Embed Size (px)
Citation preview

Improved melarsoprol therapy for
Trypanosoma brucei rhodesiense sleeping sickness
INAUGURALDISSERTATION
zur
Erlangung der Würde eines Doktors der Philosophie
Vorgelegt der
Philosophisch‐Naturwissenschaftlichen Fakultät
der Universität Basel
von
Irene Sylvie Küpfer
von Lauperswil/BE
April 2009

Genehmigt von der Philosophisch‐Naturwissenschaftlichen Fakultät auf Antrag von
Prof. Dr. Marcel Tanner, PD Dr. Christian Burri und Dr. Anne Moore
Basel, den 28. April 2009
Prof. Dr. Eberhard Parlow
Dekan

Table of contents
Table of Contents List of Abbreviations .................................................................................................................1 Acknowledgements .................................................................................................................. 3 Summary................................................................................................................................... 5 Zusammenfassung ................................................................................................................... 7 Chapter 1 .................................................................................................................................. 11 General Introduction .............................................................................................................. 11
Human African Trypanosomiasis (HAT).......................................................................................... 12 Epidemiology................................................................................................................................................. 12 Epidemiology of T.b. gambiense HAT versus T.b. rhodesiense HAT.......................................................... 14 Implications of the potential overlap of disease distribution areas.......................................................... 20
Clinical presentation ......................................................................................................................... 20 Control measures................................................................................................................................22
African and colonial control measures....................................................................................................... 22 Current control measures............................................................................................................................ 23
Diagnosis .............................................................................................................................................25 Treatment............................................................................................................................................27
First stage treatment.................................................................................................................................... 28 Second stage treatment ............................................................................................................................... 29 IMPAMEL – improved application of melarsoprol ....................................................................................... 34
Justification and goals ........................................................................................................................35 Goals ............................................................................................................................................................. 36
References .......................................................................................................................................... 38 Chapter 2..................................................................................................................................43 Safety and efficacy of the 10‐day melarsoprol schedule in the..............................................43 treatment of second stage rhodesiense sleeping sickness....................................................43
Abstract .............................................................................................................................................. 44 Methods.............................................................................................................................................. 48
Study design ................................................................................................................................................. 48 Results .................................................................................................................................................52
Proof‐of‐concept trial .................................................................................................................................. 52 Utilization study .......................................................................................................................................... 54 Comparison trial data ‐ historic data.......................................................................................................... 57
Discussion .......................................................................................................................................... 59 References .......................................................................................................................................... 65
Chapter 3 ................................................................................................................................. 67 Molecular characterization of trypanosomes from clinical trial patients in Uganda and Tanzania ................................................................................................................................. 67
Abstract .............................................................................................................................................. 68 Introduction....................................................................................................................................... 69

Materials and methods...................................................................................................................... 70 Study Sites.....................................................................................................................................................70 Study conduct and study population ..........................................................................................................70 Sample collection and DNA preparation .....................................................................................................71 Loop Mediated Isothermal Amplification (LAMP) of the SRA gene and the Random Insertion Mobile Element (RIME)............................................................................................................................................72
Results .................................................................................................................................................72 Discussion ...........................................................................................................................................73 References .......................................................................................................................................... 79
Chapter 4 ................................................................................................................................. 81 Clinical presentation of T.b. rhodesiense sleeping sickness in second stage patients from Tanzania and Uganda ............................................................................................................. 81
Abstract .............................................................................................................................................. 82 Introduction....................................................................................................................................... 82 Materials and Methods ..................................................................................................................... 84 Results ................................................................................................................................................ 85 Discussion .......................................................................................................................................... 89 References .......................................................................................................................................... 94
Chapter 5 .................................................................................................................................97 Reflections on clinical research in sub‐Saharan Africa ........................................................97
Abstract .............................................................................................................................................. 98 Introduction....................................................................................................................................... 99 Creating and maintaining a pipeline of new interventions against neglected tropical diseases 100
Neglected tropical diseases........................................................................................................................ 100 The new landscape after the year 2000..................................................................................................... 100 Searching for new medical interventions against neglected tropical diseases........................................ 101 Alternative business models for R&D in tropical diseases....................................................................... 102 Persistent and emerging complexities ‐ intellectual property rights.......................................................103 Capacity building........................................................................................................................................ 104
The conduct of clinical trials in sub‐Saharan Africa...................................................................... 106 Ethics ........................................................................................................................................................... 106 Ethics committees ...................................................................................................................................... 107 Informed consent and assent..................................................................................................................... 108 Indemnities and undue inducement......................................................................................................... 109 Publication of results and trial registration.............................................................................................. 109 Implementation and conduct of trials in resource‐limited environments.............................................. 110
Access and delivery............................................................................................................................ 113 Post marketing studies and pharmacovigilance........................................................................................ 113 Access ........................................................................................................................................................... 113
The way forward ................................................................................................................................ 114 References ..........................................................................................................................................116

Table of contents
Chapter 6.................................................................................................................................119 Discussion...............................................................................................................................119
Access to patients ............................................................................................................................. 120 Issues concerning the study design................................................................................................. 122 IMPAMEL III – study design............................................................................................................... 123 Safety ................................................................................................................................................. 124 Suramin pre‐treatment .................................................................................................................... 124 Efficacy .............................................................................................................................................. 125 Historic controls ............................................................................................................................... 129 Serious adverse events (SAEs) and case management.................................................................... 131 Case management .............................................................................................................................133 Public health challenges in the control of T.b. rhodesiense HAT ..................................................135 The potential overlap of T.b. gambiense and T.b. rhodesiense in Uganda.................................... 136 IMPAMEL III: from innovation to validation to application............................................................ 136 Conclusions....................................................................................................................................... 139 References ......................................................................................................................................... 140
Appendix 1.............................................................................................................................. 145 IMPAMEL III........................................................................................................................................ 145 Case Report Form (CRF) ‐ Utilization Study.................................................................................. 145
Appendix 2 ..............................................................................................................................161 IMPAMEL III.........................................................................................................................................161 Patient information and informed consent ‐ Tanzania ..................................................................161 English................................................................................................................................................161
Appendix 3 ............................................................................................................................. 169 IMPAMEL III........................................................................................................................................ 169 Patient information and informed consent ‐ Tanzania ................................................................. 169 Kiswahili ............................................................................................................................................ 169
Curriculum vitae ................................................................................................................... 179

Abbreviations
1
List of Abbreviations
BBB Blood Brain Barrier
BMI Body Mass Index
CATT Card Agglutination Test
CDC Centers for Disease Control and Prevention
CDM Clinical Data Management
CI Confidence Interval
CNS Central Nervous System
CRF Case Report Form
CSF Cerebrospinal Fluid
DALY Disability Adjusted Life Years
DNA Deoxyribonucleic Acid
DNDi Drugs for Neglected Diseases Initative
DSS Demographic Surveillance System
EDCTP European & Developing Countries Clinical Trial Partnership
ES Encephalopathic Syndrome
EKBB Ethikomission beider Basel / Ethics committee of both cantons of Basel
EMEA European Medicines Agency
FDA Food and Drug Administration
GCP Good Clinical Practice
GFATM Global Fund to Fight AIDS, Tuberculosis and Malaria
HLA Human Leukocyte Antigen System
IPPM Intellectual Property Protection Mechanism
ISCTRC International Scientific Committee for Trypanosomiasis Research and Control
IDP’s Internally Displaced People
i.v. Intravenous
LAMP Loop Mediated Isothermal Amplification
LIRI Livestock Health Research Institute, Uganda
LP Lumbar puncture

2
HAT Human African Trypanosomiasis
MMV Medicines for Malaria Venture
MoH Ministry of Health
MSF Médecins sans Frontières/Doctors without Borders
NIH National Institutes of Health
NIMR National Institute for Medical Research (Tanzania)
NGO Non‐governmental Organization
PATTEC Pan African Tsetse and Trypanosomiasis Eradication Campaign
PABIN Pan‐African Bioethics Initiative
PCR Polymerase Chain Reaction
PDP Product Development Partnership
p.o. per os
PPP Public Private Partnership
R&D Research and Development
RIME Random Insertion Mobile Element
SAB Scientific Advisory Board
SARETI South African Research Ethics Training Initiative
SIDCER Strategic Initiative for Developing Capacity in Ethical Review
SRA‐gene Serum‐resistance‐associated gene
SS Sleeping Sickness
STI Swiss Tropical Institute
USD US Dollar
WBC White blood cells (leucocytes)
WHO World Health Organization

Acknowledgements
3
Acknowledgements
I am greatly indebted to all the people who have accompanied me during my PhD as mentors,
scientists, colleagues, friends and family. Their contributions to this work are gratefully
acknowledged.
I am deeply thankful to my supervisor PD. Dr. Christian Burri. I profited tremendously from his
experience and skills and I particularly thank him for his tireless support in scientific thinking and
writing. I highly appreciate the loyalty and humor he shows to the entire team. Merci!
I would like to thank Prof. Marcel Tanner (Director STI) for his support and interest as well as for
taking the role of the faculty representative. I thank Prof. Reto Brun for his support and acting as
an expert on my thesis committee and Prof. Jürg Utzinger for his interest and inputs at various
stages of my thesis.
Special thanks go to Dr. Anne Moore for her participation on the safety advisory board as well as
her role as my co‐referee. I thank all the other members of the safety advisory board for valuable
inputs and guidance. Special thanks go to Prof. Martin Schumacher for helping us to overcome
the challenges of the study design and analysis.
I am very grateful to Dr. Johannes Blum, for his role as principle investigator, the valuable
discussions on sleeping sickness, his expertise and support.
I am enormously thankful to Dr. Caecilia Schmid, for her vital role as my co‐supervisor, her help
during my field work and her friendship. I thank you for the all the good times and hope more are
coming!
In Uganda, my sincerest thanks go to Dr. Abbas Kakembo. He has continuously supported me
and taught me so much about sleeping sickness and the African culture. I thank Dr. Mpairwe
Allan for his professional work and the enjoyable collaboration as well as for all the good times we
had. I greatly acknowledge the work of Dr. Andrew Edielu and his support for the project. Special
thanks go to Betty Akello for all her contributions to the project and especially for her help in
reviewing the historic patient data and the patient follow‐up. Apoyo Betty!
In Tanzania, I deeply acknowledge the contributions and support of Dr. Stafford Kibona. I
enjoyed our stays in the field and I am grateful for all his help. Asante sana! Special thanks go to
Dr. Lucas Matemba for his contributions to the project and his help with the mapping. My
greatest and warmest thanks go to all the Sisters in Kaliua. Sister Emma was my mentor in so
many aspects of work and life. I am very grateful for knowing her and working with her as well as
for our friendship. I thank Sister Bernadetta, Catharina, Theresfora and Bibi who made me feel so
comfortable and for all the unforgettable moments we shared. My sincerest thanks go to Maria

4
Charles for her constant dedication to the project and her professional way of working. Asante
sana dada!
I acknowledge all the nurses who looked so well after the patients, especially when situations
became serious, their care was always reliable. My sincerest thanks go to all the laboratory
personnel for their valuable and essential work. Thank you!
I want to express my respect and gratitude to all the patients and their families who participated
in the trials. Also I thank all the local leaders and community health workers who supported our
program activities. I am very grateful to have met all of you.
I thank Dr. Pere Simarro (WHO) and Dr. Jose Ramon Franco (WHO) for their valuable inputs as
well as for the supply of the study drugs.
I thank the Swiss Tropical Institute and the Swiss Agency for Development and Cooperation
(SDC) (grant extension to 7F‐01977.02) for the funding of the project.
My very personal thanks go to the entire team of the Pharmaceutical Medicine Unit, STI, for all
the good times and the great team spirit. I thank Monique for all her administrative and personal
support, Bettina and Andrea for being such great office mates and friends, Hermann for his
humor and belief in me, Eric for all the good laughs, Gaby for the interesting talks about life,
Sonja for her kindness, Francoise for being so dear. I am very grateful to Patrick for his
professional and patient computer support. Thank you!
I thank all my colleagues at the STI for their support, interesting discussions and friendship.
Especially Nakul Chitnis, Michael Bretscher, Ricarda Windisch, Conny Pfeiffer, Stefan Dongus,
Joshua Yukich, Karin Gross, Bianca Plüss, Sandra Alba, Lukas Camenzind, Simon Schlumpf,
Dominique Forster and Laura Gosoniu for her help with the data analysis.
In my personal life I want to thank all my friends for their support, understanding and all the
good times we shared. Especially Natalie for all her patience, Ana for her cheerfulness, Evi for
being so close, Manuela, Yolanda, Rita, Sarah, Niels…. no one could wish for better friends. Merci!
I want to express my sincerest thanks to Christian for all his help, patience and humor. I am also
very grateful to Heike Seegebarth for all her understanding and guidance.
My deepest thanks go to Evelyne. I thank you for all you have done for me. You were my greatest
supporter and motivator. Merci für alles!
I want to thank my dear parents for their continuous support, for always being there for me and
for giving me the liberty to pursue my wishes. I would like to dedicate this thesis to you. Thank
you so much ‐ I love you*

Summary
5
Summary
Human African Trypanosomiasis (HAT) is a parasitic disease that occurs in a chronic form caused
by Trypanosoma brucei gambiense in Western and Central Africa, and an acute form caused by
Trypanosoma brucei rhodesiense in Eastern and Southern Africa.
The treatment of HAT is unsatisfactory; for over 50 years melarsoprol (Arsobal®) has been the only
drug active against both forms of the disease and the only drug available to treat second stage T.b.
rhodesiense infections. However, its use is hampered by high toxicity and lengthy and
complicated treatment schedules.
Melarsoprol therapy was substantially improved by the introduction of an abridged 10‐day
melarsoprol schedule in T.b. gambiense affected areas in 2003. The new schedule was based on
pharmacological investigations and was shown to be non‐inferior compared to the standard
regimens in the framework of the clinical trial programs IMPAMEL I & II (1997‐2004). A significant
reduction in overall hospitalization time from about 25 – 35 days to 13 days and a more economic
use of the drug made it favorable to the patients and the health system. Subsequently, the
conduct of the IMPAMEL III program in T.b. rhodesiense affected areas was declared a high priority
by the WHO.
The presented thesis aimed at a) the assessment of the safety and efficacy of the 10‐day
melarsoprol schedule in T.b. rhodesiense patients and b) the rationalization of the suramin pre‐
treatment prior to melarsoprol which is proposed to control adverse drug reactions, but which is
only partially implemented in East Africa.
The IMPAMEL III program consisted of the sequential conduct of a proof‐of‐concept trial and a
utilization study using historic controls as comparator. The trials were conducted in two
treatment centers in Tanzania and Uganda. Consenting patients with confirmed second stage T.b.
rhodesiense HAT and a minimum age of 6 years were eligible for participation. Pregnant as well as
unconscious or moribund patients were excluded from the trial. The primary outcome measures
were safety and efficacy at end of treatment. The secondary outcome measure was efficacy during
follow‐up after 3, 6 and 12 months. The studies were approved by the ethics committees in
Tanzania (National Institute for Medical Research/NIMR) and Uganda (Ministry of Health) and
the ethics committee of both cantons of Basel (EKBB), Switzerland.
In the proof‐of‐concept trial a total of 60 patients were enrolled into two consecutive subgroups
(2x15 in each center) of which only the first subgroup received the suramin pre‐treatment.
Suramin as well as steroids were administered according centre‐specific guidelines. In this trial,
the incidence of the encephalopathic syndrome (ES) was significantly higher in Uganda (20%)

6
than in Tanzania (3.3%, p=0.0444). Adverse events were more frequent in patients that received
suramin (63.3%) than in patients that were directly treated with melarsoprol (23.3%, p=0.0018).
Based on these results, the utilization study was designed as an extension to the arm of the proof‐
of‐concept trial without suramin. An additional 77 patients were enrolled and directly treated
with melarsoprol.
Final data analysis was performed on the pooled data set of all patients that were directly treated
with the 10‐day melarsoprol schedule (i.e. without suramin, n=107). These results were compared
to historic controls of patients treated during past two years in the same centers. The incidence of
ES in the trial population was 11.2% (CI 5‐17%) and 13% (CI 9‐17%) in the historic data. The
respective case fatality rates were 8.4% (CI 3‐13.8%) and 9.3% (CI 6‐12.6%). The historic data did
not allow any elucidation of the efficacy of the standard treatment regimens since systematic
follow‐up of patients was not routine. However, the efficacy of the 10‐day melarsoprol schedule
was highly satisfactory: all patients were free of parasites the day after treatment. 99% of the
patients eligible for follow‐up were considered clinically cured 6 months after discharge. The 12
months follow up is currently ongoing. Based on the follow‐up results of the proof‐of‐concept
trial no issues regarding treatment efficacy are expected.
Our results show that T.b. rhodesiense patients treated with the 10‐day melarsoprol schedule were
not subject to a higher incidence of serious adverse events (ES or death) than the historic controls
treated with the national regimens. The hospitalization time was reduced from an average of 29
days to 13 days (p<0.0001).
In a separate analysis we compared the clinical presentation of the disease in Ugandan and
Tanzanian patients as a wide spectrum of disease severity has been described for T.b. rhodesiense
HAT.
In an ancillary study, the molecular characterization of the trypanosomes confirmed that all
patients were infected with T.b. rhodesiense. The fear of an overlap in the T.b. gambiense and T.b.
rhodesiense disease distribution areas could not be confirmed in our study area.
On the basis of our trial experience we were able to write a review on clinical research in resource
limited settings. Minimal standards for sponsors and host countries were suggested in order to
ensure a trial conduct in compliance with international standards.

Zusammenfassung
7
Zusammenfassung
Die Humane Afrikanische Trypanosomiasis (HAT) ist eine parasitäre Krankheit, die sowohl in
einer chronischen als auch akuten Form vorkommt. Die chronische Form wird durch
Trypanosoma brucei gambiense verursacht und kommt in West‐ und Zentralafrikanischen
Gebieten vor. Trypanosoma brucei rhodesiense verursacht die akute Form der Krankheit, die
typischerweise in Ost‐ und Südafrika vorkommt.
Die Behandlung von HAT erweist sich als sehr unbefriedigend: seit über 50 Jahren wird
Melarsoprol (Arsobal®) als einziges wirksames Arzneimittel für die Behandlung beider
Krankheitsformen eingesetzt. Es ist bis heute das einzige erhältliche Medikament für die
Behandlung von T.b. rhodesiense Infektionen die bereits zum zweiten Krankheitsstadium
fortgeschritten sind. Eine hohe Toxizität, sowie langwierige und komplizierten
Behandlungsverfahren erschweren jedoch die Therapie.
Durch die die Einführung eines 10‐Tage‐Behandlungsschemas im Jahr 2003 ist die Melarsoprol
Therapie in T.b. gambiense betroffenen Gebieten wesentlich verbessert worden. Das neue Schema
basiert auf pharmakologischen Untersuchungen und wurde im Rahmen der klinischen
Studienprogramme IMPAMEL I & II (1997‐2004) untersucht und erwies sich als nicht
minderwertiger im Vergleich zu den Standardschemata. Die signifikante Herabsetzung der
Hospitalisierungsdauer von etwa 25 bis 35 Tage auf 13 Tage kommt den Patienten zugute und der
wirtschaftlichere Einsatz des Arzneimittels begünstigt das Gesundheitssystem. Als Folge wies die
World Health Organization (WHO) der Durchführung des IMPAMEL III Programms in T.b.
rhodesiense betroffenen Gebieten eine hohe Priorität zu.
Die vorliegende Doktorarbeit hatte zwei Ziele: 1) Die Bestimmung der Sicherheit und
Wirksamkeit des 10‐Tage‐Behandlungsschemas mit Melarsoprol bei Patienten die mit T.b.
rhodesiense infiziert sind; 2) Die Rationalisierung der Vorbehandlung mit Suramin, diese sollte
der Reduzierung von schweren Nebenwirkungen der Melarsoprol Therapie dienen, ist aber zum
heutigen Zeitpunkt nur teilweise in den nationalen Behandlungsschemata implementiert.
Das IMPAMEL III Programm bestand aus der sequentiellen Durchführung einer “Proof of
Concept” Studie und einer Anwendungsstudie. Als Vergleich dienten historische Patientendaten.
Die Studien wurden in zwei Behandlungszentren in Tansania und Uganda durchgeführt.
Patienten die eine Einwilligungserklärung unterschrieben, mindestens 6 Jahren alt waren und an
einer bestätigten T.b. rhodesiense Infektion litten, wurden zur Studienteilnahme zugelassen.
Schwangere, bewusstlose oder moribunde Patienten wurden von der Studie ausgeschlossen. Der
Therapieerfolg wurde zum einen anhand der Sicherheit und Wirksamkeit am Ende der

8
Behandlung erhoben sowie mit einem zusätzlichen Wirksamkeitsnachweis nach drei, sechs und
zwölf Monaten. Die Ethikkomissionen in Tansania (National Institute for Medical Research),
Uganda (Ministry of Health) sowie die Ethikkomission Beider Basel (Schweiz), genehmigten die
Durchführung der Studien.
Die “Proof of Concept” Studie umfasste 60 Patienten, unterteilt in zwei Untergruppen (2x15
Patienten pro Zentrum) von der nur eine mit Suramin vorbehandelt wurde. Suramin, sowie
Steroide, wurden nach zentrumspezifischen Richtlinien abgegeben. Das Auftreten des
enzephalopathischen Syndroms (ES) war in Uganda (20%) signifikant höher als in Tansania (3,3%,
p=0,0444). Zudem traten andere Nebenwirkungen vermehrt bei Patienten auf, welche Suramin
erhielten (63,3%) als bei Patienten, welche direkt mit Melarsoprol behandelt wurden (23,3%,
p=0,0018). Basierend auf diesen Ergebnissen wurde die Anwendungsstudie als eine Erweiterung
der suramin‐freien Untergruppe entworfen. Zusätzliche 77 Patienten wurden in die Studie
eingeschlossen und direkt mit melarsoprol behandelt.
Die endgültige Datenanalyse umfasste die Datensätze aller Patienten, die direkt mit dem 10‐Tage‐
Behandlungsschema behandelt wurden (n=107). Der Vergleich dieser Ergebnisse mit historischen
Datensätzen von Schlafkrankheitspatienten, die während der vorhergehenden zwei Jahre in
denselben Zentren behandelt wurden, ergab folgendes Bild: In der Studienpopulation trat ES in
11,2% (CI 5‐17%) der Fälle auf und in den historischen Daten wurde ES in 13% (CI 9‐17%) der Fälle
nachgewiesen. Die entsprechenden Mortalitätsraten in beiden Populationen betrugen 8,4% (CI 3‐
13,8%) beziehungsweise 9,3% (CI 6‐12,6%). Die historischen Daten gestatteten keine Beurteilung
bezüglich der Wirksamkeit der Standardbehandlungsschemata, da routinemässig keine
systematischen Nachkontrollen durchgeführt wurden. Die Wirksamkeit des 10‐Tage‐
Behandlungsschema mit Melarsoprol war äusserst zufriedenstellend: bei allen Patienten waren 24
Stunden nach Abschluss der Behandlung keine Tryoanosomen mehr nachzuweisen. 99% aller
Patienten, die entlassen wurden, galten sechs Monate später als klinisch geheilt. Die
zwölfmonatige Nachbeobachtung dauert zur Zeit dieser Berichterstattung noch an. Jedoch sind
aufgrund des Wirksamkeitsprofils der “Proof of Concept“ Studie keine Probleme bezüglich der
Wirksamkeit der Behandlung zu erwarten.
Im Vergleich zu den historischen Daten, die den Verlauf der Melarsoprol Therapie nach
nationalen Behandlungsschemata beschreiben, zeigen die vorliegenden Studienergebnisse, dass
schwerwiegende Nebenwirkungen (wie ES oder Tod) nicht häufiger auftreten, wenn die Patienten
mit dem 10‐Tage‐Schema behandelt wurden. Jedoch führt diese Behandlungsmethode zu einer
Verkürzung des Spitalaufenthalts von durchschnittlich 29 auf 13 Tage (p<0.0001).

Zusammenfassung
9
Da unterschiedliche Krankheitsgrade in Ostafrika beschrieben sind, haben wir in einer separaten
Analyse die Krankheitsbilder in Uganda und Tansania verglichen. Eine Zusatzstudie basierend auf
der molekularen Charakterisierung der Trypanosomen bestätigte, dass alle Patienten mit T.b.
rhodesiense infiziert waren und somit die Befürchtung einer Überlappung der
Distributionsgebiete von T.b. gambiense und T.b. rhodesiense in unserem Studiengebiet nicht
bestätigt werden konnte.
Basierend auf unserer Erfahrung in der Durchführung von klinischen Forschungsprogrammen in
Gebieten mit limitierten Resourcen, schrieben wir einen Bericht, der Mindestanforderungen an
Sponsoren und Studienländer (sog. host countries) definiert. Dies soll gewährleisten, dass die
klinische Forschung auch in diesen Gebieten internationalen Qualitätsnormen entspricht.

10

Introduction
11
Chapter 1
General Introduction
Cattle herders, Urambo District, Tanzania

Chapter 1
12
Human African Trypanosomiasis (HAT)
Epidemiology
Sleeping sickness is the name used to describe the human form of African trypanosomiasis
(Trypanosoma spp.), a protozoal parasitic disease that affects humans, livestock and many sylvatic
species in much of sub‐Saharan Africa (1). The disease is concentrated in poor and rural areas and
the socio‐economic impact is considered very high. The affected population suffers from
economic losses due to reduced workforce and family disruption (2). Furthermore, estimates of
the total losses due to trypanosomiasis range from 1.3 to 5 billion US$ depending on the
methodology used (3).
If only the incidence is considered, HAT appears to be a minor health problem compared to other
parasitic diseases. But in terms of disease burden expressed in DALYs (disability‐adjusted life
years), HAT ranks third of all parasitic diseases in sub‐Saharan Africa, just behind malaria and
helminths (4).
Classically, there are three subspecies of Trypanosoma brucei. Two subspecies (T.b. gambiense and
T.b. rhodesiense) are human pathogens and transmitted by the saliva of blood‐sucking tsetse flies
(Glossina spp.). T.b. gambiense and T.b. rhodesiense are stratified according to their geographical
location but are morphologically indistinguishable (5). Their occurrence is more or less separated
by the Great African Rift Valley: T.b. gambiense is found in West and Central Africa and T.b.
rhodesiense in East and South Africa.
In contrast to the genetically heterogeneous T.b. rhodesiense of East Africa, T.b. gambiense
exhibits very limited genetic variability. For T.b. rhodesiense, the serum‐resistance‐associated
(SRA) gene is ubiquitous and conserved (6, 7) and allows an unequivocal identification. Hence,
the SRA gene has gained central importance in the differentiation of the two parasites, which
used to be possible only by the analysis of isoenzymes and DNA characteristics. The phylogenetic
relationships between the T. brucei subspecies suggest two groups of T.b. gambiense parasites
(group 1 and 2) and non monophyly for T.b. rhodesiense. Recent findings suggest the genetic
variability of T.b. rhodesiense results from multiple and independent evolutions from T.b. brucei
(8).
A characteristic feature of the epidemiology of HAT is its highly focal distribution. Today, 36 out
of 53 African countries are affected with nearly 200 separate foci, and 60 million people are living
in areas where HAT might be potentially transmitted.

Introduction
13
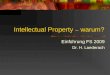
Figure 1: Reported foci for HAT (source: WHO 1998).
Also typical for the epidemiology of HAT are long periods of endemicity interspersed with
epidemics. The potential for the development of explosive epidemics is of high public health
importance (9). In the past, large scale HAT epidemics were fatal for many thousand people.
Between 1900 and 1920, Uganda experienced one of the most severe epidemics of sleeping
sickness ever recorded. In the Buganda region along the shores of Lake Victoria and its drainage
rivers, more than 200,000 people are believed to have died before the decline of the epidemic (10).
The history of sleeping sickness is characterized by such waves of epidemics, resurgences and
outbreaks. Nevertheless, the disease has been practically brought under control by the end of
colonial times. Interventions such as continuous disease surveillance, large‐scale campaigns of
active case search, vector control and depopulations of affected areas have proven to be effective
in reducing the prevalence and incidence of sleeping sickness. In the 1960s there was even a fair
chance of disease elimination. However, after independence, the priorities shifted and the
surveillance of sleeping sickness was neglected: national health authorities were not giving
attention to sleeping sickness control, and civil and political unrest as well as the lack of adequate
sources and competing national health priorities resulted in new epidemics, the recrudescence of
many old foci and the appearance of new ones (11). The prevalence rate of trypanosomiasis rose
again from 0.01 % of the population to 1‐2 %. In 1998, the number of prevalent cases per year was
estimated at 300’000 (12). In addition, there was also a dramatic lack of awareness about the
disease situation. The neglect of HAT control and surveillance also lead to the point where

Chapter 1
14
physical structures and human resources were no longer available (13) and it took a long time to
control the recrudescence. Increased control activities during the past 20 years have led to a
substantial reduction in the number of new cases reported: in 2004, 17’500 new cases were
reported, equivalent to an estimated 50’000 – 70’000 existing cases because of the significant
underreporting. In 2005, the International Scientific Council for Trypanosomiasis Research and
Control (ISCTRC) recommended that “WHO should launch an elimination program for sleeping
sickness and adopt strategies towards this goal and advocate all partners who have permanently
provided support to maintain their efforts and assistance” (14).
Epidemiology of T.b. gambiense HAT versus T.b. rhodesiense HAT
An accurate reflection of the magnitude of HAT is hampered; the rural areas are poorly covered
by national health services; less than 10% of the at‐risk population is under adequate surveillance
and there is a significant under reporting of new cases. The available epidemiological data on
HAT has to be recognized as an estimate of the real situation in the HAT affected areas.
All sub Saharan countries affected by HAT are categorized by the number of new cases reported
per year. Table 1 and table 2 summarize the data from the latest available epidemiological update
(WHO 2006) (14).
Table 2: Number of new cases reported per year in T.b. rhodesiense affected countries (WHO 2006)
50‐1500 cases Malawi, Uganda, Tanzania
Sporadically fewer than 50 cases Kenya, Mozambique, Rwanda, Zambia, Zimbabwe
Zero cases Botswana, Burundi, Ethiopia, Namibia, Swaziland
Table 1: Number of new cases reported per year in T.b. gambiense affected countries (WHO 2006)
More that 1500 cases Democratic Republic of Congo, Angola, Sudan
50‐1500 cases Central African Republic, Chad, Congo, Côte d’ Ivoire, Guinea, Uganda
Fewer than 50 cases Burkina Faso, Cameroon, Gabon, Equatorial Guinea, Nigeria
Zero cases (with surveillance activities) Benin, Ghana, Mali, Togo
Zero cases (no surveillance) Gambia, Guinea Bissau, Liberia, Niger, Senegal, Sierra Leone

Introduction
15
Over 90% of the reported HAT cases are due to T.b. gambiense (15). Currently most of those cases
originate from the Democratic Republic of Congo (DRC). In 2004, 97% of all reported cases were
T.b. gambiense infections and only 3% were T.b. rhodesiense infections (14). But the overall
decrease of reported HAT infections in the past 20 years has not been significant for T.b.
rhodesiense, indicating that the focus on the human reservoir alone is insufficient (14) for effective
disease control. T.b. rhodesiense is clearly the more neglected form of HAT. Disease awareness
and surveillance is very poor and limited to passive case detection in few health centres that have
the capacity to diagnose HAT. Not only the under reporting of new cases but also the under
detection of death related to HAT is believed to be very high. A deterministic model has been
developed to estimate the proportion of undetected T.b. rhodesiense cases in a given population
on the basis of knowledge of the early to late disease stage ratio (16). The data used for the design
of the under‐detection model were obtained from an area in Uganda with a relatively low
expected probability of under‐detection (17), as it had better health service and better
infrastructural components compared with other sleeping sickness areas in Africa. The model
estimated that with passive case detection, 20% of the first stage and 42% of the second stage
infections were reported and that for every reported death, 12 deaths went undetected. The model
was also applied for estimating the undiagnosed deaths that may have sought health care during a
HAT resurgence (2000–2002) in this same area and estimated that approximately 85% of the
patients who died undiagnosed, entered the health system at some stage, and that one‐third of
those, died undiagnosed. It would thus be expected that less‐developed areas would have an even
more alarming rate of under detection, and hence mortality. These estimates of deaths due to
HAT emphasize the magnitude of the burden of the disease, especially where it occurs in
epidemics in areas with poor surveillance (18).

Chapter 1
16
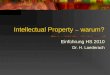
Figure 2: Distribution of HAT in sub Saharan Africa, by endemicity levels of the countries affected (© Map:
Source: WHO 2004).
The location of disease transmission and the transmission cycle differ for the two forms of HAT:
gambiense‐carrying tsetse live near water in predominantly riverine vegetation associated with
drainage lines, rivers and more permanent bodies of water such as lakes (19). These flies feed on
aquatic reptiles and with a possible exception of domestic pig; man is the only mammalian host
for T.b. gambiense. The cycle of transmission essentially involves man and tsetse (20). Since
Gambian HAT causes a chronic infection over a long period, people can function normally for
months while carrying the disease. If an infected person regularly access tsetse infested water
sources, over time, this person can infect a large number of flies who might then infect other
people (21).
The rhodesiense‐carrying tsetse are savannah species, “game flies”, ranging further from water and
feeding on wild and domestic animals. T.b. rhodesiense is a zoonotic disease and humans are
accidentals host in the transmission cycle, and rapidly killed. Because of the quick development of
the disease, infected people are soon incapacitated and resting at home. For T.b. rhodesiense HAT,
animals are the primary reservoir for the disease and transmission is usually from animals to
people (21). Men risk infection with T.b. rhodesiense through physical proximity to infected
������������� ��������������������������������������� ��������������� ����!!���������"�""�#���$������ �����������%�����
&����������"�������!"�"��'����������"��������"��"��������"�!�����������!��(����)��""�����*���(��������'���"�+��������������*���������� �����������%����������������������"����"��*���(������(,��������(,���(�����������*���"����������",������������������!���������*���"�*������"������������"-�����������"����!��"����"��������)�!������������"�*���'��������!�(�����(����*�������!��- .�� �����/-�0��������"��"�+�
���������������������� ������������������������ ��������������������������������������������������
� /�� 1�� 2��� 3���!��"
������������
������ �����
&�(����"�!��"�"4����"50����"56��!� ������!�6���!�

Introduction
17
livestock, farming and building on tsetse country or when passing through it as a traveller or a
hunter.
Situation in Tanzania
Rhodesiense sleeping sickness, which was first reported in the 1920s and 1930s, was endemic in
eight regions of Tanzania: Arusha, Kigoma, Lindi, Mbeya, Kagera, Rukwa, Ruvuma and Tabora. In
1929 a total of 2’129 cases were recorded in Kahama district. In 1939, 10 years after the original
outbreak, recrudescence occurred in the districts of Tabora and Kahama. This outbreak was
brought under control by re‐establishing the policy of preventing families from settling
themselves up in small villages scattered in the bush and by intensifying the campaign for the
diagnosis and treatment of cases.
The currently active foci of HAT are located in the poorest parts of the country. And
approximately 4 to 5 million people are at risk of infection, only 1% of these are under regular
surveillance. In the past 30 years, the number of new cases reported has risen above 500 per year
(22) which is certainly an under estimate. Transmission takes place in the three regions of Kigoma
(Kibondo and Kasulu districts), Tabora (Urambo districts) and Rukwa (Mpanda and Nkansi
districts). In those regions the health centres are sparse, some not accessible throughout the year
and many lack trained personnel, equipment and preparedness for sleeping sickness patient
management and diagnosis. Sporadically, cases are also observed in Serengeti National Park.
Especially the reports of tourists who got infected with T.b. rhodesiense during visits in Tanzanian
national parks (23) have drawn more attention to HAT and activated discussions about
interventions for disease control and surveillance (24).
As a consequence of the Great Lakes Crisis in the beginning of 1994, the International Federation
of Red Cross and Red Crescent Societies (IFRC) have established refugee camps in the regions of
Kasulu and Kigoma (1997). The Kigoma District received a massive influx of Congolese refugees
which are potentially infected with T.b. gambiense. With the ongoing civil movement, T.b.
gambiense could potentially be introduced in this region. The risk of such an overlap should be
carefully monitored.

Chapter 1
18
Figure 3: HAT endemic regions in Tanzania (source: NIMR Tabora, 2005).
Research and control of HAT in Tanzania are under the National Institute for Medical Research
(NIMR), Tabora Centre. The Tabora Research Centre is mandated to carry out, coordinate,
promote and document research and control of HAT in Tanzania. It is also mandated to
formulate priorities for HAT research and control as well as to monitor all aspects of sleeping
sickness in the country.
Situation in Uganda
Uganda is the only country affected by both forms of the disease; T.b. gambiense in the North‐
West and T.b. rhodesiense in the South‐East of the country. Three major epidemics of sleeping
sickness were recorded in south‐east Uganda since the 1890s (25). During the 1970s and 1980s
Uganda experienced extensive internal displacement of the rural population, illegal human and
cattle movements, growth of favourable tsetse habitats on cotton and coffee plantations, and a
collapse of sleeping sickness prevention and control methods. These events likely contributed to
increased human vector contact and sleeping sickness transmission. In 1976 a T.b. rhodesiense
outbreak was detected in the western Iganga district which was the beginning of an extensive
epidemic that spread throughout south‐eastern Uganda (26). The peak was between 1980 and
1988, with more than 4’000 new cases alone in 1986 (27). In 1998, first reports of local sleeping
sickness transmission were recorded in the Soroti district, a previously disease free area. During
four years prior to this outbreak, the cattle population in the district had grown by 660% as a

Introduction
19
consequence of the country wide cattle restocking projects, which were part of the national
poverty eradication action plan (PEAP). The cattle restocking activities were linked to the
introduction of the parasite: 50% of the traded cattle had originated from endemic sleeping
sickness areas (28). The disease has since spread to the adjacent districts of Kaberamaido, Kumi
and Lira which are more remote areas and were not equipped to handle the situation. These areas
had also extensively suffered from civil unrest due to the presence of rebels from the Lord
Resistance Army (LRA).
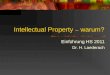
Due to the growing closeness of the two disease foci (see figure 4) and continuous movement of
the livestock reservoir, a potential overlap of the two yet distinct diseases areas has become very
likely and must be monitored carefully (29).
Figure 4: Sequential maps of HAT affected areas, Uganda (source: Picozzi et al., 2005).
In the 1990, Uganda has established the Control Council for Trypanosomiasis under the Ministry
of Agriculture. It is responsible for all activities in animal and human Trypanosomiasis. The
executive body is the Coordinating Office for Control of Trypanosomiasis in Uganda / COCTU
which coordinates all research and control activity in the country.

