Embed Size (px)
Citation preview

CARDIAC DEVICE SUMMIT BASEL 2019
GREGOR FAHRNI, OBERARZT KARDIOLOGIE
TAVI UPDATE

KLINISCHER FALL
75 JÄHRIGER MANN
• Schwere Aortenklappenstenose (KÖF 0.9 cm2, dp mean 43 mmHg)
• Dyspnoe NYHA II-III
• Normal LVEF
• berufstätig, aktiv
• 3-Gefäss-KHK mit Stents 2009-2015
• Paroxysmales Vorhofflimmern
• Schlafapnoesyndrom
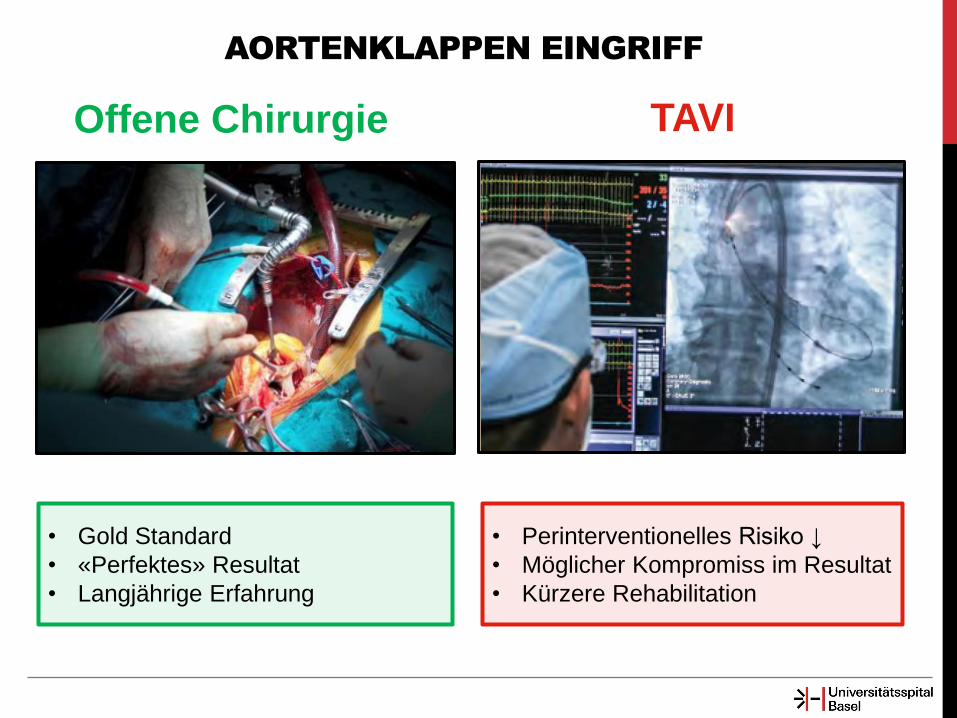
AORTENKLAPPEN EINGRIFF
• Gold Standard
• «Perfektes» Resultat
• Langjährige Erfahrung
• Perinterventionelles Risiko ↓
• Möglicher Kompromiss im Resultat
• Kürzere Rehabilitation
Offene Chirurgie TAVI
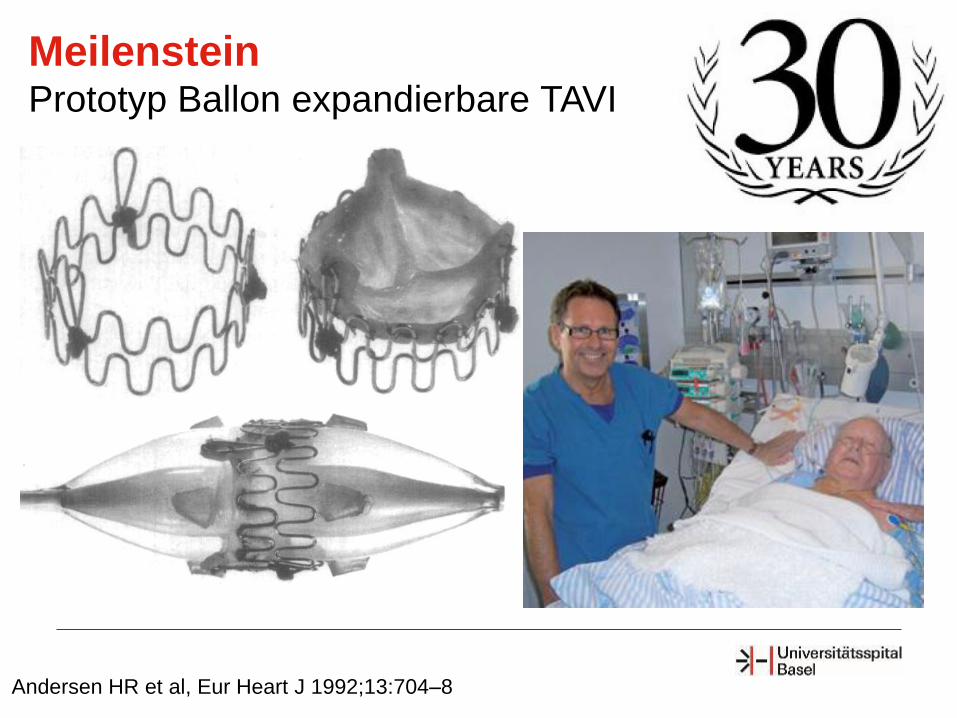
Andersen HR et al, Eur Heart J 1992;13:704–8
Meilenstein Prototyp Ballon expandierbare TAVI
Interventionelle Behandlung von Klappenvitien Technischer Vorschritt in der Automobilindustrie
916 PS 78 PS
Das Prinzip hat sich nicht verändert, nur die Technik hat sich verbessert
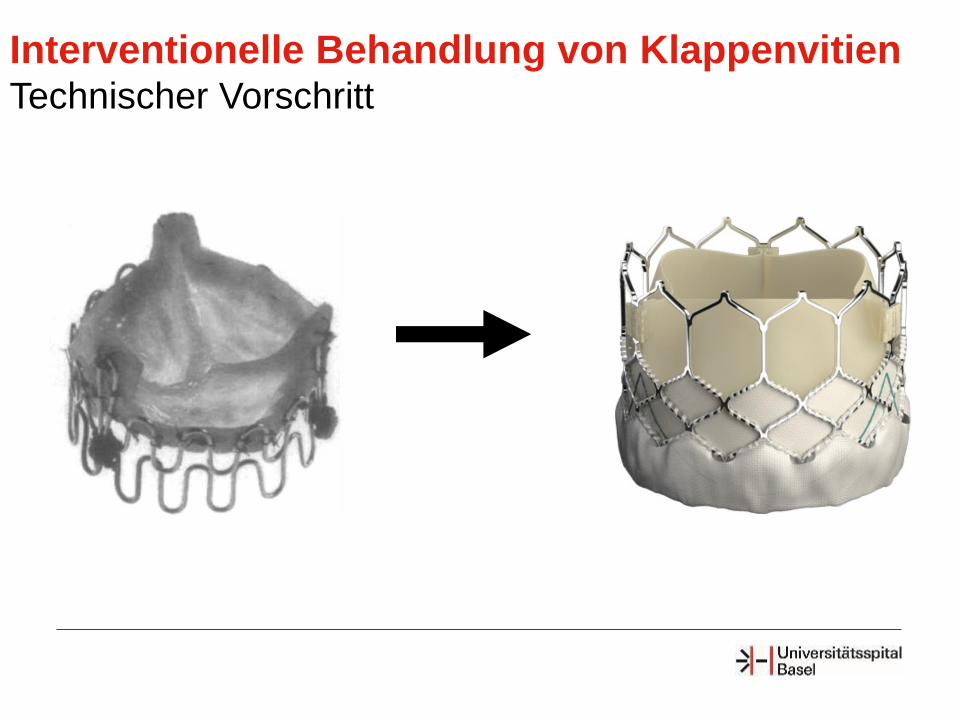
