Embed Size (px)
Citation preview
Zbl. Bakt. Hyg., I.Abr. Orig. A 255, 38~391 (1983}
A Solid-Phase Indirect Haemadsorption Assay (SPIHA) for
Detection oflmmunoglobulin M Antibodies to Toxoplasma gondii:
Application to Diagnosis of Acute Acquired Toxoplasmosis
Ein lndirekter Festphasen-Hamadsorptionstest (SPIHA) zum Nachweis von IgM-Antikorpem gegen Toxoplasma gondii: Anwendung in der Diagnostik akuter Toxoplasma-lnfektionen
KURT HF.RMENTIN, OTTO PICHER, HORST ASJ>OCK, HERBERT AllER • . md ANDREAS HASSL
:\brc:ilung ftir Mc:dizinischc: Parasirologic (l.circr: Prof. Dr. H .• <lspock) de-. Hygic:ne-lnstiturc:s dcr Univcrsirar Wicn {VorsranJ: Prof. Dr. H. Flamm)
\\ 1rh 2 Figures • Received December 20, 1982
Abstract
:\ 'olid-ph.asc indirect h.1cm:ul~orption aso;ay (Sl'IHAl for the dct~ction of immuno· !',lohulin M (I~M) :mtibod1cs to Toxopl.uma gmulii i~ dcscribt·d. Polystyrol mkrutno.·r plate~ .uc ..:onred with .u11i-human l~M (,u-chain-<;pcdlic) :mtibodics .1nd then scqucnriall~ :~.llmvcJ to rc:tcl \~ilh pariem'>~<;crum anc.! !.hccp c:rythrocytc:-. 'cn•iti7c:d With soluble: :antiJ!o:n of TuxnfJ/,r!'m.J gonJu. A tot.ll of Ill ~ra were tc'itt•J in tluore!>~nt 3ntlbody tC\1 (FAT .tnJ lg.M-1- .\'1), complement tixauon tc<ot (CF'T), inderc:CI h;u:m.t~gluun.auon .1ssay (IHA), .tnJ m SPIHA. 47 'er.t Wt're frum inJi, idual' wnh a '"~pc.:tc:d or \'c:rdic:d :Kutc '1 Hxop;,,,,.,,, infection. In most of thC$ C C;l~CS the SI11HA alluwcd ;\ cl<·ar interpretation with rc~r~·.:r Ill
:h:: ~t;ltus of the infection. even wht.:n the I~M-FAT "a' not cundusi\c. In cuntr.t•r ru lg~t-1-:\T, rhcu111atoed factor or c"o:ccdin~l)' high 'PCCifi.: I)!G :uHibodi~' o.hd nor mrc:rh:re with rl'!iulr~ m SPIH.\. i\ !.lbor.ll<•rr ·aC'<.lutrcJ 1nt.:.:uon ~."n.lhlc:J us tu demCin,fr.tr.· th.: O:OUI!>I.' of tmmunc fC'f'Oihl.' mca~urcJ b~ ~I'll{.-\ ,1< well .1< hy ~~~t-FA r. F :\ T, Cfl .. tnd IHA. 1'hc method propc>sl.'o.l hc:rc: t) wc:ll arpropri.llt•J w 1 !!~\ <.lcrcction. sunplc to l'ntnrm. inexpensive, :md thu~ reprc,cnting .Ill alrcrn.tt h·c: 111 lj~..M-f r\ T, .. unvc:nit·nt for th<.· ro HlltnC
labot.ltllr~·.
Zu!.ammenfassung
Ein lndirekter Fc:~tJ'hasen·H:im:u.lsorptiOn~tcst (SI•IHA} zum :'\.Kh'l\c:is \on 111-~t- .\nn·
ko r{M:rn gegco roxopl.lsm,, ~mldll Wtrd bc:Khnc:bc:n. Dcr Tc:-.r umfJSt 1. d·~ ~ld..mo.· .~J
<;Otpttl)ll de:r lg.M·.\nu'kl\rpcr .lU• Jc:m Parecntenwrum Jn ~hkrntl!erpbttc:n, d1( nut .1n!l·
hum:J.ncn lg~\-Anukurpern bc:schechrct 'ltnd, und .::. du: Rc:aknnn d~r ~pailischcn ~~~~-
Indirect Haemadsorption Assay for Toxoplasma 381
J\ nrikorpcr mit f.rythrozyten, welch.c mit Antigen von Toxoplasma go,dii scnsibilisic:rt sind. tnsgc:s:tmt wurden 111 Seren im lndirckten [mmuniluorcszenztest (FAT und lgM·FAT), in dcr Komplcmcntbindungsreahion (CFT), im lndirckten Himagglutinadonstcst (IHA) und im SPIHA getestct. 47 Sc:ren davon stammten \'On Personen mit cincr ' 'Ctmuteu:n odcr wrifitienen akutc:n Toxopla.sma-lnfekrion. In den mcisren d.ieser Faile erlaubtc der SPIHA eim: klatc: Aussage iibcr den Status dt:r lnfektion, und zwar auch in jenc:n Fallen, in dem:n mirrcls lgJ\tt-FAT keine schlussige Aussagc moslich war. lm Gcgcnsatz zum lgM-FAT kon.ntc: im SPil-lA keine Becinflu.~ung der Ergebnisse durch Rheumafaktor oder durch hohe Titer spezi6scher lgG·Anriko rper fcstgesrcllt werden. Einc Laborinfektion ermi5g· Iichte uns o;ljc: lkobachmng des Verl.1ufs dcr lmmunanrworr nach der lnfekrion, gemcsscn im SPIHA. lgM·FAT. FAT, CFT und IHA. Die hicr dar~csrellre Mcrhod.c isr fur den lgM~;H:hweis gur gc:eignet, sic isr einfach dur.:::hzufiihrcn und au~rdem :auch billig. Aile fiir die Durchfiihrung des Tests notwe.ndigen Materialicn sind im Handel crh3lrl ich. Somit srcllt dic:sc Methode cine fUr das Routinclabor gccignete Alternative zum lgM-FAT dar.
Introduction
The detection of specific immunoglobulin M (lgM) antibodies is a well known tool for the diagnosis of a. variety of :.tcute infectious diseases. With respect to tox:o· plasmo~is rl1c detection of specific IgM and, hence, the identification of a recently acquired Toxoplasma infection may be important in three clinical situations (\Velcb et al. , 1980) : l ) in patient.'> with debil itating or lifc·threating illness, 2) in patients with syndromes such as lymphadenopathy that must be distinguished from lymphoprolifcnltivc disorders, and 3) jn pregnant women.
