Embed Size (px)
Citation preview

Therapie
Fallbeispiele
Christian Muschitz
II. Med. Abteilung – KH Barmherzige Schwestern Wien
Medizinische Universität Wien
Agenda 2016
Medikamentöse Behandlung:
• Vitamin D ± Kalzium
• Antikatabole Therapie: Bisphosphonate, Denosumab
• Anabole Therapie: rhPTH 1-34
Mythen & Fakten zu MRONJ, AFF
Therapiealgorithmus
Beispiele
C. Muschitz Zicksee 2016
Vitamin D
Kalzium
C. Muschitz Zicksee 2016
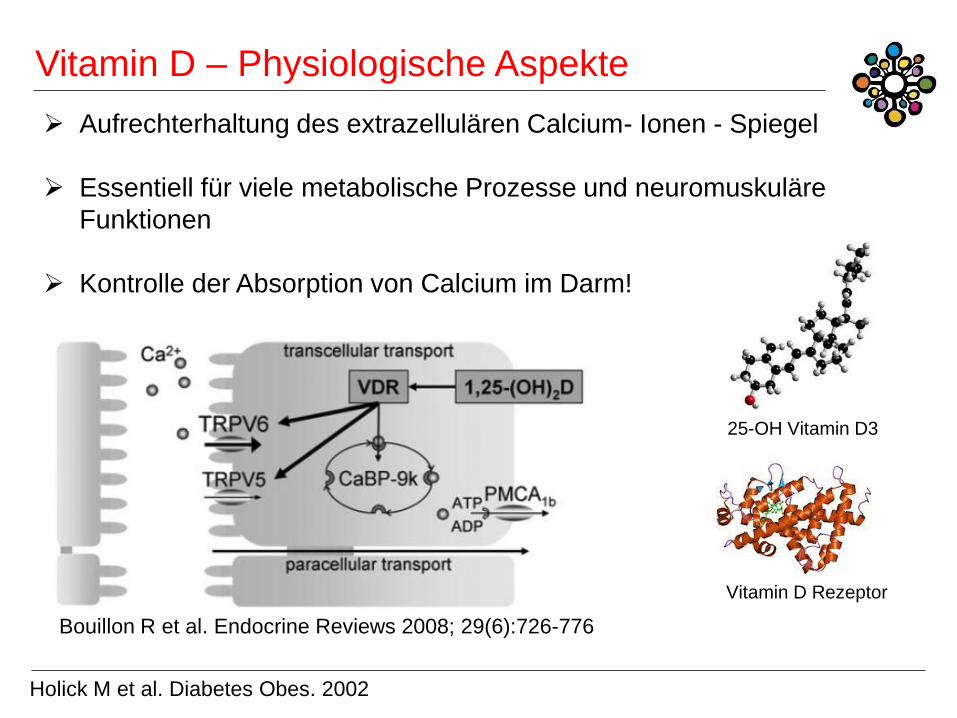
Vitamin D – Physiologische Aspekte
Aufrechterhaltung des extrazellulären Calcium- Ionen - Spiegel
Essentiell für viele metabolische Prozesse und neuromuskuläre
Funktionen
Kontrolle der Absorption von Calcium im Darm!
Bouillon R et al. Endocrine Reviews 2008; 29(6):726-776
Holick M et al. Diabetes Obes. 2002
25-OH Vitamin D3
Vitamin D Rezeptor
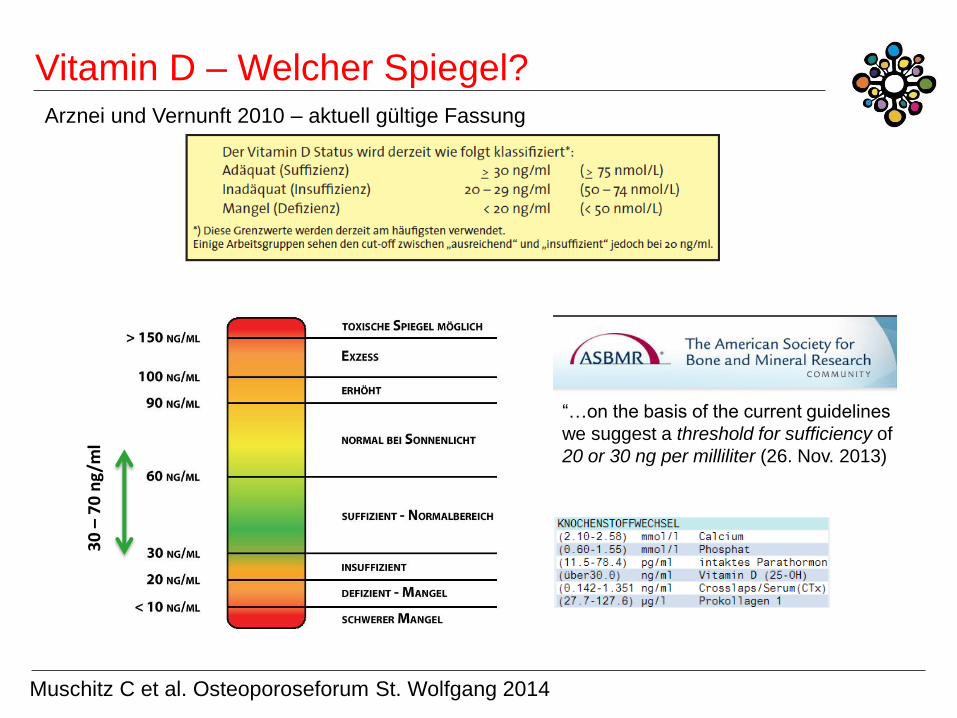
Vitamin D – Welcher Spiegel? Arznei und Vernunft 2010 – aktuell gültige Fassung
30
– 7
0 n
g/m
l
“…on the basis of the current guidelines
we suggest a threshold for sufficiency of
20 or 30 ng per milliliter (26. Nov. 2013)
Muschitz C et al. Osteoporoseforum St. Wolfgang 2014
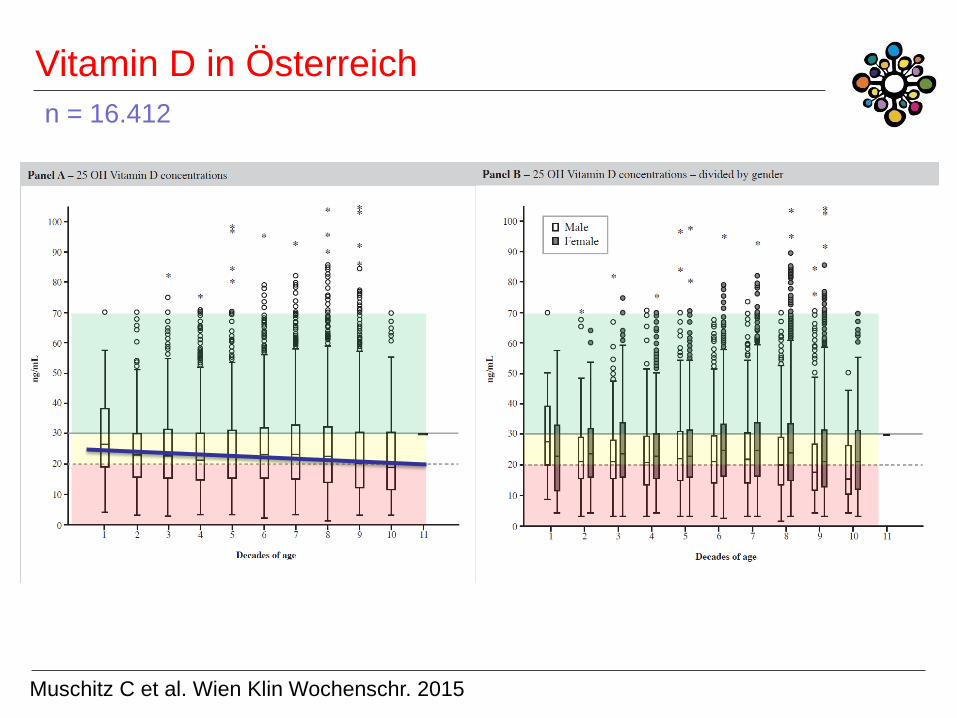
Vitamin D in Österreich
n = 16.412
Muschitz C et al. Wien Klin Wochenschr. 2015
Antikatabole Therapie:
Bisphosphonate,
Denosumab
C. Muschitz Zicksee 2016
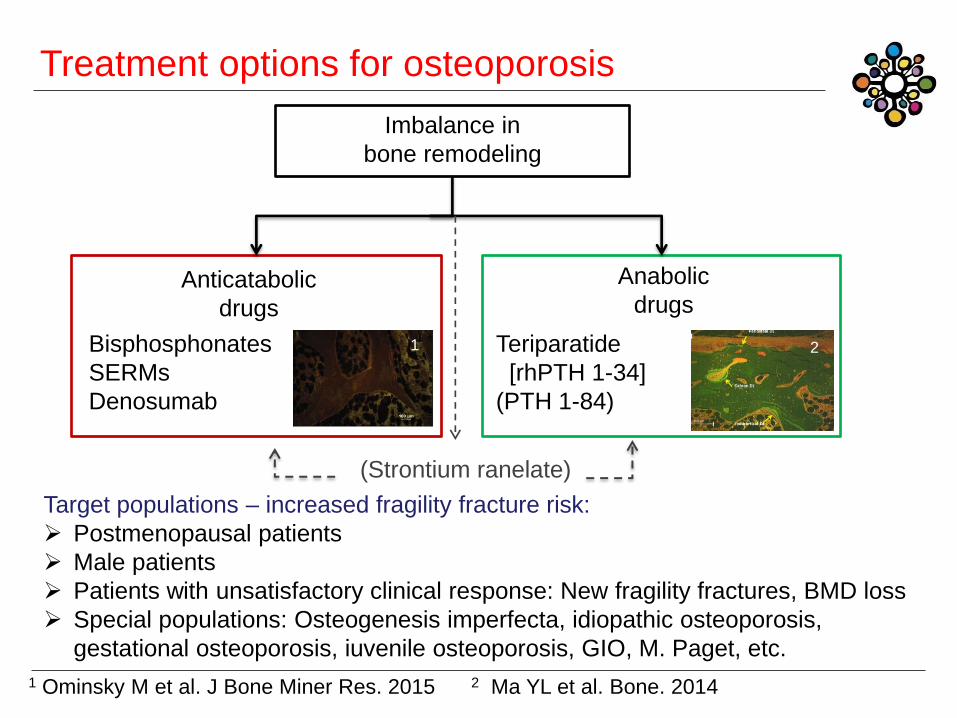
Treatment options for osteoporosis
Imbalance in
bone remodeling
Anticatabolic
drugs
Anabolic
drugs
Bisphosphonates
SERMs
Denosumab
Teriparatide
[rhPTH 1-34]
(PTH 1-84)
Target populations – increased fragility fracture risk:
Postmenopausal patients
Male patients
Patients with unsatisfactory clinical response: New fragility fractures, BMD loss
Special populations: Osteogenesis imperfecta, idiopathic osteoporosis,
gestational osteoporosis, iuvenile osteoporosis, GIO, M. Paget, etc.