Interventionelle Behandlung von Klappenvitien Technischer Vorschritt
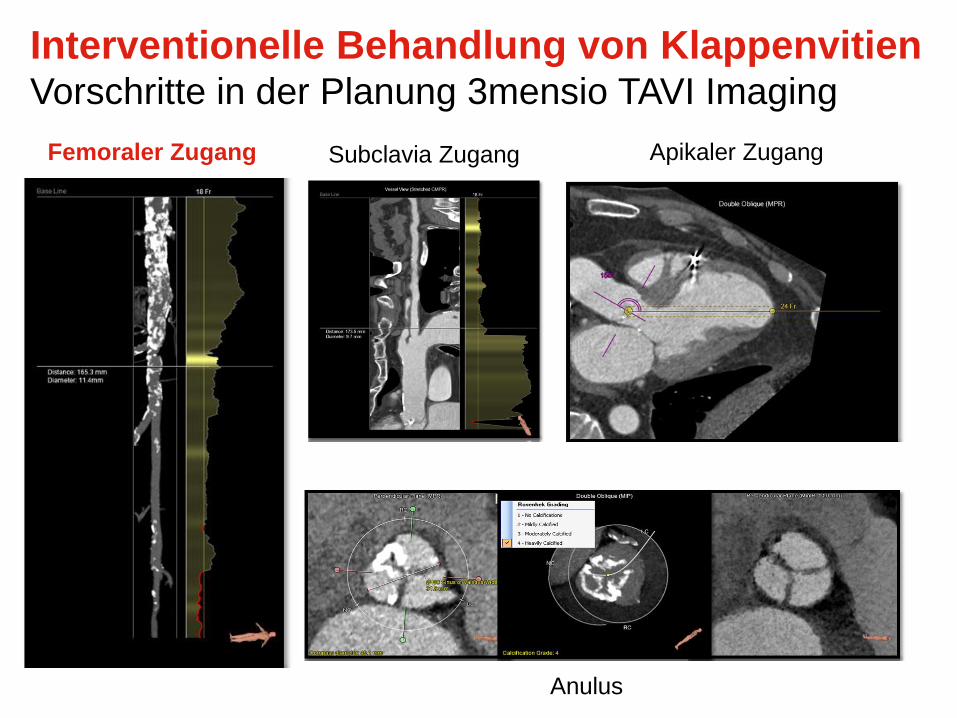
Femoraler Zugang
Anulus
Apikaler Zugang Subclavia Zugang
Interventionelle Behandlung von Klappenvitien Vorschritte in der Planung 3mensio TAVI Imaging
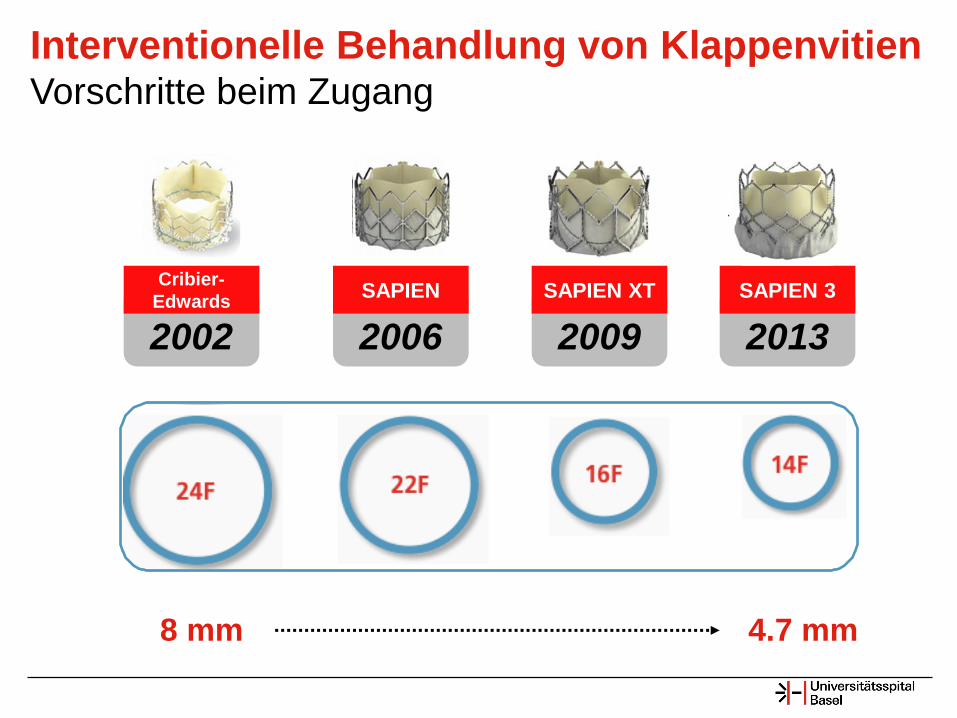
2002
Cribier-
Edwards
2006
SAPIEN
2009
SAPIEN XT
2013
SAPIEN 3
Kardiologie
Interventionelle Behandlung von Klappenvitien Vorschritte beim Zugang
8 mm 4.7 mm

TAVI
Access Routes
Vorschritte im Schutz vor Embolisation Claret Medical Sentinel™
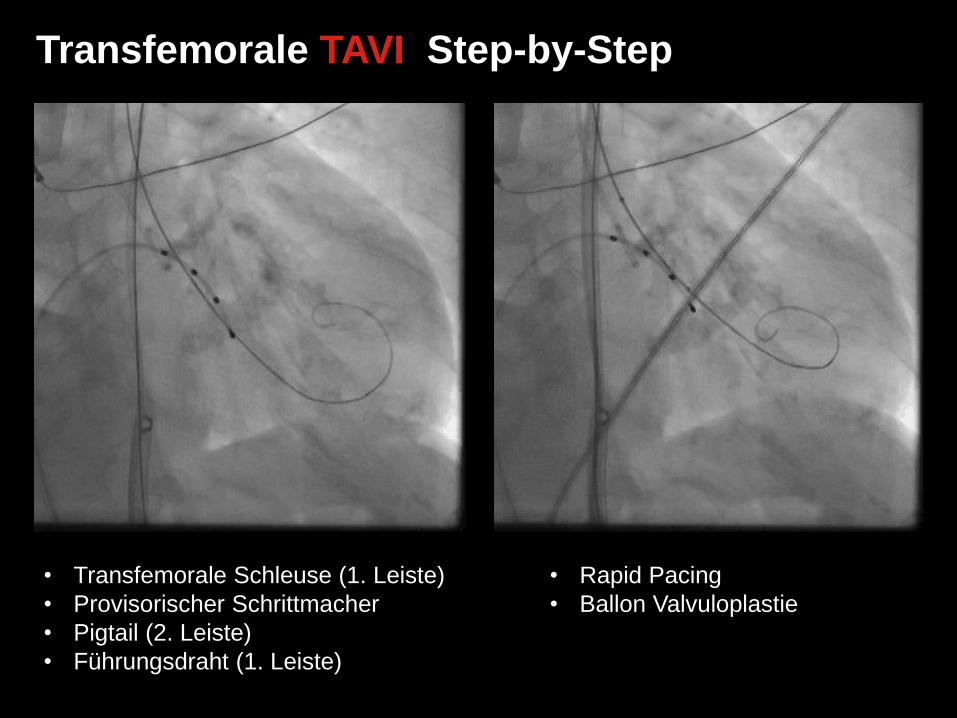
• Transfemorale Schleuse (1. Leiste)
• Provisorischer Schrittmacher
• Pigtail (2. Leiste)
• Führungsdraht (1. Leiste)
• Rapid Pacing
• Ballon Valvuloplastie
Transfemorale TAVI Step-by-Step
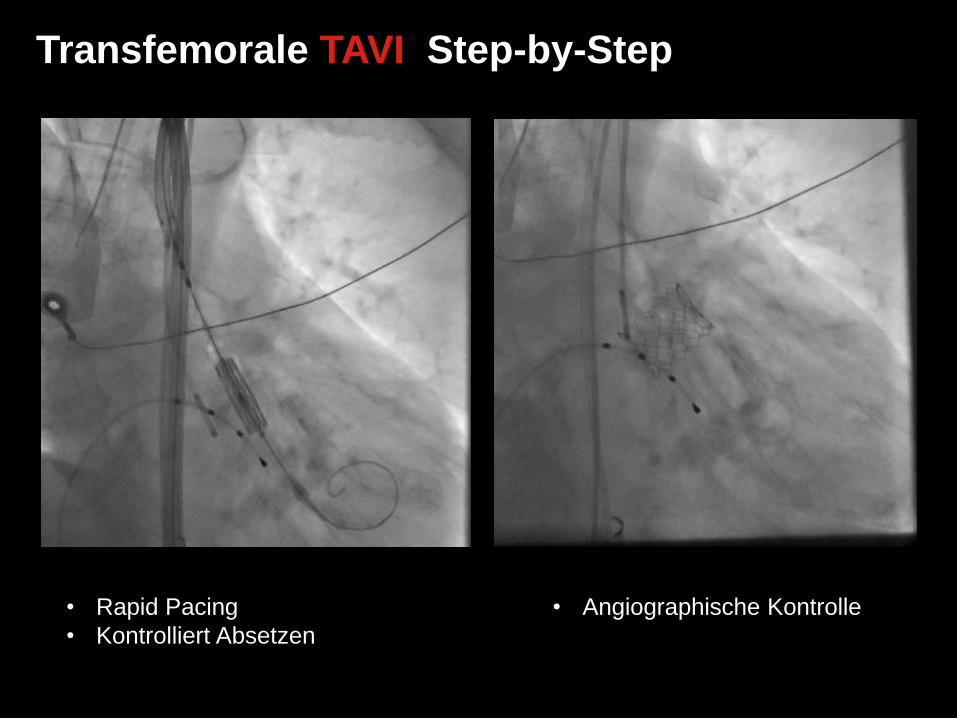
Transfemorale TAVI Step-by-Step
• Rapid Pacing
• Kontrolliert Absetzen
• Angiographische Kontrolle
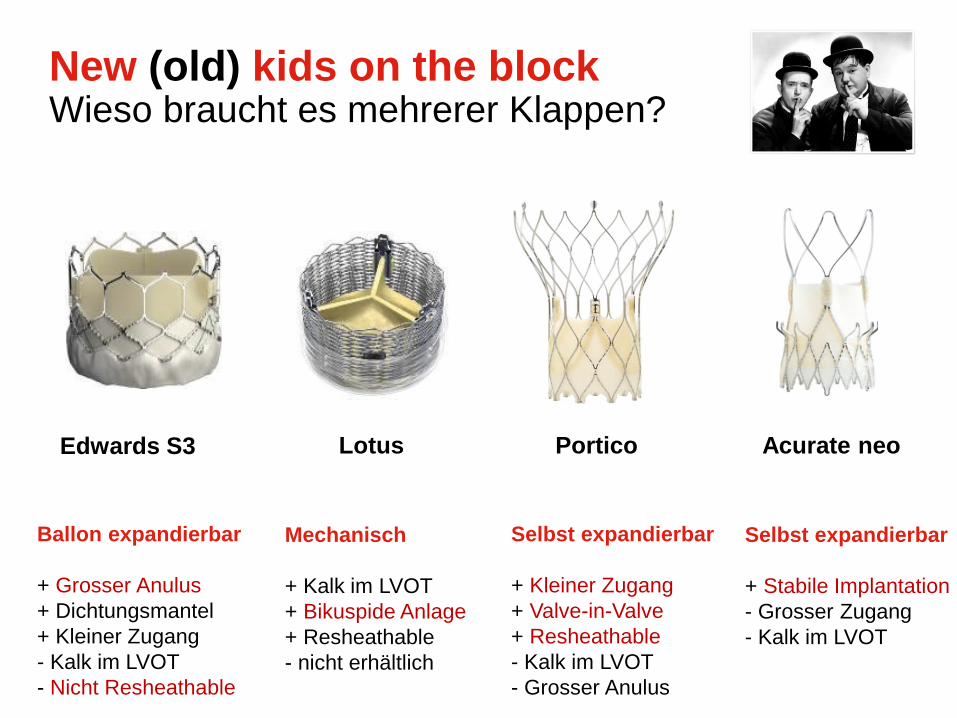
New (old) kids on the block Wieso braucht es mehrerer Klappen?
