Embed Size (px)
Citation preview
Neue Möglichkeiten bei Hypertonie und Herzinsuffizienz
Joachim Beige
Klinikum St. Georg (Abt. Nephrologie / KfH Nierenzentrum)Leipzig
www.sanktgeorg.de/nephro.html
Lopez et al. Lancet 2006;367:1747-57
Global and regional burden of disease and risk
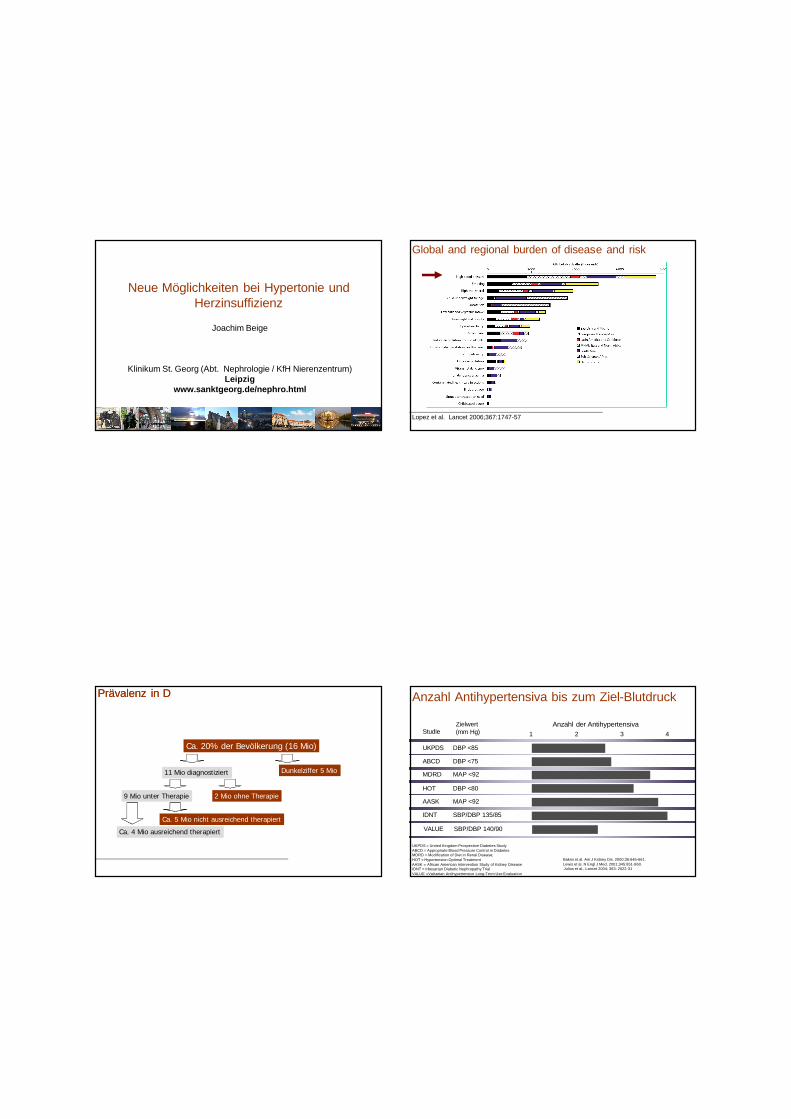
Prävalenz in DPrävalenz in D
Ca. 20% der Bevölkerung (16 Mio)
11 Mio diagnostiziert Dunkelziffer 5 Mio
9 Mio unter Therapie 2 Mio ohne Therapie
Ca. 4 Mio ausreichend therapiert
Ca. 5 Mio nicht ausreichend therapiert
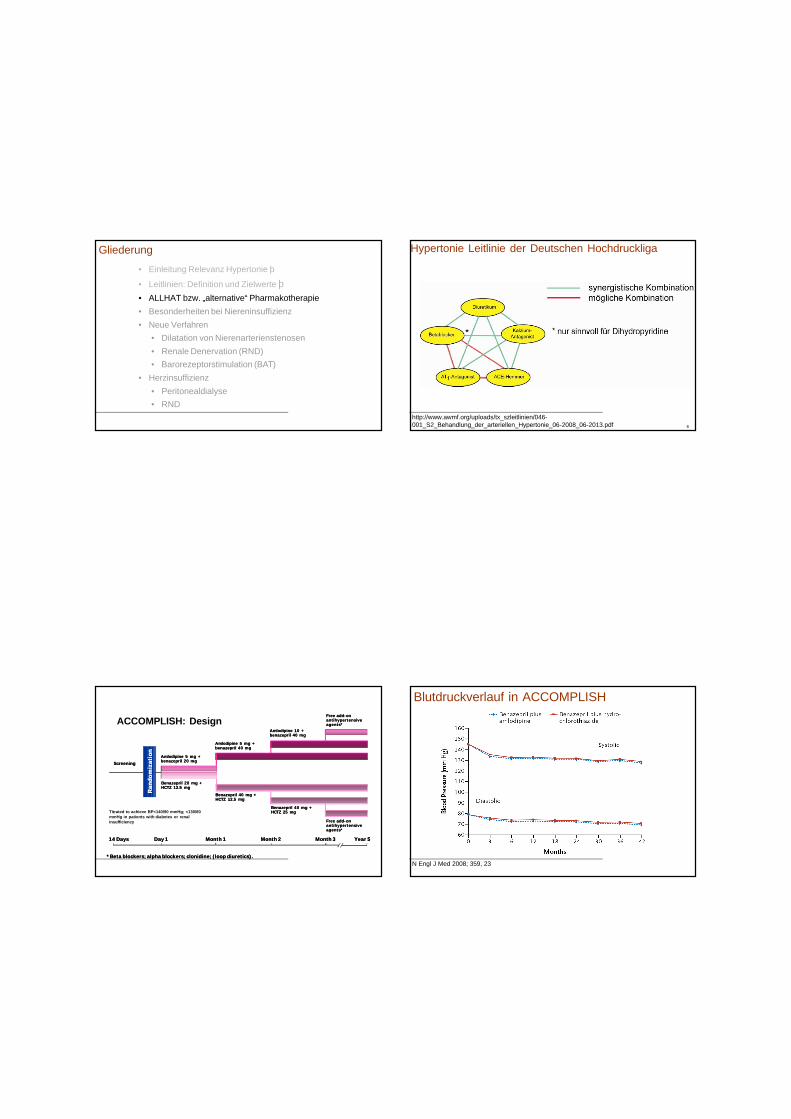
UKPDS = United Kingdom Prospective Diabetes StudyABCD = Appropriate Blood Pressure Control in DiabetesMDRD = Modification of Diet in Renal Disease; HOT = Hypertension Optimal TreatmentAASK = African American Intervention Study of Kidney DiseaseIDNT = Irbesartan Diabetic Nephropathy TrialVALUE =Valsartan Antihypertensive Long-Term Use Evaluation
AASK MAP <92
Zielwert(mm Hg)
Anzahl der Antihypertensiva1
UKPDS DBP <85
ABCD DBP <75
MDRD MAP <92
HOT DBP <80
Studie 2 3 4
IDNT SBP/DBP 135/85
VALUE SBP/DBP 140/90
Bakris et al. Am J Kidney Dis. 2000;36:646-661. Lewis et al. N Engl J Med. 2001;345:851-860.Julius et al., Lancet 2004; 363: 2022-31
Anzahl Antihypertensiva bis zum Ziel-Blutdruck
• Einleitung Relevanz Hypertonie þ
• Leitlinien: Definition und Zielwerte þ• ALLHAT bzw. „alternative“ Pharmakotherapie• Besonderheiten bei Niereninsuffizienz• Neue Verfahren
• Dilatation von Nierenarterienstenosen• Renale Denervation (RND)• Barorezeptorstimulation (BAT)
• Herzinsuffizienz• Peritonealdialyse• RND
Gliederung