Chapter 1
20
Implications of the potential overlap of disease distribution areas
Any convergence of the currently geographically distinct distributions of T.b. rhodesiense and T.b.
gambiense HAT will have important implications for patient care and national control policy (30).
The treatment of sleeping sickness differs in the two forms of the disease and the infective
subspecies directs the choice of drugs. So far, the identification of the infective strain is not
possible under field conditions, only modern laboratories are able to perform the required PCR
analysis. Proper diagnosis and treatment of the patients will impose a major public health issue to
the countries at risk of an overlap in disease distribution areas. A close monitoring of the situation
is crucial; relevant strategies to prevent the further spread of the disease and the likely overlap of
the two disease zones should be urgently implemented.
Recent findings demonstrate that the disjunct distribution of the Trypanosoma parasite in
Uganda can not be explained by a genetic heterogeneity of the vectors that theoretically could be
responsible for an incompatibility between vector populations and parasite (31). Further, the
genetic recombination of different parasite strains was successful under laboratory conditions:
two clones of Trypansoma brucei were successfully crossed indicating that the genetic
recombination between trypanosome populations transmitted within the same epidemic might
occur also under natural conditions (32).
Clinical presentation
The clinical presentation of T.b. gambiense and T.b. rhodesiense HAT is remarkably different. The
highly virulent T.b. rhodesiense causes a precipitated evolution of the disease and presents as an
acute illness that is fatal within weeks or months if left untreated (33). T.b. gambiense is a chronic
disease with elusive and mild symptoms for months, and insidious evolution towards the nervous
stage (34). A wide spectrum of disease severity has been described for T.b. rhodesiense HAT
ranging from a chronic disease pattern in southern countries of East Africa with existing reports
of asymptomatic carriers (35) to an increase in virulence towards the north (36). Even though
those differences were already described more than 60 years ago (37) there is a lack of data about
those differences.
The onset and the first stage of both forms of the disease are similar: a sign of infection may be
the development of a lesion at the site of the infective bite. Parasites proliferate and, occasionally,
lead to a nodule or ulcer called a trypanosomal chancre. This trypanosomal chancre is commonly
seen in white but rarely in black populations (20). Clinical symptoms commence by an

Introduction
21
uncharacteristic general malaise. Fever, headache, joint pains, transient oedema, pruritus,
splenomegaly and lymphadenopathy may accompany the so‐called first or haemolymphatic stage
of HAT. Typical for T.b. gambiense HAT is the so called Winterbottom sign; enlarged, painless,
rubbery cervical lymph nodes in the posterior cervical triangle. Typical for T.b. rhodesiense HAT
are signs of myocardial involvement. In general it is very difficult to distinguish such symptoms
from other tropical fevers, such as malaria, bacterial meningitis or enteric fever.
With the parasite’s penetration into the central nervous system patients enter the second or
meningo‐encephalitic stage which ends fatal if left untreated. In the second stage of the disease
neuropsychiatric signs and symptoms occur: severe endocrinological and mental disturbances,
such as impotence, infertility, amenorrhea, delirium, mania, paranoia, schizoid attacks, aggressive
behaviour and severe motor problems are the main signs. Compared to the T.b. gambiense, less
demarcation between first and second stage illness is observed in T.b. rhodesiense. The CNS
involvement in T.b. rhodesiense infections can be clinically limited to drowsiness and tremor (38).
In T.b. gambiense infections, the interval between the start of the infection and the start of the
second stage is in the order of months or years (38) Recently, the mean time to reach the second
stage has been estimated at over one year and the mean time to death at almost 3 years (39). The
study of the duration of symptoms in T.b. rhodesiense showed that the disease progressed to the
stage of central nervous system involvement between three weeks to two months of infection and
that most (> 80%) deaths occurred within six months of illness (17), often due to cardiac failure or
secondary infections.
Recently, the neuropathogenesis of second stage HAT has been reviewed. Clinical features can be
grouped into categories such as psychiatric, motor, sensory and sleep abnormalities (33). The
more advanced the disease the more deregulations of the 24‐h distribution of the sleep‐wake
pattern can be observed. An alteration of the sleep structure, with frequent sleep onset rapid eye
movement (REM) periods (SOREMPs) is seen in stage II patients (40). The fragmented sleep
patterns are perceived as daytime somnolence and nocturnal insomnia. The name of the disease is
resulting from this observation ‐ formerly also known as the Negro lethargy.
Until today, the underlying mechanisms of CNS invasion are not known in detail. Frequently
observed is meningoencephalitis. The meninges are infiltrated with lymphocytes, plasma cells and
occasional morular (Mott) cells. The inflammatory cell infiltrate extends along the Virchow‐Robin
spaces into the substance of the brain producing the characteristic picture of perivascular cuffing
(41). An immune response is certainly involved in the process; increased levels of antibodies can
be detected and thus supports the inflammatory process. Further, the number of white blood cells
(WBC) as well as the protein content is elevated in the cerebrospinal fluid (CSF).

Chapter 1
22
Even though many hypotheses are debated, there is no detailed description of the process of CNS
invasion and its direct consequences.
The ability of T. brucei ssp. to survive free in blood is due to its remarkable degree of antigenic
variation. The surface coat of densely packed glycoproteins differentiated already when specific
antibodies follow up. Thus leads to misdirection of the immune response and gradual exhaustion
of the patient’s immune system.
Control measures
African and colonial control measures
Traditionally, trypanosomiasis was controlled through bush clearing, game control, settlement
patterns and careful movement of livestock and protective ointments for animals. Pastoralists in
East Africa had sophisticated understanding of tsetse environments; herders in western Narok,
Kenya, when expanding into fly‐infested bush, first grazed goats in an area to prepare the way for
the final reoccupation by cattle (21).
Colonial powers were very concerned by epidemics of the human disease and the chronic loss of
livestock impeding both transport and agriculture (42). The first sleeping sickness mission by the
French government to French Equatorial Africa in 1906, was sent because “the economic future of
the Congo is tied to the question of human trypanosomiasis” (Congo Service de santé militaire by
Martin, Leboeuf, Roubaud, 1906‐08).
Colonial powers implemented a combination of targeting trypanosomes, tsetse and people
through biological and medical control. Major programs for tsetse control were focused on bush‐
clearing (to eliminate tsetse resting sites), wild game culling (to reduce the parasite reservoirs and
host availability for tsetse), and insecticide spraying of tsetse resting sites. Large‐scale
depopulations of tsetse infested areas were common only in East Africa. Medical interventions
emphasized on the elimination of trypanosomes in people through medical examinations, the
isolation of patients and drug treatment. Colonial doctors carried out patient observation,
examinations, segregations and drug testing in sleeping sickness camps, clinics and hospitals. The
medical control required mobile teams feeling lymph nodes, testing blood and sending infected
patients to quarantined medical facilities. A further attempt in effective disease control was
prophylactic treatment with pentamidine based on 6‐monthyl injections (43).

Introduction
23
The successes of the sum of those control measures were reflected in decreasing numbers of
patients and disease elimination was almost achieved in the 1960ies. The rarity of HAT cases, and
a decline in awareness of how the disease could return, led to a lack of interest in disease
surveillance. Over time the disease slowly returned, and some thirty years later, flare‐ups were
observed throughout past endemic areas (figure 5) (44).
Figure 5: New cases of sleeping sickness reported for all Africa between 1927 and 1997 (source: Simarro,
2008).
Current control measures
Over the past 20 years new and more sophisticated tools for trypanosomiasis control have been
developed compared to the tools available when sleeping sickness was almost eliminated. These
advantages contrast with the present epidemiological situation in which the disease is increasing
because of a number of socio economic and political factors (15).
HAT control relies on two principles: reduction of the human‐fly contact through vector control
and the reduction of the parasite reservoir through case detection and treatment. For T.b.
rhodesiense affected areas, the control of trypanosome infections in the animal reservoir is crucial:
in endemic areas, the incidence of T.b. rhodesiense in cattle is up to 20% (45) and the dynamics of
transmission during the 1988 to 1990 epidemic in Tororo, Uganda showed that tsetse were 5 times
more likely to pick up human infective parasites from cattle than from humans (46). The mass
treatment of cattle has been advocated as an effective strategy for control of the spread of the

Chapter 1
24
disease (28) but this approach can be hindered by the emergence of cross resistant trypanosomes
between the drugs in use to treat humans and animals (47). An example of current risks is the
extensive human and livestock trafficking between Uganda and southern Sudan that could
possibly lead to the introduction of T.b. rhodesiense in southern Sudan.
Tsetse control
Today, vector control strategies exist of series of control projects following administratively‐
defined boundaries rather than covering biologically‐relevant areas (48). The destruction of the
vector is possible through insecticide ground spraying and insecticide‐impregnated traps and
screens. Because of the colour and the shape of the traps, the tsetse is attracted and hold captive.
Early traps have been barely effective but improved biconical, monoconical and pyramidal traps,
also combined with olfactory baits, have improved trap efficacy. Further the development of
simple screens, impregnated with insecticides, that kill tsetse flies that come in contact with them
allowed a more wide spread use. Traps and screens have replaced insecticide spraying; they are
effective, environmentally friendly and also suitable for use by the communities themselves. The
number of traps and/or screens required for a particular location depends on the type of
vegetation and the frequency and intensity of human‐fly contact (15). Such vector control
programs are technically successful whilst in operation but unsustainable once the formal project
reached its endpoint.
Rather different was the tsetse eradication project on the island of Zanzibar sponsored by the
International Atomic Energy Agency (IAEA). Although designed as a test‐bed for tsetse control by
large‐scale release of laboratory‐reared radiation‐ sterilized male tsetse (SIT) – and so proving
rather costly – the project succeeded in complete elimination of tsetse (Glossina austeni) from the
island (49) raising the question of whether or not similar tsetse elimination might be possible on
mainland Africa.
The idea of a Pan‐African initiative against tsetse and trypanosomiasis was discussed and
recommended at the 25th ISCTRC (International Scientific Council for Trypanosomiasis Research
and Control) in Mombasa, Kenya, in October, 1999. The recommendation was presented to the
36th summit of the African Union (AU) in Lomé, July 2000. The Heads of State and Government
passed a resolution recognizing the seriousness of the tsetse and trypanosomiasis problem, and
calling on member states "to act collectively… to render Africa tsetse‐free within the shortest time
possible". With this mandate, the AU set up the Pan African Tsetse and Trypanosomiasis
Eradication Campaign (PATTEC), which is now an integral part of the AU Commission for Rural
Development. PATTEC was formally launched at the 26th ISCTRC meeting in Ouagadougou in

Introduction
25
October 2001. Within PATTEC; the responsibilities are segmented in human health (WHO),
animal health (FAO) and vector control (IAEA).
Case detection
Case detection has been the corner stone of Gambian trypanosomiasis control since the beginning
of the 20th century (15). Today, case finding surveys are only carried out in T.b. gambiense areas.
Infected cases may remain asymptomatic for many months and specialized case finding teams are
set up to detect patients while they are still healthy. To reach remote villages, achieve high
community participation and examine large numbers of people is logistically difficult, requires
skilled man power and is very expensive.
In east Africa, there is not active case detection. The limited number of patients and the lack of
adequate screening tests make active case search highly cost ineffective.
Once patients are identified, definitive diagnosis is required and these patients need to be treated.
Diagnosis
The clinical profile of HAT is too diffuse to allow for a direct differential diagnosis. Accurate
diagnosis is dependent on specific and sensitive methods which are still lacking today and
therefore, only the proof of the parasites presence in blood, lymph nodes and/or in the
cerebrospinal fluid can confirm the infection with trypanosomes.
T.b. gambiense HAT can be serologically diagnosed using the CATT test (Card Agglutination Test)
(50) followed by microscopic confirmation of the parasite in blood and/or lymph. The CATT test
detects specific trypanosomal antigens but the test lacks necessary sensitivity and specificity for a
proof of the disease and is therefore only used for screening. The CATT is very useful for the mass
screening of populations for T.b. gambiense area, but is not applicable in the detection of T.b.
rhodesiense (51). The diagnosis of T.b. rhodesiense has to entirely rely on microscopy. The
sensitivity of this method depends on the level of parasitaemia and the technicians’ experience.
An exception is the successful use of the CATT test in Malawi. This indicates closer genetic
similarities between local T.b. rhodesiense stains in Malawi with T.b. gambiense.
The standard technique to find trypanosomes is to do thick blood smears. Staining is required
and it is important to do it repetitively. Each blood smear has to be examined for at least 10
minutes. A frequently used concentration method is the microhaematocrit centrifugation
technique (m‐HCT) (52). After high speed centrifugation (haematocrit centrifugation) the
trypanosomes concentrate on the “buffy coat”, the layer of white blood cells, between the serum

Chapter 1
26
and erythrocytes. Microscopic examination at low magnification is done to see mobile
trypanosomes. Moving microfilaria can obscure the smaller trypanosomes. This method is widely
used in the field and also known as the Woo‐test. In the case of high suspicion without being able
to detect the trypanosome, the mini anion exchange centrifugation technique (mAECT) can be an
alternative (53). By anion chromatography the trypanosomes get separated from venous blood.
mAECT asks for tedious manipulation but has proved to be more sensitive than other
parasitological methods of diagnosis. As a laboratory method it is only in use in centres with a
high technical standard. A kit has been developed for field use (12) but due to high costs it never
became an analytical standard.
Iit is estimated that 20 to 30% of patients are missed by the standard parasitological techniques
(54).
A new technique in use for the detection of T.b. rhodesiense is the sensitive and selective
polymerase chain reaction (PCR) method that amplifies the SRA (serum resistance associated)
gene. This gene is found in T.b. rhodesiense strains only and it directly correlates to human
infectivity (55). The SRA gene is a low‐copy gene and therefore PCR is inadequate to amplify this
target reliably in clinical samples without resources to parasite multiplication in mice. Recently,
the loop‐mediated isothermal amplification (LAMP) of DNA has been developed. The LAMP test
is carried out under isothermal conditions of 60–65∘C and produces a large amount of DNA (56).
LAMP was successfully used to detect T.b. rhodesiense with a sensitivity of one trypanosome/ml
blood and the results can be read by visual observation of colour change. The amplification of
DNA is possible by the use of a water bath only which makes the use of LAMP an efficient and
robust test in the field. The availability of this test would finally allow that molecular diagnosis for
case detection and confirmation of cure can become feasible in regions endemic for T.b.
rhodesiense HAT. Currently, the validation process of the test is ongoing and the Foundation for
Innovative New Diagnostics (FIND) is planning the production of a diagnostic kit that is suitable
for the use in the field.
Once the presence of trypanosomes in blood and/or lymph is confirmed, a lumbar puncture has
to follow for stage determination. Correct stage determination is crucial as second stage
treatment is risky and the patients can suffer from serious adverse drug reactions. Either the
presence of trypanosomes and/or an increase of the leukocyte count (≥ 5 cells/mm3) in the
cerebrospinal fluid indicate the second stage. Increased IgM values in CSF were found to be
another marker for stage determination (57). Earlier, protein content in the CSF above 25 mg per

Introduction
27
100 ml (method of Siccard & Cantaloube) also indicted the second stage of the disease. With time
it was shown that the involvement of the CNS should be based on the WBC count only (58) as it is
more reliable than the protein determination (12).
Better tools for stage determination are urgently needed. The invasiveness of the lumbar puncture
is risky, even more under field conditions and exposes patients to other risks, such as bacterial
infections, epidural bleeding or trauma to the spinal chord. Also, the LP is not well accepted by
the local population who often see it as a threat and associate other risks like infertility and
disease transmission with it (59, 60).
Part of the Foundation for Innovative New Diagnostics (FIND) portfolio is to develop new
diagnostic tools for first and second stage HAT. FIND has contracted WHO for the establishment
of a HAT specimen bank. Throughout sub Saharan Africa specimens of saliva, urine, plasma and
CSF are collected and shipped to the Institute Pasteur, Paris, France where the specimen bank is
physically located. Research groups can access those samples after an approval of request by the
joint committee of FIND/WHO and use those samples for the development of sensitive and
specific diagnostic tools.
Treatment
Treatment of HAT is very unsatisfactory; there is no existing vaccination and only a few effective
drugs are available. Whereas new drugs for single‐dose oral treatment of many parasitic diseases
are obtainable, treatment of sleeping sickness mainly relies on drugs developed before 1950 which
are administered parenterally in repeated doses. These drugs cause many adverse drug reactions,
some of which can be even fatal. New and safe drugs for the treatment of HAT are urgently
needed. At a certain point pharmaceutical companies producing anti‐trypanosomal drugs decided
on the cessation of the production. Only through substantial efforts by WHO and the médecins
sans frontièrs (MSF) campaign to essential medicines group, contracts could be signed with and
Aventis (2001) Bayer (2002). Today, both companies supply the drugs free of charge, in the
quantities requested by the WHO.

Chapter 1
28
First stage treatment
For first stage treatment, two drugs are in use: pentamidine, an aromatic diamidine, for T.b.
gambiense infections and suramin, polysulphonated naphtylurea, for T.b. rhodesiense infections.
Pentamidine (Pentacarinat®) has a long history of clinical use. Since the beginning of the 1940’s it
has been used to treat African Trypanosomiasis and Leishmaniasis. The development of
pentamidine stems from the research on synthalin, a potent hypoglycaemic agent that exhibited
significant trypanocidal activity. Pentamidine is administered as an intramuscular injection of
4mg of pentamidine isethionate per kg bodyweight once daily for 7–10 days. Main adverse
reactions include hypotension, renal and hepatic toxicity, pancreatitis and cardiac dysfunction
(61). The mode of action is not fully understood. In‐vitro studies indicate that pentamidine
interferes with nuclear metabolism causing inhibition of DNA, RNA, phospholipids and proteins
synthesis. Pentamidine has been widely employed for chemoprophylaxis, for instance in the
former Belgian Congo (62). Applied as an intramuscular injection of 4mg/kg it was assumed to
protect against Trypanosoma infection for several months. This practice was abandonment since
the dose is sub‐curative and may mask an underlying infection. Moreover, the prophylactic use
has provoked resistance in several areas. Still, it is effective to treat first stage trypanosomiasis and
is used even though it is toxic and inactive when given orally.
Suramin (Bayer 205, Germanin, Antipyrol, Belganyl, Fourneau 309, Moranyl, naphuride, naginin,
naganol), was developed in Germany in 1916. Its development was based on the observation that
the dyestuffs trypan red, trypan blue, and afridol violet cured trypanosomiasis in mice. In 1920,
suramin was introduced into clinical use for treatment of African river blindness and early stage
human African trypanosomiasis. It is administered intravenously as suramin sodium at a dosage
of 20mg/kg every 5 or 7 days to a maximum of 5 doses. It is normal clinical practice to start with a
small dose to assess the patient’s tolerance of the drug. Therefore, a test dose of 5mg per kg of
bodyweight is given on the first day, followed by 20mg per kg of body weight (up to am maximum
of 1g) on days 3, 10, 17, 27, and 31 (12). The once a week administration schedule is sufficient, since
suramin’s plasma half life is reported to be 41‐78 days (63) or in onchocerciasis patients even 92
days (64). Suramin is a symmetrical, polysulphonated polyaromatic urea, highly charged at the
physiological pH and does not cross the BBB. After intravenous administration it circulates in the
blood in tight association with serum albumin and low density lipoproteins. Suramin accumulates
only slowly in trypanosomes and uptake occurs probably by receptor mediated endocytosis bound
to the low‐density lipoprotein. The different drug‐uptake dynamics of host and parasite are
believed to form the basis of the dissimilar toxicity profiles. Suramin is deposited in the renal
tubes and should not be administered to patients with renal disease. Urine should be checked

Introduction
29
before and during treatment for proteinuria. The major adverse drug reactions are proteinuria,
reversible liver damage, and nephrotoxicity with renal impairment. But also fever, joint pain,
pruritus, exfoliative dermatitis, haemolytic anaemia, agranulocytosis, jaundice, hepatitis and
diarrhea have been observed.
Since 1920 suramin has been tested against various other indications such as cancer,
cardiovascular diseases, autoimmune hepatitis, incontinence and heartburn. However, treatment
with suramin is not satisfactory and wouldn’t pass today’s standards for drug safety (65).
However, patients often get diagnosed in the second stage of the disease. Neither suramin nor
pentamidine cross the blood brain barrier (BBB) sufficiently to yield anti‐trypanocidal
concentrations in the CNS. Therefore it disqualifies those drugs from treating second stage
patients.
Second stage treatment
Due to the lack of drugs able to pass the BBB the second stage of the disease is more difficult to
treat. Only melarsoprol and eflornithine are able to sufficiently pass the BBB to reach required
drug levels in the CNS.
Melarsoprol (MelB, melarsen oxide‐BAL, Arsobal®), an organic, trivalent arsenical, was introduced
by Friedheim in 1949. It was the greatest advance in chemotherapy of HAT since suramin and the
pentavalent arsenical tryparsamide, both introduced in the 1920ies. At the time, tryparsamide was
the only effective drug once the central nervous system has become affected and this only in the
Gambian disease. The Rhodesian infection were totally uncurable; a person infected in East Africa
and ill for more than about one month was almost certainly doomed (20). Melarsoprol,
respectively its active metabolite melarsen oxide, is effective against both, T.b. gambiense and T.b.
rhodesiense infections. However, its high toxicity and frequent adverse drug reactions limit the
use to second stage therapy.
Eflornithine (α‐Difluoromethyl ornithine / DFMO, Ornidyl®) was first developed as a cytostatic
drug and was registered for the use against HAT in 1990 (USA) and 1991 (France), (66). It is active
in T.b. gambiense infections but for biochemical reasons it has only very limited activity in T.b.
rhodesiense (67). The widespread use of eflornithine is hampered by the complicated application
(four daily infusions for two weeks) and the high production costs of the drug. However,
eflornithine is better tolerated and when administered properly, has proven to be safer than
melarsoprol (68). Eflornithine is currently the first line treatment for second stage T.b. gambiense
HAT.

Chapter 1
30
Nifurtimox, a 5‐nitrofuran, is not registered against HAT. It was developed for the treatment of
Trypanosoma cruzi, the causative agent of Chagas' disease. It is a cheap, orally administered drug
but not yet fully validated and not registered for use in human African trypanosomiasis (69).
However, it has been in use on a compassionate basis in combination with eflornithine to treat
T.b. gambiense cases refractory to melarsoprol. Currently, the nifurtimox‐eflornithine
combination therapy (NECT) is under clinical development in T.b. gambiense areas. Preliminary
results indicate its potential as new, first line treatment for T.b. gambiense HAT.
Figure 6: chemical structure of melarsoprol.
The use of melarsoprol is hampered by its high toxicity and complicated dosing schemes. The
treatment regimens of melarsoprol used to be empirically determined and vary considerably
between countries and treatment centres and embody a real omnium‐gatherum throughout
Africa. Common schedules are three or four series of daily i.v. injections (with increasing or equal
doses up to a maximum dose of 3.6mg/kg) for 3 or 4 days, with intervening rest periods of 7‐10‐
day (12). Thus, total hospitalization times of up to one moth are common. The drug is
administered by intravenous injection as a 3.6% solution in propylene glycol. Adverse effects such
as cutaneous reactions, polyneuropathy, diarrhea, fever, or thrombophlebitis at the site of
injection are quite common . The major adverse drug reaction in melarsoprol therapy is the
potentially fatal encephalopathic syndrome (ES). The incidence for ES in Rhodesian sleeping
sickness was found to be 8% and 5% in the Gambiense form (70), the mortality rate amongst
those patients affected was approximately 50%. The concomitant use of prednisolone during
melarsoprol therapy proved to reduce the incidence of ES in T.b. gambiense patients. A reduction
of ES‐associated death was also observed, but did not reach statistical significance (71). The
concomitant use of steroids in T.b. rhodesiense patients did not reduce the incidence of ES (72,
73). Until today, the mechanism of the ES is not fully understood. The current hypothesis
proposes an immunological reaction (74). In order to investigate this hypothesis in more detail,
an association study was carried out where the occurrence of ES was correlated with the HLA‐
N
N
N
N
NH2
NH2
AsS
SCH2OH
H

Introduction
31
genotype of each patient. In a case‐control study blood samples form T.b. gambiense patients
were collected (Democratic Republic of Congo and Angola) and HLA‐genotyping was performed.
The association of the HLA‐genotype and the incidence rates of ES showed that there is a possible
correlation but the samples size is yet too small (70).
Although the drug was introduced almost half a century ago, its mode of action is not well
understood. Initially, the drug was thought to act by inhibiting the trypanosomal pyruvate kinase,
which is a key enzyme in African trypanosomes for production of ATP (75). Additional
investigations showed that melarsen oxide, trypanothion and a major cofactor form a stable
adduct. This adduct is an effective inhibitor of the trypanothione reductase. The inhibition of this
enzyme leads to disturbance of the redox balance of the parasite and thus exposing the
trypanosome to free radicals (76). However, this theory was questioned and it was suggested that
the phospho‐fructokinase, an enzyme of the glycolytic pathway and interference with energy
metabolism might be the main drug target (Wang, 1995).
A further problematic progression in melarsoprol treatment is an increasing number of refectory
cases observed in Gambiense sleeping sickness. Growing number of patients (up to 30%) not
responding to melarsoprol treatment have been reported in Uganda, (77, 78), Angola (79),
Democratic Republic of Congo, DRC (80), Sudan (unpublished data), most probable due to
resistance (18). Refractory cases are treated with eflornithine or the NECT combination therapy.
Repetitive melarsoprol treatment usually has a very limited success. Likely, the same scenario will
sooner or later also be required for treatment of T.b. rhodesiense in the lack of alternatives.
Melarsoprol treatment failures in T.b. rhodesiense patients have been reported (81) but
fortunately, not yet at alarming frequencies (22).
HAT treatment requires a long‐term follow‐up of each patient in order to monitor long‐term
efficacy of the treatment. Patients are asked to present for follow‐up visits after 3 or 6, 12, 18 and
24 months (12, 82). At each follow‐up visit, blood and CSF samples are analyzed to confirm the
absence of the trypanosomes. Due to the painful lumbar punctures and possible long
geographical distances to the health centres patients are often lost to follow up. In T.b. gambiense
areas the patient follow‐up is actively supported by the mobile teams of National Control
Programs or non‐governmental organisations (NGOs). Without active support, follow‐up
attendance is approximately 40% (personal communication Christian Burri). Hence, for the
monitoring of long‐term efficacy in patients who participate in clinical trials substantial efforts
are made to obtain high follow‐up coverage rates. The follow‐up of T.b. rhodesiense patients is
hampered by the absence of mobile teams to trace and examine patients.

Chapter 1
32
Second stage treatment in east Africa
For T.b. rhodesiense HAT, melarsoprol remains the only drug available for the treatment of
second stage disease. Only in east Africa a pre‐treatment with suramin is common and was
introduced on purely empirical basis. It is administered in order to eliminate parasites in blood
and lymph before the treatment with melarsoprol. It should prevent from (i) an initial high
antigen release which might trigger major adverse reactions and (ii) the introduction of
trypanosomes in the CNS while performing the diagnostic LP. However, there is no solid scientific
evidence for this approach. The use of suramin in this way has been criticized, and there is
evidence from West Africa (83) indicating that it is unlikely to prevent adverse reactions which
may follow an injection of melarsoprol, since this is related to the degree of infection in the
central nervous system rather than in the blood. Some authors believe that a high initial antigen
release can trigger immunological overreactions (84). The introduction of trypanosomes during
LP is theoretically possible. However, the usage of proper materials and technical skills make a LP
without blood vessel damage possible. In the rare case of trypanosome introduction to the CSF,
the parasites are hampered in growth and survival as the CSF is a suboptimal medium (85).
There is a wide variety of national treatment schedules in use in East Africa. In Kenya, the
suramin pre‐treatment is not given and in Malawi, only in some health centres. In Tanzania, two
injections of suramin (one test dose, one full dose) are given over a time period of 5 days. In
practice suramin is not given to critically ill patients so as to quickly reach curative melarsoprol
concentrations in the CNS. In Uganda, the suramin pre‐treatment is administered as a single test
dose (5mg/kg) prior to the lumbar puncture. Melarsoprol is also administered according
heterogeneous schedules: differences exist in the number of series and the dosages of
melarsoprol. Details are shown in table 4.

Introduction
33
Table 3: National treatment schedules in use in east Africa for the treatment of second stage T.b. rhodesiense HAT
Day of action Dosage Day of action Dosage Day of action Dosage Day of action DosageSuramin pre-treatment Application 01 1 5mg/kg 1 5mg/kg 1 5mg/kg Application 02 3 20mg/kg 2 20mg/kg Total suramin 5mg/kg 25mg/kg 25mg/kg Lumbar puncture (LP) 2 5 3Melarsoprol treatment Application 01 3 0.5mg/kg 5 2.2mg/kg 4 3.6mg/kg 1 3.6mg/kg Application 02 4 0.72mg/kg 6 2.52mg/kg 5 3.6mg/kg 2 3.6mg/kg Application 03 5 1.08mg/kg 7 2.88mg/kg 6 3.6mg/kg 3 3.6mg/kgResting period Application 04 11 1.44mg/kg 15 2.88mg/kg 14 3.6mg/kg 11 3.6mg/kg Application 05 12 1.80mg/kg 16 3.24mg/kg 15 3.6mg/kg 12 3.6mg/kg Application 06 13 2.2mg/kg 17 3.6mg/kg 16 3.6mg/kg 13 3.6mg/kgResting period Application 07 19 2.52mg/kg 25 3.6mg/kg 24 3.6mg/kg 21 3.6mg/kg Application 08 20 2.88mg/kg 26 3.6mg/kg 25 3.6mg/kg 22 3.6mg/kg Application 09 21 3.24mg/kg 27 3.6mg/kg 26 3.6mg/kg 23 3.6mg/kgResting period Application 10 27 3.6mg/kg 31 3.6mg/kg Application 11 28 3.6mg/kg 32 3.6mg/kg Application 12 29 3.6mg/kg 33 3.6mg/kgTotal melarsoprol 27mg/kg 28.08mg/kg 32.4mg/kg 43.2mg/kg
Total days of treatment Total days of hospitalizationAdministration of steroidsLP on dischargeFollow up (in months)
UGANDA TANZANIA MALAWI KENYA
before melarsoprol
5 days 7 days 7 days 7 days
5 days 7 days 7 days 7 days
5 days 7 days
13 11 12 1229 27 26 33
when reaction occurs standard during treatment standard during treatment standard during treatmentyes no yes yes
passive 3,6,12,24 passive 3,6,12,18,24 passive 3,6,12,24 active 3, passive 6,12,24

Chapter 1
34
IMPAMEL – improved application of melarsoprol
Even though melarsoprol was introduced in 1949 only after almost 50 years of use its
pharmacokinetic and pharmacological properties have been investigated (86‐89). Based on those
findings and computer simulations, a new schedule for the treatment of second stage sleeping
sickness was suggested: the alternative treatment schedule consists of a daily melarsoprol
application at a dosage of 2.2mg/kg for 10 consecutive days. The IMPAMEL I program assessed the
safety and efficacy of this new, abridged treatment regimen by conducting an open, randomized
equivalence trial in 500 T.b. gambiense patients in Angola. There were no significant differences in
the frequency of adverse drug reactions and efficacy, and the new schedule was found to be
favourable over the Angolan standard 26‐day treatment schedule. The positive impression of the
new treatment schedule was corroborated by the results of a multi‐national, multi‐centre study,
monitoring the application of the new schedule in over 2’800 patients in various different settings
(IMPAMEL II program) and the effectiveness was similar to the respective standard treatment
regimens (90). The IMPAMEL schedule doesn’t improve the occurrence and/or frequency of adverse
events which are related to the toxicity of melarsoprol. No significant clinical inferiority of the
new schedule could be demonstrated. But the IMPAMEL schedule is very much favourable due to
socio‐economic benefits: with a similar efficacy and effectiveness over the standard regimens, the
hospitalization time can be reduced by approximately 50%, the total amount of given melarsoprol
by about 30%. Those factors facilitate late stage treatment on different levels: no more dose‐
adjusting, reduced hospitalisation time which relieves the health facilities, the patients and their
families. Those factors have a high impact on the capacity of each treatment centre, on the
treatment quality and compliance. Within the IMPAMEL II program a cost‐effectiveness study was
undertaken and the results confirmed that the new schedule reduces treatment and
hospitalisation costs per patient (91). On request of WHO, the new 10‐day schedule for treatment
of late stage T.b. gambiense sleeping sickness with melarsoprol was recommended by the
International Scientific Council for Trypanosomiasis Control and Research / ISCTRC at the
occasion of the 27th meeting in October 2003, Pretoria, South Africa.

Introduction
35
Justification and goals
The new, abridged protocol for the treatment of T.b. gambiense patients with melarsoprol shows
significant socio‐economic benefits and better cost‐effectiveness (91). Members of the Data and
Safety Monitoring Board from the IMPAMEL I & II programs expressed their concerns regarding an
interruption of the IMPAMEL program fearing it could lead to an uncontrolled use of the 10‐day
schedule in East Africa without reliable data about safety and efficacy. Also, the WHO Scientific
Working Group 2001 recommended the urgent conduct of the necessary trials in T.b. rhodesiense
HAT, a call which was repeated by a WHO Afro meeting in Kampala, 2003. Because of the
differences in T.b. gambiense and T.b. rhodesiense HAT each therapeutic intervention has to be
tested separately. The patient’s safety can only be ensured when possible differences in
pharmacodynamics or –kinetics; or different susceptibilities to the same drug are ruled out.
The current national treatment policies in east Africa are inconsistent and complicated and lead
to lowered treatment compliance and quality. Due to the very long hospitalization times some
patients leave the health facilities before the completion of the full melarsoprol course. This
favours relapses and can possibly impact on the development of resistances. The capacities of
HAT‐treating health facilities are strained because of the long stay of patients and attendants. The
changing dosages throughout the treatment are rarely well implemented and may lead to over or
under dosed treatments. Further, the role of the suramin pre‐treatment is vague; is it ineffective,
beneficial or even unfavourable?
The assessment of the use of the 10‐day melarsoprol schedule in East Africa is essential in order to
offer the patients and the health facilities a substantial better treatment. Also it is urgently
needed as basis for potential, future combination treatments. No new drug will be available in the
next 5 to 8 years and it can not be excluded that melarsoprol will loose some of its efficacy against
T.b. rhodesiense, similar to the phenomenon recently observed in some T.b. gambiense areas (78).
However, for pharmacological reasons, combination treatments for second stage T.b. rhodesiense
HAT will be based on melarsoprol until the mergence of new drugs.
A multinational approach is advantageous for any research activities in T.b. rhodesiense HAT as it
considers the high strain heterogeneity which might affect the outcome of the research question.
When implementing the 10‐day schedule in East Africa, several aspects have to be taken into
consideration: is the pre‐treatment with suramin redundant? Is the 10‐day schedule safe for T.b.
rhodesiense patients? Is the treatment efficacious? Does the short course have any impact on the
incidence rate of the ES and / or the case fatality rates? The IMPAMEL schedule consists of 10

Chapter 1
36
consecutive melarsoprol injections at a dosage of 2.2mg/kg. Currently, starting doses of national
treatment schedules in Tanzania and Malawi are 2.2 mg/kg and 3.6 mg/kg, respectively. Only
Uganda uses a lower starting dose of 0.36 mg/kg, increasing to a maximum dose of 3.6mg/kg with
no better results regarding case fatality rates and/or ES reported. Late stage treatment according
to the IMPAMEL schedule, reduces the total amount of given melarsoprol by 20% in Uganda, by 23%
in Tanzania, by 33% in Malawi and by 50% in Kenya. Generally, there is evidence from former
studies performed in T.b. gambiense in South Sudan (92) that the 10‐day schedule leads to a
comparable frequency of adverse drug reactions as the standard treatment schedule. The only
exception may be skin reactions (like pruritus, maculopapular eruptions) or very rarely bullous
reactions, which were observed in a higher frequency in previous trials compared to the standard
treatment.
The IMPAMEL schedule does not claim clinical superiority, but the socio‐economic benefits and the
better cost‐effectiveness make it favourable to the patients, the health facilities and the national
bodies of disease control. Further, a harmonization process for all east African treatment
protocols can be envisaged if the 10‐day melarsoprol schedule proves to be safe and efficacious.
However, the limitations of clinical research in this field are the small number of patients and the
difficulties in patient’s access and diagnosis. Therefore, clinical research activities are restricted to
a small sample size.
Goals
The IMPAMEL III program was designed as a series of clinical trials in Tanzania and Uganda. Its
principle goal was the assessment of the safety and efficacy of the 10‐day melarsoprol schedule in
second stage T.b. rhodesiense HAT.
The objectives were
- to conduct clinical trials assessing the abridged melarsoprol treatment schedule in T.b.
rhodesiense patients according to international standards
- to investigate the benefit of the suramin pre‐treatment
- to monitoring the potential overlap in disease distribution areas of the two forms of HAT

Introduction
37
Prior to the IMPAMEL III program, no clinical research program compliant to international
standards had been conducted in T.b. rhodesiense affected areas. Therefore, the conduct of the
IMPAMEL III program was expected to strengthen capacities at the local level, the collaboration
between different T.b. rhodesiense affected countries and the awareness towards the disease.
After the conduct of the trial we were able to write a review on the conduct of clinical trials in
resource limited settings and suggested minimal standards for sponsors and host countries in
order to ensure a trial conduct in compliance with international standards.

