Embed Size (px)
Citation preview

Vol. 1, 377-384, April 1995 Clinical Cancer Research 377
Phase I Clinical Study with 8-Chloro-cAMP and Evaluation of
Immunological Effects in Cancer Patients’
Giampaolo Tortora,2 Fortunato Ciardiello,
Stefano Pepe, Pierosandro Tagliaferri,
Angela Ruggiero,3 Caterina Bianco,
Rosario Guarrasi, Keizaburo Mild,
and A. Raffaele Bianco
Cattedra di Oncologia Medica, FacoltI di Medicina e Chirurgia,Universit#{224} degli Studi di Napoli Federico II, Via Pansini 5, 80131
Napoli, Italy [G. T., F. C., S. P., P. T., A. R., C. B., R. G., A. R. B.],and Terumo Institute of Biomedical Sciences, Nakai, Kanagawa,
Japan [K. M.J
ABSTRACTThe site-selective cyclic AMP analogue 8-chloro-
cAMP (8-Cl-cAMP) is able to inhibit the growth of a wide
variety of cancer cell lines in vitro and in vivo. 8-Cl-cAMP
has been extensively investigated as a new potential anti-
cancer agent and, more recently, preclinical Phase I stud-
ies have been conducted in animal models to study its
toxicity. We have conducted the first Phase I trial with
8-Cl-cAMP to define the maximum tolerated dose, toxic-
ity, plasma drug levels, and immunological effects in pa-
tients with cancers refractory to standard treatments. We
have administered 36 courses of 8-Cl-cAMP to 17 patients
by continous i.v. infusion of the drug for 5 days/week for
2 weeks followed by a 1-week rest period. Six increasing
dose levels, from 0.01 to 0.25 mg/kg/h, were explored.
Drug plasma levels were determined and the expression of
interleukin 2 receptor a, amount of natural killer cells,
and cytolytic activity against K562 cells were measured in
peripheral blood lymphocytes. A grade 4 and a grade 3
increase in serum creatinine and a grade 2 increase in
blood urea nitrogen observed in two patients were the
dose-limiting toxicity. The maximum tolerated dose (0.2
mg/kg/h) determined a grade 1 increase in serum creati-
nine. An increase in calcium levels was observed in sev-
eral patients. The 8-Cl-cAMP plasma concentrations ob-
tamed at the steady state were in the range previously
shown to be effective for cancer cell growth inhibition in
vitro. Interleukin 2 receptor a expression, natural killer
cell number, and cytolytic activity from peripheral blood
lymphocytes were markedly increased after 8-Cl-cAMP
administration at all dose levels. In conclusion, at doses
below the maximum tolerated dose, 8-Cl-cAMP was not
toxic but reached plasma concentrations in the potential
therapeutic range for growth inhibition. Moreover, 8-Cl-
cAMP determined a marked biomodulatory effect and
showed antitumor activity.
INTRODUCTIONThe potential usage of cAMP4 analogues for the therapy of
cancer has been widely discussed in the past two decades (1-3).
However, the lack of selectivity and the high doses required for
the available cAMP analogues have been a major obstacle to the
development of this approach into a sound therapeutic trial. A
renewed interest has been fostered by the recent discovery of a
new class of site-selective cAMP analogues that are able to
modulate the activity of the cAMP-dependent PKA at micro-
molar concentrations (3, 4). The PKA is present in eukaryotic
cells as two different isoforms, PKAI and PKAII, consisting of
a tetrameric structure with two regulatory subunits and two
catalytic subunits. While both PKAI and PKAII share identical
catalytic subunits, they differ in the regulatory subunits which
have been defined RI in PKAI and RI! in PKAII, respectively
(5, 6). It has been shown that PKAI and/or its regulatory subunit
RIa are overexpressed in both cancer cell lines and primary
tumors and are induced by cell transformation with growth
factors such as transforming growth factor a, or oncogenes such
as ras or erbB-2 (7, 8). The increased amount of cAMP binding
proteins, which is mainly due to the overexpression of RIa, has
been recently demonstrated as a marker of poor prognosis in
breast cancer patients (9, 10). Moreover, increased RIa expres-
sion has been found in several nontransformed cells as a phys-
iological response to mitogenic stimuli produced by specific
hormones and/or growth factors (11, 12). On the other hand,
increased RI! or PKAII levels are present in normal differenti-
ated cells and precede the cell growth arrest induced by cAMP
analogues (2, 13).
Unlike intracellular cAMP, the new class of site-selective
cAMP analogues is able to selectively discriminate between the
two cAMP binding sites present on RI and RI! and to modulate
the intracellular levels of these regulatory subunits at micromo-
lar concentrations. 8-Cl-cAMP, the most potent site-selective
cAMP analogue (3, 14), is able to down-regulate RI by inducing
the degradation of the protein while up-regulating at the tran-
scriptional level RIl subunit expression (15). We have shown
Received 9/22/94; accepted 12/27/94.1 This study was supported by the Associazione Italiana per Ia Ricerca
sul Cancro.2 To whom requests for reprints should be addressed.3 Recipient of a fellowship from the Associazione Italiana per Ia Ricerca
sul Cancro.
4 The abbreviations used are: cAMP, cyclic AMP; PKA. protein kinase A;
8-Cl-cAMP, 8-chloro-cAMP; MDR, multidrug resistance; MTh, maxi-
mum tolerated dose; ECOG, Eastern Cooperative Oncology Group; DLT,dose-limiting toxicity; LDH, lactic dehydrogenase; IL-2, interleukin 2;
PBL, peripheral blood lymphocytes; PT!-!, parathyroid hormone.
Research. on March 13, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

378 Phase I Clinical Study with 8-Chloro-cAMP
that down-regulation of RIa by 8-Cl-cAMP or by antisense
oligodeoxynucleotides targeted against the RIa mRNA deter-
mine growth arrest and differentiation in a variety of human
cancer cell lines including, among others, leukemia, breast can-
cer, and colon cancer, with a 8-Cl-cAMP 50% inhibitory con-
centration (IC��) ranging between 0.05 and 5 �LM (3, 7, 8,
15-19). These effects are accompanied by an increased RII:RI
ratio and by inhibition of expression of different oncogenes and
growth factors (7, 8, 16, 20-21). Finally, it has been recently
shown that 8-Cl-cAMP is able to revert MDR in a variety of
MDR cancer cell lines (19).
