Embed Size (px)
Citation preview
Pneumonie
Maja Weisser
Infek2ologie & Spitalhygiene
Pneumonie heute
-‐ Neue Keime / Neue Resistenzen
-‐ Kombina2onstherapie
-‐ Steroide -‐ Wo wird die CAP am besten (und am billigsten)
behandelt ?
-‐ Wie lange sollte man an2bio2sch behandeln ?
-‐ Therapieversagen
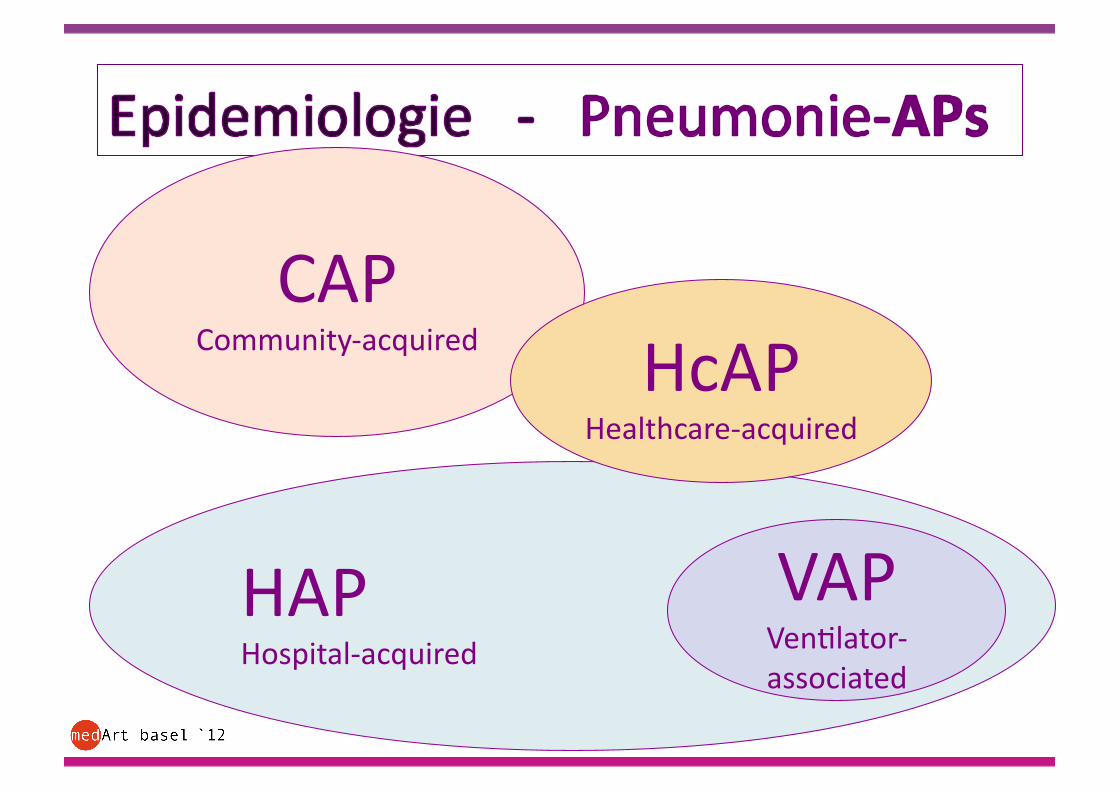
CAP Community-‐acquired
HAP Hospital-‐acquired
VAP Ven2lator-‐associated
HcAP Healthcare-‐acquired
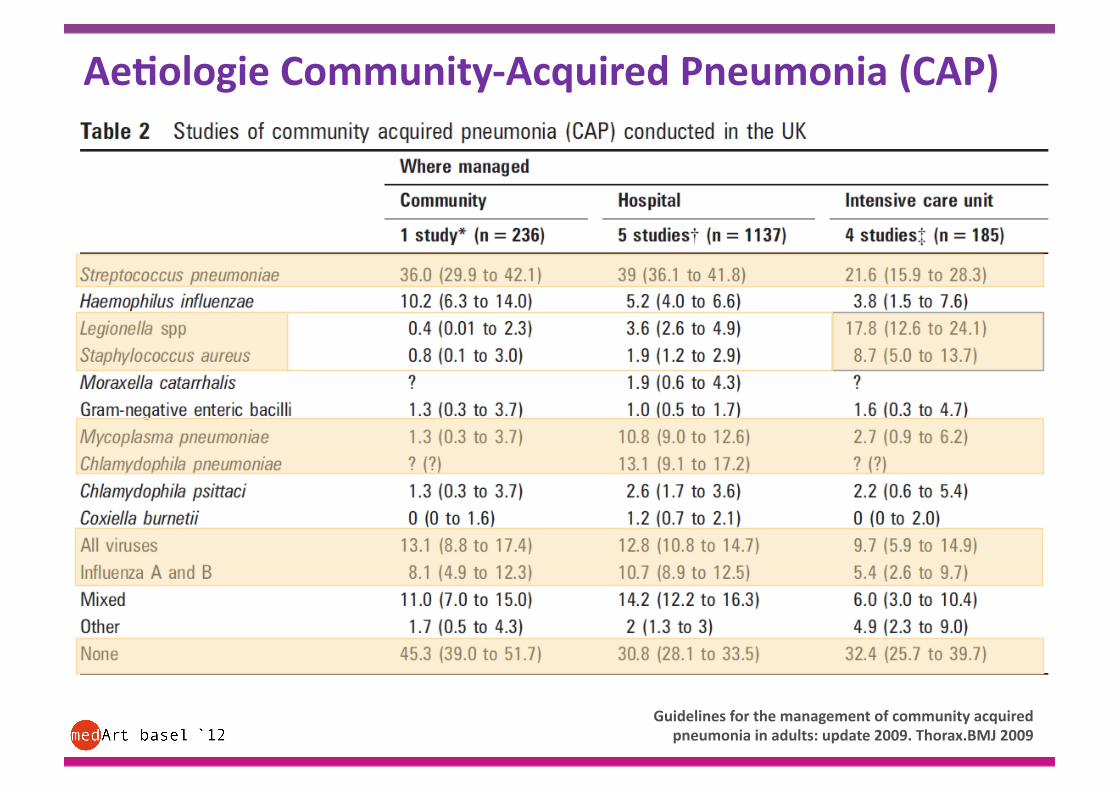
Ae,ologie Community-‐Acquired Pneumonia (CAP)
Guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax.BMJ 2009
Morozumi JIC 2010
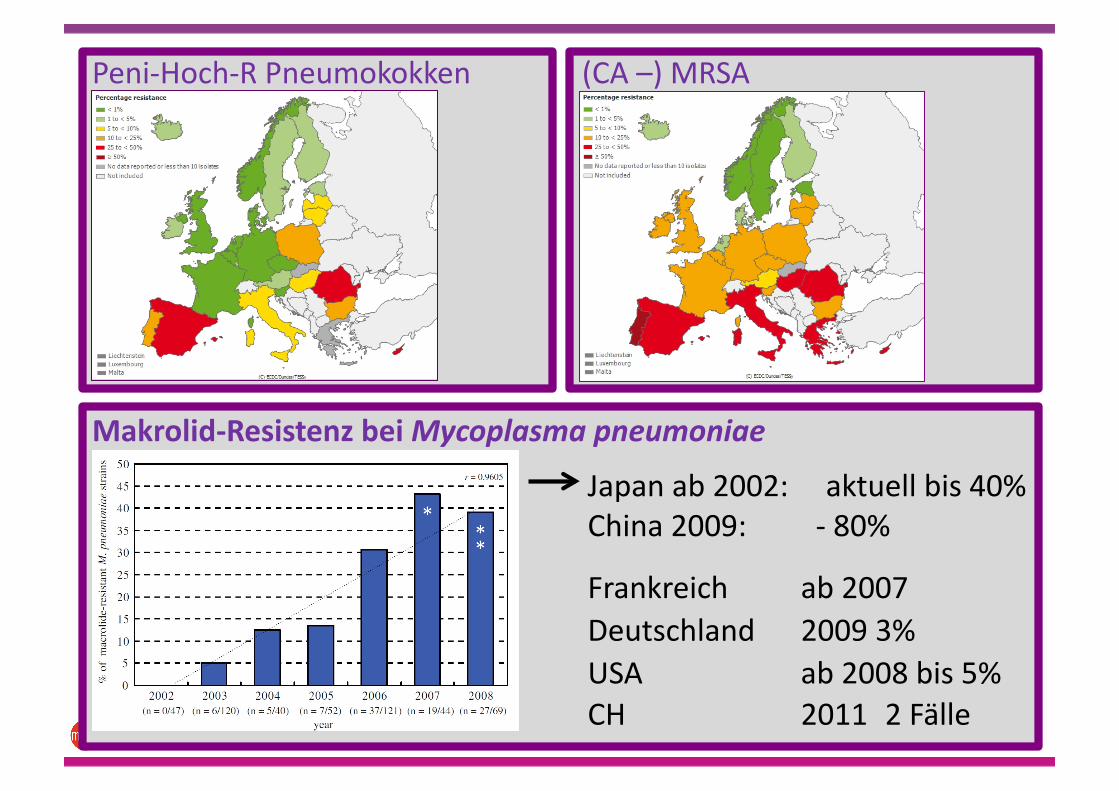
Makrolid-‐Resistenz bei Mycoplasma pneumoniae
Japan ab 2002: aktuell bis 40% China 2009: -‐ 80%
Frankreich ab 2007 Deutschland 2009 3% USA ab 2008 bis 5%
CH 2011 2 Fälle