The most con1mon serological tesrs tor the detection of hum'ln lgM antibodies to Toxoplasma go11dii use anti·llUman lgM conjugates in «indirect assays" such as fluorescent antibody test (FAn (R.:mingtott et al. , 1968), enzyme-linked immunosorbem assay (ELISA) (Voll~r et al. , 1976), radioimmunoassay (RIA) (Gehle et al., 1976). However, false-positive reactions ma)' be obtained in thC$C tests due to the presence of rheumarojd factor (RF) (Camargo et al., 1972; Hyde et al. , 1975) or antinuclear antibodies (ANA) (Araujo ct al. , 1971). Conversely, falsc-ncg:uivc results or weakened positive reactions arc likdy w occur in sera presenting high concentrations of specific, competith'e anti-parasite lgG antibodies which rapidly s:nuratc the binding sites of the amjgcn and thereby inhibit the binding of specific IgM (Cohm ct al., 1967 ; l:ifice ct al. , 1980; Frmzco ct al., 1981; Py11diah et al., 1979).
Recently several assays have been performed in toxoplasmosis serology m:1king usc of a S()lid-phase immunological entrapment of lgM: double sandwich lgMELISA (Duermeyer et al., 1980; Naot and Remingtm:, 1980; Remington, 1982), IgM-imnmnosorbent agglutination assay (Desmonts et al., 198'1; Desmonts, 1982), reverse enzyme immunoassay (Fmnco ct al., l 981; Walls and Franco, 1982). These tests are described to be more st~nsitivc and more specific th:m the lgM-FAT, although easy to perform and inexpensive.
Our :tims were, firstly, to take advantage of the initial step of these assays in which at first the patient's lgM and subsequently the patient's ami-parasite lgM are sch.:ctcd; thus, interference of RF or ANA as well as antibody competition due to excess of specific IgG is hindered.
Secondly, we attempted to .find a test system which i.o; nor so much rime consuming and intensive in work as e.g. the double sandwich lgM-ELISA is. ..
For this purpose we inrcndcd to apply a haemadsorprion technique (which has
2S Zbl. lbltt. HrJh J. Abl. Ori&- A 2.SS
382 K.Hcrmentin, 0. 'Picher, H.Aspock, H.Auer, and A. Hassi
been described for detection o£ Rubella lgM antibodies by Krech and Wilhelm, 1979; Vander Logt et al., 1981, and for detection of Treporrema pa/lidum-speci6c lgM by Schmidt, 1980) in toxoplasmosis serology.
Materials and Metbod,s
Microtiter plates: disposable U·shaped polys·ryrol pla1es {Nunc, Kamstrup, Denmu k). Specific antiserum to lmmatt lgM : lgG fraction (,u-chain·sped fic) of rabbit anti-human
JgM. Specimen 1: commerci31ly available anr iserum to human lgM (Be.hringwerke, Marburg,
FR Germany).
-!< WASH
J,
-
erythrocyte, sensitized with antigen
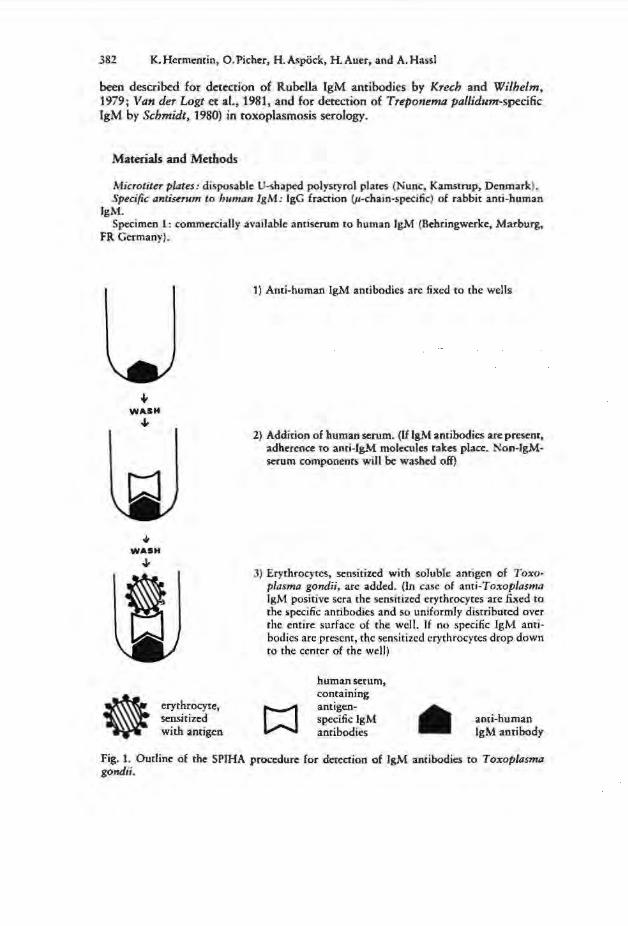
1) Anti-human IgM antibodies arc fixed to the wells
2) Addition of human serum. (If lgM antibodies are present, adherence ro anri-fg.\1 molecules rakes place. Non-lgMscrum components will be: washed off)
J) Erythrocytes, sensitized with soluble antigen of Toxoplasma gondii, arc added. (In case of anti-Toxoplasma lgM positive sera the sensit ized erythrocytes are fixed to the specific ami bodies and so uniformly distributed over rhc entire surface of the well. If no specific IgM amibodies arc present, the sensilizcd erythrocytes drop down ro 1 he ccmcr of the well)
human serum, containing antigenspecific lgM antibodies
anti-human IgM antibody
Fig. l. Outline of the SPIHA procedure for detection of JgM antibodies to Toxoplasma gondii.
Indirect Haemadsorption Assay for Toxoplasma 383
Specimen 2: highly purified antiserum, containing 90% immunoreactive antibodies to human lgM, kindly provided by Bchriogwcrkc.
Human sera: 92 sera of pregnant women, submitted to our laboratory for diagnosis in toxoplasmosis surveillance, l5 sera containing RF, and 4 sera containing ANA were tested in FAT, lgM-FAT, CFT, IHA, and in SPIHA.
Sera with rheumatoid factor were kindly supplied by Dr. ].Kovarik, II. Med. Univ. Klinik, Vienna; sera containing ANA were obtained from the IJ. Univ. Hautklinik, Vienna. Sera with IgM antibodies to Rubella virus were kindly provided by Prof. Dr. Ch.Kunz, lnst. f. Virologic, Univ. Vienna.