http://www.awmf.org/uploads/tx_szleitlinien/046-001_S2_Behandlung_der_arteriellen_Hypertonie_06-2008_06-2013.pdf 6
Hypertonie Leitlinie der Deutschen Hochdruckliga
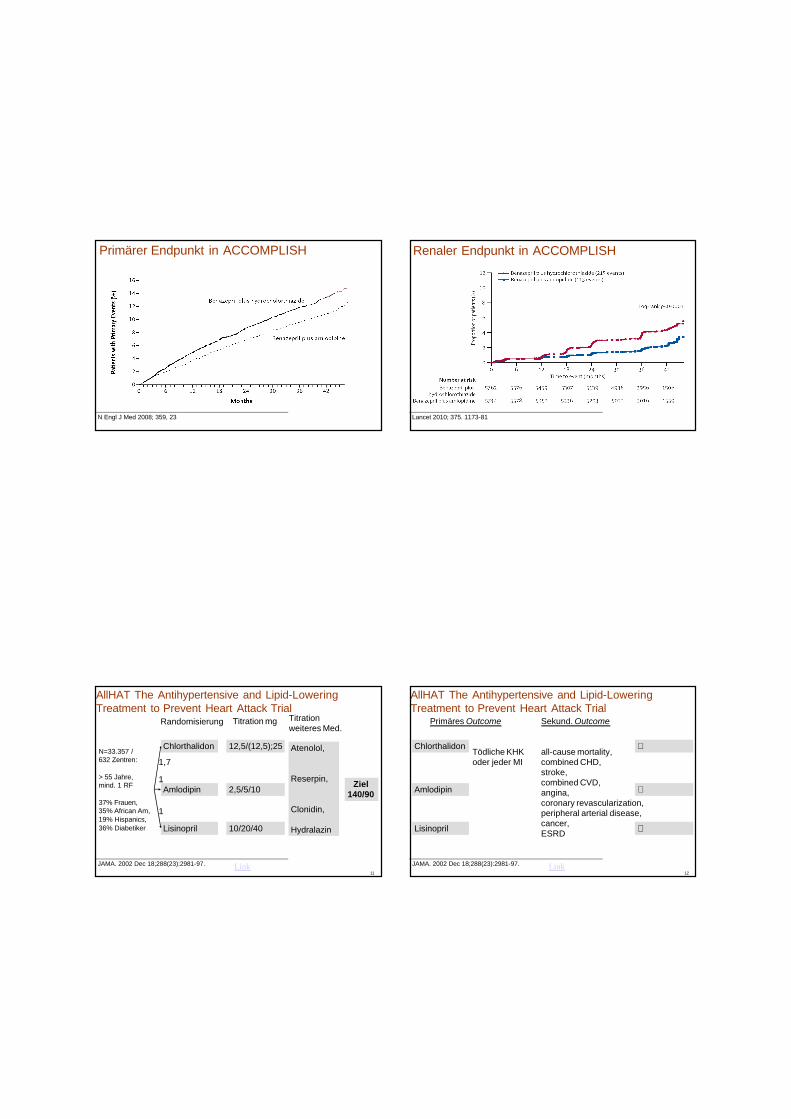
*Beta blockers; alpha blockers; clonidine; (loop diuretics).*Beta blockers; alpha blockers; clonidine; (loop diuretics).
14 Days14 Days Day 1Day 1 Month 1Month 1 Month 2Month 2 Year 5Year 5
ScreeningScreeningAmlodipine 5 mg +Amlodipine 5 mg +benazepril 20 mgbenazepril 20 mg
Ran
dom
izat
ion
Ran
dom
izat
ion
Benazepril 40 mg + Benazepril 40 mg + HCTZ 12.5 mgHCTZ 12.5 mg
Benazepril 40 mg + Benazepril 40 mg + HCTZ 25 mgHCTZ 25 mg
Free addFree add--on on antihypertensive antihypertensive agents*agents*
Month 3Month 3
Free addFree add--on on antihypertensive antihypertensive agents*agents*
Amlodipine 5 mg +Amlodipine 5 mg +benazepril 40 mgbenazepril 40 mg
Amlodipine 10 +Amlodipine 10 +benazepril 40 mgbenazepril 40 mg
Benazepril 20 mg + Benazepril 20 mg + HCTZ 12.5 mgHCTZ 12.5 mg
Titrated to achieve BP<140/90 mmHg; <130/80 mmHg in patients with diabetes or renal insufficiency
ACCOMPLISH: Design
N Engl J Med 2008; 359, 23
Blutdruckverlauf in ACCOMPLISH
N Engl J Med 2008; 359, 23
Primärer Endpunkt in ACCOMPLISH
Lancet 2010; 375. 1173-81
Renaler Endpunkt in ACCOMPLISH
JAMA. 2002 Dec 18;288(23):2981-97.11
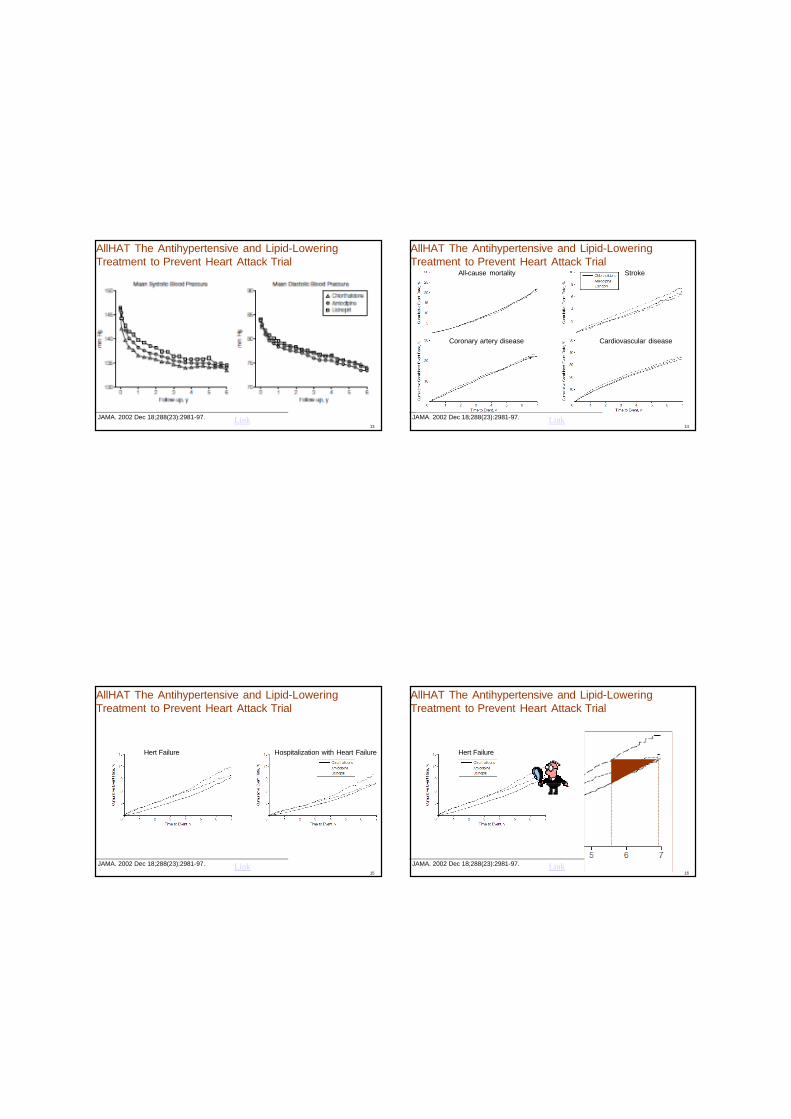
AllHAT The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial
N=33.357 /632 Zentren:
> 55 Jahre,mind. 1 RF
37% Frauen,35% African Am,19% Hispanics,36% Diabetiker
Chlorthalidon
Amlodipin
Lisinopril
1,7
1
1
Ziel140/90
Link
12,5/(12,5);25
2,5/5/10
10/20/40
Titration mg Titrationweiteres Med.
