Embed Size (px)
Citation preview
HerzrhythmusstörungenVorhofflimmern
Bernhard Zrenner
Medizinische Klinik IKrankenhaus Landshut-Achdorf
Lehrkrankenhaus der Technischen Universität München
1. UNABHÄNGIGER FORTBILDUNGSKONGRESSDER ÄRZTEKAMMER BERLIN
1. DEZEMBER 2012
conflict of interest
Referentenhonorar: St. Jude, Bard, Medtronic
Gesponserte Studien an Klinik: Biotronic, Guidant, St. Jude
AntiarrhythmikaHistorische Fakten
70er-Jahre Ventrikuläre Arhythmien im LZ-EKG nach MyokardinfarktPrädiktiv hinsichtlich Mortalität
80er Jahre Entwicklung zahlreicher Antiarrhythmika
EncainideFlecainideLorcainideMoricizinePirmenolPenticainideMescainideTocainideIndocainideRecainamPropafenoneDiprafenoneNicainoprolol
SotalolD-Sotalol

Zweifel ist der Weisheit Anfang
Descartes
90er-Jahre Randomisierte Studien bei ventrikulären Arrhythmienbei Postinfarkt-Patienten
AntiarrhythmikaKlasse-I-AA
1991 CAST Flecainide, Encainidenach 10 Monaten abgebrochenMortalität 8,3% gegen 3,5% bei Placebo
1992 CAST II MoricizineMortalität 7,2% gegen 5,4% bei Placebo
1992 Metaanalyse Klasse-I-Antiarrhythmika51 randomisierten Studien, 11.712 Infarktpatienten Mortalität 5,6% gegen 5,0% bei Placebo
D Echt, NEJM 1991CAST II Investigators, NEJM 1992K Teo, JAMA1993
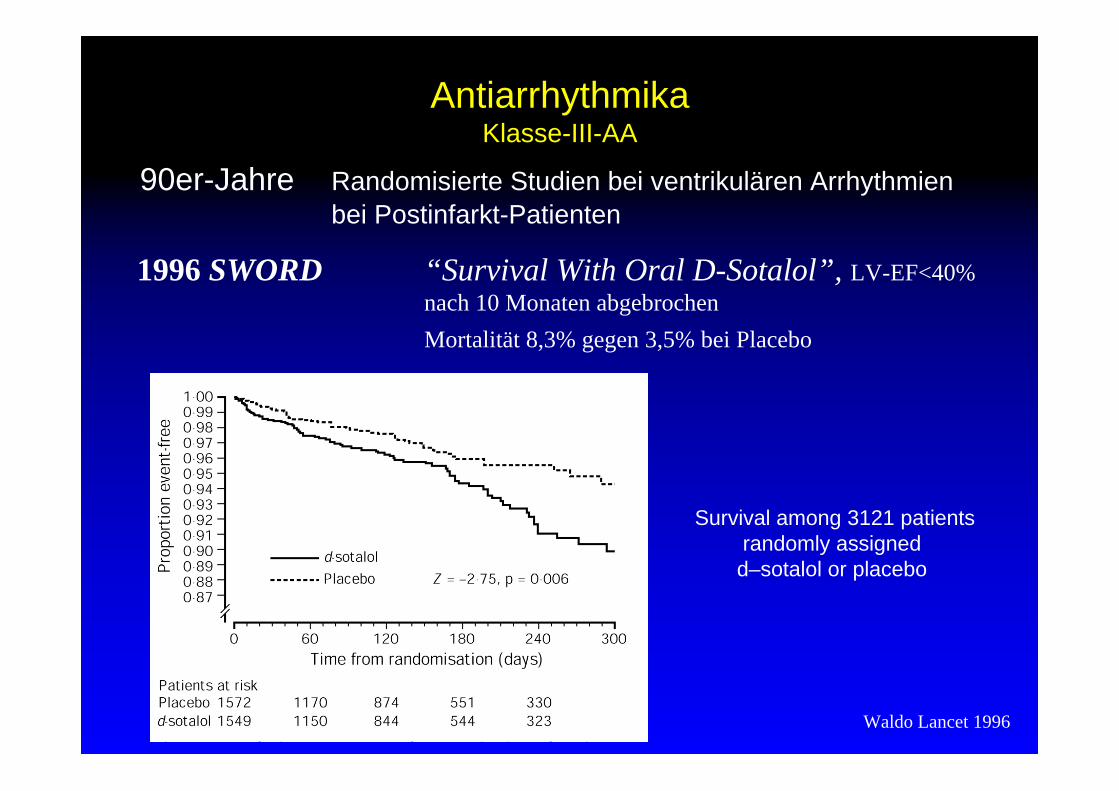
90er-Jahre Randomisierte Studien bei ventrikulären Arrhythmienbei Postinfarkt-Patienten
AntiarrhythmikaKlasse-III-AA
1996 SWORD “Survival With Oral D-Sotalol”, LV-EF<40%nach 10 Monaten abgebrochenMortalität 8,3% gegen 3,5% bei Placebo
Waldo Lancet 1996
Survival among 3121 patients randomly assignedd–sotalol or placebo
AA zur Behandlung ventrikulärer Arrhythmien
VES nicht behandlungsbedürftig/ nicht behandelbar
ICD-Therapie
Über 25 Jahre keine Neu-Zulassung von AA
Auch aus Steinen, die in den Weg gelegt werden,kann man Schönes bauen.
Johann Wolfgang von Goethe
AA zur Behandlung supraventrikulärer Arrhythmien
Elektrophysiologische Ablation-Therapie>95% Erfolgsrate, außer bei AF
Vorhofflimmern + reduzierte EF: keine AA
Frequenz- versus Rhythmuskontrolle
In allen Dingen ist hoffen besser als verzweifeln.
Johann Wolfgang von Goethe
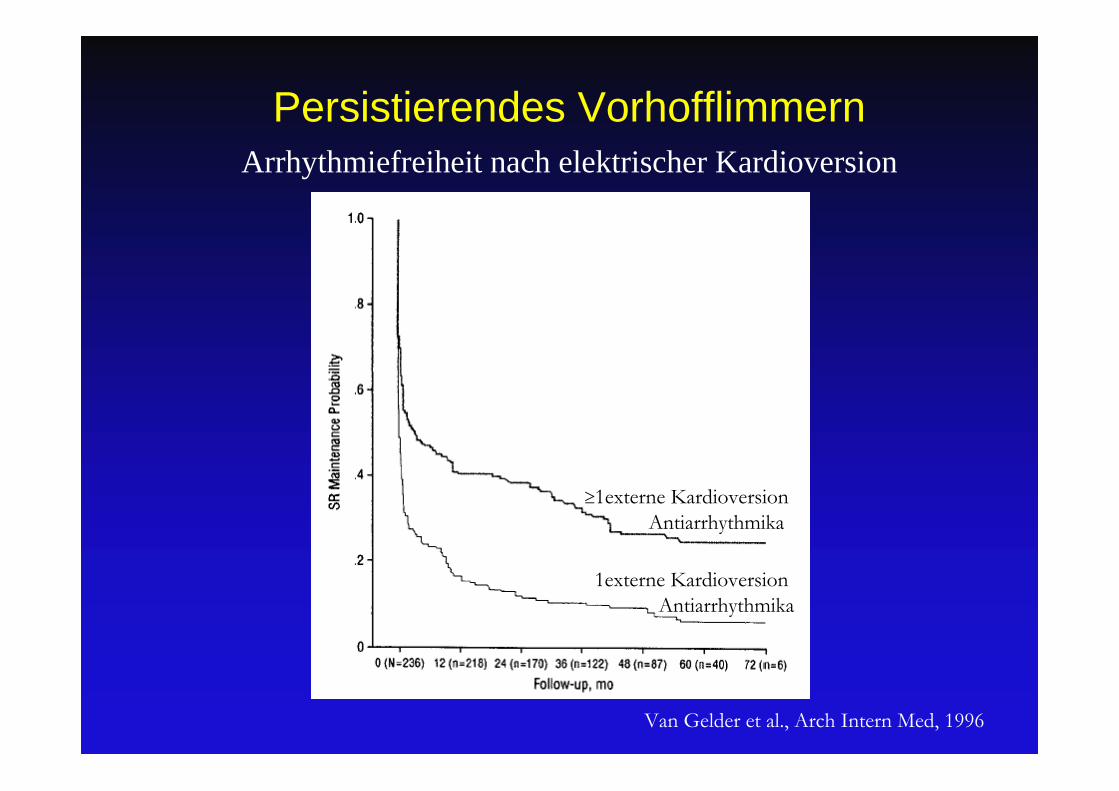
Van Gelder et al., Arch Intern Med, 1996
Persistierendes Vorhofflimmern Arrhythmiefreiheit nach elektrischer Kardioversion
1externe KardioversionAntiarrhythmika
1externe KardioversionAntiarrhythmika
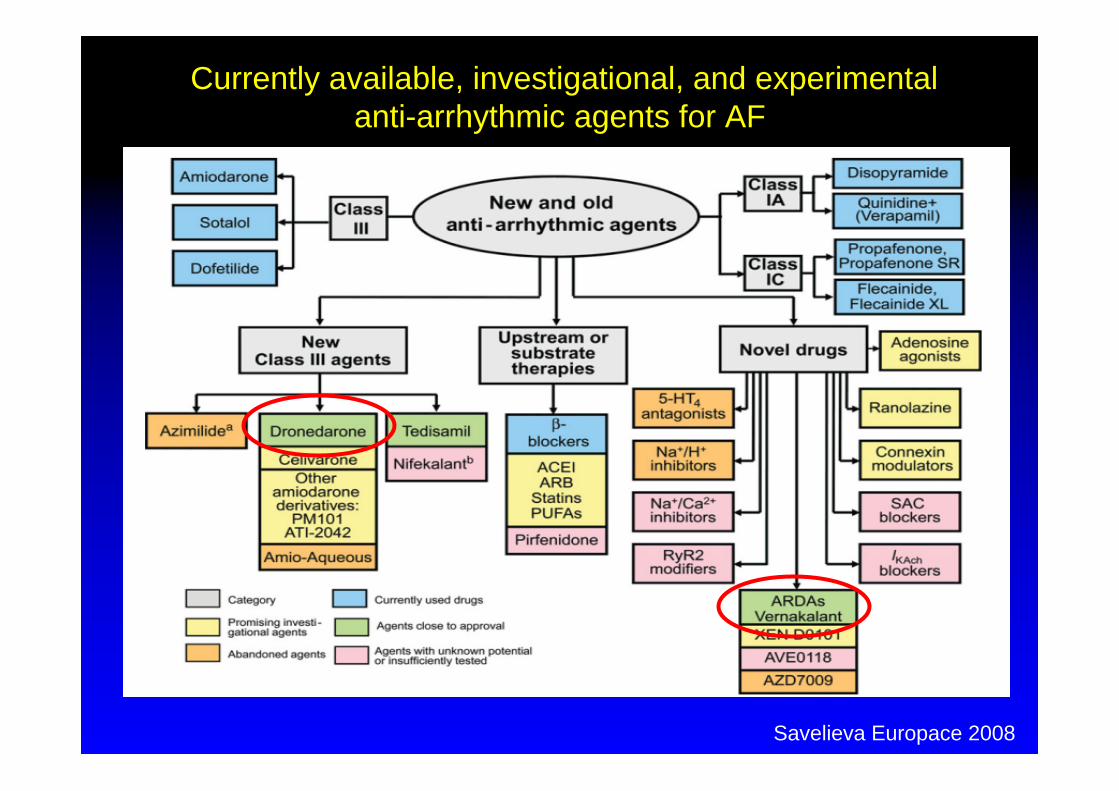
Currently available, investigational, and experimental anti-arrhythmic agents for AF
Savelieva Europace 2008
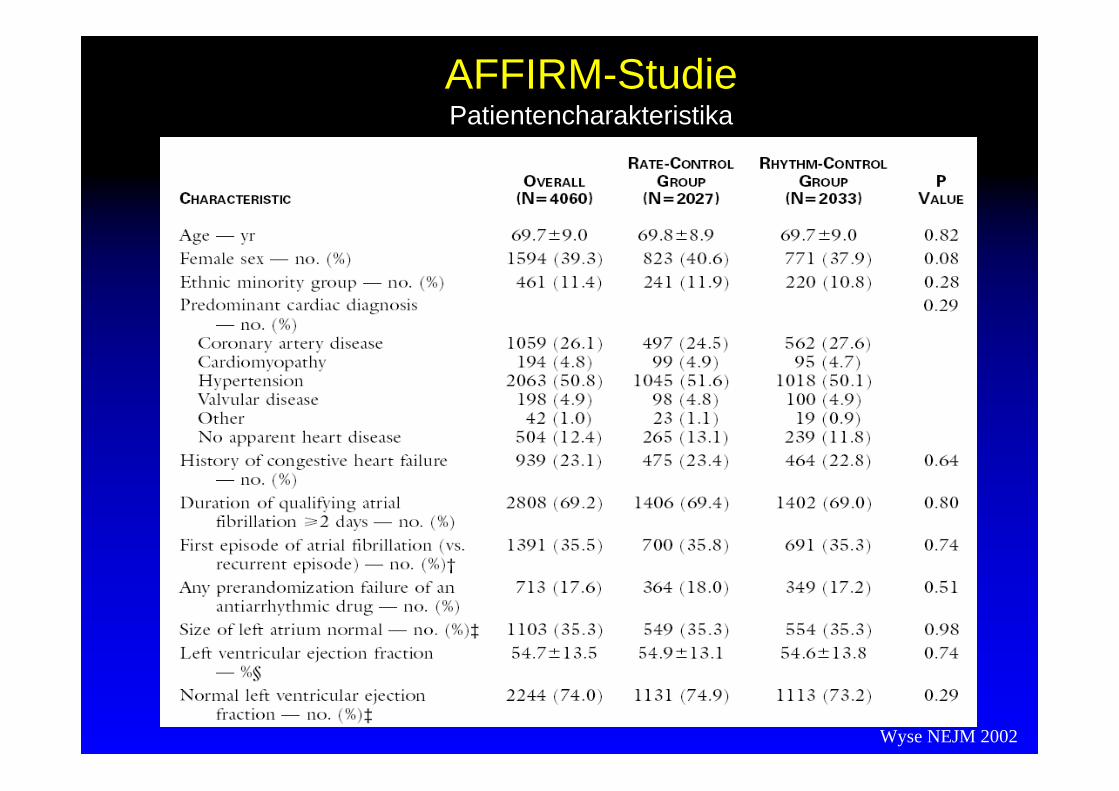
AFFIRM-StudiePatientencharakteristika
Wyse NEJM 2002
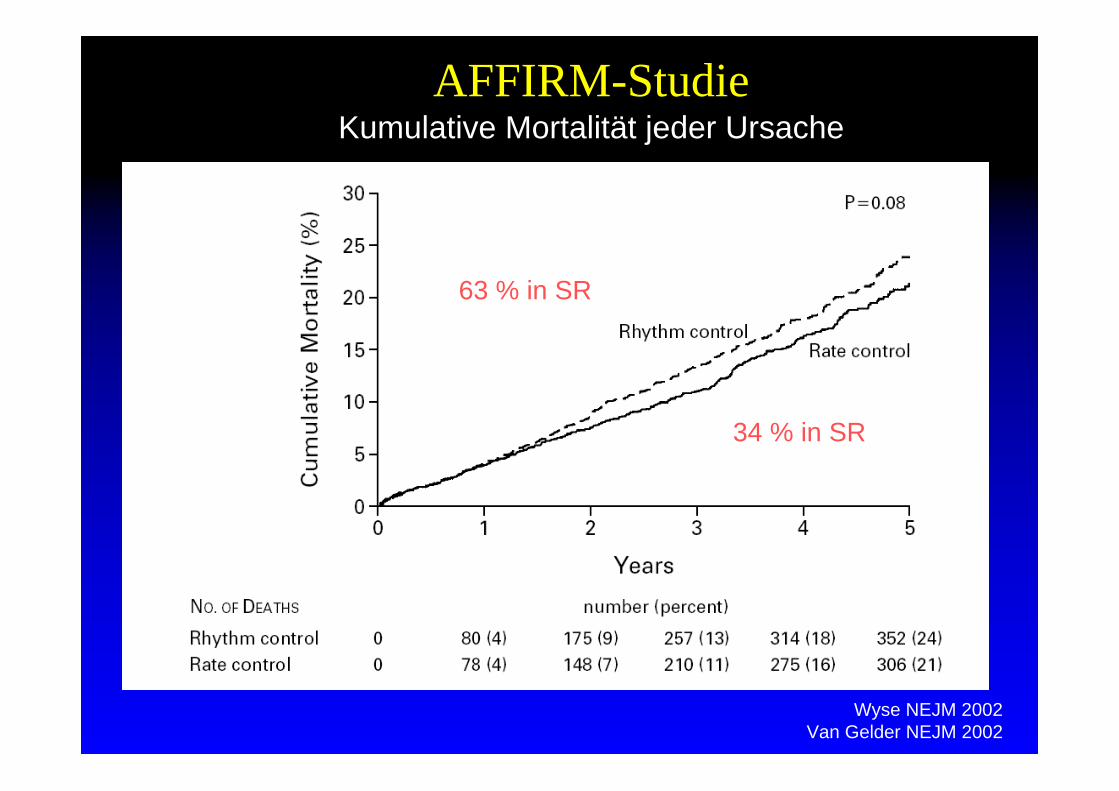
AFFIRM-StudieKumulative Mortalität jeder Ursache
63 % in SR
34 % in SR
Wyse NEJM 2002Van Gelder NEJM 2002
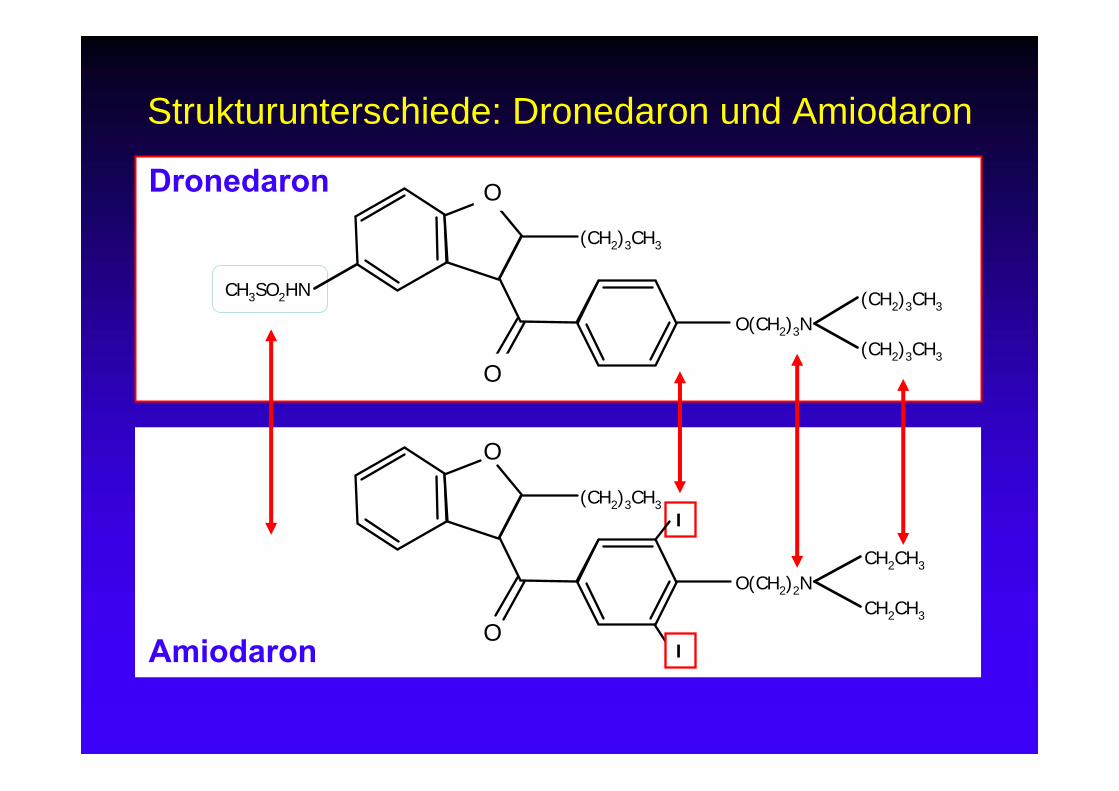
Strukturunterschiede: Dronedaron und Amiodaron
Dronedaron
CH3SO2HN
O(CH2)3N
O
O
(CH2)3CH3
(CH2)3CH3
Amiodaron
O(CH2)2N
O
O
CH2CH3
CH2CH3
(CH2)3CH3
(CH2)3CH3I
I
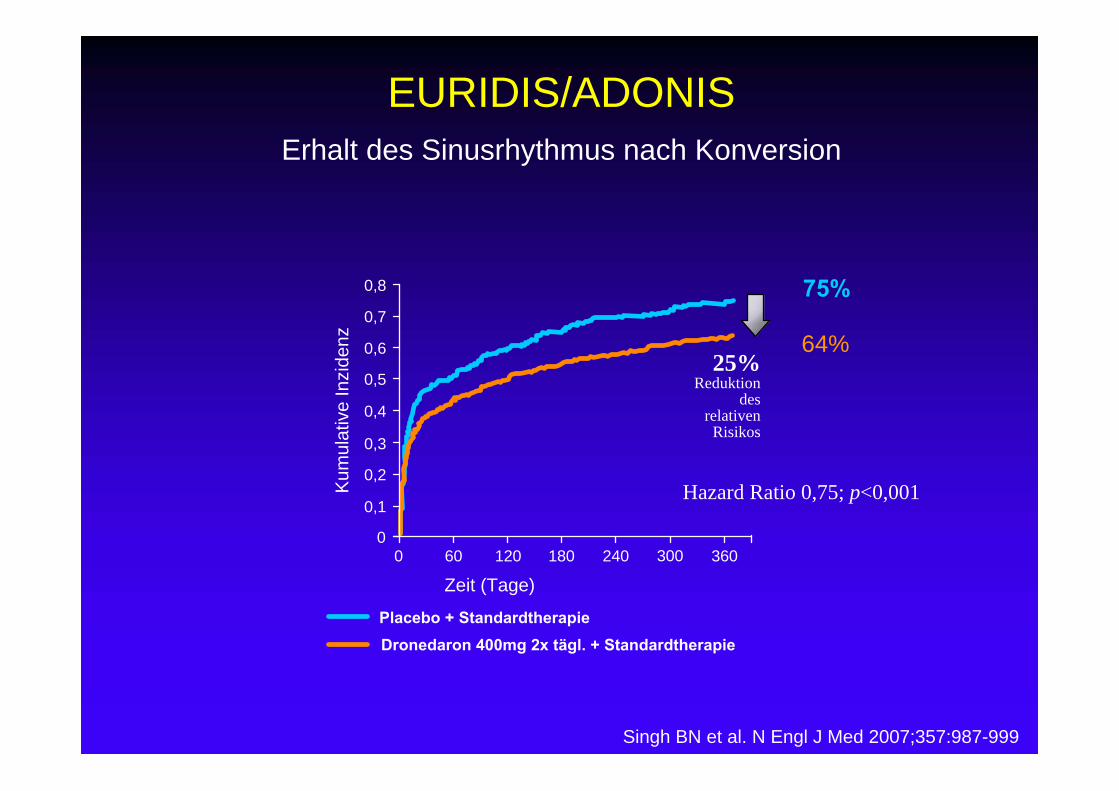
Erhalt des Sinusrhythmus nach Konversion
Singh BN et al. N Engl J Med 2007;357:987-999
Placebo + StandardtherapieDronedaron 400mg 2x tägl. + Standardtherapie
0 60 120 180 240 360
Zeit (Tage)
Kum
ulat
ive
Inzi
denz
0,7
0,6
0,5
0,4
0,3
0,2
0,1
0300
0,8
Hazard Ratio 0,75; p<0,001
25%Reduktion
des relativen
Risikos
EURIDIS/ADONIS
75%
64%
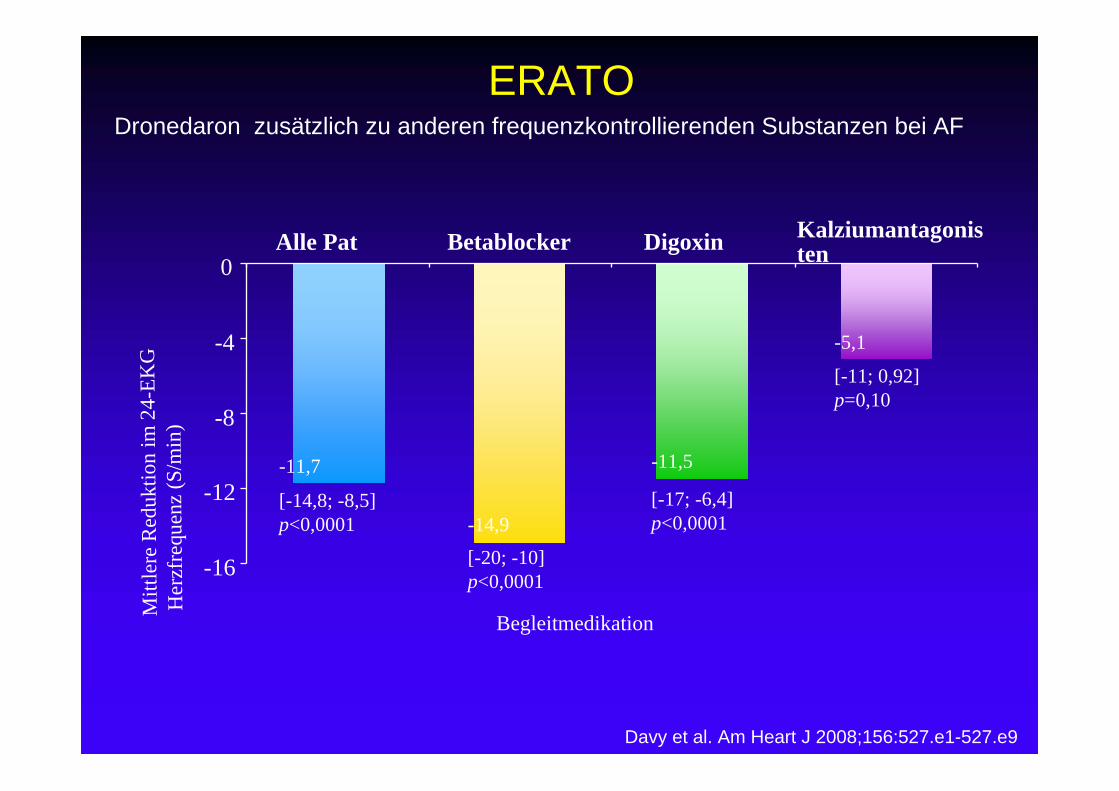
ERATODronedaron zusätzlich zu anderen frequenzkontrollierenden Substanzen bei AF
Davy et al. Am Heart J 2008;156:527.e1-527.e9
Mitt
lere
Red
uktio
n im
24-
EKG
Her
zfre
quen
z (S
/min
)
Begleitmedikation
Betablocker Digoxin KalziumantagonistenAlle Pat
-16
-12
-8
-4
0
-14,9
[-20; -10]p<0,0001
-11,7
[-14,8; -8,5]p<0,0001
-11,5
[-17; -6,4]p<0,0001
-5,1
[-11; 0,92]p=0,10
Køber L et al. NEJM 2008;358:2678-2687
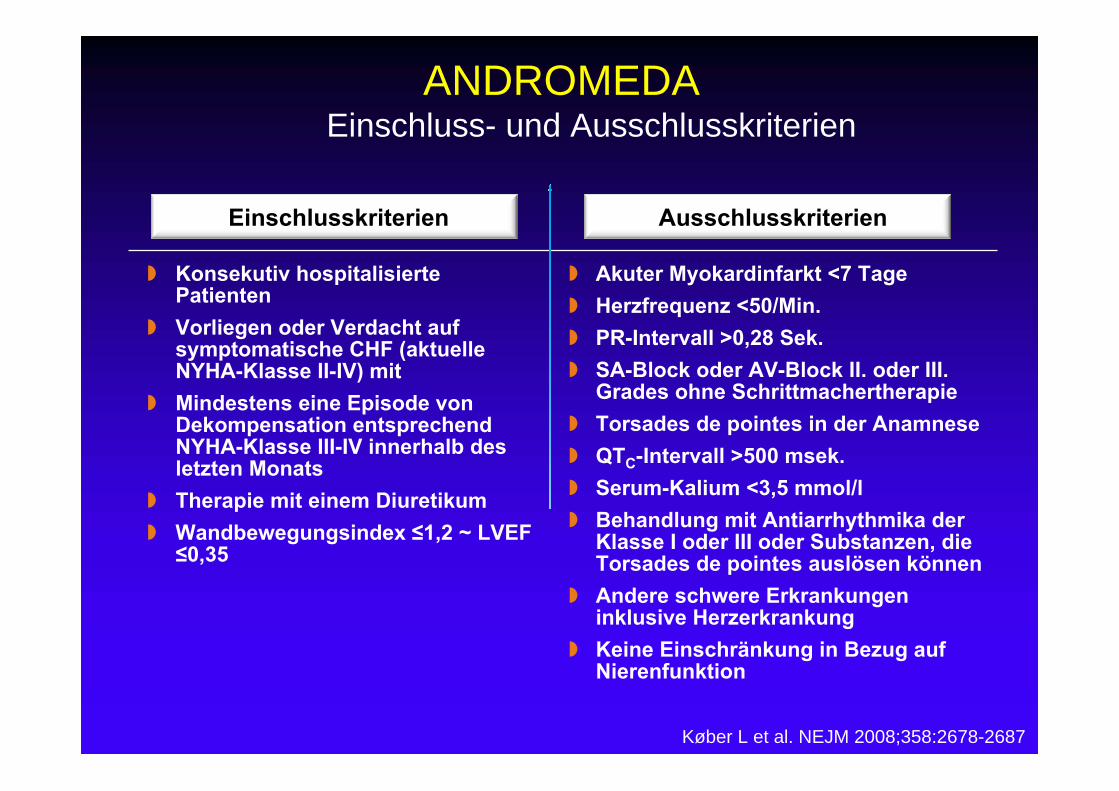
ANDROMEDAEinschluss- und Ausschlusskriterien
Einschlusskriterien Ausschlusskriterien
Konsekutiv hospitalisierte Patienten
Vorliegen oder Verdacht auf symptomatische CHF (aktuelle NYHA-Klasse II-IV) mit
Mindestens eine Episode von Dekompensation entsprechend NYHA-Klasse III-IV innerhalb des letzten Monats
Therapie mit einem Diuretikum Wandbewegungsindex ≤1,2 ~ LVEF
≤0,35
Akuter Myokardinfarkt <7 Tage Herzfrequenz <50/Min. PR-Intervall >0,28 Sek. SA-Block oder AV-Block II. oder III.
Grades ohne Schrittmachertherapie Torsades de pointes in der Anamnese QTC-Intervall >500 msek. Serum-Kalium <3,5 mmol/l Behandlung mit Antiarrhythmika der
Klasse I oder III oder Substanzen, die Torsades de pointes auslösen können
Andere schwere Erkrankungen inklusive Herzerkrankung
Keine Einschränkung in Bezug auf Nierenfunktion
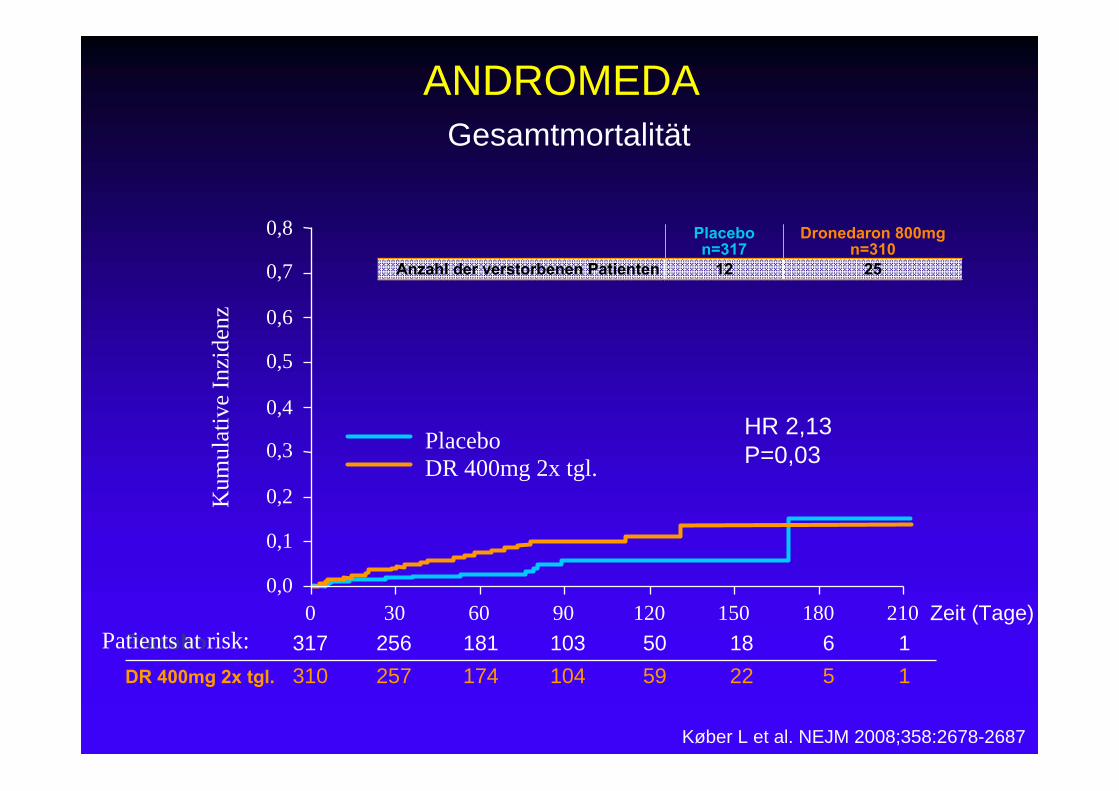
Gesamtmortalität
Zeit (Tage)
Kum
ulat
ive
Inzi
denz
Placebo 317 256 181 103 50 18 6 1DR 400mg 2x tgl. 310 257 174 104 59 22 5 1
0 30 60 90 120 150 180 2100,0
0,1
0,2
0,3
0,6
0,8
0,4
0,5
0,7
PlaceboDR 400mg 2x tgl.
