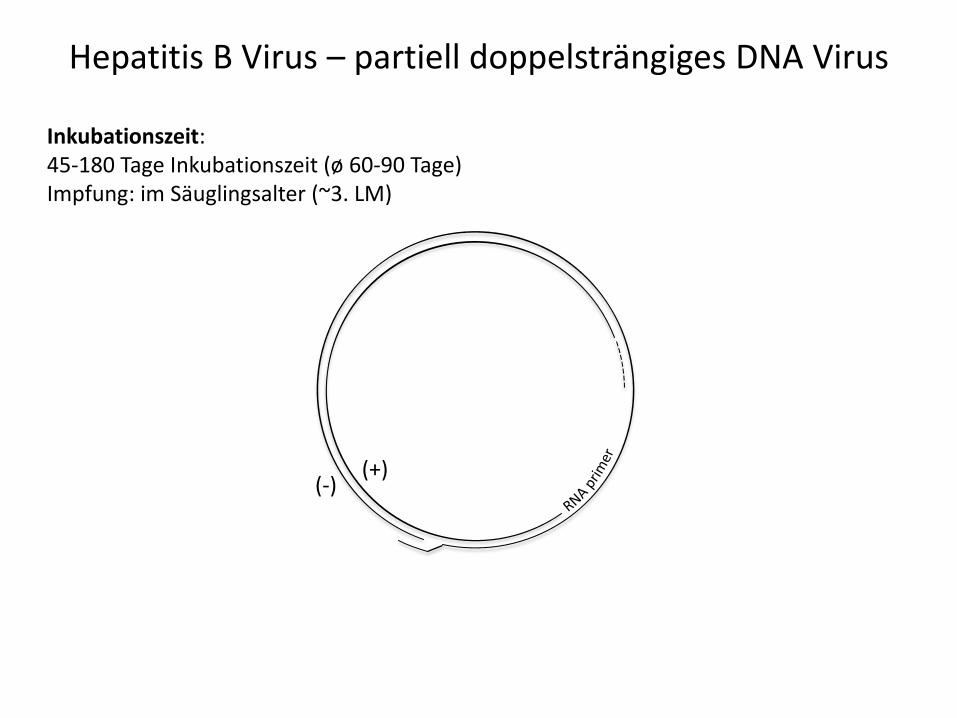
Hepatitis B Virus – partiell doppelsträngiges DNA Virus
(+) (-)
Inkubationszeit: 45-180 Tage Inkubationszeit (ø 60-90 Tage) Impfung: im Säuglingsalter (~3. LM)
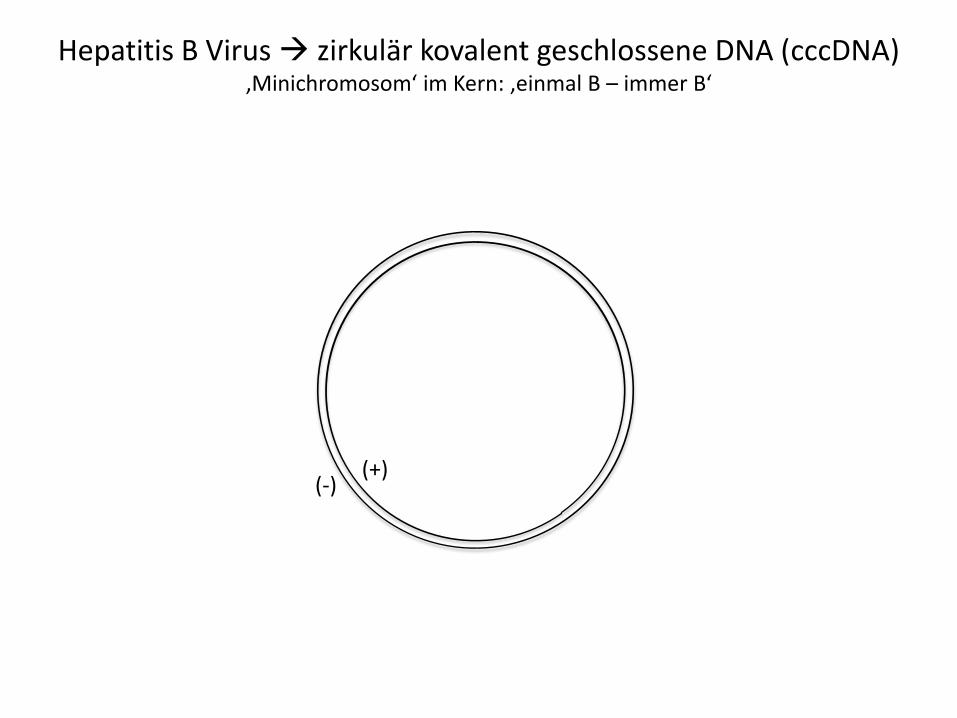
Hepatitis B Virus zirkulär kovalent geschlossene DNA (cccDNA) ‚Minichromosom‘ im Kern: ‚einmal B – immer B‘
(+) (-)
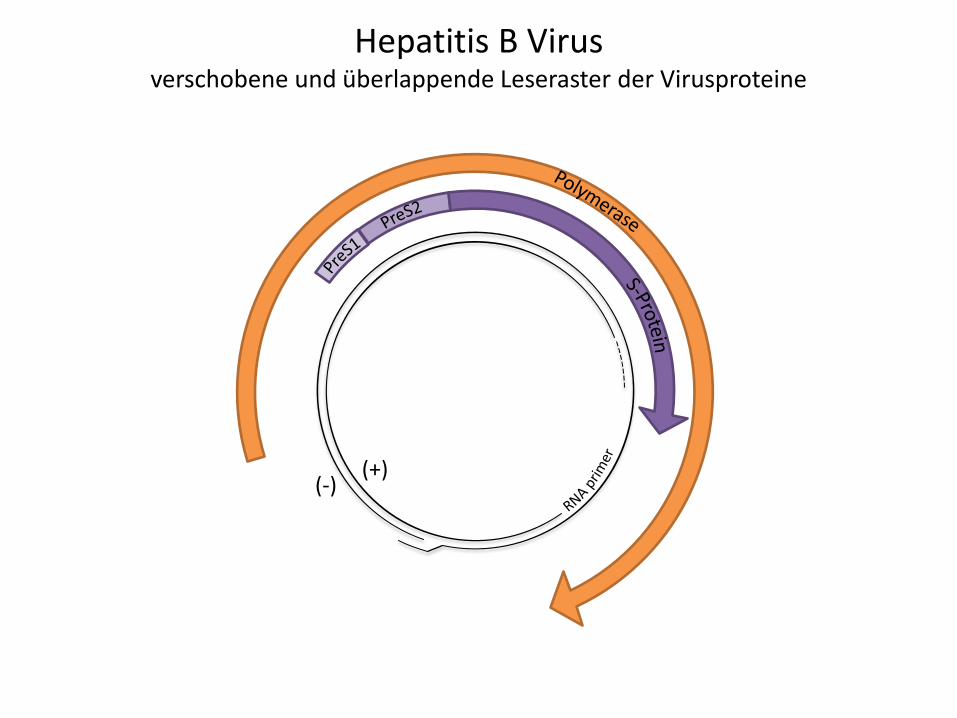
Hepatitis B Virus verschobene und überlappende Leseraster der Virusproteine
(+) (-)
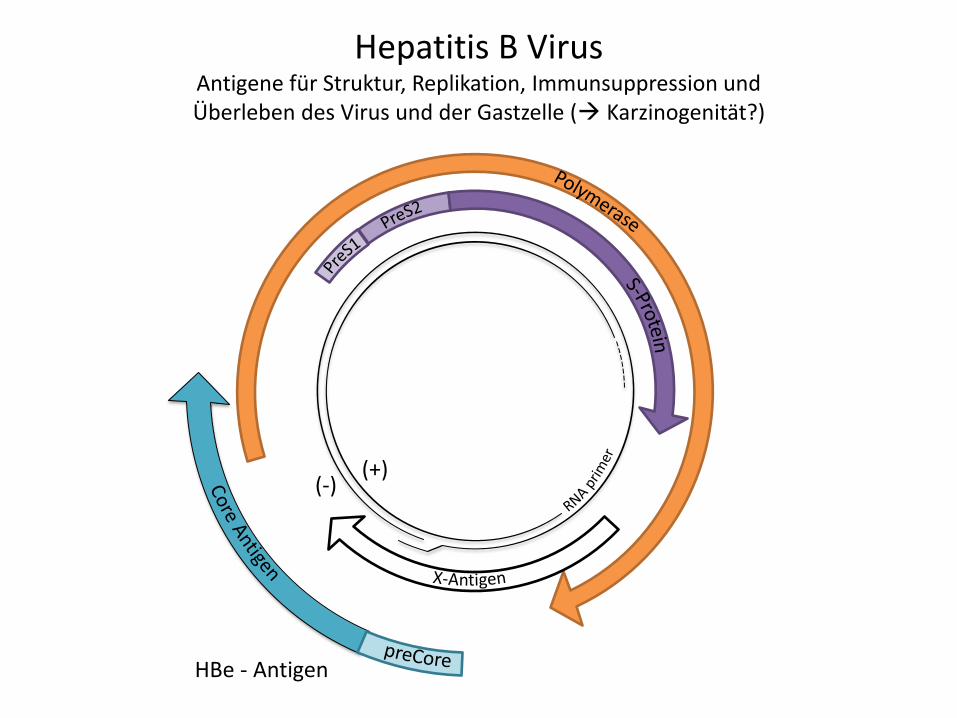
Hepatitis B Virus Antigene für Struktur, Replikation, Immunsuppression und Überleben des Virus und der Gastzelle ( Karzinogenität?)
(+) (-)
HBe - Antigen
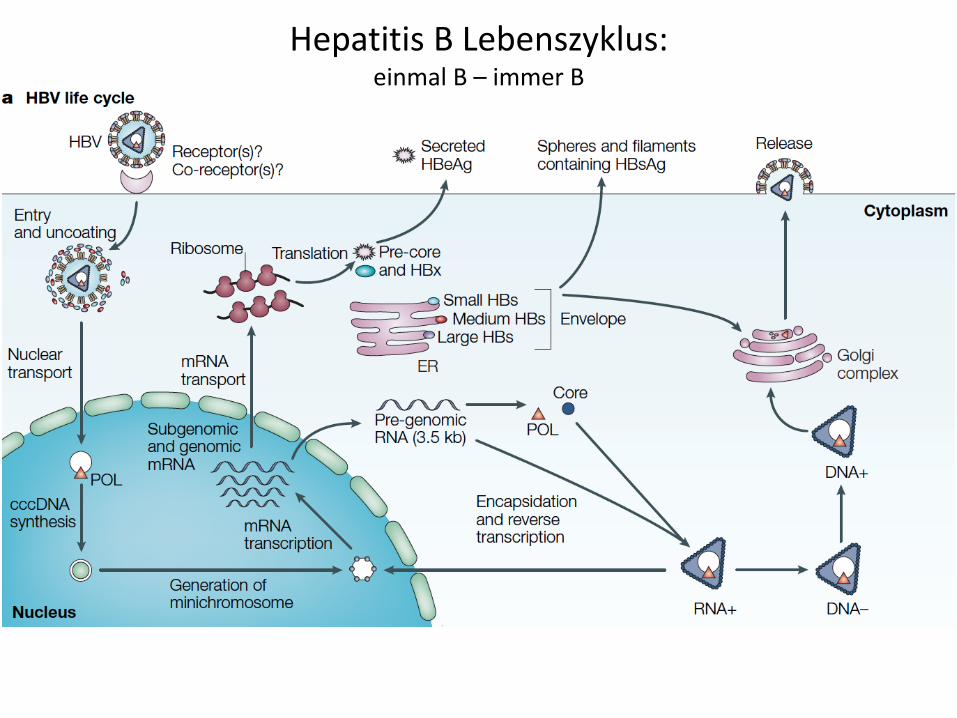
Hepatitis B Lebenszyklus: einmal B – immer B
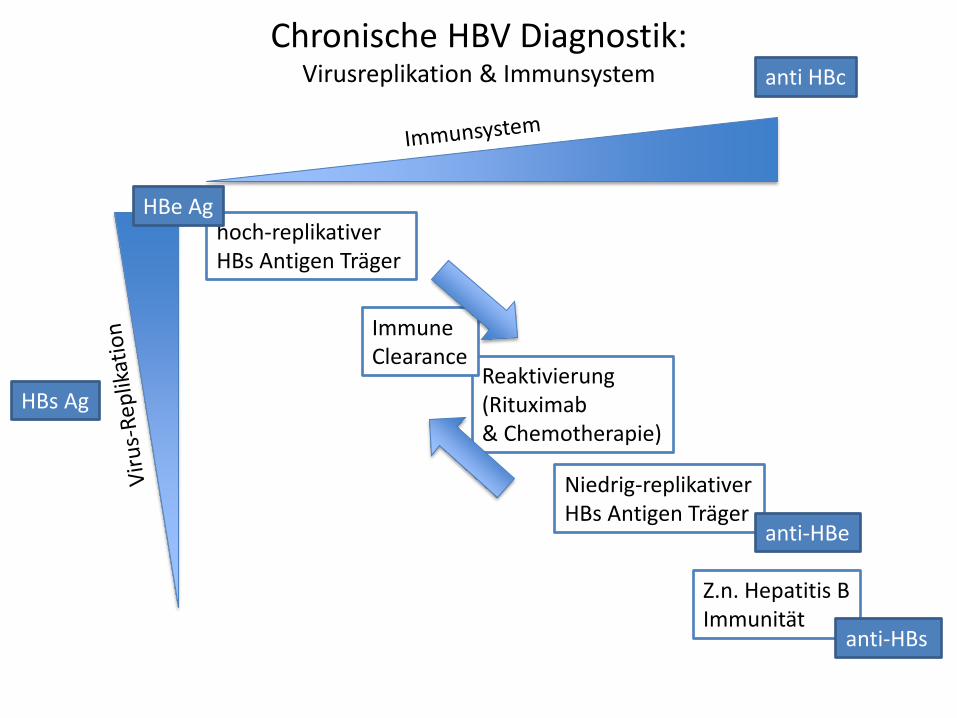
Niedrig-replikativer HBs Antigen Träger
hoch-replikativer HBs Antigen Träger