Edwards S3 Lotus Portico Acurate neo
Ballon expandierbar
+ Grosser Anulus
+ Dichtungsmantel
+ Kleiner Zugang
- Kalk im LVOT
- Nicht Resheathable
Mechanisch
+ Kalk im LVOT
+ Bikuspide Anlage
+ Resheathable
- nicht erhältlich
Selbst expandierbar
+ Kleiner Zugang
+ Valve-in-Valve
+ Resheathable
- Kalk im LVOT
- Grosser Anulus
Selbst expandierbar
+ Stabile Implantation
- Grosser Zugang
- Kalk im LVOT
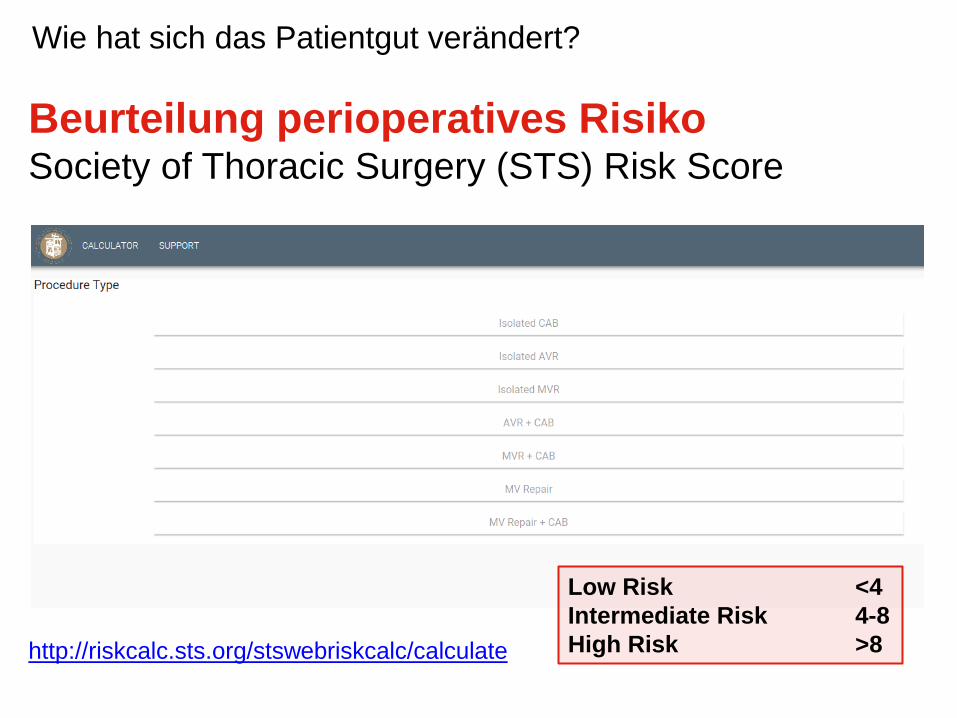
Beurteilung perioperatives Risiko Society of Thoracic Surgery (STS) Risk Score
http://riskcalc.sts.org/stswebriskcalc/calculate
Low Risk <4
Intermediate Risk 4-8
High Risk >8
Wie hat sich das Patientgut verändert?
• Age
• Sex
• Race
• Primary payor
• Weight/Height
• Hematocrit
• WBC count
• Platelet count
• Creatinine level
• Dialysis
• Hypertension
• Immuncompromise present
• POAD
• CVD
• Mediastinal radiation
• Cancer within 5 years
• Familiy history of premature CAD
• Sleep apnea
• Liver disease
• Unresponsive state
• Syncope
• Diabetes
• Endocarditis
• Chronic lung disease
• Illicit drug use
• Alcohol use
• Pneumonia
• Tobacco use
• Home oxygen
• Previous cardiac intervention
• Previous CABG
• Previous valve procedure
• Other previous cardiac interventions
• Previous PCI
• PCI performed within this episode of care
