Embed Size (px)
Citation preview
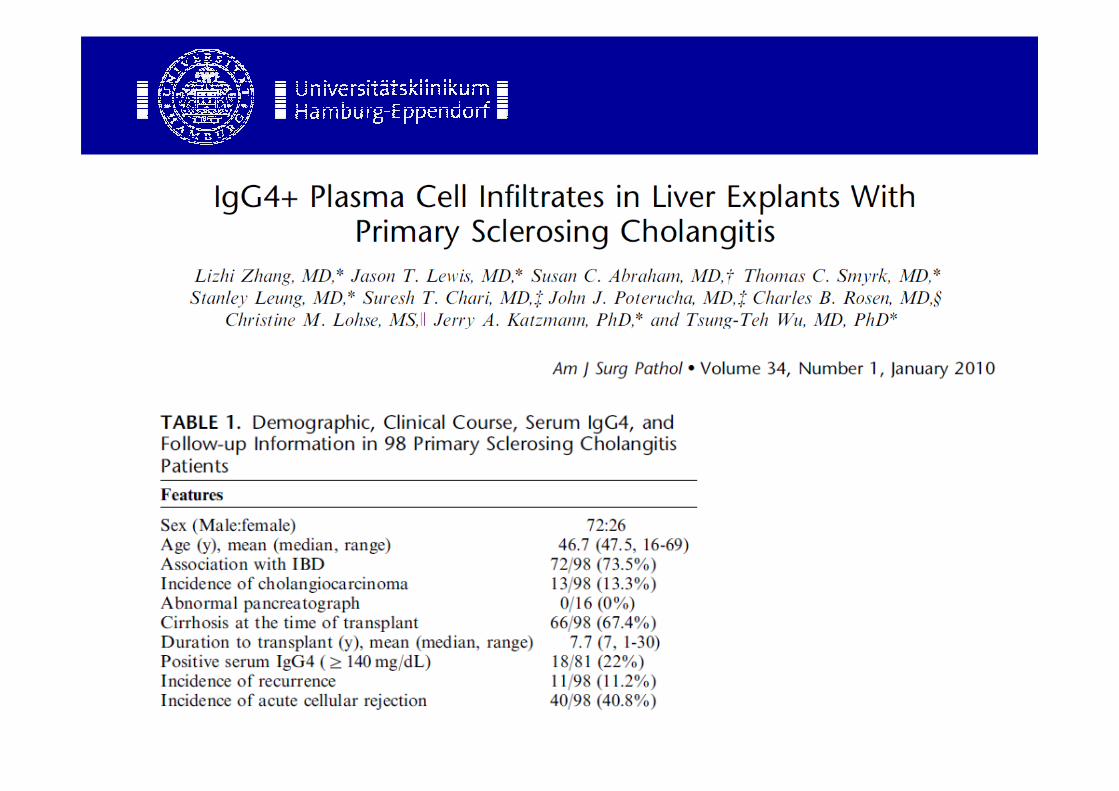
IgG4 assoziierte Cholangitis –
Ein neues Krankheitsbild?
Stefan Lüth
Fall 1
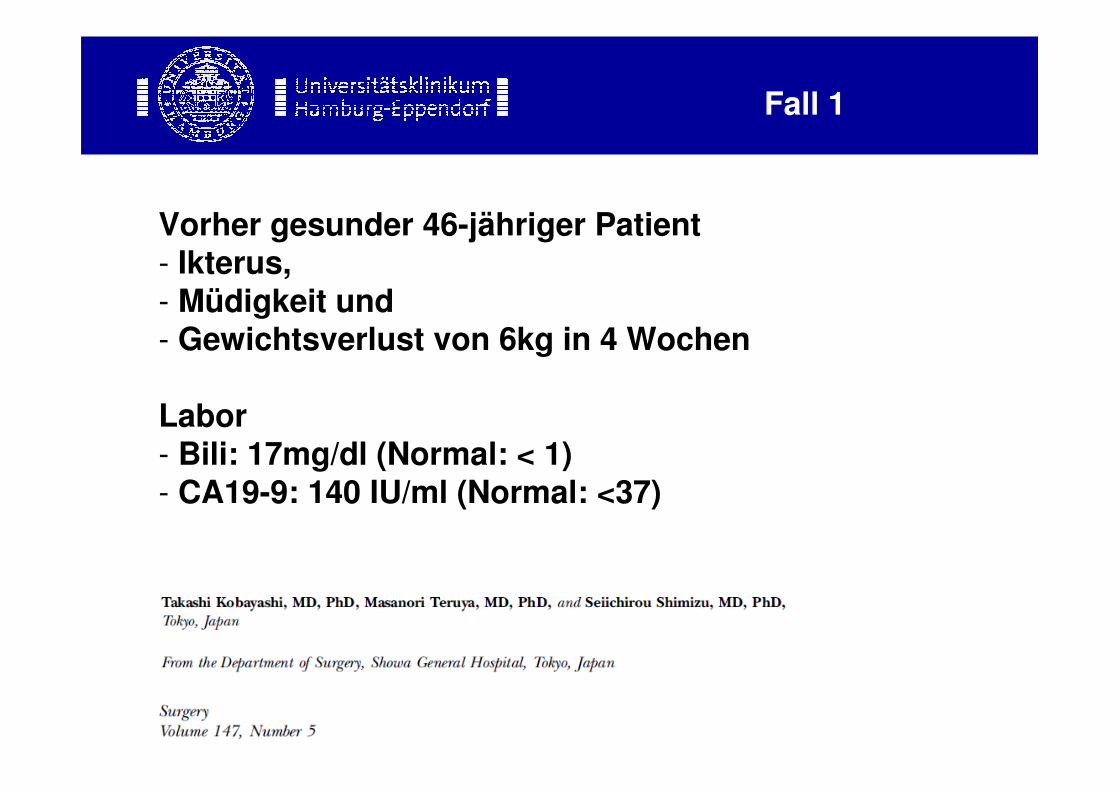
Vorher gesunder 46-jähriger Patient- Ikterus, - Müdigkeit und - Gewichtsverlust von 6kg in 4 Wochen
Labor- Bili: 17mg/dl (Normal: < 1) - CA19-9: 140 IU/ml (Normal: <37)
Fall 1
Fall 1
Klinisch, laborchemisch und radiologisch:
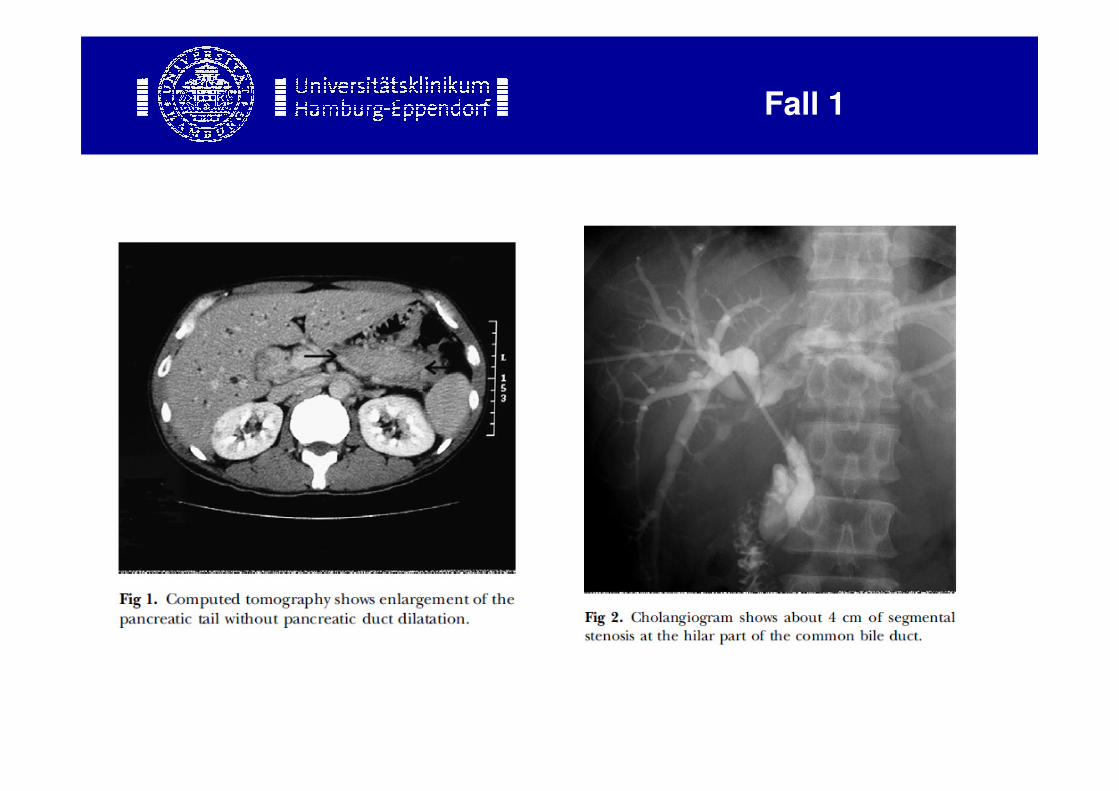
V.a. Gallengangs-Ca, DD: GB-CaNicht erklärt: Pankreasvergrösserung