Rheumatoid factor was determined and adsorbed by latclC agglutination test (Latex-Rf Reagent, Bchringwerke), consisting of an aqueous suspension of polystyrol particles coated with human lgG. ANA were detected by an indirect fluorescent antibody test, using glass slides coated with baby hamster kidney cells (Behringwerkc).
Antigen: IHA-rcagcnt, consisting of stabilized sheep erythrocytes sensitized with soluble Toxoplasma antigen (Cellognost Toxoplasmosis, Behringwerke).
Coating buff~r: 0.08 M carbonate buffer, pH 9,6, \V ashing buffu (PBS· T-BSA): phosphate-buffered saline (PBS), pH 7.2 + 0.05% Tween
20 (T) + 2'Yo bovine sc:rum albumine (BSA). SPIHA procedure (Fig. 1): Wells of microtiter plates were coated with S011I of rabbit
antiserum to human lgM diluted in 0,08 M carbonate buffer (coating buffer). After overnight incubation at + 4 •c, the plates were washed three cimes for 5 min each in PBS-TBSA and shaken dry. S01tl of the serum dilution (geometric dilution row in PBS-T-BSA) were added to washed wells. Plates were incubated for 2 h at + 37 •c and then washed again three times and shaken dry. Thereafter sequemially 50 {tl of IHA-buffer solution, pH 8.1 (Behringwerkc), and I 0 pi of Toxoplasma IHA -reagent were added. The optimal dilurion of the Toxoplasma JHA-reagent as well as the optimal dilution of the rabbit antiserum to human lgM was determined in preliminary block titrations.
Plates treated in the above described manner were covered and allowed to stand over· night at room temperature in a vibration-free place. For reading the results the scdimcnta· tion paucrn of the erythrocytes was determined from below by means of a mirror.
In case of lgM positive sera the sensitized erythrocytes arc fixed to the specific antibodies and uniformly distributed over the entire surface of the U-shapcd well. In case of lgM negative sera the sensitized erythrocytes drop down to the center of the well and a dear ring formation can be seen.
Other serological tests: FAT and CFT: performed according to the recommendations of the Bundesgesundheitsamt of FR Germany (Bundcsg.csundheitsblan, 1976).
lgM-FAT: performed according to Remington et al. (1968) IHA: Cellognost Toxoplasmosis (Behringwerkc).
Results
Optimal conditiotts for SPIHA: Jn preliminary experiments we found the concenrration of erythrocytes and the quality of the anti-human IgM antibody to be critical for obtaining good results. A too small <lmount of erythrocytes used jn the test led to false-positive or indeterminable results, whereas too many erythrocytes caused false-negative results. Therefore, the adequate concenrrar.ion of erythrocytes should be defined by block titration.
Two specimens of anti-human lgM antibodies were examined for the test: 1) a commercially available, 2) a hjghly purified antibody. Only the latter showed satisfying results in SPIHA.
Specificity: Several controls were carried out to assure the specificity of the test system:
384 K.Hcrmcntin, 0. Picher, H. Aspock, H. Auer, and A. Hassi
a) Anti-human lgM antibodies fixed to the plates and sensitized erythrocytes did not react nonspecifically an the absence of patient's serum.
b) When we used uncoated plates, no positive reactions occured with Toxoplasma lgM positive sera in SPIHA. This assured that patient's antibodies do not fix to microtirer plates nonspecifically during incubation time.
c) In order ro exclude the possibility that antibodies of the lgG class are bound nonspecifically in the test system, a serum sample obtained from a patient with acute toxoplasmosis containing both specific l.gM and IgG was dilmed to-3 in PBS and incubated for 1 b at 37 °C with different dilutions of anti-human IgM antibody (l0- 1, 10- 2, ·w-3). After centrifugation for lO min at 1000 g the serum was allowed to react in SPIHA.
Treatment of serum with 10- 1 and 10- 2 anti-tl antibodies resulted in negative reactions (all lgM antibodies had been precipitated), while serum pretreated with tO 3 anti·Jt was still positive (not all lgM antibodies had been inhibited).
d) Four sera with JgM antibodies to Rubella virus and two sera with IgM antibodies to Echinococcus were tested in SPIHA to examine cross-reactivity to other acute .infectious diseases. All sera gave negative results.
c) A control test with nonsensirized erythrocytes ran concomitantly on each plate at one serum dilution of each serum sam1'le to check for nonspecific agglutinins.
Furthermore, a positive and negative control were performed on each microtjrcr plate. A pool of sera which were llighly positive for Toxoplasma lgG but negative for IgM served as negative control. A serum sample from a patient with clinically proved acute wxoplasmosis served as positive control.
Retmulucibility: 15 sera were tested several times on different days. The variation in titers observed for positive test sera was not greater than fourfold. Negative sera remained negarivc at any time.
/{esults of SPIH A in sera: We selected 92. RF-negative sera of pregnant women, submitted to our laboratory for diagnosis .in toxoplasmosis surveillance. All sera were rested in FAT, lgM-fAT, CFT, JHA, and SPIHA and arranged in three groups: 1) sera of uninfectcd individuals, 2) sera of individuals with a chronic Toxoplasma infection, 3) sera of .individuals with a suspected or verified acute Toxoplasma infection. Assignment to these groups was carried out according to serology as de-
Table 1. Results of FAT, lgM-FAT, CFT, IHA, and SPIHA in sera from uninfected individuals and individuals with chronic 'J'oxoplasmtt infection
Source of sera
Uninfectcd individuals
individuals with chronic T oxoplasma infection
1 reciprocal
No. tested
12
3.3
FAT
12 (neg)
l (16) 7 (64)
2.S {256)
No. of sera (titer or range of titers') lgM-FAT CFT IHA SPIHA
12 (neg) 12 (neg.) t2 {neg.) 12 (neg.)
