Embed Size (px)
Citation preview
Vorlesung Innere Medizin
Modul 3.4: HämatologieMultiples Myelom, Stammzelltransplantation
Bertram Glass
Universitätsklinikum GöttingenAbteilung Hämatologie und Onkologie
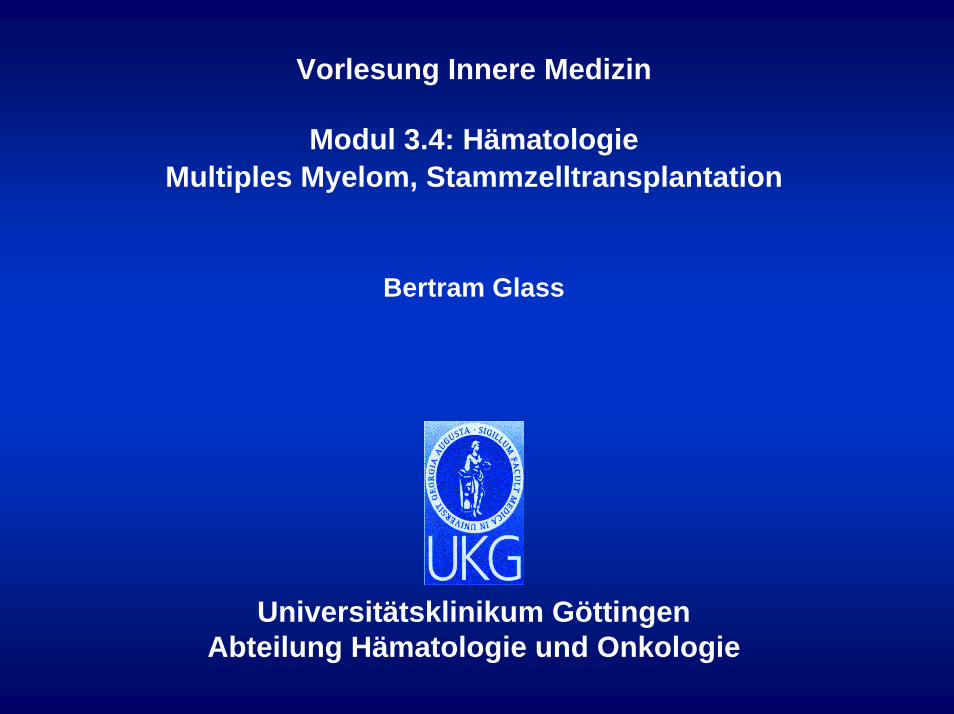
Altersspezifische Inzidenzen lymphatischer NeoplasienNorddeutsche Leukämie und Lymphomstudie1984-1998
(Alle Alter)
75+70-7465-6960-6455-5950-5445-4940-4435-4030-3425-2920-2415-1910-14
5-90-4
020406080100120140 0 20 40 60 80 100 120 140
Männer FrauenAltersgruppe
Altersspezifische Inzidenzdichte (/100.000 Personenjahre)Stand 13.3.2001
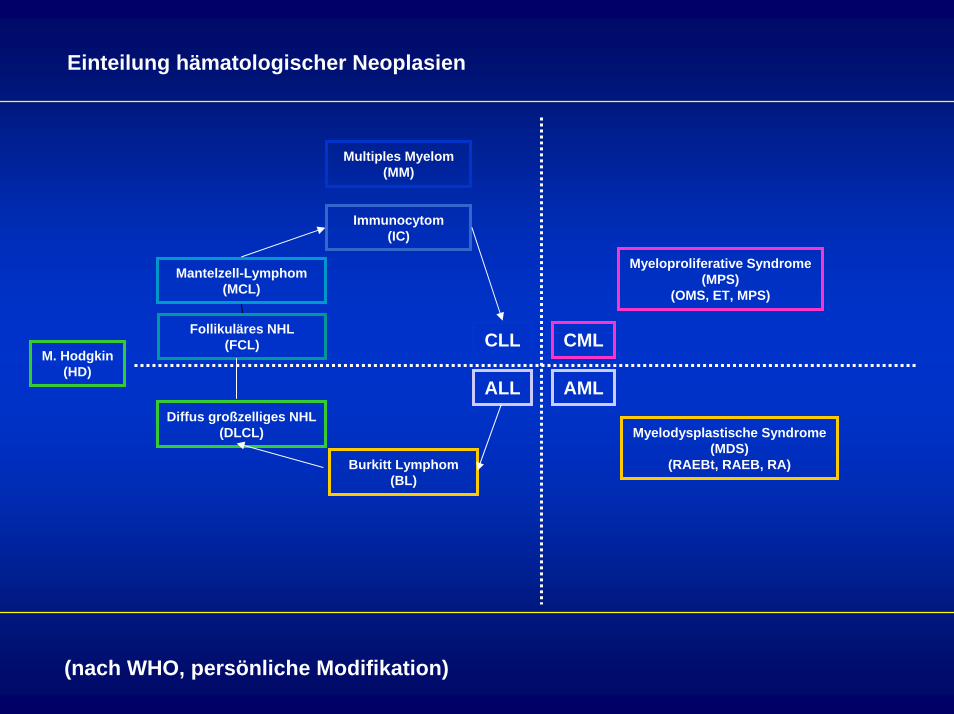
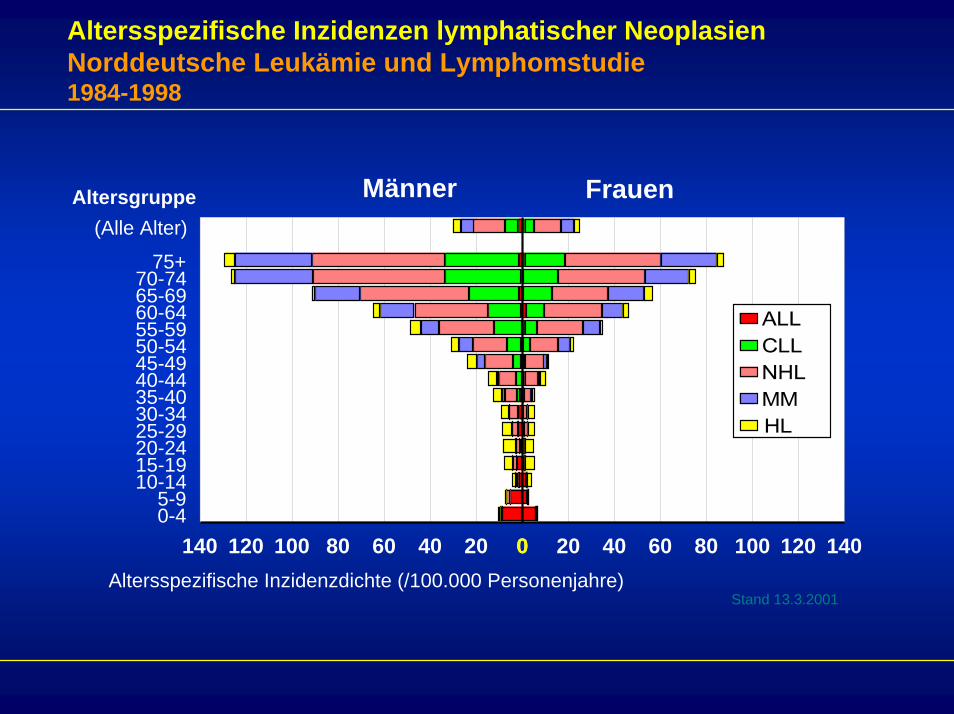
Einteilung hämatologischer Neoplasien
Multiples Myelom(MM)
Immunocytom(IC)
Myeloproliferative Syndrome(MPS)
(OMS, ET, MPS)Mantelzell-Lymphom
(MCL)
(nach WHO, persönliche Modifikation)
ALL
CLL
AML
CML
Diffus großzelliges NHL(DLCL)
Follikuläres NHL(FCL)
Burkitt Lymphom(BL)
M. Hodgkin(HD)
Myelodysplastische Syndrome(MDS)
(RAEBt, RAEB, RA)
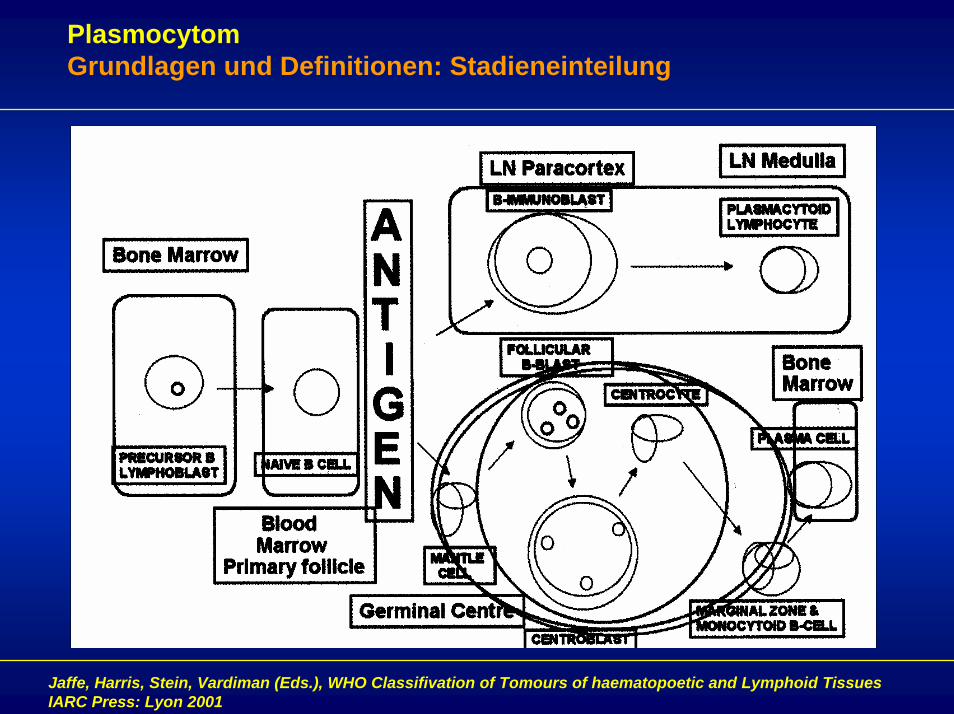
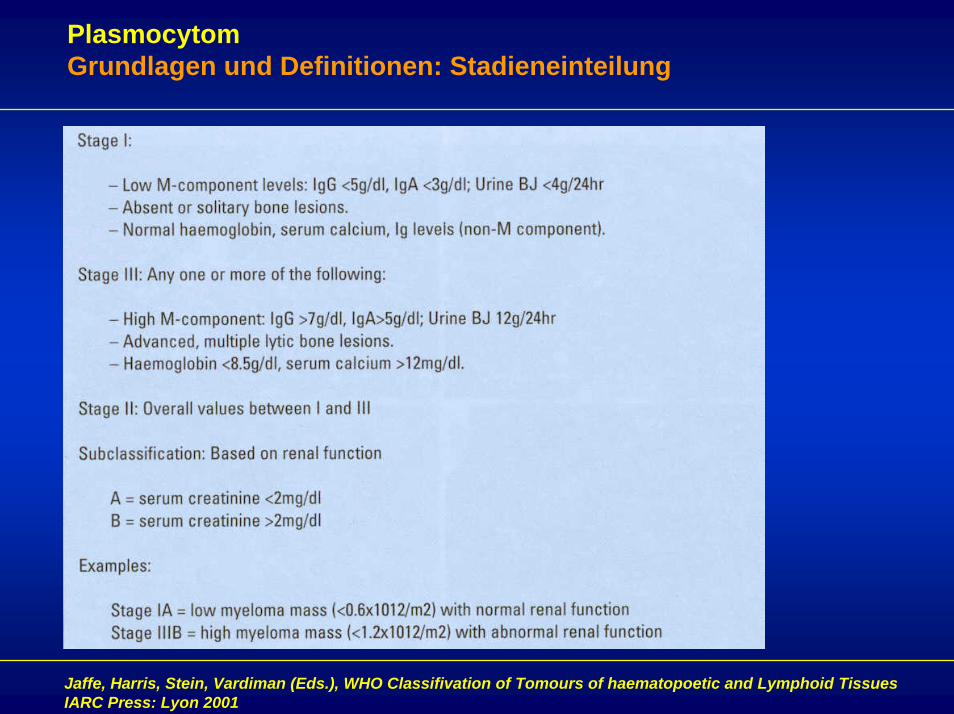
PlasmocytomGrundlagen und Definitionen: Stadieneinteilung
Jaffe, Harris, Stein, Vardiman (Eds.), WHO Classifivation of Tomours of haematopoetic and Lymphoid TissuesIARC Press: Lyon 2001
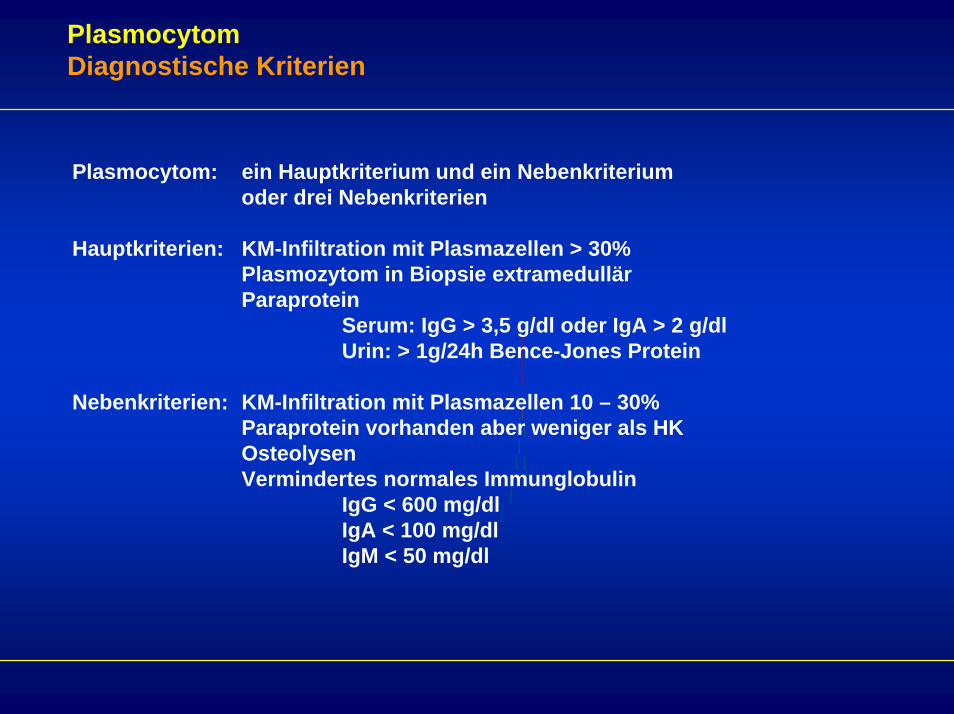
PlasmocytomDiagnostische Kriterien
Plasmocytom: ein Hauptkriterium und ein Nebenkriteriumoder drei Nebenkriterien
Hauptkriterien: KM-Infiltration mit Plasmazellen > 30%Plasmozytom in Biopsie extramedullärParaprotein
Serum: IgG > 3,5 g/dl oder IgA > 2 g/dlUrin: > 1g/24h Bence-Jones Protein
Nebenkriterien: KM-Infiltration mit Plasmazellen 10 – 30%Paraprotein vorhanden aber weniger als HKOsteolysenVermindertes normales Immunglobulin