Therapie: - Erweiterte rechtsseitige Hemi-Hepatektomie und - distale Pankreasresektion

Fall 1
Fall 1
Fall
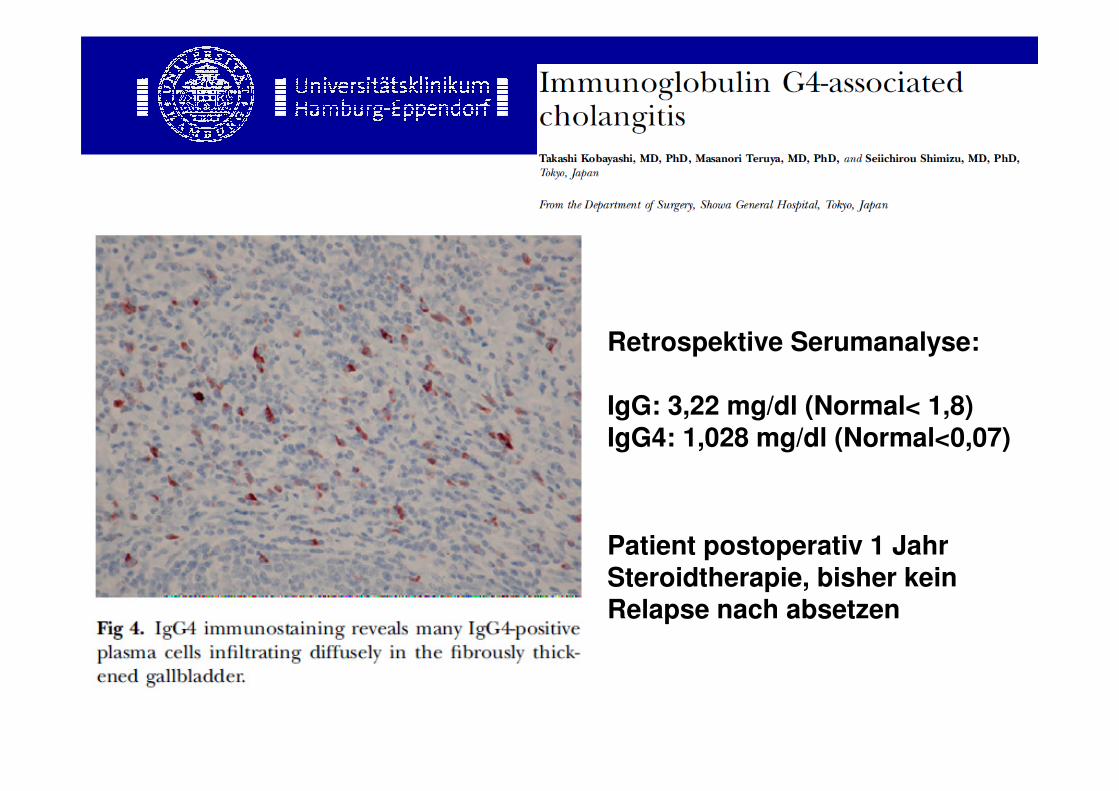
Retrospektive Serumanalyse:
IgG: 3,22 mg/dl (Normal< 1,8)IgG4: 1,028 mg/dl (Normal<0,07)
Patient postoperativ 1 Jahr Steroidtherapie, bisher kein Relapse nach absetzen
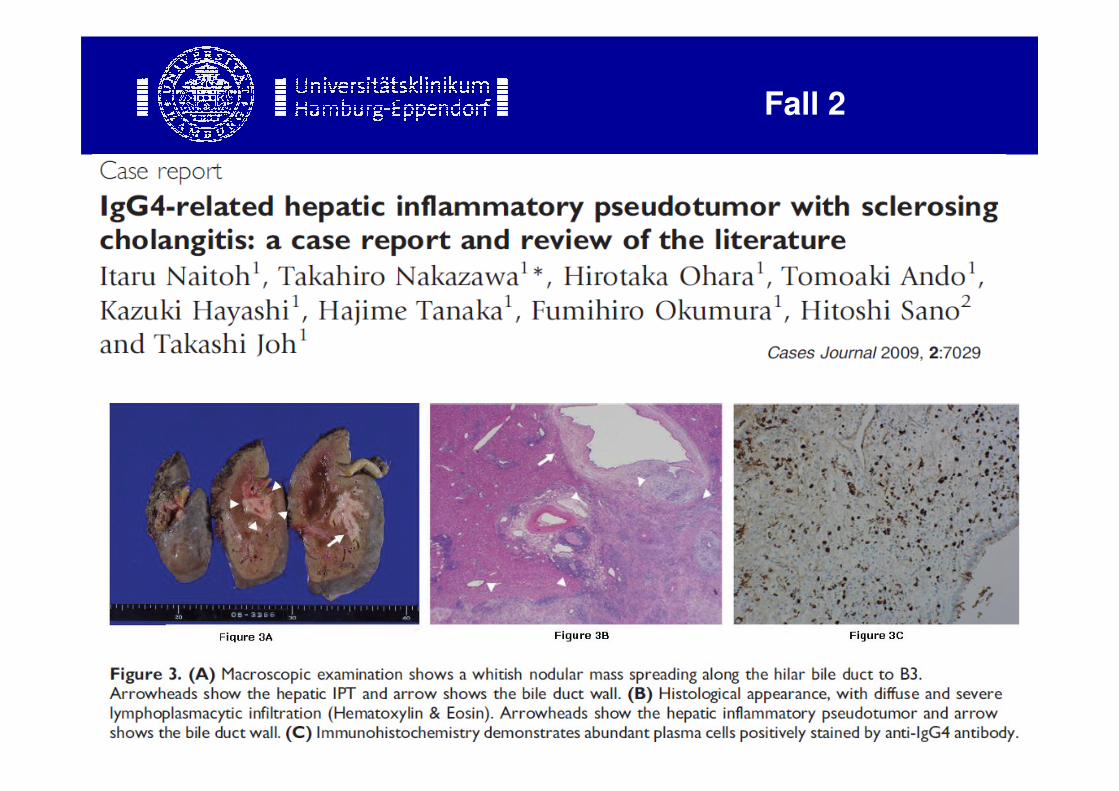
Fall 2
Autoimmunpankreatitis
1. IgG 4 assoz. Erkrankung
• Erster Fall: Sarles H. (Am J Dig Dis 1961)
• Yoshida et al. Dig Dis Sci 1995
• Epidemiologie:
– Bei 38 / 425 japanischen Patienten mit chronischer Pankreatitis wurde eine AIP diagnostiziert ~ 9%
(K. Okazaki et al. J Gastroenterol 2001)
- Bei 23 / 383 italienischen Patienten mit chronischer Pankreatitis wurde eine AIP diagnostiziert ~ 6%
(L. Frulloni et al. Pancreas 2003)
Autoimmunpankreatitis
IACDefinition
Steroid responsive biliary disease, frequently involving the
extrahepatic ducts, that is often associated with other fibrosingconditions, especially autoimmune pancreatitis
Björnsson E et al, Hepatology 2007
Autoimmune Pankreatocholangitis (AIPC)
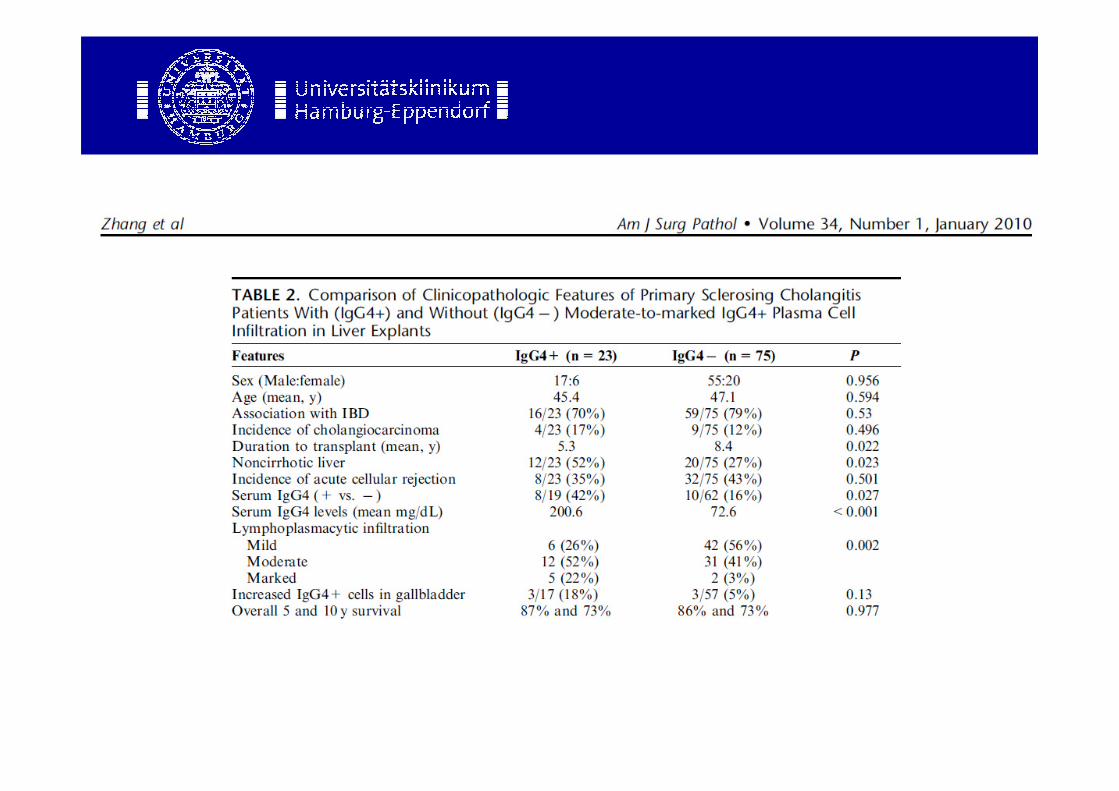
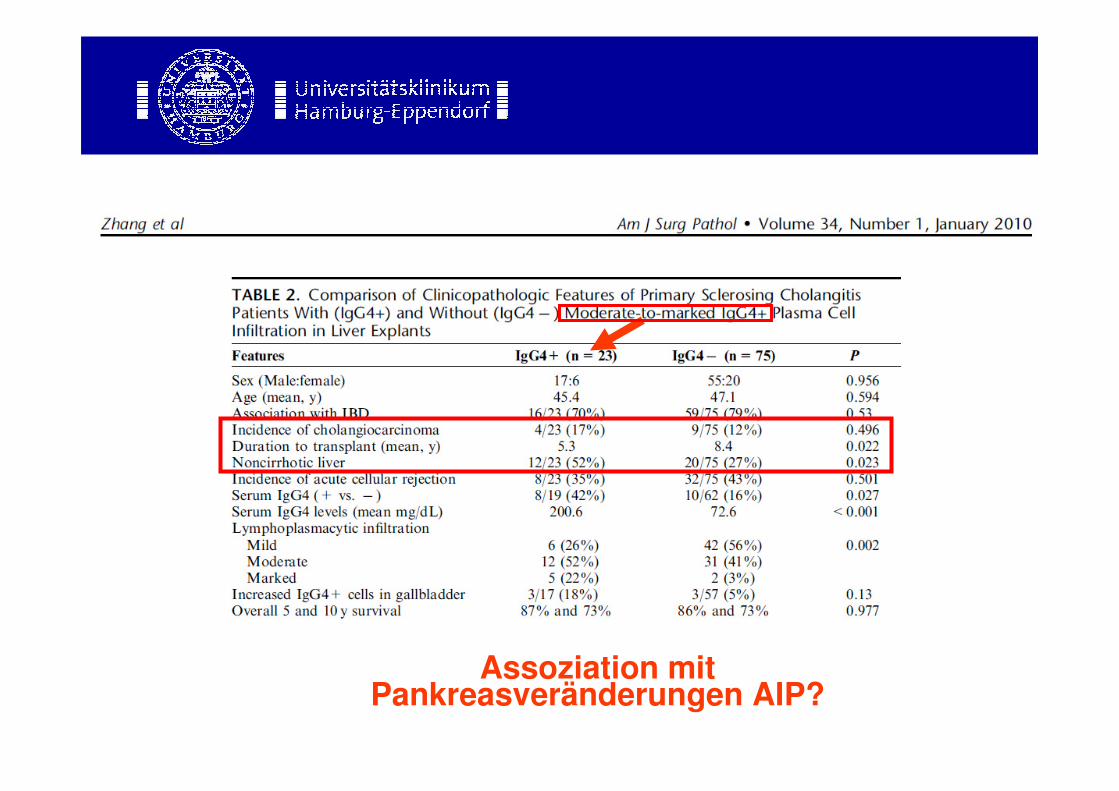
Assoziation mit Pankreasveränderungen AIP?
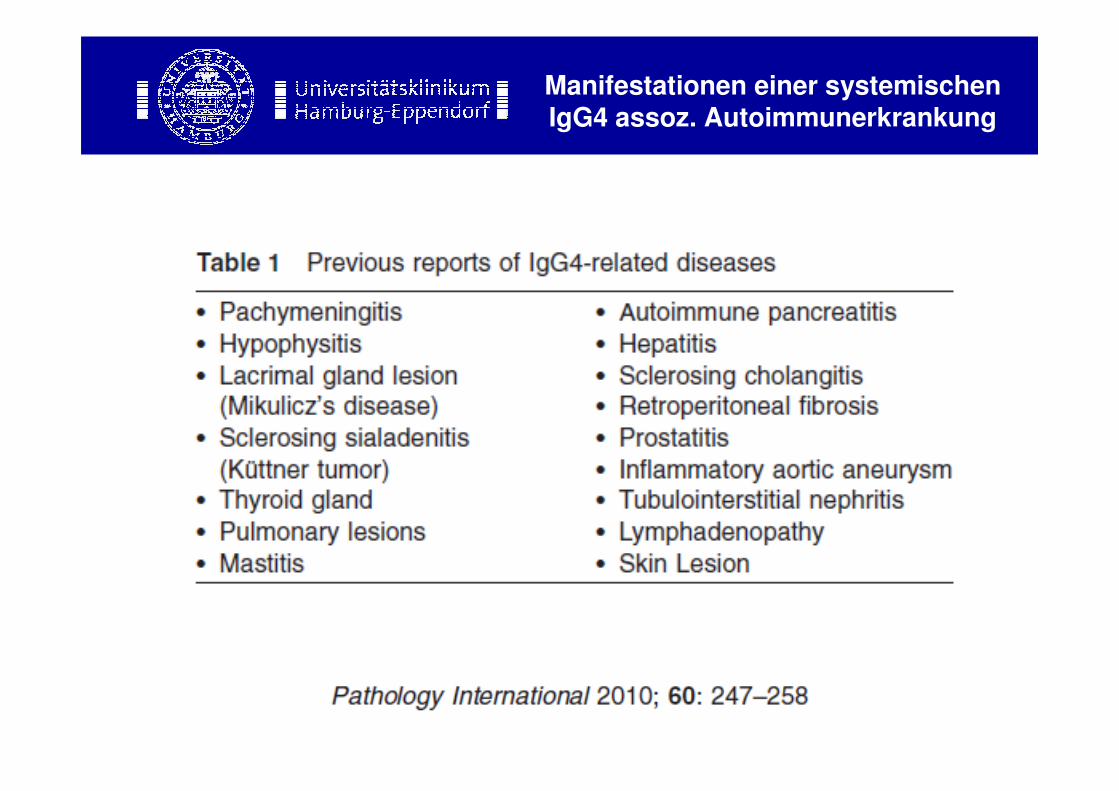
Manifestationen einer systemischen IgG4 assoz. Autoimmunerkrankung
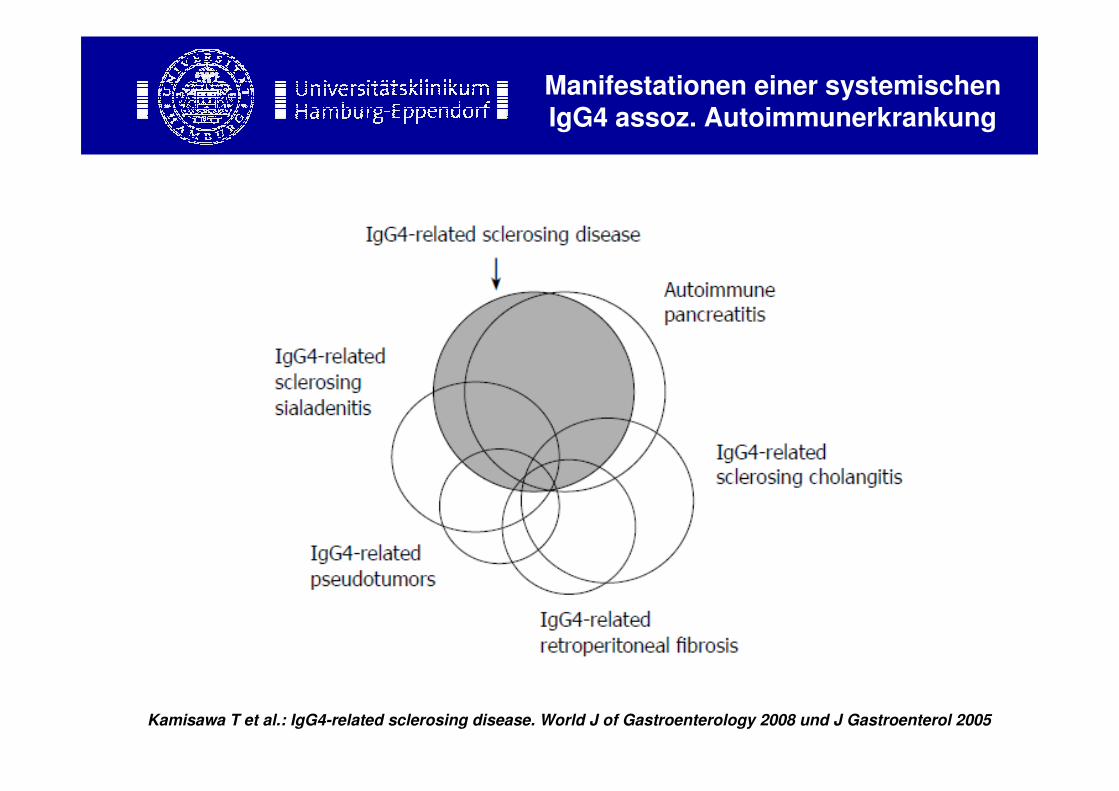
Manifestationen einer systemischen IgG4 assoz. Autoimmunerkrankung
Kamisawa T et al.: IgG4-related sclerosing disease. World J of Gastroenterology 2008 und J Gastroenterol 2005