17 (neg.) 8 (64) 24 (neg.} 33 (neg.) 9 (S) 10 {256) 3 (16)
6 (10) 9 (1000) 2 (32) 1 (20) 6 (4000) I (64)
3 (256)
Indirect Hacmadsorprion Assay for Toxoplasma 385
Table 2. Results of JgM-FAT, SPIHA, and FAT in sera from individuals wirb a suspected or verified acute To;-.:oplasma infection
Serum No. Titc:r 1
lgM-FAT SPIHA FAT
1 256 2000 4000 l 256 8000 1000 3 256 8000 1000 4 256 4000 256 5 256 2000 256 6 64 1000 4000 7 64 16000 1000 8 64 16000 1000 9 64 8000 1000
10 64 4000 1000 11 64 4000 1000 12 64 8000 256 13 64 8000 256 H 64 4000 256 1$ 64 2000 256 16 64 2000 256 17 64 2000 156 18 64 2000 2.56 19 64 2000 256 .20 64 2000 256 21 64 1000 256 .22 64 16 64
.!.l 16 2000 1000 24 16 4000 256 15 16 4000 H6 26 16 2000 2.56 11 16 1000 256
28 16 128 1000 29 16 256 156 30 16 neg. 64 31 16 neg. 64 31 16 256 64 33 16 neg. 64
34 neg. 1000 4000 35 neg. 1000 4000
36 neg. 16 64000 37 neg. neg. 4000 38 neg. neg. 4000 39 neg. 256 4000 40 nc~. neg. 4000 41 neg. 16 1000 42 neg. neg. 1000 4,~ neg. 2.56 1000 44 neg. neg. 1000 45 neg. neg. JOOO 46 neg. 256 1000 47 neg. neg. 1000
1 reciprocal
386 K. Hermcntin, 0. Picher, H.Aspodc, H. Auer, and A. Hassi
scribed elsewhere (Aspiick, 1982; Flamm and Aspock, 1981) or according to known clinical course of illness.
As can be seen in table l all sera obtained from uninfected individuals gave negative results in FAT, IgM-FAT, CFT, IHA, and SPIHA (FAT, IgM-FAT, IHA, and SPlHA titers below 1: 16 were considered negative).
33 sera were from individuals with a chronic Toxoplasma infection {Table 1). 24 of these sera were negative in IgM-FAT and SPIHA as well. 9 sera yielded weakly positive titers in Sl'JHA, while JgM-FAT was negative (FAT, CFT, IHA titers: sec Table 1).
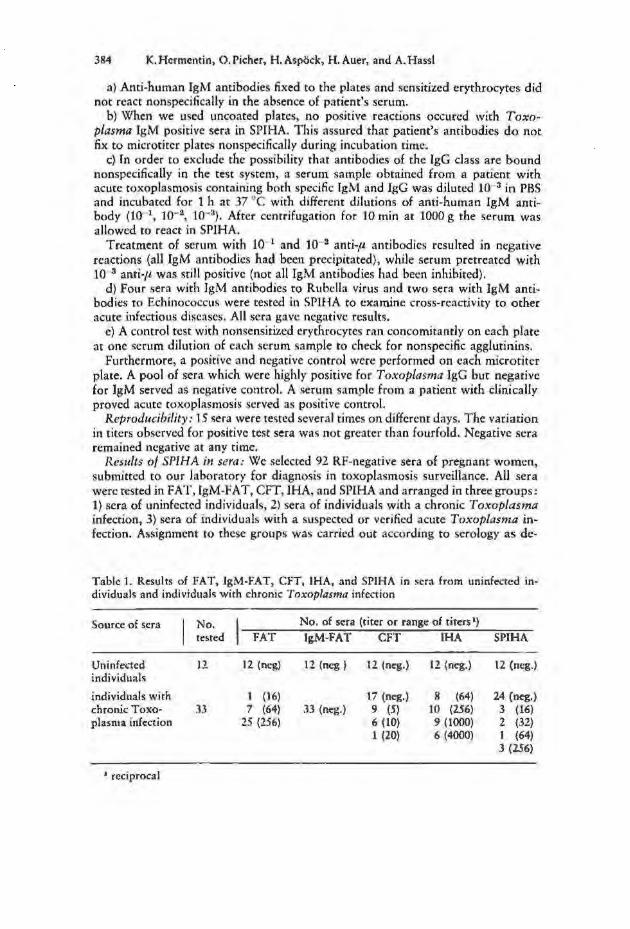
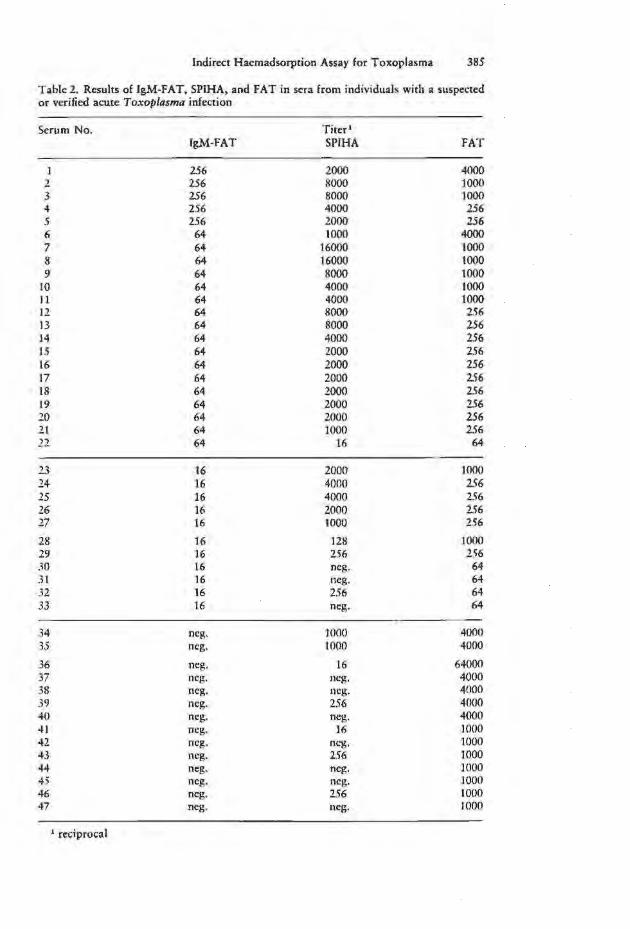
47 sera were from individuals with a suspected or verified acute Toxoplasma infection (Table 2): 21 sera (No. 1-21) yielded coincidently high titers in IgM-FAT and SPIHA. One serum (No. 22) was 1:64 positive in lgM-FAT but only 1:16 positive in SPJHA. Five out of eleven sera with IgM-FA T titers of 1:16 (No. 23-33) were highly positive in SPIHA, while six sera yielded only low titers (up to 1: 256) or were even negative. Two sera were found to be negative in IgM-FAT (No. 34, 35) but highly positive in SPJHA. 12 sera (No. 36-47) negative in IgM-FAT gave also negative or slightly positive results in SPIHA (CFT, IHA titers: not shown).