1 Ominsky M et al. J Bone Miner Res. 2015 2 Ma YL et al. Bone. 2014
1 2
(Strontium ranelate)
1
0
1
2
3
4
5
6
10 15 20 25 30 FR
EQ
UE
NC
Y [
% B
.Ar]
CALCIUM CONCENTRATION [WEIGHT %]
0
1
2
3
4
5
6
10 15 20 25 30 CALCIUM CONCENTRATION [WEIGHT %]
FR
EQ
UE
NC
Y [
% B
.Ar]
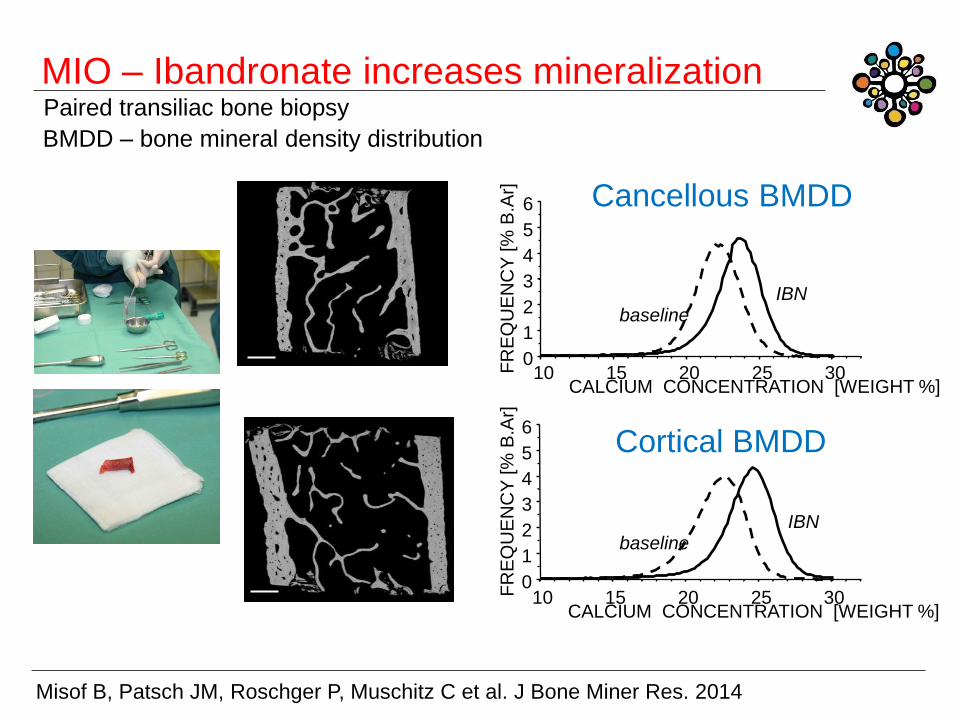
Cancellous BMDD
Cortical BMDD
baseline IBN
baseline IBN
MIO – Ibandronate increases mineralization
Misof B, Patsch JM, Roschger P, Muschitz C et al. J Bone Miner Res. 2014
Paired transiliac bone biopsy
BMDD – bone mineral density distribution
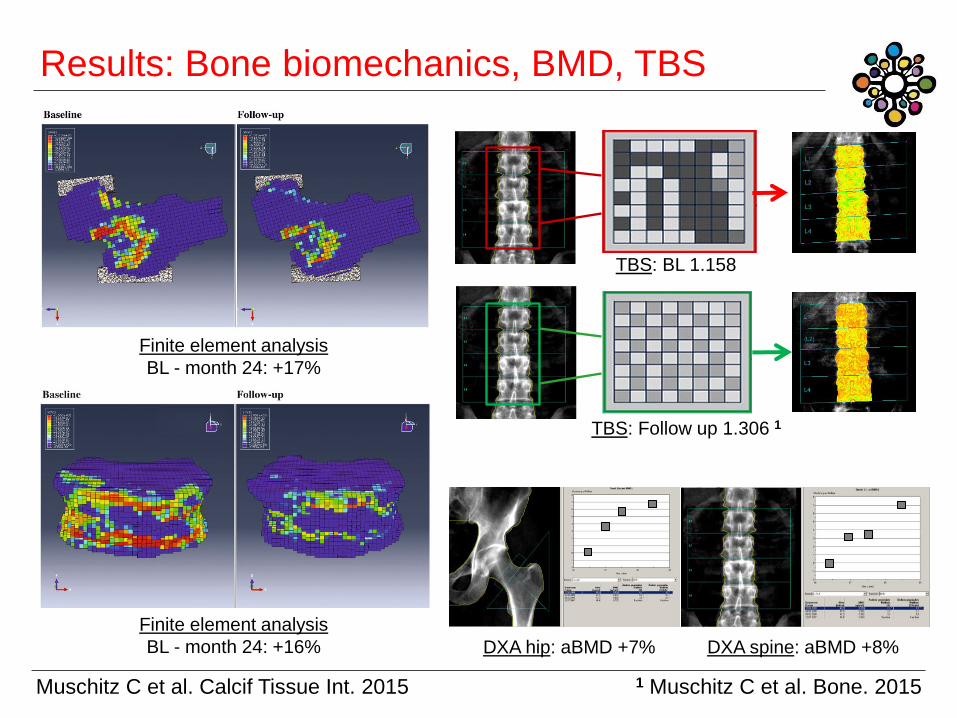
Results: Bone biomechanics, BMD, TBS
Muschitz C et al. Calcif Tissue Int. 2015
TBS: BL 1.158
TBS: Follow up 1.306 1
Finite element analysis
BL - month 24: +16% DXA hip: aBMD +7%
Finite element analysis
BL - month 24: +17%
DXA spine: aBMD +8%
1 Muschitz C et al. Bone. 2015
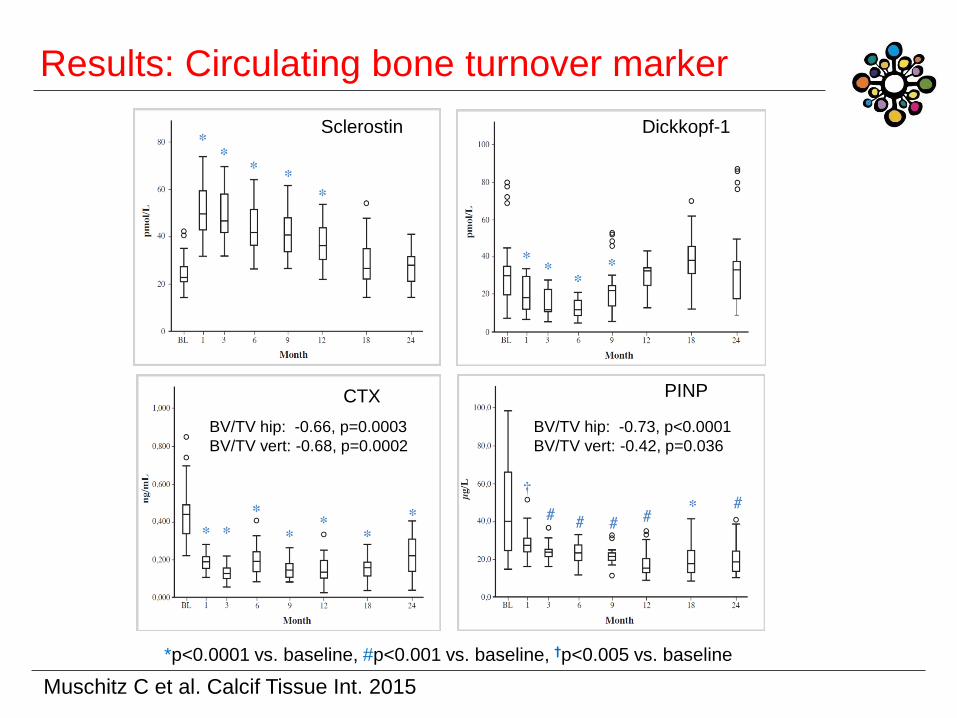
Results: Circulating bone turnover marker
Muschitz C et al. Calcif Tissue Int. 2015
*p<0.0001 vs. baseline, #p<0.001 vs. baseline, †p<0.005 vs. baseline
Sclerostin Dickkopf-1
CTX PINP
BV/TV hip: -0.66, p=0.0003
BV/TV vert: -0.68, p=0.0002
BV/TV hip: -0.73, p<0.0001
BV/TV vert: -0.42, p=0.036
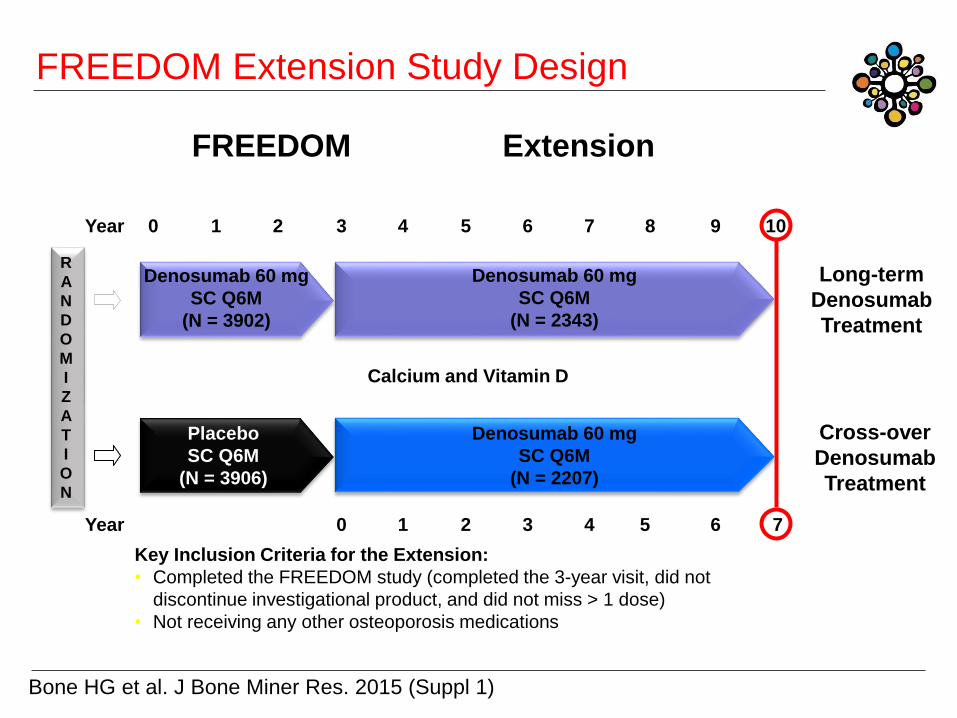
Key Inclusion Criteria for the Extension:
• Completed the FREEDOM study (completed the 3-year visit, did not
discontinue investigational product, and did not miss > 1 dose)
• Not receiving any other osteoporosis medications
FREEDOM Extension
1 2 3 Year 0 5 6 7 4 8 9 10
1 2 3 0 6 7 4 Year
R
A
N
D
O
M
I
Z
A
T
I
O
N
Denosumab 60 mg
SC Q6M
(N = 3902)
Placebo
SC Q6M
(N = 3906)
Long-term
Denosumab
Treatment
Cross-over
Denosumab
Treatment
Denosumab 60 mg
SC Q6M
(N = 2343)
Denosumab 60 mg
SC Q6M
(N = 2207)
Calcium and Vitamin D
FREEDOM Extension Study Design
5
Bone HG et al. J Bone Miner Res. 2015 (Suppl 1)
-2
0
2
4
6
8
10
12
14
16
18
20
22
24
0 1 2 3 4 5 6 7 8 9 10
Pe
rce
nt
Ch
an
ge
fro
m B
as
eli
ne