Peni-‐Hoch-‐R Pneumokokken (CA –) MRSA
R E S I S T E N Z L A G E
www.ecdc.eu
hap://www.labormedizin-‐uhbs.ch
www.anresis.ch
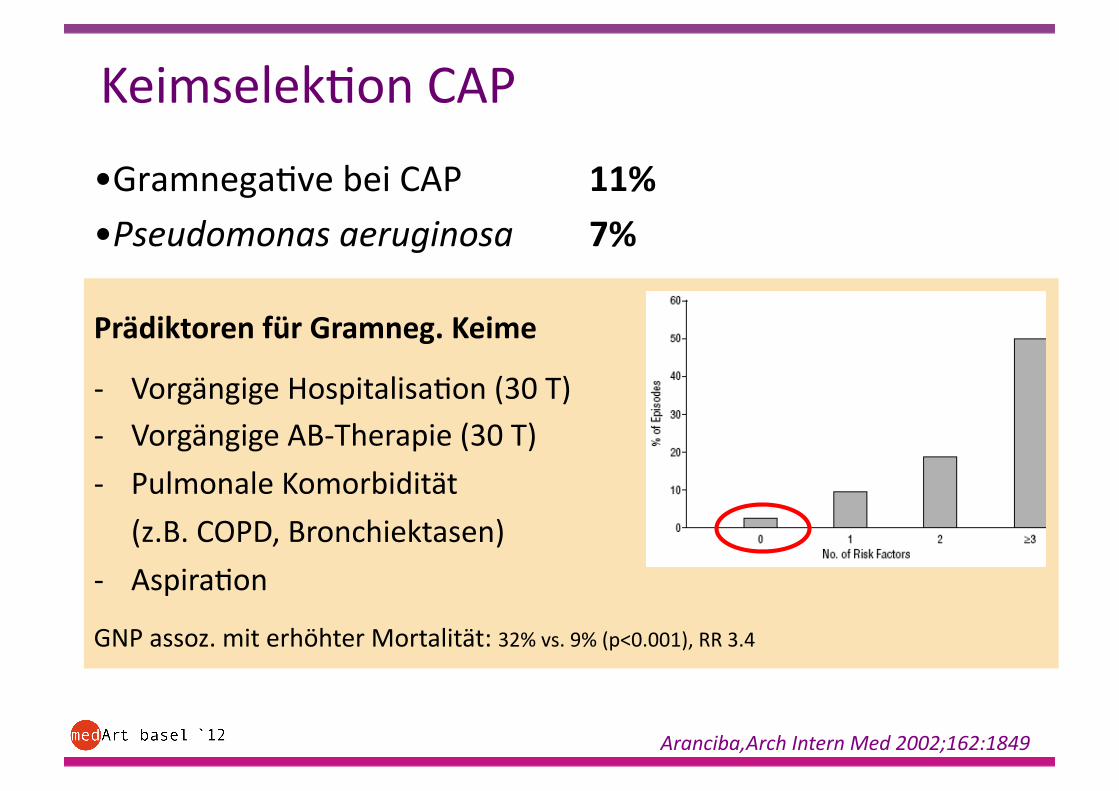
Prädiktoren für Gramneg. Keime
-‐ Vorgängige Hospitalisa2on (30 T) -‐ Vorgängige AB-‐Therapie (30 T)
-‐ Pulmonale Komorbidität
(z.B. COPD, Bronchiektasen)
-‐ Aspira2on
GNP assoz. mit erhöhter Mortalität: 32% vs. 9% (p<0.001), RR 3.4
• Gramnega2ve bei CAP 11% • Pseudomonas aeruginosa 7%
Aranciba,Arch Intern Med 2002;162:1849
Keimselek2on CAP
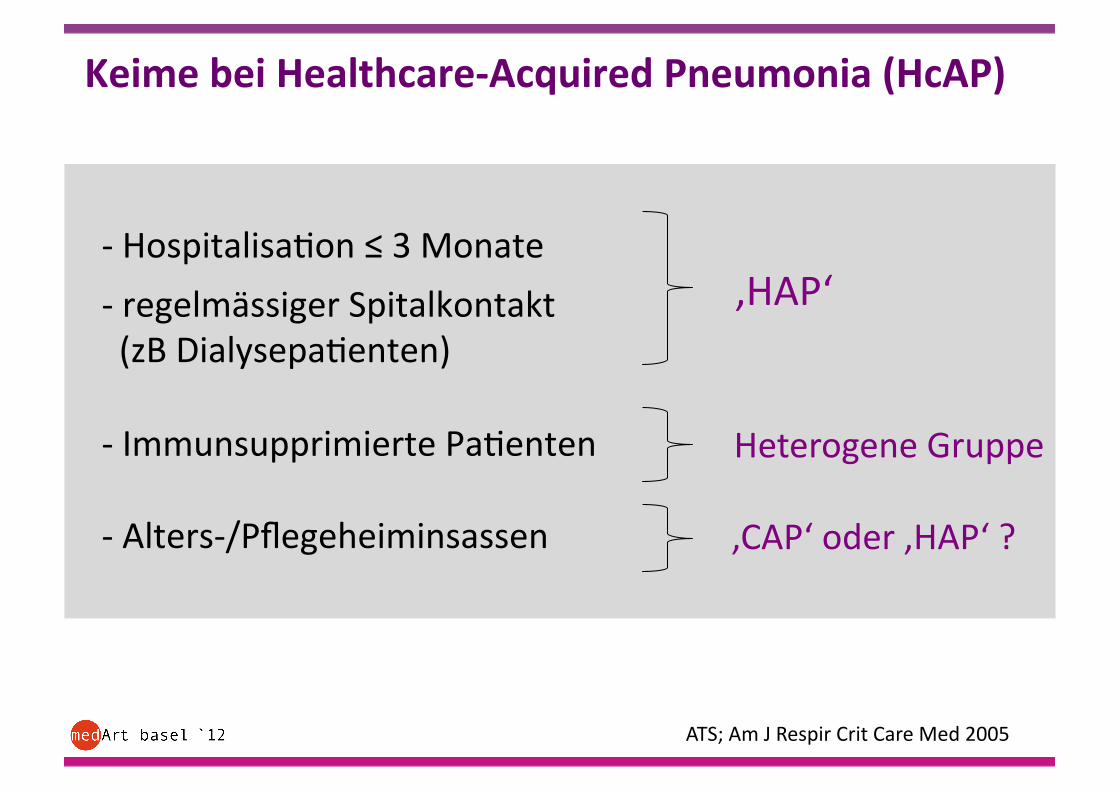
Keime bei Healthcare-‐Acquired Pneumonia (HcAP)
-‐ Hospitalisa2on ≤ 3 Monate
-‐ regelmässiger Spitalkontakt (zB Dialysepa2enten)
-‐ Immunsupprimierte Pa2enten
-‐ Alters-‐/Pflegeheiminsassen
ATS; Am J Respir Crit Care Med 2005
‚HAP‘
Heterogene Gruppe
‚CAP‘ oder ‚HAP‘ ?