In vivo studies to evaluate the effect and the pharmacoki-
netics of 8-Cl-cAMP have been performed in mice and dogs and
have shown that the drug reaches the steady-state concentrations
within few hours and that the major route of elimination is rapid
renal excretion; moreover, at doses above 0.34/mg/kg/h on a
30-day-based continuous infusion regimen in dogs, 8-Cl-cAMP
produced gastrointestinal and renal toxicity (22, 23). On the
basis of these studies, to reduce the risk of toxicity and to allow
the recovery of impaired organ function we designed an inter-
mittent exposure regimen of 8-Cl-cAMP administration (see
‘ ‘Patients and Methods’ ‘) and conducted a Phase I clinical trial
in cancer patients refractory to standard therapies.
Previous itt vitro studies suggested that 8-Cl-cAMP might
have a wide spectrum of effects on different cell types. It has
been shown that PKAI/RIa play an important role in the im-
mune response by regulating cytokine production and T lym-
phocyte activation. Moreover, RIa is associated with the T cell
receptor/CD3 complex (24-27). For these reasons we have also
evaluated whether 8-Cl-cAMP administration exerted any effect
on biomodulation in vito, such as immunological changes.
The goals of this trial were: (a) to establish the MTD, (h)
to determine the qualitative and the quantitative toxicities, (c) to
obtain informations on the pharmacokinetics, and (d) to evaluate
the biomodulatory effects on some immunological parameters
of 8-Cl-cAMP administered with this schedule.
PATIENTS AND METHODSEligibility. All patients that entered the study had a his-
tological diagnosis of solid cancers refractory to conventional
therapy. Eligibility criteria included age � 18 years, no cytotoxic
or radiation therapy in the previous 4 weeks, ECOG perfor-
mance status �2, life expectancy of at least 12 weeks, adequate
baseline organ function defined as WBC counts �3,000/pA,
platelets �l00,000/p.l, hemoglobin �9.0 g/dl, total bilirubin
�2.0 mg/dl, aspartate aminotransferase �3-fold normal values,
prothrombine time �60%, creatinine �1.S mg/dl or creatinine
clearance �50 mI/mm, detectable and measurable lesions, and
signed informed consent of the patient.
Drug Dosage and Administration. 8-Cl-cAMP was
synthesized as sodium salt by the Terumo Institute of Biomed-
ical Sciences (Nakai, Kanagawa, Japan). The trial with 8-Cl-
cAMP began at 0.01 mg/kg/h, a dose approximately 30-fold
lower than that producing toxicity in a preclinical study with
dogs (23). 8-Cl-cAMP was administered by continuous iv.
infusion for 5 days a week for 2 weeks followed by 1 week of
rest. The 3-week period was considered one course of therapy.
The daily dose of drug was dissolved in 500 ml dextrose (5%)
in water and infused over 24 h. Toxicity was evaluated accord-
ing to WHO criteria. Unaccetable toxicity was considered grade
3-4 or grade 2 persisting for more than 35 days from the start
of therapy. Additional courses of therapy were administered if
no toxicity was observed during the first cycle of therapy and
with no disease progression. Removal from the study was based
on development of unacceptable toxicity, performance status of
4 (ECOG), refusal to continue the treatment, and disease pro-
gression. The DLT occurring in at least two patients at a given
dose level was used as the end point of the study. The MTD was
therefore defined as the dose level below the DLT.
Patient Monitoring. A complete history, physical exam-
ination, and determination of performance status according to
ECOG criteria was obtained as baseline for each patient. Twelve-
lead electrocardiogram and a chest X-ray were performed at
baseline and at the beginning of each new cycle. Laboratory
studies performed at baseline and three times a week included:
complete blood cell count with leukocyte differential, serum and
urine sodium and potassium, serum calcium, LDH, alkaline
phosphatase, total bilirubin, asparate aminotransferase, alanine
amnotransferase, total protein, and albumin.
Determination of the plasma level concentration of 8-Cl-
cAMP was carried out by HPLC analysis as described below. At
the indicated days of each treatment course, the analysis of the
immunophenotype of lymphocyte subpopulations and the as-
sessment of lymphocyte cytotoxic activity were performed on
10 ml peripheral blood. For immunophenotype studies periph-
eral blood lymphocytes gated using standard FSC/SSC settings
on a FACScan flowcytometer (Becton Dickinson, San Jose, CA)
were analyzed at the indicated time points as described previ-
ously (28). mAbs aleul9 (CD56), uleull (CD16) and IL-2
receptor a (CD2S) (Becton Dickinson, Mountain View, CA)
were conjugated with FITC.
For determination of cytotoxic activity in circulating lym-
phocytes, PBL were isolated from heparinized blood by Ficoll-
Hypaque lymphocyte separation medium (ICN, Costa Mesa,
CA). Fresh PBL were used as effectors in a 4-h LDH release
assay against the human myeloid leukemia K562 cells with a
commercially available cytotoxicity kit (Promega, Madison,
WI; Ref. 29). The assays were performed in triplicate at E:T
ratios between 1 : 1 and SO: 1 . K562 cytotoxicity was expressed as
percentage of specific LDH release calculated according to the
formula:
(LDH release test - effect or spontaneous release)
- spontaneous LDH release
maximum LDH release - spontaneous LDH release
Pharmacokinetic Analysis. Heparinized blood samples
collected at different time points during drug infusion were
centrifuged and plasma was extracted for HPLC quantitative
analysis of 8-Cl-cAMP plasma concentrations. One ml acetoni-
trile was added to plasma and to control plasma + 8-Cl-cAMP,
vortexed, and centrifuged at 3000 rpm for 10 mm. The super-
natant was recovered, allowed to evaporate, reconstituted in
water, filtered, and immediately analyzed by reverse-phase
HPLC, carried out with a Shimazu system. Analytic conditions
consisted of a Tosoh TSK gel column (6 X 150 mm) with an
ammonium acetate (1 M, pH 7.0):H2O:acetonitrile (1:3:6) mo-
Research. on March 13, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Table I Patient characteristics
Patients entered
Male/female
Median age(range)
Performance Status
(ECOG)
17
11/658
(39-73)
0 7
1 8
2 2
CancerLung 2Breast 1Sarcoma 2
Colon 11Mesotelioma 1
Total number of cycles 36
Clinical Cancer Research 379
bile phase pumped at a flow rate of 1 ml/min. Detection was
monitored by fluorescence with emission wavelength set at 260
nm. The retention time of the 8-Cl-cAMP peak was 41.8 mm
and was not present in blank control plasma.