Reaktivierung (Rituximab & Chemotherapie)
Immune Clearance
Z.n. Hepatitis B Immunität
Chronische HBV Diagnostik: Virusreplikation & Immunsystem anti HBc
HBs Ag
HBe Ag
anti-HBs
anti-HBe
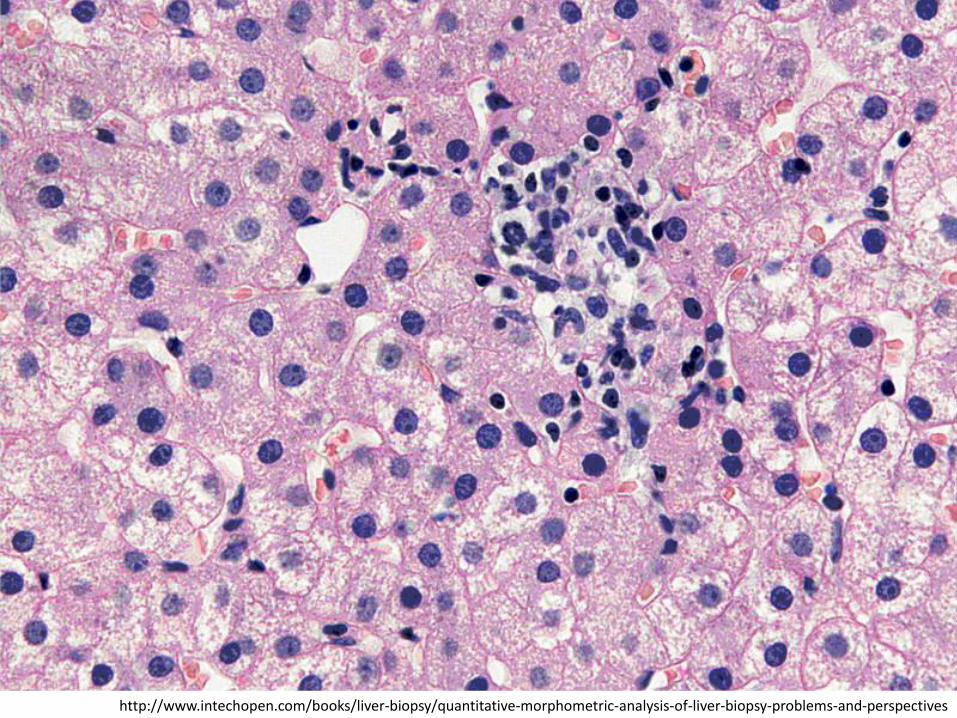
http://www.intechopen.com/books/liver-biopsy/quantitative-morphometric-analysis-of-liver-biopsy-problems-and-perspectives
http://www.ijpmonline.org/viewimage.asp?img=IndianJPatholMicrobiol_2011_54_2_355_79972_f1.jpg
INFEKTION ≠ KRANKHEIT
Wofür braucht der ÖGD ein Hepatologisches Labor an einer Universitätsklinik?
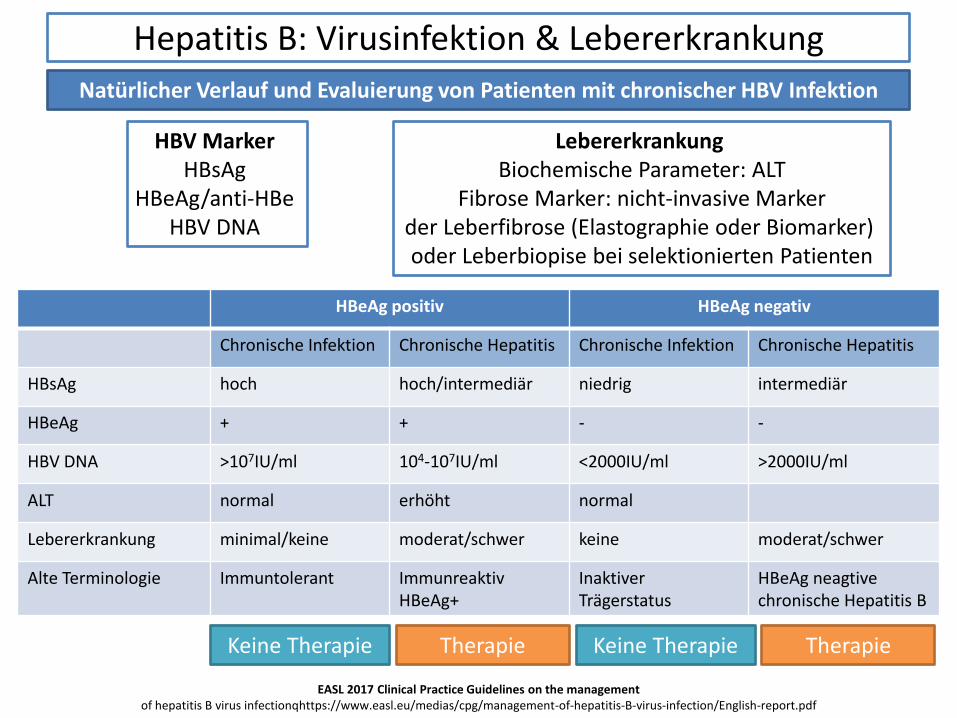
Hepatitis B: Virusinfektion & Lebererkrankung
Natürlicher Verlauf und Evaluierung von Patienten mit chronischer HBV Infektion
HBV Marker HBsAg
HBeAg/anti-HBe HBV DNA
Lebererkrankung Biochemische Parameter: ALT
Fibrose Marker: nicht-invasive Marker der Leberfibrose (Elastographie oder Biomarker) oder Leberbiopise bei selektionierten Patienten