IgG < 600 mg/dlIgA < 100 mg/dlIgM < 50 mg/dl
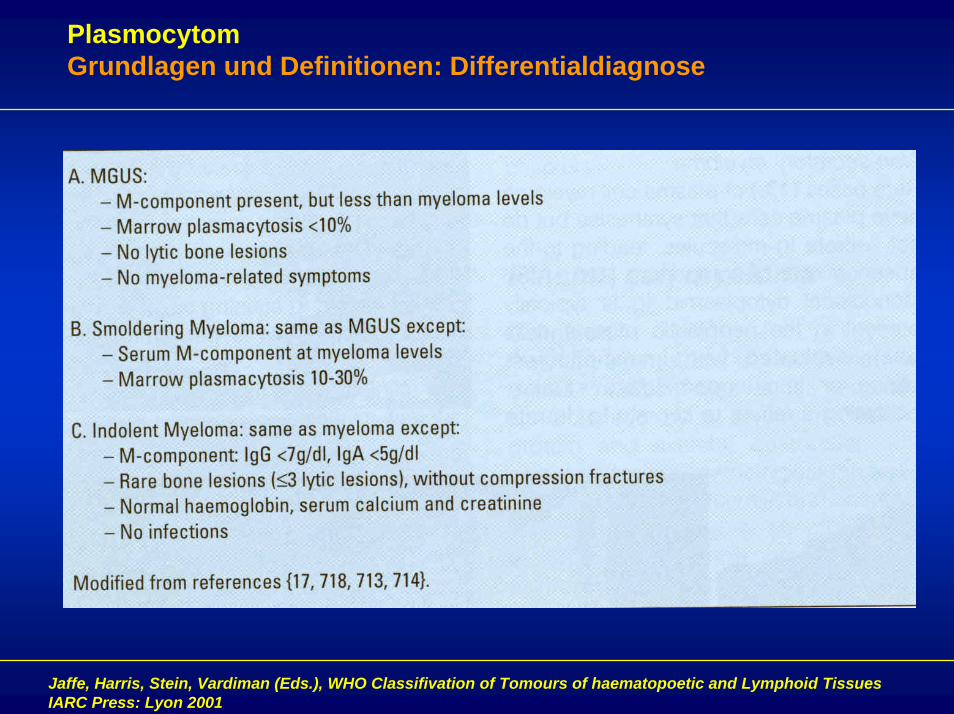
PlasmocytomGrundlagen und Definitionen: Differentialdiagnose
Jaffe, Harris, Stein, Vardiman (Eds.), WHO Classifivation of Tomours of haematopoetic and Lymphoid TissuesIARC Press: Lyon 2001
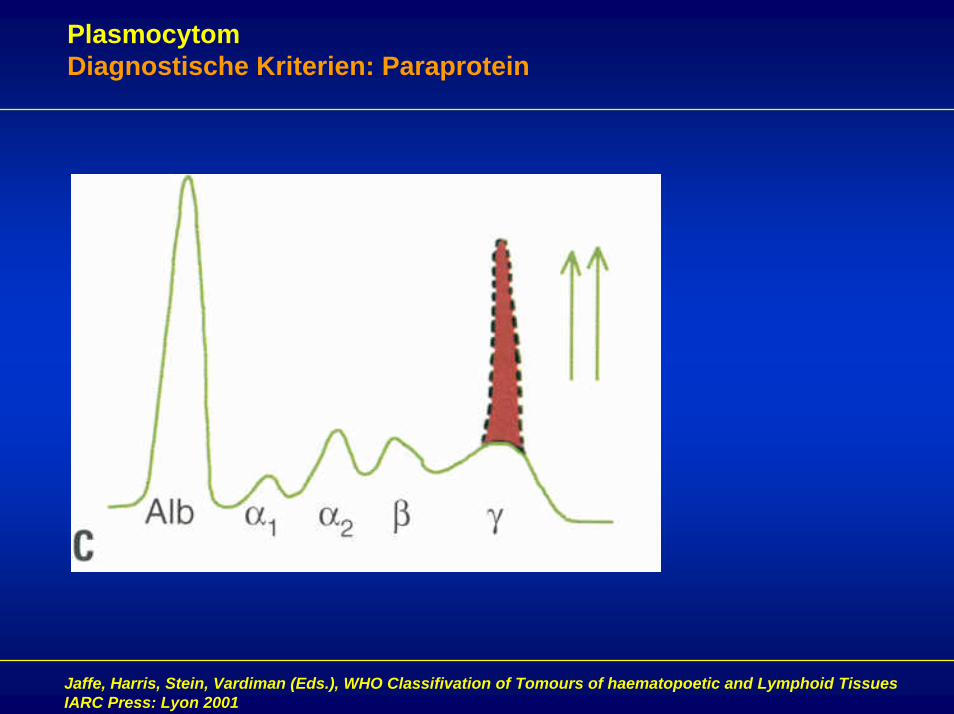
PlasmocytomDiagnostische Kriterien: Paraprotein
Jaffe, Harris, Stein, Vardiman (Eds.), WHO Classifivation of Tomours of haematopoetic and Lymphoid TissuesIARC Press: Lyon 2001
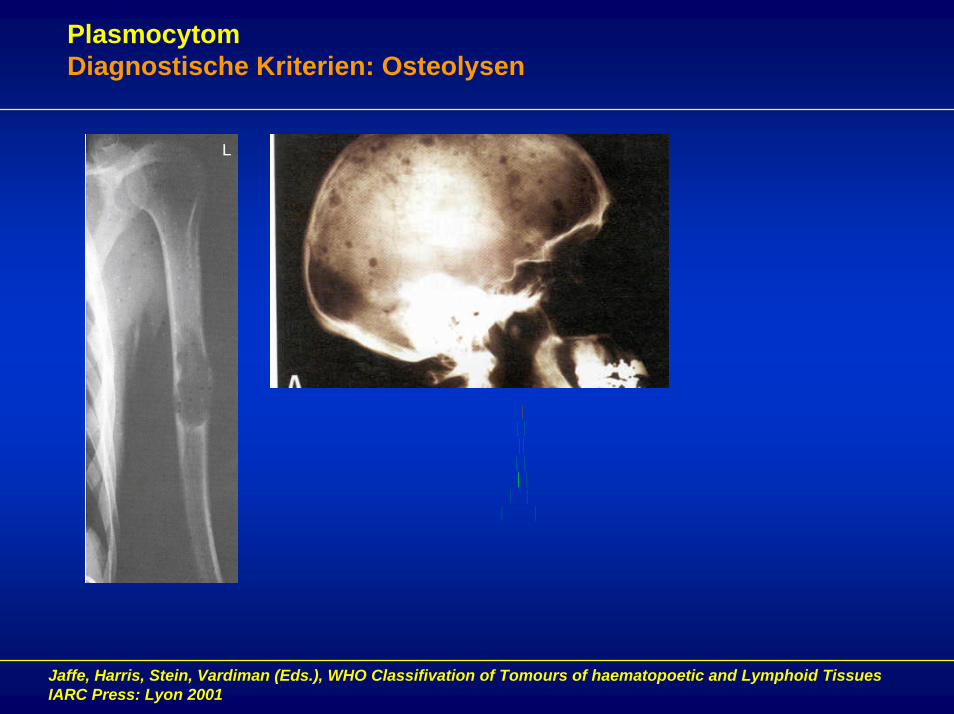
PlasmocytomDiagnostische Kriterien: Osteolysen
Jaffe, Harris, Stein, Vardiman (Eds.), WHO Classifivation of Tomours of haematopoetic and Lymphoid TissuesIARC Press: Lyon 2001
PlasmocytomKlinisches Bild
Hämatopoese: Anämie (Verdrängung, Hämolyse) – Müdigkeit, AbgeschlagenheitThrombopenie – Blutungszeichenselten: Neutropenie – InfektneigungEinschränkung der B-Zell und T-Zellfunktion: virale Infekte (Zoster, Herpes Simplex)
Knochen: Osteolysen – Schmerzen, pathologische FrakturenHypercalcämie – teilweise Notfallsituation: Nierenversagen
Niere: akutes Nierenversagen (Hypercalcämie), terminalesNierenversagen (Bence-Jones Protein)
Neurologie: fokale Symptomatik als Folge von Raumforderung oder pathologischen Frakturenpolyneuropathische Beschwerden: Amyloidose
PlasmocytomGrundlagen und Definitionen: Stadieneinteilung
Jaffe, Harris, Stein, Vardiman (Eds.), WHO Classifivation of Tomours of haematopoetic and Lymphoid TissuesIARC Press: Lyon 2001
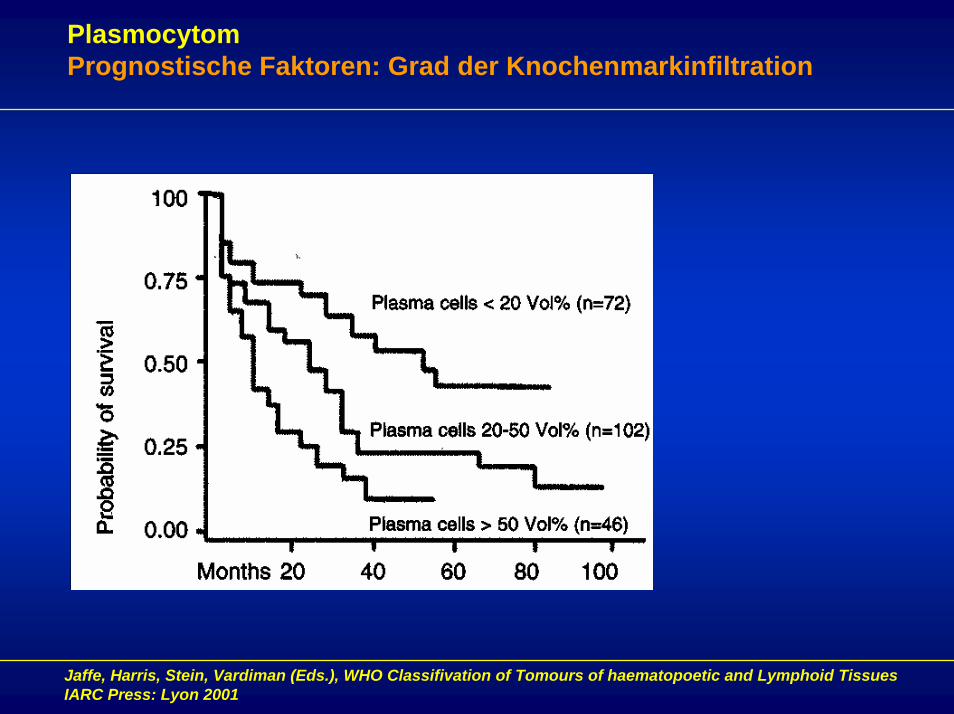
PlasmocytomPrognostische Faktoren: Grad der Knochenmarkinfiltration
Jaffe, Harris, Stein, Vardiman (Eds.), WHO Classifivation of Tomours of haematopoetic and Lymphoid TissuesIARC Press: Lyon 2001
