Embed Size (px)
Citation preview

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2100
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
EFFICACY OF PERI-OPERATIVE ADMINISTRATION OF
PRUCALOPRIDE IN ASSESSING POST-OPERATIVE BOWEL
MOVEMENTS: A PROSPECTIVE COMPARATIVE STUDY
Shaik Bobby Parveen*1, Madamanchi Manjusha
1, P. Seetharamaiah
2, Dr. S. Uma
Shanker3, Athina Jahnavi
1 and Reddy Sucharitha
1
1Pharm D Intern, Hindu College of Pharmacy, Amaravathi Road, Guntur- 522002.
2Pharm D Director, Department of Pharmacy Practice Hindu college of Pharmacy,
Amaravathi Road, Guntur- 522002.
3General Surgeon and Laproscopic Surgeon, Lalitha Super Speciality Hospital, Guntur.
ABSTRACT
Aim: There is an extensive literature on the post operative bowel
movements after abdominal surgeries. There are, however, few studies
investigating the effect of prucalopride to treat post-operative
constipation. The aim of the study is to identify the effectiveness of
Peri-operative administration of prucalopride in assessing post-
operative bowel movements after hernia repair surgery. Materials and
Methods: The surgeon-blinded prospective randomized controlled
study included 50 hernia repair surgery patients between the ages of 18
and 80. The patients were randomized into two groups: those who had
prucalopride peri-operatively (n=25) and those who did not take
prucalopride peri-operatively (n=25). The outcome measures were post operative first bowel
movement, length of hospital stay, additional laxative need, adverse effects of the drug.
Results: Among 50 patients, 28 patients were males (56%), 22 patients were females (44%).
2mg and 1 mg dose of prucalopride were given to 25 patients and the remaining half are
taken without prucalopride. Out of 25 patients who Peri-operatively took prucalopride, 1
patient passed bowel on surgery day, 6 patients on day one after surgery and 18 patients on
the second day after surgery without any complications and got discharged early. Whereas
the 25 patients without prucalopride 2 patients passed bowel on day two after surgery, 5
patients on day three and 14 patients on day four, 4 patients on day five after surgery passed
the bowel experiencing the complications of constipation and had delayed discharge from the
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.632
Volume 10, Issue 7, 2100-2120 Research Article ISSN 2278 – 4357
*Corresponding Author
Dr. Shaik Bobby Parveen
Pharm D Intern, Hindu
College of Pharmacy,
Amaravathi Road, Guntur-
522002.
Article Received on
17 May 2021,
Revised on 07 June 2021,
Accepted on 27 June 2021,
DOI: 10.20959/wjpps20217-19440

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2101
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
hospital. Conclusions: The study suggests that peri-operative administration of prucalopride
in hernia repair surgeries or any other abdominal surgeries effectively reduces postoperative
gastrointestinal complications and shortens the recovery of bowel movements and length of
hospital stay.
KEYWORDS: Prucalopride, Bowel movements, Hernia repair surgery, Post –Operative
constipation , Abdominal surgery.
INTRODUCTION
A hernia is an outpouching of the parietal peritoneum through a preformed or secondarily
established hiatus.[1]
Hernia formation is a multifactorial process involving endogenous
factors including age, gender, anatomic variations, and inheritance and exogenous factors
such as smoking, comorbidity, and surgical factors.[2]
Hernias may include intra- and
retroperitoneal organs, either permanently or intermittently. Depending on the size of the
outpouching, there are 1) Complete (total) hernias and 2) Incomplete (partial) hernias. Based
on their formation, there are 1) Congenital (e.g., umbilical hernias and indirect inguinal
hernias, if the processus vaginalis is open) and 2) Acquired hernias (e.g., direct, femoral, and
incisional hernias).[1]
Several different types of open and laparoscopic hernia surgery are
available. The type of surgery your doctor recommends may depend on factors such as the
size of the hernia and age, health, and medical history.[3,4]
Generally Abdominal surgeries are performed to treat diseases of stomach, bile duct, liver,
spleen, pancreas, small intestine, and large intestine. Complications, which occur after
abdominal surgery are specific to gastrointestinal system as in preoperative period.[5,6]
The
major GI complications seen after abdominal surgeries are paralytic ileus, bowel injury,
alterations in gastrointestinal motility, gastric dilation, bowel Obstruction, postoperative
Fecal Impaction.[7]
Problems regarding bowel elimination are quite common in patients who
underwent abdominal surgery. It was reported that this ratio was 25% to 40% in hospitalized
patients who underwent surgery.[8,9]
Constipation is an important symptom affecting
postoperative healing, quality of life, comfort, respiratory and circulatory systems of the
patients, and quality of nursing care in the postoperative period.[5,8,10-12]
Place of surgical
intervention, type of anesthesia, trauma of intestines during the operation, duration of
postoperative immobility, suppression of defecation feeling, use of bedpan, inability to
protect privacy, inability of the patients to verbally express their discomfort, using
opioids/non opioid analgesics, fluid intake and alterations in dietary habits are effective in

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2102