HBeAg positiv HBeAg negativ
Chronische Infektion Chronische Hepatitis Chronische Infektion Chronische Hepatitis
HBsAg hoch hoch/intermediär niedrig intermediär
HBeAg + + - -
HBV DNA >107IU/ml 104-107IU/ml <2000IU/ml >2000IU/ml
ALT normal erhöht normal
Lebererkrankung minimal/keine moderat/schwer keine moderat/schwer
Alte Terminologie Immuntolerant Immunreaktiv HBeAg+
Inaktiver Trägerstatus
HBeAg neagtive chronische Hepatitis B
EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infectionqhttps://www.easl.eu/medias/cpg/management-of-hepatitis-B-virus-infection/English-report.pdf
Keine Therapie Therapie Keine Therapie Therapie
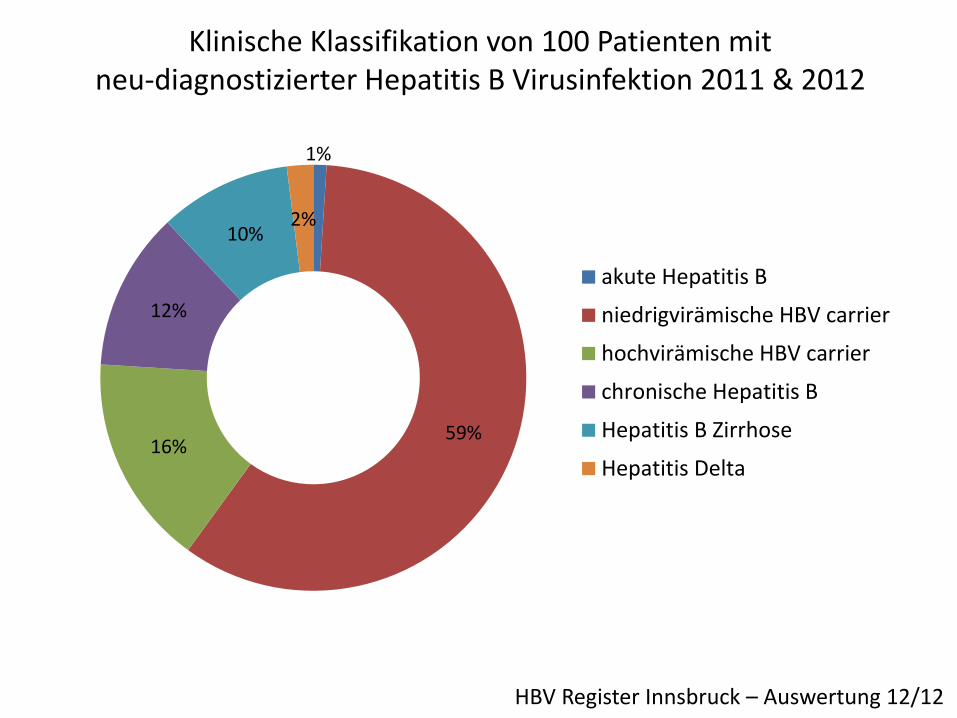
Klinische Klassifikation von 100 Patienten mit neu-diagnostizierter Hepatitis B Virusinfektion 2011 & 2012
1%
59% 16%
12%
10% 2%
akute Hepatitis B
niedrigvirämische HBV carrier