Atenolol,
Reserpin,
Clonidin,
Hydralazin
Randomisierung
JAMA. 2002 Dec 18;288(23):2981-97.12
AllHAT The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial
Chlorthalidon
Amlodipin
Lisinopril
Link
∅
∅
∅
Primäres Outcome
Tödliche KHKoder jeder MI
Sekund. Outcome
all-cause mortality, combined CHD,stroke,combined CVD,angina,coronary revascularization, peripheral arterial disease,cancer,ESRD
JAMA. 2002 Dec 18;288(23):2981-97.13
AllHAT The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial
Link JAMA. 2002 Dec 18;288(23):2981-97.14
AllHAT The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial
Link
All-cause mortality Stroke
Coronary artery disease Cardiovascular disease
JAMA. 2002 Dec 18;288(23):2981-97.15
AllHAT The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial
Link
Hert Failure Hospitalization with Heart Failure
JAMA. 2002 Dec 18;288(23):2981-97.16
AllHAT The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial
Link
Hert Failure
30 (60) mg Minoxidil25 mg Aldactone25 mg HCT300 mg Aliskiren320 mg Candesartan20 mg Amlodipin95 mg Metoprolol8 mg Doxazosin
50 mg Citalopram
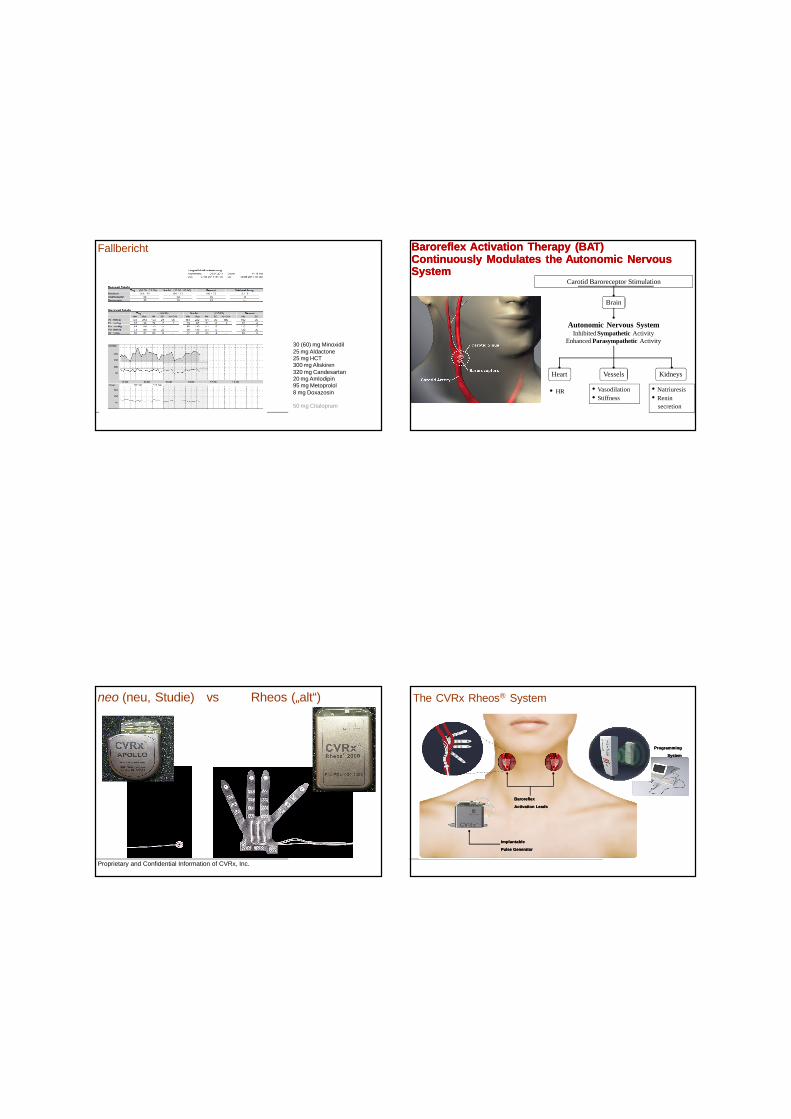
Fallbericht Baroreflex Activation Therapy (BAT) Continuously Modulates the Autonomic Nervous System
Baroreflex Activation Therapy (BAT) Continuously Modulates the Autonomic Nervous System
Kidneys
• HR • Vasodilation• Stiffness
• Natriuresis• Renin
secretion
Carotid Baroreceptor Stimulation
Heart Vessels
Brain
Autonomic Nervous SystemInhibited Sympathetic Activity
Enhanced Parasympathetic Activity
Proprietary and Confidential Information of CVRx, Inc.