Chapter 1
38
References
1. Berrang‐Ford L, Waltner‐Toews D, Charron D, Odiit M, McDermott J, Smit B. Sleeping Sickness in Uganda: A Systems Approach. EcoHealth. 2005 August 2005;2(3):183‐94.
2. Van der Stuyft P, Unger JP. Improving the performance of health systems: the World Health Report as go‐between for scientific evidence and ideological discourse. Trop Med Int Health. 2000 Oct;5(10):675‐7.
3. McDermott JJ, Coleman PG. Comparing apples and oranges‐‐model‐based assessment of different tsetse‐transmitted trypanosomosis control strategies. Int J Parasitol. 2001 May 1;31(5‐6):603‐9.
4. WorldHealthReport. World Health Report; 2004.
5. Stich A, Abel PM, Krishna S. Human African trypanosomiasis. Bmj. 2002 Jul 27;325(7357):203‐6.
6. De Greef C, Hamers R. The serum resistance‐associated (SRA) gene of Trypanosoma brucei rhodesiense encodes a variant surface glycoprotein‐like protein. Mol Biochem Parasitol. 1994 Dec;68(2):277‐84.
7. Gibson WC. The SRA gene: the key to understanding the nature of Trypanosoma brucei rhodesiense. Parasitology. 2005 Aug;131(Pt 2):143‐50.
8. MacLeod A, Welburn S, Maudlin I, Turner CM, Tait A. Evidence for multiple origins of human infectivity in Trypanosoma brucei revealed by minisatellite variant repeat mapping. J Mol Evol. 2001 Mar;52(3):290‐301.
9. Bales JD. African Trypanosomiasis. In: Strickland GT, editor. Hunter's Tropical Medicine. 7 ed. Philadelphia: Saunders Company; 1988. p. 617‐28.
10. Wallingford. Tsetse biology and ecology: their role in the epidemiology and control of Trypanosomiasis. UK: CABI Publishing in association with the International Livestock Research Institute, Nairobi, Kenya; 1999.
11. Kuzoe FA. Current situation of African trypanosomiasis. Acta Trop. 1993 Sep;54(3‐4):153‐62.
12. WHO. Control and surveillance of African trypanosomiasis. Geneva: WHO; 1998.
13. Simarro PP, Louis FJ, Jannin J. [Sleeping sickness, forgotten illness: what are the consequences in the field?]. Med Trop (Mars). 2003;63(3):231‐5.
14. WHO. Human African trypanosomiasis (sleeping sickness): epidemiological update. Weekly epidemiological record. 2006 24. Februar(TRS881):69‐80.
15. Pepin J, Meda HA. The epidemiology and control of human African trypanosomiasis. Adv Parasitol. 2001;49:71‐132.
16. Odiit M, Coleman PG, Liu WC, McDermott JJ, Fevre EM, Welburn SC, et al. Quantifying the level of under‐detection of Trypanosoma brucei rhodesiense sleeping sickness cases. Trop Med Int Health. 2005 Sep;10(9):840‐9.
17. Odiit M, Kansiime F, Enyaru JC. Duration of symptoms and case fatality of sleeping sickness caused by Trypanosoma brucei rhodesiense in Tororo, Uganda. East Afr Med J. 1997 Dec;74(12):792‐5.
18. WHO T. http://www.who.int/tdr/diseases/tryp/direction.htm. 2002 [cited; Available from:
19. Molyneux DH, Ashford RW. The biology of Trypanosoma and Leishmania, Parasites of Man and Domestic Animals. London: Taylor&Francis Ltd.; 1983.
20. Apted FIC. Present status of chemotherapy and chemoprophylaxis of human trypanosomiasis in the eastern hemisphere. Pharmacology and Therapeutics. 1980;11:391‐413.
21. Hoppe K. Lords of the Fly. Westport, USA: Praeger; 2003.
22. Kibona SN, Matemba L, Kaboya JS, Lubega GW. Drug‐resistance of Trypanosoma b. rhodesiense isolates from Tanzania. Trop Med Int Health. 2006 Feb;11(2):144‐55.

Introduction
39
23. Jelinek T, Bisoffi Z, Bonazzi L, van Thiel P, Bronner U, de Frey A, et al. Cluster of African trypanosomiasis in travelers to Tanzanian national parks. Emerg Infect Dis. 2002 Jun;8(6):634‐5.
24. Kaare MT, Picozzi K, Mlengeya T, Fevre EM, Mellau LS, Mtambo MM, et al. Sleeping sickness‐‐a re‐emerging disease in the Serengeti? Travel Med Infect Dis. 2007 Mar;5(2):117‐24.
25. Koerner T, De Raadt P, Maudlin I. The 1901 uganda sleeping sickness epidemic revisited: a case of mistaken identity? Parasitol Today. 1995 Aug;11(8):303‐6.
26. Berrang‐Ford L, Berke O, Abdelrahman L, Waltner‐Toews D, McDermott J. Spatial analysis of sleeping sickness, southeastern Uganda, 1970‐2003. Emerg Infect Dis. 2006 May;12(5):813‐20.
27. Legros D, Gastellu Etchegorry M, Mbulamberi DB. Preliminary results of a clinical trial comparing melarsoprol to pentamidine for the treatment of early stage two T. b. gambiense patients in Uganda. International Colloquium "Sleeping Sickness Rediscovered"; 1998; Antwerp: Conference proceedings; 1998.
28. Fevre EM, Coleman PG, Odiit M, Magona JW, Welburn SC, Woolhouse ME. The origins of a new Trypanosoma brucei rhodesiense sleeping sickness outbreak in eastern Uganda. Lancet. 2001 Aug 25;358(9282):625‐8.
29. Picozzi K, Fevre EM, Odiit M, Carrington M, Eisler MC, Maudlin I, et al. Sleeping sickness in Uganda: a thin line between two fatal diseases. Bmj. 2005 Nov 26;331(7527):1238‐41.
30. Fevre EM, Picozzi K, Fyfe J, Waiswa C, Odiit M, Coleman PG, et al. A burgeoning epidemic of sleeping sickness in Uganda. Lancet. 2005 Aug 27‐Sep 2;366(9487):745‐7.
31. Abila PP, Slotman MA, Parmakelis A, Dion KB, Robinson AS, Muwanika VB, et al. High Levels of Genetic Differentiation between Ugandan Glossina fuscipes fuscipes Populations Separated by Lake Kyoga. PLoS Negl Trop Dis. 2008;2(5):e242.
32. Degen R, Pospichal H, Enyaru J, Jenni L. Sexual compatibility among Trypanosoma brucei isolates from an epidemic area in southeastern Uganda. Parasitol Res. 1995;81(3):253‐7.
33. Chappuis F, Loutan L, Simarro P, Lejon V, Buscher P. Options for field diagnosis of human african trypanosomiasis. Clin Microbiol Rev. 2005 Jan;18(1):133‐46.
34. Wery M. Therapy for African trypanosomiasis. Current Opinion in Infectious Diseases. 1991;4(6):838‐44.
35. Songa EB, Hamers R, Rickman R, Nantulya VM, Mulla AF, Magnus E. Evidence for widespread asymptomatic Trypanosoma rhodesiense human infection in the Luangwa Valley (Zambia). Trop Med Parasitol. 1991 Dec;42(4):389‐93.
36. Ormerod WE. Taxonomy of the sleeping sickness trypanosomes. J Parasitol. 1967 Aug;53(4):824‐30.
37. Buyst H. The epidemiology of sleeping sickness in the historical Luangwa valley. Ann Soc Belg Med Trop. 1977;57(4‐5):349‐59.
38. Burri C, Stich A, Brun R. The trypanosomiases: CABI Publishing; 2004.
39. Checchi F, Filipe JA, Haydon DT, Chandramohan D, Chappuis F. Estimates of the duration of the early and late stage of gambiense sleeping sickness. BMC Infect Dis. 2008;8:16.
40. Buguet A, Bisser S, Josenando T, Chapotot F, Cespuglio R. Sleep structure: a new diagnostic tool for stage determination in sleeping sickness. Acta Trop. 2004 18 November;93.
41. Greenwood BM, Whittle HC. The pathogenesis of sleeping sickness. Trans R Soc Trop Med Hyg. 1980;74(6):716‐25.
42. Jordan A. Trypanosomiasis control and African Rural Development. Longman Group Ltd.; 1986.
43. Maudlin I. African trypanosomiasis. Ann Trop Med Parasitol. 2006 Dec;100(8):679‐701.

Chapter 1
40
44. Simarro PP, Jannin J, Cattand P. Eliminating human African trypanosomiasis: where do we stand and what comes next? PLoS Med. 2008 Feb;5(2):e55.
45. Hide G, Angus SD, Holmes PH, Maudlin I, Welburn SC. Trypanosoma brucei: comparison of circulating strains in an endemic and an epidemic area of a sleeping sickness focus. Exp Parasitol. 1998 May;89(1):21‐9.
46. Hide G. History of sleeping sickness in East Africa. Clin Microbiol Rev. 1999 Jan;12(1):112‐25.
47. Kagira JM, Maina N. Occurrence of multiple drug resistance in Trypanosoma brucei rhodesiense isolated from sleeping sickness patients. Onderstepoort J Vet Res. 2007 Mar;74(1):17‐22.
48. Schofield CJ, Kabayo JP. Trypanosomiasis vector control in Africa and Latin America. Parasit Vectors. 2008;1(1):24.
49. Vreysen MJ, Saleh KM, Ali MY, Abdulla AM, Zhu ZR, Juma KG, et al. Glossina austeni (Diptera: Glossinidae) eradicated on the island of Unguja, Zanzibar, using the sterile insect technique. J Econ Entomol. 2000 Feb;93(1):123‐35.
50. Magnus E, Vervoort T, Van Meirvenne N. A card‐agglutination test with stained trypanosomes (C.A.T.T.) for the serological diagnosis of T.b. gambiense trypanosomiasis. Ann Soc Belg Med Trop. 1978;58(3):169‐76.
51. Enyaru JC, Odiit M, Winyi‐Kaboyo R, Sebikali CG, Matovu E, Okitoi D, et al. Evidence for the occurrence of Trypanosoma brucei rhodesiense sleeping sickness outside the traditional focus in south‐eastern Uganda. Ann Trop Med Parasitol. 1999 Dec;93(8):817‐22.
52. Woo PT. The haematocrit centrifuge for the detection of trypanosomes in blood. Can J Zool. 1969 Sep;47(5):921‐3.
53. Lumsden WH, Kimber CD, Evans DA, Doig SJ. Trypanosoma brucei: Miniature anion‐exchange centrifugation technique for detection of low parasitaemias: Adaptation for field use. Trans R Soc Trop Med Hyg. 1979;73(3):312‐7.
54. Robays J, Miaka Bilenge M, Stuyft PV, Boelaert M. The effectiveness of active population screening and treatment for sleeping sickness control in the Democratic Republic of Congo. Trop Med Int Health. 2004 May;9(5):542‐50.
55. Njiru ZK, Ndung'u K, Matete G, Ndungu JM, Gibson WC. Detection of Trypanosoma brucei rhodesiense in animals from sleeping sickness foci in East Africa using the serum resistance associated (SRA) gene. Acta Trop. 2004 May;90(3):249‐54.
56. Notomi T, Okayama H, Masubuchi H, Yonekawa T, Watanabe K, Amino N, et al. Loop‐mediated isothermal amplification of DNA. Nucleic Acids Res. 2000 Jun 15;28(12):E63.
57. Lejon V, Legros D, Richer M, Ruiz JA, Jamonneau V, Truc P, et al. IgM quantification in the cerebrospinal fluid of sleeping sickness patients by a latex card agglutination test. Trop Med Int Health. 2002 Aug;7(8):685‐92.
58. Miezan TW, Meda HA, Doua F, Yapo FB, Baltz T. Assessment of central nervous system involvement in gambiense trypanosomiasis: value of the cerebro‐spinal white cell count. Trop Med Int Health. 1998 Jul;3(7):571‐5.
59. Robays J, Bilengue MM, Van der Stuyft P, Boelaert M. The effectiveness of active population screening and treatment for sleeping sickness control in the Democratic Republic of Congo. Trop Med Int Health. 2004 May;9(5):542‐50.
60. Hysek C. Perceptions and expectations on treatmnets of Human African Trypanosomiasis, Bandundu Province, DRC. Basel: University of Basel; 2007.

Introduction
41
61. Goa KL, Campoli‐Richards DM. Pentamidine isethionate. A review of its antiprotozoal activity, pharmacokinetic properties and therapeutic use in Pneumocystis carinii pneumonia. Drugs. 1987 Mar;33(3):242‐58.
62. Van Hoof L, Henrard C, Peel E. Pentamidine in the prevention and treatment of trypanosomiasis. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1944;37(4):271‐80.
63. McGeary RP, Bennett AJ, Tran QB, Cosgrove KL, Ross BP. Suramin: clinical uses and structure‐activity relationships. Mini Rev Med Chem. 2008 Nov;8(13):1384‐94.
64. Chijioke CP, Umeh RE, Mbah AU, Nwonu P, Fleckenstein LL, Okonkwo PO. Clinical pharmacokinetics of suramin in patients with onchocerciasis. Eur J Clin Pharmacol. 1998 May;54(3):249‐51.
65. Fairlamb AH. Future prospects for the chemotherapy of human trypanosomiasis. 1. Novel approaches to the chemotherapy of trypanosomiasis. Trans R Soc Trop Med Hyg. 1990 Sep‐Oct;84(5):613‐7.
66. Nightingale S. Drug for sleeping sickness approved. Journal of the American Medical Association. 1991;265(10):1229.
67. Iten M, Matovu E, Brun R, Kaminsky R. Innate lack of susceptibility of Ugandan Trypanosoma brucei rhodesiense to DL‐alpha‐difluoromethylornithine (DFMO). Trop Med Parasitol. 1995 Sep;46(3):190‐4.
68. Chappuis F, Udayraj N, Stietenroth K, Meussen A, Bovier PA. Eflornithine is safer than melarsoprol for the treatment of second‐stage Trypanosoma brucei gambiense human African trypanosomiasis. Clin Infect Dis. 2005 Sep 1;41(5):748‐51.
69. Legros D, Ollivier G, Gastellu‐Etchegorry M, Paquet C, Burri C, Jannin J, et al. Treatment of human African trypanosomiasis‐‐present situation and needs for research and development. Lancet Infect Dis. 2002 Jul;2(7):437‐40.
70. Seixas J. Investigations on the encephalopathic syndrome during melarsoprol treatment in human African trypanosomiasis [PhD Thesis]: Basel; 2004.
71. Pepin J, Milord F, Guern C, Mpia B, Ethier L, Mansinsa D. Trial of prednisolone for prevention of melarsoprol‐induced encephalopathy in gambiense sleeping sickness. Lancet. 1989 Jun 3;1(8649):1246‐50.
72. Arroz JO. Melarsoprol and reactive encephalopathy in Trypanosoma brucei rhodesiense. Trans R Soc Trop Med Hyg. 1987;81(2):192.
73. Onyango RJ, Bailey NM, Okach RW, Mwangi EK, Ogada T. Encephalopathy during treatment of human trypanosomiasis. EATRO report. 1969.
74. Pepin J, Milord F. African trypanosomiasis and drug‐induced encephalopathy: risk factors and pathogenesis. Trans R Soc Trop Med Hyg. 1991 Mar‐Apr;85(2):222‐4.
75. Flynn IW, Bowman IBR. The action of trypanocidal arsenical drugs on Trypanosoma brucei and Trypanosoma rhodesiense. Comparative Biochemistry and Physiology; Part B, Biochemistry and Molecular Biology. 1974;48(2):261‐73.
76. Fairlamb AH, Henderson GB, Cerami A. Trypanothion is the primary target for arsenical drugs against african trypanosomes. Proceedings of the National Academy of Sciences of the United States of America. 1989;86:2607‐11.
77. Legros D, Evans S, Maiso F, Enyaru JCK, Mbulamberi D. Risk factors for treatment failure after melarsoprol for Trypanosoma brucei gambiense trypanosomiasis in Uganda. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1999;93:439‐42.
78. Matovu E, Enyaru JC, Legros D, Schmid C, Seebeck T, Kaminsky R. Melarsoprol refractory T. b. gambiense from Omugo, north‐western Uganda. Trop Med Int Health. 2001 May;6(5):407‐11.

Chapter 1
42
79. Stanghellini A, Josenando T. The situation of sleeping sickness in Angola: a calamity. Tropical Medicine and International Health. 2001;6(5):330‐4.
80. Robays J, Nyamowala G, Sese C, Betu Ku Mesu Kande V, Lutumba P, Van der Veken W, et al. High failure rates of melarsoprol for sleeping sickness, Democratic Republic of Congo. Emerg Infect Dis. 2008 Jun;14(6):966‐7.
81. Foulkes JR. Metronidazole and suramin combination in the treatment of arsenical refractory Rhodesian sleeping sickness‐‐a case study. Trans R Soc Trop Med Hyg. 1996 Jul‐Aug;90(4):422.
82. WHO. Recommendations of the Informal Consultation on Issues for Clinical Product Development for Human African Trypanosomiasis. Geneva, Switzerland; 2007. Report No.: WHO/CDS/NTD/IDM/2007.1.
83. Whittle HC, Pope HM. The febrile response to treatment in Gambian sleeping sickness. Annals of Tropical Medicine and Parasitology. 1972;66(1):7‐14.
84. Pepin J, Ethier L, Kazadi C, Milord F, Ryder R. The impact of human immunodeficiency virus infection on the epidemiology and treatment of Trypanosoma brucei gambiense sleeping sickness in Nioki, Zaire. Am J Trop Med Hyg. 1992 Aug;47(2):133‐40.
85. Pentreath VW, Owolabi AO, Doua F. Survival of Trypanosoma brucei brucei in cerebrospinal fluid. Ann Trop Med Parasitol. 1992;86(1):29‐34.
86. Burri C, Baltz T, Giroud C, Doua F, Welker HA, Brun R. Pharmacokinetic properties of the trypanocidal drug melarsoprol. Chemotherapy. 1993;39(4):225‐34.
87. Keiser J, Ericsson O, Burri C. Investigations of the metabolites of the trypanocidal drug melarsoprol. Clinical Pharmacology and Therapeutics. 2000 May;67(5):478‐88.
88. Keiser J, Stich A, Burri C. New drugs for the treatment of human African trypanosomiasis, research and development. Trends in Parasitology. 2001;17(1):42‐9.
89. Burri C. Pharmacological aspects of the trypanocidal drug melarsoprol. Basel, Switzerland: University of Basel; 1994.
90. Schmid C, Nkunku S, Merolle A, Vounatsou P, Burri C. Efficacy of 10‐day melarsoprol schedule 2 years after treatment for late‐stage gambiense sleeping sickness. Lancet. 2004 Aug 28;364(9436):789‐90.
91. Schmid C, Santercole C, Kwete J, Lutumba P, Shaw AP. An economic appraisal of the late‐stage T.b. gambiense sleeping sickness treatment. in preparation. 2005.
92. Schmid C, Richer M, Bilenge CM, Josenando T, Chappuis F, Manthelot CR, et al. Effectiveness of a 10‐Day Melarsoprol Schedule for the Treatment of Late‐Stage Human African Trypanosomiasis: Confirmation from a Multinational Study (Impamel II). J Infect Dis. 2005 Jun 1;191(11):1922‐31.

IMPAMEL III
43
Chapter 2
Safety and efficacy of the 10‐day melarsoprol schedule in the
treatment of second stage rhodesiense sleeping sickness
Irene Kuepfer1, Emma Peter Hhary2, Allan Mpairwe3, Andrew Edielu3, Lucas Matemba4, Abbas
Kakembo5, Stafford Kibona4, Caecilia Schmid1, Johannes Blum1, Christian Burri1
1Swiss Tropical Institute, Basel, Switzerland, 2Kaliua Health Centre, Kaliua, Tanzania
3Lwala Hospital, Lwala, Uganda, 3National Institute for Medical Research, Tabora, Tanzania, 4Ministry of Health, Kampala, Uganda
This manuscript will be submitted to the British Medical Journal
Finished product of melarsoprol

Chapter 2
44
Abstract
Objective Assessment of the safety and efficacy of a 10‐day melarsoprol schedule against second
stage T.b. rhodesiense infections and the effect of a suramin pre‐treatment on the incidence of
adverse drug reactions during melarsoprol therapy.
Design Sequential conduct of a proof‐of‐concept trial (n=60) and a utilization study (n=78) using
historic controls as comparator.
Setting Two trial centres in T.b. rhodesiense endemic regions of Tanzania and Uganda.
Participants Consenting patients with confirmed second stage disease and a minimum age of 6
years were eligible for participation. Unconscious and pregnant patients were excluded.
Main outcome measures The primary outcome measures were safety and efficacy at end of
treatment. The secondary outcome measure was efficacy during follow‐up after 3, 6 and 12
months.
Results The incidence of ES in the trial population was 11.2% (CI 5‐17%) and 13% (CI 9‐17%) in the
historic data. The respective case fatality rates were 8.4% (CI 3‐13.8%) and 9.3% (CI 6‐12.6%). All
patients discharged alive were free of parasites at the end of treatment. Six months after discharge
99% of patients were considered clinically cured. The mean hospitalization time was reduced
from 29 to 13 days (p<0.0001) per patient.
Conclusions There is no increased risk for ES and death linked to the 10‐day melarsoprol
schedule compared to the national schedules in current use. In addition, there was no evidence
for an increased risk of adverse events or relapses when suramin pre‐treatment was omitted.
Trial registration: Current Controlled Trials ISRCTN40537886 (controlled‐trials.com)

IMPAMEL III
45
Introduction
Human African Trypanosomiasis (HAT), also known as sleeping sickness, is a parasitic disease
transmitted by the bite of the tsetse fly (Glossina spp.). The disease is caused by protozoan
parasites of the genus Trypanosoma and presents as two forms (1), namely the chronic form of
HAT (West and Central Africa) caused by Trypanosoma brucei gambiense and the acute form
(East and South Africa) caused by Trypanosoma brucei rhodesiense. Both forms of HAT are fatal if
left untreated. Time to death has been estimated at almost 3 years for T.b. gambiense (2) and at 6
to 12 months for T.b. rhodesiense infections (3).
The true prevalence of sleeping sickness among the 60 million people in the rural areas of 36
countries in sub Saharan Africa can only be estimated as less than 10% of the at‐risk population
are under surveillance (4). After almost having been eliminated in the 1960ies the disease re‐
emerged to a peak prevalence of an estimated 300‐500’000 cases by the mid 1990ies (4). By an
increase in control activities, the number of cases per year was reduced to an estimated 50’000 ‐
70’000, of which more than 95% were due to T.b. gambiense (5). T.b. rhodesiense HAT is clearly
the more neglected form of HAT due to its very low prevalence. However, it has a dangerous
potential for large scale epidemics which are of high public health importance (6). Between 1976
and 1998 a total of 19’974 cases were detected in south eastern Uganda (7), an area that today, has
the potential for a much larger number of patients due to the expansion of HAT to previously
disease free areas (8, 9). Sporadic T.b. rhodesiense infections in tourists have spurred discussions
about disease control and surveillance, especially in National Parks (10).
Sleeping sickness has two stages, a first (haemolymphatic) stage followed by a second (meningo‐
encephalitic) stage defined by the presence of trypanosomes and/or elevated levels of white blood
cells (≥ 5WBC/mm3) in the cerebrospinal fluid (CSF) (4). Treatment options are limited: T.b.
gambiense first stage infections are treated with pentamidine isethionate and T.b. rhodesiense
with suramin (Germanin®) respectively. For second stage treatment there are currently no other
registered drugs than melarsoprol (Arsobal®) and eflornithine (Ornidyl®). Melarsoprol is the only
drug effective against both forms of the disease. Due to its limited activity against T.b. rhodesiense
(11) eflornithine is only in use for the treatment of T.b. gambiense HAT, but its large scale use is
hampered by the complicated application of the drug. Currently a new combination treatment of
eflornithine with nifurtimox (NECT) is under clinical evaluation against second stage T.b.
gambiense sleeping sickness and appears to be a promising first‐line therapy (12). Still, for the
treatment for T.b. rhodesiense HAT, melarsoprol remains the only available drug.

Chapter 2
46
Since the introduction of melarsoprol in 1949 (13), treatment regimens were empirically developed
and they varied considerably between countries and treatment centres. Complicated dosing
schemes and repeated serial drug applications separated by 1‐week drug‐free intervals were
common and resulted in very long hospitalization times of up to 1 month. The encephalopathic
syndrome (ES) is the most severe complication of melarsoprol treatment and is observed in 5‐10%
of treated patients, being fatal in about 50% of those patients (4). The ES appears to be more
common in T.b. rhodesiense HAT than in T.b. gambiense with reported incidence rates between 5‐
18% (14). The concomitant use of steroids during melarsoprol therapy proved to reduce the
incidence of ES in T.b. gambiense patients (15) but this could not be shown in T.b. rhodesiense (16‐
18).
The suggestion of an abridged melarsoprol treatment schedule based on pharmacokinetic
investigations was the first rational approach to develop a standardized treatment. The new
schedule suggested daily melarsoprol injections of 2.2mg/kg for 10 consecutive days. In the
IMPAMEL I & II programs (1997‐2004) the use of the new schedule was validated for second stage
T.b. gambiense HAT and was shown to be clinically non‐inferior versus the standard regimens (19)
and equally effective (20). It was favoured by patients and health staff due to an over 50%
reduction in hospitalization time and a more economic use of the drug (21). In 2003, the 10‐day
melarsoprol schedule was officially recommended for use in T.b. gambiense affected areas by the
International Scientific Council for Trypanosomiasis Research and Control (ISCTRC). In view of
the increasing rates of melarsoprol treatment failures reported in T.b. gambiense patients (22‐25)
it can not be excluded that melarsoprol will also loose some of its efficacy against T.b. rhodesiense.
Melarsoprol treatment failures have been reported in T.b. rhodesiense patients (26‐29), but yet
not at alarming rates. A reduced melarsoprol susceptibility of T.b. rhodesiense isolates from
Tanzania was recently shown, indicating that drug resistance may be emerging (30). Hence, the
10‐day melarsoprol schedule might become the basis for potential combination treatments and
might allow a harmonization of all east African treatment protocols. The WHO scientific working
group (2001) recommended the urgent conduct of the necessary clinical trials in east Africa, a call
that was repeated by WHO Afro (2003).
The IMPAMEL schedule could not be introduced in east Africa without further testing; a much
higher parasitaemia, a remarkably divergent clinical pattern and potential differences in the
pharmacodynamics and –kinetics could not be disregarded as they may have an impact on
treatment outcomes. Hence, separate testing of safety and efficacy of the abridged schedule was
required in order to ensure its adequacy also in T.b. rhodesiense patients.

IMPAMEL III
47
In East Africa the empirical treatment schedules vary considerable between countries and
treatment centres. In addition, some countries (Tanzania, Uganda, parts of Malawi) administer a
suramin pre‐treatment prior to the diagnostic lumbar puncture (LP) and melarsoprol therapy.
Suramin is intended to (i) prevent a mechanical introduction of trypanosomes into the CNS
during LP and (ii) to clear trypanosomes from blood and lymph to avert initial high antigen
releases at the initiation of melarsoprol therapy. The suramin pre‐treatments is purely empirical
(31) and there is no standardized protocol. In Tanzania it is not given to critically ill patients so as
to quickly reach curative melarsoprol concentrations in the CNS. The national treatment
schedules in use for second stage T.b. rhodesiense HAT are summarized in table 1.
Given the very limited number of patients, clinical trials on T.b. rhodesiense are obviously
restricted to small sample sizes and must be executed in rural settings with very limited
infrastructure and difficult access. This has to be accounted for in the design of trials; randomized
controlled trials or other trial designs with active control groups are not feasible. The design of
the IMPAMEL III program was the conduct of two sequential trials: first a proof‐of‐concept trial was
executed to proof no harm in T.b. rhodesiense patients and to obtain preliminary efficacy data.
Two subgroups, of which only one received suramin allowed to observe a possible substantial
increase of adverse drug reactions if melarsoprol was directly administered. Based on those
findings, a second trial was designed to substantiate the results in a larger patient group. The
Table 1: National treatment schedules in use for second stage T.b. rhodesiense HAT.
Uganda Tanzania Kenya Malawi Suramin pre‐treatment (mg/kg)
1st dose 5 5 NA 5
2nd dose 20 NA 20
Melarsoprol treatment (mg/kg)
1st series 0.5, 0.72, 1.08 2.2, 2.52, 2.88 3.6, 3.6, 3.6 3.6, 3.6, 3.6 2nd series 1.44, 2.80, 2.2 2.88, 3.24, 3.6 3.6, 3.6, 3.6 3.6, 3.6, 3.6 3rd series 2.52, 2.88, 3.24 3.6, 3.6, 3.6 3.6, 3.6, 3.6 3.6, 3.6, 3.6 4th series 3.6, 3.6, 3.6 3.6, 3.6, 3.6
Total melarsoprol (mg/kg) 27 28.08 43.2 32.4
Hospitalization time (days) 29 27 33 26
NA: not applicable; i.v. melarsoprol injections at 24 hours intervals per series, each series spaced by a 5 to 7 day resting period; further variations of schedules possible at local level

Chapter 2
48
second, drug utilization trial, was designed as an extension of the selected arm of the proof‐of‐
concept trial, i.e. without suramin, thus, allowing pooling data from both trials for final analysis.
Patient records from two years prior to the IMPAMEL III program were analyzed and used as
controls. The findings of the two sequentially conducted trials are reported here collectively.
Methods
Study sites
The Kaliua Health Centre (KHC), a 50‐bed missionary hospital in Tanzania (Urambo District) and
the Lwala Hospital, a designated 100‐ bed district hospital in Uganda (Kaberamaido District)
participated in the IMPAMEL III program. Capacity building included the upgrade of the
pharmacies and laboratories and on‐site trainings in Good Clinical Practice (GCP), HAT diagnosis
and informed consent procedures.
Study design
Sequential conduct of two non‐randomized trials; a proof‐of‐concept trial (n=60) followed by a
utilization study (n=78) using historic data as comparator (n=300).
Proof‐of‐concept trial. 60 patients were prospectively enrolled into two subgroups:
participants in the first subgroup (n=30) were treated with the suramin pre‐treatment followed
by the 10‐day melarsoprol schedule. The second sub group (n=30) was directly treated with the
10‐day melarsoprol schedule. Suramin and steroids were administered according to centre‐
specific guidelines.
Utilization study. Additional 78 patients were treated with the 10‐day melarsoprol schedule.
The suramin pre‐treatment was omitted and the use of steroids was adjusted to the Tanzanian
standard in both centres (details below).
Eligibility criteria. Patients with confirmed second stage T.b. rhodesiense HAT and a minimum
age of 6 years were eligible for participation. Pregnant as well as unconscious or moribund
patients were excluded from the trial. Each participant gave written informed consent. For the
participation of children and adolescents (below 18 years) the parents, the legal representative or
the guardian gave written informed consent.
Diagnosis and staging. Diagnosis of HAT was made in blood and in the cerebrospinal fluid
(CSF). Blood was examined by direct microscopy and/or the haematocrit centrifugation technique
(32). If trypanosomes were present, a lumbar puncture was performed for disease staging. Patients
in the first subgroup of the proof‐of‐concept trial received the suramin pre‐treatment prior to the
LP. All other patients underwent LP directly after the detection of trypanosomes in blood.

IMPAMEL III
49
Analysis of the CSF was done by direct microscopy and/or single modified centrifugation
technique and white blood cell (WBC) count using counting chambers. Second stage infections
were confirmed by the presence of trypanosomes and/or ≥ 5 WBC/mm3 in the CSF.
Patient follow‐up. All patients were asked to present at the centre for follow‐up examinations
after 3, 6 and 12 months. At each follow‐up visit blood and CSF samples were taken. These were
analyzed for the presence of trypanosomes and a WBC count was performed using the CSF
sample. For patients who did not present for follow‐up visits, oral information on their general
condition was collected.
Endpoints: safety & efficacy. Based on reported case fatality rates in the trial sites and the
literature, a cut‐off point of all‐cause mortality was set at ≥10%. The computed stopping rule was
an early discontinuation of the trials if 7 or more patients per subgroup (n=30) experienced a fatal
treatment outcome (p=0.026).
The primary efficacy endpoint was cure at end of treatment. Secondary efficacy endpoint was cure
after 3, 6 and 12 months. Possible outcome measures are summarized in table 2.
A high degree of trial homogeneity was achieved by identical eligibility criteria, stopping rule and
endpoints in both trials.
Table 2: possible safety and efficacy outcome measures for IMPAMEL III trials.
Cure at end of treatment No parasites in blood and CSF
Cure during follow‐up No parasites in blood and CSF AND WBC<5/mm3
Clinical cure at end of treatment
No parasites in blood but missing results on CSF analysis (refusal of LP, hemorrhagic LP)
Clinical cure during follow‐up Oral information on general condition of the patient No parasites in blood but missing results on CSF analysis (refusal of LP, hemorrhagic LP)
Relapse (end of treatment and during follow‐up) Trypanosomes in any body fluid
Death
Patients who died during treatment or follow‐up (categorized by likely or definite cause of death): ‐ HAT ‐ Adverse events regarded by the investigator as possibly or probably related to treatment for HAT ‐ Causes unrelated to HAT or the treatment of HAT ‐ Unknown causes

Chapter 2
50
Historic controls. To reduce bias, historic controls were solely collected in the two trial sites and
limited to a time frame of maximum two years prior to study initiation. Files that contained basic
demographic data and valid information on treatment outcome were selected. If documented,
information on serious adverse events (SAEs) and concomitant treatments was collected. Of
almost 400 files reviewed, 300 were eligible as historic controls (153 in Tanzania, 147 in Uganda).
Sample size. No formal sample size was calculated for the proof‐of‐concept trial. The utilization
study had a calculated sample size requirement of minimum 100 patients in order to have a
precision of ±6% on the estimated endpoint.
Analysis plan. In a first step both trials were analyzed separately. Final safety and efficacy
analysis was performed on the pooled dataset of all patients directly treated with the 10‐day
melarsoprol schedule (n=107). Those results were compared to historic controls.
Recruitment. Patient recruitment was mainly by passive case detection at the centre. Active case
search was done with mobile diagnostic teams in the villages of index cases; but the outcome was
poor. In Uganda, the local radio station was contracted to inform the population about the
IMPAMEL III trial and invited people to present for cost‐free screening for HAT at the Lwala
hospital.
All trial participants were given an insecticide treated bed net (ITN). In case of need, the trial
participants and/or their attendants were supported with food during the hospitalization period.
Cost for transport for the patient and one attendant to present for follow‐up visits was refunded.
Ethics & trial registration. For both trials, ethical clearance was obtained from the ethics
committees in the host countries; the National Institute for Medical Research (NIMR), Tanzania
and the Ministry of Health, Uganda. In Switzerland, ethical clearance was obtained from the
ethics committee of the two cantons of Basel (EKBB). Trial registration was done in the Current
Controlled Trials database prior to first patient enrolment (ISRCTN40537886). The trials were
conducted in compliance with ICH/GCP.
Data management and statistical analysis. All data were double entered and verified using the
EpiData Version 3.1 software (www.epidata.dk). Data analysis was done using the statistical
software package STATA Version IC10.0 (STATATM, StataCorp, USA). Pearson’s chi-square test
and the Student’s t test were used to test differences in proportions and means.
Trial conduct. For each patient, a case report form (CRF) was filled containing information on
demographic, diagnostic, and clinical characteristics before and after treatment. The assessment
of adverse events used a graded scale for the severity of the event (0 to 4) and a binary outcome
for the seriousness of the event. Signs and symptoms which were spontaneously reported between

IMPAMEL III
51
the end of treatment evaluation and 30 days post‐treatment were also entered in the case report
form.
During the proof‐of‐concept trial, the blood sugar and the blood lipids were monitored daily
before food intake using the whole blood test system Cardio ChekTM PA. During the proof‐of‐
concept trial, urine analysis using COMBUR9 (Roche Diagnostics, Switzerland) was performed at
baseline and discharge examinations as well as prior to the first melarsoprol injection for all
patients who received the suramin pre‐treatment.
During both trials, vital signs were daily monitored before drug administration. For women, a
pregnancy test was performed at baseline.
Patients were treated with anti‐malarial and anti‐helminth drugs prior to HAT treatment
depending on baseline findings. During treatment, all patients received paracetamol
(acetaminophen) 3 times per day in single doses of 1000mg for adults and 500mg or 250mg
respectively for children. Suramin was administered intravenously as a 10% aqueous solution
(Germanin®, Bayer). In the proof‐of‐concept trial, suramin as well as steroids were given according
the centre‐specific guidelines. In Tanzania, a suramin test dose (5mg/kg) was administered after
the detection of trypanosomes in blood (day 1). After a resting day, a full dose (20mg/kg) was
given on day 3. Another resting day followed before the LP on day 5. Each patient was treated
with 10mg of prednisolone per os half an hour before melarsoprol injection. In Uganda, patients
received one suramin test dose (5mg/kg) after the detection of trypanosomes in the blood. On the
following day, the LP was performed and melarsoprol treatment was initiated in case of
confirmed second stage infection. Steroids were only administered in case of adverse drug
reactions to treatment. Melarsoprol treatment was for all patients 2.2mg/kg of melarsoprol for 10
consecutive days as a 3.6% solution in propylene glycol (Arsobal®; sanofi‐aventis); by slow
intravenous (i.v.) injection but maximally 5ml a day. In the utilization study, all patients
underwent LP directly after a trypanosome‐positive blood test, the use of steroids was adapted to
the Tanzanian standard in both centres and the use of suramin was omitted.
If a patient developed an encephalopathic syndrome, melarsoprol treatment was interrupted and
emergency treatment was initiated: i.v. hydrocortisone (100‐200mg/24hours) or dexamethasone
(3x15mg/24hours); if necessary, anticonvulsive drugs (diazepam, phenobarbital) were applied. The
close observation and frequent monitoring of vital signs were mandatory as well as supportive
feeding if necessary. For exclusion of cerebral malaria, blood was analyzed at the day of onset of
the ES.