The WHO serum tested for reference was highly positive in SPIHA (1: 2000) but only 1: 16 positive in IgM-FA T. These findings are in accordance with those made by Desmonts, 1982 by means of the IgM-immunosorbent agglutination assay. The low IgM -FAT titer has been attributed to antibody competition.
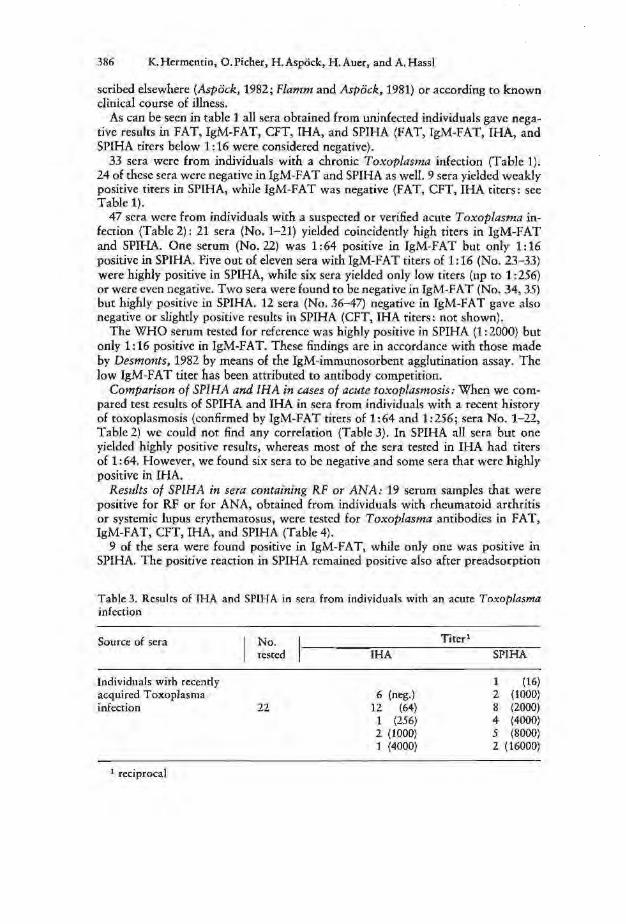
Comparison of SPIHA and IHA in cases of acute toxoplasmosis: When we compared test results of SPIHA and IHA in sera from individuals with a recent history of toxoplasmosis (confirmed by IgM-FA T titers of 1:64 and 1:2.56; sera No. 1-22, Table 2) we could not find any correlation (Table 3). In SPIHA all sera but one yjelded highly positive results, whereas most of the sera tested in IHA had titers of 1:64. However, we found six sera to be negative and some sera that were highly positive in IHA.
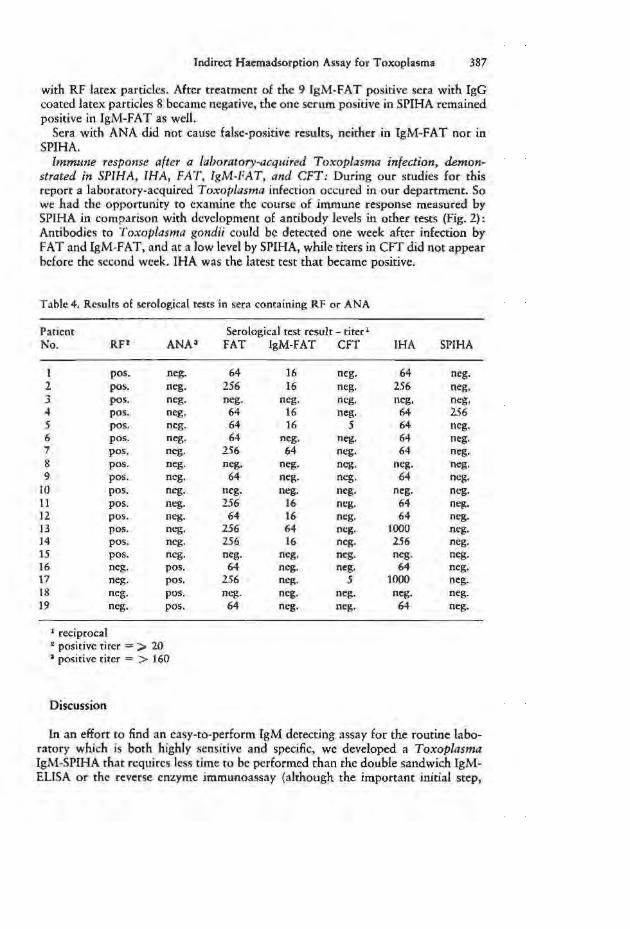
Results of SPIHA in sera containing RF or ANA: 19 serum samples that were positive for RF or for ANA, obtained from individuals with rheumatoid archritis or systemic lupus erythematosus, were tested for Toxoplasma antibodies in FAT, IgM-FAT, CFT, IHA, and SPIHA (Table 4).
9 of the sera were found positive in IgM-fAT, while only one was positive in SPIHA. The positive reaction in SPIHA remained positive also after preadsorption
Table 3. Results of IHA and SPIH A in sera from individuals with an acute Toxoplasma infection
Source of sera
Individuals with recently acquired Toxoplasma infection
' reciprocal
No. tested
22
IHA
6 (neg.) 12 (64) 1 (256) 2 (1000) 1 (4000)
Titer' SPIHA
1 (16) 2 (1000) 8 (2000) 4 (4000) 5 (8000) 2 (16000)
Indircx:t Haemadsorprion Assay f(lr Toxoplasma 387
with RF latex particles. After treatment of the 9 lgM-FAT positive sera with IgG coated latex particles 8 became negative, the one serum positive in SPIHA remained positive in IgM-F AT as well.
Sera with ANA did not cause false-positive results, neither in IgM-FAT nor in SPlHA.