• PCI interval
• MI when
• Heart failure timing
• Classification NYHA
• Symptoms at time of this admission
• Cardiogenic shock
• Afibrillation
• Aflutter
• Third degree heart block
• Second degree heart block
• Sick sinus
• Vtach/Vfib
• Inotropic, intravenous
• ADP inhibitor (includes P2Y12)
• ADP inibitor discontinuation
• ACE or ARB
• Steroids
• Glycoprotein Iib/IIIa
• Resuscitation
• Number of diseased vessels
• Percent stenosis left main
• Ejection fraction
• Percent stenosis proximal LAD
• Aortic stenosis
• Mitral stenosis
• Aortic insufficiency
• Mitral insufficiency
• Tricuspid insufficiency
• AV disease etiology
• Incidence
• Status
• IABP insertion
• Catheter based assist device used
• ECMO
Beurteilung perioperatives Risiko Society of Thoracic Surgery (STS) Risk Score
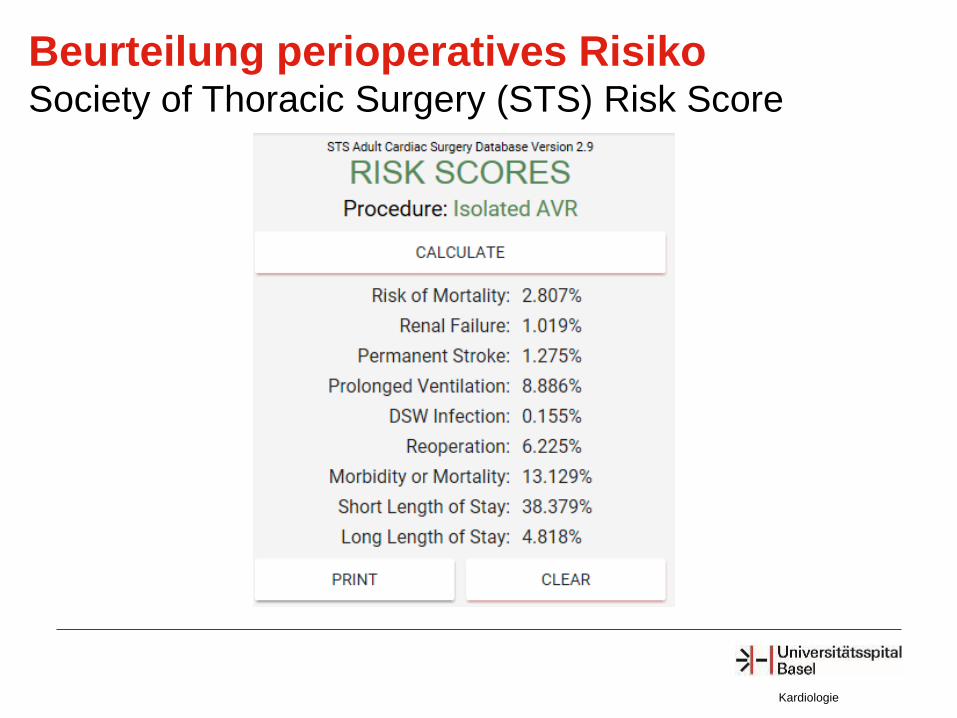
Kardiologie
Beurteilung perioperatives Risiko Society of Thoracic Surgery (STS) Risk Score
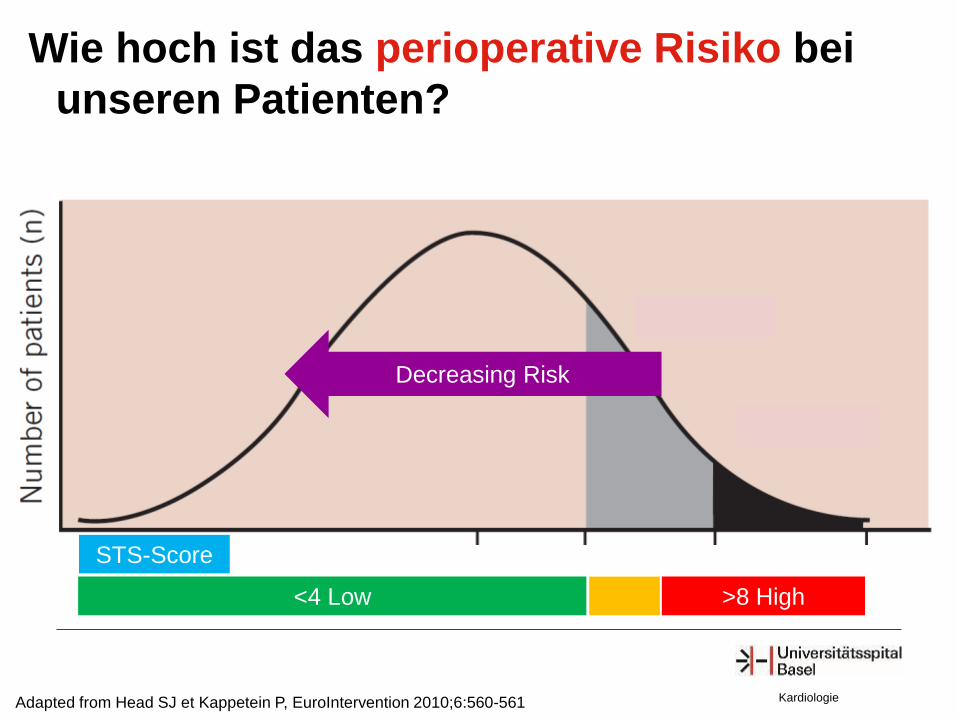
Adapted from Head SJ et Kappetein P, EuroIntervention 2010;6:560-561
Decreasing Risk
STS-Score
<4 Low >8 High
Kardiologie
Wie hoch ist das perioperative Risiko bei
unseren Patienten?
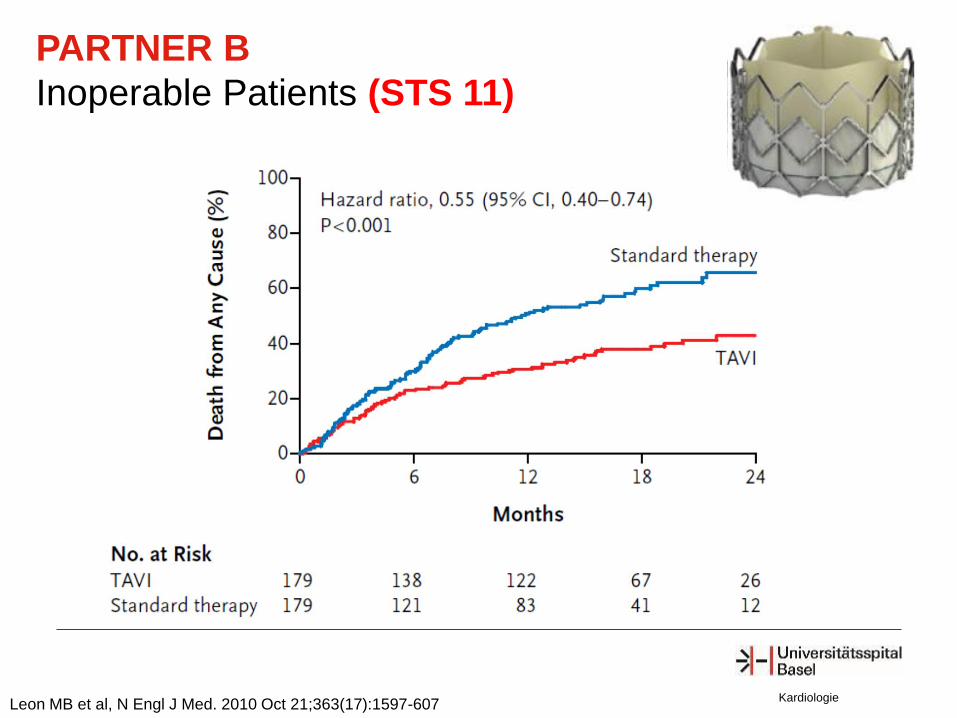
PARTNER B
Inoperable Patients (STS 11)