• Amoxicillin/Clavulansäure
• Clindamycin
• Clarythromycin
• Amoxicillin/Clavulansäure
+ Clarythromycin
• Doxycyclin • Moxifloxacin
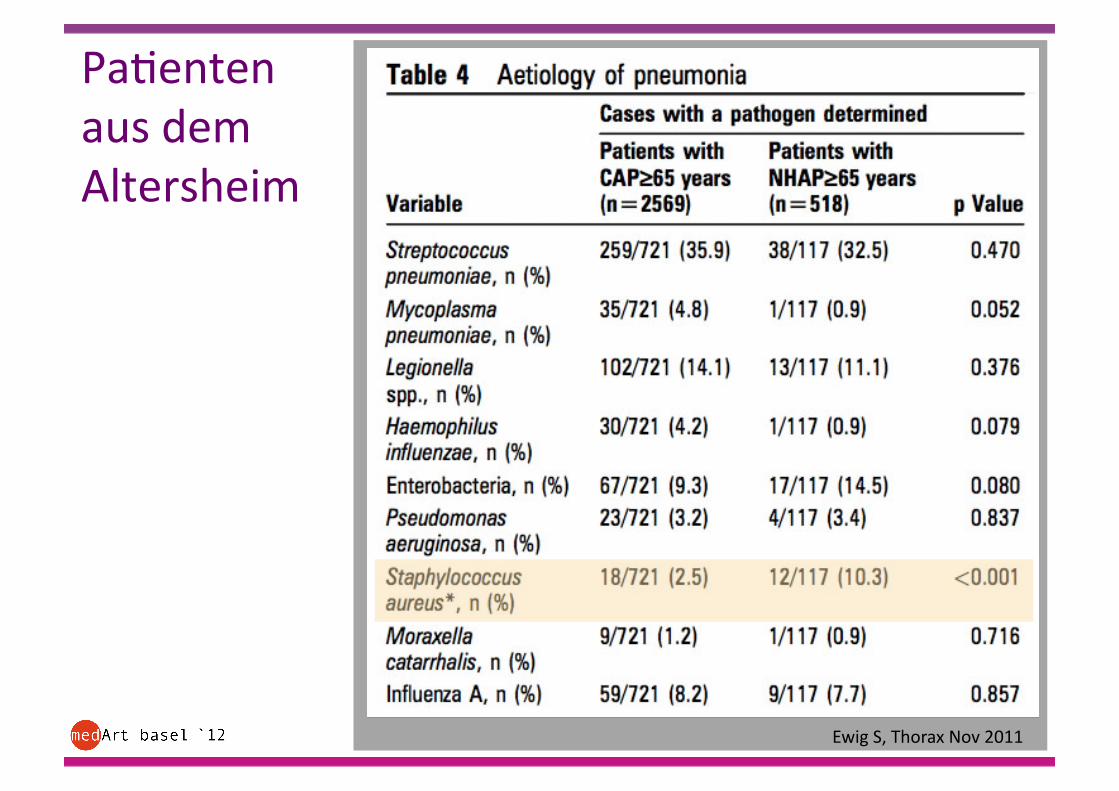
Pa2enten aus dem Altersheim
Ewig S, Thorax Nov 2011
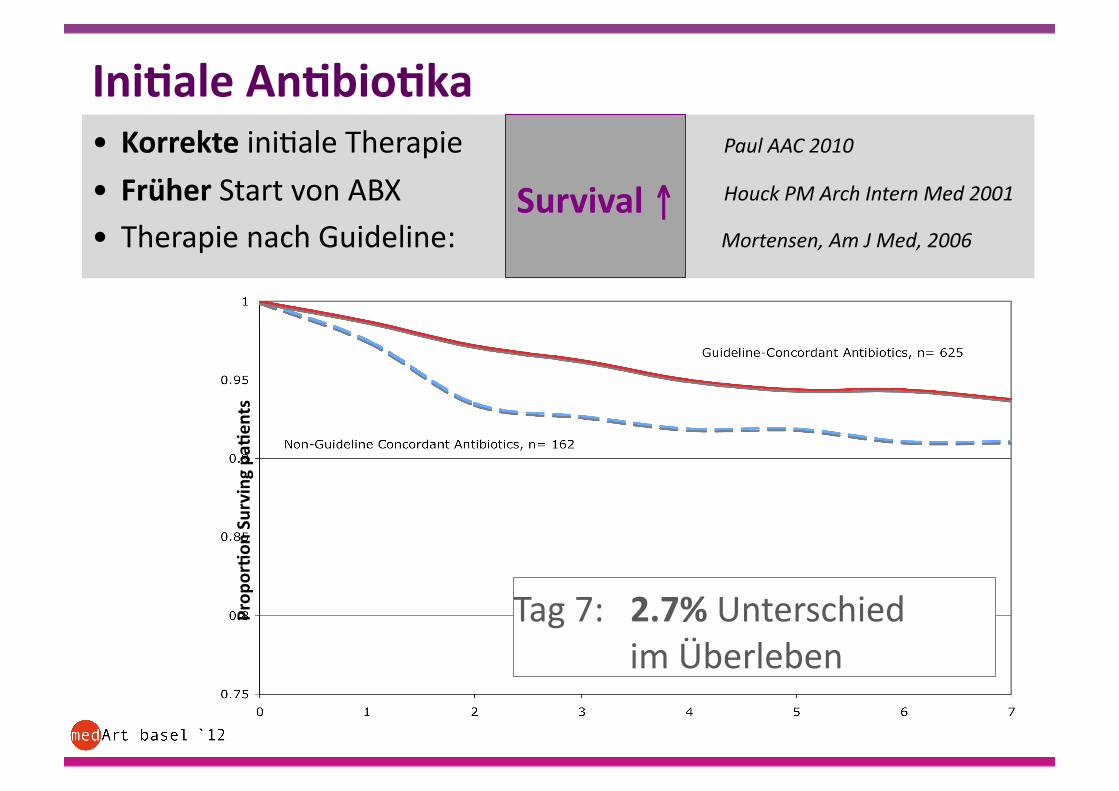
Ini,ale An,bio,ka • Korrekte ini2ale Therapie Paul AAC 2010
• Früher Start von ABX Houck PM Arch Intern Med 2001
• Therapie nach Guideline: Mortensen, Am J Med, 2006
Tag 7: 2.7% Unterschied im Überleben
Prop
or,on
Surving pa,
ents
Survival ↑
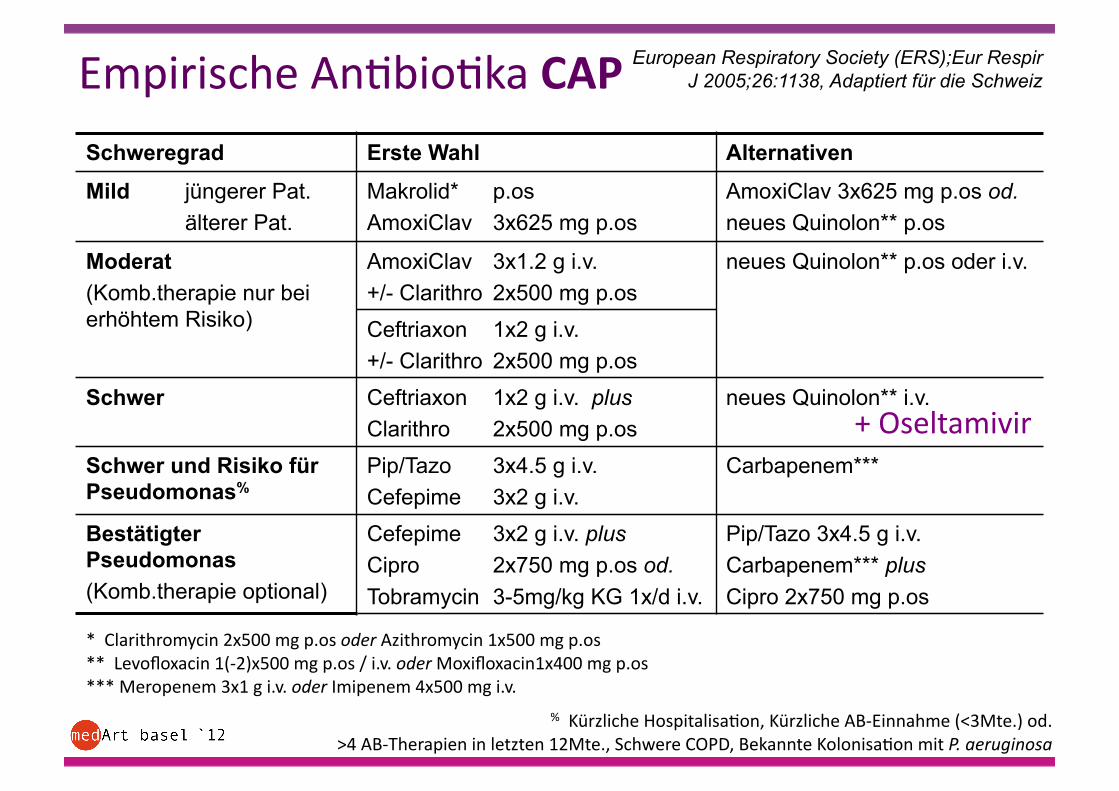
Schweregrad Erste Wahl Alternativen
Mild jüngerer Pat. älterer Pat.