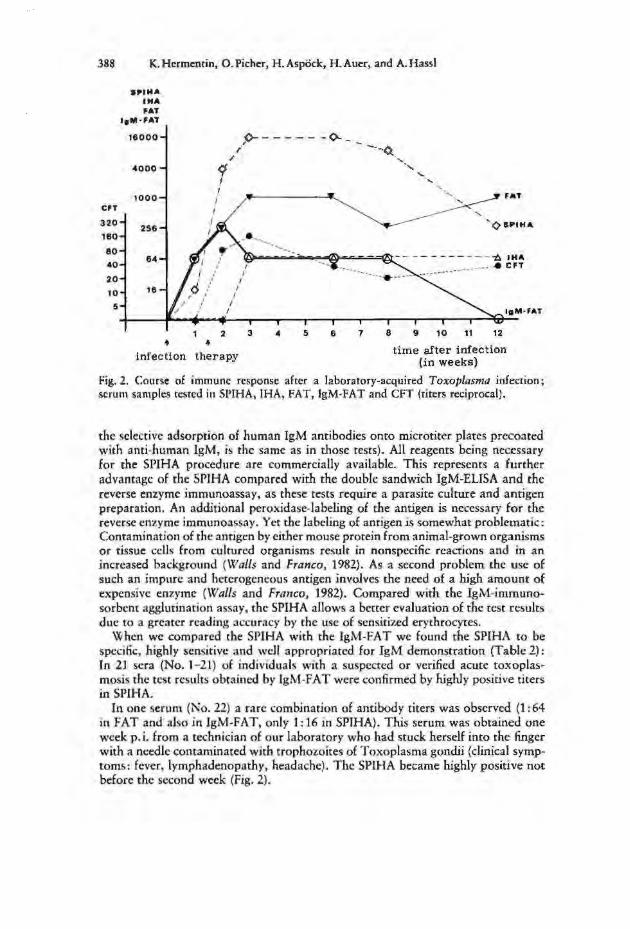
lmmttne response after a laboratory-acquired Toxoplasma infection. demonstrated in SPIHA, IHA, FAT, lgM-FAT, ami CFT: During our scudies for this report a laboratory-acquired ToxO{Jiasma infection occurcd in our department. So we had the opportunity to examine the course of immune response measured by SPJHA in comparison with development of antibody levels in other tests (Fig. 2): Antibodies ro Toxoplasma f{Ondii could be detected one week after infection by FAT and IgM-FAT, and at a low level by SPIHA, while titers in CFT did not appear before the second week. IHA was the latest test that became positive.
Tablc4. Results of scrolo~ical tests in sent containing RF or ANA
Patient Serological test result - titer 1
l':o. RP ANA3 FAT IgM-FAT CFT IHA SPIHA
I pos. neg. 64 16 neg. 64 neg. 2 pos. neg. 256 16 neg. 256 neg. 3 pos. neg. neg. neg. neg. neg. neg. 4 pas. neg. 64 16 neg. 64 256 5 pos. neg. 64 16 5 64 neg. 6 pas. neg. 64 neg. neg. 64 neg. 7 pos. neg. 2.56 64 neg. 64 neg. 8 pos. neg. neg. neg. neg. neg. neg. 9 pos. neg. 64 neg. neg. 64 neg.
10 pos. neg. neg. neg. neg. neg. neg. 11 pos. neg. 256 16 neg. 64 neg. 12 pos. neg. 64 16 neg. 64 neg. '13 po~. neg. 256 64 neg. LOOO neg. 14 pos. neg. 256 16 neg. 256 neg. 15 pos. neg. neg. neg. neg. neg. neg. 16 neg. pos. 64 neg. neg. 64 neg. 17 neg. pos. 256 neg. s 1000 neg. 18 neg. pos. "'·"S· neg. neg. neg. neg. 19 neg. pos. 64 neg. neg. 64 neg.
1 reciprocal 2 positive titer = > 20 a positive titer = > 160
Discussion
In an effort to find an easy-to-perform lgM dctectjng assay for the routine laboratory which is both highly sensitive and specific, we developed a Toxoplasma lgM-SPIHA that rcqttircs less time to be performed than the double sandwich IgMEUSA or the reverse enzyme jmmunoassay (although the important initial step,
388 K.Hcrmcnrin, O.Pichcr, H.Aspock, H.Auer, and A. Hassi
CFT
320
160
80
40
20
10
5
IPIMA IHA FAT
I1M·FAT
16000
1000
256
84
16
<I I
2 • +
" 1>- ---- - -<>--
1
3 4 5 6
infection therapy
7 8
FAT
'¢1PIHA
9 10 t1 12
time after infection (in weeks)
rig. 2. Course of immune response after a laboratory-acquired Toxoplasma infection; serum samples tested in SPIHA, IHA, FAT, lgM-FAT and CFT (titers reciprocal).
the selective adsorption of llllman IgM antibodies onto microtiter plates precoated with ami-lmman lgM, is the same as in those tests). All reagents being necessary for the SPIHA procedure are commercially available. This represents a further advantage of the SPIHA compared with the double sandwich IgM-ELISA and the reverse enzyme immunoassay, as these tests require a parasite culture and antigen preparation. An additional peroxidase-labeling of the antigen is necessary for the reverse enzyme immunoassay. Yet the labeling of antigen is somewhat problematic: Contamination of rhc antigen by either mouse protein from animal-grown organisms or tissue cells from cultured organisms result in nonspecific reactions and in an increased background (Walls and Franco, 1982). As a second problem the usc of such an impun: and heterogeneous antigen involves the need of a high amount of expensive enzyme (Walls and Fra11co, 1982). Compared with the lgM-immunosorbcnt agglutination assay, the SPIHA allows a better evaluation of the rest results due to a greater reading accuracy by the usc of sensitized erythrocytes.
When we compared the SPIHA with the IgM-FAT we found rhe SPIHA to be specific, highly sensitive :md well appropriated for IgM demonstration (Table 2): ln ll sera (No. 1- 2'1) of individuals with a suspected or verified acute toxoplasmosis the test results obtained by lgM-F AT were confirmed by highly positive titers in SPIHA.
In one serum (1\:o. 22) a rare combination of antibody titers was observed (1: 64 in FAT and also in IgM-FAT, only I: 16 in SPJHA). This serum was obtained one week p.i. from a technician of our laboratory who had stuck herself into the finger with a needle contaminated with trophozoites of Toxoplasma gondii (clinical symptoms: fever, lymphadenopathy, headache). The SPll-IA became highly positive not before the second week (Fig. 2).
Jndirect Hacmadsorption Assay for Toxoplasma 389
This example demonstrates that we cannot rule out rhe possibilit)' that a low titer in SPJHA may refle·cr an acute toxoplasmosis. Nevertheless, thl·re is only a small chance that a low titer in SPJHA rdlens an acute infection, as JgM anrjbodies rise quickly within two wcc:ks after infection to a very high le\•el (fig. 2). On the other hand, lgM antibodies to ToxopLasma gondii are present ar a low Je,·d for scvcraJ months after the onset of the infection (Braven)•, 1979 ; Naat et al., 1982).