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
bowel elimination in the early postoperative period.[10-14]
Several factors may contribute to
constipation after surgery. These include: Narcotic pain relievers such as opioids, General
anesthesia and spinal anesthesia, an inflammatory stimulus such as trauma or infection,
an electrolyte, fluid, or glucose imbalance, Prolonged inactivity, Changes to diet, especially
insufficient fiber.[15]
Gastrointestinal prokinetics promote or increase the co-ordination of the gut wall contractions
leading to enhancement of propulsive motility and, consequently, caudal displacement of
luminal contents.[16]
5-Hydroxytryptamine(4) (5-HT(4)) receptors are an interesting target for
the management of patients in need of gastrointestinal (GI) promotility treatment. They have
proven therapeutic potential to treat patients with GI motility disorders. Recent efforts have
led to the discovery of a series of selective 5-HT(4) receptor ligands, with prucalopride being
the most advanced in clinical development. The selectivity of these new compounds clearly
differentiates them from the older generation compounds by minimizing the potential of
target-unrelated side effects. Selective 5-HT(4) receptor agonists might thus prove to be
innovative drugs with an attractive safety profile for better treatment of patients suffering
from hypomotility disorders.[17]
The study was conducted in the tertiary center with the highest number of hernia repair
patients. The goal of this randomized controlled trial is to investigate whether preoperative
administration of prucalopride promotes the return of gastrointestinal activity in patients
undergoing abdominal surgeries.
MATERIALS AND METHODS
Arandomized controlled comparative study was conducted at lalitha superspeciality hospital.
The patients are randomized into 2 groups : with prucalopride and without prucalopride. All
enrolled subjects were informed about their participation in the study, written informed
consent was obtained and randomization was performed as soon as the patients were admitted
to our unit. A suitable data collection form along with a questionnaire form was designed for
the use in this study. Relavant data such as demographic details, disease history, diagnosis,
route, frequency, duration of therapy, adverse events will be collected and documented from
medical records and by the patient interview.
STUDY CRITERIA
Inclusion criteria

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2103
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
1) Patients of age group above 18 years and below 80 years are included in this study.
2) Patients who underwent abdominal surgery, majorly hernia (all types of hernia).
3) Patients with peritoneal carcinomatosis are also included.
4) Patients who are not having any laxatives in previous history (2 months).
5) Patients who are hospitalized for abdominal surgery.
Exclusion criteria
1) Patients of age group below 18 years and above 80 years of age.
2) Patient who had taken laxatives or any other drugs which increases GI motility from 2
months are excluded.
3) Patients who have suicidal ideation or depressed patients.
4) Patient with known cases of inflammatory conditions such as chron’s disease, ulcerative
colitis and toxic megacolon/megarectum.
5) Pregnant and lactating women.
6) Patients with Intestinal perforation or obstruction due to structural or functional disorder of
the gut wall, obstructive ileus.
7) Patients who are not willing to participate in this study.
8) Patients who are on calcium channel blockers and muscle relaxants
SOURCES OF DATA
All the relevant and necessary data will be collected from
1) Physical examination
2) Treatment charts
3) Interviewing the patient & patient care takers
4) Interviewing nurse, physician.
5) Any other relavent sources
The primary outcome measure of the study was first bowel movement (hours from end of
operation). Secondary outcome measures were the length of hospital stay, Patients were
evaluated three times a day by an outcome assessor who was blinded to the study allocation.
Patients bowel sounds were checked six times 2 a day postoperatively using a standard
stethoscope until the first bowel sounds were noticed. Patients were also instructed to notify
ward nurses or investigators immediately after the first passage of flatus, bowel movements,
defecation, and passing gas.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2104
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
All the raw data was collected, entered in EXCEL SHEET 2007 in windows 10 version, the
statistical analysis was done in SPSS 16.0 software by an appropriate statistical methods
independent T test for knowing the significant p-value <0.005 (confidence interval 95%).
RESULTS
The randomized controlled trial study was conducted with 50 patients. None of the patients
left the sample during the study. Flowchart of the study is demonstrated in
Tables 5.1 Age distribution of patients from the study.
Based on age, patients are grouped as following.
AGE NUMBER OF PATIENTS PERCENTAGE
18-30 YEARS 4 8%
31-42 YEARS 13 26%
43-54 YEARS 19 38%
55-66 YEARS 11 22%
67-80 YEARS 3 6%
Age of patients observed as follows, 8% of patients were between 18-30 years of age,
followed by 26% of patients were between 31-42 years years of age, 38% were between
43-54 years of age, 22% patients were between 55-66 years and 6% of patients were
between 67-80 years of age group.