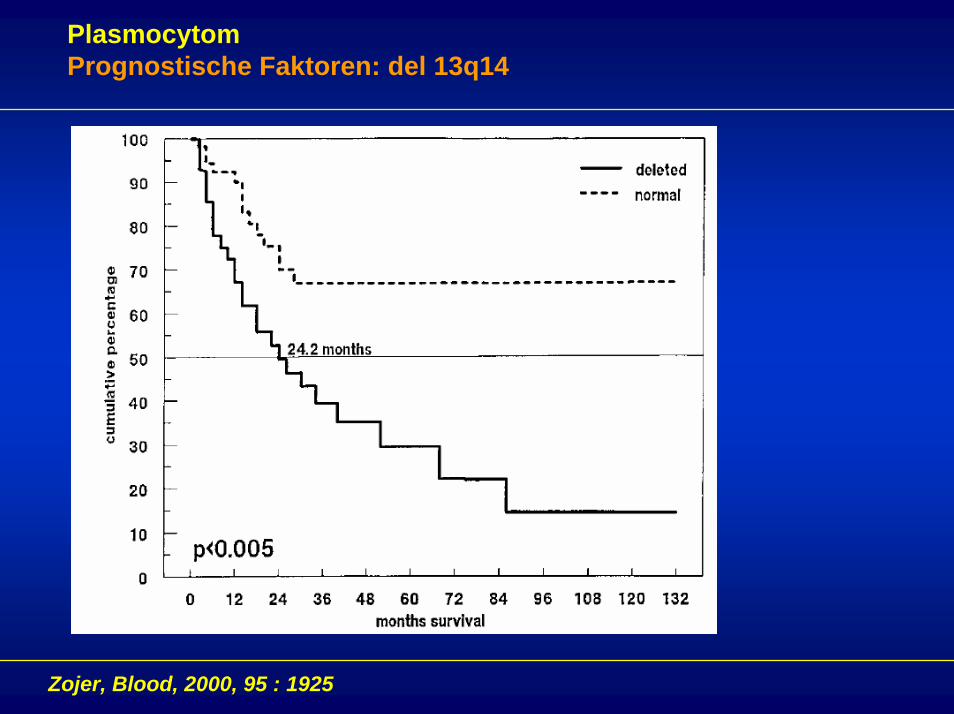
PlasmocytomPrognostische Faktoren: del 13q14
Zojer, Blood, 2000, 95 : 1925
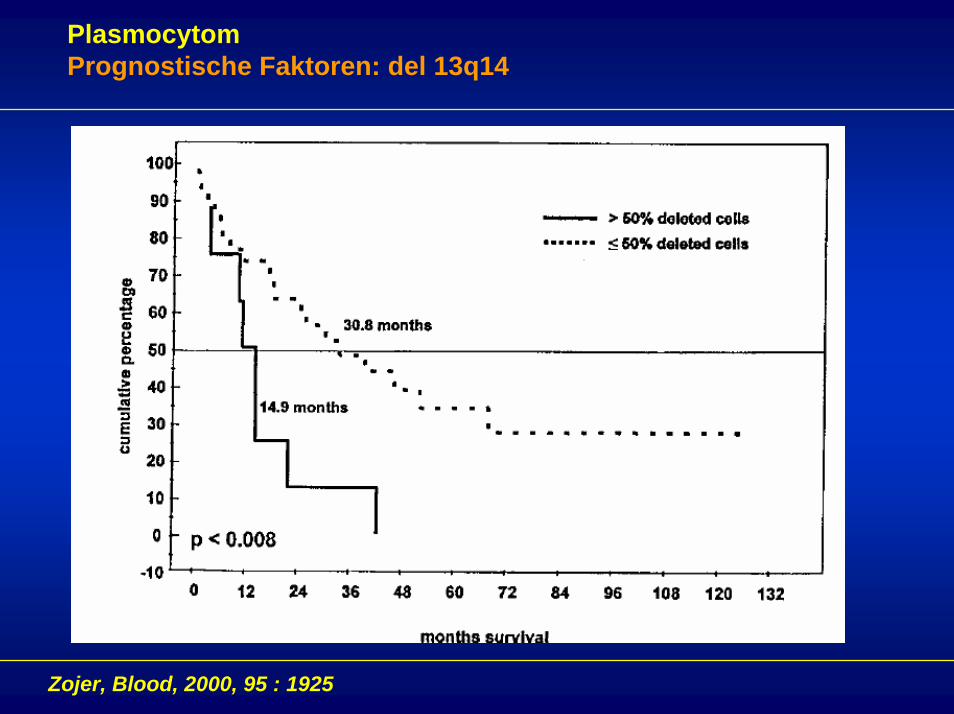
PlasmocytomPrognostische Faktoren: del 13q14
Zojer, Blood, 2000, 95 : 1925
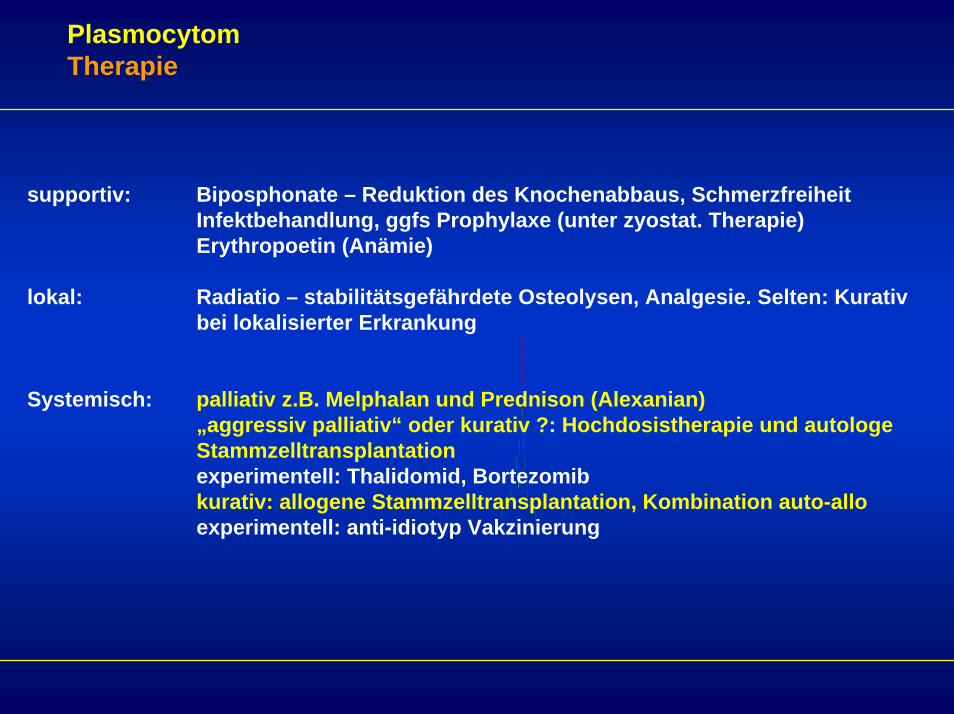
PlasmocytomTherapie
supportiv: Biposphonate – Reduktion des Knochenabbaus, SchmerzfreiheitInfektbehandlung, ggfs Prophylaxe (unter zyostat. Therapie)Erythropoetin (Anämie)
lokal: Radiatio – stabilitätsgefährdete Osteolysen, Analgesie. Selten: Kurativ bei lokalisierter Erkrankung
Systemisch: palliativ z.B. Melphalan und Prednison (Alexanian)„aggressiv palliativ“ oder kurativ ?: Hochdosistherapie und autologe Stammzelltransplantationexperimentell: Thalidomid, Bortezomibkurativ: allogene Stammzelltransplantation, Kombination auto-alloexperimentell: anti-idiotyp Vakzinierung
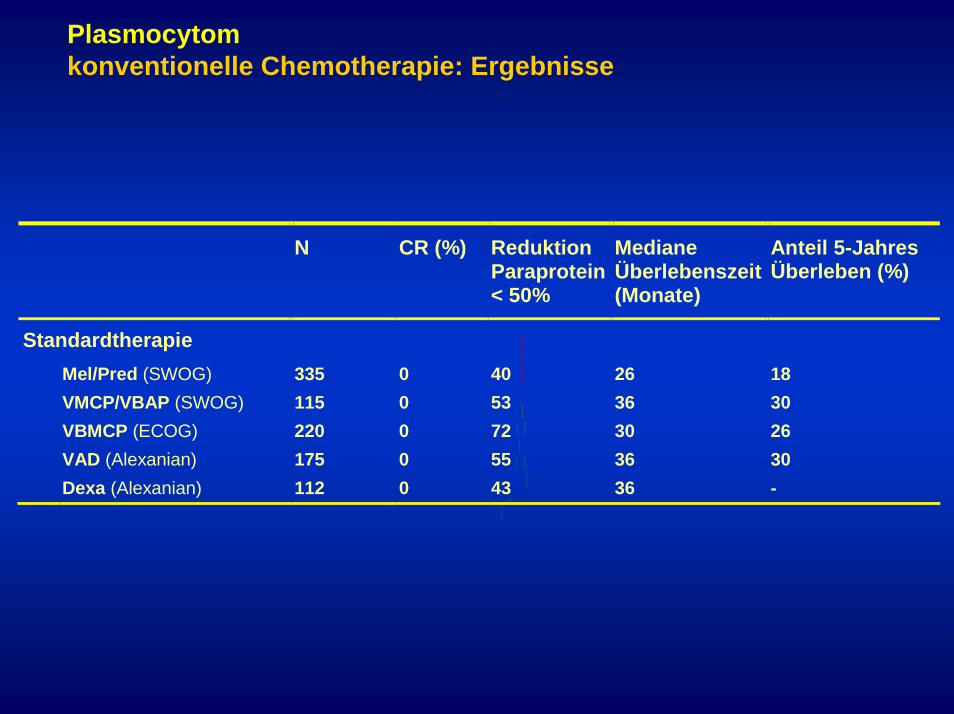
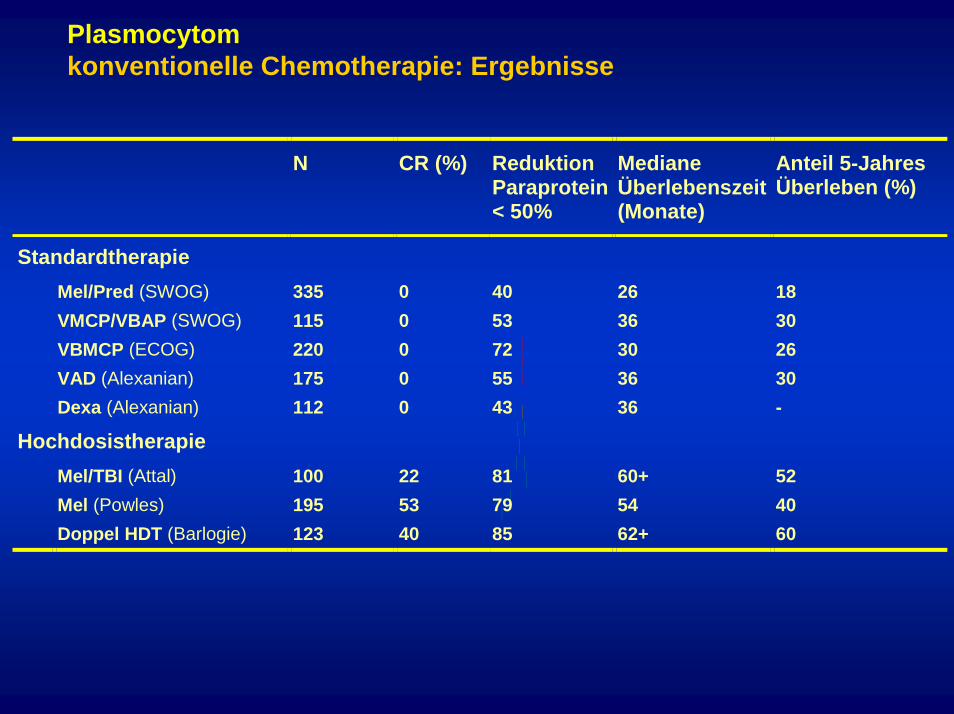
Plasmocytomkonventionelle Chemotherapie: Ergebnisse
N CR (%) Reduktion Paraprotein < 50%
Mediane Überlebenszeit (Monate)
Anteil 5-Jahres Überleben (%)
Standardtherapie Mel/Pred (SWOG) 335 0 40 26 18 VMCP/VBAP (SWOG) 115 0 53 36 30 VBMCP (ECOG) 220 0 72 30 26 VAD (Alexanian) 175 0 55 36 30 Dexa (Alexanian) 112 0 43 36 -
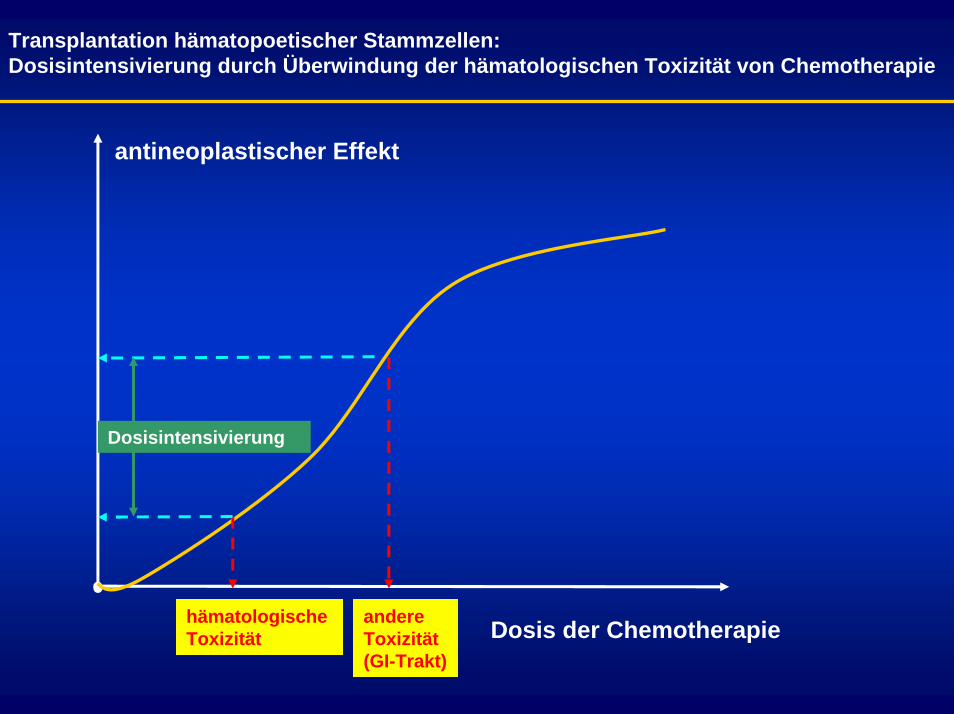
Transplantation hämatopoetischer Stammzellen:Dosisintensivierung durch Überwindung der hämatologischen Toxizität von Chemotherapie
antineoplastischer Effekt
hämatologische Toxizität
andere Toxizität(GI-Trakt)
Dosisintensivierung
Dosis der Chemotherapie
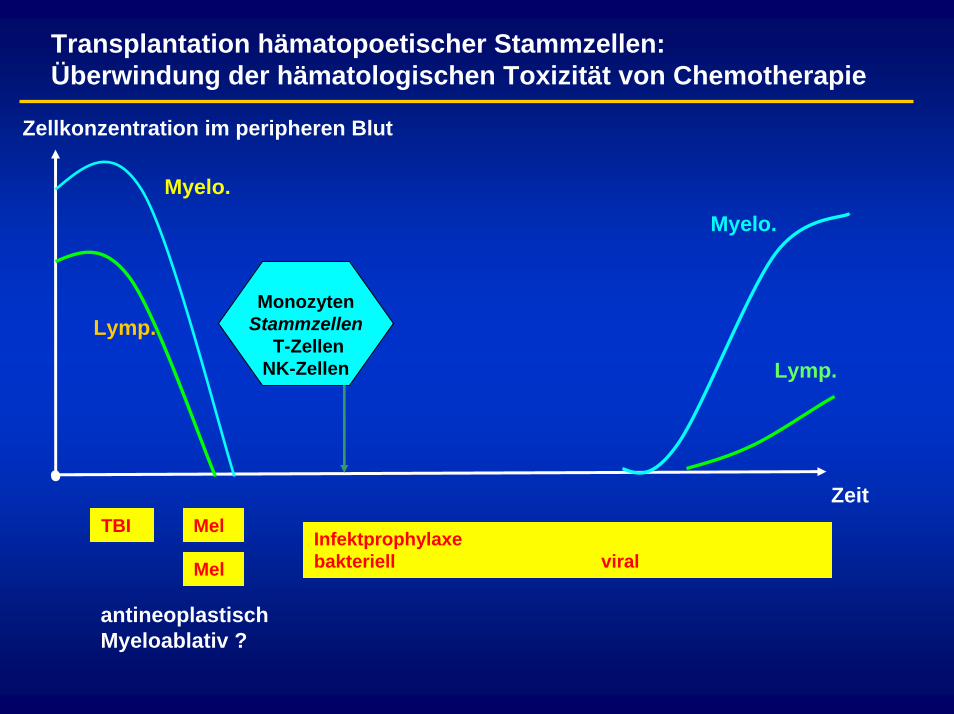
Transplantation hämatopoetischer Stammzellen:Überwindung der hämatologischen Toxizität von Chemotherapie
Zellkonzentration im peripheren Blut
ZeitTBI Mel
Mel
Myelo.