Leon MB et al, N Engl J Med. 2010 Oct 21;363(17):1597-607 Kardiologie
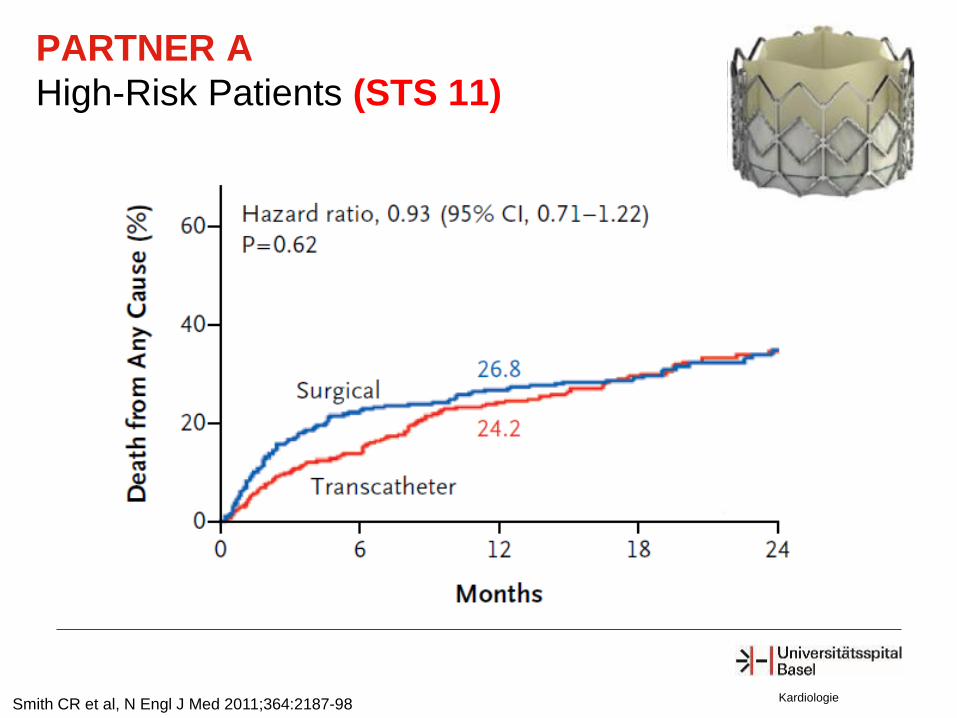
Smith CR et al, N Engl J Med 2011;364:2187-98
PARTNER A
High-Risk Patients (STS 11)
Kardiologie
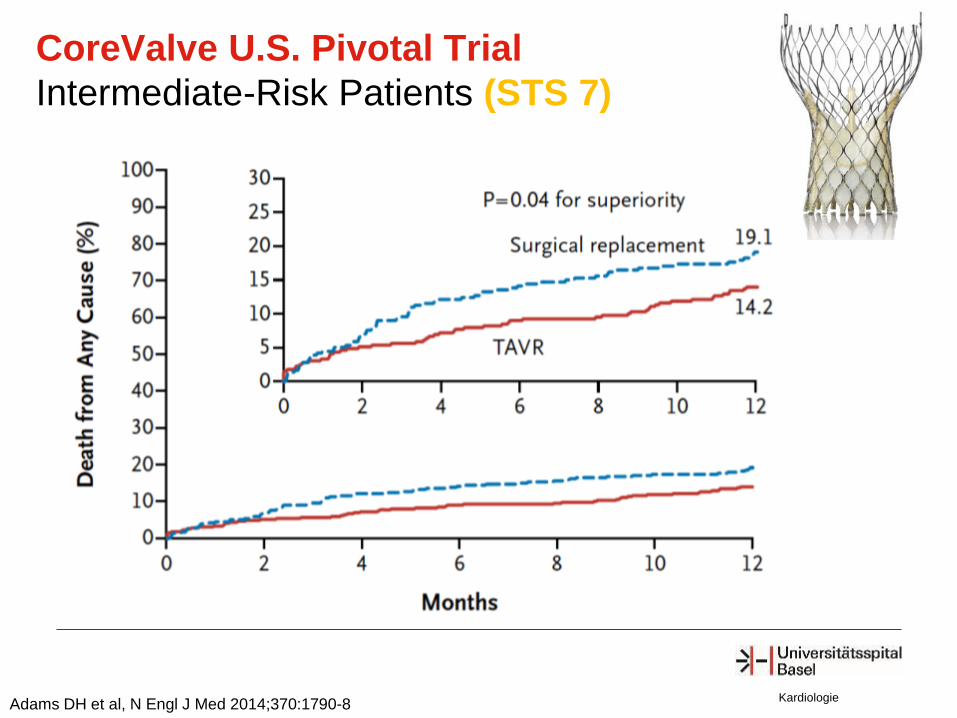
Adams DH et al, N Engl J Med 2014;370:1790-8
CoreValve U.S. Pivotal Trial
Intermediate-Risk Patients (STS 7)
Kardiologie
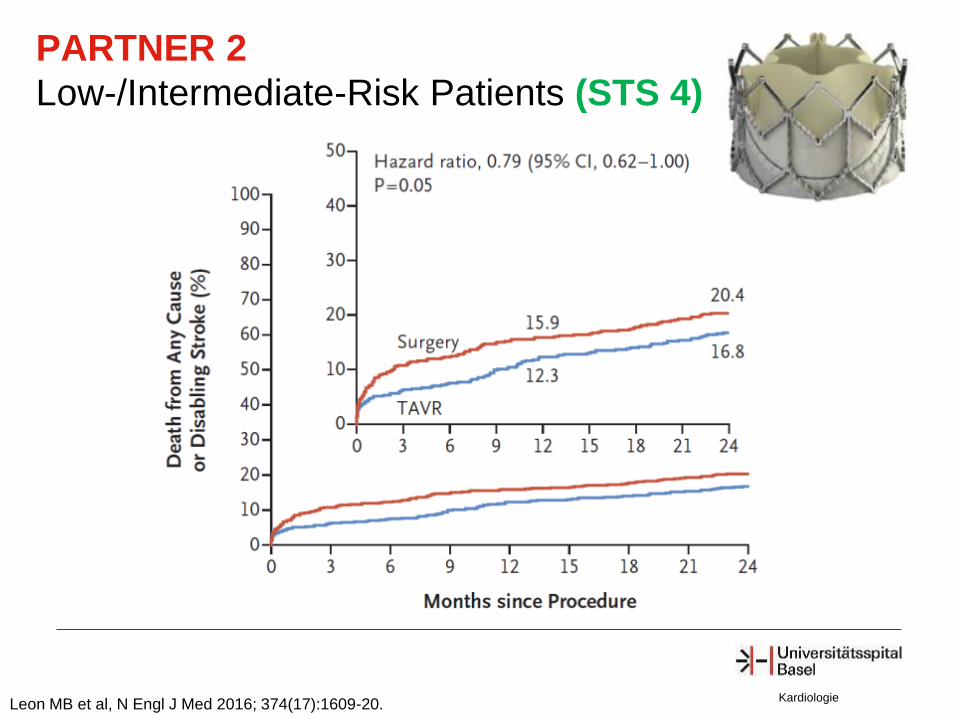
Leon MB et al, N Engl J Med 2016; 374(17):1609-20.
PARTNER 2
Low-/Intermediate-Risk Patients (STS 4)
Kardiologie
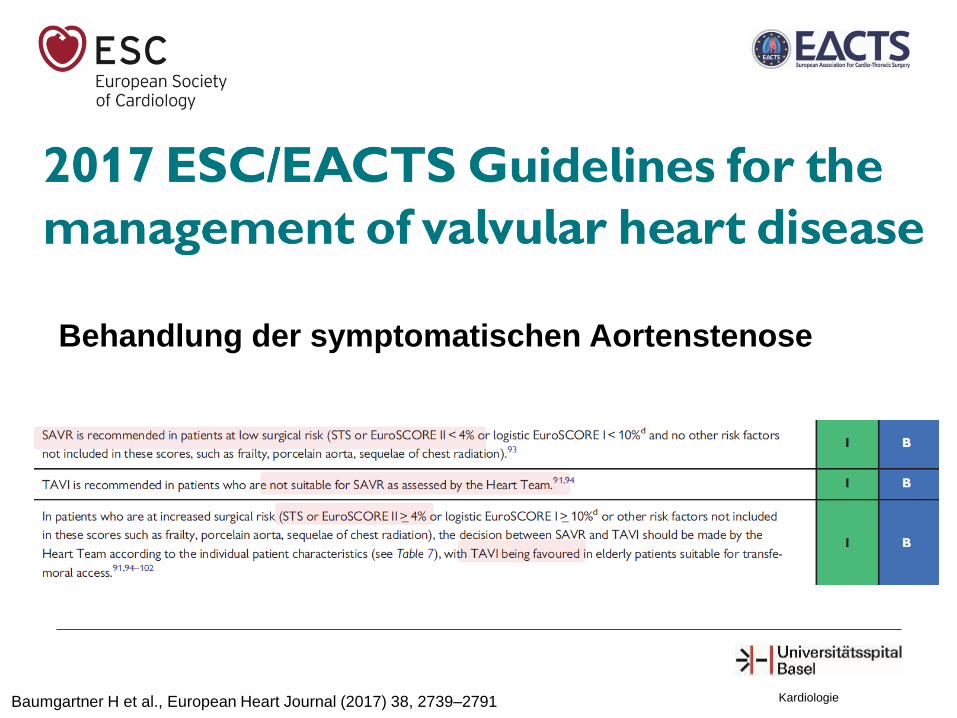
Baumgartner H et al., European Heart Journal (2017) 38, 2739–2791 Kardiologie
Behandlung der symptomatischen Aortenstenose
Popma JJ, New England Journal of Medicine 2019. Kardiologie
News - Interventional ACC March 17, 2019 - Meilenstein
Kardiologie
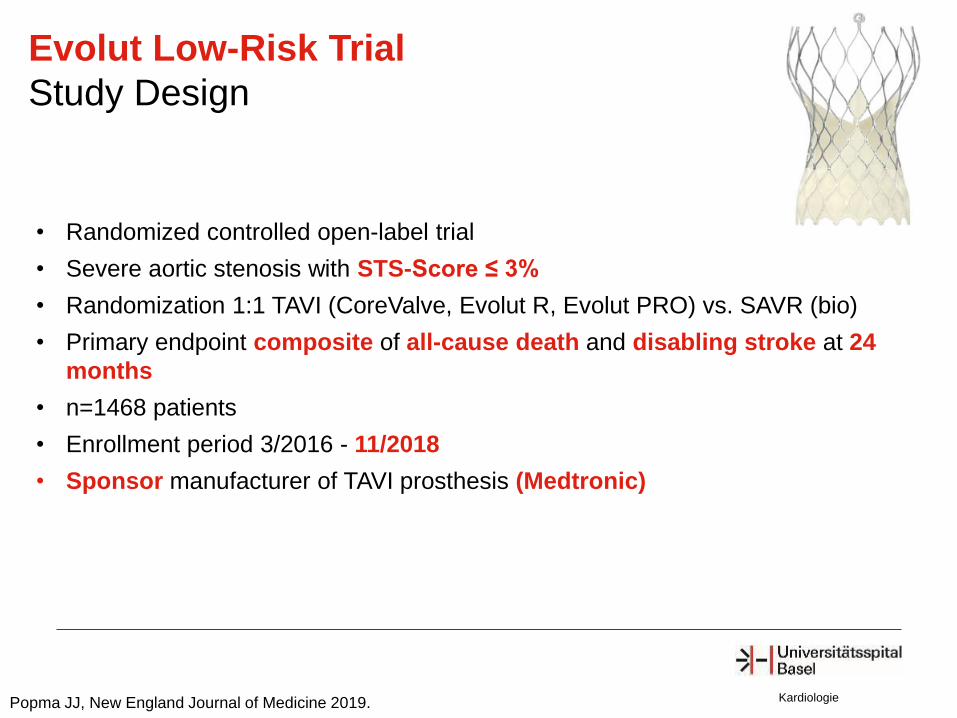
Evolut Low-Risk Trial
Study Design
• Randomized controlled open-label trial
• Severe aortic stenosis with STS-Score ≤ 3%
• Randomization 1:1 TAVI (CoreValve, Evolut R, Evolut PRO) vs. SAVR (bio)
• Primary endpoint composite of all-cause death and disabling stroke at 24
months
• n=1468 patients
• Enrollment period 3/2016 - 11/2018
• Sponsor manufacturer of TAVI prosthesis (Medtronic)
Popma JJ, New England Journal of Medicine 2019.
