-
7/29/2019 Hirschsprung's Lecture
1/46
IN THE NAME OF MERCIFULGOD
-
7/29/2019 Hirschsprung's Lecture
2/46
Hirschsprungs disease
Primary Megacolon
Khaled Ashour
JR Hospital
Oxford
-
7/29/2019 Hirschsprung's Lecture
3/46
Hirschsprungs Disease
Definition
It is a primary gastrointestinal disease
caused by congenital absence of theintestinal ganglion cells,
namely, the
submucosal Meissners, and the
intermuscular Aurbachs
-
7/29/2019 Hirschsprung's Lecture
4/46
Hirschsprungs Disease
Incidence: -
1 : 4400 to 1 : 7000 live birth.
In Classic H.D. male : female = 4 : 1. In long segment H.D. M :
F = 1 : 1.
No racial difference.
Increased incidence in familial cases (2-18%).
-
7/29/2019 Hirschsprung's Lecture
5/46
Hirschsprungs Disease
Incidence: -The affected part of the intestine:
Rectosigmoid area : 77%Long segment colonic : 14%
Total colonic : 7%
Total GIT : 2%
-
7/29/2019 Hirschsprung's Lecture
6/46
EtiologyTheories: -
- Failure of migration of the neuroenteric cellsdistally along
the alimentary canal.
- Presence of hostile environment (lack of neural
cell adhesion molecule NCAM).
- Immunologic theory: increased expression of class
II antigen.
-
7/29/2019 Hirschsprung's Lecture
7/46
PathophysiologyDue to the absence of ganglia, the affected
segment loses its receptive relaxation ability.
Thus, it becomes functionally contracted.
Proximally, the normal segment overcontracts to
pass the stool distally, which results in gradual
dilatation and hypertrophy.
-
7/29/2019 Hirschsprung's Lecture
8/46
Pathology So, the gross pathology will show 3 distinct
regions: -
1) the narrow segment affected.
2) A transitional zone hypoganglionic
3) dilated hypertrophied segment normal
-
7/29/2019 Hirschsprung's Lecture
9/46
1
2 3
-
7/29/2019 Hirschsprung's Lecture
10/46
Pathology (Cont.)Microscopically: -
1) Absence ofMeissners
andAurbachs
ganglia.2) Abundant nerve fibers.
This might be evident either by Hematoxylin &
Eosin stain, or better, using Acetyl Choline estrasestain.
-
7/29/2019 Hirschsprung's Lecture
11/46
Hirschsprungs disease Presentation:
1) Neonatal: Onset -> during neonatal period.Clinical
picture:
*Delayed passage of meconium.
*Abdominal distension.* Constipation.
* +\- bilious vomiting.
-
7/29/2019 Hirschsprung's Lecture
12/46
H.D. Presentation2) Infantile type:
* Chronic constipation.
* Abdominal distension.
* Bouts of abdominal colics
* Very infrequently vomiting.* mild growth retardation.
-
7/29/2019 Hirschsprung's Lecture
13/46
H.D Clinical pictureO/E:
- Abdominal distension, lax abdomen if
uncomplicated.
- visible intestinal loops.
- P/R: Passage of gush of stool and gases.
-
7/29/2019 Hirschsprung's Lecture
14/46
-
7/29/2019 Hirschsprung's Lecture
15/46
H.D. Investigations1) Plain X ray abdomen standing.
2) Ba enema
3) rectal biopsy.
4) Rectal manometry.
-
7/29/2019 Hirschsprung's Lecture
16/46
H.D. InvestigationsPlain X ray
abdomen
-
7/29/2019 Hirschsprung's Lecture
17/46
H.D. Investigations
Plain X ray abdomen
-
7/29/2019 Hirschsprung's Lecture
18/46
H.D. Investigations
Plain X ray abdomen
-
7/29/2019 Hirschsprung's Lecture
19/46
H.D. Investigations
Ba enema lateral view
-
7/29/2019 Hirschsprung's Lecture
20/46
H.D. Investigations
Ba enema A-P view
-
7/29/2019 Hirschsprung's Lecture
21/46
H.D. Investigations
Ba enema A-P view
-
7/29/2019 Hirschsprung's Lecture
22/46
H.D. Investigations
Ba enema A-P view.