Figure 5.1: Age distribution of patients from the study.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2105
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
Table 5.2 Gender Differentiation.
GENDER NO.OF PATIENTS PERCENTAGE
Male 28 56%
Female 22 44%
Table 5.2 shows the patient charecterstics based on gender.
Out of 50 patients 28 patients were males (56%), 22 pateints were females (44%). It may
infer that men might me more at risk of developing hernia compared to females.
Figure 5.2 Gender Differntiation of patients in the study.
Table 5.3 Comorbidities.
COMORBIDITIS NUMBER OF PATIENTS PERCENTAGE
Hypertension 13 26%
Diabetes mellitus 7 14%
Hypothyroidism 3 6%
Cardiac problems 6 12%
Table 5.3 shows the patient charecterstics with co-morbiditis.
26% of patients were reported with hypertension, 14% of patients were reported with
diabetes millites, 6% of patients with hypothyroidism and 12% of patients were reported
with cardiac problems.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2106
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure 5.3 Comorbiditis of patients in the study.
Table 5.4 Body Mass Index (BMI)
BODY MASS INDEX NO.OF PATIENTS PERCENTAGE
Normal 25 50 %
Over weight 14 28%
Obese 11 22%
Table 5.4 shows the patients BMI (BODY MASS INDEX).
In this 50% of patients (25 patients) were normal in weight, 28% of patients (14 patients)
were over weight and 22% of patients (11 patients) were obese in our study.
Figure 5.4 Body Mass Index (BMI).
www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2107
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
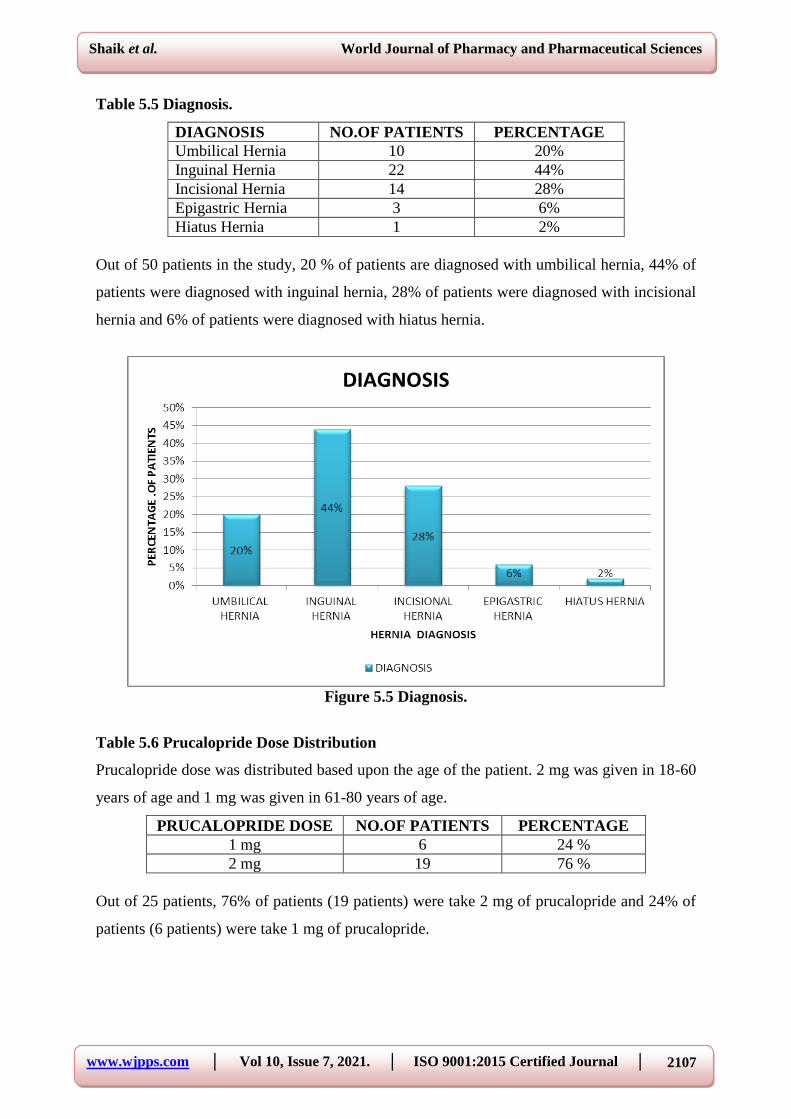
Table 5.5 Diagnosis.