Study Year
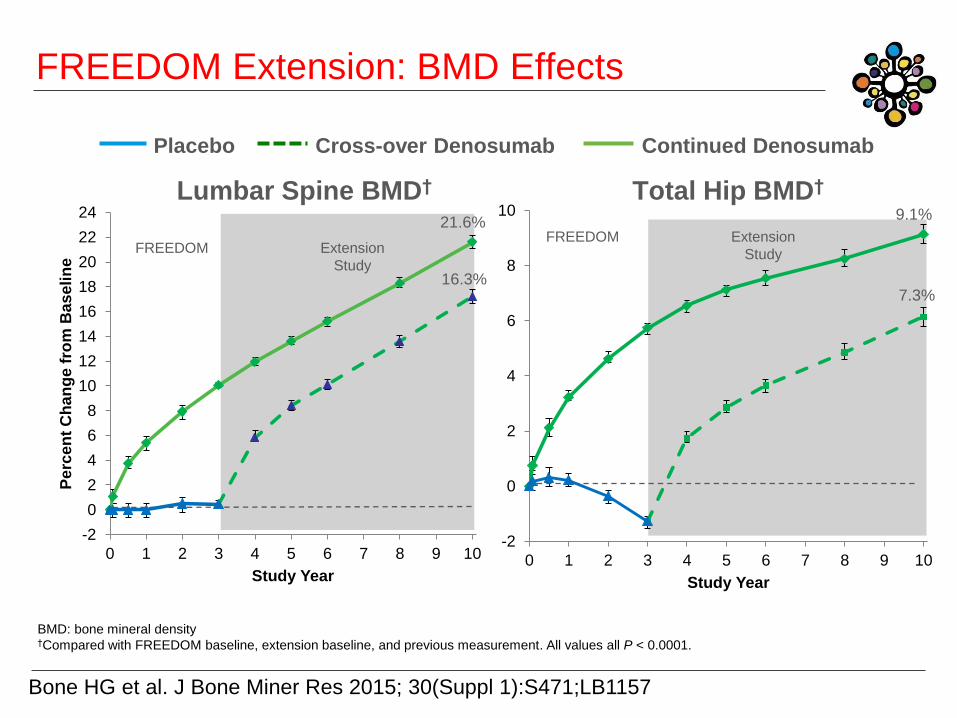
Placebo Continued Denosumab Cross-over Denosumab
Lumbar Spine BMD† Total Hip BMD†
Bone HG et al. J Bone Miner Res 2015; 30(Suppl 1):S471;LB1157
BMD: bone mineral density
†Compared with FREEDOM baseline, extension baseline, and previous measurement. All values all P < 0.0001.
-2
0
2
4
6
8
10
0 1 2 3 4 5 6 7 8 9 10
Study Year
FREEDOM Extension
Study
FREEDOM Extension
Study
21.6%
16.3% 7.3%
9.1%
FREEDOM Extension: BMD Effects
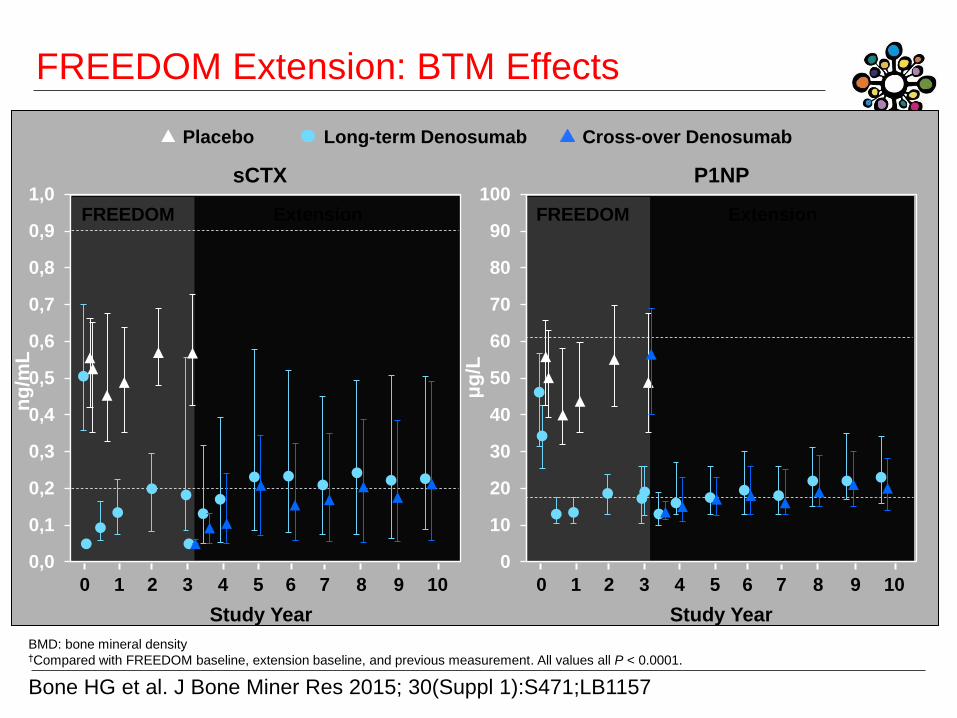
Bone HG et al. J Bone Miner Res 2015; 30(Suppl 1):S471;LB1157
BMD: bone mineral density
†Compared with FREEDOM baseline, extension baseline, and previous measurement. All values all P < 0.0001.
FREEDOM Extension: BTM Effects
Extension FREEDOM
0
10
20
30
40
50
60
70
80
90
100Extension FREEDOM
0,0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1,0
Placebo Cross-over Denosumab Long-term Denosumab
sCTX P1NP
ng
/mL
0 1 2 3 4 5 6 7 8 9 10
Study Year Study Year
0 1 2 3 4 5 6 7 8 9 10
μg
/L
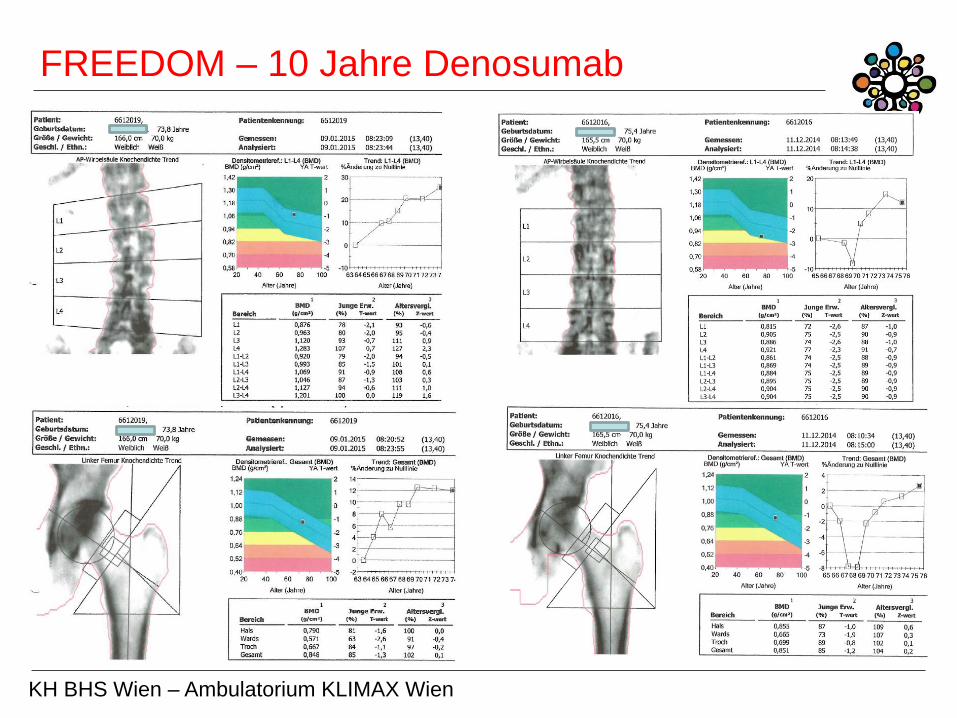
FREEDOM – 10 Jahre Denosumab
KH BHS Wien – Ambulatorium KLIMAX Wien
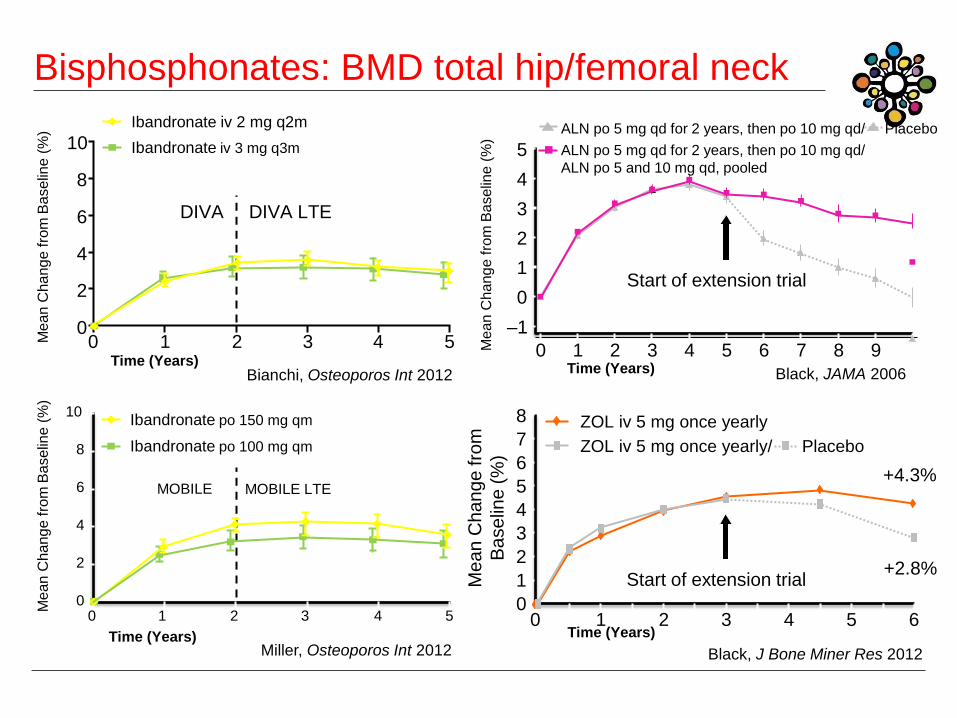
Bianchi, Osteoporos Int 2012
0
2
4
6
8
10
0 1 2 3 4 5
DIVA DIVA LTE
Ibandronate iv 2 mg q2m
Ibandronate iv 3 mg q3m
Time (Years)
Me
an
Cha
ng
e f
rom
Ba
selin
e (
%)
–1
0
1
2
3
4
5
0 1 2 3 4 5 6 7 8 9 Time (Years)
Me
an
Cha
ng
e f
rom
Ba
selin
e (
%)
Start of extension trial
ALN po 5 mg qd for 2 years, then po 10 mg qd/ Placebo
ALN po 5 mg qd for 2 years, then po 10 mg qd/
ALN po 5 and 10 mg qd, pooled
Black, JAMA 2006
Miller, Osteoporos Int 2012
Me
an
Cha
ng
e f
rom
Ba
selin
e (
%)
0
2
4
6
8
10
0 1 2 3 4 5
Time (Years)
MOBILE MOBILE LTE
Ibandronate po 150 mg qm
Ibandronate po 100 mg qm
Start of extension trial
0
1
2
3
4
5
6
7
8
0 1 2 3 4 5 6 Time (Years)
+4.3%
+2.8%
ZOL iv 5 mg once yearly
ZOL iv 5 mg once yearly/ Placebo
Me
an
Ch
an
ge
fro
m
Ba
se
line
(%
)
Black, J Bone Miner Res 2012