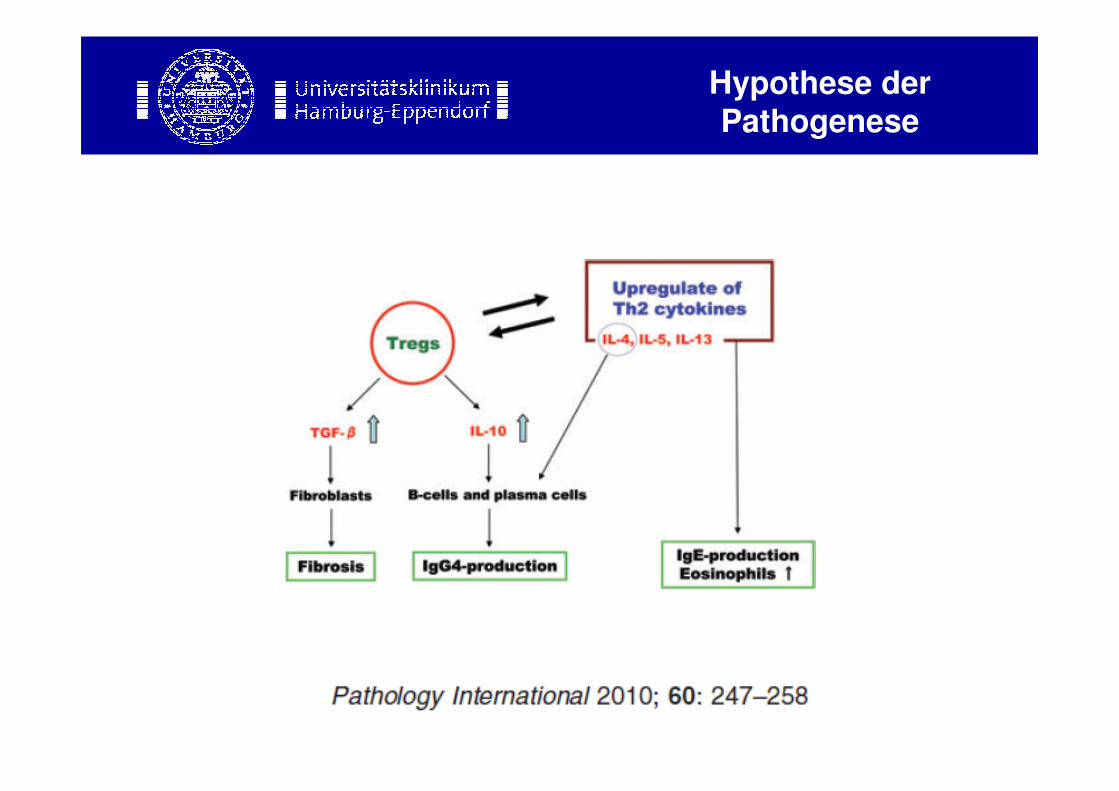
Hypothese der Pathogenese
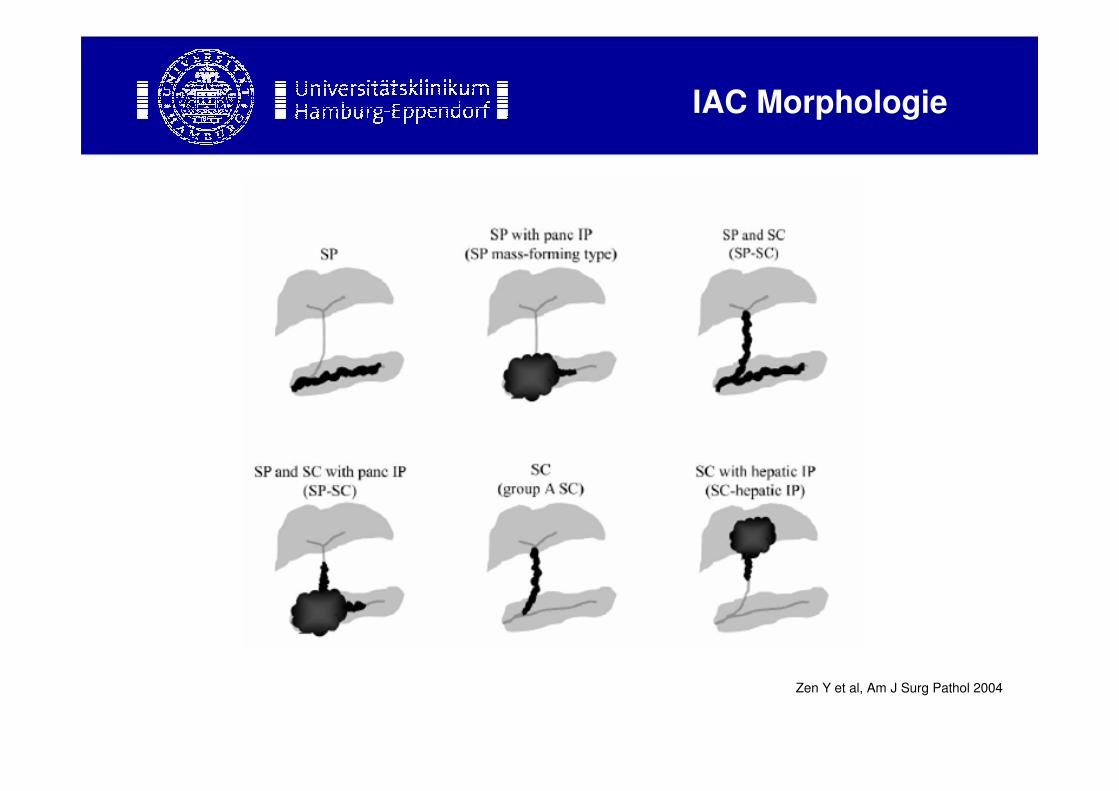
IAC Morphologie
Zen Y et al, Am J Surg Pathol 2004
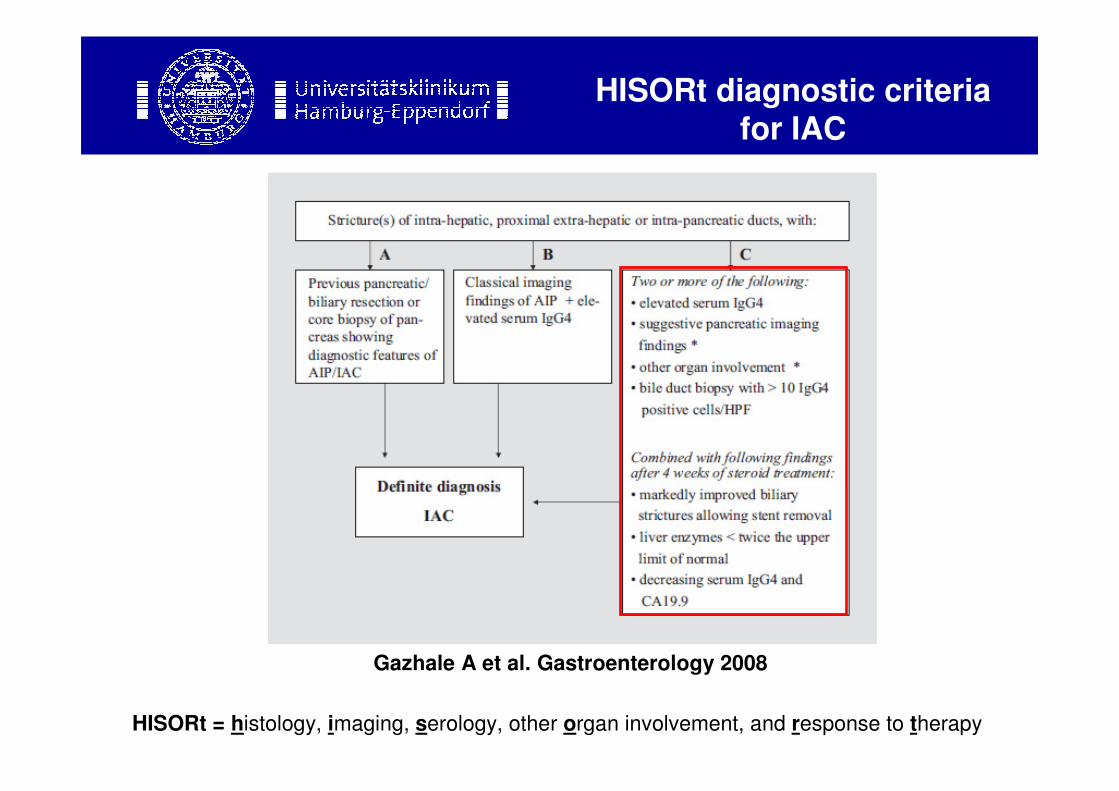
HISORt diagnostic criteriafor IAC
B: nach 4
Wochen
Cortisontherapie HISORt = histology, imaging, serology, other organ involvement, and response to therapy
Gazhale A et al. Gastroenterology 2008
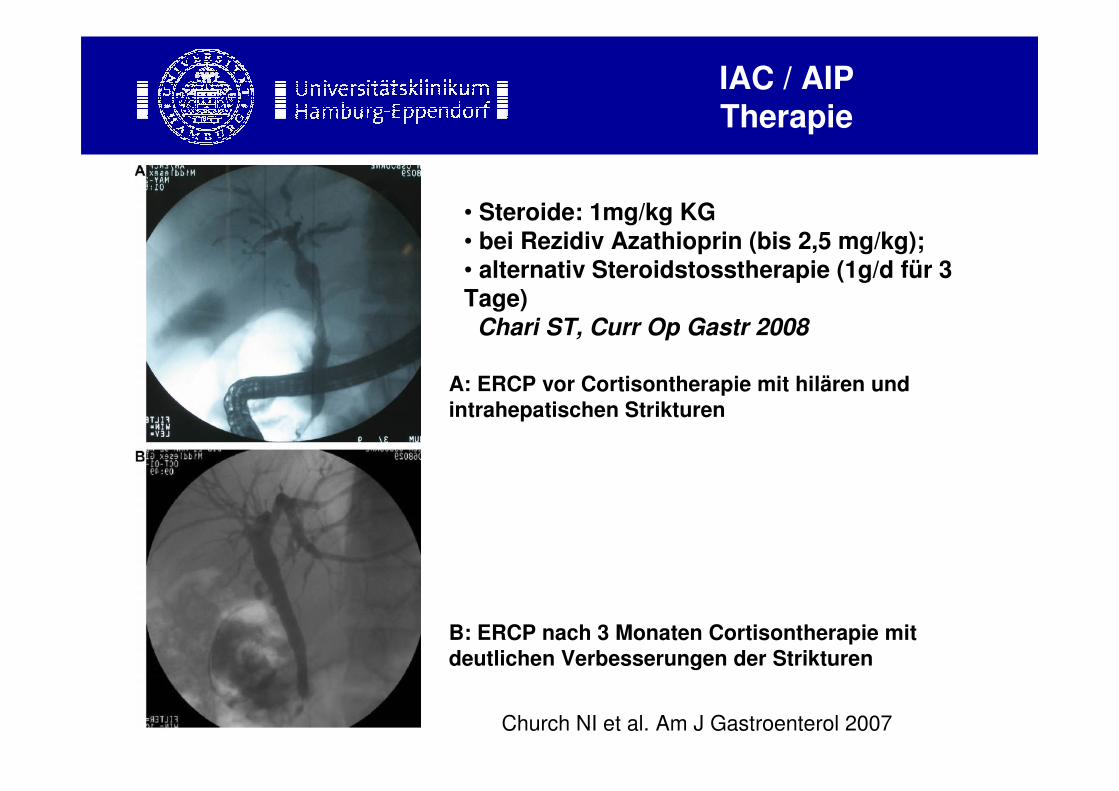
IAC / AIPTherapie
B: nach 4
Wochen
Cortisontherapie
A: ERCP vor Cortisontherapie mit hilären und