Makrolid* p.os AmoxiClav 3x625 mg p.os
AmoxiClav 3x625 mg p.os od. neues Quinolon** p.os
Moderat (Komb.therapie nur bei erhöhtem Risiko)
AmoxiClav 3x1.2 g i.v. +/- Clarithro 2x500 mg p.os
neues Quinolon** p.os oder i.v.
Ceftriaxon 1x2 g i.v. +/- Clarithro 2x500 mg p.os
Schwer Ceftriaxon 1x2 g i.v. plus Clarithro 2x500 mg p.os
neues Quinolon** i.v.
Schwer und Risiko für Pseudomonas%
Pip/Tazo 3x4.5 g i.v. Cefepime 3x2 g i.v.
Carbapenem***
Bestätigter Pseudomonas (Komb.therapie optional)
Cefepime 3x2 g i.v. plus Cipro 2x750 mg p.os od. Tobramycin 3-5mg/kg KG 1x/d i.v.
Pip/Tazo 3x4.5 g i.v. Carbapenem*** plus Cipro 2x750 mg p.os
Empirische An2bio2ka CAP
* Clarithromycin 2x500 mg p.os oder Azithromycin 1x500 mg p.os ** Levofloxacin 1(-‐2)x500 mg p.os / i.v. oder Moxifloxacin1x400 mg p.os *** Meropenem 3x1 g i.v. oder Imipenem 4x500 mg i.v.
% Kürzliche Hospitalisa2on, Kürzliche AB-‐Einnahme (<3Mte.) od. >4 AB-‐Therapien in letzten 12Mte., Schwere COPD, Bekannte Kolonisa2on mit P. aeruginosa
European Respiratory Society (ERS);Eur Respir J 2005;26:1138, Adaptiert für die Schweiz
+ Oseltamivir
Hospital-‐acquired pneumonia (HAP) Ven2lator-‐associated pneumonia (VAP)
Lokale Spitalepidemiologie !!
UHBS: Enterobacter cloacae SerraGa marcescens
selten: Pseudomonas aeruginosa Stenotrophomonas maltophilia
keine Acinetobacter
AmpC-‐Bildner
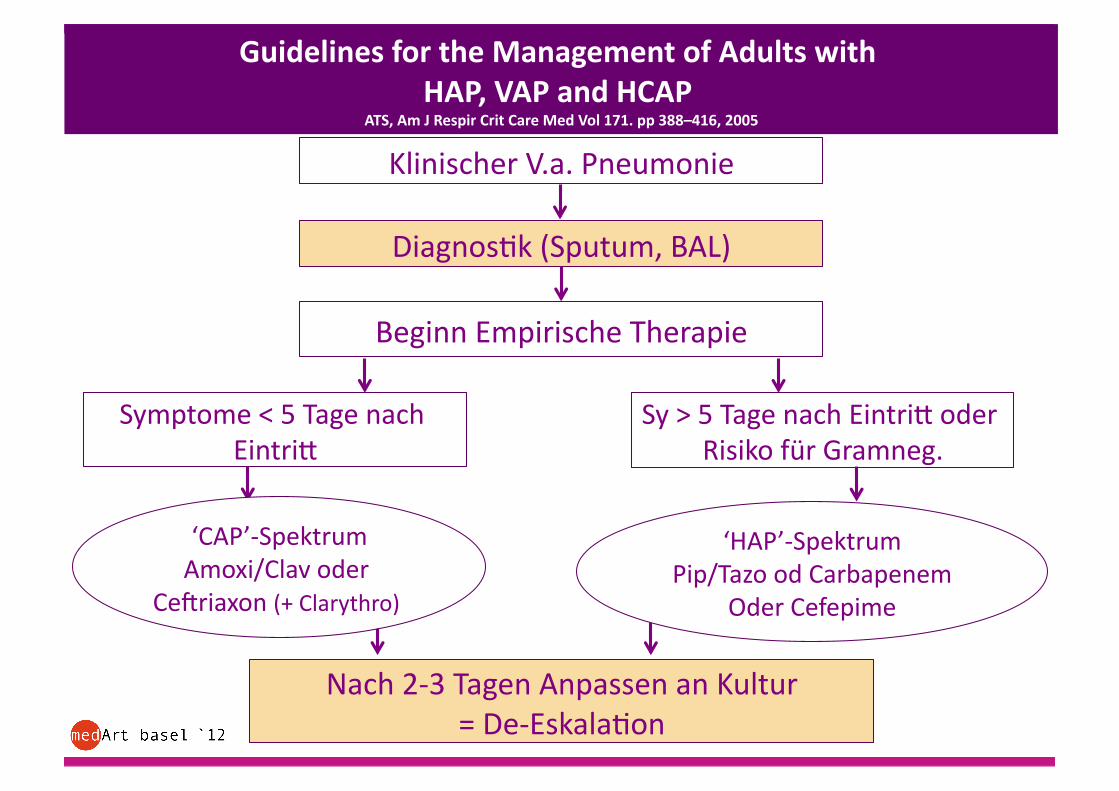
Guidelines for the Management of Adults with HAP, VAP and HCAP
ATS, Am J Respir Crit Care Med Vol 171. pp 388–416, 2005
Klinischer V.a. Pneumonie
Diagnos2k (Sputum, BAL)
Beginn Empirische Therapie
Symptome < 5 Tage nach Eintria
Sy > 5 Tage nach Eintria oder Risiko für Gramneg.
Nach 2-‐3 Tagen Anpassen an Kultur = De-‐Eskala2on
‘CAP’-‐Spektrum Amoxi/Clav oder
Ceyriaxon (+ Clarythro)
‘HAP’-‐Spektrum Pip/Tazo od Carbapenem
Oder Cefepime
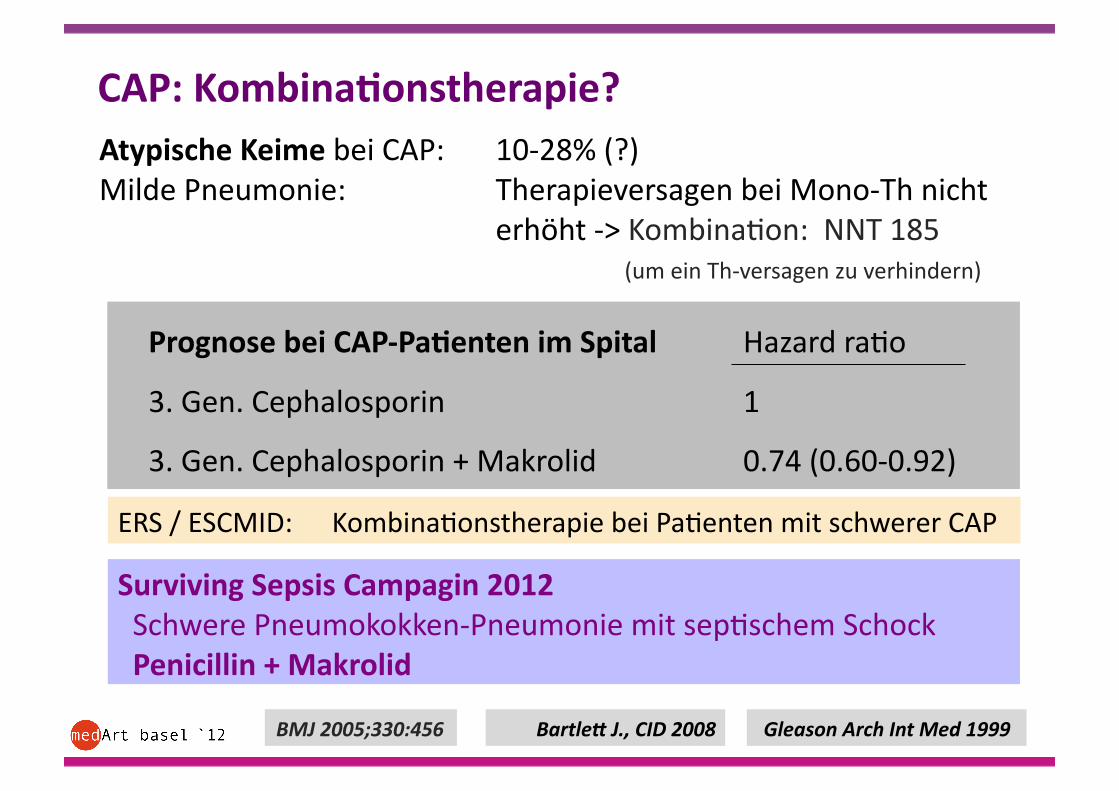
CAP: Kombina,onstherapie?