Kardiologie
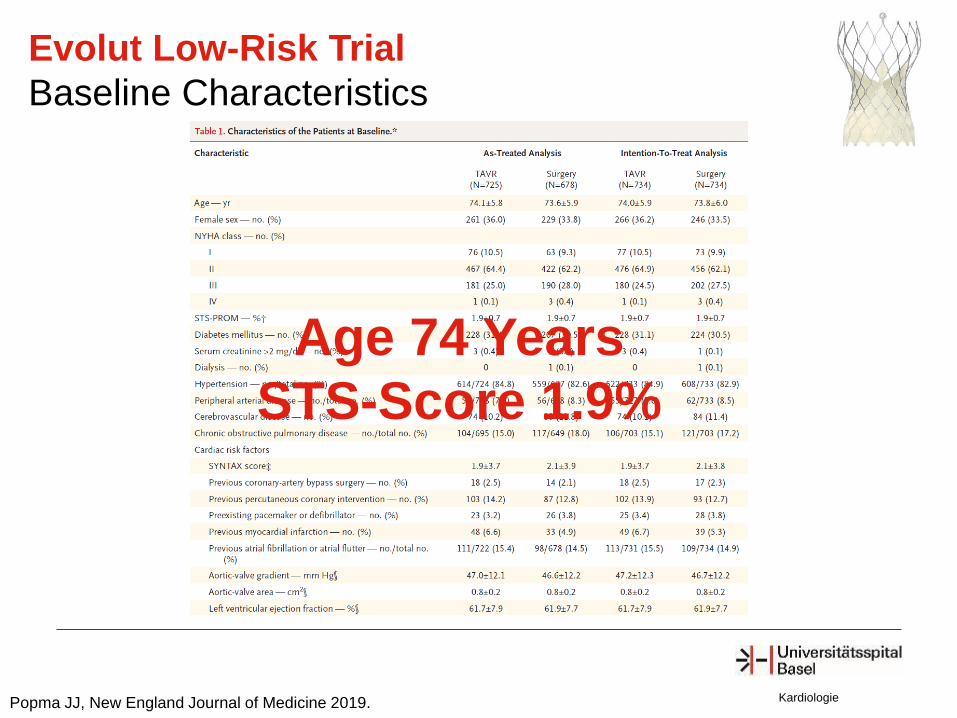
Evolut Low-Risk Trial
Baseline Characteristics
Popma JJ, New England Journal of Medicine 2019.
Age 74 Years
STS-Score 1.9%
Kardiologie
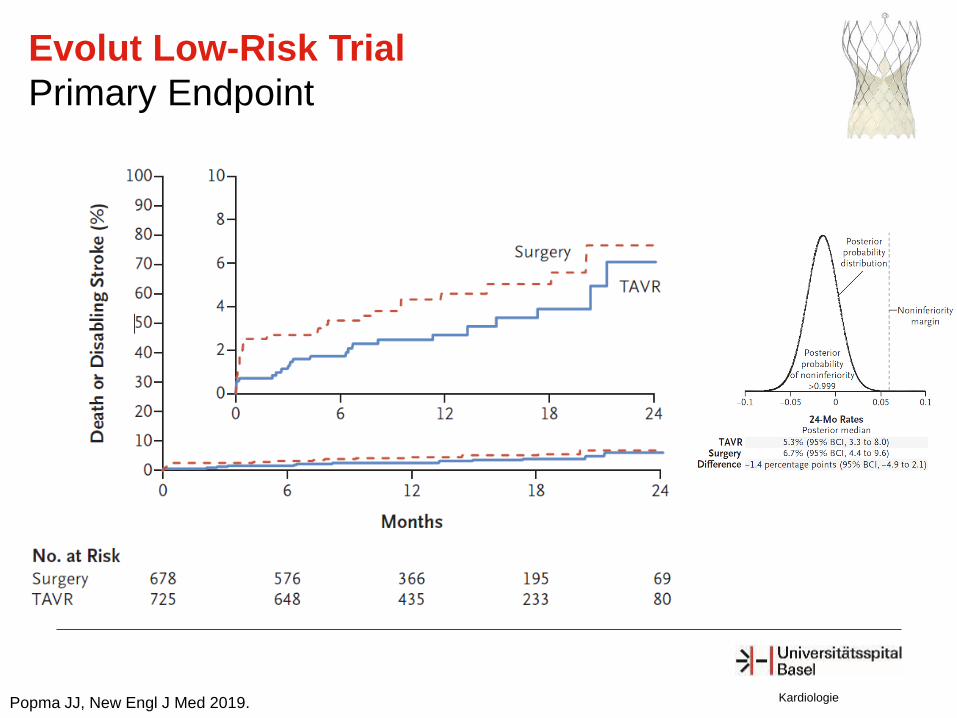
Evolut Low-Risk Trial
Primary Endpoint
Popma JJ, New Engl J Med 2019.
Kardiologie
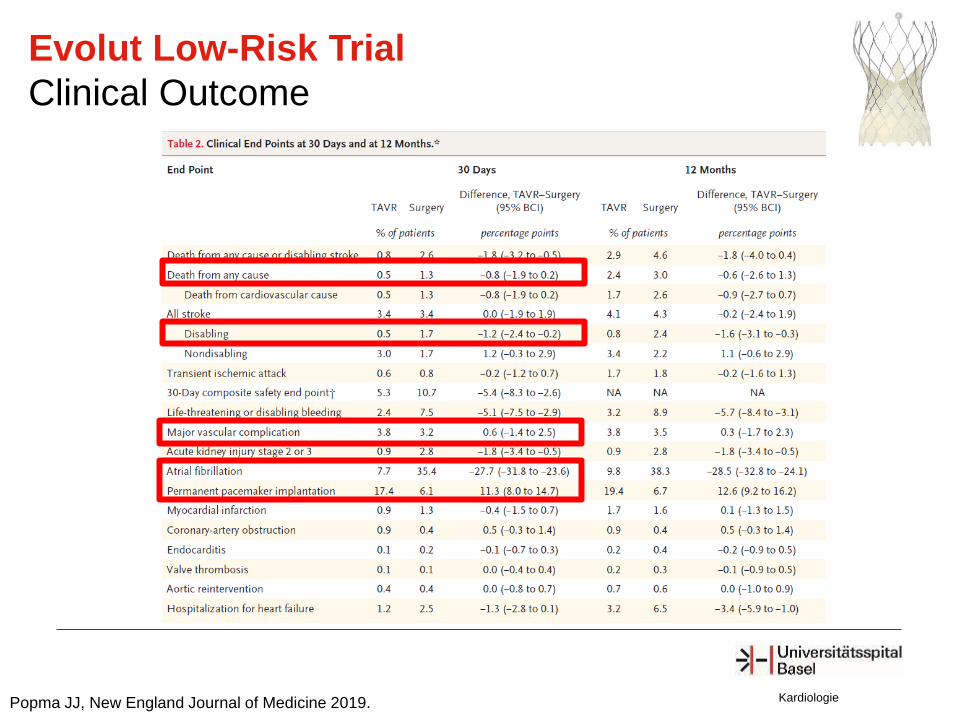
Evolut Low-Risk Trial
Clinical Outcome
Popma JJ, New England Journal of Medicine 2019.
Mack MJ, New Engl J Med 2019. Kardiologie
News - Interventional ACC March 17, 2019
Kardiologie
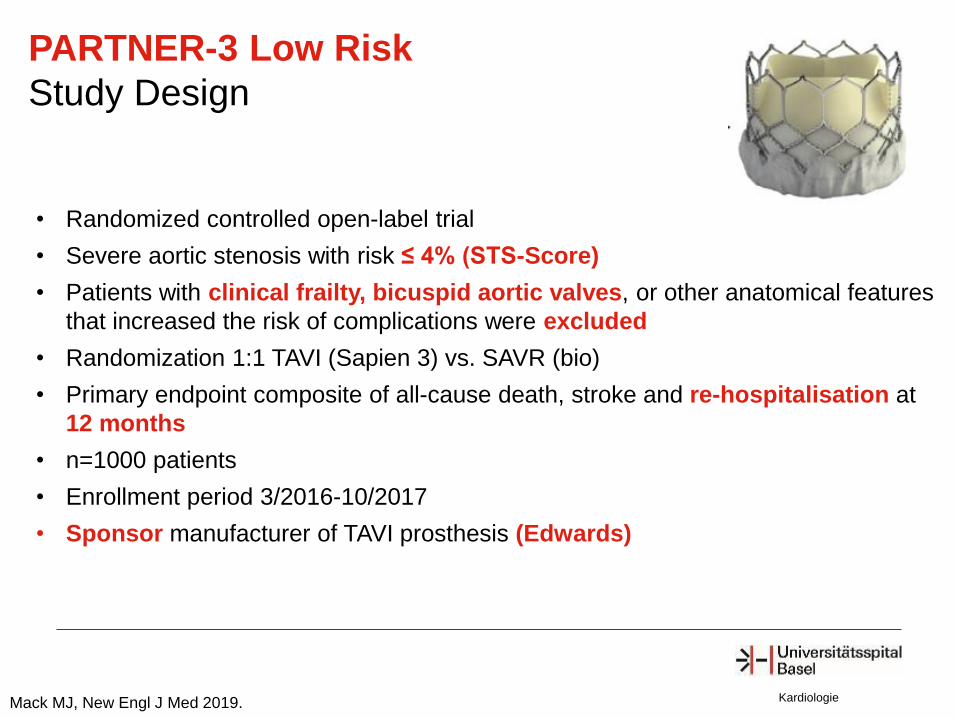
PARTNER-3 Low Risk
Study Design
• Randomized controlled open-label trial
• Severe aortic stenosis with risk ≤ 4% (STS-Score)
• Patients with clinical frailty, bicuspid aortic valves, or other anatomical features
that increased the risk of complications were excluded
• Randomization 1:1 TAVI (Sapien 3) vs. SAVR (bio)
• Primary endpoint composite of all-cause death, stroke and re-hospitalisation at
12 months
• n=1000 patients
• Enrollment period 3/2016-10/2017
• Sponsor manufacturer of TAVI prosthesis (Edwards)
Mack MJ, New Engl J Med 2019.