DIAGNOSIS NO.OF PATIENTS PERCENTAGE
Umbilical Hernia 10 20%
Inguinal Hernia 22 44%
Incisional Hernia 14 28%
Epigastric Hernia 3 6%
Hiatus Hernia 1 2%
Out of 50 patients in the study, 20 % of patients are diagnosed with umbilical hernia, 44% of
patients were diagnosed with inguinal hernia, 28% of patients were diagnosed with incisional
hernia and 6% of patients were diagnosed with hiatus hernia.
Figure 5.5 Diagnosis.
Table 5.6 Prucalopride Dose Distribution
Prucalopride dose was distributed based upon the age of the patient. 2 mg was given in 18-60
years of age and 1 mg was given in 61-80 years of age.
PRUCALOPRIDE DOSE NO.OF PATIENTS PERCENTAGE
1 mg 6 24 %
2 mg 19 76 %
Out of 25 patients, 76% of patients (19 patients) were take 2 mg of prucalopride and 24% of
patients (6 patients) were take 1 mg of prucalopride.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2108
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure 5.6 Prucalopride Dose Distribution.
Table 5.7 Surgery Procedure.
SURGERY PROCEDURE NO.OF PATIENTS PERCENTAGE
Open 12 24 %
Laproscopic 38 76 %
Out of 50 patients, open surgery was done in 24% of patients (12 patients) and laproscopic
surgery was done in 76% of patients (38 patients).
Figure 5.7 Surgery Procedure.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2109
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
Table 5.8 Type of Anesthesia Given in the Patient.
TYPE OF ANAESTHESIA NO.OF PATIENTS PERCENTAGE
General 14 28 %
spinal 36 72 %
Out of 50 patients, general anesthesia was given in 28% of patients (14 patients) and spinal
anesthesia was given in 72% of patients (36 patients).
Figure 5.8 Type of Anesthesia Given in the Patient.
Table 5.9 Type of Analgesic Given in the Patient.
TYPE OF ANALGESIC NO.OF PATIENTS PERCENTAGE
Opioid 32 64 %
Non opioid 18 36 %
Out of 50 patients, 64% of patients (32 patients) were take opioid analgesic and 36% of
patients (18 patients) were take non opioid analgesic.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2110
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure 5.9 Type of Analgesic Given in the Patient.
Table 5.10 Adverse Effects Were Occurred in the Patients Taking Prucalopride.
ADVERSE EFFECTS NO.OF PATIENTS PERCENTAGE
Diarrhoea 2 8%
Head ache 1 4%
Out of 25 patients, 2 patients were experienced diarrhoea and 1 patient was experienced head
ache.
Figure 5.10 Adverse Effects were Occurred in the Patients Taking Prucalopride.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2111
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
Table 5.11 Post Operative Mobilisation of The Patient.
POST OPERATIVE
MOBILISATION NO.OF PATIENTS PERCENTAGE
Active 31 62%
Sedentary 19 38%
Out of 50 patients, 62% of the patients (31 patients) were active and 38% of the patients (19
patiens) were sedentary.
Figure 5.11 Post Operative Mobilisation of The Patient.
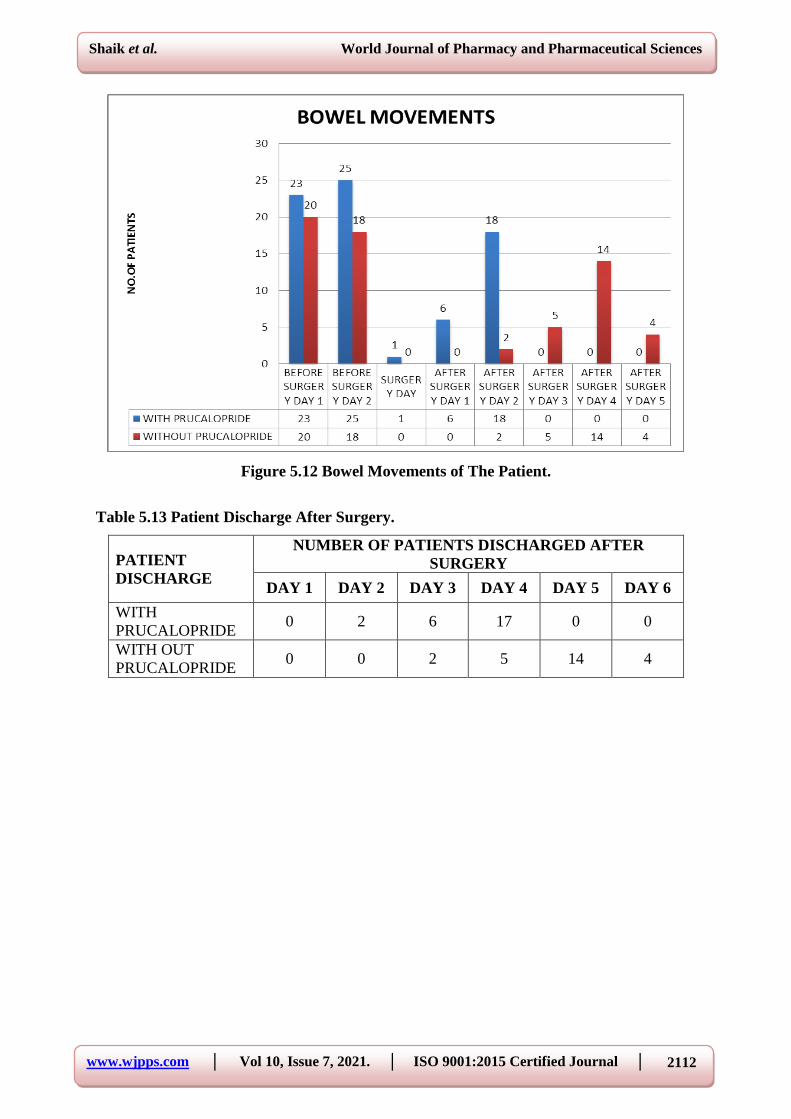
Table 5.12 Bowel Movements of The Patient.