RESULTSSeventeen patients with metastatic malignant tumors re-
ceived 36 courses of treatment. Patients characteristics are de-
scribed in Table 1. The majority (65%) of patients in this trial
had colorectal cancer; all had previously been treated with
cytotoxic therapy for metastatic disease and, at the time of
enrollment, had a performance status (ECOG scale) �2. None
of the patients went off study because of progressive disease or
unacceptable toxicity until the DLT dose level was reached. Six
dose levels were used: 0.01 mg/kg/h (I level), 0.025 mg/kg/h (II
level), 0.05 mg/kg/h (III level), 0.125 mg/kg/h (IV level), 0.2
mg/kg/h (V level), and 0.25 mg/kg/h (VI VI). The number of
patients enrolled for each dose level were two (I level), two (II
level), two (III level), six (IV level), three (V level), and two (VI
level).
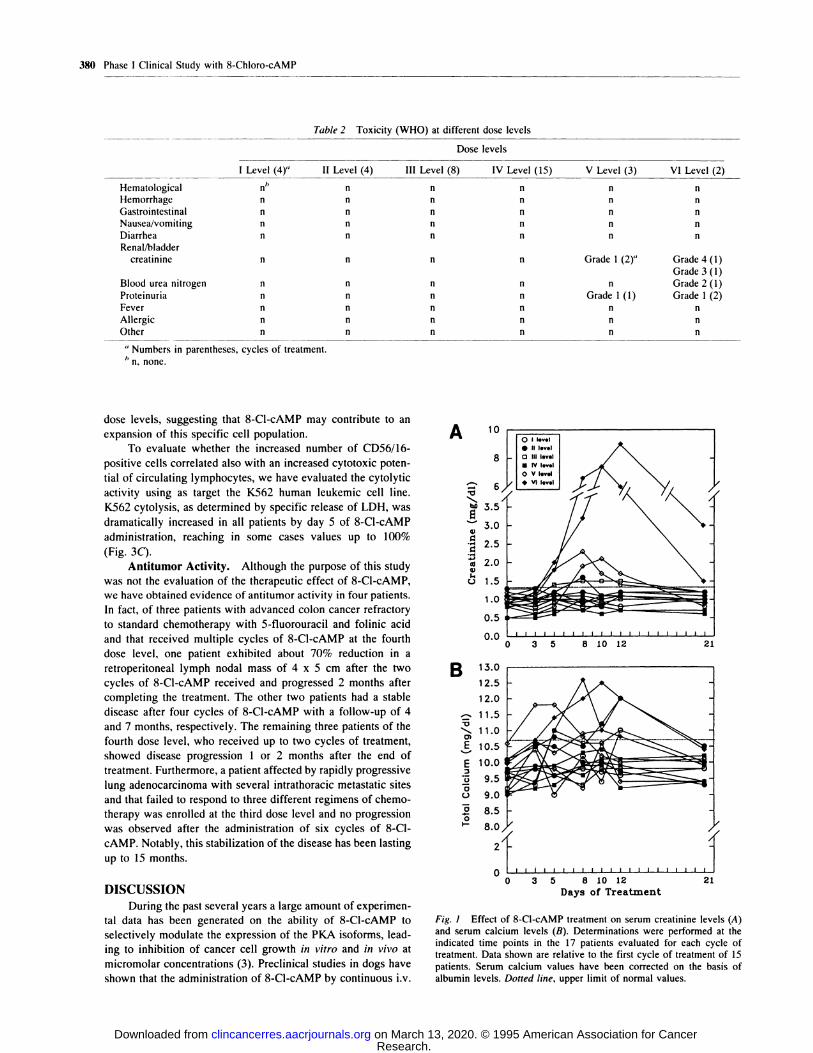
Toxicity. The only type of toxicity observed during the
36 courses of treatment was related to alterations of renal
function (Table 2). Most of the patients experienced an increase
in serum creatinine levels at the end of each week of drug
infusion, which, however, remained within normal value range
(Fig. 1A). At the fifth dose level two patients experienced a
grade 1 increase in serum creatinine and one of them a grade 1
proteinuria. At the sixth dose level a grade 4 and a grade 3
increase in serum creatinine and a grade 1 proteinuria occurred
in the two patients studied, while a grade 2 increase in blood
urea nitrogen was observed in one patient (Table 2). The serum
creatinine values for 15 patients are shown in Fig. 1A. In both
patients at the sixth dose level oligoanuria occurred at the end of
the first week of treatment, requiring the discontinuation of drug
infusion. They were both treated with infusion of saline solu-
tions with dopamine at 2.5 �i.gIkg/min, a dose capable of in-
creasing renal perfusion (30). One patient (grade 4) required
extracorporeal dialysis and renal function recovered by the end
of the cycle. The other patient refused the extracorporeal dial-
ysis, thus requiring a longer time for recovery of renal function,
which was reached by day 28. On the basis of these adverse
effects the dose of the sixth level was considered the DLT and
that of the fifth level was the MTh. Interestingly, in all patients
who experienced renal toxicity, no modifications of urine elec-
trolytes were observed, suggesting that the toxic effect may not
be due to impairment of renal perfusion. In one patient enrolled
at the third dose level and in four patients enrolled at the fourth
dose level, repeated cycles of 8-Cl-cAMP (up to six) were
administered. In these cases, several cycles of 8-Cl-cAMP treat-
ment did not influence serum creatinine levels as compared to
the first cycle of treatment, demonstrating that there is no
cumulative renal toxicity (data not shown).
No gastrointestinal, cardiovascular or toxicities other than
renal were observed during the study. Moderate asthenia devel-
oped in patients with an increase in serum creatinine levels.
An increase in total serum calcium, not requiring interrup-
tion of treatment, was observed in several patients after 3-4
days of drug infusion (Fig. 1B). In a few patients it was asso-
ciated with elevation of serum creatinine levels, suggesting a
correlation with the changes in renal function. The measurement
of PTH in two of these patients showed values below the
detectable level (data not shown).
Serial measurements of blood cell counts, hemoglobin con-
centration, and differential WBC counts showed no hematolog-
ical toxicity at any dose level or in patients that received
multiple cycles of treatment (data not shown).