Chapter 2
52
Results
First, the results of the proof‐of‐concept trial are presented, followed by the results of the pooled
data set and the comparison to the historic data. The study flow is presented in Figure 1.
Figure 1: overall study flow chart
Proof‐of‐concept trial
Study population and baseline characteristics
From August 2006 to July 2007 a total of 60 patients were enrolled. The age and sex distribution
were similar in both settings. The median age in Uganda (31 years) was slightly lower than in
Tanzania (36 years) as 10 enrolled participants were in the age of 6‐15 years. The nutritional status
of the patients in Uganda was poorer and a body mass index (BMI) <16.5 was more common than
in Tanzania (p=0.001). In Tanzania, fewer patients had trypanosomes in the CSF (p=0.0035) but
the average WBC counts were higher (p<0.0001). The majority of patients suffered from
headaches (90%), general malaise (93.3%) and joint pains (86.7%). Fever (axillary >37.5°C) at
baseline was recorded in 35% of all patients.
Assessed for eligibility n=187 (76/111)1Excluded n=49 (7/42)
1st stage HAT n=20 (0/20)Advanced disease incl. death n=16 (3/13)Age n=3 (0/3)Pregnancy n=2 (1/1)Escape n=2 (1/1)Other reasons n=6 (2/4)Allocation
Enrollment
Centre-specific suramin10-day melarsoprol n=30 (15/15)Patients treated n=25 (13/12)Incomplete treatment n=5 (2/3)
Death n=5 (2/3)
10-day melarsoprol n=30 (15/15)Patients treated n=28 (14/14)Incomplete treatment n=2 (1/1)
Death n=2 (1/1)
10-day melarsoprol n=78 (39/39)Patients treated n=70 (35/35)Incomplete treatment n=7 (4/3)
Death n=7 (4/3)
Safety analysis
Efficacyanalysis
2Safety analysis n= 60 (30/30) 2Safety analysis n= 107 (54/53)
1 numbers in brackets correspond to numbers in Tanzania/Uganda2 patients who received at least one dose of study drug 3 Intention to treat population/ITT – at 12 months for the proof-of-concept trial and at 6 months for the pooled data seta death not related to HAT b same patient as already reported in proof-of-concept trial
Eligible for follow-up n=53 (27/26)Patients followed n=53 (27/26)
Eligible for follow-up n=98 (49/49) Patients followed n=98 (49/49)
Follow up
Proof-of-concept trial Utilization study
Pooled dataset
Exclusion n=1(0/1)Death prior to 1st dosing
3Efficacy analysis n=98 (49/49)Clinical cure at 6 months n=96 (48/48)Relapse n= (1b/0)Death during follow-up n= (0/1)a
3Efficacy analysis n=53 (27/26)Clinical cure at 12 months n=50 (25/25) Relapse n=2 (1/1)Death during follow-up n=1 (1/0)a

IMPAMEL III
53
Safety
A total of 13 (21.6%) serious adverse events (SAE) were reported whereof 7 (53.8%) were fatal.
Other SAEs were due to prolonged hospitalizations and events that required medical
interventions.
In comparison, more ES were reported in Uganda than in Tanzania (6 vs. 1; p=0.0444). The time
to onset of the encephalopathic syndrome was between 3 and 11 days after the first melarsoprol
dose (median 6, mean 7). The overall survival rate for the ES was 28.6% (0% in Tanzania and 33%
in Uganda). Other adverse events reported were headache 15% (9), vomiting 13% (8), febrile
reactions 13% (8), diarrhea 8.3% (5), nausea 6.6% (4), dizziness 5% (3), skin reactions 1.6% (1) and
were controlled by symptomatic treatment. 56.7% (35) patients had an event free treatment
course.
Efficacy
Primary endpoint: 24 hours after treatment, all patients discharged alive (53/60) were free of
parasites in blood and CSF.
Secondary endpoint: during follow‐up, Tanzania and Uganda reported one relapse each: the
patient from Tanzania was enrolled into the second subgroup and was treated with melarsoprol
only. He did not present for the 3 and 6 months follow‐up because he lived far from the centre
and was in good general condition. 12 months after discharge he presented at the centre because
he felt sick again and was diagnosed with second stage HAT. The patient assumed a re‐infection
as symptoms evolved after multiple tsetse bites. The patient from Uganda presented with
trypanosomes in blood two weeks after discharge. He had been treated with suramin and
melarsoprol and developed an ES after the 6th injection of melarsoprol. After an 8‐day treatment
interruption he resumed melarsoprol treatment for 4 more days. Both patients were successfully
re‐treated with melarsoprol according the national treatment schedules. Overall safety and
efficacy outcomes of the proof‐of‐concept trial are summarized in table 3.
Blood sugar, blood lipids and urine analysis are not shown here.

Chapter 2
54
Follow‐up attendance was poorer in Tanzania, most probably due to the longer distances to the
health centre. 44% of the patients presented for the 3 months follow‐up and 30% and 19% for the
6 and 12 months, respectively. In Uganda, 88% presented for the 3 months follow‐up and 65% for
the 6 and 54% for the 12 months follow‐up respectively. For all patients not seen at the centre,
oral information on their general condition was collected. All patients were in good condition and
working after 3, 6 and 12 months, except one patient from Tanzania who died 7 months after
discharge for reasons not related to HAT. No benefit could be attributed to the suramin pre‐
treatment. In contrast, there were more ES and fatal treatment outcomes in the suramin group
(see table 3) but this trend was not significant.
Utilization study
A total of 78 patients were enrolled from October 2007 to August 2008. One patient was excluded
from the analysis as death occurred prior to first dosing (see figure 1). For final analysis data from
the proof‐of‐concept study (without suramin) and the utilization study were pooled. Table 4
compares the two patient populations prior to data pooling. None of the parameters were
significantly different.
Table 3: Safety and efficacy outcomes at discharge and at 12 months follow‐up.
Total Suramin Non‐suramin Number of patients treated n=60 n=30 n=30 Encephalopathic syndrome 7 (11.6) 4 (13.3) 3 (10) Death during treatment 7 (11.6) 5a (16.6) 2a (6.6) Relapses at discharge 0 0 0 Cure at discharge 53 (88.3) 25 (83.3) 28 (93.3) Patients eligible for follow‐up 53 25 28
at 12 months Death 1 (1.8) 0 1d Relapses 2 (3.8) 1(4) 1 (3.6) Clinical cure 52 (98) 25 (100) 27(96.5) whereof cured b 14c (26.4) 9 (36) 5 (17.9)
a two death (Tanzania) outside the trial centre as family seeked local treatment b WBC count in CSF <5cells/mm3 c all patients from Uganda d not related to HAT (Tanzania)

IMPAMEL III
55
Study population and baseline characteristics
The demographic, diagnostic, and clinical characteristics of the patients were similar in Tanzania
(Tz) and Uganda (Ug). 19 trial participants (Tz: 2, Ug: 17) were below 16 years of age with a mean
age of 11 years (± 3 years). A poor nutritional status with a BMI<16.5 was significantly more
frequent in Uganda (p<0.0001). In Tanzania, patients had less frequently trypanosomes in the CSF
(p=0.0002) but significantly higher WBC counts (p<0.0001). In line with the significant higher
WBC count, the neurological symptoms were more distinct in Tanzanian patients. Description of
the clinical course of the disease will be published separately.
Safety
A total of 27 (25.2%) SAEs were reported, summarized by criterion in figure 2. Prolonged
hospitalizations included patients who remained in the hospital due to lack of transport back to
Table 4: Baseline characteristics of patient populations prior to data pooling.
Proof‐of‐concept1 Utilization study Pooled dataset
n=30 n=77 n=107 n % n % n %
Age, mean±SD 36±18 37±19 36±19 Age, range (years) 6‐67 6‐72 6‐72 Male/female ratio 1.7 1.3 1.4 Nutritional status BMI2 (kg/m) ‐ mean±SD 18.8±3.4 18.6±3.6 18.6±3.5 BMI<16.5 8 26.6 18 23.4 26 24.3 Diagnostic findings Trypanosomes in blood 30 100.00 72 93.5 102 95.3 Trypanosomes in CSF3 28 93.33 69 89.6 97 90.7 White blood cell (WBC) count in CSF 92±57 78±64 82±62
Clinical manifestations Headache 27 90.0 73 94.8 100 93.5 Fever (>37.5) 7 23.3 13 16.9 20 18.7 Oedema 6 20.0 25 32.5 31 29.0 Joint pains 29 96.7 76 98.7 105 98.1 Daytime sleep 24 80.0 63 81.8 87 81.3 Night time sleep 23 76.7 50 64.9 73 68.2 Abnormal movements 8 26.7 20 26.0 28 26.2 Walking difficulties 13 43.3 53 68.8 66 61.7
Time period of enrolment Oct 06 ‐ May 07 Oct 07 ‐ Aug 08 Oct 06 ‐ Aug 08
Note: 1no suramin pre‐treatment; 2 body mass index; 3 cerebrospinal fluid

Chapter 2
56
their home villages and patients who were kept for observation. Medical events were treatment of
malaria (n=2), severe vomiting (n=2), severe headache (n=1), cardiac arrhythmia (n=1) and
psychosis at end of treatment (n=1).
Figure 2: Serious adverse events, by SAE criterion
6 patients died during treatment; two died within 24 hours after completion of treatment; one
patient was comatose for 6 days after the last injection of melarsoprol until death occurred.
Overall, death occurred between 2 and 16 days (median 9, mean 8.5) after the first injection of
melarsoprol. The major cause of death was the ES which contributed to 88.9% of the fatalities.
One fatality (11.1%) was attributed to advanced HAT. The onset of ES was reported after an
average of 7.5 days after the first dose of melarsoprol (range 3‐10 days). The onset was sudden, in
58.3% preceded by headache and fever (7/12) and in 41.6% (5/12) by vomiting. In 16.6% (2/12)
malaria parasites were detected at the onset of ES, which probably also caused fever and
headache. Differences were observed in the duration of ES; in Tanzania they were fatal after a
maximum of one day and in Uganda the ES could last for several days (range 1‐8) until the
patient’s condition improved or deteriorated. The overall survival rate was 33.3% (Tz: 0%; Ug:
57.1%).
Other adverse events reported included febrile reactions (37%), headache (22%), vomiting (13%),
dizziness (9%), skin reactions (6.5%), nausea (5.6%) and diarrhea (4%). 35.5% the patients had an
event‐free treatment.
Fatal; ES(29%)
Fatal; advanced HAT(4%)
Medical event(30%)
Prolonged hospitalization(22%)
Life-threatening(15%)

IMPAMEL III
57
Efficacy
Primary endpoint: all patients discharged alive (98/107) were free of parasites in blood and CSF 24
hours after treatment.
Secondary endpoint: Follow‐up attendance rates in Tanzania were 69% at the 3 months and 97%
at the 6 months follow‐up. In Uganda 91% presented for the 3 months and 46% for the 6 months
follow‐up. For all patients that did not present at the centre oral information on their well being
was collected. The 12 months follow‐up is ongoing and will be concluded in June 2009 in Tanzania
and in September 2009 in Uganda.
No relapses were reported from patients that were enrolled into the utilization study. 1 patient
from Uganda died 2 months after discharge of unknown reasons. Table 5 summarizes the main
safety and efficacy outcomes of the pooled data set at discharge and at 6 months after treatment.
Comparison trial data ‐ historic data
Patient files from 2004‐2006 were reviewed and 153 from Tanzania and 147 from Uganda were
used as comparator. Files which were incomplete having missing demographic and/or treatment
evolution details were excluded. Table 6 summarizes the demographics and the incidence of ES
and death for the historic data.
Table 5: Safety and efficacy outcomes at discharge and at 6 months follow‐up.
Total Tanzania Uganda Number of patients treated n=107 n=54 n=53 Encephalopathic syndrome 12 (11.2) 5 (9.3) 7 (13.2) Death during treatment 9 (8.4) 5(9.3) 4(7.5) Relapses at discharge 0 0 0 Cure at discharge 98 (91.6) 49 (90.7) 49 (92.5) Patients eligible for follow‐up 98 49 49
At 6 months Death 3 (1.8) 1a 1 Relapses 1 1a 0 Clinical cure 97 (99) 49 (100) 48 (98)
whereof curedb 33 (33.7) 0 33 (62.3) Note: a incident already reported in proof‐of‐concept trial, b WBC count in CSF<5cells/mm3

Chapter 2
58
The average reported incidence of ES was 13% (Tz: 11.1%, Ug: 15%) of which 67.9% were fatal. The
total hospitalization time was 27 and 32 days in Tanzania and Uganda respectively (range 3‐92).
Mean hospitalization time in our trials was 13 days (range 3 – 34) (p<0.0001). Treatment
adherence was better for the current trials than the historic data (97% vs 99%).
Comparison between trial and historic data for ES, case fatality rate (CFR) and hospitalization
time is shown in figure 3.
Table 6: Descriptive analysis of historic patient files.
Total Tanzania Uganda Number of patients 300 153 147 n % n % n %
Age, mean ± SD 29±16 34±171 25±172 Male/female ratio 1.4 2.5 0.8 Encephalopathic syndrome 39 13.0 17 11.1 22 15.0 Death 28 9.3 12 7.8 16 10.9 1missing values for age: 18, 2 missing values for age: 3

IMPAMEL III
59
Figure 3: Mean and 95% CI for ES, CFR and hospitalization time; trial data (solid line) and historic data
(dashed line).
Discussion
Given the differences between the two forms of HAT, the results of the IMPAMEL I & II programs
could not be directly extrapolated to T.b. rhodesiense patients. In the planning of the IMPAMEL III
program, treatment efficacy was not a major concern. On one hand the total exposure time of the
parasite to melarsoprol is similar in the empirical schedules and in the IMPAMEL schedule: a total
of 9 (3x3) or 12 (3x4) days spaced by resting periods versus a total of 10 consecutive days. On the
other hand the IMPAMEL schedule was extensively tested on T.b. gambiense and yielded similar
cure rates as empirical schedules (20). The main concerns were rather related to unexpected
toxicity. Given the already higher parasitaemia and reported incidence of ES in T.b. rhodesiense
patients, a further increase of ES under the 10‐day melarsoprol schedule could not be excluded.
0 5 10 15 20
Mean and confidence intervals of encephalopathic syndrome (ES) and case fatality rate (CFR)
Percentage of treated patients
ES: Historic data (n=300)
ES: IMPAMEL III (n=107)
CFR: Historic data (n=300)
CFR: IMPAMEL III (n=107)
10 15 20 25 30 35
Mean and confidence intervals of hospitalization time
Hospitalization time (days)
Historic data (n=300)
IMPAMEL III (n=107)

Chapter 2
60
However, evidence from studies in T.b. gambiense HAT showed that the pathogenesis of ES is an
immune phenomenon and dose independent (33). Hence, the 10‐day melarsoprol schedule should
theoretically not trigger an increase in the incidence of ES in T.b. rhodesiense patients.
Suramin pre‐treatment. Pre‐treatment with pentamidine and suramin have been given for
decades in the hope of reducing the risk for ES, but this remains unproved (14). In Kenya and the
northern parts of Malawi the suramin pre‐treatment is not administered. In Tanzania, a test dose
(5mg/kg) and a full dose (20mg/kg) are administered over a time period of 5 days. In Tanzania,
the pre‐treatment is not given to critically ill patients so as to quickly yield antitrypanosomal
activity in the CNS. In Uganda, a test dose (5mg/kg) is applied 1 day prior to LP which, from a
pharmacological point of view, is unlikely to efficiently clear trypanosomes as suramin is only
taken up slowly by the parasite (34).
Because we did not want to deviate from current national rules in one step, the assessment of the
ability of suramin pre‐treatment to prevent adverse drug reactions became part of the study
design.
In our data we observed more adverse events during the proof‐of‐concept trial in patients that
received suramin (63.3%) than in patients that were directly treated with melarsoprol (23.3%,
p=0.0018). Based on this result we decided to omit the suramin pre‐treatment in the utilization
study. In the pooled dataset, where none of the patients received suramin, the frequency of
adverse events was 61.7%. The difference in adverse events can most likely be explained by the
small sample size. However, no benefit of suramin pre‐treatment was observed over the direct
melarsoprol application.
Safety. 35% of the patients directly treated with melarsoprol had an event‐free treatment course.
Concomitant treatments were less frequently used in the trial population compared to the
historic data (p=0.0001), most likely indicating a better case management. Adverse events such as
vomiting, headache, skin reactions and fever were controllable with concomitant medications.
Skin reactions (rashes, pruritus) were a minor problem, reported in 6.5% of the patients. This was
surprisingly low given the high incidence of skin reactions in T.b. gambiense patients (28.4%) of
which 4.2% were fatal (bullous eruptions) (21).
The most relevant safety outcome of melarsoprol treatments is the incidence of serious adverse
events (ES and death). A systematic literature review on encephalopathic syndromes during
melarsoprol treatment of HAT (35) reported incidence rates of ES and death in T.b. rhodesiense
patients of 10.6% (1.5‐28%) and 11.6% (CI 5.2‐19%) respectively. In our historic data we found
centre‐specific incidence rates for ES and death of 13% (CI 9.2‐16.8%) and 9.3% (CI 6.0‐12.6). The
IMPAMEL III data reported ES and death of 11.2% (CI 5.1‐17.3) and 8.4% (CI 3‐13.8). Hence the 10‐

IMPAMEL III
61
day melarsoprol schedule appears not to have a higher safety risk than the national regimens in
use.
Findings from T.b. gambiense HAT of a higher risk for ES associated with the presence of
trypanosomes or more than 100 WBC in CSF (15) could not be confirmed. An immunological
background of ES was suspected for long and recent investigations indicating that a small number
of alleles of the human leukocyte antigen (HLA) were associated with a significantly increased
risk for ES have corroborated this hypothesis (35). During the proof‐of‐concept trial, patients
from Uganda developed more ES than patients in Tanzania (p=0.0444). However, the incidence of
ES equilibrated between the centres in the utilization study (p=0.5176) when steroids were
administered in both centres according the same guidelines. The evidence for the prevention of
ES with steroids in the literature is conflicting (16, 33), however, our data show a clear correlation
between the frequency of ES and the use of prednisolone.
Causes of death are difficult to establish under field conditions. To avoid bias we used a
composite safety endpoint of all‐cause mortality, also better suited for comparison of mortality
rates from literature and the historic data. We considered historic data as the most adequate
source for controls even though the reporting standards were rather poor in comparison to the
comprehensive documentation during the trials.
Efficacy. The historic data did not allow any elucidation of the efficacy of the standard treatment
regimens since systematic follow‐up of patients is not routinely implemented in East Africa. The
relapse rate for the 10‐day melarsoprol schedule in T.b. gambiense HAT was reported at 7.1% in a
controlled clinical trial (21). Due to the need for repeated lumbar punctures and possible long
distances to the health centres the follow‐up attendance is generally very low in T.b. rhodesiense
areas. Mobile teams for large scale population screenings are routinely present in T.b. gambiense
endemic regions and support the follow‐up activities effectively. Such teams are inexistent in East
Africa, requiring other approaches to support the patient follow‐up.
Follow‐up visits in T.b. gambiense areas are scheduled after 6, 12, 18 and 24 months. In clinical
trials, a test of cure visit 18 months after discharge is used to determine the efficacy of a treatment
under clinical development (36). Those recommendations are not suited for the virulent and fast
progressing T.b. rhodesiense HAT. To address this situation, the IMPAMEL III program scheduled
follow‐up visits after 3, 6 and 12 months. To anticipate missing data, the primary efficacy endpoint
was parasitological cure at end of treatment. The secondary efficacy endpoint was parasitological
cure at follow‐up examinations. Given the acuteness of this disease, relapses are certainly noted
by the patients and communities but not necessarily reported and re‐treated due to the

Chapter 2
62
difficulties described. We therefore engaged local leaders and community health workers to
collect information on the well‐being of patients who did not present for follow‐up examinations.
All IMPAMEL III trial participants will be followed for 12 months. The follow‐up of the proof‐of‐
concept trial has been completed as well as the 3 and 6 months follow‐up of patients enrolled into
the utilization study. The 12 months follow‐up of those patients is currently ongoing. We consider
the 6 months follow‐up as most adequate time point for the assessment of treatment efficacy in
T.b. rhodesiense HAT. At 12 months, follow‐up attendance is very poor and the risk of re‐
infections can not be disregarded. Therefore we present the efficacy data of the 10‐day
melarsoprol schedule in East Africa after the completion of the 6 months follow up; any relevant
changes until completion of the 12 months follow up would be communicated by the authors.
24 hours after treatment, all patients discharged alive (121/137) were free of parasites in blood and
CSF. 96% of all participants eligible for follow‐up in the proof‐of‐concept trial were in good
condition 12 months after discharge. One patient from Tanzania died due to causes not related to
HAT. In the pooled data set 97% of all participants eligible for follow‐up were in good condition 6
months after discharge. 1 patient from Uganda died, due to unknown reasons. A total of 2 relapses
were reported, both from patients allocated to the proof‐of‐concept trial (one in suramin and one
in the non‐suramin group). In one case the treatment was interrupted for 8 days because the
onset of ES after the 6th dose of melarsoprol. This patient presented two weeks after discharge
with trypanosomes in blood. For the other case, the relapse may likely be attributed to a re‐
infection according the patients account. Re‐infections are more common in the T.b. rhodesiense
HAT‐ The proximity of livestock and people increases the human‐fly contact. It is also known as
an occupational disease, putting hunters, fishermen, honey gatherers at higher risk of infection
(37). In terms of efficacy there is no evidence from the trials conducted against the use of the 10‐
day melarsoprol schedule in T.b. rhodesiense patients. The collection of oral information proved
to be a satisfactory tool as indicator for treatment efficacy in the absence of blood and CSF
examinations.
The IMPAMEL III trials were the first ones on T.b rhodesiense conducted in compliance with Good
Clinical Practice (GCP). It was of high priority by the WHO and the affected countries to offer
populations at risk of T.b. rhodesiense HAT an improved schedule for melarsoprol and, in view of
possible treatment failures the basis for potential combination treatments.
The conduct of the IMPAMEL III program strengthened local capacities especially for diagnosis,
patient management and reporting. Also disease awareness rose. Whereas the follow‐up activities
had to be extensively pushed during the proof‐of‐concept trial, access to follow‐up data has

IMPAMEL III
63
become easier during the second trial, most likely attributable to the better awareness among
patients and staff members.
The main bottleneck of clinical research in T.b. rhodesiense HAT is the limited number of patients
which impedes the conduct of properly powered trials. In two active foci a total of 138 second
stage patients were enrolled during two years of active and passive case detection, and efforts to
increase access to patients through involvement of communities and district officials for vector
control and disease surveillance. In contrast, a sample size of minimum 400 patients (200 per
arm) would have been required for the conduct of the IMPAMEL III program in the design of a
randomized control trial. However, case detection is significantly hampered by the low sensitivity
of the diagnostic tools and the prevalent lack of capacities for HAT diagnosis in the endemic
regions. Many cases die undetected, there are an estimated 12 undetected deaths per each
reported death (7).
Today, the biggest need for HAT affected populations is a new and safe treatment alternative.
This will sadly not be the case in the near future and melarsoprol will continue to play the central
role. Our results show that T.b. rhodesiense patients treated with the 10‐day melarsoprol schedule
were not subject to a higher incidence of serious adverse events (ES or death) than the historic
controls treated with the national regimens (see figure 3). Hence, evidence could be provided for
the improvement of the melarsoprol treatment schedule, the omission of the suramin‐pre‐
treatment and a standardized use of steroids. The hospitalization time was reduced from an
average of 29 days to 13 days (p<0.0001). Treatment adherence was very good; patients did not
abandon treatment as frequent as reported under the national schedules in use. Further, the fixed
dosing of 2.2mg/kg/day is less prone to dosing mistakes than varying dosing throughout
treatment. This represents substantial advantages to the patients and the health care provider.
However, as in T.b. gambiense HAT, ES still occur and continue to pose a major threat to the
patients treated.
This study will be presented during the next 30th ISCTRC Meeting in Entebbe, Uganda, 21‐25
September 2009. It is expected that WHO and the T.b. rhodesiense affected countries will discuss
the introduction of the 10‐day melarsoprol schedule in East Africa according the available data.
Acknowledgements
We are indebted to our patients and their families as well as to all members of the Kaliua Health
Centre and the Lwala Hospital for their continuous support of the IMPAMEL III trials. The Ministry
of Health in Uganda, in particular Dr. Mbulamberi and the National Institute for Medical

Chapter 2
64
Research in Tanzania, in particular Dr. Andrew Kitua and Dr. Joyce Ikingura are acknowledged
for facilitating the trials in their countries. We thank the committed drivers, without their
concerted efforts the sites would have never been reached. We acknowledge the members of the
safety advisory board: Professor Michael Schumacher (University of Freiburg, Germany),
Professor Lars Rombo (University of Eskilstuna, Sweden), Dr. Anne Moore (CDC Atlanta, USA),
Dr. Martin Odiit (Uganda AIDS Control Project, formerly Sleeping Sickness Program, Livestock
Health Research Institute, Uganda). Sincere thanks go to Dr. Pere Simarro (WHO) and Dr. Jose
Ramon Franco (WHO) for their valuable input and the supply of study drugs. The project
assistant Monique Vogel was supportive in operations and administration. EURMOMEDIX is
acknowledged for its courtesy to provide the whole blood test system Cardio ChekTM PA free of
cost.

IMPAMEL III
65
References
1. Kennedy PG. The continuing problem of human African trypanosomiasis (sleeping sickness). Ann Neurol. 2008 Aug;64(2):116‐26.
2. Checchi F, Filipe JA, Haydon DT, Chandramohan D, Chappuis F. Estimates of the duration of the early and late stage of gambiense sleeping sickness. BMC Infect Dis. 2008;8:16.
3. Odiit M, Kansiime F, Enyaru JC. Duration of symptoms and case fatality of sleeping sickness caused by Trypanosoma brucei rhodesiense in Tororo, Uganda. East Afr Med J. 1997 Dec;74(12):792‐5.
4. WHO. Control and surveillance of African trypanosomiasis. Geneva: WHO; 1998.
5. WHO. Human African trypanosomiasis (sleeping sickness): epidemiological update. Weekly epidemiological record. 2006 24. Februar(TRS881):69‐80.
6. Bales JD. African Trypanosomiasis. In: Strickland GT, editor. Hunter's Tropical Medicine. 7 ed. Philadelphia: Saunders Company; 1988. p. 617‐28.
7. Odiit M, Coleman PG, Liu WC, McDermott JJ, Fevre EM, Welburn SC, et al. Quantifying the level of under‐detection of Trypanosoma brucei rhodesiense sleeping sickness cases. Trop Med Int Health. 2005 Sep;10(9):840‐9.
8. Fevre EM, Coleman PG, Odiit M, Magona JW, Welburn SC, Woolhouse ME. The origins of a new Trypanosoma brucei rhodesiense sleeping sickness outbreak in eastern Uganda. Lancet. 2001 Aug 25;358(9282):625‐8.
9. Fevre EM, Odiit M, Coleman PG, Woolhouse ME, Welburn SC. Estimating the burden of rhodesiense sleeping sickness during an outbreak in Serere, eastern Uganda. BMC Public Health. 2008;8:96.
10.Kaare MT, Picozzi K, Mlengeya T, Fevre EM, Mellau LS, Mtambo MM, et al. Sleeping sickness‐‐a re‐emerging disease in the Serengeti? Travel Med Infect Dis. 2007 Mar;5(2):117‐24.
11. Iten M, Matovu E, Brun R, Kaminsky R. Innate lack of susceptibility of Ugandan Trypanosoma brucei rhodesiense to DL‐alpha‐difluoromethylornithine (DFMO). Trop Med Parasitol. 1995 Sep;46(3):190‐4.
12.Priotto G, Kasparian S, Ngouama D, Ghorashian S, Arnold U, Ghabri S, et al. Nifurtimox‐eflornithine combination therapy for second‐stage Trypanosoma brucei gambiense sleeping sickness: a randomized clinical trial in Congo. Clin Infect Dis. 2007 Dec 1;45(11):1435‐42.
13.Friedheim EAH. Mel B in the treatment of human trypanosomiasis. American Journal of Tropical Medicine and Hygiene. 1949;29:173‐80.
14.Pepin J, Donelson JE. African Trypanosomiasis (Sleeping Sickness). In: Guerrant RL, Walker DH, Weller PF, editors. Tropical Infectious Diseses; Principles, Pathogens & Practise. 1 ed. Philadelphia: Churchill Livistone; 1999. p. 774‐84.
15.Pepin J, Milord F, Khonde AN, Niyonsenga T, Loko L, Mpia B, et al. Risk factors for encephalopathy and mortality during melarsoprol treatment of Trypanosoma brucei gambiense sleeping sickness. Trans R Soc Trop Med Hyg. 1995 Jan‐Feb;89(1):92‐7.
16.Arroz JO. Melarsoprol and reactive encephalopathy in Trypanosoma brucei rhodesiense. Trans R Soc Trop Med Hyg. 1987;81(2):192.
17.Onyango RJ, Bailey NM, Okach RW, Mwangi EK, Ogada T. Encephalopathy during treatment of human trypanosomiasis. EATRO report. 1969.
18.Foulkes JR. An evaluation of prednisolone as a routine adjunct to the treatment of T. rhodesiense. Journal of Tropical Medicine and Hygiene. 1975;78:72‐4.

Chapter 2
66
19.Burri C, Nkunku S, Merolle A, Smith T, Blum J, Brun R. Efficacy of new, concise schedule for melarsoprol in treatment of sleeping sickness caused by Trypanosoma brucei gambiense: a randomised trial. Lancet. 2000 Apr 22;355(9213):1419‐25.
20.Schmid C, Nkunku S, Merolle A, Vounatsou P, Burri C. Efficacy of 10‐day melarsoprol schedule 2 years after treatment for late‐stage gambiense sleeping sickness. Lancet. 2004 Aug 28;364(9436):789‐90.
21.Schmid C, Richer M, Bilenge CM, Josenando T, Chappuis F, Manthelot CR, et al. Effectiveness of a 10‐Day Melarsoprol Schedule for the Treatment of Late‐Stage Human African Trypanosomiasis: Confirmation from a Multinational Study (Impamel II). J Infect Dis. 2005 Jun 1;191(11):1922‐31.
22.Legros D, Evans S, Maiso F, Enyaru JCK, Mbulamberi D. Risk factors for treatment failure after melarsoprol for Trypanosoma brucei gambiense trypanosomiasis in Uganda. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1999;93:439‐42.
23.Matovu E, Iten M, Enyaru JC, Schmid C, Lubega GW, Brun R, et al. Susceptibility of Ugandan Trypanosoma brucei rhodesiense isolated from man and animal reservoirs to diminazene, isometamidium and melarsoprol. Trop Med Int Health. 1997 Jan;2(1):13‐8.
24.Stanghellini A, Josenando T. The situation of sleeping sickness in Angola: a calamity. Tropical Medicine and International Health. 2001;6(5):330‐4.
25.Robays J, Bilengue MMC, Stuyft PVd, Boelaert M. The effectiveness of active population screening and treatment for sleeping sickness control in the Democratic Republic of Congo. Tropical Medicine & International Health. 2004;9:542.
26.Apted FI. Four years' experience of melarsen oxide/BAL in the treatment of late‐stage Rhodesian sleeping sickness. Trans R Soc Trop Med Hyg. 1957 Jan;51(1):75‐86.
27.Foulkes JR. Metronidazole and suramin combination in the treatment of arsenical refractory Rhodesian sleeping sickness‐‐a case study. Trans R Soc Trop Med Hyg. 1996 Jul‐Aug;90(4):422.
28.Bales J, Harrsion S, Mbwabi D. The treatment of Rhodesian sleeping sickness. A review of 46 cases. Manuscript. 1988:11p.
29.Robertson DH. The treatment of sleeping sickness (mainly due to Trypanosoma rhodesiense) with melarsoprol. I. Reactions observed during treatment. Trans R Soc Trop Med Hyg. 1963 Mar;57:122‐33.
30.Kibona SN, Matemba L, Kaboya JS, Lubega GW. Drug‐resistance of Trypanosoma b. rhodesiense isolates from Tanzania. Trop Med Int Health. 2006 Feb;11(2):144‐55.
31.Apted FIC. Present status of chemotherapy and chemoprophylaxis of human trypanosomiasis in the eastern hemisphere. Pharmacology and Therapeutics. 1980;11:391‐413.
32.Woo PT. The haematocrit centrifuge for the detection of trypanosomes in blood. Can J Zool. 1969 Sep;47(5):921‐3.
33.Pepin J, Milord F, Guern C, Mpia B, Ethier L, Mansinsa D. Trial of prednisolone for prevention of melarsoprol‐induced encephalopathy in gambiense sleeping sickness. Lancet. 1989 Jun 3;1(8649):1246‐50.
34.McGeary RP, Bennett AJ, Tran QB, Cosgrove KL, Ross BP. Suramin: clinical uses and structure‐activity relationships. Mini Rev Med Chem. 2008 Nov;8(13):1384‐94.
35.Seixas J. Investigations on the encephalopathic syndrome during melarsoprol treatment in human African trypanosomiasis [PhD Thesis]: Basel; 2004.
36.WHO. Recommendations of the Informal Consultation on Issues for Clinical Product Development for Human African Trypanosomiasis. Geneva, Switzerland; 2007. Report No.: WHO/CDS/NTD/IDM/2007.1.
37.Pepin J, Meda HA. The epidemiology and control of human African trypanosomiasis. Adv Parasitol. 2001;49:71‐132.

Molecular epidemiology
67
Chapter 3
Molecular characterization of trypanosomes from clinical
trial patients in Uganda and Tanzania
Enock Matovu1*, Irene Kuepfer2, Alex Boobo1, Stafford Kibona3, Christian Burri2
1Makerere University, Kampala, Uganda, 2Swiss Tropical Institute, Basel, Switzerland, 3National
Institute for Medical Research, Tabora, Tanzania.
Submitted to the Journal of Tropical Medicine & International Health
Blood sample collection at Kaliua Health Centre, Tanzania

Chapter 3
68
Abstract
OBJECTIVE The samples for this study were collected in the context of the IMPAMEL III trials
(Improved Application of Melarsoprol), two clinical trials assessing the short melarsoprol
treatment schedule for T. b. rhodesiense HAT. Our aim was to characterize the infections from
consenting patients as truly T. b. rhodesiense.
METHODS We analyzed DNA eluted from FTA cards spotted with blood from late stage HAT
patients. PCR for the Serum Resistance Associated (SRA) gene specific for T. b. rhodesiense and
the T. gambiense specific surface glycoprotein (TgSGP) were done. In addition, the Loop mediated
isothermal amplification (LAMP) of DNA targeting the Trypanozoon conserved Random Inserted
Mobile Element (RIME) and that for the SRA were performed.
RESULTS AND CONCLUSIONS: Out of 128 samples analyzed SRA‐PCR was positive in 101 (78.9%
sensitivity; 95% confidence interval of 71.1‐85.1%), the SRA‐LAMP positive in 120 (93.8%, with
88.2‐96.8% as the 95% CI), while RIME‐LAMP revealed signals in 122 (95.3%; 95% CI=90.2‐97.8%).
No amplification was possible from 3 samples, whereas all the 128 were as well negative for the
TgSGP‐PCR and a sample with known T. b. gambiense included as a control was positive.
All the successfully analysed samples were confirmed to contain T. b. rhodesiense based on the
subspecies specific PCR and/or LAMP, while signals for the TgSGP were absent. Thus the results
of IMPAMEL III will represent a true picture of the short concise melarsoprol treatment schedule
against the acute form of HAT, at least for patients from whose FTA cards DNA was successfully
amplified.
Key words: Human African trypanosomiasis (HAT), Trypanosoma brucei rhodesiense; T. b.
gambiense, molecular diagnosis.

Molecular epidemiology
69
Introduction
Effective control of Human African Trypanosomiasis is still hampered by unsatisfactory
diagnostics and limited options for chemotherapeutic intervention. Within health units, it is still
not possible to distinguish between T.b. rhodesiense (the acute form of eastern and southern
Africa) and T.b. gambiense (the chronic form of central and western Africa) infections. Thus other
parameters, mainly geographical location of the patients, case history and clinical presentation,
are used to determine the most probable subspecies in question. This becomes problematic in
areas close to borders between traditional ranges of the two diseases and also where new, non‐
historical foci emerge (1, 2).
Unequivocal identification of human infective trypanosomes up to the subspecies level is only
possible by molecular tools. These are PCR based, targeting the Serum Resistance Associated
(SRA) gene that is specific for T.b. rhodesiense (3‐5), or the T.b. gambiense Surface Glycoprotein
(TgSGP) that is diagnostic for that subspecies (6, 7). The need for specialized equipment and
constant supply of electricity has hindered integration of those techniques into the diagnostic
algorithm. Yet the type of infection directs the choice of treatment: Melarsoprol which was the
standard treatment for second stage human African trypanosomiasis (HAT) over more than 50
years frequently causes severe adverse drug reactions. T. b. gambiense infections are increasingly
treated with eflornithine which is significantly better tolerated (8) whereas for late stage T.b.
rhodesiense infections melarsoprol is the only choice due to innate resistance of this subspecies to
eflornithine (9). Since its discovery as a late stage HAT drug in 1949, melarsoprol (10) use has for
decades followed an empirical rather than rational approach. After elucidation of its
pharmacokinetics (11, 12), a rational schedule was proposed that was subsequently evaluated
against T.b. gambiense under the projects “Improved Application of Melarsoprol (IMPAMEL I and
II)”. At the request of the World Health Organization (WHO), by the International Scientific
Council for Trypanosomiasis Research and Control (ISCTRC), it was recommended as the
standard schedule (13‐16). Within the framework of the IMPAMEL III program, two multiple site
clinical trials were conducted in order to assess the safety, tolerability and efficacy of the 10‐day
melarsoprol schedule against T.b. rhodesiense sleeping sickness. Vicinity of one of the centres to
T.b. gambiense endemic areas, while the other is home to refugees from central Africa, provided a
possibility that both disease forms could co‐exist in the same epidemics. This study aimed at the
detection of potentially existing T.b. gambiense cases in T.b. rhodesiense foci and to characterize
the infections from consenting patients at the two centres as truly T.b. rhodesiense in order to
authenticate conclusions to be drawn from IMPAMEL III as a correct description of this schedule in
the acute form of HAT.

Chapter 3
70
Materials and methods
Study Sites
The IMPAMEL III program has been carried out at Lwala Hospital, Kaberamaido District in south‐
eastern Uganda and at Kaliua Health Centre, Urambo District in north‐western Tanzania. Lwala
Hospital (Northing 36N 0530894; Easting UTM 0205802) is located in an area over 100km outside
the historic T.b. rhodesiense (Busoga and Tororo) focus. Over the past 5 years the disease has
spread into districts previously free of sleeping sickness (Soroti, Kaberamaido, Dokolo) through
the movement of infected livestock. In 2004, the Lwala Hospital diagnosed the first cases of
sleeping sickness and experienced an outbreak in 2004/2005 with over 400 patients treated.
Today, the area is endemic for sleeping sickness.
Kaliua Health Centre, a missionary hospital established in 1997, is located (latitude: 5.05639,
longitude: 31.79462) within the major sleeping sickness endemic area of north‐western Tanzania.
The first cases (thought to have been T.b. gambiense) were reported in the 1920s. Presently, the
area is a known T.b. rhodesiense focus that experienced an epidemic outbreak in. 2004/2005,
during which about 300 cases were reported.
The IMPAMEL III program received ethical clearance from the Ministry of Health, Uganda, the
National Institute for Medical Research, Tanzania and from Switzerland (Ethics Committees of
both Cantons of Basel). The program was also registered with the Current Controlled Trials
database (ISRCTN40537886). These clearances refer to the entire IMPAMEL III, one of whose
objectives was to collect blood samples for identification of infecting trypanosomes in potential
overlap areas that is here reported.
Study conduct and study population
The clinical trials were initiated in August 2006 and enrolment was terminated in August 2008. In
this time period a total of 138 patients were enrolled (Uganda: 69, Tanzania: 69). All trial
participants were treated with the 10‐day melarsoprol schedule and asked to present for follow‐up
examinations after 3, 6 and 12 months in order to confirm the absence of the parasite in blood and
cerebrospinal fluid (CSF). Eligible for enrolment were patients ≥ 6 years of age with confirmed
late stage sleeping sickness (presence of the parasite in the CSF and/or ≥5 white blood cells
(WBC) per mm3), pregnant women and moribund or unconscious patients were excluded.
Written informed consent was obtained from all trial participants. For the participation of
children and adolescents (below 18 years) the parents, the legal representative or the guardian
gave written informed consent.