neo (neu, Studie) vs Rheos („alt“) The CVRx Rheos® System
Implantable
Pulse Generator
Implantable
Pulse Generator
Baroreflex
Activation Leads
Baroreflex
Activation Leads
Programming
System
Programming
System
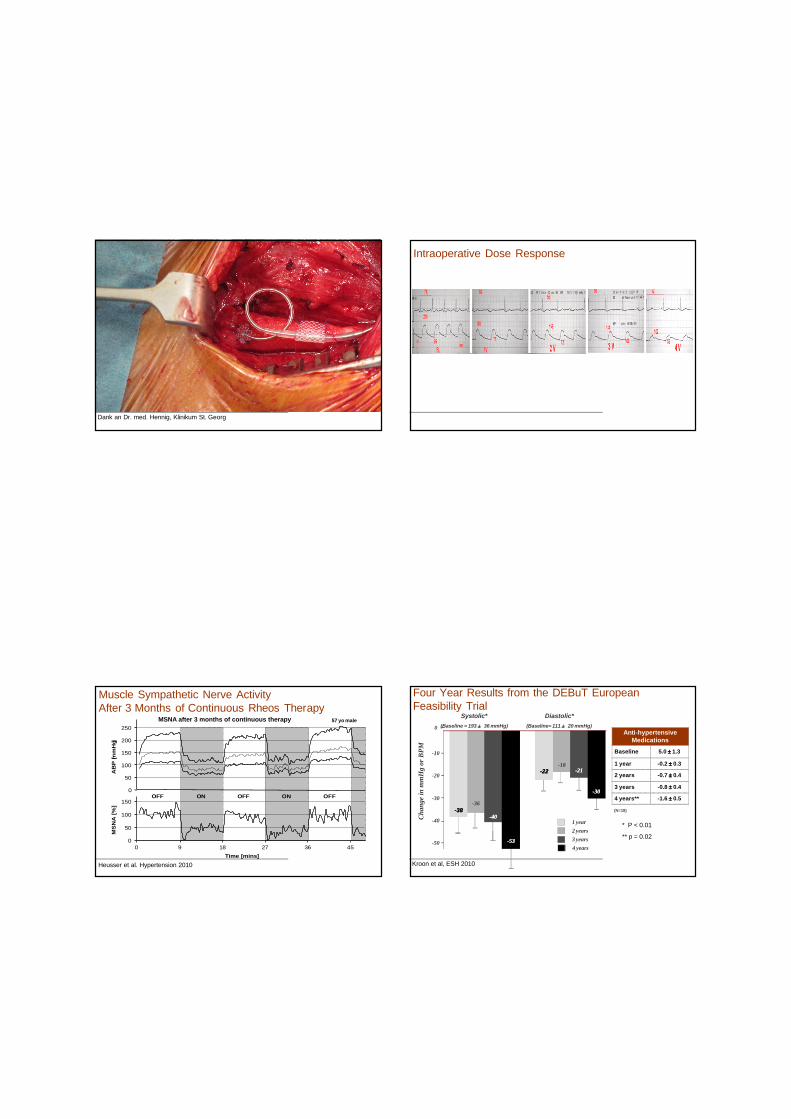
Dank an Dr. med. Hennig, Klinikum St. Georg
Operativer Situs Intraoperative Dose Response
23
Muscle Sympathetic Nerve Activity After 3 Months of Continuous Rheos Therapy
Time [mins]
0
50
100
150
200
250
0
50
100
150
0 9 18 27 36 45
AB
P [m
mH
g]M
SN
A [%
]
ONOFF ONOFF OFF
57 yo maleMSNA after 3 months of continuous therapy
Heusser et al. Hypertension 2010 Kroon et al, ESH 2010
Four Year Results from the DEBuT European Feasibility Trial
Diastolic*(Baseline= 111 ± 20 mmHg)
-18--2121--2222
Systolic*(Baseline = 193 ± 36 mmHg)
-36
--4040--3838
-30
-20
-50
-10
Chan
ge in
mm
Hg
or B
PM
-40
Anti-hypertensive Medications
Baseline 5.0 ± 1.3
1 year -0.2 ± 0.3
2 years -0.7 ± 0.4
3 years -0.8 ± 0.4
4 years** -1.6 ± 0.5
(N=18)
2 years3 years
1 year
4 years
0
--5353
--3030
* P < 0.01
** p = 0.02
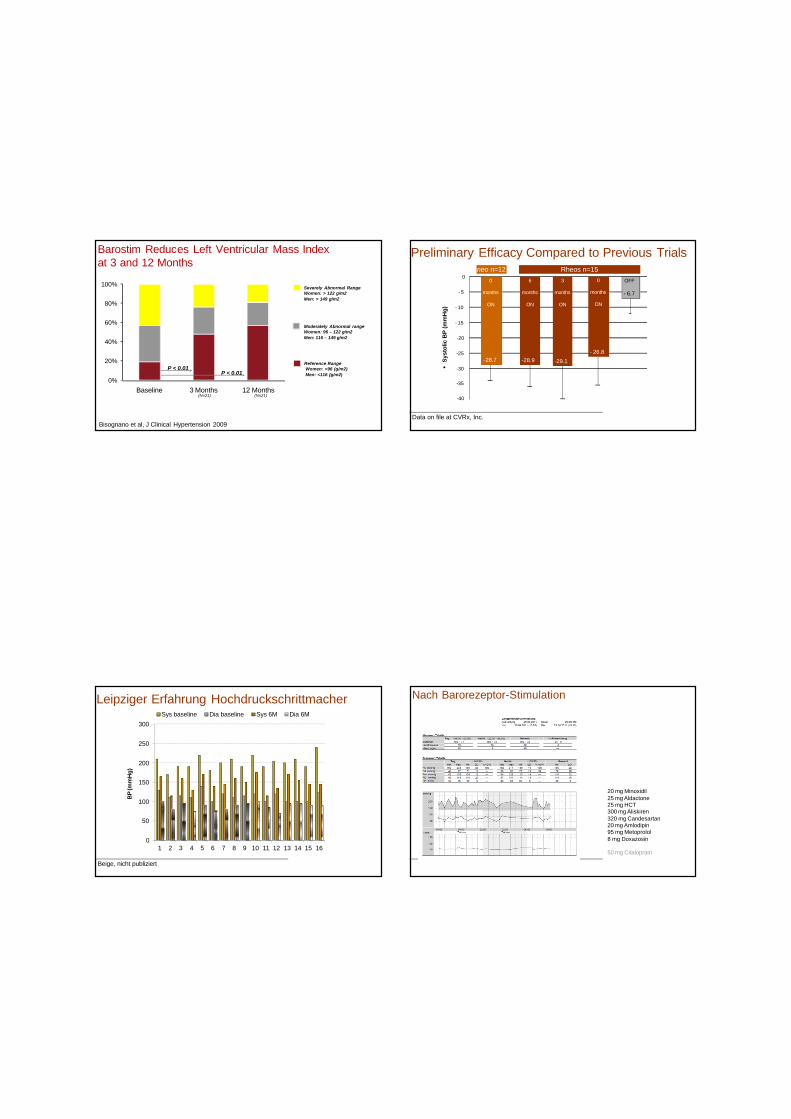
Barostim Reduces Left Ventricular Mass Index at 3 and 12 Months
P < 0.01P < 0.01
Bisognano et al, J Clinical Hypertension 2009
Severely Abnormal RangeWomen: > 122 g/m2Men: > 149 g/m2
Moderately Abnormal rangeWomen: 96 – 122 g/m2Men: 116 – 149 g/m2
Reference RangeWomen: <96 (g/m2)Men: <116 (g/m2)
(N=21) (N=21)
0%
20%
40%
60%
80%
100%
Baseline 3 Months 12 Months
Data on file at CVRx, Inc.