Lymp.Monozyten
StammzellenT-Zellen
NK-Zellen
Myelo.
Lymp.
Infektprophylaxebakteriell viral
antineoplastischMyeloablativ ?
Plasmocytomkonventionelle Chemotherapie: Ergebnisse
N CR (%) Reduktion Paraprotein < 50%
Mediane Überlebenszeit (Monate)
Anteil 5-Jahres Überleben (%)
Standardtherapie Mel/Pred (SWOG) 335 0 40 26 18 VMCP/VBAP (SWOG) 115 0 53 36 30 VBMCP (ECOG) 220 0 72 30 26 VAD (Alexanian) 175 0 55 36 30 Dexa (Alexanian) 112 0 43 36 -
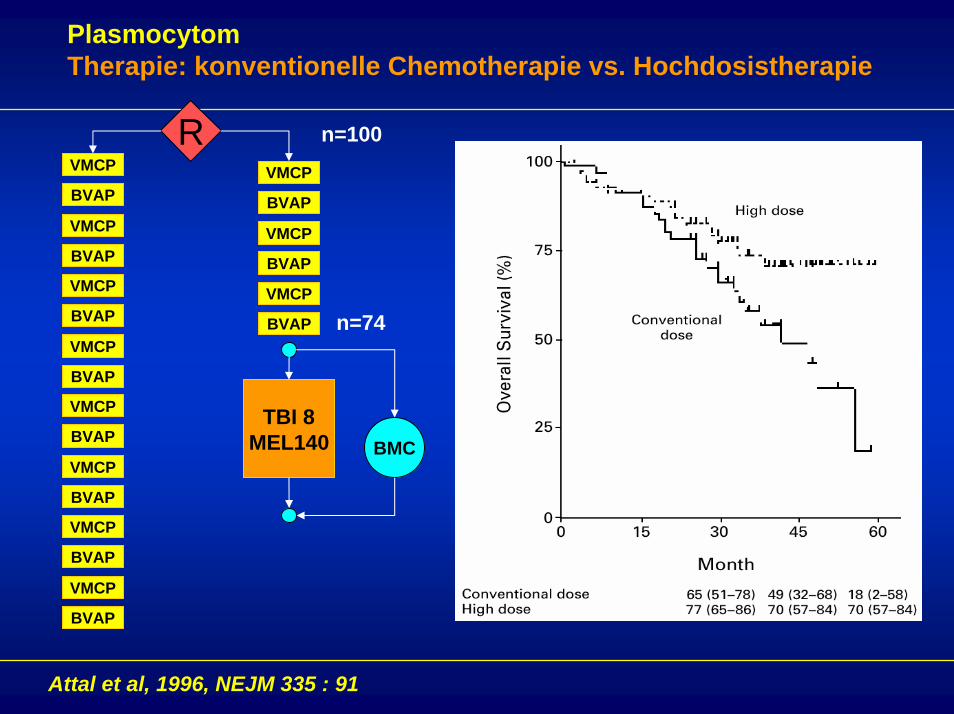
Hochdosistherapie Mel/TBI (Attal) 100 22 81 60+ 52 Mel (Powles) 195 53 79 54 40 Doppel HDT (Barlogie) 123 40 85 62+ 60
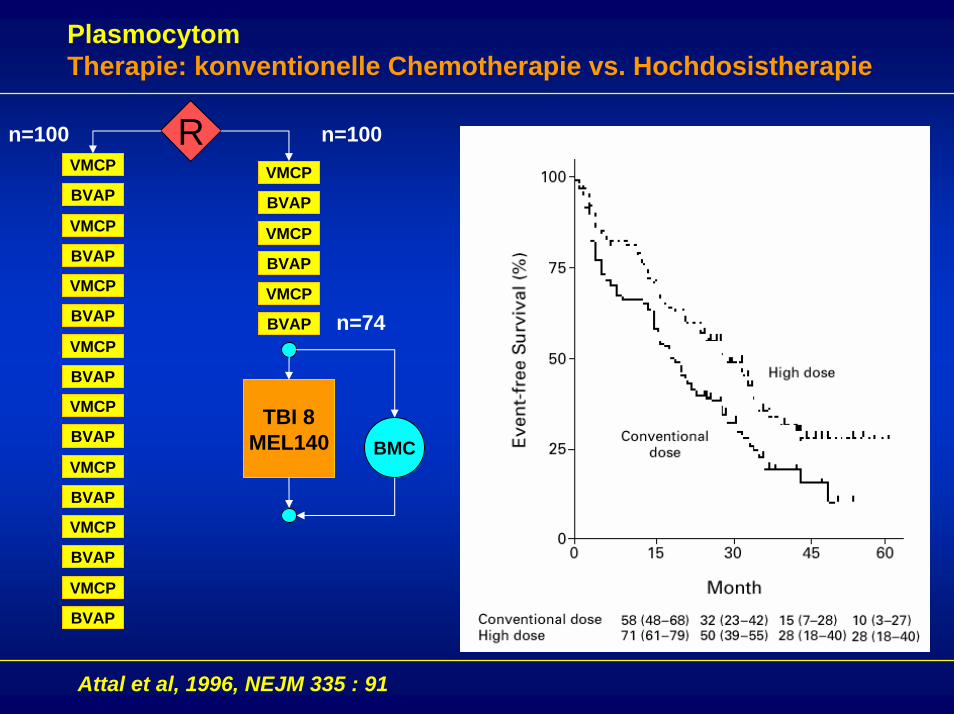
PlasmocytomTherapie: konventionelle Chemotherapie vs. Hochdosistherapie
n=100
TBI 8MEL140 BMC
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
R n=100
n=74
Attal et al, 1996, NEJM 335 : 91
PlasmocytomTherapie: konventionelle Chemotherapie vs. Hochdosistherapie
TBI 8MEL140 BMC
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
VMCP
BVAP
R n=100
n=74
Attal et al, 1996, NEJM 335 : 91
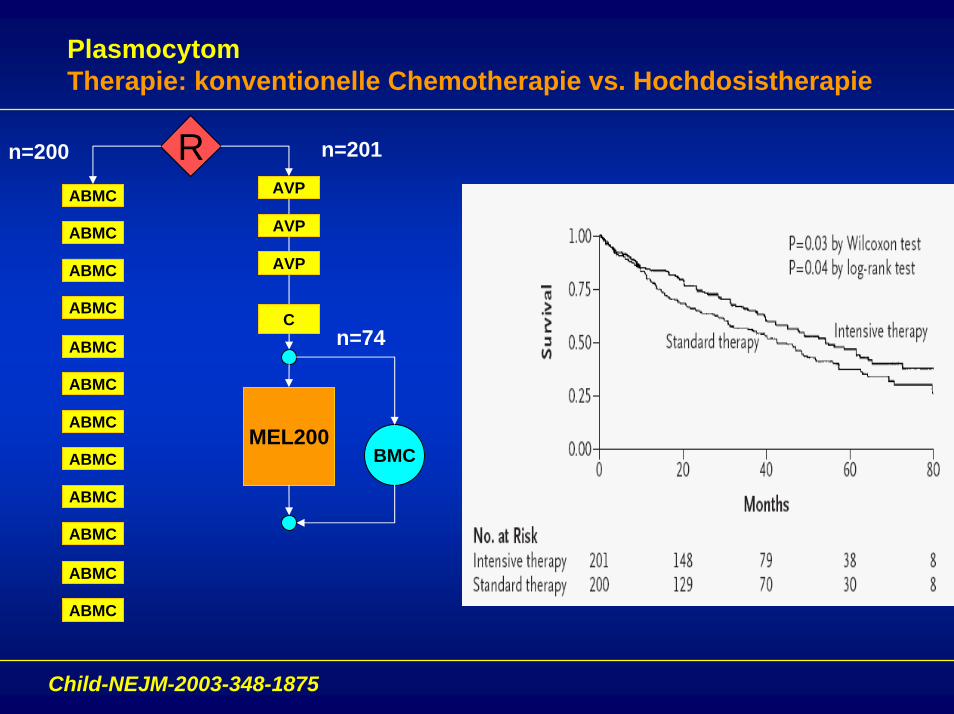
PlasmocytomTherapie: konventionelle Chemotherapie vs. Hochdosistherapie
n=200
MEL200BMC
ABMC AVP
R n=201
n=74
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
AVP
AVP
C
Child-NEJM-2003-348-1875
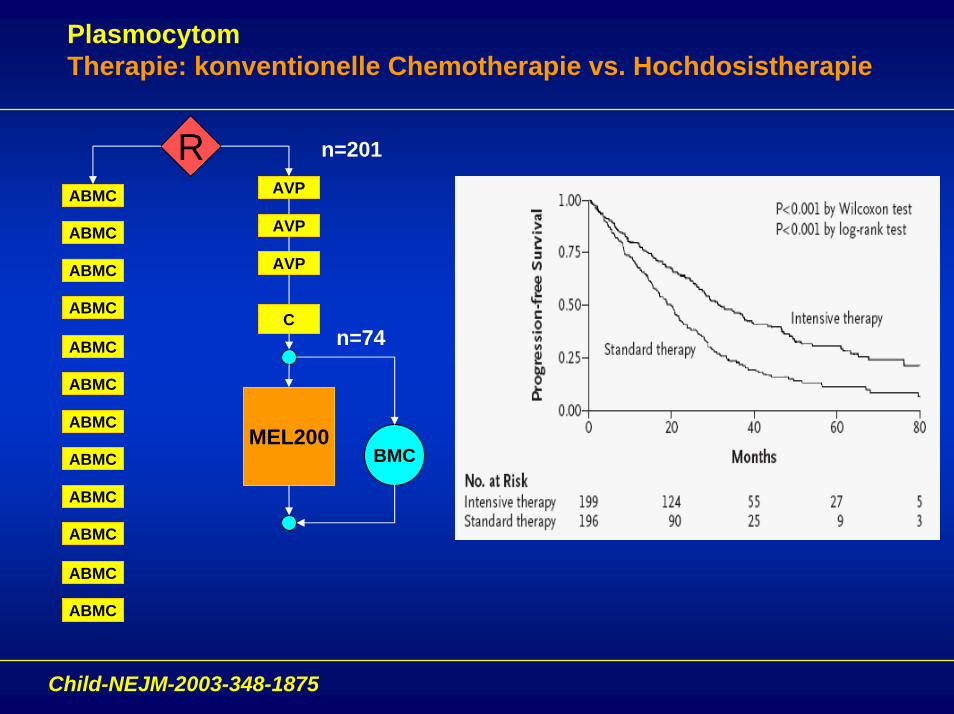
PlasmocytomTherapie: konventionelle Chemotherapie vs. Hochdosistherapie
MEL200BMC
ABMC AVP
R n=201
n=74