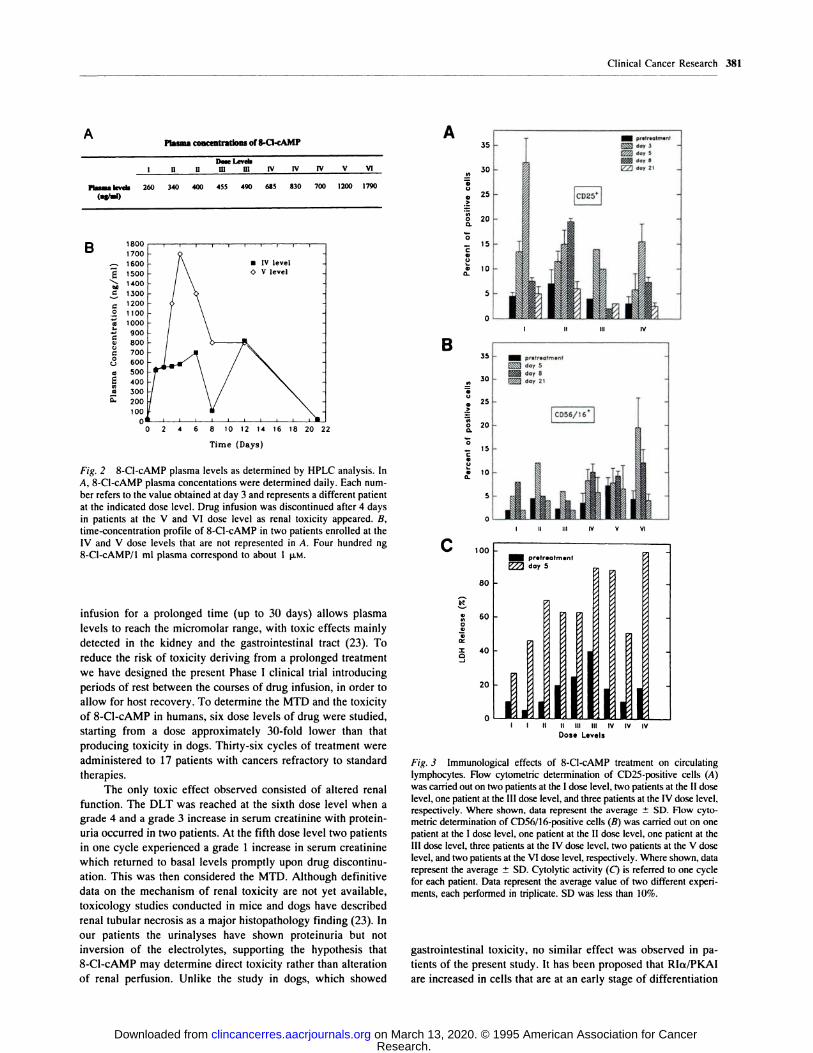
8-Cl-cAMP Plasma Levels. Determination of plasma
concentrations of 8-Cl-cAMP was performed daily in 10 pa-
tients, including at least one patient for each dose level. In
patients enrolled up to the fourth dose level the steady state was
reached rapidly and a moderate increase of drug plasma levels
was present at the end of each week of infusion, returning to
almost basal levels after resting time. In contrast, in the patients
at the fifth and sixth dose levels, in whom renal toxicity oc-
curred in spite of drug infusion discontinuation, the plasma
levels continued to increase also during the resting time, sug-
gesting that impaired renal function might contribute to drug
accumulation. Fig. 2A shows the plasma concentrations of 8-Cl-
cAMP in different patients at day 3 of drug infusion. In Fig. 2B
are shown the pharmacokinetic profiles of two different patients.
The patient enrolled at the fourth dose level did not experience
any toxicity, whereas in the patient receiving the dose of the
fifth level a grade 1 renal toxicity was observed. Since 400 ng
8-Cl-cAMP/ml of plasma correspond to about 1 p.M, it is note-
worthy that in most patients the 8-Cl-cAMP plasma concentra-
tions obtained in the absence of toxicity were within the range
of 8-Cl-cAMP 50% inhibitory concentration (0.05-S p.M) for the
majority of human cancer cell lines tested in vitro (19, 31).
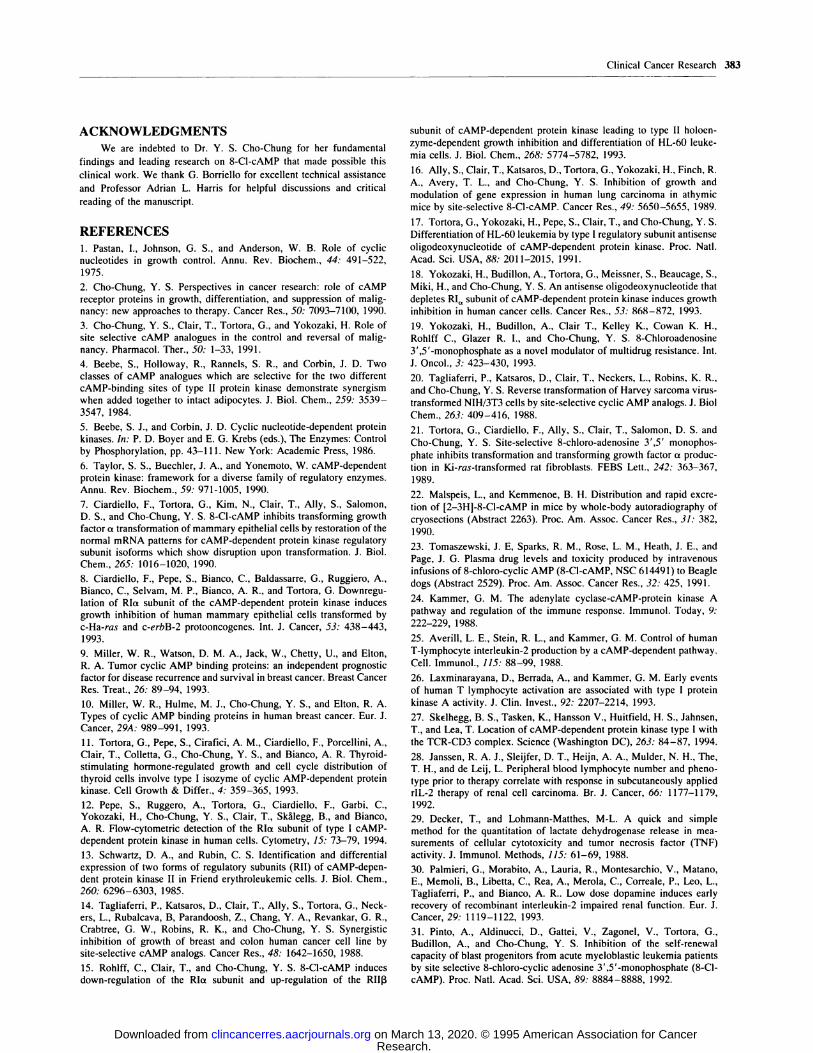
Immunophenotyping and Cytolytic Activity of Circu-lating Lymphocytes. Flow cytometric analysis of the expres-
sion of IL-2 receptor a (CD2S), considered as a marker of
functional activation of T lymphocytes, was performed on the
PBL of eight patients enrolled at the first four dose levels.