Køber L et al. NEJM 2008;358:2678-2687
Placebon=317
Dronedaron 800mgn=310
Anzahl der verstorbenen Patienten 12 25
Patients at risk:
HR 2,13P=0,03
ANDROMEDA
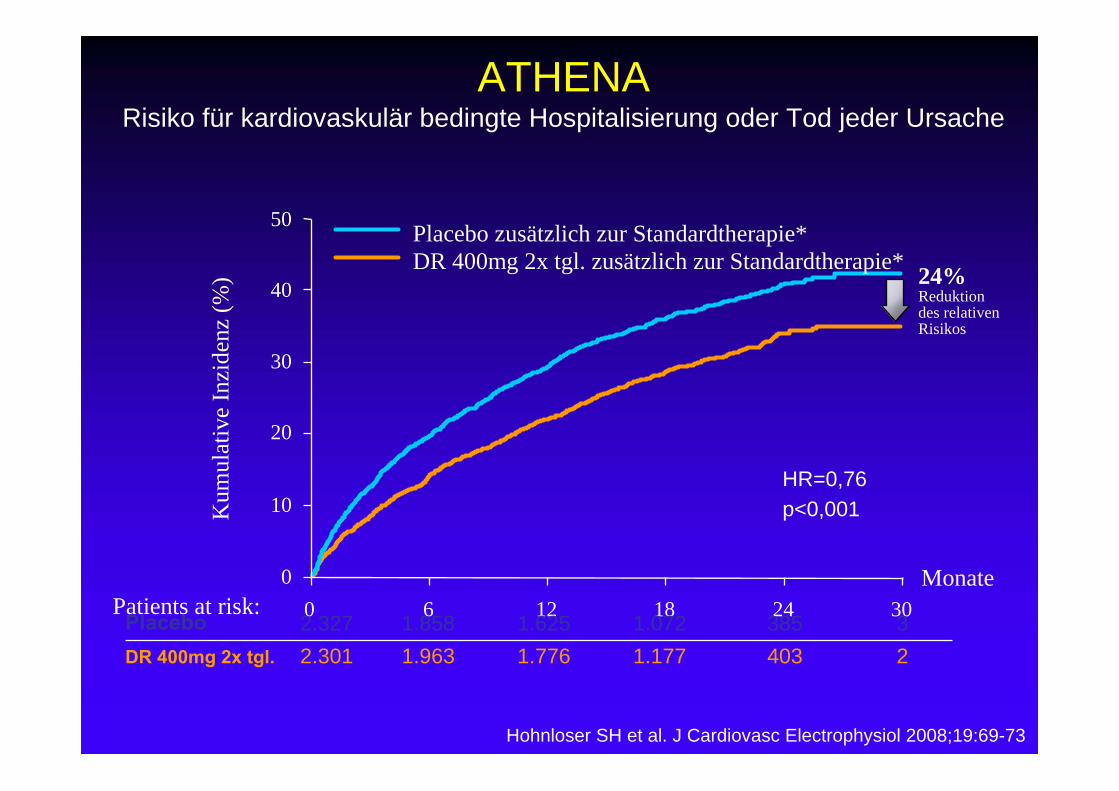
Hohnloser SH et al. J Cardiovasc Electrophysiol 2008;19:69-73
ATHENARisiko für kardiovaskulär bedingte Hospitalisierung oder Tod jeder Ursache
Monate0
10
20
40
50
30
Kum
ulat
ive
Inzi
denz
(%)
6 12 18 24 300
Placebo zusätzlich zur Standardtherapie*DR 400mg 2x tgl. zusätzlich zur Standardtherapie*
HR=0,76p<0,001
Placebo 2.327 1.858 1.625 1.072 385 3DR 400mg 2x tgl. 2.301 1.963 1.776 1.177 403 2
24%Reduktion des relativenRisikos
Patients at risk:
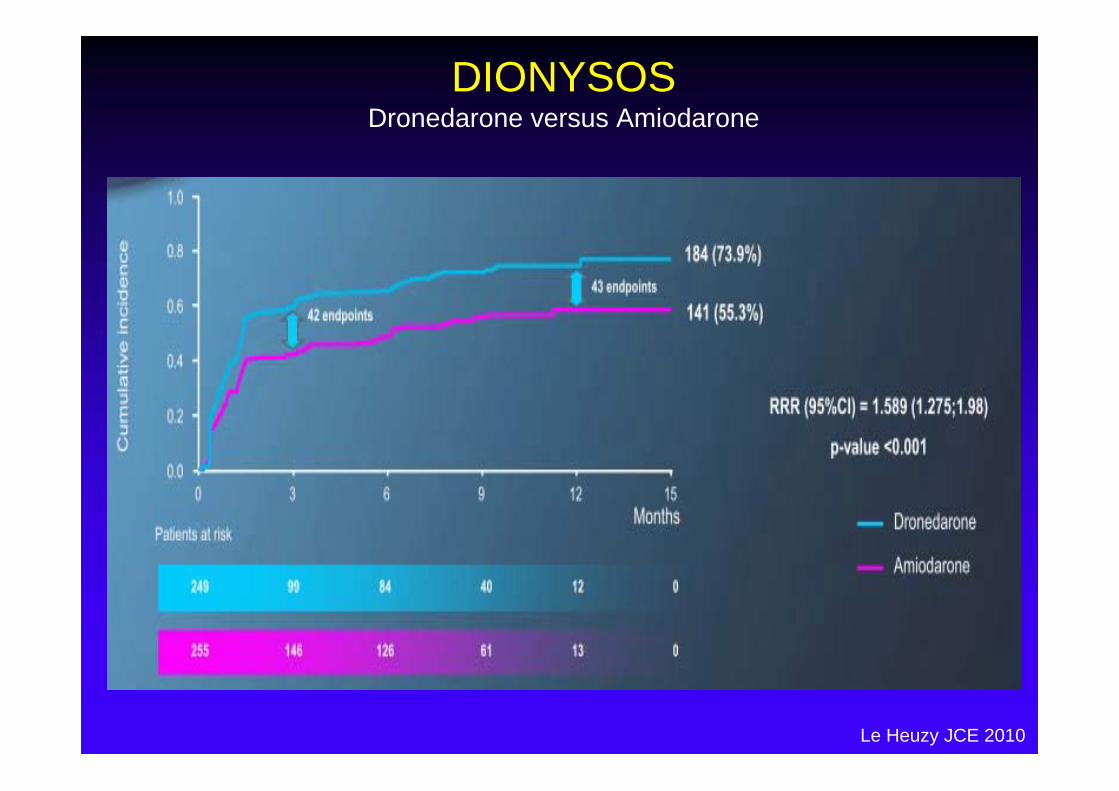
DIONYSOSDronedarone versus Amiodarone
Le Heuzy JCE 2010
PallasPermanentes AF und zusätzliche Risikofaktoren
Patientenkollektiv
•>65 J• KHK, Myokardinfarkt, AP• Z.n. TIA oder Schlaganfall• Symptomatisch Herzinsuffizienz• LV-EF<40%• PAVK
•> 75 J + Art. Hypertonie + D. mell.
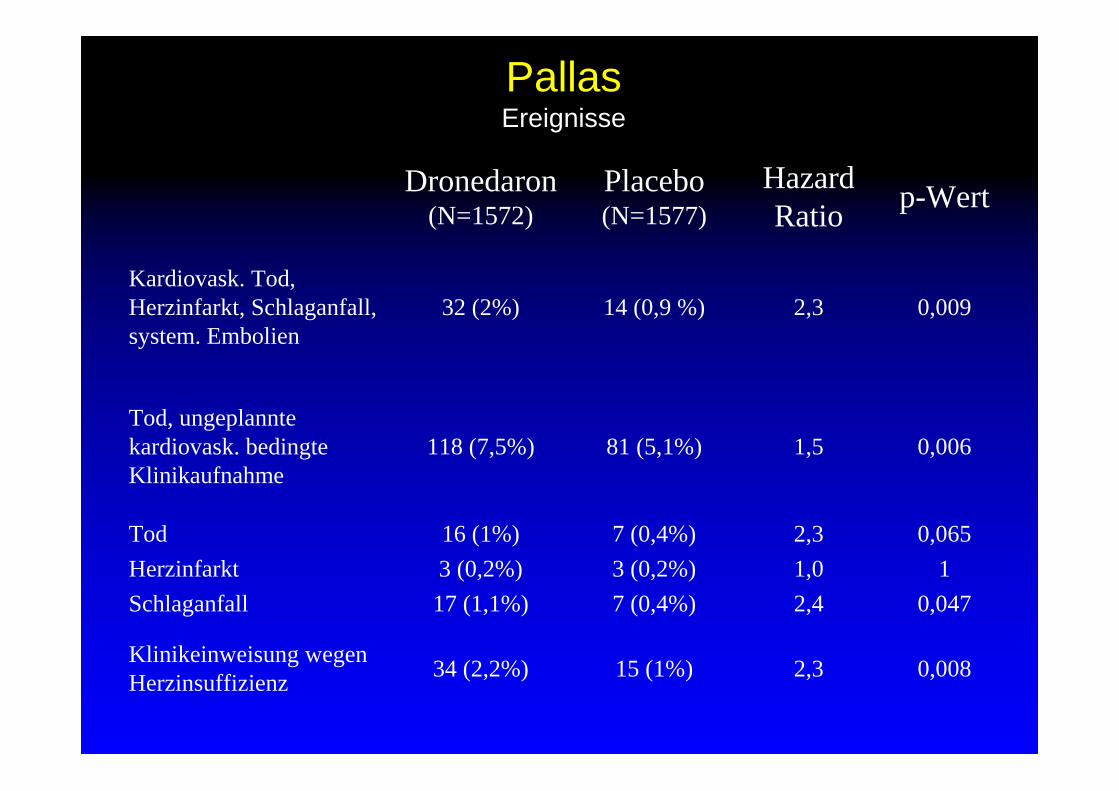
Dronedaron(N=1572)
Placebo(N=1577)
HazardRatio p-Wert
Kardiovask. Tod, Herzinfarkt, Schlaganfall, system. Embolien
32 (2%) 14 (0,9 %) 2,3 0,009
Tod, ungeplannte kardiovask. bedingte Klinikaufnahme
118 (7,5%) 81 (5,1%) 1,5 0,006
Tod 16 (1%) 7 (0,4%) 2,3 0,065Herzinfarkt 3 (0,2%) 3 (0,2%) 1,0 1Schlaganfall 17 (1,1%) 7 (0,4%) 2,4 0,047
Klinikeinweisung wegen Herzinsuffizienz 34 (2,2%) 15 (1%) 2,3 0,008
PallasEreignisse
DronedaronIndikationseinschränkung
Dronedaron nur noch zur Aufrechterhaltung von
Sinusrhythmus nach erfolgreicher Kardioversion
bei Patienten mit nichtpermanentem
Vorhofflimmern
erst, nachdem alternative Therapien in Betracht
gezogen wurden.
DronedaronIndikationseinschränkung
Kontraindiziert bei jeglicher Herzinsuffizienz und
linksventrikulärer Dysfunktion.
Bislang gehörte nur schwere Herzinsuffizienz zu den
Gegenanzeigen.
DronedaronNeue Nebenwirkungen
neu hinzugekommen: pulmonale Toxizität
US-amerikanische Produktinformation mit Hinweis auf die
nach Markteinführung von Dronedaron gemeldeten
Berichte über interstitielle Lungenerkrankung
einschließlich Pneumonitis und Lungenfibrose
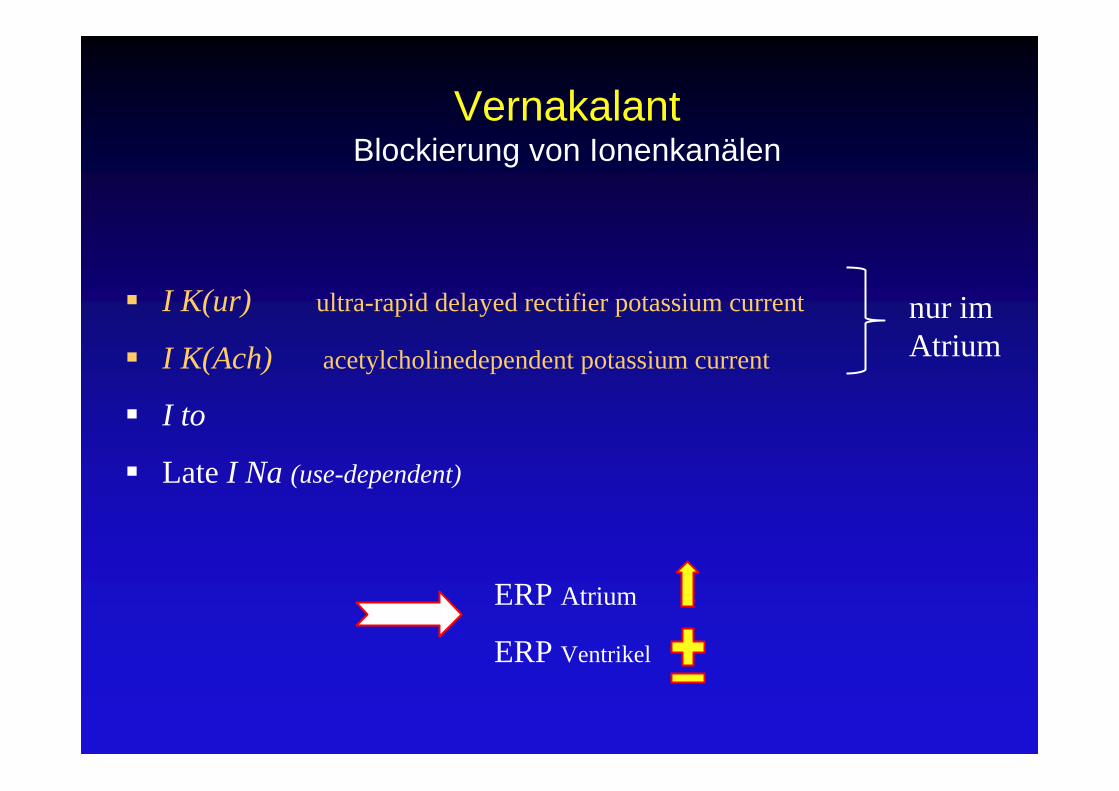
VernakalantBlockierung von Ionenkanälen
I K(ur) ultra-rapid delayed rectifier potassium current
I K(Ach) acetylcholinedependent potassium current
I to
Late I Na (use-dependent)
nur im Atrium
ERP Atrium
ERP Ventrikel
VernakalantPharmakokinetik
Intravenöse Verabreichung
Lineare Kinetik und 2-Komponenten-Modell
Mittlere Plasmakonzentration nach10-min Infusion
t1/2 2.9 h Frauen, 3.3 h in Männer
Metabolisierung über Cytochrom P450 (CYP2D6)
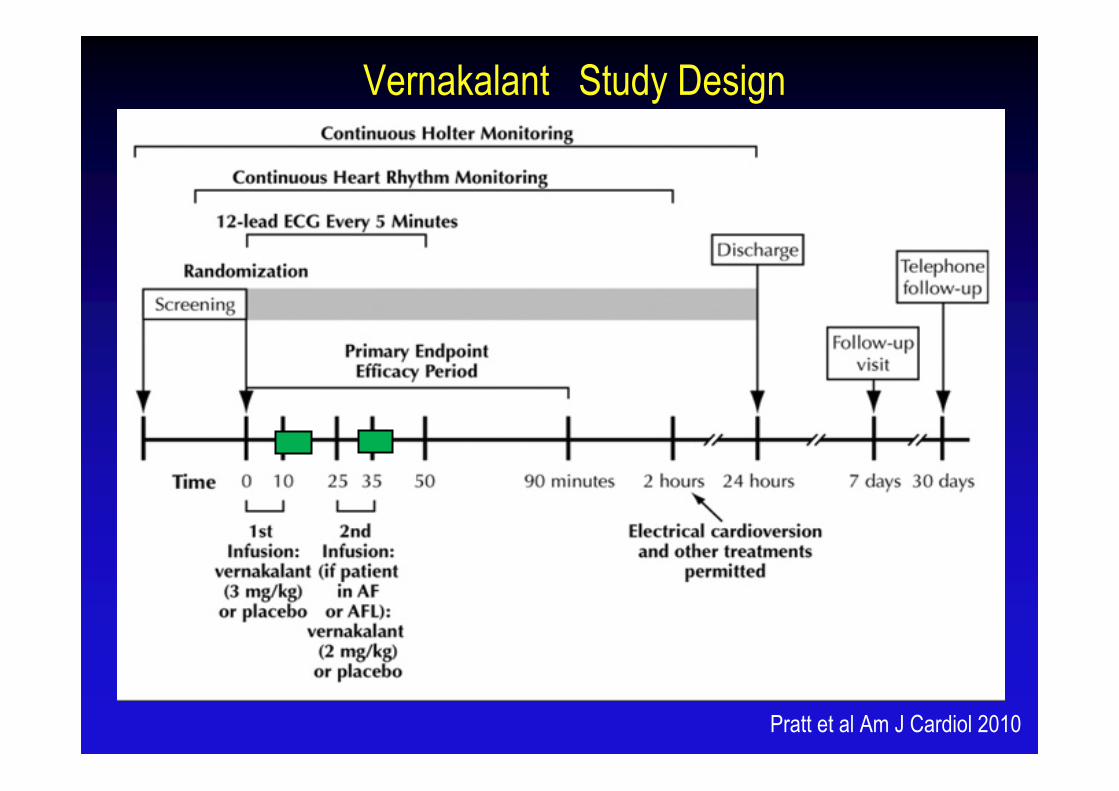
Vernakalant Study Design
Pratt et al Am J Cardiol 2010
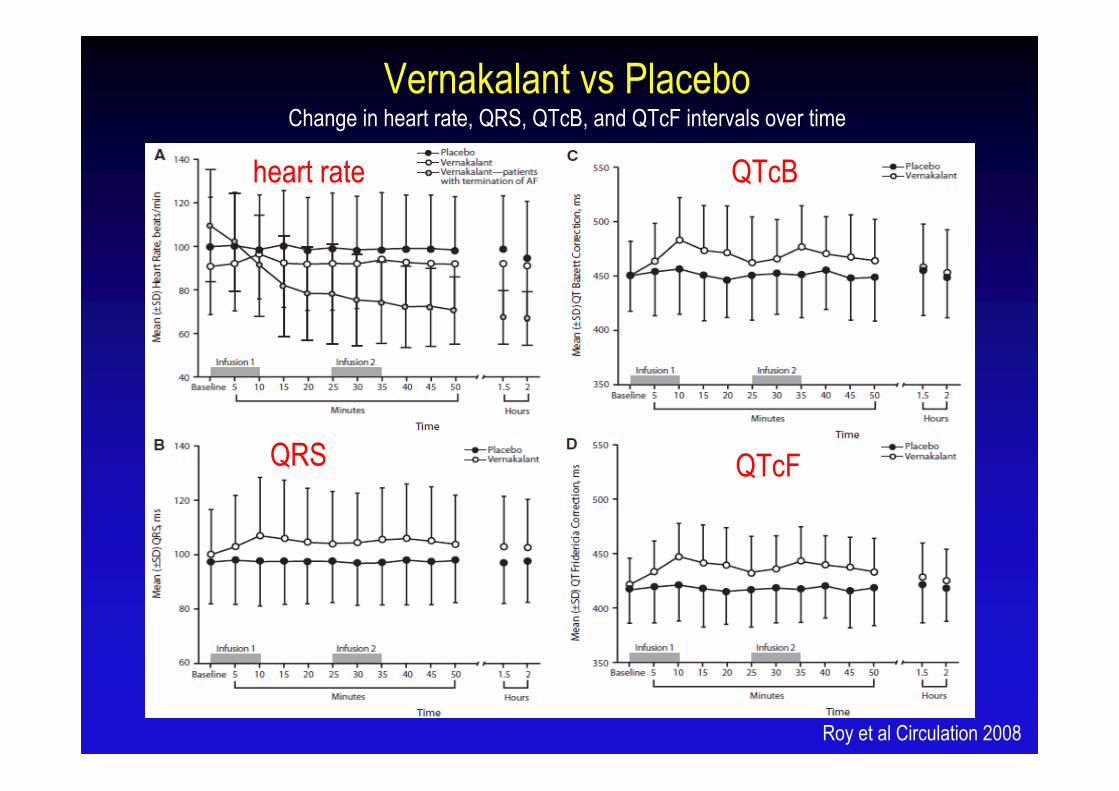
Vernakalant vs PlaceboChange in heart rate, QRS, QTcB, and QTcF intervals over time
Roy et al Circulation 2008
heart rate
QRS
QTcB
QTcF
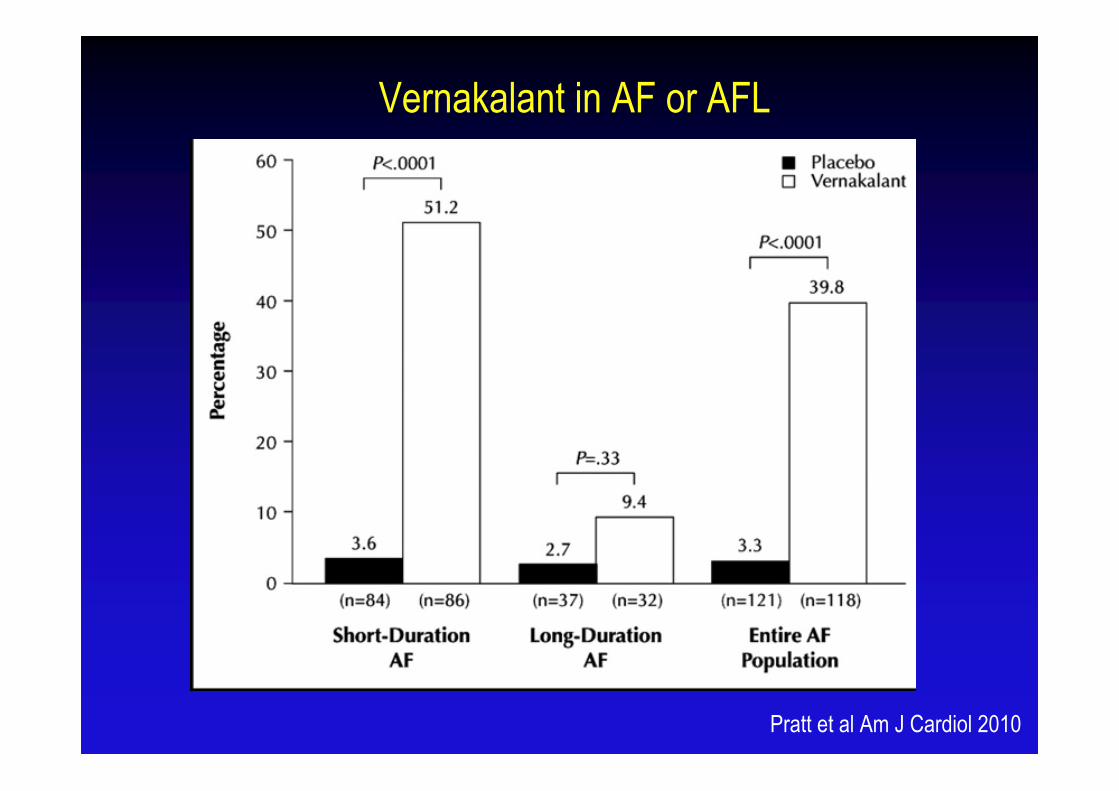
Vernakalant in AF or AFL
Pratt et al Am J Cardiol 2010
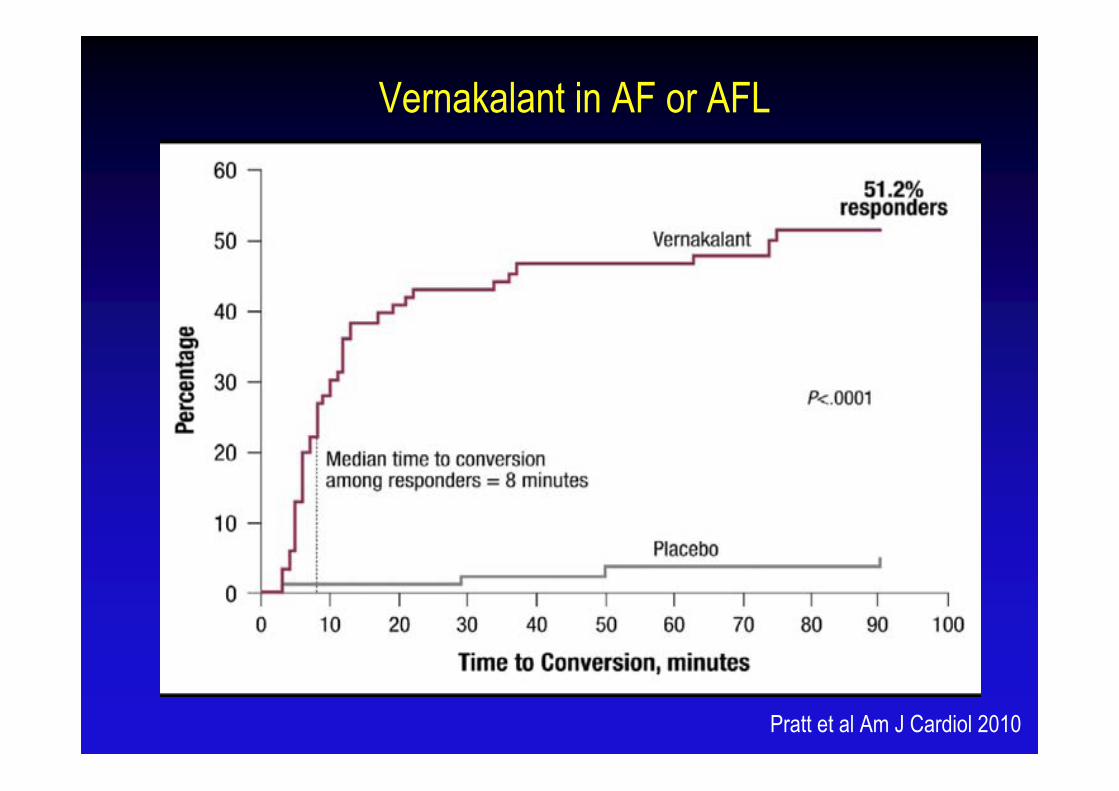
Vernakalant in AF or AFL
Pratt et al Am J Cardiol 2010
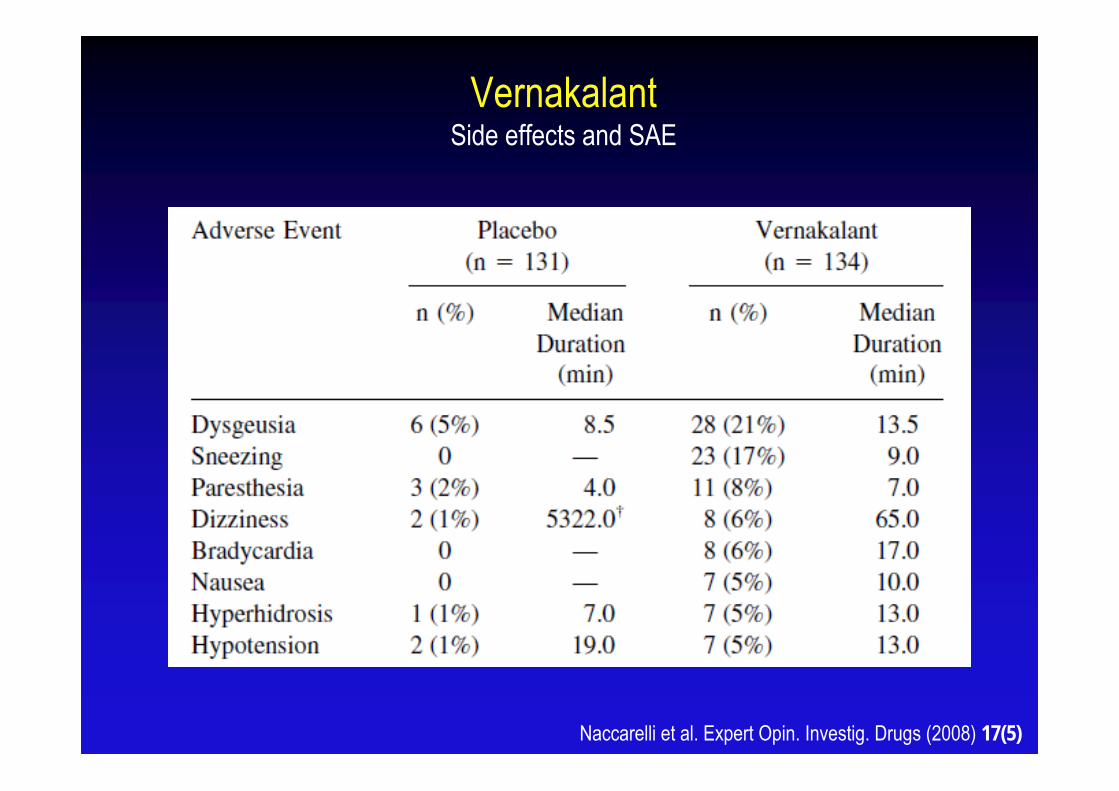
VernakalantSide effects and SAE
Naccarelli et al. Expert Opin. Investig. Drugs (2008) 17(5)
VernakalantSide effects and SAE
Maximal QT interval increase by 20 ms
Three cases of torsade de pointes
Two cases of ventricular fibrillation
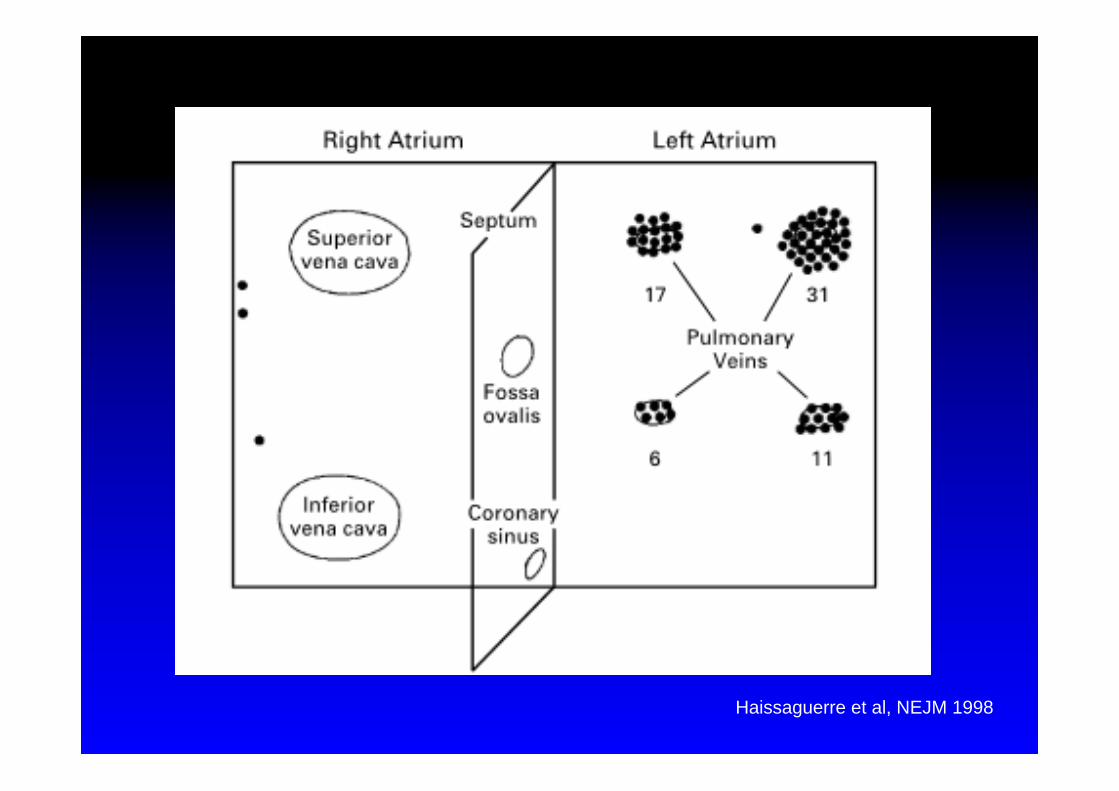
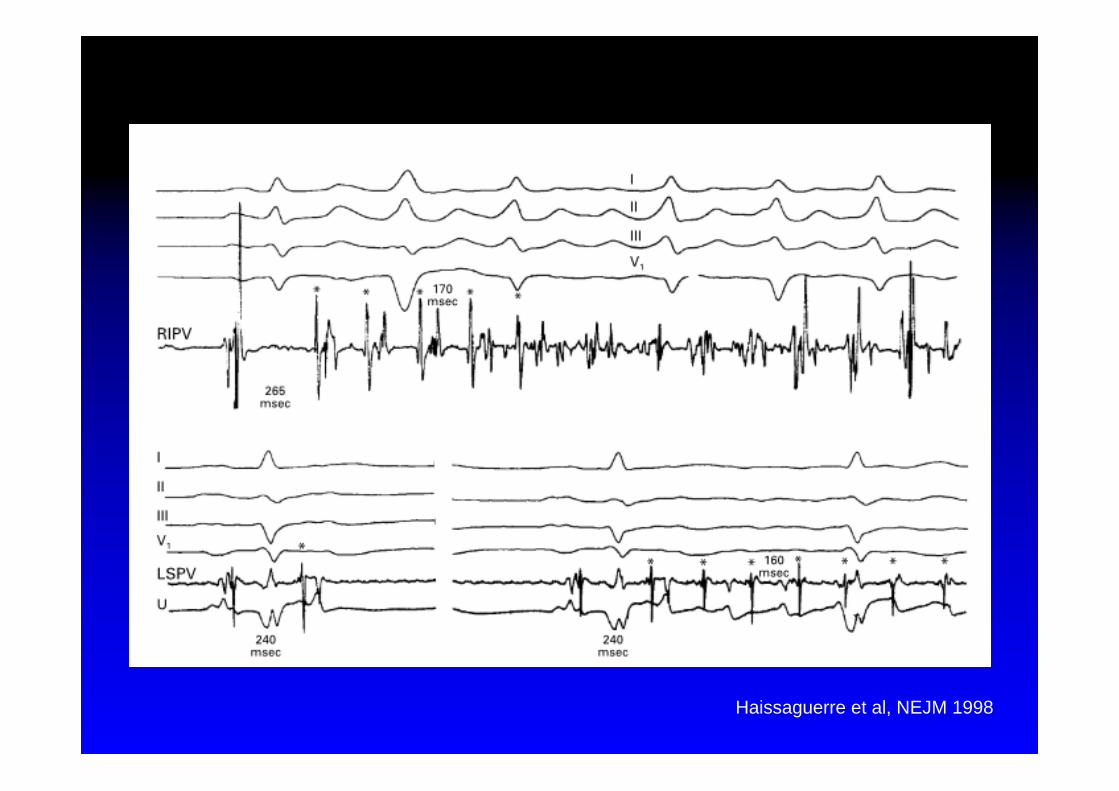
Haissaguerre et al, NEJM 1998
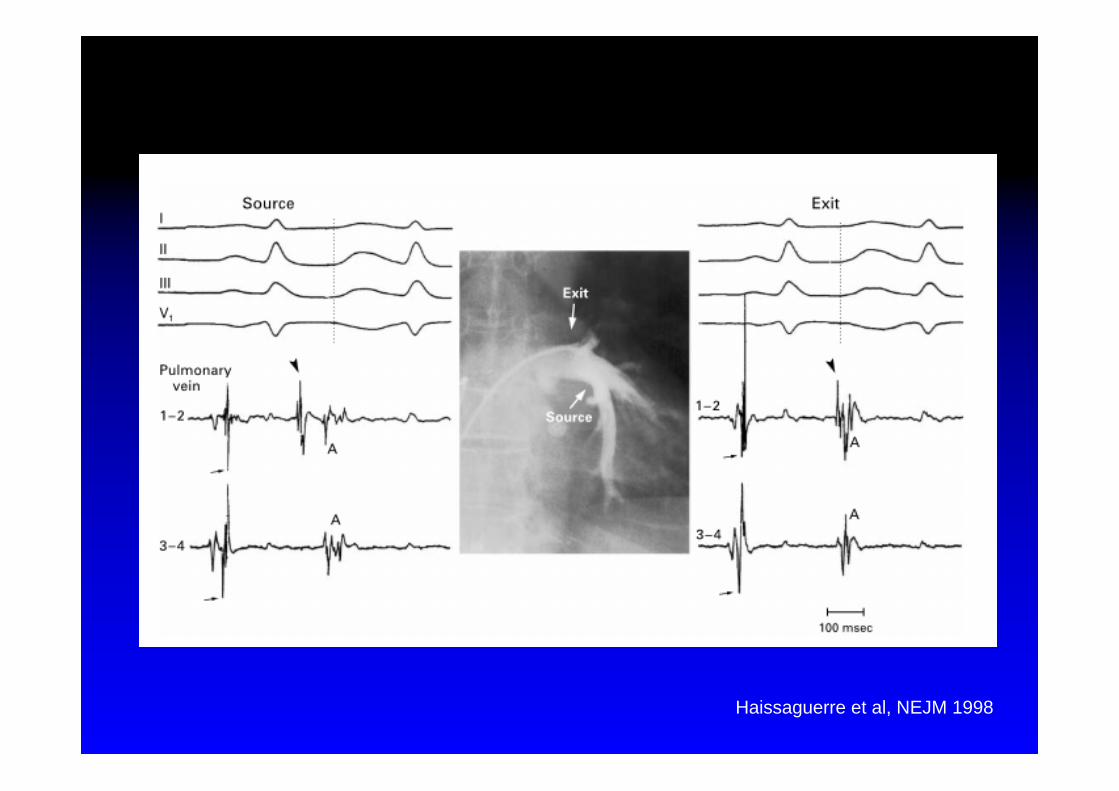
Haissaguerre et al, NEJM 1998
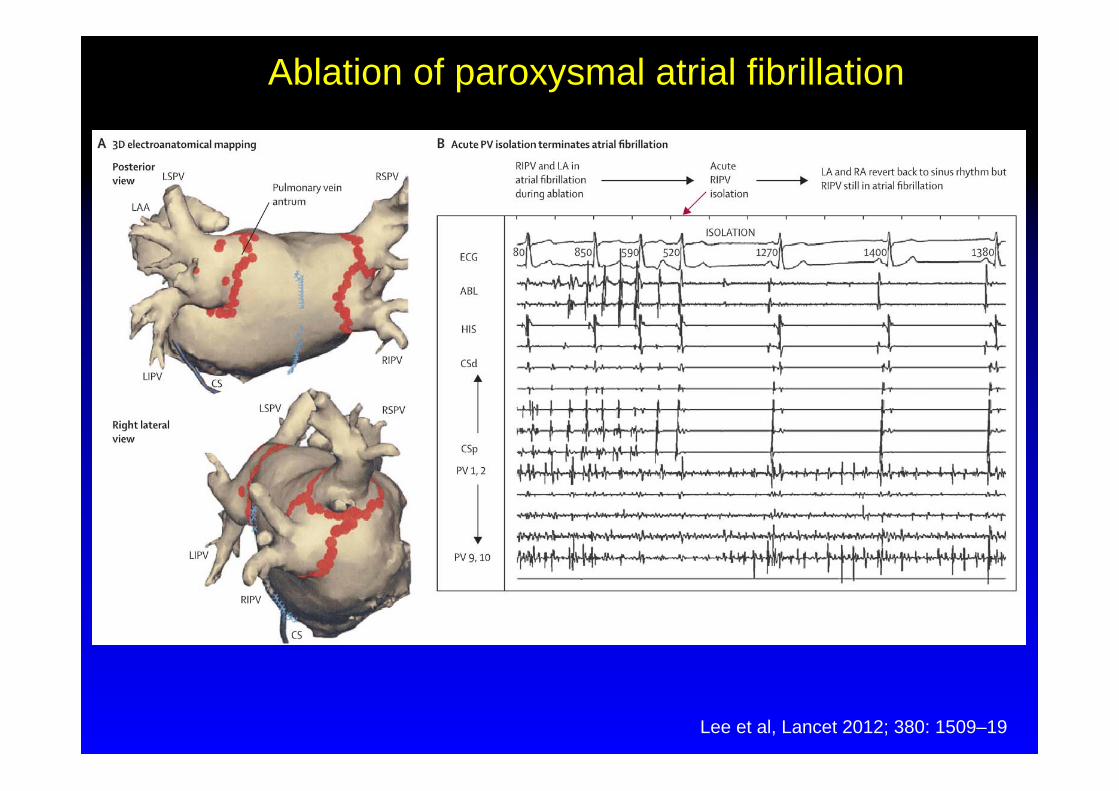
Ablation of paroxysmal atrial fibrillation
Lee et al, Lancet 2012; 380: 1509–19
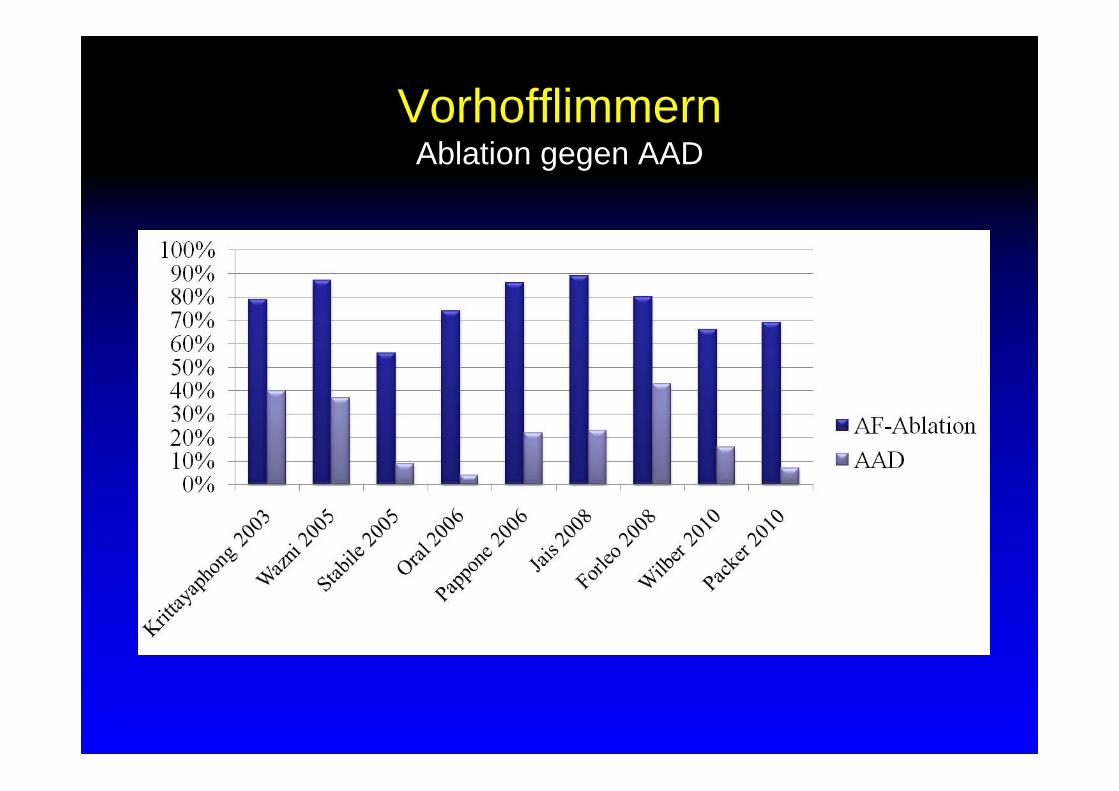
VorhofflimmernAblation gegen AAD
294 patients with paroxysmal atrial fibrillation and no history of antiarrhythmic drug use
randomization to drug therapy with class IC or class III or ablation
Follow-up included 7-day Holter-monitor recording at 3, 6, 12, 18, and 24 months
Primary end points were the cumulative and per-visit burden of atrial fibrillation
Nielsen et al, NEJM 2012
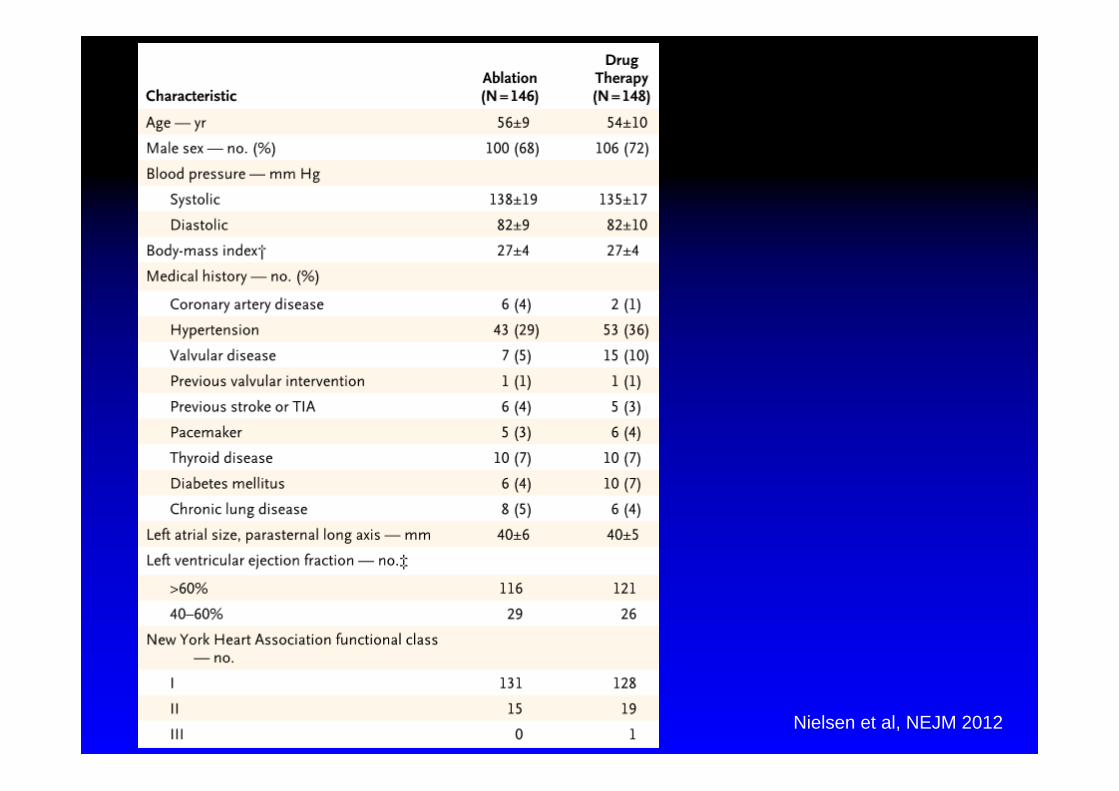
Nielsen et al, NEJM 2012
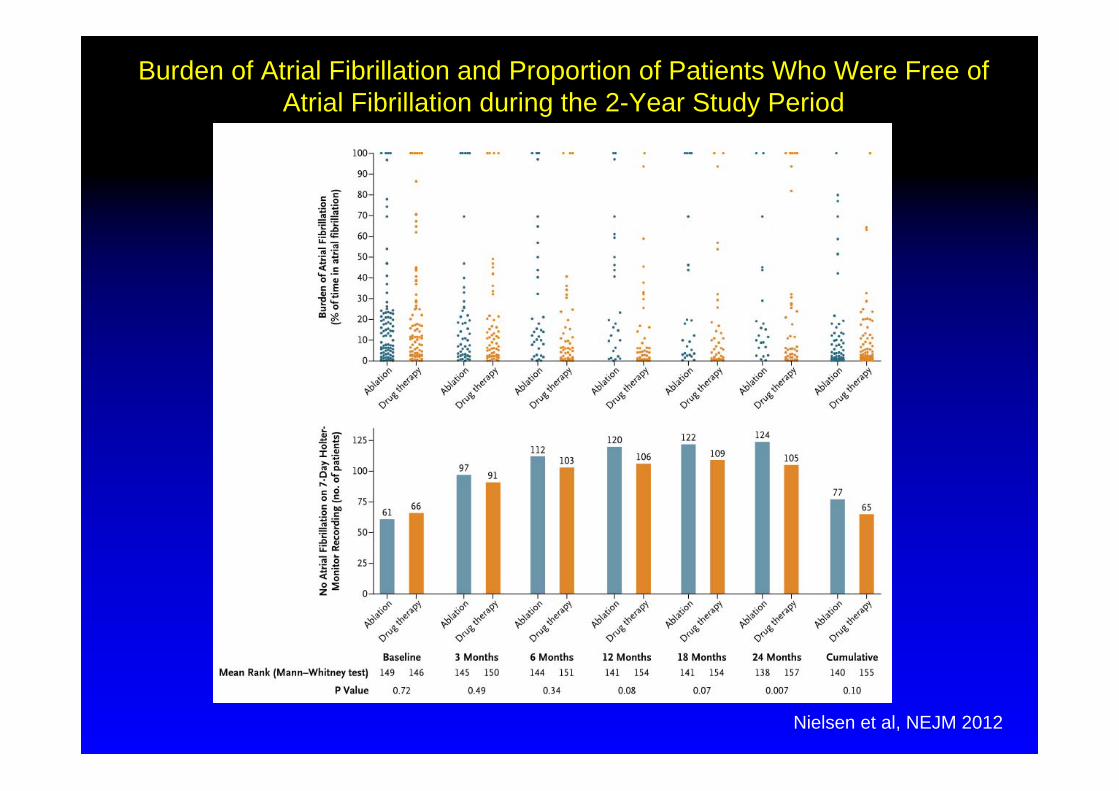
Burden of Atrial Fibrillation and Proportion of Patients Who Were Free of Atrial Fibrillation during the 2-Year Study Period
Nielsen et al, NEJM 2012
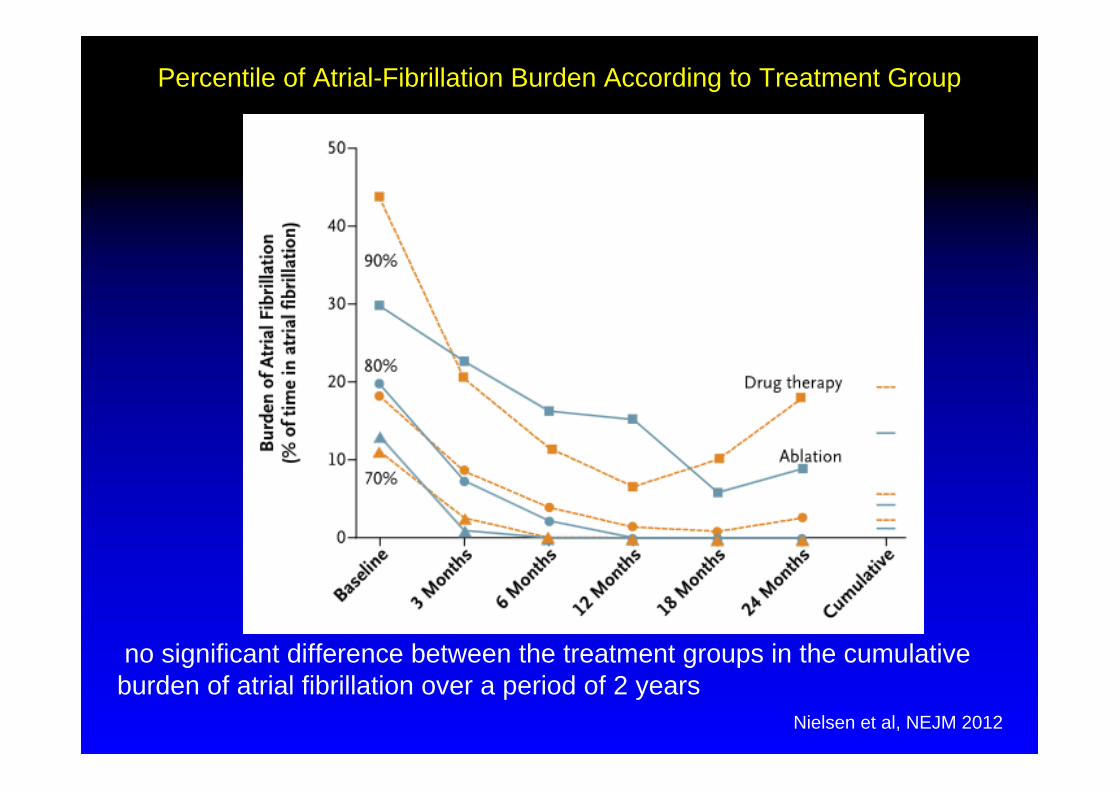
Percentile of Atrial-Fibrillation Burden According to Treatment Group
Nielsen et al, NEJM 2012
no significant difference between the treatment groups in the cumulative burden of atrial fibrillation over a period of 2 years
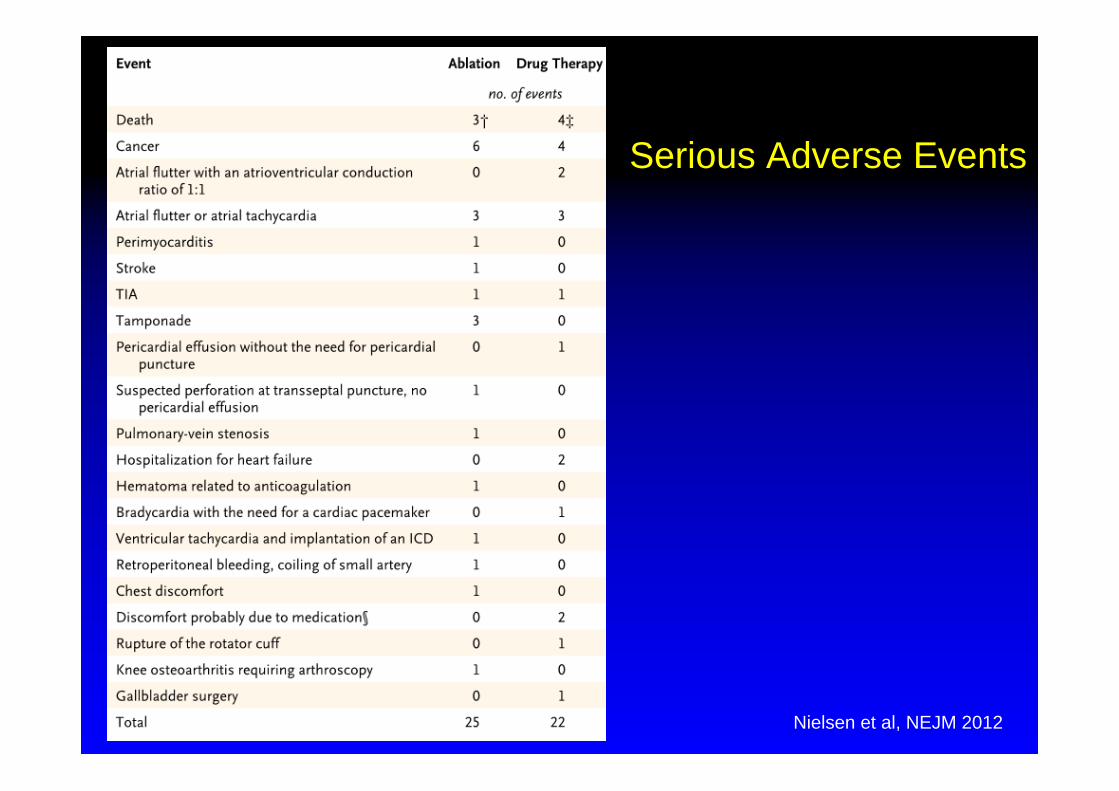
Serious Adverse Events
Nielsen et al, NEJM 2012
• Die Entwicklung neuer Antiarrhythmika ist komplex
• Kein AA ist für alle Patienten geeignet
• Cave bei Patienten mit Herzinsuffizienz
• Die Ablationstherapie ist eine Alternative
Therapie bei Arrhythmien