Preliminary Efficacy Compared to Previous Trials
-30
-25
-20
- 15
- 10
- 5
0
•Sy
stol
ic B
P (m
mH
g)
Rheos n=15neo n=12
-28.7 -28.9 -29.1- 26.8
- 6.7
-35
-40
6
months
ON
3
months
ON
0
months
ON
OFF0
months
ON
Beige, nicht publiziert
Leipziger Erfahrung Hochdruckschrittmacher
0
50
100
150
200
250
300
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Sys baseline Dia baseline Sys 6M Dia 6M
BP
(mm
Hg)
20 mg Minoxidil25 mg Aldactone25 mg HCT300 mg Aliskiren320 mg Candesartan20 mg Amlodipin95 mg Metoprolol8 mg Doxazosin
50 mg Citalopram
Nach Barorezeptor-Stimulation
RR 200/120, nach AggregatRR 200/120, nach Aggregat
RR 160/95, nach Adrenalektomie
10 mg Minoxidil25 mg Aldactone12,5 mg HCT150 mg Aliskiren160 mg Candesartan20 mg Amlodipin95 mg Metoprolol8 mg Doxazosin
Nach Adrenalektomie
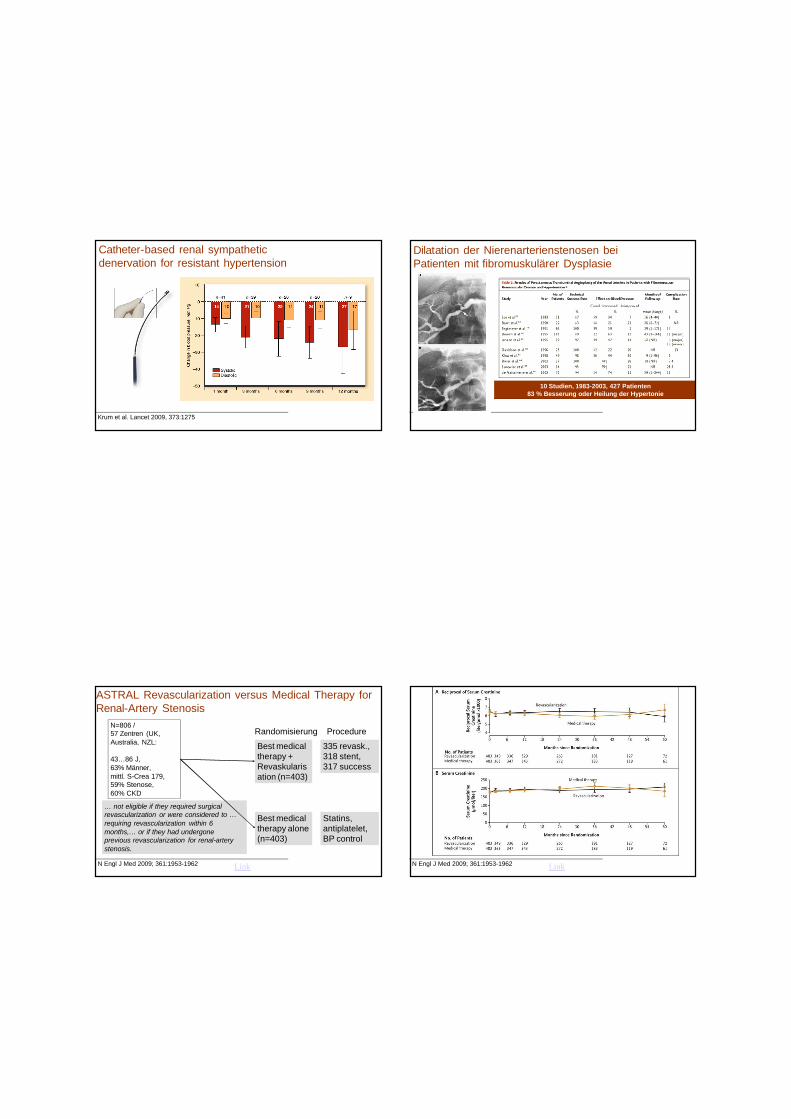
Krum et al. Lancet 2009, 373:1275
Catheter-based renal sympathetic denervation for resistant hypertension
Johnson R et al. N Engl J Med 2003;346:913-923
10 Studien, 1983-2003, 427 Patienten83 % Besserung oder Heilung der Hypertonie
Dilatation der Nierenarterienstenosen bei Patienten mit fibromuskulärer Dysplasie
N Engl J Med 2009; 361:1953-1962
… not eligible if they required surgical revascularization or were considered to … requiring revascularization within 6 months,… or if they had undergone previous revascularization for renal-artery stenosis.