Regardless of dose level, all patients analyzed showed a marked
increase in CD2S-expressing cells, peaking between days S and
8 of drug treatment (Fig. 3A). Next we analyzed the effect of
8-Cl-cAMP administration on a natural killer subpopulation of
circulating lymphocytes, as identified by immunoreaction with
anti-CDS6 and anti-CD16 antibodies. As shown in Fig. 3B, we
found a 3- to 4-fold increase of CDS6/16-positive cells at all
Research. on March 13, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
A
�0
EVaaVVIi
0
B
�0
0)
E
E
U
00
00
Fig. I Effect of 8-Cl-cAMP treatment on serum creatinine levels (A)
and serum calcium levels (B). Determinations were performed at theindicated time points in the 17 patients evaluated for each cycle of
treatment. Data shown are relative to the first cycle of treatment of 15
patients. Serum calcium values have been corrected on the basis ofalbumin levels. Dotted line, upper limit of normal values.
8 10 12
Days of Treatment
380 Phase I Clinical Study with 8-Chloro-eAMP
Table 2 Toxicit y (WHO) at different dose levels
Dose levels
I Level (4)” II Level (4) III Level (8) IV Level (15) V Level (3) VI Level (2)-
Hematological flh n n
Hemorrhage n n n n n n
Gastrointestinal n n n n n n
Nausea/vomiting n n n n n n
Diarrhea n n n n n n
Renal/bladder
creatinine n n n n Grade I (2/’ Grade 4(1)
Grade 3 (1)Blood urea nitrogen n n n n n Grade 2 (1)Proteinuria n n n n Grade I (1) Grade 1 (2)Fever n n n n n n
Allergic n n n n n n
Other n n n n n n
a Numbers in parentheses, cycles of treatment.
1� n, none.
dose levels, suggesting that 8-Cl-cAMP may contribute to an
expansion of this specific cell population.
To evaluate whether the increased number of CD56/16-
positive cells correlated also with an increased cytotoxic poten-
tial of circulating lymphocytes, we have evaluated the cytolytic
activity using as target the K562 human leukemic cell line.
K562 cytolysis, as determined by specific release of LDH, was
dramatically increased in all patients by day 5 of 8-Cl-cAMP
administration, reaching in some cases values up to 100%
(Fig. 3C).
Antitumor Activity. Although the purpose of this study
was not the evaluation of the therapeutic effect of 8-Cl-cAMP,
we have obtained evidence of antitumor activity in four patients.
In fact, of three patients with advanced colon cancer refractory
to standard chemotherapy with 5-fluorouracil and folinic acid
and that received multiple cycles of 8-Cl-cAMP at the fourth
dose level, one patient exhibited about 70% reduction in a
retroperitoneal lymph nodal mass of 4 x 5 cm after the two
cycles of 8-Cl-cAMP received and progressed 2 months after
completing the treatment. The other two patients had a stable
disease after four cycles of 8-Cl-cAMP with a follow-up of 4
and 7 months, respectively. The remaining three patients of the
fourth dose level, who received up to two cycles of treatment,
showed disease progression 1 or 2 months after the end of
treatment. Furthermore, a patient affected by rapidly progressive
lung adenocarcinoma with several intrathoracic metastatic sites
and that failed to respond to three different regimens of chemo-
therapy was enrolled at the third dose level and no progression
was observed after the administration of six cycles of 8-Cl-
cAMP. Notably, this stabilization of the disease has been lasting
up to 15 months.
DISCUSSION
During the past several years a large amount of experimen-
tal data has been generated on the ability of 8-Cl-cAMP to
selectively modulate the expression of the PKA isoforms, lead-
ing to inhibition of cancer cell growth in vitro and in vivo at
micromolar concentrations (3). Preclinical studies in dogs have
shown that the administration of 8-Cl-cAMP by continuous iv.
Research. on March 13, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
APlasma concentntlons of �-a-c�Mi’
Dose L�vthI 11 U m m IV IV IV V VI
PIu.akvth 260 340 400 455 4�I 685 830 700 1200 1790
A
U
0
>
0
0.
0
C0U
a0.
H III IV
0 2 4 6 8 10 12 14 16 18 20 22
j
1��
0
0
Time (Days)
Fig. 2 8-Cl-cAMP plasma levels as determined by HPLC analysis. In
A, 8-Cl-cAMP plasma concentations were determined daily. Each num-ber refers to the value obtained at day 3 and represents a different patientat the indicated dose level. Drug infusion was discontinued after 4 days
in patients at the V and VI dose level as renal toxicity appeared. B,
time-concentration profile of 8-Cl-cAMP in two patients enrolled at theIV and V dose levels that are not represented in A. Four hundred ng8-Cl-cAMP/i ml plasma correspond to about I p.M.
infusion for a prolonged time (up to 30 days) allows plasma
levels to reach the micromolar range, with toxic effects mainly
detected in the kidney and the gastrointestinal tract (23). To
reduce the risk of toxicity deriving from a prolonged treatment
we have designed the present Phase I clinical trial introducing
periods of rest between the courses of drug infusion, in order to
allow for host recovery. To determine the MTD and the toxicity
of 8-Cl-cAMP in humans, six dose levels of drug were studied,
starting from a dose approximately 30-fold lower than that
producing toxicity in dogs. Thirty-six cycles of treatment were
administered to 17 patients with cancers refractory to standard
therapies.
The only toxic effect observed consisted of altered renal
function. The DLT was reached at the sixth dose level when a
grade 4 and a grade 3 increase in serum creatinine with protein-
uria occurred in two patients. At the fifth dose level two patients
in one cycle experienced a grade 1 increase in serum creatinine
which returned to basal levels promptly upon drug discontinu-
ation. This was then considered the MTD. Although definitive
data on the mechanism of renal toxicity are not yet available,
toxicology studies conducted in mice and dogs have described
renal tubular necrosis as a major histopathology finding (23). In
our patients the urinalyses have shown proteinuria but not
inversion of the electrolytes, supporting the hypothesis that
8-Cl-cAMP may determine direct toxicity rather than alteration
of renal perfusion. Unlike the study in dogs, which showed
60
40
20
0
Fig. 3 Immunological effects of 8-Cl-cAMP treatment on circulating
lymphocytes. Flow cytometric determination of CD25-positive cells (A)
was carried out on two patients at the I dose level, two patients at the II dose
level, one patient at the III dose level, and three patients at the IV dose level,respectively. Where shown, data represent the average ± SD. Flow cyto-
metric determination of CD56/16-positive cells (B) was carried out on onepatient at the I dose level, one patient at the II dose level, one patient at the
III dose level, three patients at the IV dose level, two patients at the V dose
level, and two patients at the VI dose level, respectively. Where shown, data
represent the average ± SD. Cytolytic activity (C) is referred to one cycle
for each patient. Data represent the average value of two different experi-ments, each performed in triplicate. SD was less than 10%.