Kardiologie
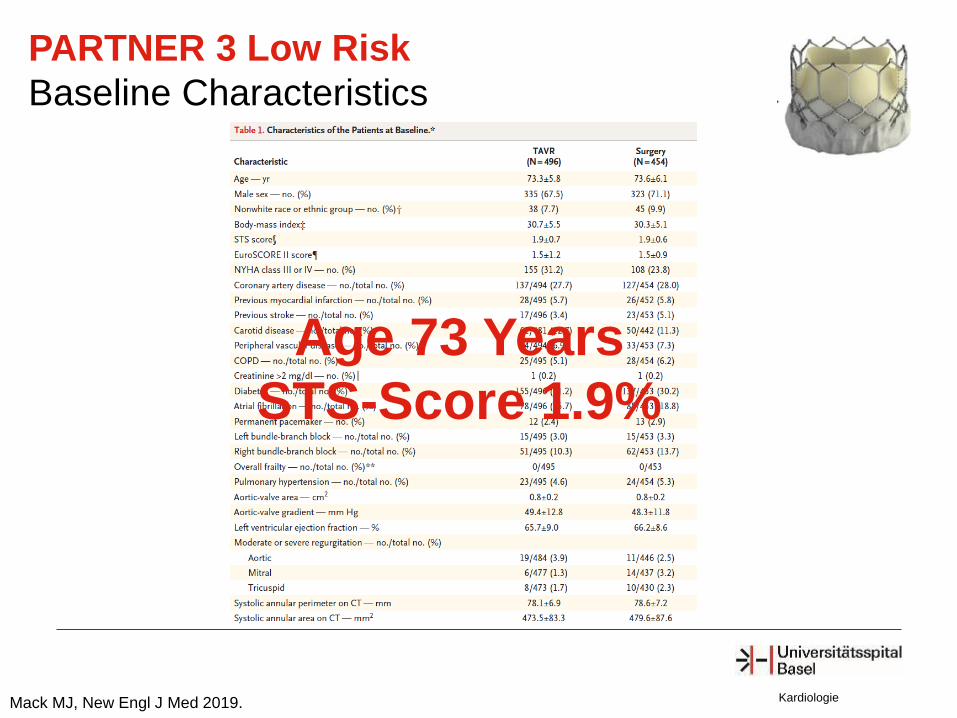
PARTNER 3 Low Risk
Baseline Characteristics
Mack MJ, New Engl J Med 2019.
Age 73 Years
STS-Score 1.9%
Kardiologie
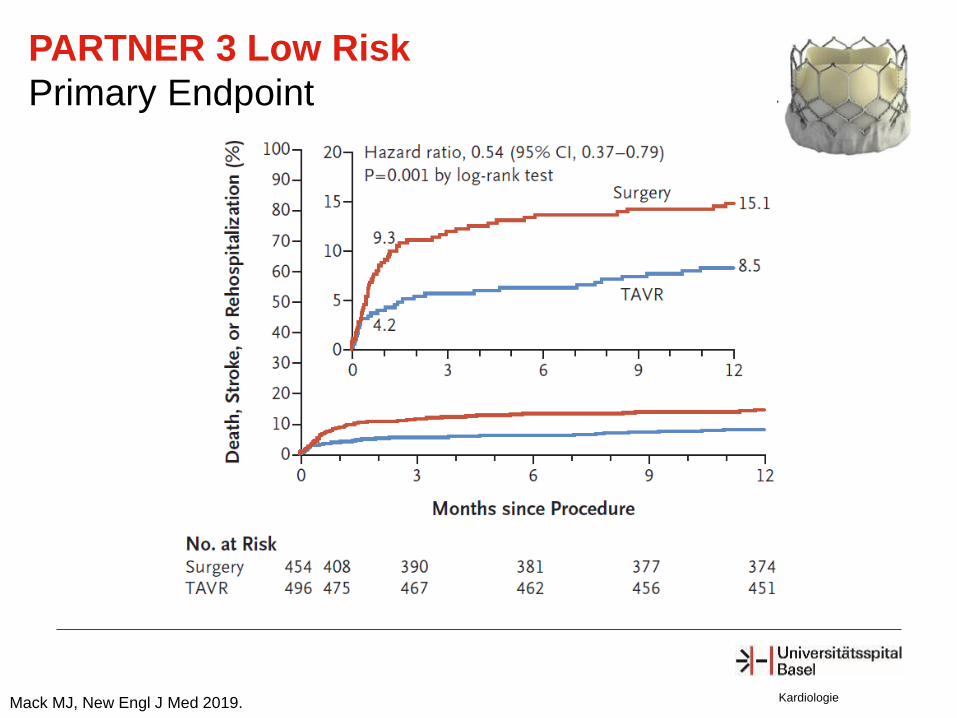
PARTNER 3 Low Risk
Primary Endpoint
Mack MJ, New Engl J Med 2019.
Kardiologie
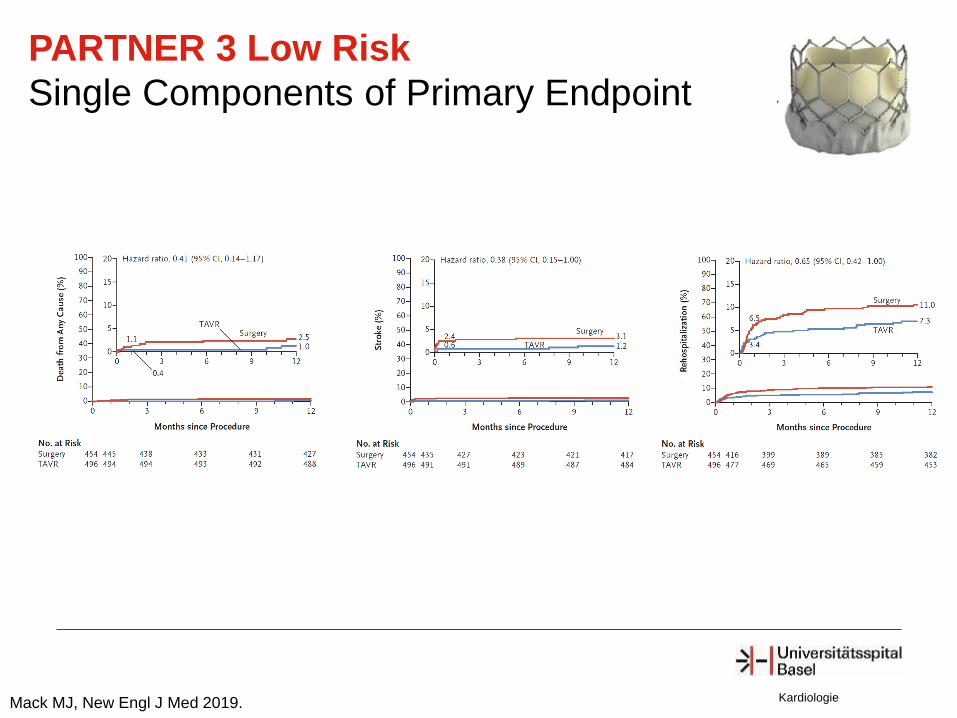
PARTNER 3 Low Risk
Single Components of Primary Endpoint
Mack MJ, New Engl J Med 2019.
Kardiologie
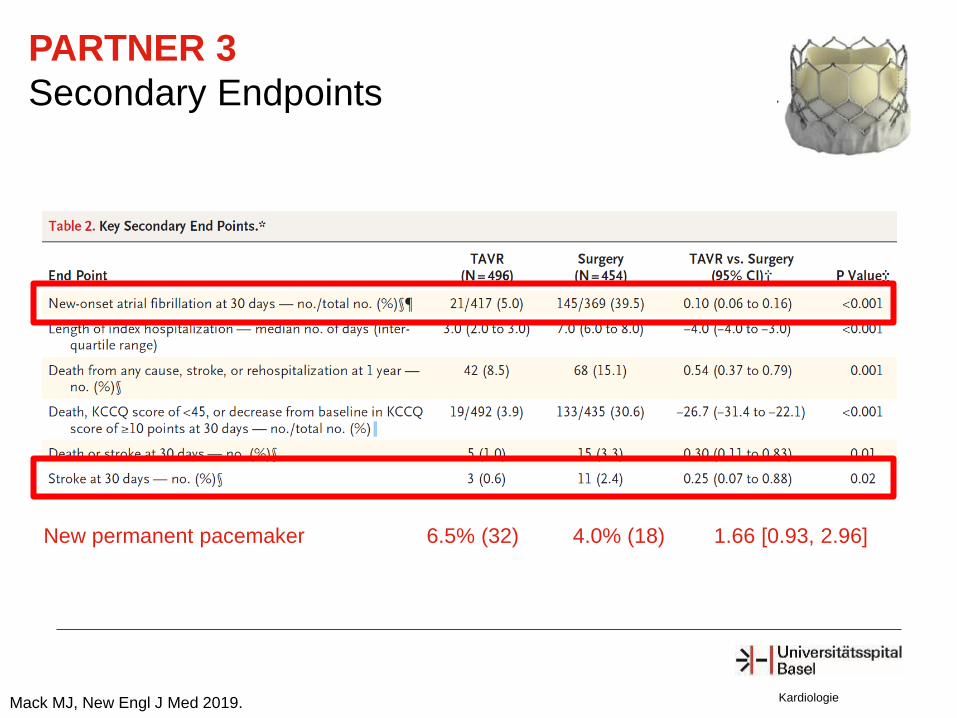
PARTNER 3
Secondary Endpoints
Mack MJ, New Engl J Med 2019.