Bartle9 J., CID 2008
Atypische Keime bei CAP: 10-‐28% (?) Milde Pneumonie: Therapieversagen bei Mono-‐Th nicht
erhöht -‐> Kombina2on: NNT 185 (um ein Th-‐versagen zu verhindern)
BMJ 2005;330:456
Prognose bei CAP-‐Pa,enten im Spital Hazard ra2o
3. Gen. Cephalosporin 1
3. Gen. Cephalosporin + Makrolid 0.74 (0.60-‐0.92)
Gleason Arch Int Med 1999
ERS / ESCMID: Kombina2onstherapie bei Pa2enten mit schwerer CAP
Surviving Sepsis Campagin 2012 Schwere Pneumokokken-‐Pneumonie mit sep2schem Schock Penicillin + Makrolid
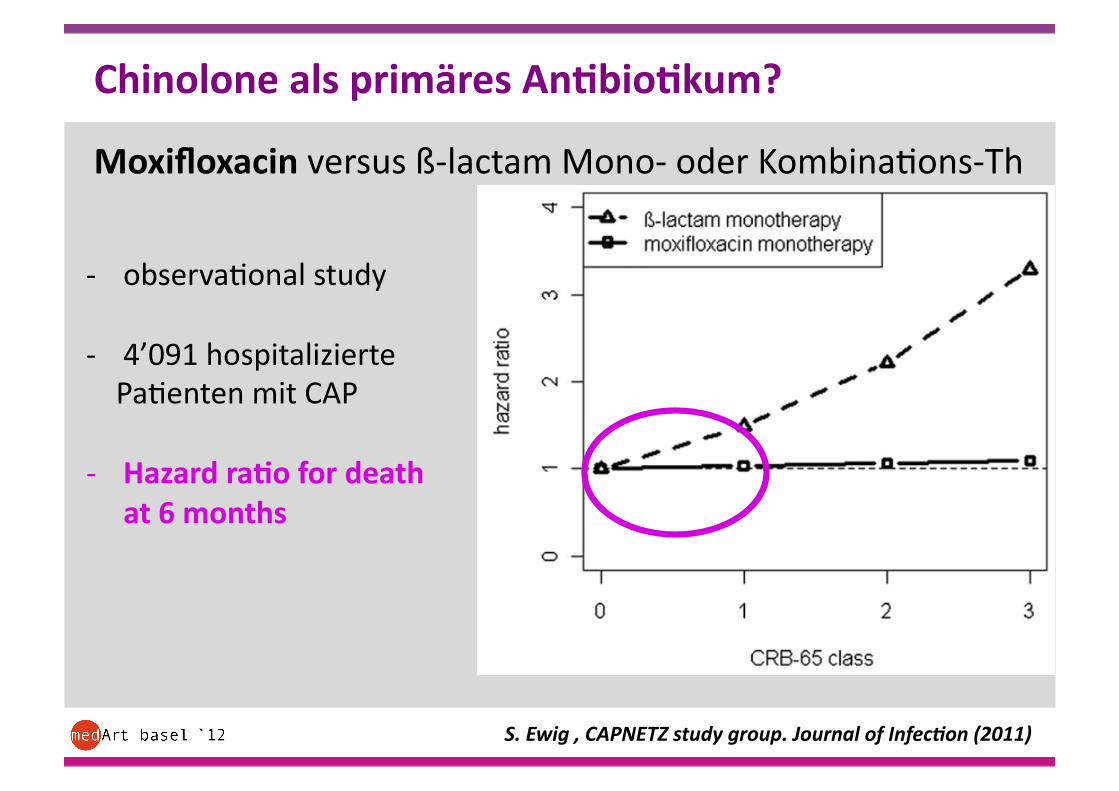
Chinolone als primäres An,bio,kum?
-‐ observa2onal study
-‐ 4’091 hospitalizierte Pa2enten mit CAP
-‐ Hazard ra,o for death at 6 months
Moxifloxacin versus ß-‐lactam Mono-‐ oder Kombina2ons-‐Th
S. Ewig , CAPNETZ study group. Journal of InfecRon (2011)
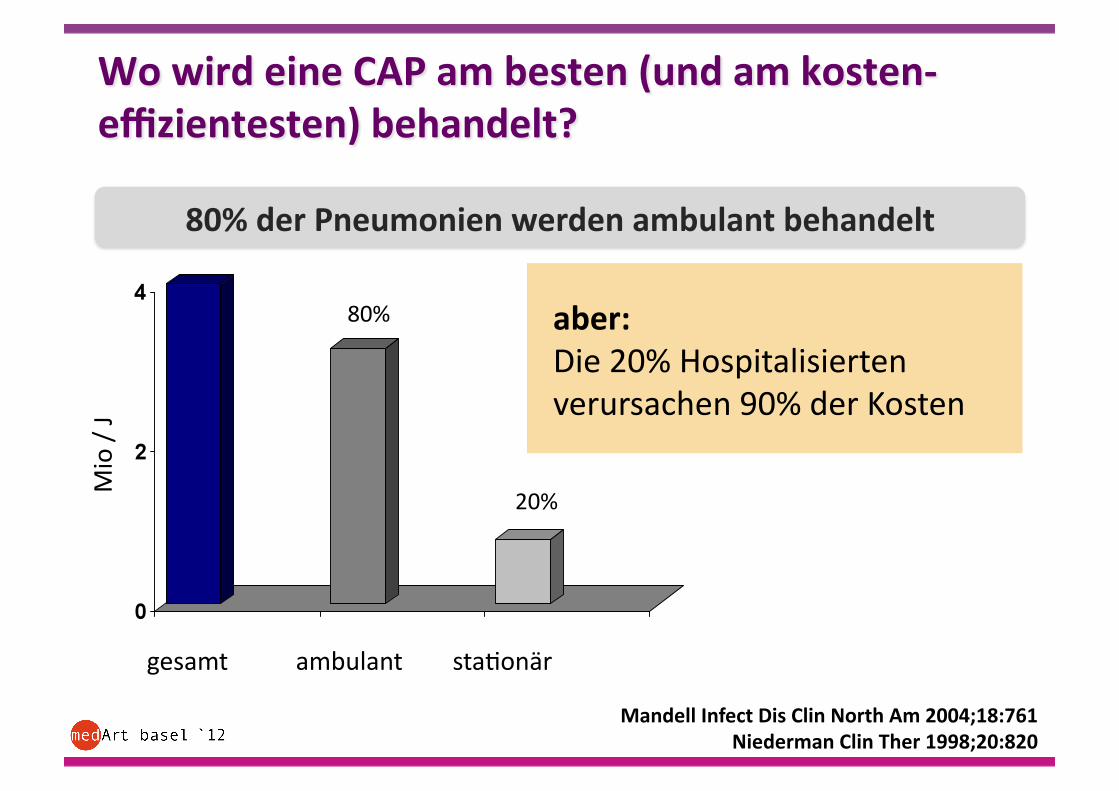
gesamt ambulant sta2onär
80%
20%
Mio / J
80% der Pneumonien werden ambulant behandelt
aber: Die 20% Hospitalisierten verursachen 90% der Kosten
Mandell Infect Dis Clin North Am 2004;18:761 Niederman Clin Ther 1998;20:820
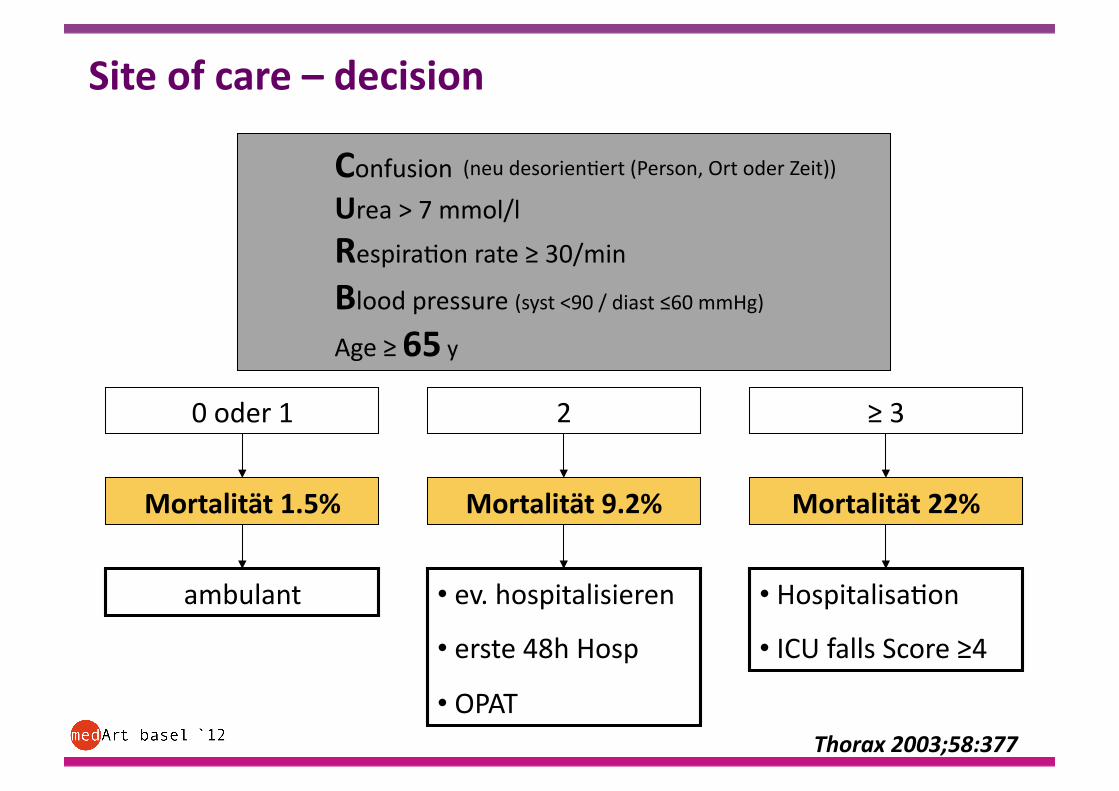
Confusion
Urea > 7 mmol/l
Respira2on rate ≥ 30/min
Blood pressure (syst <90 / diast ≤60 mmHg)
Age ≥ 65 y
0 oder 1 2 ≥ 3
Mortalität 1.5% Mortalität 9.2% Mortalität 22%
ambulant • ev. hospitalisieren • erste 48h Hosp
• OPAT
• Hospitalisa2on • ICU falls Score ≥4
Thorax 2003;58:377
(neu desorien2ert (Person, Ort oder Zeit))
Site of care – decision
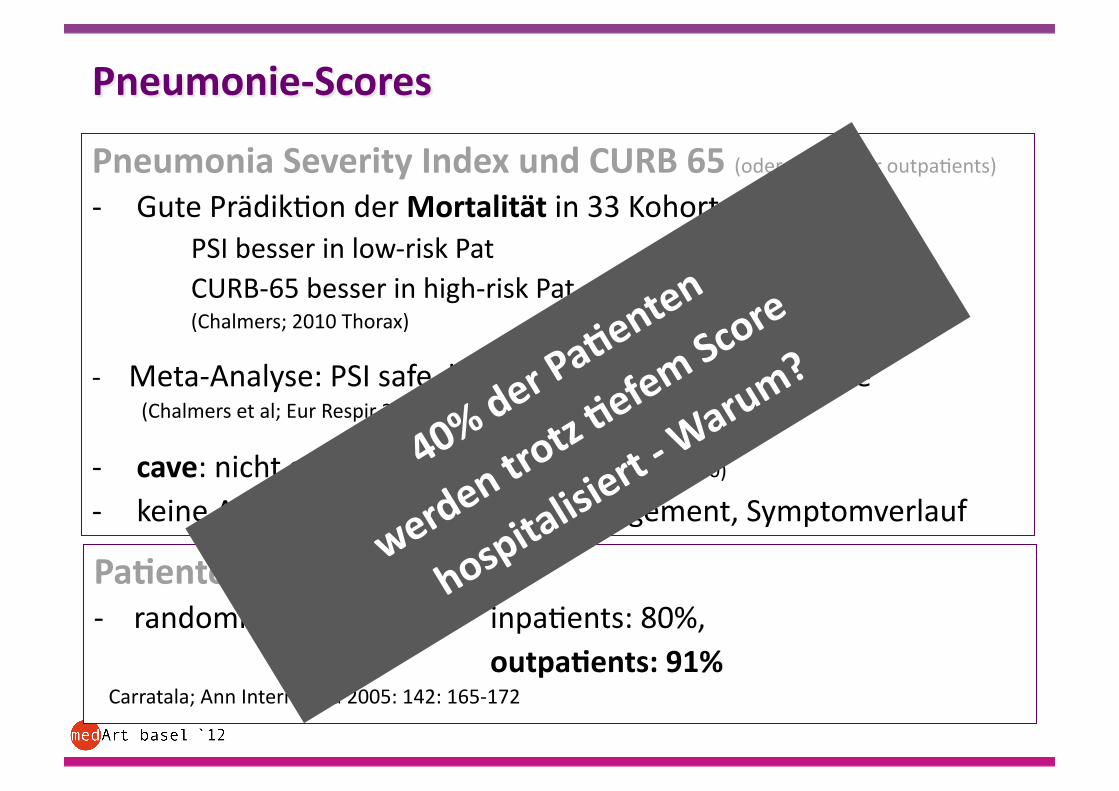
Pneumonia Severity Index und CURB 65 (oder CRB 65 für outpa2ents) -‐ Gute Prädik2on der Mortalität in 33 Kohorten PSI besser in low-‐risk Pat