gastrointestinal toxicity, no similar effect was observed in pa-
tients of the present study. It has been proposed that RIa/PKAI
are increased in cells that are at an early stage of differentiation
Clinical Cancer Research 381
B 1800
1700
�. 1600
E 1500
� 1400
a 1300
a 1200.2 1100.� 1000
.� 900
V 800
� 700
c� 600� 500E 400
.� 3000. 200
100
B35 - prstr.otm.nt
� day 5
� day 8
30
.� 25k- _____T
:� � Ic056116�10 20
0- 15
�
0
C
80
II II IV V VI
day 5
jILLII I It II III Itt IV IV IV
Dose Levels
Research. on March 13, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

382 Phase I Clinical Study with 8-Chloro-cAMP
S A. L. Harris, personal communication.
and/or are rapidly proliferating. Although a recent study by
Pinto et al. (31) on cells from acute myeloid leukemia patients
has shown that 8-Cl-cAMP is able to selectively inhibit the
self-renewal of the leukemic stem cell and therefore may not
directly affect normal hemopoiesis, there has been concern
about the potential hematological toxicity of 8-Cl-cAMP. In this
study we have performed blood cell counts and evaluated he-
moglobin concentration, and no toxicity was observed at any
dose level or following repeated courses of 8-Cl-cAMP.
Several patients experienced an increase in serum calcium
levels at the end of the first week of infusion, which recovered
during the days of rest. Determination of PTH levels in two
patients who did not experience toxicity revealed PTH values
below the detectable levels, suggesting that hormonal regulation
may be implicated for this phenomenon. Similar results were
obtained in a parallel trial at the University of Oxford where an
extensive study of this phenomenon has been conducted.5 It has
been shown that hypercalcemia is often due to PTH-like pep-
tides acting through the cAMP-mediated pathway (32). It is
possible that, at least in some of the patients, 8-Cl-cAMP
determines hypercalcemia with a negative feedback on PTH
secretion by acting downstream to PTH-related molecules.
HPLC-based determination of 8-Cl-cAMP plasma levels
demonstrated that 8-Cl-cAMP administered as continuous infu-
sion rapidly reaches the steady-state concentrations up to the
fourth dose level while, at higher doses, plasma levels increase
after a few days of infusion in parallel to the appearance of renal
toxicity. These results confirm the data previously reported in
mice and dogs and recently described in a study conducted in
humans receiving continuous infusion of 8-Cl-cAMP (33). More
important, our data show that 8-Cl-cAMP at nontoxic doses
reached micromolar concentrations that were in the range of
those effective in producing growth inhibition in the majority of
human cancer cells previously tested (3, 19). Interestingly, un-
like the results obtained in dogs, even at higher dose levels no
gastrointestinal toxicity was observed in our patients. In vitro
studies have shown that, in the presence of fresh bovine serum,
8-Cl-cAMP is cleaved by phosphodiesterases and S’-nucleoti-
dases, resulting in the production of 8-Cl-adenosine (34), a
metabolite which contributes to the growth inhibitory effect of
8-Cl-cAMP (35, 36) but is also responsible for some of the toxic
effects observed in dogs (23). However, it has been recently
demonstrated that human plasma contains a limited amount of
the cleaving enzymes, especially phosphodiesterase III, as com-
pared to cell culture conditions or to other animal models (19),
thus limiting the production of metabolites such as 8-CI-aden-
osine. A recent study conducted by Cummings et al. (33) on
humans treated with 8-Cl-cAMP in continuous infusion con-
firmed the lack of metabolites such as 8-Cl-adenosine in their
plasma. Taken together these results suggest that production of
8-Cl-cAMP metabolites may be different among species, thus
accounting also for differential sensitivity to their toxic effects.
The mechanism of action of 8-Cl-cAMP suggest that it
may have a wide spectrum of effects on different cell types and
compartments. Because of the important role played by PKAI in
the regulation of immune response, we have investigated
whether 8-Cl-cAMP may exert a modulatory effect on the
immune system. We observed that at all dose levels 8-Cl-cAMP
markedly increases the expression of IL-2 receptor a as deter-
mined by measuring the positivity of anti-CD2S-reacting lym-
phocytes. Moreover, measurement of CDS6/1 6-positive cells
showed a marked increase in this specific subset of natural killer
cells, which play a major role in antibody-dependent cell cyto-
toxicity (37). To determine whether 8-Cl-cAMP causes only an
expansion of these cell populations or enhances also their cyto-
lytic potential, we have measured the killing activity of circu-
lating lymphocytes against K562 cells by the use of a LDH
release cytotoxic assay. At all dose levels tested there was an
increase in the cytotoxicity of PBL against K562 cells which, in
some patients, reached values up to 100% LDH-specific release.
Most of the effects observed on the immunological parameters
studied are unrelated to the 8-Cl-cAMP dose, as they occur at all
dose levels. It is likely that 8-Cl-cAMP concentrations obtained
in our patients even at the lower dose levels exceed the mini-
mum required for activation of certain immune effector func-
tions.
We are currently investigating whether these effects are
directly induced by 8-Cl-cAMP on lymphocytic effectors or are
mediated by cytokines released by unidentified cell targets of
the drug. In fact, the modulatory effects of 8-Cl-cAMP strongly
resemble those produced by certain cytokines, such as IL-2 and
interferons (37).
Although the determination of the clinical activity of 8-Cl-
cAMP was not the purpose of our study we have obtained
evidence of antitumor activity in several patients.
Preclinical studies have suggested that 8-Cl-cAMP, an
analogue of a physiological molecule, may be an anticancer
drug through its peculiar action on one of the key mechanisms
of neoplastic transformation (3). In addition, 8-Cl-cAMP is able
to revert the MDR phenotype in several MDR cancer cell lines
(19). From the present study it appears that 8-Cl-cAMP also
produces immunological effects in vivo, which may themselves
turn to be of therapeutic benefit.
To our knowledge the present study is the first Phase I
clinical trial of 8-Cl-cAMP in cancer patients. We have dem-
onstrated that the MTD for the schedule of administration ana-
lyzed is 0.2 mg/kg/h and that toxicity is confined to the kidney.