Bisphosphonates: BMD total hip/femoral neck
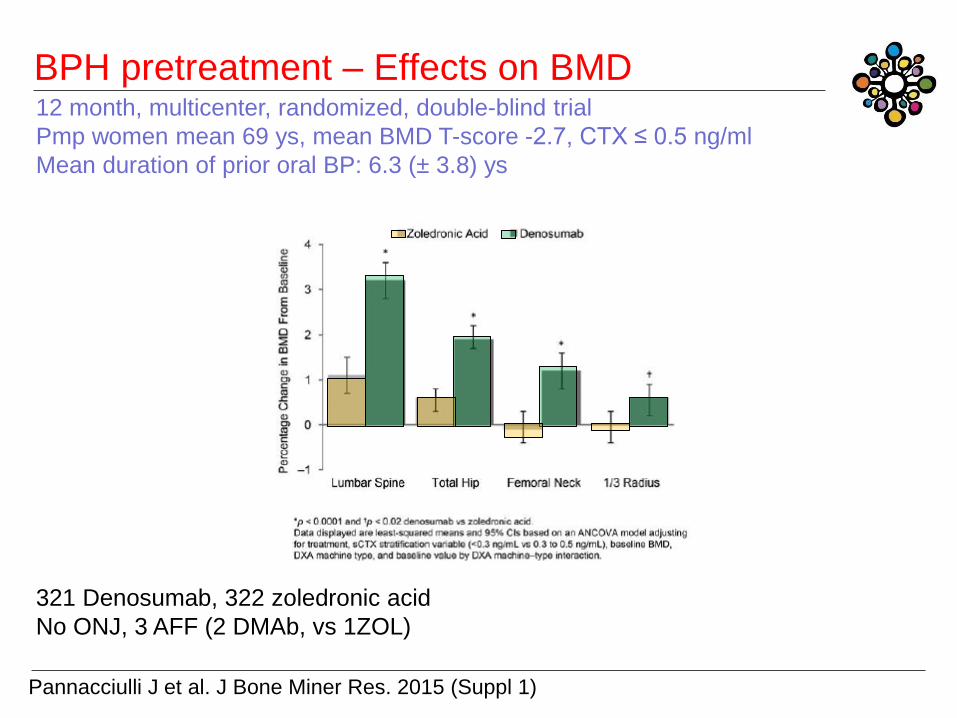
BPH pretreatment – Effects on BMD
Pannacciulli J et al. J Bone Miner Res. 2015 (Suppl 1)
12 month, multicenter, randomized, double-blind trial
Pmp women mean 69 ys, mean BMD T-score -2.7, CTX ≤ 0.5 ng/ml
Mean duration of prior oral BP: 6.3 (± 3.8) ys
321 Denosumab, 322 zoledronic acid
No ONJ, 3 AFF (2 DMAb, vs 1ZOL)

Anabole Therapie mit
rhPTH 1-34 - Teriparatid
C. Muschitz Zicksee 2016
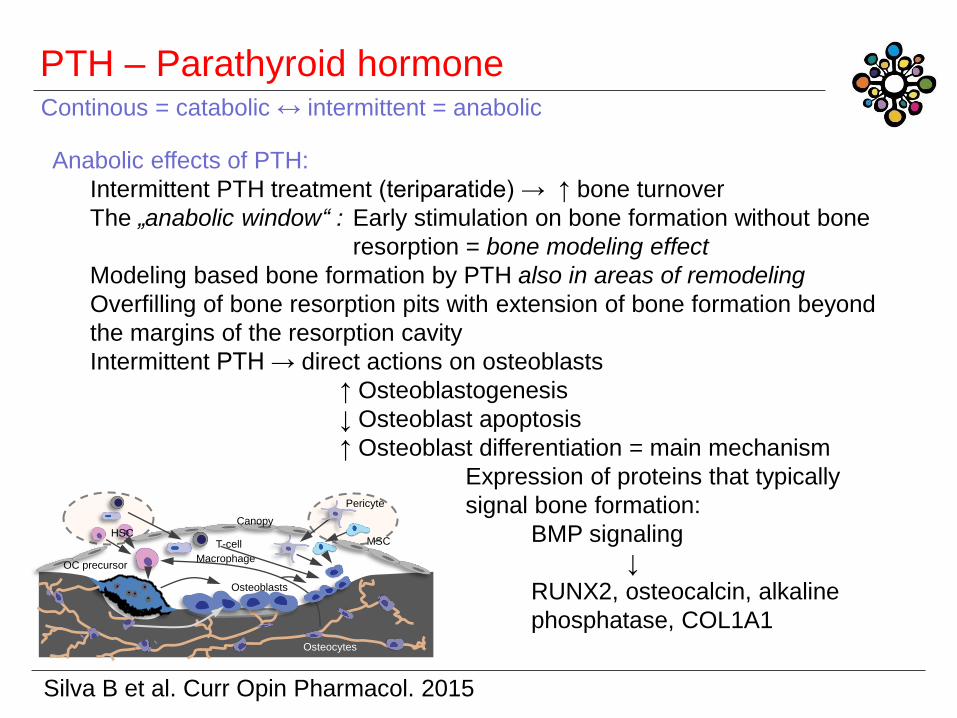
PTH – Parathyroid hormone
MSC HSC
Pericyte
Canopy
Macrophage
T-cell
Osteoblasts
OC precursor
Osteocytes
Silva B et al. Curr Opin Pharmacol. 2015
Continous = catabolic ↔ intermittent = anabolic
Anabolic effects of PTH:
Intermittent PTH treatment (teriparatide) → ↑ bone turnover
The „anabolic window“ : Early stimulation on bone formation without bone
resorption = bone modeling effect
Modeling based bone formation by PTH also in areas of remodeling
Overfilling of bone resorption pits with extension of bone formation beyond
the margins of the resorption cavity
Intermittent PTH → direct actions on osteoblasts
↑ Osteoblastogenesis
↓ Osteoblast apoptosis
↑ Osteoblast differentiation = main mechanism
Expression of proteins that typically
signal bone formation:
BMP signaling
↓
RUNX2, osteocalcin, alkaline
phosphatase, COL1A1
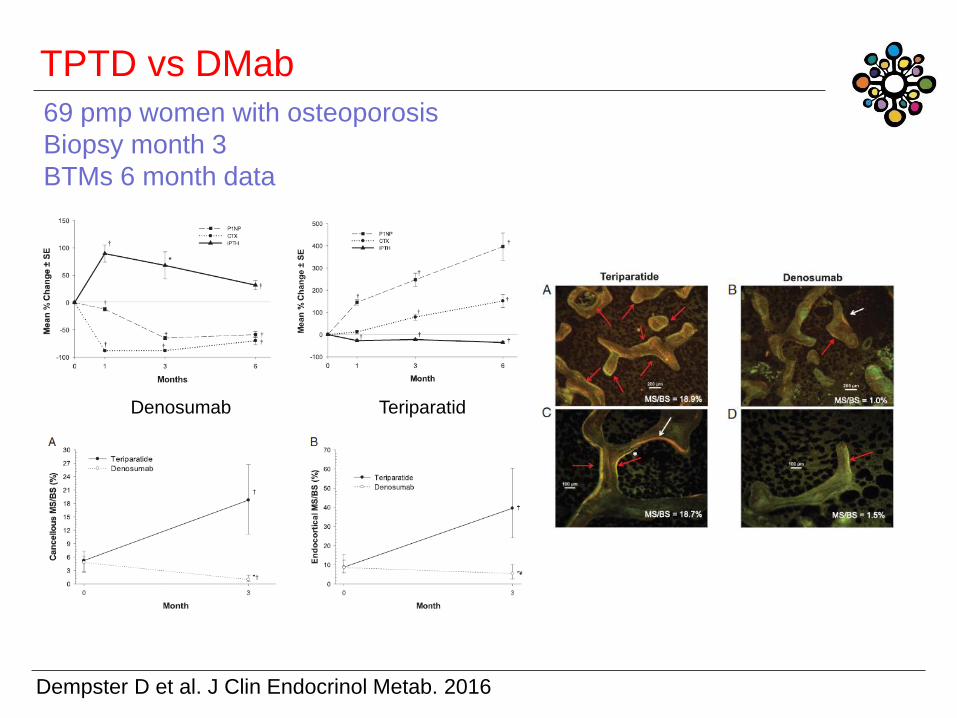
TPTD vs DMab
Dempster D et al. J Clin Endocrinol Metab. 2016
Denosumab Teriparatid
69 pmp women with osteoporosis
Biopsy month 3
BTMs 6 month data
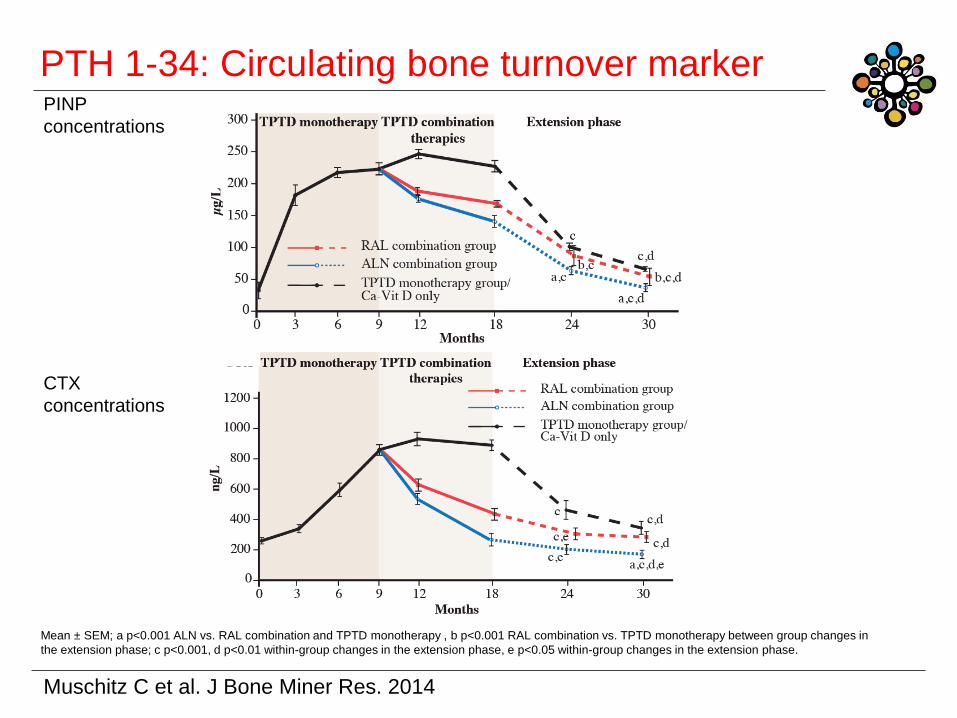
PTH 1-34: Circulating bone turnover marker
Muschitz C et al. J Bone Miner Res. 2014
Mean ± SEM; a p<0.001 ALN vs. RAL combination and TPTD monotherapy , b p<0.001 RAL combination vs. TPTD monotherapy between group changes in
the extension phase; c p<0.001, d p<0.01 within-group changes in the extension phase, e p<0.05 within-group changes in the extension phase.