CURB-‐65 besser in high-‐risk Pat (Chalmers; 2010 Thorax)
-‐ Meta-‐Analyse: PSI safe, keine erhöhte Readmission rate (Chalmers et al; Eur Respir 2011)
-‐ cave: nicht gut <5J / >65Jahre (Chen Thorax, 2010) -‐ keine Aussage über outpa2ent management, Symptomverlauf
Pa,entenzufriedenheit -‐ randomisierte Studie: inpa2ents: 80%,
outpa,ents: 91% Carratala; Ann Intern Med 2005: 142: 165-‐172
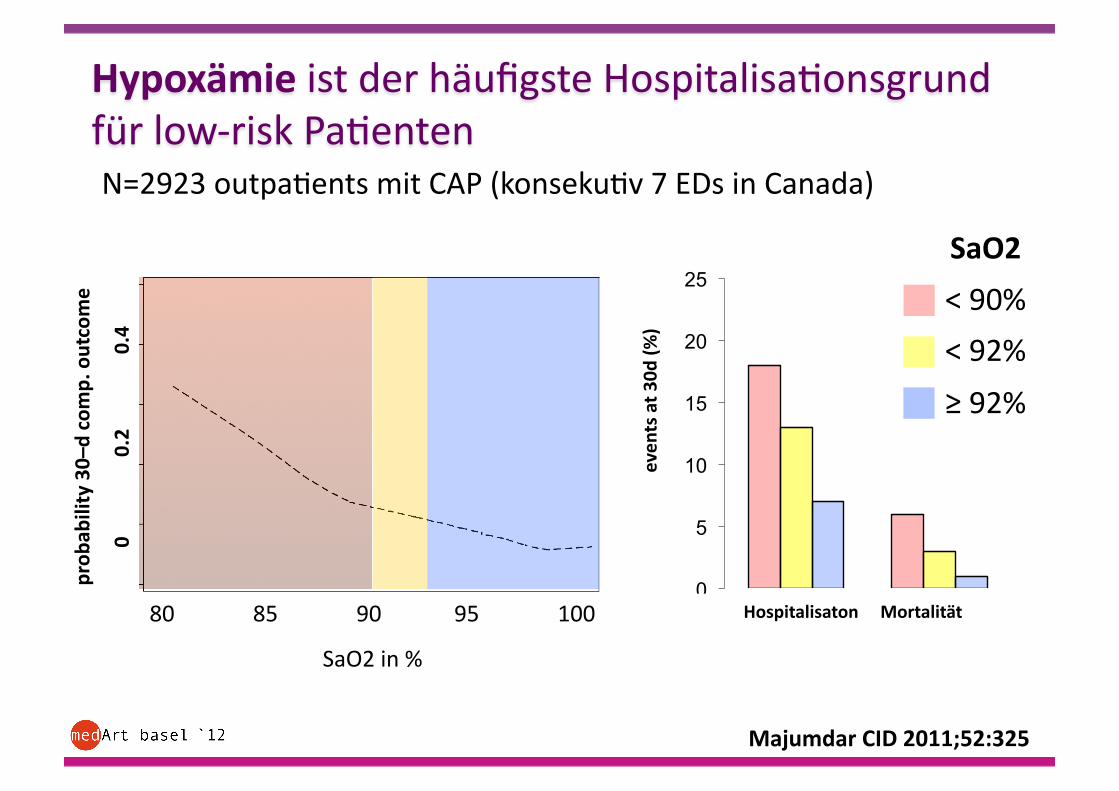
Majumdar CID 2011;52:325
N=2923 outpa2ents mit CAP (konseku2v 7 EDs in Canada)
80 85 90 95 100
SaO2 in %
prob
ability 30–d comp. outcome
0 0.2 0.4
0
5
10
15
20
25
even
ts at 3
0d (%
)
Hospitalisaton Mortalität
SaO2
< 90%
< 92%
≥ 92%
Hypoxämie ist der häufigste Hospitalisa2onsgrund für low-‐risk Pa2enten
Steroide Zytokine ↑ in BAL -‐> Mortality increase
Meduri Chest 1995
Klinische Studien mit Conflic,ng Results
-‐ CAP needing hosp: no benefit Katsumaka Mikami Lung 2007
-‐ CAP: beneficial Garcia-‐Vidal Eur Respir J 2007
-‐ Ven2lated pa2ents: no benefit Mouton Eur Respir J 1999
-‐ Severe CAP: sign. beaer survival Confadonieri M;
Am J Respir Crit Care 2005
-‐ CAP (Rand): kein Benefit Snijders D, Am J Respir Crit Care
Med, 2010
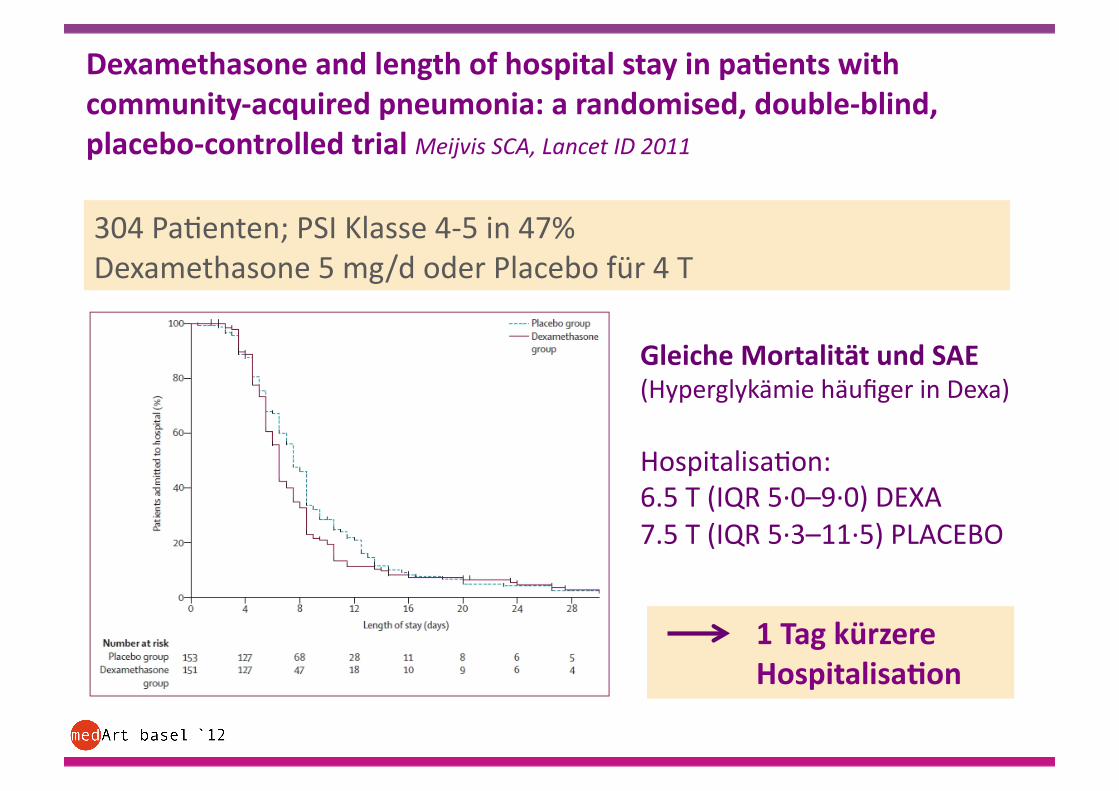
1 Tag kürzere Hospitalisa,on
304 Pa2enten; PSI Klasse 4-‐5 in 47% Dexamethasone 5 mg/d oder Placebo für 4 T
Dexamethasone and length of hospital stay in pa,ents with community-‐acquired pneumonia: a randomised, double-‐blind, placebo-‐controlled trial Meijvis SCA, Lancet ID 2011
Gleiche Mortalität und SAE (Hyperglykämie häufiger in Dexa)