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
ABMC
AVP
AVP
C
Child-NEJM-2003-348-1875
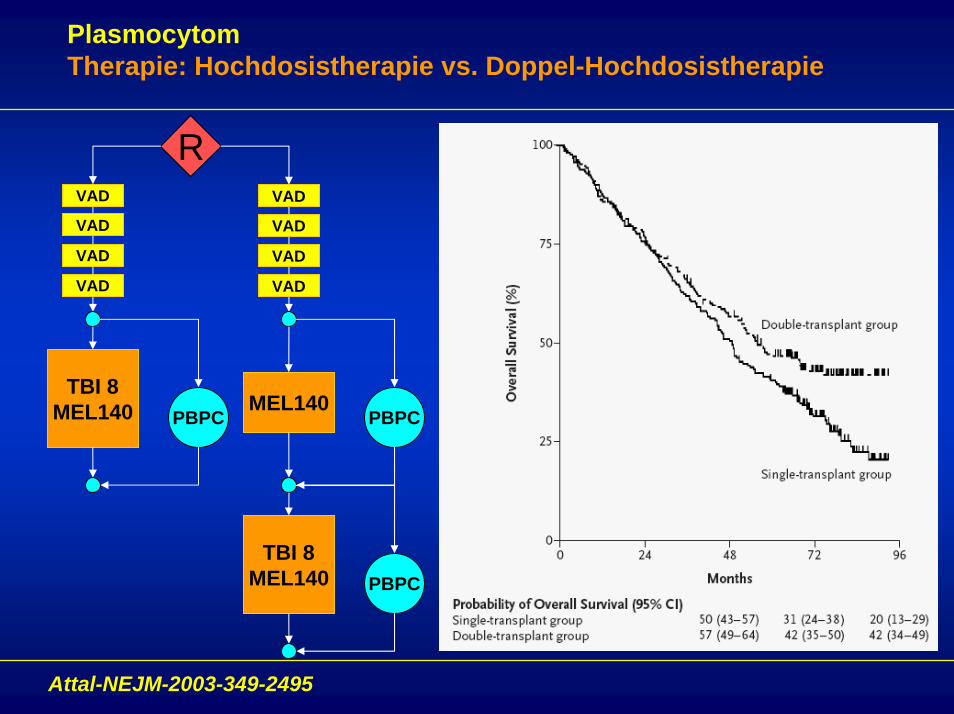
PlasmocytomTherapie: Hochdosistherapie vs. Doppel-Hochdosistherapie
Attal-NEJM-2003-349-2495
VAD
R
VAD
VAD
VAD
VAD
VAD
VAD
VAD
TBI 8MEL140 PBPC
MEL140PBPC
TBI 8MEL140 PBPC
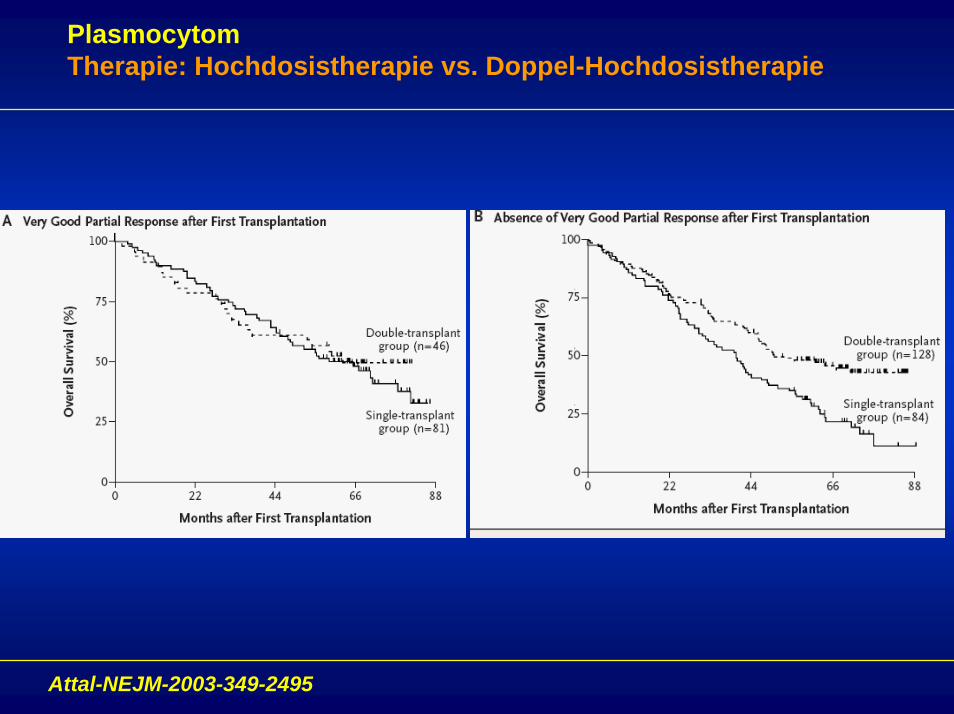
PlasmocytomTherapie: Hochdosistherapie vs. Doppel-Hochdosistherapie
Attal-NEJM-2003-349-2495
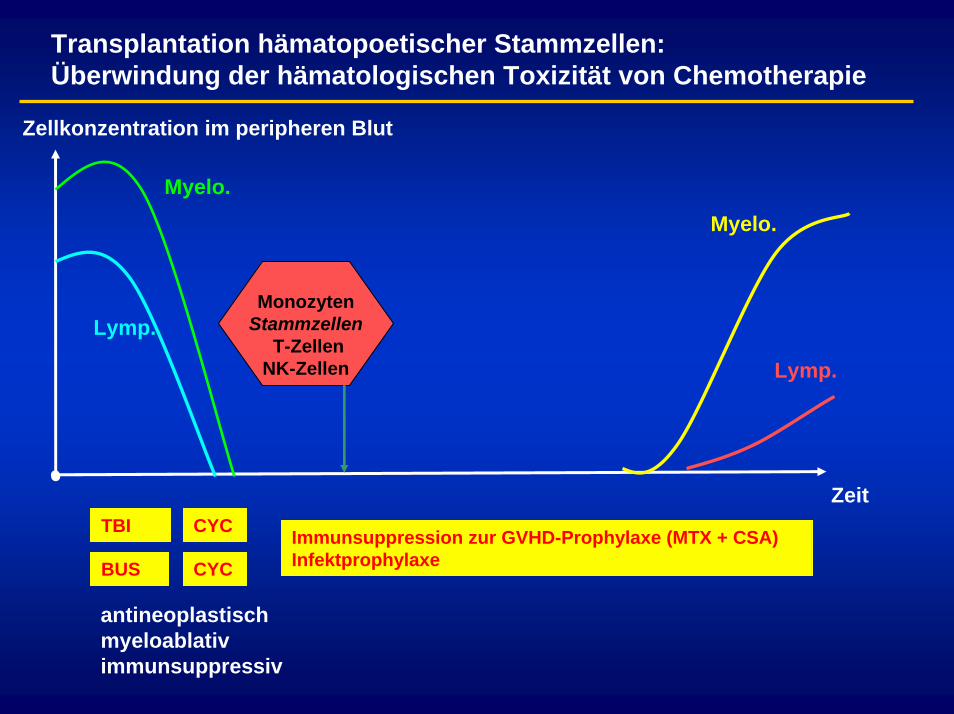
Transplantation hämatopoetischer Stammzellen:Überwindung der hämatologischen Toxizität von Chemotherapie
Zellkonzentration im peripheren Blut
ZeitTBI CYC
BUS CYC
Myelo.
Lymp.Monozyten
StammzellenT-Zellen
NK-Zellen
Myelo.
Lymp.
Immunsuppression zur GVHD-Prophylaxe (MTX + CSA)Infektprophylaxe
antineoplastischmyeloablativimmunsuppressiv
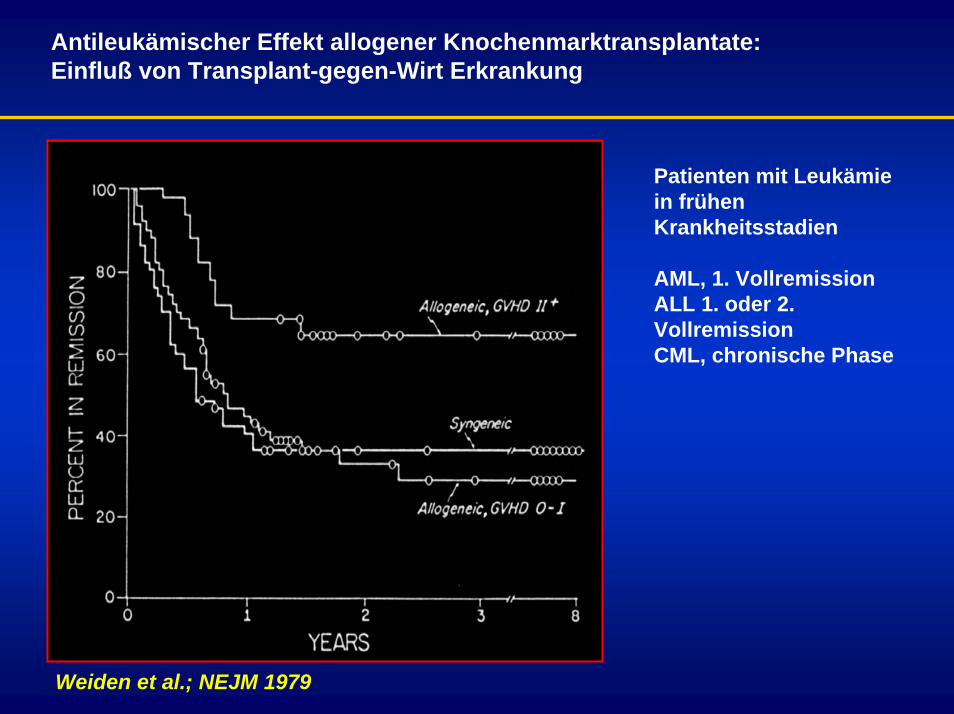
Antileukämischer Effekt allogener Knochenmarktransplantate:Einfluß von Transplant-gegen-Wirt Erkrankung
Weiden et al.; NEJM 1979
Patienten mit Leukämie in frühen Krankheitsstadien
AML, 1. VollremissionALL 1. oder 2. VollremissionCML, chronische Phase
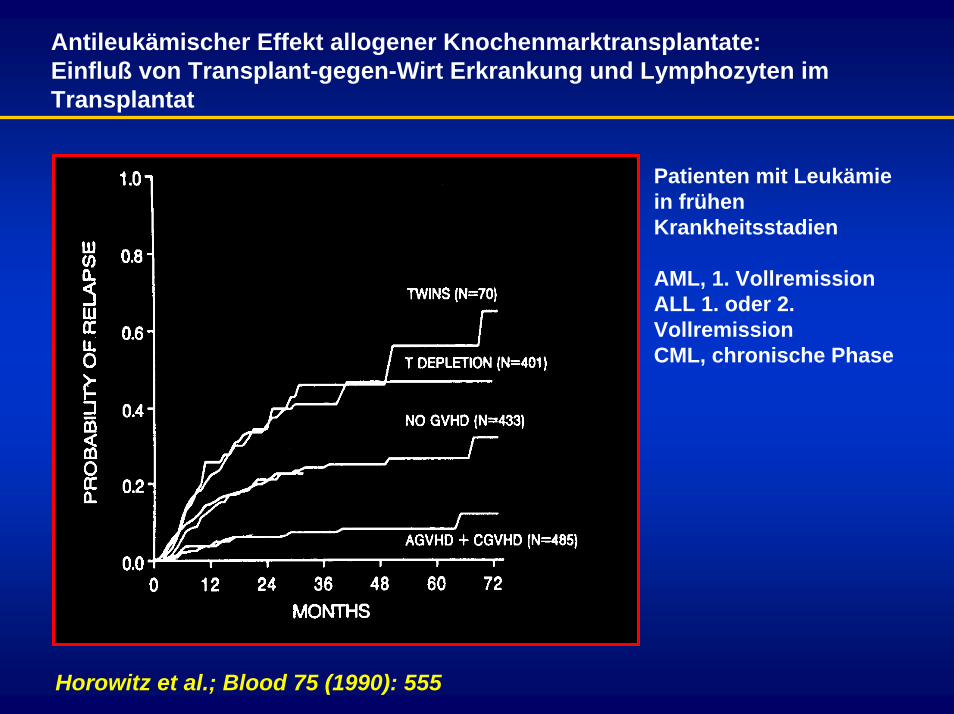
Antileukämischer Effekt allogener Knochenmarktransplantate:Einfluß von Transplant-gegen-Wirt Erkrankung und Lymphozyten im Transplantat
Patienten mit Leukämie in frühen Krankheitsstadien
AML, 1. VollremissionALL 1. oder 2. VollremissionCML, chronische Phase
Horowitz et al.; Blood 75 (1990): 555