Molecular epidemiology
71
Sample collection and DNA preparation
Blood samples were collected on FTA cards (Whatman) by making 4 spots using the blood
remaining after diagnostic procedures. About 200μl was applied on each spot and the coded cards
were allowed to air dry. The FTA cards were enclosed in self sealing bags containing silica and
transported to the laboratory where they were stored at 4oC. Trypanosome DNA adhering to the
FTA cards was cleared of blood contaminants and PCR inhibitors using the FTA purification
reagent following the manufacturer’s instructions. A 2.0 mm disc was punched from a dried blood
spot using a Harris micro punch tool (Whatman). After 3 washes with 200μl of FTA purification
reagent and 5 minute incubations between washes at room temperature, the FTA reagent was
removed and the disc rinsed twice in a similar manner with 200μl TE buffer. The buffer was
discarded and the disc carrying purified DNA air‐dried at room temperature. From each card
(patient), 5 such discs were prepared and finally pooled in a single tube per patient after drying.
The DNA was then eluted from the discs by incubating in 100μl of a 5% chelex suspension at 90oC
for 30 minutes (17). After a pulse spin at 13000g, the eluted DNA was pipetted off and used
immediately, or stored at ‐20 for use within 3 days of its preparation. In all subsequent
amplifications, 5μl of the DNA solution was added as the template.
PCR for the SRA and TgSGP genes
PCR for the SRA gene was carried out in nested manner as described by Maina et al. 2007 (18)
using the primers SRA‐outer‐s 5´‐CTGATAAAACAAGTATCGGCAGCAA‐3´; SRA‐outer‐as 5´‐
CGGTGACCAATTCATCTGCTGCTGTT‐3´ and 5μl of eluted DNA in a 25μl reaction. For the
second PCR, 3μl of the first product was included as template in the reaction with the primers
SRA‐inner‐s 5´‐ATAGTGACATGCGTACTCAACGC‐3´); SRA‐inner‐as 5´‐AATGTGTTCGAGTACTT
CGGTCACGCT‐3´. Similarly, nested PCR for the T. b. gambiense specific gene was done with the
primers TgSGP‐outer‐s 5´‐GCGTATGCGATACCGCAGTAA‐3´ and TbsGP‐outer‐as 5´‐
CTTCAACCGCCGCTGCTTCTA‐3_ as well as TbsGP‐s 5´‐GCTGCTGTGT TCGGAGAGC‐3´) and
TgSGP‐as 5´‐GCCATCGTGCTTGCCGCTC‐3´. In all cases, the annealing temperature was
maintained at 60oC for 1 minute, the same timing allowed for denaturation and extension. Initial
denaturation was at 94oC for 5 minutes. PCR products were loaded on 2% agarose and stained
with ethidium bromide for UV trans‐illumination.

Chapter 3
72
Loop Mediated Isothermal Amplification (LAMP) of the SRA gene and the
Random Insertion Mobile Element (RIME)
For the SRA‐LAMP, we made use of primers recently described by Njiru et al. 2008 (19) namely
SRA‐F3 GCGGAAGCAAGAATGACC, SRA‐B3 CTTACCTTGTGACGCCTG,
SRA‐FIP GGA CTGCG TTGAGTACGCATCCGCAAGCACAGACCACAGC,
SRA‐BIP CGCTCTTACAAGTCTTGCGCCCTTCTGAGATGTGCCCACTG,
SRA‐LF CGCGGCATAAAGCGCTGAG,
and SRA‐LB GCAGCGACCAACGGAGCC. The total reaction volume was 25μl into which the
above primers were added to final concentrations of 0.2μM of F3 and B3, 2μM for FIP and BIP, and
0.8μM of LF and LB. In addition 200μM dNTPs, 0.8M Betaine and 8U of Bst polymerase (Large
fragment; New England Biolabs) was added to the mix containing 1X reaction buffer supplied with
the enzyme. To this 4μl of DNA eluted from the FTA cards was added to make up to 25μl total
reaction volume. The reaction was incubated for 1 hour at 62oC followed by inactivation of the Bst
polymerase at 80oC for 4 minutes. Two micro litres of a 1/20 dilution of SYBR Green in water was
then added and the tube gently agitated as it was observed for colour change.
Similar conditions and reagent concentrations were applied for the RIME‐LAMP using the
primers described by Njiru et al.2008 (20).
Results
The content of this paper is limited to the characterization of infecting trypanosomes in patient
blood spotted on FTA cards. The results of the clinical trials and the patient follow‐up are
reported elsewhere (Kuepfer et al., manuscript in preparation).
A total of 128 samples (59 from Uganda and 69 from Tanzania) were analyzed. Signals could be
obtained from PCR only after nesting with products of the first round amplification. Even then,
TgSGP‐PCR was only positive in a laboratory strain included as a control (Figure 1.), but yielded
no signal from any of the DNAs eluted from FTA cards. Overall, SRA‐PCR was positive in 101
samples (78.9% sensitivity; 95% CI of 71.1‐85.1%),), but was less sensitive for samples from
Tanzania (49/69; 71.0% with 95% CI of 59.4‐80.4%) than for Ugandan samples (52/59; 88.1% with
95% CI of 77.5‐94.1%). The difference was significant (χ2 = 5.6; P = 0.018) and could not be
attributed to differences in parasitaemia. All the cases, but one Ugandan, had parasites
demonstrated in stained smears at diagnosis (table 1), indicating presence of similar parasite
numbers within the samples. So the observed difference could have been a result of an event

Molecular epidemiology
73
happening at some stage from FTA preparation, storage, or transportation to Makerere
University.
SRA‐LAMP on the other hand was positive in 120 of the cases, yielding an overall sensitivity of
93.8% (88.2‐96.8% as the 95% CI). Upon discrimination between the 2 centres, it was found
positive in 66/69 samples from Tanzania (95.7% sensitivity; 95% CI of 88.0‐98.5%) while Ugandan
samples (54/59) could be detected with 91.5% sensitivity (95% CI=81.7‐96.3%). The difference in
sensitivity of SRA‐LAMP for the two countries was insignificant (χ2 = 0.9; P >0.05).
RIME‐LAMP detected the highest number of cases and was positive in 122 samples, giving an
overall sensitivity of 95.3% (95% CI=90.2‐97.8%). It missed 2 samples from Tanzania (97.1%
sensitivity; 95% CI=90.0‐99.2%) and 4 from Uganda (93.2% sensitivity; 95% CI=83.8‐97.3%): this
was again not a significant difference in sensitivity of RIME‐LAMP in samples from the 2
countries (χ2 = 1.1; P >0.05).
For all the 4 methods executed, no amplification was possible in 3 of the samples from Uganda,
although trypanosomes had been demonstrated in stained smears. Amplification results were
consistent with those expected from the control samples: SRA‐PCR and both LAMPs were
positive in the laboratory T. b. rhodesiense strain (ALo1), while RIME‐LAMP but not SRA‐PCR or
SRA‐LAMP was positive for the T. b. brucei strain (GVR35, table 1)
Discussion
Continued lack of new drugs is a serious problem for HAT control whose mainstay is
chemotherapeutic intervention. The latest drug to have been registered is eflornithine, way back
in the 1990s following its evaluation against T.b. gambiense (21). More recently, the clinical
programme assessing pafuramidine maleate (DB289) was terminated in Phase III due to
previously unobserved toxicity (22). Thus for a long time to come control will still solely depend
on the existing “ancient” tools of which melarsoprol continues to play a central role particularly
for treatment of T.b. rhodesiense. The IMPAMEL III trials were conducted to assess the safety and
efficacy of the abridged 10‐day schedule recently recommended for treatment of late stage T.b.
gambiense sleeping sickness with melarsoprol (13‐16). The alternative treatment schedule is
advantageous because of its practical application (no dose adjustments, shortened treatment) and
the apparent socio‐economic advantages (shorter hospitalisation, less drug per patient, cheaper,
increased hospital capacity). However, it remained uncertain whether the observation could be
extrapolated to the case of the acute T.b. rhodesiense. Some fears could arise from the school of
thought that melarsoprol accumulation in the central nervous system could be different in the

Chapter 3
74
two disease forms, probably resulting from differential damage to the blood‐brain‐barrier by the
two sub‐species. The major problem with melarsoprol is characteristic encephalopathic
syndromes that occur in up to 10% of treated patients (23) leading to the death of about 50% of
those affected (24). It was therefore essential that patients enrolled to the IMPAMEL III trials were
confirmed as true T.b. rhodesiense infections, especially given the epidemiological circumstances
at each of the two trial sites. Lwala hospital caters for the new outbreak areas stretching as far
north as Lira District where a T.b. rhodesiense was isolated within 150km of known T.b. gambiense
foci (2). North‐western Tanzania on the other hand has over the past decade seen refugee influx
from areas affected by civil strife in Central Africa. These refuges are feared to be a possible route
of introduction of T.b. gambiense to co‐exist with the east and southern African disease. In this
study, we have not encountered any T.b. gambiense in samples taken at the two centres until
August 2008, as determined by specific PCRs and LAMP. This data is welcome given the risk of
the possible co‐existence of the two subspecies. If they become sympatric, it will be a great
challenge for HAT control and create a major public health problem. Patient management
requires high‐level, disease‐specific expertise for proper diagnosis, treatment and follow‐up of the
patients. In the case of diagnosis: screening with the Card Agglutination Test for Trypanosomiasis
(CATT) (25) is part of the diagnostic algorithm for T.b. gambiense (26), but the test misses most
T.b. rhodesiense infections. On one hand, the latter has no field adapted serological screening and
all suspicious cases are directly subjected to the laborious parasitological tests. On the other
hand, if used for screening without concentration of the body fluids, parasitological tests are
likely to miss more T.b. gambiense due to the characteristically lower parasitaemia than the acute
disease. In addition, medical staff used to the prominent appearance of T.b. rhodesiense infections
might inevitably overlook a T.b. gambiense infection which is characterized by rather unspecific
and often subtle signs and symptoms. Thus, co‐existence of the two could lead to a number of
patients passing undetected by inappropriate diagnostic approaches.
For treatment, it is known that T.b. rhodesiense exhibits innate resistance to eflornithine (9), such
that any such diagnosed in presumed T.b. gambiense foci is likely to be non‐responsive to this
intervention. Further, patients generally present in very advanced disease stages. Given the
acuteness of T.b. rhodesiense HAT, there is not much time left to initiate treatment and major
delays can be fatal.
Molecular diagnostics are theoretically of unmatched sensitivity since they involve amplification
of specific targets within the parasite. Although they are of unrivalled specificity, these methods
when used for HAT detection so far fall short of the expected sensitivity and usually yield much
lower figures when compared to parasitological methods. The main reason behind this are the

Molecular epidemiology
75
characteristically low parasitaemia in HAT and the fact that the patient tissue (blood or CSF) has
to be processed to isolate DNA and get rid of potential PCR inhibitors. It is inevitable that during
the elaborate purification processes, some of the scanty parasite DNA could be lost. Besides, the
subspecies specific targets happen to be single copy genes whose abundance in a low parasitaemic
tissue is further compromised. Thus, nested PCR has to be done to amplify the SRA and TgSGP to
a level that can be visualized on a gel, adding to the duration between sampling and actual
reading of the results. For those reasons and the high level technology required, it is presently
inconceivable that PCR based methods will in the near future be integrated into routine point of
care diagnosis.
This is the first study to publish data on such a big collection of field samples. It has generated
current information on the potential strain overlap and allowed for comparison of molecular
diagnostic techniques that would otherwise not have been possible. Of particular interest was the
use of the recently published LAMP tests (19, 20). Although our primary aim was to identify
infecting subspecies, it gave an opportunity to gain insights into the diagnostic potential of this
technique. The sensitivities observed in this study (compared to PCR based methods) are the
highest so far reported, yet the method is relatively easier to execute. Comparing RIME‐LAMP to
SRA‐PCR, there was a poor agreement between the two tests (kappa 0.11) with the latter detecting
only 80.3% of the samples detected by RIME‐LAMP as positive (n=122). This points to a significant
difference in sensitivities of the two tests (χ2 = 15.3; P<0.001). Similarly, there was poor agreement
between SRA‐PCR and SRA‐LAMP (Kappa 0.08) and the former detected 80% of the samples
SRA‐LAMP confirmed as positive. The difference in sensitivities of SRA‐PCR (78.9%) and SRA‐
LAMP (93.8%) was found to be significant (χ2 = 11.9; P=0.001). Neither was there a strong
agreement between SRA‐LAMP and RIME‐LAMP (kappa value 0.39): however, the former
detected 95.9% of what RIME‐LAMP detected as positive. Their overall sensitivities were 93.8%
and 95.3% respectively, and there was no significant difference between the two (χ2 = 0.302;
P>0.05). That means that either test can be reliably used to detect HAT due to T.b. rhodesiense.
The advantages of LAMP can not be over emphasized: we could get results within 1 hour of
initiation by adding SYBR Green and observing for colour change as previously reported (19, 20).
LAMP therefore has great potential application in resource poor settings since it can as well be
done in a water bath. What would be required is further reduction of required manipulations by
provision of kits in which all reactants (preferably lyophilized) are included. In this way,
personnel at the diagnostic centre would only need to add the reaction buffer and patient sample
before starting the reaction. LAMP could also be used to confirm cure. Our results warrant bigger
case‐control studies to particularly generate more data on sensitivity, specificity as well as positive

Chapter 3
76
and negative predictive values of LAMP. This will pave the way for its implementation as a
routine diagnostic which may eventually decrease the number of cases that still go undetected by
the characteristically low sensitivity of parasitological tests in current use. Efforts should also be
made to devise a T.b. gambiense specific LAMP based on TgSGP, to keep track of possible merger
of the two diseases in suspect epidemics.
It has to borne in mind however, that even in presence of molecular diagnostics of unprecedented
sensitivity, HAT case definition will remain demonstration of trypanosomes in some body fluid.
The molecular methods will nevertheless go a long way to detect aparasitaemic cases on which
extra effort will be made by health personnel to search for trypanosomes before prescriptions can
be made.
Acknowledgements
The authors wish to acknowledge Dr. Emma Peter Hhary and Betty Akello as well as the entire
teams at Lwala Hospital and Kaliua Health Centre for their active participation during sampling,
treatment and follow‐up of the trial participants. Dr. Abbas Kakembo at the Uganda Ministry of
Health, Dr. Mpairwe Allan and Dr. Andrew Edielu of Lwala Hospital as well as Dr. Lucas
Matemba are acknowledged for their untiring support throughout the project. Dr. John Enyaru
(Makerere University Faculty of Science) is thanked for provision of some of the LAMP primers.
Funding was provided by the Swiss Agency for Development and Cooperation (SDC) Grant
Number 7F‐01977.02 (phase extension), the International Consortium for Parasitic Drug
Discovery (CPDD) led by the University of North Carolina, Chapel Hill, USA which is supported
by the Bill & Melinda Gates Foundation, the Swiss Tropical Institute and the Makerere University
Faculty of Veterinary Medicine to whom we are indebted.

Molecular epidemiology
77
Trypanosomes were demonstrated by stained smears in all except 12008, indicating comparable
parasitaemia that should have been detected by molecular methods. All patient samples analysed
were negative for the T. b. gambiense specific (TgSGP)‐PCR. n.a.= not applicable.
Table 1. Samples for which the SRA‐PCR or LAMP were negative.
Code Site Stained blood SRA‐PCR SRA‐LAMP RIME‐LAMP 11007 Kaliua + ‐ + + 11013 Kaliua + ‐ + + 11020 Kaliua + + + ‐ 11025 Kaliua + + ‐ + 11035 Kaliua + + + ‐ 11038 Kaliua + + ‐ + 11044 Kaliua + + ‐ + 11050 Kaliua + ‐ + + 11051 Kaliua + ‐ + + 11052 Kaliua + ‐ + + 11053 Kaliua + ‐ + + 11054 Kaliua + ‐ + + 11055 Kaliua + ‐ + + 11056 Kaliua + ‐ + + 11057 Kaliua + ‐ + + 11058 Kaliua + ‐ + + 11059 Kaliua + ‐ + + 11060 Kaliua + ‐ + + 11061 Kaliua + ‐ + + 11062 Kaliua + ‐ + + 11063 Kaliua + ‐ + + 11064 Kaliua + ‐ + + 11065 Kaliua + ‐ + + 11066 Kaliua + ‐ + + 11068 Kaliua + ‐ + + 12004 Lwala + + ‐ + 12006 Lwala + ‐ + + 12008 Lwala ‐ ‐ + + 12009 Lwala + ‐ + + 12025 Lwala + + + ‐ 12041 Lwala + + ‐ + 12058 Lwala + ‐ + + 12061 Lwala + ‐ ‐ ‐ 12062 Lwala + ‐ ‐ ‐ 12065 Lwala + ‐ ‐ ‐ ALo1 Lab T.b.rh n.a. + + ‐ GVR35 Lab T.b.b. n.a. ‐ ‐ +

Chapter 3
78
Figure 1: Representative gels to show signals obtained for the SRA‐ and TgSGP‐ PCRs from corresponding
templates. Lane 1 had laboratory T. b. rhodesiense strain (ALO1) and lane 2 had the Laboratory T. b.
gambiense strain (ELIANE) while lanes 3‐10 had samples from patients. No TgSGP signals were obtained
from any of the FTA cards spotted with patient blood.
Figure 2. Representative RIME‐LAMP reactions from selected patient samples. Templates in tubes 1‐18 were
samples from Tanzania while 19‐38 contained samples from Uganda. Tube 39 had the laboratory T. b.
rhodesiense (ALo1), tube 40 had the laboratory T. b. brucei (GVR35) while tubes 41 and 42 were negative
controls in which 5μl water was added as template.

Molecular epidemiology
79
References
1. Fevre EM, Coleman PG, Odiit M, Magona JW, Welburn SC, Woolhouse ME. The origins of a new Trypanosoma brucei rhodesiense sleeping sickness outbreak in eastern Uganda. Lancet. 2001 Aug 25;358(9282):625‐8.
2. Picozzi K, Fevre EM, Odiit M, Carrington M, Eisler MC, Maudlin I, et al. Sleeping sickness in Uganda: a thin line between two fatal diseases. Bmj. 2005 Nov 26;331(7527):1238‐41.
3. De Greef C, Chimfwembe E, Kihang'a Wabacha J, Bajyana Songa E, Hamers R. Only the serum‐resistant bloodstream forms of Trypanosoma brucei rhodesiense express the serum resistance associated (SRA) protein. Ann Soc Belg Med Trop. 1992;72 Suppl 1:13‐21.
4. Gibson W, Backhouse T, Griffiths A. The human serum resistance associated gene is ubiquitous and conserved in Trypanosoma brucei rhodesiense throughout East Africa. Infect Genet Evol. 2002 May;1(3):207‐14.
5. Radwanska M, Chamekh M, Vanhamme L, Claes F, Magez S, Magnus E, et al. The serum resistance‐associated gene as a diagnostic tool for the detection of Trypanosoma brucei rhodesiense. Am J Trop Med Hyg. 2002 Dec;67(6):684‐90.
6. Berberof M, Perez‐Morga D, Pays E. A receptor‐like flagellar pocket glycoprotein specific to Trypanosoma brucei gambiense. Mol Biochem Parasitol. 2001 Mar;113(1):127‐38.
7. Radwanska M, Claes F, Magez S, Magnus E, Perez‐Morga D, Pays E, et al. Novel primer sequences for polymerase chain reaction‐based detection of Trypanosoma brucei gambiense. Am J Trop Med Hyg. 2002 Sep;67(3):289‐95.
8. Chappuis F, Udayraj N, Stietenroth K, Meussen A, Bovier PA. Eflornithine is safer than melarsoprol for the treatment of second‐stage Trypanosoma brucei gambiense human African trypanosomiasis. Clin Infect Dis. 2005 Sep 1;41(5):748‐51.
9. Iten M, Matovu E, Brun R, Kaminsky R. Innate lack of susceptibility of Ugandan Trypanosoma brucei rhodesiense to DL‐alpha‐difluoromethylornithine (DFMO). Trop Med Parasitol. 1995 Sep;46(3):190‐4.
10.Friedheim EAH. Mel B in the treatment of human trypanosomiasis. American Journal of Tropical Medicine and Hygiene. 1949;29:173‐80.
11. Burri C, Baltz T, Giroud C, Doua F, Welker HA, Brun R. Pharmacokinetic properties of the trypanocidal drug melarsoprol. Chemotherapy. 1993;39(4):225‐34.
12.Burri C, Keiser J. Pharmacokinetic investigations in patients from northern Angola refractory to melarsoprol treatment. Trop Med Int Health. 2001 May;6(5):412‐20.
13.Burri C, Nkunku S, Merolle A, Smith T, Blum J, Brun R. Efficacy of new, concise schedule for melarsoprol in treatment of sleeping sickness caused by Trypanosoma brucei gambiense: a randomised trial. Lancet. 2000 Apr 22;355(9213):1419‐25.
14.Blum J, Burri C. Treatment of late stage sleeping sickness caused by T.b. gambiense: a new approach to the use of an old drug. Swiss Med Wkly. 2002 Feb 9;132(5‐6):51‐6.
15.Schmid C, Nkunku S, Merolle A, Vounatsou P, Burri C. Efficacy of 10‐day melarsoprol schedule 2 years after treatment for late‐stage gambiense sleeping sickness. Lancet. 2004 Aug 28;364(9436):789‐90.
16.Schmid C, Richer M, Bilenge CM, Josenando T, Chappuis F, Manthelot CR, et al. Effectiveness of a 10‐Day Melarsoprol Schedule for the Treatment of Late‐Stage Human African Trypanosomiasis: Confirmation from a Multinational Study (Impamel II). J Infect Dis. 2005 Jun 1;191(11):1922‐31.
17.Becker S, Franco JR, Simarro PP, Stich A, Abel PM, Steverding D. Real‐time PCR for detection of Trypanosoma brucei in human blood samples. Diagn Microbiol Infect Dis. 2004 Nov;50(3):193‐9.

Chapter 3
80
18.Maina NW, Oberle M, Otieno C, Kunz C, Maeser P, Ndung'u JM, et al. Isolation and propagation of Trypanosoma brucei gambiense from sleeping sickness patients in south Sudan. Trans R Soc Trop Med Hyg. 2007 Jun;101(6):540‐6.
19.Njiru ZK, Mikosza AS, Armstrong T, Enyaru JC, Ndung'u JM, Thompson AR. Loop‐Mediated Isothermal Amplification (LAMP) Method for Rapid Detection of Trypanosoma brucei rhodesiense. PLoS Negl Trop Dis. 2008;2(1):e147.
20.Njiru ZK, Mikosza AS, Matovu E, Enyaru JC, Ouma JO, Kibona SN, et al. African trypanosomiasis: sensitive and rapid detection of the sub‐genus Trypanozoon by loop‐mediated isothermal amplification (LAMP) of parasite DNA. Int J Parasitol. 2008 Apr;38(5):589‐99.
21.Van Nieuwenhove S, Schechter PJ, Declercq J, Bone G, Burke J, Sjoerdsma A. Treatment of gambiense sleeping sickness in the Sudan with oral DFMO (DL‐alpha‐difluoromethylornithine), an inhibitor of ornithine decarboxylase; first field trial. Trans R Soc Trop Med Hyg. 1985;79(5):692‐8.
22.Pohlig G, Bernhard S, Blum J, Burri C, Mpanya Kabeya A, Fina Lubaki J‐P, et al. Phase 3 trial of pafuramidine maleate (DB289), a novel, oral drug, for treatment of first stage sleeping sickness: Safety and Efficacy. 57th Meeting of the American Society of Tropical Medicine & Hygiene; 2008; New Orleans; 2008. p. Accepted.
23.Pepin J, Milord F. African trypanosomiasis and drug‐induced encephalopathy: risk factors and pathogenesis. Trans R Soc Trop Med Hyg. 1991 Mar‐Apr;85(2):222‐4.
24.WHO. Epidemiology and control of African trypanosomiasis. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1986;739:1‐127.
25.Magnus E, Vervoort T, Van Meirvenne N. A card‐agglutination test with stained trypanosomes (C.A.T.T.) for the serological diagnosis of T.b. gambiense trypanosomiasis. Ann Soc Belg Med Trop. 1978;58(3):169‐76.
26.Chappuis F, Loutan L, Simarro P, Lejon V, Buscher P. Options for field diagnosis of human african trypanosomiasis. Clin Microbiol Rev. 2005 Jan;18(1):133‐46.

Clinical presentation
81
Chapter 4
Clinical presentation of T.b. rhodesiense sleeping sickness in
second stage patients from Tanzania and Uganda
Irene Kuepfer1, Mpairwe Allan2, Andrew Edielu2, Emma Peter Hhary3, Enock Matovu4, Christian
Burri1, Johannes Blum1
1Swiss Tropical Institute, Basel, Switzerland, 2Lwala Hospital, Lwala, Uganda, 3Kaliua Health
Centre, Kaliua, Tanzania, 4Makerere University, Kampala, Uganda
This manuscript will be submitted to the American Journal of Tropical Medicine and Hygiene
Patient treated at Lwala Hospital, Uganda

Chapter 4
82
Abstract
In the framework of a clinical trial program we collected the first prospective and structured data
on the clinical presentation of the T.b. rhodesiense sleeping sickness in 138 second stage patients
from Tanzania and Uganda. Significant differences in diagnostic parameters and clinical signs and
symptoms were observed: the mean white blood cell (WBC) counts in Tanzania (135 cells/mm3)
was significantly higher than in Uganda (37 cells/mm3; p<0.0001). Unspecific signs of infection
(lymphadenopathy, hepatomegaly, splenomegaly) and pruritus were more common in Ugandan
patients whereas neuro‐psychiatric signs and symptoms such as sleeping disorders, tremor and
aggressiveness were more common in Tanzanian patients. Bias due to observation, co‐infections
or differences in the patient cohorts appeared to be unlikely and differences in health seeking
behaviour leading to a late onset of treatment could be ruled out. The two trypanosome
populations could not be genetically distinguished with the currently available primers.
Introduction
Human African Trypanosomiasis (HAT), better known as sleeping sickness, is caused by the
protozoan parasites T.b. gambiense (West and Central Africa) and T.b. rhodesiense (East and
South Africa). The disease is solely transmitted by tsetse flies (Glossina ssp.). 60 Mio. people in
the rural areas of most of sub Saharan Africa live at risk of infection, but less than 10% are under
adequate surveillance (1), reflecting its neglected status. Sleeping sickness caused by either
subspecies presents in two disease stages defined as the first, or haemo‐lymphatic stage and the
second, meningo‐encephalitic stage. Diagnosis of HAT is made in blood and the staging of the
disease by analysis of the cerebrospinal fluid (CSF). The second stage is defined by the presence of
trypanosomes and/or an elevated white blood cell (WBC) count (≥5WBC/mm3). The stage of the
disease as well as the type of infection direct the choice of treatment. However, T.b. gambiense
and T.b. rhodesiense can only be genetically distinguished by PCR analysis. The detection of the
human serum resistance‐associated (SRA) gene unequivocally identifies T.b. rhodesiense
trypanosomes (2, 3). In the field, the type of infection is entirely determined by the geographical
location of the patient. In Uganda, the only country where both forms of the disease are present, a
potential geographical overlap of the two endemic areas has become likely (4) and would hamper
proper diagnosis and treatment of HAT.
While often considered together, Gambiense and Rhodesiense HAT are different diseases,
clinically and epidemiologically (5). While T.b. gambiense HAT is a chronic disease, T.b.
rhodesiense has an acute disease progression. If left untreated, both forms of HAT are fatal. The

Clinical presentation
83
mean time to reach the second stage has been estimated at over one year for T.b. gambiense (6)
but only 3 weeks for T.b. rhodesiense HAT (7). Correspondingly, average times from infection to
death are almost 3 years and 6 to 12 months, respectively (6, 7). There are no specific clinical signs
and symptoms in the first stage; fever, headache and loss of appetite are common. In T.b.
rhodesiense the presence of a chancre at the site of the infective bite may be indicative for a
trypanosome infection. In the second stage of the disease characteristic neuro‐psychiatric signs
and symptoms occur: severe endocrinological and mental disturbances and severe motor
problems are the main signs (8).
A diversity of forms of clinical progression from asymptomatic to acute have been reported for
T.b. gambiense infections (9‐11). This seems to be even more pronounced for T.b. rhodesiense,
where a wide spectrum of disease severity ranging from a chronic disease pattern in southern
countries of East Africa with existing reports of asymptomatic carriers (12) to an increase in
virulence towards the north had been described (13). Even though those differences were already
described more than 60 years ago (14) the first comparative study was only carried out in 2004: on
the basis of the SRA gene polymorphism, trypanosomes isolates from Uganda (acute profile) and
Malawi (chronic profile) confirmed to be of different genotypes. However, the clinical description
of patients in this study was limited to the presence of chancre and the self‐reported duration of
illness (15). Another hypothesis postulates that the differences in disease severity could be
attributed to differences in genetic resistance to trypanosomiasis among host populations (14).
From the estimated 50’000 to 70’00 cases per year (16) , over 97% are T.b. gambiense cases and
only a few thousand are due to T.b. rhodesiense (17). Therefore, most literature concentrates on
T.b. gambiense HAT and its clinical picture and related cardiac and endocrinological disorders
have been extensively described (18‐25). On the other hand, the literature on the clinical aspects
of T.b. rhodesiense HAT is scarce. We could identify four studies describing its clinical
presentation (see table 1) and only one was based on a standardized questionnaire (26).

Chapter 4
84
In this paper we describe the first prospective and structured study of the clinical presentation of
T.b. rhodesiense HAT and will compare our findings to the existing literature.
Factors that could explain the different clinical presentation in the two countries include an
observation bias, concomitant infections, differences in the patient cohorts or the admission of
the patients at different time points of infection and will be discussed. We will also consider
differences in host and parasite genetics.
Materials and Methods
Study design and data collection. The IMPAMEL III program (2006‐2009) was conducted in
order to assess the safety and efficacy of the abridged, 10‐day melarsoprol schedule for the
treatment of second stage HAT (27, 28) in T.b. rhodesiense patients. Two trials, first a proof‐of‐
concept trial in 60 patients and a utilization study in an additional 78 patients were sequentially
conducted in the T.b. rhodesiense endemic regions of Tanzania and Uganda. The studies have
been approved by the ethics committees in Tanzania (National Institute for Medical
Table 1: Published literature on the clinical aspects of T.b. rhodesiense HAT.
Buyst (1977) Boatin (1986) Wellde (1989) Mbulamberi (1987) Number of patients 385 60 96 3152 Country Zambia Zambia Zambia Uganda Disease stage of patients 2nd stage 2nd stage 2nd stage 1st stagea Male/female ratio NA 1.73 1.53 1.1 Clinical signs and symptoms (%)
Chancre NA 5 15.6 19 Headache 66.2 73.3 95.8 95.8 Fever 31.2 71.7 36.4 96.8 Lymphadenopathy 80.5 NA 86.4 17.6 Itching or pruritus N.A. 35 53.1 NA Oedema of face 30.1b 21.7 3.1 27.5 Swelling of legs NA 43.3 25.3 NA Joint pains NA 65 88.5 95 Daytime sleep NA 63.3 70.8 26.8c Nighttime sleep NA 28.3 NA NA Abnormal coordination NA NA 51 NA Abnormal speech NA NA 38.5 NA Mental confusion 17.4 NA NA NA
NA: not applicable; a 98.7% of the patients were in the first stage and 1.3% of the patients in the second stage of the disease; b reported as oedema, c reported as somnolence

Clinical presentation
85
Research/NIMR) and Uganda (Ministry of Health) and the ethics committee of both cantons of
Basel (EKBB), Switzerland. Before first patient enrolment the study was registered in the database
of the current controlled trials (ISRCTN40537886).
Eligible for enrolment were second stage patients with a minimum age of 6 years and confirmed
second stage HAT. Moribund or unconscious patients as well as pregnant women and patients
with first stage infection were excluded.
Diagnosis of HAT was made in blood and in the cerebrospinal fluid (CSF). Blood was examined
using microscopy and/or the haematocrit centrifugation technique (29). If trypanosomes were
present, a lumbar puncture was performed for disease staging. Analysis of the CSF was done by
direct microscopy and/or single modified centrifugation technique and white blood cell (WBC)
count using counting chambers. Second stage infections were confirmed by the presence of
trypanosomes and/or ≥ 5 WBC/mm3 in the CSF.
For all 138 patients enrolled, the local principle investigator recorded data in an individual set of
case report forms (CRF): information on demographics, diagnosis, duration of signs and
symptoms prior to the diagnosis and clinical signs and symptoms at admission were collected.
The assessment of clinical signs and symptoms used a graded scale for severity (grade 1, 2).
Data management and statistical analysis. All data were double entered and verified using Epi
Data 3.1 software (www.epidata.dk) and analysis was accomplished with the statistical software
package STATA Version IC10.0 (STATATM, StataCorp, USA). The statistical analysis was performed
comparing proportions with the Pearson chi square, means with the Student’s t test and
distributions with the Kruskal‐Wallis test.
Results
A total of 138 late stage T.b. rhodesiense patients were enrolled. Demographic and diagnostic
baseline characteristics of the study population are shown in table 2. The proportion of male
(57.2%) and female (42.8%) patients was similar. 18.8% (26) trial participants were younger than
16 years whereof 88.5% (23) were enrolled in Uganda. Significantly more patients from Uganda
had a body mass index (BMI) below 16.5 (p<0.0001). Trypanosomes were more often identified in
the blood of Tanzanian patients, although the difference did not reach statistical significance
(99% vs. 91%, p=0.0524) whereas the frequency of trypanosomes in CSF did not differ (80% vs.
86%, p=0.3690). Country specific differences were observed for the WBC counts in the CSF: the
mean WBC count in Tanzania was 135 (±85) and 37 (±40) in Uganda (p<0.0001).

Chapter 4
86
Table 2: Demographic and diagnostic baseline characteristics of the study population.
Total (n=138) Tanzania (n=69) Uganda (n=69) n % n % n % Age, mean ± SD 35±19 38±15 32±22 Age, range 6‐85 9‐70 6‐85 Male female ratio 1.34 1.38 1.3 Age below 16 years 26 3 23 Nutritional status BMI1 (kg/m2) ‐ mean ± SD 18.5±3.4 19.6±2.5 17.3±3.8 BMI<16.5 38 28 5 7 33 48 Malaria positive on admission 57 41 55 80 2 3 Diagnostic findings Trypanosomes in blood 131 95 68 99 63 91 Trypanosomes in CSF2 114 83 55 80 59 86 WBC3 count in CSF 0 ‐ 20 cells/ul ‐ no. (%) 35 25 0 35 51 21 ‐ 100 cells/ul ‐ no. (%) 52 38 23 33 29 42 > 100 cells/ul ‐ no. (%) 51 37 46 67 5 7 Median 70 134 20 Mean ± SD 86±82 135±85 37±40 Note: 1Body Mass Index, 2 CSF: cerebrospinal fluid, 3 WBC: white blood cell

Clinical presentation
87
The clinical signs and symptoms reported at baseline are summarized in table 3. The level of
significance (95%) between patients in Tanzania and Uganda is also shown.
Table 3: Clinical signs and symptoms of study population at baseline.
Total (n=138) Tanzania (n=69) Uganda (n=69) Statistical n % n % n % test Self reported duration of illness up to 1month 40 29 15 22 25 36 2‐3 months 52 38 32 46 20 29 more than 3 months 46 33 22 32 24 35 Mean reporting time to health facility in months (range)
3 (0‐12) 3.2
(1‐12) 2.8 (0‐7) p=0.2683
Clinical manifestations Lymphadenopathy 27 19.6 7 10.1 20 29.0 p=0.0053 General Body Pain 132 95.7 69 100.0 63 91.3 p=0.0123 Headache 128 92.8 65 94.2 63 91.3 p=0.5114 Fever (>37.5°C) 41 29.7 20 29.0 21 30.4 p=0.8522 Fever (>38.5°C) 9 6.5 3 4.3 6 8.7 p=0.3010 Joint pains 129 93.5 67 97.1 62 89.9 p=0.0847 Diarrhea 9 6.5 1 1.4 8 11.6 p=0.0158 Pruritus 21 15.2 4 5.8 17 24.6 p=0.0003 Oedema 40 29.0 26 37.7 14 20.3 p=0.0244 Dyspnoe 10 7.2 1 1.4 9 13.0 p=0.0086 Cough 27 19.6 8 11.6 19 27.5 p=0.0183 Tremor 54 39.1 43 62.3 11 15.9 p<0.0001 Hepatomegaly 25 18.1 4 5.8 21 30.4 p=0.0002 Splenomegaly 51 37.0 11 15.9 40 58.0 p<0.0001 Walking difficulties 75 54.3 35 50.7 40 58.0 p=0.3928 Abnormal movements 36 26.1 31 44.9 5 7.2 p<0.0001 Sleeping disorder daytime 105 76.1 66 95.7 39 56.5 p<0.0001 Sleeping disorder nighttime 88 63.8 64 92.8 24 34.8 p<0.0001 Strange behaviour 25 18.1 15 21.7 10 14.5 p=0.2691 Disturbed appetite 120 87.0 60 87.0 60 87.0 p=1 Inactivity 100 72.5 57 82.6 43 62.3 p=0.0076 Speech impairment 16 11.6 6 8.7 10 14.5 p=0.2875 Aggressiveness 45 32.6 43 62.3 2 2.9 p<0.0001 Note: 1Body Mass Index, 2 CSF: cerebrospinal fluid, 3 WBC: white blood cell

Chapter 4
88
Unspecific signs of infection (lymphadenopathy, hepatomegaly, splenomegaly) and pruritus were
more frequent in Uganda than in Tanzania. Also diarrhea, dyspnoe and cough were more
frequent in Uganda than in Tanzania. General body pain and oedema were more common in
Tanzania than in Uganda as well as most of the characteristic signs and symptoms related to CNS
involvement: tremor, abnormal movement, sleeping disorders at day and night time, inactivity
and aggressiveness. No difference was observed for strange behaviour, walking difficulties,
disturbed appetite and speech impairment.
Clinical suspicion for cardiac insufficiency was found in both centres: indication for left heart
insufficiency (combination of cough and dyspnoe) and right heart insufficiency (combination of
odemea and hepatomegaly) was seen for each in 3.6% of the patients.
To draw conclusions on changes in clinical presentation and diagnostic findings over time, the
study population was categorized in 3 groups according the self‐reported time of illness. 29%
reported to the health centre within one month of illness, 38% reported after 2‐3 months and 33%
after more that 3 months of illness (see table 3). We analyzed the differences in distributions of
clinical signs and symptoms and diagnostic findings among those groups. Significant differences
were found for tremor (p=0.0026), abnormal movements (p=0.0378), walking difficulties
(p=0.0331) and aggressiveness (p=0.0033). No difference was found for cough (p=0.8716), dyspnoe
(p=0.7403), oedema (p=0.0854), hepatomegaly (p=0.2321), splenomegaly (p=0.8439), daytime
sleep (p=0.0626) and night time sleep (p=0.2244) and unusual behaviour (p=0.7824). There was
no significant change over time for the presence of trypanosomes in blood (p=0.7259) and CSF
(p=0.8020). As shown in figure 1 also the WBC count did not change in relation to the reporting
time (p=0.4549).