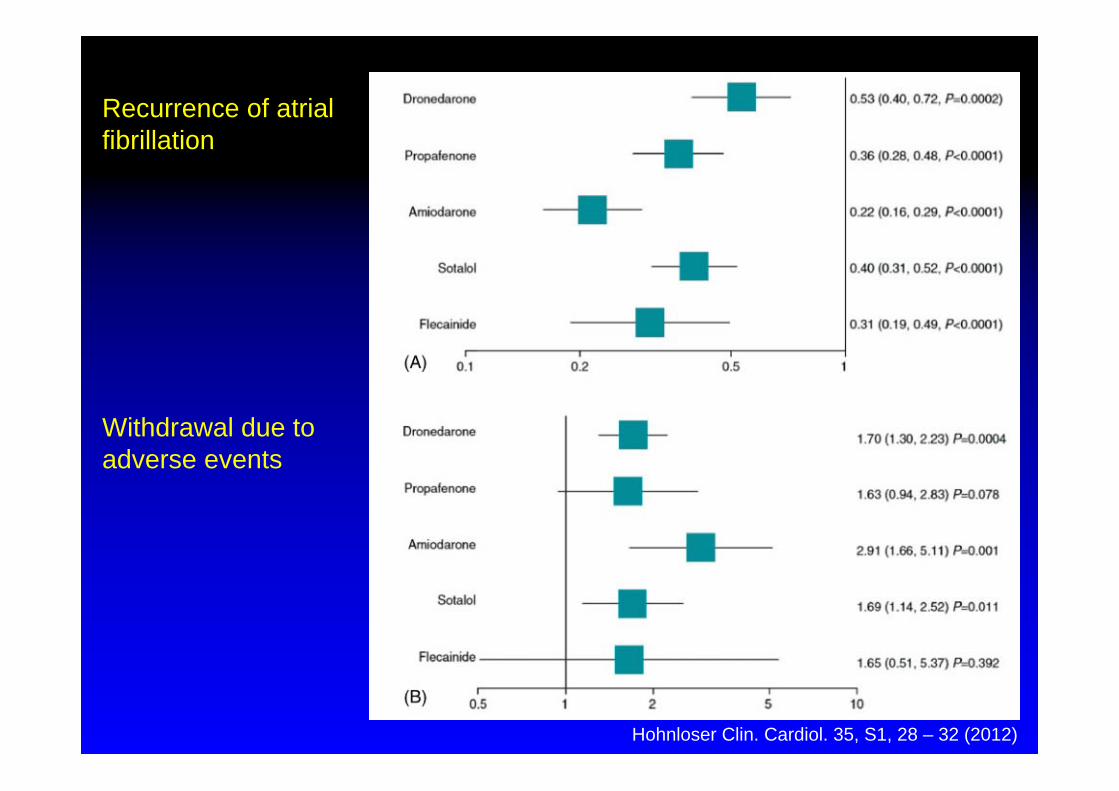
Recurrence of atrial fibrillation
Withdrawal due to adverse events
Hohnloser Clin. Cardiol. 35, S1, 28 – 32 (2012)
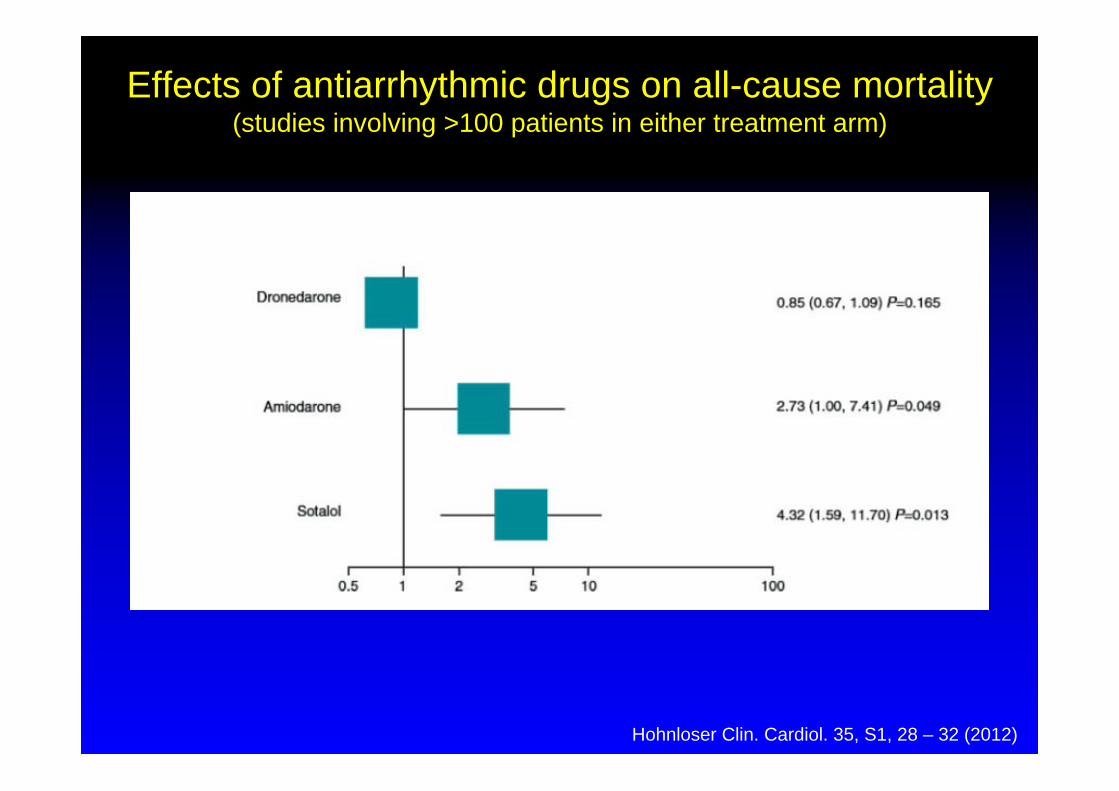
Effects of antiarrhythmic drugs on all-cause mortality (studies involving >100 patients in either treatment arm)
Hohnloser Clin. Cardiol. 35, S1, 28 – 32 (2012)
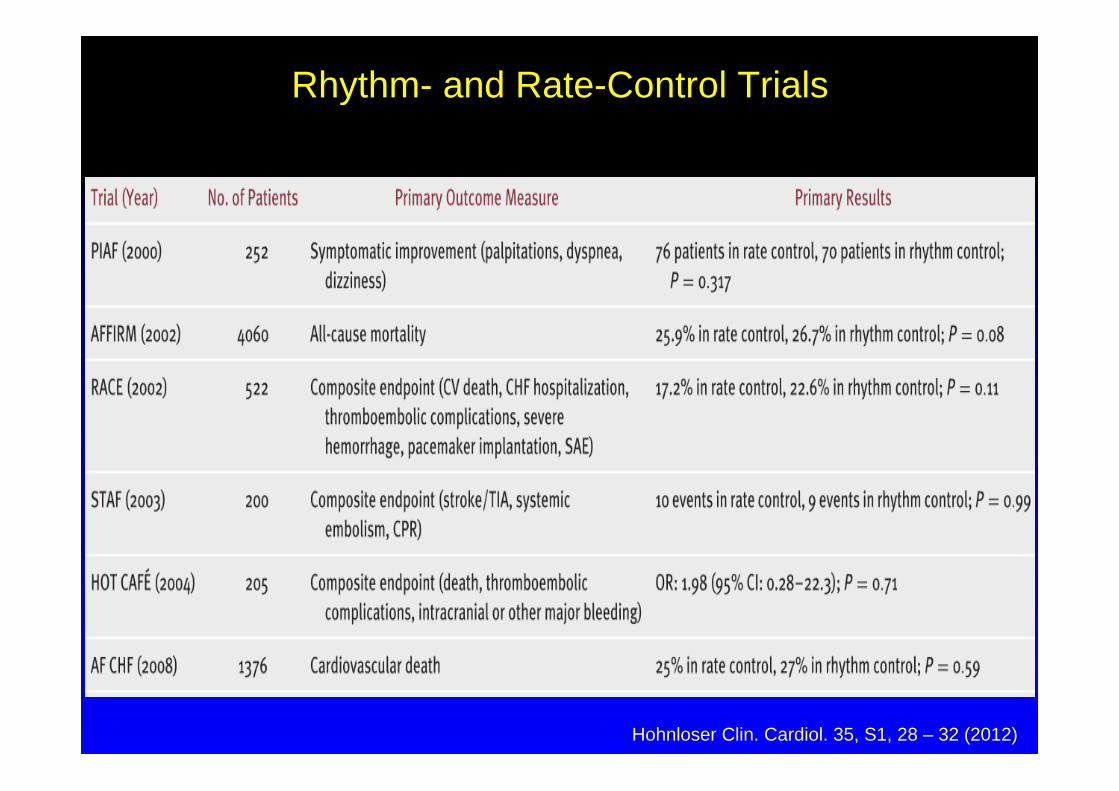
Rhythm- and Rate-Control Trials
Hohnloser Clin. Cardiol. 35, S1, 28 – 32 (2012)