Pharmacokinetic analysis demonstrated that 8-Cl-cAMP at the
concentration of 0.125 mg/kg/h, a dose devoided of toxicity
corresponding to the fourth dose level, achieves plasma concen-
trations in the potential therapeutic range. Finally, 8-Cl-cAMP
has a clear biomodulatory effect as shown by the changes in
some immunological parameters. The studies conducted thus far
in vitro and in animal models demonstrate that 8-Cl-cAMP is a
cytostatic and a differentiating agent rather than a cytotoxic
drug, suggesting that administration for prolonged time may be
a more successful treatment modality. For these reasons we
believe that a dose completely devoid of any toxicity should be
used for further studies. In this regard, a dose of 0.125 mg/kg/h
may be suggested for a Phase II clinical trial and/or for combi-
nation with other anticancer agents. Such studies are currently in
progress at our institution.
Research. on March 13, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Clinical Cancer Research 383
ACKNOWLEDGMENTS
We are indebted to Dr. Y. S. Cho-Chung for her fundamental
findings and leading research on 8-Cl-cAMP that made possible this
clinical work. We thank G. Borriello for excellent technical assistance
and Professor Adrian L. Harris for helpful discussions and critical
reading of the manuscript.
REFERENCES
1. Pastan, I., Johnson, G. S., and Anderson, W. B. Role of cyclic
nucleotides in growth control. Annu. Rev. Biochem., 44: 491-522,
1975.
2. Cho-Chung, Y. S. Perspectives in cancer research: role of cAMP
receptor proteins in growth, differentiation, and suppression of malig-nancy: new approaches to therapy. Cancer Res., 50: 7093-7100, 1990.
3. Cho-Chung, Y. S., Clair, T., Tortora, G., and Yokozaki, H. Role of
site selective cAMP analogues in the control and reversal of malig-
nancy. Pharmacol. Ther., 50: 1-33, 1991.
4. Beebe, S., Holloway, R., Rannels, S. R., and Corbin, J. D. Two
classes of cAMP analogues which are selective for the two different
cAMP-binding sites of type II protein kinase demonstrate synergism
when added together to intact adipocytes. J. Biol. Chem., 259: 3539-
3547, 1984.
5. Beebe, S. J., and Corbin, J. D. Cyclic nucleotide-dependent proteinkinases. In: P. D. Boyer and E. G. Krebs (eds.), The Enzymes: Control
by Phosphorylation, pp. 43-111. New York: Academic Press, 1986.
6. Taylor, S. S., Buechier, J. A., and Yonemoto, W. cAMP-dependent
protein kinase: framework for a diverse family of regulatory enzymes.
Annu. Rev. Biochem., 59: 971-1005, 1990.
7. Ciardiello, F., Tortora, G., Kim, N., Clair, T., Ally, S., Salomon,
D. S., and Cho-Chung, Y. S. 8-Cl-cAMP inhibits transforming growth
factor a transformation of mammary epithelial cells by restoration of the
normal mRNA patterns for cAMP-dependent protein kinase regulatory
subunit isoforms which show disruption upon transformation. J. Biol.
Chem., 265: 1016-1020, 1990.
8. Ciardiello, F., Pepe, S., Bianco, C., Baldassarre, G., Ruggiero, A.,
Bianco, C., Selvam, M. P., Bianco, A. R., and Tortora, G. Downregu-lation of RIa subunit of the cAMP-dependent protein kinase induces
growth inhibition of human mammary epithelial cells transformed by
c-Ha-ras and c-erbB-2 protooncogenes. Int. J. Cancer, 53: 438-443,
1993.
9. Miller, W. R., Watson, D. M. A., Jack, W., Chetty, U., and Elton,R. A. Tumor cyclic AMP binding proteins: an independent prognosticfactor for disease recurrence and survival in breast cancer. Breast Cancer
Res. Treat., 26: 89-94, 1993.
10. Miller, W. R., Hulme, M. J., Cho-Chung, Y. S., and Elton, R. A.
Types of cyclic AMP binding proteins in human breast cancer. Eur. J.Cancer, 29A: 989-991, 1993.
11. Tortora, G., Pepe, S., Cirafici, A. M., Ciardiello, F., Porcellini, A.,Clair, T., Colletta, G., Cho-Chung, Y. S., and Bianco, A. R. Thyroid-
stimulating hormone-regulated growth and cell cycle distribution of
thyroid cells involve type I isozyme of cyclic AMP-dependent protein
kinase. Cell Growth & Differ., 4: 359-365, 1993.
12. Pepe, S., Ruggero, A., Tortora, G., Ciardiello, F., Garbi, C.,Yokozaki, H., Cho-Chung, Y. S., Clair, T., SkAlegg, B., and Bianco,A. R. FIow-cytometric detection of the RIa subunit of type I cAMP-
dependent protein kinase in human cells. Cytometry, 15: 73-79, 1994.
13. Schwartz, D. A., and Rubin, C. S. Identification and differential
expression of two forms of regulatory subunits (RI!) of cAMP-depen-
dent protein kinase II in Friend erythroleukemic cells. J. Biol. Chem.,
260: 6296-6303, 1985.
14. Tagliaferri, P., Katsaros, D., Clair, T., Ally, S., Tortora, G., Neck-
ers, L., Rubalcava, B, Parandoosh, Z., Chang, Y. A., Revankar, G. R.,Crabtree, G. W., Robins, R. K., and Cho-Chung, Y. S. Synergistic
inhibition of growth of breast and colon human cancer cell line by
site-selective cAMP analogs. Cancer Res., 48: 1642-1650, 1988.
15. Rohlff, C., Clair, 1., and Cho-Chung, Y. S. 8-Cl-cAMP inducesdown-regulation of the RIa subunit and up-regulation of the RIII3
subunit of cAMP-dependent protein kinase leading to type II holoen-
zyme-dependent growth inhibition and differentiation of HL-60 leuke-
mia cells. J. Biol. Chem., 268: 5774-5782, 1993.
16. Ally, S., Clair, T., Katsaros, D., Tortora, G., Yokozaki, H., Finch, R.
A., Avery, T. L., and Cho-Chung, Y. S. Inhibition of growth and
modulation of gene expression in human lung carcinoma in athymic
mice by site-selective 8-Cl-cAMP. Cancer Res., 49: 5650-5655, 1989.
17. Tortora, G., Yokozaki, H., Pepe, S., Clair, T., and Cho-Chung, Y. S.
Differentiation of HL-60 leukemia by type I regulatory subunit antisense
oligodeoxynucleotide of cAMP-dependent protein kinase. Proc. NatI.
Acad. Sci. USA, 88: 2011-2015, 1991.
18. Yokozaki, H., Budillon, A., Tortora, G., Meissner, S., Beaucage, S.,
Miki, H., and Cho-Chung, Y. S. An antisense oligodeoxynucleotide that
depletes RI�,, subunit of cAMP-dependent protein kinase induces growth
inhibition in human cancer cells. Cancer Res., 53: 868-872, 1993.