Clinical presentation
89
Figure 1: Mean and 95% confidence interval for white blood cell (WBC) count in the central nervous system
(CNS) by country and reporting time.
Discussion
In this paper, clinical symptoms and signs of patients with second stage HAT due to T.b.
rhodesiense are described for a cohort of 138 patients treated in a prospective study in Tanzania
and Uganda. The only specific neurological signs in the Ugandan patients were sleeping disorders
and walking difficulties whereas in Tanzanian patients the neuro‐psychiatric signs such as
sleeping disorders, aggressiveness, inactivity as well as abnormal movements and tremor
dominated the clinical picture (see table 3). Headache and general body pain/joint pains were
common in all patients whereas unspecific signs of infections such lymphadenopathy,
hepatomegaly and splenomegaly was more frequently found in Ugandan patients.
Fever is a leading symptom in Ugandan first stage patients (97%) and in non‐African patients
with first and second stage HAT (close to 100%) (30). Fever was reported in a lower extend of
second stage patients from Zambia (31‐71%) and was only occasionally found in T.b. gambiense
patients (16%) (22). We report fever in 30% of the patients. High fever (>38.5) was seen in 6.5% of
the patients whereof three cases were children (33.3%). This is different to the findings of T.b.
gambiense HAT where high fever was most frequently reported in children (2‐14 years) (22). Fever
0
20
40
60
80
100
120
140
160
180
200
White blood cell (WBC) count by reporting time and country
Reporting time (months)
WB
C/m
m3
≤ 1 1−3 > 3 ≤ 1 1−3 > 3
Tanzania Uganda

Chapter 4
90
seems to be a rather typical sign in the early stages of T.b. rhodesiense HAT but decreases over
time.
Whereas the heart involvement is typical but rarely of clinical relevance in T.b. gambiense
patients (31) we have limited knowledge in the role of cardiac involvement in T.b. rhodesiense
patients. However, there is evidence that perimyocarditis seems to play an important part in the
clinical course and fatal outcomes in T.b. rhodesiense HAT patients (32, 33). Based on our findings
the symptoms oedema (swelling of legs) (29%), hepatomegaly (18%), dyspnoea (7%) and cough
(20%) could be caused by a cardiac failure. Given the limitations for examination under field
conditions this is only an assumption. More specific examinations such as auscultation of the
lungs and interpretations of the congestion of the neck veins or a positive hepatojugular reflux
would be needed. However, this could not be done under field conditions as the examination
beds do not allow the assessment of the jugular veins at 45° and the medical workers were not
trained for diagnosis of heart failure.
The percentage of neuro‐psychiatric signs and symptoms is surprisingly high in the Tanzanian
group and comparable to the clinical presentation of T.b. gambiense HAT. The clinical
presentation of the Ugandan patients corresponds more to the clinical pattern of a first stage
HAT. The literature described the CNS involvement on the basis of daytime sleep, night time
sleep, abnormal coordination, abnormal speech and mental confusion (see table 1). The study on
first stage patients in Uganda reported somnolence in 26.8% of the patients compared to 63.3% ‐
70.8% of the second stage patients from Zambia. In our study, daytime sleep in Tanzania was
reported in 96% and in Uganda in 57% of the patients which corroborates the notion that daytime
sleep is characteristic for second stage disease. Sleeping disorders at night were more frequent in
Tanzania (92.8%) than in Uganda (34.8%). One study from the literature reported night time
sleep in 28.3% of the patients which compares well with our findings in Uganda. Conclusively,
sleep disorders correlate with the degree of CNS involvement. The literature reported abnormal
speech in 38.5% of the patients whereas we report speech impairment only in 11.6% of the
patients. No striking differences to the literature were seen for abnormal coordination (51%) that
we compared to walking difficulties (54.3%) and mental confusion (17.4%) that we compared to
strange behaviour (18.1%). None of the studies from the literature indicated tremor; either tremor
was not present in those patients or it was outbalanced by other signs and symptoms.
Most of the literature described second stage HAT in patients from Zambia. The study from
Mbulamberi et al. (34) describes the disease in first stage patients and so far, no information was
available on the clinical presentation of second stage HAT in Tanzanian patients.

Clinical presentation
91
Our data confirm a wide spectrum of disease severity: a high variability of the symptoms and
signs were observed between the two study populations as well as to the presented literature (see
table 1).
Underlying causes could include an observation bias, concomitant infections, different cohorts of
patients, and the admission of patients at different time points after infection. Differences in host
or parasite genetics also need to be considered.
An observations bias cannot be ruled out. However, the same structured CRF and monitoring
person and the variability as well for signs with a clear definition observed by the health
personnel (e.g. lymphadenopathy, abnormal movements or tremor) as for subjective symptoms
declared by the patient (e.g. insomnia, headache or inactivity) makes an observations bias less
likely.
Malaria was a concomitant disease (80%) and could explain at least partially the presence of fever
in the Tanzanian group. There were no observations of filariasis or scabies that could explain the
differences in the frequency of pruritus in the two countries. No further concomitant diseases
were reported. Based on the clinical assessment it was not possible to attribute the significant
lower body mass index of Ugandan patients to cachexia or malnutrition. However, food security is
very poor in this part of Uganda and most likely the reason for the poor nutritional status of the
population. This could explain a weakness leading to inactivity and walking difficulties in the
absence of neurological symptoms.
We consider differences in the patient collectives as rather unlikely. The male/female ratio from
the literature (see table 1) was comparable to the ratio of 1.4 in the study population. Also, the
children (18.8%) in the study population did not show differences for the incidence of fever nor
for the incidence of neuro‐psychiatric signs and symptoms.
The hypothesis of admission of the patients at different times of disease evolution could be
possible and is supported by the fact that neurological symptoms correlate with the progression
of the disease. However, the duration of self‐reported symptoms was comparable in both groups.
Further, sleeping disorders and presence of trypanosomes in blood and CSF and/or WBC counts
did not correlated with the duration of symptoms.
Host genetics and eventually previous infections may be likely determinants for the severity of
response to infection. There are speculations that apathogenic forms of the disease could
influence the immune response to pathogenic infections (34, 35). Further, the clinical
presentation is more acute in the white than in the black population (30, 36). Also high variability
is seen among African populations (13) and might be related to their decent: people of Bantu

Chapter 4
92
descent, whose ancestors have been exposed to human trypanosomes for several thousand years,
may have greater tolerance than people of Nilotic descent, who migrated into the East African
region from tsetse‐free areas during the past 2,000 years (14). However, this can not be confirmed
by our data since in Tanzania the majority of the population is of Bantu origin and in Uganda the
majority of the population is of nilotic origin. In summary, our data show a clear difference in the
clinical presentation of the disease in Tanzania and Uganda but do not allow conclusive remarks
on the influence of host factors.
Different parasite genotypes could be responsible for the observed spectrum of disease severity.
This hypothesis has already been raised 60 years ago based on observation of epidemiological and
clinical patterns (12, 13, 37). Different parasite genotypes were confirmed for trypanosomes
isolates from Uganda and Malawi on the basis of the SRA gene polymorphism (15). The two
spatially distinct Tororo and Soroti foci of T.b. rhodesiense in Uganda were shown to be
genetically distinct T.b. rhodesiense parasites (38).
In an ancillary study to the molecular characterization of trypanosome DNA from all IMPAMEL III
participants (see chapter 3) we analyzed the two trypanosomes populations by microsattellite
analysis. For a first analysis we used the primers by MacLean et.al. (38) but the populations did
not appear to be different. In a second analysis we used primers recently designed at the
University of Glasgow (not yet published) but again the two populations did not appear to be
significantly different. However, we don’t consider these results as fully conclusive. Future
attempts should be made designing different sets of primers in order to rule out potential
limitations of the method. The assumption that the parasite belong to the same population
contradicts recent findings on the phylogenetic relationship between different T.b. rhodesiense
strains that showed that the high variability of the T.b. rhodesiense genome is attributed to
multiple and independent evolutions from T.b. brucei (39).
The Ugandan picture of second stage T.b. rhodesiense HAT resembles more a first or an early
second stage infection whereas in Tanzania it presents as an advanced second stage disease with
predominance of neuro‐psychiatric symptoms.
Biases caused by observation, co‐infections and different patient cohorts appeared to be unlikely.
Differences due to initiation of treatment at different time points of infections could be ruled out
as the duration of self‐reported symptoms was comparable in both groups.
Host factors such as genetic makeup or previous infections with apathogenic trypanosomes could
contribute to the observed differences in the clinical presentation in patients from Tanzania and
Uganda. However, the analyses of those factors were beyond the scope of our study.

Clinical presentation
93
Despite the evidence of different parasite genotypes in Uganda and Malawi we were not able to
genetically distinguish the trypanosomes from Tanzania and Uganda with the currently available
methods. However, limitations of the method can not be excluded and other sets of primers
might allow differentiation.

Chapter 4
94
References
1. WHO. Control and surveillance of African trypanosomiasis. Geneva: WHO; 1998.
2. De Greef C, Hamers R. The serum resistance‐associated (SRA) gene of Trypanosoma brucei rhodesiense encodes a variant surface glycoprotein‐like protein. Mol Biochem Parasitol. 1994 Dec;68(2):277‐84.
3. Gibson WC. The SRA gene: the key to understanding the nature of Trypanosoma brucei rhodesiense. Parasitology. 2005 Aug;131(Pt 2):143‐50.
4. Picozzi K, Fevre EM, Odiit M, Carrington M, Eisler MC, Maudlin I, et al. Sleeping sickness in Uganda: a thin line between two fatal diseases. Bmj. 2005 Nov 26;331(7527):1238‐41.
5. Fevre EM, Picozzi K, Jannin J, Welburn SC, Maudlin I. Human African trypanosomiasis: Epidemiology and control. Adv Parasitol. 2006;61:167‐221.
6. Checchi F, Filipe JA, Haydon DT, Chandramohan D, Chappuis F. Estimates of the duration of the early and late stage of gambiense sleeping sickness. BMC Infect Dis. 2008;8:16.
7. Odiit M, Kansiime F, Enyaru JC. Duration of symptoms and case fatality of sleeping sickness caused by Trypanosoma brucei rhodesiense in Tororo, Uganda. East Afr Med J. 1997 Dec;74(12):792‐5.
8. Burri C, Stich A, Brun R. The trypanosomiases: CABI Publishing; 2004.
9. Truc P, Formenty P, Diallo PB, Komoin‐Oka C, Lauginie F. Confirmation of two distinct classes of zymodemes of Trypanosoma brucei infecting man and wild mammals in Cote d'Ivoire: suspected difference in pathogenicity. Ann Trop Med Parasitol. 1997 Dec;91(8):951‐6.
10. Garcia A, Jamonneau V, Magnus E, Laveissiere C, Lejon V, N'Guessan P, et al. Follow‐up of Card Agglutination Trypanosomiasis Test (CATT) positive but apparently aparasitaemic individuals in Cote d'Ivoire: evidence for a complex and heterogeneous population. Trop Med Int Health. 2000 Nov;5(11):786‐93.
11. Sternberg JM. Human African trypanosomiasis: clinical presentation and immune response. Parasite Immunol. 2004 Nov‐Dec;26(11‐12):469‐76.
12. Songa EB, Hamers R, Rickman R, Nantulya VM, Mulla AF, Magnus E. Evidence for widespread asymptomatic Trypanosoma rhodesiense human infection in the Luangwa Valley (Zambia). Trop Med Parasitol. 1991 Dec;42(4):389‐93.
13. Ormerod WE. Taxonomy of the sleeping sickness trypanosomes. J Parasitol. 1967 Aug;53(4):824‐30.
14. Buyst H. The epidemiology of sleeping sickness in the historical Luangwa valley. Ann Soc Belg Med Trop. 1977;57(4‐5):349‐59.
15. MacLean L, Chisi JE, Odiit M, Gibson WC, Ferris V, Picozzi K, et al. Severity of human african trypanosomiasis in East Africa is associated with geographic location, parasite genotype, and host inflammatory cytokine response profile. Infect Immun. 2004 Dec;72(12):7040‐4.
16. WHO. Human African trypanosomiasis (sleeping sickness): epidemiological update. Weekly epidemiological record. 2006 24. Februar(TRS881):69‐80.
17. Simarro PP, Jannin J, Cattand P. Eliminating human African trypanosomiasis: where do we stand and what comes next? PLoS Med. 2008 Feb;5(2):e55.
18. Haller L, Adams H, Merouze F, Dago A. Clinical and pathological aspects of human African trypanosomiasis (T. b. gambiense) with particular reference to reactive arsenical encephalopathy. Am J Trop Med Hyg. 1986 Jan;35(1):94‐9.
19. Nkanga NG, Kazadi K, Kazyumba GL, Dechef G. [Clinical neurological signs of human African trypanosomiasis at the meningoencephalitis stage (apropos of 23 cases)]. Bull Soc Pathol Exot Filiales. 1988;81(3 Pt 2):449‐58.

Clinical presentation
95
20. Noireau F, Apembet JD, Frezil JL. [Clinical review of endocrine disorders observed in adults with trypanosomiasis]. Bull Soc Pathol Exot Filiales. 1988;81(3 Pt 2):464‐7.
21. Reincke M, Allolio B, Petzke F, Heppner C, Mbulamberi D, Vollmer D, et al. Thyroid dysfunction in African trypanosomiasis: A possible role for inflammatory cytokines. Clinical Endocrinology. 1993;39(4):455‐61.
22. Blum J, Schmid C, Burri C. Clinical aspects of 2541 patients with second stage human African trypanosomiasis. Acta Trop. 2006 Jan;97(1):55‐64.
23. Blum JA, Burri C, Hatz C, Kazumba L, Mangoni P, Zellweger MJ. Sleeping hearts: the role of the heart in sleeping sickness (human African trypanosomiasis). Trop Med Int Health. 2007 Dec;12(12):1422‐32.
24. Blum JA, Schmid C, Hatz C, Kazumba L, Mangoni P, Rutishauser J, et al. Sleeping glands? ‐ The role of endocrine disorders in sleeping sickness (T.b. gambiense Human African Trypanosomiasis). Acta Trop. 2007 Oct;104(1):16‐24.
25. Jamonneau V, Garcia A, Frezil JL, N'Guessan P, N'Dri L, Sanon R, et al. Clinical and biological evolution of human trypanosomiasis in Côte d'Ivoire. Annals of Tropical Medicine and Parasitology. 2000;94(8):831‐5.
26. Wellde BT, Chumo DA, Reardon MJ, Mwangi J, Asenti A, Mbwabi D, et al. Presenting features of Rhodesian sleeping sickness patients in the Lambwe Valley, Kenya. Ann Trop Med Parasitol. 1989 Aug;83 Suppl 1:73‐89.
27. Burri C, Nkunku S, Merolle A, Smith T, Blum J, Brun R. Efficacy of new, concise schedule for melarsoprol in treatment of sleeping sickness caused by Trypanosoma brucei gambiense: a randomised trial. Lancet. 2000;355(9213):1419‐25.
28. Schmid C, Richer M, Bilenge CM, Josenando T, Chappuis F, Manthelot CR, et al. Effectiveness of a 10‐day melarsoprol schedule for the treatment of late‐stage human African trypanosomiasis: Confirmation from a multinational study (Impamel II). Journal of Infectious Diseases. 2005 Jun 1;191(11):1922‐31.
29. Woo PT. The haematocrit centrifuge for the detection of trypanosomes in blood. Can J Zool. 1969 Sep;47(5):921‐3.
30. Duggan AJ, Hutchinson MP. Sleeping sickness in Europeans: a review of 109 cases. J Trop Med Hyg. 1966 Jun;69(6):124‐31.
31. Blum JA, Zellweger MJ, Burri C, Hatz C. Cardiac involvement in African and American trypanosomiasis. Lancet Infect Dis. 2008 Oct;8(10):631‐41.
32. de Raadt P, Koten JW. Myocarditis in Rhodesiense trypanosomiasis. East Afr Med J. 1968 Mar;45(3):128‐32.
33. Koten JW, De Raadt P. Myocarditis in Trypanosoma rhodesiense infections. Trans R Soc Trop Med Hyg. 1969;63(4):485‐9.
34. Mbulamberi DB. A clinical analysis of 3151 cases of Rhodesian sleeping sickness treated in the South Eastern Uganda, during the year 1985. Proceedings of the International Scientific Council for Trypanosomiasis Research and Control 19th Meeting, Lomé, Togo. 1987:188‐95.
35. Jamonneau V, Ravel S, Garcia A, Koffi M, Truc P, Laveissiere C, et al. Characterization of Trypanosoma brucei s.l. infecting asymptomatic sleeping‐sickness patients in Cote d'Ivoire: a new genetic group? Ann Trop Med Parasitol. 2004 Jun;98(4):329‐37.
36. Blum J, Beck BR, Brun R, Hatz C. Clinical and serologic responses to human 'apathogenic' trypanosomes. Trans R Soc Trop Med Hyg. 2005 Oct;99(10):795‐7.
37. Jelinek T, Bisoffi Z, Bonazzi L, van Thiel P, Bronner U, de Frey A, et al. Cluster of African trypanosomiasis in travelers to Tanzanian national parks. Emerg Infect Dis. 2002 Jun;8(6):634‐5.

Chapter 4
96
38. Apted FI, Smyly DP, Ormerod WE, Stronach BW. A comparative study of the epidemiology of endemic Rhodesian sleeping sickness in different parts of Africa. J Trop Med Hyg. 1963 Jan;66:1‐16.
39. MacLean L, Odiit M, Macleod A, Morrison L, Sweeney L, Cooper A, et al. Spatially and genetically distinct African Trypanosome virulence variants defined by host interferon‐gamma response. J Infect Dis. 2007 Dec 1;196(11):1620‐8.
40. MacLeod A, Welburn S, Maudlin I, Turner CM, Tait A. Evidence for multiple origins of human infectivity in Trypanosoma brucei revealed by minisatellite variant repeat mapping. J Mol Evol. 2001 Mar;52(3):290‐301.

Review
97
Chapter 5
Reflections on clinical research in sub‐Saharan Africa
Irene Kuepfer, Christian Burri
Swiss Tropical Institute, Pharmaceutical Medicine Unit, Socinstrasse 57, CH‐4002 Basel,
Switzerland
Published in the International Journal for Parasitology
Pharmacy at the Lwala Hospital, Uganda

Chapter 5
98
Abstract
The urgent need for new, safe and sustainable interventions against diseases that
disproportionally affect the poor is finally receiving global attention and the funding landscape
for development projects has significantly improved during the past decade. For the development
of new drug and vaccine candidates, clinical trials have become the most important tool to assess
their safety and efficacy. Recently, there has been a seismic shift in the number of clinical trials
conducted in resource‐limited settings. We discuss the current framework of clinical research in
sub‐Saharan Africa, from building product pipelines to the capacities needed for the conduct of
trials according the harmonized Good Clinical Practice (GCP) ICH E6 guideline. We place
emphasis on clinical research in neglected tropical diseases which still frequently has to be
conducted with limited financial, logistical and human resources. Given those short‐comings we
recommend minimum standards needed at the local, national and sponsor levels to provide GCP‐
compliant clinical research.
Keywords: Neglected tropical diseases; Sub‐Saharan Africa; Research and development; Clinical
research; Good clinical practice (GCP); Minimum standards

Review
99
Introduction
Clinical studies and trials are the most important tools to assess the evidence of new medical
interventions including drugs and vaccines. The correct and fair conduct of the investigations is
essential and this was one of the key messages of the first International Clinical Trials Day of 20th
May 2005 which was organized to boost clinical research worldwide (http://www.ecrin.org).
Almost 10 years ago, the term ‘10/90 gap’ was coined, recognizing that in the preceding 30 years
only 10% of global health research has been dedicated to diseases that accounted for 90% of the
global disease burden (1). Fortunately, since 2000 the funding landscape for tropical disease
research has significantly improved (2) and as a result, the number of clinical trials conducted in
sub‐Saharan Africa has multiplied. Today, a new challenge in certain fields is coordination of the
efforts of numerous global initiatives and consortia contributing to new, sustainable interventions
against diseases which disproportionately affect the poor.
During the same period, international rules for the conduct of trials have been advanced from
guidelines to laws in the Western world and largely implemented. The harmonized Good Clinical
Practice (GCP) ICH E6 guideline (3) set a quality standard, but has also added an unprecedented
dimension of complexity to clinical research. Whereas many sub‐Saharan drug authorities are still
not in the position to impose fully GCP‐compliant trials, most international funding agencies and
sponsors do so and clinical research in resource‐limited countries has to satisfy international laws
and regulations. This has the advantage of increasing quality standards and credibility of the data
produced, but may also lead to conflicts with cultural, political and socio‐economic facts and
values.
Trials on interventions against rare diseases or those which have a mainly rural distribution often
have to be carried out with limited finances, logistics and human resources. It stands to reason
that finding the equilibrium between those different realities remains a challenge. Those
conditions and settings also stand in sharp contrast to the growing number of high standard
research centers in sub‐Saharan Africa.
In this article we review the current framework and the practical aspects of clinical research in
sub‐Saharan Africa with an emphasis on clinical trials for the most neglected diseases. Given the
various challenges and restrictions of such research in collaboration, we attempt also to present
minimum standards for the appropriate conduct of clinical trials and studies.

Chapter 5
100
Creating and maintaining a pipeline of new interventions against neglected
tropical diseases
Neglected tropical diseases
Respiratory infections and diarrheal diseases are the two main categories of infectious diseases
responsible for a high burden of disease in resource‐poor settings
(http://www.who.int/mediacentre/factsheets/fs310_2008.pdf). In addition, the “Big Three” ‐
HIV/AIDS, malaria and tuberculosis account for 5.6 million deaths and the annual loss of 166
million disability‐adjusted life years (DALYs) (4). Premature mortality and high morbidity are also
caused by another category of illnesses referred to as neglected tropical diseases, e.g. Human
African Trypanosomiasis, Chagas disease, schistosomiasis, leishmaniasis, dengue fever and
leprosy. Together those diseases cause approximately 534,000 deaths annually and are responsible
for a very large number of years of life lost as a result of from premature disability (DALYs). Some
estimates suggest that the neglected tropical diseases result in 57 million DALYs lost annually, a
number that is almost as high as that of each of the ‘Big Three’ (4).
Neglected tropical diseases share three common characteristics. Firstly, they are only prevalent in
resource‐limited settings and hence the market incentives are far too low to trigger corporate
investments for new interventions. Second, the target product profile of new diagnostics and
chemotherapies for such diseases must allow their use under very difficult field conditions and be
stable under extreme conditions of heat and humidity (5). Third, the interventions need to be
cost‐effective to have a fair chance to be delivered to the target population by the typically weak
health systems or non‐governmental organizations (NGOs).
Undoubtedly, we are significantly lacking the tools to properly diagnose and treat many neglected
tropical diseases. The withdrawal of pharmaceutical companies from tropical disease research and
development (R&D) in the 1970s left a very large gap in the development of new and affordable
drugs (6). From 1975 to 1999, 1,393 new pharmaceuticals were marketed worldwide of which only
13 were against tropical diseases (7), mainly for malaria and tuberculosis.
The new landscape after the year 2000
The landscape for neglected disease R&D has dramatically changed since the beginning of the
new millennium (2) and the reasons are manifold. An in‐depth analysis performed in 2004
showed that 63 neglected disease drug projects were under way, including two new drugs in

Review
101
registration status and 18 new products in clinical trials, half of which were already in Phase III.
With sufficient funding these projects were expected to deliver eight to nine new neglected‐
disease drugs until 2009, even if no further projects would have commenced after this (2).
Searching for new medical interventions against neglected tropical diseases
Due to the recognized need for new, rapid and sustainable interventions, and due to lengthy and
expensive pharmaceutical development processes, short‐ and long‐term strategies are combined
in order to deliver new drugs and vaccines to this neglected market. One of the central pillars is
the extensive screening of existing compound libraries. Rapid success and a comparatively low
attrition rate can be expected from compounds which have already undergone pre‐clinical and/or
partial clinical development but were abandoned by industry due to economic reasons or
inefficacy for the original indication. Unfortunately, such compounds are hard to come by,
possibly due to potential embarrassment should the compound be successful and the fear of
important trade secrets being passed on unintentionally. Other shorter‐term strategies involve
the development of follow‐on drugs in the same class, fixed dose combinations of existing drugs,
and of new pediatric formulations to make childhood treatment easier. Exciting results can also
come from re‐directing compounds developed for other diseases towards neglected diseases, also
called “therapy‐switching” or “piggy‐backing” (8).
However, to create a sustainable pipeline of compounds, long‐term strategies are important.
There the focus is on “breakthrough” innovation; i.e. novel compounds with a novel mechanism
of action against the pathogens (2). This approach is of primary importance to cope with the
increasing problem of resistances in diseases where treatments exist (e.g. malaria and
tuberculosis) but also to find acceptable therapies for those diseases where acceptable solutions
are so far lacking (e.g. sleeping sickness, leishmaniasis). A recent example of drug resistance is the
report of artemisinin‐resistant malaria in western Cambodia (9).
On the positive side, a number of new screening centers tackling the above‐mentioned tasks
became operational during the past few years and the number of hits and lead compounds is
increasing. However, a major challenge and persisting bottleneck appears to be the professional
selection of the leads and particularly the advancement of the most promising compounds into
funded professional pre‐clinical programs.

Chapter 5
102
Alternative business models for R&D in tropical diseases
Private sector investments in R&D are not triggered by commercial incentives, thus a system that
not only shares the risk but also the cost of a highly expensive undertaking was established and
became known as Public Private Partnerships (PPPs), now called Product Development
Partnerships (PDPs). Examples of PPPs/PDPs such as the special program in research and training
of tropical diseases (TDR) date back to 1975. Today, the development of new partnerships has
accelerated and examples are numerous. The Initiative on Public Private Partnerships for Health
lists over 90 such organizations in its database (http://www.globalforumhealth.org).
These organizations mostly operate like virtual drug companies and are largely responsible for the
recent seismic shift in R&D for tropical diseases (6). At present the range of funding is mainly
provided by philanthropic organizations led by the Bill & Melinda Gates Foundation
(http://www.gatesfoundation.org). In 2005, philanthropic organizations contributed over 78% of
the total funding of R&D partnerships for neglected diseases, whereas public funding was
calculated at a mere 16%.
Public funding has a long history at the National Institutes of Health (NIH, USA) mainly in the
form of competitive research grants, whereas other institutions such as the Institut Pasteur
(France) or the Medical Research Council (MRC, United Kingdom) made targeted investments in
satellite centers. Broad public funding is a major factor for sustainable tropical disease R&D, as
only governments can guarantee a long‐term commitment (10). The report of the World Health
Organization’s (WHO’s) commission on public health, innovation and intellectual property rights
released in April 2006, urged the WHO to develop a global plan of action to secure enhanced and
sustainable funding for developing and making accessible products to address diseases that
disproportionately affect developing countries (11).
An example of targeted public funding is the European & Developing Countries Clinical Trials
Partnership (http://www.edctp.org) which was created in 2003. During the past year it has gained
substantial momentum, funding drug and vaccine development in HIV/AIDS, malaria and
tuberculosis.
Areas where governments can indirectly encourage corporate interest in rare and/or neglected
diseases are indemnification strategies. Since 1983 the U.S. Food and Drug Administration (FDA)
has offered tax incentives for clinical trials as well as 7 years of marketing exclusivity for drugs
developed for rare diseases in the US through the Orphan Drug Act
(http://www.fda.gov/orphan/oda.htm). In 2007, the U.S. Congress approved an amendment to
the FDA Revitalization Act (http://www.fda.gov/oc/initiatives/HR3580.pdf), which created a

Review
103
transferable voucher to encourage treatments for tropical diseases. The sponsor of a newly
approved drug which prevents or treats an eligible tropical or neglected disease will receive a
priority review voucher, which can then be transferred to the submission of another human drug
or sold to another company. Priority review reduces the time period for the review of the
registration dossier from an average of 18 months to no longer than 6 months. Economists
estimate that the priority review voucher used for a potential blockbuster drug could be worth
more than US$ 300 million. In comparison, the average costs of developing a new chemical entity
were estimated to be US$ 800 million in the year 2003 including capitalization. The voucher could
thus enable a company to recoup a significant portion of the cost of developing a new drug
(http://www.iavi.org/viewfile.cfm?fid=47963). This seemingly straight forward system awaits its
first application, with some critical voices cautioning against potential misuse or a decreased
quality of the review process (12).
In 2000 the European Union adopted the Orphan Medicinal Products legislation under which
companies with an orphan designation for a medicinal product benefit from incentives such as
protocol assistance (scientific advice during the product‐development phase); marketing
authorization (10‐year marketing exclusivity); financial incentives (fee reductions or exemptions);
and national incentives detailed in an inventory made available by the European Commission
(http://www.emea.europa.eu/pdfs/human/comp/29007207en.pdf). The European Union
pharmaceutical legislation may support authorities that lack regulatory capacity; those authorities
can obtain scientific opinion from the European Medicines Evaluation Agency (EMEA) through
WHO on products intended exclusively for markets outside the community (13).
Last but not least, the pharmaceutical industry has renewed its interest and engagement in
tropical diseases. Examples for new industry sponsored research facilities are the Novartis
Institute for Tropical Diseases (http://www.novartis.com/research/nitd), GlaxoSmithKline’s
Diseases of the Developing World Initiative (http://www.gsk.com
/research/about/about_diseases.html), Sanofi‐Aventis’ Malaria Initiative (http://en.sanofi‐
aventis.com/sustainability/sustainability.asp) and Astra‐Zeneca’s (http://new.tballiance.org
/newscenter/view‐brief.php?id=52) effort in tuberculosis research. These institutions will have a
major impact in coming years (6).
Persistent and emerging complexities ‐ intellectual property rights
A key aspect of cooperative R&D is the role of intellectual property protection mechanisms
(IPPM). Through adequate management of the resulting intellectual property (IP), the public

Chapter 5
104
sector can benefit from its R&D investments through the availability of the most modern products
with conditions that are beneficial for the developing world, eliminating otherwise significant
barriers to access (14). Joint research ventures such as partnerships among developing countries,
the private sector, academic institutions and NGO’s depend on IP management strategies.
However, recent publications indicated that intellectual property rights negotiations are more
complex in horizontal research joint ventures (same industry) and when universities are involved
(15).
Patents are the most frequently used IPPM (15). For example, the Medicines for Malaria Venture
(MMV) arrangement for the synthetic peroxide antimalarial project involved the assignment of a
patent from a U.S. university. The patent included claims for treating cancer and schistosomiasis,
which are retained by MMV. The compound was licensed to an Indian company, Ranbaxy, with a
provision for reversion of the rights to MMV should Ranbaxy fail to meet certain milestones (such
as meeting public sector demand in target developing countries at affordable prices). Likewise,
further segmentation of the market into a “traveler’s market” and worldwide private sector sales
provides potential commercial incentives for Ranbaxy once they meet the criteria for public
health interest (14). But innovative partnerships have also come up with non‐patented drugs. The
Drugs for Neglected Diseases Initiative (DNDi) partnered with French pharmaceutical company
Sanofi‐Aventis in 2007 and brought fixed‐dose artesunate‐based combination therapies to the
African market. This patent‐free model is now also implemented for delivering anti‐malarial
treatment to South American patients (http://www.ip‐watch.org/weblog/2008/04/17/innovative‐
partnership‐to‐create‐another‐patent‐free‐malaria‐drug).
Capacity building
During the past two decades, numerous research centers have been developed in sub‐Saharan
Africa, where high quality research is conducted. The majority has strong links with a Northern
partner and the number of regional and supra‐regional networks of excellence is growing. In
addition, many of the centers are linked to patient cohorts or even demographic surveillance
systems (http://www.indepth‐network.org). However, there exists a substantial regional
imbalance with the majority of these centers being located in South and East Africa, a few in West
Africa (http://www.africaclinicaltrials.org) and only limited activities exist in Central Africa.
Furthermore, most of these centers are involved in research in the area of malaria and HIV/AIDS
or tuberculosis, but almost never in neglected diseases.

Review
105
Many of the research centers have evolved from being trial sites conducting epidemiological
studies or single trials to project sites, and some have become research centers with all the
capacities needed to maintain a portfolio of trials and to be involved in different fields of activity
(see Table 1).
The development of a trial site to a research centre is a long process in which well‐planned and
sustainable capacity building has a central function. A critical mass of local researchers needs to
be trained and given a career perspective to avoid excessive “brain drain”; the institution must
build up the leadership to not only deliver research excellence, but also provide adequate
governance, administrative, financial and management functions (17); the respective
infrastructures needs to be built; and the quality assurance systems necessary for the compliant
conduct of the trials must be implemented and enforced. In the experience of our team, which is
routinely involved in monitoring and auditing of a substantial number of trials and research
centers, this latter aspect still needs attention. The level of detail requested today is considerable
and the main findings include the confusion of document versions, incomplete tracking of
processes and unwanted deviations from protocols or procedures. Clear and practical internal
standard operating procedures at all levels and the installation of internal quality control help to
avoid such verdicts.
The creation of such sustainable and comparatively independent research centers may not always
be achievable. Many of the most neglected diseases (e.g. human African Trypanosomiasis, Buruli
ulcer, trachoma) are characterized by a rural distribution and may be locally controlled or even
eliminated through dedicated disease control activities. Conducting clinical trials in such regions
requires the involvement of small treatment facilities with often very basic infrastructure and very
Table 1. Characteristics of the evolution from a trial site to a research centre (16)
Trial site Project site Research centre What is core? Informal alliance of
projects and trial sites Established infrastructure to projects/trials
Fully established entity that provides all science infrastructure
Core funding Resources from projects fund the core
Small amount of core ‐ funding and resources
Funding of core established and projects contribute to core
Portfolio Single or small number of projects that drive core
Small number of projects ‐ able to add different diseases or interventions
Different interventions and/or different diseases
Time focus Short term Mid term (3‐5 years) Long term (> 10 years)
Infrastructure Very basic and dependent on project funding
Established basics that survive individual trials/projects
Full infrastructure maintained over time with projects paying share

Chapter 5
106
limited human resources. The conduct of a single clinical trial often leads to a significant
reduction in the relevant patient number in the catchment area, preventing follow‐up projects.
The switch to other diseases or projects is normally impossible due to the remoteness of the
center and the mentioned limitations.
Particular attention has to be paid in such situations to the appropriate information about the
intentions of the researchers, the adequate training of local staff and site improvement. The
minimum obligation is to leave behind a team well‐trained in the relevant areas and a laboratory
with specific improvements for the daily routine.
The conduct of clinical trials in sub‐Saharan Africa
Ethics
The goals of research are always secondary to the well‐being of the participants. This requirement
is made clear in the Declaration of Helsinki and is regarded as the fundamental guiding principle
of research involving human subjects (18). Discussions on bioethics of clinical research in
resource‐limited settings are manifold and include the therapeutic areas, the quality and quantity
of research as well as discussion on the use of placebo or the use of the best versus the locally
available standard of care.
Guidelines on bioethics and clinical research are numerous and sometimes conflicting. Where the
Declaration of Helsinki has established the guiding principles of research involving human
subjects, it does not cover all relevant aspects for the conduct of clinical research. Currently, the
correct overall reference for the conduct of clinical trials is being discussed. The guiding role of
the Helsinki Declaration was contested by the U.S. FDA and it was decided to replace it by the
standards described in the ICH GCP (19). On the other hand the ICH guideline itself had been
seen as being too comprehensive and strict for the conduct of clinical trials in resource‐limited
countries (20). The increase in clinical trials conducted in such settings goes hand in hand with
an increasing capacity and this discussion will continue with a yet unknown outcome.
In this article, we only discuss ethical aspects that have a direct and/or practical impact on the
trial and the trial participants. In this respect, we take post‐treatment access to successful
interventions for the relevant populations for granted, although this may be a very challenging
issue in specific cases.
Essential literature on research involving human subjects is listed in Table 2.