intrahepatischen Strikturen
B: ERCP nach 3 Monaten Cortisontherapie mit
deutlichen Verbesserungen der Strikturen
Church NI et al. Am J Gastroenterol 2007
• Steroide: 1mg/kg KG
• bei Rezidiv Azathioprin (bis 2,5 mg/kg); • alternativ Steroidstosstherapie (1g/d für 3 Tage)
Chari ST, Curr Op Gastr 2008
Schlussfolgerung 1
• IAC und AIP Teil einer systemischen IgG4 assoziierten (Autoimmun-) Erkrankung
• Debatte über eigene Entität (AIPC) hält an
• Pathogenese unklar
Schlussfolgerung 2
• Diagnose: HISORt Kriterien
• Serum IgG4 nicht immer erhöht
• Autoantikörper nicht wegweisend (anti-Lactoferrin, anti-Carboanhydrase-II, ANA, RF)
• Histologie abhängig von Materialart
• IgG4-Immunhistochemie: „Cut-off“ nicht definiert,
Spezifität unbekannt
Schlussfolgerung 3
• Therapie: Steroide sind Therapie der Wahl
• Pankreas-Ca, häufigste Fehldiagnose (>80%) bei AIP
(DD: Lymphom, Plasmozytom, idiopathische
Pankreatitis)
• PSC sollte von IAC unterschieden werden

B: nach 4
Wochen
Cortisontherapie
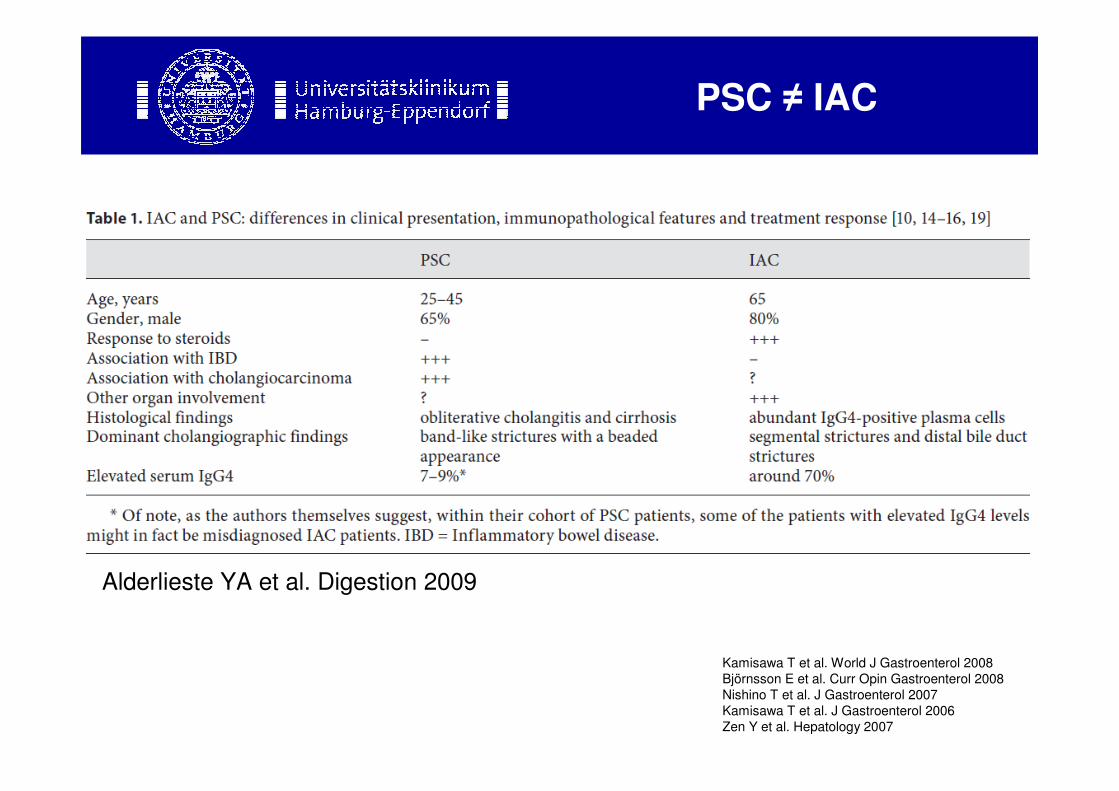