Hospitalisa2on: 6.5 T (IQR 5·∙0–9·∙0) DEXA 7.5 T (IQR 5·∙3–11·∙5) PLACEBO
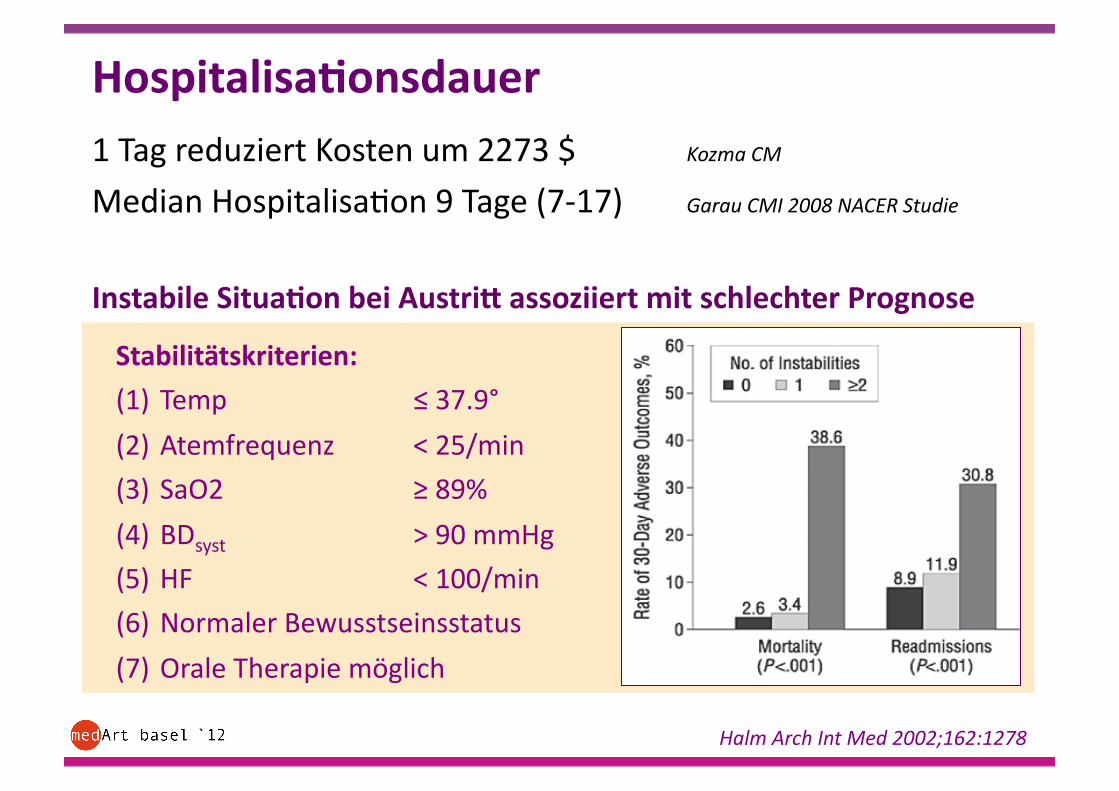
Hospitalisa,onsdauer 1 Tag reduziert Kosten um 2273 $ Kozma CM
Median Hospitalisa2on 9 Tage (7-‐17) Garau CMI 2008 NACER Studie
Instabile Situa,on bei Austril assoziiert mit schlechter Prognose
Halm Arch Int Med 2002;162:1278
Stabilitätskriterien:
(1) Temp ≤ 37.9°
(2) Atemfrequenz < 25/min
(3) SaO2 ≥ 89%
(4) BDsyst > 90 mmHg
(5) HF < 100/min
(6) Normaler Bewusstseinsstatus
(7) Orale Therapie möglich
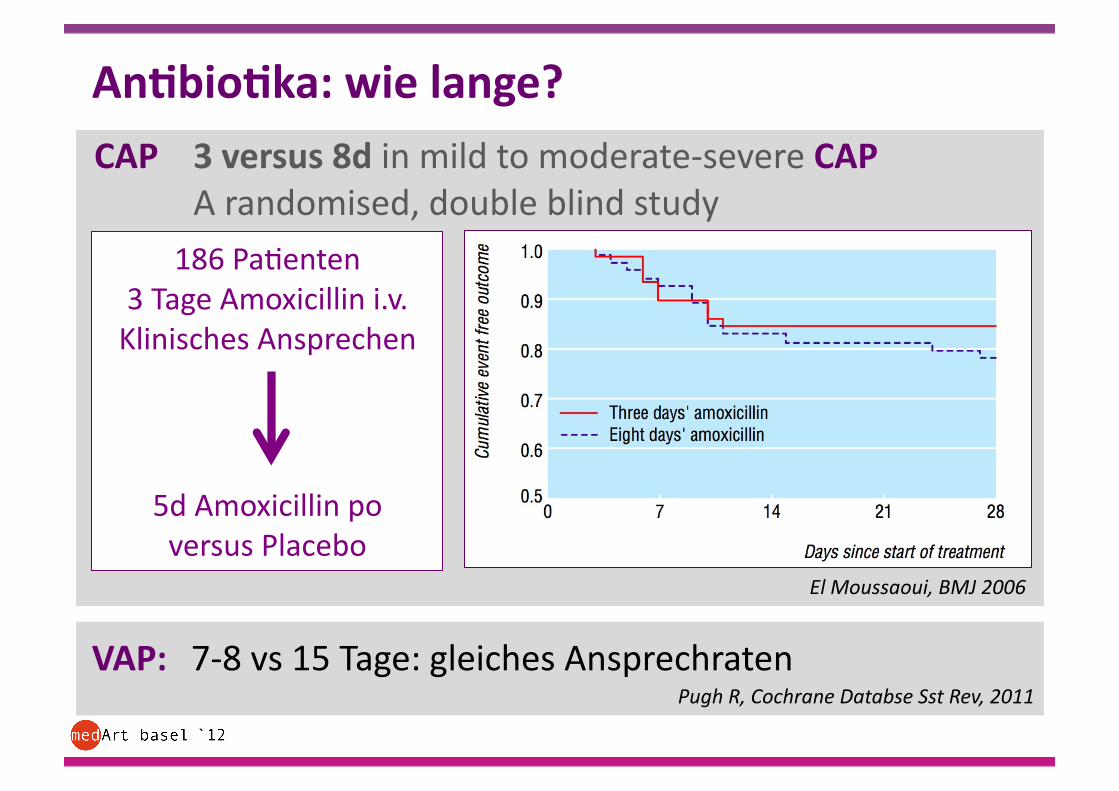
An,bio,ka: wie lange? CAP 3 versus 8d in mild to moderate-‐severe CAP
A randomised, double blind study
VAP: 7-‐8 vs 15 Tage: gleiches Ansprechraten
El Moussaoui, BMJ 2006
186 Pa2enten 3 Tage Amoxicillin i.v. Klinisches Ansprechen
5d Amoxicillin po versus Placebo
Pugh R, Cochrane Databse Sst Rev, 2011
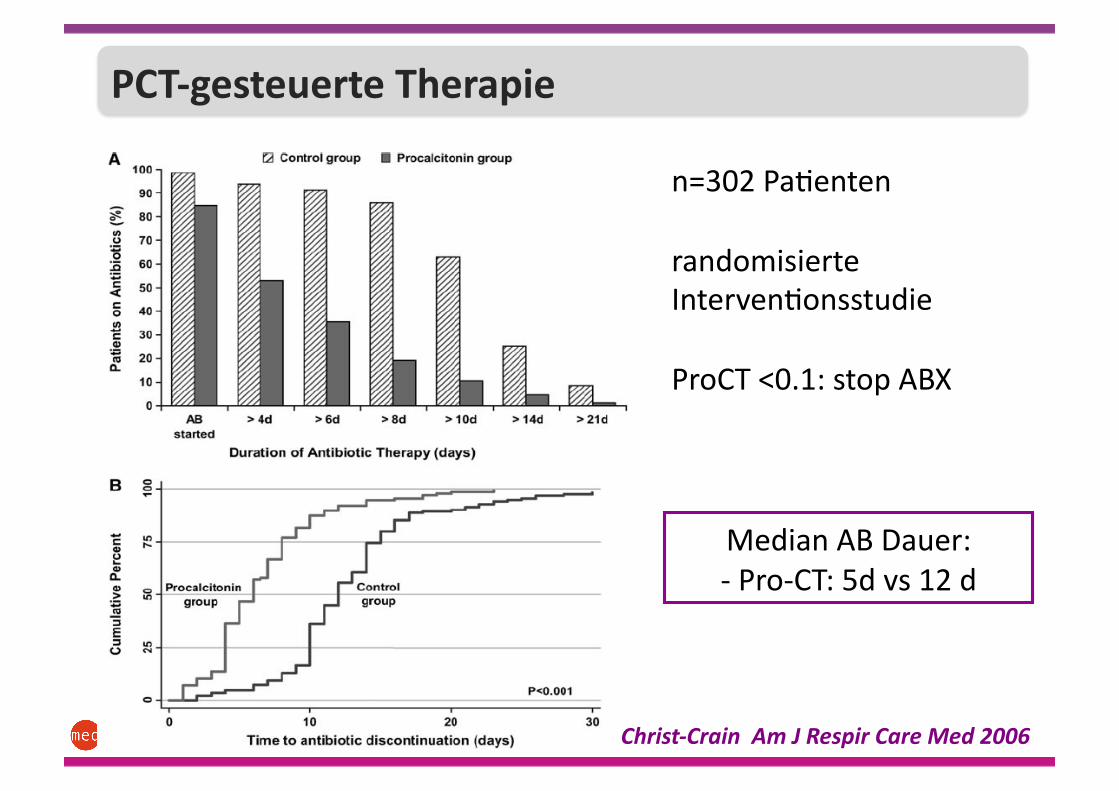
n=302 Pa2enten
randomisierte Interven2onsstudie
ProCT <0.1: stop ABX
Christ-‐Crain Am J Respir Care Med 2006
Median AB Dauer: -‐ Pro-‐CT: 5d vs 12 d
PCT geleitete Therapie PCT-‐gesteuerte Therapie
Mögliche Gründe
-‐ Pharmakokine2k / dynamik?
Unterdosierung (Adipöse Pa2enten?)
Unterschiedliche Lungenpenetra2on von An2bio2ka
-‐ Inokulumgrösse ?
-‐ Inadäquates An2bio2kum
-‐ Polymikrobielle Infek2onen
Roson Ann Intern Med 2004; Boselli et al Crit Care Med. 2005; Rodriguez Crit Care Med 2007 Rello Chest, 2009; 136;832, Johansson Scan Inf Dis, Crit Care 2011; Cohen, Clin Microb Inf 2009;
Menendez, Thorax 2008; O9 Eur Resp. J 2012
Früh !
klinisches Follow-‐up
1Ewig AJRCC 1998;158:1102; 2Minogue Ann Emerg Med 1998;31:376