hochvirämische HBV carrier
chronische Hepatitis B
Hepatitis B Zirrhose
Hepatitis Delta
HBV Register Innsbruck – Auswertung 12/12
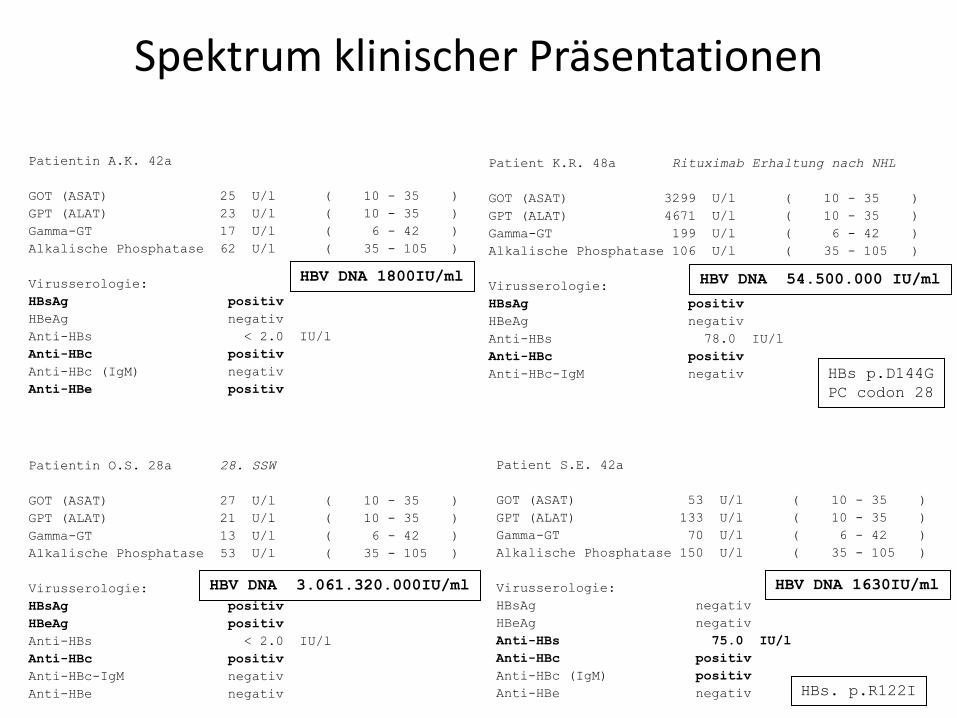
Spektrum klinischer Präsentationen
Patientin A.K. 42a
GOT (ASAT) 25 U/l ( 10 - 35 )
GPT (ALAT) 23 U/l ( 10 - 35 )
Gamma-GT 17 U/l ( 6 - 42 )
Alkalische Phosphatase 62 U/l ( 35 - 105 )
Virusserologie:
HBsAg positiv
HBeAg negativ
Anti-HBs < 2.0 IU/l
Anti-HBc positiv
Anti-HBc (IgM) negativ
Anti-HBe positiv
Patient K.R. 48a Rituximab Erhaltung nach NHL
GOT (ASAT) 3299 U/l ( 10 - 35 )
GPT (ALAT) 4671 U/l ( 10 - 35 )
Gamma-GT 199 U/l ( 6 - 42 )
Alkalische Phosphatase 106 U/l ( 35 - 105 )
Virusserologie:
HBsAg positiv
HBeAg negativ
Anti-HBs 78.0 IU/l
Anti-HBc positiv
Anti-HBc-IgM negativ
HBV DNA 1800IU/ml HBV DNA 54.500.000 IU/ml
HBs p.D144G
PC codon 28
Patientin O.S. 28a 28. SSW
GOT (ASAT) 27 U/l ( 10 - 35 )