BOWEL
MOVEMENTS OF
THE PATIENT
NUMBER OF PATIENTS
BEFORE
SURGERY SURGERY
DAY
AFTER SURGERY
DAY 1 DAY 2 DAY 1 DAY 2 DAY 3 DAY 4 DAY 5
WITH
PRUCALOPRIDE 23 25 1 6 18 0 0 0
WITH OUT
PRUCALOPRIDE 20 18 0 0 2 5 14 4
www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2112
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure 5.12 Bowel Movements of The Patient.
Table 5.13 Patient Discharge After Surgery.
PATIENT
DISCHARGE
NUMBER OF PATIENTS DISCHARGED AFTER
SURGERY
DAY 1 DAY 2 DAY 3 DAY 4 DAY 5 DAY 6
WITH
PRUCALOPRIDE 0 2 6 17 0 0
WITH OUT
PRUCALOPRIDE 0 0 2 5 14 4

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2113
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure 5.13 Patient Discharge After Surgery.
Table 5.14 Patient Recovery with Prucalopride.
PATIENT RECOVERY
WITH PRUCALOPRIDE NO.OF PATIENTS
Early 23
Delayed 2
Out of 25 patients, recovery of 23 patients were early and recovery of 2 patients were
delayed.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2114
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure 5.14 Patient Recovery with Prucalopride.
Table 5.15 Patient Recovery with Out Prucalopride.
PATIENT RECOVERY WITH
OUT PRUCALOPRIDE NO.OF PATIENTS
Early 3
Delayed 22
Out of 25 patients, recovery of 3 patients were early and recovery of 22 patients were
delayed.
Figure 5.15 Patient Recovery with Out Prucalopride.
www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2115
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
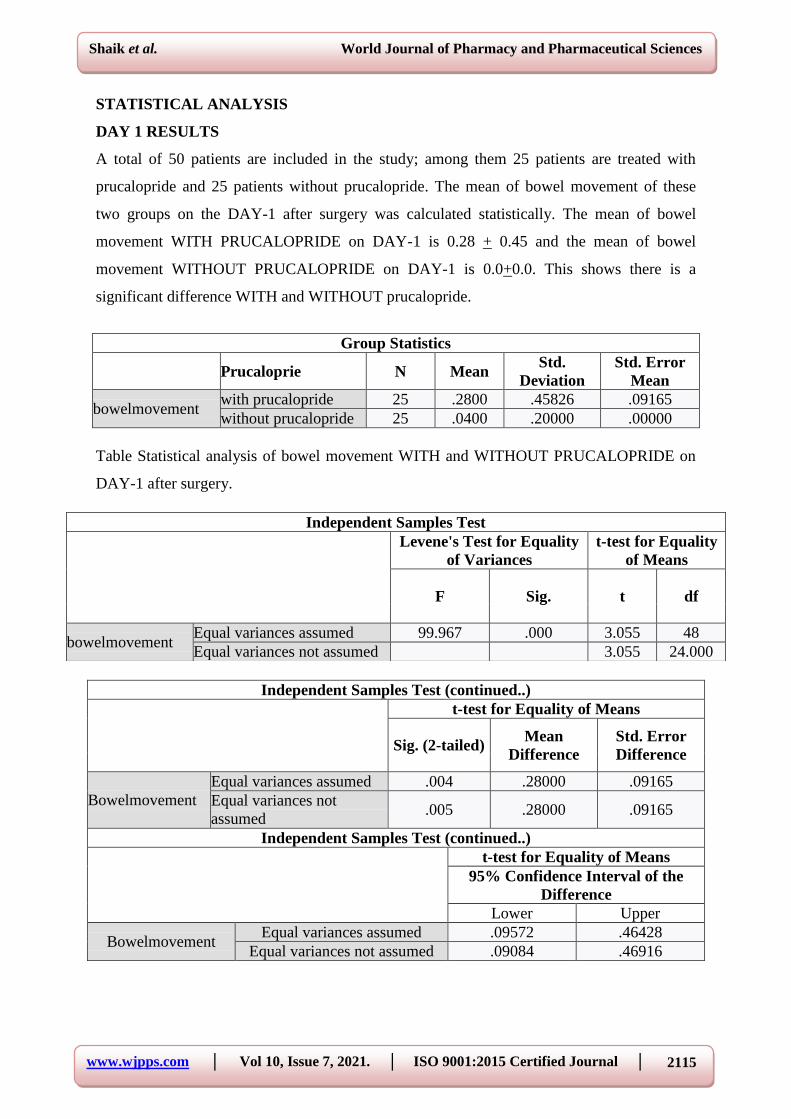
STATISTICAL ANALYSIS
DAY 1 RESULTS
A total of 50 patients are included in the study; among them 25 patients are treated with
prucalopride and 25 patients without prucalopride. The mean of bowel movement of these
two groups on the DAY-1 after surgery was calculated statistically. The mean of bowel
movement WITH PRUCALOPRIDE on DAY-1 is 0.28 + 0.45 and the mean of bowel
movement WITHOUT PRUCALOPRIDE on DAY-1 is 0.0+0.0. This shows there is a
significant difference WITH and WITHOUT prucalopride.
Group Statistics
Prucaloprie N Mean Std.
Deviation
Std. Error
Mean
bowelmovement with prucalopride 25 .2800 .45826 .09165
without prucalopride 25 .0400 .20000 .00000
Table Statistical analysis of bowel movement WITH and WITHOUT PRUCALOPRIDE on