Review
107
Ethics committees
The ethical clearance by an independent ethics committee in the host as well as in the sponsoring
country is one of the key requirements. The first African ethics committee was established in
South Africa, 1967 (24). But in 2005, 36% of the WHO African Region countries still had no ethics
committees. Capacity development in the area of research ethics was promoted (25) and the
establishment of ethics committees and the provision of training and capacity building is today
actively supported by, for example, the Pan‐African Bioethics Initiative (PABIN)
(http://www.pabin.org) as a member of the global Strategic Initiative for Developing Capacity in
Ethical Review (SIDCER) and the South African Research Ethics Training Initiative (SARETI)
funded by the Fogarty International Center of the US NIH (http://www.fic.nih.gov). However,
many committees are not yet fully functional due to lack of funding, infrastructure, training,
standard operating procedures and sometimes simply the lack of political commitment from the
governments.
Besides national ethical clearance of the research project in the host country we strongly
encourage ethical clearance by local ethics committees. Local ethics committees can best
represent the cultural, political and economic values of the region and can act as a hinge between
community needs and research priorities. The value of the implementation of a local ethics
committee depends on the number of clinical research projects conducted in the particular
area/region and will likely be linked to a well‐established research center.
Today, the lack of capacity of National Regulatory Authorities (NRA) leads to the situation that
ethics committees often fill the role of local drug regulators, too. However, not only for this
reason, strengthening of NRA capacities has a very high priority. Efforts must include the
authorization and monitoring of clinical trials, the evaluation of clinical data for product
registration, and quality control and pharmacovigilance of medicinal products.
Table 2. Essential literature on research including human subjects.
Documents
International Conference on Harmonization / ICH Harmonized tripartite guideline: Guideline for Good Clinical Practice GCP E6 (3)
World Medical Association Declaration of Helsinki (http://www.wma.net/e/policy/b3.htm)
Council for International Organizations of Medical Sciences / CIOMS: International ethical guidelines for biomedical research involving human subjects (in collaboration with WHO) (21)
Nuffield Council on Bioethics: The ethics of research related to healthcare in developing countries (22)
National Bioethics Advisory Commission / NBAC: Ethical and Policy Issues in International Research: Clinical Trials in Developing Countries (23)

Chapter 5
108
In view of this formidable task, systems supporting NRAs and optimizing the use of regional
resources and expertise are needed. An example is the WHO African Vaccine Regulatory Forum
(AVAREF) which can be considered as an "ad‐hoc" scientific advisory body that can help
regulators to make an informed regulatory decision with regards to authorizations of clinical
trials, evaluation of registration dossiers or any other challenging issues regarding evaluation of
vaccines (11).
Informed consent and assent
Patient information and written informed consent are two of the most sensitive and complex
parts of clinical research. This is true for all clinical research conducted but even more so in sub‐
Saharan Africa. In contrast to Western culture, communal consciousness and living is the norm in
many African societies and for decision‐making processes, the importance of community leaders
and families cannot be eroded (26). Patient information forms which are long, complex and
sometimes inappropriate in the cultural context where they are used, may confuse, rather than
inform, participants and can be refused by the local Ethics committees (27). Balancing
completeness versus simplicity is a real challenge in the preparation of patient information. An
appropriate patient information and informed consent procedure is key in the prevention of the
therapeutic misconception; when participants believe that they are receiving a new form of
treatment rather than participating in research (28).
If children are involved, the parents or the legal guardian must give consent. However, children
capable of making decisions (depending on the society and the disease of an age of 7 or older)
should be asked for their assent which must be respected if the response is negative (29).
A further sensitive issue is the requirement for written informed consent (3). In certain cultures
or situations, signing of a consent form has very negative connotations and may even be rejected
(22). Whether written consent forms are adequate for use with illiterate patients has also been
debated and the National Bioethics Advisory Commission has issued a recommendation to waive
written consent in such situations (23) and to replace it with an alternative appropriate process
which must be specified in the protocol (e.g. independent witnesses).
Finally, if the language in which the information is to be provided is different from the one used
for the protocol, the text must be translated to a locally spoken language and should be back‐
translated to detect and rule out misunderstandings. This process may be particularly difficult
and tedious in settings where indigenous languages with a limited modern word pool are spoken
and where the translation and back translation process requires particular attention. If a language

Review
109
is not written, the information must be read and explained from a sheet written in an alternative
official language. In this case, the presence of a knowledgeable witness seems to be appropriate.
Indemnities and undue inducement
Particular attention is required for the adequate indemnification of study participants. One has to
be aware of the coercion or undue inducement (30) of overpaid indemnities and of exclusive
payments linked to completion of the trial. It is clear that the patients in resource‐poor settings
need to receive a fair compensation for their efforts such as transportation or sometimes for the
working time lost during hospitalization. The local representatives often opt for paying in kind,
particularly in rural settings. However, there is a fine line and one should be aware that trial or
project sites can comply with the research proposals because they bring work, salaries, technology
transfer and materials to their locations.
Publication of results and trial registration
The publication of positive and negative trial results is an ethical requirement as stated in the
Declaration of Helsinki (http://www.wma.net/e/policy/b3.htm). However, in reality the
publication of results is frequently delayed or even omitted. Corporate involvement in clinical
research may lead to the exclusive disclosure of results to regulators. The very long follow‐up
periods typical to a number of neglected diseases such as human African trypanosomiasis,
contribute to extensive delays in the publication of data.
The increasing acceptance of the importance of public information and the reduction of selective
reporting is reflected in the mandatory registration of clinical trials. In 2004, the International
Committee of Medical Journal Editors published a respective joint editorial: before first patient
enrolment any clinical trial must be registered in a public database to allow publication. There are
various public registries for clinical trials but since 2005 the “WHO International Clinical Trial
Registry Platform” (http://www.who.int/trialsearch/) has taken the lead. As another mechanism
which might assist the timely publication of data on diseases requiring a long patient follow‐up,
we suggest discussion of the option to separately publish the safety and efficacy data in two linked
publications. Table 3 summarizes the minimum ethical standards to be met at local, national and
sponsor level.

Chapter 5
110
Implementation and conduct of trials in resource‐limited environments
In the case that a clinical research project is carried out in collaboration with a rural trial site, the
sponsor is confronted with challenges that do not exist in other settings. The absence of well
educated health personnel, high staff turnover, poor infrastructure, lack of standard operating
procedures and difficult accessibility are common. Often the situation is complicated by an
unstable security situation created by political conflicts. Importantly, traditional beliefs and
stigma have a strong impact on the behavior of the population and health staff, and may influence
the research activities.
For the conduct of clinical trials in such situations, centre assessment and site selection are of
paramount importance. The capacities and infrastructures very often must be built up and
maintained on a continuous basis. Issues which are practically unknown in the implementation of
trials in Western settings must be considered: the presence of an educated physician and other
staff members, appropriate laboratories including (stable) energy supply, laboratory staff training
and the installation of communication tools may be issues. The appropriate level of site
improvements should be balanced between the requirements of the trial and the maximum
capacities of the staff.
Table 3. Minimum ethical standards for research involving human subjects.
LOCAL LEVEL NATIONAL LEVEL SPONSOR LEVEL
Staff understanding of the importance of a correct patient information and a correct informed consent process Respect of right for anonymity of trial participants Community information and involvement Fair information of all potential participants (complete, simple wording) Consent at relevant levels Individual consent of all participant Written consent as a standard option; alternatives with sufficient justification where necessary Fair compensation for trial participation
Timely ethical review by designated national or thematic Ethics committee Timely approbation of cleared trial by drug authorities or Ministry of Health and controlled importation of the investigational product
Study design respecting the local situation, capacities and cultural constraints Ethical review in sponsor (or CRO) home‐country unless host country IEC is certified Trial registration

Review
111
Quite often the questions asked in a protocol have to be adapted to the limited possibilities of the
sites. It is wiser to focus on the key topics and to refrain from obtaining information on all details.
The basic principle of GCP, that anything not documented does not exist, necessitates a thorough
and clean recording of data and the creation of an appropriate and easy‐to‐monitor filing and
recording system. Such consistent systems rarely exist in rural health facilities where records are
usually kept in various books and booklets. Furthermore, long‐term storage of the study and
patient records must be assured, which can be problematic considering heat, humidity and the
often precarious room situations.
Dedicated pharmacies and adequate clean and air‐conditioned storage with limited access are
often non‐existent in such facilities and practical solutions must be found to protect the
experimental product from misuse, to guarantee its quality and to account for its receipt, use and
return or destruction.
A difficult and critical issue is the reporting of adverse and serious adverse events (SAEs). If not
stressed, adverse events may not be recorded at all as they are not considered unusual. For SAEs it
is important to (i) convey the difference between severeness (clinical term) and seriousness
(technical and legal term) and (ii) to implement a reliable, monitorable communication system
that allows timely reporting of SAEs to the sponsor/contract research organization and the Ethics
committee.
Clinical data management (CDM) is a particularly delicate topic. Under the new regulations CDM
has become a highly regulated field. Specialized software and tedious validation of the programs,
systems, data transfer and trial setup are necessary. To avoid post‐trial or even approval
difficulties the CDM for multi‐center, multi‐country trials is usually concentrated at dedicated
contract research companies. But centralized data collection and storage may conflict with the
intentions and ambitions of the local investigators. In particular, sites with links to a demographic
surveillance system or which routinely run large‐scale epidemiological studies may have
sophisticated equipment and statistical knowledge and opt for local CDM. In our experience with
such situations, a pragmatic approach is advantageous, since inconsistent data quality and
complicated trial structures cannot be in anyone’s interest.
Final study reports to the regulatory authorities should be written by professional scientific
writers but the sponsors should clearly recognize the needs and interests of their partners to
publish results and their active involvement should already be defined in the study protocol.
For the control of certain diseases, e.g. human African trypanosomiasis and onchocerciasis,
specialized mobile teams visiting the population at risk are necessary. Those teams have to be
integrated in the work flow of the respective clinical trials and can be used for the information of

Chapter 5
112
the population, for pre‐screening of potential patients and even enroll participants in a trial. To
maintain a coherent technical standard, a strong presence of technical advisors, supervisors and
specialized monitors familiar with the disease, the local situation and the language, and intensive
external support in site management have to be warranted. Typically, this approach is only
possible through a joint venture of the implementing organization with the responsible national
and/or district authority. Such partnerships have to be built and preserved carefully, as the
enrolment in trials on neglected diseases tends to be very slow. An example for this is given in the
accounts of the Phase II trial for Moxidectin against onchocerciasis (31).
In summary, the conduct of clinical trials in rural settings is certainly not a low‐cost option and
entails particular challenges. Table 4 summarizes the minimum standards required to conduct
GCP‐compliant trials.
Table 4. Minimum standards for the conduct of clinical trials according to the International Conference on Harmonization/ Good Clinical Practice (3).
LOCAL LEVEL NATIONAL LEVEL SPONSOR LEVEL
The presence of educated medical staff and nursing care Capacities for documentation and archiving Assurance of confidentiality Accurate reporting and verification of the data Adherence to the protocol Version control for protocol and informed consent Correct, timely reporting and handling of adverse and serious adverse drug reactions Infrastructures for correct storage and use of the investigational medicinal product
Monitoring and surveillance of ongoing projects
Responsibility for quality assurance and quality control Qualified personnel for the trial design, trial management and medical expertise Trial registration Insurance for participants Financing Notification and submission to regulatory authorities Information on investigational product (investigators brochure) Manufacturing, packaging, labeling, (coding) and supply of investigational product Notification of end of study Reporting

Review
113
Access and delivery
This topic, although of paramount importance for every intervention, goes beyond the scope of
this paper and we will only summarily examine it.
Post marketing studies and pharmacovigilance
When a marketing application is filed for regulatory approval, the documentation for a new drug
will typically comprise a few thousand patients with data mainly collected through Phase I to III
trials (32). Although these data are considered to be sufficient to describe the safety and efficacy
profile of a new compound, at this stage there is no data about the effectiveness of the drug in the
real‐life situation. Questions about unforeseen drug interaction, rare adverse events, effects of
poor patient compliance and dynamics of resistances have not yet been addressed. This
information is needed for the safe use of a drug, particularly in high risk groups such as pregnant
and lactating women, children, malnourished and HIV‐infected patients. In addition, the
information is an important element in making a decision whether a new intervention should be
added to the essential drug list of a country. At the global level, the WHO program for
international drug monitoring at the Uppsala monitoring centre collates adverse drug reaction
reports via the national pharmacovigilance centers of the 81 member countries (www.who‐
umc.org). Currently there are only six sub‐Saharan African countries (South Africa, Zimbabwe,
Tanzania, Mozambique, Nigeria and Ghana) that are full members of the program. In fact, less
than 27% of lower middle income countries have national pharmacovigilance systems registered
with the WHO program, compared with 96% of the high income countries in the Organization
for Economic Co‐operation and Development. The main reasons for this are lack of resources,
infrastructure and expertise. Thus, although access to medicines is increasing in developing
countries, there is a danger that their risk‐benefit profiles in indigenous populations will not be
fully monitored (33). To make up for this shortcoming of local data, at least substantial Phase IIIb
or drug utilization trials should be conducted.
Access
The effectiveness of an intervention depends on many factors which may be linked to a product
or be parameters of the health system, such as affordable market price, distribution channels and
their accessibility, sustained availability of the product, quality control, information for health

Chapter 5
114
care professionals and the general public, and correct diagnosis. At each level, those involved may
have conflicting interests, and poor populations are the first to suffer the effects of frail links in
this long chain (34).
Recent experience indicates that the drugs developed in PDPs have a faster introduction to the
market. This puts a lot of pressure on public health systems and currently, many projects fail
because the health systems are not strong enough to deliver new interventions to the target
populations. Also the Global Fund to fight AIDS, tuberculosis and malaria
(http://www.theglobalfund.org) recognizes this need and supports the strengthening of health
systems (35). An important aspect is health information. It is recognized that inadequate access to
information is a significant factor in development, and particularly in health care development.
Despite major global progress in access to information during the last decade, there is little
evidence that health professionals, especially those working in rural primary health care, are
better informed than they were 10 years ago (36). The unequal distribution of health care between
developed and developing countries is matched by a similar unequal distribution of health
information (37) and the 10/90 gap in health research probably translates into a 1/99 gap in health
information (36).
The way forward
The development and provision of new interventions to prevent, diagnose, treat and control
diseases that affect the poorest and most vulnerable populations finally is receiving global
attention and support. Today, numerous initiatives, consortia and PDPs are engaged in those
activities and the funding has reached unprecedented dimensions. This results in a large number
of ongoing research projects and the proportion of clinical trials being truly performed according
to GCP is increasing. This development has already led to tangible results. For instance, several
new chemical entities for the treatment of malaria have been or will be registered shortly by first
tier drug authorities. A number of new research centers in sub‐Saharan Africa have emerged and
are gaining momentum. A strong generation of scientists is developing and is reasonably well‐
supported through various competitive fellowship grants. This also opens the possibility that
researchers will increasingly see career opportunities at home which may reduce the “brain drain”
effect and with this, innovation and leadership will be strengthened in the long term.
So, can we lean back and wait for better days dawning? There are still serious gaps and short‐
comings which will require enormous effort to be overcome. It now seems critical to maintain
impetus in the research area and to continue the processes started at all levels. This will not be

Review
115
achieved solely by continuing funding but also through genuine political interest and backing by
the governments and institutional leaders of the developing countries. From the R&D point of
view, there is a need for the technical strengthening of all divisions or drug regulatory authorities,
participatory involvement of research scientists at institutional levels and the reduction of
artificial logistical hurdles.
The treatment of many of the most neglected diseases is still dreadful and this will certainly still
need increasing attention. However, the transition of health (i.e. the epidemiologic shift from
infectious to chronic diseases particularly in urban areas) will incontestably create new
challenges, but potentially also new opportunities for the research centers involved in R&D.
Acknowledgements
We would like to thank Marcel Tanner and Juerg Utzinger for discussions and valuable input. We
are grateful to Benjamin Dahl for critical reading and correction of the manuscript.

Chapter 5
116
References
1. MSF/DNDi. Fatal Imbalance: The crisis in Research and Development for Drugs for Neglected Diseases. Geneva: Médecins Sans Frontières Access to Essential Medicines Campaign, Drugs for Neglected Diseases Working Group; 2001.
2. Moran M. A breakthrough in R&D for neglected diseases: new ways to get the drugs we need. PLoS Med. 2005 Sep;2(9):e302.
3. ICH/GCP. ICH harmonized tripartite guideline, Guideline for good clinical practice E6 (R1). Surrey: Canary Publications, UK; 1996.
4. Hotez P, Stoever K, Fenwick A, Molyneux D, Savioli L. The Lancet's chronic diseases series. Lancet. 2006 Feb 18;367(9510):563‐4; author reply 4‐5.
5. Perrin D, Scheer A, Wells T. Collaborating to find new approaches to tropical diseases. European Pharmaceutical Review. 2006 23.05.2006;3:1‐4.
6. Nwaka S, Ridley RG. Virtual drug discovery and development for neglected diseases through public‐private partnerships. Nat Rev Drug Discov. 2003 Nov;2(11):919‐28.
7. Trouiller P, Olliaro P, Torreele E, Orbinski J, Laing R, Ford N. Drug development for neglected diseases: a deficient market and a public‐health policy failure. Lancet. 2002 Jun 22;359(9324):2188‐94.
8. Gelb MH, Hol WG. Parasitology. Drugs to combat tropical protozoan parasites. Science. 2002 Jul 19;297(5580):343‐4.
9. Noedl H, Se Y, Schaecher K, Smith BL, Socheat D, Fukuda MM. Evidence of artemisinin‐resistant malaria in western Cambodia. N Engl J Med. 2008 Dec 11;359(24):2619‐20.
10. Chirac P, Torreele E. Global framework on essential health R&D. Lancet. 2006 May 13;367(9522):1560‐1.
11. WHO. Human African trypanosomiasis (sleeping sickness): epidemiological update. Weekly epidemiological record. 2006 24. Februar(TRS881):69‐80.
12. Kesselheim AS. Drug development for neglected diseases ‐ the trouble with FDA review vouchers. N Engl J Med. 2008 Nov 6;359(19):1981‐3.
13. EMEA. Guidance for companies requesting scientific advice or protocol assistance. Guideline. London: European Medicine Agency; 2005 17. November.
14. Garner C. Dealmaking and Intellectual Property Management for Public Interest. Meeting Report. Bethesday, Mayland: The Initiative on Public‐Private Partnerships for Health (IPPPH), The Centre for Management of Intellectual Property in Health Research and Development (MIHR), Aeras Global TB Vaccine Foundation; 2004 29‐30. Nov.
15. Hertzfeld H, Link A, Vonortas N. Intellectual property protection mechanisms in research parnerships. Research Policy. 2006;35:825‐38.
16. Whitworth JA, Kokwaro G, Kinyanjui S, Snewin VA, Tanner M, Walport M, et al. Strengthening capacity for health research in Africa. Lancet. 2008 Nov 1;372(9649):1590‐3.
17. Gyapong J, Ofori‐Adjei D. Capacity building for relevant health research in developing countries. Knowledge on the Move; 2008 26.02.2008; The Hague: Netherlands organization for international cooperation in higher education (nuffic); 2008.
18. Angell M. The ethics of clinical research in the Third World. N Engl J Med. 1997 Sep 18;337(12):847‐9.
19. FDA. Human subject protection; foreign clinical studies not conducted under an Investigational New Drug Application. CDER 200482 ed: Food and Drug Administration; 2008. p. 22800‐16.

Review
117
20. White NJ. Editorial: clinical trials in tropical diseases: a politically incorrect view. Trop Med Int Health. 2006 Oct;11(10):1483‐4.
21. CIOMS. International ethical guidelines for biomedical research involving human subjects. Bull Med Ethics. 2002 Oct(182):17‐23.
22. NCOB. The ethics of research related to healthcare in developing countries. Report. London: Nuffield Council on Bioethics; 2002 April 2002.
23. NBAC. Ethical and Policy Issues in International Research: Clinical Trials in Developing Countries. Bethesda, Maryland: National Bioethics Advisory Commission; 2001 30.04.
24. Kass NE, Hyder AA, Ajuwon A, Appiah‐Poku J, Barsdorf N, Elsayed DE, et al. The structure and function of research ethics committees in Africa: a case study. PLoS Med. 2007 Jan;4(1):e3.
25. Kirigia JM, Wambebe C, Baba‐Moussa A. Status of national research bioethics committees in the WHO African region. BMC Med Ethics. 2005 Oct 20;6:E10.
26. Bhutta ZA. Beyond informed consent. Bull World Health Organ. 2004 Oct;82(10):771‐7.
27. Mueller J, Schellenberg D, Owens S. Third‐World Barriers ‐ Getting past consent and ethical issues endemic in underserved populations to ensure quality GCP. Applied Clinical Trials. 2007 01.10.2007;October 2007:58‐64.
28. Fairlamb AH, Henderson GB, Cerami A. Trypanothion is the primary target for arsenical drugs against african trypanosomes. Proceedings of the National Academy of Sciences of the United States of America. 1989;86:2607‐11.
29. Broome ME. Consent (assent) for research with pediatric patients. Semin Oncol Nurs. 1999 May;15(2):96‐103.
30. Emanuel EJ, Currie XE, Herman A. Undue inducement in clinical research in developing countries: is it a worry? Lancet. 2005 Jul 23‐29;366(9482):336‐40.
31. Kuesel A, Lazdins J. A new drug for river blindness? TDRnews. 2007 December 2007;79:14‐9.
32. Rawlins MD. Pharmacovigilance: paradise lost, regained or postponed? The William Withering Lecture 1994. J R Coll Physicians Lond. 1995 Jan‐Feb;29(1):41‐9.
33. Pirmohamed M, Atuah KN, Dodoo AN, Winstanley P. Pharmacovigilance in developing countries. Bmj. 2007 Sep 8;335(7618):462.
34. Pecoul B, Chirac P, Trouiller P, Pinel J. Access to essential drugs in poor countries: a lost battle? Jama. 1999 Jan 27;281(4):361‐7.
35. WHO/GFATM. The Global Fund Strategic Approach to Health Systems Strengthening. Report. Geneva: The Global Fund to fight AIDS, Tuberculosis and Malaria; 2007 September. Report No.: WHO/HSS/2007.1.
36. Godlee F, Pakenham‐Walsh N, Ncayiyana D, Cohen B, Packer A. Can we achieve health information for all by 2015? Lancet. 2004 Jul 17‐23;364(9430):295‐300.
37. Katikireddi SV. HINARI: bridging the global information divide. Bmj. 2004 May 15;328(7449):1190‐3.

118

Discussion
119
Chapter 6
Discussion
Lwala Hospital, Kaberamaido District, Uganda
Kaliua Hospital, Urambo District, Tanzania

Chapter 6
120
Access to patients
The two main bottlenecks for clinical research in T.b. rhodesiense endemic areas are the limited
number of available patients and the difficulty of finding them. Populations at risk of contracting
sleeping sickness live scattered in remote rural areas with limited access to health services.
Patterns of health seeking behaviour and difficulties of the service provider to diagnose HAT lead
to long delays in diagnosis and therefore in treatment.
Traditional beliefs, distance and cost of transport usually influence negatively health seeking and
patients often attempt first to make use of local medicine. This is usually expensive and patients
may be kept for weeks in the care of traditional healers. Family members bringing patients in a
terminal disease stage to a health centre is unfortunately not a rare event, and often such patients
die within a few hours after arrival.
Another difficulty is the lack of technical capacity for HAT diagnosis at the provider side. On one
hand there is a limited sensitivity of the diagnostic tools in use, and on the other hand there are
also major issues with the professional performance and disease awareness at provider level.
Especially clinical officers and nurses should be aware of the signs and symptoms and the
geographical distribution of the disease. They are in contact with patients whose condition is not
improving despite repetitive antimalarial and antibiotic treatments. Also, they are in the position
to request the laboratory to check for trypanosomes. It is therefore of central importance to
inform health personnel working in HAT endemic regions regularly about the disease in order to
improve case detection. In areas where the disease has newly emerged the competence of health
services to response adequately is even further limited, and the capacity to identify and diagnose
HAT should be built quickly.
Only 35% of the IMPAMEL III participants were diagnosed with HAT upon their first visit at the
health centre. 44% had 2‐3 and 21% had more than 3 contacts with health care providers before
diagnosis was made. The delay in HAT diagnosis was significantly longer in the site in Uganda
where patients had to visit a health facility in average 2.2 times (CI 2‐2.5) compared to Tanzania
where the diagnosis was made in average after 1.6 visits (CI 1.4‐1.7). This is obviously problematic
for remote rural populations for whom the cost of repeated trips to health centres is prohibitive.
A study carried out on the patterns of health‐seeking behaviour in an established T.b. rhodesiense
focus in Uganda showed that the median total delay from onset of illness to diagnosis was 60
days. The median delay of the service provider to diagnose sleeping sickness among symptomatic
individual was markedly longer (30 days) than the median delay of the patients (17 days) to
present at the health facility (1). Further findings were that a large proportion of the patients were
either referred to the sleeping sickness hospital by members of their community or presented

Discussion
121
there on their own initiative. Only few patients were referred by other tiers of the health system
(1).
The WHO and the Foundation for Innovative and new Diagnostics (FIND) established a
consortium for the research and development of new human African trypanosomiasis diagnostic
tools appropriate for use in low‐income countries in 2006 (2). In this framework WHO is
currently establishing a HAT specimen bank by collecting reference materials from well
characterized patients and controls. The specimen bank is physically located at the Institute
Pasteur, Paris, France which is responsible for cryopreservation, and managing the distribution of
specimens (3). The accessibility of the samples to public and private partners is controlled by a
joint WHO/FIND committee. Hopefully these efforts will results in the delivery of new diagnostic
tools for diagnosis and disease staging in the near future.
As of today, the loop‐mediated isothermal amplification (LAMP) technique is the most promising
tool for detection of T.b. rhodesiense HAT under field conditions (4, 5) and might be available
commercially in the near future (http://www.finddiagnostics.org).
Control of T.b. gambiense sleeping sickness is largely based on active surveillance using serology
(CATT) (6). However, for T.b. rhodesiense HAT this approach is of limited success due to the lack
of a serological test with sufficient sensitivity (7). Diagnosis during active mass screening
campaigns in T.b. rhodesiense affected areas has to rely on direct microscopy and if logistically
possible, on the haematocrit centrifugation technique. Further, sick individuals often do not show
up at community‐based screenings a bottleneck of population screenings also described for in
T.b. gambiense areas (8). The effectiveness of active population screenings in endemic T.b.
rhodesiense settings is doubtful due to the low prevalence, the diagnostic constrains and the
variability of the attendance rates. According WHO active screening should therefore be confined
to areas where there is evidence of an outbreak (9). As an example, during an epidemic in Zambia
(1980‐1984) a total of 23’751 individuals were screened by mobile field teams and only 102 cases
(0.43%) were diagnosed (10).
For the IMPAMEL III trials access to patients was increased by complementary activities to the
standard passive case detection. In the catchment areas of the Kaliua Health Centre in Tanzania
and the Lwala Hospital in Uganda we performed active case searches. On the basis of index cases
mobile teams screened the local population using direct microscopy. Due to the low success rate
in the first round of active case searches the index cases were followed up to household level at
the second round but this did not yield better outcomes. Community sensitization was done
through local councils, local leaders and churches. In Uganda, the missionary radio station
informed the population about the IMPAMEL III program. Such advertisements were very effective

Chapter 6
122
in mobilizing people. However, mostly healthy people came for screening and the sick (weak and
often unable to walk) were not seen. At district level, the officers for vector control and disease
surveillance were informed, not only to support case identification but also the follow‐up
activities, which are known to be difficult. In the end, the most successful strategy to identify
patients turned out to be visits to the surrounding health facilities and requesting blood slides for
all inpatients.
Issues concerning the study design
Because of the existence of two forms of HAT the results of the IMPAMEL I&II programs could not
be extrapolated to East African patients. The assessment of the abridged treatment schedule was
regarded essential in order to provide access to the improved melarsoprol therapy also in T.b.
rhodesiense affected areas and therefore, the IMPAMEL III trials were of high priority for the WHO
and the affected countries. In addition, the alternative schedule may also provide the basis for
future combination treatments and a harmonization of all East African treatment protocols. For
the latter, it was important to assess as well the benefit of the suramin pre‐treatment, which is
only partially implemented in East Africa. For the IMPAMEL III program it was decided to use
centre‐specific suramin protocols. The heterogeneity of the protocols in use did not allow us to
agree on a single one.
Concerns during the planning of Impamel III were the fear of unexpected toxicity because of the
higher parasitaemia and reported higher incidence of encephalopathic syndromes (ES) in T.b.
rhodesiense patients (11). However, the ES is most likely not an acute reaction to the disruption of
trypanosomes (12) as it occurs in most cases after several days of melarsoprol treatment. Also it
was shown in several instances that the development of ES is unrelated to either dosage or
administration schedule (13, 14). The current hypothesis for the development of ES suggests an
immune mechanism (15) which is corroborated by the efficacy of prednisolone in its prevention
(15, 16) and the significantly increased risk of ES associated with a small number of alleles of the
human leukocyte antigen (HLA) (17). Based on this evidence the 10‐day melarsoprol schedule was
not expected to trigger an increased incidence of ES in T.b. rhodesiense patients.
The efficacy of the 10‐day melarsoprol schedule was expected to be similar to the efficacy of the
national regimes in use. For these, the total exposure time of the parasite to melarsoprol was 9
days in Tanzania (3 series each for 3 days) and 12 days in Uganda (4 series each for 3 days). Each
series was interrupted by resting periods of 5 to 7 days. Based on the pharmacokinetic properties
of melarsoprol investigated in uninfected vervet monkeys and computer simulations it was shown

Discussion
123
that melarsoprol concentration in the CSF drops to sub curative levels during the resting periods
(18). As maximum CSF concentrations of melarsoprol are reached about 10 hours after drug
application (19) the parasites are exposed to a much higher drug pressure under the 10‐day
melarsoprol schedule. Therefore the efficacy of the 10‐day melarsoprol schedule was considered
unproblematic in comparison to the national regimens in use. Further, compared to the 10‐day
melarsoprol schedule patient hospitalization times were much longer in the national treatment
schedules which negatively affected patient compliance and with this treatment efficacy.
Given the high genetic heterogeneity of T.b. rhodesiense and the wide spectrum of disease severity
(20) a multinational approach had to be considered in order to rule out significant differences in
responses to treatment. In terms of reported number of cases per year, Uganda, Tanzania and
Malawi were potential sites and centre assessments were done in the three countries. Finally, two
were selected in Tanzania and Uganda. This decision was based on the experiences of the
respective centre in HAT diagnosis and treatment, on the reported case numbers in the previous
6 months and on the accessibility of the centres.
IMPAMEL III – study design
The preferred design to test the effect size of any biomedical intervention is the randomized
controlled trial. Our sample size calculations indicated that we would require a minimum of 400
patients (200 per arm) to show a difference of 10% between the 10‐day melarsoprol schedule and
the national regimens in use. The IMPAMEL I & II programs demonstrated the clinical non‐
inferiority of the 10‐day melarsoprol schedule and demonstrating such non‐inferiority would have
required even a larger sample size. Hence, this approach was impossible given the number of
expected patients.
As a result, we first performed a proof‐of‐concept trial to verify the safety of the 10‐day
melarsoprol schedule, collect preliminary efficacy data and assess the effect of the suramin pre‐
treatment. Based on that analysis, and after the decision had been taken that suramin might be
omitted without pertinent risk of the patients, a utilization study was designed as an extension to
the non‐suramin arm of the proof‐of‐concept trial. This utilization study had a calculated sample
size requirement of 100 patients. The sample size of 100 was chosen in order to have a precision of
±6% on the estimated endpoint. Since the pooling of the data of the 30 patients from the proof‐of‐
concept trial with the data of the utilization study was planned to increase the total evaluable
sample, the latter was carried out according the same eligibility criteria, endpoints and stopping
rule. The design of the IMPAMEL III program is schematically shown in figure 1.

Chapter 6
124
Figure 1: Study design IMPAMEL III
Safety
Based on the reported case fatality rates of the two trial centres, as well as literature, the cut‐off
point for case fatality under the 10‐day melarsoprol schedule was set at ≥10%. Causes of death are
difficult to determine under field conditions and in order to avoid difficulties in the causal
relationship of death and the study drug, we used a composite endpoint of all‐cause mortality.
The censoring of the different risks attributable to the death was avoided and reduced bias. Such
composite end‐points of all‐cause mortality are commonly used in toxicological studies and are a
valuable endpoint also for melarsoprol trials.
Suramin pre‐treatment
Our investigations on the risk‐benefit ratio of the suramin pre‐treatment were first based on the
comparison of the two subgroups of the proof‐of‐concept trial (2x30) and in a second step on the
comparison of all the patients who received suramin (n=30) and all the patients who were directly
treated with melarsoprol (n=107).
The results of the proof‐of‐concept trial indicated a potential harm of the suramin pre‐treatment;
adverse events were significantly higher in the patient group that received the suramin pre‐
treatment (63.3%) than in patients who were directly treated with melarsoprol (23.3%, p=0.0018).
Also more serious adverse events (SAEs) were reported in patients who received suramin; ES (4
vs. 3) and death (5 vs. 2) but this trend was not significant. The suramin pre‐treatment was
Proof-of-concept trial (n=60)
Suramin pre-treatment; 10-day melarsoprol schedule (n=30)
10-day melarsoprol schedule (n=30)
Utilization study (n=77)
10-day melarsoprol schedule
Final analysispooled dataset (n=107)
Comparatorhistoric controls (n=300)
1
2
Interim analysis (n=60)

Discussion
125
administered according to centre‐specific guidelines; in Tanzania patients received a total dose of
25mg/kg and in Uganda 5mg/kg but no centre‐specific differences in the frequency of adverse
reactions were seen (p=0.7048).
However, comparing the 30 patients that received suramin and the 107 patients that were directly
treated with melarsoprol we did not see statistically significant differences in the proportion of
patients that experienced adverse events (63.3% vs. 61.7%; p=0.8692) and serious adverse events
(26.6%, 16.8%; p=0.2243).
Overall, our data provided neither evidence of harm nor of benefit of the suramin pre‐treatment.
This confirms previous findings on the use of pre‐treatments prior to melarsoprol: for T.b.
gambiense HAT little or no value was found for a pentamidine pre‐treatment (13, 21) and for T.b.
rhodesiense HAT the suramin pre‐treatment improved the condition of two patients (22) which
triggered its use prior to melarsoprol. But in other patients it showed no effects (23).
Dose‐escalating studies to determine the dose to be tested in Phase II trials are commonly
designed according the classical 3+3 design: the dose‐limiting toxicity is assessed in cohorts of 3 to
6 patients (24). Our study provided a larger sample size to assess suramin‐related adverse and
serious adverse events and we are confident that our results make an important contribution to
this discussion.
Efficacy
The latest WHO technical report series recommends a 2‐year patient follow‐up of HAT patients
in order to monitor the long‐term efficacy of treatments. The clinical condition of the patient and
the blood and cerebrospinal fluid (CSF) should be examined after 3, 6, 12, 18 and 24 months. The
leukocyte number in the CSF should be determined though the interpretation is stated as difficult
as the leukocyte number can be slow in returning to a normal level (9).
Based on the WHO recommendation of the informal consultation on issues for clinical product
development for HAT (25), patients with no trypanosomes after treatment are classified as
responders and should be followed up after 3 or 6, 12 and 18 months (25). The CSF WBC counts
should not be taken into account to evaluate treatment efficacy at end of treatment as they may
not have normalized at that time (26). A test of cure visit is recommended after 18 months: cure
can be confirmed in case of no parasitological evidence of relapse and a WBC count
<20cells/mm3. Patients in whom trypanosomes are detected in any body fluid are classified as
relapses. Patients without parasitological evidence of relapse and who have WBC count>20/mm3
that can not be explained by a disease other than HAT are classified as probable relapse (25). The

Chapter 6
126
threshold of 20 WBC is due to an additional disease stage in Gambian HAT which has recently
been suggested and is known as the “early‐late stage”. The proposal is based on the observation
that patients who had trypanosomes in the CSF but a WBC count below 20cells/mm3 were
successfully treated with the first stage drug pentamidine (27‐29). However, this classification is
debated; a retrospective analysis of data where the criterion for second stage disease set to a WBC
count of >10cells/mm3 showed that this threshold led to a higher risk of relapse compared to the
figure of 5 cells/mm3 (30). Intermediate disease stages were also described for T.b. rhodesiense
HAT; e.g. if the CNS was only “slightly affected” suramin was said to possibly be curative. But for
such cases a close follow‐up with repeated lumbar punctures at relatively short intervals (at most
two months) was made essential. If such surveillance was not possible melarsoprol should be
given rather than suramin (31). The treatment of intermediate T.b. rhodesiense HAT stages with
suramin never became operational in the field.
However, there is currently not sufficient data on the relationship of WBC counts and
parasitological and clinical evidence of cure and relapse. Surrogate markers to determine the
stage of the disease and to diagnose a relapse as early as possible is important in T.b. gambiense
HAT since patients can be asymptomatic for long periods of time. Given the acuteness of T.b.
rhodesiense HAT where the disease progresses to CNS involvement within 3 weeks to 1 month (32)
we believe that surrogate markers are less important for the diagnosis of relapse and cure.
There are currently no guidelines on how to monitor treatment efficacy in T.b. rhodesiense
patients. The WHO recommendation of the informal consultation on issues for clinical product
development for HAT states that “while the data summarized deal with T.b. gambiense HAT,
similar considerations apply to T.b. rhodesiense HAT” (25). This 79 pages document mentions
“T.b. rhodesiense” a mere 6 times and not once in relation to second stage disease; a further
indicator of how neglected T.b. rhodesiense HAT is.
It has been stated that T.b. rhodesiense patients should be monitored as in Gambian HAT except
that the LP during the first year should be performed every 3 months (33). This approach is not
feasible as no active patient follow‐up in East Africa is implemented in practice. WHO stated that
given the severity of the disease it is considered that patients would volunteer for treatment (9).
Under non‐trial conditions the most reliable source of data on treatment efficacy in T.b.
rhodesiense areas is the HATSENTINEL network, a sentinel surveillance network active in 9 sites;
7 sites are located in areas endemic for T.b. gambiense (Angola, Democratic Republic of the
Congo, Sudan) and two sites are in areas endemic for T.b. rhodesiense (Uganda, United Republic
of Tanzania) (25).

Discussion
127
However, patient follow‐up is mandatory for treatments in clinical development. The IMPAMEL III
study protocol had two endpoints for efficacy; the primary endpoint (clinical and parasitological
cure) at end of treatment in order to mitigate the problem of missing data. The secondary
endpoint was during follow‐up after 3, 6 and 12 months with a test of cure evaluation at the 12
months follow‐up visit. Relapses were defined as the presence of trypanosomes in any
compartment. Cure was defined as no parasitological and clinical evidence of relapse and a WBC
count <5cells/mm3. Patients that did not present for follow‐up examinations or refused LP were
considered clinically cured if they were in good general condition (see chapter 2).
Despite our efforts to emphasize the importance of the follow‐up and reimbursing transport costs
for patients as well as for one attendant we saw important losses to follow‐up in the IMPAMEL III
program. Common obstructions for follow‐up activities in HAT are the fear of the painful lumbar
puncture and lack of transport (34, 35) but also the perception on its importance, especially when
patients are in good condition.
To obtain information on all patients that did not present at the centre for follow‐up
examinations we engaged community health workers and district officials. Through those
channels we collected oral information on the general condition of the patients. Given the
acuteness of T.b. rhodesiense HAT relapses or re‐infections would not go undetected by the
patients or the communities, but possibly unreported. A similar approach of engaging village
health workers/sleeping sickness assistants for disease control was a successful control strategy in
the past in Uganda (36). We consider this approach also as a satisfactory tool for monitoring long‐
term efficacy in patients not returning for follow‐up visits.
The progression of WBC counts in the IMPAMEL III patients over time and per country are shown
in figure 2. Thresholds for WBC counts (WBC=20cells/mm3 and WBC=5cells/mm3) are also
shown.