GPT (ALAT) 21 U/l ( 10 - 35 )
Gamma-GT 13 U/l ( 6 - 42 )
Alkalische Phosphatase 53 U/l ( 35 - 105 )
Virusserologie:
HBsAg positiv
HBeAg positiv
Anti-HBs < 2.0 IU/l
Anti-HBc positiv
Anti-HBc-IgM negativ
Anti-HBe negativ
HBV DNA 3.061.320.000IU/ml
Patient S.E. 42a
GOT (ASAT) 53 U/l ( 10 - 35 )
GPT (ALAT) 133 U/l ( 10 - 35 )
Gamma-GT 70 U/l ( 6 - 42 )
Alkalische Phosphatase 150 U/l ( 35 - 105 )
Virusserologie:
HBsAg negativ
HBeAg negativ
Anti-HBs 75.0 IU/l
Anti-HBc positiv
Anti-HBc (IgM) positiv
Anti-HBe negativ
HBV DNA 1630IU/ml
HBs. p.R122I
DIAGNOSTIK ≠ EIN TESTERGEBNIS
Wofür braucht der ÖGD ein Hepatologisches Labor an einer Universitätsklinik?
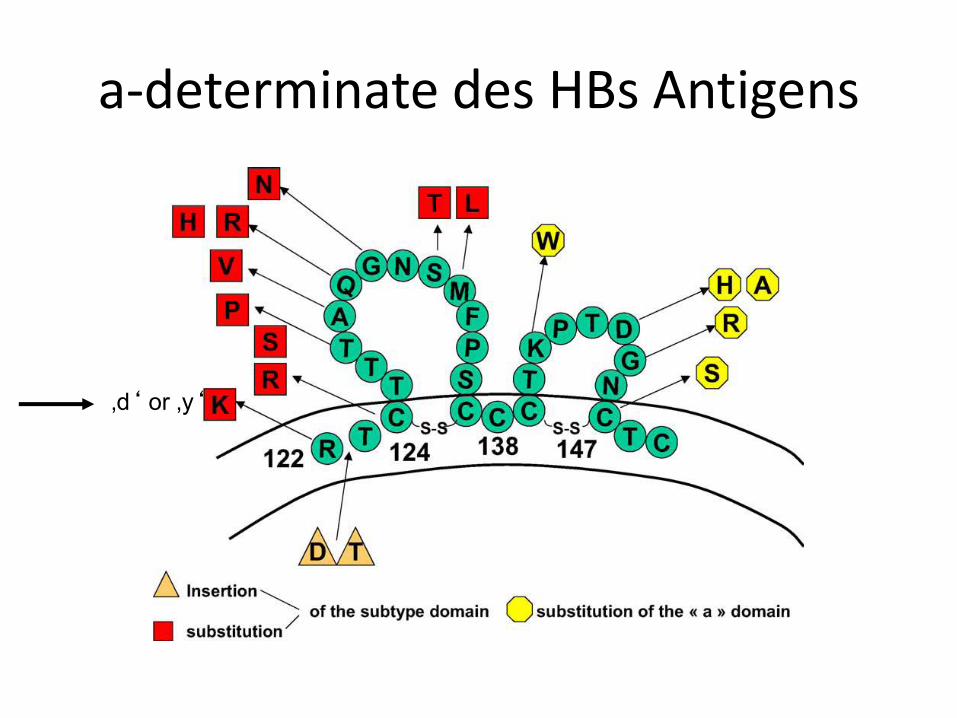
a-determinate des HBs Antigens
‚d‘ or ‚y‘
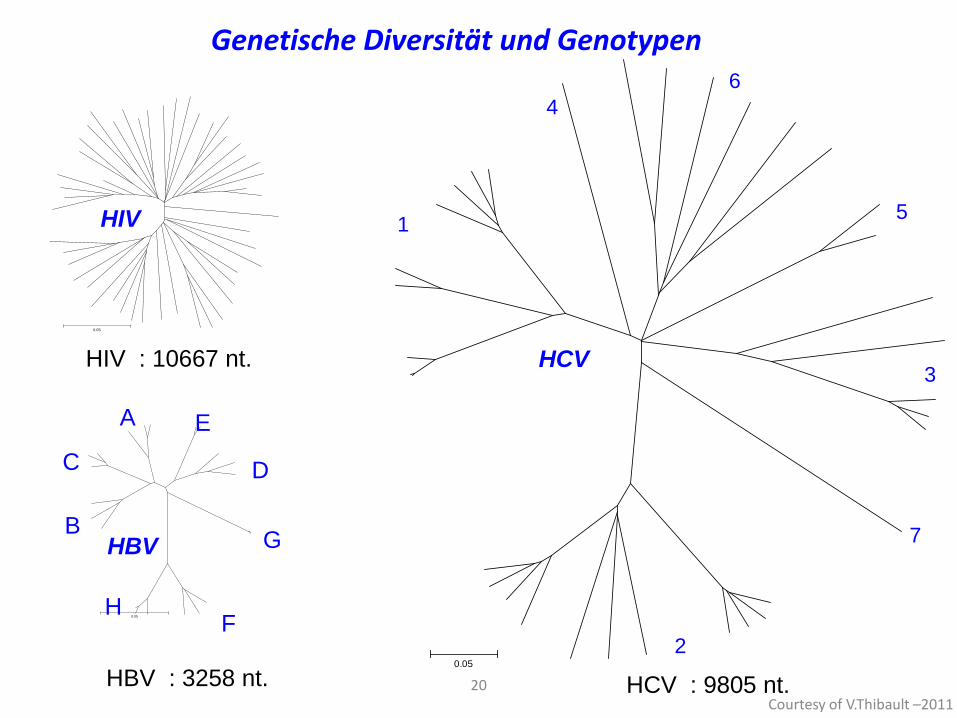
Courtesy of V.Thibault –2011 20
Genetische Diversität und Genotypen
0.05
1
4
6
5
3
7
2
HCV
HCV : 9805 nt.