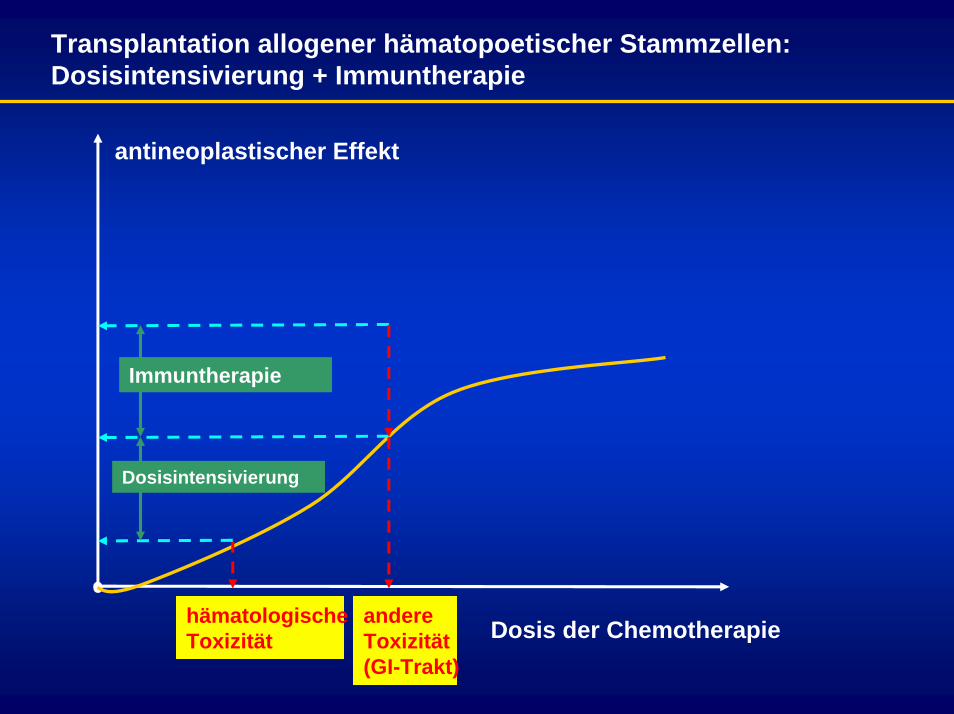
Transplantation allogener hämatopoetischer Stammzellen:Dosisintensivierung + Immuntherapie
antineoplastischer Effekt
hämatologische Toxizität
andere Toxizität(GI-Trakt)
Dosisintensivierung
Immuntherapie
Dosis der Chemotherapie
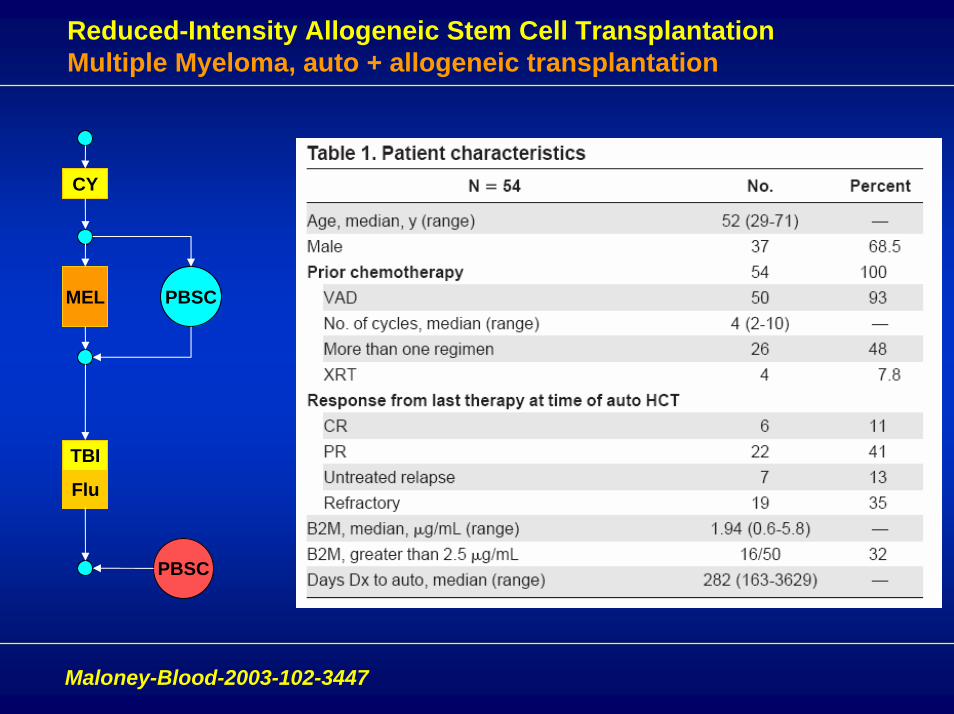
Reduced-Intensity Allogeneic Stem Cell TransplantationMultiple Myeloma, auto + allogeneic transplantation
MEL
CY
PBSC
TBI
Flu
PBSC
Maloney-Blood-2003-102-3447
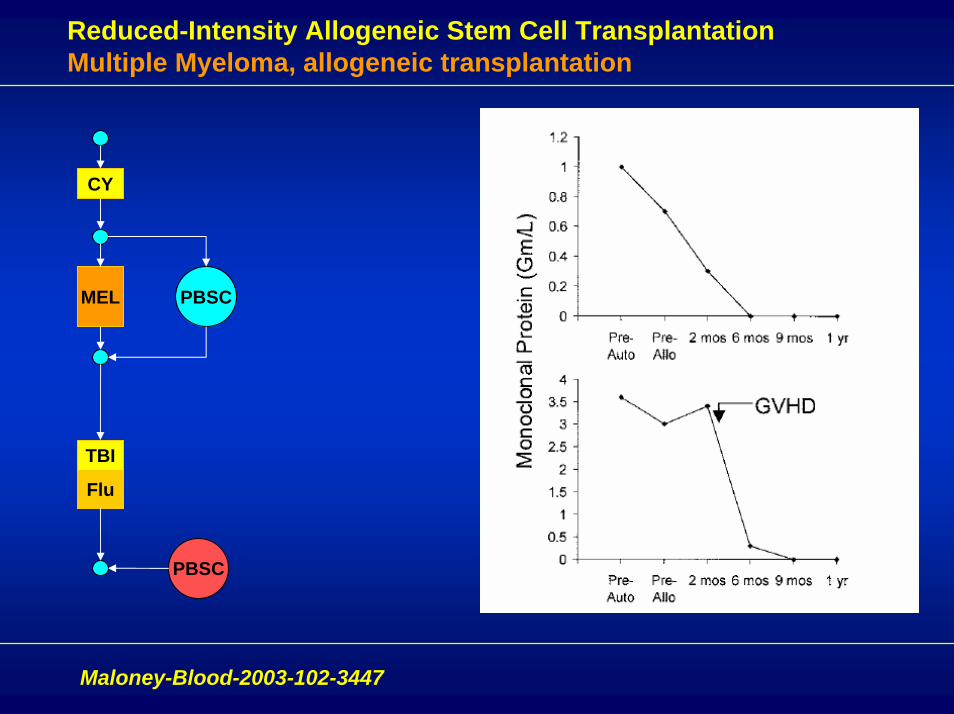
Reduced-Intensity Allogeneic Stem Cell TransplantationMultiple Myeloma, allogeneic transplantation
TBI
Flu
PBSC
MEL
CY
PBSC
Maloney-Blood-2003-102-3447
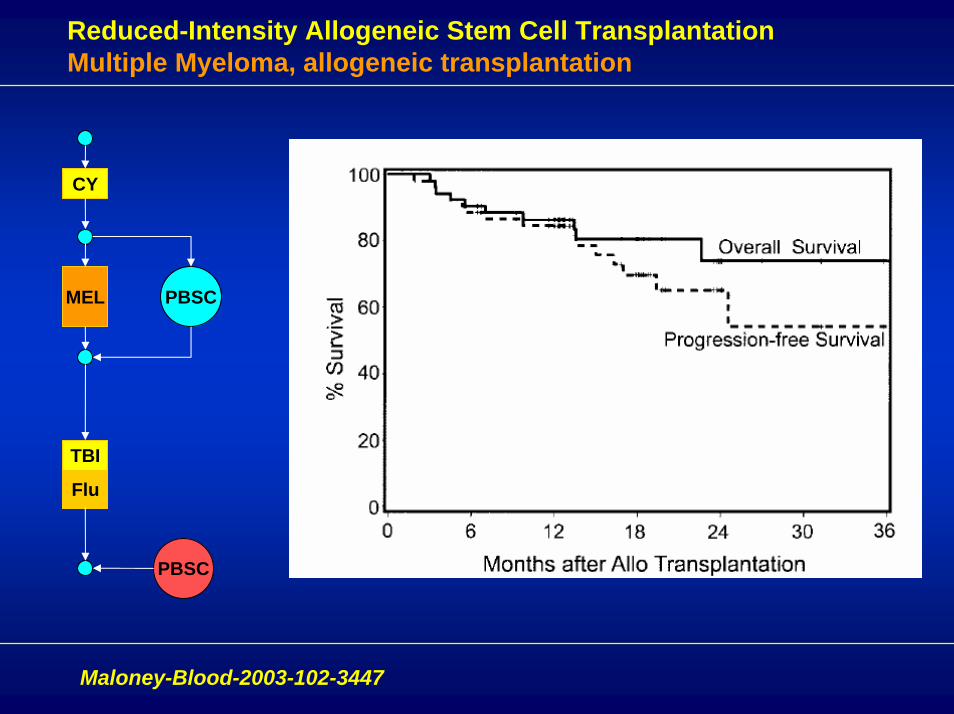
Reduced-Intensity Allogeneic Stem Cell TransplantationMultiple Myeloma, allogeneic transplantation
TBI
Flu
PBSC
MEL
CY
PBSC
Maloney-Blood-2003-102-3447
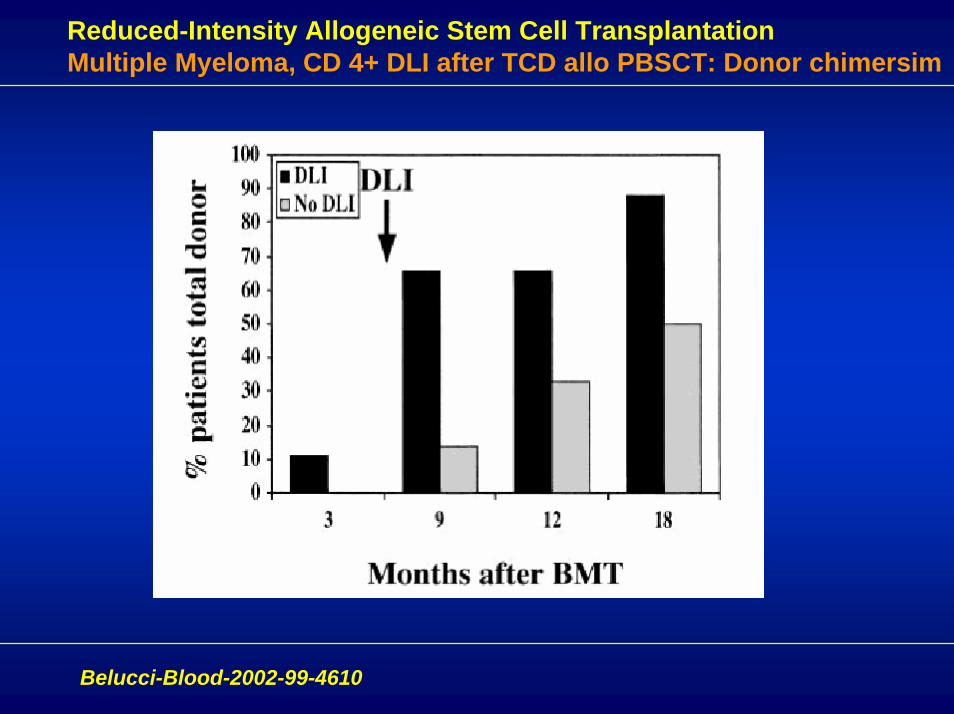
Reduced-Intensity Allogeneic Stem Cell TransplantationMultiple Myeloma, CD 4+ DLI after TCD allo PBSCT: Donor chimersim
Belucci-Blood-2002-99-4610
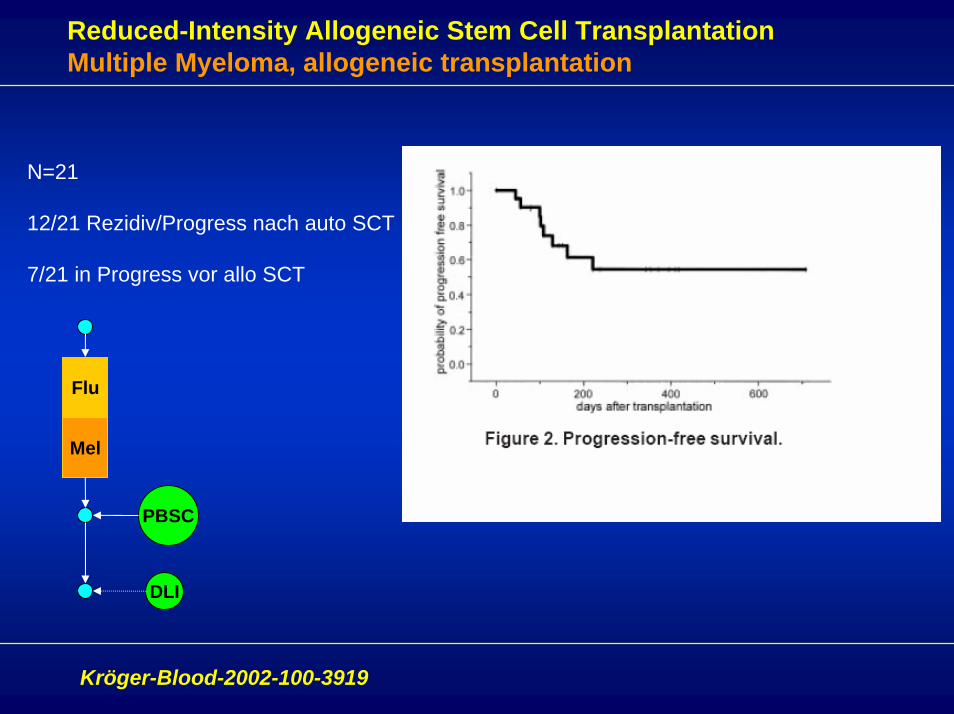
Reduced-Intensity Allogeneic Stem Cell TransplantationMultiple Myeloma, allogeneic transplantation
N=21
12/21 Rezidiv/Progress nach auto SCT
7/21 in Progress vor allo SCT
Flu
Mel
PBSC
DLI
Kröger-Blood-2002-100-3919
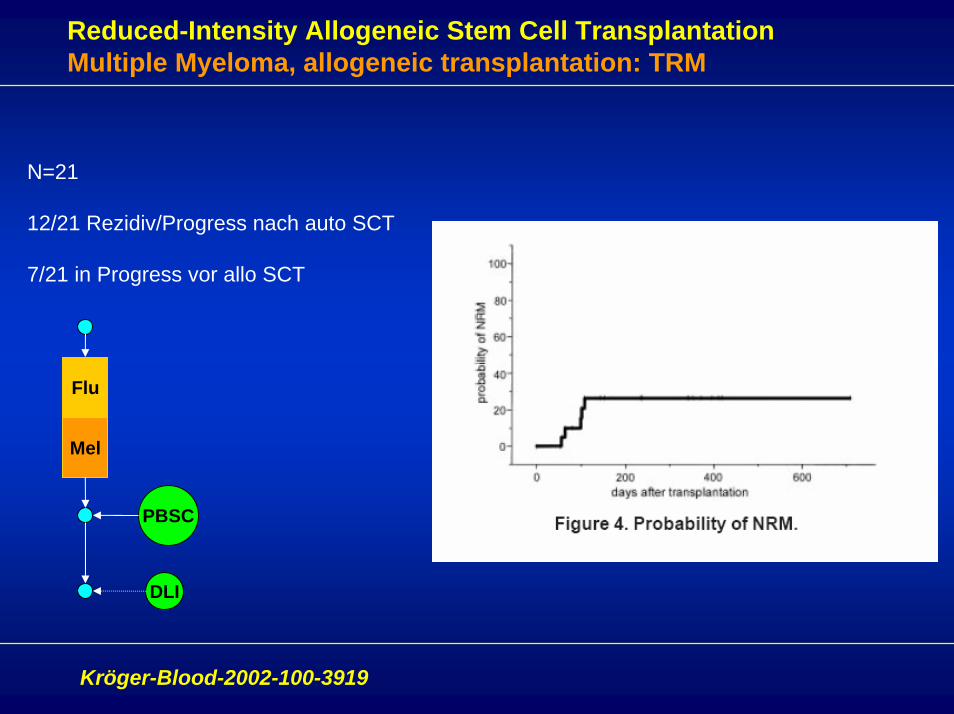
Reduced-Intensity Allogeneic Stem Cell TransplantationMultiple Myeloma, allogeneic transplantation: TRM
N=21