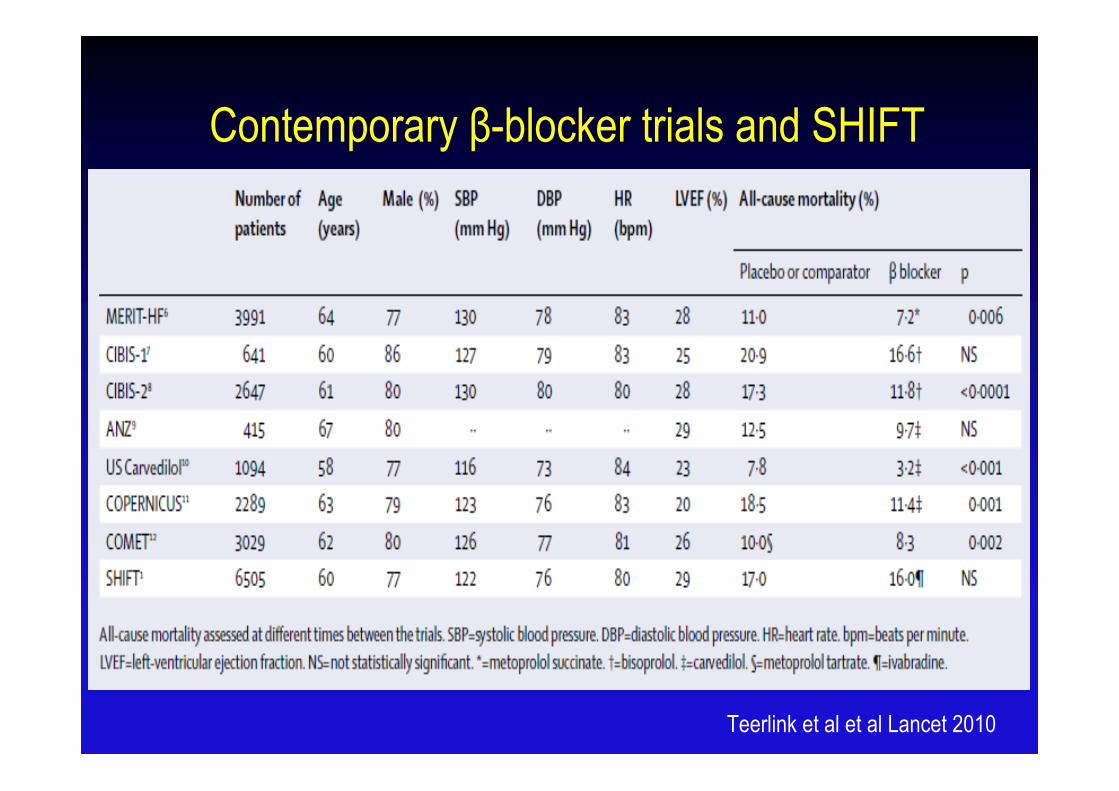
Contemporary β-blocker trials and SHIFT
Teerlink et al et al Lancet 2010
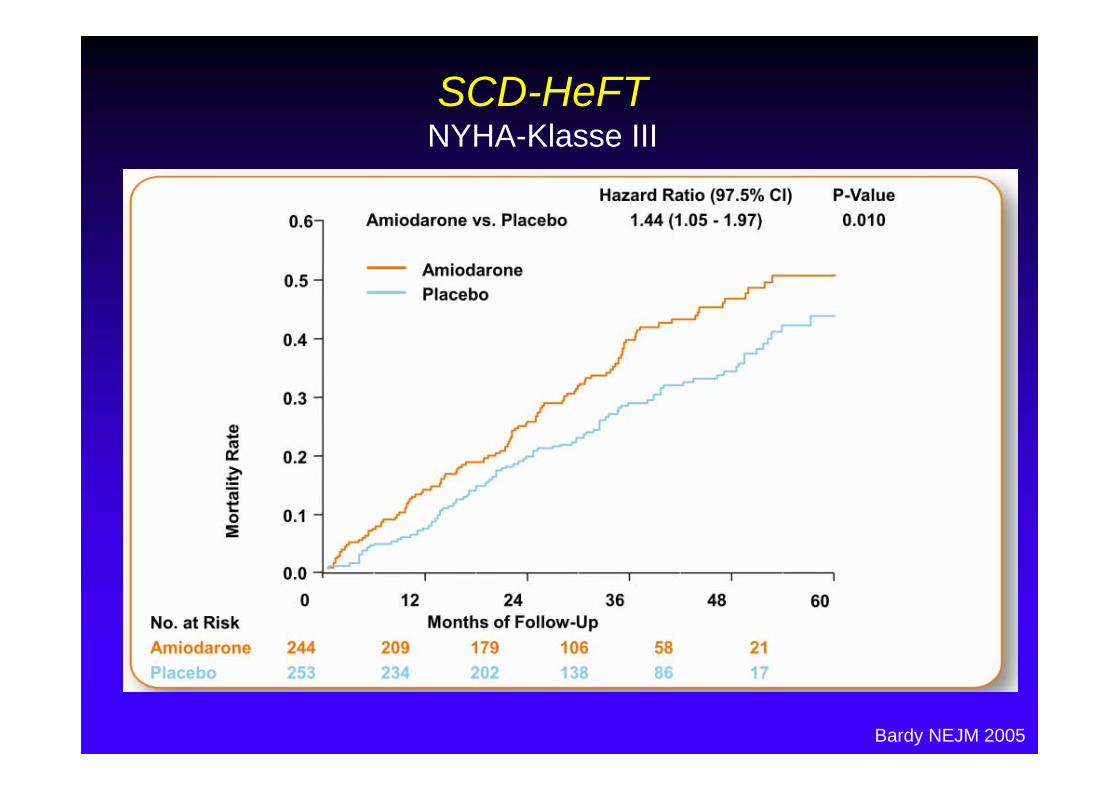
SCD-HeFTNYHA-Klasse III
Bardy NEJM 2005
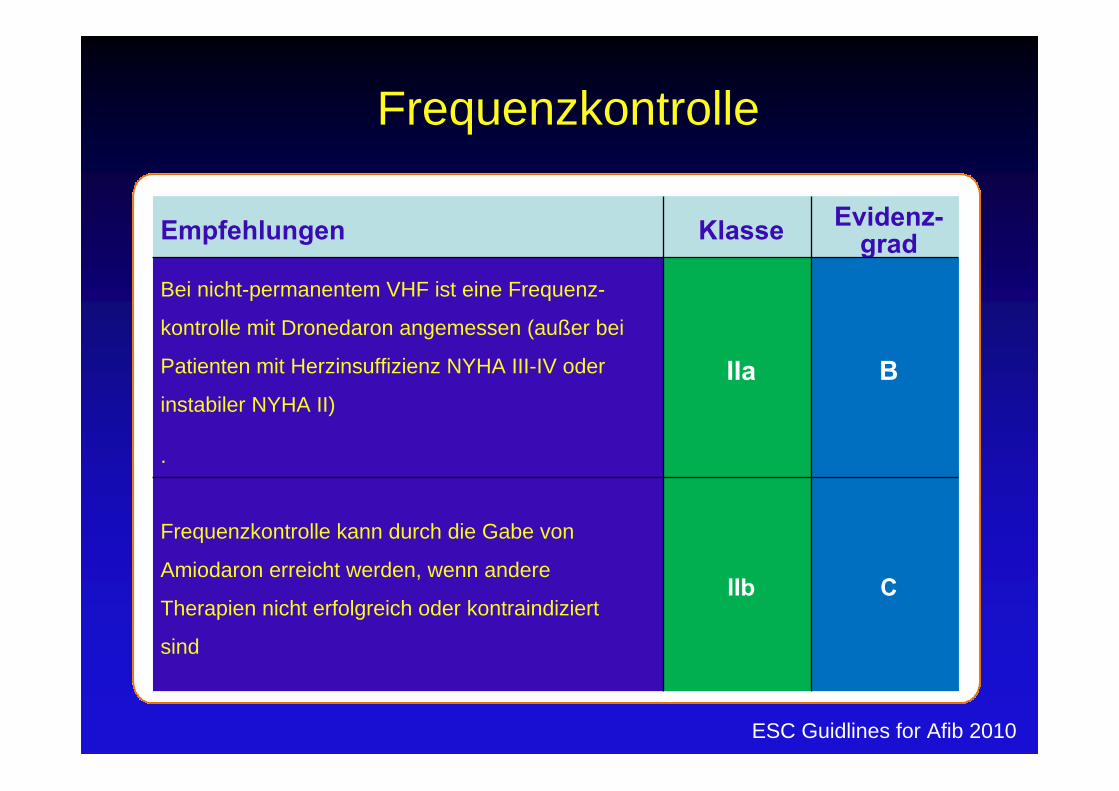
Frequenzkontrolle
Frequenzkontrolle kann durch die Gabe von Amiodaron oral erreicht werden, wenn andere Maßnahmen nicht erfolgreich oder kontraindiziert sind
C
Empfehlungen Klasse Evidenz-grad
Bei nicht-permanentem VHF ist eine Frequenz-
kontrolle mit Dronedaron angemessen (außer bei
Patienten mit Herzinsuffizienz NYHA III-IV oder
instabiler NYHA II)
.
IIa B
Frequenzkontrolle kann durch die Gabe von
Amiodaron erreicht werden, wenn andere
Therapien nicht erfolgreich oder kontraindiziert
sind
IIb C
ESC Guidlines for Afib 2010
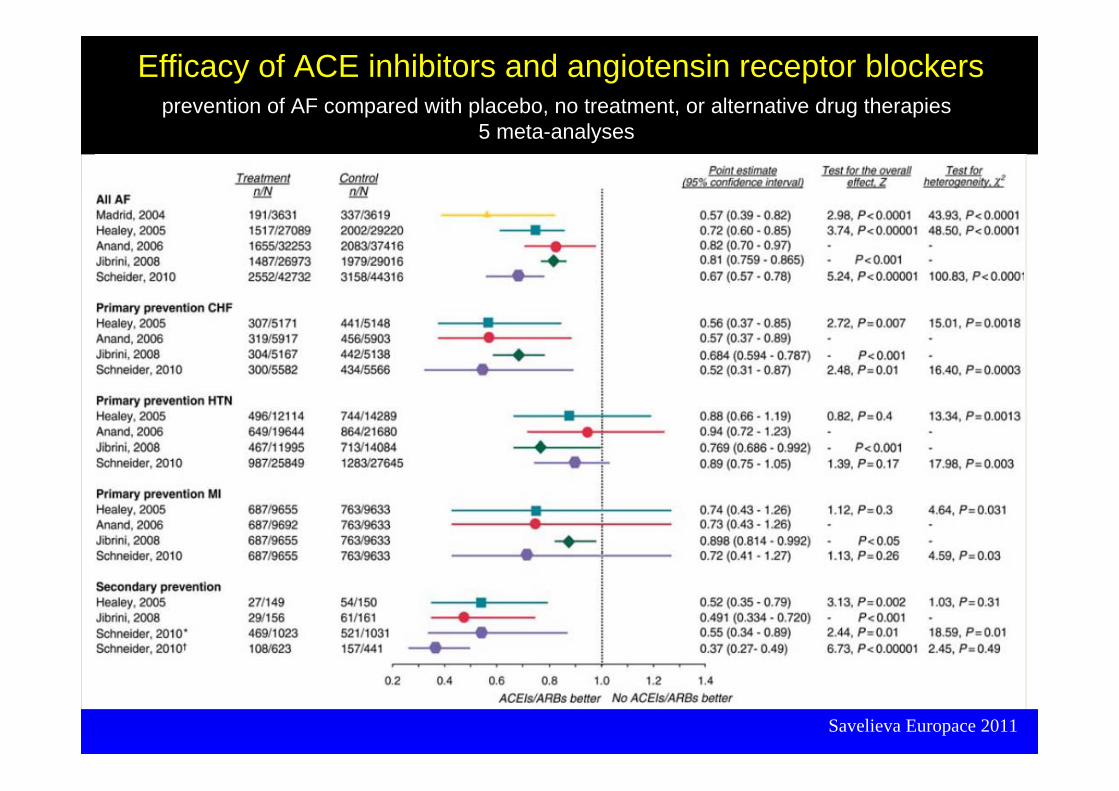
Savelieva Europace 2011
Efficacy of ACE inhibitors and angiotensin receptor blockers prevention of AF compared with placebo, no treatment, or alternative drug therapies
5 meta-analyses
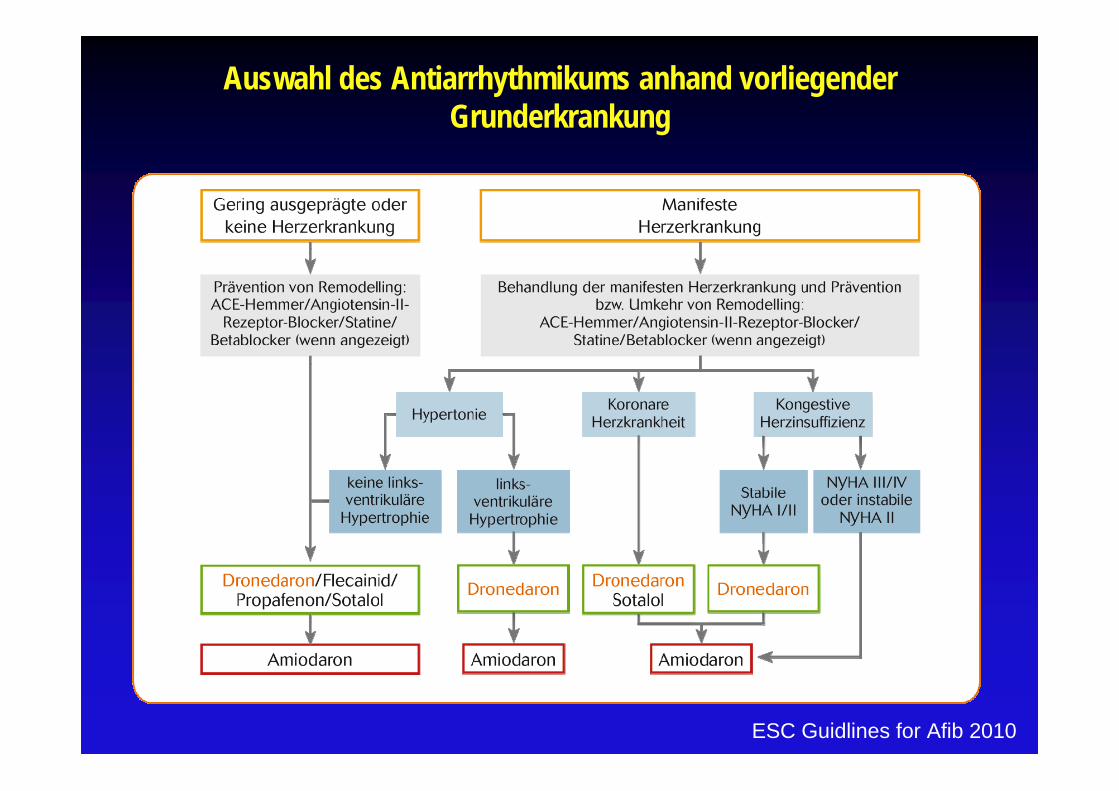
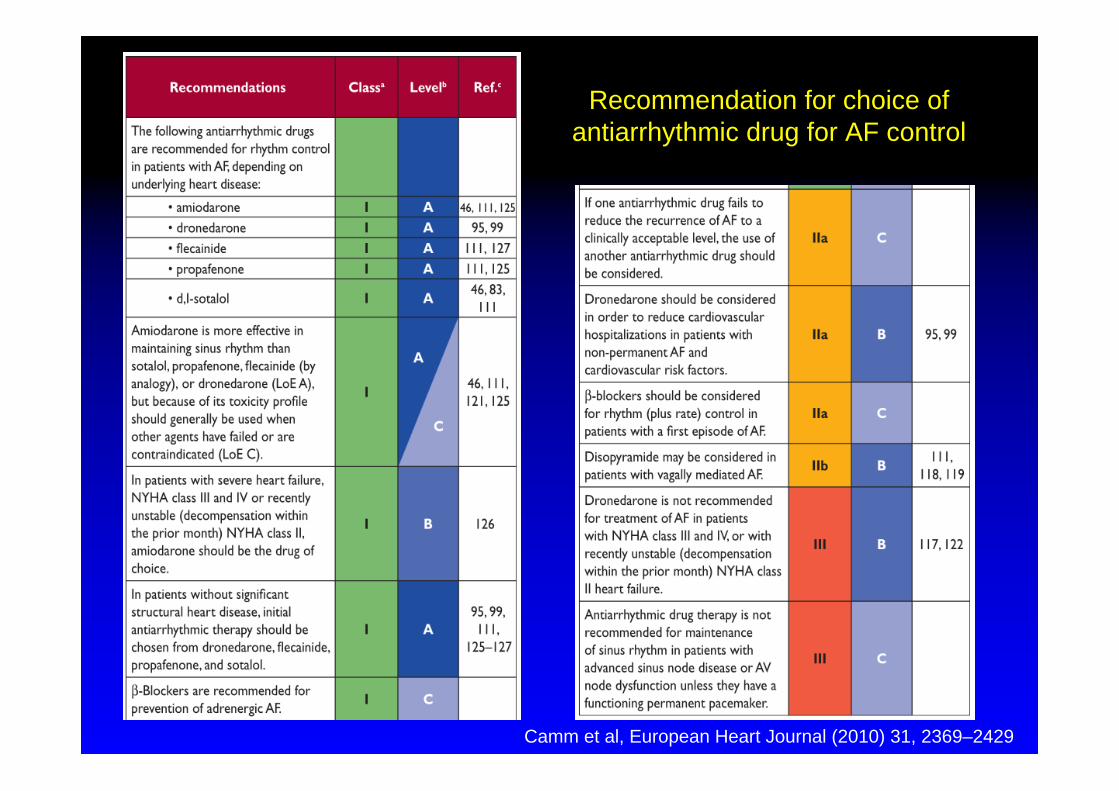
Auswahl des Antiarrhythmikums anhand vorliegender Grunderkrankung
ESC Guidlines for Afib 2010
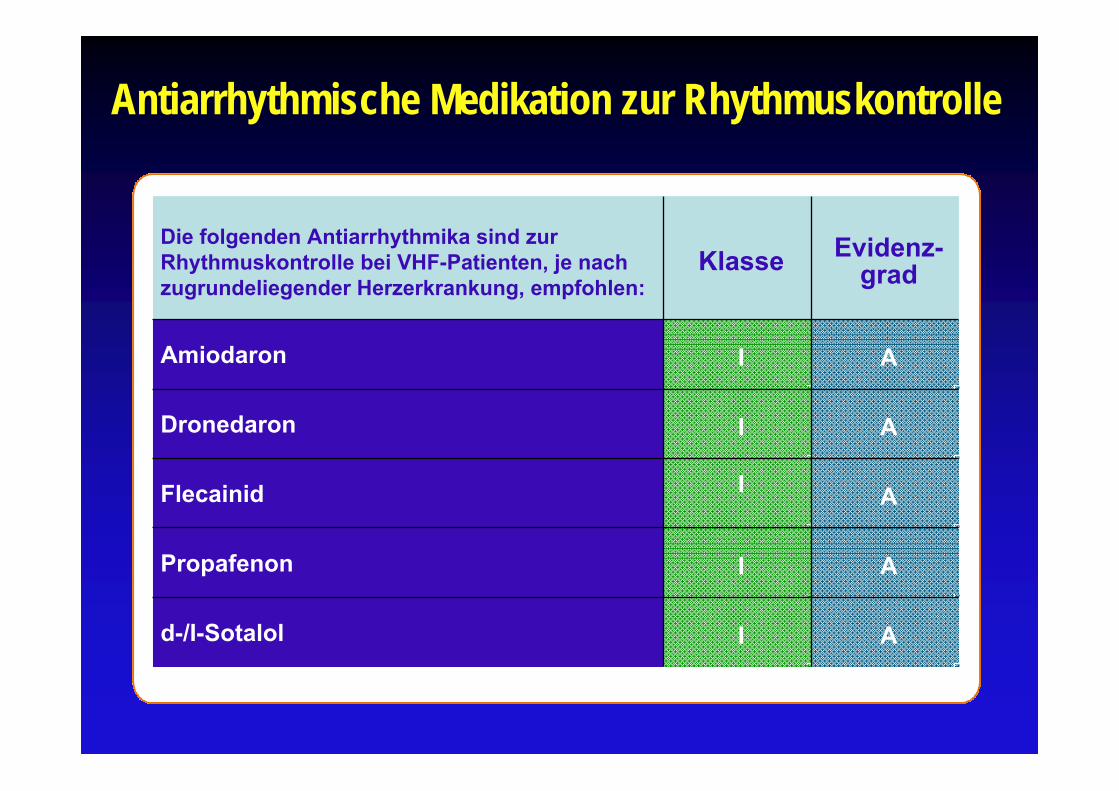
Antiarrhythmische Medikation zur Rhythmuskontrolle
Die folgenden Antiarrhythmika sind zur Rhythmuskontrolle bei VHF-Patienten, je nach zugrundeliegender Herzerkrankung, empfohlen:
Klasse Evidenz-grad
Amiodaron I A
Dronedaron I A
Flecainid I A
Propafenon I A
d-/I-Sotalol I A
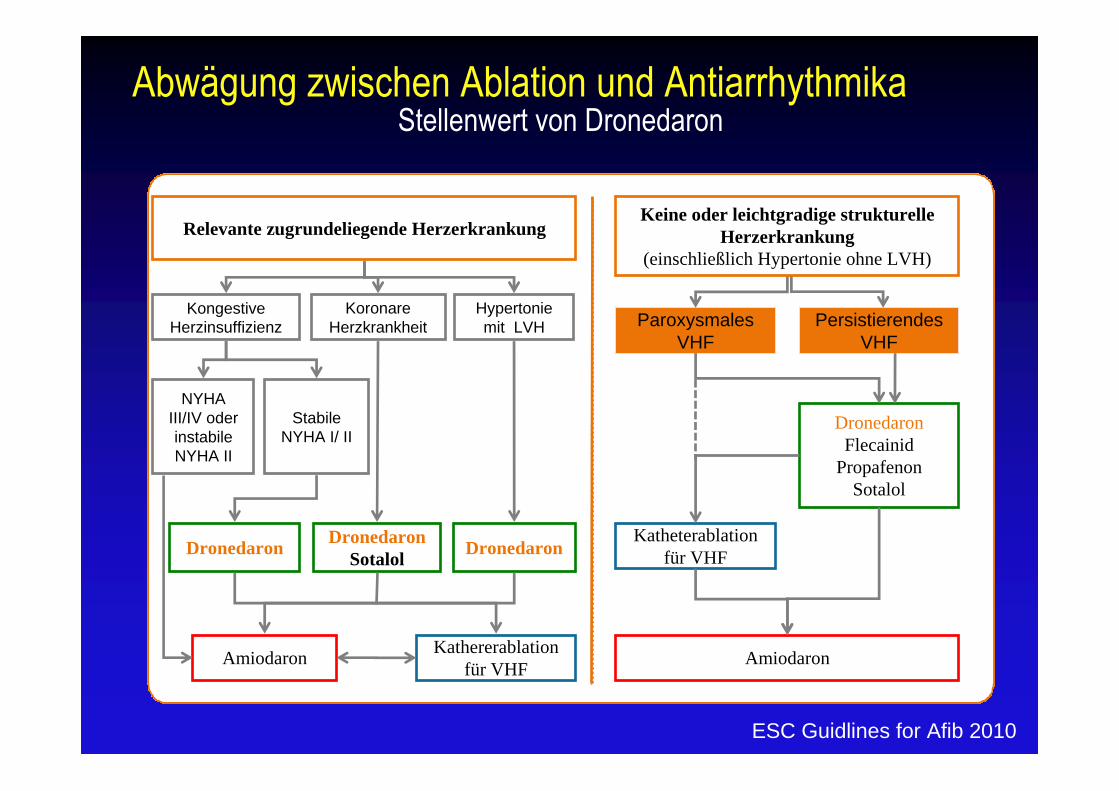
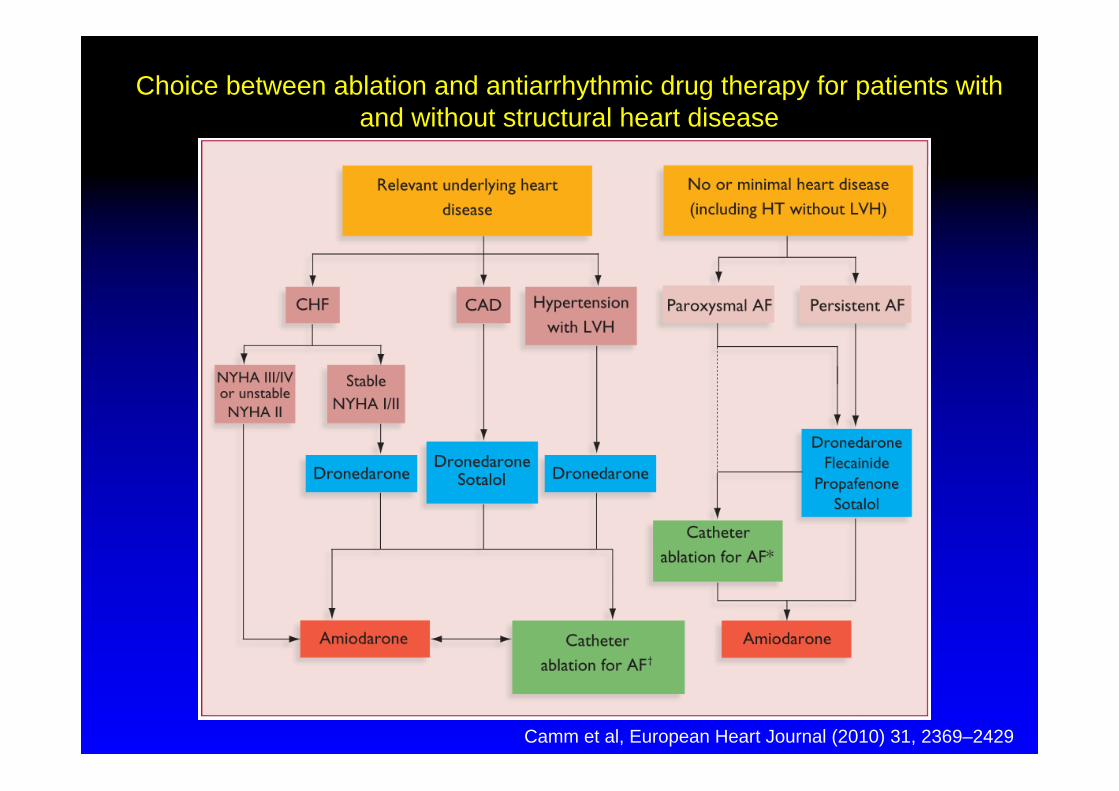
Abwägung zwischen Ablation und AntiarrhythmikaStellenwert von Dronedaron
Amiodaron
DronedaronFlecainid
PropafenonSotalol
Katheterablation für VHF
ParoxysmalesVHF
PersistierendesVHF
Amiodaron Kathererablation für VHF
Relevante zugrundeliegende Herzerkrankung
Hypertoniemit LVH
Koronare Herzkrankheit
Kongestive Herzinsuffizienz
NYHA III/IV oder instabile NYHA II
Stabile NYHA I/ II
Dronedaron DronedaronSotalol Dronedaron
Keine oder leichtgradige strukturelle Herzerkrankung
(einschließlich Hypertonie ohne LVH)
ESC Guidlines for Afib 2010
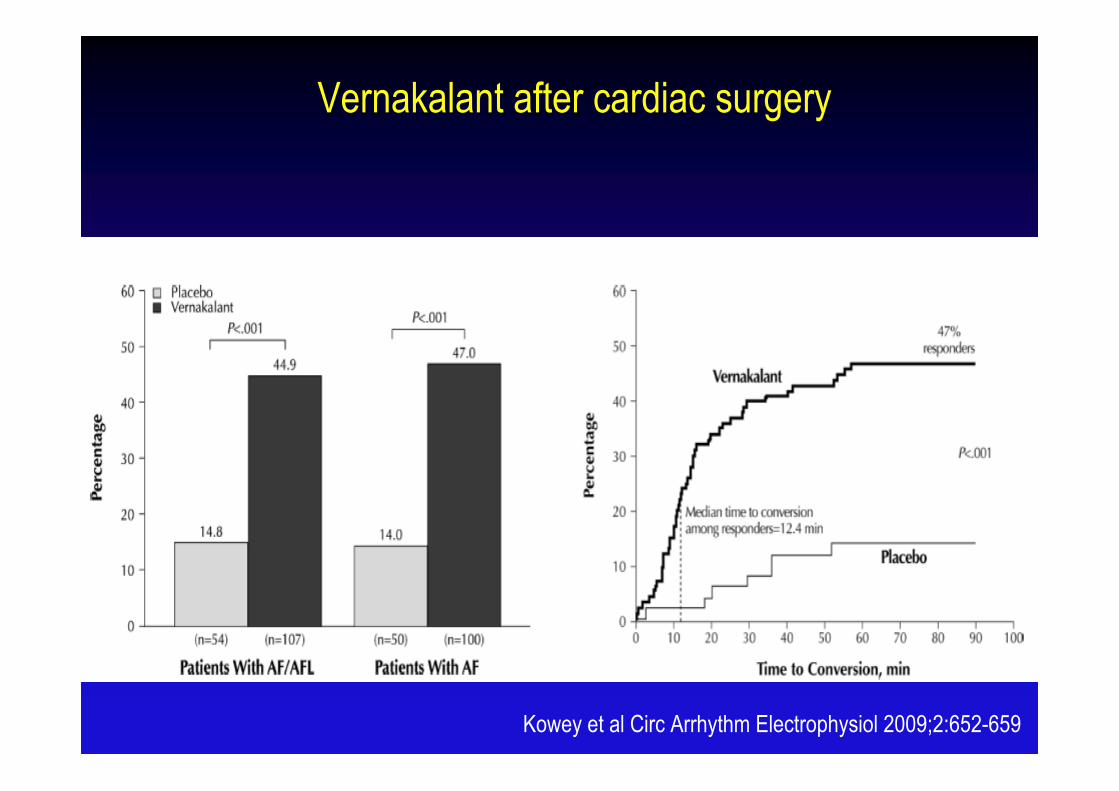
Vernakalant after cardiac surgery
Kowey et al Circ Arrhythm Electrophysiol 2009;2:652-659
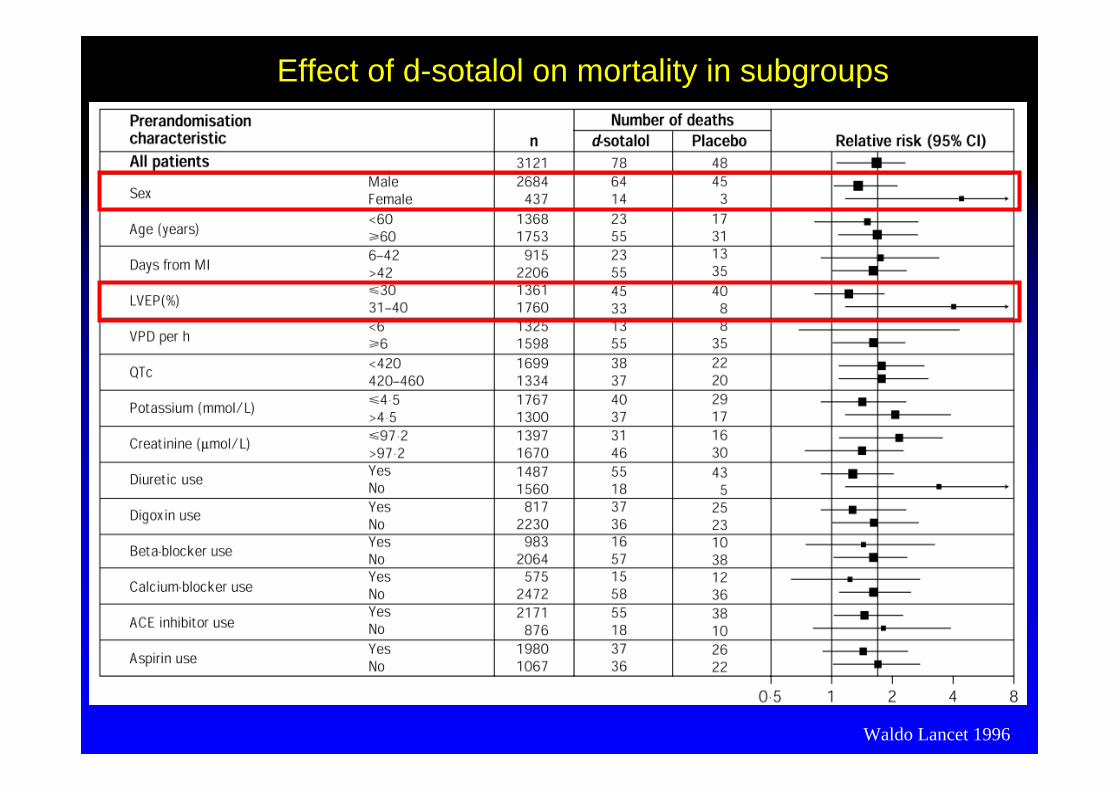
Effect of d-sotalol on mortality in subgroups
Waldo Lancet 1996
Singh BN et al. N Engl J Med 2007;357:987-999
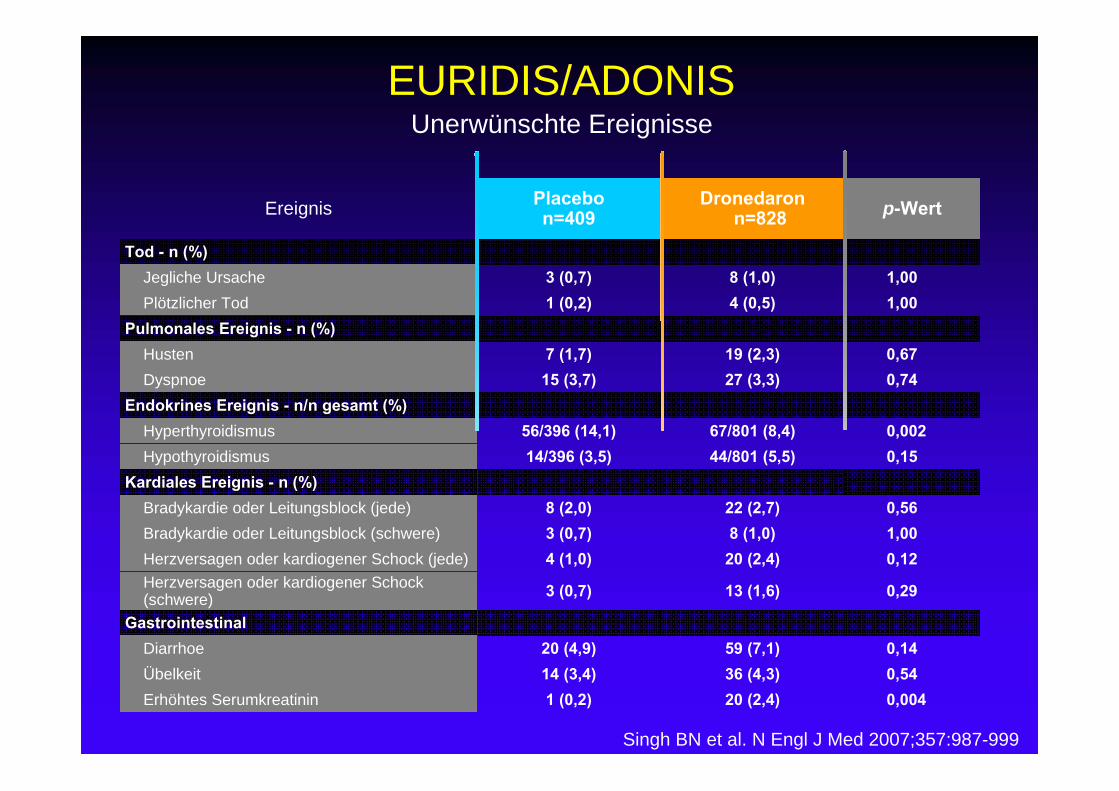
EURIDIS/ADONIS
Ereignis Placebon=409
Dronedaronn=828 p-Wert
Tod - n (%)Jegliche Ursache 3 (0,7) 8 (1,0) 1,00Plötzlicher Tod 1 (0,2) 4 (0,5) 1,00
Pulmonales Ereignis - n (%)Husten 7 (1,7) 19 (2,3) 0,67Dyspnoe 15 (3,7) 27 (3,3) 0,74
Endokrines Ereignis - n/n gesamt (%)Hyperthyroidismus 56/396 (14,1) 67/801 (8,4) 0,002Hypothyroidismus 14/396 (3,5) 44/801 (5,5) 0,15
Kardiales Ereignis - n (%)Bradykardie oder Leitungsblock (jede) 8 (2,0) 22 (2,7) 0,56Bradykardie oder Leitungsblock (schwere) 3 (0,7) 8 (1,0) 1,00Herzversagen oder kardiogener Schock (jede) 4 (1,0) 20 (2,4) 0,12Herzversagen oder kardiogener Schock (schwere) 3 (0,7) 13 (1,6) 0,29
GastrointestinalDiarrhoe 20 (4,9) 59 (7,1) 0,14Übelkeit 14 (3,4) 36 (4,3) 0,54Erhöhtes Serumkreatinin 1 (0,2) 20 (2,4) 0,004
Unerwünschte Ereignisse
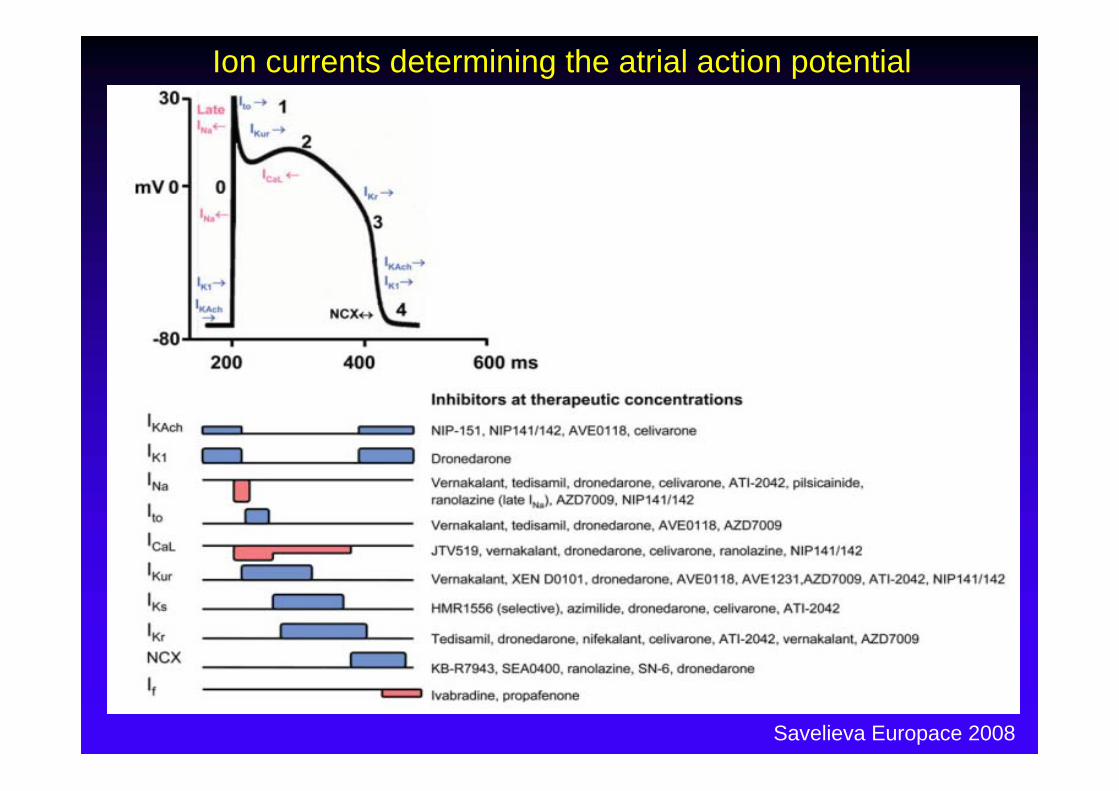
Savelieva Europace 2008
Ion currents determining the atrial action potential
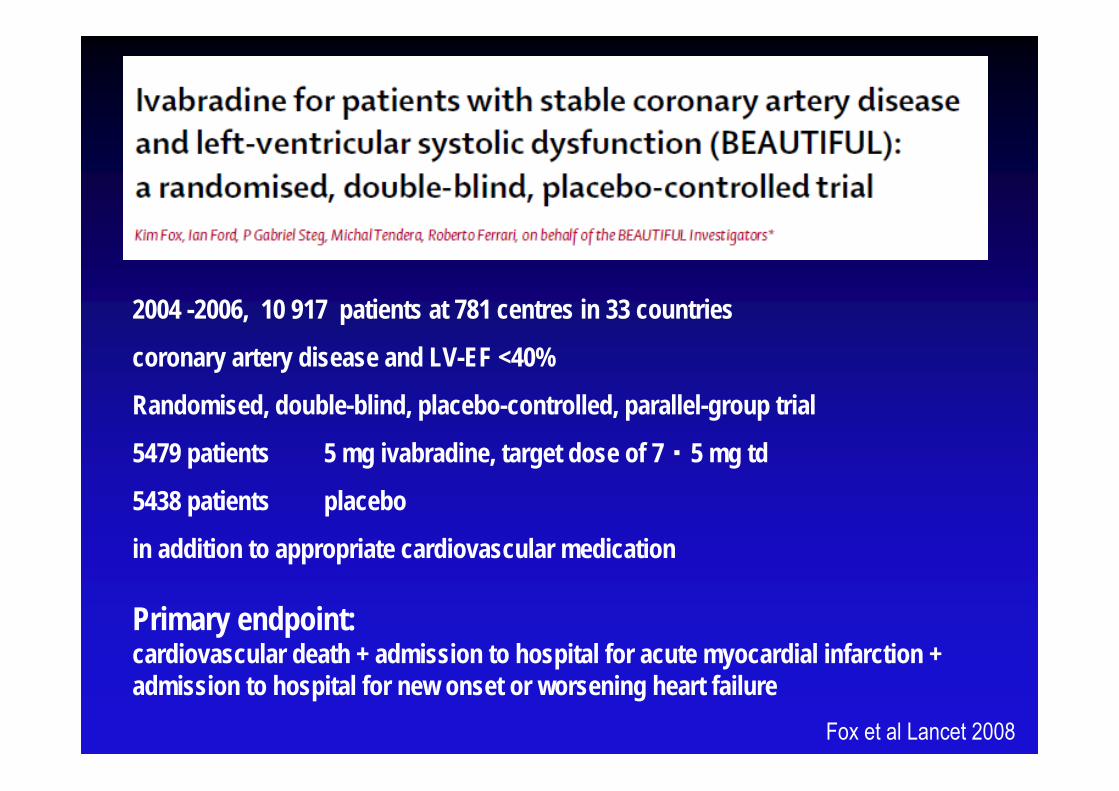
2004 -2006, 10 917 patients at 781 centres in 33 countries
coronary artery disease and LV-EF <40%
Randomised, double-blind, placebo-controlled, parallel-group trial
5479 patients 5 mg ivabradine, target dose of 7・5 mg td
5438 patients placebo
in addition to appropriate cardiovascular medication
Primary endpoint: cardiovascular death + admission to hospital for acute myocardial infarction + admission to hospital for new onset or worsening heart failure
Fox et al Lancet 2008
IvabradinIvabradin
selektive und spezifische If -Kanal-Hemmer
If –Kanal: verschiedene Charakteristika (z.B. Aktivierung durch Hyperpolarisation oder gemischtem Strom aus Natrium- und Kaliumionen)
If für Schrittmacherdepolarisation entscheidend
Kontrolle durch autonomes Nervensystem
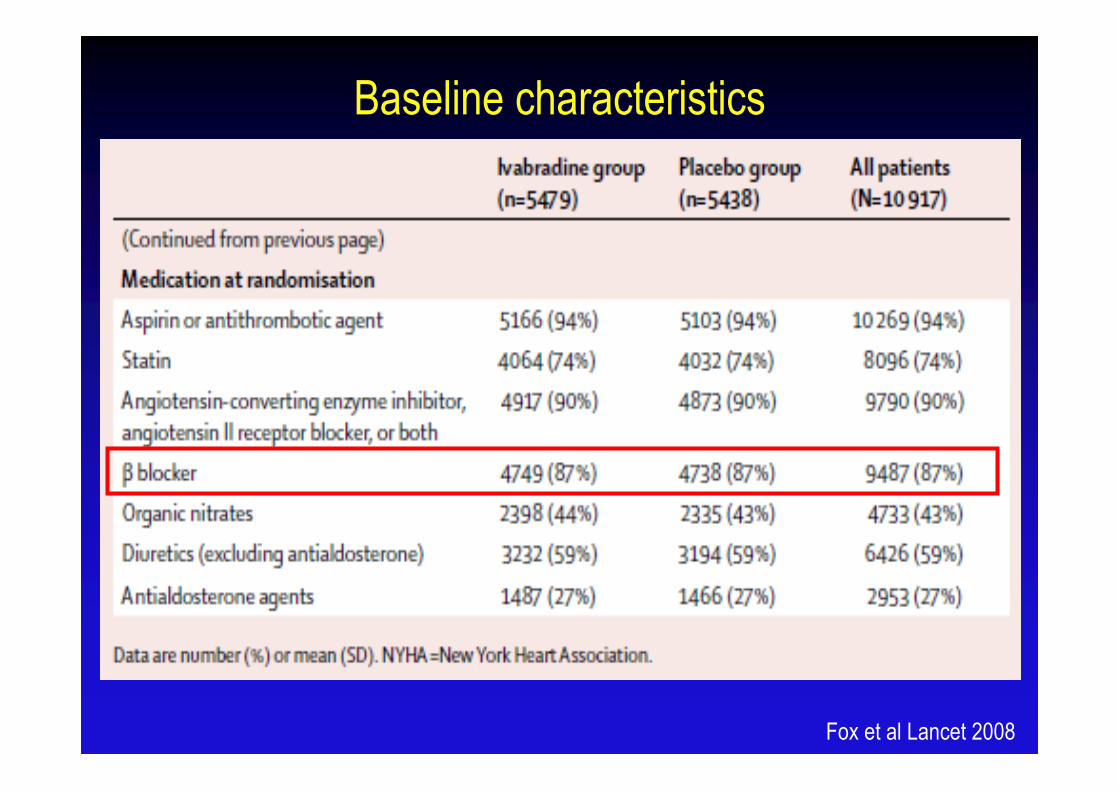
Baseline characteristics
Fox et al Lancet 2008
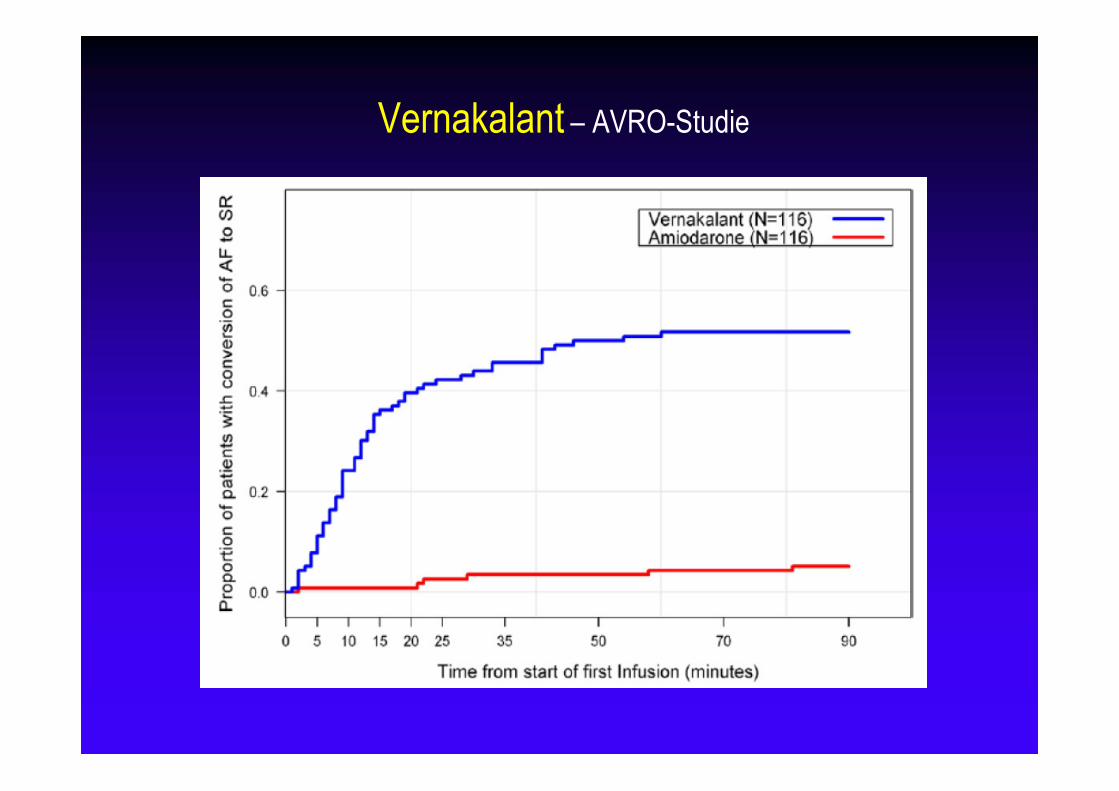
Vernakalant – AVRO-Studie
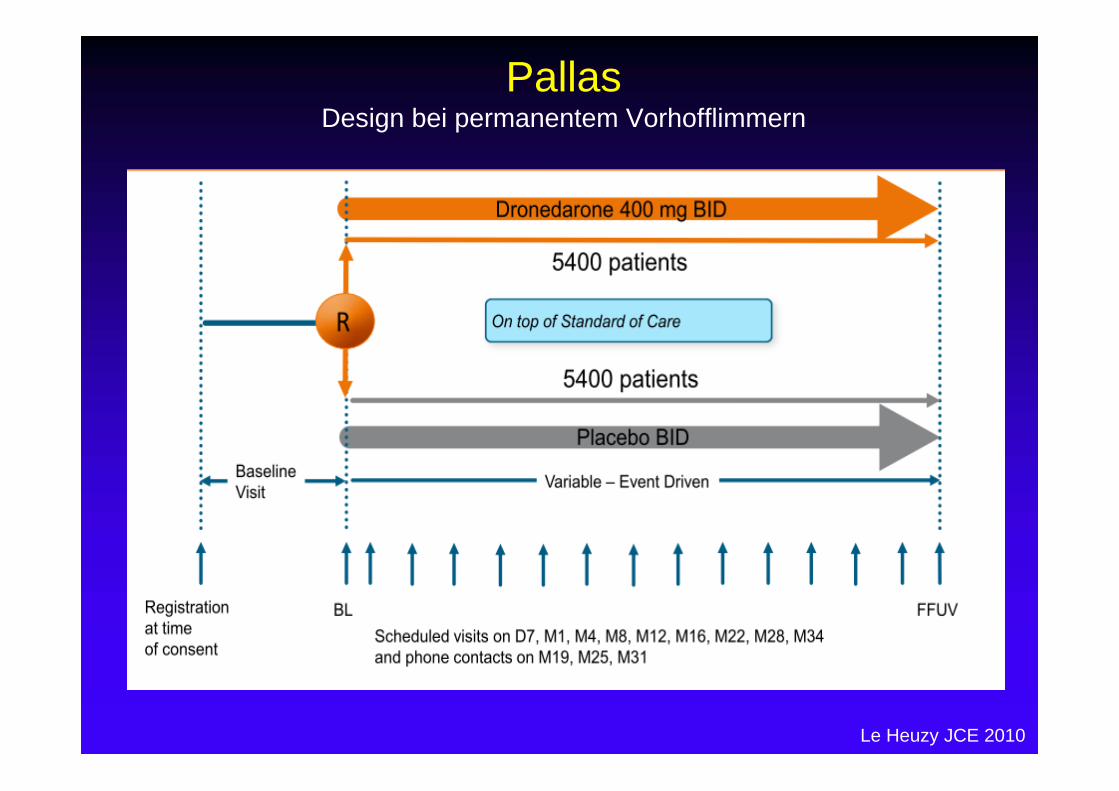
PallasDesign bei permanentem Vorhofflimmern
Le Heuzy JCE 2010
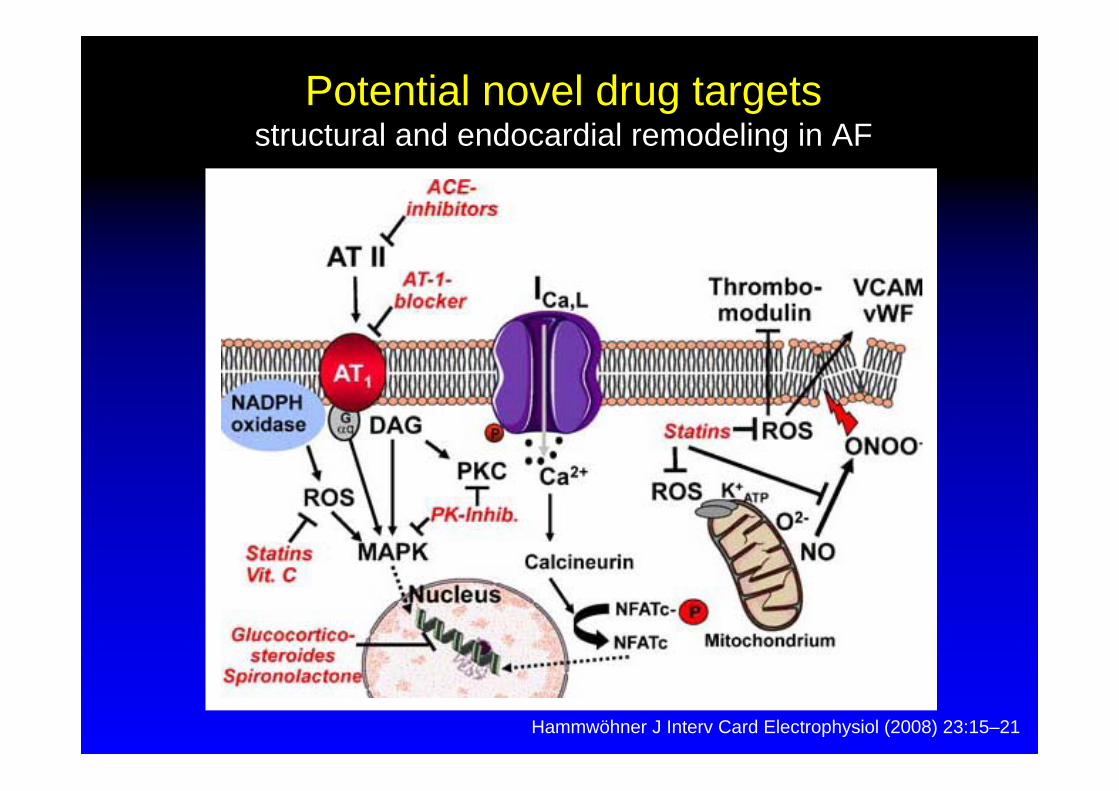
Potential novel drug targetsstructural and endocardial remodeling in AF
Hammwöhner J Interv Card Electrophysiol (2008) 23:15–21
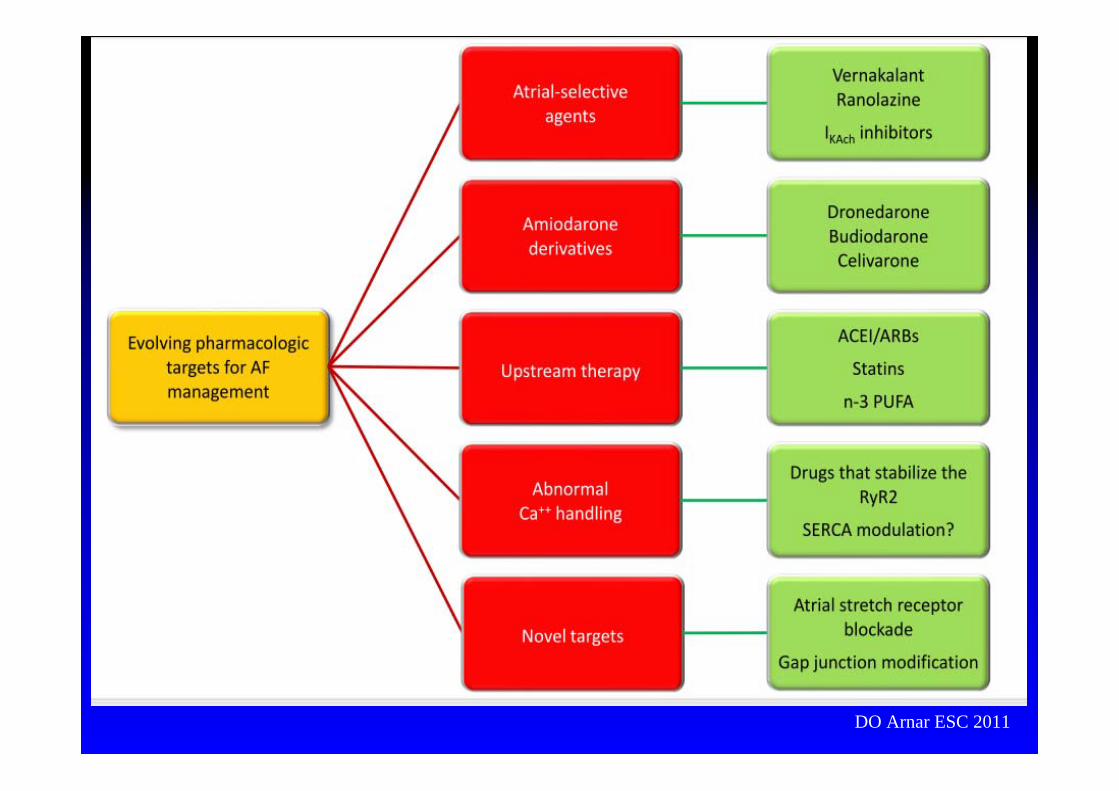
DO Arnar ESC 2011