0.05
A
B
C D
E
F
G
H
HBV : 3258 nt.
HBV
0.05
HIV
HIV : 10667 nt.
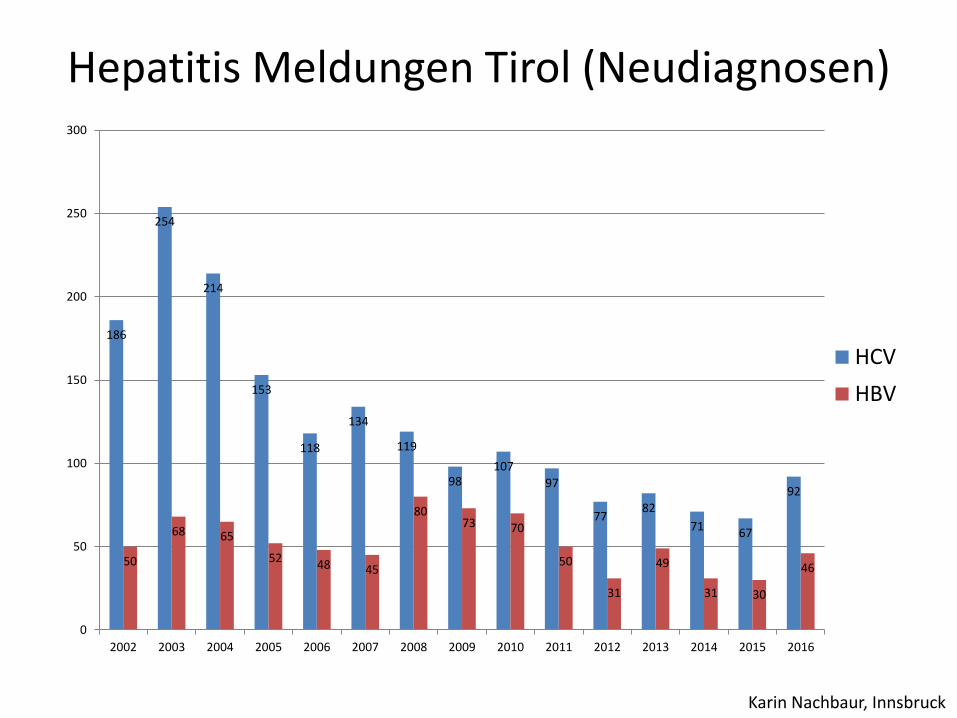
Hepatitis Meldungen Tirol (Neudiagnosen)
186
254
214
153
118
134
119
98 107
97
77 82
71 67
92
50
68 65
52 48 45
80 73 70
50
31
49
31 30
46
0
50
100
150
200
250
300
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
HCV
HBV
Karin Nachbaur, Innsbruck
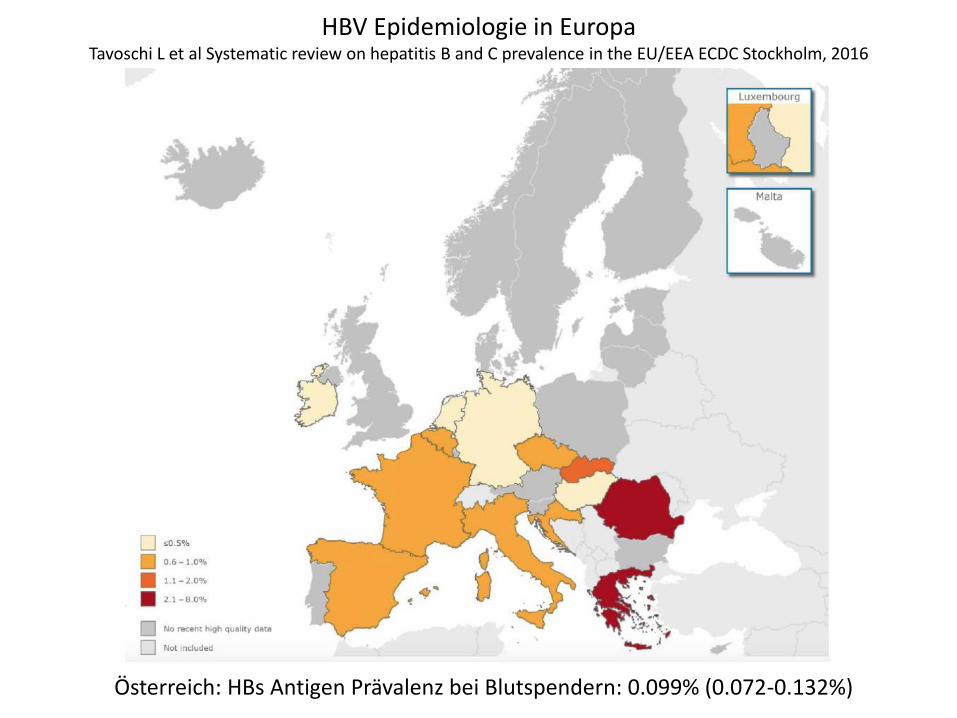
HBV Epidemiologie in Europa Tavoschi L et al Systematic review on hepatitis B and C prevalence in the EU/EEA ECDC Stockholm, 2016
Österreich: HBs Antigen Prävalenz bei Blutspendern: 0.099% (0.072-0.132%)
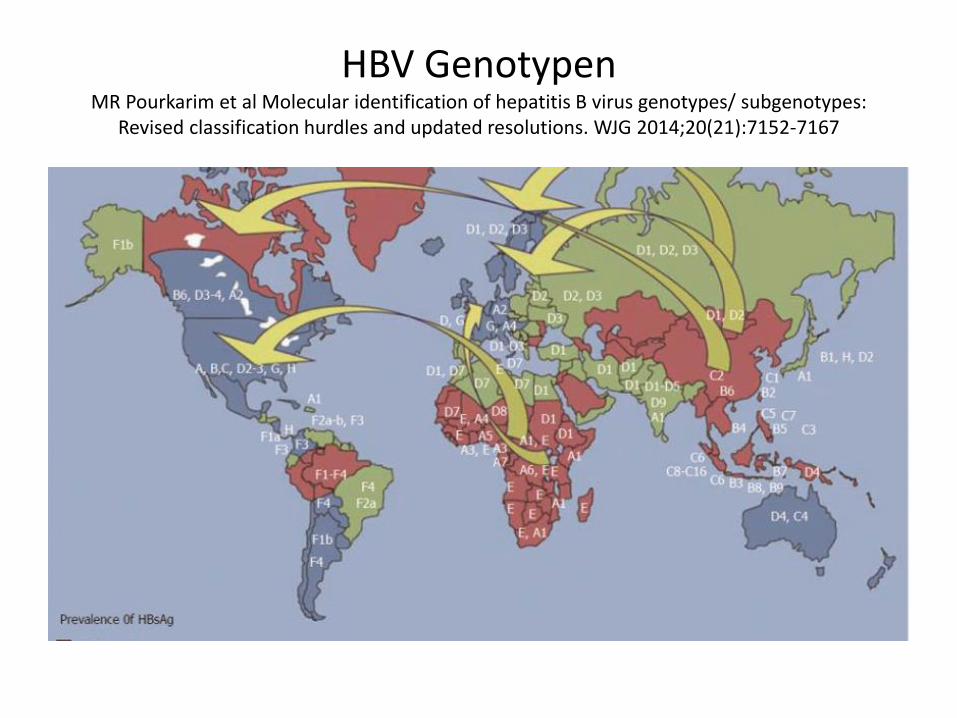
HBV Genotypen MR Pourkarim et al Molecular identification of hepatitis B virus genotypes/ subgenotypes:
Revised classification hurdles and updated resolutions. WJG 2014;20(21):7152-7167
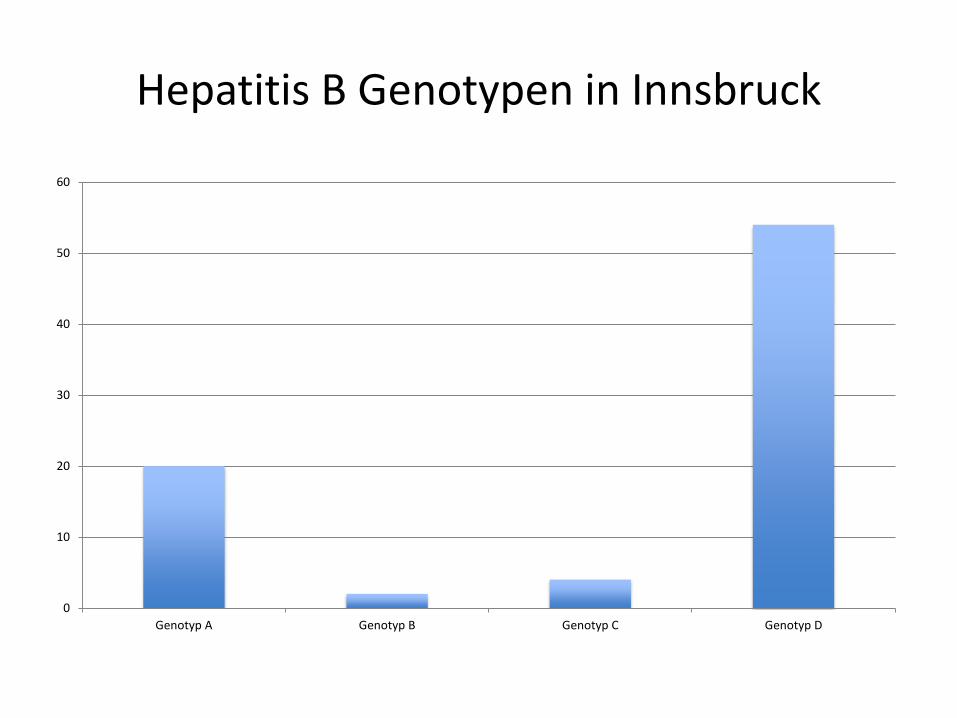