The fact that the SPIHA gave a dearly positi\•c reaction a few da}'S later than the lgM-FAT might be due to the source of antigen: In IgM-FAT and FAT surface antigen is used, while in SPIHA, fHA, CfT, :tnd ELISA soluble antigens arc reactive to the antibodies. When Ambroise-Tlwmas et al. (1978) used a "whole mixed antigen" in IHA, they were able to detect antibodies in sera of acute infected iodividuals as early as in FAT. Therefore, we assume rhat the usc of another type of antigen (e.g. whole mixed antigen) .in SPIHA may also expedite the antibody demonstration.
In ll sera (No. 23-33) the JgM-FAT was only 1:16 positive. 1gM-FAT titers below 1 :64 are not accepted as an indication for acute toxoplasmosis by many authors (Aspock, 1982; Braveny, 1979; Naot and Remingtm:, 1980) so that these sera could not be dearly identified by lgM-FAT. A convincing interpretation with respect to the onset of the infection was, however, possible by SPIHA; a SPJHA titer of > l :256 was considered highly suggestive of recent infection.
Among the sera No. 34-47 the eventual icy of a recent infection had to be taken into consideration on the basis of resultS obtained by FAT. although these sera wen: negative in lgM-F AT. In 11 of the.o;e sera the SPIHA ga,·c negative or sli3htly posirivc reaaio!ls, thus con6rming tes t results obtained b}' lgM-FA T. Therefore, the :.uspicion on recent infections could be dropped. Jn two sera (No. 34, 35), however, rbt: lgM-FAT failed to detect lg.M antibodies, whereas the SPIHA was highly positive. This test resulr- in correlation w•th bighlr positive titers in FAT and CFTled us ro the assumption rhat these sera g:n•e fa I c-negativc resul ts in JgM-FA T due ro amibody compc.tition. (Unfortunatdy, no mme serum was available for further confirm:u ion by chromatographic separation.)
In some sera (rom chronically infected individuals we were able to find low antibody titers in SPIHA bur not in lgM-F AT (Table 1). This can be amibuted to the higher sensitivit~· of the SPIHA and to rhc prolonged pcrsisrance of l:;M antibodies in toxoplasmosis mentioned before.
In SPfHA lgM and IgG antibodies arc separated in the initial step of the assay, and thus cannot compete for antigenic binding sites. No interference of rheumatoid factor occured in SPIHA, whereas in lgM-FAT most (but nor all) of RF positive scn1 gave false-positive rcsulrs. One RF positive serum which yielded a positive result also in SPIHA (Table 4) remained anti-Toxoplttsma IgM positive after preadsorprion with lgG coated latex panicles. Therefore, it was considered as a truly positive reaction for anti-Toxoplasma IgM.
RF m;ty be a source of false-positive reactions even in tests such as the double sandwich lgM·EUSA: Schmit?. ct 31. (1980) found a strong nonspecific binding of the RF-IgM with peroxidase-labeled hum3n or animal IgG. Naot et al. {1981) observed that in sera containing both rheumawid factor and antinuclear antibodies false·posiriw results mar occur due to interactions of RF-ANA-complcx with the Fc-portion of the antigenspecific lgG antibody used for the enzyme conjugate- In
390 K.H«mcnrin, O.Pichcr, H.Asp&k, H.Aucr, and A. Hassi
SPJHA, however, these nonspecific reactions cannot occur, since no labeled antibodies are used a.~ a conjugate.
In a comparative study of SPIHA and IHA we could nor find any correlation (Tablc3). This can be simply explained by the fact that in SPJHA and [HA different classes of antibodies are reacting. A laboratory-acquired in(ccdon, the course of which we observed in detail (Fig. 2} illustrates d1e difference between antibody levels in IHA and SPIHA. Antibody titers measured in IHA l>howed only a slow rise some weeks after infection. Therefore, in agreement with rcsuhs of pre,·ious studies (Balfour cr al., 1980; Picher and A.spock, 1981 ; Welch et aL 1980}, we consider the fHA as inadequate for dctecrion of a recently acquired Toxoplasma in· fection. In contra~>t, antibodies in SPlHA reached rhdr maximum alrcad\• three we(·ks after infection and decreased afrer six weeks {but were 'itill present when lgM-FAT already became negati,·c).
The Solid-Phase Indirect Haemadsorption Assay provides a simple, sensiti\'C and accurate detection of specific lgM antibodies. The resr is we.ll appropriated for the routine laboratory (even for the short-equipped}, and thus representing an altcrn:nivc method to lgM-FAT. The advantages of this assay suggest that the SPIHA should be applied also for the diagnosis of other acute parasitic diseases.