ASTRAL Revascularization versus Medical Therapy for Renal-Artery Stenosis
N=806 /57 Zentren (UK, Australia, NZL:
43…86 J,63% Männer,mittl. S-Crea 179, 59% Stenose,60% CKD
Best medical therapy +Revaskularisation (n=403)
Best medical therapy alone (n=403)
Link
335 revask., 318 stent, 317 success
Statins, antiplatelet, BP control
ProcedureRandomisierung
N Engl J Med 2009; 361:1953-1962
ASTRAL Renal Function
Link
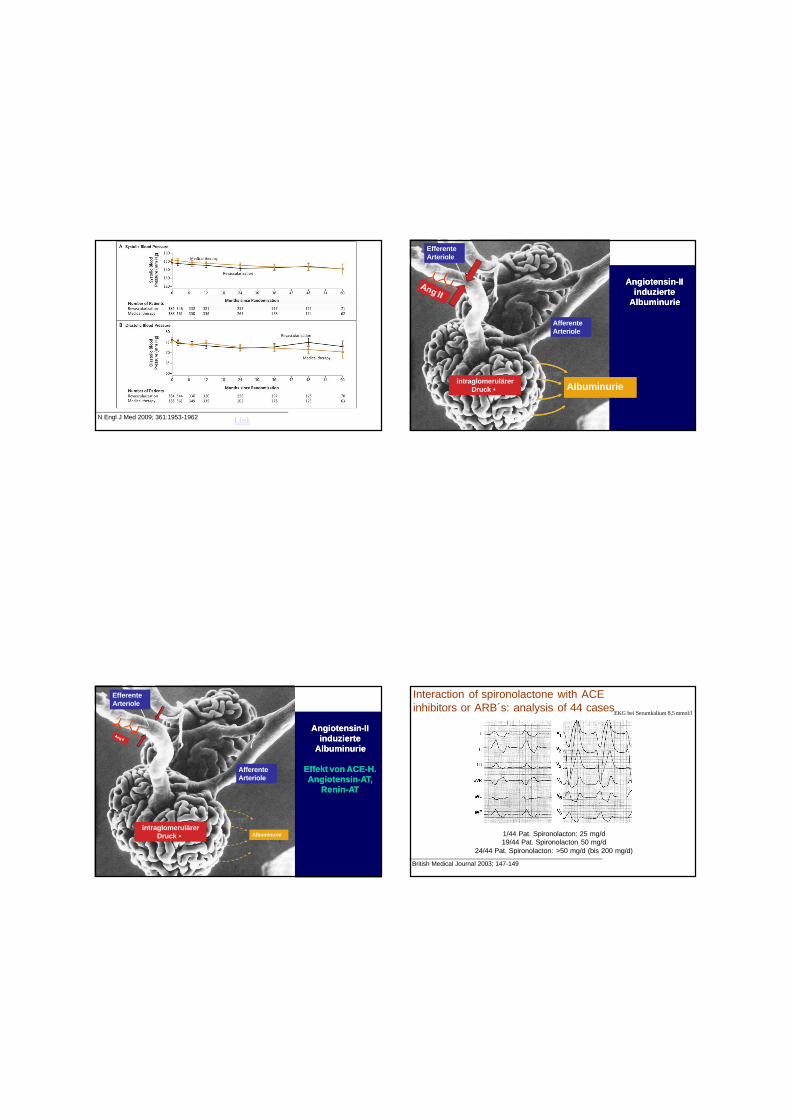
N Engl J Med 2009; 361:1953-1962
ASTRAL Blood Pressure
Link
AfferenteArteriole
EfferenteArteriole
intraglomerulärerDruck •
Angiotensin-IIinduzierte
Albuminurie
Angiotensin-IIinduzierte
Albuminurie
Albuminurie
AfferenteArteriole
EfferenteArteriole
intraglomerulärerDruck • Albuminurie
Angiotensin-IIinduzierte
Albuminurie
Effekt von ACE-H.Angiotensin-AT,
Renin-AT
Angiotensin-IIinduzierte
Albuminurie
Effekt von ACE-H.Angiotensin-AT,
Renin-AT
British Medical Journal 2003; 147-149
EKG bei Serumkalium 8,5 mmol/l
1/44 Pat. Spironolacton: 25 mg/d19/44 Pat. Spironolacton 50 mg/d
24/44 Pat. Spironolacton: >50 mg/d (bis 200 mg/d)
Interaction of spironolactone with ACE inhibitors or ARB´s: analysis of 44 cases
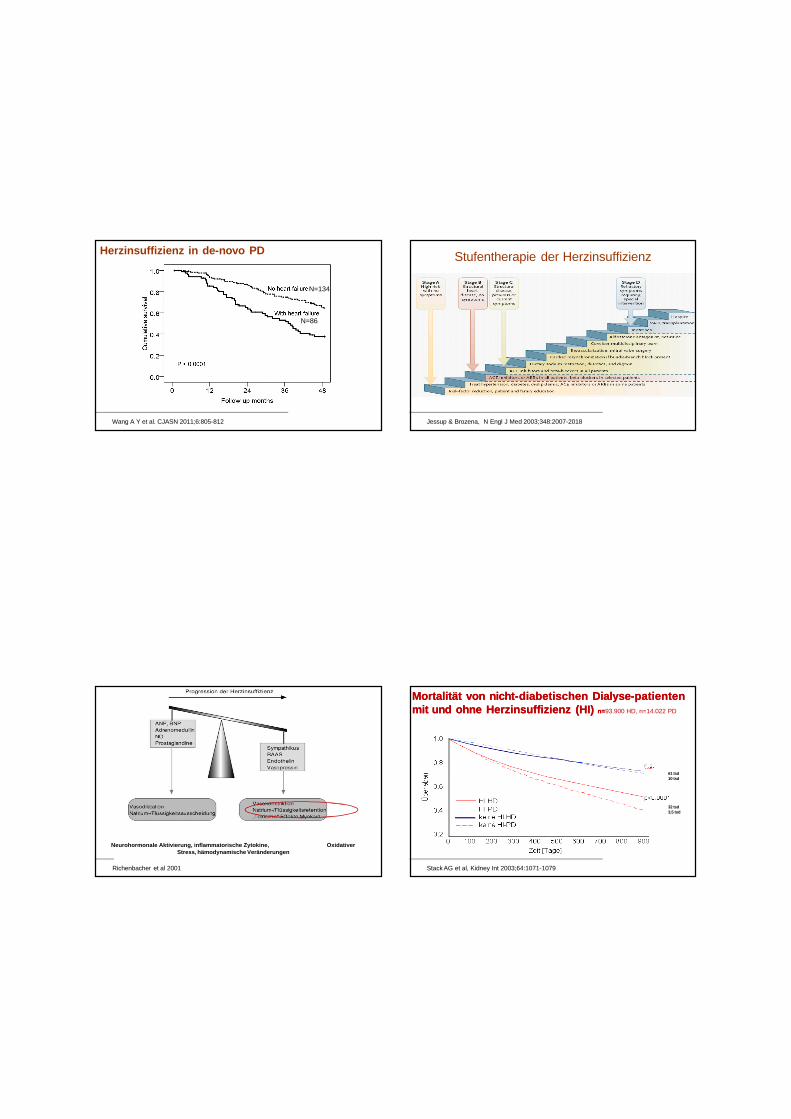
Wang A Y et al. CJASN 2011;6:805-812
Herzinsuffizienz in de-novo PD
N=134
N=86
Stufentherapie der Herzinsuffizienz
Jessup & Brozena, N Engl J Med 2003;348:2007-2018
Neurohormonale Aktivierung, inflammatorische Zytokine, Oxidativer Stress, hämodynamische Veränderungen
Richenbacher et al 2001
MortalitätMortalität von von nichtnicht--diabetischendiabetischen DialyseDialyse--patientenpatientenmitmit und und ohneohne HerzinsuffizienzHerzinsuffizienz (HI) (HI) n=n=93.900 HD, n=14.022 PD