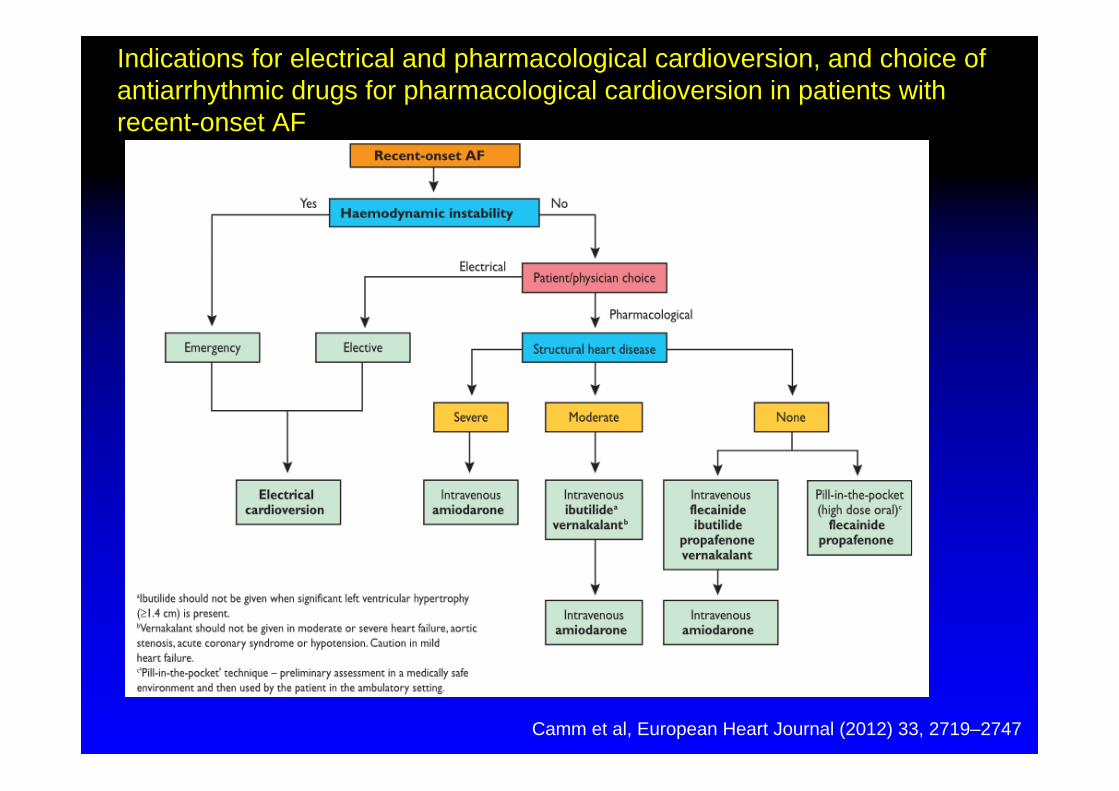
Camm et al, European Heart Journal (2012) 33, 2719–2747
Indications for electrical and pharmacological cardioversion, and choice of antiarrhythmic drugs for pharmacological cardioversion in patients with recent-onset AF
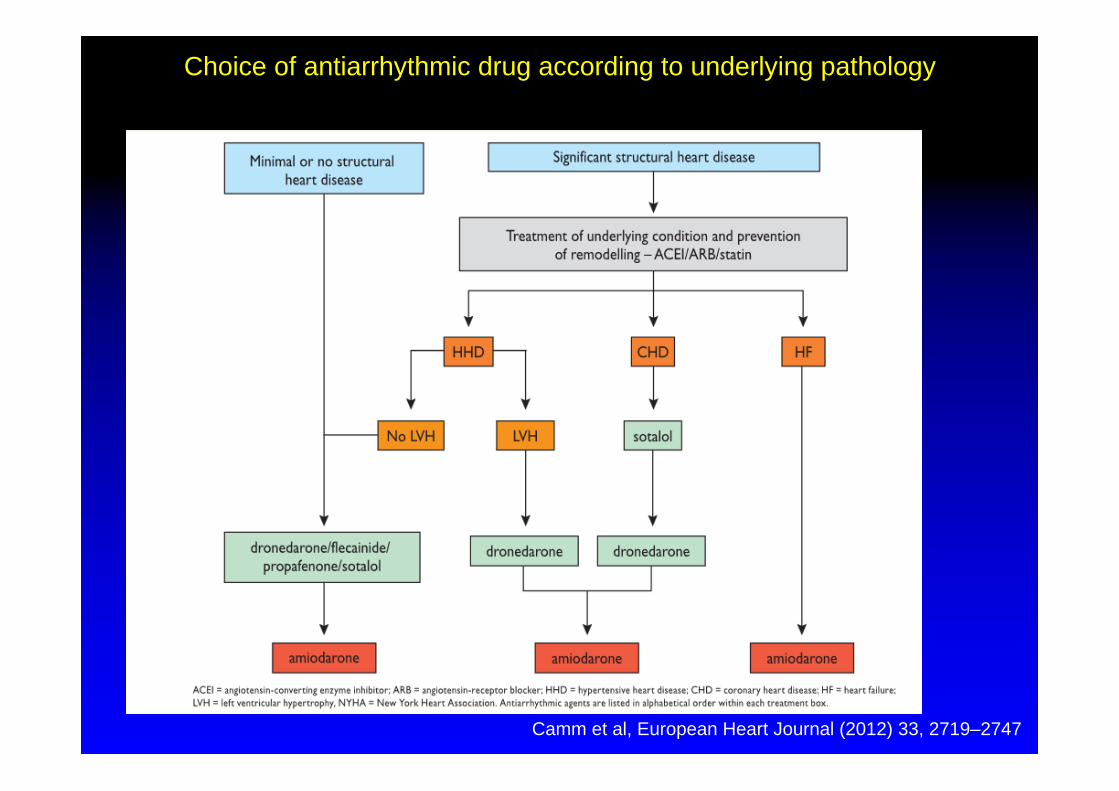
Camm et al, European Heart Journal (2012) 33, 2719–2747
Choice of antiarrhythmic drug according to underlying pathology
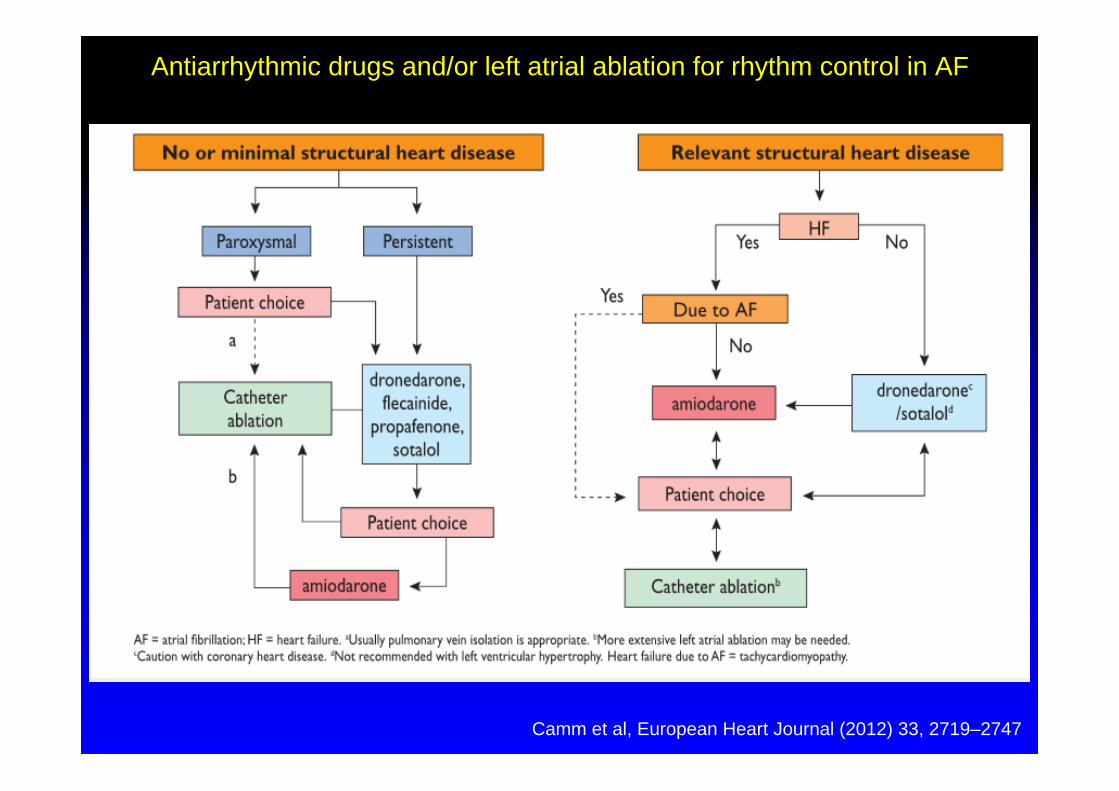
Camm et al, European Heart Journal (2012) 33, 2719–2747
Antiarrhythmic drugs and/or left atrial ablation for rhythm control in AF
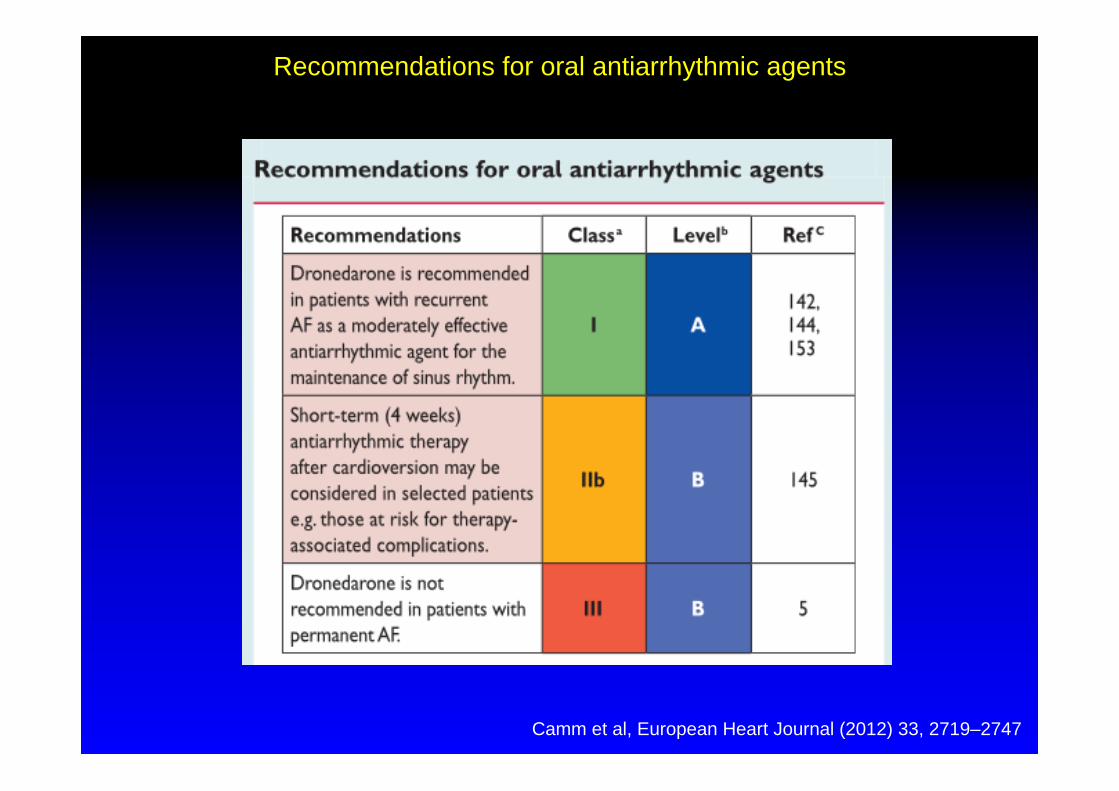
Camm et al, European Heart Journal (2012) 33, 2719–2747
Recommendations for oral antiarrhythmic agents

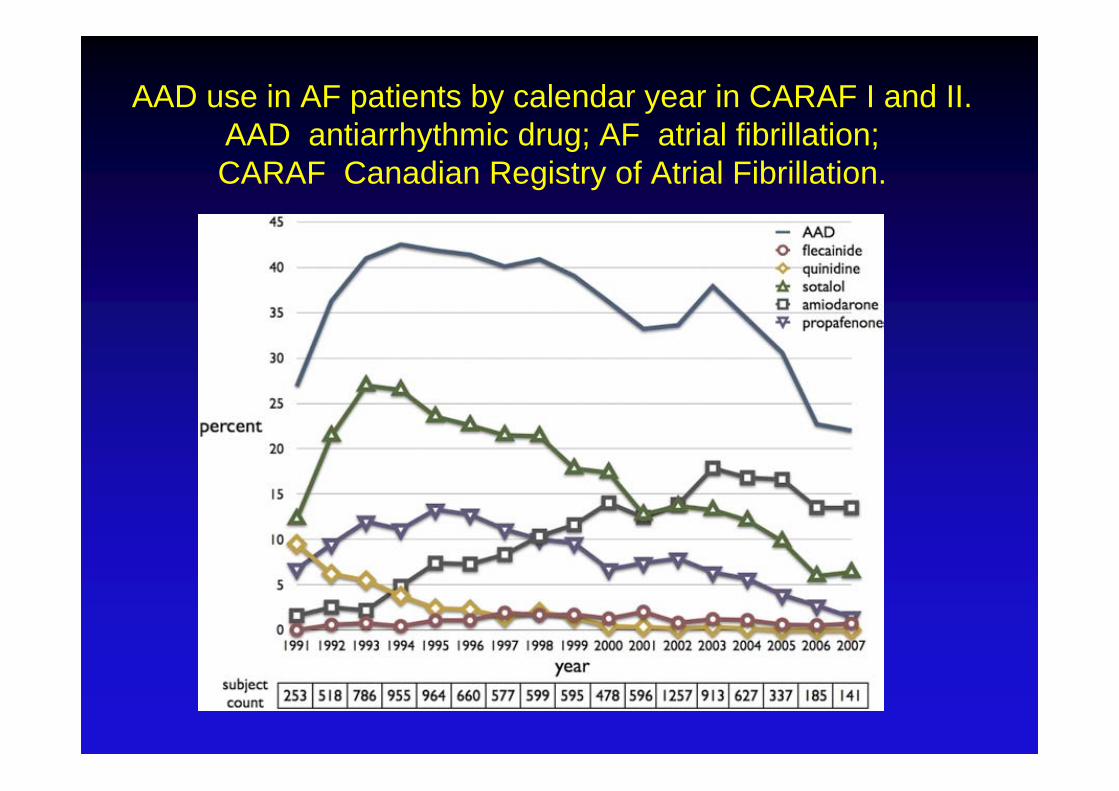
AAD use in AF patients by calendar year in CARAF I and II.AAD antiarrhythmic drug; AF atrial fibrillation; CARAF Canadian Registry of Atrial Fibrillation.
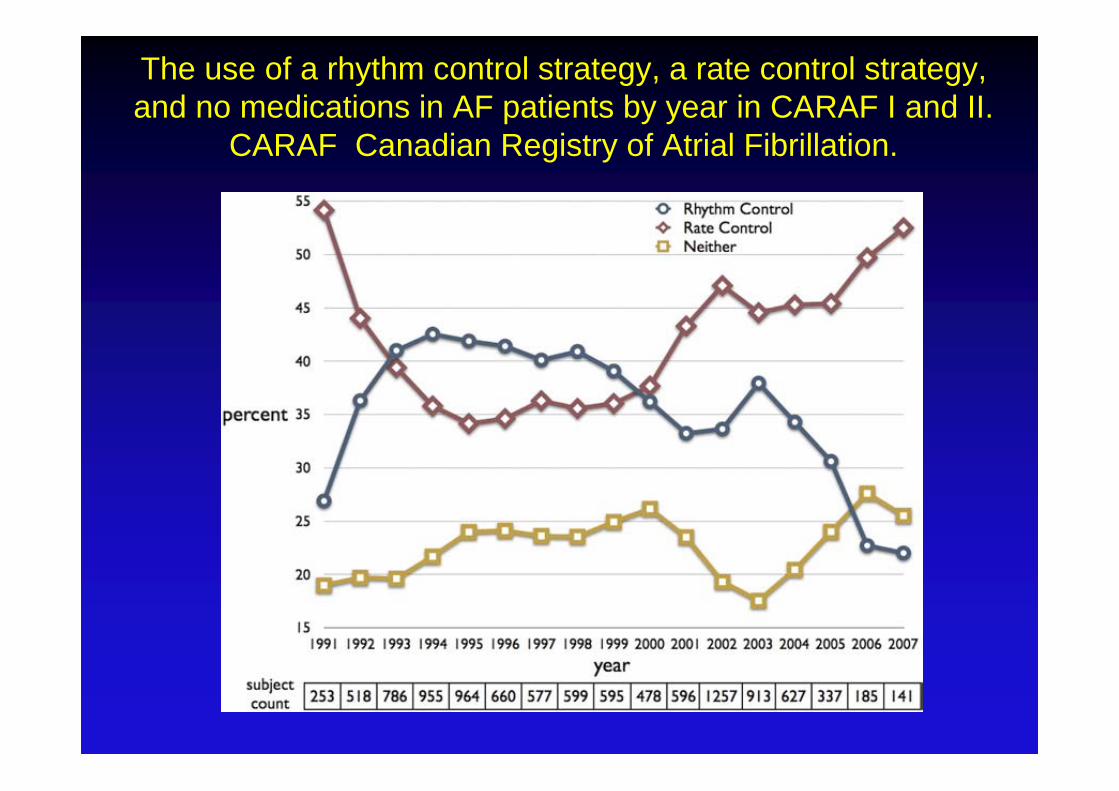
The use of a rhythm control strategy, a rate control strategy, and no medications in AF patients by year in CARAF I and II.
CARAF Canadian Registry of Atrial Fibrillation.

Cappato et al Circulation Arrhythm Electrophysiol. 2010; 3:32-38
Fragebogen mit 46 Fragen
521 Zentren in 26 Ländern
85 Zentren berichten über 20825
Katheterablationen bei 16309 Patienten mit
VorhofflimmernCappato et al Circulation Arrhythm Electrophysiol. 2010; 3:32-38
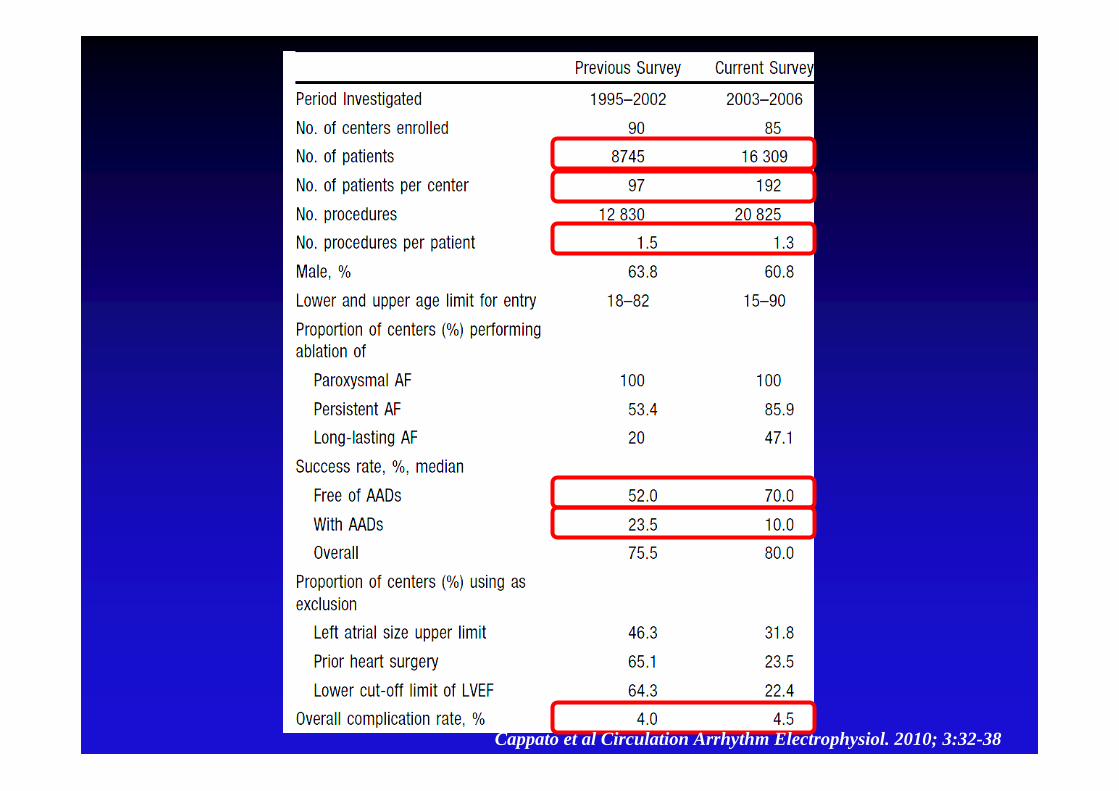
Cappato et al Circulation Arrhythm Electrophysiol. 2010; 3:32-38
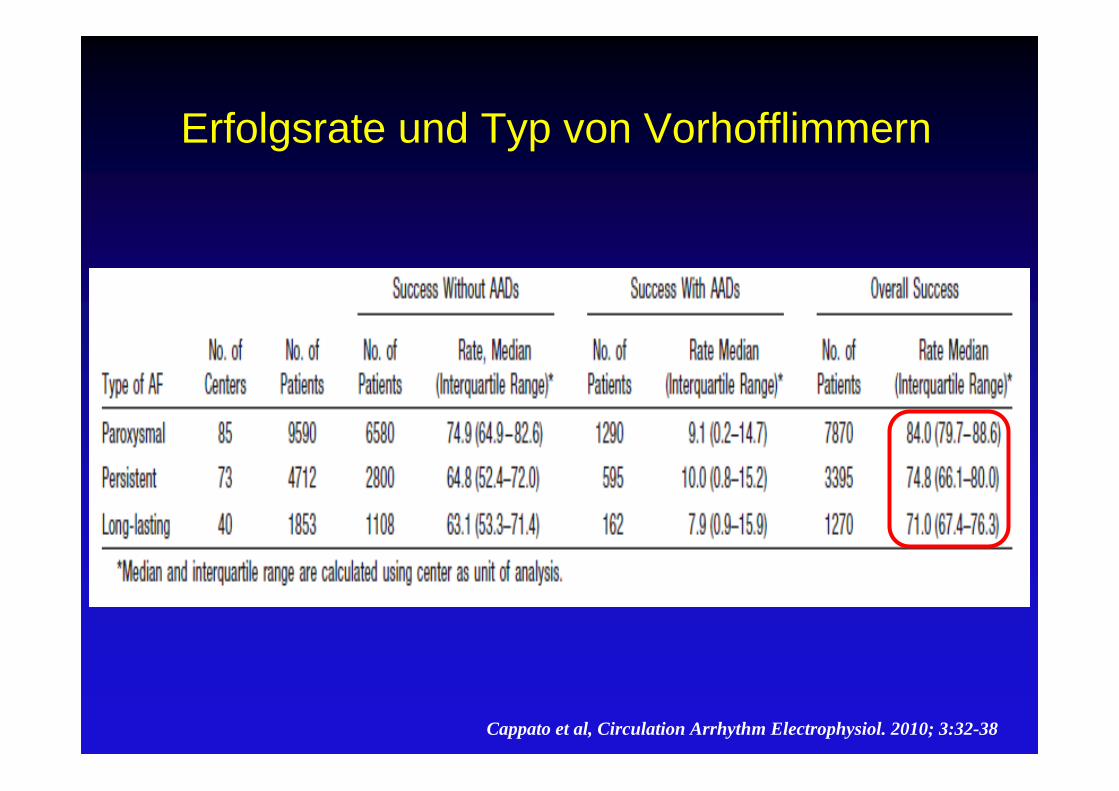
Erfolgsrate und Typ von Vorhofflimmern
Cappato et al, Circulation Arrhythm Electrophysiol. 2010; 3:32-38
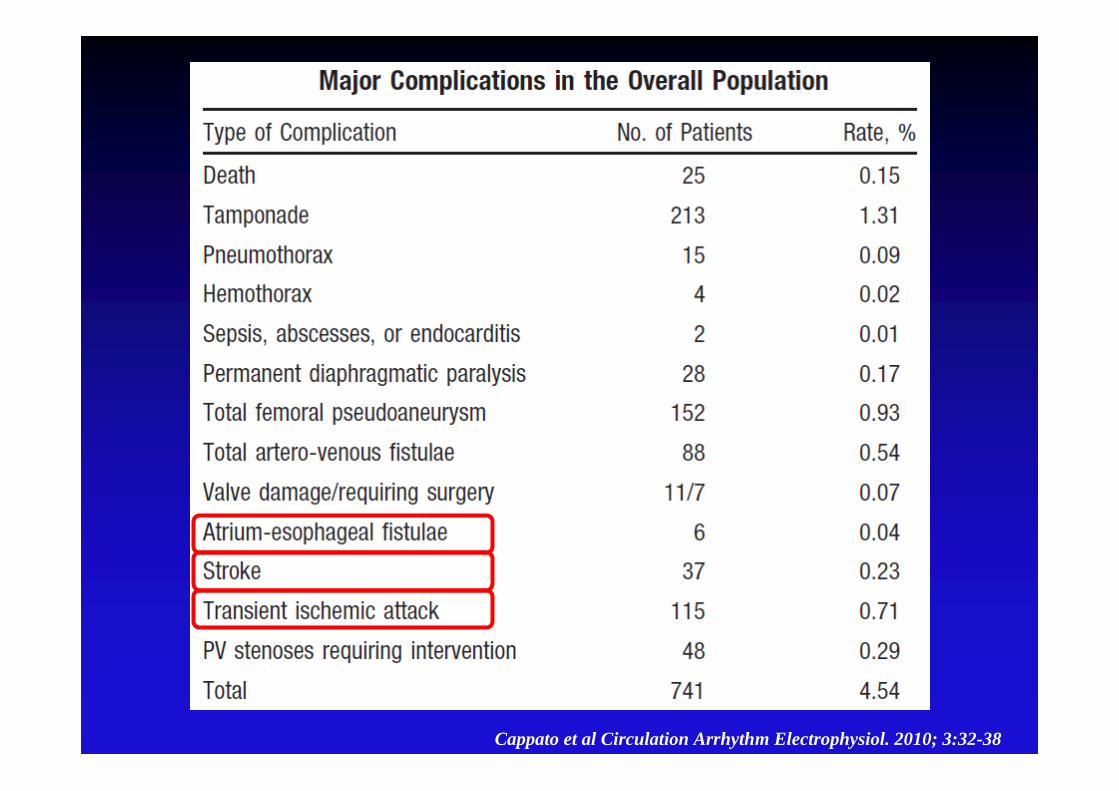
Cappato et al Circulation Arrhythm Electrophysiol. 2010; 3:32-38