PINP
concentrations
CTX
concentrations
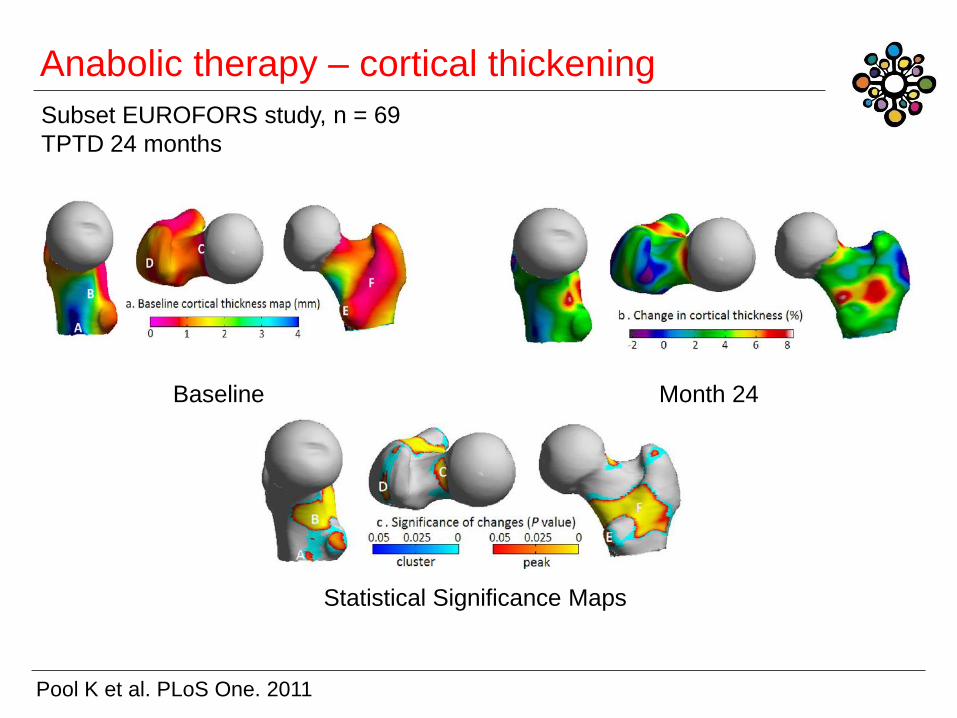
Anabolic therapy – cortical thickening
Pool K et al. PLoS One. 2011
Baseline Month 24
Statistical Significance Maps
Subset EUROFORS study, n = 69
TPTD 24 months
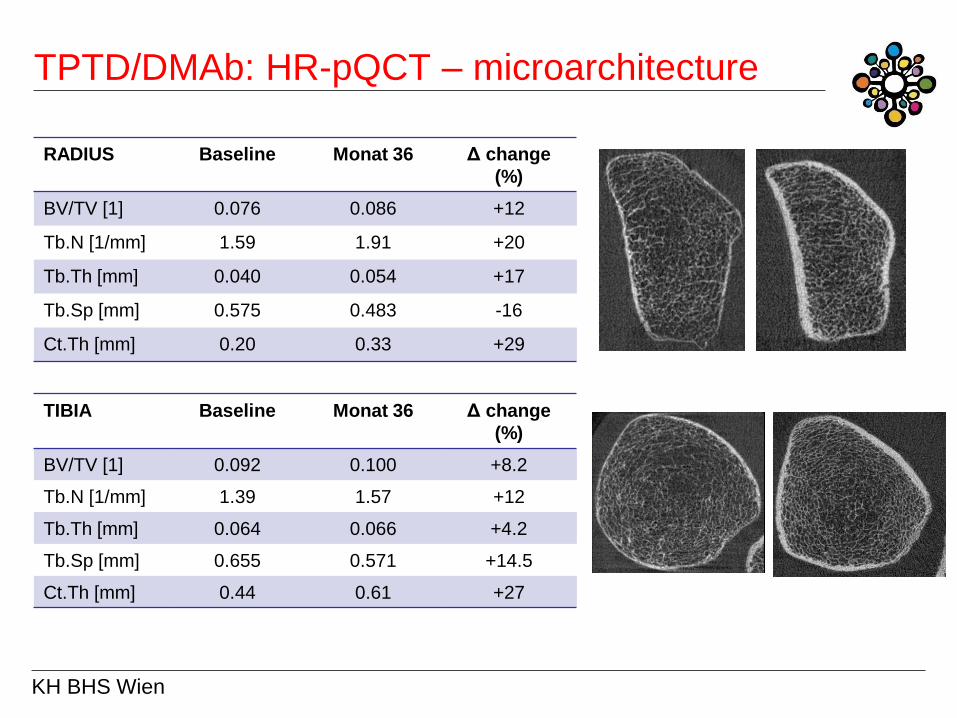
TPTD/DMAb: HR-pQCT – microarchitecture
KH BHS Wien
RADIUS Baseline Monat 36 Δ change
(%)
BV/TV [1] 0.076 0.086 +12
Tb.N [1/mm] 1.59 1.91 +20
Tb.Th [mm] 0.040 0.054 +17
Tb.Sp [mm] 0.575 0.483 -16
Ct.Th [mm] 0.20 0.33 +29
TIBIA Baseline Monat 36 Δ change
(%)
BV/TV [1] 0.092 0.100 +8.2
Tb.N [1/mm] 1.39 1.57 +12
Tb.Th [mm] 0.064 0.066 +4.2
Tb.Sp [mm] 0.655 0.571 +14.5
Ct.Th [mm] 0.44 0.61 +27
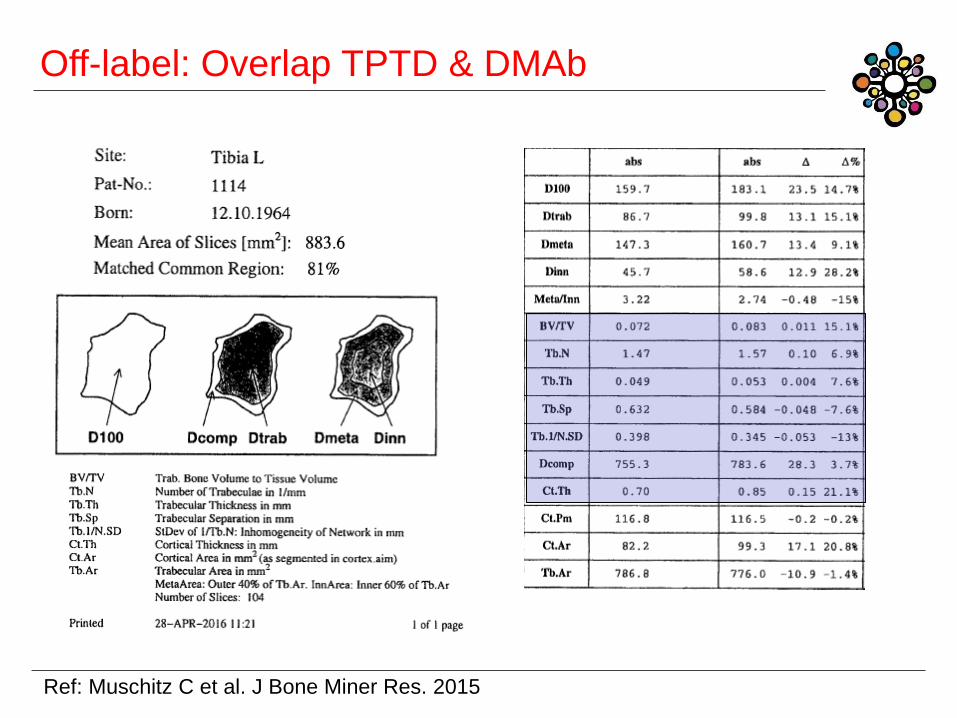
Off-label: Overlap TPTD & DMAb
Ref: Muschitz C et al. J Bone Miner Res. 2015
ONJ Medication related
osteonecrosis of the jaw
AFF Atypische Femurfrakturen
C. Muschitz Zicksee 2016
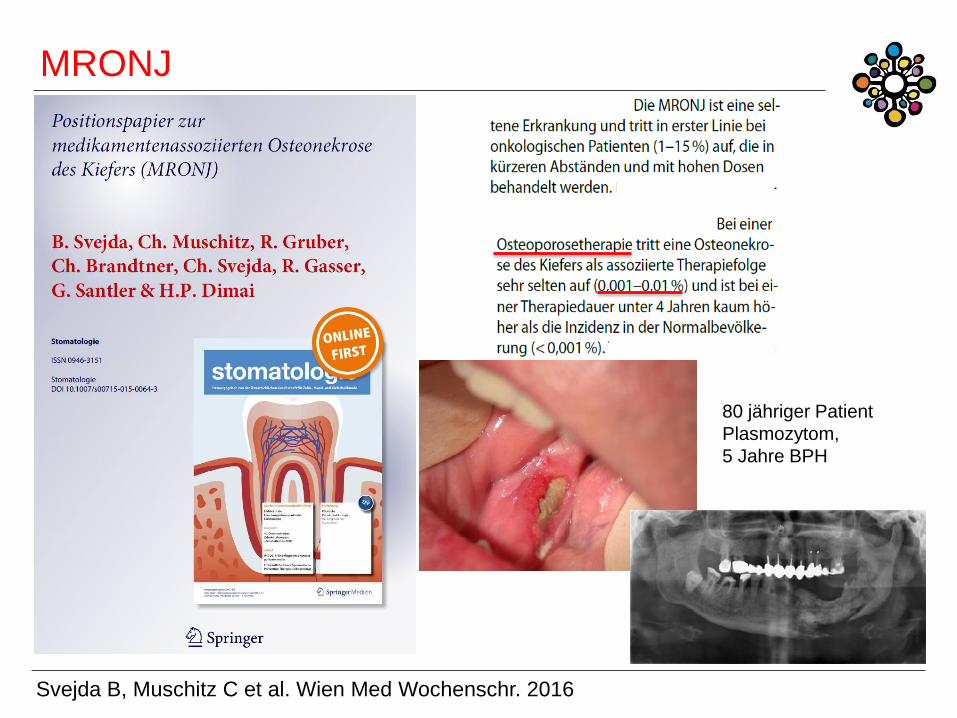
MRONJ
Svejda B, Muschitz C et al. Wien Med Wochenschr. 2016
80 jähriger Patient
Plasmozytom,
5 Jahre BPH
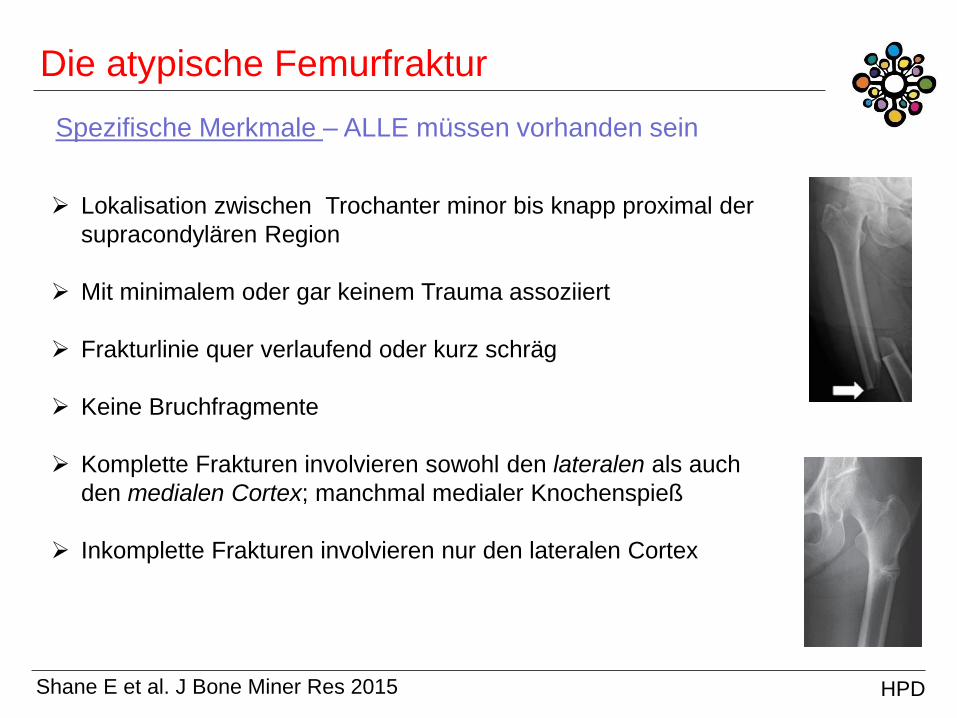
Die atypische Femurfraktur
Lokalisation zwischen Trochanter minor bis knapp proximal der
supracondylären Region
Mit minimalem oder gar keinem Trauma assoziiert
Frakturlinie quer verlaufend oder kurz schräg
Keine Bruchfragmente
Komplette Frakturen involvieren sowohl den lateralen als auch
den medialen Cortex; manchmal medialer Knochenspieß
Inkomplette Frakturen involvieren nur den lateralen Cortex
Spezifische Merkmale – ALLE müssen vorhanden sein
Shane E et al. J Bone Miner Res 2015 HPD
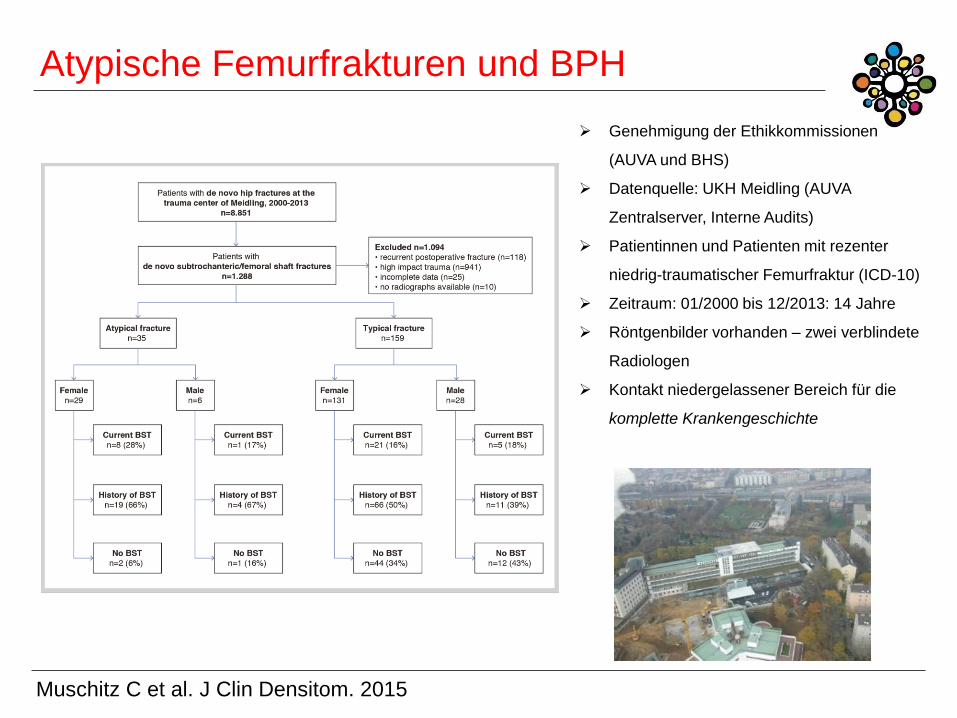
Atypische Femurfrakturen und BPH
Muschitz C et al. J Clin Densitom. 2015