61 tsd10 tsd
32 tsd3,5 tsd
Stack AG et al, Kidney Int 2003;64:1071-1079
Kardio-Renales Syndrom
Typ Definition Anmerkung1 Akute Verschlechterung der HF (akute LHI,
kardiogener Schock, RHV)Renale Hypoperfusion
2 Chronische Herzinsuffizienz Chron. HypoperfusionMikro-/MakroangiopathieInflammation, Fibrose, Apoptose
3 Akute NI (Ischämie, GN, ANV) Akute Arrhythmie, IschämieAcidose, Elektrolytentgleis.Urämie
4 Chron. NI Variable hormonelle und SW-VeränderungenFibrose, Inflammation,Calcifikation
5 Sek. Veränderungen bei Diabetes, Amyloidose, Sepsis, SLE, Sakoidose etc.
s. Typ 2-4
Ronco et al. JACC 2008; 52: 1527-39
• 2 Wochen nach Shuntanlage: Schlagvolumen ↑, peripherer Widerstand ↓, linksventrikulärer enddiastolischer Durchmesser ↑, ANP ↑, BNP ↑Ori Y et al (Nephrol Dial Transplant 1996;11:94-97)
• Innerhalb von 2 Wochen nach Shuntanlage: Schlagvolumen ↑, linksventrikulärer enddiastolischer Durchmesser ↑Iwashima Y et al (Am J Kidney Dis 2002;40:974-982)
Kardiale Belastung nach Anlage Kardiale Belastung nach Anlage eines Shuntseines Shunts
Kardiale Effekte Kardiale Effekte der Beseitigung des der Beseitigung des DialyseshuntsDialyseshunts
Rückgang der Linksherzhypertrophie nach Shuntligatur:
• 4-5 Monate nach Shuntligatur (Shuntfluss 1790 ± 648 ml/min): linksventrikulärer enddiastolischer Durchmesser ↓, linksventrikuläre Masse ↓, Herzfrequenz ↓, BP unverändertDuijnhoven ECM et al (NDT 2001;16:368-372)
• 21 Monate nach Shuntligatur (Shuntfluss 1371 ± 727 ml/min): linksventrikuläre Masse ↓, linksventrikulärer enddiastolischer Durchmesser ↓, diastolischer Blutdruck ↑Unger P et al (Am J Transplant 2004;4:2038-2044)
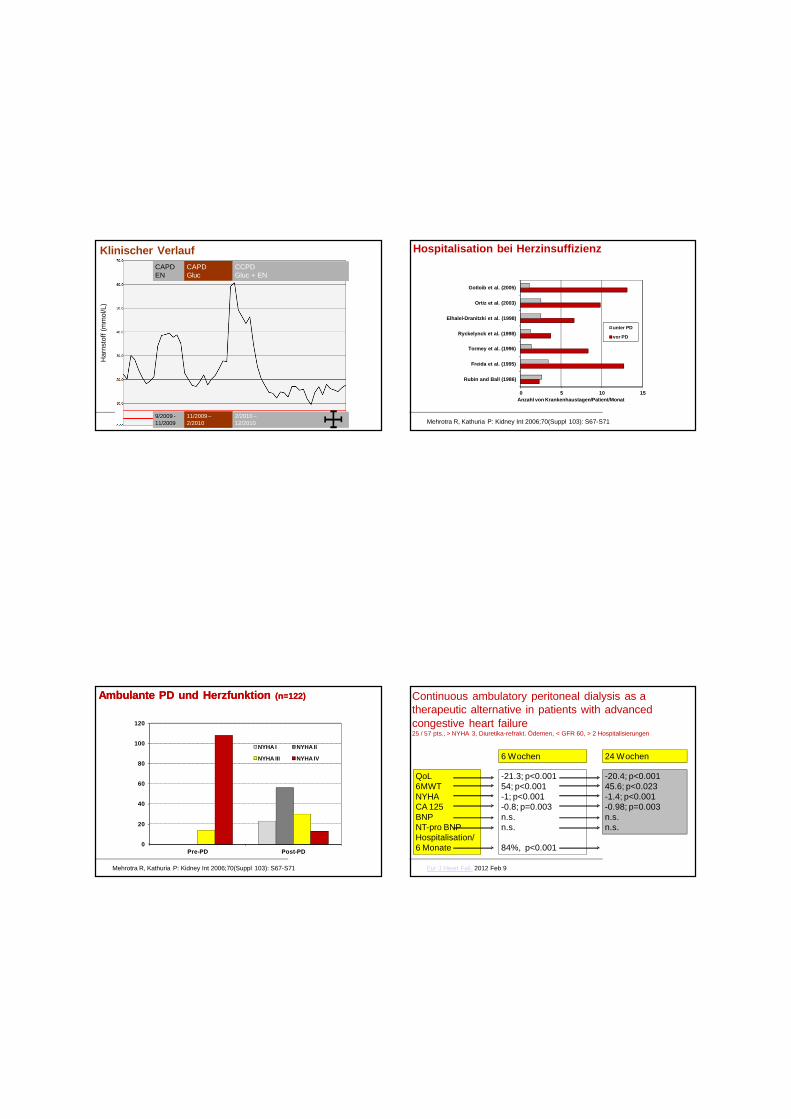
Klinischer Verlauf
Klinischer Verlauf
Har
nsto
ff (m
mol
/L)
CAPDEN
CAPDGluc
CCPDGluc + EN
9/2009 -11/2009
11/2009 –2/2010
2/2010 –12/2010
Hospitalisation bei Herzinsuffizienz
0 5 10 15
Rubin and Ball (1986)
Freida et al. (1995)
Tormey et al. (1996)
Ryckelynck et al. (1998)
Elhalel-Dranitzki et al. (1998)
Ortiz et al. (2003)
Gotloib et al. (2005)
unter PD
vor PD
Anzahl von Krankenhaustagen/Patient/Monat
Mehrotra R, Kathuria P: Kidney Int 2006;70(Suppl 103): S67-S71
Ambulante PD und Ambulante PD und Herzfunktion Herzfunktion (n=122)(n=122)
0
20
40
60
80
100
120
Pre-PD Post-PD
NYHA I NYHA II
NYHA III NYHA IV
n
Mehrotra R, Kathuria P: Kidney Int 2006;70(Suppl 103): S67-S71
Continuous ambulatory peritoneal dialysis as a therapeutic alternative in patients with advanced congestive heart failure25 / 57 pts., > NYHA 3, Diuretika-refrakt. Ödemen, < GFR 60, > 2 Hospitalisierungen
Eur J Heart Fail. 2012 Feb 9
-21.3; p<0.00154; p<0.001-1; p<0.001-0.8; p=0.003n.s.n.s.