References
I. Anrbroist· Tbom.Js, P.,}. Simon, and ,\f. Ba·yard: lnd•rcct hemagglutination using whole mil'cd anri~cn for checking roxopl.nmosis immuni t~· anJ for serodiagnosis of human roxoplasmoJ>is, compared with immunolluorescence. J3•omed. 29 (1978) 245- 248
2. Ar.mjo, F. G.,£. V. Hamt'lt, L. 0. Gentry, and ].S. Rt>nrb1gton: Falsc-positi"l'e anti-Toxoplasma lluorcsccnt-antibody tests in patients with ant inuclear anrilx>dics. Appl. Micro· bioi. 22 (197 1) 270-27.5
3. As(Jikk, II.: Toxoplasmose. Hoffmann-la Roche, Wien ( 1982) 4. Balfour, A. H .. ]. 8. Bridges, and }.1'. /larford: An evaluation of the ToxHA rest for rhe
detection of antihoJies to 1'o:cot,lolsm'l gondii in hum.1n serum.). Clin. Path. 33 (1980) 644-6 .. 7
S .. liral•t>ll )'.l. : Sc:rolo~rc: Jer Toxupl.l<imosc: Neuerc: .Mcthodcn unJ ihre Bewcrrung. Oh.:h .• :S. rztcbl. .! 9 ( 1979) J9()Y-I Y T T
6. BunJ~gc:sundhcu-.bbrr: I.mpfchlunf:en fur d ie Durchfj;hrung dc:r Toxoplasma-~ rc ak t iunc:n mmeb M ik romcthodc. Bu ndes~csundh hi. 20 ( 1976) 108-112
i . C,mrargo , M. E .• P. G. Lt>ser, and A. R oaa: Rheumatoid factors as a c.ausc for false posirrvc lgM 3nn-To.Toplasma lluorcKent tests. A technique for spcdfic result~. Rev. lnst. Mcd. Trop. S.io Paulo 14 (1'172) J IO-JJJ
8. Colm1, I. R .• L. C. Nori11s, and A.]. Julian: Co mpetition between, and dfccti\·cncss of, lgG and lg.M antibotfic:s in indirect tluoresccnr antibody and other tests .. .1. lmmun.ol. 98 ( 1967) 143-149
9. Dl.'smotlts, G.: Lc:s rc..:herchc:s d'ant icorps TgM sptcifiqucs par immuno-adsorprion (lmmunosorbent assJy ou ISA). l yon mcd. HS, Suppl. (19SZ) 37-.. 1
10. Demro,ts, G. , Y. N'llll, and J.S. Rt>mi,gtmr: Immunoglobulin J\1 - immunosorbc:nt a~hmnarion assay for d•:agnos•o; of mfccrious dl\ca...:s : Diagnosis of acute congenital and ao:quircd ToxO()/asma infe..:non<>. J. Clin. Microb1ol. H (1981) 41!6- 491
I I. f>uertn~yt'r, \t'., F. Wit'la.mJ, H. Vo~n Grrujth11ijsc,, and j .S1vinkds: Enz) me-linked immunosorbent a~~ay for detection uf 1mmunoglohulin M antibod.ic:s .tl!ainsr T oxoplasm11 !i(Otldit. ]. Clrn. ~trcrobiol. 12 (1980) 805-806
12. Frlict, G .• -\., A. S. Ytaf,f!r, and j .S .. Rt>mi~rRtO": I>iagnosric significance: of immunoglo-
Indirect Hacmadsorption Assay for Toxoplasma 391
bulin M antibodit:s to 'To:copitlS"UI go,dii detected a fter separation of immunoglobulin M from immunoglobulin G antibodic:s. j. Clin. Microbiol. IZ (1980) 336-J4Z
13. Flamm, H. und H.Aspock: Die Toxoplasmosc-Obcrwachung der Schwangerschafr in Ostt:rrcich - Ergebnisse und Problemc. Pad. Grcnzgcb. 20 (1981) 27-34
14. Franco, E.L, K. W. Walls, and A.j.Sul;.er: Rcvt:rse enzyme immunoassay for detection of specific and· Toxoplasma immunoglobulin M :mribodics. J. Clin. Microbial. 13 ( 1981} 859-864
15. Gehle, \V. D., K. 0. Smith, and D. A. C:ucci/lo: Radioimmunoassay for toxoplasmosis. Infect. lmmun. 14 (1976} 1253-1255
16. Hyde, 8., E. V. Barnett, and J.S. RemingtoPI: Mcth<)d for differentiation of nonspecific from specific Toxoplasma lgM fluoresccm antihodics in patients with rheumatoid f<tctor. Proc. Soc. exp. Bioi. (N.Y.) 148 (1975) 1184-1188
17. Krech, U. and J.A. Wilhelm: A solid-phase immunosorbcnt technique for the rapid detection of Rubella lgM by hacmagglutination inhibition. j. gen. Virol. 44 (1979) 281-286
18. Naot, Y., E. V.Bamett, and J.S.Remington: Method for avoiding fal se-positive results occuring in immunoglobulin M enzyme-linked immunosorbcnt assays due to presence of both rheumatoid factor and antinuclear antibodies . .J. Clin. Micro biol. 14 (1981) 73-78
19. Naot, Y., D.R.Gupti/1, and ].S.R.emh1gton: Duratiorl of lgM antibodies to Toxoplasma go11dii after acute acquired toxoplasmosis. J. infect. Dis. 145 (1982) 770
20. Naot, Y. and J. S. Remingto11: An enzyme-linked immunosorbcnt assay for detection of lgM antibodies to Toxoplasma gondii: Use for diagnosis of acute acquired toxo· plasmosis. j. infect. Dis. 142 (1980) 757-766
21. Picher, 0. und II. Aspock: Die diagnostischc Bedeutung des indirekren 1-liimagglutina· tionstesrs Hir dit: Toxoplasmoseiibcrwachung wahrend der Schwangcrsch:tft. Wicn. mcd. Wschr. 131 (198'1) 14-22
22. i>yndiab, N., U. Krech, P.l'rice, and /.Wilhelm: Simplified chromamgraphic separation of immunoglobulin M from G and its application to 'foxop/asntt~ indirect immuno· fluorescence. J. Clin. Microbial. 9 (1979) 170-174
23. Remingtmr, ]. S.: A d<>ublc-sandwich lgM -ELISA for diagnosis of acute acquirt:d and congenital Toxoplasma infection. Lyon med. 248, Suppl. (1982} 31-35
24. Remingtott, }.S., M.J.Miller, and l.Broumlee: JgM antibodies in acute toxoplasmosis. II. Prevalence and significance in acquired cases. J. Lab. Clin. Med. 71 (1968) 855-866
25. Schmidt, B. L.: Sol id-phasc hem adsorption: a method for rapid detection of 'Treponema pal/idum-specific lgM. Sex. Trans. Dis. 7 (1980) 53-56
26. Schmitz, H., U. von Deimlit1g, and H. Flehmig: Detection of IgM antibodies to Cytomegalovirus (CMV) using an enzymc-l:lbelled antigen (ElA). J. gen. Virol. 50 (1980) 59-68
27. Van der Logt, ]. T.M., A.M. Van l.om1, and J. Van der Vun: Hcmadsorption immunosorbent technique for determination of Rubella immunoglobulin M antibody. J. Clin. Microbial. 13 (1981) 410-415
28. Voller, A., J).E.Bidwe/1, A. Bartlett, D.C. Fleck , M.PerkhiS, and B.Oiadehin: A microplate enzyme-immunoassay for Toxoplasma antibody. J. Clin. Path. 29 (1976) 150-153
29. Walls, K. W. and f..L Franco: Reversed cnzymt: immunoassay. l.yon mcd. 248, Suppl. (1982) 43-49
30. Welch, 1'. C., H. Masur, T. C.]o11es, and ).S.Remittgtmr: Serologic diagnosis of acute lymphadenopathic toxoplasmosis. J. infect. Dis. 142 (1980) 256-164
Mag. K. Hermentin, Dr. 0. Picher, Univ.-Prof. Dr. H. Aspoclt, Dr. H. Auer, Dr. A. Ha{JI, Department of Mcd. Parasitology,lnstitute of Hygiene, Kinderspitalgasse IS, A·1095 Vienna, Austria
r.