DAY-1 after surgery.
Independent Samples Test (continued..)
t-test for Equality of Means
Sig. (2-tailed) Mean
Difference Std. Error
Difference
Bowelmovement
Equal variances assumed .004 .28000 .09165
Equal variances not
assumed .005 .28000 .09165
Independent Samples Test (continued..)
t-test for Equality of Means
95% Confidence Interval of the
Difference
Lower Upper
Bowelmovement Equal variances assumed .09572 .46428
Equal variances not assumed .09084 .46916
Independent Samples Test
Levene's Test for Equality
of Variances
t-test for Equality
of Means
F Sig. t df
bowelmovement Equal variances assumed 99.967 .000 3.055 48
Equal variances not assumed 3.055 24.000

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2116
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
STATISTICAL ANALYSIS
DAY 2 RESULTS
A total of 50 patients are included in the study; among them 25 patients are treated with
prucalopride and 25 patients without prucalopride. The mean of bowel movement of these
two groups on the DAY-2 after surgery was calculated statistically. The mean of bowel
movement WITH PRUCALOPRIDE on DAY-2 is 0.72+0.45 and the mean of bowel
movement WITHOUT PRUCALOPRIDE on DAY-2 is 0.08+0.27. This shows there is a
significant difference WITH and WITHOUT prucalopride.
Group Statistics
prucalopride N Mean Std.
Deviation
Std. Error
Mean
bowelmovement with prucalopride 25 .7200 .45826 .09165
without prucalopride 25 .0800 .27689 .05538
Independent Samples Test
Levene's Test for Equality
of Variances
t-test for Equality of
Means
F Sig. t df
bowelmovement
Equal variances assumed 17.291 .000 5.977 48
Equal variances not
assumed 5.977 39.463
Independent Samples Test (continued..)
t-test for Equality of Means
Sig. (2-tailed) Mean
Difference
Std. Error
Difference
bowelmovement
Equal variances assumed .000 .64000 .10708
Equal variances not
assumed .000 .64000 .10708
Independent Samples Test (continued..)
t-test for Equality of Means
95% Confidence Interval of the
Difference
Lower Upper
Bowelmovement Equal variances assumed .42470 .85530
Equal variances not assumed .42349 .85651
When the coefficient of variation was calculated betweenthe WITH PRUCALOPRIDE
and WITHOUT PRUCALOPRIDE, the CV of WITHPRUCALOPRIDE is less than
CV of WITHOUT PRUCALOPRIDE.