Hepatitis B Genotypen in Innsbruck
0
10
20
30
40
50
60
Genotyp A Genotyp B Genotyp C Genotyp D
EPIDEMIOLOGIE ≠ STRATEGIEPLANUNG
Wofür braucht der ÖGD ein Hepatologisches Labor an einer Universitätsklinik?
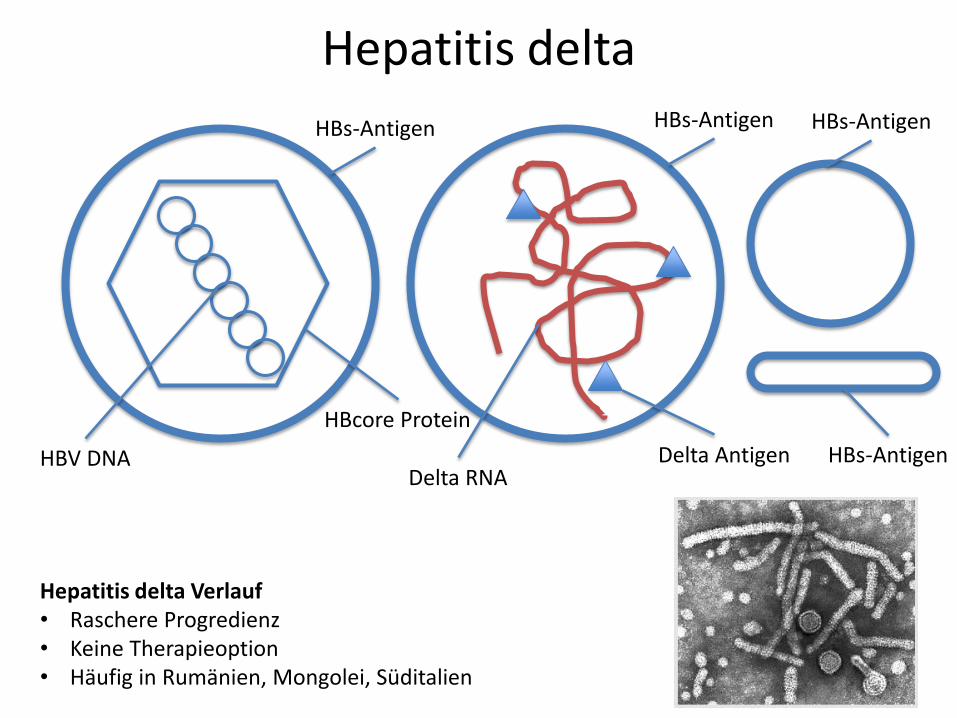
HBs-Antigen
HBV DNA
HBcore Protein
Delta Antigen Delta RNA
HBs-Antigen HBs-Antigen
HBs-Antigen
Hepatitis delta Verlauf • Raschere Progredienz • Keine Therapieoption • Häufig in Rumänien, Mongolei, Süditalien
Hepatitis delta
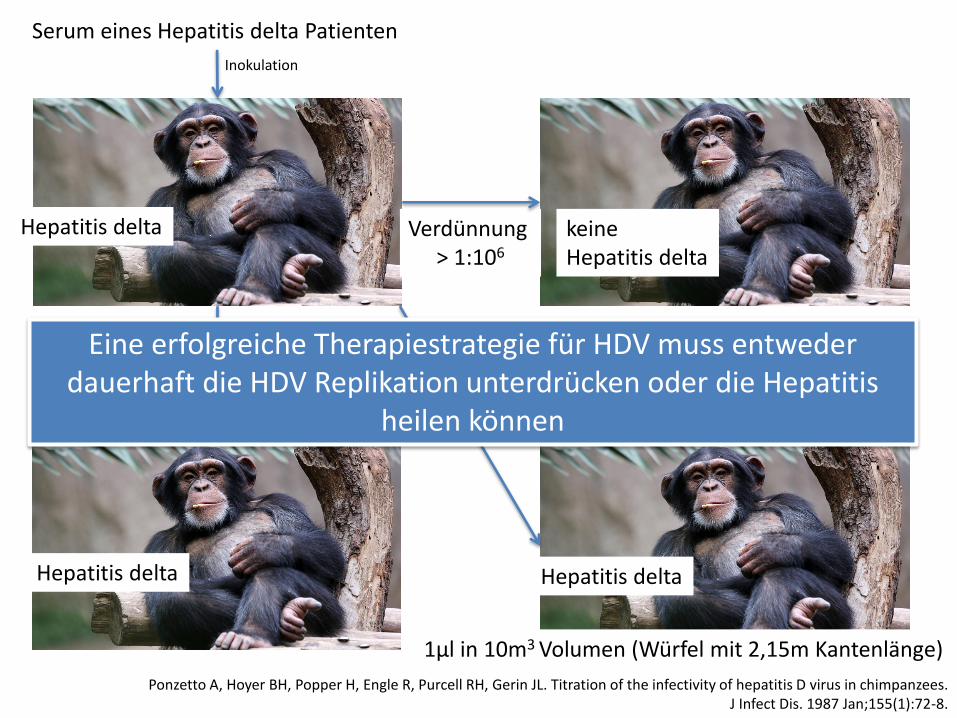
Ponzetto A, Hoyer BH, Popper H, Engle R, Purcell RH, Gerin JL. Titration of the infectivity of hepatitis D virus in chimpanzees. J Infect Dis. 1987 Jan;155(1):72-8.
Serum eines Hepatitis delta Patienten
Inokulation
Hepatitis delta
Verdünnung ≤ 1:106
(1µl in 1l)
Hepatitis delta
Verdünnung > 1:106
keine Hepatitis delta
Hepatitis B Virusinfektion vor delta Infektion (HBs positiv)
Verdünnung ≤ 1:1011