12/21 Rezidiv/Progress nach auto SCT
7/21 in Progress vor allo SCT
Flu
Mel
PBSC
DLI
Kröger-Blood-2002-100-3919
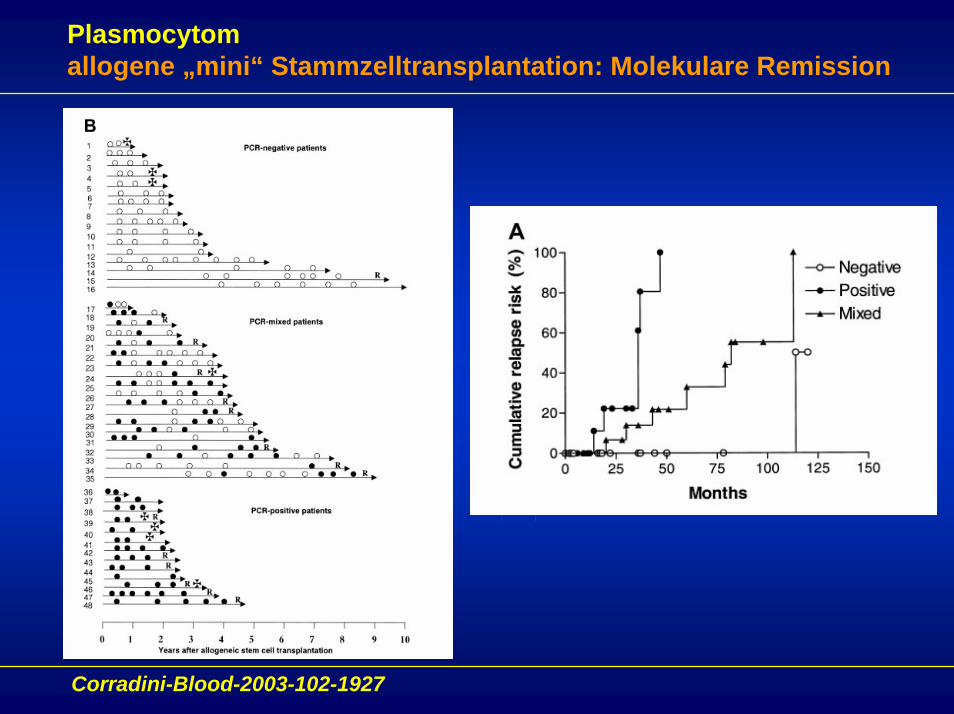
Plasmocytomallogene „mini“ Stammzelltransplantation: Molekulare Remission
Corradini-Blood-2003-102-1927
PlasmocytomZusammenfassung systemische Therapie
Konventionell dosierte Chemotherapieaktive Substanzen: Melphalan, Anthrazykline, Steroidepalliatives Therapieziel: Beseitigung von Symptomen, Lebensverlängerung ?
Hochdosistherapie + autologe Transplantationeinfach- oder doppel- HDT, Durchführbarkeit bis ca. 70 Jahrepalliatives Therapieziel in der Mehrheit der Patienten, Lebensverlängerung möglich, kleinere Gruppe mit Langzeitremissionen ?
Allogene Stammzelltransplantationzelluläre Immuntherapie des Plasmocytomskuratives Ziel für eine Subgruppe von Patienten erreichbar.hohe therapieassozierte Morbidität und Mortalität
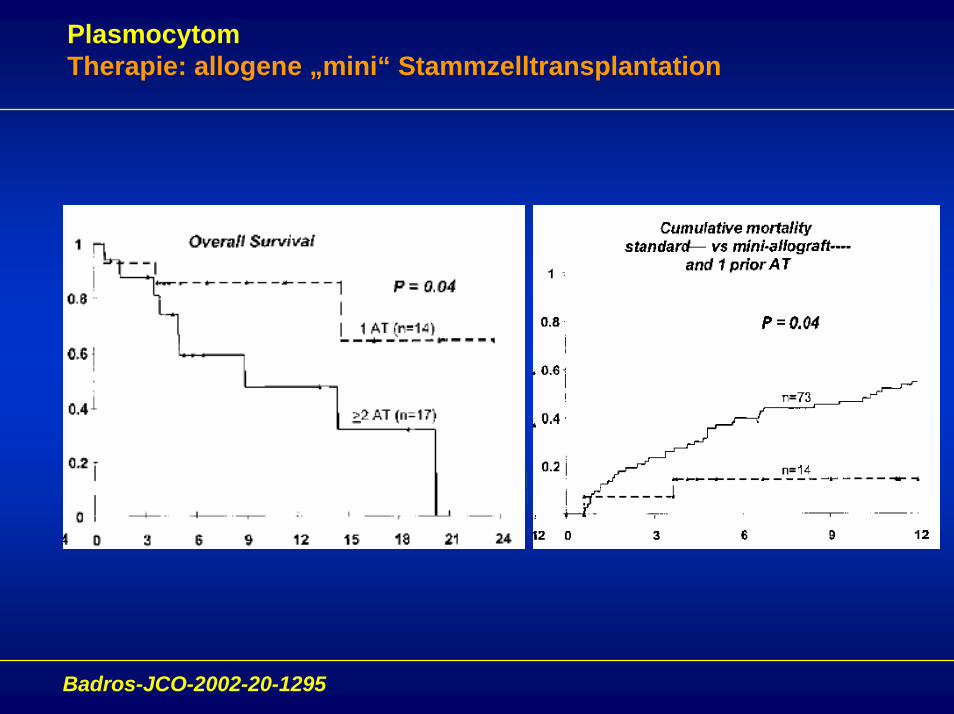
PlasmocytomTherapie: allogene „mini“ Stammzelltransplantation
Badros-JCO-2002-20-1295
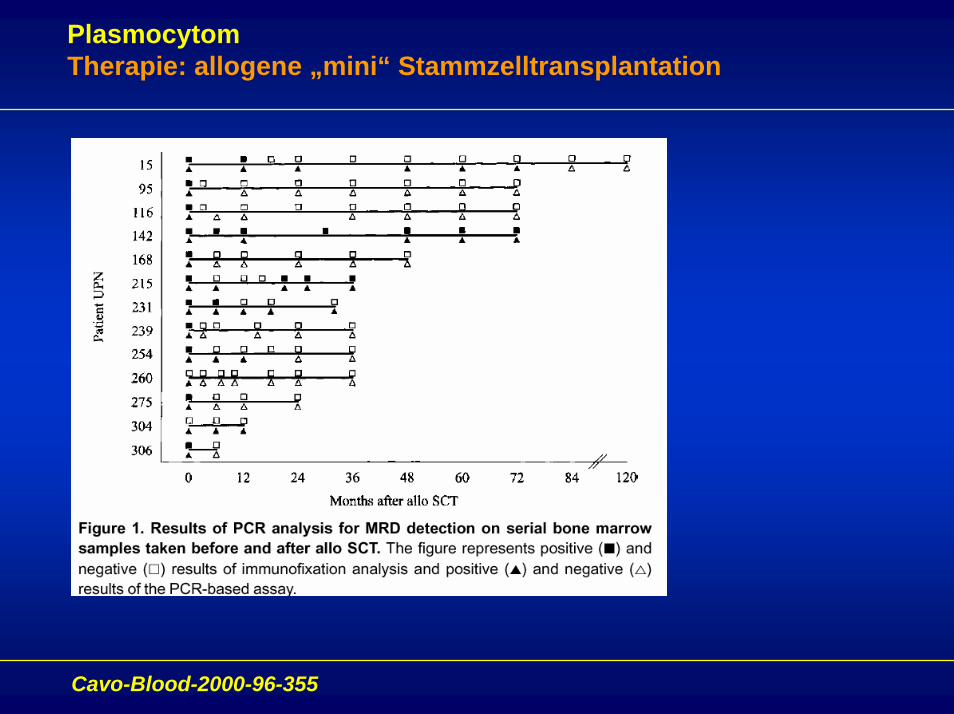
PlasmocytomTherapie: allogene „mini“ Stammzelltransplantation
Cavo-Blood-2000-96-355
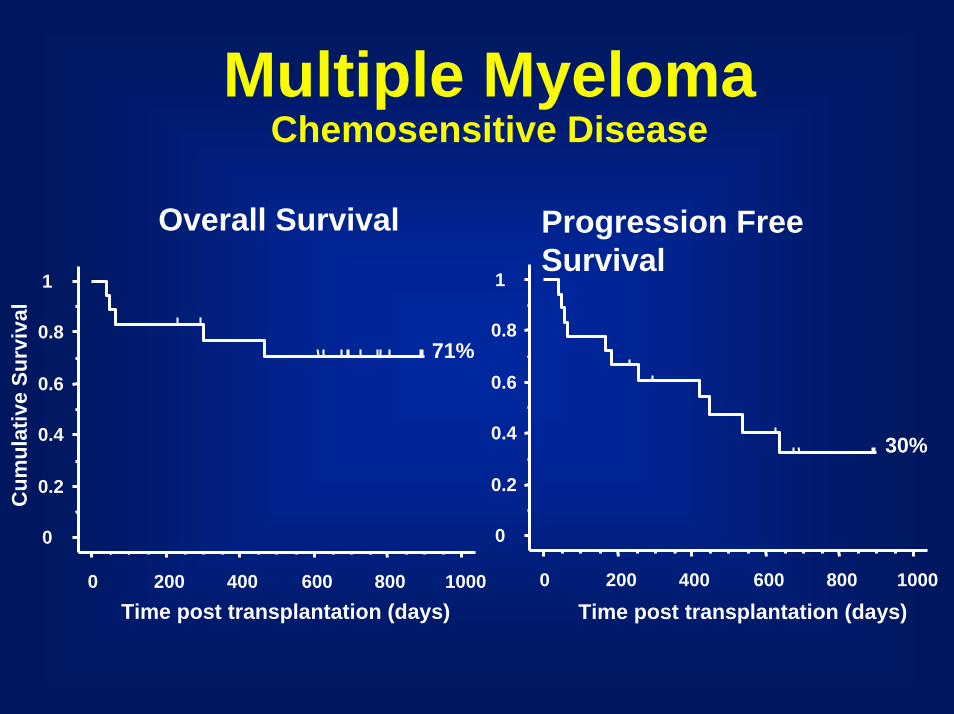
Multiple MyelomaChemosensitive Disease
Overall Survival Progression Free Survival
0
0.2
0.4
0.6
0.8
1
0 200 400 600 800 1000
71%
0
0.2
0.4
0.6
0.8
1
0 200 400 600 800 1000
Time post transplantation (days)
30%
Time post transplantation (days)
Cum
ulat
ive
Surv
ival