Genehmigung der Ethikkommissionen
(AUVA und BHS)
Datenquelle: UKH Meidling (AUVA
Zentralserver, Interne Audits)
Patientinnen und Patienten mit rezenter
niedrig-traumatischer Femurfraktur (ICD-10)
Zeitraum: 01/2000 bis 12/2013: 14 Jahre
Röntgenbilder vorhanden – zwei verblindete
Radiologen
Kontakt niedergelassener Bereich für die
komplette Krankengeschichte
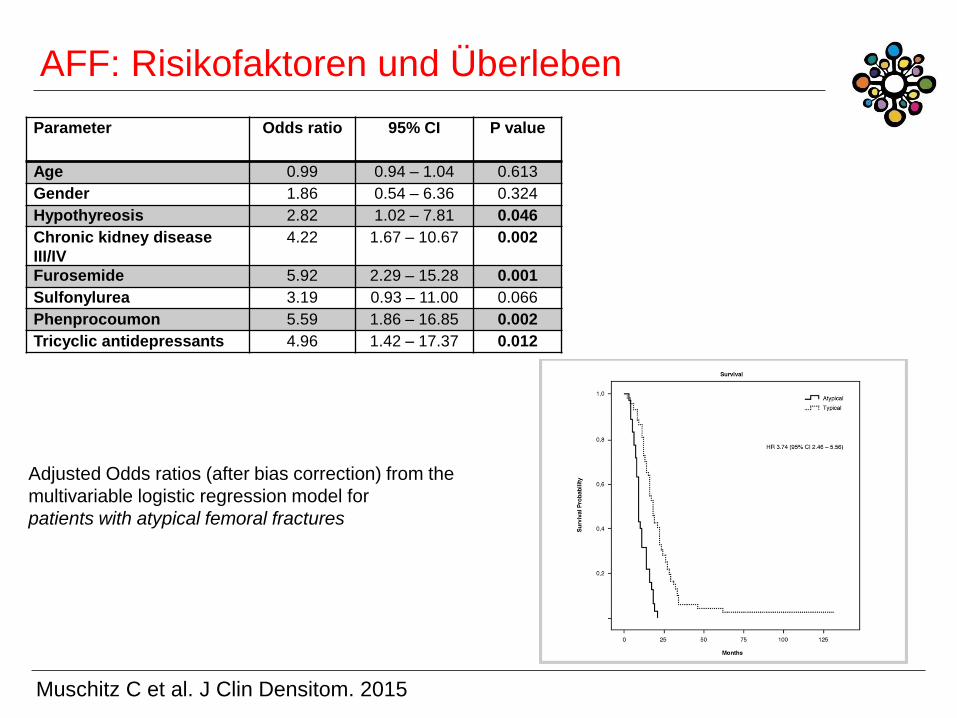
AFF: Risikofaktoren und Überleben
Parameter Odds ratio
95% CI P value
Age 0.99 0.94 – 1.04 0.613
Gender 1.86 0.54 – 6.36 0.324
Hypothyreosis 2.82 1.02 – 7.81 0.046
Chronic kidney disease
III/IV
4.22 1.67 – 10.67 0.002
Furosemide 5.92 2.29 – 15.28 0.001
Sulfonylurea 3.19 0.93 – 11.00 0.066
Phenprocoumon 5.59 1.86 – 16.85 0.002
Tricyclic antidepressants 4.96 1.42 – 17.37 0.012
Adjusted Odds ratios (after bias correction) from the
multivariable logistic regression model for
patients with atypical femoral fractures
Muschitz C et al. J Clin Densitom. 2015
Therapiemonitoring
C. Muschitz Zicksee 2016
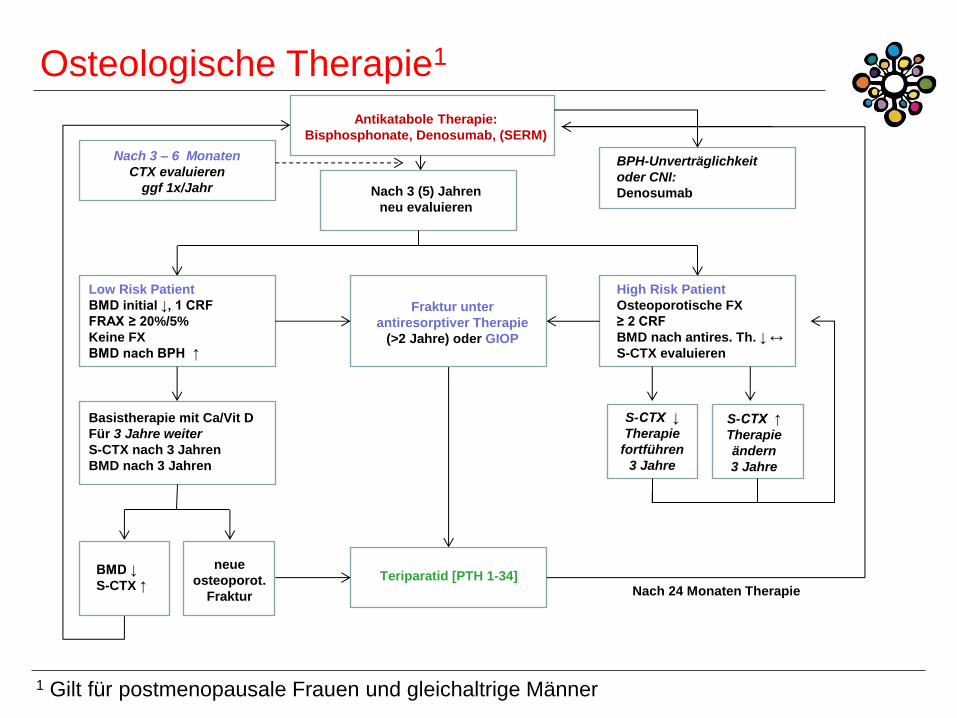
Antikatabole Therapie:
Bisphosphonate, Denosumab, (SERM)
Nach 3 (5) Jahren
neu evaluieren
BPH-Unverträglichkeit
oder CNI:
Denosumab
Low Risk Patient
BMD initial ↓, 1 CRF
FRAX ≥ 20%/5%
Keine FX
BMD nach BPH ↑
Basistherapie mit Ca/Vit D
Für 3 Jahre weiter
S-CTX nach 3 Jahren
BMD nach 3 Jahren
BMD ↓
S-CTX ↑
High Risk Patient
Osteoporotische FX
≥ 2 CRF
BMD nach antires. Th. ↓ ↔
S-CTX evaluieren
Teriparatid [PTH 1-34]
Fraktur unter
antiresorptiver Therapie
(>2 Jahre) oder GIOP
Osteologische Therapie1
Nach 24 Monaten Therapie
S-CTX ↓
Therapie
fortführen
3 Jahre
S-CTX ↑
Therapie
ändern
3 Jahre
1 Gilt für postmenopausale Frauen und gleichaltrige Männer
neue
osteoporot.