-
7/29/2019 Hirschsprung's Lecture
23/46
Classical managementPerforming defunctioning colstomy.
Followed later on by the definite pull-through operation.
Finally, closure of colostomy
-
7/29/2019 Hirschsprung's Lecture
24/46
H.D. Management Pull through techniques:
1) Soave endorectal pull-through.
2) Swenson pull-through.
3) Duhamel pull-through.
4) Rhebein anterior resection.
-
7/29/2019 Hirschsprung's Lecture
25/46
H.D. Surgical treatment
Child with Rt. TV.
Colostomy
-
7/29/2019 Hirschsprung's Lecture
26/46
Duhamel Pull-through
-
7/29/2019 Hirschsprung's Lecture
27/46
Swenson
Pull-through
-
7/29/2019 Hirschsprung's Lecture
28/46
Soave pull-through Identification of the
pathological segment.
-
7/29/2019 Hirschsprung's Lecture
29/46
Soave pull-through
Development of the
seromuscular cuff.
-
7/29/2019 Hirschsprung's Lecture
30/46
Soave pull-through
The healthy colon is
ready to be pulledthrough the
seromuscular cuff.
-
7/29/2019 Hirschsprung's Lecture
31/46
Soave pull-through
The colon after being
pulled through the cuff
to outside the body.
-
7/29/2019 Hirschsprung's Lecture
32/46
New trends in management Two-stages modality: First leveling
pelvic colostomy, followed by definitepull-through.
Performing the one stage pull-through
technique without preliminary
colostomy (in older age group).
-
7/29/2019 Hirschsprung's Lecture
33/46
More recentThe introduction of one stage transanal pull-
through technique by De la Torrein 1998.
Yet, few reports are available about its application
in the neonatal period.
-
7/29/2019 Hirschsprung's Lecture
34/46
Technique for transanal pull-through
-
7/29/2019 Hirschsprung's Lecture
35/46
Technique of TAPTPerforming anal
dilatation.
-
7/29/2019 Hirschsprung's Lecture
36/46
Technique of TAPTRetraction is effected
using Langenbeck
retractor instead of theclassical Lone-Starretractor
-
7/29/2019 Hirschsprung's Lecture
37/46
Technique of TAPTTension sutures
application.
-
7/29/2019 Hirschsprung's Lecture
38/46
Technique of TAPTSecond layer of
tension sutures.
-
7/29/2019 Hirschsprung's Lecture
39/46
Technique of TAPTDissection of the
mucosa leavingthe seromuscular
cuff.
-
7/29/2019 Hirschsprung's Lecture
40/46
Technique of TAPTProceeding
dissection till
peritoneal reflection.
-
7/29/2019 Hirschsprung's Lecture
41/46
Technique of TAPTThe cuff is opened,
and full thickness
dilated colon is
now pulled with
mesentericdevascularization.
-
7/29/2019 Hirschsprung's Lecture
42/46
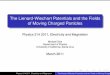
Technique of TAPTThe excised colorectal
segment, showing the
coning of H.D.
relatively long
segment H.D.
-
7/29/2019 Hirschsprung's Lecture
43/46
Technique of TAPTAfter the pulled
segment is cut, the
cut edge is sutured
to the anal mucosa.
-
7/29/2019 Hirschsprung's Lecture
44/46
Technique of TAPTRectal tube +/-
drain is left for one
day.
-
7/29/2019 Hirschsprung's Lecture
45/46
Postoperative barium enemaBa enema was
done in thecourse of thefollow-up toevaluate
thecolonpostoperatively
-
7/29/2019 Hirschsprung's Lecture
46/46
Thank you