19. Yokozaki, H., Budillon, A., Clair T., Kelley K., Cowan K. H.,
Rohlff C., Glazer R. I., and Cho-Chung, Y. S. 8-Chloroadenosine3’,5’-monophosphate as a novel modulator of multidrug resistance. Int.
I. Oncol., 3: 423-430, 1993.
20. Tagliaferri, P., Katsaros, D., Clair, T., Neckers, L., Robins, K. R.,
and Cho-Chung, Y. S. Reverse transformation of Harvey sarcoma virus-transformed NIH/3T3 cells by site-selective cyclic AMP analogs. J. Biol
Chem., 263: 409-416, 1988.
21. Tortora, G., Ciardiello, F., Ally, S., Clair, T., Salomon, D. S. and
Cho-Chung, Y. S. Site-selective 8-chloro-adenosine 3,5’ monophos-phate inhibits transformation and transforming growth factor a produc-
tion in Ki-ras-transformed rat fibroblasts. FEBS Lett., 242: 363-367,
1989.
22. Malspeis, L., and Kemmenoe, B. H. Distribution and rapid excre-
tion of [2-3H]-8-Cl-cAMP in mice by whole-body autoradiography of
cryosections (Abstract 2263). Proc. Am. Assoc. Cancer Res., 31: 382,
1990.
23. Tomaszewski, J. E, Sparks, R. M., Rose, L. M., Heath, J. E., andPage, 1. G. Plasma drug levels and toxicity produced by intravenousinfusions of 8-chloro-cyclic AMP (8-Cl-cAMP, NSC 614491) to Beagle
dogs (Abstract 2529). Proc. Am. Assoc. Cancer Res., 32: 425, 1991.
24. Kammer, G. M. The adenylate cyclase-cAMP-protein kinase A
pathway and regulation of the immune response. Immunol. Today, 9:
222-229, 1988.
25. Averill, L. E., Stein, R. L., and Kammer, G. M. Control of humanT-lymphocyte interleukin-2 production by a cAMP-dependent pathway.Cell. Immunol., 115: 88-99, 1988.
26. Laxminarayana, D., Berrada, A., and Kammer, G. M. Early events
of human T lymphocyte activation are associated with type I proteinkinase A activity. J. Clin. Invest., 92: 2207-2214, 1993.
27. Sk#{128}lhegg, B. S., Tasken, K., Hansson V., Huitfield, H. S., Jahnsen,
T., and Lea, T. Location of cAMP-dependent protein kinase type I with
the TCR-CD3 complex. Science (Washington DC), 263: 84-87, 1994.
28. Janssen, R. A. J., Sleijfer, D. T., Heijn, A. A., Mulder, N. H., The,
T. H., and de Leij, L. Peripheral blood lymphocyte number and pheno-
type prior to therapy correlate with response in subcutaneously applied
rlL-2 therapy of renal cell carcinoma. Br. I. Cancer, 66: 1177-1179,
1992.
29. Decker, T., and Lohmann-Matthes, M-L. A quick and simple
method for the quantitation of lactate dehydrogenase release in mea-
surements of cellular cytotoxicity and tumor necrosis factor (TNF)
activity. I. Immunol. Methods, 115: 61-69, 1988.
30. Palmieri, G., Morabito, A., Lauria, R., Montesarchio, V., Matano,
E., Memoli, B., Libetta, C., Rea, A., Merola, C., Correale, P., Leo, L.,
Tagliaferri, P., and Bianco, A. R.. Low dose dopamine induces early
recovery of recombinant interleukin-2 impaired renal function. Eur. J.
Cancer, 29: 1119-1122, 1993.
31. Pinto, A., Aldinucci, D., Gattei, V., Zagonel, V., Tortora, G.,Budillon, A., and Cho-Chung, Y. S. Inhibition of the self-renewalcapacity of blast progenitors from acute myeloblastic leukemia patients
by site selective 8-chloro-cyclic adenosine 3’,5’-monophosphate (8-Cl-
cAMP). Proc. Natl. Acad. Sci. USA, 89: 8884-8888, 1992.
Research. on March 13, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

384 Phase I Clinical Study with 8-Chloro-cAMP
32. Moseley, I. M., Kuboyta, M., and Diefenbach-Jagger, H. Parathy-
roid hormone-related protein purified from a human lung cancer cell
line. Proc. Natl. Acad. Sci. USA, 84: 5048-5052, 1987.
33. Cummings, I., Leonard, R. C. F., and Miller, W. R. Sensitive
determination of 8-chloroadenosine 3 ‘-5 ‘-monophosphate and 8-chloro-
adenosine in plasma by high-performance liquid chromatography. J.
Chromatogr., 658: 183-188, 1994.
34. Van Lookeren Campagne, M. M., Diaz, F. V., Jastorif, B., and
Kessin, R. 8-Chioroadenosine 3’,5’-monophosphate inhibits the growth
of Chinese hamster ovary and Molt-4 cells through its adenosine me-
tabolite. Cancer Res., 51: 1600-1605, 1991.
35. Langeveld, C. H., Jongenelen, C. A. M., Heimans, J. J., and Stoof,J. C. Growth inhibition of human glioma cells induced by 8-chloroad-
enosine, an active metabolite of 8-chloro cyclic adenosine 3 ‘ :5 ‘-mono-phosphate. Cancer Res., 52: 3994-3999, 1992.
36. Lange-Carter, C. A., Vuillequez, I. I., and Malkinson, A. M.
8-Chloroadenosine mediates 8-chloro-cyclic AMP-induced down-regu-lation of cyclic AMP-dependent protein kinase in normal and neoplastic
mouse lung epithelial cells by a cyclic AMP-independent mechanism.
Cancer Res., 53: 393-400, 1993.
37. Voss, D. S., and Sondel, P. M. The clinical biology and mechanism
of action of systemically administered IL-2. In: M. Mitchell (ed),Biological Approaches to Cancer Treatment: Biomodulation, pp. 411-439. New York: McGraw-Hill, 1993.
Research. on March 13, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
1995;1:377-384. Clin Cancer Res G Tortora, F Ciardiello, S Pepe, et al. immunological effects in cancer patientsPhase I clinical study with 8-chloro-cAMP and evaluation of
Updated version
http://clincancerres.aacrjournals.org/content/1/4/377
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/1/4/377To request permission to re-use all or part of this article, use this link
Research. on March 13, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from





