84%, p<0.001
-20.4; p<0.00145.6; p<0.023-1.4; p<0.001-0.98; p=0.003n.s.n.s.
QoL6MWTNYHACA 125BNPNT-pro BNPHospitalisation/6 Monate
6 Wochen 24 Wochen
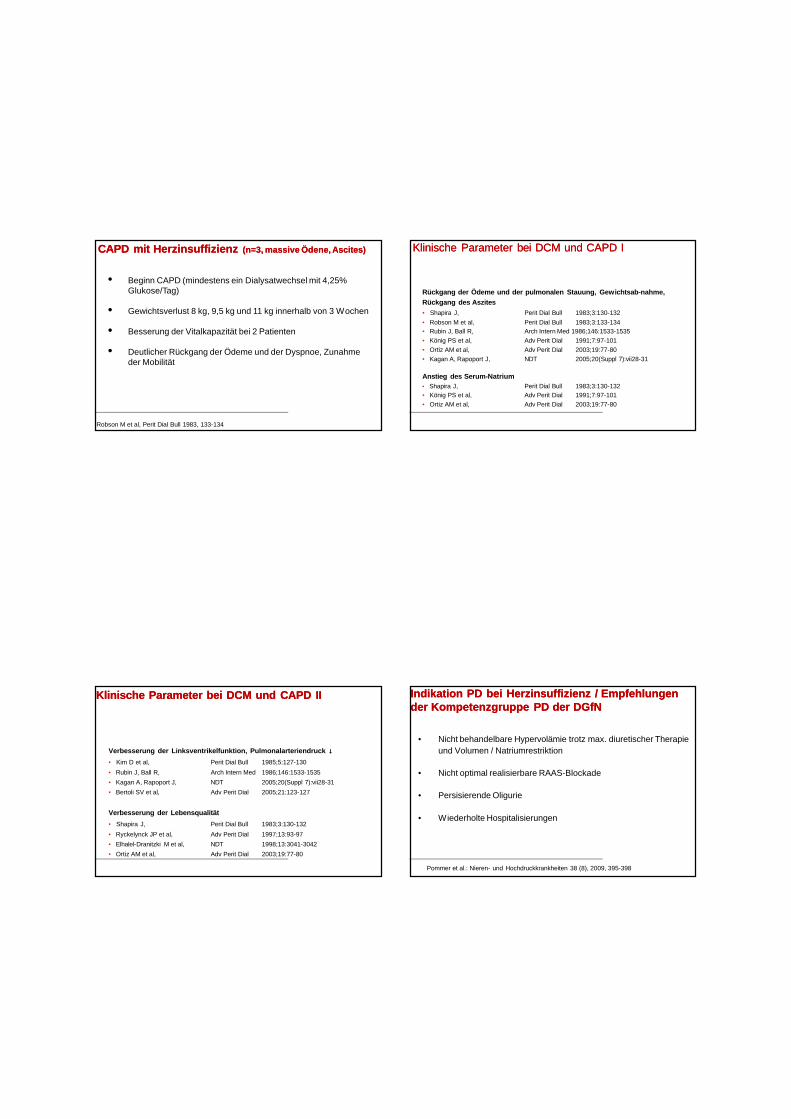
• Beginn CAPD (mindestens ein Dialysatwechsel mit 4,25% Glukose/Tag)
• Gewichtsverlust 8 kg, 9,5 kg und 11 kg innerhalb von 3 Wochen
• Besserung der Vitalkapazität bei 2 Patienten
• Deutlicher Rückgang der Ödeme und der Dyspnoe, Zunahme der Mobilität
CAPD mit CAPD mit Herzinsuffizienz Herzinsuffizienz (n=3, massive (n=3, massive ÖdeneÖdene, , AscitesAscites))
Robson M et al, Perit Dial Bull 1983, 133-134
Klinische Parameter Klinische Parameter bei bei DCM und CAPD IDCM und CAPD I
Rückgang der Ödeme und der pulmonalen Stauung, Gewichtsab-nahme, Rückgang des Aszites • Shapira J, Perit Dial Bull 1983;3:130-132• Robson M et al, Perit Dial Bull 1983;3:133-134• Rubin J, Ball R, Arch Intern Med 1986;146:1533-1535• König PS et al, Adv Perit Dial 1991;7:97-101• Ortiz AM et al, Adv Perit Dial 2003;19:77-80• Kagan A, Rapoport J, NDT 2005;20(Suppl 7):vii28-31
Anstieg des Serum-Natrium• Shapira J, Perit Dial Bull 1983;3:130-132• König PS et al, Adv Perit Dial 1991;7:97-101• Ortiz AM et al, Adv Perit Dial 2003;19:77-80
Klinische Parameter bei DCM und CAPD IIKlinische Parameter bei DCM und CAPD II
Verbesserung der Linksventrikelfunktion, Pulmonalarteriendruck ↓
• Kim D et al, Perit Dial Bull 1985;5:127-130• Rubin J, Ball R, Arch Intern Med 1986;146:1533-1535• Kagan A, Rapoport J, NDT 2005;20(Suppl 7):vii28-31• Bertoli SV et al, Adv Perit Dial 2005;21:123-127
Verbesserung der Lebensqualität• Shapira J, Perit Dial Bull 1983;3:130-132• Ryckelynck JP et al, Adv Perit Dial 1997;13:93-97• Elhalel-Dranitzki M et al, NDT 1998;13:3041-3042• Ortiz AM et al, Adv Perit Dial 2003;19:77-80
Indikation PD bei Herzinsuffizienz / Empfehlungen Indikation PD bei Herzinsuffizienz / Empfehlungen der Kompetenzgruppe PD der der Kompetenzgruppe PD der DGfNDGfN
• Nicht behandelbare Hypervolämie trotz max. diuretischer Therapie und Volumen / Natriumrestriktion
• Nicht optimal realisierbare RAAS-Blockade
• Persisierende Oligurie
• Wiederholte Hospitalisierungen
Pommer et al.: Nieren- und Hochdruckkrankheiten 38 (8), 2009, 395-398
Einfluss von Einfluss von IcodextrinIcodextrin bei Patienten mit bei Patienten mit dilatativerdilatativer KardiomyopathieKardiomyopathie
Zusammenfassung verschiedener Fallberichte (n=27)
• EF <20 –35%
• Nierenfunktion: normal bis CKD 4
• 1-2 Verweilzeiten mit Icodextrin, 2 Patienten auch Dialysatwechsel mit
Glukoselösungen
• Mittlere Ultrafiltration 1046 mL/Tag
• Klinische Verbesserung, keine Hypotonie, Anstieg der EF
• Rückgang der Krankenhausaufenthalte
• Peritonitisrate (1 Fallbericht): 1 Episode/100 Patientenmonate
Guest SS: Perit Dial Int 27 (Suppl 3): S13, 2007