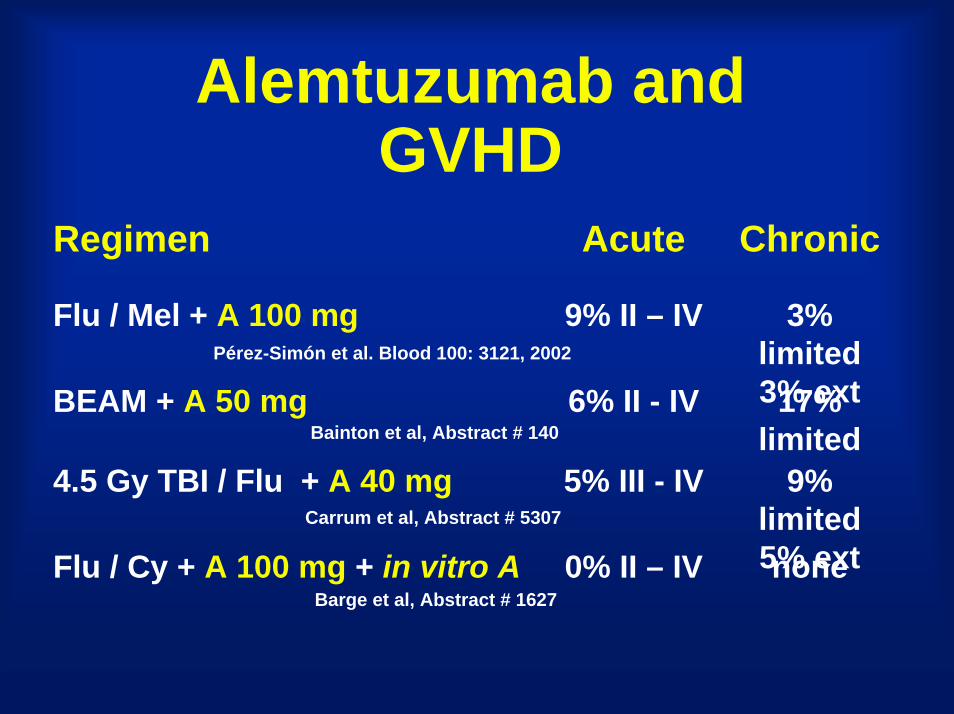
Alemtuzumab and GVHD
Regimen Acute Chronic
Flu / Mel + A 100 mg 9% II – IV 3% limited 3% extBEAM + A 50 mg 6% II - IV 17% limited
4.5 Gy TBI / Flu + A 40 mg 5% III - IV 9% limited 5% ext Flu / Cy + A 100 mg + in vitro A 0% II – IV none
Bainton et al, Abstract # 140
Pérez-Simón et al. Blood 100: 3121, 2002
Barge et al, Abstract # 1627
Carrum et al, Abstract # 5307
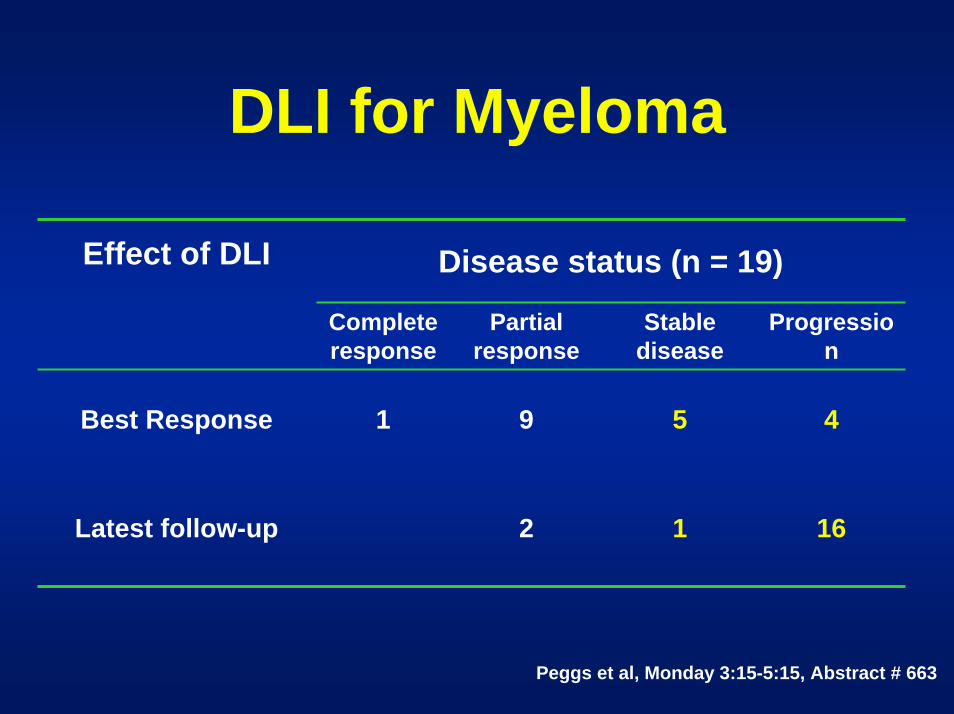
DLI for Myeloma
Disease status (n = 19)Effect of DLI
Complete response
Partial response
Stable disease
Progression
Best Response 1 9 5 4
Latest follow-up 2 1 16
Peggs et al, Monday 3:15-5:15, Abstract # 663
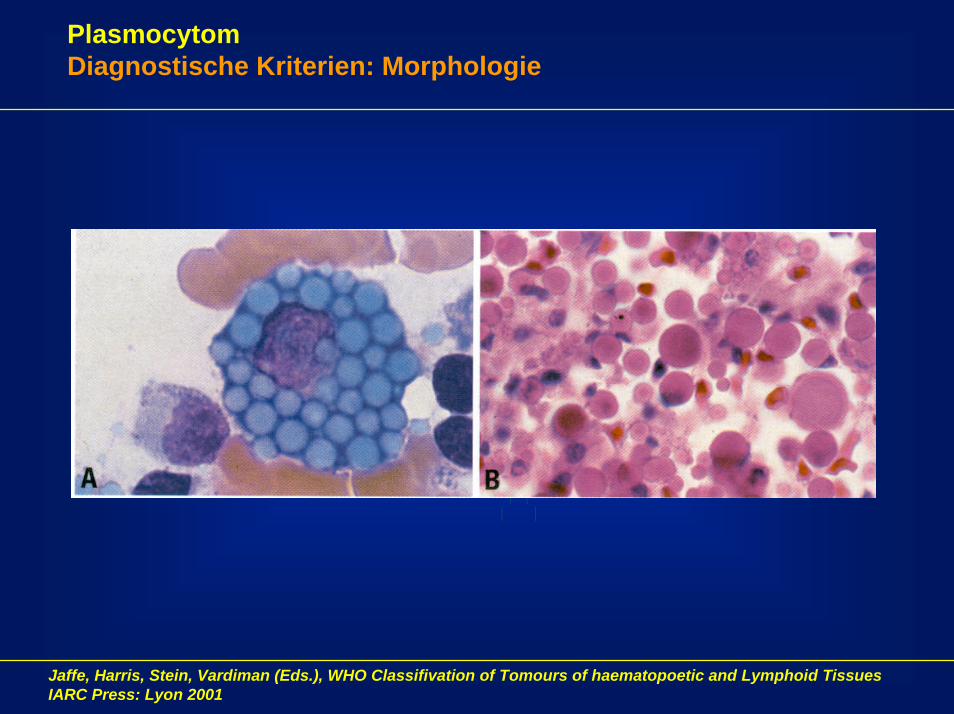
PlasmocytomDiagnostische Kriterien: Morphologie
Jaffe, Harris, Stein, Vardiman (Eds.), WHO Classifivation of Tomours of haematopoetic and Lymphoid TissuesIARC Press: Lyon 2001
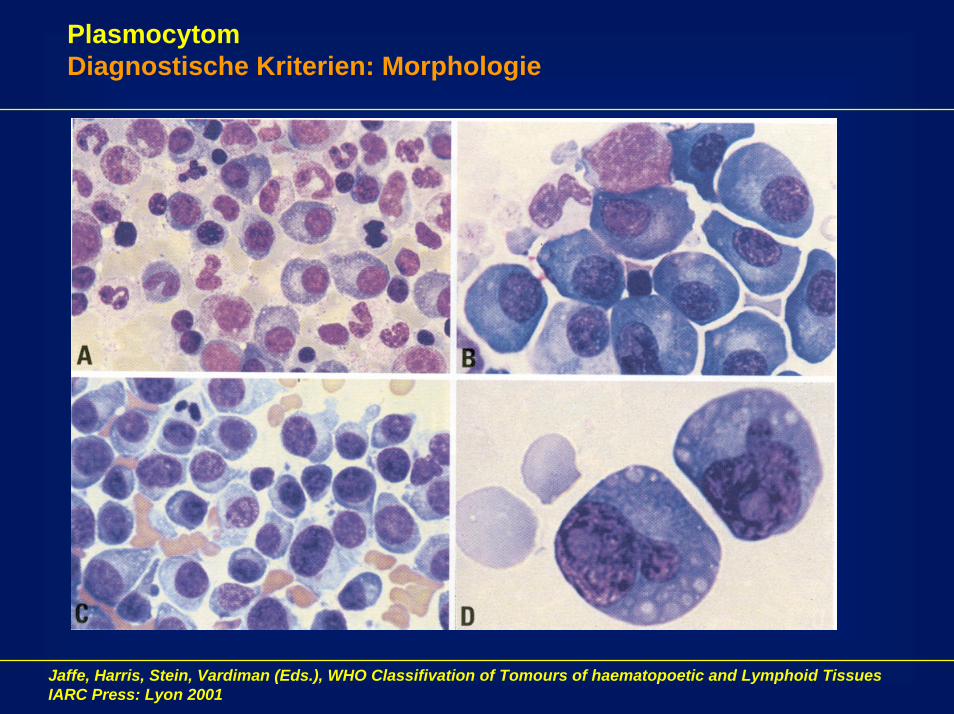
PlasmocytomDiagnostische Kriterien: Morphologie
Jaffe, Harris, Stein, Vardiman (Eds.), WHO Classifivation of Tomours of haematopoetic and Lymphoid TissuesIARC Press: Lyon 2001
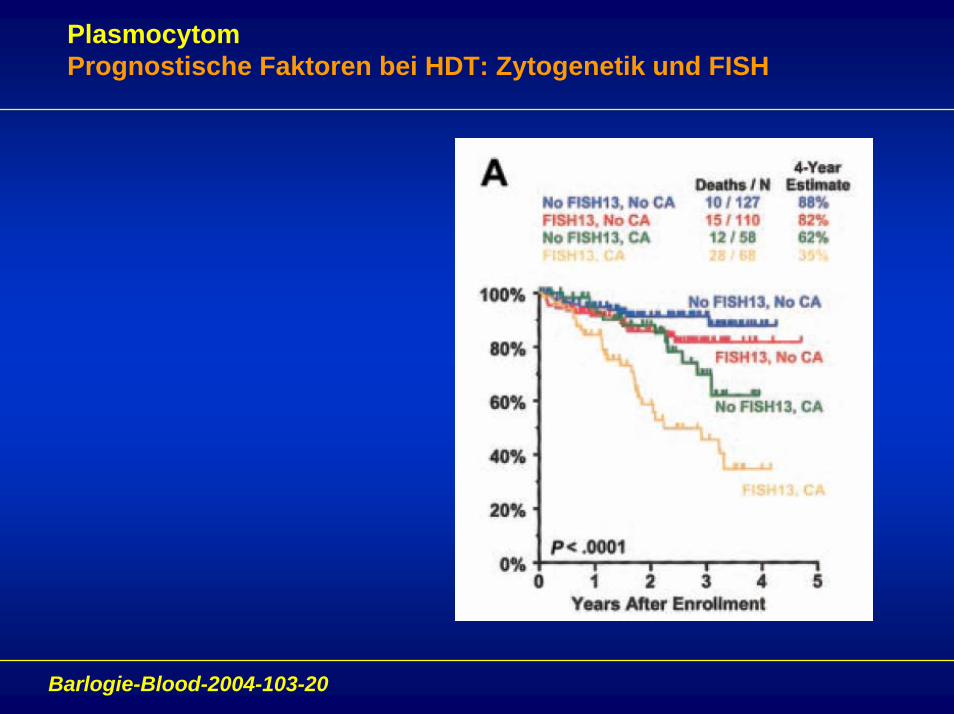
PlasmocytomPrognostische Faktoren bei HDT: Zytogenetik und FISH
Barlogie-Blood-2004-103-20
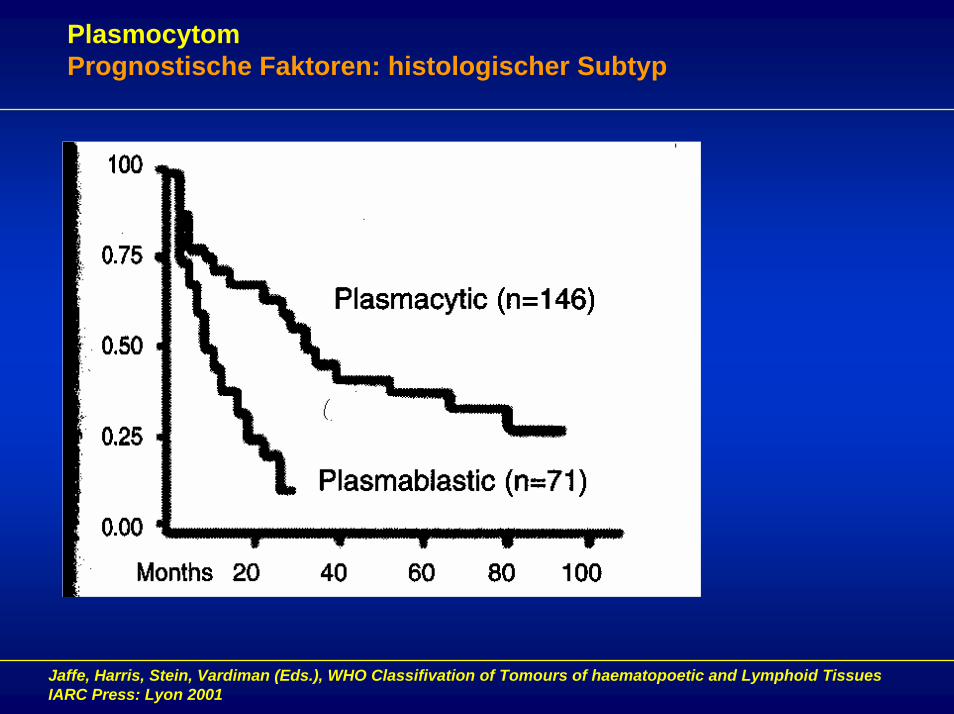
PlasmocytomPrognostische Faktoren: histologischer Subtyp
Jaffe, Harris, Stein, Vardiman (Eds.), WHO Classifivation of Tomours of haematopoetic and Lymphoid TissuesIARC Press: Lyon 2001