Warum Antiarrhythmika ?
Symptomatik Suppression von Vorhofflimmern
Reduktion der Überleitungsfrequenz zur Kammer
Reduktion der Häufigkeit
Verbesserung der Lebensqualität
Mortalität Reduktion der Mortalität ?
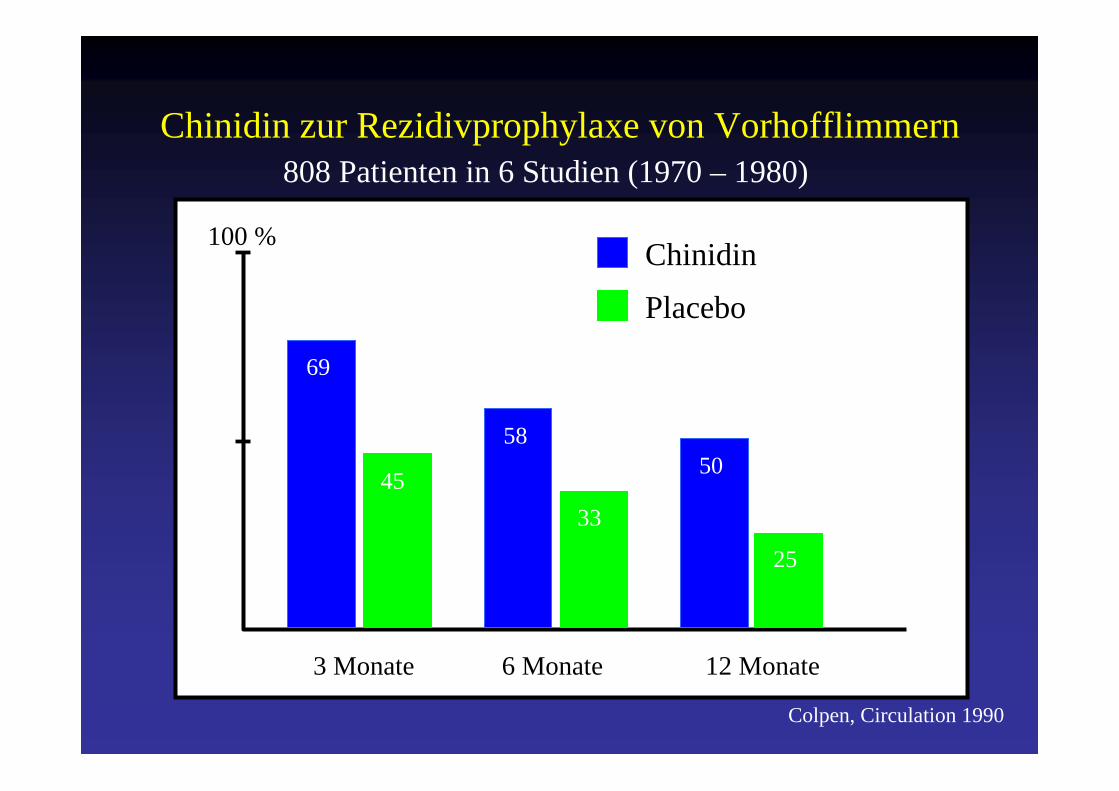
Chinidin zur Rezidivprophylaxe von Vorhofflimmern
100 %
3 Monate 6 Monate 12 Monate
69
45
58
33
50
25
Chinidin
Placebo
808 Patienten in 6 Studien (1970 – 1980)
Colpen, Circulation 1990
Chinidin zur Rezidivprophylaxe von Vorhofflimmern
Colpen, Circulation 1990
Mortalität
unter Chinidin 2,9 %
unter Placebo 0,8 %
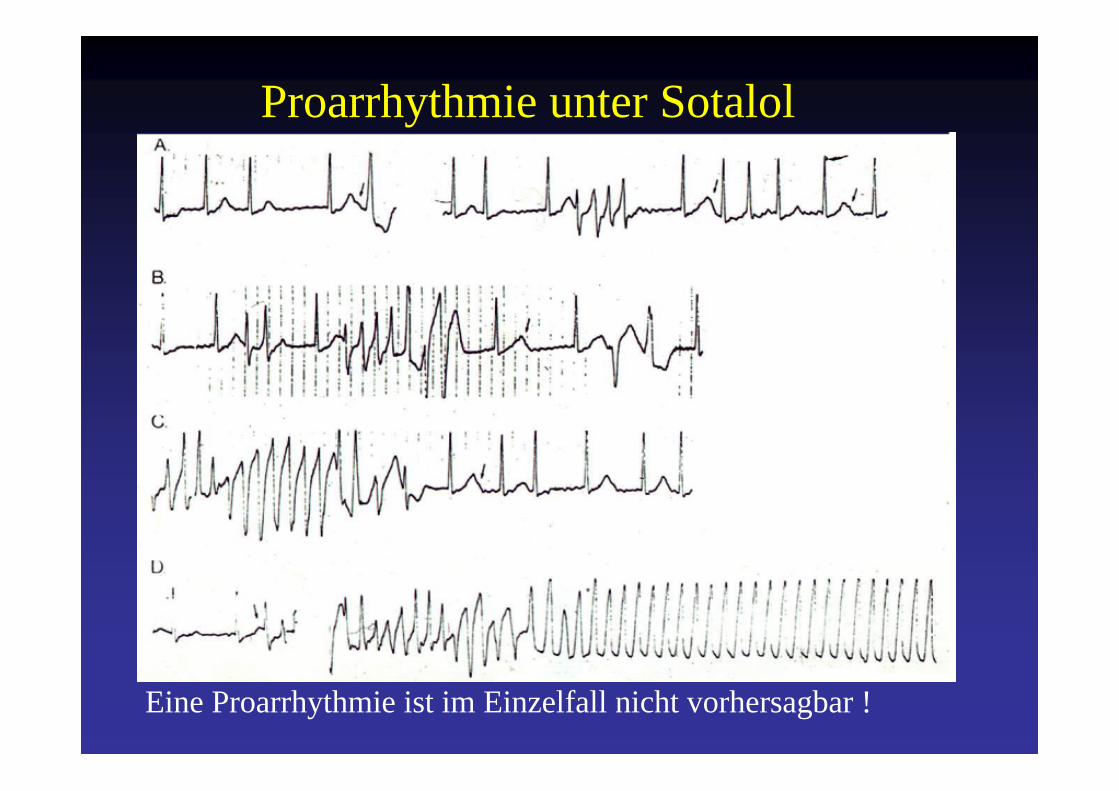
Proarrhythmie unter Sotalol
Eine Proarrhythmie ist im Einzelfall nicht vorhersagbar !


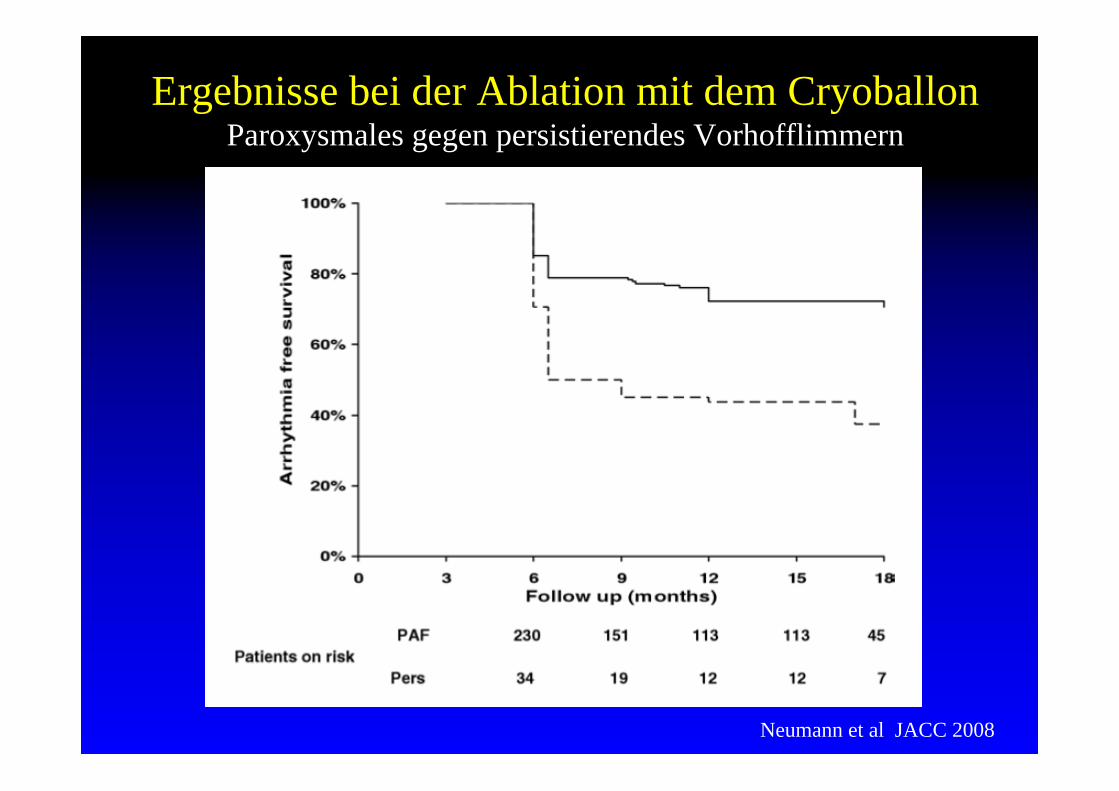
Ergebnisse bei der Ablation mit dem CryoballonParoxysmales gegen persistierendes Vorhofflimmern
Neumann et al JACC 2008

Camm et al, European Heart Journal (2010) 31, 2369–2429
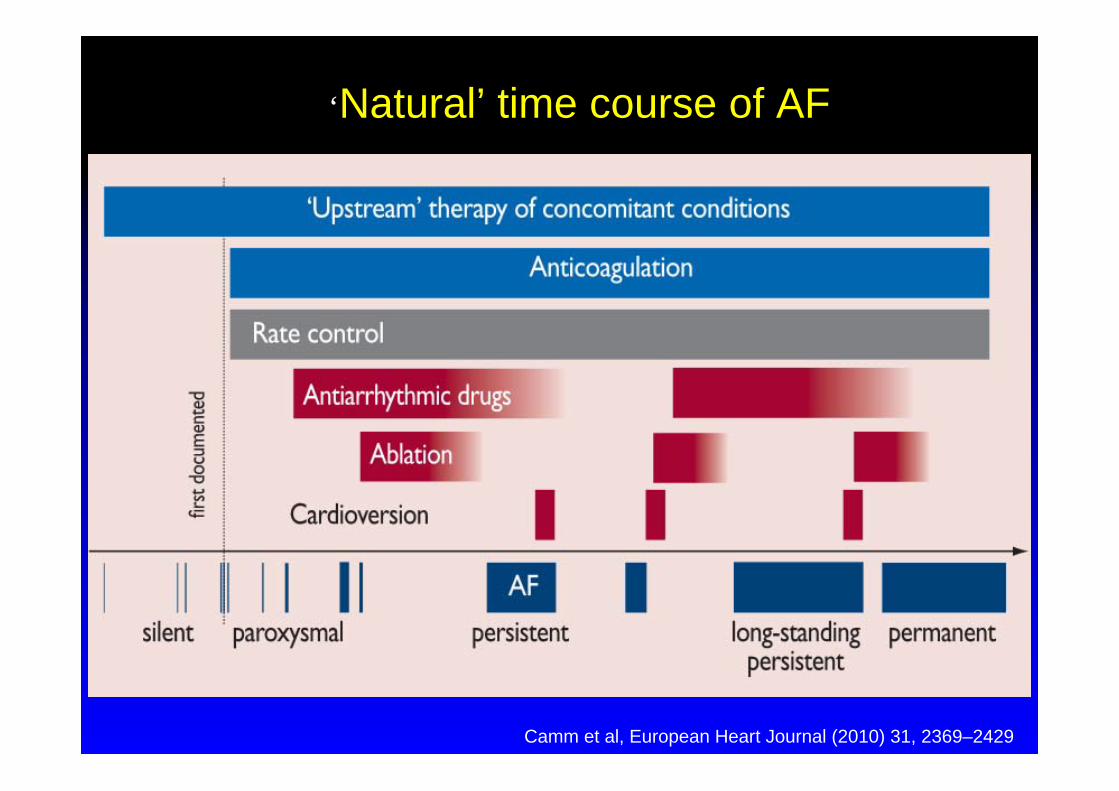
‘Natural’ time course of AF
Camm et al, European Heart Journal (2010) 31, 2369–2429
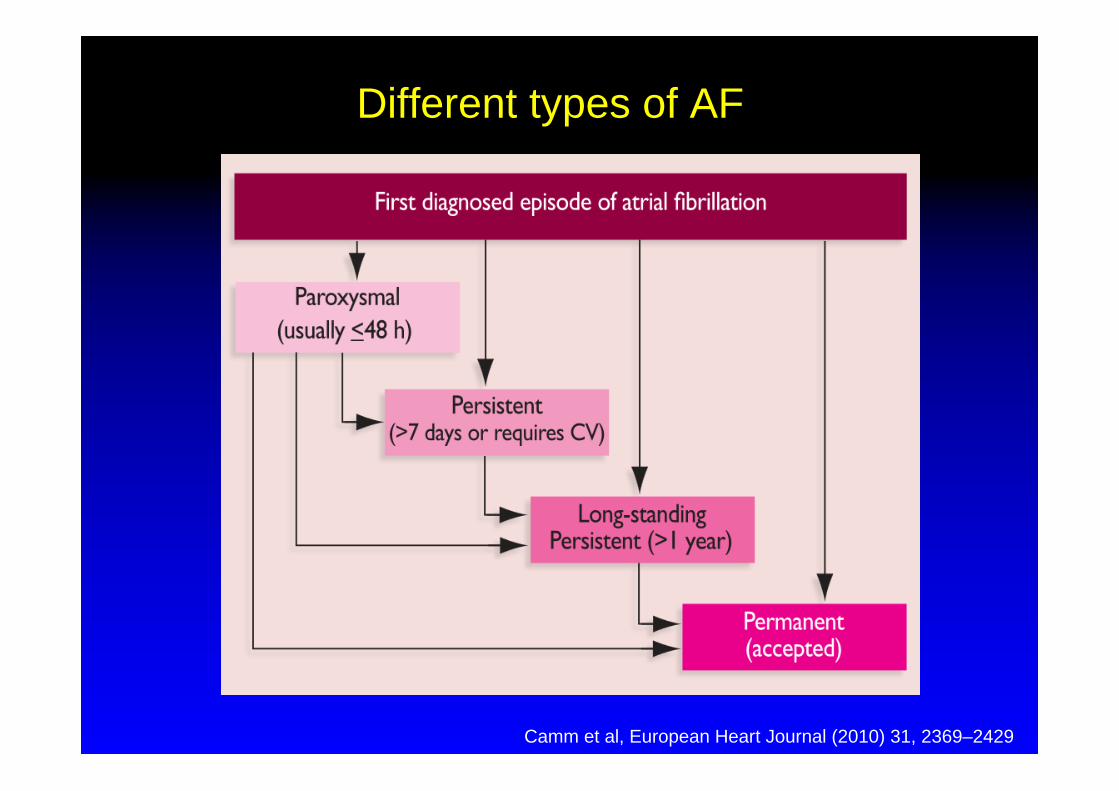
Different types of AF
Camm et al, European Heart Journal (2010) 31, 2369–2429
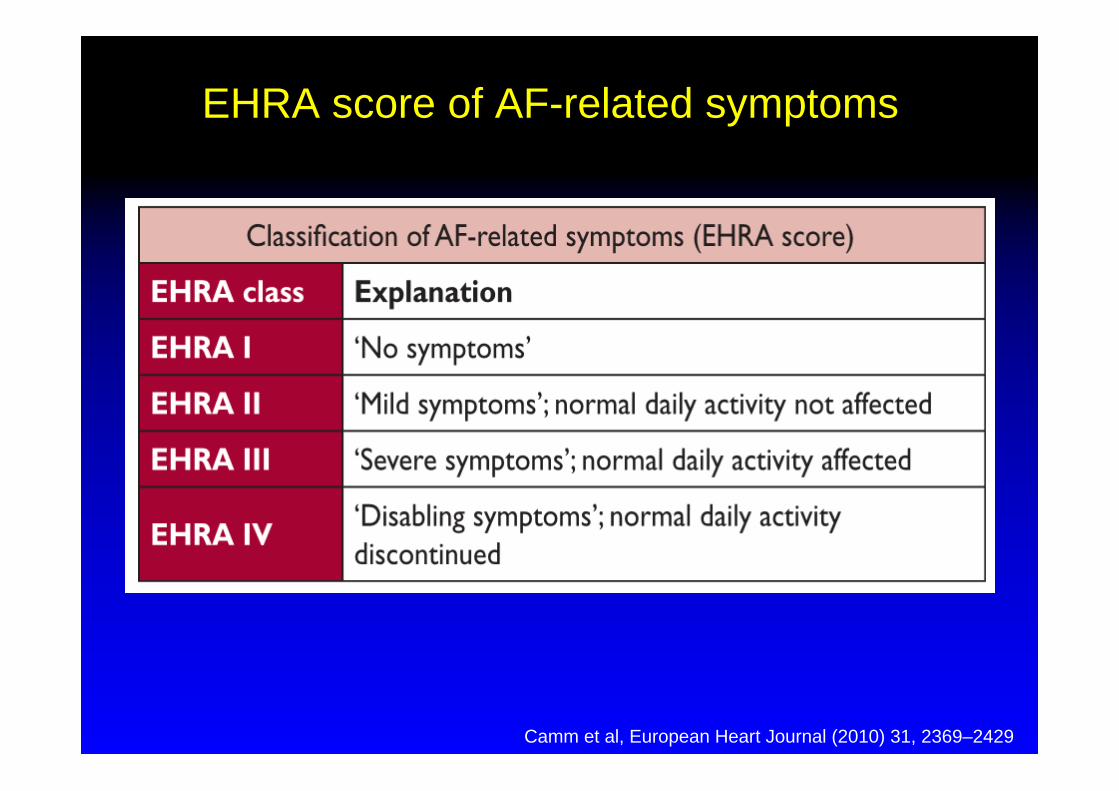
EHRA score of AF-related symptoms
Camm et al, European Heart Journal (2010) 31, 2369–2429
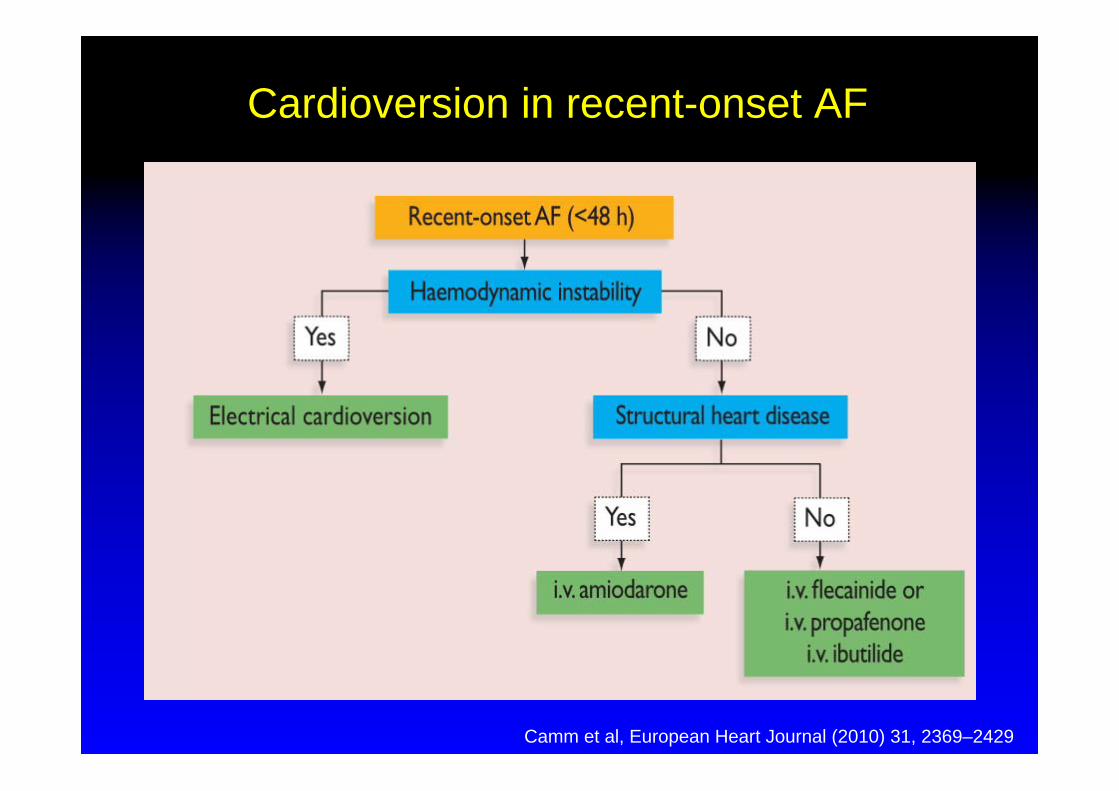
Cardioversion in recent-onset AF
Camm et al, European Heart Journal (2010) 31, 2369–2429
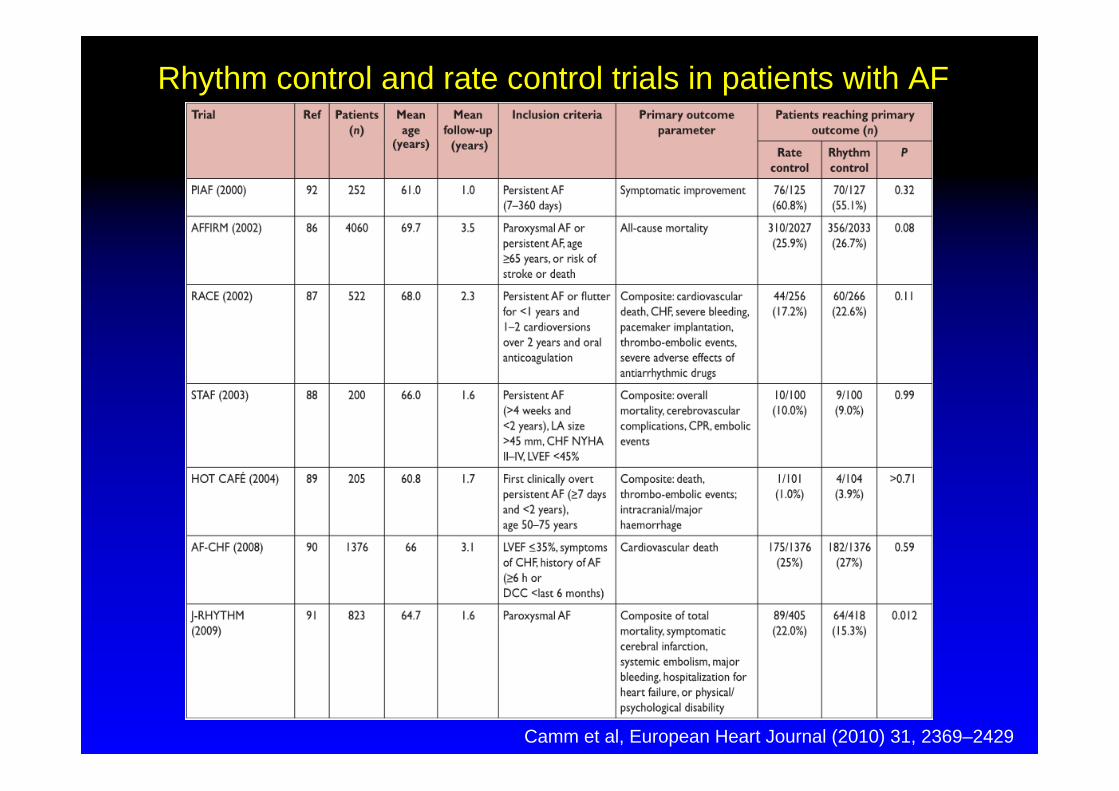
Rhythm control and rate control trials in patients with AF
Camm et al, European Heart Journal (2010) 31, 2369–2429
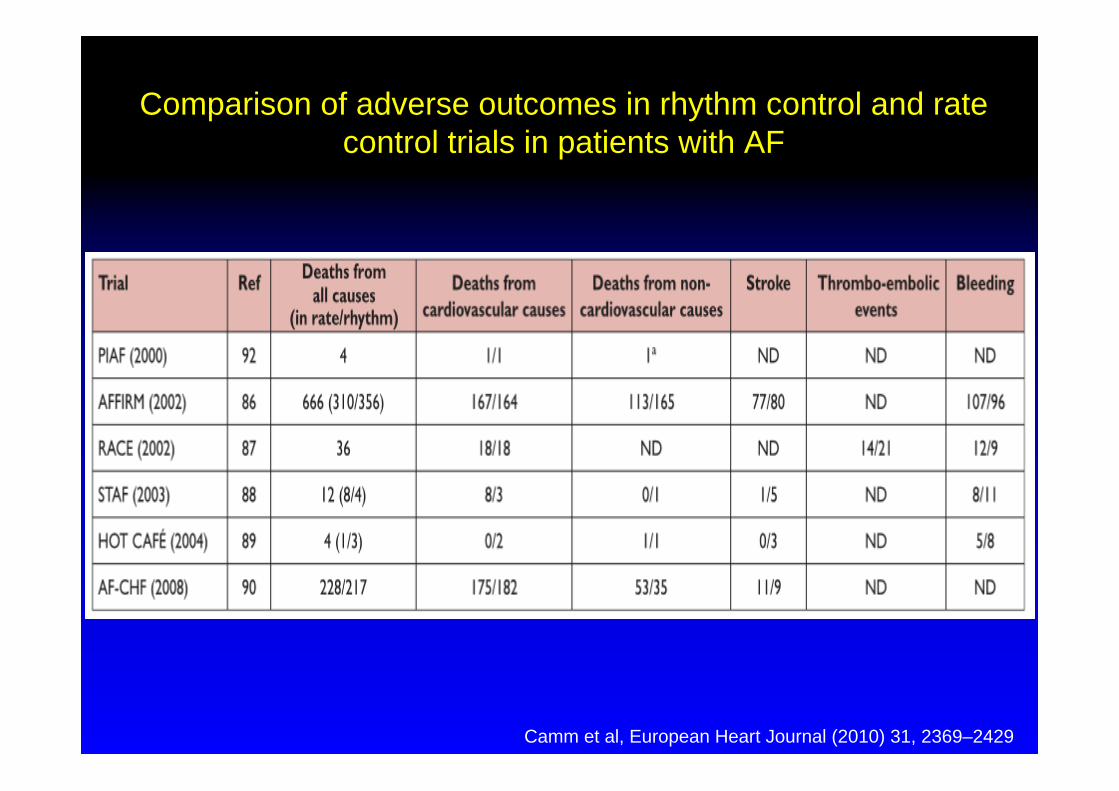
Camm et al, European Heart Journal (2010) 31, 2369–2429
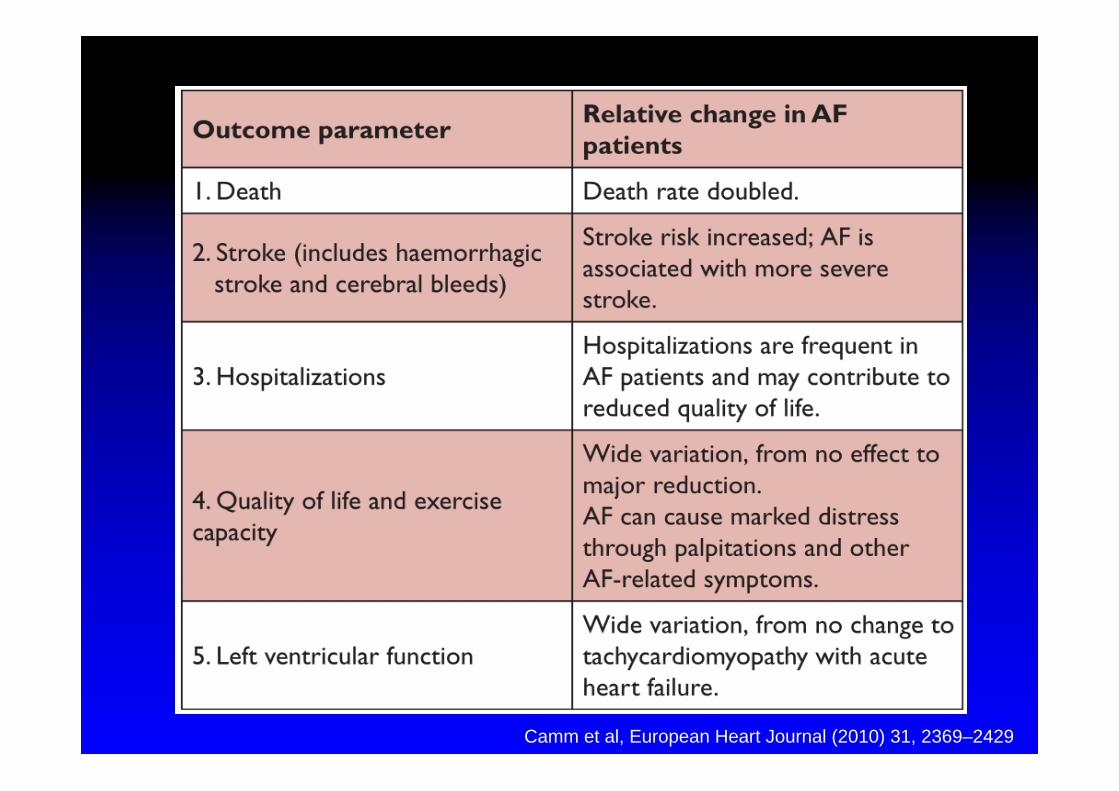
Comparison of adverse outcomes in rhythm control and rate control trials in patients with AF
Camm et al, European Heart Journal (2010) 31, 2369–2429
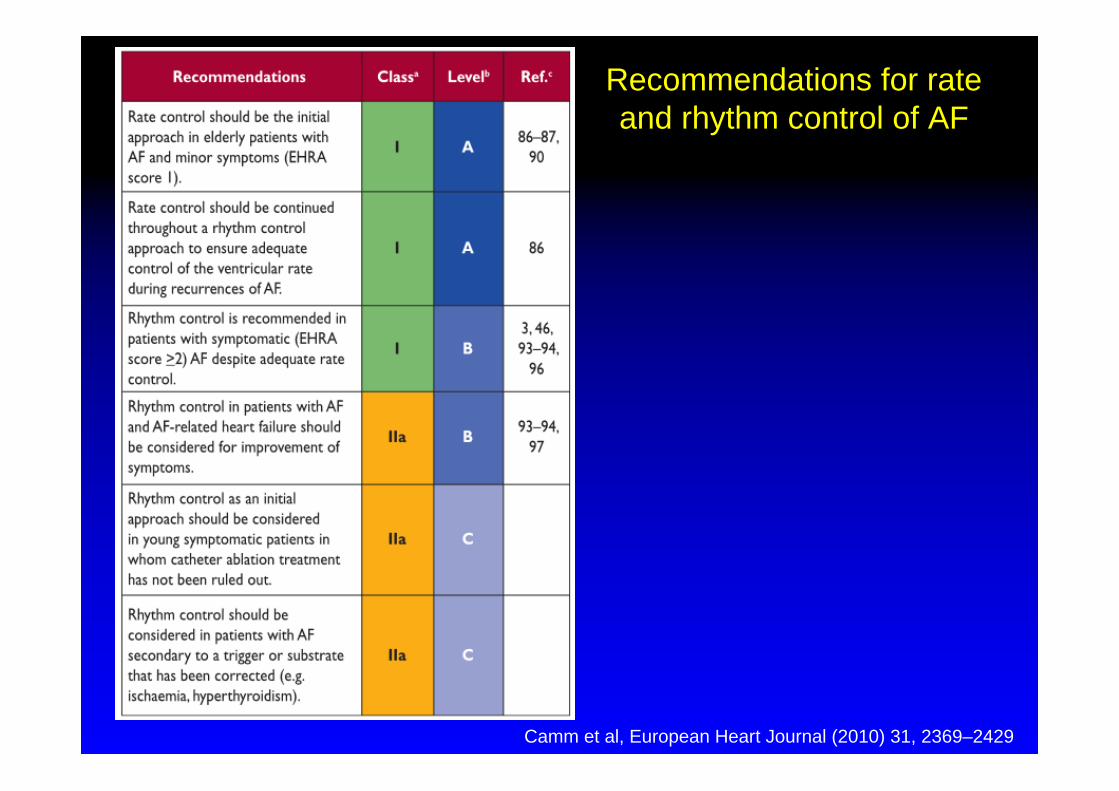
Recommendations for rate and rhythm control of AF
Camm et al, European Heart Journal (2010) 31, 2369–2429
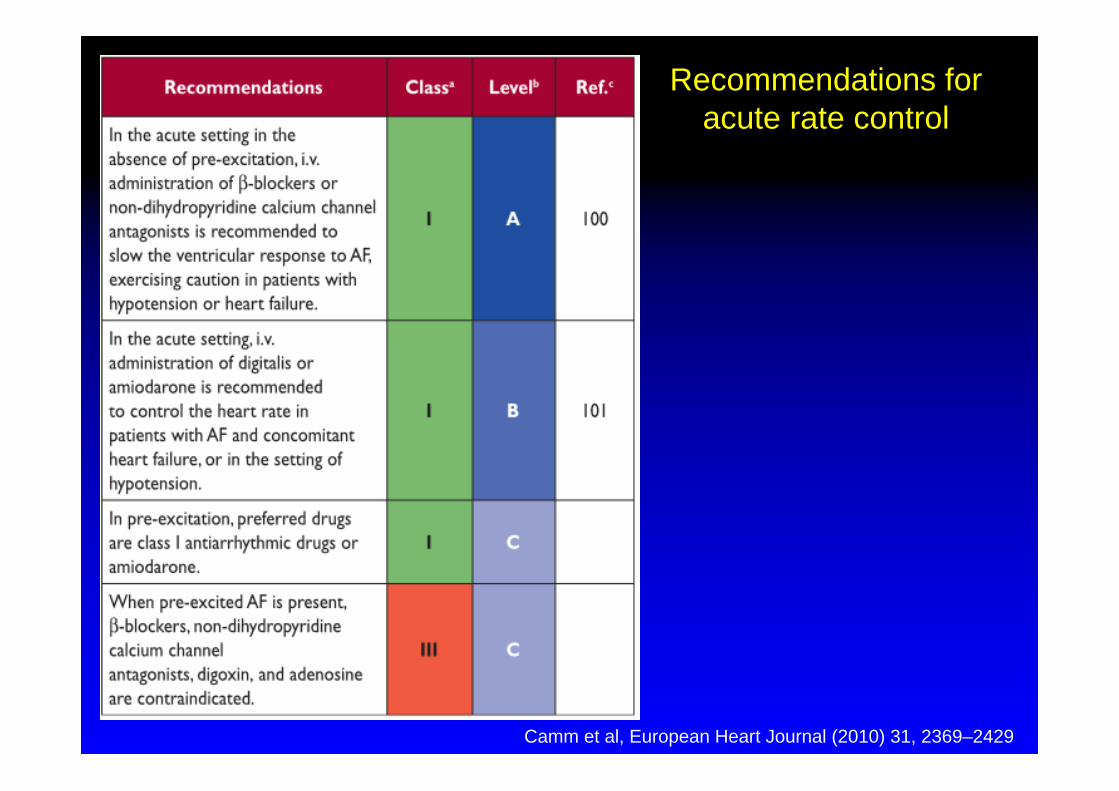
Recommendations for acute rate control
Camm et al, European Heart Journal (2010) 31, 2369–2429
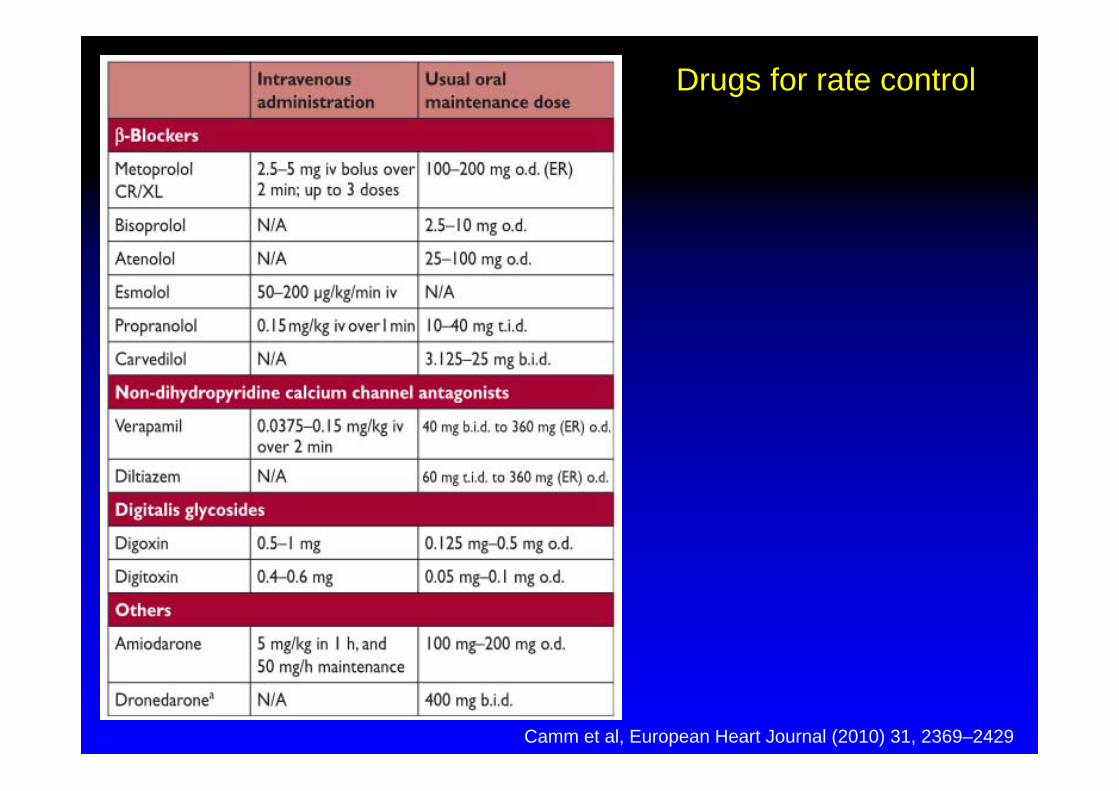
Drugs for rate control
Camm et al, European Heart Journal (2010) 31, 2369–2429
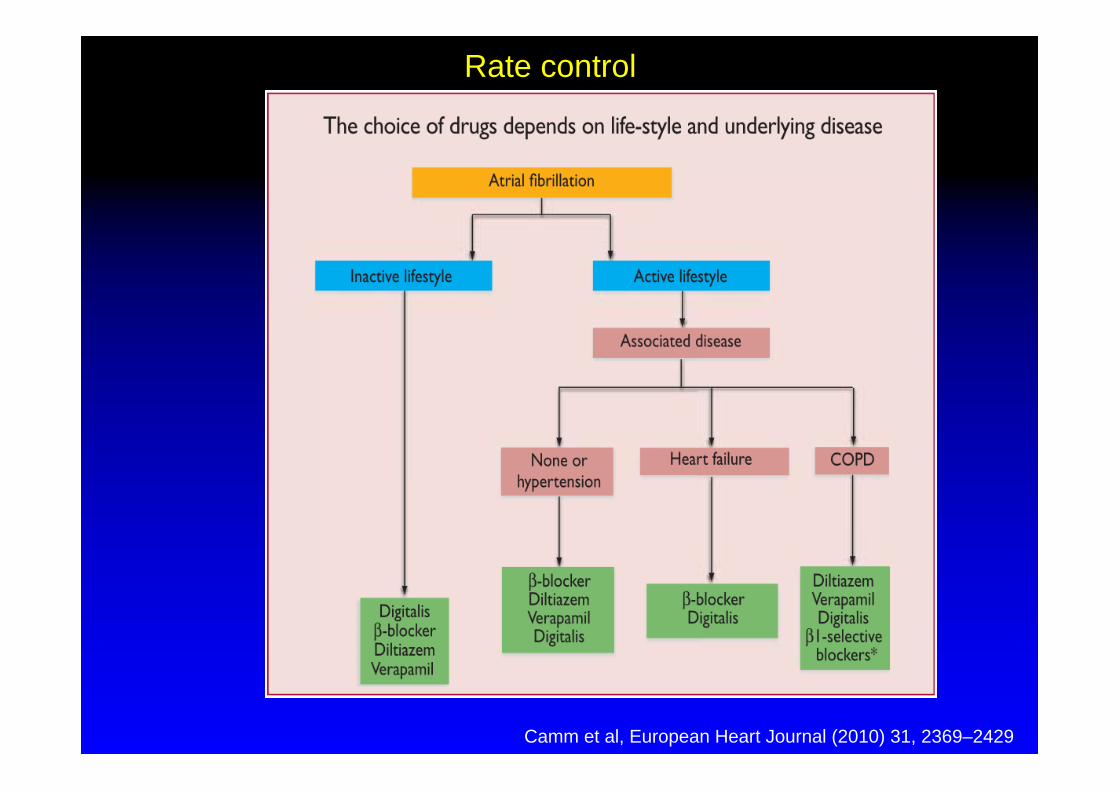
Rate control
Camm et al, European Heart Journal (2010) 31, 2369–2429
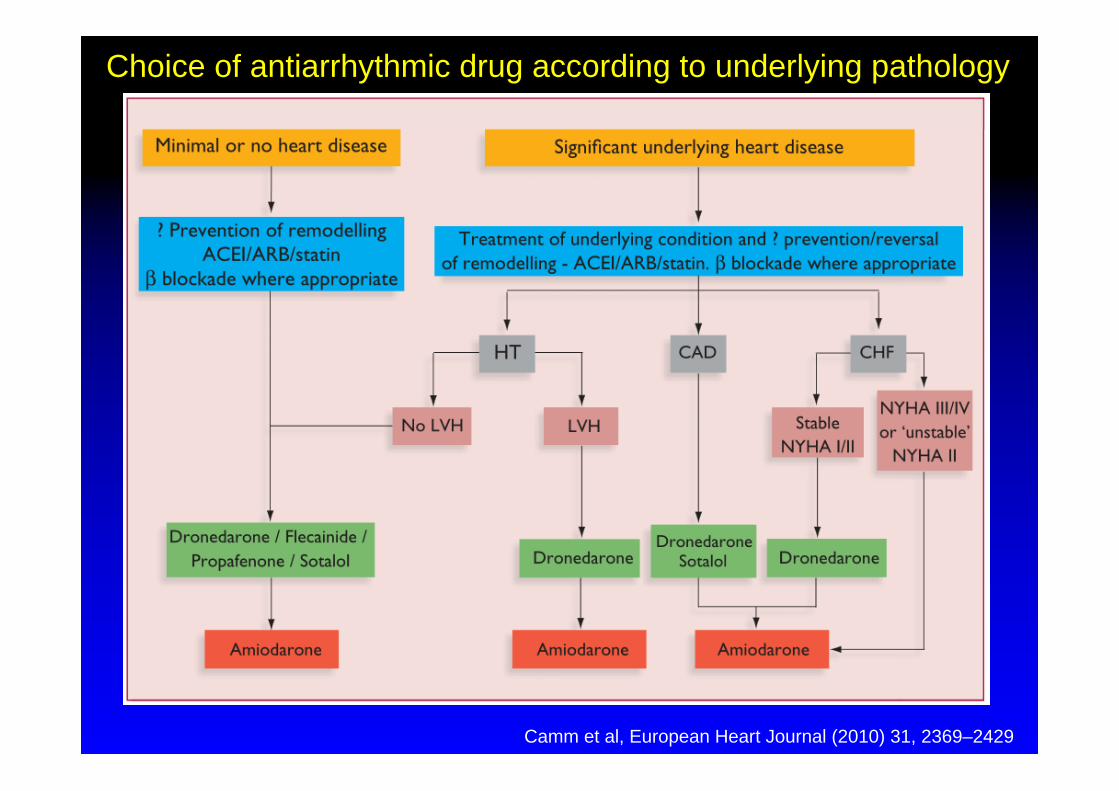
Choice of antiarrhythmic drug according to underlying pathology
Camm et al, European Heart Journal (2010) 31, 2369–2429
Recommendation for choice of antiarrhythmic drug for AF control
Camm et al, European Heart Journal (2010) 31, 2369–2429
Choice between ablation and antiarrhythmic drug therapy for patients with and without structural heart disease