So, WITH PRUCALOPRIDE is efficient than WITHOUT PRUCALOPRIDE

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2117
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
DISCUSSION
This study is to determine the effectiveness of prucalopride in assessing post operative bowel
movements after abdominal surgeries majorly hernia surgeries. The prevalence of hernia
disease was greater in male subjects than in female subjects that are 56% in Males and 44%
in Females. The prevalence of hernia disease was greater in male subjects than in female
subjects that are 56% in Males and 44% in Females. In the taken sample 26% patients are
hyper tensive, 14% of the patients are diabetic, 12% of the patients have cardiac problems
and 6% have hypothyroidism. Based on the diagnosis most of the subjects i.e; 44% were
diagnosed with inguinal hernia, 28% with incisional hernia, 20% of patients with umbilical
hernia, 6% of patient’s with epigastric hernia and 2% of patients with hiatus hernia. In our
study of 50 subjects, 25 subjects were prescribed with prucalopride. We used two doses of
Prucalopride. They are 2mg, 1mg. where as 2 Mg was prescribed to patients of age group
between 18-60 years where as 1 mg of prucalopride was prescribed to patients of age group
between 60 -80 years. Out of these 25 subjects 2mg was prescribed in more patients i.e, 76%
(19 patients) where as 1 mg was prescribed to 24% (6 patients). We observed that both doses
2mg and 1 mg of prucalopride are efficient and showed significant improvement in the bowel
movement in almost all the patients prescribed. In our study we mainly concentrated on the
improvement of bowel movements in patients after hernia surgeries by monitoring the bowel
movements of patients day wise. According to our study results 18 patients out of 25 patients
prescribed with prucalopride passed bowel after the second day of the surgery, where as 6
patients out of 25 patients passed bowel after the day of the surgery and 1 patient out of 25
patient passed bowel on the surgery day itself without experiencing any difficulties or
complications. In this study the patients without prucalopride the patients suffered from post
operative constipation where as the 4 subjects out of 25 passed bowel on the fifth day after
surgery, the highest number of 14 subjects out of 25 passed bowel on the fouth day after
surgery, 5 subjects out of 25 on day 3 and 2 subjects out of 25 on day 2. The patients who
passed the bowel mainly on the day 4 and day 5 after surgery experienced problems of
constipation like hard stools, straining, pain while passing bowel secondary to straining,
excessive time needed to pass the bowel and sensation of incomplete bowel evacuation after
passing bowel. According to the prospective randomized trail conducted by Eur J Surg, on
how the enemas given before abdominal surgeries are useful to patients they came to a
conclusion that preoperative enemas delay rather than improve the return of normal
peristalsis after surgery. Instead the study has also recommend this practice should be

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2118
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
abandoned. Now a days as the usage of enemas before abdominal surgeries are adandoned by
the surgeons, the newly approved selective serotonin agonist drug prucalopride has been
choosen for this study to know its efficacy and safety on post operative bowel movement
when given peri operatively to the selected subjects. In this study the effect of factors such as
general anesthesia, surgery procedure and analgesic usage is also considered as these factors
also majorly causes post operative constipation. General anesthesia is found to be one of the
factor for post operative constipation, and here in our study out of 50 subjects, spinal
anesthesia was given to the 28% of the subjects general anesthesia was given to 72% of
subjects. Out of these 72% of the subjects of general anesthesia, 36% are with prucalopride
who passed the bowel within the second day and remaining 36% of subjects took upto 5 days
after surgery to eliminate the bowel. In our study of total 50 subjects, the opiod analgesic
tramadol was prescribed to to a total of 32 subjects i,e 64% of the subjects where as to the 18
subjects the non opiod analgesic diclofenac was prescribed. Out of these 64% of subjects
with opiod analgesic the subjects to whom prucalopride is prescribed is 36 % and all these
36% subjects passed bowel within the second day after surgery without any complication
where as the remaining 28% of the subjects without prucalopride eliminated bowel mostly on
the day 4 after surgery experiencing difficulty in bowel elimination. In this study the effect of
factors such as general anesthesia, surgery procedure and analgesic usage is also considered
as these factors also majorly causes post operative constipation. General anesthesia is found
to be one of the factor for post operative constipation, and here in our study out of 50
subjects, spinal anesthesia was given to the 28% of the subjects general anesthesia was given
to 72% of subjects. Out of these 72% of the subjects of general anesthesia, 36% are with
prucalopride who passed the bowel within the second day and remaining 36% of subjects
took upto 5 days after surgery to eliminate the bowel. In our study of total 50 subjects, the
opiod analgesic tramadol was prescribed to to a total of 32 subjects i,e 64% of the subjects
where as to the 18 subjects the non opiod analgesic diclofenac was prescribed. Out of these
64% of subjects with opiod analgesic the subjects to whom prucalopride is prescribed is 36%
and all these 36% subjects passed bowel within the second day after surgery without any
complication where as the remaining 28% of the subjects without prucalopride eliminated
bowel mostly on the day 4 after surgery experiencing difficulty in bowel elimination. In our
study, 50 out of 48 subjects with prucalopride got dischared on the third day after surgery
where as out of the 50 subjects without prucalopride most of the subjects got discharged on
the sixth day after surgery. That means with the help of our study we had reduced the extra 3
day hospital stay and their medical expenses to the subjects with prucalopride.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2119
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
CONCLUSION
In this study with the help of the drug prucalopride we minimized many complications
occuring due to post operative constipation after surgery. we not only increased patients
quality of life but also economically decreased patients burden by decreasing the hospital stay
of the patients. As the patients with prucalopride recovered and got discharged early
compared to the patients without prucalopride.