ambulante Betreuung
nach 24-‐48 Std.
• Verschlechtern bei Nichtansprechen auf Therapie bei meisten Pa2enten innerhalb 24-‐48 Std.1
• Sekundäre Hospitalisa2on selten notwendig;
diese Pa2enten haben erhöhte Mortalität und längere Erholungszeiten2

DANKE
LITERATUR • Guidelines for the management of community acquired pneumonia in adults:
update 2009. Thorax.BMJ 2009
• Physician judgement is a crucial adjunct to pneumonia severity scores in low-‐risk pa2ents G. Choudhury, Eur Respir J 2011; 38: 643–648
• Nursing-‐home-‐acquired pneumonia in Germany: an 8-‐year prospec2ve mul2centre study. Ewig S, Thorax 2012;67:132e138
• Dexamethasone and length of hospital stay in pa2ents with community-‐acquired pneumonia: a randomised, double-‐blind, placebo-‐controlled trial. Meijvis SCA, Lancet Inf Dis 2011; 377: 2023-‐2030
• Oxygen satura2ons less than 92% are associated with major adverse events in outpa2ents with pneumonia: a popula2on-‐based cohort study. Majumdar CID 2011;52:325
• Increasing outpa2ent treatment of mild community-‐acquired pneumonia: systema2c review and meta-‐analysis Chalmers JD , Eur Respir J 2011; 37: 858–864
guidelines: ERS/ECCMID 2005
CAP: Monitorisierung bei ambulantem Mangement
Instruk,on: Pat. Soll sich melden bei:
persis2erend Fieber > 4d Dyspnoe verschlechtert sich Pat. hört auf zu trinken Bewusstsein eingeschränkt bei AB-‐Th: keine klinische Verbesserung nach 3 d falls irgendein Symptom länger als 3 Wo anhält
Follow-‐up nach 2 d bei ≥ 2 der folgenden:
hohes Fieber Tachypnoe Dypnoe relevante Co-‐Morbidität Alter > 65 J





