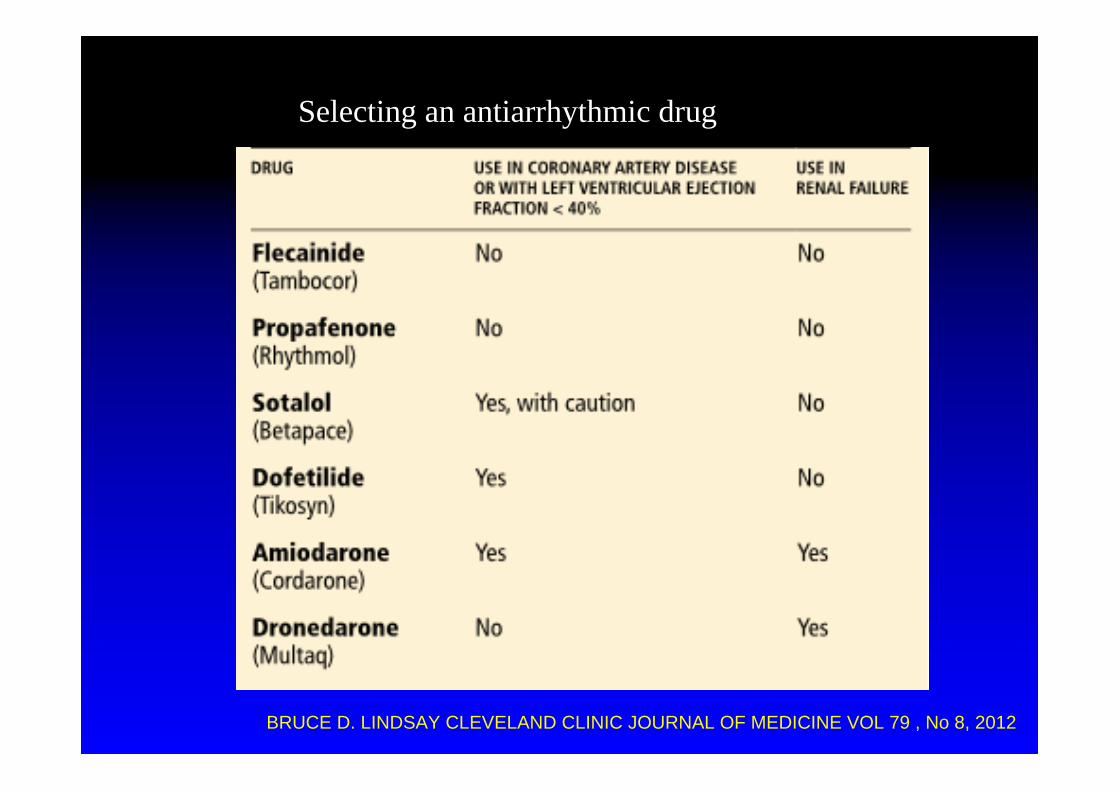
Selecting an antiarrhythmic drug
BRUCE D. LINDSAY CLEVELAND CLINIC JOURNAL OF MEDICINE VOL 79 , No 8, 2012

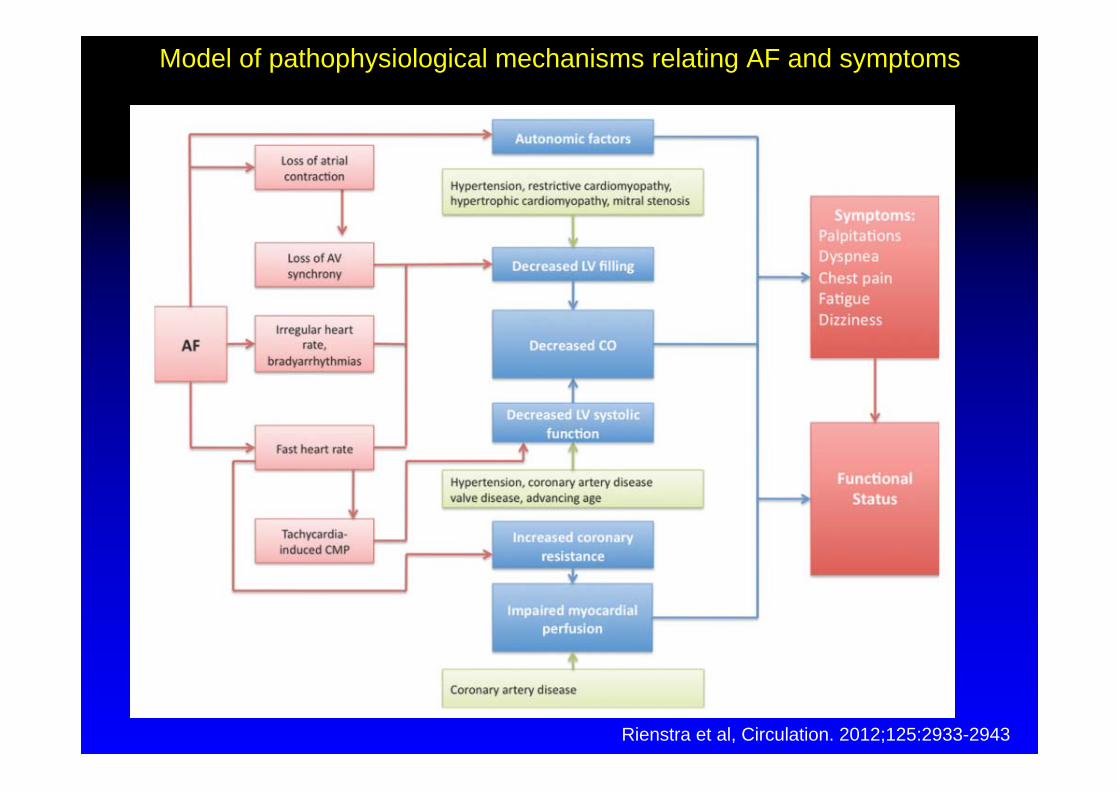
Rienstra et al, Circulation. 2012;125:2933-2943
Model of pathophysiological mechanisms relating AF and symptoms

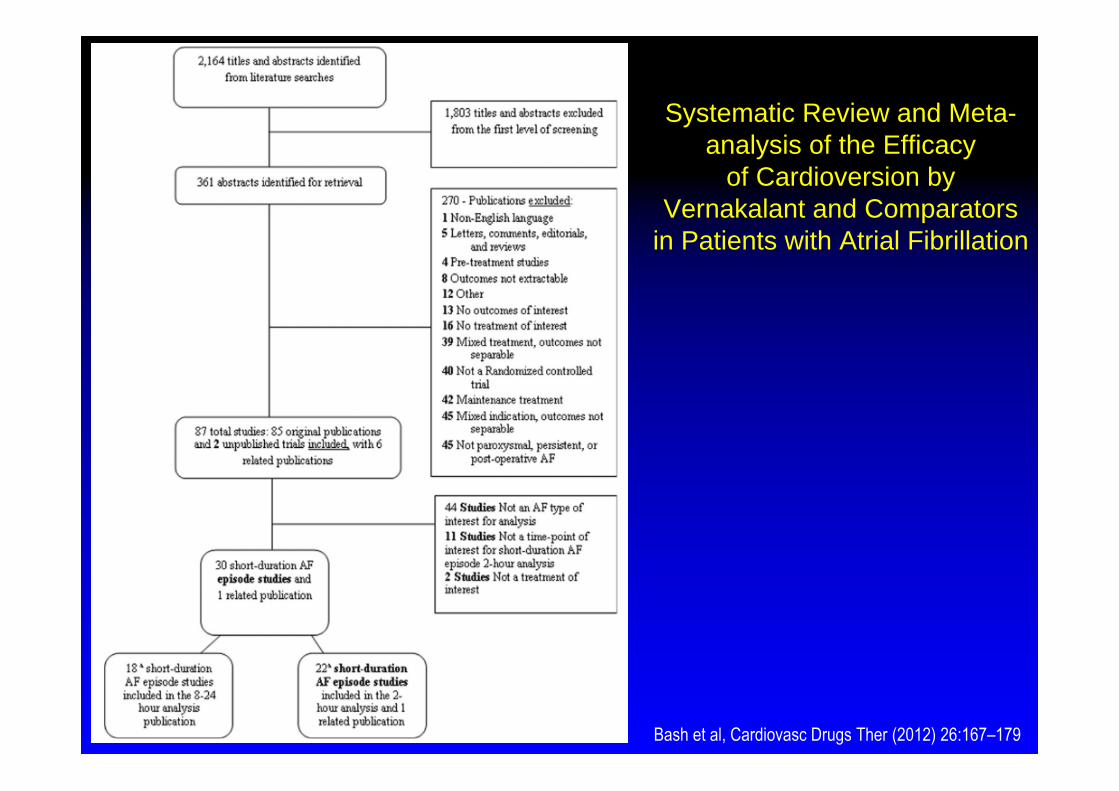
Systematic Review and Meta-analysis of the Efficacy
of Cardioversion by Vernakalant and Comparators
in Patients with Atrial Fibrillation
Bash et al, Cardiovasc Drugs Ther (2012) 26:167–179
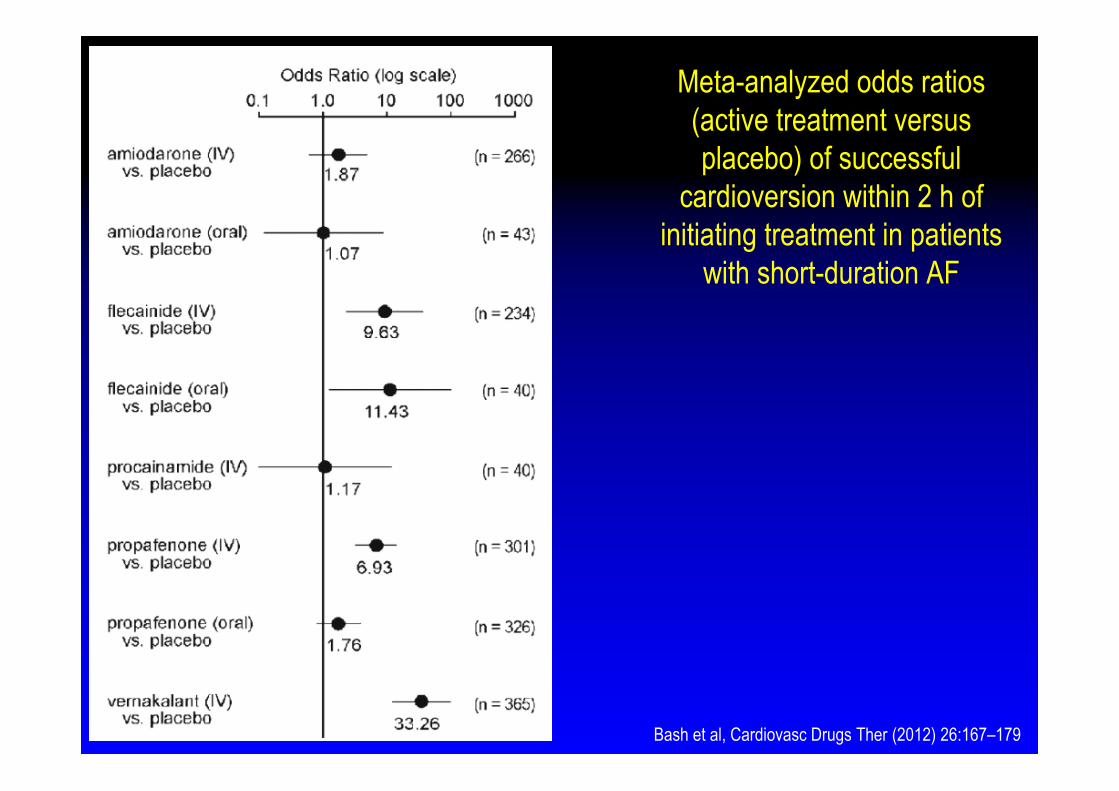
Meta-analyzed odds ratios (active treatment versus placebo) of successful
cardioversion within 2 h of initiating treatment in patients
with short-duration AF
Bash et al, Cardiovasc Drugs Ther (2012) 26:167–179
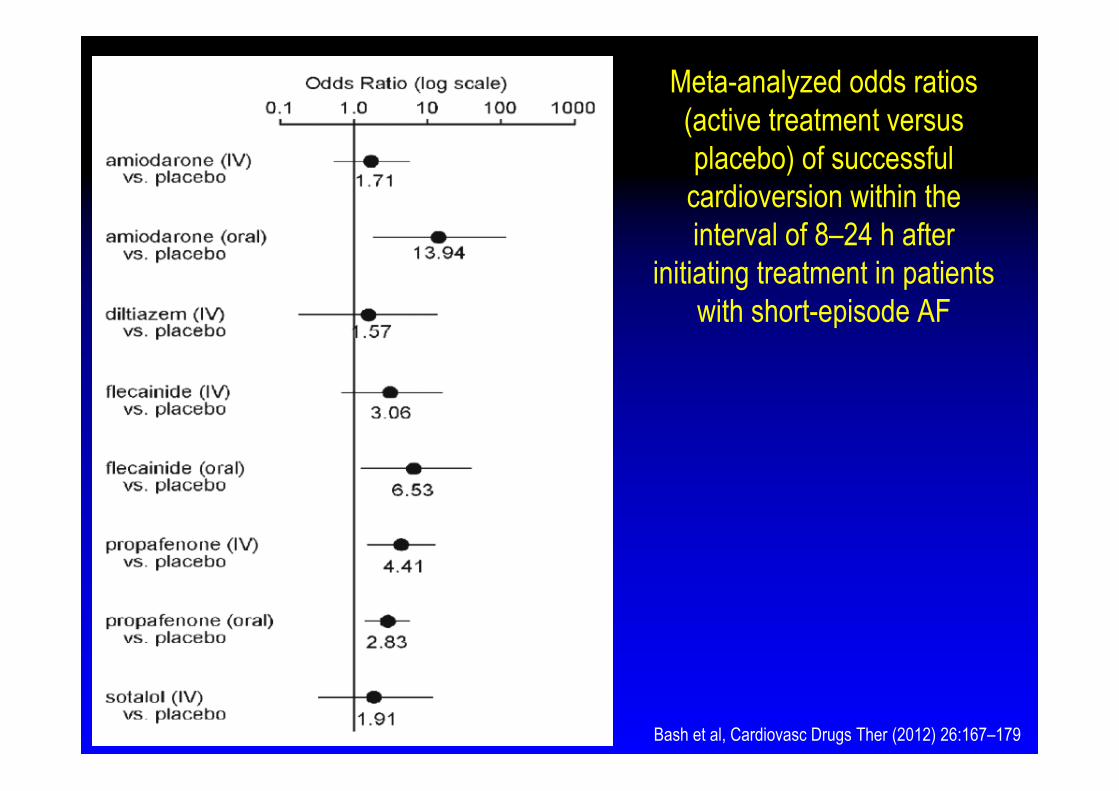
Meta-analyzed odds ratios (active treatment versus placebo) of successful cardioversion within the interval of 8–24 h after
initiating treatment in patients with short-episode AF
Bash et al, Cardiovasc Drugs Ther (2012) 26:167–179

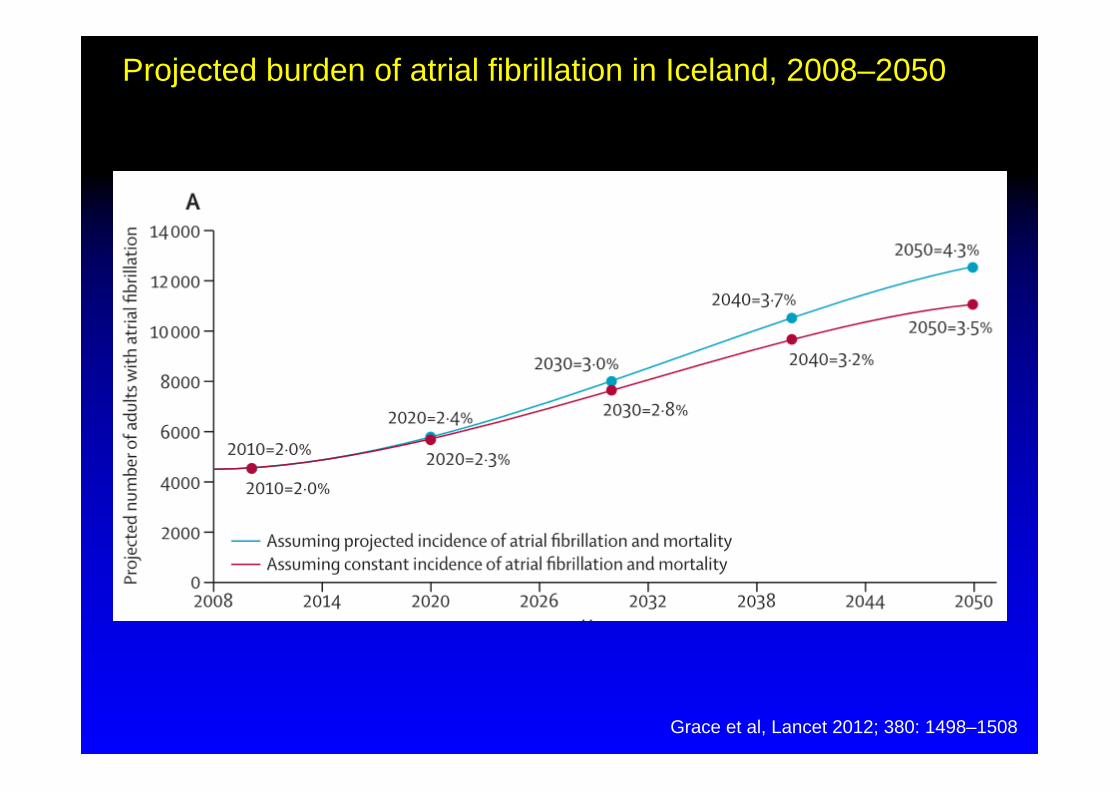
Grace et al, Lancet 2012; 380: 1498–1508
Projected burden of atrial fibrillation in Iceland, 2008–2050
Grace et al, Lancet 2012; 380: 1498–1508
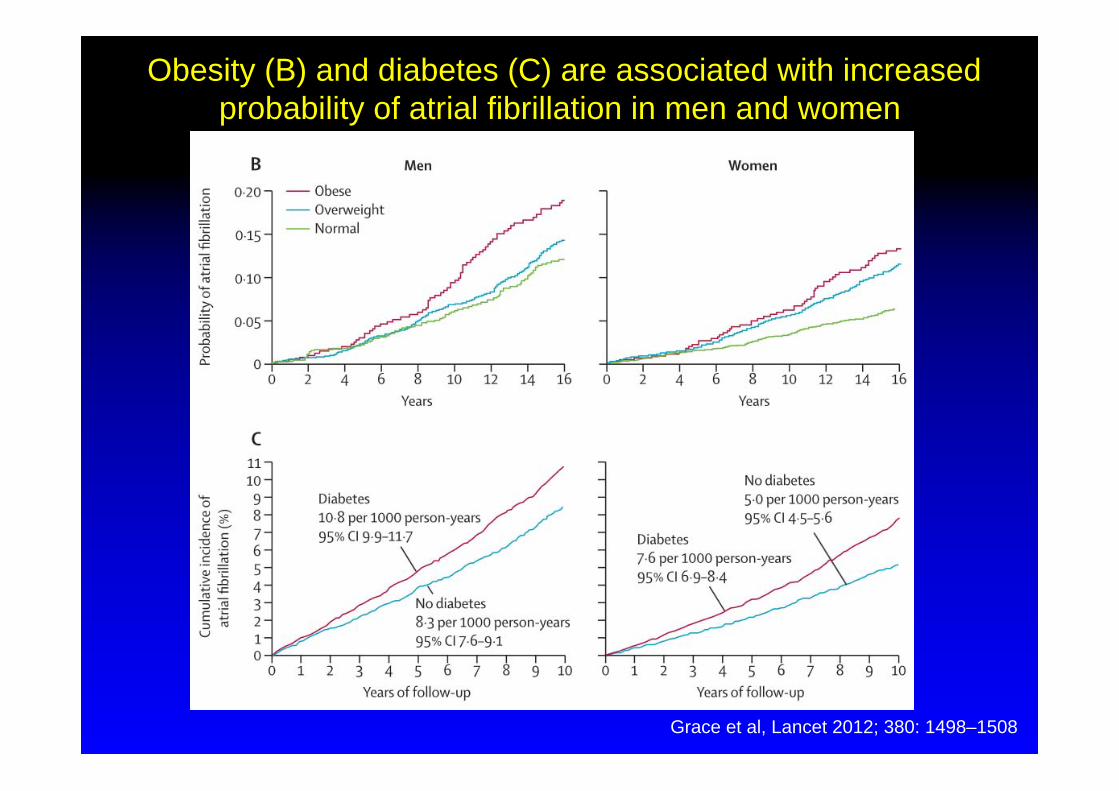
Obesity (B) and diabetes (C) are associated with increased probability of atrial fibrillation in men and women
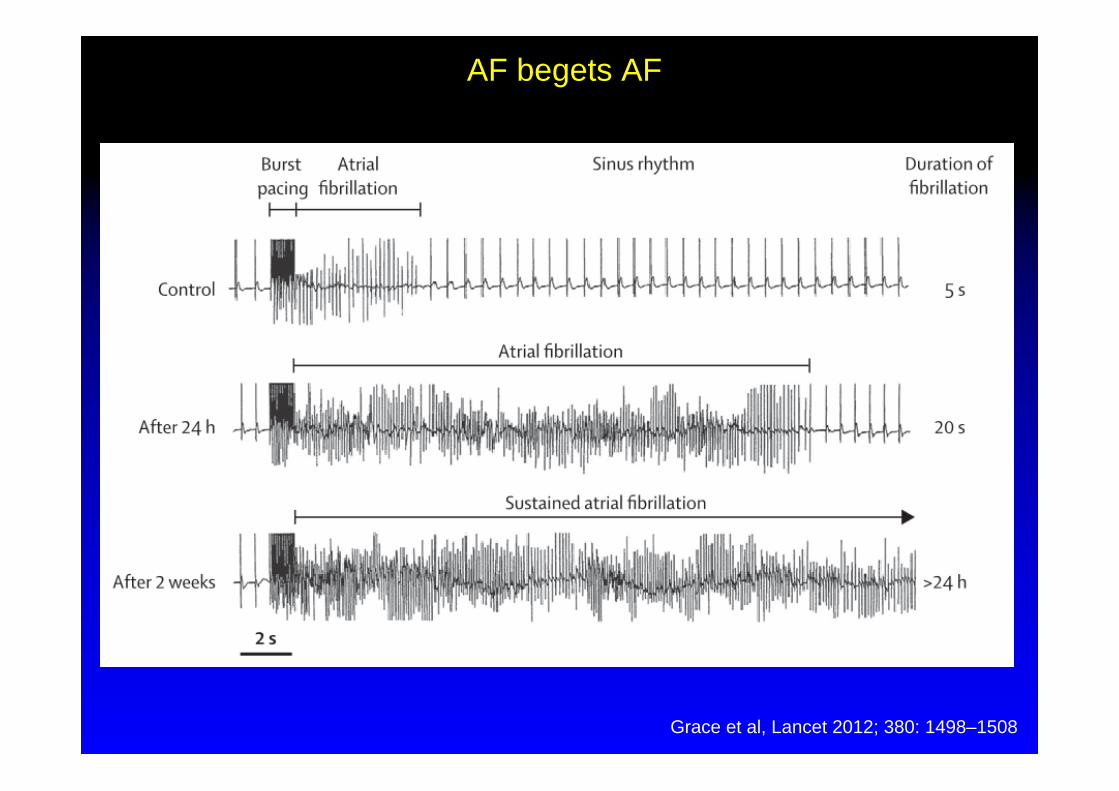
Grace et al, Lancet 2012; 380: 1498–1508
AF begets AF


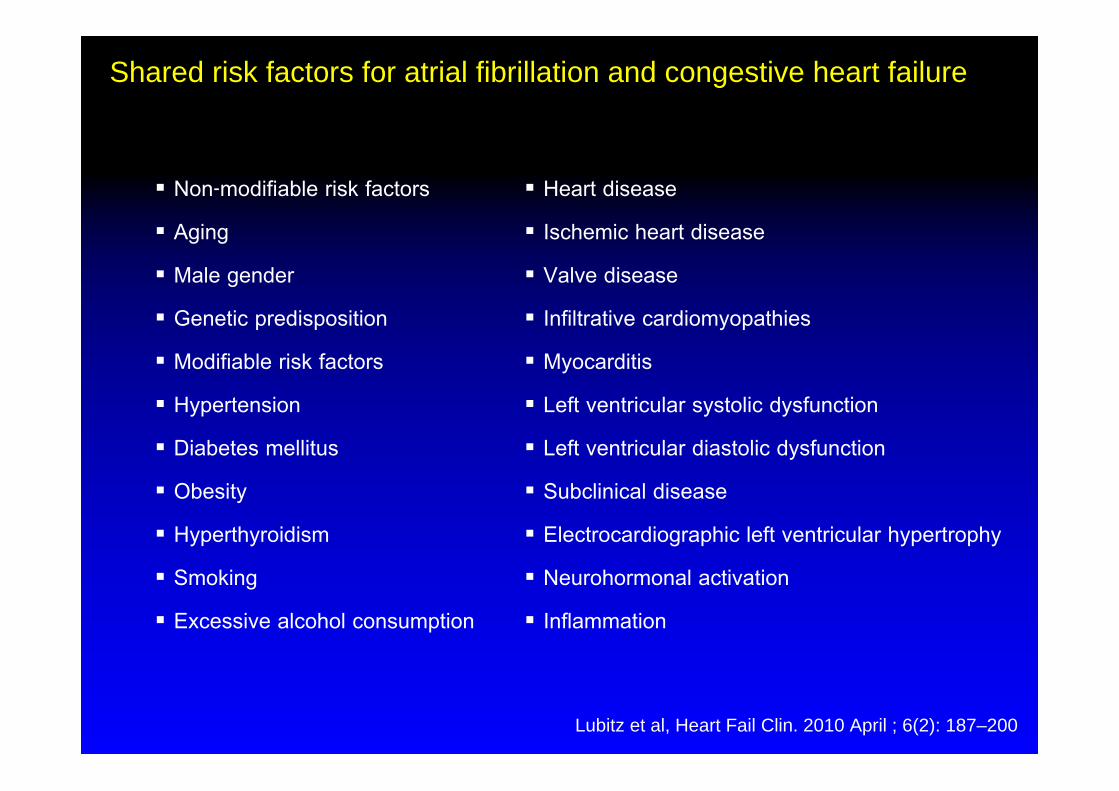
Non-modifiable risk factors
Aging
Male gender
Genetic predisposition
Modifiable risk factors
Hypertension
Diabetes mellitus
Obesity
Hyperthyroidism
Smoking
Excessive alcohol consumption
Shared risk factors for atrial fibrillation and congestive heart failure
Lubitz et al, Heart Fail Clin. 2010 April ; 6(2): 187–200
Heart disease
Ischemic heart disease
Valve disease
Infiltrative cardiomyopathies
Myocarditis
Left ventricular systolic dysfunction
Left ventricular diastolic dysfunction
Subclinical disease
Electrocardiographic left ventricular hypertrophy
Neurohormonal activation
Inflammation