REFERENCES
1. Schumpelick V, Zimmer M (eds) (1990) Atlas of hernia surgery. Decker, New York.
2. Jansen PL, Mertens PP, Klinge U, Schumpelick V. The biology of hernia formation.
Surgery, 2004; 136(1): 1–4. Doi:10.1016/j. surg.2004.01.004.
3. The Hernia Surge Group. International guidelines for groin hernia management. Hernia,
2018; 22: 1–165.
4. Fitzgibbons RJ, Ramanan B, Arya S, et al. Long-term results of a randomized controlled
trial of a nonoperative strategy (watchful waiting) for men with minimally symptomatic
inguinal hernias. Annals of Surgery, 258(3): 508–515.
5. Asdemir N, Celik SS. Hastaların cerrahi girişim sonrası abdominal distansiyona yönelik
deneyimleri. Ege Univ Sch Nurs J., 2010; 26(3): 23–31. [Google Scholar]
6. Uysal N, Khorshid L, Eser I. healthy young bireylerde konstipasyon sorununun
belirlenmesi. TAF Prev Med Bull, 2010; 9(2): 127–32. [Google Scholar]
7. Current diagnosis and treatment surgery by Lange.
8. Sendir M, Buyukiylmaz F, Asti T, Gurpinar S, Yazgan I. Postoperative constipation risk
assessment in Turkish orthopedic patients. Gastroenterol Nurs., 2012; 35(2): 106–13. doi:
10.1097/SGA.0b013e31824d2945. [PubMed] [CrossRef] [Google Scholar].
9. Lee JL, Yang SS, Park IJ, Yu CS, Kim JC. Comparison of abdominal and perineal
procedures for complete rectal prolapse: an analysis of 104 patients. Ann Surg Treat Res.,
2014; 86(5): 249–55. doi: 10.4174/astr.2014.86.5.249. [PMC free article] [PubMed]
[CrossRef] [Google Scholar]
10. Ayaz S, Hisar F. The efficacy of education programme for preventing constipation in
women. Int J Nurs Pract., 2014; 20(3): 275–82. doi: 10.1111/ijn.12144. [PubMed]
[CrossRef] [Google Scholar].
11. Rasmussen LS, Pedersen PU. Constipation and defecation pattern the first 30 days after
thoracic surgery. Scand J Caring Sci., 2010; 24(2): 244–50. doi: 10.1111/j.1471-
6712.2009.00713.x. [PubMed] [CrossRef] [Google Scholar].

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
2120
Shaik et al. World Journal of Pharmacy and Pharmaceutical Sciences
12. Miaskowski C. A review of the incidence, causes, consequences, and management of
gastrointestinal effects associated with postoperative opioid administration. J Perianesth
Nurs., 2009; 24(4): 222–8. doi: 10.1016/j.jopan.2009.05.095. [PubMed] [CrossRef]
[Google Scholar].
13. Koo HY, Park KJ, Oh JH, Kang SB, Oh ST, Lee WY. Investigation of clinical
manifestations in korean colorectal cancer patients. Ann Coloproctol, 2013; 29(4):
139–43. doi: 10.3393/ac.2013.29.4.139. [PMC free article] [PubMed] [CrossRef] [Google
Scholar].
14. Richmond JP, Wright ME. Establishing reliability and validity of a constipation risk
assessment scale. Journal of Orthop Nurs., 2008; 12(3-4): 139–50. doi:
10.1016/j.joon.2008.10.003. [CrossRef] [Google Scholar].
15. Medically reviewed by Debra Sullivan, Ph.D., MSN, R.N., CNE, COI on April 26, 2020
New — Written by Annette McDermot.
16. Tonini M. Recent advances in the pharmacology of gastrointestinal prokinetics.
Pharmacol Res., 1996 Apr-May; 33(4-5): 217-26.
17. De Maeyer JH, Lefebvre RA, Schuurkes JA. 5-HT4 receptor agonists: similar but not the
same. Neurogastroenterol Motil, 2008 Feb; 20(2): 99-112. doi:10.1111/j.1365-
2982.2007.01059.x.





