Hepatitis delta
1µl in 10m3 Volumen (Würfel mit 2,15m Kantenlänge)
Eine erfolgreiche Therapiestrategie für HDV muss entweder dauerhaft die HDV Replikation unterdrücken oder die Hepatitis
heilen können
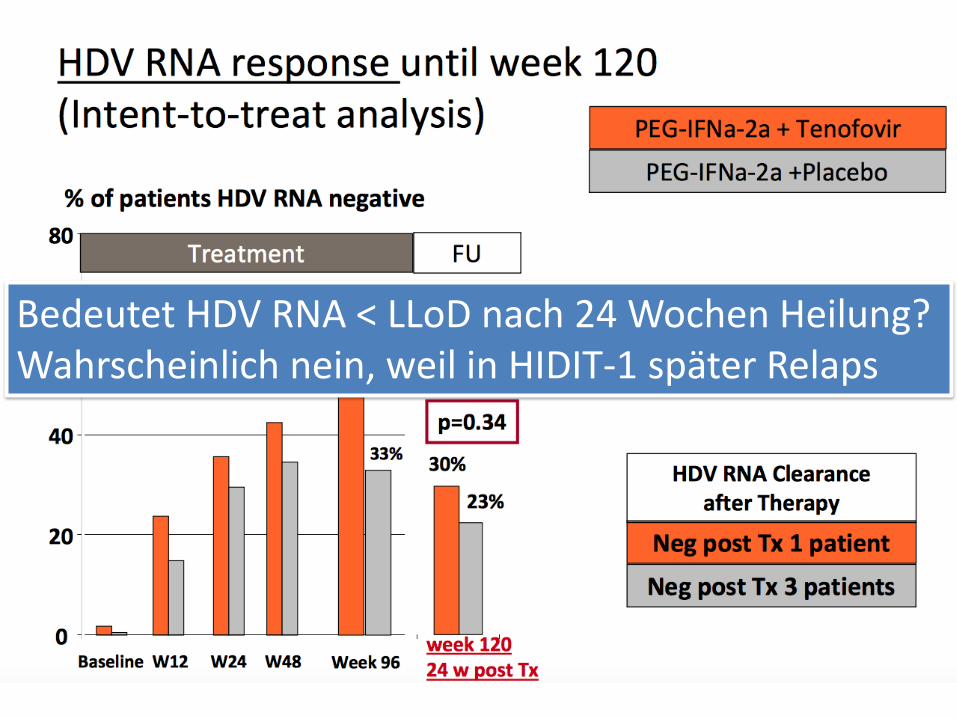
Bedeutet HDV RNA < LLoD nach 24 Wochen Heilung? Wahrscheinlich nein, weil in HIDIT-1 später Relaps
Wofür braucht der öffentliche Gesundheitsdienst es ein Hepatologisches
Labor an einer Universitätsklinik?
Chronische Hepatitis B und Hepatitis delta Virusinfektion ≠
Chronische Hepatitis Zirrhose Karzinom
Testergebnisse aus Serologie und Molekularbiologie &
Klinische Korrelation (zB Immunescape Varianten)
Migration
Epidemiologie (HBV Genotypen)
Hepatitis Delta... ungelöstes Problem
Hepatitis B – Fortschritte Erste Krebsvakzine
Dauerhafte Virussuppression durch Polymerasehemmer offene Fragen: Hepatitis B Heilung & Reaktivierung....