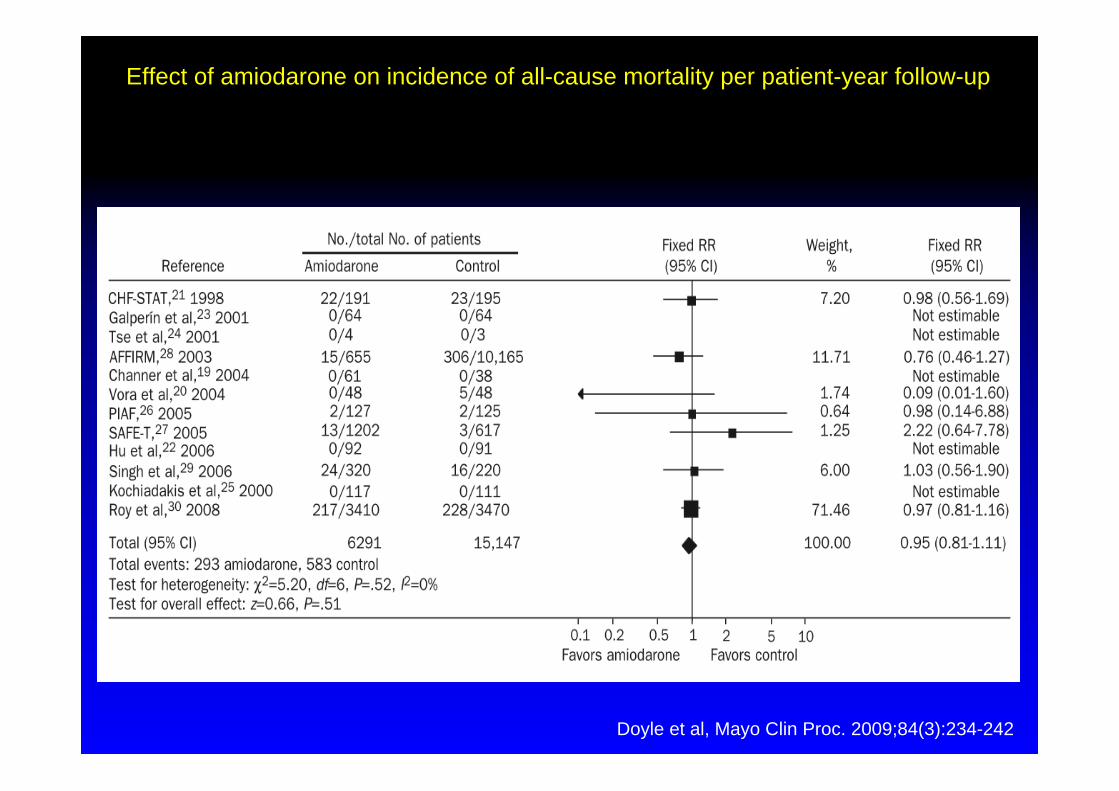
Effect of amiodarone on incidence of all-cause mortality per patient-year follow-up
Doyle et al, Mayo Clin Proc. 2009;84(3):234-242
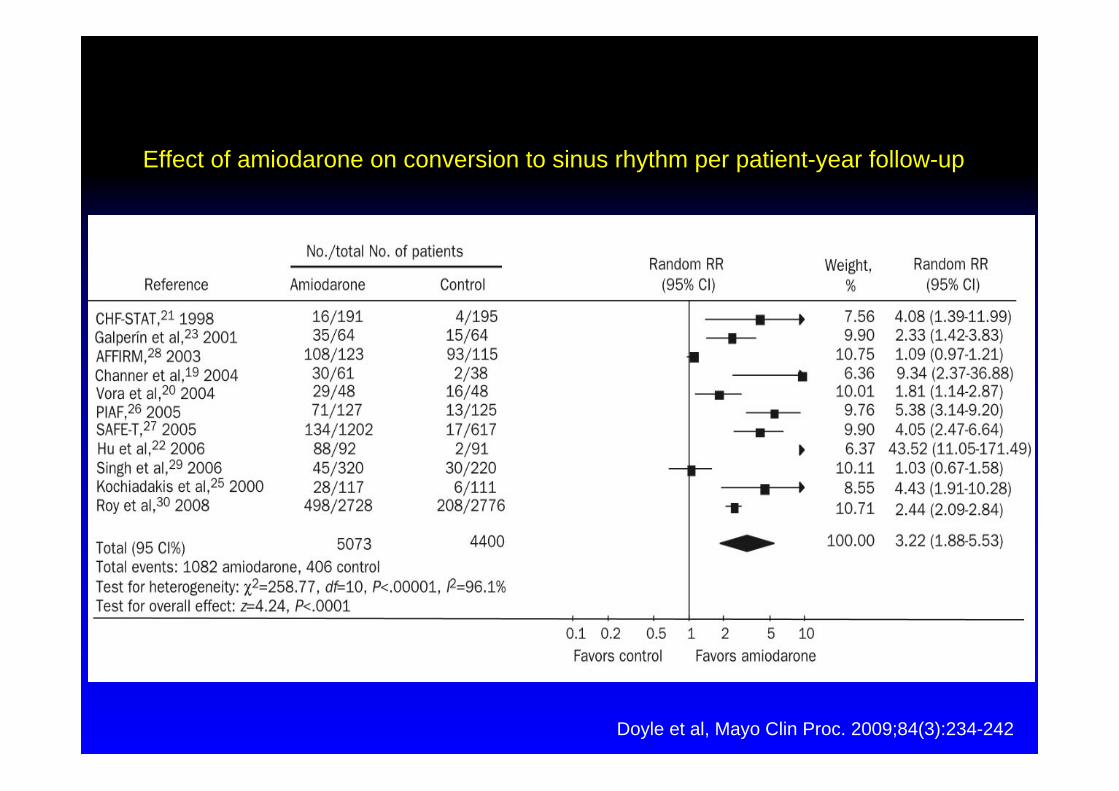
Effect of amiodarone on conversion to sinus rhythm per patient-year follow-up
Doyle et al, Mayo Clin Proc. 2009;84(3):234-242
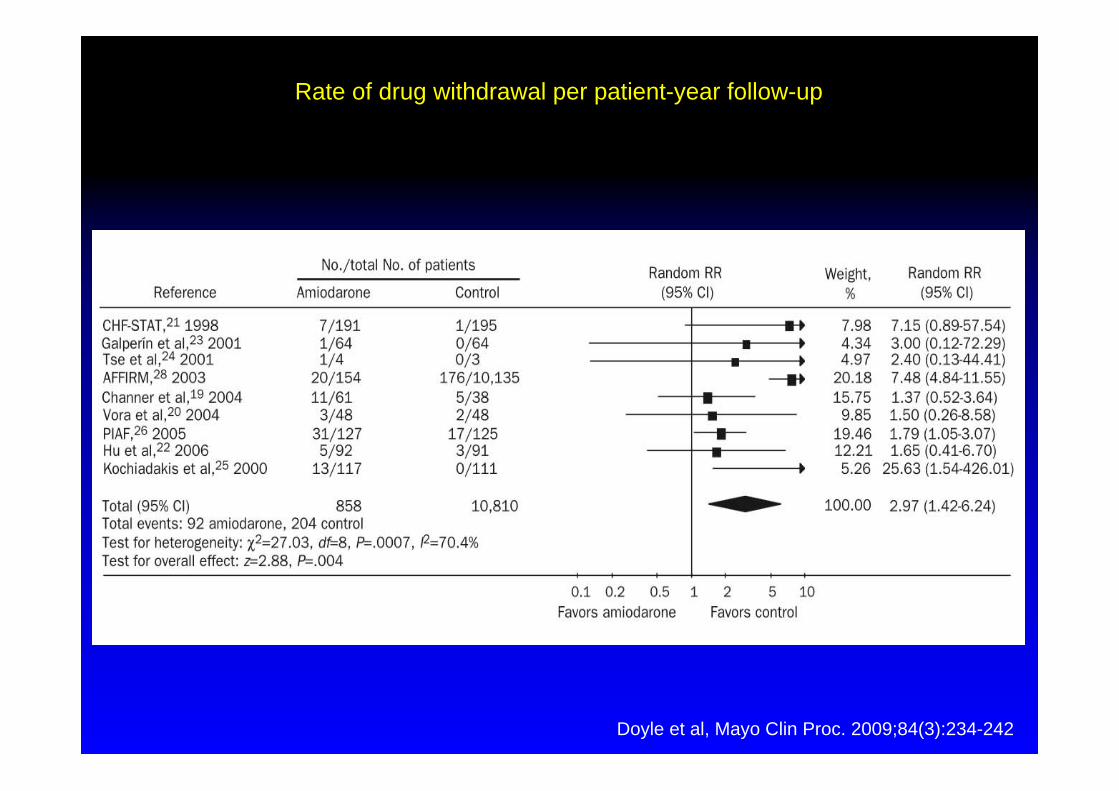
Rate of drug withdrawal per patient-year follow-up
Doyle et al, Mayo Clin Proc. 2009;84(3):234-242
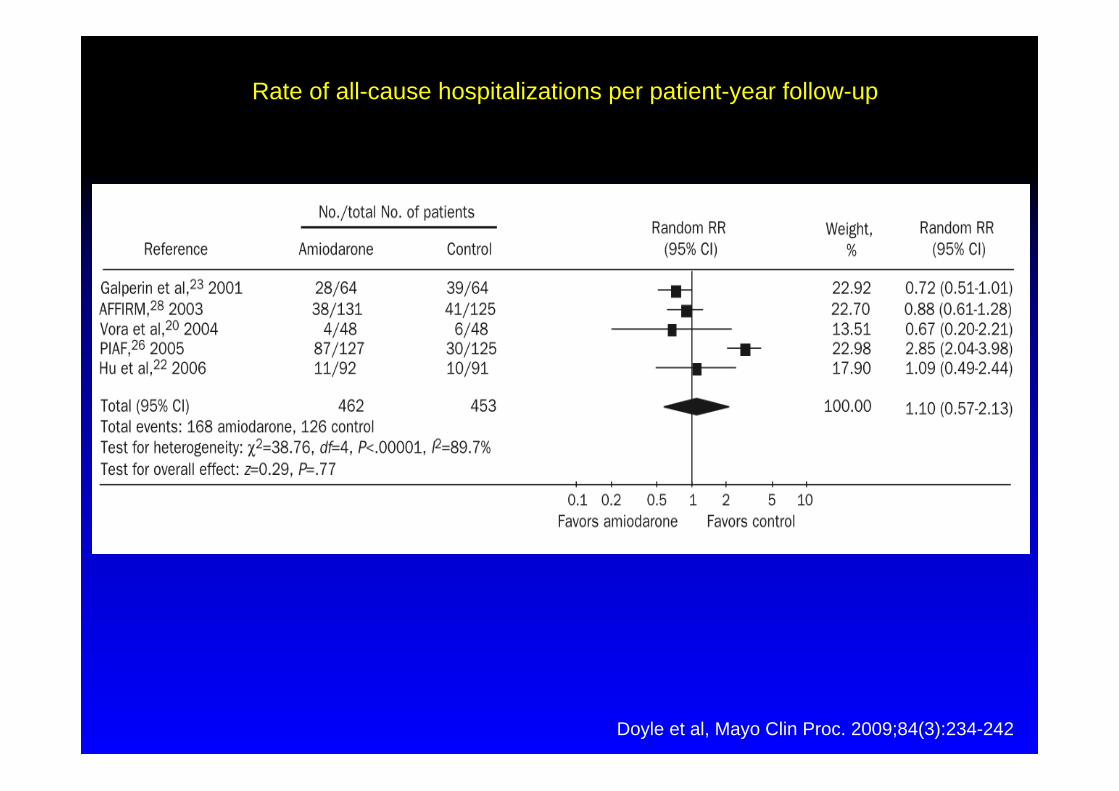
Rate of all-cause hospitalizations per patient-year follow-up
Doyle et al, Mayo Clin Proc. 2009;84(3):234-242
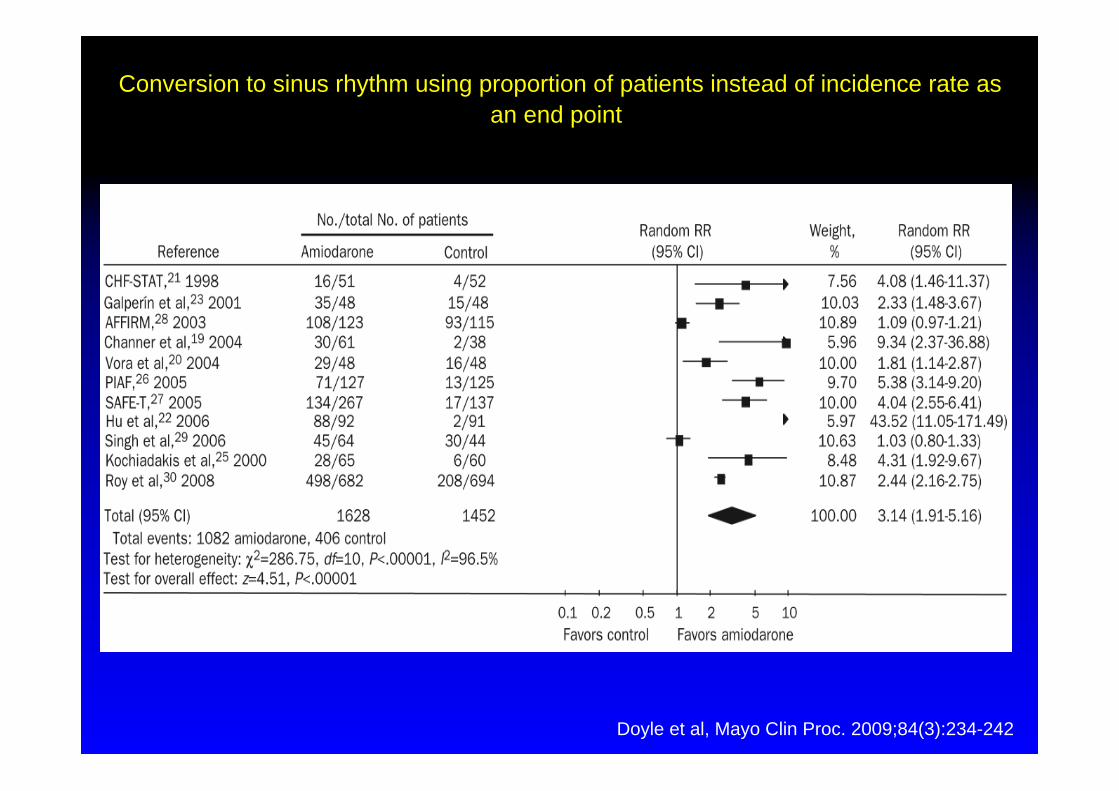
Conversion to sinus rhythm using proportion of patients instead of incidence rate as an end point
Doyle et al, Mayo Clin Proc. 2009;84(3):234-242

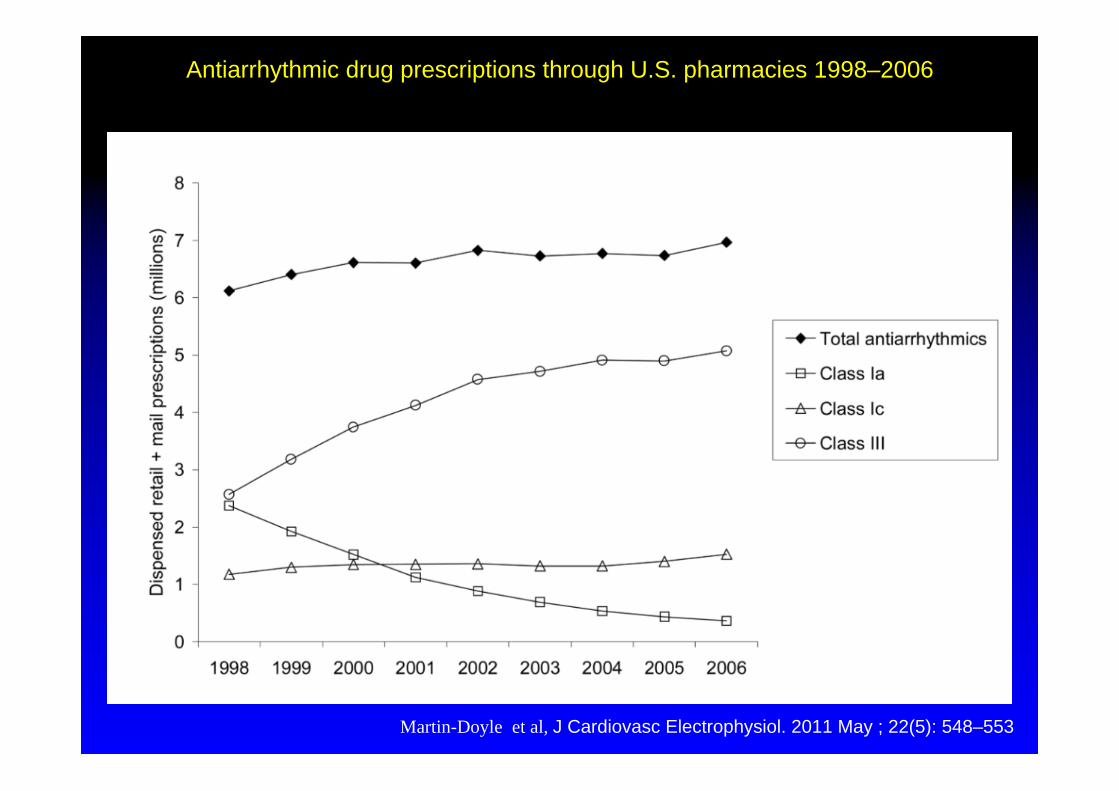
Antiarrhythmic drug prescriptions through U.S. pharmacies 1998–2006
Martin-Doyle et al, J Cardiovasc Electrophysiol. 2011 May ; 22(5): 548–553

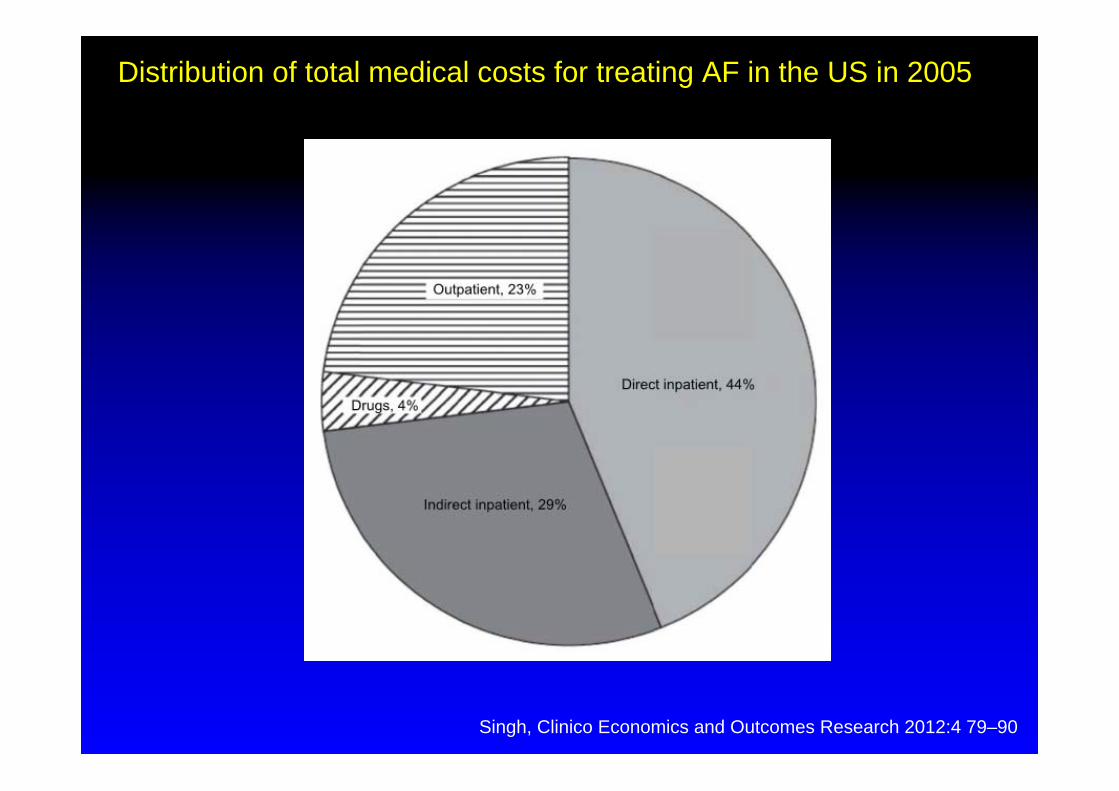
Distribution of total medical costs for treating AF in the US in 2005
Singh, Clinico Economics and Outcomes Research 2012:4 79–90

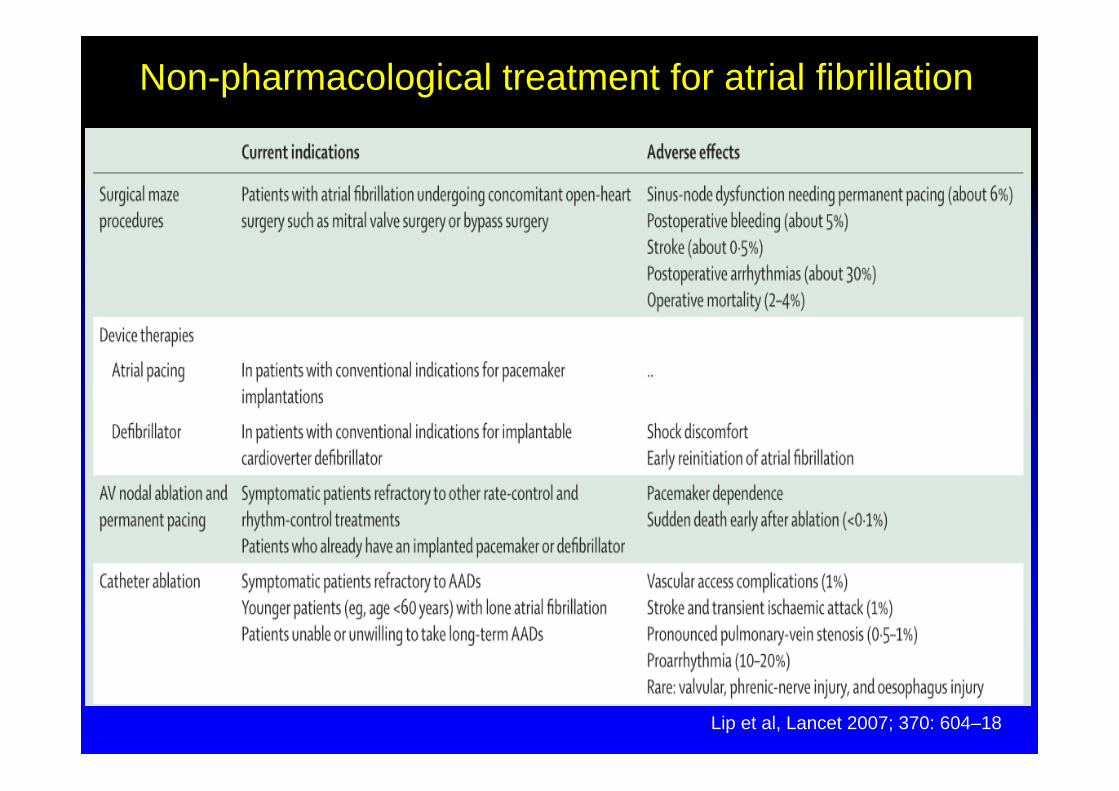
Non-pharmacological treatment for atrial fibrillation
Lip et al, Lancet 2007; 370: 604–18

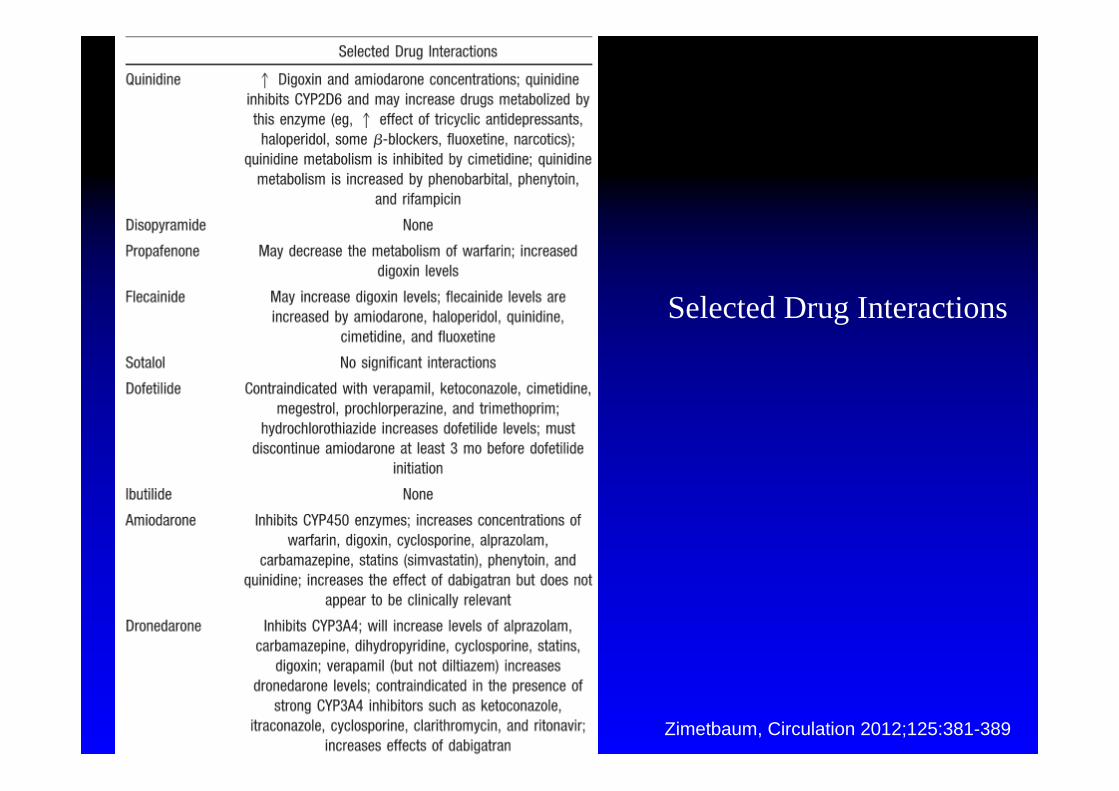
Selected Drug Interactions
Zimetbaum, Circulation 2012;125:381-389
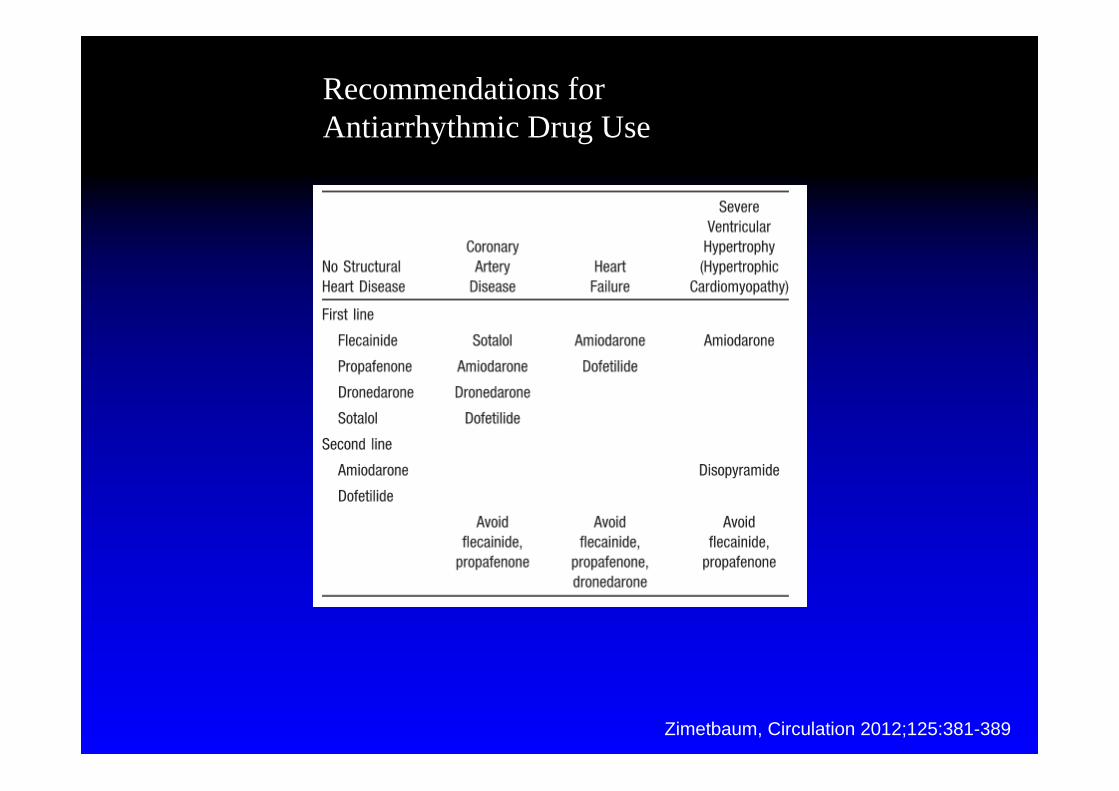
Recommendations for Antiarrhythmic Drug Use
Zimetbaum, Circulation 2012;125:381-389
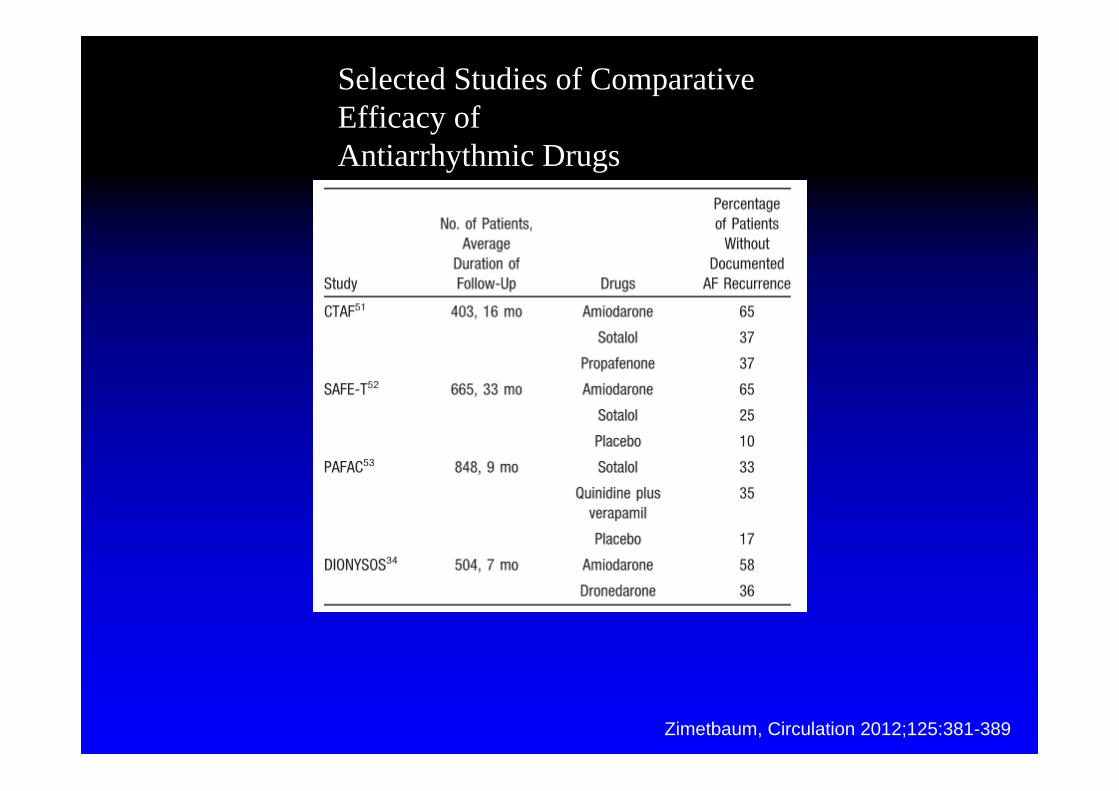
Selected Studies of Comparative Efficacy ofAntiarrhythmic Drugs
Zimetbaum, Circulation 2012;125:381-389


Haissaguerre et al, NEJM 1998

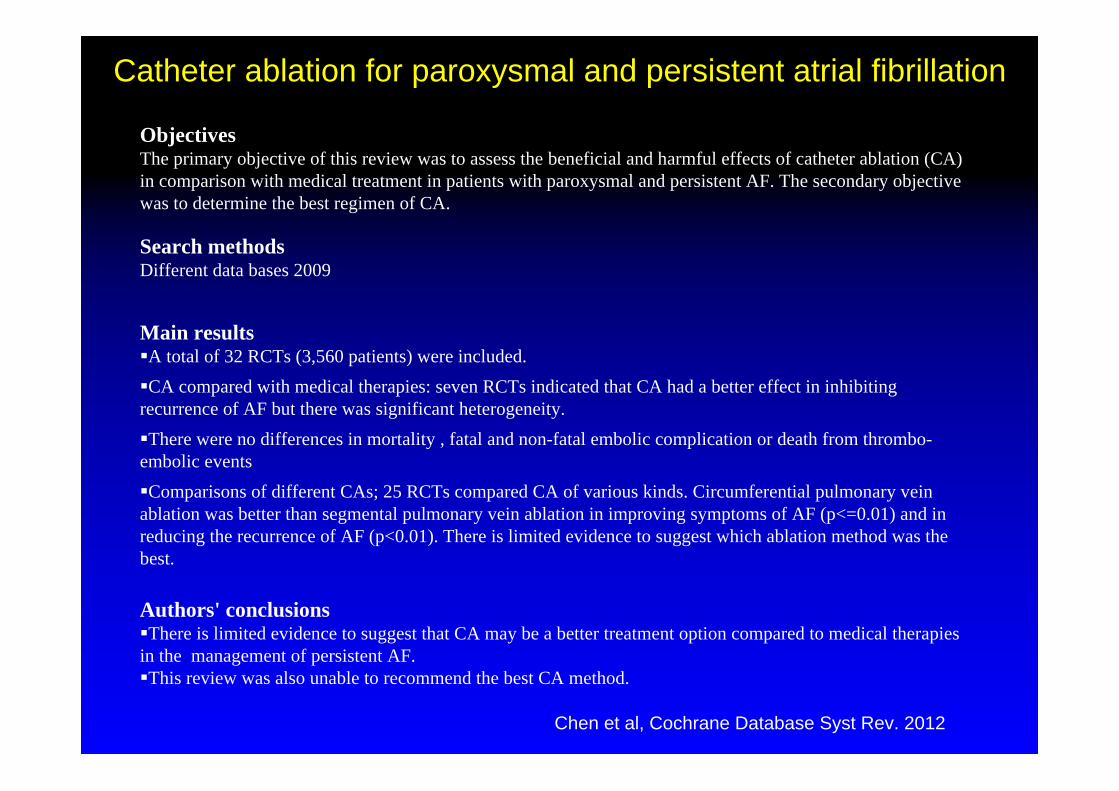
ObjectivesThe primary objective of this review was to assess the beneficial and harmful effects of catheter ablation (CA) in comparison with medical treatment in patients with paroxysmal and persistent AF. The secondary objective was to determine the best regimen of CA.
Search methodsDifferent data bases 2009
Main resultsA total of 32 RCTs (3,560 patients) were included. CA compared with medical therapies: seven RCTs indicated that CA had a better effect in inhibiting recurrence of AF but there was significant heterogeneity. There were no differences in mortality , fatal and non-fatal embolic complication or death from thrombo-embolic events Comparisons of different CAs; 25 RCTs compared CA of various kinds. Circumferential pulmonary vein ablation was better than segmental pulmonary vein ablation in improving symptoms of AF (p<=0.01) and in reducing the recurrence of AF (p<0.01). There is limited evidence to suggest which ablation method was the best.
Authors' conclusionsThere is limited evidence to suggest that CA may be a better treatment option compared to medical therapies in the management of persistent AF. This review was also unable to recommend the best CA method.
Chen et al, Cochrane Database Syst Rev. 2012
Catheter ablation for paroxysmal and persistent atrial fibrillation

Ranolazine
Antianginöse Wirkung
komplexe elektrophysiologische Effekte, einschließlich late Ina
Atriale Wirkung mit Anhebung der diastolischen Reizschwelle und Verlängerung der Postrepolarisationsrefraktärität
Verhinderung von Arrhythmien in vitro
MERLIN-TIMI 36: neues Auftreteten von AF um 30% reduziert
Keine kontrollierten Studien