Fraktur
Nach 3 – 6 Monaten
CTX evaluieren
ggf 1x/Jahr
Kasuistik 1
C. Muschitz Zicksee 2016
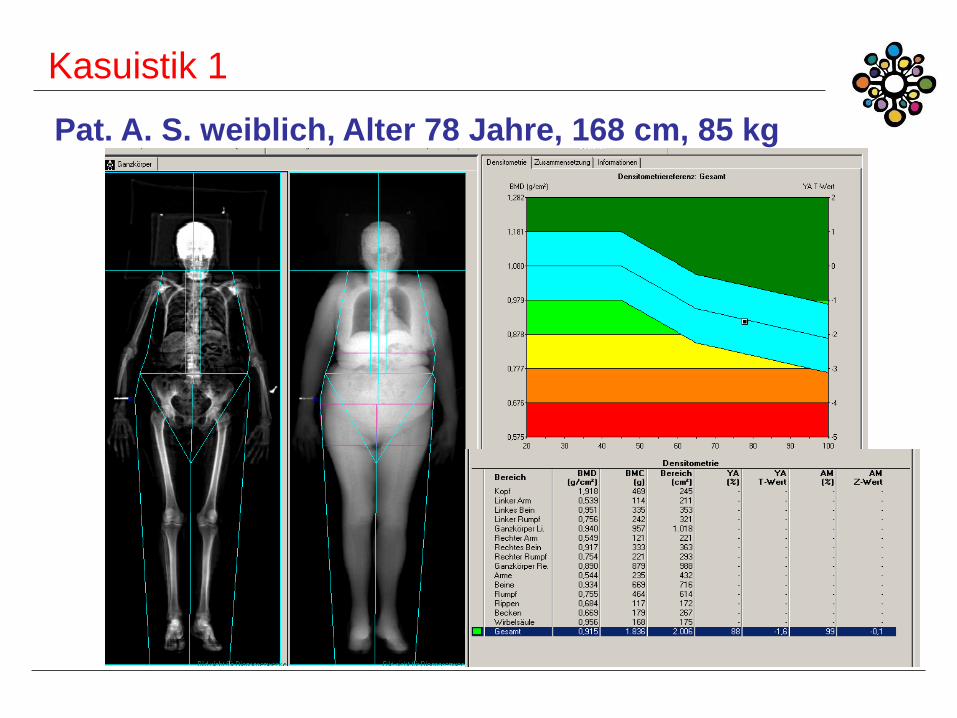
Kasuistik 1
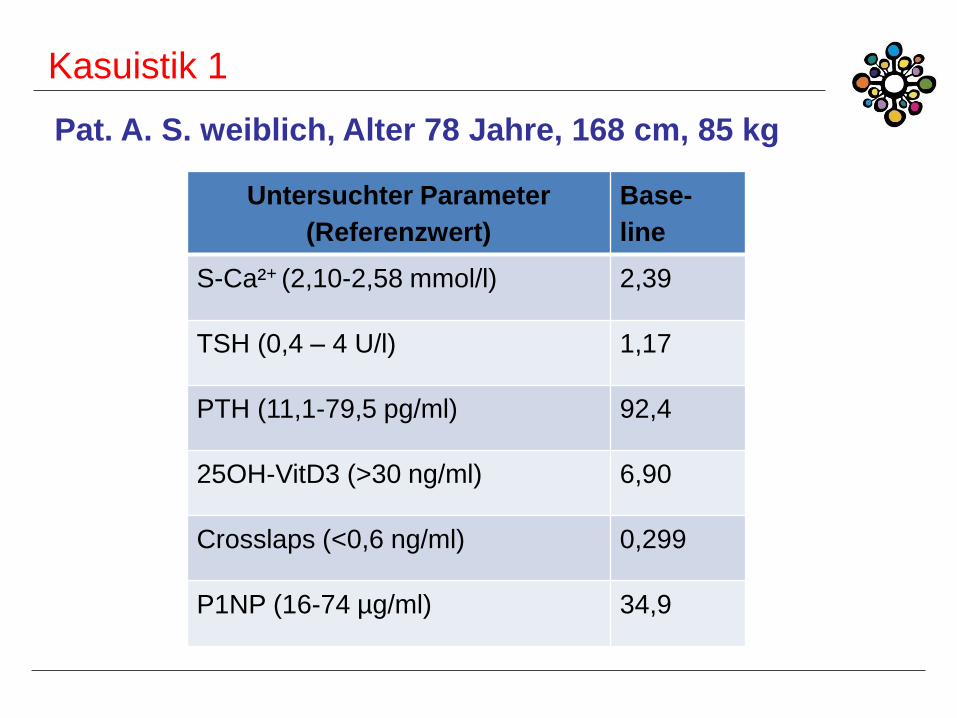
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
Erkrankungen:
art. Hypertonie
T2DM – HbA1c 7,4mg%
St.p. CHE
Chronische Lumboischialgie
Kasuistik 1
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
Familien - Anamnese:
Mutter: Diabetes
Vater: MCI
Bruder: art. Hypertonie
Genußmittel - Anamnese:
Nikotin: 20 Zigaretten/Tag (60 py)
Alkohol: selten
Kasuistik 1
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
Fraktur – Anamnese:
Keine Frakturen
Fraktur – Anamnese Verwandtschaft:
Mutter: fragliche Radius-Fraktur
Vater: Hüftfraktur
Bruder: nicht erinnerlich
Kasuistik 1
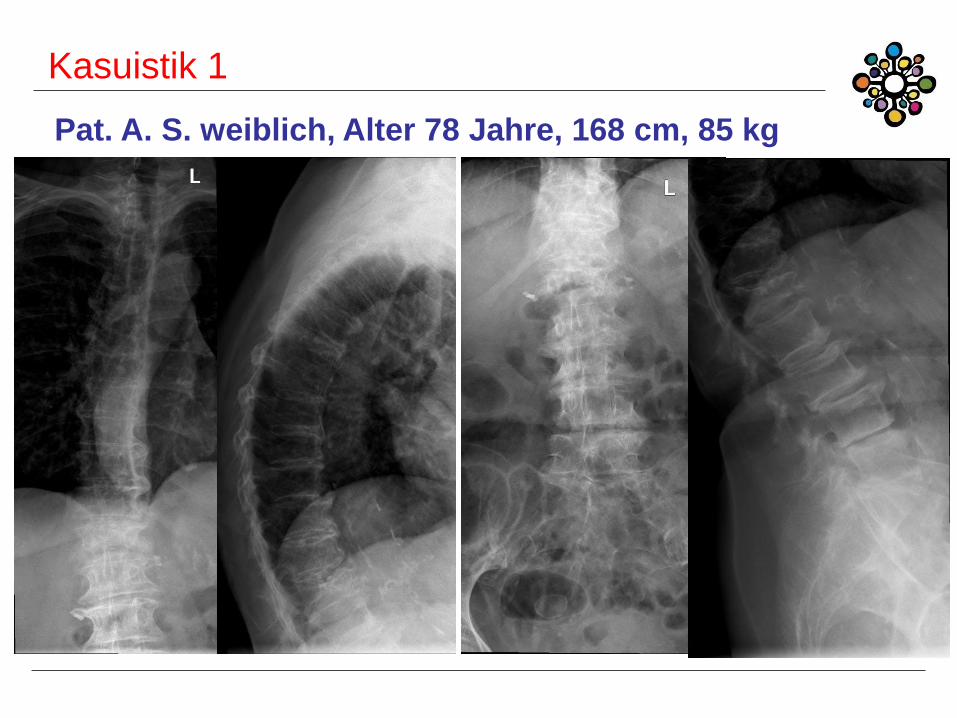
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
Jetzige Erkrankung:
Plötzlich aufgetretene Schmerzen in der LWS seit
etwa 14 Tagen ohne Ausstrahlung in die Beine
Starke Einschränkung der Mobilität aufgrund
Lumboischialgie
Geringgradige Belastungsdyspnoe
Kasuistik 1
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
Untersuchter Parameter
(Referenzwert)
Base-
line
S-Ca²+ (2,10-2,58 mmol/l) 2,39
TSH (0,4 – 4 U/l) 1,17
PTH (11,1-79,5 pg/ml) 92,4
25OH-VitD3 (>30 ng/ml) 6,90
Crosslaps (<0,6 ng/ml) 0,299
P1NP (16-74 µg/ml) 34,9
Kasuistik 1
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