Alderlieste YA et al. Digestion 2009
PSC ≠ IAC
Kamisawa T et al. World J Gastroenterol 2008
Björnsson E et al. Curr Opin Gastroenterol 2008
Nishino T et al. J Gastroenterol 2007
Kamisawa T et al. J Gastroenterol 2006
Zen Y et al. Hepatology 2007
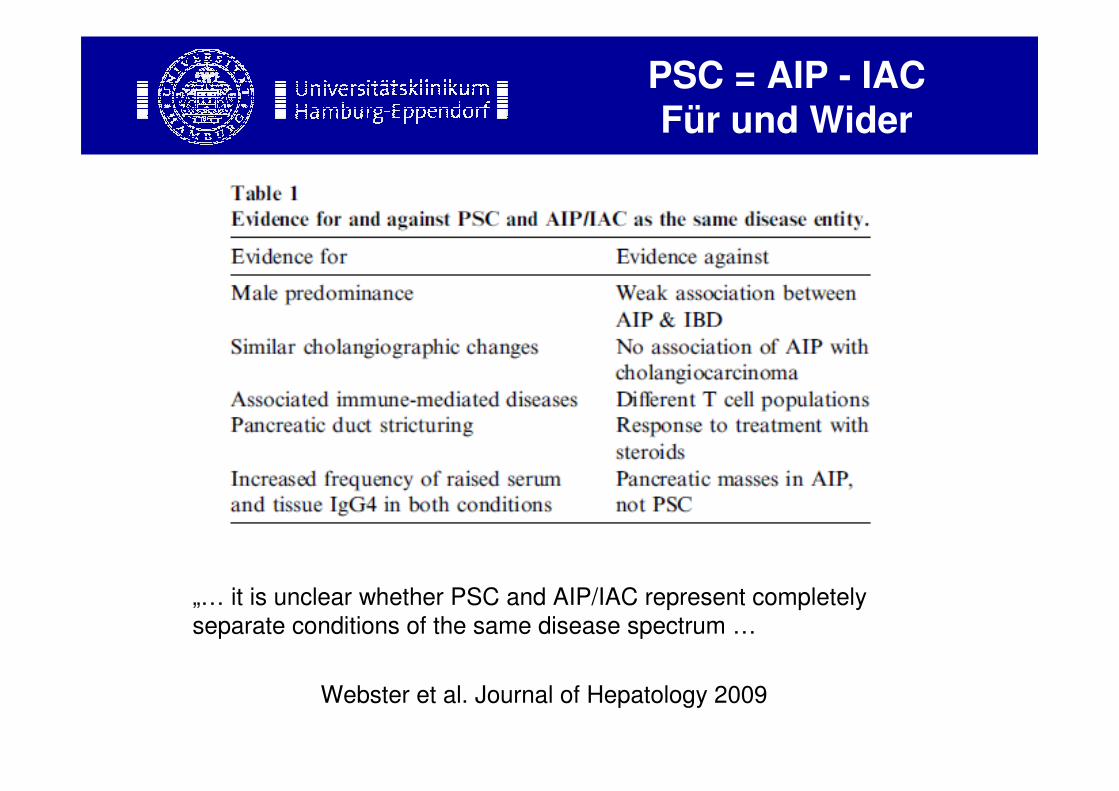
PSC = AIP - IACFür und Wider
B: nach 4
Wochen
Cortisontherapie Webster et al. Journal of Hepatology 2009
„… it is unclear whether PSC and AIP/IAC represent completely
separate conditions of the same disease spectrum …