Chapter 6
128
Figure 2:WBC counts (±SE) during treatment and follow‐up. And threshold levels of WBC counts for
definition of cure.
In both countries a clear tendency of leukocyte decrease over time was observed. The WBC
counts in Tanzania did not fall below 5cells/mm3 during 12 months of follow‐up. However, this
was not surprising given the significantly higher WBC counts on admission.
Despite that the 12 months follow‐up of the utilization study is currently ongoing we do not
expect any significant changes in our findings. Data shown in figure 5 includes follow‐up results
of all IMPAMEL III patients up to the end of March 2009. At this point in time the 12 months
follow‐up was concluded in 74% of the patients form Tanzania and in 51% of the patients from
Uganda.
According to the WHO definition of cure (no evidence of parasitological relapse and WBC count
<20WBC/mm3 at 18 months after discharge) (25) patients from Uganda were cured at end of
treatment and patients from Tanzania were cured 6 months after discharge.
According the IMPAMEL III definition of cure (no evidence of parasitological relapse and WBC
count <5cells/mm3 at 12 months after discharge) patients from Uganda were cured after 3 months
and patients from Tanzania could not be considered cured 12 months after discharge. Yet, we do
not doubt the cure of patients in Tanzania as the trend in CSF WBC is more important than the
absolute value; also many T.b. gambiense patients who were genuinely cured had slightly elevated

Discussion
129
CSF WBC 6 months after treatment (11). Further, the significance of CSF WBC counts is inferior to
clinical and parasitological evidence.
We consider a patient follow‐up of 12 months as reasonable. Any follow‐up examination beyond
12 months would be less appropriate given the fulminant progression of the disease. However, for
the test of cure evaluation we found the 6 months follow‐up visit provided better evidence than
the 12 months follow‐up. The attendance rate has decrease over time and at 12 months
conclusions on treatment efficacy were mainly based on oral information on the general
condition of the patients. From all patients enrolled into the proof‐of‐concept trial 51% presented
at the centre for the 6 months and 34% for the 12 months follow‐up. For patients enrolled into the
utilization study the attendance rate at the 6 months follow‐up visit was 70% and so far 17% for
the 12 months follow‐up. Follow‐up attendance rates could probably be improved if patients
would only have to come back once, but knowing that this single appointment can not be missed
in order to confirm cure.
Given the acute nature of the disease we believe that most patients with a relapse / re‐infection
would report again to a health facility. Hence it would be reasonable to assume under non‐trial
conditions that most patients who are not seen again on follow‐up at the health facility would
likely to be cured. However, for clinical product development more specific guidelines for the
assessment of long‐term efficacy should be elaborated and a test of cure evaluation at 6 months
after discharge could be considered.
For the assessment of treatment efficacy in T.b. rhodesiense HAT the risk of re‐infection can not
be disregarded. There is an increased human–fly contact due to the proximity of livestock and
people (37) and certain patients returning to their sources of income are at higher risk of (re)
infection such as hunters, fishermen, railway workers, honey gatherers and firewood collectors
(38, 39).
Historic controls
The use of historic controls is generally considered as suboptimal due to the potential for
selection bias. Clinical trial criteria for inclusion in the treatment group are usually more
stringent than in historic controls that generally include all patients seen who meet the diagnostic
criteria for the disease under study (40). However, we believe that in our case the trial population
was comparable to the historic controls: the IMPAMEL III program clearly aimed at the inclusion of
a patient population that reflects to large extends the reality in the T.b. rhodesiense endemic
regions. All patients with confirmed second stage infection were eligible for participation;

Chapter 6
130
excluded were children below the age of 6 years, pregnant women and unconscious or moribund
patients. Also, the age distribution of HAT patients reflects the active adult population (80% of
cases are adults) (41) and populations in endemic regions have similar sources of livelihood which
makes them comparable for e.g. risk of infection, co‐morbidities, nutritional status and health
seeking behaviour.
Yet, many efforts were taken to minimize bias: we only considered patient files from the two trial
centres and a maximum time period of two years prior to study initiation because ancillary care
and referral patterns can differ between centres and change over time. A very thorough review
process of all files was done. In comparison to the comprehensive trial documentation the historic
files were poorly reported. We found that a large number of files were incomplete and some were
missing completely. We selected only files that contained basic demographic data and valid
information on treatment outcome. Fatal treatment outcomes were mostly clearly reported but
information on clinical and diagnostic baseline findings, concomitant medications and adverse
events were not reported in detail. We collected data on serious adverse events (SAEs) with
extreme caution. The thorough review process and the excellent memory of the head nurses for
most patient histories ameliorated the quality of the data. The final data set (n=300) was
considered a robust source.
The mean age in the historic population was 29 years and the male/female ration was 1.4. The trial
population was in average older with a mean age of 36 years and had the same male/female ratio
of 1.4. As 7% of cases from the historic dataset were younger than 6 years the difference in the
mean age of the two populations can be partially explained by the exclusion of this age group
from the IMPAMEL III trials. There is little knowledge on HAT in children. We identified one study
that compared the clinical presentation and treatment outcomes of T.b. rhodesiense HAT in
children and adults. Similar to findings in T.b. gambiense HAT the symptomatology of HAT was
described similar for children and adults, with the exception of the first years of life, where
symptoms such as headache, sleeping disorder or motor weakness are difficult to evaluate (42,
43). However, data on treatment outcomes were not discussed due to co‐infections of the
children with measles (42).
In order to control for potential confounders we calculated the incidence of ES and death in the
historic data once on the basis of all selected patient files and once by exclusion of all files of
children younger than 6 years. However, no significant differences were found and for the
comparison with the trial data the entire data set of historic controls was used (see chapter 2).

Discussion
131
The incidence of ES and death reported in the historic data (13%; 9.3%) compared well with data
on ES and death in T.b. rhodesiense patients from a systematic literature review on the ES during
melarsoprol treatment (10.6%; 11.6%) (17) and provided confidence on the quality of the data.
We conclude that despite the controversies on historic controlled trials, the historic data
generated in the framework of the IMPAMEL III program in Kaliua Health Centre and the Lwala
Hospital were adequate controls.
Serious adverse events (SAEs) and case management
Surprising at the SAE profile of the 10‐day melarsoprol schedule in T.b. rhodesiense patients was
the high proportion (35%) of patients that had an event‐free treatment course. Also the much
lower rate of skin reactions (6.5%) compared to the IMPAMEL I & II programs that reported skin
reactions in 28% of the patients (44, 45) was surprising. So far, the understanding of skin reaction
was either a hypersensitivity reaction or the accumulation of heavy metal in the skin (44) and a
dose relationship. Our results trigger thoughts on other causalities and possibly host or parasite
genetics may influence the development of skin reactions.
The encephalopathic syndrome (ES) is the most severe SAE of melarsoprol therapy. Even though
melarsoprol has been in use for more than 50 years, many aspects of the development of ES
remain unclear. However, a rather specific aspect in the development of ES is the time to onset. In
the IMPAMEL III trial population the median time to onset of ES was 7.5 days (range 3‐10days)
which was comparable to the median time of onset reported in the IMPAMEL II (median 9 days,
range 1‐28 days) (45). Thus, the suspected mechanism of a delayed immune reaction against
immune complexes (46) seem to be similar for both forms of HAT.
However, the health personnel actually treating the patients would benefit from evidence on risk
factors associated with a higher risk of ES and could either adopt preventive measures or monitor
those patients extremely attentively. Several risk factors for ES were proposed and included
selenium deficiency (47), seasonality, treatment with thiabendazole, bad general condition of the
patient and alcohol intake during treatment (48). However, none of these were properly assessed
or showed significant association. So far, the only risk factor for ES with useful implications in the
field was shown in T.b. gambiense patients: the presence of trypanosomes in the CSF or WBC
counts higher than 100 were associated with a higher risk of ES (49). The risk factor analysis of
our data did so far not yield interesting results. We will extend the analysis with other statistical
approaches which might enable us to describe risk factors for ES in T.b. rhodesiense patients.
However, in order to investigate possible geographical patterns of ES we mapped the home

Chapter 6
132
villages of the patients and the villages of the patients who developed ES. In Uganda data was only
available up to parish level.
In both countries no obvious clustering of ES events was found ‐ see figure 3 for results in
Tanzania and figure 4 for results in Uganda.
Figure 3: Location of home villages of patients with uncomplicated melarsoprol treatment (green) and
patients who developed ES (red).

Discussion
133
Figure 4: Parishes of patients with uncomplicated melarsoprol treatment and parishes with patients who
developed ES.
Note: HAT patients from Soroti district are usually diagnosed and treated at the Serere Health centre. Only
four patient of the IMPAMEL III trial came from Soroti district and none developed ES.
Case management
A much debated topic with regard to the treatment guidelines for sleeping sickness is the
concomitant use of steroids (50). For T.b. gambiense HAT a randomized controlled trial
conducted in 620 second stage patients showed a significant reduction in the incidence of ES and
a non‐significant but prominent reduction of the ES related mortality in the patient group that
received prednisone (15).
We were able to identify three studies that investigated the concomitant use of steroids in T.b.
rhodesiense HAT. One study reported no benefit of a concomitant use of dexamethasone.
However, the study had three arms and compared two groups of 34 patients that received

Chapter 6
134
dexamethasone with one control group of 25 patients that did not receive dexamethasone. All
three groups were treated with different treatment protocols for diminazene aceturate (Berenil®)
and melarsoprol (51). Another study showed no reduction in the incidence of ES by the co‐
administration of corticosteroids (not specified which one). However, this was a retrospective
study in two patient groups (n=200; n=183) that were treated according different melarsoprol
schedules (52). One trial compared the use of prednisone in two patients groups (n=2x18) treated
with the same melarsoprol schedule. But a reduction of the incidence of ES could not be shown
(53).
The results of the IMPAMEL III program are clearly in favour of the concomitant use of steroids for
the treatment of second stage T.b. rhodesiense HAT. During the proof‐of‐concept trial, steroids
were used according to centre‐specific guidelines: patients in Tanzania received 10mg of
prednisolone daily. In Uganda steroids were given in case of adverse drug reactions. ES was
observed at a higher incidence in Uganda (p=0.0444) and during the utilization study the use of
steroids was adapted to the Tanzanian standard in both centres. The incidence rate of ES was
subsequently similar between the two centres (p=0.5176).
A high variability of case fatality rates between different treatment centres has been reported (45)
and certainly goes beyond the variability in the use of steroids. The treatment of patients with
melarsoprol requires some experience and an early recognition of warning signs has an impact on
the clinical outcome. Mental excitements, twitching movements, headache, dizziness, vomiting
are predictor signs for ES and should lead to the immediate discontinuation of melarsoprol (54,
55). Further it is important to be vigilant for a possible malaria. Inexperienced staff would
attribute drowsiness and fits during treatment to the severity of the disease and a diagnosis of
severe malaria might be missed. Therefore, blood slides for malaria should be mandatory (42).
Inexperienced staff is often overwhelmed by the management of HAT patients, especially in the
case of ES and this often results in an irrational use of drugs to cover all eventualities such as
malaria, meningitis, shock, severe bacterial infections or raised intracranial pressure. Given the
potential for adverse effects and interactions this is hazardous, especially in the case of a critically
ill ES patient. The only realistic solution to this problem is to refer sleeping sickness patients to
centres who have experience in the management of HAT and to provide staff in such centres with
the best possible medical training. However, this solution can potentially aggravate the poor
access to health services and could only me maintained by standard referral patterns.

Discussion
135
Public health challenges in the control of T.b. rhodesiense HAT
While the incidence of reported T.b. gambiense HAT appeared to have decreased across Africa
over the past five years (56), T.b. rhodesiense foci in Uganda have expanded with potential for a
much larger number of cases (57).
The control of the two forms of sleeping sickness is fundamentally different. The cornerstone for
the control of T.b. gambiense HAT is the early detection of cases as infected subjects remain
asymptomatic and contagious for months before the disease develops. In contrast, T.b.
rhodesiense HAT is mainly controlled by disease surveillance and vector control (11). The
deployment of tsetse traps and screens has proven to be an efficient method of vector control. A
highly successful example is the vector control project that was launched in the Busoga focus in
Uganda to stop disease transmission. The tsetse population was reduced by more than 95% and
some parishes even achieved elimination (58). Since the animal reservoir plays an important role
in the epidemiology of T.b. rhodesiense HAT, tsetse control is crucial in order to reduce the risk of
outbreaks (59‐61). It was shown that tsetse were 5 times more likely to get infected from a blood
meal on cattle than humans (62) and mass chemotherapy of animals has been advocated as an
effective strategy for control of the spread of T.b. rhodesiense HAT (59). However, this approach
can be hindered by the emergence of resistant trypanosomes which can be spread from humans
to cattle and vice versa (63). In addition, many zoonotic diseases are not controlled effectively
because adequate policies and funding are lacking (64). This also applies to the control of T.b.
rhodesiense HAT. The Pan African Tsetse and Trypanosomiasis Eradication Campaign (PATTEC)
makes substantial efforts to control the vectors but there is still room for improvements to
achieve a well coordinated control of animal and human trypanosomiasis. This would be
economically beneficial with substantial benefits to livestock production as well as to the public
health sector through reducing the burden on health services (57). Tsetse control as well as
treatment of cattle falls under the Ministries of Agriculture in most governments of Africa and
coordination with the Ministry of Health is a major limiting factor.
The most problematic factor in the control of T.b. rhodesiense HAT is the substantial
underreporting of the disease. It has been estimated that for every deceased patient that is
reported, another 12 die undetected. Approximately 85% of the unreported deaths do enter the
health system at some stage, of which one‐third die undiagnosed (65). The underreported cases
account for 93% of the total DALY estimate of rhodesiense HAT (57). There are great benefits in
reducing this hidden burden of disease and the cost for each DALY averted has been calculated at
USD 10 (57). This is amongst the most cost‐effective interventions in resource‐limited countries
(66).

Chapter 6
136
The potential overlap of T.b. gambiense and T.b. rhodesiense in Uganda
The foci of T.b. gambiense and T.b. rhodesiense are moving towards each other in Uganda and an
imminent overlap of the two disease forms is feared (67).We could not find any evidence for this
in our study area (see chapter 3). However, this development has to be carefully monitored as
such an overlap will have a major impact on the already strained health system and hamper
proper diagnosis and treatment. The type of infection, as well as the stage of the disease, is of
central importance for patient management. Currently, the type of infection is entirely dependent
on the geographical location of the patient and implies the choice of treatment. Since the two
parasites can only be distinguished by PCR analysis which is impossible under field conditions
such an overlap would pose great problems.
A potential disease overlap would also raise issues of mixed infections in human, animal and
vector populations. Genetic recombination of trypanosome isolates from the same epidemic area
has been shown under laboratory conditions (68). Also, an overlap of the two disease
distributions is unlikely to be prevented by an incompatibility between vector populations and
parasite (69) This would aggravate the problems of diagnosis and treatment that we face already.
IMPAMEL III: from innovation to validation to application
14 years ago the 10‐day melarsoprol schedule was first suggested for the treatment of second stage
T.b. gambiense HAT (70). A series of IMPAMEL programs validated the use of the 10‐day
melarsoprol schedule in second stage sleeping sickness patients in West and Central Africa (1997‐
2004) (44, 45, 71) and recently in East Africa (2006‐2009). In both forms of the disease, a clinical
non‐inferiority of the abridged schedule over the standard regimens could be demonstrated.
Given the major socio‐economic benefits of the 10‐day melarsoprol schedule this brought a great
benefit to the patients as well as to the health care provider.
The development process of new and successful interventions can be divided in the three
categories of innovation, validation and application. For the 10‐day melarsoprol schedule these
processes are schematically shown in Figure 5.

Discussion
137
Figure 5: Innovation, validation and application of the 10‐day melarsoprol schedule in HAT affected
countries (arrow indicates official recommendation of 10‐day melarsoprol schedule in T.b. gambiense areas
at global level)
Only a successful translation of research findings into policy and practice at global, national and
at local level will ensure the access of the target populations. Today, it is widely accepted that the
traditional model of research dissemination through publication in peer reviewed journals has
failed (72). In order to bridge the so‐called “know‐do gap”, institutions and mechanisms that
systematically promote interactions between researchers, policy makers and other stakeholders
need to be strengthened (73). The WHO as well as national and international agencies take an
active role in knowledge translation and emphasize that “research should lead to development,
and development lead to more research relevant to development needs” (74). Further, the
translation of generated knowledge and evidence into policy decisions and program management
is vital for health system strengthening, scaling up health interventions and to tackle the health
human resource crisis in developing countries (75).
New research findings have to first be disseminated at global level. For HAT, the biannual
meeting of the International Scientific Council for Trypanosomiasis Research and Control
(ISCTRC) is the main platform for discussion and dissemination of research findings at
Implementation & use of the 10-day melarsoprol schedule for the treatment of second stageT.b. gambiense & T.b. rhodesiense HAT
IMPAMEL I Safety and efficacy in the treatment of T.b. gambiense HAT
1997-2000
IMPAMEL II From efficacy to effectiveness in T.b. gambiense endemic areas
2000-2004
2006-2009IMPAMEL IIISafety and efficacy in the treatment of T.b. rhodesiense HAT
Validation
Abridged 10-day melarsoprol schedulePharmacokinetics, animal models, computer modelling
1990-1994Innovation
Application
Note: implementation & use of the 10-day melarsoprol schedule in T.b. gambiense HAT started after the official recommendation in 2003

Chapter 6
138
international level. The use of the 10‐day melarsoprol schedule for all T.b. gambiense affected
areas was officially recommended at the ISCTRC meeting in Pretoria in 2003. The same strategy is
attempted for the findings of the IMPAMEL III program and the data will be presented during the
30th ISCTRC meeting in Entebbe, Uganda, 21‐25 September 2009. It is expected that WHO and the
T.b. rhodesiense affected countries will discuss the introduction of the 10‐day melarsoprol
schedule for T.b. rhodesiense according the data we have made available.
Knowledge translation at national levels can take some time, especially for neglected diseases due
to their low priority setting on the health agendas. In case of an official recommendation for the
use of the 10‐day melarsoprol schedule, a successful implementation at national level could be
supported by the Regional East African Community Health (REACH) Policy Initiative that
mediates between policy makers and research communities (76). Another platform to be
integrated in the dissemination of the IMPAMEL III results at national levels is the Eastern Africa
Network for Trypanosomiasis / EANETT. Since 2001 the member countries (Sudan, Kenya,
Uganda, Tanzania, Malawi, Switzerland) meet annually to strengthen the collaboration in
research, training and control of trypanosomiasis in the East African region.
The third and last step is the implementation of the new treatment schedule in all treatment
centres in a given country. Unfortunately, a successful translation from research into policy does
not ensure a successful dissemination also at local level. Even though the 10‐day schedule has
been recommended for use in the treatment of second stage T.b. gambiense HAT six years ago,
numerous centres in T.b. gambiense endemic areas still do not use this form of treatment. For the
dissemination of the IMPAMEL III results at local level, a regional training should be organized
inviting district medical officers, doctors, clinical officers, nurses, laboratory staff and a
community representative of the HAT treating centres. Further, regular supervision should be
done during the initial phase to monitor case fatality rates and cure rates at the individual
centres.
All these processes would allow to reach the end line for this new intervention and ensure that a
maximum number of patients benefit from this important advance in the treatment of HAT.

Conclusions
139
Conclusions
The IMPAMEL III program was the first clinical trial conducted in compliance with international
standards of good clinical practice/GCP (ICH E6, GCP) in T.b. rhodesiense HAT and it allowed to
generate representative data on clinical presentation and disease parameters.
The conduct of the program strengthened the local capacities for diagnosis and case
management. In addition, the continuous mobilization of the affected communities and
surrounding health centres have led to an increase in disease awareness, which is crucial for the
timely detection of new cases. Due to the limited number of T.b. rhodesiense patients and the difficulty to find patients it is
almost impossible to conduct properly powered trials for this disease in the ordinary sequence of
Phase II and Phase III. The sequential design of the IMPAMEL III program with the use of historic
controls proved to be a good alternative design and provided conclusive results. The findings of the IMPAMEL I & II programs could be confirmed in T.b. rhodesiense HAT. Patients
treated with the 10‐day melarsoprol schedule were not at higher risk of serious adverse drug
reactions or death compared to patients treated according to previous national regimens. Also,
the patients and the different levels of the health system favoured the abridged schedule due to
the socio‐economic benefits. The suramin pre‐treatment did not lead to a reduction of serious adverse reactions during
melarsoprol therapy.
The short as well as long term efficacy of the 10‐day melarsoprol schedule was very high.
Due to the acute nature of the disease we considered oral information on a patient in good health
as a satisfactory tool to confirm long‐term efficacy in patients not presenting at a health facility.
The lack of specific guidelines on monitoring treatment efficacy in T.b. rhodesiense HAT should
be addressed and our study could provide the basis for that.
The fear of a potential overlap in T.b. rhodesiense and T.b. gambiense disease distribution areas
could not be confirmed in our study area. However, continuous monitoring of the situation is
crucial.
Melarsoprol remains the only drug to treat second stage T.b. rhodesiense HAT. However, it is still
highly unsatisfactory and there is an urgent need for new drugs which are equally effective but
less toxic.

Chapter 6
140
References
1. Odiit M, Shaw A, Welburn SC, Fevre EM, Coleman PG, McDermott JJ. Assessing the patterns of health‐seeking behaviour and awareness among sleeping‐sickness patients in eastern Uganda. Ann Trop Med Parasitol. 2004 Jun;98(4):339‐48.
2. WHO. Request for proposals ‐ human African trypanosomiasis specimen bank. 2007 [cited 2007 07.04.]; Available from:
3. Steverding D. A new initiative for the development of new diagnostic tests for human African trypanosomiasis. Kinetoplastid Biol Dis. 2006;5:1.
4. Kuboki N, Inoue N, Sakurai T, Di Cello F, Grab DJ, Suzuki H, et al. Loop‐mediated isothermal amplification for detection of African trypanosomes. J Clin Microbiol. 2003 Dec;41(12):5517‐24.
5. Njiru ZK, Mikosza AS, Armstrong T, Enyaru JC, Ndung'u JM, Thompson AR. Loop‐Mediated Isothermal Amplification (LAMP) Method for Rapid Detection of Trypanosoma brucei rhodesiense. PLoS Negl Trop Dis. 2008;2(1):e147.
6. Chappuis F, Loutan L, Simarro P, Lejon V, Buscher P. Options for field diagnosis of human african trypanosomiasis. Clin Microbiol Rev. 2005 Jan;18(1):133‐46.
7. Simarro PP, Jannin J, Cattand P. Eliminating human African trypanosomiasis: where do we stand and what comes next? PLoS Med. 2008 Feb;5(2):e55.
8. Robays J, Bilengue MM, Van der Stuyft P, Boelaert M. The effectiveness of active population screening and treatment for sleeping sickness control in the Democratic Republic of Congo. Trop Med Int Health. 2004 May;9(5):542‐50.
9. WHO. Control and surveillance of African trypanosomiasis. Geneva: WHO; 1998.
10. Wellde BT, Chumo DA, Reardon MJ, Nawiri J, Olando J, Wanyama L, et al. Diagnosis of Rhodesian sleeping sickness in the Lambwe Valley (1980‐1984). Ann Trop Med Parasitol. 1989 Aug;83 Suppl 1:63‐71.
11. Pepin J, Donelson JE. African Trypanosomiasis (Sleeping Sickness). In: Guerrant RL, Walker DH, Weller PF, editors. Tropical Infectious Diseses; Principles, Pathogens & Practise. 1 ed. Philadelphia: Churchill Livistone; 1999. p. 774‐84.
12. Adams JH, Haller L, Boa FY, Doua F, Dago A, Konian K. Human African trypanosomiasis (T.b. gambiense): A study of 16 fatal cases of sleeping sickness with some observations on acute reactive arsenical encephalopathy. Neuropathology and Applied Neurobiology. 1986;12:81‐94.
13. Sina G, Triolo N, Trova P, Clabaut JM. [Arsenic encephalopathy in the treatment of human African trypanosomiasis due to T. gambiense (apropos of 16 cases)]. Ann Soc Belg Med Trop. 1977;57(2):67‐74.
14. Buyst H. The epidemiology of sleeping sickness in the historical Luangwa valley. Ann Soc Belg Med Trop. 1977;57(4‐5):349‐59.
15. Pepin J, Milord F, Guern C, Mpia B, Ethier L, Mansinsa D. Trial of prednisolone for prevention of melarsoprol‐induced encephalopathy in gambiense sleeping sickness. Lancet. 1989 Jun 3;1(8649):1246‐50.
16. Pepin J, Milord F. African trypanosomiasis and drug‐induced encephalopathy: risk factors and pathogenesis. Trans R Soc Trop Med Hyg. 1991 Mar‐Apr;85(2):222‐4.
17. Seixas J. Investigations on the encephalopathic syndrome during melarsoprol treatment in human African trypanosomiasis [PhD Thesis]: Basel; 2004.
18. Burri C, Onyango JD, Auma JE, Burudi EM, Brun R. Pharmacokinetics of melarsoprol in uninfected vervet monkeys. Acta Trop. 1994 Oct;58(1):35‐49.
19. Burri C. Pharmacological aspects of the trypanocidal drug melarsoprol. Basel, Switzerland: University of Basel; 1994.

Conclusions
141
20. Ormerod WE. Taxonomy of the sleeping sickness trypanosomes. J Parasitol. 1967 Aug;53( Whittle HC, Pope HM. The febrile response to treatment in Gambian sleeping sickness. Annals of Tropical Medicine and Parasitology. 1972;66(1):7‐14.
22. Apted FI. The treatment of advanced cases of Rhodesian sleeping sickness by Mel. B. and arsobal. Trans R Soc Trop Med Hyg. 1953 Sep;47(5):387‐98.
23. Apted FI. Four years' experience of melarsen oxide/BAL in the treatment of late‐stage Rhodesian sleeping sickness. Trans R Soc Trop Med Hyg. 1957 Jan;51(1):75‐86.
24. Holländer N, Schumacher M. Planung und Auswertungen von Phase I und II Studien. Methodik klinischer Studien, methodische Grundlagen der Planung, Durchführung und Auswertung. 3 ed: Springer; 2008. p. 436.
25.WHO. Recommendations of the Informal Consultation on Issues for Clinical Product Development for Human African Trypanosomiasis. Geneva, Switzerland; 2007. Report No.: WHO/CDS/NTD/IDM/2007.1.
26. Dumas M, Breton JC, Pestre Alexandre M, Girard PL, Giordano C. [Current status of the therapy of human African trypanosomiasis]. La Presse Médicale. 1985;14(5):253‐6.
27. Kennedy PG. Human African trypanosomiasis of the CNS: current issues and challenges. J Clin Invest. 2004 Feb;113(4):496‐504.
28. Doua F, Miezan TW, Sanon Singaro JR, Boa Yapo F, Baltz T. The efficacy of pentamidine in the treatment of early‐late stage Trypanosoma brucei gambiense trypanosomiasis. Am J Trop Med Hyg. 1996 Dec;55(6):586‐8.
29. Lejon V, Legros D, Savignoni A, Etchegorry MG, Mbulamberi D, Buscher P. Neuro‐inflammatory risk factors for treatment failure in "early second stage" sleeping sickness patients treated Balasegaram M, Harris S, Checchi F, Hamel C, Karunakara U. Treatment outcomes and risk factors for relapse in patients with early‐stage human African trypanosomiasis (HAT) in the Republic of the Congo. Bull World Health Organ. 2006 Oct;84(10):777‐82.
31. Apted FI. Present status of chemotherapy and chemopropylaxis of human trypanosomiasis in the Eastern Hemisphere. Pharmacol Ther. 1980;11(2):391‐413.
32. Odiit M, Kansiime F, Enyaru JC. Duration of symptoms and case fatality of sleeping sickness caused by Trypanosoma brucei rhodesiense in Tororo, Uganda. East Afr Med J. 1997 Dec;74(12):792‐5.
33. Pepin J. African Trypanosomiasis. In: Strickland GT, editor. Hunter's Tropical Medicine and Emerging Infectious Diseases. Eighth Edition ed. Philadelphia: Saunders Company; 2000. p. 643‐54.
34. Robays J, Miaka Bilenge M, Stuyft PV, Boelaert M. The effectiveness of active population screening and treatment for sleeping sickness control in the Democratic Republic of Congo. Trop Med Int Health. 2004 May;9(5):542‐50.
35. Veeken HJ, Ebeling MC, Dolmans WM. Trypanosomiasis in a rural hospital in Tanzania. A retrospective study of its management and the results of treatment. Trop Geogr Med. 1989 Apr;41(2):113‐7.
36. Mbulamberi DB. A review of human African trypanosomiasis (HAT) in Uganda. East Afr Med J. 1989 Nov;66(11):743‐7.
37. Pepin J, Meda HA. The epidemiology and control of human African trypanosomiasis. Adv Parasitol. 2001;49:71‐132.
38. Apted FI, Smyly DP, Ormerod WE, Stronach BW. A comparative study of the epidemiology of endemic Rhodesian sleeping sickness in different parts of Africa. J Trop Med Hyg. 1963 Jan;66:1‐16.
39. Wellde BT, Chumo DA, Reardon MJ, Waema D, Smith DH, Gibson WC, et al. Epidemiology of Rhodesian sleeping sickness in the Lambwe Valley, Kenya. Ann Trop Med Parasitol. 1989 Aug;83 Suppl 1:43‐62.

Chapter 6
142
40. Sacks H, Chalmers TC, Smith H, Jr. Randomized versus historical controls for clinical trials. Am J Med. 1982 Feb;72(2):233‐40.
41. Odiit M. The epidemiology of Trypanosoma brucei rhodesiense in Eastern Uganda. Edinburgh: University of Edinburgh; 2003.
42. Buyst H. Sleeping sickness in children. Ann Soc Belg Med Trop. 1977;57(4‐5):201‐12.
43. Blum J, Schmid C, Burri C. Clinical aspects of 2541 patients with second stage human African trypanosomiasis. Acta Trop. 2006 Jan;97(1):55‐64.
44. Burri C, Nkunku S, Merolle A, Smith T, Blum J, Brun R. Efficacy of new, concise schedule for melarsoprol in treatment of sleeping sickness caused by Trypanosoma brucei gambiense: a randomised trial. Lancet. 2000 Apr 22;355(9213):1419‐25.
45. Schmid C, Richer M, Bilenge CM, Josenando T, Chappuis F, Manthelot CR, et al. Effectiveness of a 10‐Day Melarsoprol Schedule for the Treatment of Late‐Stage Human African Trypanosomiasis: Confirmation from a Multinational Study (Impamel II). J Infect Dis. 2005 Jun 1;191(11):1922‐31.
46. Pepin J, Milord F. The treatment of human African trypanosomiasis. Adv Parasitol. 1994;33:1‐47.
47. Golden MH. Arsenic, selenium, and African trypanosomiasis. Lancet. 1992 Jun 6;339(8806):1413.
48. Ancelle T, Barret B, Flachet L, Moren A. [2 epidemics of arsenical encephalopathy in the treatment of trypanosomiasis, Uganda, 1992‐1993]. Bull Soc Pathol Exot. 1994;87(5):341‐6.
49. Pepin J, Milord F, Khonde AN, Niyonsenga T, Loko L, Mpia B, et al. Risk factors for encephalopathy and mortality during melarsoprol treatment of Trypanosoma brucei gambiense sleeping sickness. Trans R Soc Trop Med Hyg. 1995 Jan‐Feb;89(1):92‐7.
50. Atouguia JLM, Kennedy PGE. Neurological aspects of human African trypanosomiasis. In: Davis LE, Kennedy PGE, ed Infectious diseases of the nervous system 1th ed Oxford: Reed Educational and Professional Publishing Ltd. 2000(321‐372).
51. Onyango RJ, Bailey NM, Okach RW, Mwangi EK, Ogada T. Encephalopathy during treatment of human trypanosomiasis. EATRO report. 1969.
52. Arroz JO. Melarsoprol and reactive encephalopathy in Trypanosoma brucei rhodesiense. Trans R Soc Trop Med Hyg. 1987;81(2):192.
53. Foulkes JR. An evaluation of prednisolone as a routine adjunct to the treatment of T. rhodesiense. Journal of Tropical Medicine and Hygiene. 1975;78:72‐4.
54. Buyst H. The treatment of T. rhodesiense sleeping sickness, with special reference to its physio‐pathological and epidemiological basis. Ann Soc Belg Med Trop. 1975;55(2):95‐104.
55. Apted FIC. Present status of chemotherapy and chemoprophylaxis of human trypanosomiasis in the eastern hemisphere. Pharmacology and Therapeutics. 1980;11:391‐413.
56. WHO. Human African trypanosomiasis (sleeping sickness): epidemiological update. Weekly epidemiological record. 2006 24. Februar(TRS881):69‐80.
57. Fevre EM, Odiit M, Coleman PG, Woolhouse ME, Welburn SC. Estimating the burden of rhodesiense sleeping sickness during an outbreak in Serere, eastern Uganda. BMC Public Health. 2008;8:96.
58. Lancien J. [Campaign against sleeping sickness in South‐West Uganda by trapping tsetse flies]. Ann Soc Belg Med Trop. 1991;71 Suppl 1:35‐47.
59. Fevre EM, Coleman PG, Odiit M, Magona JW, Welburn SC, Woolhouse ME. The origins of a new Trypanosoma brucei rhodesiense sleeping sickness outbreak in eastern Uganda. Lancet. 2001 Aug 25;358(9282):625‐8.

Conclusions
143
60. Welburn SC, Fevre EM, Coleman PG, Odiit M, Maudlin I. Sleeping sickness: a tale of two diseases. Trends Parasitol. 2001 Jan;17(1):19‐24.
61. Wendo C. Uganda revises cattle treatment to protect humans from sleeping sickness. Lancet. 2002 Jan 19;359(9302):239.
62. Hide G. History of sleeping sickness in East Africa. Clin Microbiol Rev. 1999 Jan;12(1):112‐25.
63. Matovu E, Iten M, Enyaru JC, Schmid C, Lubega GW, Brun R, et al. Susceptibility of Ugandan Trypanosoma brucei rhodesiense isolated from man and animal reservoirs to diminazene, isometamidium and melarsoprol. Trop Med Int Health. 1997 Jan;2(1):13‐8.
64. Zinsstag J, Schelling E, Roth F, Bonfoh B, de Savigny D, Tanner M. Human benefits of animal interventions for zoonosis control. Emerg Infect Dis. 2007 Apr;13(4):527‐31.
65. Odiit M, Coleman PG, Liu WC, McDermott JJ, Fevre EM, Welburn SC, et al. Quantifying the level of under‐detection of Trypanosoma brucei rhodesiense sleeping sickness cases. Trop Med Int Health. 2005 Sep;10(9):840‐9.
66. Fraser DW. Overlooked opportunities for investing in health research and development. Bull World Health Organ. 2000;78(8):1054‐61.
67. Picozzi K, Fevre EM, Odiit M, Carrington M, Eisler MC, Maudlin I, et al. Sleeping sickness in Uganda: a thin line between two fatal diseases. Bmj. 2005 Nov 26;331(7527):1238‐41.
68. Degen R, Pospichal H, Enyaru J, Jenni L. Sexual compatibility among Trypanosoma brucei isolates from an epidemic area in southeastern Uganda. Parasitol Res. 1995;81(3):253‐7.
69. Abila PP, Slotman MA, Parmakelis A, Dion KB, Robinson AS, Muwanika VB, et al. High Levels of Genetic Differentiation between Ugandan Glossina fuscipes fuscipes Populations Separated by Lake Kyoga. PLoS Negl Trop Dis. 2008;2(5):e242.
70. Burri C, Blum J, Brun R. Alternative application of melarsoprol for treatment of T. b. gambiense sleeping sickness. Preliminary results. Annales de la Société Belge de Médecine Tropicale. 1995;75(1):65‐71.
71. Schmid C, Nkunku S, Merolle A, Vounatsou P, Burri C. Efficacy of 10‐day melarsoprol schedule 2 years after treatment for late‐stage gambiense sleeping sickness. Lancet. 2004 Aug 28;364(9436):789‐90.
72. Ager A. Turning knowledge into health benefits of the poor. Global Forum Update on Reasearch for Health, Poverty, Equity and Health Research. 2005;2:192.
73. Haines A, Kuruvilla S, Borchert M. Bridging the implementation gap between knowledge and action for health. Bull World Health Organ. 2004 Oct;82(10):724‐31; discussion 32.
74. Wasi P. “Triangle That Moves The Mountain” and Health Systems Reform Movement in Thailand. Human Resources for Health Development Journal. 2000 August;4(2):106‐10.
75. Canadian Coalition for Global Health Research C. Strengthening leadership capacity to improve the production and use of health knowledge in Africa Pilot Program. 2006.
76. van Kammen J, de Savigny D, Sewankambo N. Using knowledge brokering to promote evidence‐based policy‐making: The need for support structures. Bull World Health Organ. 2006 Aug;84(8):608‐12.

Chapter 6
144

Appendix 1
145
Appendix 1
IMPAMEL III
Case Report Form (CRF) ‐ Utilization Study

Appendix 1
146

Appendix 1
147

Appendix 1
148

Appendix 1
149

Appendix 1
150

Appendix 1
151

Appendix 1
152

Appendix 1
153

Appendix 1
154

Appendix 1
155

Appendix 1
156

Appendix 1
157

Appendix 1
158

Appendix 1
159

Appendix 1
160

Appendix 2
161
Appendix 2
IMPAMEL III
Patient information and informed consent ‐ Tanzania
English

Appendix 2
162

Appendix 2
163

Appendix 2
164

Appendix 2
165

Appendix 2
166

Appendix 2
167

Appendix 2
168

Appendix 3
169
Appendix 3
IMPAMEL III
Patient information and informed consent ‐ Tanzania
Kiswahili

Appendix 3
170

Appendix 3
171

Appendix 3
172

Appendix 3
173

Appendix 3
174

Appendix 3
175

Appendix 3
176

Appendix 3
177