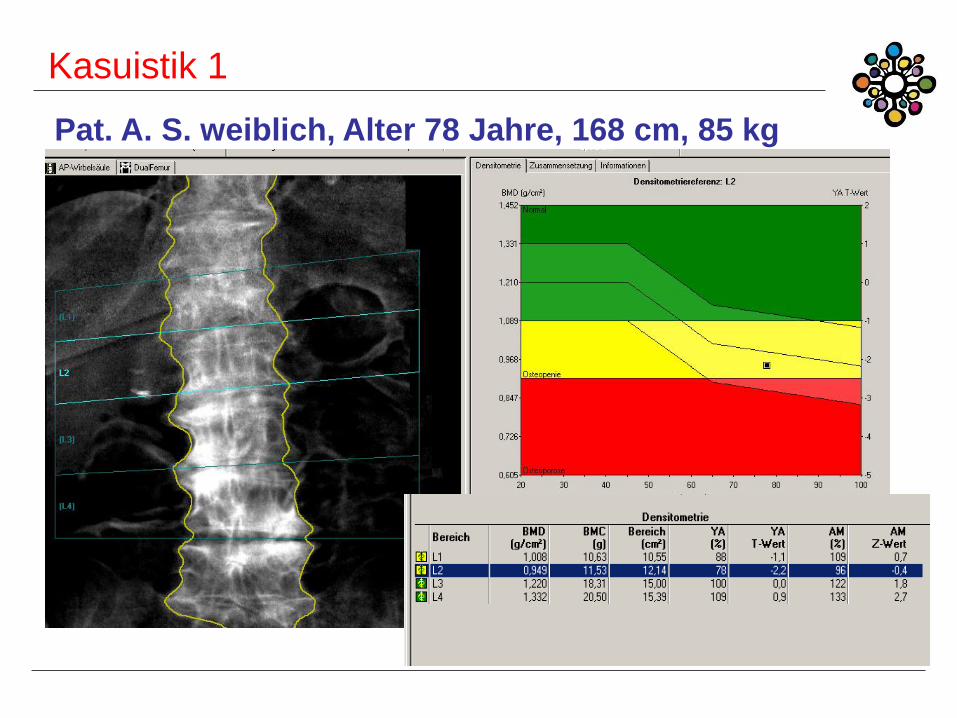
Kasuistik 1
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
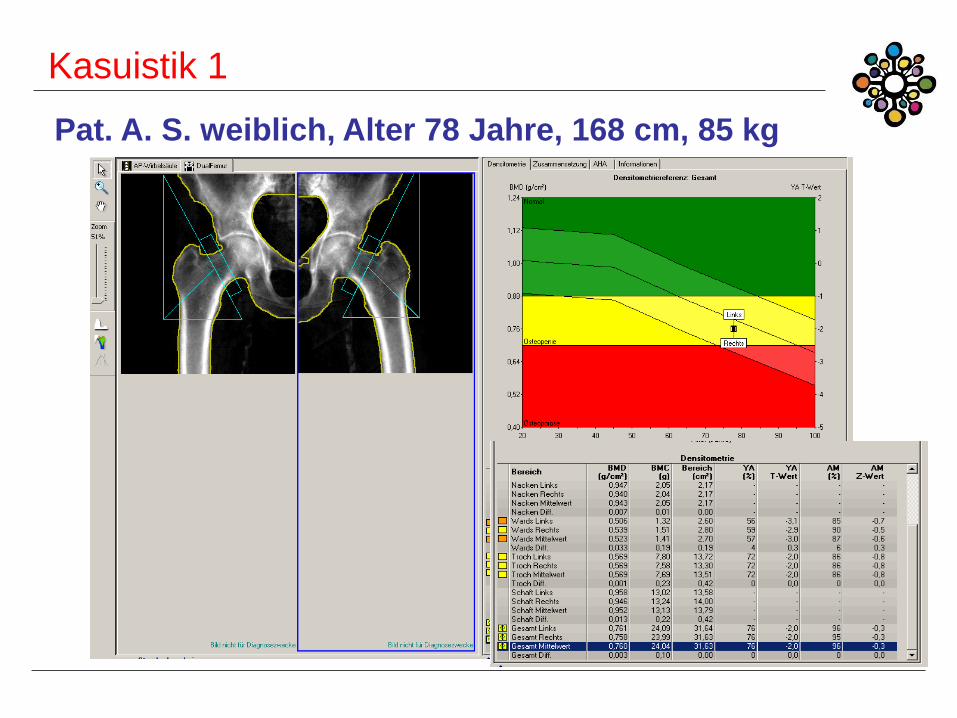
Kasuistik 1
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
Kasuistik 1
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
Kasuistik 1
Pat. A. S. weiblich, Alter 78 Jahre, 168 cm, 85 kg
Diagnostik??
Therapie??
Kasuistik 2
C. Muschitz Zicksee 2016
Kasuistik 2
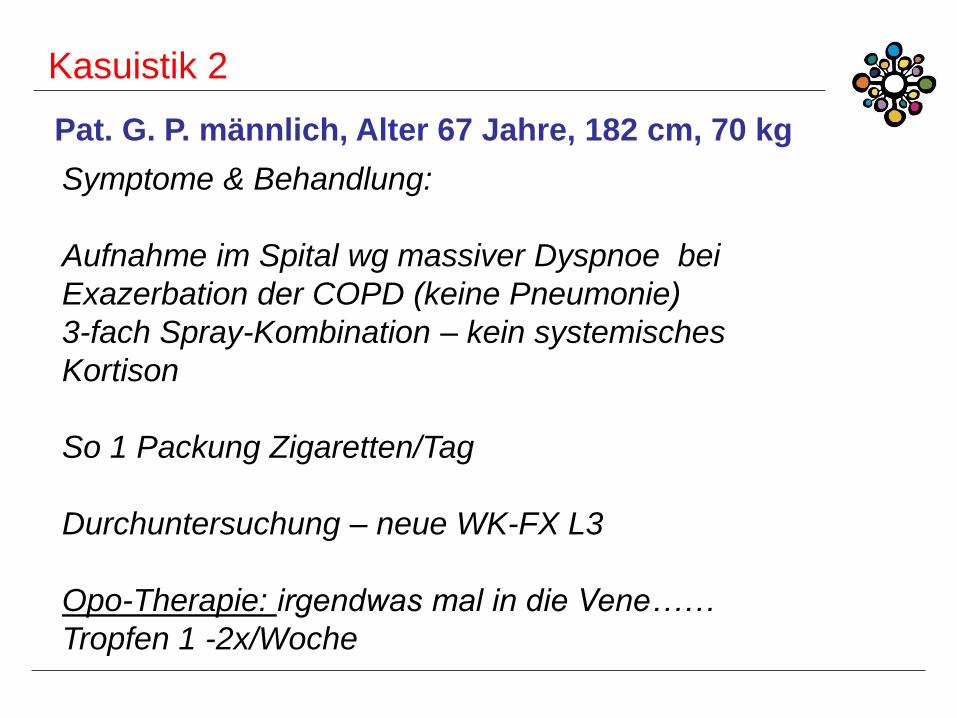
Pat. G. P. männlich, Alter 67 Jahre, 182 cm, 70 kg
Erkrankungen:
COPD – Gold III
Art. Hypertonie
KHK – PTCA mit DES 2009
pAVK
WK-FX Th11, L2 (Sturz)
Kasuistik 2
Symptome & Behandlung:
Aufnahme im Spital wg massiver Dyspnoe bei
Exazerbation der COPD (keine Pneumonie)
3-fach Spray-Kombination – kein systemisches
Kortison
So 1 Packung Zigaretten/Tag
Durchuntersuchung – neue WK-FX L3
Opo-Therapie: irgendwas mal in die Vene……
Tropfen 1 -2x/Woche
Pat. G. P. männlich, Alter 67 Jahre, 182 cm, 70 kg
Kasuistik 2
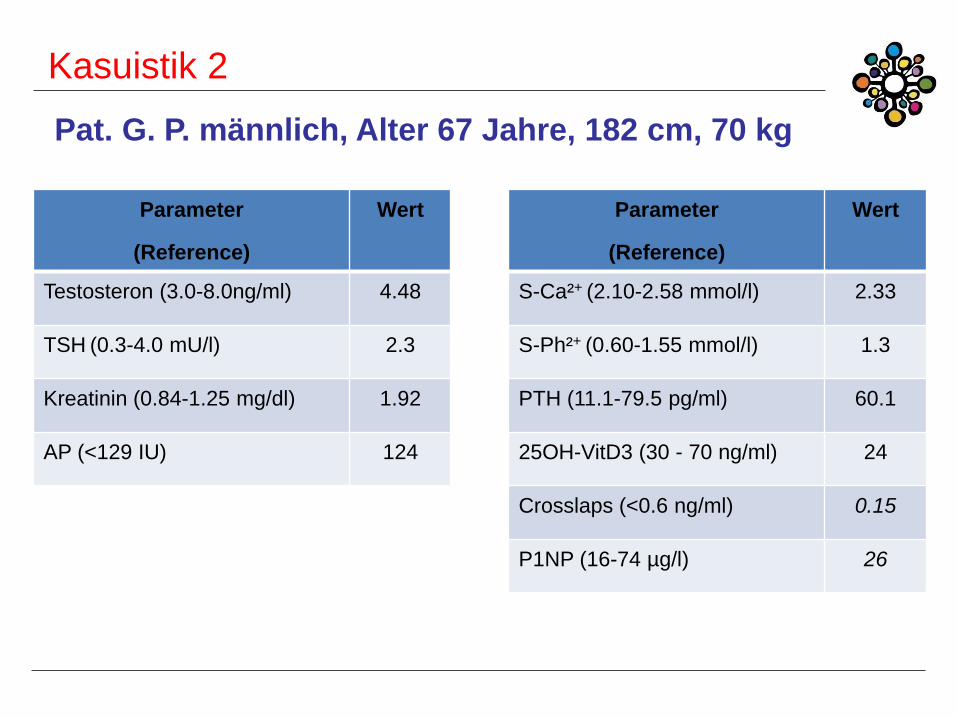
Pat. G. P. männlich, Alter 67 Jahre, 182 cm, 70 kg
Parameter
(Reference)
Wert
S-Ca²+ (2.10-2.58 mmol/l) 2.33
S-Ph²+ (0.60-1.55 mmol/l) 1.3
PTH (11.1-79.5 pg/ml) 60.1
25OH-VitD3 (30 - 70 ng/ml) 24
Crosslaps (<0.6 ng/ml) 0.15
P1NP (16-74 µg/l) 26
Parameter
(Reference)
Wert
Testosteron (3.0-8.0ng/ml) 4.48
TSH (0.3-4.0 mU/l) 2.3
Kreatinin (0.84-1.25 mg/dl) 1.92
AP (<129 IU) 124