New permanent pacemaker 6.5% (32) 4.0% (18) 1.66 [0.93, 2.96]
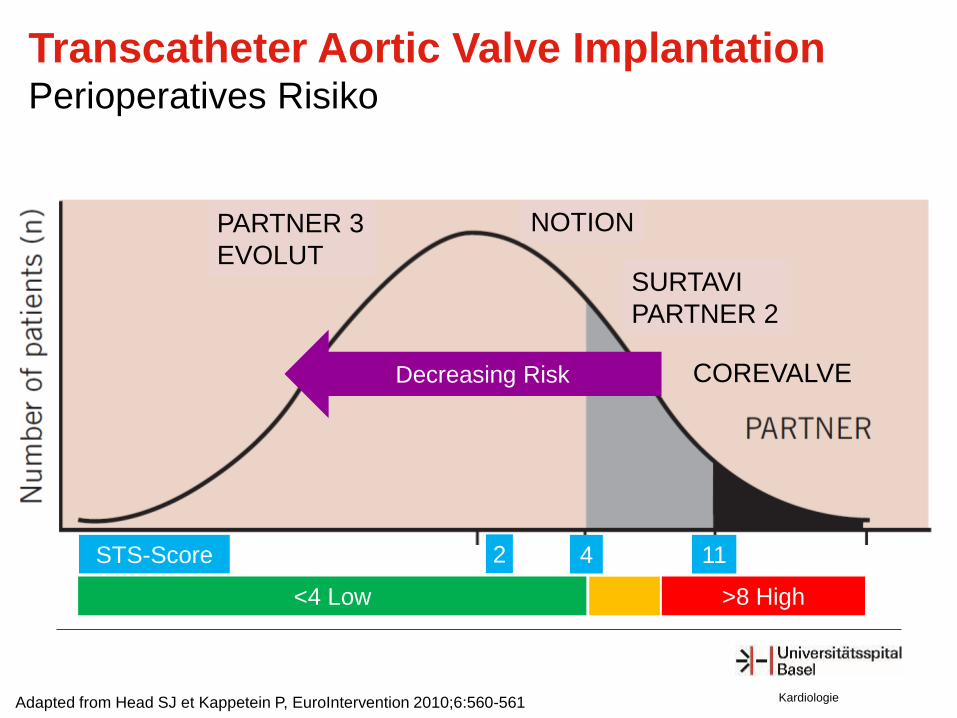
COREVALVE
Adapted from Head SJ et Kappetein P, EuroIntervention 2010;6:560-561
Decreasing Risk
STS-Score 4 11
SURTAVI
PARTNER 2
<4 Low >8 High
Kardiologie
NOTION
2
PARTNER 3
EVOLUT
Transcatheter Aortic Valve Implantation Perioperatives Risiko
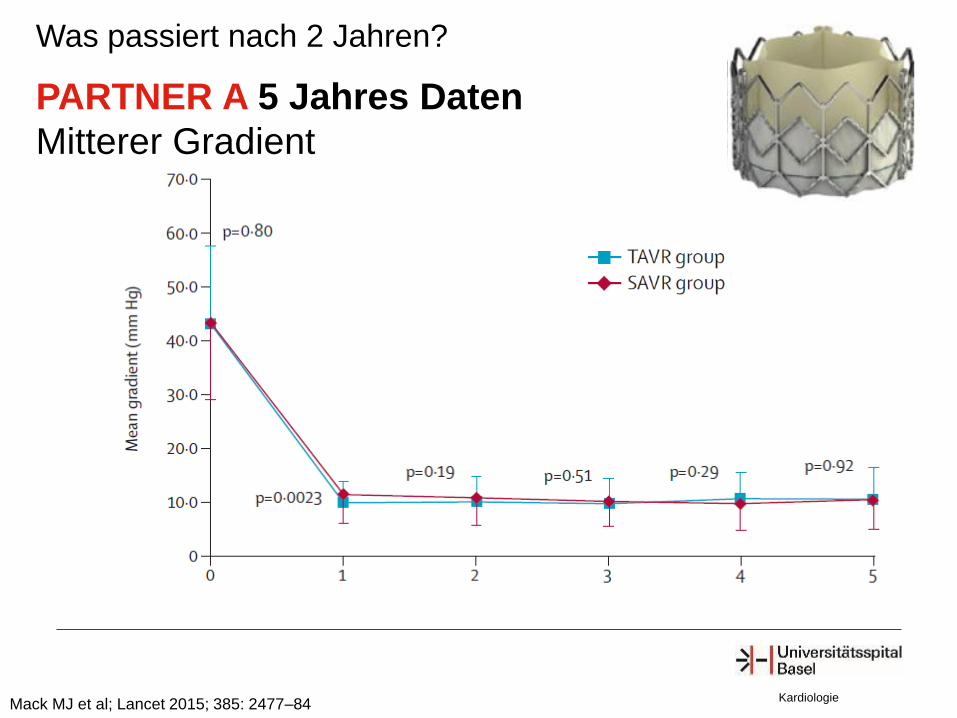
PARTNER A 5 Jahres Daten
Mitterer Gradient
Mack MJ et al; Lancet 2015; 385: 2477–84 Kardiologie
Was passiert nach 2 Jahren?
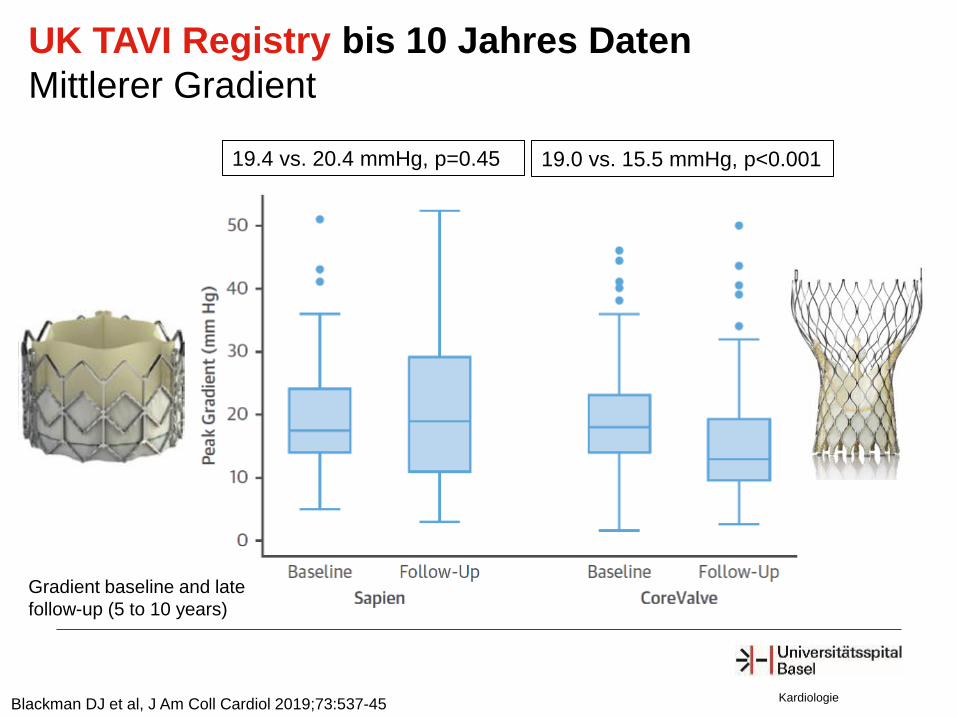
UK TAVI Registry bis 10 Jahres Daten
Mittlerer Gradient
Kardiologie Blackman DJ et al, J Am Coll Cardiol 2019;73:537-45
19.4 vs. 20.4 mmHg, p=0.45 19.0 vs. 15.5 mmHg, p<0.001
Gradient baseline and late
follow-up (5 to 10 years)

CAVE für TAVI Welche Anatomie ist weniger geeignet?
Bikuspide
Aortenklappe Typisch jüngre Patienten
Kalksporn
im LVOT

5. April 2019